Embed Size (px)
DESCRIPTION
Haematology revision lecture one of three. White blood cells
Citation preview

What are blood cells?• RBC– Bone marrow
• Proerythroblasts – large, nucleus– Peripheral
• Reticulocytes – no nucleus, contain RNA (Hb synthesis)• Erythrocytes – loose RNA
• WBC– Granulocytes
• Nphil, Bphil, Ephil– Agranulocytes (lymphocytes)
• Lymphocytes (B and T cells), macrophages• Platelets

Leucocytosis( WCC)
• Neutrophilia– Bacterial infection, (physiological stress, MPD, steroids)
• Lymphocytosis– Viral infection, (CLL, chronic infection e.g. TB, hepatitis)
• Eosinophilia– Allergies, parasites

Haematological malignancies1. Leukaemias– malignant cells in BM and blood
2. Lymphomas– malignant cells in LNs
3. MDS– dysplastic cells of all 3 lineages (erythrocytes, leucocytes,
thrombocytes)4. MPD– excess production of cells in BM
5. Myeloma– malignancy of plasma cells

Case 1• A 63 year old woman who always tries to look her best, had noticed some
swelling in the cervical region, and that her neck size had increased from 10 to 11 inches. Apart from that she felt well in herself.
• Blood tests done at the GP surgery showed the following:– Hb 12.1 g/dL (12-16)– WCC 97.0 x 109/L (3.5-9) (lymphocytes 98%, Nphil 2%)– Plts 197 x 109/L (150-450)
• She was referred privately to see a haematologist. What is the best therapeutic option?
A. Bone marrow transplantationB. Long term steroidsC. Combination chemotherapy with “CHOP”D. ObservationE. Oral cyclophosphamide

Leukaemias
• Def – malignant cells in BM and blood• Classification
1. Maturity• Acute – blasts in BM and blood, rapid onset• Chronic – excess mature cells in BM and blood
2. Lineage• Myeloid – granulocytes• Lymphoid – B or T cells

Leukaemias
• Classification– AML– ALL– CML– CLL
• General CFs• Lymphadenopathy, splenomegaly, systemic (malaise, wt loss)• BM failure - anaemia, leucopenia (infection), plt (bleeding)

AML(Acute myeloblastic leukaemia)
• Epi – Adults• Ix
– Auer rods (needles which are cytoplasmic granular clumps)• Rx – Chemo (cures 30%), BMT• Subtypes
• APML (acute promyelocytic leukaemia)– Def – Abnormal granulocyte precursors contain procoagulant material– Aet – t(15;17) – Fusion PML/RARα– Path – Interferes with myeloid differentiation– CF – Presents in DIC– Rx
– ATRA (remission), bld product support (plt, FFP)– Chemo (maintain remission)
– Prog – Good if don’t die from DIC

ALL(Acute lymphoblastic leukaemia)
• Epi – Child• Rx – Chemo (>80% cure), BMT• Prog – Good, boys do worse

CML(Chronic myelocytic leukaemia)
• Epi – Adult• Path
– Philadelphia chromosome – somatic mutation in a stem cell• t(9;22) – BCR/ABL tyrosine kinase, constitutively active, myeloid replication• (also in 1% AML, 5% ALL – bad prog)
• Progression1. Chronic phase (clonal proliferation)2. Accelerated phase ( WCC)3. Acute transformation ( blasts – rapidly fatal)
• Aet – Idiopathic (most), RT• CF – Massive splenomegaly• Ix – WCC, N, Ph chr (95%), BM hyperplasia• Complications
– Blast crisis (acute transformation – untreated within 10y, v. difficult to Tx)• Rx
– Imatinib (Gleevec) – bcr-abl tyr kinase inhibitor (persistent BCR/ABL but 90% remission)– Chemo, BMT (if imatinib fails)

CLL(Chronic lymphocytic leukaemia)
• Def – Indolent, incidental finding• Epi – elderly• Complications
• Autoimmune – Haemolytic anaemia, thrombocytopenia• Immunodeficiency – Clonal B cells suppress normal cells• Herpes zoster reactivation (shingles)• Richter’s large cell lymphoma – Transformation in LN (rare, serious)
• Classification• RAI
• 0 (lymphocytosis), I (lymphadenopathy), II (hepatosplenomegaly), III (anaemia), IV (thrombocytopenia)
• Binet• A (≤ 2 organs), B (≤ 5 organs), C (anaemia, thrombocytopenia)
• Rx– Incurable – No treatment required in most – die unrelated causes– If symptomatic
– Supportive – Early Abx in infec, annual influenza vacc, Fe, folate– Chemo– Prednisolone (improves cytopenia), Campath 1H (CD52 on mature lymphocytes), rituximab (CD20 on B cells)– Splenectomy
– Young – BMT

Case 1• A 63 year old woman who always tries to look her best, had noticed some
swelling in the cervical region, and that her neck size had increased from 10 to 11 inches. Apart from that she felt well in herself.
• Blood tests done at the GP surgery showed the following:– Hb 12.1 g/dL (12-16)– WCC 97.0 x 109/L (3.5-9) (lymphocytes 98%, Nphil 2%)– Plts 197 x 109/L (150-450)
• She was referred privately to see a haematologist. What is the best therapeutic option?
A. Bone marrow transplantationB. Long term steroidsC. Combination chemotherapy with “CHOP”D. ObservationE. Oral cyclophosphamide

Case 1
• D. Observation.• CLL is incurable. Most patients are diagnosed
incidentally. It is more common in elderly. Indications for Tx include BM failure, acute transformation, autoimmune complications

Case 2• A 54 year old man presented to his GP with 2 months of fatigue and non-
tender swellings in his groins.• On examination the GP discovered inguinal lymphadenopathy and mild
splenomegaly.• Blood tests revealed the following:
– Hb 9.8 g/dL (12-16)– WCC 315 x 109/L (3.5-9) (lymphocytes 8%, Nphil 92%)– Plt 190 x 109/L (150-450)
• Which of the following chromosomal translocations is pathognomic of this condition?
A. Translocation 8:14B. Translocation 9:22C. Translocation 15:17D. Translocation 14:18E. Translocation 2:8

Case 2
• B. t(9;22)• CML is unique amongst the haematological
malignancies in demonstrating a genetic rearrangement. The Philadelphia chromosome, a truncated Chr 22, is the hallmark. It represents a reciprocal translocation between Chr 9 and 22, and generates a new fusion gene, bcr-abl, a constitutively active tyrosine kinase. The Philadelphia Chr is present in 95% of cases
• t(8:14) is found in Burkitt's lymphoma• t(15:17) is found in APML

Case 3• Helen, a 24 year old Caucasian hairdresser born and bred in Essex, noticed some retrosternal
discomfort over the last few weeks. She also complained of a dry tickly cough, episodes of high fevers for a few days at a time, and has lost 1.5kg over the last month. Her chest pain was exacerbated when she was out drinking with friends.
• Her GP conducted a detailed examination and found generalised lymphadenopathy.• A CXR showed mediastinal lymphadenopathy.• Blood tests revealed the following:
– Hb 11.2 g/dL (12-16)– MCV 90 fl (80-95)– WCC 15 x 109/L (3.5-9) (98% lymphocytes)– Plt 600 x 109/L (150-450)– ESR 65 mm/h (0)
• What is the most likely diagnosis?A. Infectious mononucleosisB. ToxoplasmosisC. Hodgkin's lymphomaD. SarcoidosisE. Chronic lymphocytic leukaemia

Lymphomas
• Def – Malignant cells in LNs• Path – Classified by histology:• Hodgkin’s lymphoma• Non-Hodgkin’s lymphoma (NHL)
• Epi – Commoner than leukaemias• CF – Lymphadenopathy, B Sx

Hodgkin’s lymphoma
• Def – Lymphoma with orderly spread from LN to LN• Epi – Bimodal – Young adult (20y), elderly• Aet – Unknown – EBV genome in 80%• Grade (histology)
• Stage (clinical)– NB: A = no B Sx, B = B Sx (fever, night sweats, wt loss)

Hodgkin’s lymphoma
• CF– Painless lymphadenopathy – Cervical (70%), mediastinal
• Pain with ETOH
– B Sx
• Ix– Anaemia (normocytic), ESR/CRP, N/E– LN Bx
• Reed Sternberg cells – derived from B cells – large binucleated (owl’s eyes)
• Rx – Early (RT), Late (chemo), some (both)• Prog – Good – early cure rate >80%, B Sx worse prog

NHL• Def – Collection of lymphomas – 80% B cell, 20% T cell• CF
– Widespread painless lymphadenopathy, hepatosplenomegaly, B Sx– Unusual sites of presentation
• CNS (lymphoblastic), jaw (Burkitt’s), GIT (MALToma)
• Classification:

NHL• Ix– Pancytopenia, CRP and ESR– Blood film, paraprotein, staging CT, LN and BM Bx
• Rx– Single site – RT– Chemo
• Low grade (follicular, Waldenstroms) – single agent• High grade (DLBCL, Burkitt’s)
– Combination chemo, rituximab (CD20 on B cells)
– Specific• MALT lymphoma – H. pylori eradication
– BMT – graft vs leukaemia effect

Case 3• Helen, a 24 year old Caucasian hairdresser born and bred in Essex, noticed some retrosternal
discomfort over the last few weeks. She also complained of a dry tickly cough, episodes of high fevers for a few days at a time, and has lost 1.5kg over the last month. Her chest pain was exacerbated when she was out drinking with friends.
• Her GP conducted a detailed examination and found generalised lymphadenopathy.• A CXR showed mediastinal lymphadenopathy.• Blood tests revealed the following:
– Hb 11.2 g/dL (12-16)– MCV 90 fl (80-95)– WCC 15 x 109/L (3.5-9) (98% lymphocytes)– Plt 600 x 109/L (150-450)– ESR 65 mm/h (0)
• What is the most likely diagnosis?A. Infectious mononucleosisB. ToxoplasmosisC. Hodgkin's lymphomaD. SarcoidosisE. Chronic lymphocytic leukaemia

Case 3•C. Hodgkin's disease is malignancy of the lymphatic system. It has a
bimodal distribution, peaking in the 3rd decade and elderly. 70% present with mediastinal lymphadenopathy, and alcohol ingestion has been known to exacerbate sternal pain.
•The commonest subtype is Nodular sclerosing (60%).•HD is characterised by the presence of Reed Sternberg cells.•She has extensive disease (generalised lymphadenopathy) and would
require chemotherapy. Cure is achievable in up to 80%. •Sarcoidosis is common in black patients and can also present with
generalised lymphadenopathy.•CLL is more a disease of the elderly.

Case 4• A 75 year old man has noticed repeated spontaneous bleeding from his gums
lately. He had put it down to poor dentition. He also noticed he was becoming progressively more tired after moderate exertion. He presented to the local hospital where he was seen, and ultimately referred to the haematology registrar who requested some investigations.– Hb 9.6 g/dL (12-16)– MCV 107 fl (80-95)– WCC 1.47 x109/L (3.5-9)– Plt 56 x109/L (150-450)– Blood film: Pelger-Huet neutrophils– Haematinics: B12 and folate normal– Bone marrow biopsy: Normocellular marrow.
• What is the most likely diagnosis?A. Chronic lymphocytic leukaemiaB. Myelodysplastic syndromeC. Idiopathic thrombocytopenic purpuraD. Chronic myeloid leukaemiaE. Pernicious anaemia

Myelodysplasia (MDS)
• Def – Unusual clonal anaemias with abnormal mature cells• Epi – Elderly• Aet – Idiopathic, post-chemo• Path
– Hypercellular marrow, peripheral cytopenias (high apoptosis)– Cells – Abnormal form and function (RBCs, WBCs, plts)
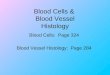
• Pelger-Huet neutrophils (bilobed, few granules)
– Genetic errors accumulate – Acute transformation (AML)
• Classification– NB: >20% blasts in BM is considered AML
Pelger-Huet neutrophils
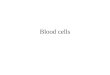
Ring sideroblasts

Myelodysplasia (MDS)
• Ix– Cytopenias ( Hb, leucopenia, plt)– Blood film, BM Bx
• Rx– Supportive• RBC Tx with iron chelation, plt Tx, early Abx in
neutropenic sepsis, EPO
– High risk – Chemo, BMT

Case 4• A 75 year old man has noticed repeated spontaneous bleeding from his gums
lately. He had put it down to poor dentition. He also noticed he was becoming progressively more tired after moderate exertion. He presented to the local hospital where he was seen, and ultimately referred to the haematology registrar who requested some investigations.– Hb 9.6 g/dL (12-16)– MCV 107 fl (80-95)– WCC 1.47 x109/L (3.5-9)– Plt 56 x109/L (150-450)– Blood film: Pelger-Huet neutrophils– Haematinics: B12 and folate normal– Bone marrow biopsy: Normocellular marrow.
• What is the most likely diagnosis?A. Chronic lymphocytic leukaemiaB. Myelodysplastic syndromeC. Idiopathic thrombocytopenic purpuraD. Chronic myeloid leukaemiaE. Pernicious anaemia

Case 4•B. MDS.•This patient has peripheral blood cytopenias. Thrombocytopenia causes
bleeding, anaemia causes fatigue. Neutropenia predisposes to infection. Blood film may show bilobed Pelger Huet neutrophils.
•CLL is characterised by anaemia and thrombocytopenia with lymphocytosis. •The normal haematinics exclude megaloblastic anaemia, and therefore
pernicious anaemia. CML would also have a Lymphocytosis.• ITP is an autoimmune thrombocytopenia where autoantibodies are formed
against platelets, which are then removed by the RES (spleen). In children it is often self limiting, occuring after viral infection. In adults it tends to run a chronic courses. It is treated by splenectomy and steroids.

Case 5• A 63 year old man presents to the accident and emergency department with chest pain and shortness
of breath. His ECG shows anterolateral ST segment depression. He is managed for acute coronary syndrome. A troponin 12 hours later was raised, at 0.5 ng/ml (<0.1).
• Over the last 3 months he had presented to his GP several times complaining of headaches, mild generalised itchiness and increasing fatigue and lethargy over the last month, but was frustrated by the GPs lack of interest.
• On examination he had a ruddy complexion and his blood pressure was 140/90. There was mild splenomegaly.
• Tests revealed the following:– Hb 22 g/dl (12-16)– WCC 15 x 10^9/L (3.5-9) (80% neutrophils)– Plt 525 x 10^9/L (150-450)– Bone marrow biopsy: Hypercellular
• What is the most likely diagnosis?A. Polycythaemia secondary to myocardial infarctionB. Chronic myeloid leukaemiaC. AtherosclerosisD. Polycythaemia rubra veraE. Antiphospholipid syndrome

Myeloproliferative disorders(MPD)
• Def – Clonal proliferation of one or more cell lines• Path– Often overlap (RBC, WBC, plts)– Cells morphologically normal
• Types– CML – Myelocytes (granulocyte leucocytes)– PRV – Erythrocytes– Essential thrombocythaemia – Thrombocytes– Myelofibrosis – Follows other MPD (e.g. PRV, ET)

Chronic myelocytic leukaemia(CML)
• Already done with leukaemias

Polycythaemia rubra vera(PRV)
• Def – Clonal proliferation of RBCs• Epi – Adult (50y)• Aet
– Apparent polycythaemia (normal RCM, PV) – dehydration– Absolute polycythaemia ( RCM)
• 1* polycythaemia (normal EPO)– PRV – JAK2 (nearly 100%)
• 2* polycythaemia ( EPO)– chronic hypoxia (COPD), EPO (renal cancer)
• CF– Plethora, pruritis (aquagenic – hot bath), headache, splenomegaly– Arterial and venous thrombosis (stroke, MI, DVT, PE)
• Ix – Hb, HCT, RCM, EPO normal• Rx – Venesection (500ml/wk until HCT 45%), CV risk (aspirin), chemo• Prog – Good• Complications – Myeofibrosis, acute transformation (AML)

Essential thrombocythaemia(ET)
• Def – Clonal proliferation of thrombocytes• Epi – elderly• Aet
– 1* thrombocytosis – ET – idiopathic (JAK2 often positive – 50%)– 2* thrombocytosis (reactive) – infec, inflam, bleeding
• CF– Arterial and venous thrombosis (stroke, MI, DVT, PE)– Bleeding (impaired plt func), splenomegaly
• Ix – plt• Rx
– Aspirin, observe– Thrombotic event:
• Hydroxyurea, Anagrelide (inhib plt maturation from megakaryocytes)• Prog – Good (10y survival 70%), few transform to AML, myelofibrosis

Myelofibrosis• Def – Clonal stem cells -> release GFs (PDGF), cytokines -> BM fibrosis• Epi – Elderly• Aet
– Follows other MPD (PRV, ET)– Idiopathic
• Path– BM fibrosis (pancytopenia)– Extramedullary haematopoiesis by spleen -> massive splenomegaly
• (Distinguish CML as no WCC)• (NB massive splenomegaly – MF, CML, leishmaniasis, Gaucher’s)
• CF – Massive splenomeg (abdo pain), pancytopenia (anaemia)• Ix
– Anaemia– Blood film: Leukoerythroblastic change, teardrop poikilocytes (almost pathognomic)– BM Bx – Aspirate (dry tap), trephine (fibrosis)
• Rx – Tx unsatisfactory – Splenectomy, RBC Tx, EPO• Prog – survival 4y

Case 5• A 63 year old man presents to the accident and emergency department with chest pain and shortness
of breath. His ECG shows anterolateral ST segment depression. He is managed for acute coronary syndrome. A troponin 12 hours later was raised, at 0.5 ng/ml (<0.1).
• Over the last 3 months he had presented to his GP several times complaining of headaches, mild generalised itchiness and increasing fatigue and lethargy over the last month, but was frustrated by the GPs lack of interest.
• On examination he had a ruddy complexion and his blood pressure was 140/90. There was mild splenomegaly.
• Tests revealed the following:– Hb 22 g/dl (12-16)– WCC 15 x 10^9/L (3.5-9) (80% neutrophils)– Plt 525 x 10^9/L (150-450)– Bone marrow biopsy: Hypercellular
• What is the most likely diagnosis?A. Polycythaemia secondary to myocardial infarctionB. Chronic myeloid leukaemiaC. AtherosclerosisD. Polycythaemia rubra veraE. Antiphospholipid syndrome

Case 5
• D. PRV.• PRV is a clonal proliferation of RBCs.
Polycythaemia can also be accompanied raised WCC and Plts too, thereby differentiating it from secondary polycythaemia. PRV often present with thrombosis, which can be arterial or venous. Other features include pruritis, worse after a hot bath, fatigue and haemorrhage.

Case 6• A 73 year old lady is brought to hospital by her neighbor who found her wandering in the street,
confused. She had been complaining of increasing back pain over the last few months and had recently been treated by her GP with oral antibiotics for two chest infections.
• A urine dipstick is normal.• Blood tests showed the following:
– Hb 9.8 g/dl (12-16)– MCV 90 fl (80-95)– WCC 7 x 109/L (3.5-9)– U 38 mmol/L (7-18)– Cr 210 mg/dL (50-90)– Ca 2.1 mmol/L (1-1.23)
• Spinal X-rays show several lumbar lytic lesions.• What is the most appropriate next investigation?
A. Renal ultrasound scanB. Bone marrow biopsyC. Serum and urine electrophoresisD. Bone scanE. 24 hour urinary protein collection

Multiple myeloma• Def – Clonal proliferation of plasma cells• Epi – Elderly• Path – Plasma cells secrete substances, infiltrate BM:
– Paraprotein – Single Ig type, normal Ig suppressed (immunoparesis)• BJ protein – can’t make complete Ig, only light chains – filtered by glomerulus• Renal failure – BJ proteins obstruct tubules
– Cytokines – Osteoclast activation – dissolve bone - Ca, pathological #
• CF – Bacterial infection, bone pain, pathological #, Ca (bones, stones, abdo, psychic)• Ix
– Anaemia, renal failure, Ca– Electrophoresis (serum, urine), XR skeletal survey (lytic lesions), BM Bx (excess plasma cells)
• Diagnosis– Serum or urine paraprotein– End-organ damage – CRAB ( Ca, renal, anaemia, bone lesions)– >10% clonal plasma cells in BM
• Rx– Young – Combination chemo, BMT (autologous stem cell)– Older (>70y) – single agent chemo, RT (e.g. vertebral), thalidomide (inhib cytokine release), bisphosphonate (reduce #)
• Prog – Most die of their disease (5y survival 35%). Only successful Tx is BMT in young

MGUS(Monoclonal gammopathy of uncertain significance)
• Def – Benign paraproteinaemia – incidental finding• Epi – Inc with age• Path – No other myeloma features• Rx – No Tx, monitor• Prog – 10% myeloma at 5y, 50% at 15y

Case 6• A 73 year old lady is brought to hospital by her neighbor who found her wandering in the street,
confused. She had been complaining of increasing back pain over the last few months and had recently been treated by her GP with oral antibiotics for two chest infections.
• A urine dipstick is normal.• Blood tests showed the following:
– Hb 9.8 g/dl (12-16)– MCV 90 fl (80-95)– WCC 7 x 109/L (3.5-9)– U 38 mmol/L (7-18)– Cr 210 mg/dL (50-90)– Ca 2.1 mmol/L (1-1.23)
• Spinal X-rays show several lumbar lytic lesions.• What is the most appropriate next investigation?
A. Renal ultrasound scanB. Bone marrow biopsyC. Serum and urine electrophoresisD. Bone scanE. 24 hour urinary protein collection

Case 6• C. Serum and urine electrophoresis• Multiple myeloma is a clonal proliferation of plasma cells. These produce a
paraprotein which can be detected by serum electrophoresis. Immunoglobulin light chains are filtered by the glomerulus and detected in in urine as Bence Jones proteins by urine electrophoresis. BJ proteins can obstruct renal tubules, causing renal failure.
• Confusion is caused by hypercalcaemia. The clonal plasma cells secrete factors activating osteoclasts. This also produces lytic lesions.
• Suppression of normal immunoglobulin synthesis predisposes to infection.• Diagnosis depends on demonstration of paraprotein, end organ damage,
and a BM biopsy showing excess plasma cells. The next most appropriate investigation is therefore protein electrophoresis, ahead of bone marrow biopsy.