Embed Size (px)
Citation preview

THYROID FNA
DR ZAHID MAHMOODFCPS(HISTOPATHOLOGY)
KING EDWARD MEDICAL UNIVERSITY LAHORE

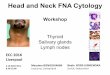
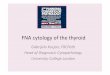
Thyroid FNA Procedure
• US guidance
• 25 gauge needle
• 3-4 passes
FNA Thyroid

Fine Needle Non Aspiration (FNNA) biopsy showing needle, position & direction for biopsy.
Immediately after FNA, firm pressure is applied to biopsy sites

Technique and Equipment (Contd…)
Biopsy Procedure without aspiration

Difference between core and FNA biopsy

Needle is removed from syringe Air is aspirated into the syringe
Aspirated material is expelled onto the slides & smears are prepared

Technique and Equipment (Contd…)
Material in the hub of needle

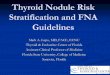
Thyroid FNA Preparations
• Direct smears
- Air-dried, Diff Quik stained
- Ethanol fixed, Pap stained
• Cytospins • Cell block
• Liquid-based preparation
FNA Thyroid
DQ
PAP
CB
Core Biopsy

Thyroid FNA The Cell Pattern Approach
• CELLS– Arrangement– Nuclear features– Cytoplasmic features
• COLLOID
• BACKGROUND FEATURES

Clues to Diagnosis!
• More colloid ….more likely benign• More cells …. more likely neoplastic

The Bethesda System for Reporting Thyroid Cytopathology: 6 Diagnostic Categories
• I. NONDIAGNOSTIC or UNSATISFACTORY•• II. BENIGN
• III. ATYPIA OF UNDETERMINED SIGNIFICANCE or FOLLICULAR LESION OF UNDETERMINED SIGNIFICANCE
• IV. FOLLICULAR NEOPLASM or SUSPICIOUS FOR A FOLLICULAR NEOPLASM
• - specify if Hürthle cell (oncocytic) type
• V. SUSPICIOUS FOR MALIGNANCY
• VI. MALIGNANT•

TBRTC: Relationship to Clinical Algorithms
Category Cancer Risk Management
Nondiagnostic or Unsatisfactory
1-4% Repeat FNA with U/S
Benign <1-3 % Follow-up clinically
AUS, FLUS ~5-15 % Repeat FNA
Follicular Neoplasm, orSuspicious for a Follicular Neoplasm*
20-30 % Lobectomy
Suspicious for Malignancy(usually papillary CA)
60-75 % Lobectomy or total thyroidectomy
Malignant 97-99 % Total thyroidectomy
* Specify if Hürthle cell type

Thyroid FNA: made Easy
• Granulomatous Thyroiditis Giant cells munching on colloid• Hashimoto’s Thyroiditis Lymphocytes and oncocytes• Papillary carcinoma Papillae, nuclei and cytoplasm• Medullary carcinoma Carcinoid and amyloid • Anaplastic carcinoma Ugly giant and spindle cells• Follicular lesions? Colloid vs. follicular cells


Follicular Neoplasm
CYTOMORPHOLOGY
• Marked cellularity• Discohesion, single cells • Predominantly microfollicles
and/or trabeculae• Uniformly enlarged cells• Crowding • Scant colloid • Marked nuclear atypia, mitosis
and necrosis is uncommon

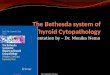
Papillary carcinoma
Follicular variant

VI: Malignant Papillary thyroid carcinoma
• Papillae- not very common
• Sheets: flat or syncytial
• Sheets/ clusters with well defined borders
• Clusters: 3-D

VI: Malignant Medullary thyroid carcinoma
Plasmacytoid cells Spindle cells

VI: Malignant Anaplastic carcinoma

FNA Breast lesions (reporting Categories)
C-1 Inadequate C-2 Benign
C-5 Malignant
C-3 Atypia (probably benign) C-4 Suspicious for malignancy








![Cytopathologic diagnosis of fine needle aspiration …...Thyroid FNA State of the Science Conference with a group of experts at Bethesda, MD, in October 2007[7]. This conference established](https://img.pdfslide.net/doc/110x75/5f58ba8c2659e94ec243e3b2/cytopathologic-diagnosis-of-fine-needle-aspiration-thyroid-fna-state-of-the.jpg)