Embed Size (px)
Citation preview

Common glomerular disease
Kajohnsak Noppakun, MDAssistant Professor of Medicine
Renal DivisionDepartment of Internal Medicine
Chiang Mai University1
•Isolated proteinuria / hematuria•Glomerular diseases commonly presented with nephrotic syndrome
•Glomerular diseases commonly presented with nephritic syndrome
SCOPE
2
A 56-yr-old woman is found to have normochromic normocytic anemia, renal insufficiency (serum creatinine of 2.6 mg/dl), proteinuria (1+ by dipstick), hypophosphatemia, hypouricemia, and glucosuria. Urine protein excretion was 3.1 g/day.Which ONE of the following is the MOST likely cause of this constellation of findings?
A. Diabetic nephropathyB. Lead intoxicationC. Aristolochic acid intoxicationD. Multiple myelomaE. AL amyloidosis
3
•Overproduction (overflow proteinuria) e.g., multiple myeloma, lymphomas, (amyloidosis)
•Tubular proteinuria e.g., Fanconi syndrome, interstitial disease
•Glomerular proteinuria i.e., glomerular disease
Proteinuria
4

•Thin basement membrane disease•Ig A nephropathy•Hereditary nephritis (Alport syndrome)
Isolated hematuria•Lower tract: ureter, bladder, prostate•Kidney: cystic disease, renal cell carcinoma, hypercalciuria, renal vein thrombosis, interstitial nephritis
•Glomerular disease – dysmorphic RBCs, RBC cast, no clot
5
•“Benign familial hematuria”•Mutation of COL4A3 or COL4A4 •Autosomal dominant transmission •Age at presentation: any age•Hematuria (persistent or intermittent), no/mild - HTN, proteinuria, renal impairment•No deafness, no ocular change
•Differentiate with carrier state of Alport syndrome in female
Thin basement membrane disease
6
•Mutation of COL4A5 •X-linked recessive transmission (majority, 85%) •Age at presentation: children or young adult (male), any age (female)
•Males: hematuria, proteinuria and HTN, ESRD at age 30 (70%), deafness (30-50%), ocular defect (15-30%) (pathognomonic: anterior lenticonus, “dot and fleck” retinopathy)
•Females: microscopic hematuria without progression, renal impairment (25%)
•Diagnosis: absent of α5-subunit of type IV collagen in epidermal basement membrane (and kidney)
Alport syndrome
7
“Anterior lenticonus”
Ocular manifestations in Alport syndrome
Savige J, et al. Kidney Int 2003;64:1169.
“Dot and fleck” retinopathy
8

•Autoimmune disease: SLE, RA, MCTD, PSS, HSP (including Ig AN), small vessel vasculitides, cryoglobulinemia
•Infections: HBV, HCV, HIV, malaria, schistosomiasis, syphilis, PSGN, IE, shunt nephritis
•Drugs: NSAIDs, pamidronate, bevacizumab, mercury, gold, penicillamine, heroin, captopril, lithium, interferon-α
Secondary causes of nephrotic syndrome•Malignancies: solid tumors (lung, colon, stomach, breast, cervix, kidney, thyroid, ovary, prostate), hematologic tumors (HD, NHL, CLL)
•Metabolic disease: diabetes, amyloidosis
•Miscellaneous: bee sting, preeclampsia, transplant glomerulopathy, renal artery stenosis, morbid obesity, vesicoureteral reflux
Bolds are the common causes of nephrotic syndrome; italics are the causes usually present with nephritic syndrome9
Alternative pathway (C3)
Classical pathway (C4)
Lupus nephritis ↓ ↓Membranoproliferative GN (type I) ↓ ↓Dense deposit disease (Membranoproliferative GN type II) ↓ ↔Cryoglobulinemia ↔ , ↓ ↓Post-streptococcal GN ↓ ↔ , mildly ↓Infective endocarditis ↓ ↔Shunt nephritis ↓ ↔HBV/HCV-associated GN ↔ , ↓ ↔ , ↓Atheroembolic disease ↓ ↔
Complements: First test to do
10
Hematuria Hypertension Renal impairment Children Uncommon Uncommon Uncommon Adults 20% 10% ~20% (age >60 y)
Minimal change disease•10-15% of 1º NS in adults (70-90% in children)•Clinical features: 100% nephrotic (abrupt onset), mean proteinuria 10 g/d
•Mechanisms of renal insufficiency: intrarenal hemodynamic or intrarenal edema (nephrosarca)
•Common associated conditions:•Drugs: NSAIDs, lithium, interferon-α•Malignancies: Hodgkin’s disease, CLL•Miscellaneous: viral infection, allergies, bee sting
11
•Treatment: prednisolone 1 mg/kg/d at a daily single dose (response: children 90-95%, adults 80-85%) (1C), minimum period 4 weeks / maximum period 16 weeks (2C), and tapered slowly over a total period of up to 6 mo (2D)•CYC or CNIs (cyclosporine and tacrolimus) for patients with relative contraindications or intolerance to steroids (2D)
Minimal change disease•Pathogenesis: abnormal regulation of T cell subset
2012 KDIGO Clinical Practice Guideline for Glomerulonephritis.
Foot process effacement
12

•The most common cause of 1º NS in adult Thais???
•Clinical features: the incidence of hematuria, hypertension, or renal impairment is higher than that of in minimal change disease (but how much???, 10-20%?)
•No associated condition reported•Pathogenesis: abnormal regulation of T cell subset•Treatment: steroids, 16-20 wk (response ~50?? to 80%)
Ig M nephropathy
Vanikar A. J Nephropathology. 2013;2:98-103.13
•Increasing incidence (~1/3 in adults)•Clinical features: nephrotic 90%•Hematuria 60-80%, HTN 80%, renal impairment ~80%
•Pathogenesis: podocyte injury, permeability factor (soluble urokinase-type plasminogen activator receptor, suPAR)
Focal segmental glomerulosclerosis
2012 KDIGO Clinical Practice Guideline for Glomerulonephritis.
Perihilar Tip lesions Collapsing Cellular
14
•Associated conditions: •HIV infection, parvovirus B19•Heroin, pamidronate, interferon-α •Glomerulomegaly — morbid obesity, cyanotic heart disease
•Reduced nephron number — single kidney, reflux nephropathy
•50% developed ESRD in 6-8 years•Treatment: as in MCD (response 20-45%), however, CNIs be considered as first line therapy for patients with relative contraindications or intolerance to steroids
Focal segmental glomerulosclerosis
2012 KDIGO Clinical Practice Guideline for Glomerulonephritis.15
•One of the most common cause of NS in adults (~30%), peak incidence 30-50 years
•Secondary causes (25-30% of cases):•Autoimmune diseases e.g., SLE, autoimmune thyroiditis, myasthenia gravis
•Infection e.g., HBV, HCV, malaria, syphilis, leprosy•Drug e.g., penicillamine, gold, mercury•Malignancy e.g., lung, prostate, stomach, breast, colon•Incidence is significantly higher (9-12 times)•20-30% of patients who are older than 60 years •~50% are asymptomatic•Median diagnosis time after MN is 60 mo (usually 12 mo)
Membranous nephropathy
16

•Clinical features: nephrotic 80%, ↑risk of thrombosis•Hematuria 50%, HTN 50%, renal impairment <10%
•Pathogenesis: subepithelial immune deposits•Antigen: M-type phospholipase A2 receptor (PLA2R) — for primary MN, sensitivity 75%, specificity 100%
• 1/3 each: spontaneous remission, relapsing, renal failure
• Consider treatment if persistent high-grade proteinuria (>4 g/d) despite at least 6 mo of conservative management
• Treatment: 6-mo course of alternating monthly cycles of oral and IV steroids and oral CYC (1B) or CNIs monotherapy (1C)• Steroid monotherapy not be used
Membranous nephropathy
2012 KDIGO Clinical Practice Guideline for Glomerulonephritis.17
A 68-year-old woman noticed bilateral lower extremity edema. Her past medical history included 50 pack-years of cigarette smoking with ongoing tobacco abuse. Her vital signs (including BP) were normal. Laboratory workup revealed 10 g/d proteinuria, creatinine of 0.7 mg/dl, total cholesterol of 350 mg/dl, and albumin of 2.6 g/dl. The following tests were negative/normal: ANA, C3 and C4, hepatitis B and C. A renal biopsy revealed membranous nephropathy.What is the most appropriate next step in managing this patient?
A. Request serologic testing for anti-M-type phospholipase receptor (anti-PLA2R) antibodies
B. Request IF staining of the biopsy for anti-PLA2R antibodiesC. Start prophylactic anticoagulation with warfarinD. Arrange age- and risk factor-appropriate cancer screeningE. Recommend first-line immunosuppressive therapy of
steroids+alkylating agent18
•Etiologic factors:•Urinary loss of anticoagulants (antithrombin III, protein S) and fibrinolytics (plasminogen)
•Hepatic overproduction in response to hypoalbuminemia — factor V, factor VIII, fibrinogen
•Increased synthesis of platelet proaggregants —thromboxane A2
•MN is at the greatest risk — unknown reason•Risk increased significantly when serum albumin <2.8 g/dl•Prophylaxis (suggestion???): depends on serum albumin•<2.0 g/dl — LMWH or low-dose warfarin•2.0-3.0 g/dl — low dose aspirin
Hypercoagulable state in NS
Bomback AS, et al. Clin J Am Soc Nephrol 2015;10:ccc–ccc. 19
•Uncommon in adults•Clinical features: nephrotic 60%•Hematuria (60-80%), HTN (80%), renal impairment (~80%), rapid deterioration in renal function (25%)
•70% hypocomplementemia (C3 in all and C4 in some)•50% developed ESRD at 10 years•Pathophysiologic classification: subepithelial immune deposits, membrane splitting•Immune-complex mediated: chronic infections (hepatitis C and B, endocarditis, shunt nephritis), autoimmune diseases, monoclonal gammopathies
•Complement mediated: dysregulation of the alternative complement pathway due to mutations or autoantibodies
Membranoproliferative GN
Sethi S and Fervenza FC. N Engl J Med 2012;366:1119-31. 20

DDD, dense deposit disease; MPGN membranoproliferative GN
Granular IF staining for immunoglobulin and C3
Membranoproliferative GN by LM
Granular IF staining for C3 with little or no immunoglobulin
Immune complex MPGN C3 glomerulpathy
Infectious MPGN
•Treatment: treat secondary causes; (if progressive decline of kidney function) CYC or MMF plus low-dose steroids for less than 6 mo• Plasmapheresis, rituximab, plasma infusion, or eculizumab
Autoimmune MPGN
Monoclonal MPGN
Dense deposit disease
C3 glomerulpathy
Evidence for infection e.g., HCV, (HBV),
IE, shunt nephritis
Evidence for autoimmune disease e.g.,
SLE, cryoglobulinemia
Evidence for monoclonal
immunoglobulin
GBM dense deposits by EM
No GBM dense deposits by EM - dysregulation of
alternative complement pathway
21
•Secondary (AA, serum amyloid A): chronic infection/inflammation – RA (40%), AS and psoriatic arthritis (10%)
Renal amyloidosis•Positive Congo red, “apple green appearance”: kidney or liver (90%), abdominal fat (70%)
•Primary (AL, light chains): lambda 75%, MM 10-20%, age >50 •Kidney (50%): proteinuria (80%), nephrotic syndrome (30%), renal impairment (20%), rare hematuria, pRTA
•Heart (40%): restrictive cardiomyopathy•Neuromuscular (≤25%): neuropathy, orthostatic hypotension•Hepatomegaly (25%), macroglossia (10%), purpura (15%)•Treatment: melphalan + pred (30% effectiveness) ± HSCT
•Rare cardiac involvement, NS (common), ESRD 40-60%•Treatment: treat underlying disease
22
•Proteinuria (non-nephrotic or nephrotic), normal renal function, hematuria (uncommon)
•Low complement levels (~20%)•Chronic HBV (positive HBsAg) •Mildly elevated AST and ALT (~100-200 IU/L)•Treatment: interferon-! or nucleoside analogues (1C)
HBV-associated GN•Membranous nephropathy (followed by MPGN)
2012 KDIGO Clinical Practice Guideline for Glomerulonephritis.
•Renal artery aneurysms or renal infarction•ACR criteria: “Presence of HBsAg or Ab in serum”
•HBV-associated polyarteritis nodosa
23
•MPGN with/without mixed cryoglobulinemia (type II) (followed by membranous nephropathy)
•Nephrotic syndrome, hematuria (common), impaired renal function (common)
•Low complement levels (50-90%) and positive cryoglobulinemia (~60-70%)
•Transaminitis in most patients•50% showed extrarenal manifestations: vasculitic purpura, arthralgia, and neuropathy
•Treatment: pegylated interferon + ribavirin (2C)•Cryoglobulinemia: plasmapheresis, rituximab, or CYC, in conjunction with IV methylprednisolone (2D)
HCV-associated GN
2012 KDIGO Clinical Practice Guideline for Glomerulonephritis.24

A 50-year-old obese woman with a 5-year history of hypertension controlled by enalapril is being evaluated because of proteinuria. Physical examination disclosed obese woman, BP 130/80 mmHg, and trace pedal edema. Laboratory: creatinine 1.4 mg/dl, BUN 18 mg/dl; urinalysis: pH 5.0, protein 3+, no glucose, RBC 10-20/hpf. Urine protein 5.9 gm/day. A renal biopsy demonstrates that 60% of the glomeruli have segmental scarring.The most likely diagnosis is:
A. Hypertensive nephrosclerosisB. Primary focal and segmental sclerosisC. Secondary focal and segmental sclerosis D. Membranous nephropathyE. Crescentic glomerulonephritis
25
A 20-year-old female in excellent health suddenly develops periorbital and pretibial edema. Three weeks ago, she went to Loi Krathong Festival and developed a respiratory tract infection, from which she has now recovered. On PE, BP is 150/100 mmHg. There are crackles in both lung bases and bilateral tibial pitting edema. Laboratory studies reveal low C3 and normal C4, BUN 30 mg/dl, serum creatinine 1.5 mg/dl, serum albumin 3.8 mg/dl. Urinalysis reveals no protein, RBC casts, and dysmorphic RBCs.Which ONE of the following is the MOST likely diagnosis?
A. Ig A nephropathyB. Goodpasture’s syndromeC. ANCA-associated small vessel vasculitisD. Post-infectious glomerulonephritisE. Systemic lupus erythematosus nephritis
26
• Poststreptococcal glomerulonephritis• Infective endocarditis• Ig A nephropathy• Lupus nephritis • Goodpasture disease/anti-GBM disease • Small vessel vasculitides:
Glomerular diseases with predominant nephritic syndrome
• Wegener’s granulomatosis (granulomatosis with polyangiitis, GPA)
• Microscopic polyangiitis (MPA)
• Churg-Strauss syndrome (eosinophilic granulomatosis with polyangiitis, EGPA)
• Henoch-Schonlein purpura (Ig A vasculitis)
• Cryoglobulinemic vasculitis27
Post-streptococcal GN•Antigen:•Streptococcal pyrogenic exotoxin B (SPEB) generated by proteolysis of a zymogen precursor (zSPEB)
•Nephritis-associated plasmin receptor (NAPlr)
•Latent period: •Pharyngitis (1-3 weeks)•Impetigo (2-6 weeks)
•Streptococcus group A (nephritogenic strains) particularly M type 12
Supepithelial hump
28

•Wide spectrum of severity: abrupt onset of edema (>90%), proteinuria and hematuria (100%)•Gross hematuria (30%), nephrotic-range proteinuria (20%)•Hypertension (>75%)•Transient oliguria (50%), creatinine >2 mg/dl (20%, 60% in patients >55 years), RPGN (<5%)
•Clinical manifestations typically resolve within 1-2 wk•In children, complete resolution of hematuria and proteinuria in 3-6 weeks, ESRD (~1%)
•In adults, may not have complete recovery and high incidence ESRD in elderly
•Treatment: supportive•No evidence that early treatment of streptococcal disease will alter the risk of glomerulonephritis
Post-streptococcal GN
29
•Positive throat/skin cultures: inconsistently present (10-70%)
•Positive antistreptolysin O (30%), anti-DNAse B (70%), or antihyaluronidase (40%)•Positive rheumatoid factor (30-40%), cryoglobulins and circulating immune complexes (60-70%), and MPO-ANCA (10%)
•Reduced C3 and CH50 (>90%) which returns to normal within 6-8 wk, normal or mildly reduced C4•Persistent hypocomplementemia: MPGN, IE, LN, occult infection, atheroembolic disease
Post-streptococcal GN
30
•Renal complications in IE: embolic infarcts, renal abscesses, and GN
•~20% of IE patients developed GN•Acute kidney injury (80%) •Hematuria (97%), proteinuria 80-90% (nephrotic 5%)
•Low C3 (50%), C4 (20%)•Positive ANCA (30%)•Organisms: S. aureus (53%), Streptococcus species (23%)
•Treatment: appropriate antibiotics
Endocarditis-associated GN
Boils CL, et al. Kidney Int online publication, 21 January 2015; doi:10.1038/ki.2014.424.31
A 36-year-old woman is found to have intermittent hematuria and proteinuria (2+ by dipstick). There is no family history of renal disease. Her BP is 150/92 mmHg, and serum creatinine is 1.4 mg/dl. A urine protein-to-creatinine ratio is 1.2 g/g. Serum albumin and C3 complement are normal; ANA level is 1:40.Which ONE of the following is the MOST likely to be present on further study?
A. Elevated serum levels of C-reactive proteinB. Elevated serum levels of undergalactosylated Ig A1C. Reduced serum levels of C4D. Decreased ratio of Ig A to C3 in serumE. Elevated serum levels of Ig A
32

Ig A nephropathy
•Male preponderance, a peak incidence in the 2nd and 3rd decades of life, and rare familial clustering
•Associated disease: SNSA especially AS, cirrhosis, HIV, dermatitis herpetiformis, Crohn’s disease, celiac disease, mycosis fungoides, leprosy, relapsing polychondritis, and Sjögren’s syndrome
•One of, if not the, most common glomerular disease (30% in Asia Pacific, 20% in southern Europe)
•Serum Ig A levels do not correlate with disease: increased in 20-50% of patient
Mesangial Ig A deposit
33
Pathogenic Ig A molecule: aberrantly glycosylated Ig A1
Coppo R, et al. Kidney Int 2004;65:1544.
Reduced galactose (Gal) and/or sialic acid (Neu5Ac) and increased exposure of
N-acetylgalactosamine (GalNAc)
34
Ig A nephropathy: Clinical features
ESRD: 1-2%/yr,(overall) 25% in
10-25 yrs
•Diagnosis: serum Ig A?, Ig A-fibronectin?, increased Ig A to C3 ratio, abnormally glycosylated Ig A1
40-50%, synpharyngitic nephritis30-40%, ± proteinuria
35
•Pathology: Oxford-MEST classification (Mesangial hypercellularity, Endocapillary proliferation, Segmental sclerosis, Tubular atrophy/interstitial fibrosis)
•Persistent microscopic hematuria (compared to recurrent gross hematuria)•AKI associated with macroscopic hematuria does not affect long term prognosis
Ig A nephropathy: Poor prognostic factors
•Older age at disease onset•Sustained hypertension•Persistent proteinuria (>1 g/d) or nephrotic syndrome•Impaired renal function
36

Floege, J. & Feehally, J. Nat Rev Nephrol 2013;9:320–327. 2012 KDIGO Clinical Practice Guideline for Glomerulonephritis, Floege, J. & Feehally, J. Nat Rev Nephrol 2013;9:320–327.
Ig A nephropathy: Treatment•Macroscopic hematuria with normal renal function
•Aggressive hydration (no role of antibiotics or tonsillectomy)Low risk
Microscopic hematuria ± proteinuria ≥0.5 g/day, GFR normal, no HTN
Intermediate riskProteinuria >0.5-1 g/day ± reduced GFR ± HTN
High riskAcute or rapid loss of GFR
Annual or Bi-annual screeningfor at least 10 years
Optimized supportive therapyFor 3-6 months
• RAAS blockade titrated as far as tolerated to achieve proteinuria <1 g/d (2C)• BP <130/80 mmHg if proteinuria <1 g/d and <125/75 mmHg if proteinuria >1
g/day (Not graded)
GFR >50 ml/min/1.73 m2
GFR 30-50 ml/min/1.73 m2
GFR <30 ml/min/1.73 m2
Proteinuria <1 g/day and GFR stable
Proteinuria >1 g/day ± GFR decline
Continue supportive therapy
Continue supportive therapy
Continue supportive therapy
Value of immunosuppression
unknownCritically weigh pros and cons
Continue supportive therapy
No immunosuppression
(except if RPGN)
+ 6-mo course of steroids± fish oil???
Nephrotic syndrome or
crescentic GN with RPGN
course
AKI due to macroscopic
hematuria
Continue supportive therapy
+ Immuno-suppression
(steroids + cyclophosphamide)
Supportive therapy
Renal biopsy is mandatory if AKI persists >5 day
37
T h e n e w e ngl a nd j o u r na l o f m e dic i n e
n engl j med 373;23 nejm.org December 3, 2015 2225
The authors’ affiliations are listed in the Appendix. Address reprint requests to Dr. Floege at the Division of Nephrol-ogy and Clinical Immunology, RWTH Aachen University, Pauwelsstr. 30, 52057 Aachen, Germany, or at juergen . floege@ rwth-aachen . de.
* A complete list of participating centers and investigators in the Supportive Ver-sus Immunosuppressive Therapy for the Treatment of Progressive IgA Nephrop-athy (STOP-IgAN) trial is provided in the Supplementary Appendix, available at NEJM.org.
Drs. Rauen and Eitner contributed equally to this article.
N Engl J Med 2015;373:2225-36.DOI: 10.1056/NEJMoa1415463Copyright © 2015 Massachusetts Medical Society.
BACKGROUNDThe outcomes of immunosuppressive therapy, when added to supportive care, in patients with IgA nephropathy are uncertain.METHODSWe conducted a multicenter, open-label, randomized, controlled trial with a two-group, parallel, group-sequential design. During a 6-month run-in phase, supportive care (in particular, blockade of the renin–angiotensin system) was adjusted on the basis of pro-teinuria. Patients who had persistent proteinuria with urinary protein excretion of at least 0.75 g per day were randomly assigned to receive supportive care alone (supportive-care group) or supportive care plus immunosuppressive therapy (immunosuppression group) for 3 years. The primary end points in hierarchical order were full clinical remission at the end of the trial (protein-to-creatinine ratio <0.2 [with both protein and creatinine measured in grams] and a decrease in the estimated glomerular filtration rate [eGFR] of <5 ml per minute per 1.73 m2 of body-surface area from baseline) and a decrease in the eGFR of at least 15 ml per minute per 1.73 m2 at the end of the trial. The primary end points were analyzed with the use of logistic-regression models.RESULTSThe run-in phase was completed by 309 of 337 patients. The proteinuria level decreased to less than 0.75 g of urinary protein excretion per day in 94 patients. Of the remaining 162 patients who consented to undergo randomization, 80 were assigned to the supportive-care group, and 82 to the immunosuppression group. After 3 years, 4 patients (5%) in the supportive-care group, as compared with 14 (17%) in the immunosuppression group, had a full clinical remission (P = 0.01). A total of 22 patients (28%) in the supportive-care group and 21 (26%) in the immunosuppression group had a decrease in the eGFR of at least 15 ml per minute per 1.73 m2 (P = 0.75). There was no significant difference in the annual decline in eGFR between the two groups. More patients in the immunosuppres-sion group than in the supportive-care group had severe infections, impaired glucose tolerance, and weight gain of more than 5 kg in the first year of treatment. One patient in the immunosuppression group died of sepsis.CONCLUSIONSThe addition of immunosuppressive therapy to intensive supportive care in patients with high-risk IgA nephropathy did not significantly improve the outcome, and during the 3-year study phase, more adverse effects were observed among the patients who received immu-nosuppressive therapy, with no change in the rate of decrease in the eGFR. (Funded by the German Federal Ministry of Education and Research; STOP-IgAN ClinicalTrials.gov number, NCT00554502.)
A BS TR AC T
Intensive Supportive Care plus Immunosuppression in IgA Nephropathy
Thomas Rauen, M.D., Frank Eitner, M.D., Christina Fitzner, M.Sc., Claudia Sommerer, M.D., Martin Zeier, M.D., Britta Otte, M.D., Ulf Panzer, M.D.,
Harm Peters, M.D., Urs Benck, M.D., Peter R. Mertens, M.D., Uwe Kuhlmann, M.D., Oliver Witzke, M.D., Oliver Gross, M.D.,
Volker Vielhauer, M.D., Johannes F.E. Mann, M.D., Ralf-Dieter Hilgers, Ph.D., and Jürgen Floege, M.D., for the STOP-IgAN Investigators*
Original Article
The New England Journal of Medicine Downloaded from nejm.org at CHIANG MAI UNIVERSITY on February 25, 2016. For personal use only. No other uses without permission.
Copyright © 2015 Massachusetts Medical Society. All rights reserved.
n engl j med 373;23 nejm.org December 3, 2015 2231
Supportive Care plus Immunosuppression in IgA Nephropathy
in the immunosuppression group, 1.15; 95% confidence interval, 0.62 to 2.14; P = 0.66).
Secondary End PointsNo significant differences were observed between the supportive-care group and the immunosup-pression group at the end of the trial phase with respect to the mean absolute change in eGFR, the mean annual change in the slope of the re-ciprocal of serum creatinine concentration, the number of patients with a decrease in the eGFR of at least 30 ml per minute per 1.73 m2, and the number of patients with the onset of end-stage renal disease (Table 2).
Twelve months after randomization, patients in the immunosuppression group had a signifi-cantly lower mean proteinuria level than did those in the supportive-care group (Table 2). At month 36, the difference was no longer signifi-
cant. Microhematuria, as assessed by means of a urine dipstick or sediment test, was noted in 87% of the patients at baseline (67 in the sup-portive-care group and 74 in the immunosup-pression group). Among these patients, micro-hematuria was no longer present in 9 in the supportive-care group and in 24 in the immuno-suppression group at the end of the study (P = 0.004). In the immunosuppression group, more patients receiving glucocorticoid mono-therapy than those receiving combination immu-nosuppressive therapy had remission of protein-uria, hematuria, or both (see Table S2 in the Supplementary Appendix).
The time courses of blood pressure levels, eGFR, and proteinuria are shown in Figure S1 in the Supplementary Appendix. Values were simi-lar in the two study groups over the 3-year trial phase.
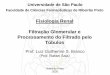
Figure 2. Primary End Points.
Panel A shows the first primary end point: full clinical remission at the end of the 3-year trial phase (protein-to-creati-nine ratio <0.2 [with both protein and creatinine measured in grams] and a decrease in the estimated glomerular filtra-tion rate [eGFR] of <5 ml per minute per 1.73 m2 of body-surface area from baseline). Panel B shows the second pri-mary end point: a decrease in the eGFR of at least 15 ml per minute per 1.73 m2 during the trial phase. A subgroup analysis was performed for both end points with the use of a full-analysis set and an available-case analysis set. In the full-analysis set, missing values in all events in all patients who underwent randomization were substituted by the worst clinical case (i.e., no clinical remission and decrease in the eGFR of at least 15 ml per minute per 1.73 m2); in the available-case analysis set, only documented events among patients with available data were included in the analysis.
Supportive Care plusImmunosuppression
Better
Supportive CareBetter
SupportiveCare
Better
Full-analysis setAvailable-case analysis
SupportiveCare
Supportive Care plusImmunosuppression Odds Ratio (95% CI)
Odds Ratio (95% CI)
Subgroup
4.82 (1.43–16.30)5.38 (1.55–18.66)
P Value
4/804/72
14/8214/71
0.010.008
no. of events/total no.
A In Full Clinical Remission
SupportiveCare�plusImmuno-
suppressionBetter
Full-analysis setAvailable-case analysis
SupportiveCare
Supportive Care plusImmunosuppressionSubgroup
0.89 (0.44–1.81)0.89 (0.41–1.90)
P Value
22/8018/76
21/8217/78
0.750.76
no. of events/total no.
B eGFR Decrease ≥15 ml/min/1.73 m2
0.50.25 1 2 5 10 20
0.50.25 1 2 5 10 20
The New England Journal of Medicine Downloaded from nejm.org on December 10, 2015. For personal use only. No other uses without permission.
Copyright © 2015 Massachusetts Medical Society. All rights reserved.
STOP-Ig A nephropathy trials
Rauen T, et al. N Engl J Med 2015;373:2225-36.
n engl j med 373;23 nejm.org December 3, 2015 2231
Supportive Care plus Immunosuppression in IgA Nephropathy
in the immunosuppression group, 1.15; 95% confidence interval, 0.62 to 2.14; P = 0.66).
Secondary End PointsNo significant differences were observed between the supportive-care group and the immunosup-pression group at the end of the trial phase with respect to the mean absolute change in eGFR, the mean annual change in the slope of the re-ciprocal of serum creatinine concentration, the number of patients with a decrease in the eGFR of at least 30 ml per minute per 1.73 m2, and the number of patients with the onset of end-stage renal disease (Table 2).
Twelve months after randomization, patients in the immunosuppression group had a signifi-cantly lower mean proteinuria level than did those in the supportive-care group (Table 2). At month 36, the difference was no longer signifi-
cant. Microhematuria, as assessed by means of a urine dipstick or sediment test, was noted in 87% of the patients at baseline (67 in the sup-portive-care group and 74 in the immunosup-pression group). Among these patients, micro-hematuria was no longer present in 9 in the supportive-care group and in 24 in the immuno-suppression group at the end of the study (P = 0.004). In the immunosuppression group, more patients receiving glucocorticoid mono-therapy than those receiving combination immu-nosuppressive therapy had remission of protein-uria, hematuria, or both (see Table S2 in the Supplementary Appendix).
The time courses of blood pressure levels, eGFR, and proteinuria are shown in Figure S1 in the Supplementary Appendix. Values were simi-lar in the two study groups over the 3-year trial phase.
Figure 2. Primary End Points.
Panel A shows the first primary end point: full clinical remission at the end of the 3-year trial phase (protein-to-creati-nine ratio <0.2 [with both protein and creatinine measured in grams] and a decrease in the estimated glomerular filtra-tion rate [eGFR] of <5 ml per minute per 1.73 m2 of body-surface area from baseline). Panel B shows the second pri-mary end point: a decrease in the eGFR of at least 15 ml per minute per 1.73 m2 during the trial phase. A subgroup analysis was performed for both end points with the use of a full-analysis set and an available-case analysis set. In the full-analysis set, missing values in all events in all patients who underwent randomization were substituted by the worst clinical case (i.e., no clinical remission and decrease in the eGFR of at least 15 ml per minute per 1.73 m2); in the available-case analysis set, only documented events among patients with available data were included in the analysis.
Supportive Care plusImmunosuppression
Better
Supportive CareBetter
SupportiveCare
Better
Full-analysis setAvailable-case analysis
SupportiveCare
Supportive Care plusImmunosuppression Odds Ratio (95% CI)
Odds Ratio (95% CI)
Subgroup
4.82 (1.43–16.30)5.38 (1.55–18.66)
P Value
4/804/72
14/8214/71
0.010.008
no. of events/total no.
A In Full Clinical Remission
SupportiveCare�plusImmuno-
suppressionBetter
Full-analysis setAvailable-case analysis
SupportiveCare
Supportive Care plusImmunosuppressionSubgroup
0.89 (0.44–1.81)0.89 (0.41–1.90)
P Value
22/8018/76
21/8217/78
0.750.76
no. of events/total no.
B eGFR Decrease ≥15 ml/min/1.73 m2
0.50.25 1 2 5 10 20
0.50.25 1 2 5 10 20
The New England Journal of Medicine Downloaded from nejm.org on December 10, 2015. For personal use only. No other uses without permission.
Copyright © 2015 Massachusetts Medical Society. All rights reserved.
Lower BP <125/75 mmHg~30% on both ACEIs + ARBs
(UPCI <0.2 + ↓eGFR <5 ml/min/1.73 m2)
38
• 30-50% of SLE patients have renal disease at the time of diagnosis•60% of adults and 80% of children develop renal
disease at some point of their diseases• Risk for severe nephritis: children, males, non-
Caucasian• Anti-dsDNA correlates best with renal disease• ~5-10% positive for MPO-ANCA• Monitoring: anti-dsDNA, complement, ESR,
dysmorphic RBCs• Dialysis and transplantation
Lupus nephritis
39
Class Description ClinicalI Minimal mesangial LN Minimal renal manifestation,
rare nephrotic-range proteinuria, and normal creatinine II Mesangial proliferative LN
III(A, A/C, C)
Focal proliferative LN (<50% of glomeruli)
Varied course: HTN, active sediments, nephrotic-range proteinuria (25-33%) and ↑creatinine (25%)
IV(A, A/C, C)
Diffuse proliferative LN (≥50% of glomeruli) – segmental (IV-S) or global (IV-G)
↑Anti-dsDNA Ab, ↓complement levels, HTN, active sediments, nephrotic- range proteinuria (50%), and ↑creatinine
V Membranous LN Uncommon HTN and renal dysfunction, nephrotic-range proteinuria (60%)
VI Sclerotic nephritis ↑Creatinine
Lupus nephritis: 2004 ISN/RPS classification
Active lesions: endocapillary hypercellularity with or without leukocyte infiltration; karyorrhexis; fibrinoid necrosis, rupture of GBM; crescents, cellular or fibrocellular; subendothelial deposits (wireloops); intraluminal immune aggregates (hyaline thrombi)Chronic lesions: glomerular sclerosis (segmental, global); fibrous adhesions; fibrous crescents
40

Treatment schema for lupus nephritisClass IV with crescents/
with impaired renal functionClass III, IV, (V) without crescents/
without impaired renal function
Induction protocolOral prednisolone 0.5-1 mg/kg/d, WITH1) MMF (1.5-2 g/day) x 6 mo, OR2) Pulse cyclophosphamide 0.5-1 g/m2 monthly
(NIH) x 6 mo ORPulse cyclophosphamide 500 mg q 2 wk (EuroLupus) x 6 doses ±
3) Pulse methylprednisolone 0.5-1 g x 1-3 d at the start of therapy
4) Cyclosporine/Tacrolimus may be used in class V
Induction protocolPulse methylprednisolone 1 g x 3 d followed by oral prednisolone 0.5-1 mg/kg/d WITHPulse cyclophosphamide 0.5-1 g/m2 monthly x 6 mo
Response Resistance
Maintenance protocolLow dose prednisolone 0.125-0.5 mg/kg/d, WITH1) MMF (1-2 g/d), OR2) Azathioprine (1-2 mg/kg/d) OR3) [Pulse cyclophosphamide 0.5-1 g/m2 q 3 mo x
2 yr]
Switch to alternating agentsCyclophosphamide in place of MMF or vice versa ORRituximab OR plasma exchange OR IVIG
Mittal T and Rathi M. Int J Rhem Dis 2014;17:834-844.41
Management of lupus nephritis in AsiaMild or
moderate disease
(e.g., class II)
Severe disease
(Class III/IV±V or class V with
significant proteinuria)
• Initial treatment with moderate-dose steroids or in combination with AZA or mycophenolate
• Antimalarial treatment unless contraindicated
• Initial treatment with steroids (PRED 0.8 mg/kg/d) and either mycophenolate or CYC (IV or PO)
• Pulse MP (0.5-1 g/d) for 3 d recommended when renal biopsy shows crescentic involvement >10% or evidence of deteriorating renal function
• Steroid tapering begins after 2 wk except in patients with no sign of improvement, aiming to reach <20 mg/d after 3 mo and ≤7.5 mg/d after 6 mo
• IV CYC advisable when compliance doubtful• Mycophenolate dose during induction should be 1.5-2 g/d for at least 24 wk• CNI (in particular tacrolimus, on which there is more data) to be considered:
• As induction, in combination with steroids in patients who do not tolerate standard treatment
• As maintenance, especially in patients with membranous features on biopsy and persistent proteinuria after induction phase
• Immunosuppressive treatment recommended for (pure) class V with proteinuria ≥2 g/d
Yap D and Chan TM. Int J Rhem Dis 2014;17:834-844.42
•General treatment: all patients of any class are treated with hydroxychloroquine (2C)
•Systemic lupus and thrombotic microangiopathy•APS: anticoagulation (target INR 2-3) (2D)•TTP: plasma exchange (2D)
•Systemic lupus and pregnancy•Delay pregnancy until complete remission (2D)•CYC, MMF, ACEI, or ARBs should not be used (1A)•Hydroxychloroquine can be continued (2B)•Switch MMF to AZA (1B)•Steroids or AZA should not be tapered during pregnancy or for at least 3 mo after delivery (2D)
•Low-dose aspirin to decrease the risk of fetal loss (2C)
Lupus nephritis: Treatment
2012 KDIGO Clinical Practice Guideline for Glomerulonephritis.43
A 32-yr-old man develops acute kidney injury. PE is unremarkable with BP 130/82 mmHg. His medications include aspirin and omeprazole. Serum creatinine 5.2 mg/dl, and leukocyte and differential count are normal. The kidneys are of normal size as determined by ultrasound. Urinalysis reveals 1+ protein, 3-5 RBCs/hpf, 10-12 WBCs/hpf and a few granular casts, no bacteria or eosinophils found.Which ONE of the following is the MOST likely cause of his acute kidney injury?
A. Acute tubular necrosisB. Microscopic polyangiitisC. Ig A nephropathyD. Acute hypersensitivity interstitial nephritisE. Anti-GBM-mediated crescentic nephritis
44

Rapidly progressive GN (RPGN)
45
•Acute interstitial nephritis•Acute tubular necrosis•Scleroderma•Malignant hypertension•Light chain nephropathy•TTP/HUS•Renal vein thrombosis•Renal artery obstruction•Thromboembolic renal disease
Pseudo-RPGN!!!
Bolton KW. Nephrology 1995;1:257-268.
Chronic GN
46
Immune complex: Granular deposit
Pauci-immune: No deposit
Anti-GBM: Linear deposit
47
Category Immunopathogenesis Primary renal disease
Systemic disease
I. Anti-GBM mediated, rare
Circulating anti-GBM Ab and glomerular linear Ig G deposit
Anti-GBM Ab disease Complicating DN or MN
Goodpasture's disease
II. Immune complex mediated, 80%
Circulating immune complex and granular Ig G deposit
Post-infectious GN Ig A nephropathy Membranous GN MPGN
Lupus nephritis Henoch-Schonlein purpura Cryoglobulinemic vasculitis
III. Pauci-immune, 20%
No glomerular deposit
A. ANCA positive (80-90%) [30%]ANCA-positive GN (PR3-ANCA, 30%) (MPO-ANCA, 70%)
[70%]Wegener granulomatosis Microscopic polyangiitis Churg-Strauss syndrome
B. ANCA negative (10-20%) Idiopathic crescentic GN
RPGN is just a syndrome
48

DDD, dense deposit disease; EGPA, eosinophilic granulomatosis with polyangiitis; GBM, glomerular basement membrane; GPA, granulomatosis with polyangiitis; MPA, microscopic polyangiitis; MPGN, membranoproliferative glomerulonephritis.
Crescentic GN
Anti-GBM disease
Linear GBM immunoglobulin
IF staining
Granular IF staining for C3
and immunoglobulin
Granular IF staining for C3 and no or little
immunoglobulin
Paucity of IF staining for
immunoglobulin and complement
No lung hemorrhage
Lung hemorrhage
Immune complex GN
C3 glomerulopathy ANCA disease
Anti-GBM GN
Goodpasture’s syndrome
DDD C3 GN ANCA GN
MPA GPA EGPA
Dense deposits in GBM
No dense deposits in GBM
No systemic vasculitis
Vasculitis without
granulomas or asthma
Vasculitis with
granulomas, no asthma
Vasculitis with
granulomas, and asthma
Ig AN Ig A vasculitis
Lupus nephritis
Post infectious GN
Immune complex MPGN
Membranous GN
Other immune complex GN
Dominant Ig A and
no vasculitis
Dominant Ig A and vasculitis
SLE Acute strep or staph
infection
Thick capillaries and hypercellularity
Other features
Thick capillaries, no hypercellularity
49
•Two peaks of incidence:•Young men in the late 20s, more often with pulmonary hemorrhage (usually smoker)
•Women > men in the late 60-70s, more often with renal-limited disease
•The Goodpasture epitope: non-collagenous (NC1) domain of the α3 chain of collagen type IV•Environmental factors (hydrocarbons, tobacco, infections, and endogenous oxidants) can expose the epitopes
Anti-GBM disease
50
•Abrupt onset of GN, severe oliguria ± pulmonary hemorrhage •Anti-GBM Ab: positive in 95% of patients•MPO-ANCA: positive in 10-15% → better prognosis
•Poor prognostic factors: serum creatinine is >5-6 mg/dl, oliguria, and need for dialysis
•Treatment: steroids + CYC + plasmapheresis except those who are dialysis-dependent at presentation and do not have pulmonary hemorrhage (1B)•No maintenance immunosuppressive therapy (1D)
•Renal survival 60%, patient survival 85%•Recurrent disease is rare
Anti-GBM disease
2012 KDIGO Clinical Practice Guideline for Glomerulonephritis.51
•Anti-neutrophilic cytoplasmic autoantibodies: proteinase-3 (PR3), myeloperoxidase (MPO), lysosomal membrane protein-2 (LAMP-2)•Sensitivity: 81-91%; specificity: 70-90%
•Relapses occur in up to 40% of patients•High risk of relapse:•PR3-ANCA (compared to MPO-ANCA) •Upper respiratory tract or lung involvement (compared to ANCA associated GN alone)
ANCA-associated GN
52

Cytoplasmic (c)-ANCA: Proteinase 3
Perinuclear(p)-ANCA: Myeloperoxidase
IF ANCA ELISA Disease c-ANCA Anti-PR3 + Wegner granulomatosis p-ANCA Anti-MPO + Microscopic polyangiitis
Churg-Strauss syndromeRenal-limited ANCA vasculitisAnti-GBM diseaseDrug-induced e.g., PTU, methimazole
Anti-MPO - Chron diseaseUlcerative colitisChronic active hepatitisPrimary sclerosing cholangitisPrimary biliary cirrhosisChronic arthritides
53
WG, Wegener’s granulomatosis (granulomatosis with polyangiitis, GPA); MPA, microscopic polyangiitis; CSS, Churg-Strauss syndrome (eosinophilic granulomatosis with polyangiitis, EGPA).
ANCA in small vessel vasculitidesWG MPA CSS Renal-limited
PR3-ANCA 70-80 25-30 30-40 20-30MPO-ANCA 5-10 45-55 40-50 60-70Negative ANCA 10-20 20-30 20-40 10-20
• Specificity of PR3-ANCA for WG, 98-99% • PR3-ANCA is seen in >90% of patients with diffuse WG, but in only ~50%
with limited WG (limited = typically no renal involvement)
54
•MPO-ANCA•Strongest association: PTU, hydralazine and minocycline
•Arthralgia/arthritis, cutaneous vasculitis, crescentic GN and pulmonary hemorrhage
•PTU-induced ANCA•Usually take medication for months or years•27% of patients receiving long-term treatment with PTU developed MPO-ANCA
Drug-induced ANCA
55
•Necrotizing granulomatous inflammation primarily involved upper and lower respiratory tracts and GN
•Mean age: 40-60 years•Upper respiratory tract (>90%): sinusitis, nasal discharge, nasal ulcer, nasal septum perforation
•Lung (75%): nodules (±cavitation), hemorrhage•Kidney (50-95%): GN, proteinuria (0.5-1 g/d)•Eye (65%): uveitis, conjunctivitis, retro-bulbar inflammation
•Skin (40%): purpura, nodules, livedo reticularis•Relapse after achieving remission is more common than the other ANCA-associated vasculitis
Wegener’s granulomatosis
56

•Mean age: 50 years•The most common cause of pulmonary renal syndrome??
•Kidney (80-100%): mostly RPGN, rare nephrotic •Upper respiratory tract (not typical)•Lung (60%): alveolar hemorrhage, pulmonary nodules (not typical)•CXR: patchy or diffused infiltration
•Biopsy: non-granulomatous inflammation
Microscopic polyangiitis
57
•Initial therapy: CYC and steroids (1A)•Rituximab and steroids as an alternatives in patients without severe disease or in whom CYC is contraindicated (1B)
•Plasmapheresis: patients requiring… •Dialysis or with rapidly increasing creatinine (1C), or •Diffuse pulmonary hemorrhage (2C)
•Maintenance therapy: at least 18 mo (2D)•Agents: AZA (1B), or MMF (2C), or MTX (1C)•TMP-SMX as an adjunct to maintenance therapy in patients with upper respiratory tract disease (2B)
•Monitoring: not changing immunosuppression based on changes in ANCA titer alone (2D)
ANCA-associated GN: Treatment
2012 KDIGO Clinical Practice Guideline for Glomerulonephritis.58
A 42-year-old man has a 3-week history of progressive dyspnea and coughing up blood. He has a long history of chronic rhinitis. On PE, BP is 150/90 and his chest has scattered crackles. BUN 62, creatinine 3.1 mg/dl, hemoglobin 10.5 gm/dl. Urinalysis: 2+ protein, no glucose, 15-20 RBCs/hpf, 5-7 WBCs/hpf. Chest x-ray: diffuse bilateral patchy infiltrates. Renal biopsy demonstrates cellular crescents with negative immunofluorescence.Which of the following statements is correct?
A. PR3-ANCA is likely to be positiveB. Plasmapheresis should be initiated immediatelyC. Anti-GBM antibody is likely to be positiveD. This patient is likely to have a significant eosinophiliaE. Complement levels will be low
59
• Diagnosis: pathology (Ig A positive vasculitis)
• Prognosis: excellent (children), ~10% ESRD (adults)
• Treatment: if persistent proteinuria >1 g/d after ACEIs/ARBs and GFR >50 ml/min/1.73 m2, be treated with a 6-month course of steroids (2D)
Henoch-SchÖnlein purpura•Skin purpura from the waist
down (almost 100%), GI tract (25-90%: abdominal pain, GI bleeding), joints, and GN (20-100%)
•Young age (<20 years), preceding infection, and abdominal complaints•More severe renal disease in older children and adults
2012 KDIGO Clinical Practice Guideline for Glomerulonephritis.60

•Cryoglobulins: circulating immunoglobulins that precipitate upon cooling and resolubilize on warming
•Type I (10-15%): monoclonal Ig M or Ig G, associated with lymphoproliferative disorders
•Mixed cryoglobulinemia:•Type II (50-60%): monoclonal Ig M rheumatoid factor attached polyclonal Ig G, associated with HCV
•Type III (25-30%): polyclonal Ig M rheumatoid factor and polyclonal Ig G, 1/2 associated with HCV, 1/2 associated with autoimmune disease (e.g, SLE) or lymphoproliferative disorders
Cryoglobulinemic vasculitis
Ferri C. Orphanet J Rare Dis 2008;3:25.61
•Purpuric-vasculitic skin lesions (90-95%) and ulceration (10-25%), hepatosplenomegaly with abnormal LFT (70-75%) and peripheral neuropathy (5-40%)
•Glomerulonephritis (25-50%)•Laboratory: cryoglobulin, low C3
•Low C4 level is a characteristic•Treatment: treat underlying disease, antiviral agents (HCV-associated), corticosteroids ± CYC (idiopathic)
Cryoglobulinemic vasculitis
62
Nephrotic features
Nephritic features
Minimal change disease ++++ ---- Ig M nephropathy Membranous nephropathy Amyloidosis
++++ +
Focal segmental glomerulosclerosis Membranoproliferative GN +++ ++ Lupus nephritis +++ +++ Ig A nephropathy ++ +++ Postinfectious GN ANCA-associated GN + ++++ Thin basement membrane disease Anti-GBM disease and Goodpasture syndrome Endocarditis-associated GN Cryoglobulinemia
---- ++++
Manifestations of nephrotic and nephritic features by glomerular diseases
63
A 23-yr-old woman presents with rapid deterioration of renal function. She was diagnosed as having SLE at age 19. Her serum creatinine and urinalysis were normal at that time. PE reveals a BP of 150/96 mmHg. There are no rashes and her joints are normal. Serum creatinine is 5.4 mg/dl and the urine shows 2+ proteinuria and 2+ blood. Hematocrit 28%, platelet count 80,000 /mm3, and numerous schistocytes are seen in the peripheral blood smear.Which ONE of the following laboratory tests would be most useful to identify the cause of her disease?
A. Complement levels B. Anti-nuclear antibodyC. Anti-double strand DNAD. Anti-phospholipid antibodyE. Direct and indirect Coombs’ test
64

A 19-year-old man is seen for evaluation of hematuria. He has always been healthy; but yesterday, he developed an upper respiratory infection. Last night, when he urinated, he noted that his urine appeared to be grossly bloody. He has no family history of anyone having any similar problems. His physical examination is entirely normal. BUN 11, creatinine 0.8 mg/dl. Urinalysis: 4+ blood numerous RBCs and occasional RBC casts, and trace protein.Which of the following is the most appropriate next step in the evaluation and management of this patient?
A. Immediate referral for renal biopsyB. Referral to urologistC. Order complement levelsD. Begin prednisolone 60 mg dailyE. Hearing evaluation
65
Thank you for your attention66