Embed Size (px)
Citation preview
Retinal DetachmentRetinal Detachment
Learning AimLearning Aim
Definition of Retinal Detachment
Predisposing factors
Symptoms, signs, and evaluation
Treatment of retinal detachment
Retinal DetachmentRetinal Detachment
Seperation of neurosensory retina from the
retinal pigment epithelium (RPE) is called
retinal detachment.
Types of Retinal DetachmentTypes of Retinal Detachment
Rhegmatogenous
Tractional
Exudative
Rhegmatogenous RDRhegmatogenous RD
Results from liquid vitreous seeping into
the potential space between neurosensory
retina and the RPE through degenerative or
traumatic break in the retina.
Tractional RDTractional RD
Tractional RD results from retina being
pulled away from its bed by the vitreous
membranes in conditions like, penetrating
injuries and diabetic retinopathy.
Exudative or secondary RDExudative or secondary RD
Exudative RD results from:
Choroidal neovascularisation
Exudative choroiditis
Toxaemia of pregnancy
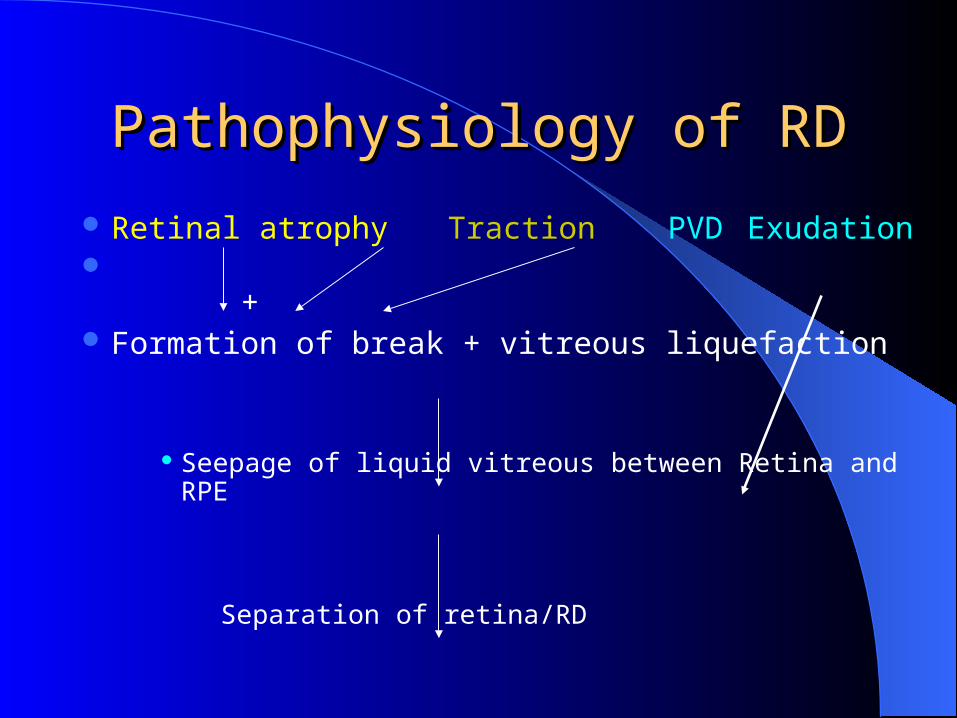
Pathophysiology of RDPathophysiology of RD Retinal atrophy Traction PVD Exudation + Formation of break + vitreous liquefaction
Seepage of liquid vitreous between Retina and RPE
Separation of retina/RD
Predisposing factorsPredisposing factors
MyopiaAphakia /pseudophakiaFamily history of RD/detachment in fellow
eyeTraumaInflammationAcute retinal necrosis and CMV retinitis
Clinical featuresClinical features
Shallow detachment symptom may be absent
Floaters,flashes,curtain/veil in front of eyesDiminution of visionField defect Retinal detachment is a cause of painless
loss of vision.
DiagnosisDiagnosis
Ophthalmoscopy Diagnosis is likely to be missed in a
shallow detachment
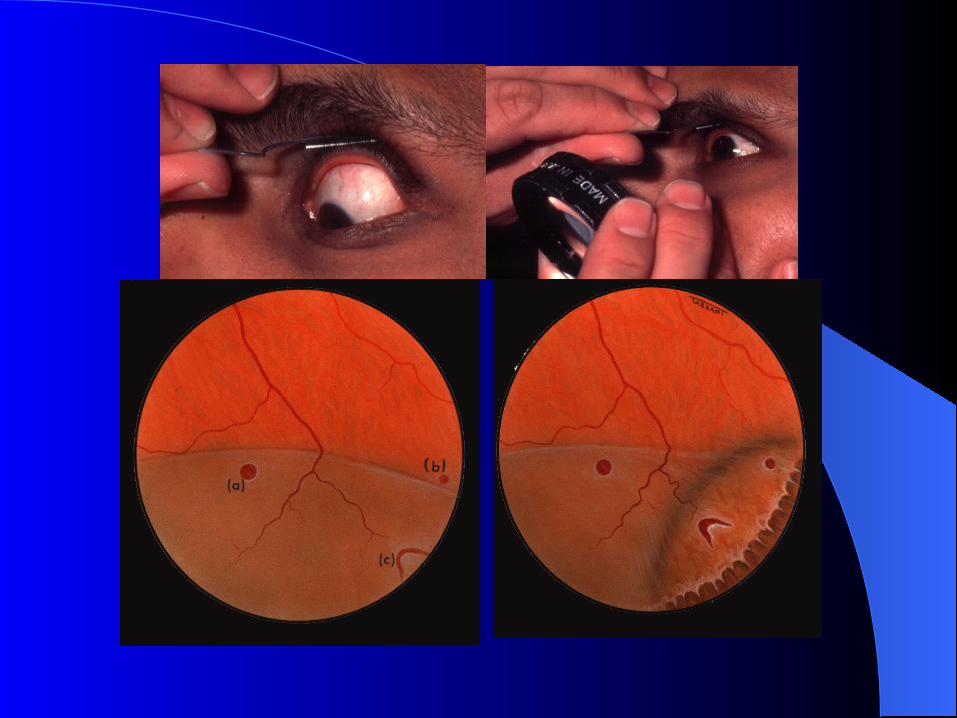
Methods of examinationMethods of examination
Preliminary examination by mirror Indirect ophthalmoscopy -in eyes with
clear mediaUSG B-scan in eyes with hazy media
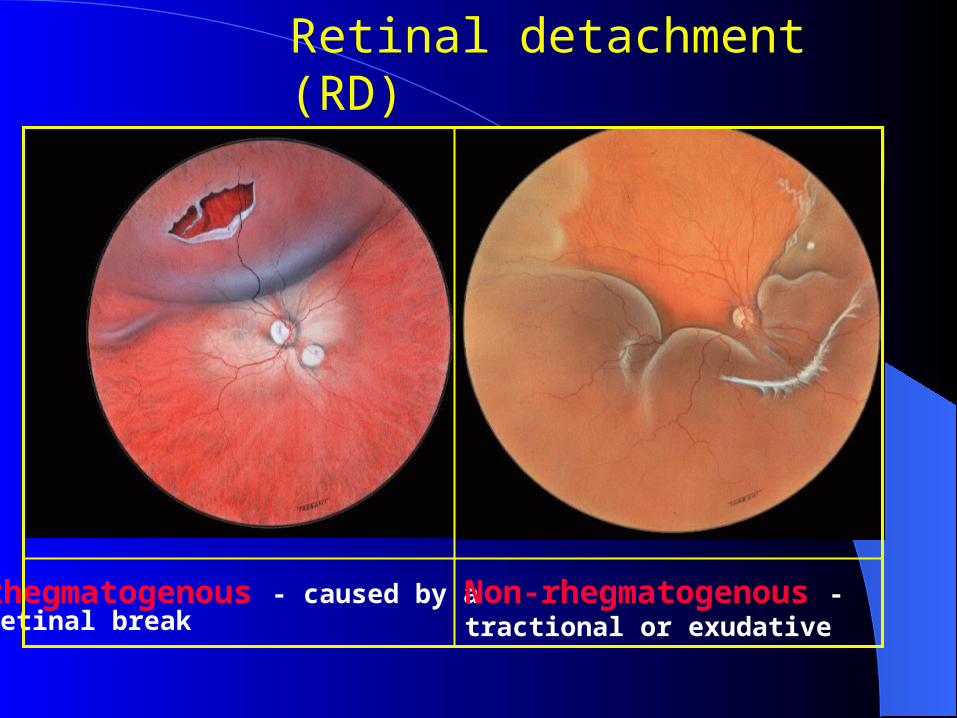
Retinal detachment (RD)
Rhegmatogenous - caused by a retinal break
Non-rhegmatogenous - tractional or exudative
ProphylaxisProphylaxis
Cryotherapy
Laser therapy in predisposed
Principles of managementPrinciples of managementIdentify retinal breaks,vitreous or,preretinal
tractionSeal the break with
diathermy,cryotherapy,Laser Release of vitreous/preretinal traction Drainage of SRFChorioretinal apposition by internal or
external temponade
Chorioretinal appositionChorioretinal apposition
External temponade
Scleral buckling or local plombage by sponge,tyre or encircling band
Internal temponadeSF6 gas, C3F8 gas,Silicon oil
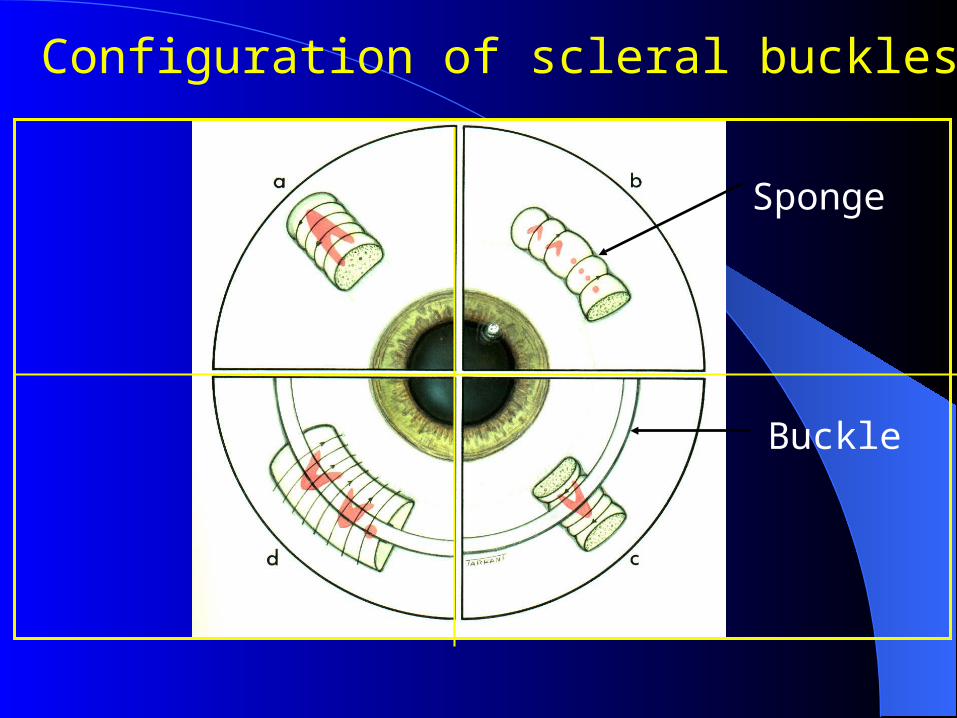
Configuration of scleral buckles
Sponge
Buckle
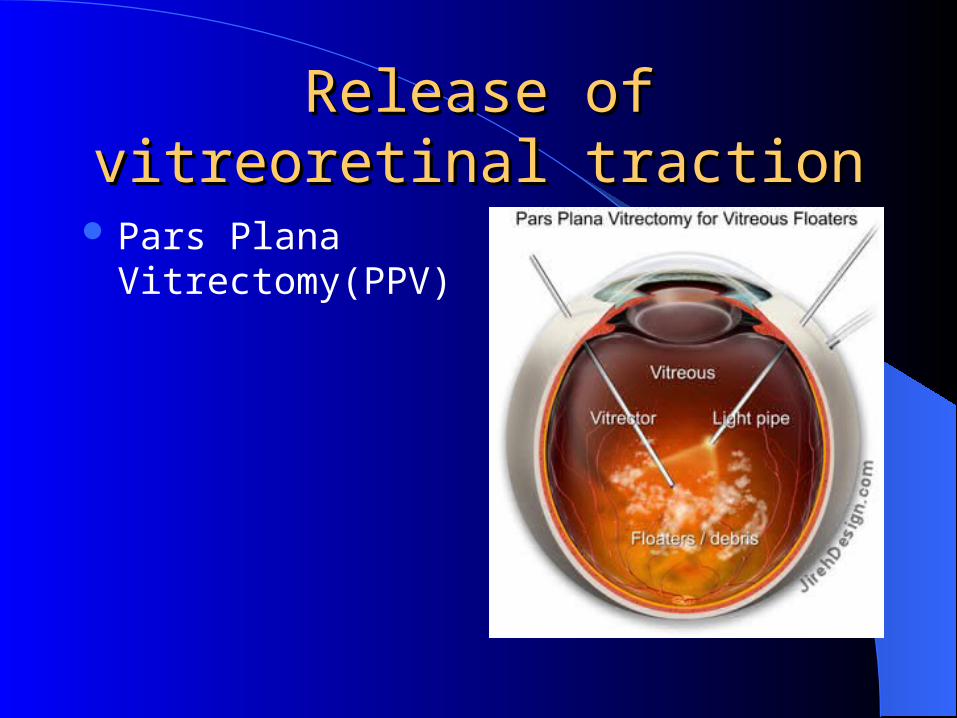
Release of vitreoretinal Release of vitreoretinal tractiontraction
Pars Plana Vitrectomy(PPV)
Complications of RD surgeryComplications of RD surgery
Failure to reattach and recurrence
Diplopia due to EOM damage
Anterior segment ischaemia
PVR and macular pucker
PrognosisPrognosis
Untreated RRD: unfavourable
Anatomical success rate 95%.
Visual prognosis depends upon duration Poor
in gross degeneration of retina,choroid and
vitreous,PVR,high myopia and detachment
present for more than 9 mo.
Points to RememberPoints to Remember
Retinal detachment results in painless loss of vision.
High myopia and eye injuries are important predisposing events.
Examinations include indirect ophthalmoscopy, or ultrasound B-scan of the eye.
Treatment requires vitreoretinal consultation.





























