Embed Size (px)
Citation preview


University of Washington-Group Health Research Team
Michael Parchman, MD, MPHDirector, MacColl Center for InnovationGroup Health Research [email protected]
Laura-Mae Baldwin, MD, MPHProfessor, Department of Family MedicineUniversity of [email protected]
Brooke Ike, MPHProject Manager and Practice FacilitatorUniversity of [email protected]
David Tauben, MDChief of Pain MedicineUniversity of Washington


Key Components of the Team Based Opioid Management Approach
Support for the Project

Support for the Project

Quality Improvement AND Research

Funded by AHRQ Grant # 1R18HS023750-01




IN WASHINGTON STATE, THERE ARE
77 OPIOIDS OR PRESCRIPTION PAIN
MEDICATIONS
WRITTEN FOR EVERY 100
PEOPLE.



0
2,000
4,000
6,000
8,000
10,000
12,000
14,000
16,000
18,000
1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013
Rx Opioids Benzodiazepines Psychostimulants

• Hydrocodone/acetaminophen (119 Million)

0
2
4
6
8
10
Group Health 2010 VHA 2011
Od
ds
Ra
tio
Re
lati
ve t
o L
ow
Do
se C
OT
<20 mg. MED 20 to < 50 mg. MED 50 to <100 mg. MED 100+ mg. MED
2007 Guidance recommending increased caution in COT
2010 Multi-faceted COT risk mitigation initiative
Trescott, Beck, Seelig & Von Korff
Health Affairs, 2011
Group Health Actions Regarding Opioids Prescribing
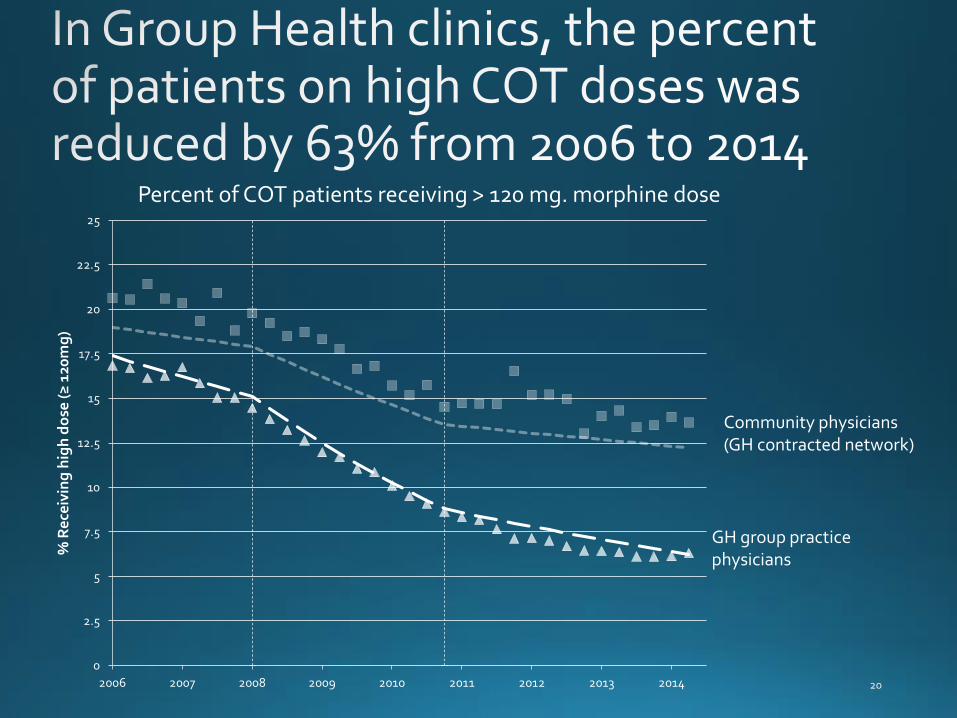
Percent of COT patients receiving > 120 mg. morphine dose
0
2.5
5
7.5
10
12.5
15
17.5
20
22.5
25
2006 2007 2008 2009 2010 2011 2012 2013 2014
% R
ece
ivin
g h
igh
do
se (
≥ 1
20m
g)
GH group practice physicians
Community physicians (GH contracted network)

Learning from Effective Ambulatory Practices
PRIMARY CARE TEAMS:


Registry Element Suggested
Frequency
Type of Data
Patient demographics: age, sex, marital
state, race/ethnicity
Baseline Categorical and Numeric
Medication, Dose and frequency Every visit Numeric
Med review for concurrent use of
sedatives
Every visit Categorical (yes/no)
Random Urine Drug Screen All new patients;
prn per policy
Categorical (positive:
yes/no)
PEG Scale (Function and Pain) Every visit Numeric
State Prescription Registry Check Every 6 months Categorical (yes/no)
Prescription Opioid Misuse Index (POMI)
survey
Every 6 months Numeric
PHQ-2 Every 6 months Numeric






Diverse Perspectives
• First step: gather an accurate baseline picture
• Different roles and clinics = different perspectives
It is essential to get a sense of these different understandings to help build consensus & inform the quality improvement
initiatives.

• Divide into groups
Two tasks:1. For each item, circle the description that best matches your
clinic. If your group cannot agree, write that down too.
2. On each sheet, write down which of the listed topics is most ripe for improvement at your organization and why.
• Be prepared for one member to share
• No right or wrong answers
Want to give additional feedback? Please feel free to email me at [email protected] or call me
at 206-685-1052.


Shared Vision 1 2 3 4
1. A shared vision for
safer and more cautious
opioid prescribing…
…has not been formally
considered or discussed
by clinicians and staff.
…has been discussed, and
preliminary conversations
regarding a clinic-wide
opioid prescribing
standard have begun.
…has been partially
achieved, but consensus
regarding a clinic-wide
opioid prescribing
standard has not yet
been reached.
…has been fully achieved,
including defining COT
and dose safety
thresholds. Clinicians and
staff consistently follow
prescribing standards and
practices.
Responsibilities Assigned 1 2 3 4
2. Responsibilities for
practice change related
to chronic opioid therapy
(COT)…
…has not been assigned
to designated leaders.
…has been assigned to
leaders, but no resources
have been committed.
…is shared by leaders and
a quality improvement
group that has dedicated
resources.
…is shared by all staff,
from leadership to team
members. Dedicated
resources support
protected time to meet
and engage in practice
change.
Leader Driven Policies &
Guidelines1 2 3 4
3. Leaders responsible for
COT practice change
initiatives…
…have not developed
COT policies and
guidelines.
…have developed COT
policies and guidelines
but have not
implemented them.
…have developed COT
policies and guidelines
and started working with
providers and teams to
implement them.
…have worked with
providers and clinical
teams and have made
substantial progress in
implementing COT
policies, guidelines, and
the necessary standard
work.

COT Registry Used 1 2 3 4
4. Use of a COT registry
to pro-actively monitor
COT patients and their
opioid dose levels to
ensure their safety…
…is not possible with
existing data systems.
…is technically possible,
but it is difficult to get
useful reports.
…is relatively easy.
Reports are provided on
a regular basis, but aren’t
consistently used to
monitor progress.
…is easy, and reports are
actively used to monitor
progress toward more
cautious opioid
prescribing.
Registry Workflows
Established1 2 3 4
5. Registry workflows to
manage the registry, use
registry data to prepare
for patient visits, improve
patient care, and monitor
progress toward overall
opioid reduction…
…have not been
developed.
…are in development, but
not established.
…are established, but
aren’t consistently
implemented.
…are established and
consistently
implemented.
Responsibilities are
assigned and protected
time is available to
complete assigned
responsibilities.

Polices & Standard
Work1 2 3 4
6. COT policies and
standard work for all
opioid prescribing
(including refills, dose
escalation, tapering)…
…either do not exist or
do not cover many
prescribing situations.
…are well-defined but
have not been discussed
with all clinic staff and
providers
…are well-defined and
have been discussed
with all clinic staff and
providers, but the
training needed to
implement them has not
yet taken place.
…are well-defined and
have been discussed
with all clinic staff and
providers, and the
training needed to
implement them has
taken place.
Treatment Agreements 1 2 3 4
7.Formal written COT
treatment agreements…
…do not exist. …have been developed
but are not in use.
…have been developed
and are partially
implemented into
routine care and/or
reminders.
…are fully implemented.
Most patients have a
signed treatment
agreement.
Urine Drug Screening 1 2 3 4
8. A urine drug screening
policy…
…does not exist. …has been developed,
but is not in use.
…has been developed
and is partially
implemented into
routine care and/or
reminders.
…is fully implemented.
Urine drug screening is
consistently
implemented according
to clinic policy.

Co-Prescribing Sedatives 1 2 3 4
9. Formal written policies
and standard work for
avoiding co-prescribing of
opioids and sedatives…
…have not
been
discussed or
developed.
…have been discussed or
developed but do not
influence care.
…have been developed and
are partially implemented
into routine care and/or
reminders.
…are fully implemented so
that co-prescribing of
opioids and sedatives is
consistently avoided.
PDMP Monitoring 1 2 3 4
10. Formal written policies
and standard work for
periodically checking the
PDMP for COT patients…
…have not
been
discussed or
developed.
…have been discussed or
developed but the PDMP
data are rarely checked.
…have been developed and
the PDMP data are
sometimes checked.
…are fully implemented so
that PDMP data are
consistently checked.
Patient Education 1 2 3 4
11. Patient education
materials that include
explanation of the risks, and
limited benefits of long-term
opioid use…
…have not
been
discussed or
developed.
…have been developed but
are rarely used in routine
clinical care.
…have been developed and
are partially implemented
into routine care.
…are fully implemented and
used routinely in patient care
when COT is considered or
prescribed.

Prepared COT Patient
Visits1 2 3 4
12. Before routine clinic
visits, patients receiving
COT …
…are not identified.
There is no advance
preparation for patient
visits for chronic opioid
therapy.
…are sometimes
identified, but there is
no discussion or
advance preparation for
visits with COT patients.
…are identified, and a
discussion or chart
review to prepare for
the visit sometimes
occurs.
…are consistently
identified, and are
discussed before the
visit. The chart is
reviewed and
preparations made to
address safe COT use.
Standard Work for
Prepared Visits1 2 3 4
13. The work needed to
prepare for a visit with
patients receiving or
potentially initiating
COT…
…has not been defined. ...has been partially
defined, but work/tasks
are not delegated across
the team, and
implementation is
inconsistent.
...has been clearly
defined, work is
delegated across the
team, and is often
implemented.
...has been clearly
defined, work has been
delegated across the
team, and is consistently
implemented.

Empathic
Communication1 2 3 4
14. Patient-centered,
empathic
communication
emphasizing patient
safety…
…is not used in visits
with COT patients to
discourage COT use
and dose escalation or
to encourage tapering.
…is infrequently used to
discuss COT use, dose
escalation, or to
encourage tapering.
…is sometimes used to
discuss COT use, dose
escalation, or to encourage
tapering.
…is consistently used to
discuss COT use, dose
escalation, or to
encourage tapering.
Patient Involvement 1 2 3 4
15. Involving COT
patients in decision-
making, setting goals
for improvement and
providing support for
self-management…
…is not done routinely. …is sometimes
implemented by
discussing treatment
options and goals, but
this is not documented in
a care plan. Patient
education pamphlets are
available.
…is usually implemented.
Patient goals and action
plans are documented in a
care plan. Follow visits
refer to and update goals
and plans.
…is consistently
implemented. Patient
goal setting, action plans
and self-management
skills are supported by
practice teams trained in
shared decision making
and self-management
support techniques.
Care Plans 1 2 3 4
16. Care plans for
chronic pain
management and
COT…
…have not been
developed
…are developed and
recorded but reflect only
the prescribing clinician,
the medication regimen
and a monitoring
schedule.
…are developed
collaboratively with
patients and include self-
management and clinical
goals, but they are not
routinely recorded or used
to guide care.
…are developed
collaboratively, include
self-management and
clinical goals, and are
routinely recorded and
used to guide care.

Identifying Complex Patients 1 2 3 4
17. The work needed to
identify opioid misuse,
diversion, abuse, addiction
and for recognizing complex
opioid dependence…
…is not done
routinely.
…is sometimes
done.
…is usually done, but
follow-up when
problems are identified
is inconsistent.
…is consistently done, with
consistent follow-up when
problems are identified.
Behavioral Health Resources 1 2 3 4
18. Behavioral health (mental
health and chemical
dependency) services…
…are difficult
to obtain
reliably.
…are available
from behavioral
health specialists
but aren’t timely
or convenient.
…are available from
behavioral health
specialists and are
usually timely and
convenient.
…are readily available from
behavioral health specialists who
are onsite or who work in an
organization that has a referral
protocol or agreement with our
practice setting.

Monitoring Progress 1 2 3 4
19. A system to measure
and monitor progress in
COT practice change…
…has not been
developed.
…has been developed,
including overall tracking
goals, but regular
tracking reports on
specific objectives have
not been produced.
…is used to produce
regular tracking reports
on specific objectives.
Leadership reviews are
done occasionally, but
not on a formal
schedule.
…has been is fully
implemented to
measure and track
progress on specific
objectives. Leadership
reviews progress reports
regularly and
adjustments and
improvements are
implemented.
Assessing and Modifying 1 2 3 4
20. Adjustments to achieve
safer opioid prescribing
based on monitoring data…
…are not being
made.
…are occasionally made,
but are limited in scope
and consistency.
…are often made and
are usually timely.
…are consistently made
and are integrated in
overall quality
improvement strategies.





BUILDING
BLOCKS
BRAINSTORM CHANGES WE WANT TO MAKE
(REVIEW THE SIX BUILDING BLOCKS HIGH-IMPACT CHANGES @ WWW.IMPROVINGOPIOIDCARE.ORG FOR IDEAS)
30, 60 OR 90-DAY GOAL
MAKE IT SMART: SPECIFIC, MEASUREABLE, ACTIONABLE, REALISTIC,
AND TIME-BOUND
Leadership & consensus
Use a registry to proactively manage patients
Revise policies and standard work
Prepared, patient-centered visits
Caring for complex patients
Measuring success

GOAL 1:
LIST THE STEPS NECESSARY
TO ACHIEVE THIS AIM
(WHAT)
PERSON RESPONSIBLE
(WHO)WHEN WHERE
1.
2.
3.
4.
5.
6.

GOAL 2:
LIST THE STEPS NECESSARY
TO ACHIEVE THIS AIM
(WHAT)
PERSON RESPONSIBLE
(WHO)WHEN WHERE
1.
2.
3.
4.
5.
6.