Embed Size (px)
Citation preview

SEMINAR PRESENTATION ON THYRIOD
CANCER
BY SALMA TASNEEMROLLNO:2O
PHARM:DINTERN
Thyroid Cancer:• Thyroid cancer is a cancer originating from
follicular or parafollicular thyroid cells. These cells give rise to both well-differentiated cancers (i.e., papillary and follicular) and anaplastic thyroid cancer. The second cell type, the C or parafollicular cell, produces the hormone calcitonin and is the cell of origin for medullary thyroid carcinoma (MTC).
Signs and Symptoms:
• A lump or swelling in your neck. This is the most common symptom.
• Pain in your neck and sometimes in your ears.• Difficulty swallowing.• Difficulty breathing or constant wheezing.• Hoarseness that is not related to a cold.• A cough that continues and is not related to a cold.• Some people may not have any symptoms. Their doctors
may find a lump or nodule in the neck during a routine physical exam.
• Thyroid cancer is usually found in a euthyroid patient, but symptoms of hyperthyroidism or hypothyroidism may be associated with a large or metastatic well-differentiated tumor.
• Thyroid nodules are of particular concern when they are found in those under the age of 20. The presentation of benign nodules at this age is less likely, and thus the potential for malignancy is far greater.
Causes:
• Thyroid cancers are thought to be related to a number of environmental and genetic predisposing factors, but significant uncertainty remains regarding its causes.
• Environmental exposure to ionizing radiation from both natural background sources and artificial sources is suspected to play a significant role, and there are significant increased rates of thyroid cancer in those exposed to mantlefield radiation for lymphoma, and those exposed to iodine-131 following the Chernobyl and Fukushima nuclear disasters.Thyroiditis and other thyroid diseases also predispose to thyroid cancer.
• Genetic causes include multiple endocrine neoplasia type 2 which markedly increases rates, particularly of the rarer medullary form of the disease.
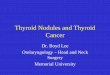
Diagnosis• After a thyroid nodule is found during a physical
examination, a referral to an endocrinologist or a thyroidologist may occur. Most commonly an ultrasound is performed to confirm the presence of a nodule and assess the status of the whole gland. Measurement of thyroid stimulating hormone and anti-thyroid antibodies will help decide if there is a functional thyroid disease such as Hashimoto's thyroiditis present, a known cause of a benign nodular goiter. M easurement of calcitonin is necessary to exclude the presence of medullary thyroid cancer.
• Finally, to achieve a definitive diagnosis before deciding on treatment, a fine needle aspiration cytology test is usually performed and reported according to the Bethesda system.
Classification: Thyroid cancers can be classified according to their
histopathological characteristics. The following variants can be distinguished (distribution over various subtypes may show regional variation):
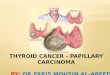
• Papillary thyroid cancer (75% to 85% of cases – often in young females – excellent prognosis. May occur in women with familial adenomatous polyposis and in patients with Cowden syndrome.
• Follicular thyroid cancer (10% to 20% of cases occasionally seen in patients with Cowden syndrome
• Medullary thyroid cancer (5%to 8% of cases)- cancer of the parafollicular cells, often part of multiple endocrine neoplasia type 2
Poorly differentiated thyroid cancer• Anaplastic thyroid cancer (less than 5% of cases[12]) is not
responsive to treatment and can cause pressure symptoms.• Others Thyroid lymphoma• Squamous cell thyroid carcinoma• Sarcoma of thyroid
• Anaplastic thyroid cancer (less than 5% of cases[12]) is not responsive to treatment and can cause pressure symptoms.
• Others Thyroid lymphoma• Squamous cell thyroid carcinoma• Sarcoma of thyroid
Goal Of Treatment• The goal of treatment for thyroid cancer is to get rid of the cancer cells
in your body. How this is done depends on your age, the type of thyroid cancer you have, the stage of your cancer, and your general health.
• Sometimes a suspicious lump or nodule has to be surgically removed before you will know if you have cancer or not.
• After surgery, you may need treatment with radioactive iodine to destroy any remaining thyroid tissue.
• When you no longer have all or part of your thyroid gland, you will probably need to take thyroid hormone medicines for the rest of your life. These medicines replace necessary hormones that are normally made by the thyroid gland and prevent you from having hypothyroidism-too little thyroid hormone.
Treatment• Surgery to remove the part of the thyroid gland that contains
cancer. Removing one part (lobe) is called a lobectomy. Removing both lobes is called a total thyroidectomy. Removing all but a very small part of the thyroid is called a near-total thyroidectomy. Lymph nodes may also be removed during surgery.
• Radioactive iodine, which is used after surgery to destroy any remaining thyroid tissue. After you have your thyroid surgically removed, you may have to wait several weeks before having radioactive iodine treatment to destroy any remaining thyroid tissue.
• During the waiting period, you may have symptoms of hypothyroidism such as fatigue, weakness, weight gain, depression, memory problems, or constipation.
• Thyroid-stimulating hormone (TSH) suppression therapy. TSH suppression therapy reduces the TSH in your body, which may help prevent the growth of any remaining cancer cells.
• If thyroid cancer is advanced when it is diagnosed, initial treatment may also include chemotherapy or radiation therapy.
Ongoing treatment
• After treatment for thyroid cancer, you may need to take thyroid hormone medicine for the rest of your life to replace the hormones that your body no longer makes. You will also need follow-up visits with your doctor every 6 to 12 months. In addition to scheduling regular visits, be sure to call your doctor if you notice another lump in your neck or if you have trouble breathing or swallowing.
• At your follow-up visits, your doctor may order a blood test to measure your thyroid-stimulating hormone (TSH) level.
• This test helps your doctor know if you are taking the right amount of thyroid hormone medicine. Your doctor may order other tests, such as a radioiodine scan, X-rays, or a CT scan.
• THYROID HORMONE THERAPY: After thyroid cancer surgery, thyroid hormone medication levothyroxine is given for life. This pill has two benefits: It supplies the missing hormone that thyroid would normally produce, and it suppresses the production of thyroid stimulating hormone from pitutiary gland. High TSH levels could stimulate any remaining cancer cells to grow.
• Check thyroid hormone levels for proper dosing.
• RADIOACTIVE IODINE THERAPY:• Radioactive iodine treatment uses large doses of radioactive
iodine. It is often after thyroidectomy to destroy any remaining healthy thyroid tissue, as well as microscopic areas of thyroid cancer that weren’t removed during surgery. This treatment may also be used to treat thyroid cancer that reoccurs after treatment or that spreads to other areas of the body.
• Side effects: Nausea, dry mouth, dry eyes, altered sense of taste or smell, plan where thyroid cancer cells have spread, such as neck or chest.
• Precautions: Temporarily avoid close contact with people, especially children and pregnant women
• External radiation therapy:• Radiation therapy is given externally using a
machine that aims high-energy beams at precise points on the body. This treatment is typically administered a few minutes at a time, five days a week, for about six weeks. This is generally used to treat thyroid cancer that has spread to the bones.
CHEMOTHERAPY:
• The tyrosine kinase inhibitors (TKIs), vandetanib and cabozantinib, have been approved by the FDA for thyroid cancer.
• Vandetanil:300mg PO daily• Cabozantir: 140mg PO daily• Dosage adjustment for TKIs may be required
depending on toxicity and coadministered drugs.
Side effects of treatment
• The side effects of surgery for thyroid cancer are usually mild and last a couple of days. Your doctor will talk to you about medicine you can take if you are having pain. You will likely need to take thyroid hormone medicine for the rest of your life to replace the hormones that your body no longer makes.
• Taking high doses of thyroid hormone may cause a rapid or irregular heartbeat. High doses taken over time may also cause weakness in your bones (osteoporosis).

THANK YOU