Embed Size (px)
Citation preview

KHALED EL SAYED EL HADIDY. MD Head of Internal Medicine Department.
Head of Diabetes and Endocrinology Unit.Beni - Suef University.
Thyroid Nodules In Practice
By

Definition“A discrete lesion within the thyroid gland that is palpably and/or
ultrasonographically distinct from surrounding thyroid parenchyma”
*ATA Management Guidelines for Patients with Thyroid Nodules and Differentiated Thyroid Cancer (2006 & 2009 Task Force)

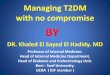
Prevalence
0
10
20
30
40
50
60
10 20 30 40 50 60 70
Palpation
Autopsy
Ultrasound
Palpable 5% women & 1% men living in iodine-sufficient parts of the world
(U / S) 19–67% higher frequencies in women & elderly.
Thyroid cancer 5–15% ------------- (90%) (DTC) papillary and follicular cancer.

Causes

Guidelines
------ 2015
TI-RADS ………….. Elastography

The American Thyroid Association (ATA) Guidelines Taskforce on Thyroid Nodules and Differentiated Thyroid Cancer 2009

The American Thyroid Association (ATA) Guidelines Taskforce on Thyroid Nodules and Differentiated Thyroid Cancer 2009

The American Thyroid Association (ATA) Guidelines Taskforce on Thyroid Nodules and Differentiated Thyroid Cancer 2009

The American Thyroid Association (ATA) Guidelines Taskforce on Thyroid Nodules and Differentiated Thyroid Cancer 2009

The American Thyroid Association (ATA) Guidelines Taskforce on Thyroid Nodules and Differentiated Thyroid Cancer 2009

American Thyroid Association (ATA) Guidelines Taskforce on Thyroid Nodules and Differentiated Thyroid Cancer 2009

High-risk history: History of thyroid cancer in one or more first degree relatives.History of external beam radiation as a child. Exposure to ionizing radiation in childhood or adolescence. Prior hemithyroidectomy with discovery of thyroid cancer. 18FDG avidity on PET scanning.MEN2/FMTC-associated RET protooncogene mutation.Calcitonin >100 pg/mL.
Suspicious features: Microcalcifications.Hypoechoic. Increased nodular vascularity.Infiltrative margins. Taller than wide on transverse view.
NCCN 2013
1cm
1.5
All + LN.
The American Thyroid Association (ATA) Guidelines Taskforce on Thyroid Nodules and Differentiated Thyroid Cancer 2009

The American Thyroid Association (ATA) Guidelines Taskforce on Thyroid Nodules and Differentiated Thyroid Cancer 2009


Consider biopsy > 1cm
Consider biopsy > 1.5 cm
Consider biopsy > 2 cm
FNA is not recommended for nodules thatdo not meet the above criteria, Including all nodules < 1 cm



FNAB


Thyroid U/S Elastography

The goals:
Stratify the risk of malignancy of a lesion based on the US features of the lesion.
Standardize and simplify the reports, allowing effective communication between radiologists, cytologists, and clinicians.
Improve quality of care and cost-effectiveness, avoiding unnecessary biopsies.
TI-RADS (Thyroid Imaging - Reporting and Data System) :
Are We There Yet?

TIRADS by Horvath et al.
Research group from Chile Study lasted 8 years, published in 2009 1959 thyroid nodules submitted for fine needle
aspiration biopsy (FNAB) Study introduced 6 TIRIADS categories and 10
US patterns
Horvath E, Majilis S, Rossi R, Franco C, Niedmann J, Castro A & Dominguez M. An ultrasonogram reporting system for thyroid nodules stratifying
cancer risk for clinical management. Journal of Clinical Endocrinology and Metabolism 2009 90 1748–1751
Description Risk of malignancy
TIRADS 1 Normal thyroid gland 0
TIRADS 2 Benign 0
TIRADS 3 Probably benign <5%
TIRADS 4A Suspicion for malignancy 5-10%
TIRADS 4B Intermediate suspicion for malignancy 10-80%
TIRADS 5 Highly suggestive of malignancy >80%
TIRADS 6 Biopsy proven malignancy

TIRADS by Russ et al
Research group from France Prospective study on 4550 nodules, lasted 2 years
(early paper included 500 nodules were published in 2011 in French language).
Authors proposed the following flowchart to assign a nodule to one of TIRADS categories
Suspect pattern Benign pattern
Thyroid Nodule
High Suspect:Taller-than-wideIrregular borders
MicrocalcificationsMarkedly hypoechoic
High stiffness on sonoelastography
Very probably
No signs of high suspect.
Mildly hypoecoic
1-2 signs,no metastatic lymph
nodes
3-5 signs and/or metastatic lymph
nodes
TIRADS 4ATIRADS 4BTIRADS 5
Constantly
No sign of high suspicion: regular
shape and borders, no micro-
calcifications and iso/hyperecoic
- Simple cyst- Spongiform nodule- “white knight”- isolated macro-
calcifications- Nodular hyperplasia
TIRADS 2TIRADS 3
Russ B, Royer B, Bigorgne C, et al. Prospective evaluation of thyroidimaging reporting and data system on 4550 nodules with and without elastography. Eur J Endocrinol. 2013;168:649–655.

TIRADS by Kwak et al
Research group from Korea. Prospective study 8 years, published in 2011. 1959 thyroid nodules submitted for FNA.
Kwak JY, Han KH, Yoon JH, Moon HJ, Son EJ, Park SH, Jung HK, Choi JS, Kim BM & Kim E-K. Thyroid imaging reporting and data system for US features of nodules: a step in establishing better stratification of cancer risk. Radiology 2011 260 892–899
The following features were associated with malignancy: solid component, hypo-echogenicity, marked hypoechogenicity, microlobulated or irregular margins, micro-calcifications, taller-than-wide shape. As
the number of suspicious US features increased, the fitted probability and risk of malignancy also increased:
DescriptionNumber of suspicious
featuresRisk of
malignancy
TIRADS 1 Negative 0 0
TIRADS 2 Benign 0 0
TIRADS 3 Probably benign 0 1.7%
TIRADS 4A Low suspicion for malignancy 1 3.3%
TIRADS 4B Intermediate suspicion for malignancy 2 9.2%
TIRADS 4C Moderate concern but not classic for malignancy 3-4 44.4-72.4%
TIRADS 5 Highly suggestive of malignancy 5 87.5%



( > 50% volume or 20%increase in at least two nodule dimensions with a minimal increase of 2mm in solid nodules or in the solid portion of mixed cystic–solid nodules )

Pregnancy • Nodule with PTC in early pregnancy monitored U/S :
if it grows substantially by 24 weeks gestation, surgery should be performed at that point.if it remains stable by midgestation or if it is diagnosed in the second half of pregnancy, surgery may be performed after delivery.
• with more advanced disease : surgery in the second trimester is reasonable. C
• with FNA that is suspicious for or diagnostic of PTC, consideration could be given to administration of LT4 therapy to keep the TSH in the range of 0.1–1mU=L. C

Thank you