Embed Size (px)
Citation preview
Spinal Tuberculosis
Spinal tuberculosisAlwan Hussein Dr
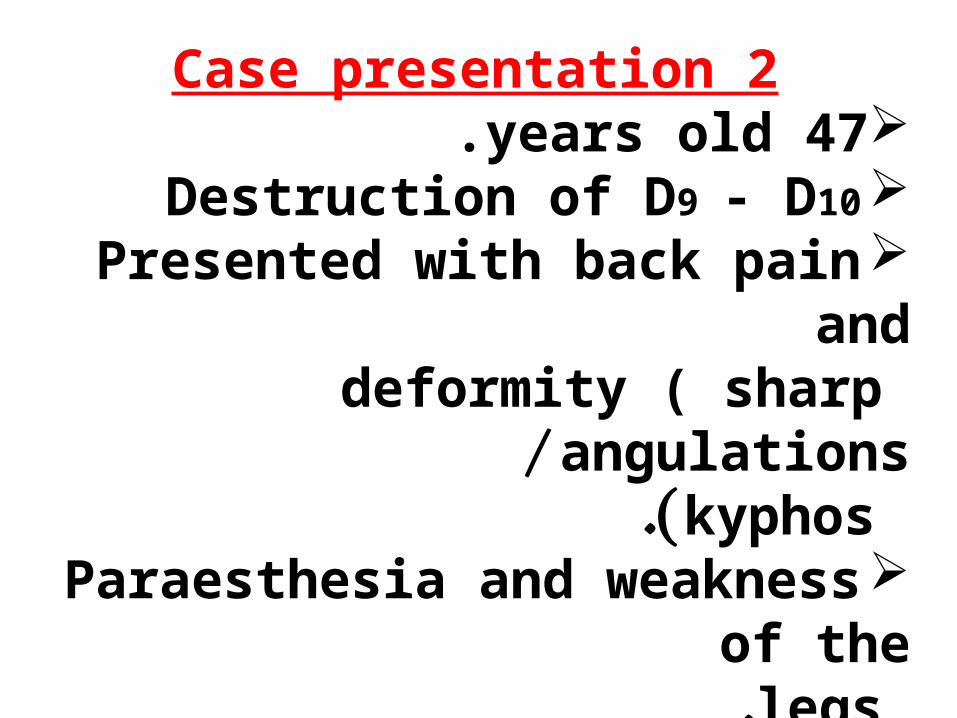
Case presentation 247 years old . Destruction of D9 - D10 Presented with back pain and deformity ( sharp angulations / kyphos .( Paraesthesia and weakness of the legs.
courtesy of MR. DAWOOD S. ALOBIDIF.R.C.S , MSc (ortho.)

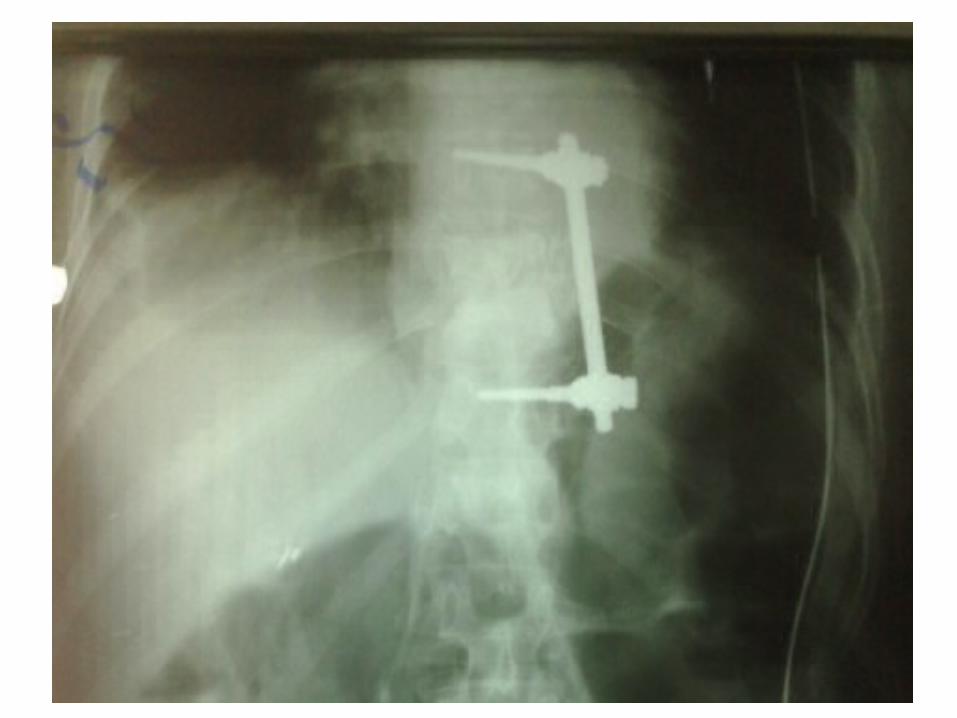
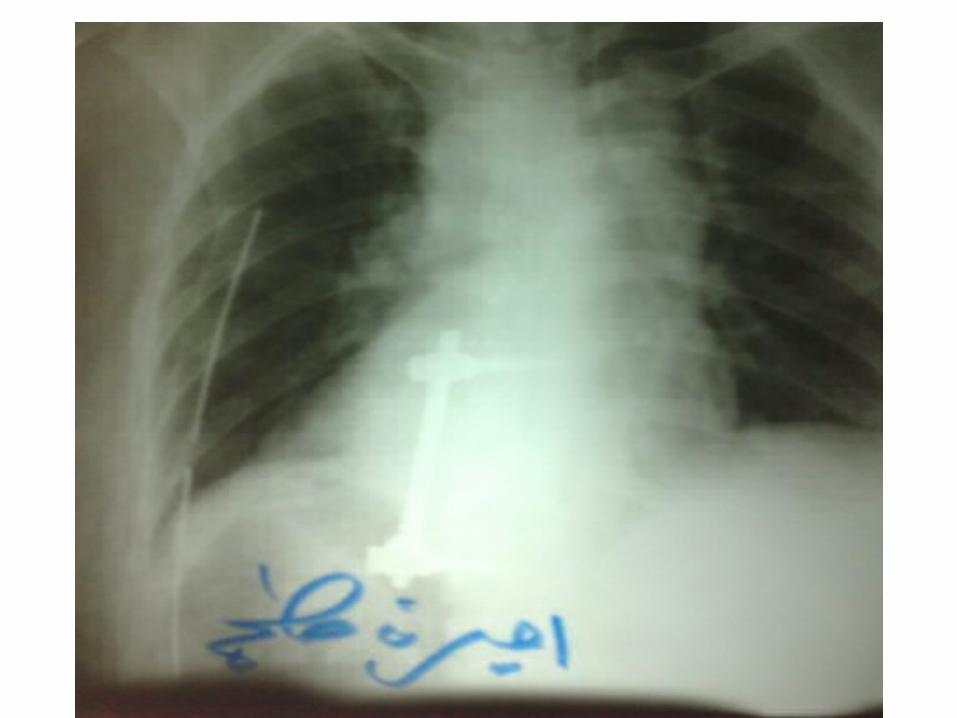
TreatmentAnterior approach .
( Left lateral decubitus position (Corpectomy (removal of all destructed and dead tissue with drainage of abscess( + screws & rod fixation + bone graft (rib graft( .
*tuberculosis of the spine accounts for more than 50% of musculoskeletal tuberculosis.*In the developing countries, the disease commonly afflicts children and young adults and tends to be more aggressive in extent and abscess formation.*Consequently, neurologic complications and spinal deformities are seen frequently*In the developed countries, musculoskeletal tuberculosis is uncommon, but its incidence is reported
to be greater in older individuals *
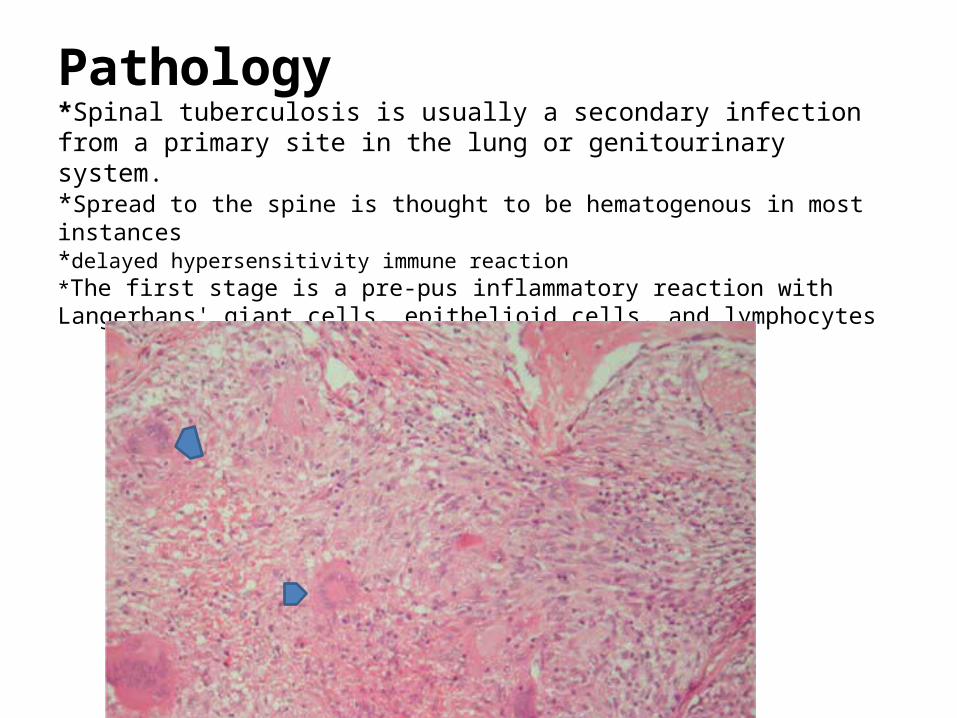
Pathology*Spinal tuberculosis is usually a secondary infection from a primary site in the lung or genitourinary system.*Spread to the spine is thought to be hematogenous in most instances*delayed hypersensitivity immune reaction*The first stage is a pre-pus inflammatory reaction with Langerhans' giant cells, epithelioid cells, and lymphocytes
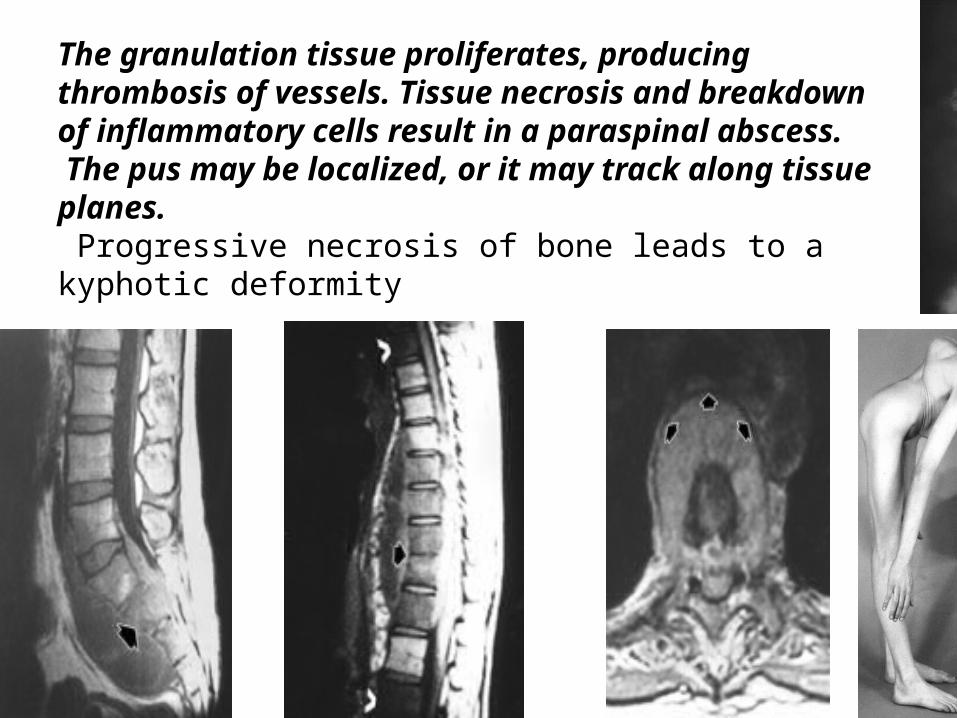
The granulation tissue proliferates, producing thrombosis of vessels. Tissue necrosis and breakdown of inflammatory cells result in a paraspinal abscess. The pus may be localized, or it may track along tissue planes. Progressive necrosis of bone leads to a kyphotic deformity
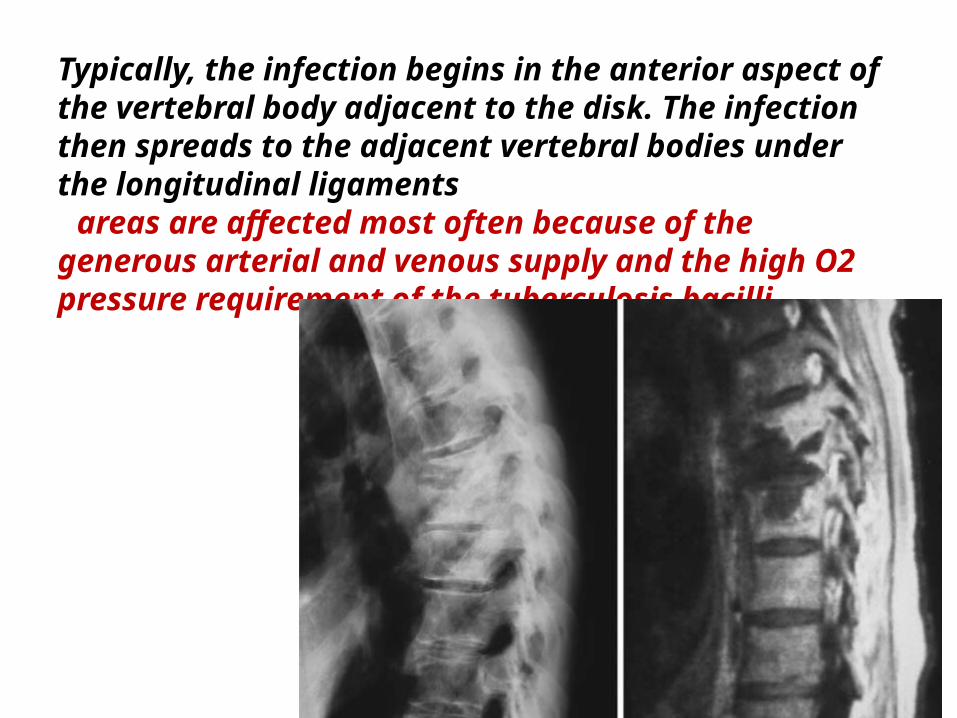
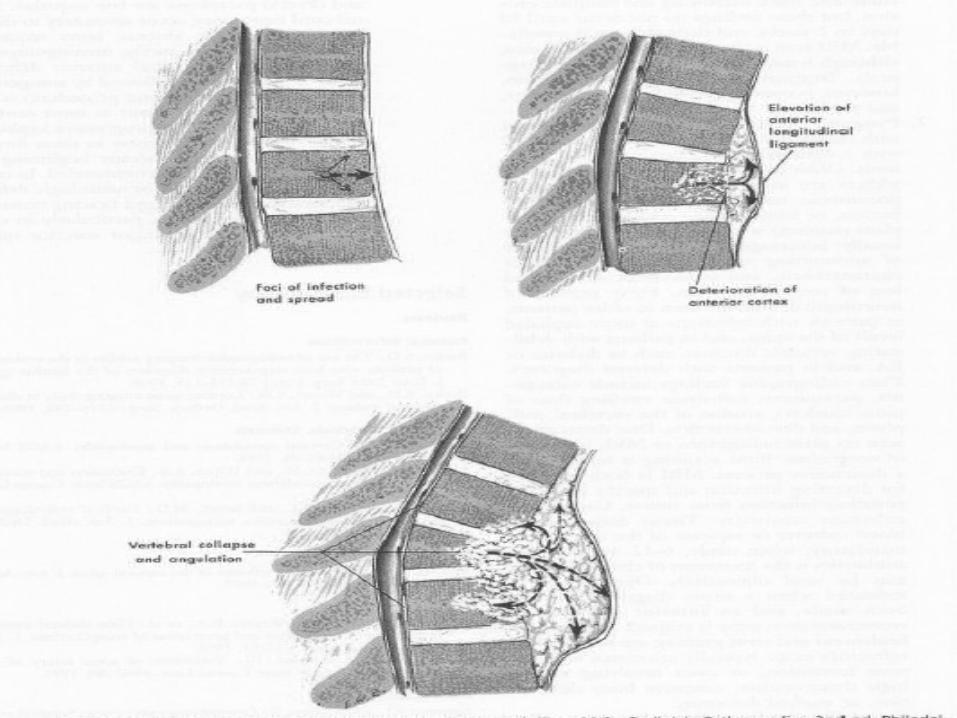
Typically, the infection begins in the anterior aspect of the vertebral body adjacent to the disk. The infection then spreads to the adjacent vertebral bodies under the longitudinal ligaments areas are affected most often because of the generous arterial and venous supply and the high O2 pressure requirement of the tuberculosis bacilli
SiteThe most frequent site of spinal tuberculosis is the thoracolumbar junction . The incidence decreases above and below this level. However, any segment of the spine can be involved
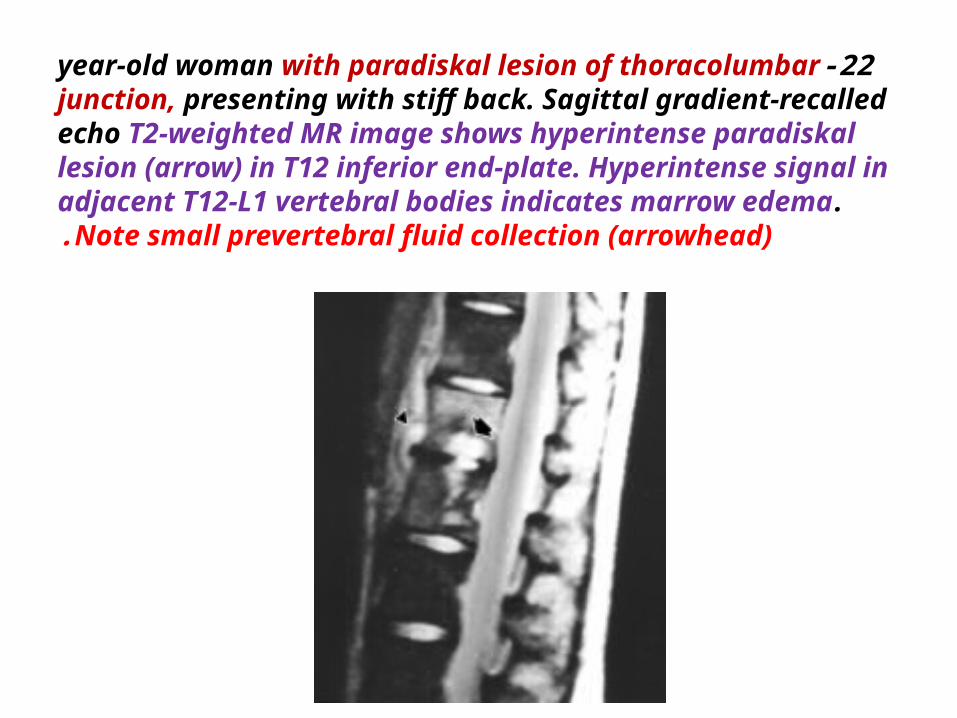
22-year-old woman with paradiskal lesion of thoracolumbar junction, presenting with stiff back. Sagittal gradient-recalled echo T2-weighted MR image shows hyperintense paradiskal lesion (arrow) in T12 inferior end-plate. Hyperintense signal in adjacent T12-L1 vertebral bodies indicates marrow edema. Note small prevertebral fluid collection (arrowhead).
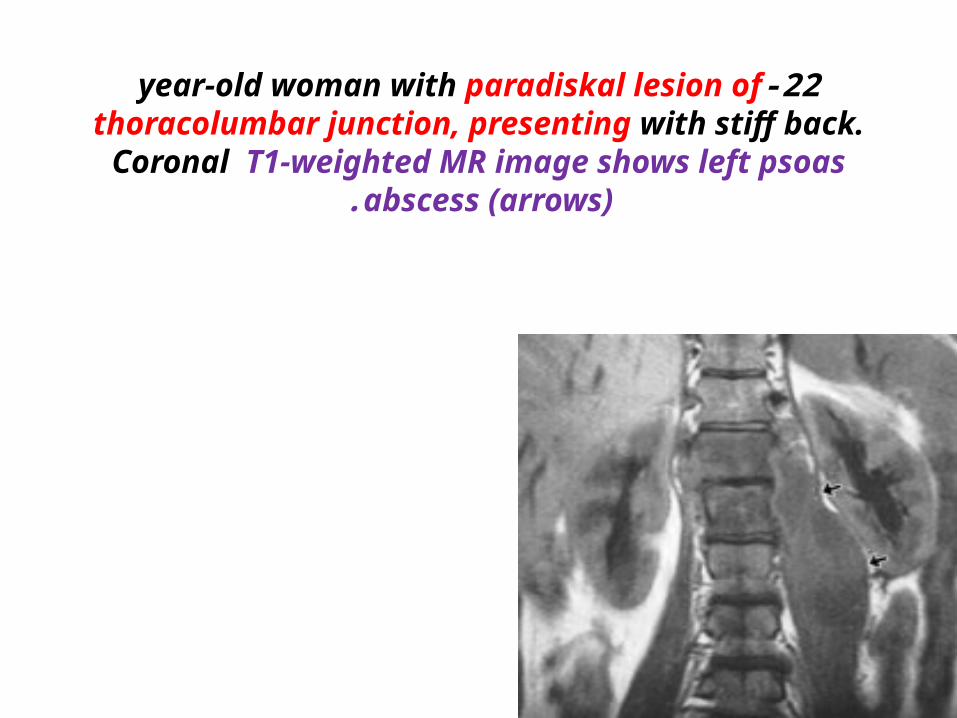
22-year-old woman with paradiskal lesion of thoracolumbar junction, presenting with stiff back. Coronal T1-weighted MR
image shows left psoas abscess (arrows).
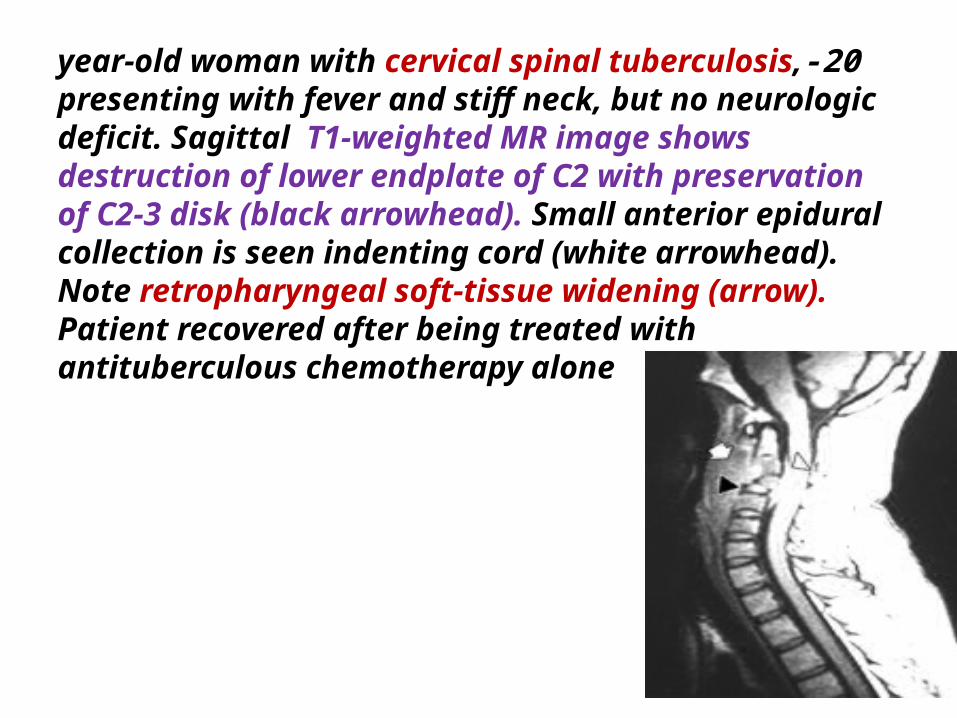
20-year-old woman with cervical spinal tuberculosis, presenting with fever and stiff neck, but no neurologic deficit. Sagittal T1-weighted MR image shows destruction of lower endplate of C2 with preservation of C2-3 disk (black arrowhead). Small anterior epidural collection is seen indenting cord (white arrowhead). Note retropharyngeal soft-tissue widening (arrow). Patient recovered after being treated with antituberculous chemotherapy alone
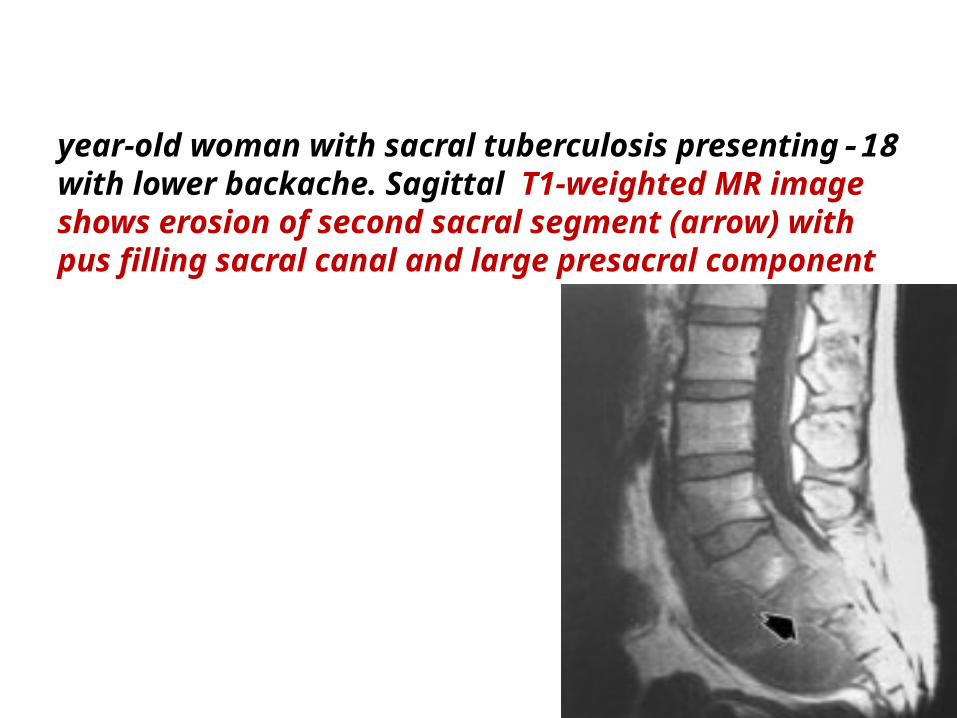
18-year-old woman with sacral tuberculosis presenting with lower backache. Sagittal T1-weighted MR image shows erosion of second sacral segment (arrow) with pus filling sacral canal and large presacral component
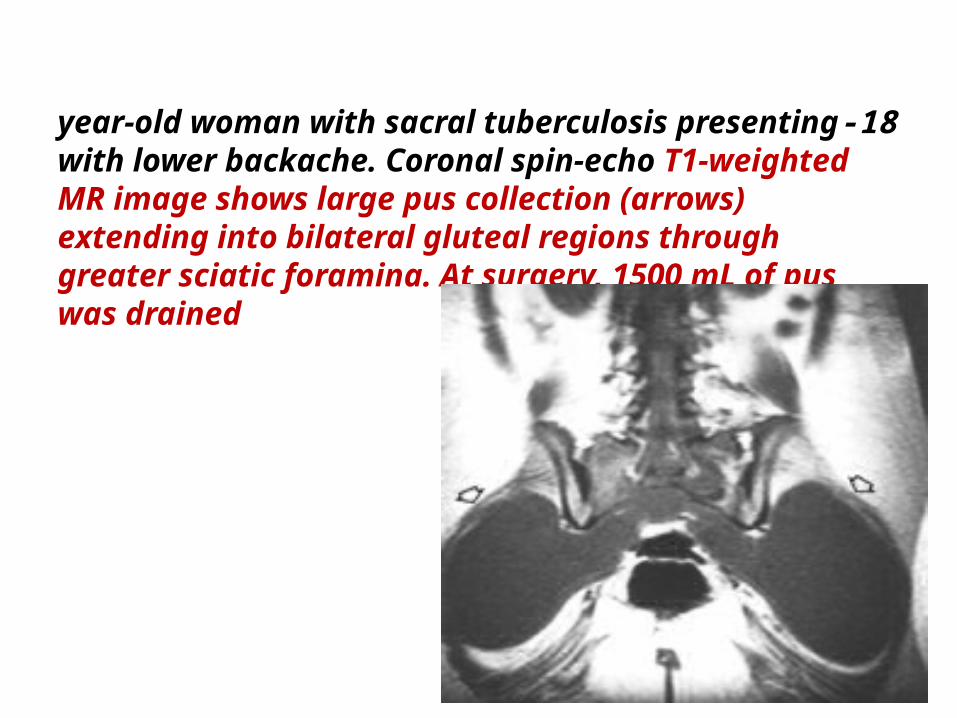
18-year-old woman with sacral tuberculosis presenting with lower backache. Coronal spin-echo T1-weighted MR image shows large pus collection (arrows) extending into bilateral gluteal regions through greater sciatic foramina. At surgery, 1500 mL of pus was drained
Patterns of Vertebral
Involvement
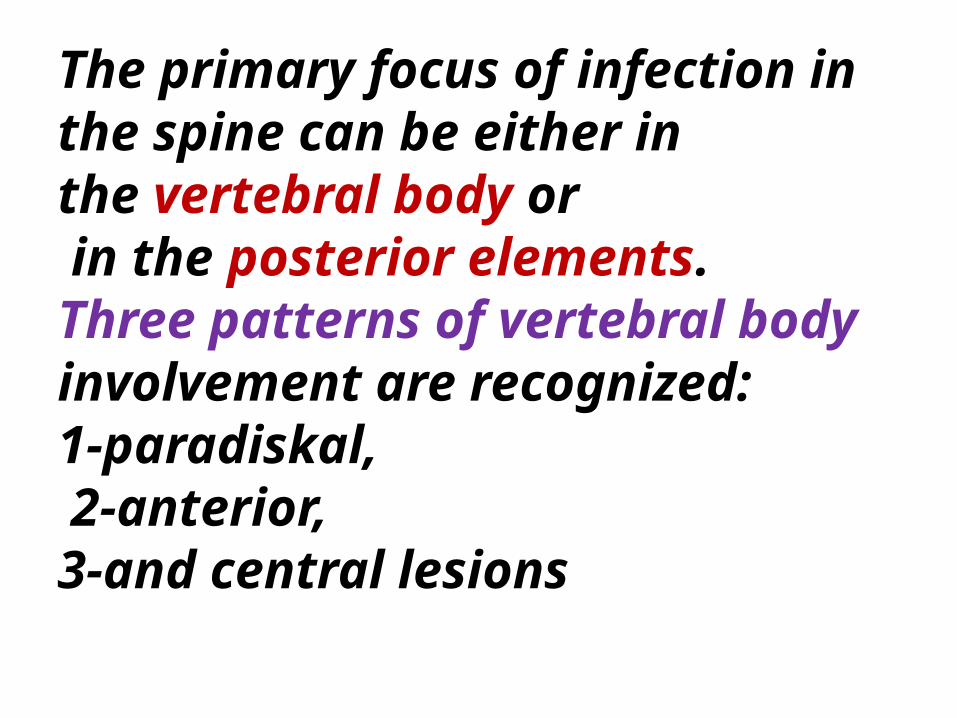
The primary focus of infection in the spine can be either in the vertebral body or in the posterior elements. Three patterns of vertebral body involvement are recognized: 1-paradiskal, 2-anterior, 3-and central lesions
Paradiskal LesionsA paradiskal lesion is adjacent to the intervertebral disk leading to a narrowing of the disk space . The disk space narrowing is caused either by 1-destruction of subchondral bone with subsequent herniation of the disk into the vertebral body 2-or by direct involvement of the disk . This is the most common pattern of spinal tuberculosis. MR imaging shows low signal on T1-weighted images and high signal on T2-weighted images in the endplate, narrowing of the disk, and large paraspinal and sometimes epidural abscesses
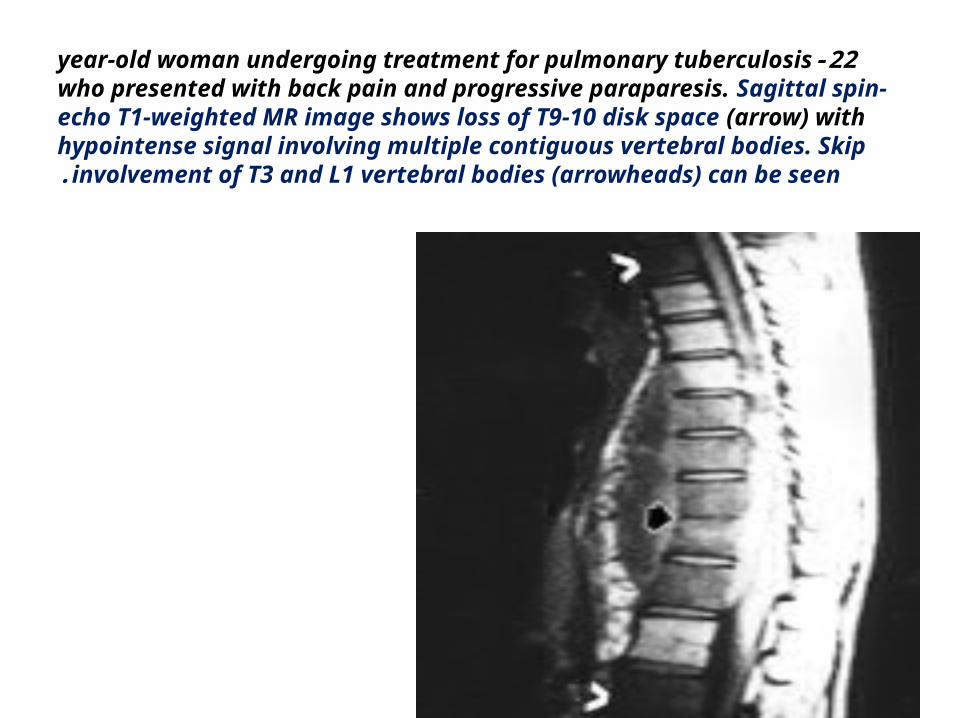
22-year-old woman undergoing treatment for pulmonary tuberculosis who presented with back pain and progressive paraparesis. Sagittal spin-echo T1-weighted MR image shows loss of T9-10 disk space (arrow) with hypointense signal involving multiple contiguous vertebral bodies. Skip involvement of T3 and L1 vertebral bodies (arrowheads) can be seen.
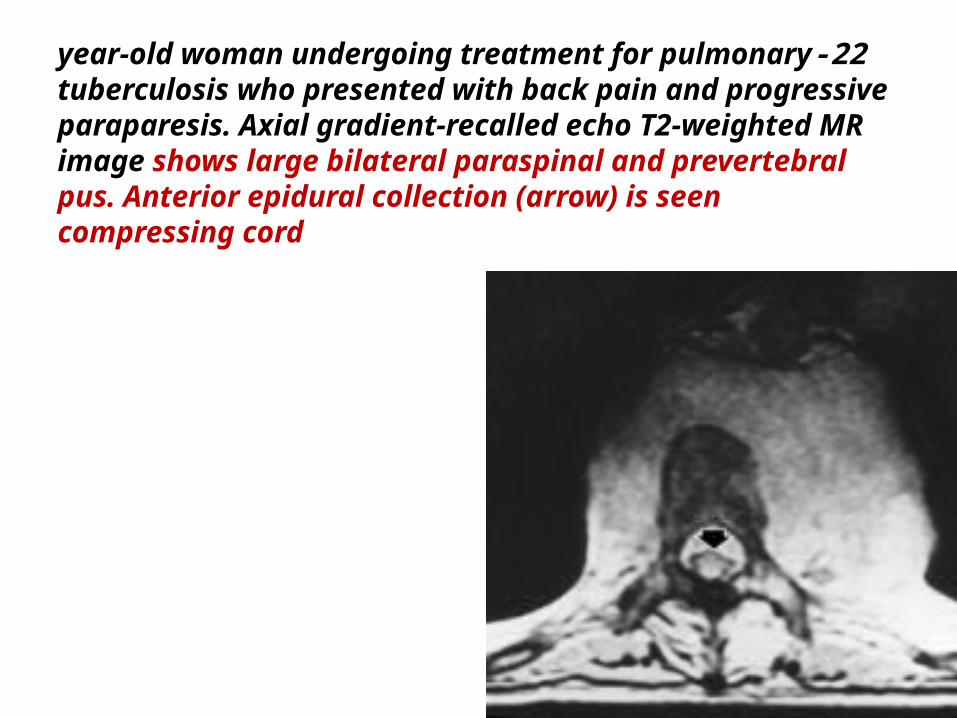
22-year-old woman undergoing treatment for pulmonary tuberculosis who presented with back pain and progressive paraparesis. Axial gradient-recalled echo T2-weighted MR image shows large bilateral paraspinal and prevertebral pus. Anterior epidural collection (arrow) is seen compressing cord
Anterior Lesions*The anterior type is a subperiosteal lesion under the anterior longitudinal ligament . *Pus spreads over multiple vertebral segments, stripping the *periosteum and anterior longitudinal ligament from the anterior surface of the vertebral bodies.*The periosteal stripping renders the vertebrae avascular and susceptible to infection. Both pressure and ischemia combine to produce anterior scalloping . MR imaging shows the subligamentous abscess, preservation of the disks, and abnormal signal involving multiple vertebral segments representing vertebral tuberculous osteomyelitis.
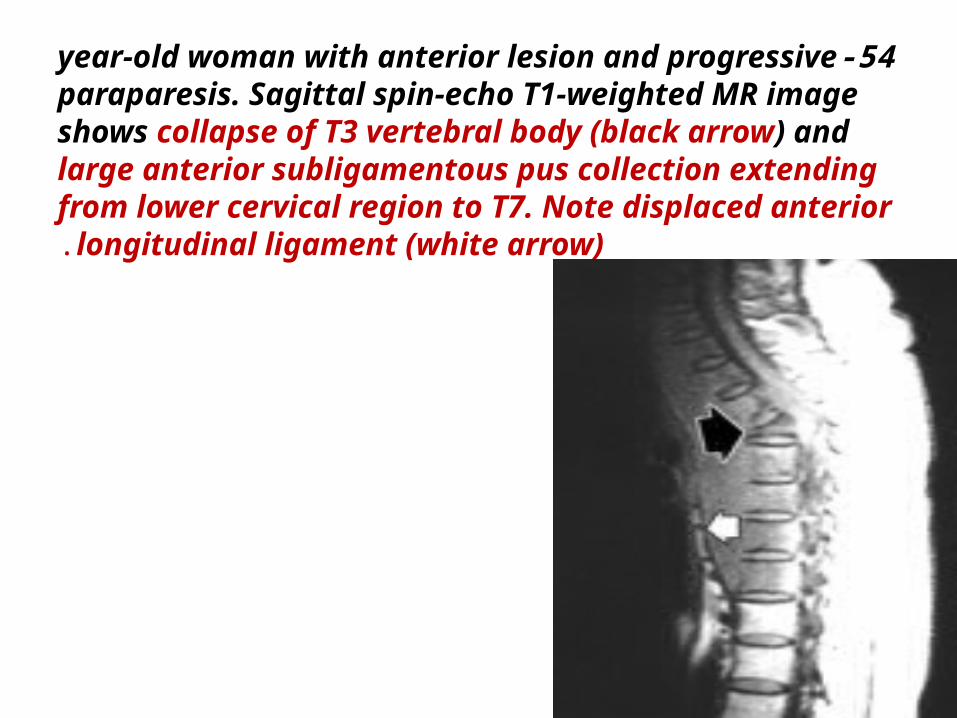
54-year-old woman with anterior lesion and progressive paraparesis. Sagittal spin-echo T1-weighted MR image shows collapse of T3 vertebral body (black arrow) and large anterior subligamentous pus collection extending from lower cervical region to T7. Note displaced anterior longitudinal ligament (white arrow).
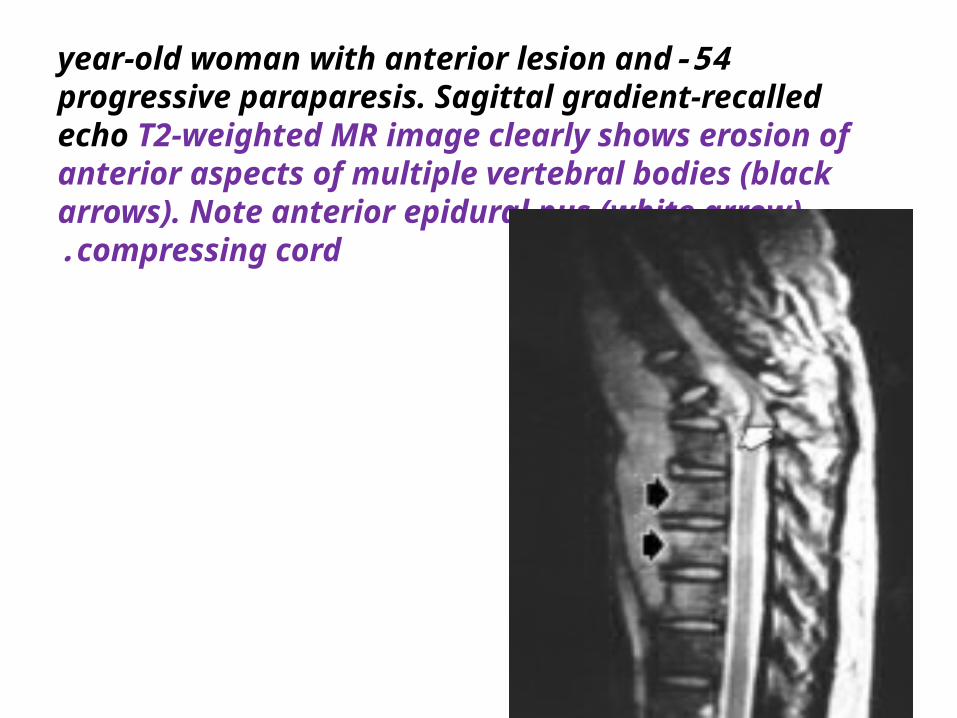
54-year-old woman with anterior lesion and progressive paraparesis. Sagittal gradient-recalled echo T2-weighted MR image clearly shows erosion of anterior aspects of multiple vertebral bodies (black arrows). Note anterior epidural pus (white arrow) compressing cord.
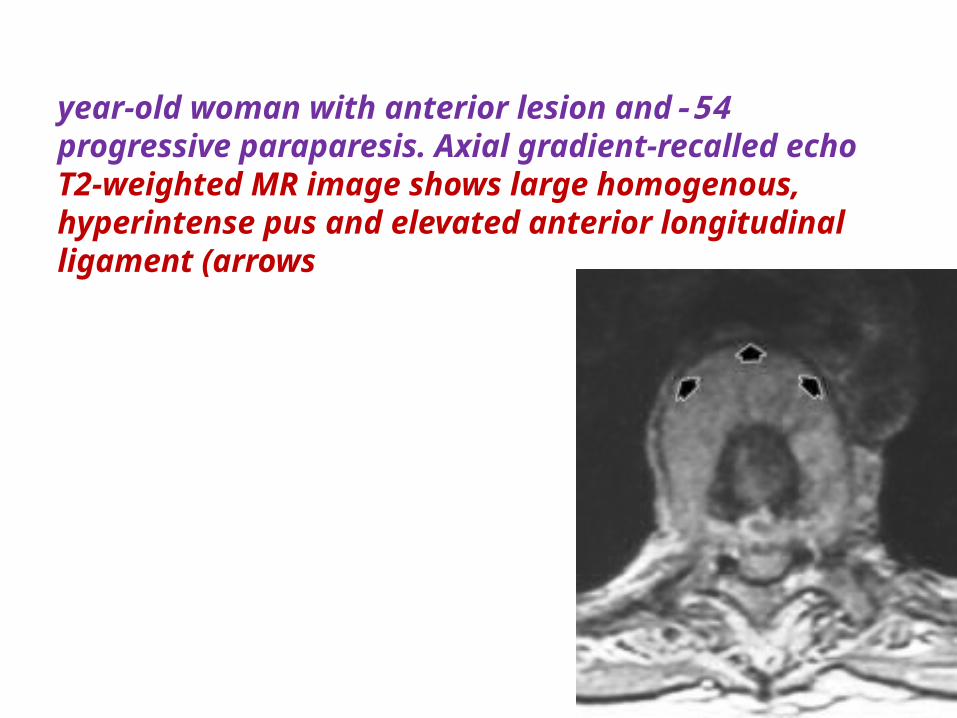
54-year-old woman with anterior lesion and progressive paraparesis. Axial gradient-recalled echo T2-weighted MR image shows large homogenous, hyperintense pus and elevated anterior longitudinal ligament (arrows
Central LesionsThe central lesion is centered on the vertebral body. The disk is not involved . Vertebral collapse can occur, producing a vertebra plana appearance . MR imaging shows a signal abnormality of the vertebral body with preservation of the disk. The appearance is indistinguishable from that of lymphoma or metastasis
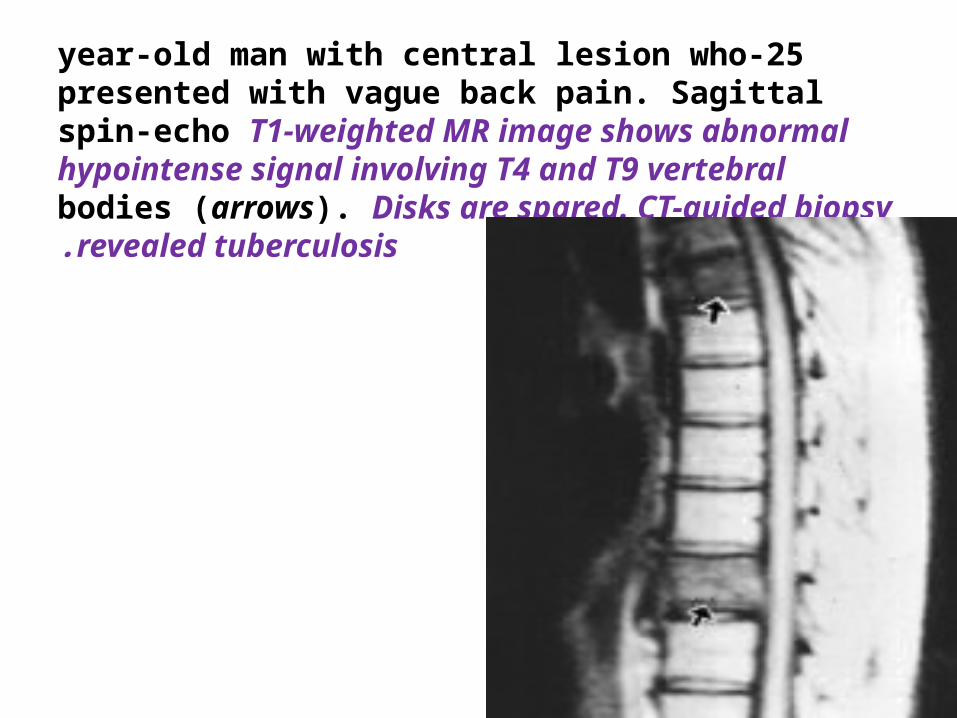
25-year-old man with central lesion who presented with vague back pain. Sagittal spin-echo T1-weighted MR image shows abnormal hypointense signal involving T4 and T9 vertebral bodies (arrows). Disks are spared. CT-guided biopsy revealed tuberculosis.
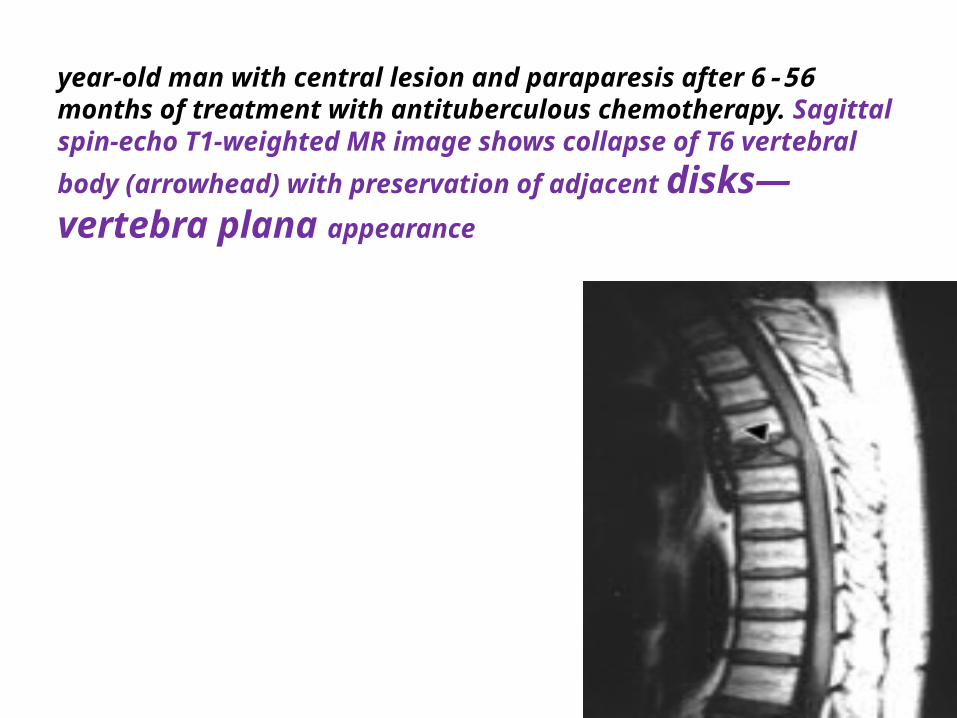
56-year-old man with central lesion and paraparesis after 6 months of treatment with antituberculous chemotherapy. Sagittal spin-echo T1-weighted MR image shows collapse of T6 vertebral body (arrowhead) with
preservation of adjacent disks—vertebra plana appearance
Posterior ElementTuberculous involvement of the posterior elements is rare . MR imaging shows evidence of bone erosion and the associated abscess
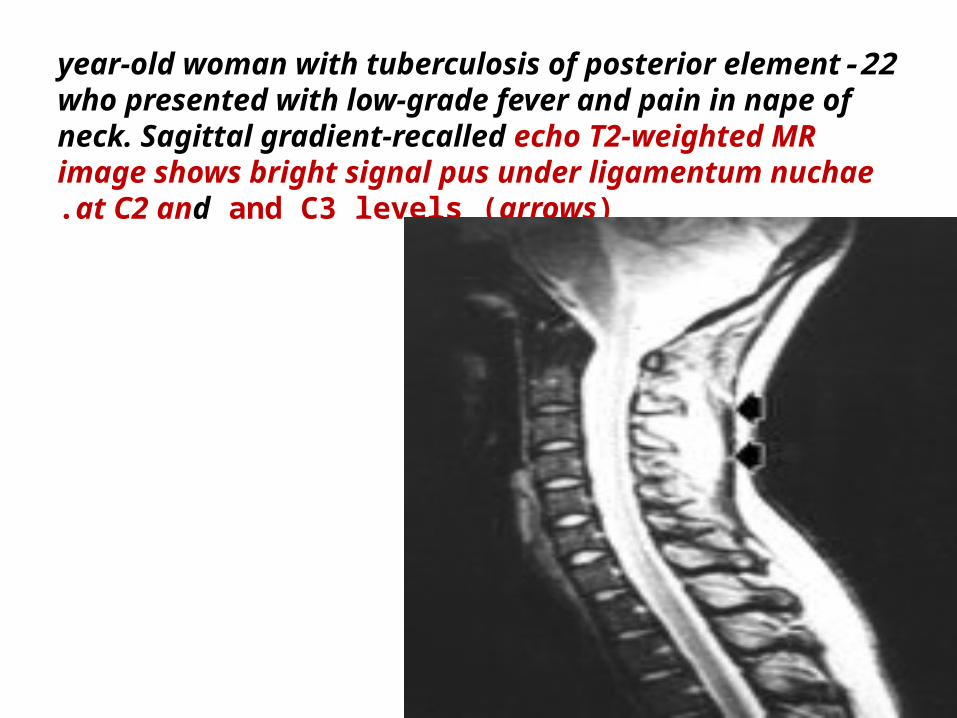
22-year-old woman with tuberculosis of posterior element who presented with low-grade fever and pain in nape of neck. Sagittal gradient-recalled echo T2-weighted MR image shows bright signal pus under ligamentum nuchae at C2 and and C3 levels (arrows).
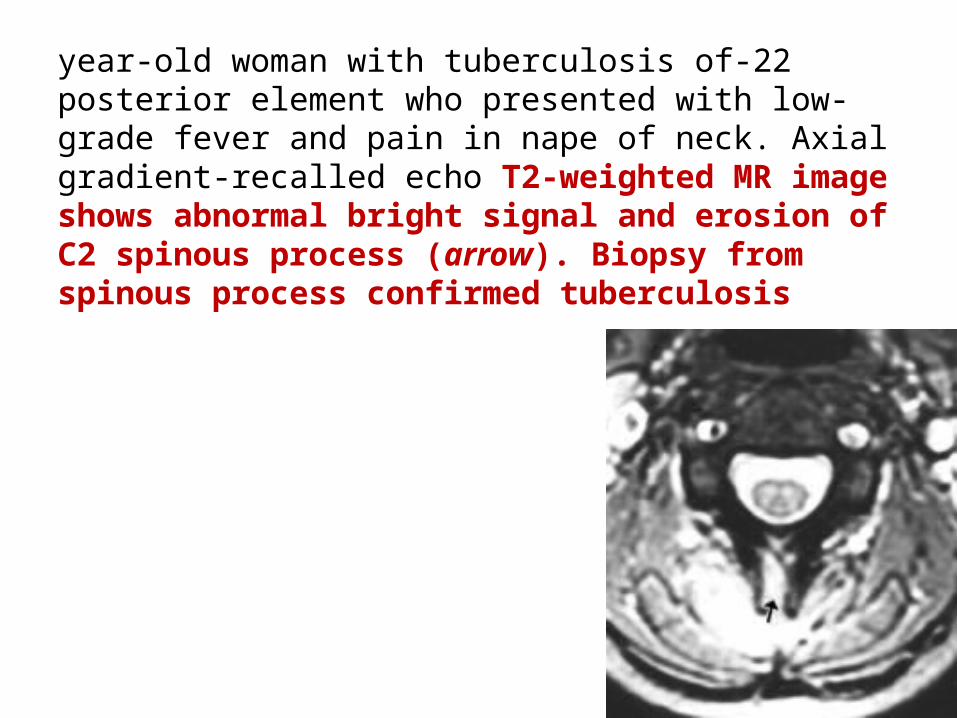
22-year-old woman with tuberculosis of posterior element who presented with low-grade fever and pain in nape of neck. Axial gradient-recalled echo T2-weighted MR image shows abnormal bright signal and erosion of C2 spinous process (arrow). Biopsy from spinous process confirmed tuberculosis
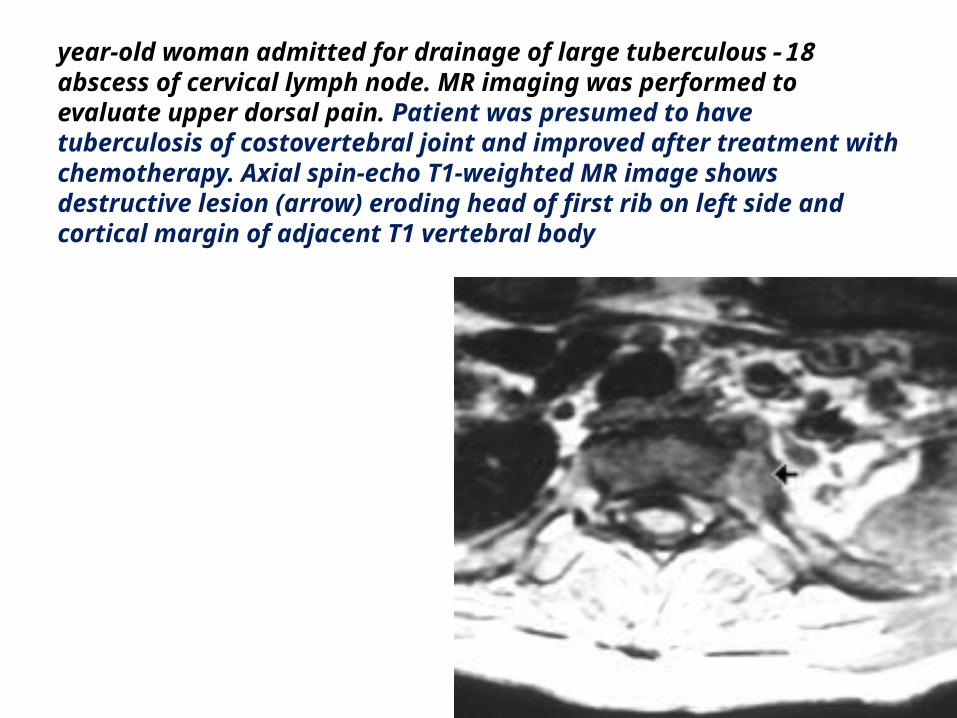
18-year-old woman admitted for drainage of large tuberculous abscess of cervical lymph node. MR imaging was performed to evaluate upper dorsal pain. Patient was presumed to have tuberculosis of costovertebral joint and improved after treatment with chemotherapy. Axial spin-echo T1-weighted MR image shows destructive lesion (arrow) eroding head of first rib on left side and cortical margin of adjacent T1 vertebral body
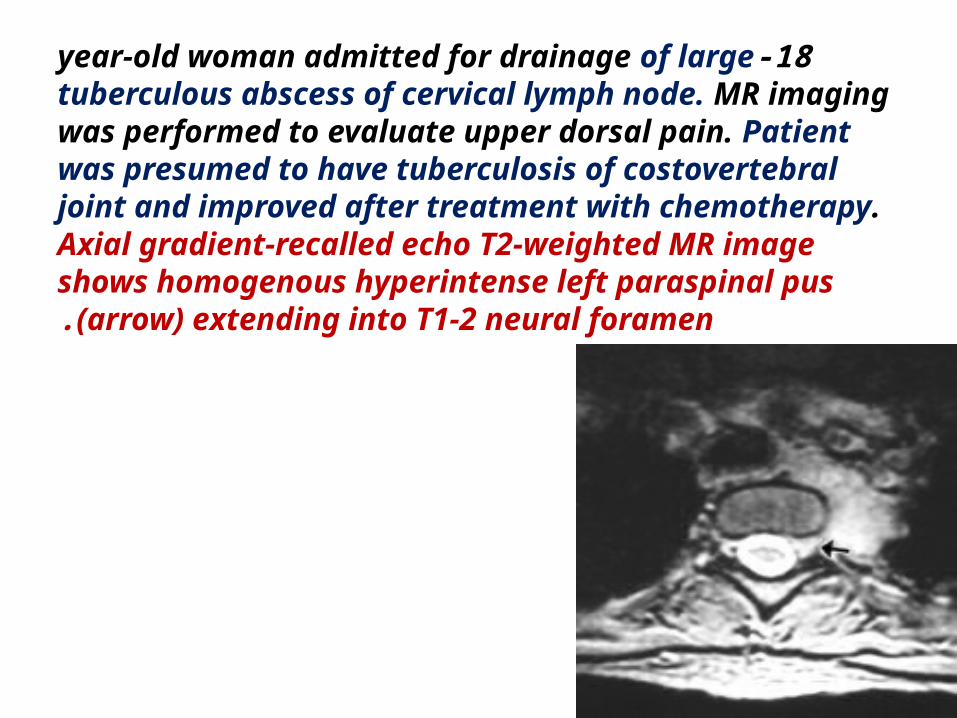
18-year-old woman admitted for drainage of large tuberculous abscess of cervical lymph node. MR imaging was performed to evaluate upper dorsal pain. Patient was presumed to have tuberculosis of costovertebral joint and improved after treatment with chemotherapy. Axial gradient-recalled echo T2-weighted MR image shows homogenous hyperintense left paraspinal pus (arrow) extending into T1-2 neural foramen.
Complications of the Tuberculous Spine*Paraplegia and sometimes quadriplegia are serious complications of the tuberculous spine seen in approximately 10% of patients . 1-Copious epidural pus and granulation tissue alone2- or in combination with vertebral collapse, subluxation, or dislocation ( produce cord compression.
Rarely, the pus penetrates the dura resulting in severe meningomyelitis
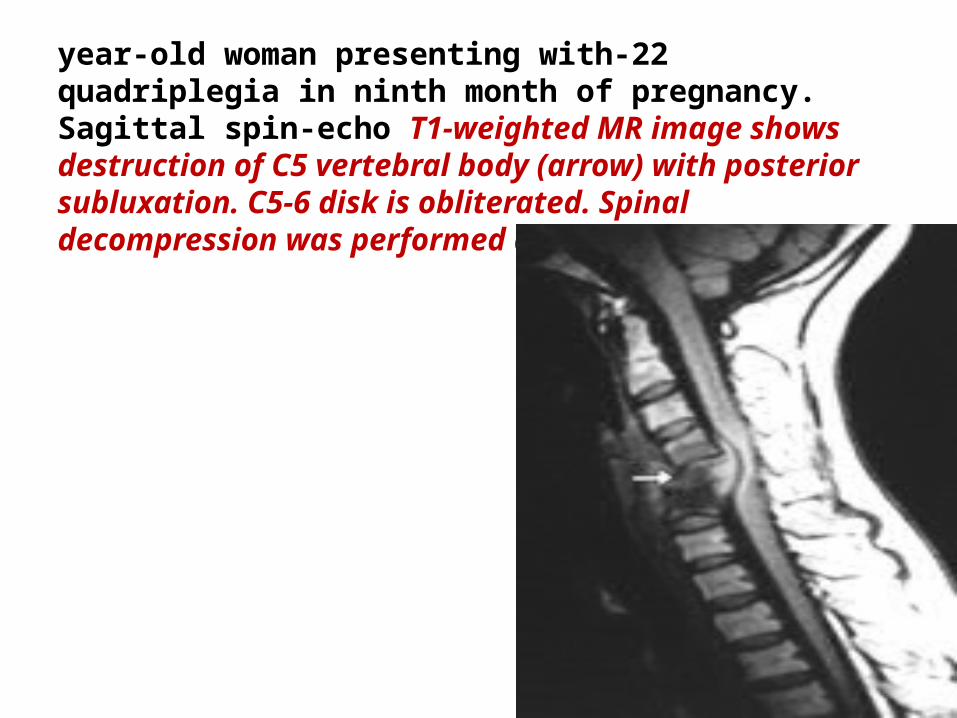
22-year-old woman presenting with quadriplegia in ninth month of pregnancy. Sagittal spin-echo T1-weighted MR image shows destruction of C5 vertebral body (arrow) with posterior subluxation. C5-6 disk is obliterated. Spinal decompression was performed after induction of labor
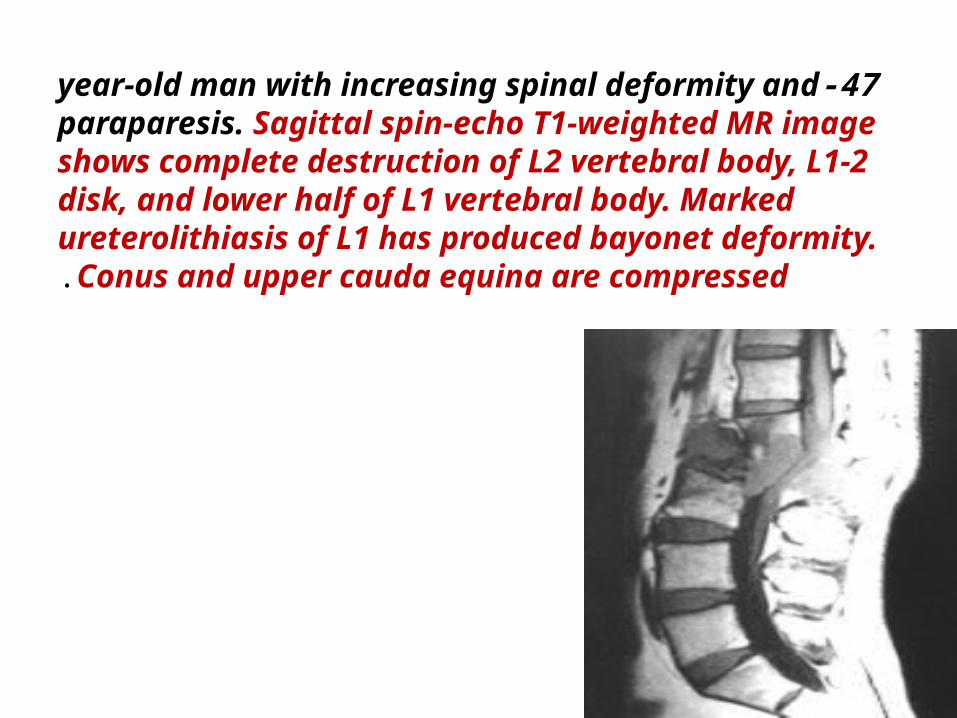
47-year-old man with increasing spinal deformity and paraparesis. Sagittal spin-echo T1-weighted MR image shows complete destruction of L2 vertebral body, L1-2 disk, and lower half of L1 vertebral body. Marked ureterolithiasis of L1 has produced bayonet deformity. Conus and upper cauda equina are compressed.
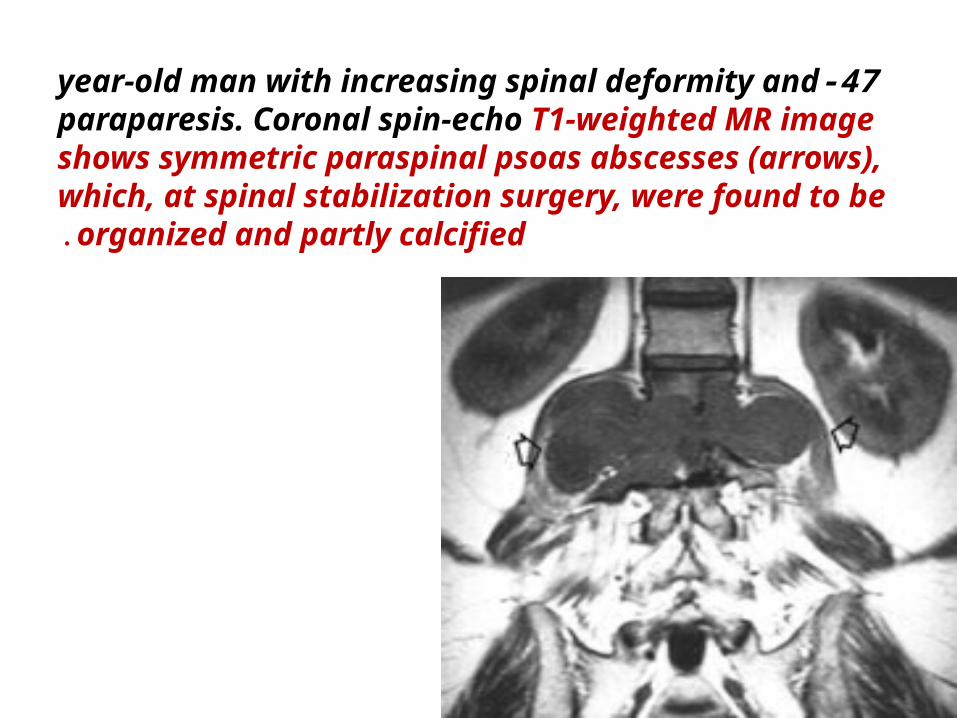
47-year-old man with increasing spinal deformity and paraparesis. Coronal spin-echo T1-weighted MR image shows symmetric paraspinal psoas abscesses (arrows), which, at spinal stabilization surgery, were found to be organized and partly calcified.
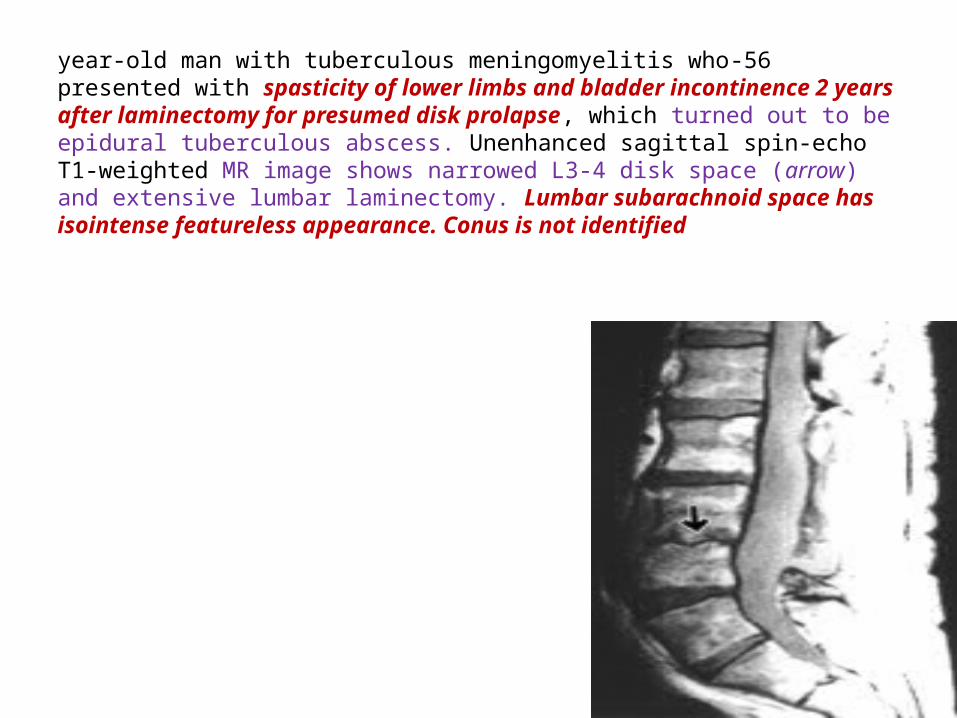
56-year-old man with tuberculous meningomyelitis who presented with spasticity of lower limbs and bladder incontinence 2 years after laminectomy for presumed disk prolapse, which turned out to be epidural tuberculous abscess. Unenhanced sagittal spin-echo T1-weighted MR image shows narrowed L3-4 disk space (arrow) and extensive lumbar laminectomy. Lumbar subarachnoid space has isointense featureless appearance. Conus is not identified
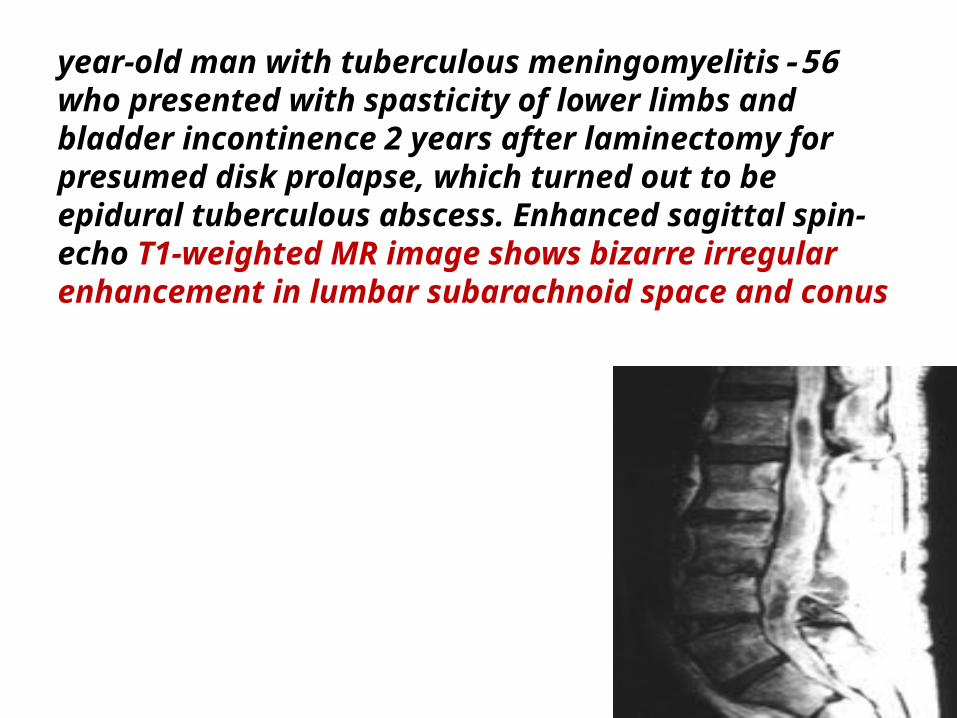
56-year-old man with tuberculous meningomyelitis who presented with spasticity of lower limbs and bladder incontinence 2 years after laminectomy for presumed disk prolapse, which turned out to be epidural tuberculous abscess. Enhanced sagittal spin-echo T1-weighted MR image shows bizarre irregular enhancement in lumbar subarachnoid space and conus
ConclusionThe differential diagnosis of the tuberculous spine includes * pyogenic * and fungal infections, *sarcoidosis, *metastasis, and lymphoma. No pathognomonic imaging signs allow tuberculosis to be readily distinguished from other conditions.Orthopedic principles----------------------------------- 1-Typically, infectious spondylitis is characterized by involvement of the intervertebral disk. 2-A history of chronicity and slow progression is suggestive of tuberculosis. 3-Moreover, inflammatory collections tend to be larger in tuberculosis than in pyogenic spondylitis. 4-In the central and posterior element forms of tuberculosis, only biopsy can achieve a provide diagnosis
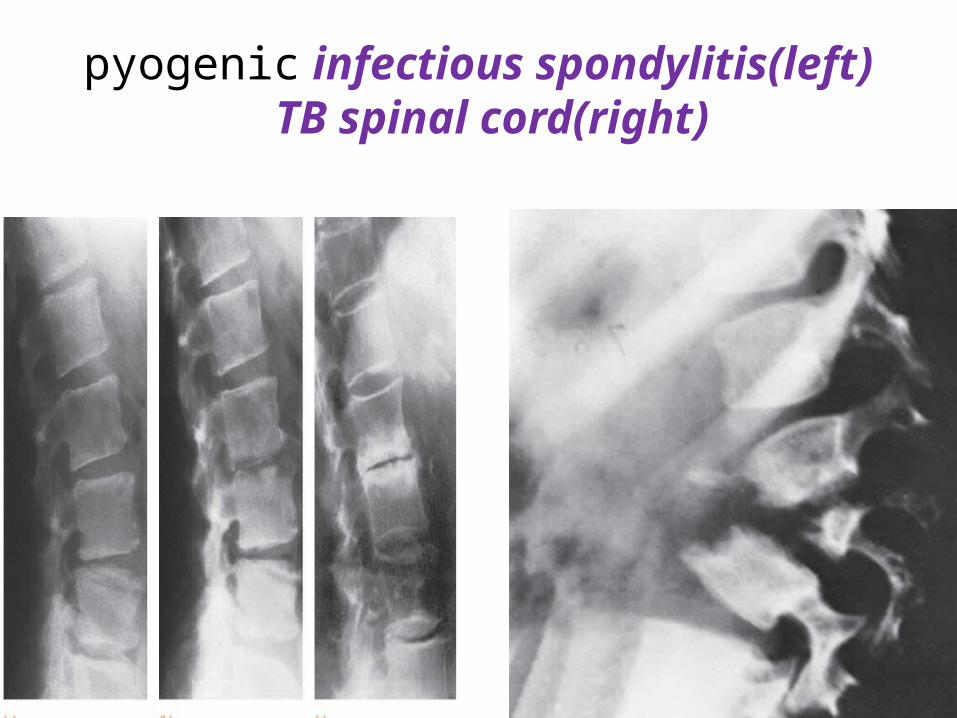
pyogenic infectious spondylitis(left)TB spinal cord(right)
What about MR imaging role? 1-MR imaging is sensitive for detecting vertebral osteomyelitis and is therefore the imaging technique of choice in spinal infections . 2-In spinal tuberculosis, the superior contrast resolution of MR imaging is useful for showing contiguous vertebral involvement, skip lesions, and paraspinal collections.3- MR imaging provides critical information about the spinal cord and the extent of the epidural pus
in patients presenting with neurologic deficits ..
Familiarity with the spectrum of MR findings in tuberculosis spondylitis, especially in a high-risk patient population, can prevent a delay in diagnosis and may limit the morbidity that can be caused by this aggressive but curable infectious disease

Treatment
begins with chemotherapy and generalmeasures to improve the patient’s physiologic state.Studies undertaken by the Medical Research Council of Great Britain found that outpatient chemotherapy is highly effective for “uncomplicated” spinal tuberculosis(90 %,)

2RHZE/4RH

Prof.mohammed Reza M.D chicago
Indication for surgery
I/ The development of neurological deficit is a
strong indicationfor surgical treatment
II/ The indications for surgery in the
absence of neurologicalsymptoms
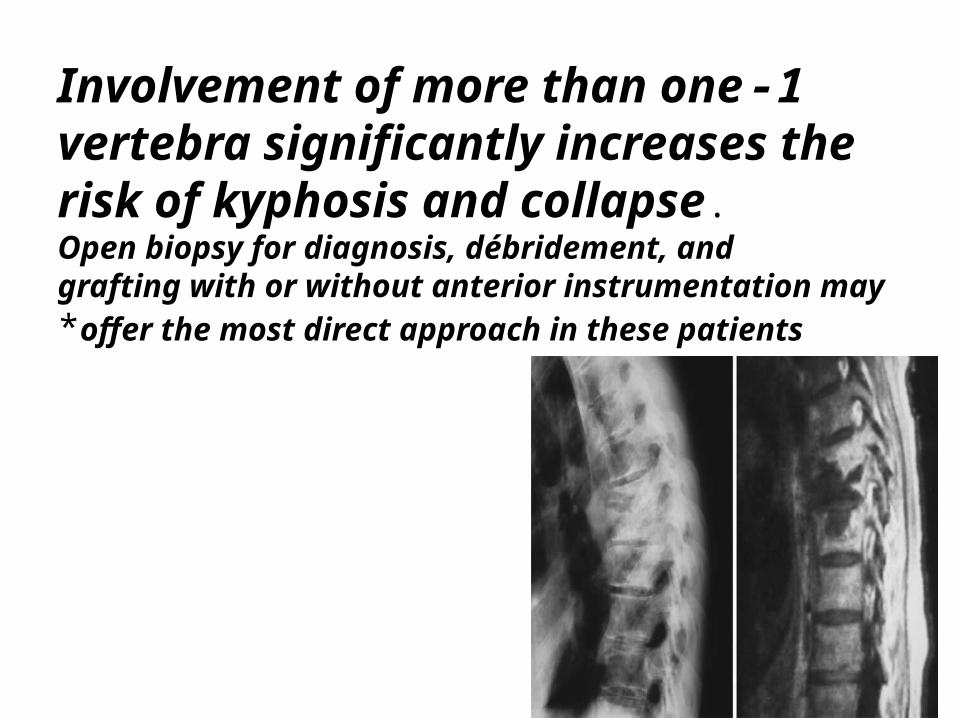
1-Involvement of more than one vertebra significantly increases the risk of kyphosis and collapse.Open biopsy for diagnosis, débridement, andgrafting with or without anterior instrumentation may
offer the most direct approach in these patients*
2-Resistance to chemotherapy and recurrence of the disease are other indications for radical surgical treatment
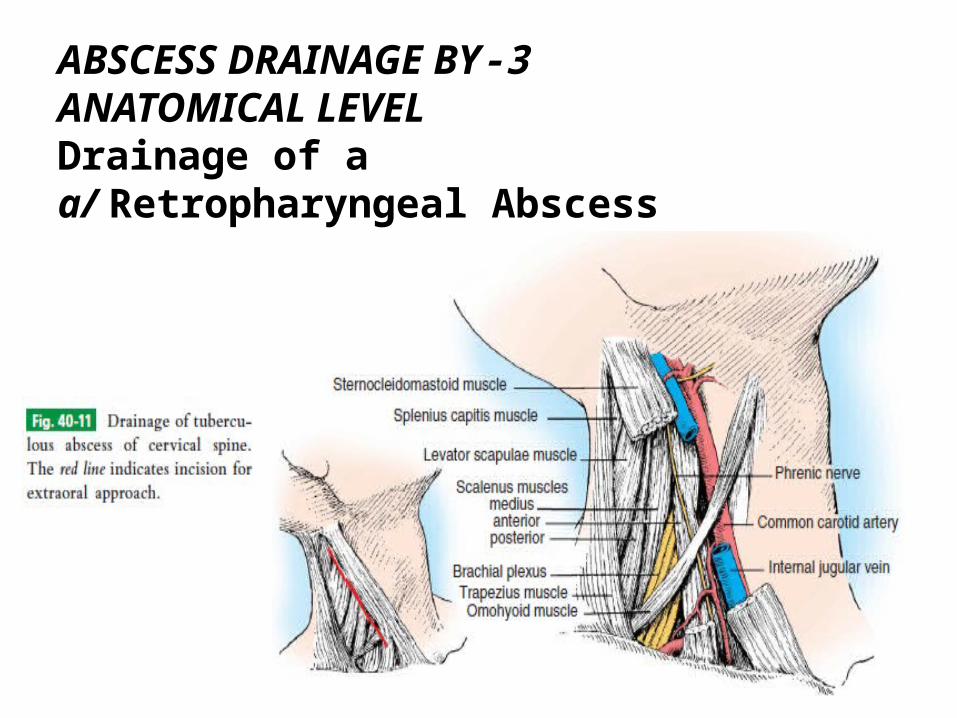
3-ABSCESS DRAINAGE BYANATOMICAL LEVELDrainage of a a/ Retropharyngeal Abscess
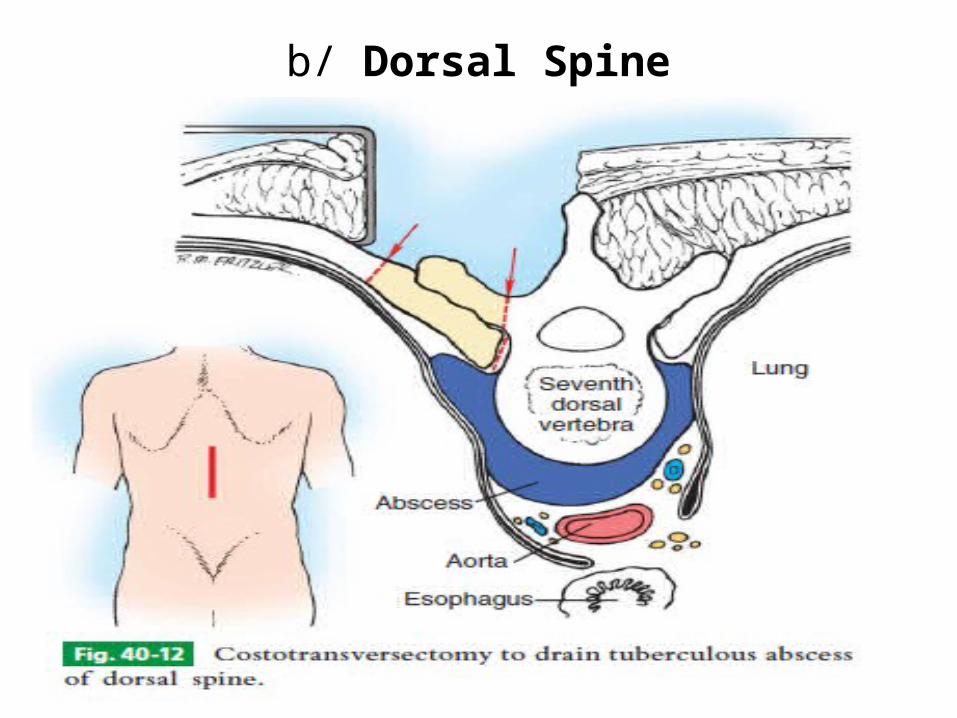
b/ Dorsal Spine
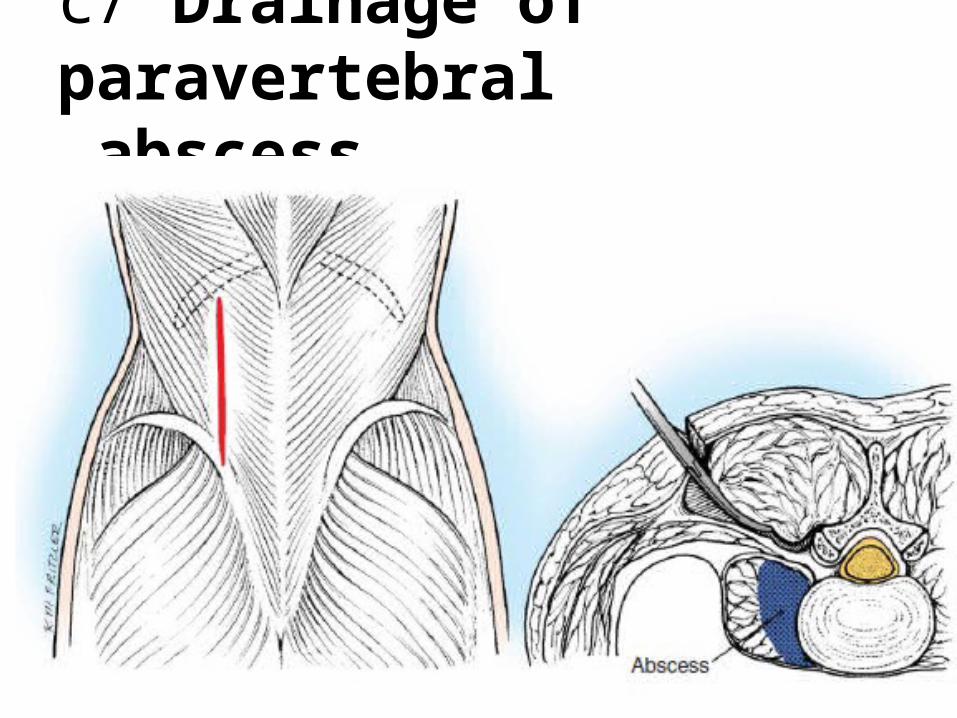
c/ Drainage of paravertebralabscess.
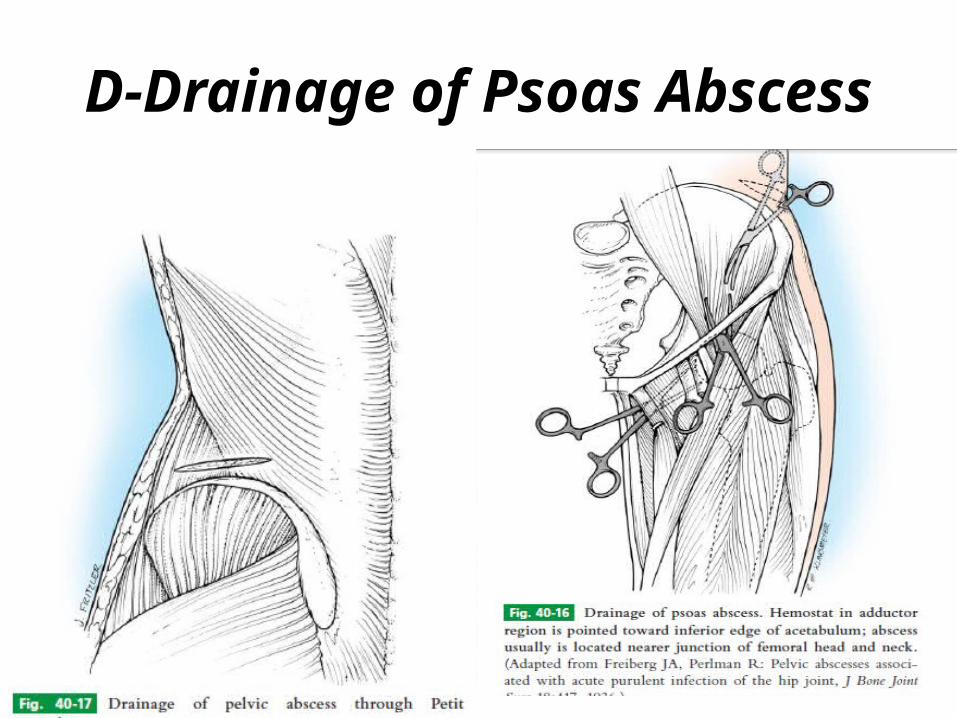
D-Drainage of Psoas Abscess
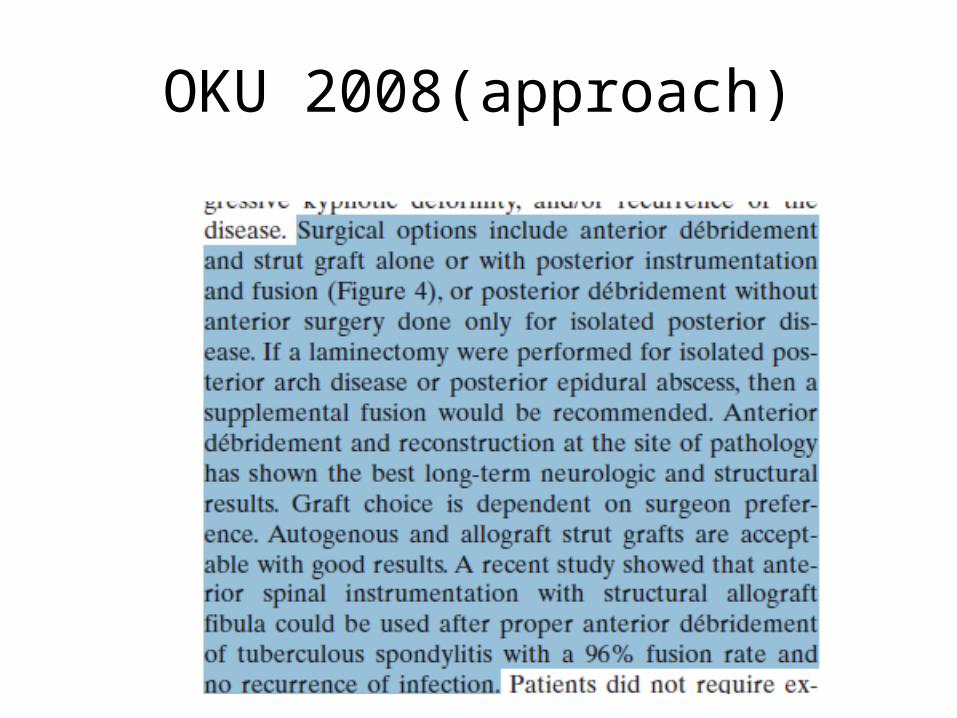
OKU 2008(approach)




![MultifocalTubercularOsteomyelitis:ACasewith ...downloads.hindawi.com/journals/trt/2011/483802.pdf · of TB and 10% of all cases of extrapulmonary TB [1]. Spinal tuberculosis accounts](https://img.pdfslide.net/doc/110x75/5fc50df01ca4e1756528a853/multifocaltubercularosteomyelitisacasewith-of-tb-and-10-of-all-cases-of-extrapulmonary.jpg)