Embed Size (px)
Citation preview

Successful transition from paediatric to adult services

Outline
• Understanding young peoples’ care– What is (special about) adolescence– Transition impossible without acknowledging this
• What is transition?– More than just transfer…..
• How can/should you do transition?– Or even better: how to deliver age and
developmentally appropriate care


“That awkward period between sexual maturation and the attainment of adult roles and responsibilities”
Biological
Delayed growth/ puberty
Psychological
Sick role, regression, mental health (esp
girls), body image, less resilient
independence, failure of peer
relationships, poor school attendance,
family dynamics (other siblings)
Social + emotional
WHAT AGE?

Tasks of AdolescenceMove from dependent child to independent, resilient, autonomous (healthcare using) adult– Puberty– Adult thinking and
personal identity– Sex, drugs ‘n’ rock
and roll…..risky behaviours
– Education/vocation– Social media– Social pressures

Adolescents are a big population
• Paediatrics caters for small children
• Adult medicine caters for middle/older age
• 16-25 big population– Utilise health care– 85% seek medical care at
least x1 pa (average x2)• Noncommunicable
disease starts here!

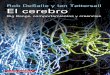
Timelapse MRI age 5-20 (Grey matter is red) synaptic pruning reduces GM through adolescence
Neurocognitive development

The developing adolescent brain• Adult brain (‘yourself’) develops ability to– Abstract think– Impulse control/delay gratification– Act independently from peers– Understand long term consequences
• More related to experience than age• Risk taking (hallmark behaviour)in adolescence– necessary– appropriate – Ask about it (HEEADSSS) and ask alone….
Steinberg 2004, 2008

Communicating with adolescents – standard care for 10-24 year olds
HEEADSSS 3.0• Home• Education• Eating• Activities• Drugs and alcohol• Sexual health• Suicide/spirituality/sleep• Social media/general safety
•http://contemporarypediatrics.modernmedicine.com/contemporary-pediatrics/content/tags/adolescent-medicine/heeadsss-30-psychosocial-interview-adolesce?page=full

The mismatch
Early adolescence Middle adolescence
Late adolescence + young adulthood
puberty
Brain development
‘Starting the engine without training the driver’

The Gap
‘Children’ (0-16) looked
after by paediatricians
‘Adults’ (16+) looked after in adult services
Development in all aspects

The mismatch
Early adolescence Middle adolescence
Late adolescence
puberty
Brain development
‘Starting the engine without training the driver’
Paediatric to Adult
Gap

Transition bridges the gap
ALL children move from childhood to adulthoodYoung people with ill health have more to lose if they ‘fall into the
gap’ while growing up
multi-faceted, active process attending to the medical, psychological and
educational/vocational needs of adolescents as they move from child to adult-centered care

How to do transition?
Need identified and enshrined in policy• 2010 Kennedy Report• DOH 2012, 2013– Moving on well– You’re welcome
• CQC report 2014• NICE Guidance 2016• Ready, Steady, Go!

Paediatrics
AdolescentOPD
Young AdultOPD
LetterOr via GP
Adult
Transition Models:
Same Dr
Different Dr
Nurse / Therapist

General Barriers
Reasons for failure of successful transition into adult healthcare:
• Financing / politics• Lack of incentive to invest• Lack of service• Lack of planning for transition• Information transfer /admin• Time• Training*
*43% health professionals in national survey reported unmet training needs as barrierMcDonagh JE 2004

Current Sheffield ‘mirror’ service
10 - 16 16 - 25
Weekly YP clinic 10-15
Monthly transfer clinic 15+YP clinic 16-25

Both paed and adult services need to:
• provide YPF care – HEEADSSS, see YP alone, promote resilience etc– Train and support each other
• agree how they will prepare/receive YP and what transition for their service looks like– Write a policy and stick to it (don’t reinvent wheels)– Transition is MUCH more than transfer– Ready steady go?
• Address barriers– Collect and audit data, harangue managers, get patients involved,
invoke NICE• Start low, go slow!

Summary
• Adolescence is a distinct developmental stage• NHS systems constrain good adolescent care• Work across + within systems in ‘YP friendly way’• Prioritise – good communication– Engagement– Choice– Resilience
• Remain open to change and challenge!

?