Embed Size (px)
Citation preview

CORE CURRICULUM IN NEPHROLOGY- AJKD Agnes B. Fogo. MDs Francis
Kuwait
APPROACH TO RENAL BIOPSY

Sample Size (number of glomeruli)
Focal lesions involving a small number of glomeruli - minimum 25
Membranous glomerulonephritis - single
Transplant kidney biopsy diagnoses - minimum 7
For most light microscopic assessment - 8 - 10

Sample Location (Juxtamedullary vs Cortical)
Subcapsular cortical samples have overrepresentation of global sclerosis related to aging/hypertension and non-specific scarring.
Juxtamedullary glomeruli are the earliest to be involved with segmental sclerosis in focal segmental glomerulosclerosis (FSGS). Preferred location.

Microscopy preferrences
Native renal biopsies should include Light microscopy (LM), Immunofluorescence microscopy (IF), Electron microscopy (EM).
For transplant biopsy LM and IF are considered the standard Repeat biopsies only needing LM in many cases

Allocation of the biopsy tissue
EM - 1mm LM – largest IF - 3-4 mm

Fixatives LM- Formalin (10% neutral buffered) Paraformaldehyde Bouin’s or Zenker’s (infrequent)
IF- Directly frozen, Transport media such as Michel’s (Tissue is stable at room temperature for mailing to
central laboratories in this media within one hour)
EM- Glutaraldehyde.

Handling of Tissue
No forceps, manipulate with thin wooden stick to avoid crush artifact.
Avoid touching tissue with a LM or EM fixative-contaminated scalpel or razor blade (this contaminates the tissue for IF).

Inadequate tissue IF tissue frozen for IF stains —The remaining frozen tissue may be fixed in formalin and processed for LM.
LM tissue fixed on the paraffin block- 1) EM study can be done by processing remaining tissue on paraffin block
2) IF study can sometimes be done satisfactorily in tissue that has not been in paraffin blocks too long

Staining and processing
1) LM- Dehydrated and placed in paraffin block, and multiple serial sections are obtained and stained.
Usual stains are- • Hematoxylin & eosin, • Periodic acid–Schiff (PAS),• Silver methenamine (Jones)• Masson trichrome. Usual processing time – 5 hours

2) IF- Tissue for IF is surrounded with OCT compound and frozen, and sections are produced
Stains - stained with • Fluorescein-tagged antibodies against IgG, IgA,
IgM, • Complements C3 and C1q, and light chain. • Complement product C4d may also be stained (best on frozen tissue, with more technical difficulty in staining on paraffin-block tissue) Usual processing time – 2 hours

3) EM- EM tissue is processed and embedded in a plastic, hard media and scout sections (so-called thick sections) are obtained Stain - with toluidine blue
Usual processing time – 2 days

Glomerulus
Tubules
Interstitium Vascular disease
Assessment
Morphological Localisation

Category of Injury- Active Versus Fibrosing
Active lesions• Proliferation• Necrosis• Crescents• Edema• Active inflammation ( glomerulitis, tubulitis, vasculitis)
Fibrosing• Glomerulosclerosis• Fibrous crescents• Tubular atrophy• Interstitial fibrosis• Vascular sclerosis

Stains Best assessment of
1. HE Cellularity and morphology
2 . PAS Basement Membrane Mesangial matrix
3. Masson’s Trichrome Fibrosis

Stains Best assessment of
4. Jones Silver Basement Membrane Mesangial matrix
5.Congo red Amyloid
6) MSB Fibrin

STAINING OF RENAL TISSUE COMPONENTSFEATURE HE PAS TRICHROME JONES/GMS
Cellularity Excellent Excellent Poor Poor
Mesangial M Poor Excellent Variable Excellent
Glom. Sclerosis Poor Excellent Excellent Good
Immune Cox. Poor Poor Variable Negative
Basement M. Poor Excellent Good Excellent
Fibrosis Poor Poor Excellent Excellent
Vascular hyaline Good Poor Good Negative
Thrombi Good Poor Good Variable


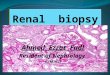
• Green- Epithelial cells a) Visceral- capillary walls i.e PODOCYTESb) Parietal- Bowmans capsule & Proximal tubules
• Yellow – Endothelial cells lining capillary lumen
• Red – mesangial cells
• Blue – mesangial matrix






Lamina rara externaLamina rara internaLamina densa
Endothelial cell
Podocyte

Minimal change disease- LM

EM
Effacement of foot processess
Condensation of cytoskeleton to BM

Effacement of foot processess

Membranous - LM
Thick capillary wall

EM

Effacement of foot processess
Subepithelial immune deposits
BM projection between deposits


IF- mostly IgG global, rarely IgM and IgA

FSGS – LM
Sclerosis Hyalinosis
Adhesion to Bowmans capsule

FSGS

IF – IgM and C3

Thank You