- 1. Urinary System Presented By: Milani, Mandeep, Karthiga,
Gladyz, Elisa
2. KIDNEYS-Location and Structure
- Although many believe that the kidneys are located in the lower
back, this is not their location.
- These small, dark red organs with a kidney bean shape lie
against the dorsal body wall in a retroperitoneal position (beneath
the parietal peritoneum) in the superior lumbar region.
- The kidneys extend from the T12 to the L3 vertebra; thus they
receive some protection from the lower part of the rib cage.
- Right kidney is slightly lower then the left
- It is convex laterally and has a medial indentation called the
renal hilus.
- Atop each kidney is an adrenal gland, which is part of the
endocrine system and is a distinctly separate organ
functionally.
- A fibrous, transparentrenal capsuleencloses each kidney and
gives a fresh kidney a glistening appearance.
- The adipose capsule, surrounds each kidney and helps hold it in
place against the muscles of the trunk wall.
3.
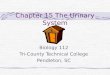
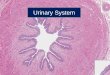
- When a kidney is cut lengthwise, three distinct regions become
apparent, as can be seen in this picture.
- The outer region, which islightin color, is therenal
cortex.
- Deep to the cortex is a darker reddish-brown area, therenal
medulla.
- The broader base of each pyramid faces toward the cortex; its
tip, the apex, points toward the inner region of the kidney.
- The pyramids are separated by extensions of cortex like tissue,
therenal columns.
Renal Column Renal Cortex Renal Medull a 4.
- Medial to the hilus is a flat, basinklike cavity, the renal
pelvis
- Pelvis is continuous with the ureter leaving the hilus.
- Extension of the pelvis, calyces (calyx), form cup-shaped areas
that enclose the tips of the pyramids.
- The calyces collect urine, which continuously drains from the
tips of the pyramids into the renal pelvis.
- Urine then flows from the pelvis into the ureter, which
transport it to the bladder for temporary storage.
5. Blood supply
- The kidneys continuously cleanse the blood and adjust its
composition, so it is not surprising that they have a very rich
blood supply
- One-quarter of the total blood supply of the body passes
through the kidneys each minute.
6.
- The arterial supply of each kidney is therenal artery
- As the renal artery approaches the hilus, it divides
intoSegmental arteries .
- Once in side the pelvis, the segmental arteries break up
intolobar arteries
- Each of which gives off several branches calledinterlobar
arteriesthen branch off the arcuate arteries and run outward to
supply the cortical tissue.
- The venous blood draining from the kidney flows through veins
that trace the pathway of the arterial supply but in a reverse
direction-interlobular veinstoarcuate veinstointerlobar veinsto
therenal vein , which emerges from the kidney hilus
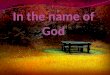
7. Nephrons and Urine Formation
- Each kidney contains over a million tiny structures called
nephrons.
- Nephrons are the structural and functional units of the kidneys
and, as such, are responsible for forming urine.
- Each nephron consists of two main structures: aglomerulus ,
which is a knot of capillaries, and arenal tubule .
- The cup- shaped of the renal tubule is called the glomerular,
or Bowmans, capsule.
- The inner layer of the capsule is made up of highly modified
octopus- like cells calledpodocytes
8.
- Extends from the glomerular capsule, it coils and twists before
forming a hairpin loops and then again becomes coiled and twisted
before entering a collecting tubule called thecollecting duct.
(these different regions of the tubule have specific names)
- These different regions of the tubule have specific names.
- Most nephrons are calledcortical nephronsbecause they are
located almost entirely within the cortex.
- Thecollecting ducts , each of which receives urine from many
nephrons, run downward through the medullary pyramids, giving them
their striped appearance.
9.
- Theafferent arteriole , which arises from an interlobular
artery, is the feeder vessel, and theefferent arteriolereceives
blood that has passed through the glomerulus.
- The glomerulus, specialized for filtration, is unlike any other
capillary bed in the entire body.
- The second capillary bed, theperitubular capillaries , arises
from the efferent arteriole that drain the glomerulus.
- Unlike the high-pressure glomerulus, these capillaries are low-
pressure, porous vessels that are adapted for absorption instead of
filtration.
- The peritubular capillaries drain into interlobular veins
leaving the cortex.
10. Urine Formation
- It is a result of three processes:
11. Filtration
- Glomerulus Acts as a Filter
- Water and solutes smaller than proteins are forced through the
capillary walls and pores of the glomerular capsule into the renal
tubule.
- Both proteins and blood cells normally too large to pass
through the filtration membrane and when either one of these appear
in urine it is evident there is a problem with the glomerular
filters
12. Cont
- Also, systemic blood pressure has to be normal in order for
filtration to happen
- If the arterial blood pressure falls too low, the glomerular
pressure becomes inadequate to force substances out of the blood
and into the tubules, and filtrate formation stops
13. Homeostatic Imbalance
- Oliguria: an abnormal low urinary output if it is between 100
and 400 ml/day
- Anuria if it is less than 100ml/day
- Low urinary output indicates that glomerural blood pressure is
too low to cause filtration
- However, Anuria may also result from transfusion reactions and
acute inflammation or from crush injuries of the kidneys
14. Cont
- Blood from afferent arteriole flows into the glomerulus
(capillaries)
- Due to blood pressure in the glomerulus, filtration occurs
- Water and small molecules (such as salts, amino acids, urea,
uric acid, glucose) move from the blood plasma into the
capsule
- Small molecules that escape being filtered and the
nonfilterable components leave the glomerulus by the Efferent
arteriole
- This produces a filtrate of blood, called glomerular
filtrate
15.
- Filterable Blood Components
- Nonfilterable Blood Components
- Formed elements (blood cells and platelets)
16. Tubular Reabsorption
- As the filtrate moves along the tubule some of the molecules
and ions are actively and passively (by diffusion) reabsorbed into
the capillary bed from the tubule
- Active transport: transport of molecules against a
concentration gradient (from regions of low concentration to
regions of high concentrations) with the aid of proteins in the
cell membrane and energy from ATP
17. Cont
- About 99% of filtered water and many useful molecules (such as
salts, urea, nutrients, glucose, amino acids, sodium Ion Na+,
chloride ion Cl-) returned to the blood
- Reabsorption of water is by osmosis
- Most of the reabsorption occurs in the proximal convoluted
tubules, but the distal and the collecting duct are also
active
18. Tubular Secretion
- More substances such as ions (hydrogen ion, creatinine, some
drugs (penicillin), toxic substances, are actively secreted from
the capillary network to tubules
- The fluid (urine), from filtration that was not reabsorbed and
from tubular secretion, then flows into the collecting duct, then
renal pelvis
- Substances found in urine are water, salts, urea, uric acid,
ammonia, creatinine (NOT large molecules (proteins, blood cells),
glucose
- Also, if all those substances weren't reabsorbed by tubules
(glucose, water, salts, urea) than the body would continually lose
water, salt and nutrients
19. 20. Characteristics of Urine
- Nephrons filter 125 ml of body fluid per minute; filtering the
entire body fluid component 16 times each day
- In a 24 hour period nephrons produce 180 liters of filtrate, of
which 178.5 liters are reabsorbed.
- The remaining 1.5 liters forms urine
21. Cont
- Freshly voided urine is generally clear and pale to deep
yellow
- The more solutes are in a urine, the deeper yellow its color;
whereas dilute urine is a pale, straw color
- When formed, urine is sterile,and its odor is slightly
aromatic
- Ph is slightly acid (around 6)
- Urine weight more than distilled water (because it has water
plus solutes)
22. Ureters
- It is a slender tube each 25-30 cm long and 6mm in
diameter
- Each tube descends beneath the peritoneum, from the hilum of a
kidney, to enter the bladder at its dorsal surface
23. Cont
- The ureters is a passageway that carry urine from the kidneys
to the bladder
- Although it may seem like urine may drain to the bladder by
gravity, but the uretersdoplay an active role in urine
transport
- Smooth muscle layers in their walls contract to propel urine
into the bladder by peristalsis (even if a person is laying
down)
- Once urine has entered the bladder, it is prevented from
flowing back into the ureters by small valvelike folds of bladder
mucosa that flap over the ureter openings
24. Homeostatic Imbalance
- When urine becomes extremely concentrated, solutes such as uric
acid salts form crystals that precipitate in the renal pelvis
- These crystals are called renal calculi, orkidney stones
- The crystals may grow into a stone ranging in size from a grain
of sand to a golf ball. Most stones form in the kidneys.
- Very small stones can pass through the urinary system without
causing problems. However, larger stones, when traveling from the
kidney through the ureter to the bladder, can cause severe pain
called colic.
- Most stones (70 to 80 percent) are made of calcium oxalate. A
smaller number are made of uric acid or cystine
25. Cont
- For treatment, surgery is a choice
- However, a newer noninvasive procedure (lithotripsy) may be
used
- Uses ultrasound waves to break the stones into small fragments
(about the size of grain of sand)
- They then can be eliminated painlessly in the urine
26. Urinary Bladder
- The urinary bladder stores urine until it is expelled from the
body
- The bladder is located in the pelvic cavity, behind the public
symphysis and beneath the peritoneum
- The bladder has three openings---two for the ureters and one
for the urethra, which drains the bladder
27. Cont
- The smooth triangular region of the bladder base outlined by
these three openings is called the tridone
- The trigone is important clinically because infections tend to
persist in this region
- In males the prostate gland surrounds the neck of the bladder
were it empties into the urethra
- The bladder wall contains three layers of smooth muscle called
the detrusor muscle and its mucosa is a special type of epithelium:
transitional epithelium
- When the bladder is empty it is collapsed, 5-7.5 cm long at
most and its walls are thick and thrown into folds
28. Cont
- As urine accumulates, the bladder expands and rises superiorly
in the abdominal cavity Fig 15.7
- Its muscle wall stretches and the transitional epithelial layer
thins, allowing the balder to store more urine without
substantially increasing its internal pressure
- A full bladder is about 12.5 cm long and hold about 500 ml of
urine, but it is capable of holding more than twice that
amount
- When the bladder is really distended, or stretched by urine, it
becomes firm and pear shaped and may be felt just above the public
symphysis
- Although urine is formed continuously by the kidneys, it is
usually stored in the bladder until its release is convenient
29. Urethra 30. The anatomy of the urethra
- The epithelium of the urethra starts off as transitional cells
as it exits the bladder. Further along the urethra there are
stratified columnar cells, then stratified squamous cells near the
external meatus (exit hole).
- There are small mucus-secreting urethral glands, that help
protect the epithelium from the corrosive urine
31. The female urethra
- In the human female, the urethra is about 1 1/2-2 inches (3-5
cm) long and opens in the vulva between the clitoris and the
vaginal opening.
- Because of the short length of the urethra, women tend to be
more susceptible to infections of the bladder (cystitis) and the
urinary tract.
32.
- The female urethra is a narrow membranous canal, extending from
the internal to the external urethral orifice.
- It is placed behind the symphysis pubis, imbedded in the
anterior wall of the vagina, and its direction is obliquely
downward and forward; it is slightly curved with the concavity
directed forward.
- Its lining is composed of stratified squamous epithelium, which
becomes transitional near the bladder.
- The urethra consists of three coats: muscular, erectile, and
mucous, the muscular layer being a continuation of that of the
bladder.
- The release of urine is controlled by two sphincters.
-
- Internal urethral sphincter
-
- External urethral sphincter
33. Male urethra
- Themale urethraextends from the internal urethral orifice in
the urinary bladder to the external urethral orifice at the end of
the penis.
- It presents a double curve in the ordinary relaxed state of the
penis.
- Its length varies from 17.5 to 20 cm.; and it is divided into
three portions, theprostatic, membranous,andcavernous,the structure
and relations of which are essentially different.
- Except during the passage of the urine or semen, the greater
part of the urethral canal is a mere transverse cleft or slit, with
its upper and under surfaces in contact; at the external orifice
the slit is vertical, in the membranous portion irregular or
stellate, and in the prostatic portion somewhat arched.
34.
- 1.Theprostatic portion( pars prostatica ), the widest and most
dilatable part of the canal, is about 3 cm. long.
- 2. Themembranous portion( pars membranacea ) is the shortest,
least dilatable, and, with the exception of the external orifice,
the narrowest part of the canal It extends downward and forward,
with a slight anterior concavity, between the apex of the prostate
and the bulb of the urethra, perforating the urogenital diaphragm
about 2.5 cm. below and behind the pubic symphysis.
- 3. Thecavernous portion( pars cavernosa; penile or spongy
portion ) is the longest part of the urethra, and is contained in
the corpus cavernosum urethr. It is about 15 cm. long, and extends
from the termination of the membranous portion to the external
urethral orifice.
35. The structure of the male urethra
- The structure of the urethra (tube) itself is a
continuousmucous membranesupported bysubmucous tissueconnecting it
to the other structures through which it passes.
- Themucous coatis continuous with the mucous membrane of the
bladder, ureters and kidney. In the membranous and spongy sections
(2. and 3. above), the mucous membrane is arranged in longitudinal
folds when the tube is empty.
- Thesubmucous tissueconsists of a vascular (i.e. containing many
blood vessels) erectile layer surrounded by a layer of smooth
(involuntary) muscle fibers
- These muscle fibres are arranged in a circular configuration
that separates the mucous membrane and submucous tissue from the
surrounding structure - which is the tissue of the corpus
spongiosum (labeled simply "penis" in the diagram above).
- Unlike the female urethra, the male urethra has a reproductive
function in addition to it's urinary function - it conveys semen
out of the body at ejaculation. For further information about this
function red the section about the male reproductive system.
36. The Function of the Urethra
-
- The females only carries urine.
-
- The males carries urine and is a passageway for sperm
cells.
37. Micturition of the urethra Male and female
- Both sphincter muscles must open to allow voiding.
-
- The internal urethral sphincter is relaxed after stretching of
the bladder
-
- Activation is from an impulse sent to the spinal cord and then
back via the pelvic splanchnic nerves.
-
- The external urethral sphincter must be voluntarily
relaxed.
38. Fluid, Electrolyte, and Acid-Base Balance
- Blood composition depends on three major factors:
- In general, thekidneyshave four major roles to play, which help
keep the blood composition relatively constant.
- Excretion of nitrogen containing wastes
- Maintaining water in the blood
- Maintaining electrolyte balance in the blood, and
39. Maintaining Water and Electrolyte Balance of Blood
- Body Fluids and Fluid Compartments:
- Of the hundreds of compounds present in your body, the most
abundant is water.
- Males weighing 154 pounds will have an average of 60% of their
body weight, nearly 40L, as water.Females about 50%. (based on
nonobese individuals).
- The more fat present in the body, the less total water content
per kg of body weight .
- Female body contains slightly less water per kg of weight
because it contains slightly more fat than the male body.
40.
- In a newborn, water may account for up to 80% of body weight.
That percentage increases if the infant is born premature.
- The percentage of body water decreases rapidly during the first
10 years of life.
- In elderly individuals, the amount of water per kg of body
weight increases (because old ages is often accompanied by a
decrease in muscle mass -65% water- and in increase in fat -20%
water-)
- Water is the universal body solvent within which all solutes
(including the very important electrolytes) are dissolved.
41.
- Total body water can be subdivided into two major fluid
compartments called extracellular and intracellular fluid
compartments.
- Extracellular : consists mainly of the liquid fraction of
wholeblood called the plasma, found in the blood vessels and the
interstitial fluid that surrounds the cell.In addition, lymph,
cerebrospinal fluid, humors of the eye, and the specialized joint
fluids are also considered extracellular fluid.
- Intracellular : largest volume of water by far. Located inside
of the cells.
42. Mechanisms that maintain fluid balance
- 3 sources of fluid intake: the liquids we drink, the water in
the food we eat, and the water formed by catabolism of foods.
- Fluid output from the body occurs through four organs: the
kidneys, lungs, skin, and intestines.The fluid output that changes
the most is that from the kidneys.
- The body maintains fluid balance mainly by changing the volume
of urine excreted to match changes in the volume of fluid
intake
43. Regulation ofFluidIntake
- When fluid loss from the body exceeds fluid intake, salivary
excretion decreases, producing a dry mouth feeling, and the
sensation of thirst.The individual then drinks water, thereby
increasing fluid intake and compensating for previous fluid losses.
This tends to restore fluid balance.
- Water is continually lost from the body through expired air and
diffusion through the skin.
- Although the body adjusts fluid intake, factors that adjust
fluid output, such as electrolytes and blood proteins, are far more
important.
44. Balance between typical fluid intake and output in a 70 kg
adult. 45. What are electrolytes?
- Electrolyte is a "medical/scientific" term for salts,
specifically ions. The term electrolyte means that this ion is
electrically-charged and moves to either a negative (cathode) or
positive (anode) electrode:
- ions that move to the cathode (cations) are positively
charged
- ions that move to the anode (anions) are negatively
charged
- For example, your body fluids -- blood, plasma, interstitial
fluid (fluid between cells) -- are like seawater and have a high
concentration of sodium chloride (table salt, or NaCl). The
electrolytes in sodium chloride are:
- sodium ion (Na+) - cation
- chloride ion (Cl-) - anion
- As for your body, the major electrolytes are as follows:
46.
- Electrolytes play indispensible roles in transmitting nerve
impulses, contracting muscles, and keeping proper fluid levels in
the body
- Serve as essential minerals
- Control osmotic pressure between body fluid compartments
- Maintain acid base balance in the body
- Very small changes in electrolyte balance (solute
concentrations in various fluid compartments) cause water to move
from one fluid compartment to another.This alters blood volume and
blood pressure, but it can also severely impair the activity of
irritable cells like the nerve and muscle cell.
- A variety of electrolytes have important nutrient or regulatory
roles in the body.
- For example, Iron required for hemoglobin production.Iodine
must be available for synthesis of thyroid hormones.
- Electrolytes are also needed for many cellular activities such
as nerve conduction and muscle contraction.
- The most abundant of electrolytes aresodium , potassium, and
chloride.
47.
- Electrolytes are important because they are what your cells
(especially nerve, heart, muscle) use to maintain voltages across
their cell membranes and to carry electrical impulses (nerve
impulses, muscle contractions) across themselves and to other
cells.
- Your kidneys work to keep the electrolyte concentrations in
your blood constant despite changes in your body. For example, when
you exercise heavily, you lose electrolytes in your sweat,
particularly sodium and potassium. These electrolytes must be
replaced to keep the electrolyte concentrations of your body fluids
constant. So, many sports drinks have sodium chloride or potassium
chloride added to them. They also have sugar and flavorings to
provide your body with extra energy and to make the drink taste
better.
- The kidney acts as the chief regulator of sodium levels in body
fluids.
48.
- When blood volume drops for any reason (ie excessive sweating
or diarrhea), arterial blood pressure drops, which in turn decrease
amount of filtrate formed in the kidneys
- Highly sensitive cells in the hypothalamus called osmoreceptors
react to change blood composition (less water and more solutes) by
becoming more active. Result is the nerve impulses are sent to the
posterior pituitary, which releases anti-diuretic hormone
(ADH)
- ADH travels in the blood to its main target, the kidneys
collecting ducts, whiere it causes the duct cells to reabsorb more
water. As more water is returned to the blood stream, blood volume
and blood pressure increase to normal levels, and only a small
amount of very concentrated urine is formed.
- ADH is released more or less continually unless the solute
concentration of the blood drops too low. When this happens, the
osmoreceptors become quiet and excses water is allowed to leave the
body in the urine.
Reabsorption of water and electrolytes: 49.
- A second hormone helps to regulate blood composition and blood
volume by acting on the kidney : ALDOSTERONE
- Aldosterone is the major factor regulating sodium ion content
of the ECF and in the process helps regulate the concentration of
other ions (calcium, potassium, and magnesium) as well.
- Sodium ion is responsible osmotic water flow. When too little
sodium is in theblood, the blood becomes too dilute. Consequently,
the water leaves the bloodstream and flows out into the tiusse
spaces, causing edema and possibly a shutdown of the cirulatory
system.
- For each sodium ion that is reabsorbed in the kidney, a
chloride ion follows and a potassium ion is secreted into the
filtrate. Thus, as the sodium content of the blood increases,
potassium concentration decreases, bringing the two ions back to
their normal balance in the blood.
- Another effect of aldosterone is to increase water
reabsorption. Because as sodium is reclaimed, water follows it
passively back into theblood (WATER FOLLOWS SALT)
50.
- Reabsorption of water and electrolytes by the kidney is
regulated primarily by hormones.
- When blood volume drops for any reason, (ie due to hemorrhage
or excessive water loss sweating or diarrhea), arterial blood
pressure drops, which in turn decreases amount of filtrate formed
by kidneys. In addition, highty sensitive cells in the hypothalamus
called somoreceptions react to the change in blood composition.
(That is. Less water and more solutes.)
51. Fluid and Electrolyte Imbalances
- Dehydration:the fluid imbalance seen most often. In this
potentially dangerous condition, IF volume decreases first, but
eventually, if treatment has not been given, IFC and plasma volumes
also decrease below normal levels. Prolonged diarrhea or vomiting
may result in dehydration due to the loss of body fluids.
- Overhydration:much less common that dehydration.Giving IV
fluids too rapidly or in too large of an amount, or consuming an
extremely high amount of liquid can put too heavy a burden on the
heart.
- Any disruption in a homeostatic mechanism controlling the level
or normal checmical activity of a particular electrolyte in any of
the different body fluids produces an electrolyte imbalance. Such
imbalances are widespread and often very serious and sometimes
fatal, preventing electrolytes to do their job.
52. Maintaining Acid Base Balance
- For the cells of the Body to function, blood pH (potential of
Hydrogen) must be maintained between 7,35 and 7.45.
- When the pH rises above 7.45, a person is said to have
alkalosis.
- A drop in arterial pH to below 7.35 results in acidosis.
- Because a 7 is neutral, 7.35 is not acidic, chemically
speaking; however, it represents a higher than optimal hydrogen ion
concentration for the functioning of most body cells.
- Therefore, any arterial pH between 7.35 and 7.45 is called
physiological acidosis
53.
- Although some acidic substances enter the body through
ingestion, most hydrogen ions originate as by-products of cellular
metabolism, which continually adds substances to the blood that
tend to disturb its acid base.
- Ie phosphoric acid, lactic acid, and many types of fatty
acids.
- Carbon dioxide, which is released during energy production,
forms carbonic acid.
- Ammonia and other basic substances are also released to the
blood as cells go about their usual business.
- Although the chemical buffers in the blood can temporarily tie
up excess acids and bases, the lungs have the chief responsibility
for eliminating carbon dioxide from the body, the kidneys assume
most of the load for maintaining accid base balance of the
blood.
- There are two pH controlling systems: Blood buffers and
respiratory system.
54. Blood Buffers
- Chemical buffers are systems of one or two molecules that act
to prevent dramatic changes in hydrogen ion concentration when
acids or bases are added.
- They bind to hydrogen ions whenever the pH drops and by
releasing hydrogen ions when the pH rises.
- Chemical buffers are the first line of defense in resisting pH
changes.
- How does a chemical buffer system work??
- Acids are proton (H+) donors, and that the acidity of a
solution reflects only the free hydrogen ions, not those still
bound to anions.
- Strong acids dissociate completely and liberate all their H+ in
water.
- Weak acids dissociate only partially and have a slighter
effect.
- (weak acids are very effective at preventing pH changes since
they are forced to dissociate and release more H+ when the pH
rises).
- Bases are proton or hydrogen ion acceptors.
- Strong bases like hydroxides dissociate easily in water and
quickly tie up H+
- Weak bases are slower to accept H+ (however, as pH drops, weak
bases become stronger and begin to tie up more hydrogen ions).
55.
- There are 3 major chemical buffer systems of the body:
- They all maintain pH balance in one or more fluid
compartment.
- They all work together, and anything that causes a shift in H+
concentration in one compartment also causes changes in the
others.
56. Respiratory System Controls
- The respiratory system eliminates carbon dioxide (CO2) from the
blood while it loads oxygen into the blood.
- When CO2 enters the blood from the tissue cells, most of it
enters the red blood cells where it is converted to bicarbonate
ions for transport in the plasma.
- In healthy people, carbon dioxide is expelled from the lungs at
the same rate as it is formed in the tissues. Thus, the H+ released
when carbon dioxide is loaded into the blood is not allowed to
accumulate because it is tied up in water when CO2 is unloaded in
the lungs. So, under normal conditions, the hydrogen ions produced
by carbon dioxide transport have no effect on blood pH.
- However, when Carbon dioxide accumulates in the blood (ie
during restricted breathing), the chemoreceptors in the respiratory
control centers of the brain are activated. As a result, breathing
reate and depth increase, the excess H+ is blown off as more CO2 is
removed from the blood.
- On the other hand, when blood pH begins to rise (alkalosis),
the respiratory center is depressed. The respiratory rate begins to
fall, allowing carbon dioxide (hence, H+) to accumulate in the
blood. Again, blood pH is restored.
57. Renal Mechanisms
- Chemical buffers can tie up excess acids and bases only
temporarily, but they cannot eliminate them from the body. While
the lungs can dispose of carbonic acid by eliminating carbon
dioxide, Only the KIDNEYS can rid the body of other acids
generated. (although the kidneys act slowly and require hours or
days to bring about changes in blood pH, they are the most potent
of mechanisms for regulating blood pH).
- To maintain acid base balance, the kidneys:
- Excrete bicarbonate ions and
- Conserving (reabsorbing) or generating new bicarbonate
ions
- As blood pH rises, bicarbonate ions are excreted and hydrogen
ions are retained by the tubule cells. Conversely, when blood pH
falls, bicarbonate is reabsorbed and hydrogen ions are secreted.
Urine pH varies from 4.5-8.0, which reflects the ability of the
renal tubules to excrete basic or acid ions to maintain blood pH
homeostasis.
58. Development of the urinary and reproductive organs
- Thedevelopment of the urinary and reproductive organsis a part
of the prenatal development, and concerns the urinary system and
sex organs. The latter is a part of the stages of sexual
differentiation. The urinary and reproductive organs are developed
from the intermediate mesoderm. The permanent organs of the adult
are preceded by a set of structures which are purely embryonic, and
which with the exception of the ducts disappear almost entirely
before the end of fetal life. These embryonic structures are on
either side; the pronephros, the mesonephros and the metanephros of
the kidney, and the Wolffian and Mllerian ducts of the sex organ.
The pronephros disappears very early; the structural elements of
the mesonephros mostly degenerate, but the gonad is developed in
their place, with which the Wolffian duct remains as the duct in
males, and the Mllerian as that of the female. Some of the tubules
of the metanephros form part of the permanent kidney.
59.
- Intermediate mesodermis a type of mesoderm that is located
between the paraxial mesoderm and the lateral plate. It develops
into the part of the urogenitasystem (kidneys and gonads)
- forms of urogenital system
- series of short evaginations from each segment grows dorsally
caudally
- vestiges of the future kidney, the pronephros briefly
appears.
- pronephric duct arises in the intermediate mesoderm just
ventral to the anterior somites
- grows caudally until it becomes the cloaca
- it is distinct from the lateral mesoderm, as it is not
influenced by the secretion of BMP-4 by the ectoderm, possibly due
to the lack of receptors.
60.
- Pronephrosthe most primitive of the three excretory organs that
develop in vertebrate, corresponding to the first stage of kidney
development.
- The pronephros develops in the anterior nephrotomes of all
vertebrates. It is a paired organ, consisting of a series of
nephrons filtering urine from both the pericardium fluids via
openings called nephrostomes and blood from the glomerulus.
- The organ is active in adult forms of some primitive fish, like
lampreys or hagfish. It is present at the embryo of more advanced
fish and at the larval stage of amphibians. In human beings, it is
rudimentary, appears at the end of the third week (day 20) and
replaced by mesonephros after 3.5 weeks.
61.
- Themesonephros(Latin for "middle kidney") is one of three
excretory organs that develop in vertebrates. It serves as the main
excretory organ of aquatic vertebrates and as a temporary kidney in
higher vertebrates
62.
- TheWolffian duct(also known asarchinephric duct ,Leydig's duct
,mesonephric duct , ornephric duct ) is a paired organ found in
mammals including humans during embryogenesis.
- It connects the primitive kidney Wolffian body (ormesonephros )
to the cloaca and serves as the anlage for certain male
reproductive organs.
- In both the male and the female the Wolffian duct develops in
to the trigone of urinary bladder, a part of the bladder wall.
However, further development differentiates between the sexes in
the development of the urinary and reproductive organs.
63.
- In the female, in the absence of testosterone support, the
Wolffian ducts develop and wither.
- TheMllerian ducts(orparamesonephric ducts ) are paired ducts of
the embryo which run down the lateral sides of the urogenital ridge
and terminate at the mullerian eminence in the primitive urogenital
sinus. In the female, it will develop to form the fallopian tubes,
uterus, and the upper portion of the vagina. It is tissue of
mesodermal origin.
- Thegonadis the organ that makes gametes. The gonads in males
are the testes and the gonads in females are the ovaries. The
product, gametes, are haploid germ cells. For example, spermatozoon
and egg cells are gametes. Although medically the gonad term can
refer to either male gonads (testicles) or female gonads (ovaries),
the vernacular, or slang use of "gonads" (or "nads") usually only
refers to the testicles.
64. Sources
- Mader, S.S (2006)Inquiry into Life
- Marieb, E.N (2006)Essentials of Human Anatomy &
Physiology
- http://www.kidney.ca/page.asp?intNodeID=22132