Embed Size (px)
Citation preview

MAY | JUNE 2016
THEGREAT JUGGLING ACTDr. William Alec Tisdall Serves San Antonio with Personal, Precision Pain Care
48
54
HEARTTOHEARTChristus Spohn’s TAVR Program Gives The Gift of Life To Cardiac Patients
70
21STCENTURY
CRAFTSMANSan Antonio Plastic
Surgeon Dr. Thomas Jeneby Employs The Latest
Surgical Technology andMedical Know-How
to Help Patients
62
DR. JENNIFER WALDEN BLENDS BEAUTY AND HEALTH WITHSTATE-OF-THE-ART TECHNOLOGY
By B. KAY RICHTER
AUTHENTICALLY BEAUTIFUL HEALTH
MDMONTHLY.COM

36 TxMD MAY/JUNE 2016
tx
MDMONTHLY.COM
INFORMED PATIENT / HOUSTON
ILLU
STR
ATIO
N C
OU
RTE
SY O
F M
EM
OR
IAL
PLA
STIC
SU
RG
ER
Y.
ChangingWith The TimesDIEP Flap: A More EffectiveBreast ReconstructionBY DR. KENDALL R. ROEHL
BOUT 1 IN 8 U.S. WOMEN, or roughly 12 percent, will develop invasive breast cancer over the course of their lifetime. In 2016, an estimated 246,660 new cases of invasive
breast cancer are expected to be diagnosed in women in the U.S., along with 61,000 new cases of non-invasive breast cancer. Because of its prevalence in women, reconstructive surgery after breast cancer has consumed a large portion of many plastic surgeon’ practices. The American Society of Plastic Surgeons reported 102,215 breast reconstructions were performed in 2014. This was a 30 percent increase over the 78,832 reconstructions done in 2000, and breast reconstructive surgeries continue to rise.
In breast restoration, women have three options for reconstruction after mastectomy: implants, their own tissue, or a combination of implants and their own tissue. Implant-based breast reconstruction was the first option available to women with breast cancer, and it remains the most common form to date. However, as of 1982, women also have the option of using their own tissue to reconstruct their breasts. There are multiple options available for natural tissue breast reconstruction, but the most favorable is the lower
abdominal tissue.The original
version of this reconstruction was called the transverse rectus abdominus myocutaneous flap, or TRAM flap, and
it used the tissue from the belly button to the pubic hair and hip bone to hip bone to reconstruct the breast. The abdomen, or donor site as it is referred to, is then closed similar to a cosmetic tummy tuck after the abdominal tissue is transferred and shaped. However, this flap sacrifices rectus abdominus, one of the six-pack muscles, in order to provide a blood supply for the transferred skin and fat. The tummy tissue and
one six-pack muscle remain connected, and they are swung into the chest as one unit then shaped in the form of a breast.
As time and science has evolved, the abdominal flap-based techniques have improved to limit the amount of damage that is done to the abdominal donor site in borrowing this tissue to create a breast. The flaps are referred to as muscles-sparing TRAM flaps and more recently deep inferior epigastric flaps, or DIEP flaps as
they are commonly referred to. The two main benefits of the DIEP flap are that the entire six-pack muscle remains intact and functional on the abdomen limiting weakness and bulging of the abdomen, as in the TRAM flap, and
blood supply to the flap is hardier, creating a more reliable transfer of skin and fat to the breast with less partial tissue loss after transfer.
DIEP flaps are performed by the most technically skilled and most highly trained plastic surgeons in the world. Most of these surgeons have spent additional years training in transplanting tissues called reconstructive microsurgery. The tissue used from the abdomen remains as that from the belly-button to pubic hair and hip bone to hip bone, but the deeper dissection is the challenging part. Blood supply to the skin and fat comes from perforating vessels off
ADR. KENDALL ROEHL, DR. PATRICK HSU, AND DR. MELISSA CROSBY OF MEMORIAL PLASTIC SURGERY IN HOUSTON AND MEMORIAL PLASTIC SURGERY CLEAR LAKE IN WEBSTER TEXAS WERE ALL TRAINED AT THE PRESTIGIOUS MD ANDERSON CANCER CENTER IN RECONSTRUCTIVE MICROSURGERY. THEY HAVE OVER 26 YEARS OF COMBINED PLASTIC AND RECONSTRUCTIVE SURGERY EXPERIENCE AND WELL OVER 2000 MICROVASCULAR FLAPS COMBINED. THEIR FOCUS IS NOT ONLY ON BREAST RESTORATION BUT PERSONALIZED AND COMPASSIONATE CARE AS WELL AS EXCELLENT AESTHETIC OUTCOMES, OFTEN THE SILVER LINING OF THE BREAST CANCER JOURNEY.
“ In 2016, an estimated 246,660 new
cases of invasive breast cancer are
expected to be diagnosed
in women inthe U.S.”
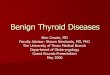
Other Abdominal Flaps
SIEA (Superficial InferiorEpigastric Artery)
DIEP (Deep InferiorEpigastric Perforator)
Muscle Sparing

2016 MAY/JUNE TxMD 37
Monthly.com
the deeper deep inferior epigastric vessels that arise from the external iliac artery and vein. These vessels are dissected free, leaving all of the rectus muscle behind. They are then transected at their take off from the external iliac vessels and transplanted to the chest. Here they are attached to the internal mammary artery and vein beneath the bench press muscle and the underlying rib, but just above the lung. The blood vessels, the size of a coffee stirring straw, are attached together artery to artery and vein to vein with sutures the diameter of a piece of hair using high-powered magnification, either a microscope or glasses called loupes.
The benefits of performing breast reconstruction using a woman’s own tissue is a breast that is all their own skin and fat allowing for texture and movement most like a natural breast, eliminating the risk of implants and the need for maintenance as well. In time, these abdominal tissue reconstructions age with the woman, and symmetry to a non-cancerous contralateral breast is easier to achieve. Often, the abdomen provides enough tissue for bilateral reconstruction if the patient opts to have the opposite breast removed to decrease their risk of a second case of breast cancer or in the case of bilateral breast cancer. On the abdomen, women gain the cosmetic benefits of a flatter, smoother, tighter abdomen, and in a DIEP, they retain their muscle strength and have a much lower risk of abdominal weakness or bulging, which is often seen in TRAM and muscle-sparing TRAM surgeries.
Recovery from this surgery usually involves three to four days in the hospital for monitoring and pain control. Patients have three to four drains and have to wear a panty-girdle for six weeks. Activity is limited to lifting 10 to 15 pounds or less for the first six weeks. Patients often return to work in three to six weeks depending on their job requirements.
Breast reconstruction is usually a three- to four-step process. After the initial transfer, patients often undergo a second surgery about three months later to improve the shape and symmetry of their breasts and to touch up any scarring on the abdomen. The third step is reconstruction of the actual nipple, and the last step is to re-create the pigmented areola, most often done with tattoo techniques.
DIEP flaps and other microvascular breast reconstructions should only be performed by the most highly skilled microsurgeons certified by the American Board of Plastic Surgery and members of the American Society of Plastic Surgeons.
FOR MORE INFORMATION ON MEMORIAL PLASTIC SURGERY—CLEAR LAKE VISIT WWW.MEMORIALCLEARLAKE.COM OR CALL 713.609.9335.
FOR MORE INFORMATION ON MEMORIAL PLASTIC SURGERY VISIT WWW.MEMORIALPLASTICSURGERY.COM OR 713.633.4411.
Monthly.com