Embed Size (px)
Citation preview

Getting Started with In-Vitro Blood Vessel Research
Getting Started with In-Vitro Blood Vessel Research
1. History of the Pressurized Arteriograph (Gerry Herrera)
2. Anatomy of an Arteriograph System (Gerry Herrera)
3. Introduction to Research Applications and Methodology (Scott Earley)
4. Getting Started: (Scott Earley)
• KCl and PE induced constriction • ACh-induced dilation • Myogenic constriction
5. Tips & Troubleshooting (Scott Earley)
6. Q&A Session (Scott Earley & Gerry Herrera)

InsideScientific is an online educational environment designed for life science researchers. Our goal is to aid in
the sharing and distribution of scientific information regarding innovative technologies, protocols, research
tools and laboratory services.
Getting Started with In-Vitro Blood Vessel Research
Gerry Herrera, PhD
President,
Catamount Research & Development Inc.,
Living Systems Instrumentation
Copyright 2015 InsideScientific & Living Systems Instrumentation. All Rights Reserved.

The Halpern/Mulvany Wire Myograph
Pioneering The Way…
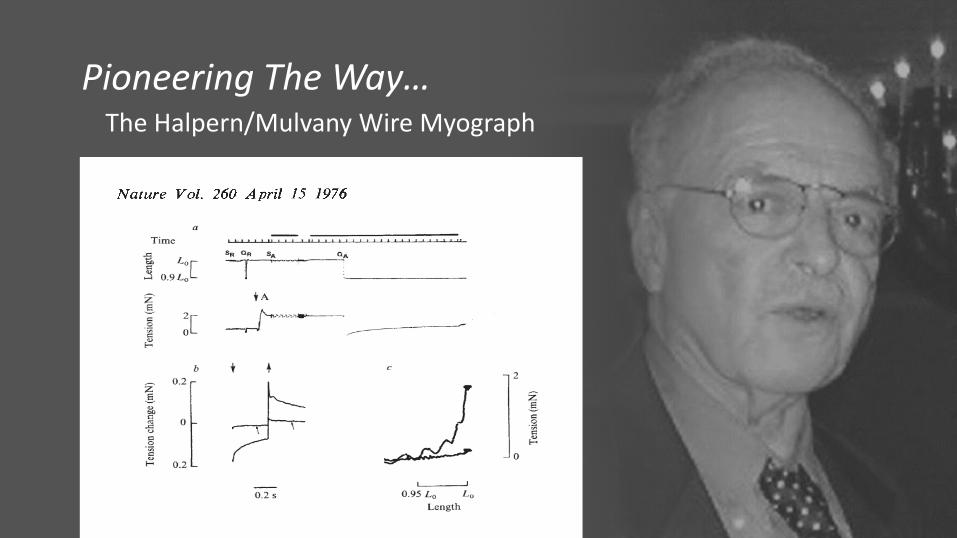
The Halpern/Mulvany Wire Myograph
Pioneering The Way…
The Halpern/Mulvany Wire Myograph
Pioneering The Way…
The First Arteriograph for In Vitro Vessel Research
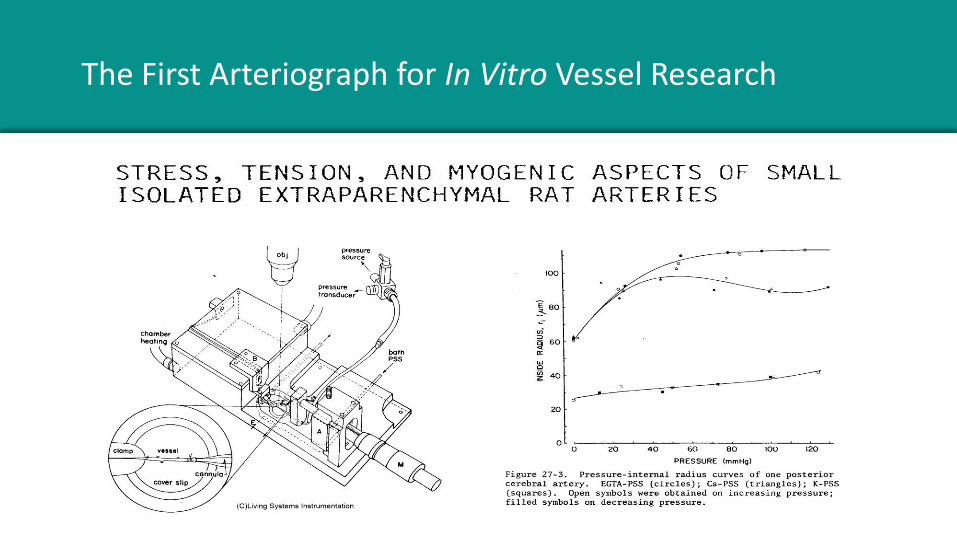
The First Arteriograph for In Vitro Vessel Research
Automating Data Collection: Edge Detection
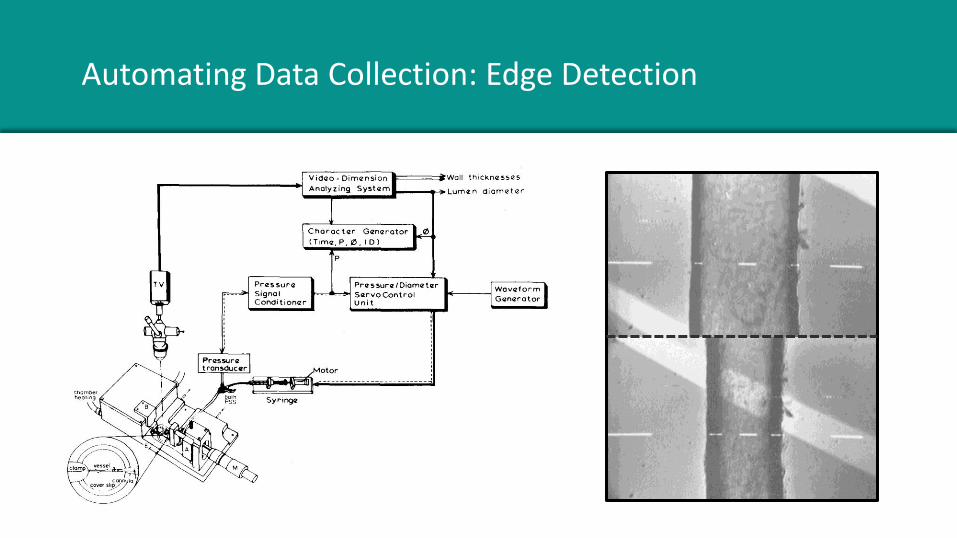
Automating Data Collection: Edge Detection
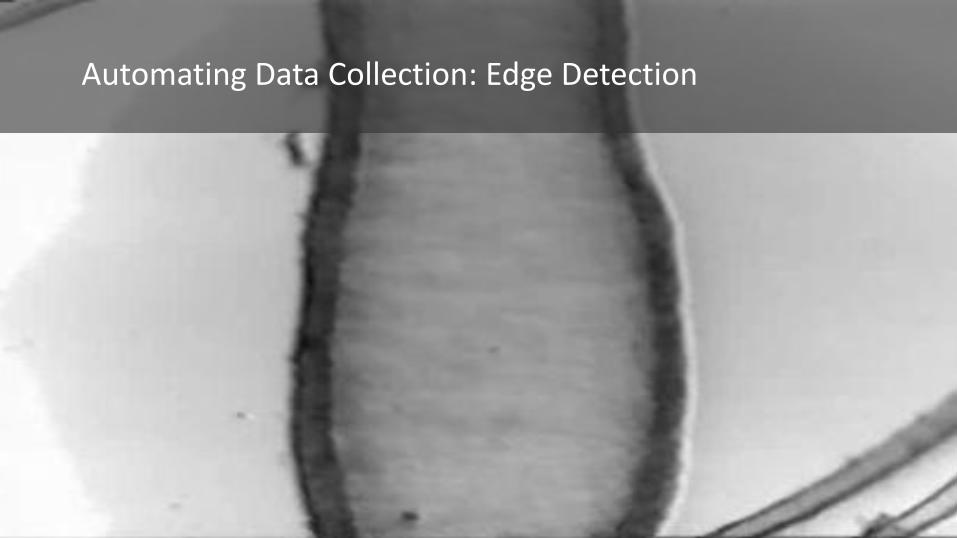
Automating Data Collection: Edge Detection
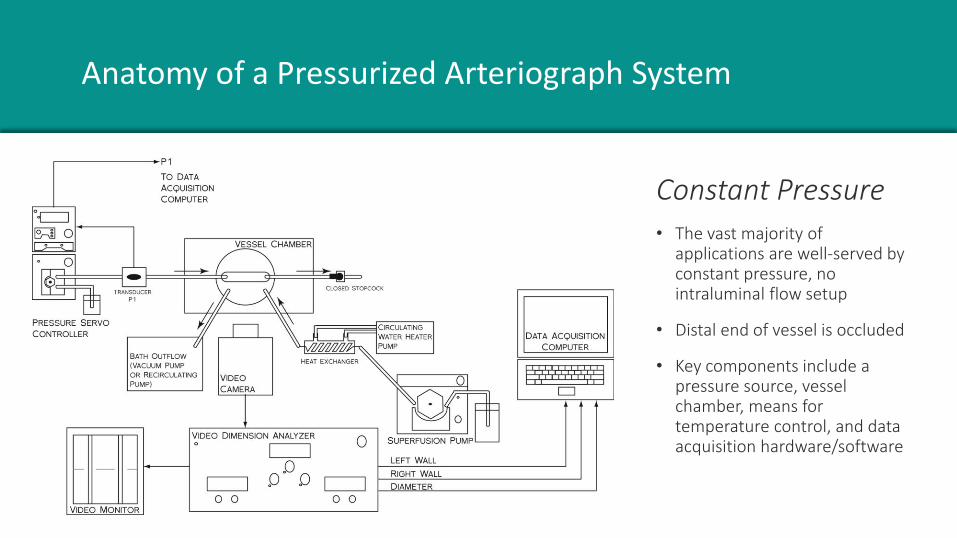
Anatomy of a Pressurized Arteriograph System
To be modified…
Constant Pressure • The vast majority of
applications are well-served by constant pressure, no intraluminal flow setup
• Distal end of vessel is occluded
• Key components include a pressure source, vessel chamber, means for temperature control, and data acquisition hardware/software

Perfused Resistance Vessels
Advanced Application: • It is also possible to measure vascular
responses at either constant or variable intraluminal flow rate
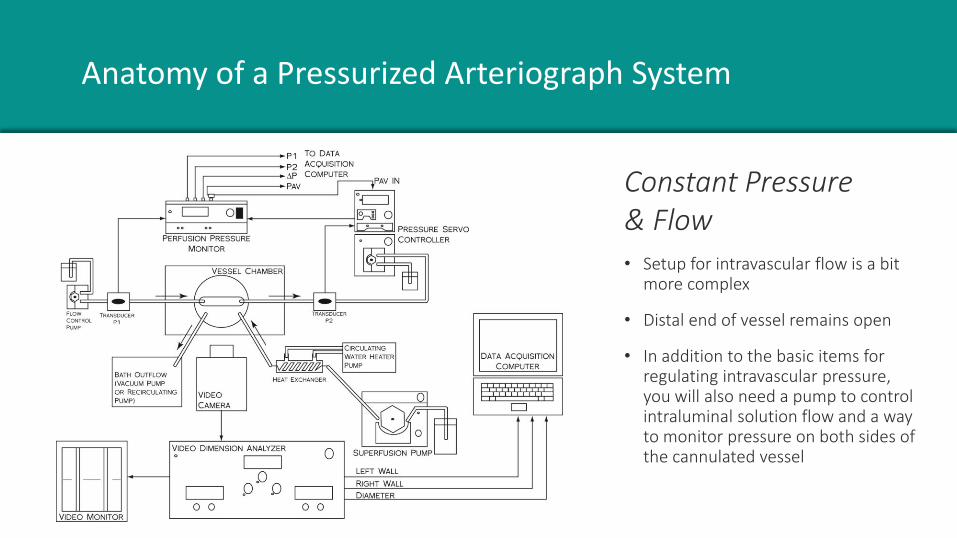
Anatomy of a Pressurized Arteriograph System
To be modified…
Constant Pressure & Flow • Setup for intravascular flow is a bit
more complex
• Distal end of vessel remains open
• In addition to the basic items for regulating intravascular pressure, you will also need a pump to control intraluminal solution flow and a way to monitor pressure on both sides of the cannulated vessel

Shown with optional thermistor (THRS)
• Vessel is mounted between the cannulae and tied in place with nylon thread (provided with the chamber)
• Blood is flushed out of the vessel
• Superfusion of desired buffer into chamber and into vessel
Parts of a Pressure Arteriograph
Click Here for Chamber Information
Additional Information on Equipment Required for Setting up a Pressurized Arteriograph System
• Vessel Chambers
• Specialty Chambers
• Myographs
• Pressure Control
• Flow Control
• Video Analyzers
• Temperature Control
• Aeration & Oxygenation
• pH Measurements
• Dissection Tools
• Microscopes
• Data Acquisition
Getting Started with In-Vitro Blood Vessel Research
Scott Earley, PhD
Associate Professor of Pharmacology,
University of Nevada School of Medicine
Copyright 2015 InsideScientific & Scott Earley. All Rights Reserved.
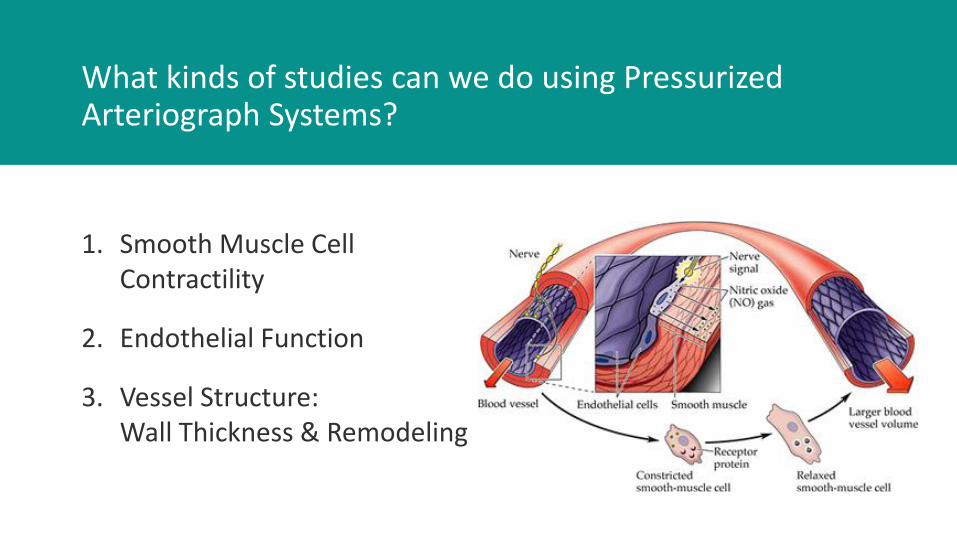
What kinds of studies can we do using Pressurized Arteriograph Systems?
1. Smooth Muscle Cell Contractility
2. Endothelial Function
3. Vessel Structure: Wall Thickness & Remodeling
1. Basic Equipment and Procedures
2. Example Experiments:
• KCl- and PE-induced constriction of mouse mesenteric arteries
• ACh-induced dilation of mouse mesenteric arteries
• Myogenic constriction - mouse cerebral parenchymal arterioles
3. Tips and Troubleshooting
What are we going to cover today?

How To Get Started
• MOPS buffered Saline
• Physiological Saline Solution (PSS)
• High K+ PSS
• Ca2+-free PSS
• Prepare all solutions the day of the experiment
Prepare the Solutions
Physiological Solutions
Recipes for solutions that Dr. Earley uses can be found in his publications. Here, we provide a few saline formulations that can be useful specifically for cases in which you cannot bubble your saline solution – for example, when you need to keep the bath solution stagnant without superfusion to minimize amounts of expensive drugs being added. In most other cases, you should use a bicarbonate buffered saline in which you bubble the saline with at CO2 mixture to get pH control. There are
many recipes for bicarbonate buffered saline in the literature.
Physiological Solutions
The following saline formulations are buffered by HEPES, including the HEPES-bicarbonate recipe. These solutions do not require bubbling.
• HEPES-PSS Solution: This is a general purpose saline.
• High K+ (40 mM) HEPES: This is a saline in which K+ concentration has been increased to ~40 mM by equimolar substitution with Na+. Use this for eliciting K+-induced vasoconstrictions. Some labs increase K+ to 60 mM. If you do this, make sure to use equimolar substitution of K+ and Na+ to avoid osmolalility problems.
• 0 Ca2+ HEPES: This is a saline used to monitor the passive responses of the vessel. Ca2+ has been removed and a Ca2+ chelator (EGTA) has been added.
• HEPES-Bicarbonate Solution: This is a general purpose saline. Many labs prefer to have bicarbonate present in the saline to maintain cellular bicarbonate transporter function. If you use this solution as a standard solution, you can also prepare High K+ and 0 Ca2+ versions.

HEPES-PSS Solution
Compound M.W. mM g/L
NaCl 58.44 141.9 8.29
KCl 74.55 4.7 0.35
MgSO4 (7H2O) 246.28 1.7 0.42
EDTA 292.25 0.5 0.15
CaCl2 (2H2O) 147.02 2.8 0.41
HEPES 238.30 10.0 2.38
KH2PO4 136.09 1.2 0.16
Glucose 180.16 5.0 0.90
Titrate to pH 7.4 with 10 N NaOH. Prepare fresh daily.
(This buffer does not require bubbling)

High K+ (40 mM) HEPES
Compound M.W. mM g/L
NaCl 58.44 95.8 5.60
KCl 74.55 38.0 2.84
MgSO4 (7H2O) 246.28 1.7 0.42
EDTA 292.25 0.5 0.15
CaCl2 (2H2O) 147.02 2.8 0.41
HEPES 238.30 10.0 2.38
KH2PO4 136.09 1.2 0.16
Glucose 180.16 5.0 0.90
Use this equimolar substitution of KCl and NaCl. All other reagent amounts stay the same. Titrate to pH 7.4 with 10 N NaOH . Prepare fresh daily.
(This buffer does not require bubbling)
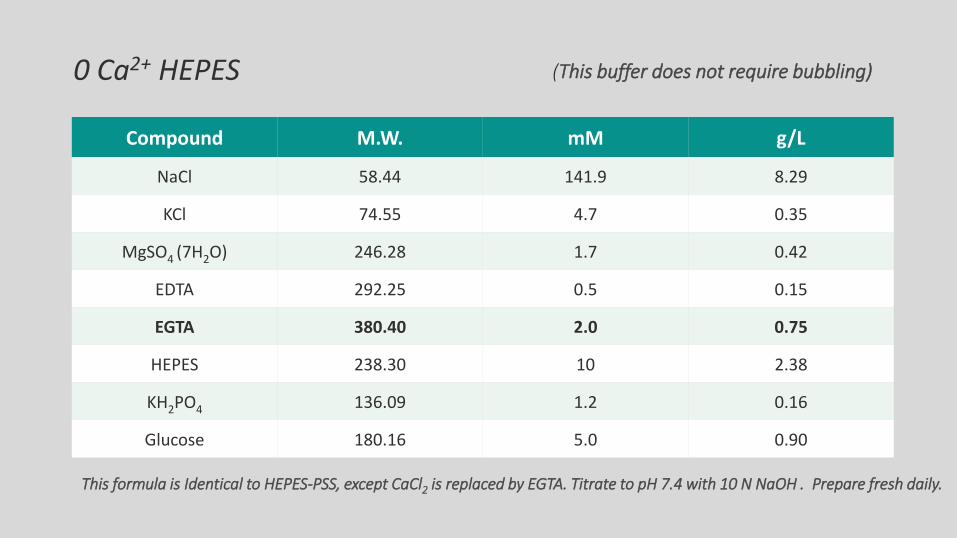
0 Ca2+ HEPES
Compound M.W. mM g/L
NaCl 58.44 141.9 8.29
KCl 74.55 4.7 0.35
MgSO4 (7H2O) 246.28 1.7 0.42
EDTA 292.25 0.5 0.15
EGTA 380.40 2.0 0.75
HEPES 238.30 10 2.38
KH2PO4 136.09 1.2 0.16
Glucose 180.16 5.0 0.90
This formula is Identical to HEPES-PSS, except CaCl2 is replaced by EGTA. Titrate to pH 7.4 with 10 N NaOH . Prepare fresh daily.
(This buffer does not require bubbling)
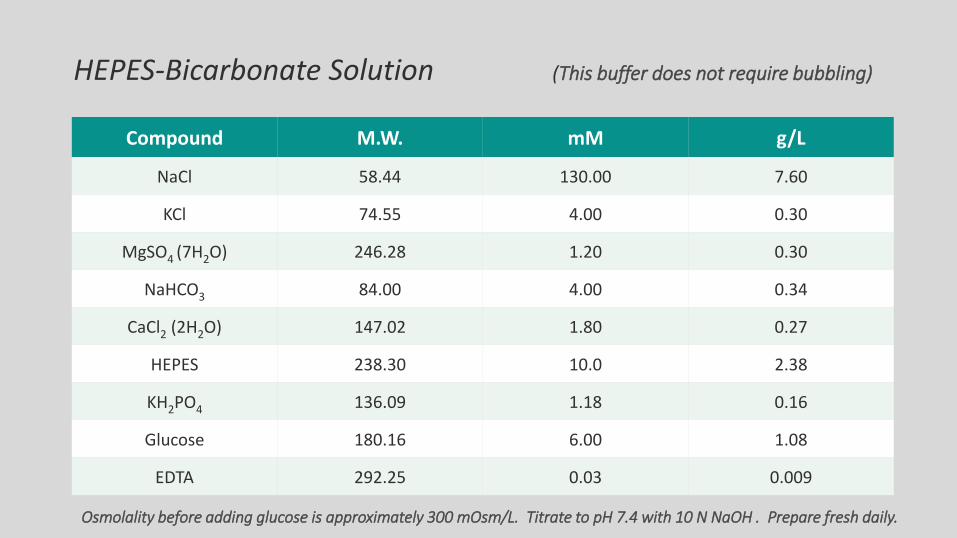
HEPES-Bicarbonate Solution (This buffer does not require bubbling)
Compound M.W. mM g/L
NaCl 58.44 130.00 7.60
KCl 74.55 4.00 0.30
MgSO4 (7H2O) 246.28 1.20 0.30
NaHCO3 84.00 4.00 0.34
CaCl2 (2H2O) 147.02 1.80 0.27
HEPES 238.30 10.0 2.38
KH2PO4 136.09 1.18 0.16
Glucose 180.16 6.00 1.08
EDTA 292.25 0.03 0.009
Osmolality before adding glucose is approximately 300 mOsm/L. Titrate to pH 7.4 with 10 N NaOH . Prepare fresh daily.
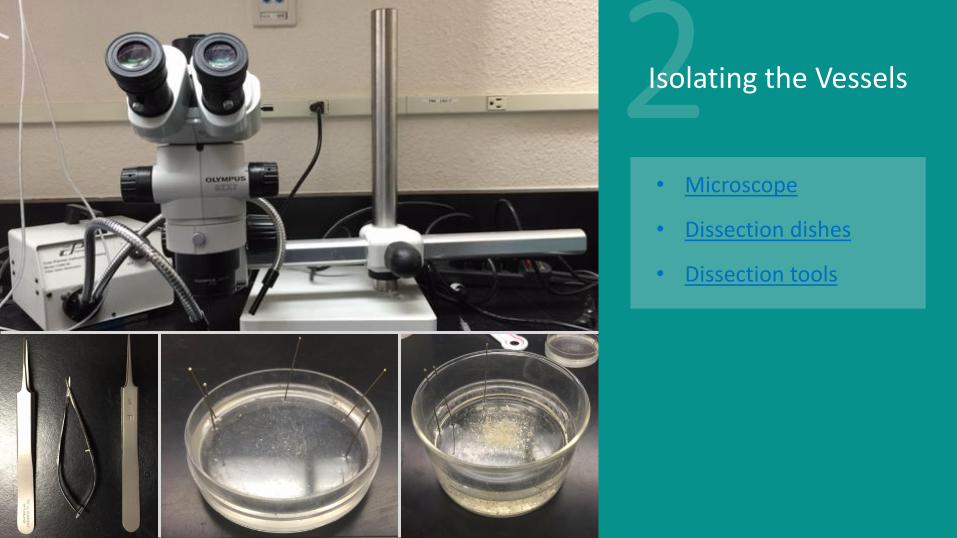
Isolating the Vessels
• Microscope
• Dissection dishes
• Dissection tools

Mesentery Brain
Isolating the Vessels
• Mesentery pinned out and fat removed
• Veins and Arteries
Isolating the Vessels
• We weren’t able to come up with any images for this – Gerry, do you have anything?
• ….
• ….
• ….
Making Vessel Ties
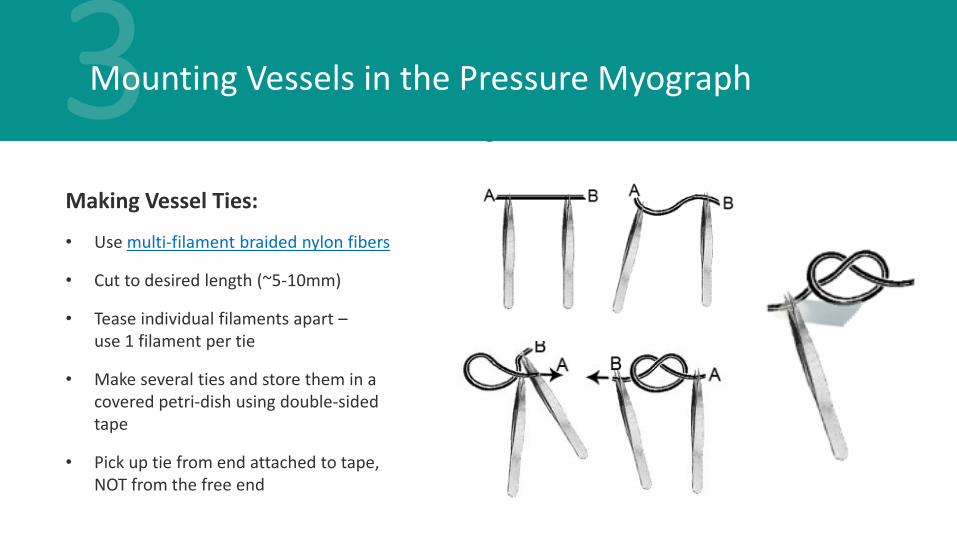
Mounting Vessels in the Pressure Myograph
Making Vessel Ties:
• Use multi-filament braided nylon fibers
• Cut to desired length (~5-10mm)
• Tease individual filaments apart – use 1 filament per tie
• Make several ties and store them in a covered petri-dish using double-sided tape
• Pick up tie from end attached to tape, NOT from the free end

• We weren’t able to come up with any images for this – Gerry, do you have anything?
• ….
• ….
• ….
Attach proximal end & flush out blood…
Attach distal end.
Mounting Vessels in the Pressure Myograph

Transfer Chamber to Recording System
• Place chamber on the microscope stage
• Connect inlet and outlet superfusion
• Connect pressure control system

Keeping the Vessels Alive and Happy
Intraluminal Pressure
Temperature Flow Rate pH
Follow links for additional information on suggested equipment

Collecting Data
• Edge Detection
• Data Acquisition System

The Complete System
Example Experiments

Example 1: KCl-Induced Constriction
• Expose the vessel to elevated extracellular KCl (60 mM) – High K+ PSS.
• Collapses the K+ gradient, resulting in depolarization of the smooth muscle cell plasma membrane.
• Ca2+ influx through L-type Ca2+
channels causes vascular smooth muscle contraction and vasoconstriction.
K+
K+ K+
K+ K+ K+ Ca2+
SMC
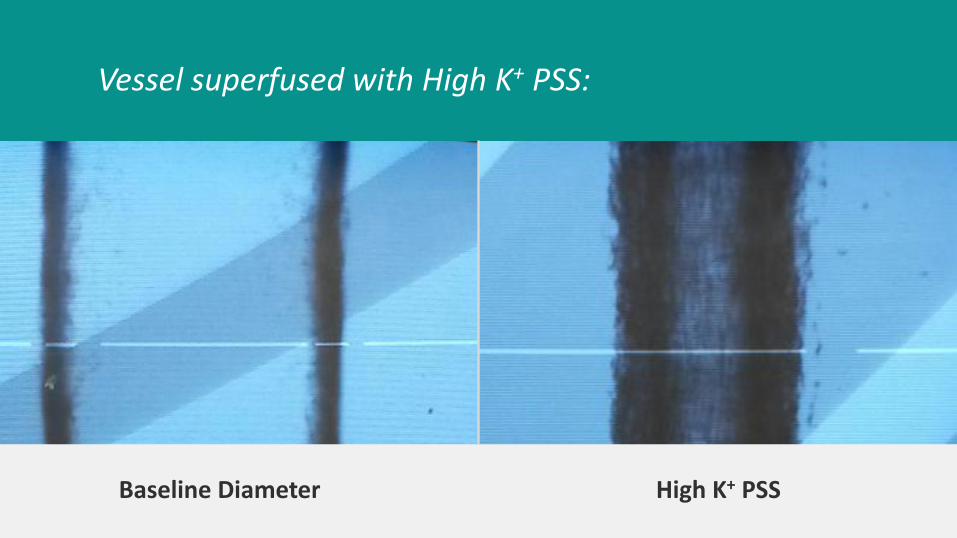
Vessel superfused with High K+ PSS:
Baseline Diameter High K+ PSS
Example 2: PE-Concentration Response Curve
• Phenylephrine (PE) binds to the type-1 adrenergic receptor (α1 receptor) on the smooth muscle cell plasma membrane.
• This causes an increase in intracellular Ca2+, resulting in smooth muscle cell contraction and vasoconstriction.
PE
Ca2+ SMC

10-9 M PE 10-8 M PE 10-7 M PE 10-6 M PE 10--5 M PE
Vessel superfused with increasing concentrations of PE:
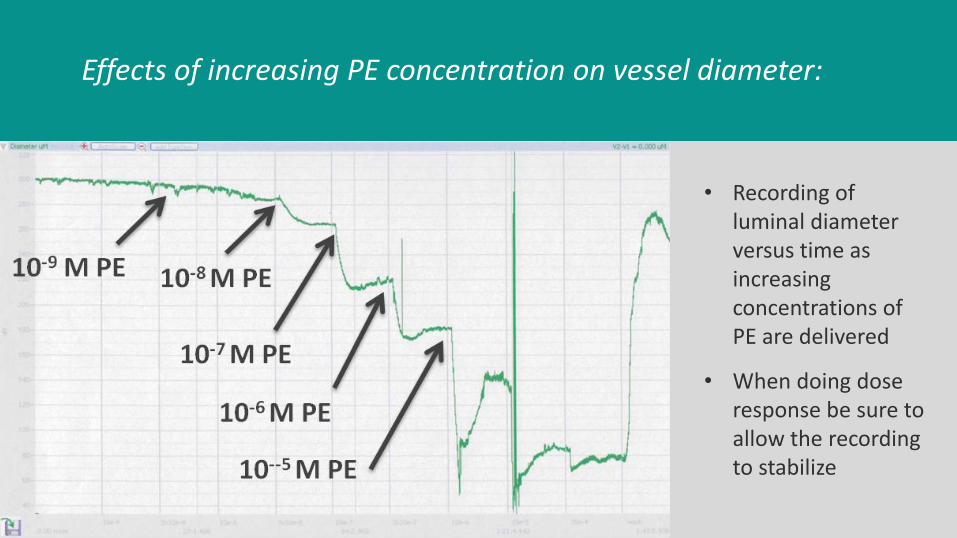
Effects of increasing PE concentration on vessel diameter:
• Recording of luminal diameter versus time as increasing concentrations of PE are delivered
• When doing dose response be sure to allow the recording to stabilize
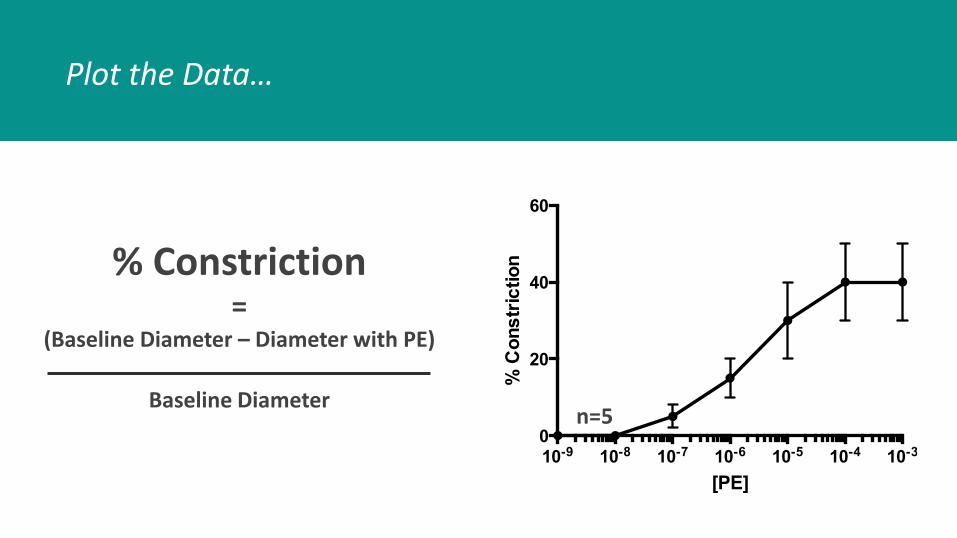
Plot the Data…
10-9 10-8 10-7 10-6 10-5 10-4 10-30
20
40
60
[PE]
% C
on
str
ictio
n
n=5
% Constriction =
(Baseline Diameter – Diameter with PE)
Baseline Diameter
Example 3: ACh-Induced Relaxation (Endothelium Viability)
• Acetylcholine (ACh) binds to muscarinic type-2 (M2) receptors on the endothelial cell plasma membrane.
• This causes the release of NO and EDHF.
• These factors diffuse to the underlying vascular smooth muscle cells to decrease intracellular Ca2+ and cause dilation.
• Gold standard for intact endothelial function.
Endothelial cell
SMC
ACh
Ca2+
NO EDHF
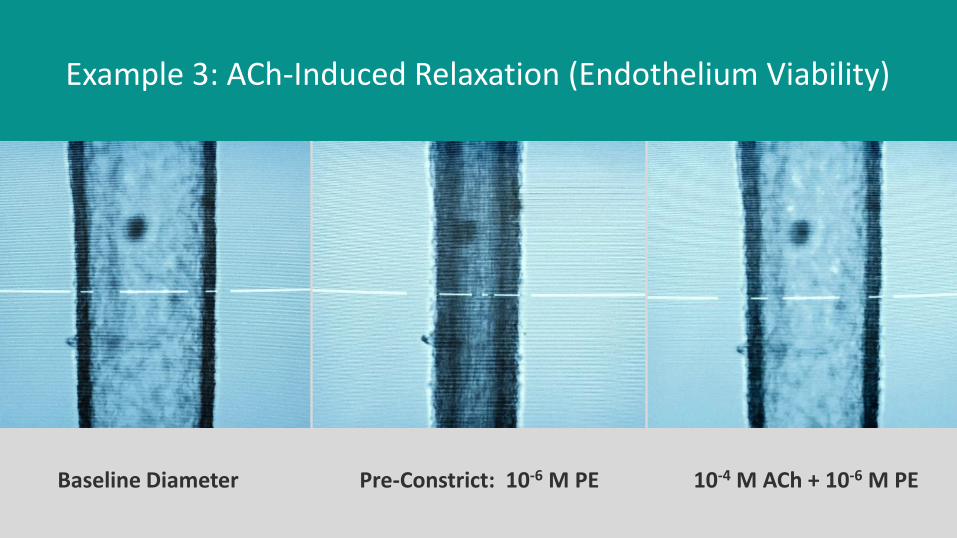
Baseline Diameter Pre-Constrict: 10-6 M PE 10-4 M ACh + 10-6 M PE
Example 3: ACh-Induced Relaxation (Endothelium Viability)

ACh
Example 3: ACh-Induced Relaxation (Endothelium Viability)
• Vessel was pre-constricted with PE
• ACh was applied at the peak of the steady-state PE-constriction
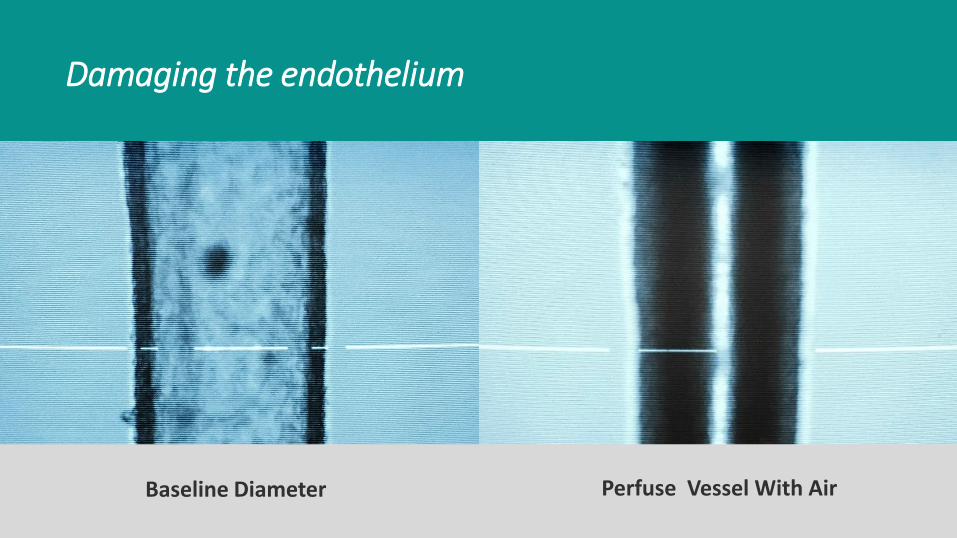
Damaging the endothelium
Perfuse Vessel With Air Baseline Diameter
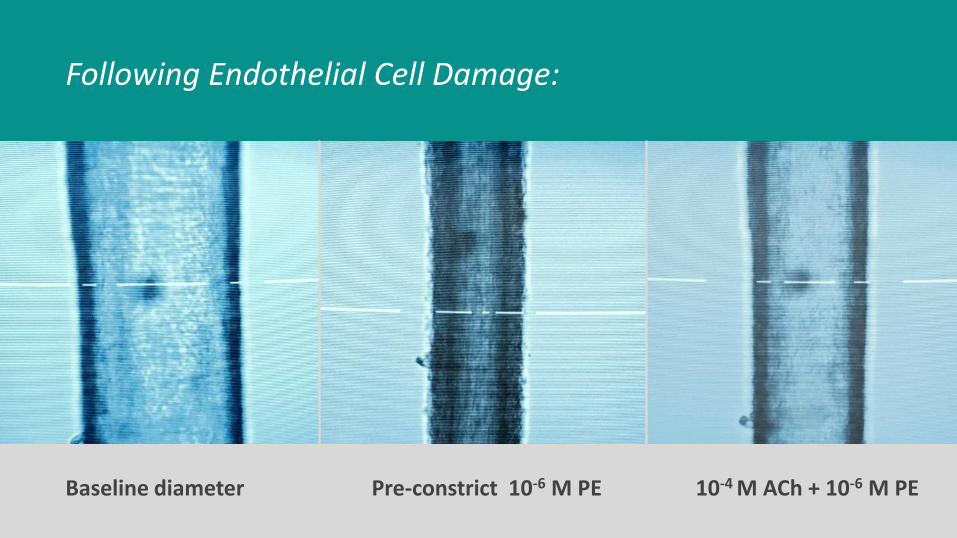
Following Endothelial Cell Damage:
Baseline diameter Pre-constrict 10-6 M PE 10-4 M ACh + 10-6 M PE
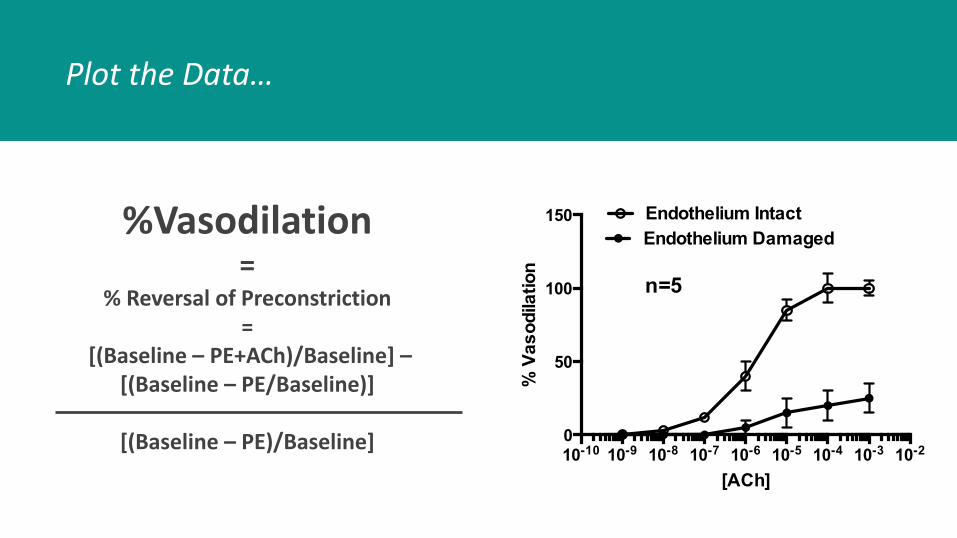
Plot the Data…
10-10 10-9 10-8 10-7 10-6 10-5 10-4 10-3 10-20
50
100
150
[ACh]
% V
as
od
ila
tio
n
Endothelium Intact
Endothelium Damaged
n=5
%Vasodilation =
% Reversal of Preconstriction =
[(Baseline – PE+ACh)/Baseline] – [(Baseline – PE/Baseline)]
[(Baseline – PE)/Baseline]
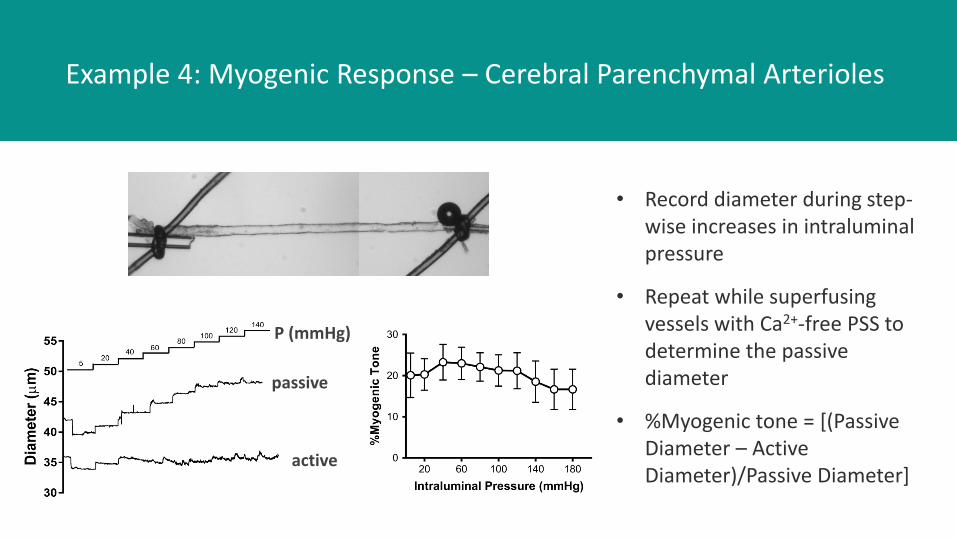
Example 4: Myogenic Response – Cerebral Parenchymal Arterioles
• Record diameter during step-wise increases in intraluminal pressure
• Repeat while superfusing vessels with Ca2+-free PSS to determine the passive diameter
• %Myogenic tone = [(Passive Diameter – Active Diameter)/Passive Diameter]
P (mmHg)
passive
active
• The learning curve – do the procedure in examples 1-3 (KCl-induced constriction, PE-concentration response curve, ACh-induced dilation) using second order mesenteric arteries until you get reproducible results.
• Work fast- remove organs and isolate vessels as quickly as possible
• Make solutions fresh each day.
• Stretching the vessel in the initial prep
• pH/O2/temperature
Tips & Pointers
Thank You! For additional information on Pressure Arteriograph Systems, Wire Myographs, and solutions for studying vessel function in-vitro visit:
http://www.livingsys.com/index.html