Embed Size (px)
Citation preview
Individual and Socio-familial Risk and Protective Factors in Two Generations of the
Mauritius Joint Child Health Project
S. E. Luczak, C. Dalais, A. Raine,
P. H. Venables, F. Schulsinger, & S. A. Mednick
Funded by WHO, Danish State Department, DANIDA, Medical Research
Council (UK), Leverhulme Trust, Wellcome Trust, Ford Foundation, Scottish
Rite, US National Institutes of Health (K02MH01114, K08AA14265,
R01AA10206,, R01AA18179, R01HD42259, R01RR13642) & Mauritian
Ministries of Health and Education
Overview
Mauritius background
Joint Child Health Project
– Childhood precursors (birth records, ages 3, 8, 11, 17 y/o)
– Adult outcomes (intervention, aggression/criminality, schizotypy, substance use)
– Multigenerational transmission (current study)
– Future directions (additional outcomes, co-morbidity)

Mauritius
Mauritius
Mauritius
Mauritius
Mauritius
Human Development Index
Language
Economy
Government
Medical
Education
Disease
Joint Child Health Project
Birth cohort (100%) from two towns
N = 1,795
Followed since 1972 when 3 years of age
Religioethnic diversity matches population
– 52% Hindu
– 26% Creole
– 19% Muslim
– 4% Chinese, French, other
Joint Child Health Project: Age 3 Years
Assessment (N = 1,795)
– Psychophysiology, cognitive ability, temperament/behavior
– Parent-child interaction, home visit
– Medical evaluation, pregnancy & birth records
Intervention (n = 200)
– Preschool as usual vs. enriched (nutrition, stimulation)
– Selected by psychophysiological reactivity (hyper-, hypo-respond)
– Followed at ages 4, 5, 6, and 8 years (behavior, psychophysiology)
Joint Child Health Project: Childhood Phases Age 8 (n = 1,173)
– Teacher behavior ratings
– School medical evaluation
Age 11 (n = 1,264)
– Psychophysiology, cognitive ability, behavior problems
– Home visit for family environment, medical
Age 17 (n = 615)
– Behavior problems (e.g., schizotypy, hyperactivity)
– Neuropsychology
Joint Child Health Project: Adult Phases
Ages 23-30 (n = 1,023-1,795)
– Crime (self-report and official records)
– Mental health diagnoses (depression, schizotypy, alcohol)
Age 35-40 (n = 932-1,208)
– Alcohol, smoking, gambling
– Depression, anxiety, deviance
– Parenting, family environment
– Positive outcomes (satisfaction, happiness)
JCHP Findings: Intervention Effects Intervention was associated with:
conduct disorder, hyperactivity, schizotypal behavior at 17
criminal behavior (self-report & official) by 23
Better effects in malnourished children
JCHP Findings: Childhood Outcomes
Aggression:
– Age 3 low heart rate, fearlessness, stimulation-seeking predict age 11 aggression
– Birth complications & age 3 malnutrition predict externalizing at age 11 (and 17)
Cognition:
– Age 3 low stimulation seeking (after psychosocial adversity) predict lower age 11 IQ
– Age 11 low verbal IQ and executive functioning predict lifetime alcohol problems
JCHP Findings: Schizotypal Behavior
Schizotypy:
– Prenatal influenza exposure associated with age 17 schizotypy
– Age 3 adversity predicts age 23 schizotypy, which is partially mediated by performance IQ
– Impaired habituation to aversive stimuli at ages 3 & 11 predict schizotypal behavior at age 23, particularly cognitive-perceptual features
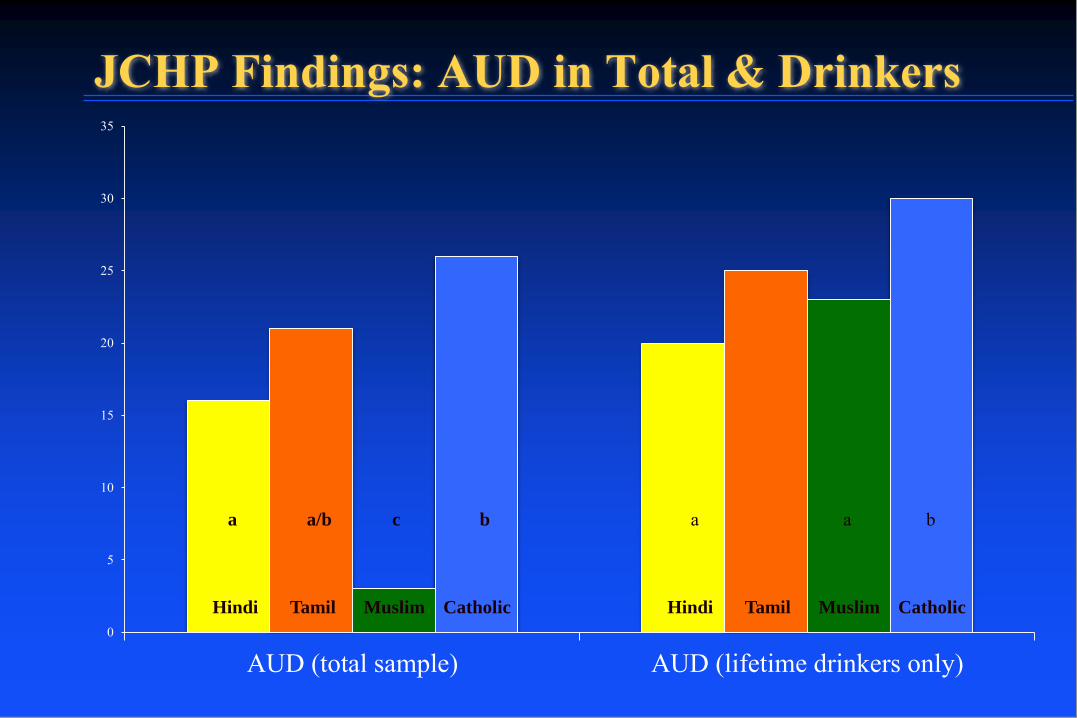
JCHP Findings: AUD in Total & Drinkers
0
5
10
15
20
25
30
35
AUD (total sample) AUD (lifetime drinkers only)
a a/b c b a a b
Hindi Tamil Muslim Catholic Hindi Tamil Muslim Catholic
JCHP Findings: Alcohol Problems 4 latent classes
Non-problematic (66%)
Hazardous (11%)
Moderate (16%)
Severe (6%)
Severe
Externalizing
Academic achievement
Psychosocial adversity
Hazardous
IQ total score
Psychosocial adversity
JCHP Offspring
Prior testing on offspring 3-5 y/o and 8-13 y/o
- Psychophysiology
- Cognitive ability
- Temperament/behavior
- Parent-child interaction
- Home/family environment
Intervention: Omega-3
200 children (10-13 y/o)
SmartFish juice with omega-3 for 6 months
Assessment (psychophysiology, cognitive, behavioral)
Current Phase: Intergenerational Transmission
Substance use & misuse (alcohol, smoking, illicit)
Behavior problems (internalizing, externalizing)
Medical history (conditions, hospitalizations, head injury)
Health (nutrition, activities, medications)
Genes (5-HTTLPR, DRD2, GABRA2, ALDH & ADH)
Personality (5 Factor)
Family/peers (bonding/monitoring, support, conflict tactics)
Ethnicity/religion/culture (behavior, individual/collectivistic)
JCHP Future Directions
Drinking & smoking
Onset & progression
Differences across cohorts, gender, religion
Diabetes
Childhood (pregnancy, malnutrition)
Adult (obesity, nutrition, activity)
Cognitive abilities
Developmental pattern
Verbal abilities
US Acknowledgements
Jo Ann Farver, John Horn, Jack McArdle, Carol Prescott (co-Is, mentors)
Sandy Brown, Marc Schuckit, Ken Sher, Bob Zucker (Consultants)
Howard Edenberg, Tiebing Liang (Collaborators)
Elizabeth Chernei, Rubin Khoddam, Marsha Sargeant, Jackie Tilley, Lisa Yarnell; Omar Arid, Kelsey Bradshaw, Nicole Chow, Anna Schwartz (Research lab)
Mauritius Acknowledgements
Ministry of Health
JCHP participants
JCHP staff (Tashneem Mahoomed, Shameem Oomur)

Joint Child Health Project Staff (K08)

Joint Child Health Project Staff (R01)





























