Embed Size (px)
DESCRIPTION
Surgery for aortic root pathologies
Citation preview

Mohammad Shihata

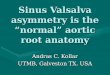
What is the Aortic Root?
The Aortic Root, represents the outflow tract fromthe left ventricle, provides the supporting structuresfor the leaflets of the aortic valve, and forms thebridge between the left ventricle and the ascendingaorta.
It extends from the basal attachments of the leafletsWithin the left ventricle to the sinotubular junction

The Aortic Root Consists of :
Aortic annulus
Aortic cusps
Aortic Sinuses
Sinotubular Junction (STJ)

The Aortic Annulus has muscular attachments ( themuscular IVS ) 45% of the circumference and fibrousattachment ( fibrous septum and anterior mitralleaflet ) 55% of the circumference.





Too small ( small annulus ) Too large ( Root Aneurysm )
Enlargement- Nicks ( Post. ) procedure- Manouguian ( Post.) Procedure- Konno ( Ant.) Procedure
Replacement- Bentall Procedure- Ross Procedure
Replacement + Enlargement- Ross – Konno- Modified Ross – Konno
Replacement Bentall
- Mechanical- Stented tissue- Stentless tissue
Valve Sparing- Remodelling- Reimplantation

Root Abscess ( Endocarditis ) Type A Dissection
Replacement- Bentall- Mechanical- Stented tissue- Stentless tissue
+/-Mitral / LA
Reconstruction
Bentall- Mechanical- Stented tissue- Stentless tissue
Valve Sparing- Remodelling- Reimplantation

Degenerative
Connective Tissue Disorders
Bicuspid Aortopathy
Post Stenotic
Chronic Dissections

Replacement of theAortic root & Ascending Arota isindicated If thediameter is > 55mm,or >50mm in case of CTD or family historyof dissections

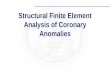
Reimplantation ( David I) Remodelling ( Yacoub)

1- Aortic root dilatation secondary to ascendingaortic aneurysm:
The mechanism of aortic insufficiency in this diseasestate is a consequence of the dilatation of thesinotubular junction (STJ) with distraction at thecommissures of the valve leaflets.

2-Annulo-aortic ectasia and connective tissuesyndromesCTD such as Marfan’s and Ehlers-Danlos:
The mechanism Is dilatation of the sinuses, the sinotubular junction, as well as the annulus, due topathologic cystic medial necrosis. Interestingly, theleaflets tend to be spared.

3-Aortic root and ascending aortic dissection—acute or chronic:
in aortic dissection, there is dilatation of thesinotubular junction with either or both (a) acutedistraction of the valve leaflets; and (b) unhingingand prolapse of the leaflets secondary to sinus walldissection.

In 1992, David and Feindel published a series of 10 patients






167 patients , 10 year follow up Survival (92%) Freedom from moderate to severe AI (94%) Freedom from Aortic reoperation (95%)

325 (David I), 59 Marfans
80% freedom from reoperation at 10y
8.5% late mortality


• Gold Standard for young patients ( < 65y )
• Permanent Anticoagulation
-Contraindications-Life style-Patient preference
• Higher risk for TE
•Most Durable
•Higher risk for infection ( or Re infection)
In 1968, Bentall and De Bono reported (in a two page case report), a single patient treated with a composite graft and mechanical valve replacement of the aortic root and ascending aorta with coronary reimplantation

Improved Hemodynamics
Ideal for Root Abscess
Reduced infection (?)
Low ThromboembolicComplications
---------------------------------- Availability
Risk of Calcification ( >50% SVD in 20 y )( immune mediated? )
Homovital ( Fresh) Cryopreserved

• 0.2% Preserved in glutaraldehyde
•Polyester sewingcuff
•Alfa amino oleic acid( anticalcification )
•Zero net pressure fixation of the leaflets

Root Aneurysm 43.8% Small Annulus 45.2% Type A dissection 6.6% Root Abscess 4.4%
Operative mortality 5.4%
100% freedom from TECand SVD at 5y

Bach DS, Metras J, Doty JR, Yun KL, Dumesnil JG, Kon ND
Freedom from structural valve deterioration among patients aged < 60 years undergoing Freestyle stentless aortic valve replacement.J Heart Valve Dis. 2007 Nov;16(6):649-55;]
725 patients, 92.4% freedom from SVD at 12 years

57 Reoperations in 12 y ( 1993 - 2005)
10 Freestyles, 2 SVD (7 & 9 years) & 8Endocarditis
Reop within 1 y was an independant risk factor for mortality

Sizes 21 mm - 27mm




Care must be takenwhen excising thePulmonary Autograftdue to the closeproximity of thePulmonary valve tothe left main andfirst septal perforatorcoronary arteries


No Anticoagulation/ Thromboembolic complications
Potential for Growth
Improved hemodynamics
Reduced risk of Endocarditis



Scalloped ( Subcoronary )
Inclusion Cylinder
Freestanding Root
Supported Root

Subcoronary Inclusion Cylinder



Two centres, 347 patients, 1994 – 2005 ( Subcoronary )
0.6% hospital mortality FU 3.9 +/- 2.7 years 95% freedom from all cause reoperation

487 patients 80% freedom from Aortic reoperation 84% freedom from Allograft reoperation 95% freedom from endocarditis 1 TEC












![Native Aortic Valve Endocarditis—A Case Report · aortic cusps, resulting in a bicuspid aortic valve and a weakened aortic root 3], [which may complicate infective endocarditis](https://img.pdfslide.net/doc/110x75/6015ccdee1b3dd30591e4f45/native-aortic-valve-endocarditisaa-case-report-aortic-cusps-resulting-in-a-bicuspid.jpg)