Embed Size (px)
Citation preview

G l o m e r u l o n e p h r I t I s
HELLOK I D N E Y

ANATOMY OF MR KIDNEY
LET’S CHECK IT OUT!!!

GLOMERULUS

Functions of ME (MR.KIDNEY)
Without me, YOU will UNABLE to:
Remove wastes and water from the blood
Balanced chemicals in your body Release hormones Help to control blood pressure Help to produce red blood cells Produce vitamin D, which keeps
the bones strong and healthy

DEFINITION

What is glomerulonephristis?
Glomerulonephritis is
is a kidney condition
that involves damage
/inflammation to the
glomeruli.

Types of glomerulonephritis
Acute glomerulonephritis
- begins suddenly
Chronic glomerulonephritis
-develops gradually over
several years.

Approach to patient with glomerular disease

ACUTE GLOMERULONEPHRITIS (AGN)


Acute Glomerulonephritis
Acute glomerulonephritis (AGN) is an abrupt onset of one or more features of an Acute Nephritic Syndrome :• Oedema e.g. facial puffiness
• Microscopic / macroscopic haematuria
• Decreased urine output (oliguria)
• Hypertension
• Azotemia

Presenting features of AGN
Acute nephritic syndrome (most common)Nephrotic syndromeRapidly progressive glomerulonepritisHypertensive encephalopathyPulmonary oedemaSubclinical (detected on routine
examination)

Causes of Acute Nephritis
Post streptococcal AGNPost-infectious acute glomerulonephritis (other
than Grp A B-Haemolytic Stretococci)Subacute bacterial endocarditisHenoch- Schoelein Purpura IgA nephropathyHereditary nephritis SLESystemic vasculitis

ACUTE POST-STREPTOCOCCAL GLOMERULONEPHRITIS

In children, the commonest cause of acute nephritic syndrome is post-infectious AGN, mainly due to post-streptococcal infection of the pharynx or skin.
Post streptococcal AGN is commonest at 6-10 years age.
Definition
AGN that follows an infection with a nephritogenic strain of group A beta hemolytic streptococci.
The classic example of the acute nephritic syndrome.
Nelson Textbook of Pediatrics, 7th Edition

Streptococcal infection of the throat ( strep throat) or skin ( impetigo)

epiDemiology
Most commonly – sporadic.
Peak incidence - age 2-14 y/o, uncommon <3y/o.
Males are commonly affected than females.

etiology anD pathogenesis M types of streptococci (nephritogenic strains)
M types 47, 49, 55, 2, 60, and 57 - following impetigo
M types 1, 2, 4, 3, 25, 49, and 12 – pharyngitis
Incubation period:
2–6 weeks after skin infection
1–3 weeks after streptococcal pharyngitis.

etiology anD pathogenesis
Antibodies to streptoccocus (eg antistreptolysin O) are formed in the circulation
Antigen-antibody circulating immune complexes are subsequently deposited along the glomerular basement membrane (GBM).

Streptococcal infection
immune complex formation + deposited in GBM
complement system activated
immune injuries
cellular proliferation GBM fracture
capillary lumen narrowed hematuria
glomerular blood flow decreased proteinuria
oliguria GFR↓ distal sodium reabsorption
retention of water & sodium
blood volume ↑
edema hypertension
Low serum complement



light microscopenot specific for post streptococcal nephritis
•Glomeruli appear enlarged and hypercellular. •Diffuse mesangial cell proliferation with an increase in mesangial matrix.•Polymorphonuclear leukocytes are common in glomeruli during the early stage of the disease.

Deposits localize in the mesangium and along the capillary wall in a subepithelial pattern and stain dominantly for C3 and to a lesser extent for IgG

typical manifestation
1. Edema75% of the patientsFace, periorbital area lower extremities generalized
(ascites, pleural effusions)2. Proteinuria – usually normalize after 4 weeks3. Oliguria

Sign and symptoms
Kidney pain normally happens in the “flank” region, which is just below the bottom of rib cage.

Sign and symptoms
Cola-colored or diluted, iced-tea-colored urine from red blood cells in your urine (hematuria)
Foamy urine due to excess protein (proteinuria)

Sign and symptoms
High blood pressure (hypertension)
Fluid retention (edema) with swelling evident in your face, hands, feet and abdomen
Fatigue/SOB from anemia or kidney failure.
Less frequent urination than usual.
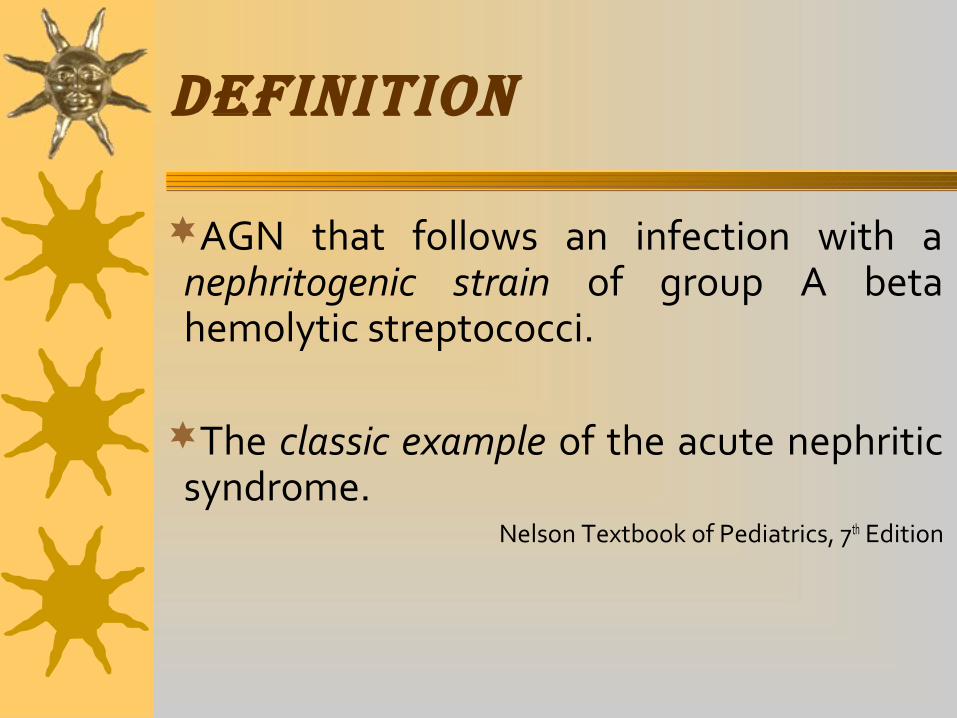
Clinical course
Spontaneous improvement typically begins within 1 wk
with resolution of edema in 5-10 days and hypertension
in 2-3 wk, but urinalysis may be abnormal (persistent
microscopic hematuria) for a year.

InvestIgatIons
Urinalysis and culture
• Haematuria – present in all patients.
• Proteinuria (trace to 2+, but may be in the
nephrotic range; usually associated with more
severe disease.)
• Red blood cell casts (pathognomonic of acute
glomerulonephritis).
• Other cellular casts.
• Pyuria may also be present.

InvestIgatIons
Urinalysis and culture
• Red blood cell casts (pathognomonic of acute
glomerulonephritis)
• Other cellular casts
• Pyuria may also be present

InvestIgatIons
Bacteriological and serological evidence of antecedent streptococcal infection:
• Raised ASOT ( > 200 IU/ml ).
• Increased anti-DNAse B (if available) – a
better serological marker of preceding
streptococcal skin infection.
• Throat swab or skin swab.

InvestIgatIons
Renal function test
• The BUN - elevated in 75% of patients,
• serum creatinine level is increased in one half of the patients
• Hyperkalemia, hypocalcaemia, hyponatremia, and metabolic acidosis are seen only in severe patients.
Full blood count
• A mild normochromic anemia may be present from
hemodilution and low-grade hemolysis.
• Leucocytosis may be present.

InvestIgatIons
Complement levels
• C3 level – low at onset of symptoms, normalizes by 6wks
• C4 is usually within normal limits in post-streptococcal
AGN.
Ultrasound of the kidneys
• Not necessary if patient has clear cut acute nephritic
syndrome.

IndIcatIons for renal BIopsy Severe acute renal failure requiring dialysis. Features suggesting non post-infectious AGN as the
cause of acute nephritis. Delayed resolution
• Oliguria > 2 weeks
• Azotaemia > 3 weeks
• Gross haematuria > 3 weeks
• Persistent proteinuria > 6 months

dIagnosIs
Acute onsetSymptoms: edema, oliguria, dark urine,
hypertensionUrinalysis: RBCs, protein, castsEvidences of streptococcal infection:
– Elevated serum titers of Abs to streptozymes(ASO)
Serum C3 - Reduced

Lupus
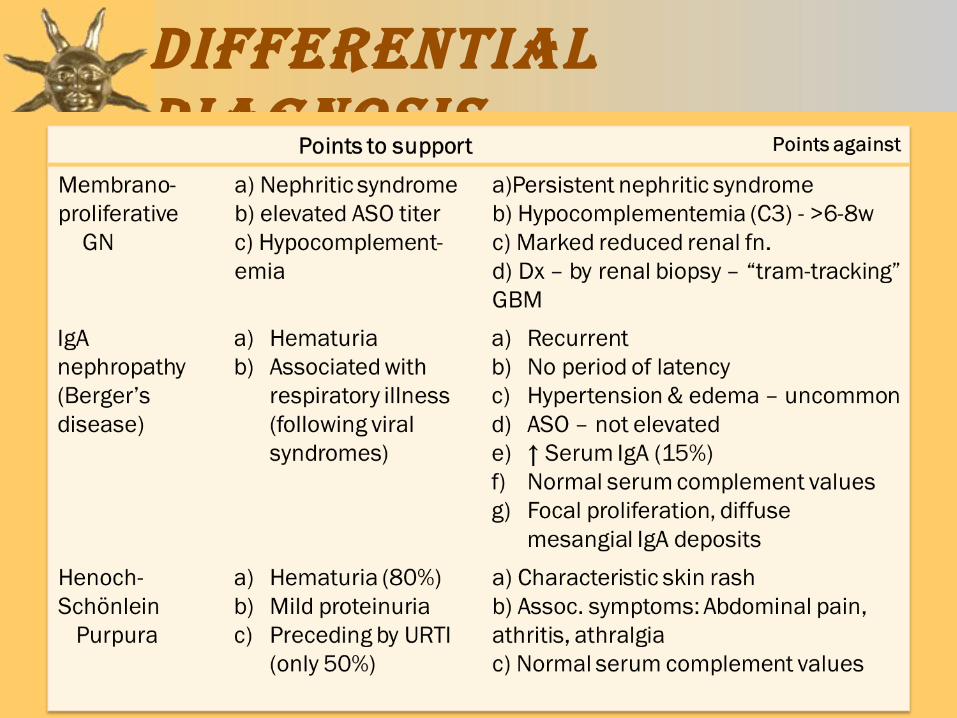
dIfferentIal dIagnosIs

dIfferentIal dIagnosIs

ManageMent
Strict monitoring - fluid intake, urine output, daily weight, BP (Nephrotic chart)
Penicillin V for 10 days (give erythromycin if penicillin is contraindicated)
Fluid restriction

MANAGEMENT
Diuretic (e.g. Frusemide) should be given in children with pulmonary oedema.
Diet – no added salt to diet.
COMPLICATIONS
Look out for complications of post-streptococcal AGN:
• Hypertensive encephalopathy usually presenting with seizures
• Pulmonary oedema (acute left ventricular failure)
• Acute renal failure
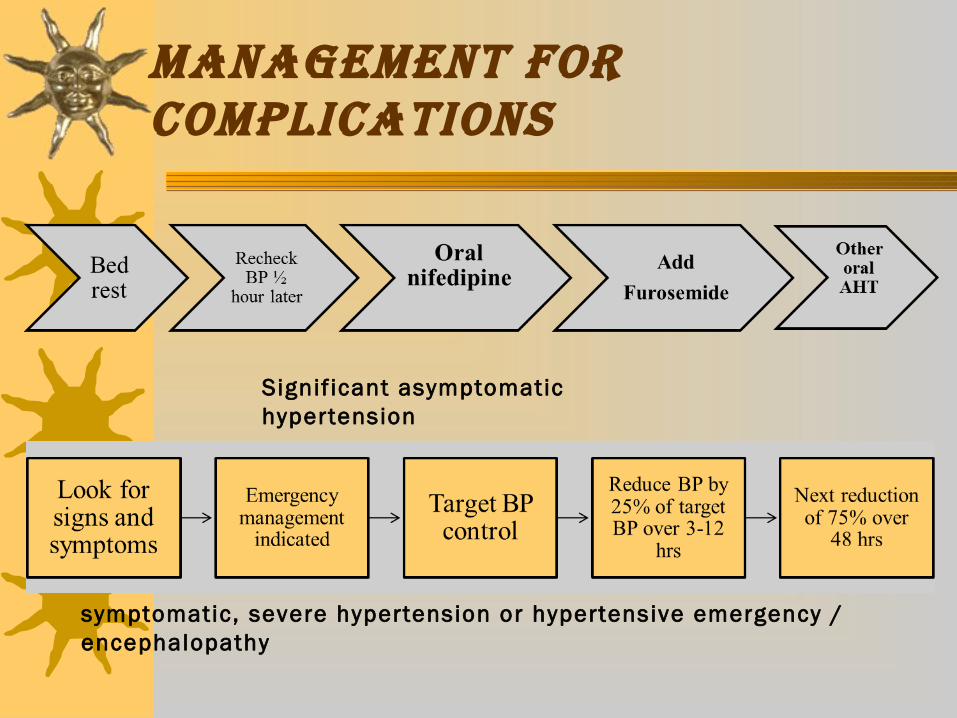
MANAGEMENT fOr COMPLICATIONS
Signif icant asymptomatic hypertension
symptomatic, severe hypertension or hypertensive emergency / encephalopathy


Prehypertension is defined as a blood pressure in at least the 90th percentile, but less than the 95th percentile, for age, sex, and height, or a measurement of 120/80 mm Hg or greater.
Hypertension is defined as blood pressure in the 95th percentile or greater.


Acute pulmonary edema
MANAGEMENT fOr COMPLICATIONS

MANAGEMENT fOr COMPLICATIONS
Acute Renal Failure

fOLLOw-uP
For at least 1 year. Monitor BP at every visit Do urinalysis and renal function to
evaluate recovery. Repeat C3 levels 6 weeks later if not
already normalised by the time of discharge.

OuTCOME
Short term outcome: Excellent, mortality <0.5%.
Long term outcome: 1.8% of children develop chronic kidney disease following post streptococcal AGN.
These children should be referred to the paediatric nephrologists for further evaluation and management.

KIDNEY SAY !!!!
Thanks for watching