Embed Size (px)
Citation preview

Daniele Alberti, Oncology Medical Director Novartis Farma S.p.A., Origgio (VA) Biobang, Lecce, 12 novembre 2014
Production scale-up e mercato farmaceutico
Disclosures su potenziali conflitti di interesse
§ Dipendente Novartis da 32 anni
§ Oncology Medical Director Italia da 8 anni
§ Coordinatore Gruppo Ricerca Clinica Assobiotech da due mesi
§ Abito a Monza
Daniele Alberti – Biobang Lecce – 12 novembre 2014
Perchè sono qui con voi oggi?
Daniele Alberti – Biobang Lecce – 12 novembre 2014
Farmaceutica – la carta da giocare
Daniele Alberti – Biobang Lecce – 12 novembre 2014

La Vision di Novartis Oncology Region Europe
Be the leading company transforming science into
innovative solutions to cure cancer patients in Europe
Essere l’azienda leader che trasforma la ricerca in soluzioni innovative per la cura
dei pazienti oncologici in Europa
Assobiotec’s Vision
Transparent collaboration among Research Industry, Academy, Health Care Professionals and National and
Regional Institutions, focussing on Patients and, consequently, on Associations representing them.
Source:
D. Alber) -‐ Biotech Week -‐ Roma ISS 9-‐10-‐2014

Universities
Hospitals
Institutions Companies
Perchè siamo qui oggi?
Daniele Alberti – Biobang Lecce – 12 novembre 2014
Agenda
14.00 – 14.10 Introduzione e agenda
14.10 – 14.50 Strategia di sviluppo nuovi prodotti in indicazioni onco- ematologiche
14.50 - 15.10 Opportunità di rilancio: Clinical Trial Center (CTC), Reti Oncologiche ed Ematologiche e laboratori regionali
15.10 - 15.30 Discussione / Presentazione Lavori di gruppo
15.30 – 16.30 Lavori di gruppo
16.30 – 17.00 Feedback in plenaria dai Gruppi di lavoro
17.00 – 17.15 Conclusioni
Daniele Alberti – Biobang Lecce – 12 novembre 2014
Agenda
14.00 – 14.10 Introduzione e agenda
14.10 – 14.50 Strategia di sviluppo nuovi prodotti in indicazioni onco- ematologiche
14.50 - 15.10 Opportunità di rilancio: Clinical Trial Center (CTC), Reti Oncologiche ed Ematologiche e laboratori regionali
15.10 - 15.30 Discussione / Presentazione Lavori di gruppo
15.30 – 16.30 Lavori di gruppo
16.30 – 17.00 Feedback in plenaria dai Gruppi di lavoro
17.00 – 17.15 Conclusioni
Daniele Alberti – Biobang Lecce – 12 novembre 2014
Chi è Novartis Oncology
§ Business Unit di Novartis Corporation
§ Creata per focalizzazione nell’innovazione in campo oncologico per i pazienti
§ Pioniere delle Target Therapy
§ Portafoglio di 12 prodotti e promettente pipeline
§ Market Leader in ematologia
§ 2° impresa in onco-ematologia
§ Pur senza prodotti chemioterapici
«Revolutionary therapy with
Imatinib» (NCCN Guidelines)
Daniele Alberti – Biobang Lecce – 12 novembre 2014
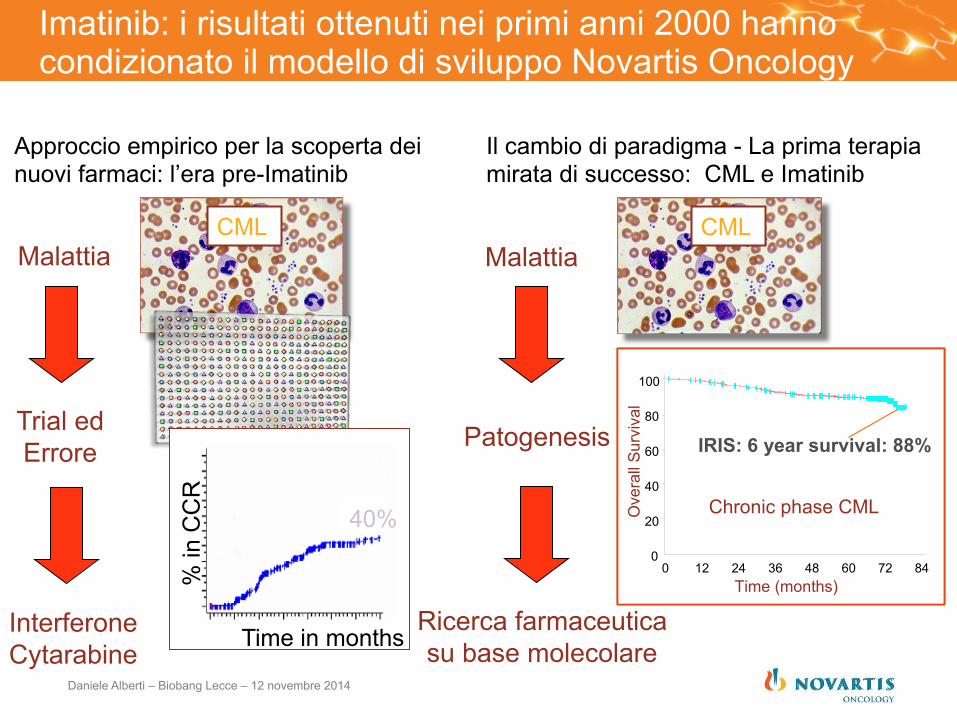
Imatinib: i risultati ottenuti nei primi anni 2000 hanno condizionato il modello di sviluppo Novartis Oncology
CML Malattia
Trial ed Errore
Interferone Cytarabine Time in months
% in
CC
R
40%
Approccio empirico per la scoperta dei nuovi farmaci: l’era pre-Imatinib
Il cambio di paradigma - La prima terapia mirata di successo: CML e Imatinib
Malattia CML
Ove
rall
Surv
ival
0
20
40
60
80
100
0 12 24 36 48 60 72 84
IRIS: 6 year survival: 88%
Chronic phase CML
Time (months)
Ove
rall
Surv
ival
0
20
40
60
80
100
0 12 24 36 48 60 72 84
IRIS: 6 year survival: 88%
Chronic phase CML
Time (months)
Ricerca farmaceutica su base molecolare
Patogenesis
Daniele Alberti – Biobang Lecce – 12 novembre 2014
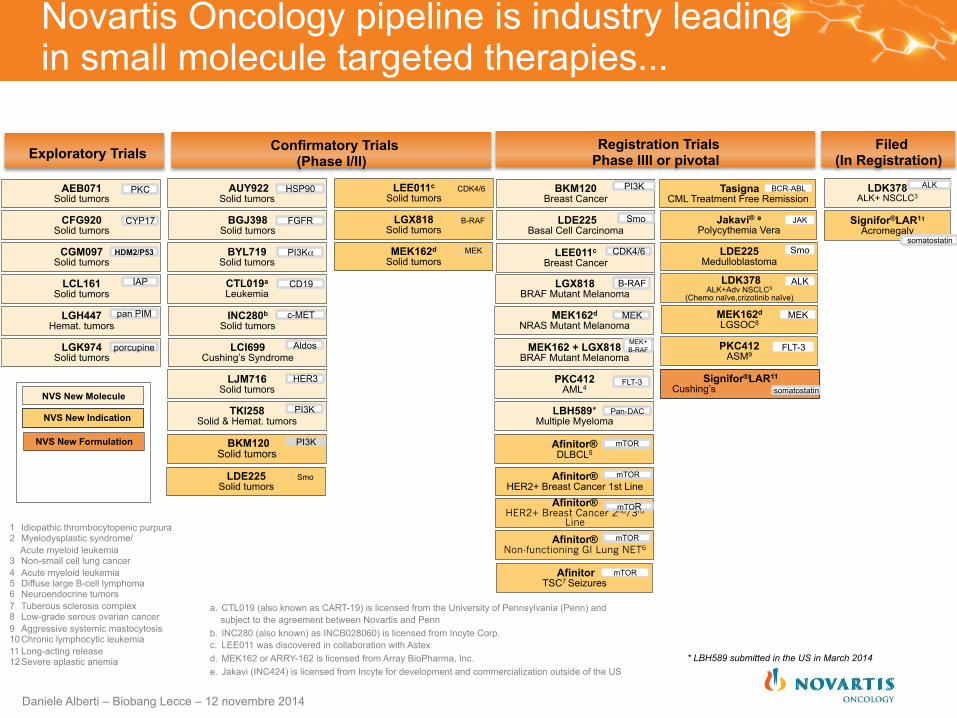
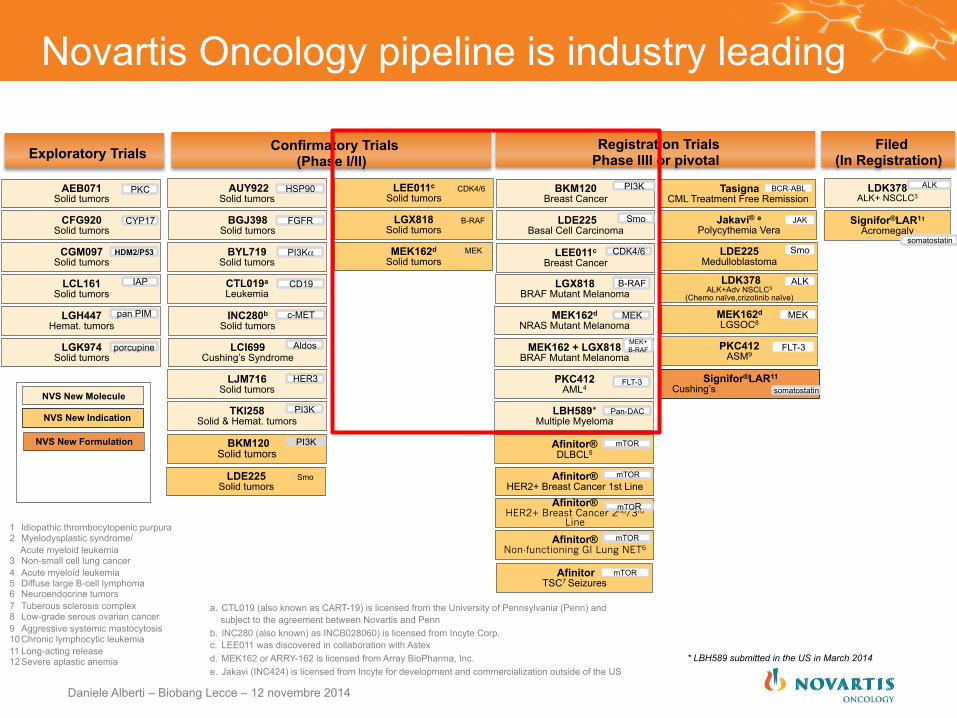
LGK974 Solid tumors
LCL161 Solid tumors
CGM097 Solid tumors
CFG920 Solid tumors
AEB071 Solid tumors
LGH447 Hemat. tumors
LDK378 ALK+ NSCLC3
BYL719 Solid tumors
LJM716 Solid tumors
LCI699 Cushing’s Syndrome
TKI258 Solid & Hemat. tumors
MEK162d NRAS Mutant Melanoma
BGJ398 Solid tumors
AUY922 Solid tumors
PKC412 AML4
MEK162 + LGX818 BRAF Mutant Melanoma
LGX818 BRAF Mutant Melanoma
LEE011c Breast Cancer
LDE225 Basal Cell Carcinoma
BKM120 Breast Cancer
LBH589* Multiple Myeloma
Signifor®LAR11 Acromegaly
Afinitor® HER2+ Breast Cancer 2nd/3rd
Line
Afinitor® HER2+ Breast Cancer 1st Line
Afinitor® DLBCL5
Afinitor® Non-functioning GI Lung NET6
CTL019a Leukemia
INC280b Solid tumors
Pan-DAC
CYP17
IAP
PI3K
porcupine
CDK4/6
Aldos
pan PIM
mTOR
MEK
CD19
Smo
HER3 FLT-3 Signifor®LAR11 Cushing’s somatostatin
PKC
HDM2/P53
c-MET
HSP90
PI3Kα
FGFR
mTOR
mTOR
mTOR
somatostatin
MEK+ B-RAF
PI3K
B-RAF
ALK
LDE225 Solid tumors
Smo
MEK162d Solid tumors
MEK
LEE011c Solid tumors
CDK4/6
LGX818 Solid tumors
B-RAF
NVS New Molecule
NVS New Indication
Tasigna CML Treatment Free Remission
LDE225 Medulloblastoma
PKC412 ASM9
Jakavi® e Polycythemia Vera
MEK162d LGSOC8
LDK378 ALK+Adv NSCLC3
(Chemo naïve,crizotinib naïve)
Smo
ALK
BCR-ABL
MEK
FLT-3
JAK
NVS New Formulation
1 Idiopathic thrombocytopenic purpura 2 Myelodysplastic syndrome/
Acute myeloid leukemia 3 Non-small cell lung cancer 4 Acute myeloid leukemia 5 Diffuse large B-cell lymphoma 6 Neuroendocrine tumors 7 Tuberous sclerosis complex 8 Low-grade serous ovarian cancer 9 Aggressive systemic mastocytosis 10 Chronic lymphocytic leukemia 11 Long-acting release 12 Severe aplastic anemia
a. CTL019 (also known as CART-19) is licensed from the University of Pennsylvania (Penn) and subject to the agreement between Novartis and Penn
b. INC280 (also known) as INCB028060) is licensed from Incyte Corp. c. LEE011 was discovered in collaboration with Astex d. MEK162 or ARRY-162 is licensed from Array BioPharma, Inc. e. Jakavi (INC424) is licensed from Incyte for development and commercialization outside of the US
* LBH589 submitted in the US in March 2014
BKM120 Solid tumors
PI3K
Registration Trials Phase IIII or pivotal
Filed (In Registration)
Confirmatory Trials (Phase I/II) Exploratory Trials
Afinitor TSC7 Seizures
mTOR
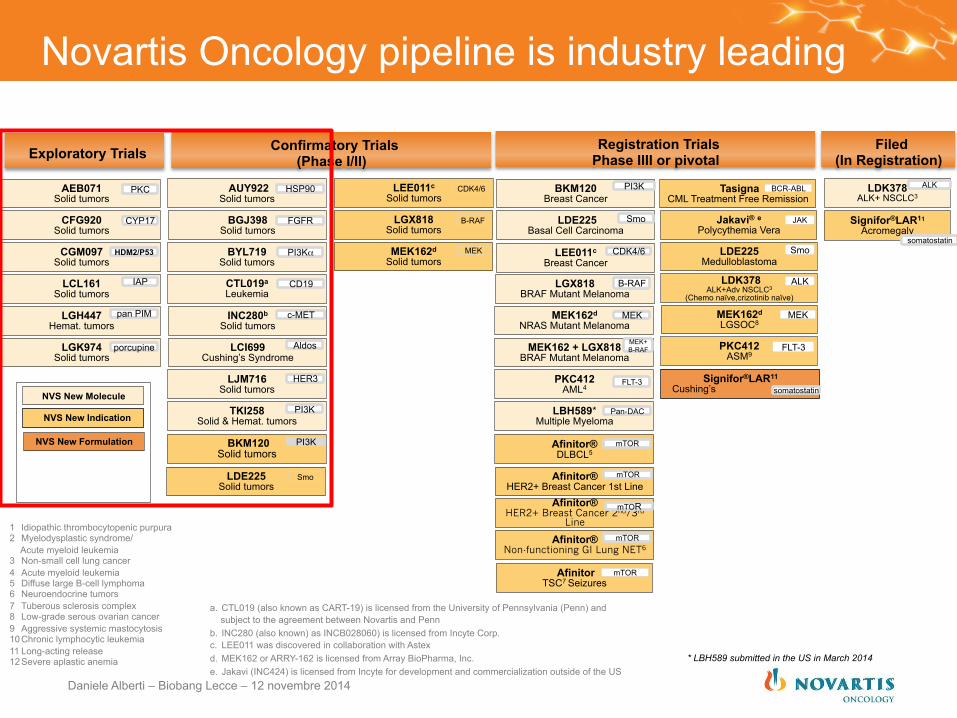
Novartis Oncology pipeline is industry leading in small molecule targeted therapies...
Daniele Alberti – Biobang Lecce – 12 novembre 2014
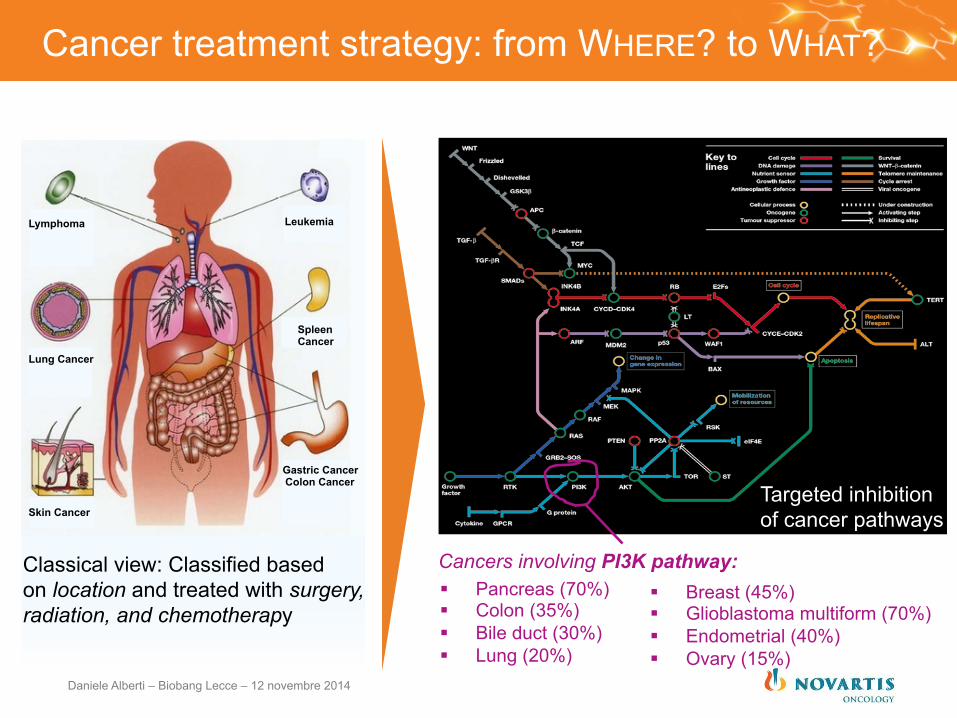
Classical view: Classified based on location and treated with surgery, radiation, and chemotherapy
Cancers involving PI3K pathway: § Pancreas (70%) § Colon (35%) § Bile duct (30%) § Lung (20%)
§ Breast (45%) § Glioblastoma multiform (70%) § Endometrial (40%) § Ovary (15%)
Lymphoma Leukemia
Lung Cancer
Skin Cancer
Gastric Cancer Colon Cancer
Spleen Cancer
Targeted inhibition of cancer pathways
Cancer treatment strategy: from WHERE? to WHAT?
Daniele Alberti – Biobang Lecce – 12 novembre 2014
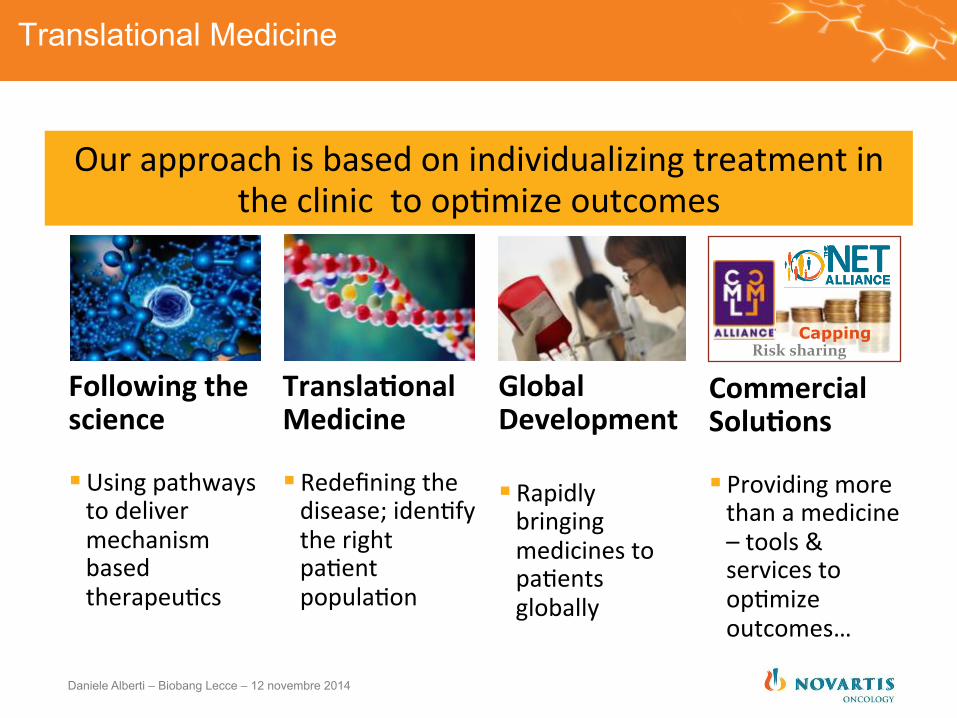
Translational Medicine
Our approach is based on individualizing treatment in the clinic to op)mize outcomes
Following the science
§ Using pathways to deliver mechanism based therapeu)cs
Global Development § Rapidly bringing medicines to pa)ents globally
Transla7onal Medicine
§ Redefining the disease; iden)fy the right pa)ent popula)on
Capping Risk sharing
Commercial Solu7ons
§ Providing more than a medicine – tools & services to op)mize outcomes…
Daniele Alberti – Biobang Lecce – 12 novembre 2014
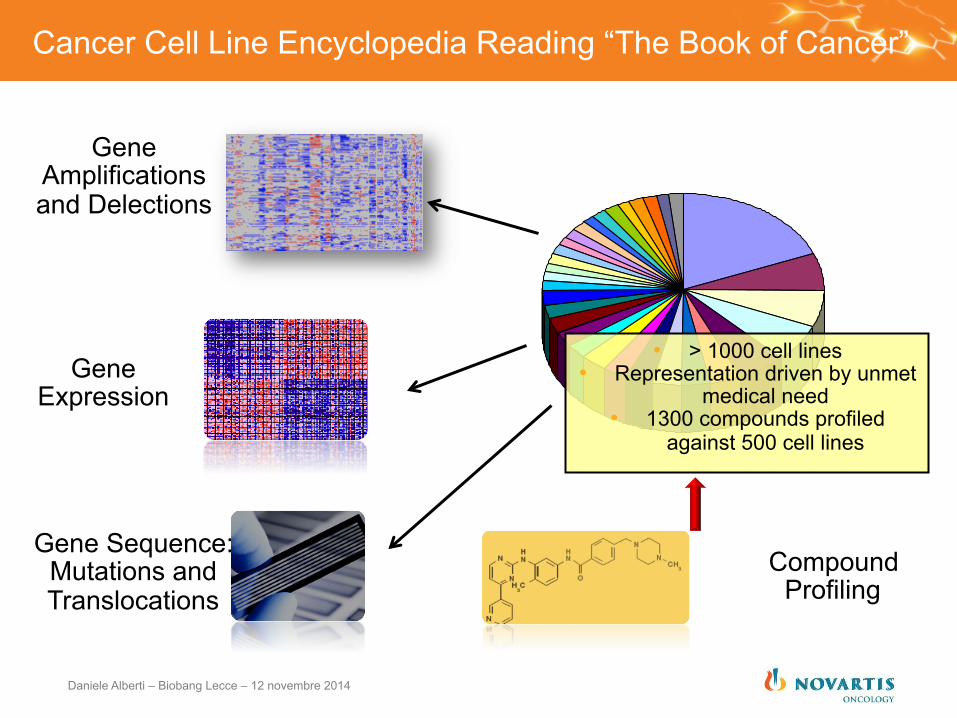
Cancer Cell Line Encyclopedia Reading “The Book of Cancer”
Gene Amplifications and Delections
Gene Expression
Gene Sequence: Mutations and Translocations
• > 1000 cell lines • Representation driven by unmet
medical need • 1300 compounds profiled
against 500 cell lines
Compound Profiling
Daniele Alberti – Biobang Lecce – 12 novembre 2014
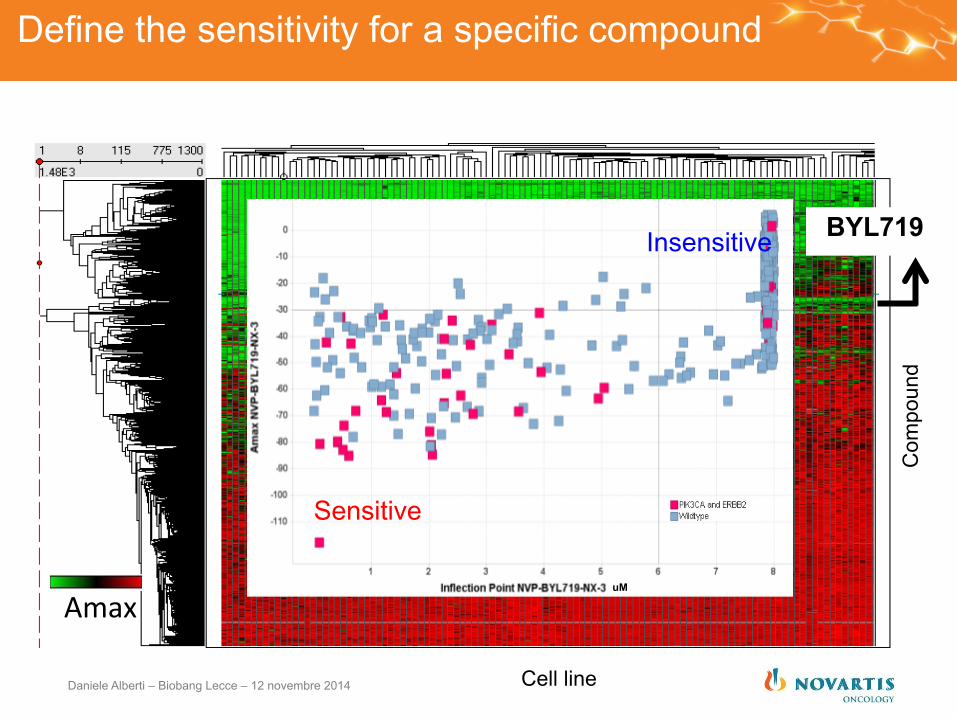
Define the sensitivity for a specific compound
Amax
Com
poun
d
Cell line
Sensitive
Insensitive
uM
BYL719
Daniele Alberti – Biobang Lecce – 12 novembre 2014
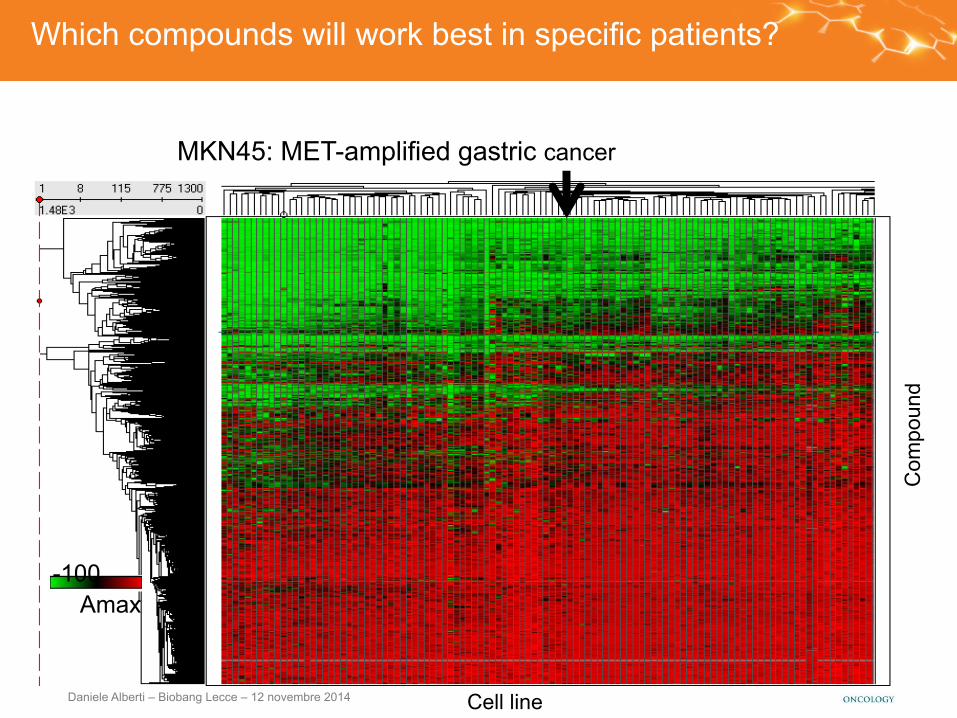
-100 0 Amax
Com
poun
d
Cell line
Which compounds will work best in specific patients?
MKN45: MET-amplified gastric cancer
Daniele Alberti – Biobang Lecce – 12 novembre 2014
Response Prediction Biomarkers and Targeted Cancer Drug Development
Drives: § Improved patient benefit because tumors are
uniquely dependent on the drug target
§ Increased probability of success by enriching studies for likely responders and excluding non-responders
§ Maximal benefits to payers with drugs used only in patients likely to benefit
§ Faster time to market with lower development cost through smaller studies with stronger signals
Daniele Alberti – Biobang Lecce – 12 novembre 2014
What is a companion diagnostics?
FROM “One Size Fits All”
TO “Personalized Medicine”
Saves life and money by using biomarkers to improve safety, effectiveness, and health outcome of patients via targeted risk stratification, prevention and tailored treatment approaches: The Right drug for the right patient at the right time and the right dose.
Moving from “One Size Fits All” to “Personalized Medicine” using diagnostic test methods (mostly in vitro diagnostic tests performed on patients derived specimens)
Daniele Alberti – Biobang Lecce – 12 novembre 2014
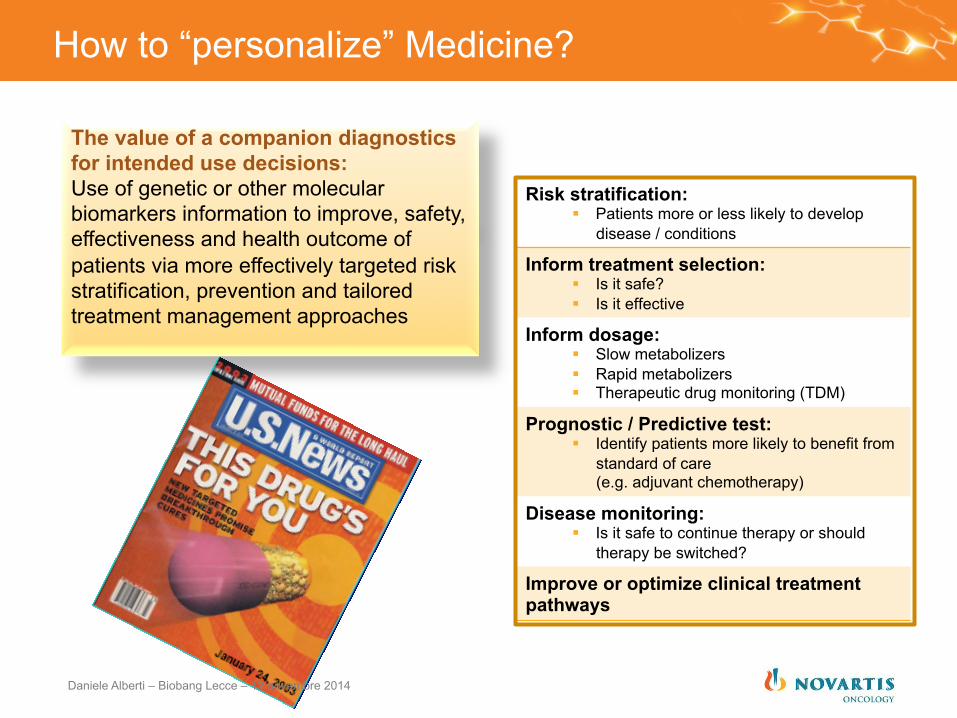
How to “personalize” Medicine?
The value of a companion diagnostics for intended use decisions: Use of genetic or other molecular biomarkers information to improve, safety, effectiveness and health outcome of patients via more effectively targeted risk stratification, prevention and tailored treatment management approaches
Risk stratification: § Patients more or less likely to develop
disease / conditions
Inform treatment selection: § Is it safe? § Is it effective
Inform dosage: § Slow metabolizers § Rapid metabolizers § Therapeutic drug monitoring (TDM)
Prognostic / Predictive test: § Identify patients more likely to benefit from
standard of care (e.g. adjuvant chemotherapy)
Disease monitoring: § Is it safe to continue therapy or should
therapy be switched?
Improve or optimize clinical treatment pathways
Daniele Alberti – Biobang Lecce – 12 novembre 2014
21 | Portfolio Prioritisation| Portfolio Management| Aug 2010 | Business Use Only
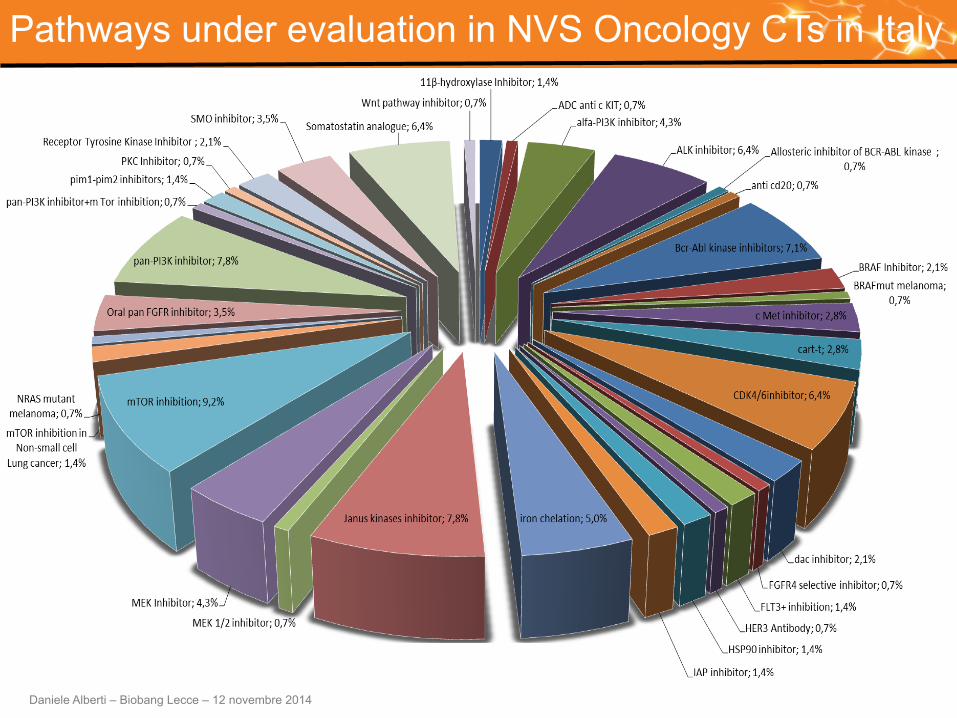
Pathways under evaluation in NVS Oncology CTs in Italy
Daniele Alberti – Biobang Lecce – 12 novembre 2014
LGK974 Solid tumors
LCL161 Solid tumors
CGM097 Solid tumors
CFG920 Solid tumors
AEB071 Solid tumors
LGH447 Hemat. tumors
LDK378 ALK+ NSCLC3
BYL719 Solid tumors
LJM716 Solid tumors
LCI699 Cushing’s Syndrome
TKI258 Solid & Hemat. tumors
MEK162d NRAS Mutant Melanoma
BGJ398 Solid tumors
AUY922 Solid tumors
PKC412 AML4
MEK162 + LGX818 BRAF Mutant Melanoma
LGX818 BRAF Mutant Melanoma
LEE011c Breast Cancer
LDE225 Basal Cell Carcinoma
BKM120 Breast Cancer
LBH589* Multiple Myeloma
Signifor®LAR11 Acromegaly
Afinitor® HER2+ Breast Cancer 2nd/3rd
Line
Afinitor® HER2+ Breast Cancer 1st Line
Afinitor® DLBCL5
Afinitor® Non-functioning GI Lung NET6
CTL019a Leukemia
INC280b Solid tumors
Pan-DAC
CYP17
IAP
PI3K
porcupine
CDK4/6
Aldos
pan PIM
mTOR
MEK
CD19
Smo
HER3 FLT-3 Signifor®LAR11 Cushing’s somatostatin
PKC
HDM2/P53
c-MET
HSP90
PI3Kα
FGFR
mTOR
mTOR
mTOR
somatostatin
MEK+ B-RAF
PI3K
B-RAF
ALK
LDE225 Solid tumors
Smo
MEK162d Solid tumors
MEK
LEE011c Solid tumors
CDK4/6
LGX818 Solid tumors
B-RAF
NVS New Molecule
NVS New Indication
Tasigna CML Treatment Free Remission
LDE225 Medulloblastoma
PKC412 ASM9
Jakavi® e Polycythemia Vera
MEK162d LGSOC8
LDK378 ALK+Adv NSCLC3
(Chemo naïve,crizotinib naïve)
Smo
ALK
BCR-ABL
MEK
FLT-3
JAK
NVS New Formulation
1 Idiopathic thrombocytopenic purpura 2 Myelodysplastic syndrome/
Acute myeloid leukemia 3 Non-small cell lung cancer 4 Acute myeloid leukemia 5 Diffuse large B-cell lymphoma 6 Neuroendocrine tumors 7 Tuberous sclerosis complex 8 Low-grade serous ovarian cancer 9 Aggressive systemic mastocytosis 10 Chronic lymphocytic leukemia 11 Long-acting release 12 Severe aplastic anemia
a. CTL019 (also known as CART-19) is licensed from the University of Pennsylvania (Penn) and subject to the agreement between Novartis and Penn
b. INC280 (also known) as INCB028060) is licensed from Incyte Corp. c. LEE011 was discovered in collaboration with Astex d. MEK162 or ARRY-162 is licensed from Array BioPharma, Inc. e. Jakavi (INC424) is licensed from Incyte for development and commercialization outside of the US
* LBH589 submitted in the US in March 2014
BKM120 Solid tumors
PI3K
Registration Trials Phase IIII or pivotal
Filed (In Registration)
Confirmatory Trials (Phase I/II) Exploratory Trials
Afinitor TSC7 Seizures
mTOR
Novartis Oncology pipeline is industry leading in small molecule targeted therapies...
Daniele Alberti – Biobang Lecce – 12 novembre 2014
IGF1R
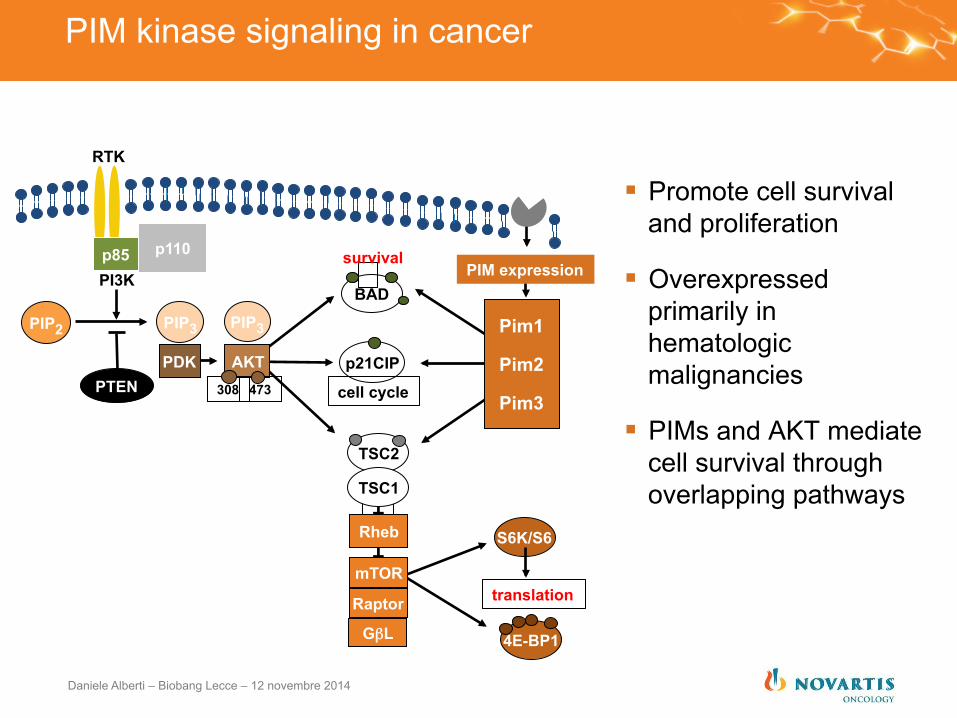
PIM kinase signaling in cancer
§ Promote cell survival and proliferation
§ Overexpressed primarily in hematologic malignancies
§ PIMs and AKT mediate cell survival through overlapping pathways
p110
RTK
PI3K p85
PIP2
PTEN
PIP3 PIP3
PDK AKT 308 473
Raptor
mTOR
GβL
p21CIP
BAD
T
T Rheb
survival
cell cycle
TSC2
TSC1
Pim1
Pim2
Pim3
4E-BP1
S6K/S6
translation
PIM expression
Daniele Alberti – Biobang Lecce – 12 novembre 2014
0.5 0
-0.5 -1
-1.5 -2
-2.5
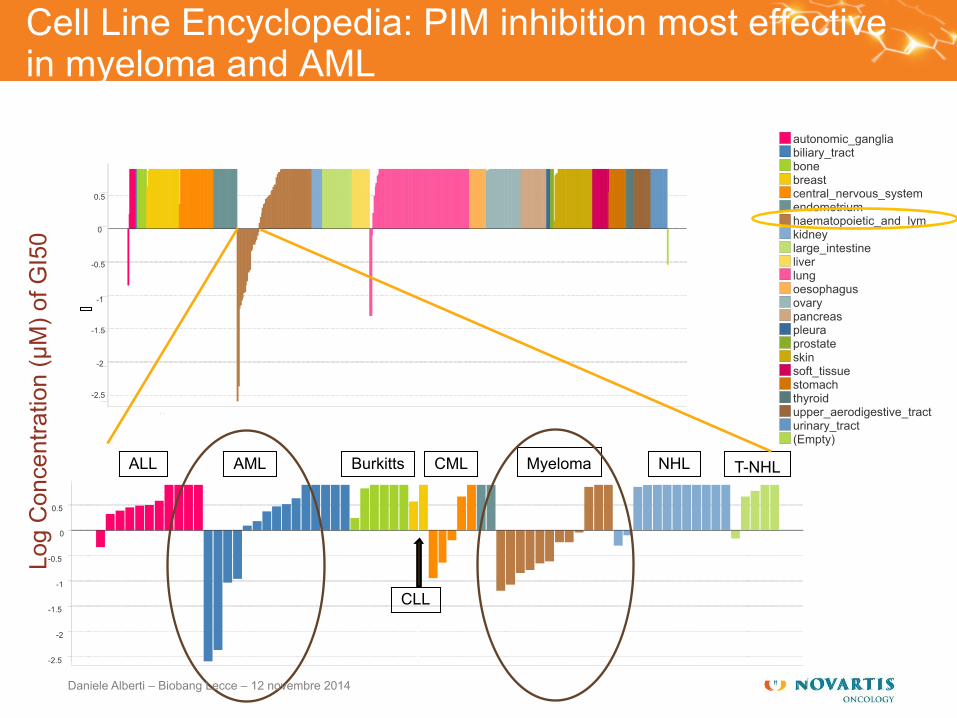
Cell Line Encyclopedia: PIM inhibition most effective in myeloma and AML
0.5 0
-0.5 -1
-1.5 -2
-2.5
autonomic_ganglia biliary_tract bone breast central_nervous_system endometrium haematopoietic_and_lym kidney large_intestine liver lung oesophagus ovary pancreas pleura prostate skin soft_tissue stomach thyroid upper_aerodigestive_tract urinary_tract (Empty)
Log
Con
cent
ratio
n (µ
M) o
f GI5
0
AML ALL Burkitts T-NHL NHL Myeloma
CLL
CML
Daniele Alberti – Biobang Lecce – 12 novembre 2014
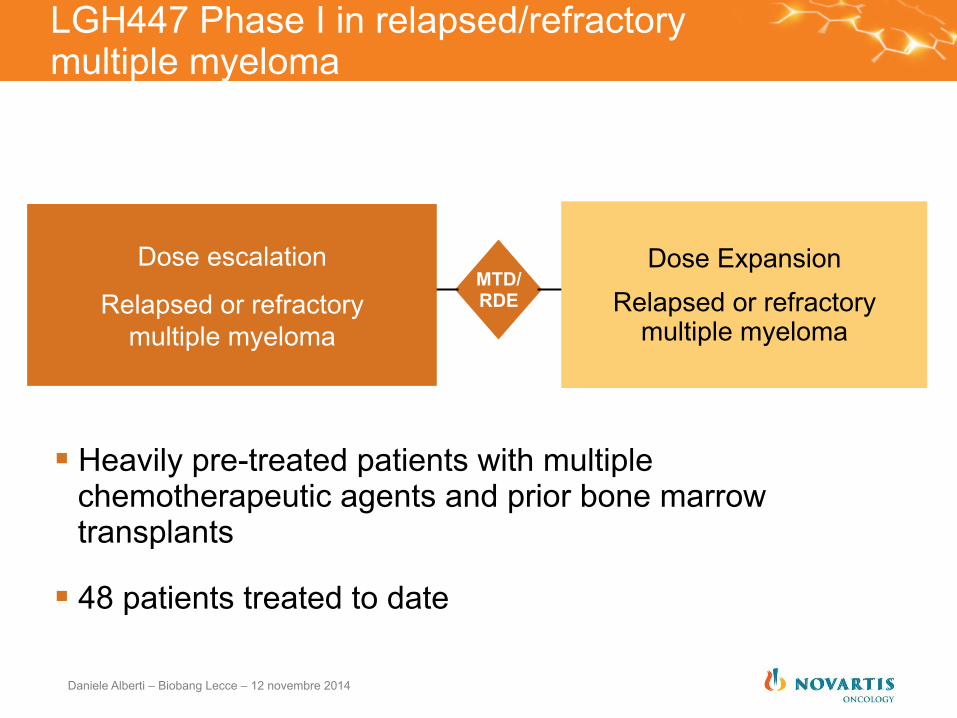
LGH447 Phase I in relapsed/refractory multiple myeloma
§ Heavily pre-treated patients with multiple chemotherapeutic agents and prior bone marrow transplants
§ 48 patients treated to date
Dose Expansion Relapsed or refractory
multiple myeloma
Dose escalation
Relapsed or refractory multiple myeloma
MTD/ RDE
Daniele Alberti – Biobang Lecce – 12 novembre 2014
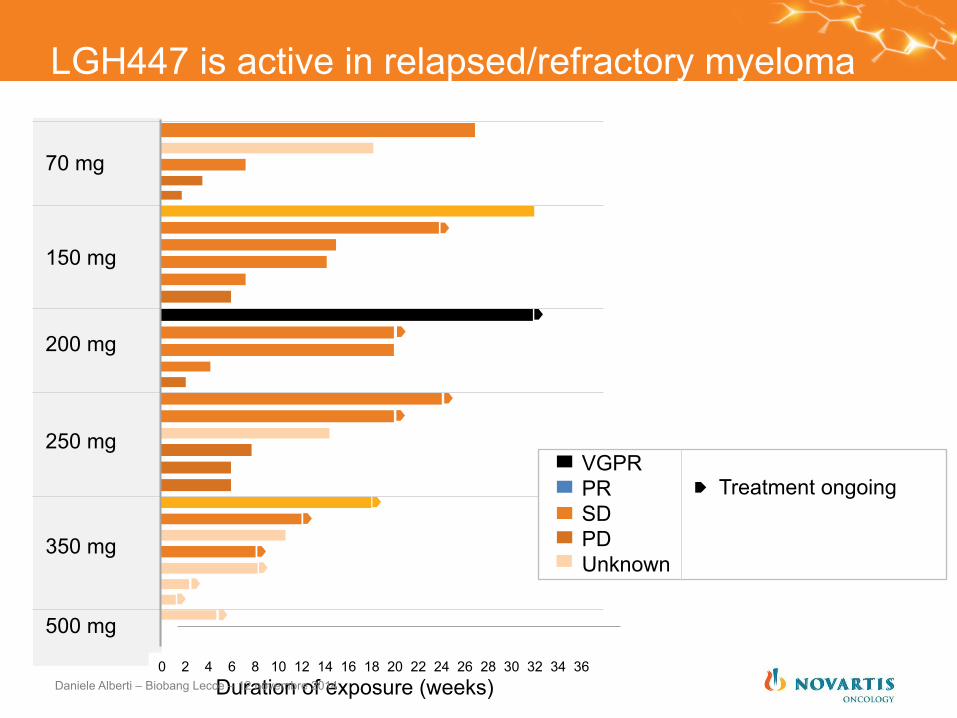
LGH447 is active in relapsed/refractory myeloma
70 mg
150 mg
200 mg
250 mg
350 mg
500 mg
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36
Treatment ongoing
VGPR PR SD PD Unknown
Duration of exposure (weeks) Daniele Alberti – Biobang Lecce – 12 novembre 2014
CDK4/6
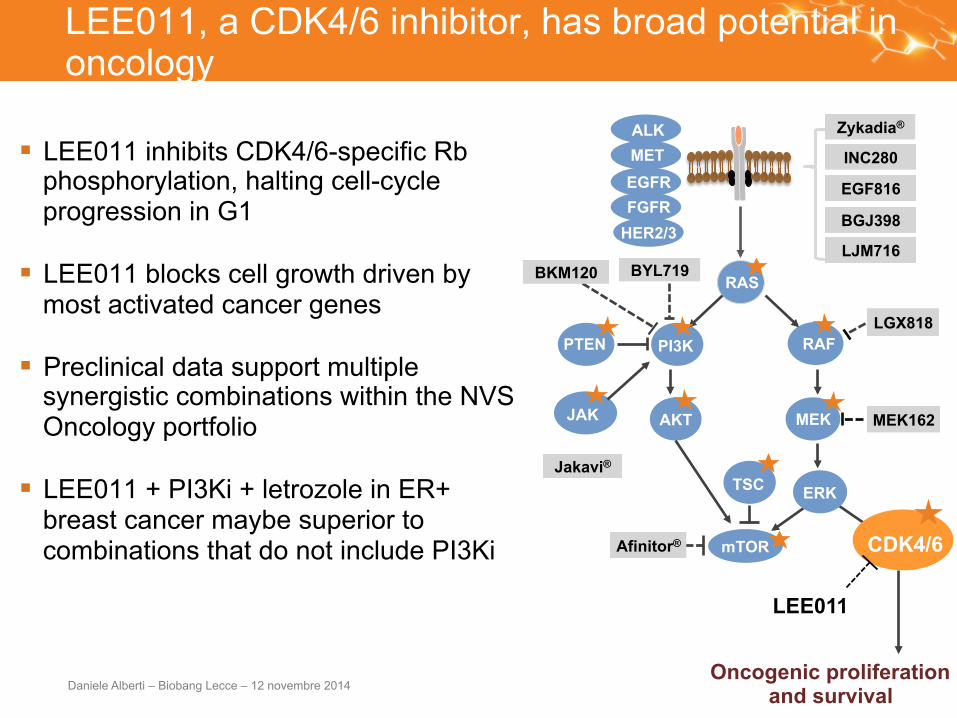
LEE011, a CDK4/6 inhibitor, has broad potential in oncology
§ LEE011 inhibits CDK4/6-specific Rb phosphorylation, halting cell-cycle progression in G1
§ LEE011 blocks cell growth driven by most activated cancer genes
§ Preclinical data support multiple synergistic combinations within the NVS Oncology portfolio
§ LEE011 + PI3Ki + letrozole in ER+ breast cancer maybe superior to combinations that do not include PI3Ki
E2F
RAS
RAF
MEK
ERK
PI3K
AKT
mTOR
BKM120
Afinitor®
BYL719
BGJ398
LEE011
LJM716
EGF816
INC280
Jakavi®
Zykadia®
MEK162
LGX818
JAK
TSC
PTEN
Oncogenic proliferation and survival
HER2/3 FGFR EGFR MET ALK
Daniele Alberti – Biobang Lecce – 12 novembre 2014
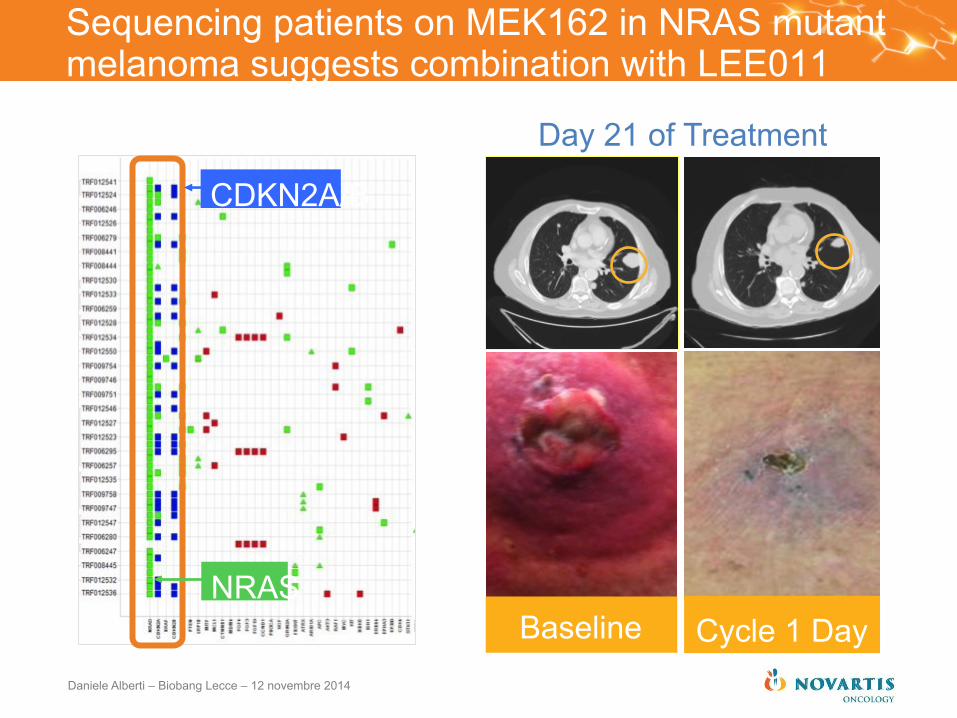
Sequencing patients on MEK162 in NRAS mutant melanoma suggests combination with LEE011
Day 21 of Treatment
Cycle 1 Day 31
Baseline
CDKN2A/B
NRAS
Daniele Alberti – Biobang Lecce – 12 novembre 2014
LGK974 Solid tumors
LCL161 Solid tumors
CGM097 Solid tumors
CFG920 Solid tumors
AEB071 Solid tumors
LGH447 Hemat. tumors
LDK378 ALK+ NSCLC3
BYL719 Solid tumors
LJM716 Solid tumors
LCI699 Cushing’s Syndrome
TKI258 Solid & Hemat. tumors
MEK162d NRAS Mutant Melanoma
BGJ398 Solid tumors
AUY922 Solid tumors
PKC412 AML4
MEK162 + LGX818 BRAF Mutant Melanoma
LGX818 BRAF Mutant Melanoma
LEE011c Breast Cancer
LDE225 Basal Cell Carcinoma
BKM120 Breast Cancer
LBH589* Multiple Myeloma
Signifor®LAR11 Acromegaly
Afinitor® HER2+ Breast Cancer 2nd/3rd
Line
Afinitor® HER2+ Breast Cancer 1st Line
Afinitor® DLBCL5
Afinitor® Non-functioning GI Lung NET6
CTL019a Leukemia
INC280b Solid tumors
Pan-DAC
CYP17
IAP
PI3K
porcupine
CDK4/6
Aldos
pan PIM
mTOR
MEK
CD19
Smo
HER3 FLT-3 Signifor®LAR11 Cushing’s somatostatin
PKC
HDM2/P53
c-MET
HSP90
PI3Kα
FGFR
mTOR
mTOR
mTOR
somatostatin
MEK+ B-RAF
PI3K
B-RAF
ALK
LDE225 Solid tumors
Smo
MEK162d Solid tumors
MEK
LEE011c Solid tumors
CDK4/6
LGX818 Solid tumors
B-RAF
NVS New Molecule
NVS New Indication
Tasigna CML Treatment Free Remission
LDE225 Medulloblastoma
PKC412 ASM9
Jakavi® e Polycythemia Vera
MEK162d LGSOC8
LDK378 ALK+Adv NSCLC3
(Chemo naïve,crizotinib naïve)
Smo
ALK
BCR-ABL
MEK
FLT-3
JAK
NVS New Formulation
1 Idiopathic thrombocytopenic purpura 2 Myelodysplastic syndrome/
Acute myeloid leukemia 3 Non-small cell lung cancer 4 Acute myeloid leukemia 5 Diffuse large B-cell lymphoma 6 Neuroendocrine tumors 7 Tuberous sclerosis complex 8 Low-grade serous ovarian cancer 9 Aggressive systemic mastocytosis 10 Chronic lymphocytic leukemia 11 Long-acting release 12 Severe aplastic anemia
a. CTL019 (also known as CART-19) is licensed from the University of Pennsylvania (Penn) and subject to the agreement between Novartis and Penn
b. INC280 (also known) as INCB028060) is licensed from Incyte Corp. c. LEE011 was discovered in collaboration with Astex d. MEK162 or ARRY-162 is licensed from Array BioPharma, Inc. e. Jakavi (INC424) is licensed from Incyte for development and commercialization outside of the US
* LBH589 submitted in the US in March 2014
BKM120 Solid tumors
PI3K
Registration Trials Phase IIII or pivotal
Filed (In Registration)
Confirmatory Trials (Phase I/II) Exploratory Trials
Afinitor TSC7 Seizures
mTOR
Novartis Oncology pipeline is industry leading in small molecule targeted therapies...
Daniele Alberti – Biobang Lecce – 12 novembre 2014
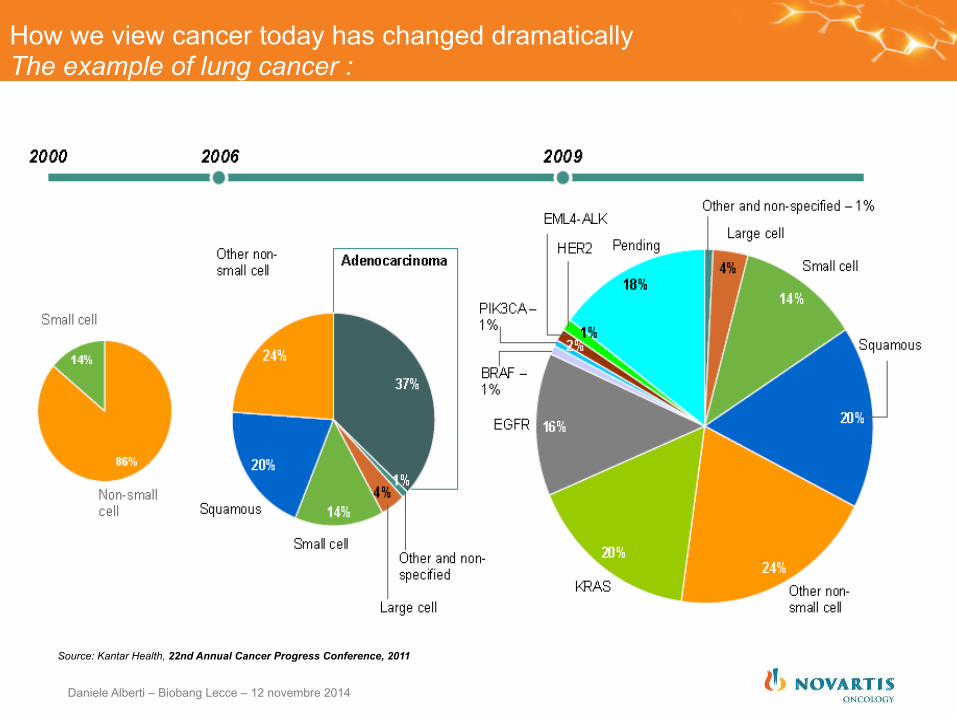
How we view cancer today has changed dramatically The example of lung cancer :
Source: Kantar Health, 22nd Annual Cancer Progress Conference, 2011
Daniele Alberti – Biobang Lecce – 12 novembre 2014
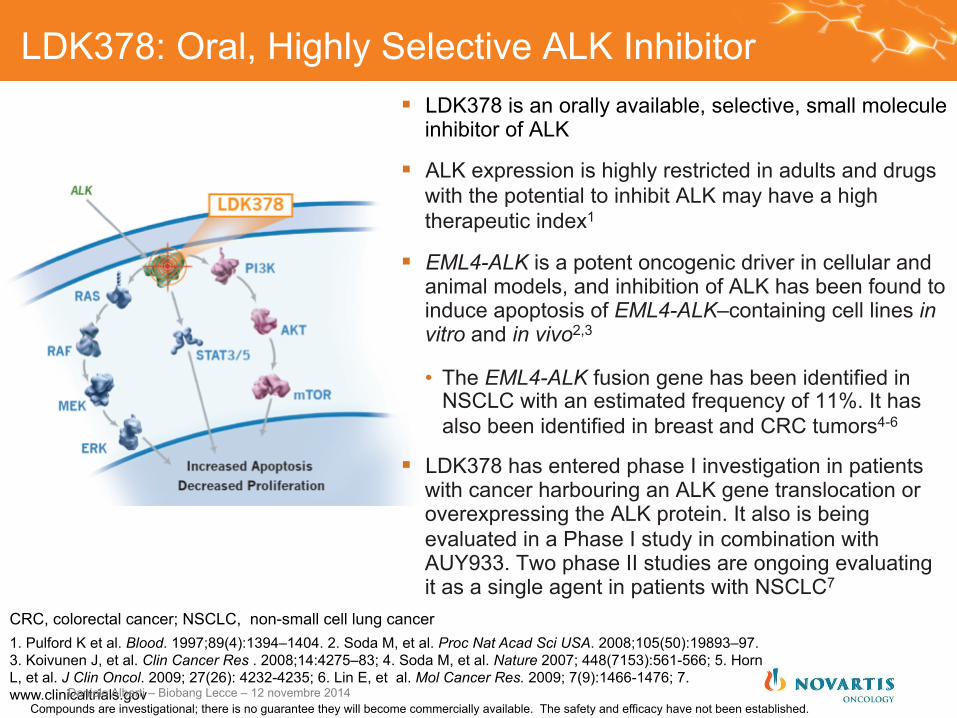
LDK378: Oral, Highly Selective ALK Inhibitor § LDK378 is an orally available, selective, small molecule
inhibitor of ALK
§ ALK expression is highly restricted in adults and drugs with the potential to inhibit ALK may have a high therapeutic index1
§ EML4-ALK is a potent oncogenic driver in cellular and animal models, and inhibition of ALK has been found to induce apoptosis of EML4-ALK–containing cell lines in vitro and in vivo2,3
• The EML4-ALK fusion gene has been identified in NSCLC with an estimated frequency of 11%. It has also been identified in breast and CRC tumors4-6
§ LDK378 has entered phase I investigation in patients with cancer harbouring an ALK gene translocation or overexpressing the ALK protein. It also is being evaluated in a Phase I study in combination with AUY933. Two phase II studies are ongoing evaluating it as a single agent in patients with NSCLC7
1. Pulford K et al. Blood. 1997;89(4):1394–1404. 2. Soda M, et al. Proc Nat Acad Sci USA. 2008;105(50):19893–97. 3. Koivunen J, et al. Clin Cancer Res . 2008;14:4275–83; 4. Soda M, et al. Nature 2007; 448(7153):561-566; 5. Horn L, et al. J Clin Oncol. 2009; 27(26): 4232-4235; 6. Lin E, et al. Mol Cancer Res. 2009; 7(9):1466-1476; 7. www.clinicaltrials.gov
CRC, colorectal cancer; NSCLC, non-small cell lung cancer
Compounds are investigational; there is no guarantee they will become commercially available. The safety and efficacy have not been established. Daniele Alberti – Biobang Lecce – 12 novembre 2014
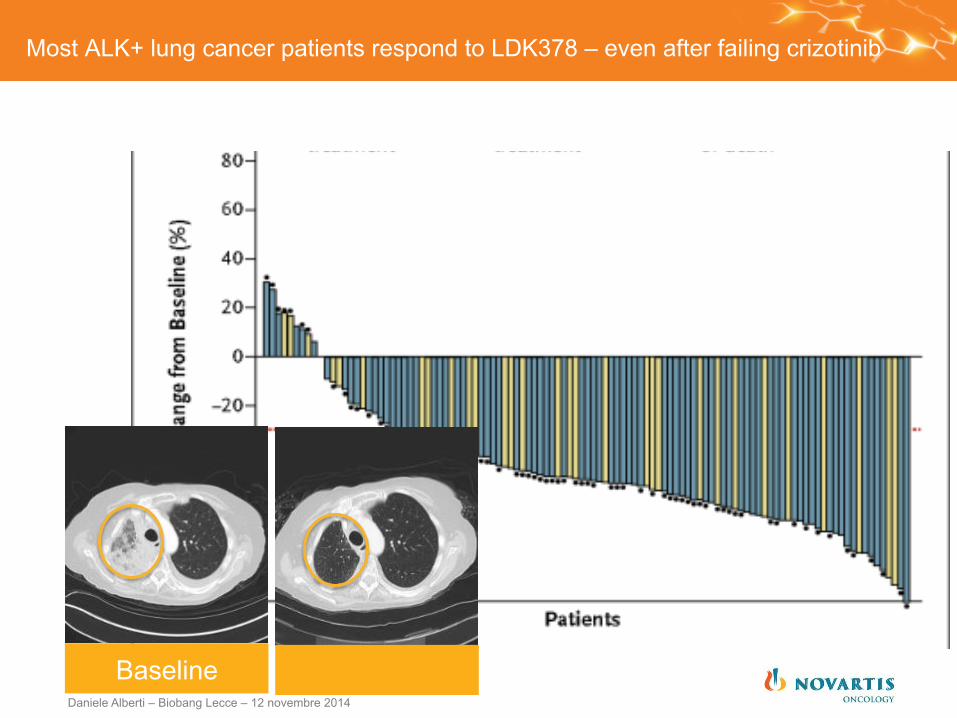
Most ALK+ lung cancer patients respond to LDK378 – even after failing crizotinib
Baseline Daniele Alberti – Biobang Lecce – 12 novembre 2014

Typical response to LDK378
AQer 3.5 weeks Baseline
Daniele Alberti – Biobang Lecce – 12 novembre 2014
The LDK378/ceritinib/Zykadia story began just three years ago
§ March 2011 first patient treated
§ November 2012 FDA Breakthrough Therapy designation
§ December 2013 FDA filing
§ April 2014 APPROVED!!!!
37 months from FPFV to filing
Italy contributed with 2 centers and 13 pts in dose escalation/espansion
Daniele Alberti – Biobang Lecce – 12 novembre 2014
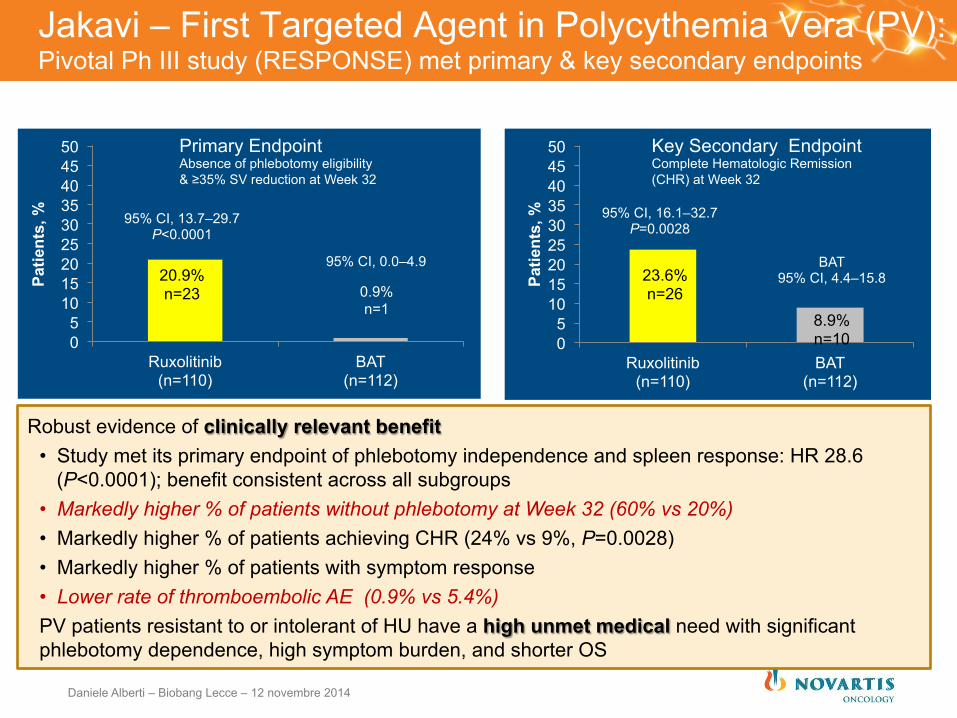
Jakavi – First Targeted Agent in Polycythemia Vera (PV): Pivotal Ph III study (RESPONSE) met primary & key secondary endpoints
0 5
10 15 20 25 30 35 40 45 50
Ruxolitinib (n=110)
BAT (n=112)
Patie
nts,
%
20.9% n=23 0.9%
n=1
95% CI, 13.7–29.7
P<0.0001
95% CI, 0.0–4.9
Primary Endpoint Absence of phlebotomy eligibility & ≥35% SV reduction at Week 32
0 5
10 15 20 25 30 35 40 45 50
Ruxolitinib (n=110)
BAT (n=112)
Patie
nts,
%
95% CI, 16.1–32.7
P=0.0028
23.6% n=26
8.9% n=10
BAT 95% CI, 4.4–15.8
Key Secondary Endpoint Complete Hematologic Remission (CHR) at Week 32
Robust evidence of clinically relevant benefit • Study met its primary endpoint of phlebotomy independence and spleen response: HR 28.6
(P<0.0001); benefit consistent across all subgroups • Markedly higher % of patients without phlebotomy at Week 32 (60% vs 20%) • Markedly higher % of patients achieving CHR (24% vs 9%, P=0.0028) • Markedly higher % of patients with symptom response • Lower rate of thromboembolic AE (0.9% vs 5.4%) PV patients resistant to or intolerant of HU have a high unmet medical need with significant phlebotomy dependence, high symptom burden, and shorter OS
Daniele Alberti – Biobang Lecce – 12 novembre 2014
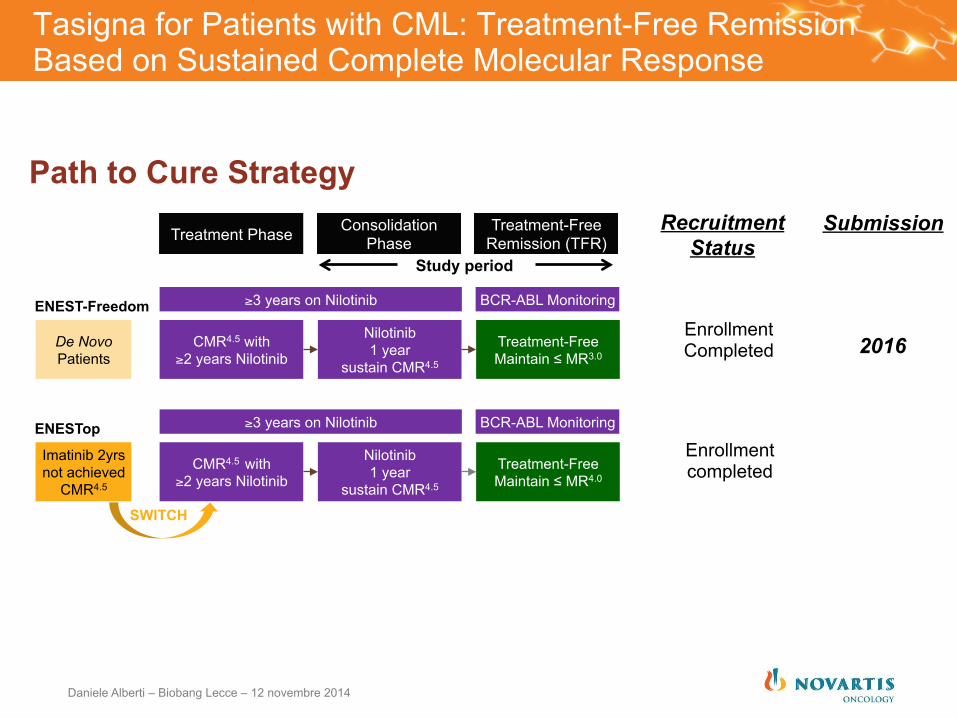
Tasigna for Patients with CML: Treatment-Free Remission Based on Sustained Complete Molecular Response
Path to Cure Strategy
Treatment Phase Consolidation Phase
Treatment-Free Remission (TFR)
≥3 years on Nilotinib BCR-ABL Monitoring
Nilotinib 1 year
sustain CMR4.5
CMR4.5 with ≥2 years Nilotinib
Treatment-Free Maintain ≤ MR3.0
De Novo Patients
ENEST-Freedom
≥3 years on Nilotinib BCR-ABL Monitoring
Nilotinib 1 year
sustain CMR4.5
CMR4.5 with ≥2 years Nilotinib
Treatment-Free Maintain ≤ MR4.0
Imatinib 2yrs not achieved
CMR4.5
ENESTop
SWITCH
Study period
Recruitment Status
Submission
2016
Enrollment completed
Enrollment Completed
Daniele Alberti – Biobang Lecce – 12 novembre 2014
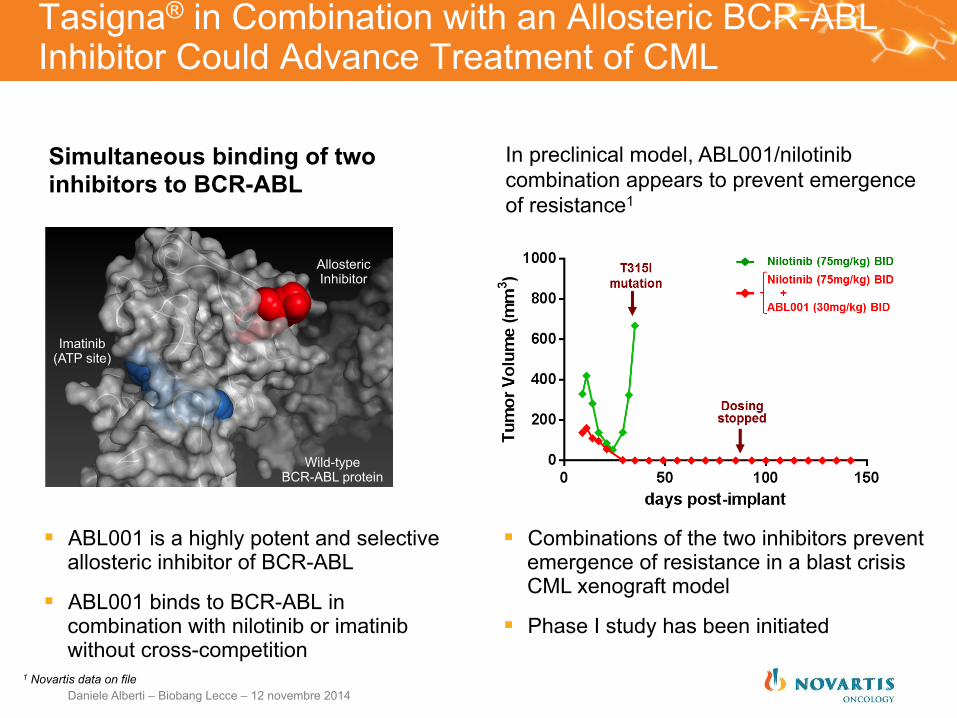
Tasigna® in Combination with an Allosteric BCR-ABL Inhibitor Could Advance Treatment of CML
Simultaneous binding of two inhibitors to BCR-ABL
§ ABL001 is a highly potent and selective allosteric inhibitor of BCR-ABL
§ ABL001 binds to BCR-ABL in combination with nilotinib or imatinib without cross-competition
Imatinib (ATP site)
Allosteric Inhibitor
Wild-type BCR-ABL protein
In preclinical model, ABL001/nilotinib combination appears to prevent emergence of resistance1
§ Combinations of the two inhibitors prevent emergence of resistance in a blast crisis CML xenograft model
§ Phase I study has been initiated
1 Novartis data on file Daniele Alberti – Biobang Lecce – 12 novembre 2014
CONCLUSIONS
§ Clonal heterogeneity is prevalent
§ Minor clones can be lethal
§ Mutuation profiling has potential to identify drug resistant clones and remission status in real time
§ Clinical Markers of drug response are emerging
§ IMiD: Cereblon, Ikaros, IRF4
§ Proteasome: IRE1, XBP1
Daniele Alberti – Biobang Lecce – 12 novembre 2014
Potential future applications
§ Diagnostic: Predictive biomarker for distinct disease subtype
§ Therapeutic: Different predicted response to epigenetic and/or tyrosine kinase inhibitors
§ Paradigm for other cancers: Does the order of acquisition matter in other cancers?
Daniele Alberti – Biobang Lecce – 12 novembre 2014
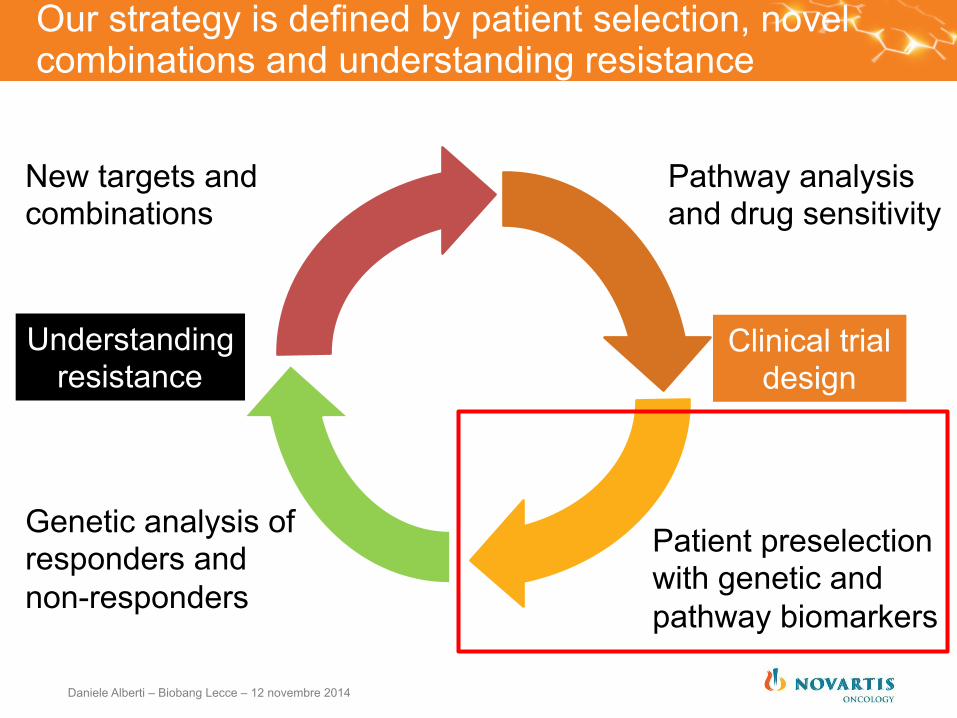
Our strategy is defined by patient selection, novel combinations and understanding resistance
Pathway analysis and drug sensitivity
Patient preselection with genetic and pathway biomarkers
Genetic analysis of responders and non-responders
New targets and combinations
Clinical trial design
Understanding resistance
Daniele Alberti – Biobang Lecce – 12 novembre 2014
Window of opportunity trials Rationale § With many new targeted therapies, there are limitations in measuring response by
traditional methods, such as response rate defined by RECIST criteria, which may lead to erroneous conclusions about a drug’s benefit.
§ Evaluating molecular end points can be hindered by difficulties in procuring tumor tissue before and after drug administration and by heterogeneity in previous exposure to cancer therapies.
§ A method to circumvent this issue is to assess novel agents in pre-surgical (window-of-opportunity) trials. In this model, women with newly diagnosed breast cancer, for instance, receive a study drug between the diagnostic breast biopsy and planned surgical resection (typically 2-4 week period).
§ Goals of these trials include: • Evaluation of target modulation after drug exposure • Pharmacokinetic assessments of a potential anticancer agent • Improve understanding of an agent’s biologic effect early in its development • Validate markers that may predict subsets of patients who will/will not benefit • Targeting select patients in subsequent clinical trials that are powered to detect
changes in clinical outcome
Kalinsky J Clin Oncol. 30(21):2573-5
Daniele Alberti – Biobang Lecce – 12 novembre 2014
FDA Guidance
§ The US Food and Drug Administration issued Guidance on “Exploratory Investigational New Drug Studies” in 2006 in which it was described that: • Exploratory IND studies usually involve very limited human exposure and
have no therapeutic or diagnostic intent. Such studies can serve a number of useful goals. For example, an exploratory IND study can help sponsors 1. Determine whether a mechanism of action defined in experimental
systems can also be observed in humans (e.g., a binding property or inhibition of an enzyme)
2. Provide important information on pharmacokinetics (PK) 3. Select the most promising lead product from a group of candidates
designed to interact with a particular therapeutic target in humans, based on PK or pharmacodynamic (PD) properties
§ An example of 3. also includes “window of opportunity pre-surgical trials”
Daniele Alberti – Biobang Lecce – 12 novembre 2014
Novartis’ Bayesian Phase I: External Outreach
§ Engaging Health Authorities and Gaining Acceptance • Presented to FDA Biostatisticians and Oncologists at White Oak Campus
(Jun 2009) • Commented on Draft FDA Adaptive Design Guidance (May 2010) • Discussed with Japanese PMDA to gain acceptance to implement in several
Phase I studies (Jan 2009) • Presentation to PMDA on Bayesian Statistics (Nov 2010)
§ Scientific Leadership • Session #493 at Joint Statistical Meetings on Aug 5, 2009 (Discussant:
Michael Brave, FDA Oncologist) • Roundtable #44 at 2010 FDA-Industry Workshop on Sept 21, 2010
(Discussant: Sue-Jane Wang, FDA Biostatistician) • Phase I Design Workshop, New York, Oct 2009
Daniele Alberti – Biobang Lecce – 12 novembre 2014

Dose Escalation Study Challenges and design overview
Right Regimen? Right Recipients? Robustly? Rapidly?
Safely determine with limited sample size
Daniele Alberti – Biobang Lecce – 12 novembre 2014
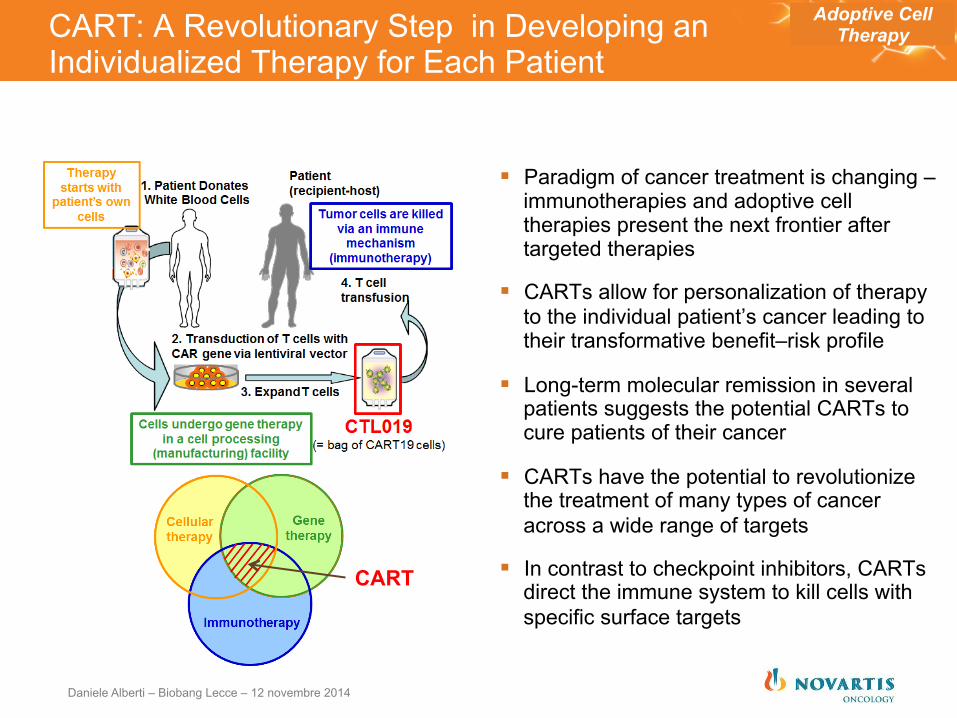
CART: A Revolutionary Step in Developing an Individualized Therapy for Each Patient
§ Paradigm of cancer treatment is changing – immunotherapies and adoptive cell therapies present the next frontier after targeted therapies
§ CARTs allow for personalization of therapy to the individual patient’s cancer leading to their transformative benefit–risk profile
§ Long-term molecular remission in several patients suggests the potential CARTs to cure patients of their cancer
§ CARTs have the potential to revolutionize the treatment of many types of cancer across a wide range of targets
§ In contrast to checkpoint inhibitors, CARTs direct the immune system to kill cells with specific surface targets
Adoptive Cell Therapy
CART
Daniele Alberti – Biobang Lecce – 12 novembre 2014
Agenda
14.00 – 14.10 Introduzione e agenda
14.10 – 14.50 Strategia di sviluppo nuovi prodotti in indicazioni onco- ematologiche
14.50 - 15.10 Opportunità di rilancio: Clinical Trial Center (CTC), Reti Oncologiche ed Ematologiche e laboratori regionali
15.10 - 15.30 Discussione / Presentazione Lavori di gruppo
15.30 – 16.30 Lavori di gruppo
16.30 – 17.00 Feedback in plenaria dai Gruppi di lavoro
17.00 – 17.15 Conclusioni
Daniele Alberti – Biobang Lecce – 12 novembre 2014
Il Trial Office o Trial Center Alcuni centri di ricerca clinica all’avanguardia si stanno orientando verso la creazione di Trial Office o Trial Centre.
Di cosa si tratta?
Si tratta di una organizzazione che ha lo scopo di supportare e coordinare la conduzione e la gestione della ricerca clinica presso il centro e in centri sperimentali afferenti, supportare gli sperimentatori nel garantire l’aderenza alle Good Clinical Practices (GCP) nello studio di nuovi farmaci e dispositivi, e offrire servizi di Contract Research Organization (CRO) accademica alle aziende farmaceutiche.
Daniele Alberti – Biobang Lecce – 12 novembre 2014

Il «ciclo di vita» di una ricerca clinica
Pianificazione
• Stesura del protocollo e della documentazione a supporto • Selezione dei fornitori (lab centralizzati, logistica farmaco, data management, CRO, ecc.) • Analisi di fattibilità e selezione dei centri • Definizione del team di studio e relative attività di formazione • Definizione delle tempistiche dello studio
Avvio e Conduzione
• Ottenimento delle autorizzazioni regolatorie e etico-amministrative • Attivazione centri • Arruolamento • Monitoraggio e data management
Chiusura Analisi e report finale
• Completamento delle attività di cleaning e chiusura del database • Analisi statistica • Chiusura dei centri • Conclusioni cliniche in base ai risultati dell’analisi statistica • Stesura del report clinico statistico integrato ed eventuali pubblicazioni • Sottomissione alle autorità regolatorie
Daniele Alberti – Biobang Lecce – 12 novembre 2014
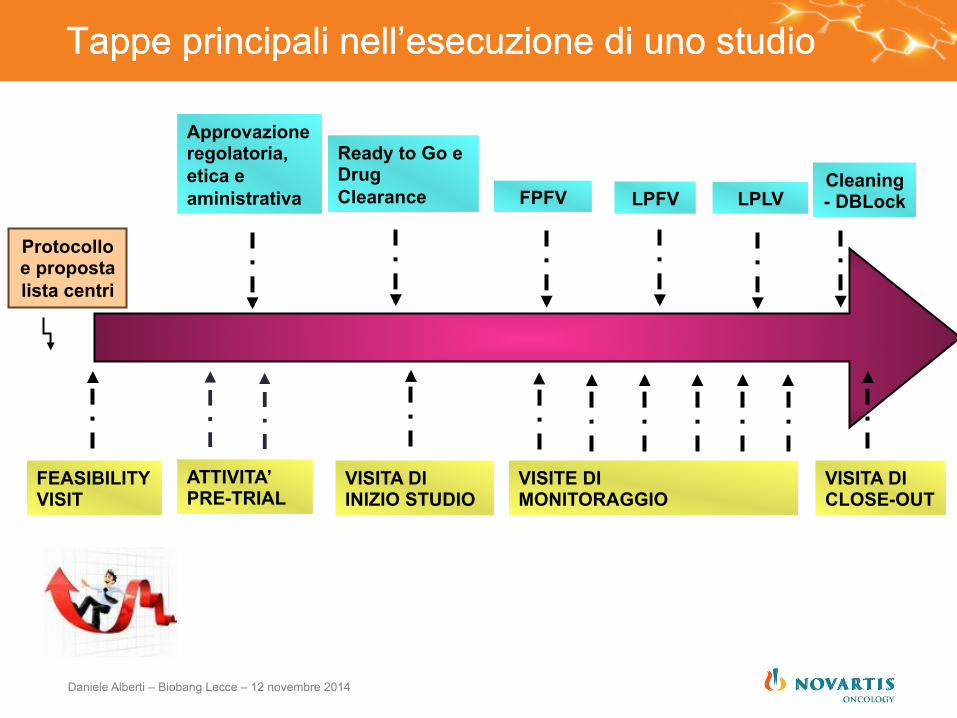
Protocollo e proposta lista centri
FEASIBILITY VISIT
ATTIVITA’ PRE-TRIAL
VISITA DI INIZIO STUDIO
VISITE DI MONITORAGGIO
VISITA DI CLOSE-OUT
Approvazione regolatoria, etica e aministrativa
Ready to Go e Drug Clearance FPFV LPLV LPFV
Cleaning - DBLock
Tappe principali nell’esecuzione di uno studio Tappe principali nell’esecuzione di uno studio
Daniele Alberti – Biobang Lecce – 12 novembre 2014
Il valore aggiunto del Trial Center nell’attivazione del centro
§ Preparazione della documentazione per sottomissione ad AIFA* (Autorità Competente) e ai CE • Segnalazione allo Sponsor della documentazione necessaria per la
prevalutazione dello studio • Preparazione della documentazione aggiuntiva per la pre-valutazione dello
studio
§ Sottomissione al CE coordinatore e ai CE dei Centri satellite e AIFA* • Valutazione in parallelo a AIFA*/ISS/Centro Coordinatore • Interazione con il CE al fine di ottenere tempestivamente il verbale
* per studi di fase I, AIFA si avvale dell’Ufficio Sperimentazioni Cliniche di ISS per la valutazione
1. supporto attività di Trial Start Up
Daniele Alberti – Biobang Lecce – 12 novembre 2014
§ Gestione pratiche amministrative (delibera, convenzione economica) con centro sperimentale • Finalizzazione degli accordi economici prima della seduta di
prevalutazione • Supporto nell’approvazione della bozza di convenzione dopo la
seduta del CE • Supporto nella raccolta delle firme della convenzione e della delibera
2. supporto nella gestione contrattuale
3. supporto nella raccolta dei documenti per l’attivazione del centro § Raccolta tempestiva e precoce dei documenti
necessari al team di monitoraggio per l’apertura del centro e l’invio del farmaco
Il valore aggiunto del Trial Center nell’attivazione del centro
Daniele Alberti – Biobang Lecce – 12 novembre 2014
Prima della visita del paziente: organizzazione e preparazione delle visite dei pazienti
§ contatti con gli specialisti, § preparazione di kit di laboratorio, § Identificazione del farmaco da assegnare ai pazienti § consensi previsti dallo studio o documenti a supporto della visita
del paziente § Gestione del farmaco
Durante la visita del paziente
§ Supporto al team dello studio nella gestione appropriata della visita e delle valutazioni (gestione dei kit di laboratorio, questionari e diari paziente, appuntamenti con gli specialisti...)
§ compilazione della drug accountability e supporto al team medico per la verifica della compliance
Il valore aggiunto del Trial Office: la gestione operativa dello studio
Daniele Alberti – Biobang Lecce – 12 novembre 2014
Dopo la visita del paziente § Inserimento tempestivo dei dati in CRF e
risposta alla queries § Invio tempestivo dei campioni al laboratorio
centrale § Invio tempestivo degli ECG e delle immagini
radiologiche al vendor § Visite di monitoraggio e interazione continua
con i team di monitoraggio § Interazione con i team locali e internazionali
dello sponsor e i vendors
Il valore aggiunto del Trial Office: la gestione operativa dello studio
Per gli studi di fase I ma non solo § Partecipazione a teleconferenze di aggiornamento dello studio
(es Dose Escalation Meeting per gli studi di fase I) § SIV o training di protocollo in TC con il clinical team § Contatti con il clinical team per discutere problematiche
specifiche dei pazienti § Identificazione e gestione delle DLT § Disponibilità 24 ore/24
Daniele Alberti – Biobang Lecce – 12 novembre 2014
Ma non dimentichiamo... § Completamento dei training richiesti § Conservazione e mantenimento della
documentazione di studio § Revisione della documentazione di studio
§ Protocolli e emendamenti § Manuali § Comunicazioni dello sponsor § Comunicazioni di safety (es IB e SUSAR)
§ Allineamento dello staff del centro § Contatti con il Comitato Etico § Contatti con i vendor § Conservazione del farmaco durante lo studio
Il valore aggiunto del Trial Center: la gestione operativa dello studio
Daniele Alberti – Biobang Lecce – 12 novembre 2014
Si stanno introducendo ormai da qualche tempo nuovi paradigmi di monitoraggio, quindi il monitoraggio cosiddetto on-site viene sostituito o alternato al cosiddetto monitoraggio remoto
Questi nuovi paradigmi di monitoraggio sfruttano le tecnologie oggi disponibili e permettono l’accesso remoto e in tempo reale, ai dati degli studi clinici (eCRF web-based, EMR –Electronic Medical Records)
Il valore aggiunto del Trial Center: il monitoraggio da remoto
Daniele Alberti – Biobang Lecce – 12 novembre 2014
Monitoraggio dello studio: cosa sta cambiando
Daniele Alberti – Biobang Lecce – 12 novembre 2014
Il monitoraggio da remoto si affianca quindi alle tradizionali attività di monitoraggio dei CRA effettuate “on-site“ (al Centro):
• Il CRA può monitorare i dati dello studio da remoto tramite un accesso diretto al database clinico
• I dati vengono rivisti da remoto, in "tempo reale", e vengono valutati per completezza, qualità e coerenza
• Contatti regolari con il centro via telefono, e-mail e visite “on-site” permettono di assicurare qualità e disponibilità dei dati in eCRF
• Le visite “on-site” presso il centro sono programmate in funzione dell’arruolamento dei pazienti e della qualità dei dati valutata durante il monitoraggio remoto
L’inserimento tempestivo dei dati da parte del centro è il prerequisito essenziale per l’effettuazione del
monitoraggio remoto da parte del CRA
Agenda
14.00 – 14.10 Introduzione e agenda
14.10 – 14.50 Strategia di sviluppo nuovi prodotti in indicazioni onco- ematologiche
14.50 - 15.10 Opportunità di rilancio: Clinical Trial Center (CTC), Reti Oncologiche ed Ematologiche e laboratori regionali
15.10 - 15.30 Discussione / Presentazione Lavori di gruppo
15.30 – 16.30 Lavori di gruppo
16.30 – 17.00 Feedback in plenaria dai Gruppi di lavoro
17.00 – 17.15 Conclusioni
Daniele Alberti – Biobang Lecce – 12 novembre 2014
Contenuto & obiettivi progetto
Ø Realizzazione cluster biotecnologico della REL per l'implementazione dell'analisi genomica e lo sviluppo di trattamenti innovativi nelle neoplasie ematologiche
Ø Implementazione di sistemi diagnostici/prognostici Ø Creazione piattaforma bioinformatica Ø Realizzazione REL Clinical Trial Unit Ø Valorizzazione capitale umano e integrazione di
giovani ricercatori
Un esempio: Bando Regione Lombardia – Fondazione Cariplo
Daniele Alberti – Biobang Lecce – 12 novembre 2014
Risultati attesi in numeri
Ø L’aiuto finalizzato alla realizzazione di REL Clinical Trial Unit, consentirà un aumento delle dimensioni del progetto pari al 25% (in termini assoluti 400.000 euro), con un incremento contestuale del numero di persone assegnate ad attività di RSI (con un investimento in termini assoluti di 240.000 euro).
Ø In termini quantitativi ci aspettiamo che attraverso la realizzazione di REL Clinical Trial Unit, rispetto agli indicatori di attività del progetto, vi sia un aumento del 20% del numero di studi clinici realizzati con farmaci a bersaglio molecolare.
Daniele Alberti – Biobang Lecce – 12 novembre 2014
Tempistica
q Sett 2013: sottomissione progetto al bando Cariplo-Regione Lombardia
q Dic 2013: conferma ammissione
q Feb 2014: • incontro con Dr. Della Porta per definire step di
attivazione progetto • procedure amministrative da seguire
q Ongoing: • Realizzazione progetto • Rendicontazione
Daniele Alberti – Biobang Lecce – 12 novembre 2014
Agenda
14.00 – 14.10 Introduzione e agenda
14.10 – 14.50 Strategia di sviluppo nuovi prodotti in indicazioni onco- ematologiche
14.50 - 15.10 Opportunità di rilancio: Clinical Trial Center (CTC), Reti Oncologiche ed Ematologiche e laboratori regionali
15.10 - 15.30 Discussione / Presentazione Lavori di gruppo
15.30 – 16.30 Lavori di gruppo
16.30 – 17.00 Feedback in plenaria dai Gruppi di lavoro
17.00 – 17.15 Conclusioni
Daniele Alberti – Biobang Lecce – 12 novembre 2014
Some suggestions for Clinical Research regarding the“Sistema Paese”
• University – professional training/educa7on:
– MDs & biotechnologists à clinical research
– Data manager – Research Nurses
• Hospitals/University – take advantage of clinical research:
– Clinical Trial Centers – Dedicated human resourses – Integrated mul)disciplinary
approach: clinical medicine, imaging, pathological anatomy, labs
– Administra)ons facilita)ng authorizing processes
– Coordinated & Aligned Ethical Commi[ees
• Elimina7on of “Ins7tu7onal Silos” and ra7onaliza7on of rules in order to facilitate inves7ments in clincal research:
– Ministry of Health – AIFA – ISS – Regions – Assurance Companies – Privacy Authority – Tax Benefits
• Pharmaceu7cal / Biotec Companies: – Willingness to invest in Italy – Recognize contribu)on of Italian
Centers of Excellence – Partnership with local, regional and
na)onal organiza)ons – A[en)on to Pa)ents’ Associa)ons 62
Daniele Alberti – Biobang Lecce – 12 novembre 2014
Daniele Alberti – Biobang Lecce – 12 novembre 2014
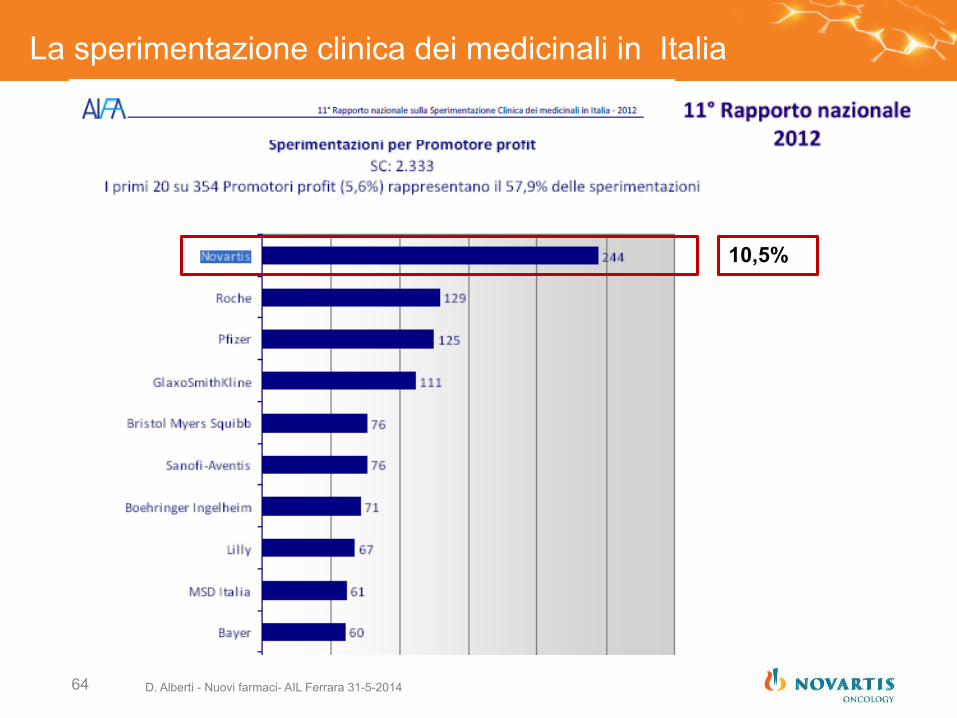
10,5%
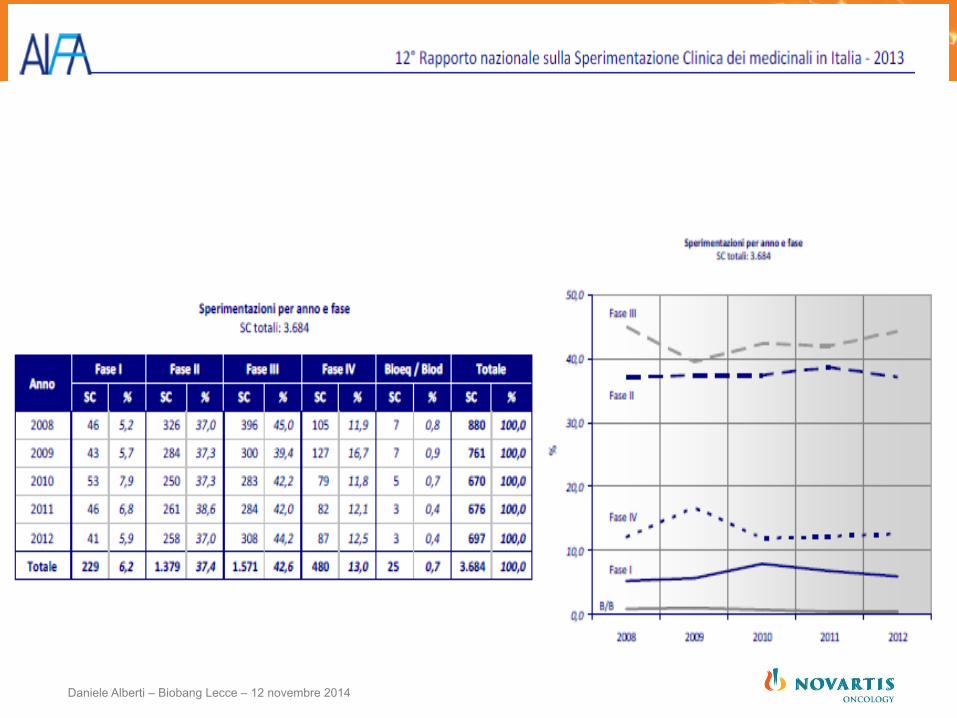
La sperimentazione clinica dei medicinali in Italia
D. Alberti - Nuovi farmaci- AIL Ferrara 31-5-2014 64
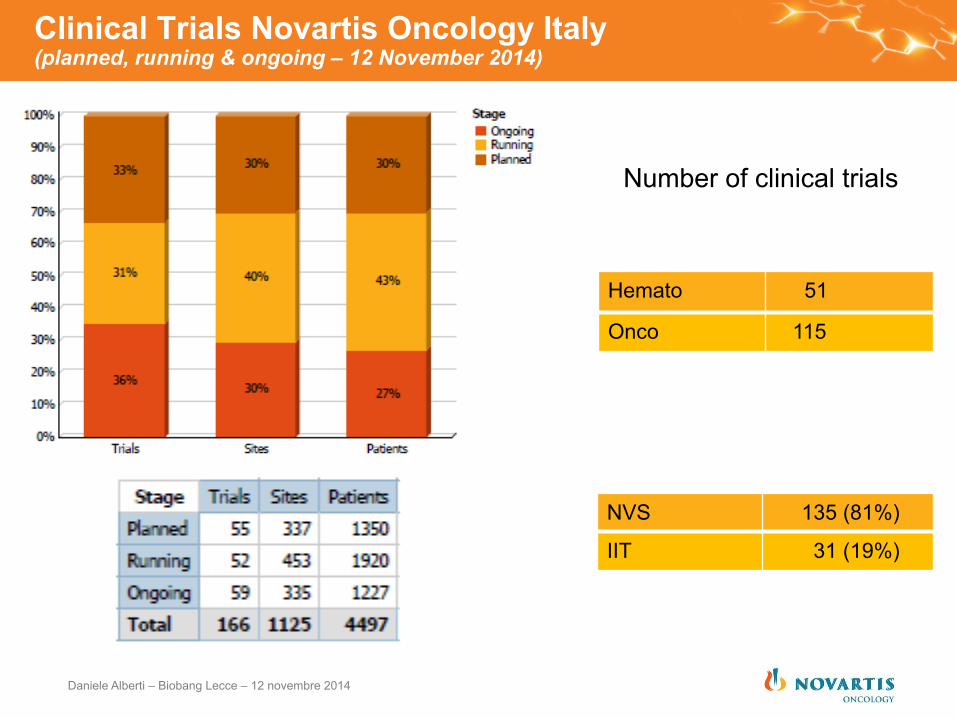
Clinical Trials Novartis Oncology Italy (planned, running & ongoing – 12 November 2014)
NVS 135 (81%)
IIT 31 (19%)
Hemato 51
Onco 115
Number of clinical trials
Daniele Alberti – Biobang Lecce – 12 novembre 2014
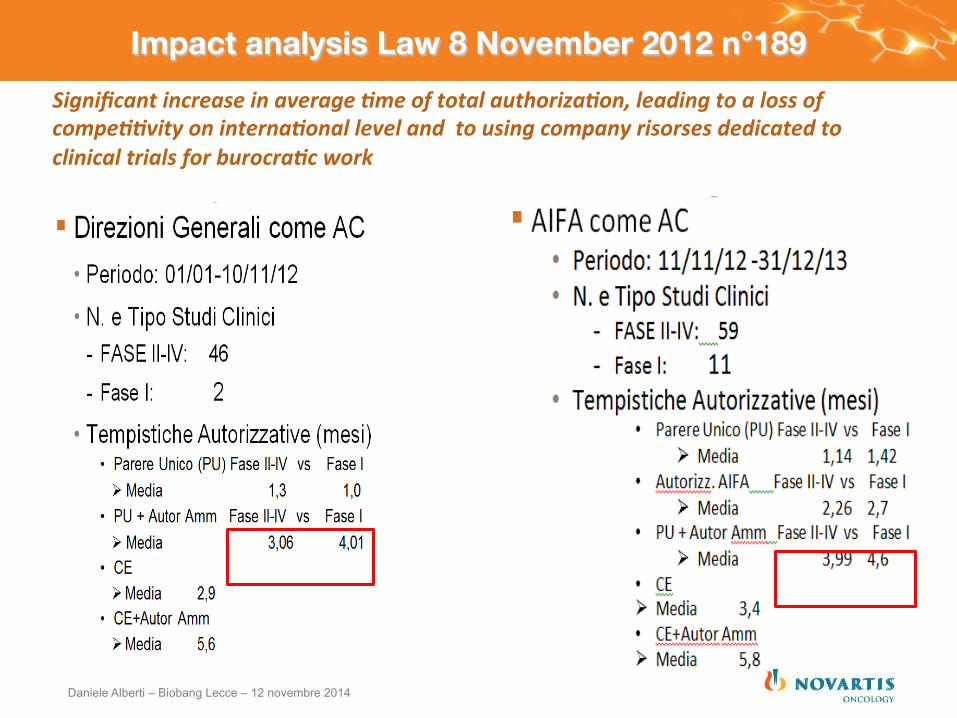
Impact analysis Law 8 November 2012 n°189 Significant increase in average .me of total authoriza.on, leading to a loss of compe..vity on interna.onal level and to using company risorses dedicated to clinical trials for burocra.c work
Daniele Alberti – Biobang Lecce – 12 novembre 2014

Some state-of –the-art Clinical Research Centers are creating Trial Offices or Trial Centers.
Organization to support and coordinate:
§ Implementation and managing of Clinical Research in the site as well as in afferent sites
§ Support researchers in respecting Good Clinical Practices (GCP) while studying new drugs and devices,
§ Offer accademical Contract Research Organization (CRO) services to pharmaceutical / biotech companies.
Clinical Trial Office / Trial Center
Daniele Alberti – Biobang Lecce – 12 novembre 2014
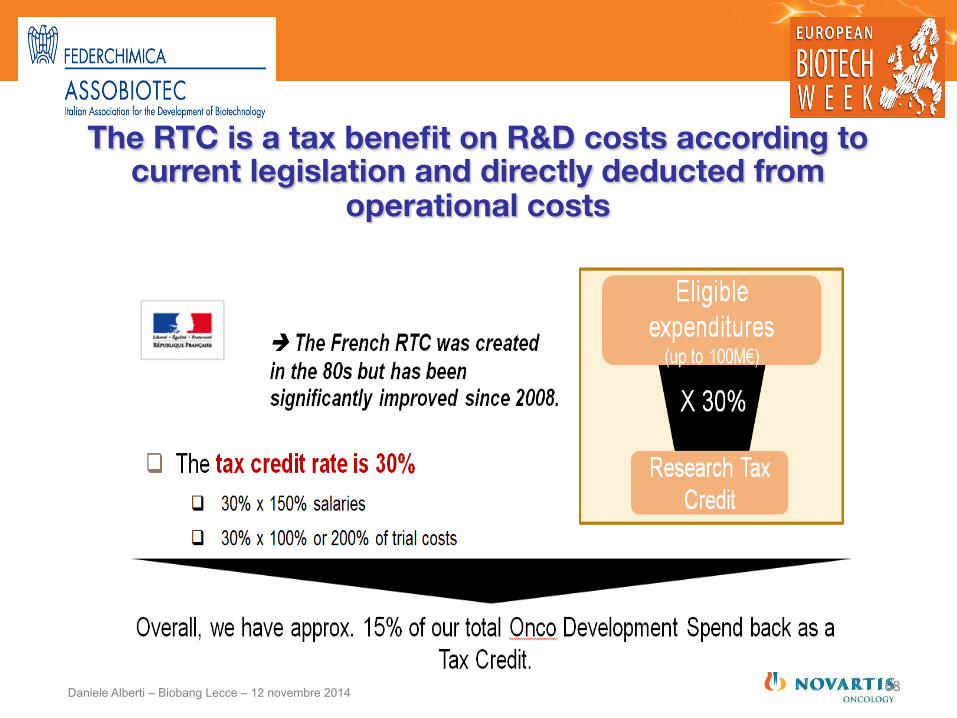
The RTC is a tax benefit on R&D costs according to current legislation and directly deducted from
operational costs
68 Daniele Alberti – Biobang Lecce – 12 novembre 2014
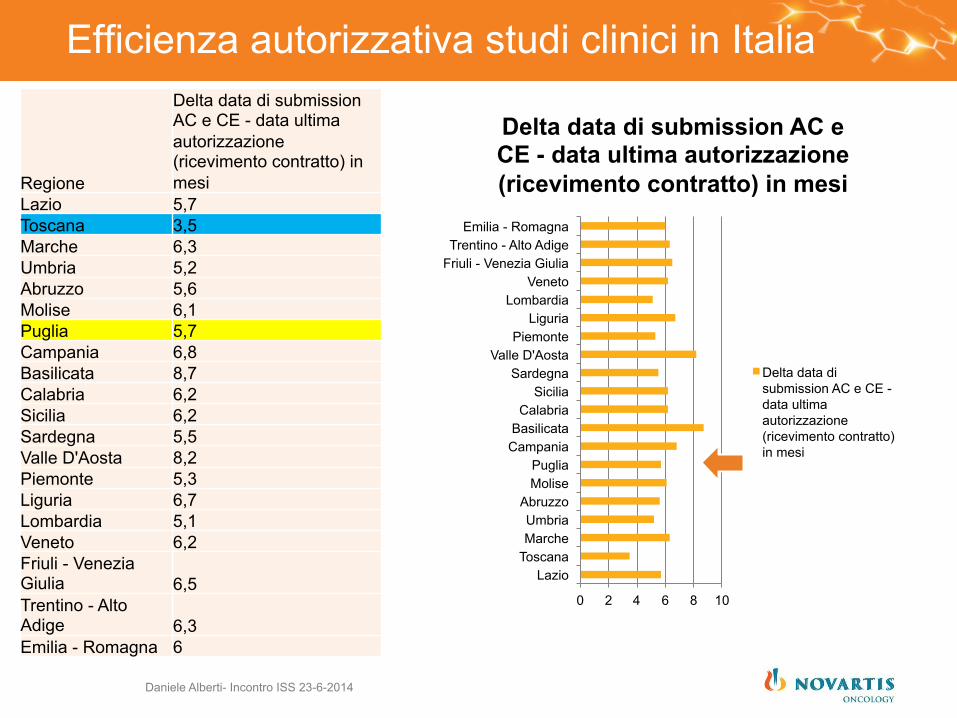
Efficienza autorizzativa studi clinici in Italia
Daniele Alberti- Incontro ISS 23-6-2014
Regione
Delta data di submission AC e CE - data ultima autorizzazione (ricevimento contratto) in mesi
Lazio 5,7 Toscana 3,5 Marche 6,3 Umbria 5,2 Abruzzo 5,6 Molise 6,1 Puglia 5,7 Campania 6,8 Basilicata 8,7 Calabria 6,2 Sicilia 6,2 Sardegna 5,5 Valle D'Aosta 8,2 Piemonte 5,3 Liguria 6,7 Lombardia 5,1 Veneto 6,2 Friuli - Venezia Giulia 6,5 Trentino - Alto Adige 6,3 Emilia - Romagna 6
0 2 4 6 8 10
Lazio Toscana Marche Umbria
Abruzzo Molise Puglia
Campania Basilicata Calabria
Sicilia Sardegna
Valle D'Aosta Piemonte
Liguria Lombardia
Veneto Friuli - Venezia Giulia Trentino - Alto Adige
Emilia - Romagna
Delta data di submission AC e CE - data ultima autorizzazione (ricevimento contratto) in mesi
Delta data di submission AC e CE - data ultima autorizzazione (ricevimento contratto) in mesi
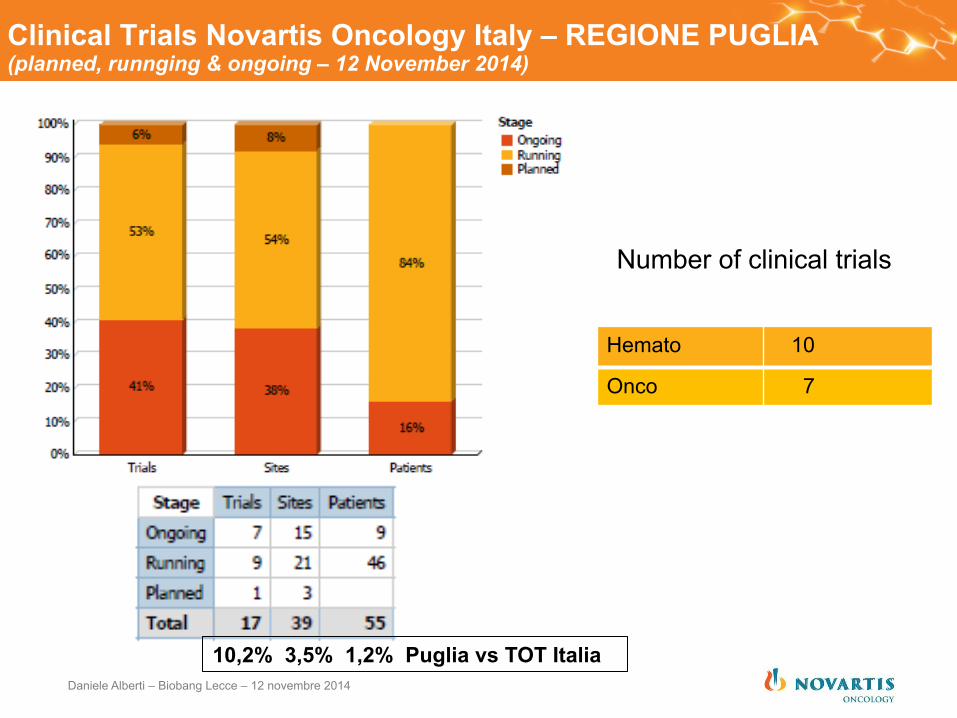
Clinical Trials Novartis Oncology Italy – REGIONE PUGLIA (planned, runnging & ongoing – 12 November 2014)
Hemato 10
Onco 7
Number of clinical trials
Daniele Alberti – Biobang Lecce – 12 novembre 2014
10,2% 3,5% 1,2% Puglia vs TOT Italia
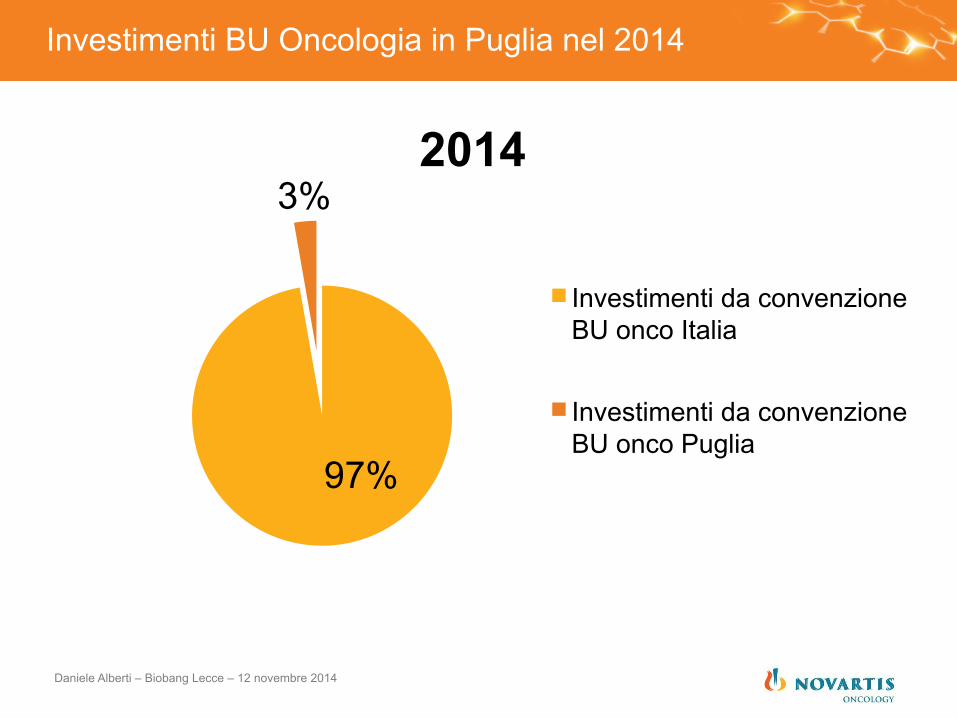
Investimenti BU Oncologia in Puglia nel 2014
97%
3% 2014
Investimenti da convenzione BU onco Italia
Investimenti da convenzione BU onco Puglia
Daniele Alberti – Biobang Lecce – 12 novembre 2014
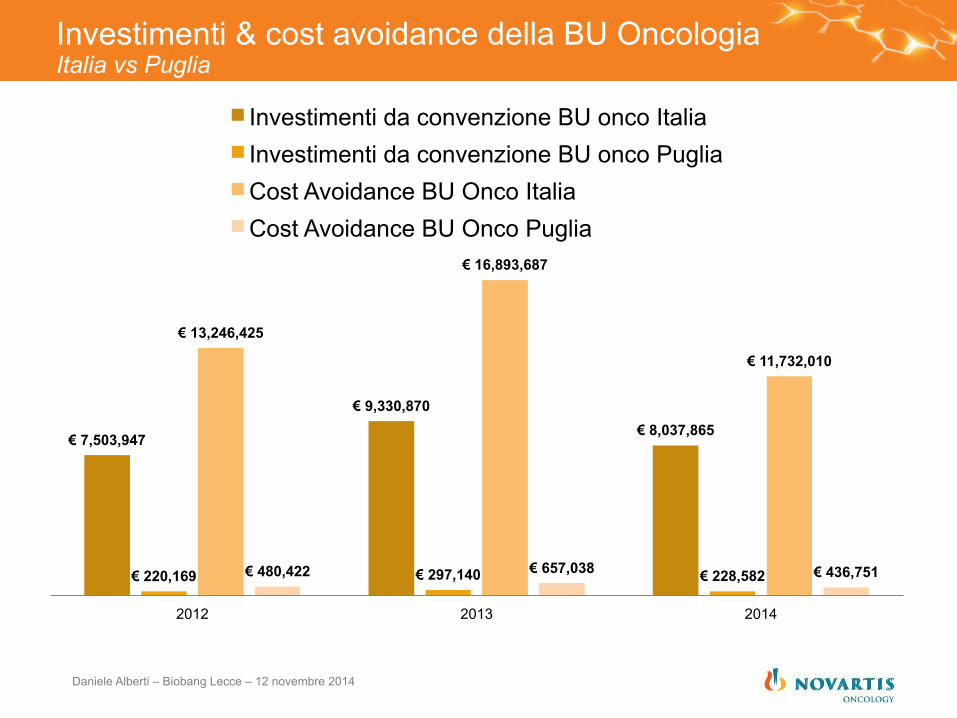
Investimenti & cost avoidance della BU Oncologia Italia vs Puglia
€ 7,503,947
€ 9,330,870 € 8,037,865
€ 220,169 € 297,140 € 228,582
€ 13,246,425
€ 16,893,687
€ 11,732,010
€ 480,422 € 657,038 € 436,751
2012 2013 2014
Investimenti da convenzione BU onco Italia Investimenti da convenzione BU onco Puglia Cost Avoidance BU Onco Italia Cost Avoidance BU Onco Puglia
Daniele Alberti – Biobang Lecce – 12 novembre 2014
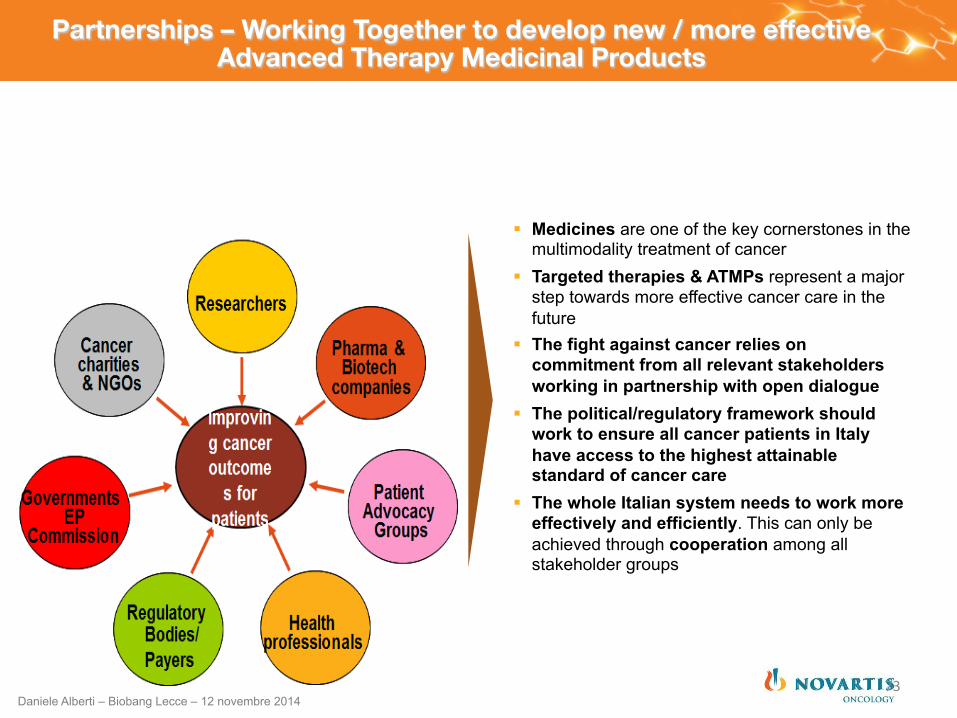
Partnerships – Working Together to develop new / more effective Advanced Therapy Medicinal Products
§ Medicines are one of the key cornerstones in the multimodality treatment of cancer
§ Targeted therapies & ATMPs represent a major step towards more effective cancer care in the future
§ The fight against cancer relies on commitment from all relevant stakeholders working in partnership with open dialogue
§ The political/regulatory framework should work to ensure all cancer patients in Italy have access to the highest attainable standard of cancer care
§ The whole Italian system needs to work more effectively and efficiently. This can only be achieved through cooperation among all stakeholder groups
73 Daniele Alberti – Biobang Lecce – 12 novembre 2014
Q&As
Grazie per l’attenzione
Daniele Alberti – Biobang Lecce – 12 novembre 2014
Agenda
14.00 – 14.10 Introduzione e agenda
14.10 – 14.50 Strategia di sviluppo nuovi prodotti in indicazioni onco- ematologiche
14.50 - 15.10 Opportunità di rilancio: Clinical Trial Center (CTC), Reti Oncologiche ed Ematologiche e laboratori regionali
15.10 - 15.30 Discussione / Presentazione Lavori di gruppo
15.30 – 16.30 Lavori di gruppo
16.30 – 17.00 Feedback in plenaria dai Gruppi di lavoro
17.00 – 17.15 Conclusioni
Daniele Alberti – Biobang Lecce – 12 novembre 2014
Agenda
14.00 – 14.10 Introduzione e agenda
14.10 – 14.50 Strategia di sviluppo nuovi prodotti in indicazioni onco- ematologiche
14.50 - 15.10 Opportunità di rilancio: Clinical Trial Center (CTC), Reti Oncologiche ed Ematologiche e laboratori regionali
15.10 - 15.30 Discussione / Presentazione Lavori di gruppo
15.30 – 16.30 Lavori di gruppo
16.30 – 17.00 Feedback in plenaria dai Gruppi di lavoro
17.00 – 17.15 Conclusioni
Daniele Alberti – Biobang Lecce – 12 novembre 2014
Lavori di Gruppo
q 3-4 Gruppi q Argomenti proposti q Fattibilità Clinical Trial Center in Puglia q Proposte di Formazione finalizzate a impiego permanente in CTC q Bandi / Application con Partnership Pubblico-Privato q Venture Capital da Big Pharma
q Materiale q 1 slide riassuntiva progetto q 1 slide SWOT analysis
q Tempo 1 h: discussione, decisioni, proposte
q 3’ per condivisione in plenaria
Daniele Alberti – Biobang Lecce – 12 novembre 2014
Proposte Progetto
q Scopo
q Razionale
q Metodi
q Risultati Attesi
q Tempi di conduzione
q Stima Risorse Umane e Budget richiesti dal Progetto
q Break-even point: tempo necessario per il ritorno degli investimenti richiesti dalprogetto
Daniele Alberti – Biobang Lecce – 12 novembre 2014
SWOT ANALYSIS
STRENGHTS WEAKNESSES
Descrivere brevemente (max 4 punti) i punti di forza del progetto
INDICARE IN QUESTA SEDE SE NON SONO STATE PREIDENTIFICATE OBIEZIONI ISTITUZIONI
Descrivere brevemente (max 4 punti) le problematiche del progetto o che potrebbero impattare sull a sua approvazione / implementazione
OPPORTUNITY THREATS
Descrivere brevemente (max 4 punti) le opportunità che il progetto potrebbe fornire chi lo propone, Regione, Università, Istituzioni, Pazienti
Descrivere brevemente (max 4 punti) i rischi che il protogretto potrebbe arrecare chi lo propone, Regione, Università, Istituzioni, Pazienti
Team 1 - proposte
Daniele Alberti – Biobang Lecce – 12 novembre 2014
Agenda
14.00 – 14.10 Introduzione e agenda
14.10 – 14.50 Strategia di sviluppo nuovi prodotti in indicazioni onco- ematologiche
14.50 - 15.10 Opportunità di rilancio: Clinical Trial Center (CTC), Reti Oncologiche ed Ematologiche e laboratori regionali
15.10 - 15.30 Discussione / Presentazione Lavori di gruppo
15.30 – 16.30 Lavori di gruppo
16.30 – 17.00 Feedback in plenaria dai Gruppi di lavoro
17.00 – 17.15 Conclusioni
Daniele Alberti – Biobang Lecce – 12 novembre 2014
Agenda
14.00 – 14.10 Introduzione e agenda
14.10 – 14.50 Strategia di sviluppo nuovi prodotti in indicazioni onco- ematologiche
14.50 - 15.10 Opportunità di rilancio: Clinical Trial Center (CTC), Reti Oncologiche ed Ematologiche e laboratori regionali
15.10 - 15.30 Discussione / Presentazione Lavori di gruppo
15.30 – 16.30 Lavori di gruppo
16.30 – 17.00 Feedback in plenaria dai Gruppi di lavoro
17.00 – 17.15 Conclusioni
Daniele Alberti – Biobang Lecce – 12 novembre 2014





























