Embed Size (px)
Citation preview

Dr D Mwale – Presenter
Prof Munkonge - Moderator

1. Introduction
2. Skin structure and function
3. Definitions
4. Classification of wound healing
5. Cellular basis of wound healing
6. Factors influencing wound healing
7. Outcomes of wound healing
8. Wound Care

Type of injury in which skin/epithelium is
torn,cut or punctured (open wound), or
where blunt force causes a contusion (a
closed wound)

1. According to the type of exposure to the
environment.
2. According to risk of sepsis.
3. Classification according to Velocity of
inflicting object.
4. Classification according to Inflicting
substance

wounds
open
incision
avulsion
abrasion
puncture
penetration
gunshot
laceration
closed
haematoma
contusion
Crush injury

1) Lacerations – Injury where tissue is cut or torn. For treatment, tissue is first cleansed of any blood clots and foreign material, derided and irrigated. Local anesthetic is administered and a traumatic technique of wound closure is employed, where wound margins are realigned with careful regard to prevention of any further crush injury to tissues. Sterile dressings are applied and immobilization is recommended for complex extremity wounds.
2.) Incision – wound cause by sharp edged instrument/object i.eknife resulting in a clean, regular edges.
3.) Contusions – Injuries resulting from a forceful blow to the skin and soft tissue, however leaving the outer layer of skin intact. These injuries generally require minimal care as there is no open wound. However, contusions should be evaluated for possible hematoma deep to the surface or other tissue injuries that may indicate more severe morbidity.
4.) Avulsions – Injuries where a section of tissue is torn off, either partially or in total. In partial avulsions, the tissue is elevated but remains attached to the body.
5.) Abrasions – Injury where a superficial layer of tissue is removed, as seen with 1st degree burns. The wound is cleansed of any foreign material, sometimes employing a scrub brush to prevent traumatic tattooing by dirt and gravel, and should be performed within the first day of injury.

6.)Puncture wounds - caused by an object puncturing the skin, such as a splinter, nail or needle.
7.)Penetration wounds - caused by an object such as a knife entering and coming out from the skin.
8.)Gunshot wounds - caused by a bullet or similar projectile driving into or through the body. There may be two wounds, one at the site of entry and one at the site of exit, generally referred to as a "through-and-through.
9.)Hematomas - also called a blood tumor, caused by damage to a blood vessel that in turn causes blood to collect under the skin.
• Hematomas that originate from internal blood vessel pathology are petechiae, purpura, and ecchymosis.The different classifications are based on size.
• Hematomas that originate from an external source of trauma are contusions, also commonly called bruises.
10.)Crush injury - caused by a great or extreme amount of force applied over a long period of time resulting in damage to overlying skin and underlying tissue such as bone,cartilage,muscle.






wound
Clean woundClean
contaminated wound
contaminated wound
Dirty wound

No viscus entry
No septic area
No break in aseptic technique
Such wounds if get infected risk = 3%

Operation enters a non infected area but
may encounter bacteria
Careful control of the area should result in
minimal spillage of organisms
E.g upper GIT surgery,Respiratory tract
infection
Infection rates = 10%

Gross spillaqge of organisms,where there
is infection already present but without pus
formation.
There is major break of aseptic technique
There is an open wound that has been
exposed for less than 4 hrs (i.e following
major trauma)
Infection risk > 30%
There is an operation in an infected area
(e.g peforated viscus,abscess or traumatic
wound) that has been exposed for over
4hrs.

Response of an organism to a physical disruption of a tissue/organ with an aim to repair or reconstitute the defect and to re-establish homeostasis.
Can be achieved by 2 processes: scar formation & tissue regeneration.
Dynamic balance between these 2 is different in different tissues.

During healing, a complex cascade of cellular events occur to achieve resurfacing, reconstitution and restoration of tensile strength of injured tissue.
4 classic but overlapping phases occur: I. HaemostasisII. Inflammation, III. Proliferation IV. Maturation/Remodeling..

1. Primary healing
2. secondary healing

feature Primary healing Secondary healing
cleaness clean Unclean
Infection Generally uninfected May be infected
Margins Surgically clean Irregular
Healing Scanty granulation tissue Granulation tissue fills
the wound gap
Healing period short Long
Healing direction Direct healing From the bottom to the
top
outcome Neat linear scar Contracted irregular
wound



Clot formation
Initiates inflammatory response
Transient vasoconstriction, platelet plugging,
fibrin clot formation
Controls bleeding, provides a framework for
cellular infiltrate support
Coagulation pathways activated leading to
fibrin formation
[ Please revisit lecture on Hemostasis]

Blood vessels are disrupted, resulting in
bleeding. Hemostasis is achieved by
formation of platelet plug & activation of
extrinsic & intrinsic clotting pathways.
Formation of a provisional fibrin matrix.
Recruitment of inflammatory cells into the
wound by potent chemoattractants.


Fibrin and fibronectin form a lattice that provides
scaffold for migration of inflammatory,
endothelial, and mesenchymal cells.
Neutrophilic infiltrate appears: removes dead
tissue & prevent infection.
Monocytes/macrophages follow neutrophils:
orchestrated production of growth factors &
phagocytosis.


Entry of lymphocytes.
Appearance of mast cell: aberrant
scarring?


i. Angiogenesis
ii. Fibroblast migration
iii. Granulation tissue formation (composed
of fibroblasts, macrophages and
emdothelial cells).
iv. Re-epithelialization (begins immediately
after injury)

Angiogenesis reconstructs vasculature in areas
damaged by wounding, stimulated by high
lactate levels, acidic pH, decreased O2 tension
in tissues.
Recruitment & assembly of bone marrow derived
progenitor cells by cytokines is the central
theme.
FGF-1 is most potent angiogenic stimulant
identified. Heparin important as cofactor, TGF-
alpha, beta, prostaglandins also stimulate.

Fibroblasts are the major mesenchymal cells involved in wound healing, although smooth muscle cells are also involved.
Macrophage products are chemotactic for fibroblasts. PDGF, EGF, TGF, IL-1, lymphocytes are as well.
Replacement of provisional fibrin matrix with type III collagen.


Basal cell layer thickening, elongation, detachment & migration via interaction with ECM proteins via integrin mediators.
Generation of a provisional BM which includes fibronectin, collagens type 1 and 5.
Epithelial cells proliferation contributes new cells to the monolayer. Contact inhibition when edges come together.



i. Programmed regression of blood vessels
& granulation tissue.
ii. Wound contraction.
iii. Collagen remodeling.

Begins approximately 4-5 days after wounding by action of myofibroblasts.
Represents centripetal movement of the wound edge towards the center of the wound.
Maximal contraction occurs for 12-15 days, although it will continue longer if wound remains open.
The wound edges move toward each other at an average rate of 0.6 to .75 mm/day.
Wound contraction depends on laxity of tissues, so a buttock wound will contract faster than a wound on the scalp or pretibial area.
Wound shape also a factor, square is faster than circular.

Contraction of a wound across a joint can
cause contracture.
Can be limited by skin grafts, full better
than split thickness.
The earlier the graft the less contraction.
Splints temporarily slow contraction.
Physiotherapy will reduce wound
contraction

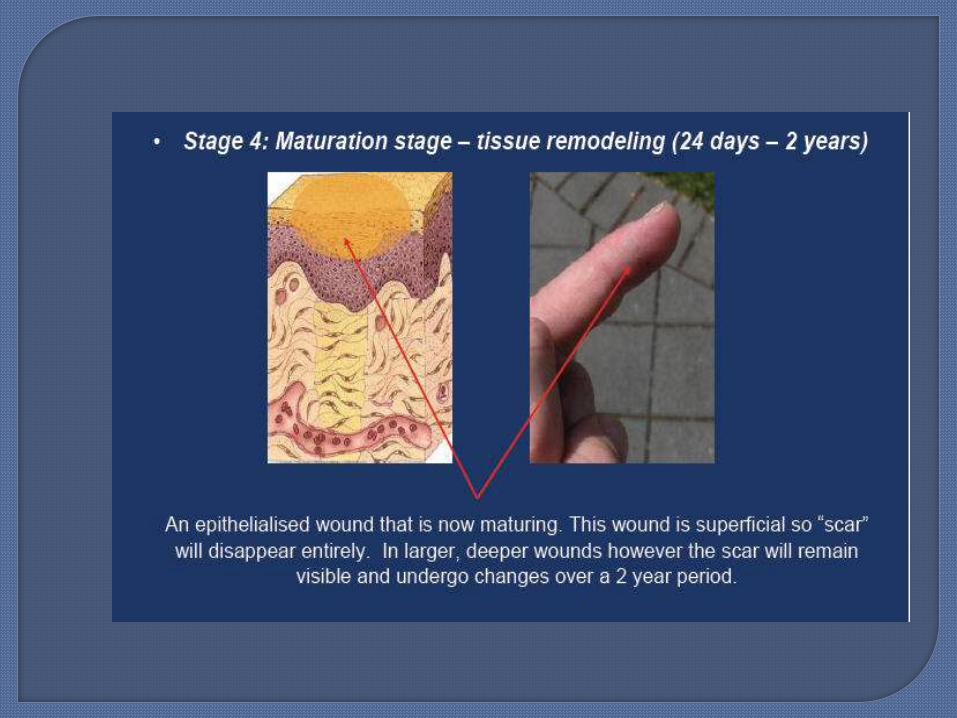
After 21 days, net accumulation of
collagen becomes stable. Bursting
strength is only 15% of normal at this
point. Remodeling dramatically increases
this.
3-6 weeks after wounding greatest rate of
increase, so at 6 weeks we are at 80% to
90% of eventual strength and at 6months
90% of skin breaking strength.

The number of intra and intermolecular cross-links between collagen fibers increases dramatically.
A major contributor to the increase in wound breaking strength.
Quantity of Type 3 collagen decreases replaced by Type 1 collagen
Remodeling continues for 12 mos, so scar revision should not be done prematurely.

19 types identified. Type 1(80-90%) most
common, found in all tissue. The primary
collagen in a healed wound.
Type 3(10-20%) seen in early phases of
wound healing. Type V smooth muscle,
Types 2,11 cartilage, Type 4 in BM.


Local factors
Systemic factors
Infection: impairs healing. Surgical Technique : type of sutures, suturing
tecnique,placement of incision, careful haemostasis
Wound tension : the higher tension the more difficult the healing – across Langer’s lines, near joints.
Radiation: endarteritis, abnormal fibroblasts. Foreign bodies – endogenous or exogenous
delay healing Blood supply: areas with poorer blood supply
healing is delayed i.e. pinna. Size

Nutrition status - Malnutrition Age – poor healing in old age, best healing in pre
and adolescent ages. Chronic diseases – Diabetes Mellitus(impaired
neutrophil chemotaxis, phagocytosis),cancers. Therapeutic drugs -Steroids and
immunosuppressants suppresses macrophage migration, fibroblast proliferation, collagen accumulation, and angiogenesis. Reversed by Vitamin A 25,000 IU per day.
Recreational Substances i.e. Smoking: increased platelet adhesiveness, decreased O2 carrying capacity of blood, abnormal collagen

Vitamin A- Fat soluble vitamin
- Maintains epithelial and cell membrane integrity
- Cofactor in collagen synthesis
- Deficiency results in decreased collagen synthesis and
decreased rates of epithelialisation
- Supplementation should be given in severe burns , major
trauma , oncotherapy , steroid therapy, stress ulcers, etc

Vitamin C
- Cofactor in collagen synthesis
- Deficiency leads to immature fibroblast and defective capillary
formation , increased susceptibility to wound infection and
reduced neutrophil function

Vitamin B complex- Eg Folic acid , pyridoxine , pentotheric acid - Cofactors in a variety of enzyme systems- Deficiency leads to impaired antibody formation and
function- Supplementation required severe injury and acute
illness
Vitamin D- Deficiency results in reduced bone strength and
retarded bone healing

Vitamin K- Used for synthesis of clotting factors and calcium building
proteins
Vitamin E- Powerful antioxidant
- Important in membrane stabilization
- Has antitumor and antiaging effects
- High doses inhibit wound healing
- Supplements should be stopped 1-3 weeks before planned
surgery

Wound healing
Normal
Incisional Hernia
Hypertrophic scar
Keloids
Inadequate regeneration
Inadequate scar formation
Infection
Dehiscence
Contractures

CNS injuries
Bone nonunion
Corneal ulcers

Diabetic foot ulcers.
Sacral pressure sores.
Venous stasis ulcers.

Excessive healing results in a raised, thickened scar, with both functional and cosmetic complications.
Hypertrophic scars develop soon after injury,
If it stays within margins of wound it is hypertrophic.
Hypertrophic scars more likely to cause contracture over joint surface also found in the presternal or deltoid area, wounds that cross langerhans lines.
Hypertrophic scars may subside in time

Keloids more familial. Dark
skinned, ages of 2-40.
Keloids scar tissue extends
beyond the confines of the
original injury due to
excessive fibroblasts and
collagen proliferation.
Keloids continue forming up
to a year later.
keloids rarely subside with
time.

Can occur in any wound
More common with delayed
(secondary)healing.
Contracture across a joint will cause
limited movement.
Avoid vertical incisions across joints.
Treatment : Skin grafting, Local flaps,
wound Z – plasty.


1. Optimize systemic parameters
2. Debride nonviable tissue
3. Reduce wound bioburden
4. Optimize blood flow
5. Reduce edema
6. Use dressings appropriately
7. Use pharmacologic therapy
8. Close wounds with grafts/flaps as indicated

Age: cannot be reversed, usage of growth factors, aggressive optimization of systemic parameters & supplementation.
Avoidance of ischemia & malnutrition.Correction of diabetes, removal of FB.Avoidance of steroids, alcohol, smoking.Avoidance of reperfusion injury: total
contact casting, compression therapy.
Surface irrigation with saline.
Debridement: surgical, enzymatic (papain with
urea, collagenase), mechanical (pressurized
water jet), autolytic, maggots.
Antibiotics: cellulitis, decreased rate of healing,
increased pain, straw colored oozing from skin,
contaminated wounds, mechanical implants.
Removal of FB.
Warmth
Hydration
Surgical revascularization
Hyperbaric O2 therapy: limb salvage.

Elevation CompressionNegative pressure wound therapy:
removes pericellular transudate & wound exudate as well as deleterious enzymes. Cannot be used in ischemic, badly infected or inadequately debrided wounds or in malignancy.

Absorption characteristics: none – films, low –hydrogels, moderate - hydrocolloids, high –foams, alginates, collagen.
Hydrogels (eg. starch) rehydrate wounds (benefit in small amounts of eschar, infected wounds).
Hydrocolloids promote wound debridement by autolysis.
Antimicrobial dressings: silver, cadexomer iodine, mupirocin, neomycin.

Autologous keratinocyte sheets. Biobrane Oasis Alloderm Integra (sites prone to contracture, coverage of
tendons, bone, surgical hardware) TransCyte Dermagraft Orcel

Antimicrobials
PDGF
EGF
VEGF
Vit A: steroid use
Absolutely of no use in normally healing
wounds
Radiation wounds require flaps.
Chronic nonhealing ulcers.
Extensive areas of ulceration.
Major soft tissue loss.
Other therapies: electrical stimulation for
recalcitrant ulcers.

Manuka honey (apitherapy) in venous leg ulcers.
Hyperbranched polyglycerol electrospun nanofibers.
Androstenediol in steroid inhibited healing.GM-CSF hydrogel in deep 2nd deg burns.LASER therapy enhances tissue repair?Nitric oxide containing nanoparticles.
MERRY CHRISTMAS AND A WONDERFUL
NEW YEAR !





























