Embed Size (px)
Citation preview

PAEDIATRICSKIN DISORDERS
Richie Chacko
Paediatric & Nonatal Nursing

• Impetigo is one of the most common skininfections in children. It can occur in adultsbut is seen far more often in children.Impetigo is contagious and can be spread toothers through close contact or by sharingtowels, sheets, clothing, toys, or other items.Scratching can also spread the sores to otherparts of the body.

DEFINITION
• Impetigo is a bacterial skin infection.It causes red sores that can breakopen, ooze fluid, and develop ayellow-brown crust. These sores canoccur anywhere on the body.

ETIOLOGY
• Impetigo is caused by group of bacteria-streptococcus pyogenes , staphylococcus aureus orGroup A beta-hemolytic streptococcus.
• Often these bacteria enter the body when the skinhas already been irritated or injured because ofother skin problems such as eczema, , insect bites,burns, animal bites or cuts.
• Children may get impetigo after they have had acold or allergies.
• skin-to-skin contact.

RISK FACTORS
• Age. Impetigo most commonly occurs in children ages 2 to 5.
• Crowded conditions. Impetigo spreads easily in schools and child care settings.
• Warm, humid weather. Impetigo infections are more common in summer.
• Certain sports. Participation in sports that involve skin-to-skin contact, such as football or wrestling, increases your risk of developing impetigo.
• Broken skin. The bacteria that cause impetigo often enter your skin through a small skin injury, insect bite or rash.
• poor hygiene• Other skin conditions, such as scabies or eczema

Common causes for Broken skin include the following:
• Scratching• Dermatophytosis• Varicella• Herpes simplex• Scabies• Pediculosis• Thermal burns• Surgery• Trauma• Radiation therapy• Insect bites, animal bites

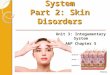
TYPES OF IMPETIGO
Impetigo contagiosa
• This may also be called nonbullous impetigo, and is the most common type of impetigo in children. It is very contagious. This type of impetigo usually begins with red sores around the nose and mouth.
• The blisters burst, leaving a weeping, red rash that becomes crusted. This rash may be itchy but is not painful. Swollen lymph nodes may also occur with impetigo contagiosa.

Bullous impetigo
• This form of impetigo is most common in children under age two. Blisters usually appear first on the torso, arms, and legs. These blisters may initially appear clear and then turn cloudy.
• Blisters tend to last longer than blisters caused by other types of impetigo. The areas around the blisters may be red and itchy.

Ecthyma
• This is the most serious form of impetigobecause it affects the epidermis and dermislayers of the skin, rather than just the toplayer. Blisters tend to be painful and may turninto ulcers, or aggravated, open sores. Swollenlymph nodes and scars may also occur.

SYMPTOMS• red sores that pop easily and leave a yellow
crust
• fluid-filled blisters
• itchy rash
• skin lesions
• Red bumps
• Sores that are filled with fluid, draining fluid, or crusted over
• Areas that are red, swollen, and may itch
• Swelling of nearby lymph glands (nodes)

DIAGNOSIS• Child’s symptoms, health history and physical
examination.
• A sample of the pus from the sores may besent for culture.
• blood or urine tests to assess systemicinfection.
• Swab test.

MEDICAL MANAGMENT
• Topical Antibiotic Cream: mupirocin & fusidicacid.
• Oral Antibiotics: broad-spectrum penicillins,cephalosporins & cefuroxime.
• Topical Disinfectants: hexachlorophene
• Cleaning and bandaging: The affected areashould be cleaned several times per day, usingeither water or an antibacterial wash.

COMPLICATIONS
• Worsening or spreading of the infection
• Cellulitis
• Guttate psoriasis
• Scarlet fever
• Bacteremia or sepsis
• Post-streptococcal glomerulonephritis
• rheumatic fever

PREVENTION• Wash the affected areas with a neutral soap and
running water• Then cover the area lightly with gauze• Do not touch the sores and encourage the patient not
to touch the sores• The patient's clothes, bedding, towels, and other
toiletries should be washed daily• The patient's clothes must not be shared or worn by
other people• When applying antibiotic ointment, gloves should be
worn, washing hands thoroughly afterward• Keep the patient's nails short to reduce scratching• Wash hands and the patient's hands often• Isolate the patient until they are not contagious

FOLLICULITIS
• Folliculitis occurs when the skin depressionsthat hold hair follicles become inflamed. Inmost cases, bacteria are the cause behind thisskin problem. One bacteria in particular,Staphylococcus aureus, causes the most harm.This bacteria lives on the skin and isresponsible for other skin issues too

ETIOLOGY
• Staphylococcus aureus• Friction from tight clothing• A pre-existing skin condition such as eczema,
acne, or other inflammation of the skin (dermatitis)
• Injuries to the skin such as surface scrapes (abrasions)
• Prolonged contact with plastic bandages or adhesive tape
• Irritation from shaving

Risk Factors
• Skin conditions such as eczema, acne, or another dermatitis
• Excessive sweating due to regular exercise
• Living in a warm, humid climate
• Diabetes
• Obesity
• Weakened immune system due to HIV/AIDS, organ transplantation, or cancer
• Frequent shaving

TYPES
• Superficial folliculitis: This type is that affectsindividuals predisposed by lack of cleanliness.The lesion begins as a small dom-shaped pustulewhere it may rupture, exuding yellowish exudate.
• Deep folliculitis: The lesion in deep folliculitis isspreading deep into the follicles and causingperifolliculitis. The condition may be extensiveinvolving a wide area especially the scalp ininfants and young children.

The most common locations for folliculitis in children include:
• Scalp
• Face
• Buttocks
• Arms and legs

SYMPTOMS
• Pus-filled lesions on hair follicles surrounded by inflamed skin.
• Itchiness
• Tenderness
• Pain
• Scarring
• Permanent hair loss

SYMPTOMSThe lesions may be:• Red• Warm• Swollen• Painful• Leaking fluid (Weeping pus)
Symptoms that affect the whole body can include:• Fever and chills• Fast heart beat• Low blood pressure

DIAGNOSIS
• Health history & physical examination
• Repeated swabs
• Bacterial cultures
• Tissue sampling for histopathologic analysis
• Blood & urine analysis.

MANAGEMENT
• Warm cloths (compresses) may help easysymptoms and speed healing.
• Incision and drainage• antibacterial wash: hexachlorophene• Topical antibiotic lotion or gel such as
erythromycin or clindamycin• Oral antibiotic pills or syrups such as cephalexin• A combination of 2 different oral antibiotics,
including trimethoprim-sulfamethoxazole,clindamycin, amoxicillin or tetracycline

PREVENTION
• Avoid tight clothing
• Maintain personal hygiene
• Wash towels, washcloths, and bed linens frequently
• Keep the skin dry
• Use antibacterial soap to clean the affected area
• Apply hot, moist compresses
• Apply some corticosteroid lotion to get relief from itchy skin

FURUNCLE
Furuncles (boils) are skin abscesses caused bystaphylococcal infection, which involve hairfollicles. Furuncles are common on the neck,breasts, face, and buttocks. They areuncomfortable and may be painful when closelyattached to underlying structures (eg. on thenose, ear, or fingers). Appearance is a nodule orpustule that discharges necrotic tissue andsanguineous (blood+pus). Furuncles may beaccompanied by fever and prostration( fatigue).

ETIOLOGY
• Most Furuncles are caused by Methicillin-resistant Staphylococcus aureus(MRSA) bacteria, which inhabit the skinsurface, throat, and nasal passages. Thesebacteria can cause infection by entering theskin through a hair follicle, small scrape, orpuncture, although sometimes there is noobvious point of entry.

CLINICAL MANIFESTATION• The skin around the boil becomes infected. It
turns red, painful, warm, and swollen.
• More boils may appear around the originalone.
• A fever may develop.
• swollen lymph nodes.
• The skin around the boil turns red or redstreaks appear.
• Severe pain .
• The boil does not drain.

DIAGNOSIS
• History collection & physicalexamination
• Sample of the pus from the infectionmay be sent for culture.

COMPLICATIONS
Possible complications may include:
• Infection spreading to other parts of the body
• Return of the infection
• Scarring

MEDICAL MANAGEMENT
• Topical antibiotics : applying liquid soapcontaining either chlorhexidine gluconate withisopropyl alcohol or 2 to 3% chloroxylenol
• Oral or intravenous (IV) antibiotics (to treat theinfection): for 5 to 10 days; choicesinclude trimethoprim/ sulfamethoxazole160/400 mg.
• A warm compress to help promote drainage ofthe lesion (for carbuncles and boils)
• Possible removal of the boils

PREVENTIVE MEASURES• Avoid squeezing, irritation and trauma to the
lesions.
• Treatment of the colonized areas and the primaryfocus as in nostrils.
• Topical antibacterial cream such as Muperacincream applied twice daily .
• Using a suitable anti septic soap as Cidal soapmay have some good effect.
• Avoiding much hyperhidrosis(hyper or excessivesweat) and occlusion of the crural (betweenthighs )area.

• Care of the crural areas especially in new bornand small children by frequent aeration andchanging diapers repeatedly should be takeninto consideration.
• Washing the hands especially when blowingthe nose and using non perfumed smoothtissue papers as cotton ones for cleaning thenose.
• Care of both the ears and nostrils is veryimportant and should not be neglected.
• Long cotton underwear is better used andchanged daily if possible

CARBUNCLE
• A carbuncle is a red, swollen, and painfulcluster of boils that are connected to eachother under the skin. Usually single, acarbuncle is most likely to occur on a hairyarea of the body such as the back or nape ofthe neck. But a carbuncle also can develop inother areas of the body such as the buttocks,thighs, groin, and armpits. This condition cancause permanent skin scarring.

ETIOLOGY
• Most carbuncles are caused by Staphylococcusaureus bacteria.
• Friction from clothing or shaving
• Poor hygiene
• Poor overall health
• Persons with diabetes, dermatitis, and aweakened immune system are more likely todevelop this infections that can causecarbuncles.

RISK FACTORS
• poor hygiene
• diabetes
• a weak immune system
• dermatitis
• kidney disease
• liver disease
• shaving and other activities that break the skin

CLINICAL MANIFESTATION• Itching before the lump appears
• Bodily aches
• Fatigue
• Fever
• skin crustiness or oozing
• The carbuncle fills with pus and develops whiteor yellow tips that weep, ooze, or crust.
• Over a period of several days, many untreatedcarbuncles rupture, discharging a creamy whiteor pink fluid.
• Swelling may occur in nearby tissue and lymphnodes

DIAGNOSIS
• History collection & physicalexamination
• Sample of the pus from the infectionmay be sent for culture.
• Boil lasts longer than two weeks.
• urine or blood tests to check youroverall health(like diabetes).

COMPLICATIONS
• Bacteria from a carbuncle can escape into thebloodstream and cause serious complications,including sepsis and infections in other partsof the body such as the lung, bones,joints, heart, blood, and central nervoussystem.

MANAGEMENTS• The cardinal rule is to avoid squeezing or irritating
a carbuncle, which increases the risk of complications and severe scarring.
• Warm compresses may promote the drainage and healing of carbuncles.
• clean, dry cloth and gently applying a heating pad or hot water bottle for 20 minutes several times per day.
• Cloths should be washed in hot water and dried at a high temperature.
• covering the area with a sterile bandage

MEDICAL MANAGEMENT• Medications such as acetaminophen or ibuprofen can
help relieve the pain
• Antibacterial soaps .
• A carbuncle may be drained with a scalpel or needle.
• Topical antibiotics : applying liquid soap containingeither chlorhexidine gluconate with isopropyl alcoholor 2 to 3% chloroxylenol
• Oral or intravenous (IV) antibiotics (to treat theinfection): for 5 to 10 days; choicesinclude trimethoprim/ sulfamethoxazole 160/400 mg.
• A warm compress to help promote drainage of thelesion (for carbuncles and boils)
• Possible removal of the boils

PREVENTION• Wash your hands before eating and after
using the bathroom.
• Shower often to keep your skin free ofbacteria.
• Avoid squeezing boils or rubbing any brokenskin.
• Wash clothes, sheets, and towels regularly inhot water.
• See your doctor if you think you have achronic illness or other skin issues that causebreaks in the skin.

BURNSSUPERFICIAL OR EPIDERMAL
• Epidermis only involved
• Burn appears red, no blistering, is painful
• Heals quickly without cosmetic blemish
PARTIAL THICKNESS
• Superficial partial thickness or Superficial Dermal
• Superficial part of dermis as well as epidermis involved
• Burn has blisters, base of blister is pink, normal caprefill, is painful
• Should heal spontaneously by epithelialisation within14 days, colour match defect only

• Deep partial thickness or Deep Dermal
• Destruction of the dermal vascular plexus
• May have some blistering, base of blisters areblotchy (marked) red, loss of capillary refill,loss of sensation
• Do not heal spontaneously
FULL THICKNESS
• Destruction of epidermis and dermis
• White/waxy/charred appearance, no capillary refill, no sensation
• Do not heal spontaneously

ETIOLOGYBurns and Scalds
• Hot drinks, water on stoves, kettles and hot tap water are most commonly involved.
Electrical
• Usually low voltage in children (<1000 volts).
Chemical
• Ingested dishwasher powder (alkali) is the most common cause of chemical burns to children, household acids like toilet cleaners.

PATHOPHYSIOLOGY
• Thermal injury->protein denaturation andcoagulation->irreversible tissue damage
• Surrounding zone of decreased perfusion-potentially salvageable( to save surroundingtissues)
• Depth determined by intensity and duration ofexposure

DEGREES OF BURN INJURIESBased on depth of burn injuries
• 1st degree: damage to epidermis
– Heals in ~2-5 days with peeling; minimal scarring
• 2nd degree: damage to dermis
– Partial thickness
– Heals in ~ 1-3 weeks with no grafting
• 3rd degree: damage to multiple layers including subcutaneous tissue
– Full thickness
– Heals in ~3-5 weeks; requires grafting


CLINICAL MANIFESTATION• Children’s skin is much thinner and therefore
more susceptible to deep burns.
Depth Colour Blisters Cap refill Sensation Heal withdressings
Epidermal Red No Normal Normal Yes
SuperficialDermal
Pale pink Yes Normal/Sluggish Normal Yes/usually
Deep Dermal Blotchy red +/- Absent Absent No
Full thickness
White No Absent Absent No

• Hypovolemia. Due to decreased perfusion and oxygen delivery.
• Decreased cardiac output. Due to significant change in blood volume is evident.
• Edema. Edema forms rapidly after burn injury.
• Decreased circulating blood volume. Due to shock.
• Hyponatremia. as water shifts from the interstitial space to the vascular space.
• Hyperkalemia. due to massive cell destruction.
• Hypothermia

Deeper Burns
• more common in young children with thinner skin
• Prolonged contact
• High heat
Large Burns
• Can see myocardial depression
• Red Blood Cell destruction
Local destruction of up to 15% of RBCs
Decreased RBC survival time- can-> additional 25% reduction

EXAMINATIONThorough general examination, obtain weight if
possible• Skin exam:• Size and depth of burn• Early eye exam look for corneal burns• Note external ear burns.• Circumferential burns- very close monitoring
of distal perfusion/capillary refill(compartment syndrome), and respiratorystatus

DIAGNOSTIC STUDIES
• History collection and physicalexamination.
• Baseline CBC, electrolytes
• myoglobinuria level, if muscle injury
• Carbon monoxide levels
• Consider CXR, soft tissue neck films
• Others based on presentation


COMPLICATIONS• Infection.
• Low blood volume.
• Dangerously low body temperature.
• Breathing problems.
• Scarring.
• Bone and joint problems.
• Ischemia.
• Tissue hypoxia.
• Respiratory failure.

MEDICAL MANAGEMENT• Transport.• Priorities. airway, breathing, and circulation.• Airway. 100% humidified• Chemical burns. All clothing and jewelry are
removed and chemical burns should be flushed.• Intravenous access. A IV catheter is inserted in
the non-burned area.• Gastrointestinal access. If the burn exceeds 20%
to 25% TBSA, a nasogastric tube is inserted andconnected to low intermittent suction becausethere are patients with large burns that becomenauseated.
• Clean beddings.• Fluid replacement therapy.

• After debridement, gently cleanse theburn with 0.25% (2.5 g/litre)chlorhexidine solution, 0.1% (1 g/litre)cetrimide solution, or another mildwaterbased antiseptic.
• Administer topical antibioticchemotherapy daily. Silver nitrate (0.5%aqueous)
• silver sulfadiazine (1% miscible ointment)

• Intravenous (IV) fluids containing electrolytes
• Intravenous (IV) or oral antibiotics if your child develops an infection
• Antibiotic ointments or creams
• A warm, humid environment for the burn
• Nutritional supplements and a high-protein diet
• Pain medications
• Skin grafting (may be required to achieve closure of the wounded area)
• Functional and cosmetic reconstruction
• Tetanus shot

Acute Phase
• Goal: close the wound
• Reduce infection risk
• Remove eschar (dead skin) by debridement
• Apply topical dressings
• Use dressings to reduce fluid and heat loss
• Perform autografting surgery
• Use tissue-cultured skin as last resort

Rehabilitation Phase
• Surgical procedures
• Physical therapy
• Nutritional concerns
• Pressure garments

NURSING MANAGEMENT• Focus on the major priorities of any trauma patient.• Assess circumstances surrounding the injury.• Monitor vital signs frequently.• Start cardiac monitoring if indicated.• Check peripheral pulses• Monitor fluid intake (IV fluids) and output (urinary
catheter) and measure hourly.• Obtain history.• Arrange for patients with facial burns to be assessed
for corneal injury.• Continue to assess the extent of the burn.• Assess neurologic status: consciousness, psychological
status, pain and anxiety levels, and behavior.• Assess patient’s and family’s understanding of injury
and treatment.• Assess patient’s support system and coping skills.

PREVENTION
• Never leave items cooking on the stoveunattended.
• Turn pot handles toward the rear of thestove.
• Keep hot liquids out of the reach of children.
• Keep electrical appliances away from water.
• Test food temperatures before serving achild. Don't heat a baby's bottle in themicrowave.

• Keep a fire extinguisher on every floorof your house.
• Keep chemicals, lighters and matchesout of the reach of children.
• Set your water heater's thermostatbelow 120 F (48.9 C) to preventscalding. Test bath water before placinga child in it.
• Test food temperatures before serving achild. Don't heat a baby's bottle in themicrowave.

• If a small child is present, block his or heraccess to heat sources such as a stove,outdoor grill, fireplace and space heater.
• Before placing a child in a car seat, checkfor hot straps or buckles.
• Unplug irons and similar devices when notin use. Store them out of reach of smallchildren.
• Cover unused electrical outlets with safetycaps. Keep electrical cords and wires out ofthe way so that children don't chew onthem.