Embed Size (px)
Citation preview
Defence Sciencc Journal, Vol 44, No 4, October 1994, pp 331-340@ 1994, DESIDOC
-Mechanism of Cyanide Toxicity and Efficacy of its Antidotes
S.K. Raza * and D.K. Jaiswal
Defence Re.~eurch & Deve[opment E!;'lub[ishment, Gwa[ior-474002
ABSTRACT
This paper attempts to review the various antidotes available for countering cyanide threat inthe light of the toxicity associatcd with it. It also critically evaluates the drawbacks and advantagesof these antidotes for their thcrapcutic and/or prophylactic utility. The physico-chemical propertiesof hydrogen cyanide which make it a chemical warfare agent have also been highlighted. In an attempt
to make the complex chemical and biological processes understandable, the chemical structures ofthe antidotes have been included ~nd simple mechanistic pathways have been used to show the role
of antidotes in activating the inhibited enzymes.
.INTRODUCTION
Hydrogen cyanide, discovered by a Swedish chemist
C.W. Scheele in 1782, has been recognised as one of
the most rapid poisons. Cyanide toxicity has long been
a problem in livestock grazing range containingcyanogenic plantsl. The toxicity of these plants is
associated with specific glycosides which contain a
cyanide moiety. The worldwide industrial development
has become a major threat so far as cyanide is
concerned. Cyanogenic materials are produced in
electroplating, steel, aluminium, paints and
petrochemical industries2. The major problem,however, comes from the intentional ingestion of
cyanide for suicidal and homicidal purposes. The high
toxicity associated with hydrogen cyanide (HCN) has
made it a useful chemical warfare (CW) a~ent. The
French were the first to use it in 'the Battle of Somme
in July 1916 and since then it has been used as a CW
agent. A very recent example of its use is by Iraq in
her cQnflict with Iran.
coloured HCN is considered to be less dangerous
because it is in the process of alteration. In the gaseous
state it is colourless with a vapour density lower than
air. Some of the salient physico-chemical properties of
HCN have been listed in Table I.
Because of its high vapour pressure' and low density
it is difficult to maintain a high concentration of HCN
in an open place. To make it more persistent, numerous
Table I. Physico-chemical properties of hydrogen cyanide
Molecularwpioht
Boiling point
Freezing point
Vapourdensity
Specific gravity
27
26.5°C
-13.4°C
0.948
0.7058 (7 OC)
0.6969 ( 18 OC)
138.5 C
53.5atm
210.7 caVg
873,{XX) mg/mJ
Critical temperature
Critical pressure
Heat of vaporisation
Volatility at 20 oC
Solubility at 20°C
(a) Organic solvents2. PHYSICO-CHEMICAL PROPERTIES
The physico-chemical properties of HCN make it a
useful CW agent. Pure anhydrous HCN is a colourless
liquid with a peculiar odour of bitter almond. The
Alcohol, ether, glycerol,chlorofonn, benzene.
Dissolves to give acidic solution.(b) Water
--~Received II February 1993, revised 12 August 1993.Present address : Professorial Unit, Institute of Dermatology, St. Thomas Hospital, London SE1 7EH.
331
brought to you by COREView metadata, citation and similar papers at core.ac.uk
provided by Defence Science Journal
DEF SCI I, VOL 44, NO 4, ocrOBER 1994
artifices have been used during the war. HCN is miscible
in all proportions with alcohol, ether, glycerol,
chloroform, benzene, etc. It dissolves in water to fonD
a weak acidic solution. Even in the anhydrous
conditions, HCN cannot be kept for long as it gradually
decomposes, occasionally with explosive force. The
decomposition may be prevented or retarded by the
addition of small amounts of mineral acids.
A
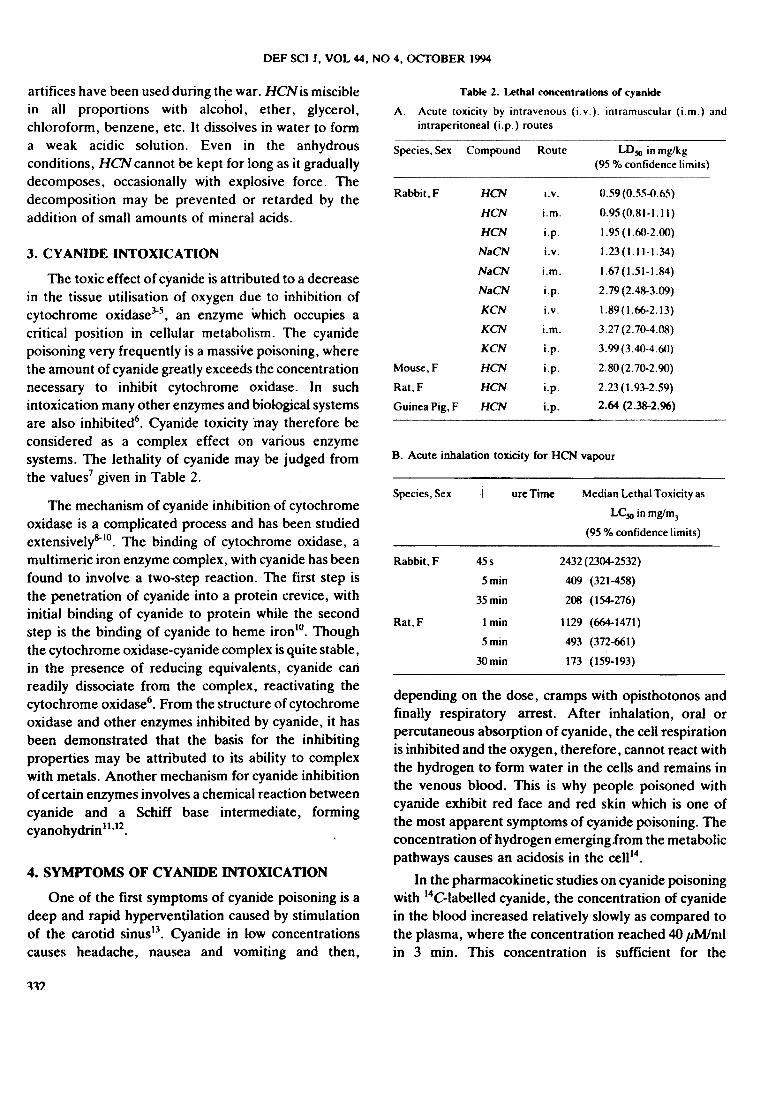
Table 2. Lethal concentrations or cyanide
Acute toxicity by intravenous (iv.). intramuscular (i.m.) and
intraperitoneal (i.p.) routes
Species. Sex Compound Route LD~ in mg/kg(95% confidence limits)
HCN
HCN
HCN
NaCN
NaCN
NaCN
KCN
KCN
KCN
HCN
HCN
HCN
0.59 (0.55-0.65)
0.95(0.81-1.11)
1.95 (1.~>-2.(X)
1.23(1.11-1.34)
1.67(1.51-1.84)
2.79(2.48-3.09)
1.89(1.66-2.13)
3.27 (2.70-4.08)
3.99(3.40-4.60)
2.80(2.70-2.90)
2.23(1.93-2.59)
2.64 (2.38-2.96)
Rabbit, F I. v.
i.m.
i.p.
i.v.
i.m.
i.p.
i.v.
I.m.
i.p.
i.p.
i.p.
i.p.
Mouse,F
Rat,F
Guinea Pig, F
B. Acute inhalation toxicity for HCN vapour
Exposure TimeSpecies, Sex
3. cy ANIDE INTOXICA nON
The toxic effect of cyanide is attributed to a decreasein the tissue utilisation of oxygen due to inhibition ofcytochrome oxidase3-5, an enzyme which occupies acritical position in cellular metabolism. The cyanidepoisoning very frequently is a massive poisoning, wherethe amount of cyanide greatly exceeds the concentrationnecessary to inhibit cytochrome oxidase. In suchintoxication many other enzymes and biological systemsare also inhibited6. Cyanide toxicity "may therefore beconsidered as a complex effect on various enzymesystems. The lethality of cyanide may be judged fromthe values7 given in Table 2.
The mechanism of cyanide inhibition of cytochromeoxidase is a complicated process and has been studiedextensively8-IO. The binding of cytochrome oxidase, amultimeric iron enzyme complex, with cyanide has beenfound to involve a two-step reaction. The first step isthe penetration of cyanide into a protein crevice, withinitial binding of cyanide to protein while the secondstep is the binding of cyanide to heme iron 10. Thoughthe cytochrome oxidase-cyanide complex is quite stable,in the presence of reducing equivalents, cyanide calireadily dissociate from the complex, reactivating thecytochrome oxidase6. From the structure of cytochromeoxidase and other enzymes inhibited by cyanide, it hasbeen demonstrated that the basis for the inhibitingproperties may be attributed to its ability to complexwith metals. Another mechanism for cyanide inhibitionof certain enzymes involves a chemical reaction betweencyanide and a Schiff base intermediate, formingcyanohydrin! !.!2.
Median Lethal Toxicity as
LC.10 in mg/m]
(95% confidence limits)---
Rabbit, F 2432(2304-2532)
409 (321-458)
208 (154-276)
1129 (664-1471)
493 (372-661)
173 (159-193)
Rat.F
depending on the dose, cramps with opisthotonos andfinally respiratory arrest. After inhalation, oral orpercutaneous absorption of cyanide, the cell respirationis inhibited and the oxygen, therefore, cannot react withthe hydrogen to form water in the cells and remains inthe venous blood. This is why people poisoned withcyanide exhibit red face and red skin which is one ofthe most apparent symptoms of cyanide poisoning. Theconcentration of hydrogen emerging from the metabolicpathways causes an acidosis in the celll4.
In the pharmacokinetic studies on cyanide poisoningwith 14C-Iabelled cyanide, the concentration of cyanidein the blood increased relatively slowly as compared tothe plasma, where the concentration reached 40 JlM/mlin 3 min. This concentration is sufficient for the
4. SYMPTOMS OF CY ANIDE INTOXICATION
One of the first symptoms of cyanide poisoning is adeep and rapid hyperventilation caused by stimulationof the carotid sinus13. Cyanide in low concentrationscauses headache, nausea and vomiting and then,
n1
45s
5min
35min
1 min
5min
3Omin
RAZA & JAISW AL: MECHANISM OF CY ANIDE TOXICITY AND EFFICACY
respiratory arrest. If, however, the concentration of
cyanide in plasma falls below this level, respiration
occurs spontaneously without any artificial respiration.
On the other hand, if the concentration of cyanide in
plasma reached 70p. M/ml, the heart beat ceases about
5 min after the respiratory arrestl5.
s. ESSENTIALS OF DIAGNOSIS
Cyanide poisoning is notoriously difficult todiagnose without a history of exposure 16-11. Thepresence of an odour of oil 'of bitter almond inrespiration and the appearance of red face and skin arethe most apparent diagnostic symptoms. The finaldiagnosis for the oral consumption of cyanide comes byperforming the Lee Jones test in gastric aspirate, thegreen-blue colouration of ferricyanide confirms thepresence of cyanidel8.
ACTION MECHANISMS OF TREA TMENTAPPROACHES
6.
Once diagnosed, a variety of approaches have beenproposed for the treatment of cyanide poisoning. Theseapproaches may be classified under three main headsdepending upon their mechanisms of action.
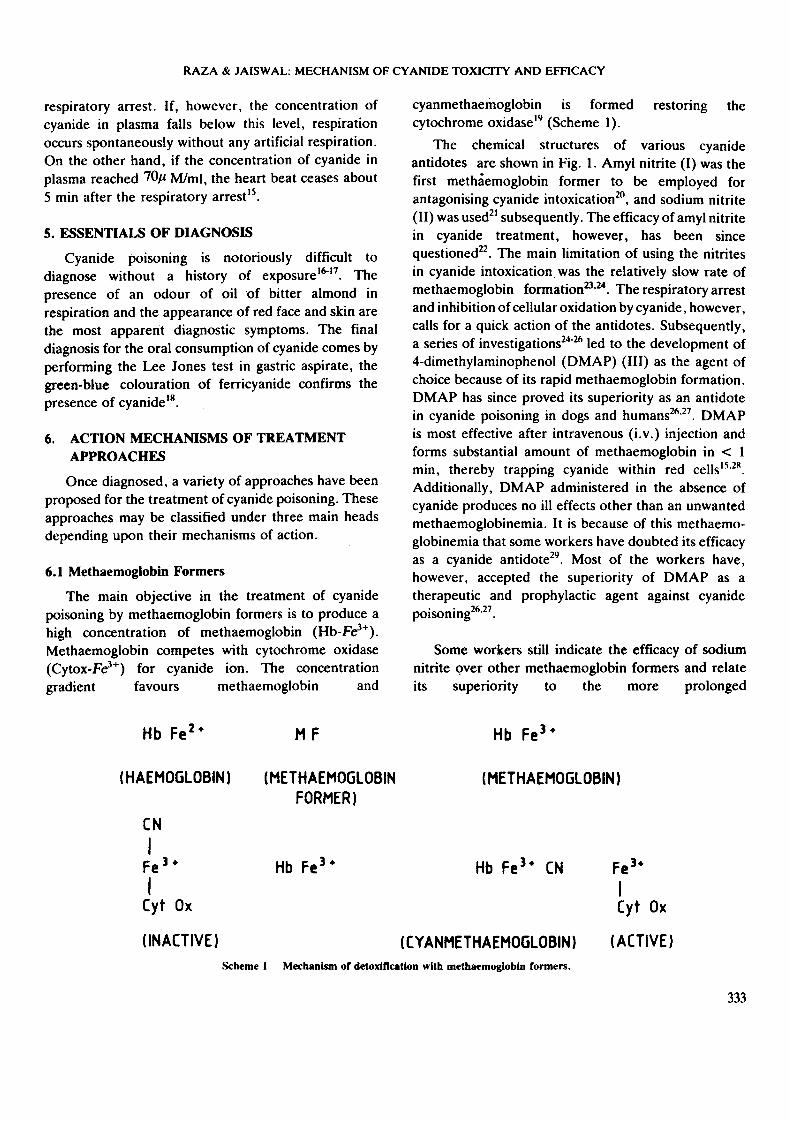
cyanmethaemoglobin is formed restoring the
cytochrome oxidasel9 (Scheme I).
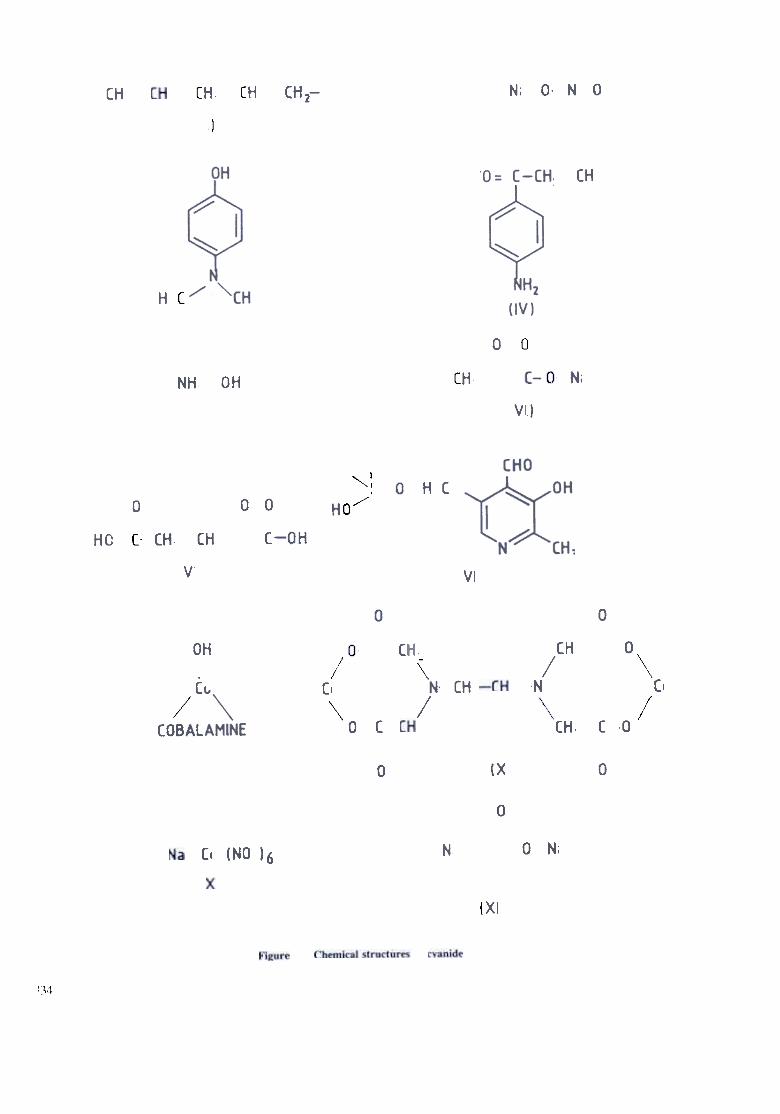
The chemical structures of various cyanide
antidotes are shown in Fig. I. Amyl nitrite (I) was the
first methaemoglobin former to be employed for
antagonising cyanide intoxication2o, and sodium nitrite
(11) was used21 subsequently. The efficacy of amyl nitrite
in cyanide treatment, however, has been since
questioned22. The main limitation of using the nitrites
in cyanide intoxication. was the relatively slow rate of
methaemoglobin formation23.24. The respiratory arrest
and inhibition of cellular oxidation by cyanide, however ,
calls for a quick action of the antidotes. Subsequently,
a series of investigations24-26 led to the development of
4-dimethylaminophenol (DMAP) (111) as the agent of
choice because of its rapid methaemoglobin formation.
DMAP has since proved its superiority as an antidote
in cyanide poisoning in dogs and humans26.27. DMAP
is most effective after intravenous (i. v. ) injection and
forms substantial amount of methaemoglobin in < I
min, thereby trapping cyanide within red cellsI5.2R.
Additionally, DMAP administered in the absence of
cyanide produces no ill effects other than an unwanted
methaemoglobinemia. It is because of this methaemo-
globinemia that some workers have doubted its efficacy
as a cyanide antidote29. Most of the workers have,
however, accepted the superiority of DMAP as a
therapeutic and prophylactic agent against cyanide
poisoning26.27.
6.1 Methaemoglobin Formers
The main objective in the treatment of cyanidepoisoning by methaemoglobin formers is to produce ahigh concentration of methaemoglobin (Hb-Fe3+).Methaemoglobin competes with cytochrome oxidase(Cytox-Fe3+) for cyanide ion. The concentrationgradient favours methaemoglobin and
Some workers still indicate the efficacy of sodiumnitrite Qver other methaemoglobin fonners and relateits superiority to the more prolonged
Hb Fe2+ Hb Fe3+MF
( HAEMOGLOBIN ) ( METHAEMOGlOBIN
FORMER)
( METHAEMOGLOBIN )
Hb Fe.3+ Hb Fe3+ CN Fe3.
I
Cyt Ox
CN
I
Fe3.
I
Cyt Ox
( INACTIVE ) (ACTIVE)( cy ANMETHAEMOGLOBIN )
MechanIsm of detoxification with methaemoglobln formers.Scheme I
333
RAZA & J AISW AL: MECHANISM OF CYANIDE TOXICITY AND EFFICACY
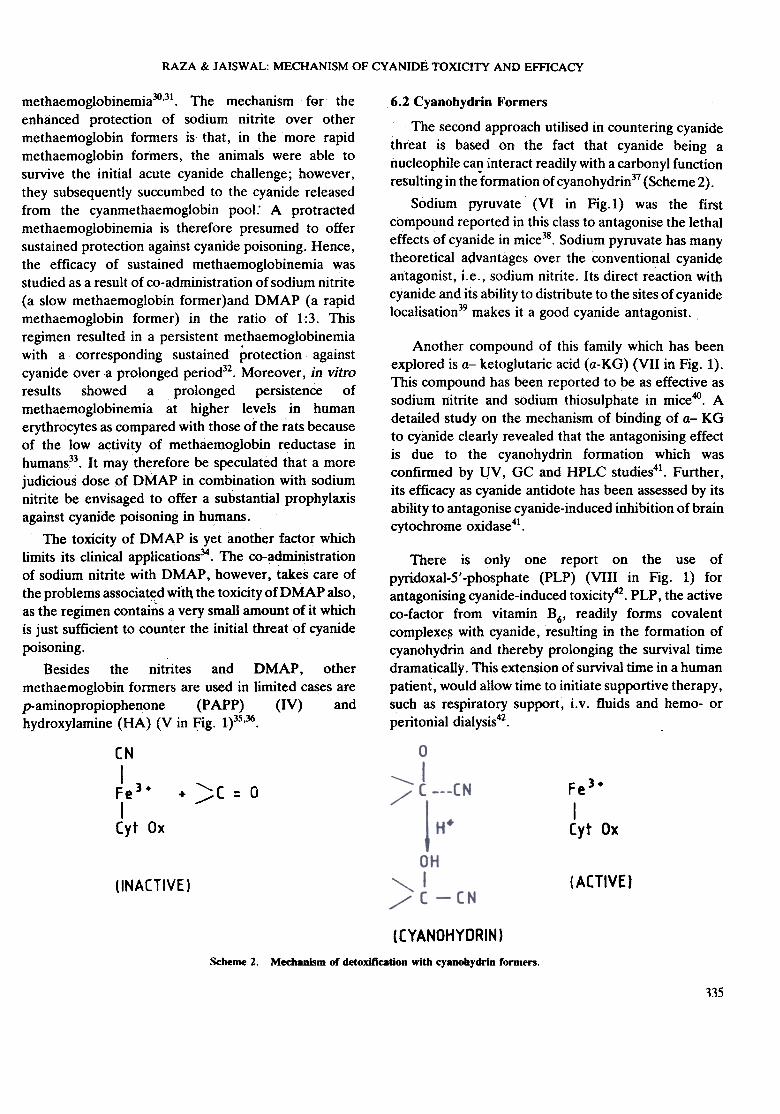
6.2 Cyanohydrin Formers
The second approach utilised in countering cyanidethreat is based on the fact that cyanide being anucleophile can interact readily with a carbonyl functionresulting in the-formationof cyanohydrin37 (Scheme 2).
Sodium pyruvate (VI in Fig.l) was the firstcompound reported in this class to antagonise the lethaleffects of cyanide in mice38. Sodium pyruvate has manytheoretical advantages over the conventional cyanideantagonist, i.e. , sodium nitrite. Its direct reaction withcyanide and its ability to distribute to the sites of cyanidelocalisation39 makes it a good cyanide antagonist.
Another compound of this family which has beenexplored is a- ketoglutaric acid (a-KG) (VII in Fig. I).This compound has been reported to be as effective assodium nitrite and sodium thiosulphate in mice40. Adetailed study on the mechanism of binding of a- KGto cyanide clearly revealed that the antagonising effectis due to the cyanohydrin formation which wasconfirmed by l!V, GC and HPLC studies41. Further,its efficacy as cyanide antidote has been assessed by itsability to antagonise cyanide-induced inhibition of braincytochrome oxidase41.
There is only one report on the use ofpyridoxal-5'-phosphate (PLP) (VIII in Fig. 1) forantagonising cyanide-induced toxicity42. PLP, the activeco-factor from vitamin B6, readily forms covalentcomplexe~ with cyanide, resulting in the formation ofcyanohydrin and thereby prolonging the survival timedramaticaUy. This extension of survival time in a humanpatient, would allow time to initiate supportive therapy,such as respiratory support~ i. v. fluids and hemo- or
peritonial dialysis42.
methaemoglobinemia30.31. The mechanism fer theenhanced protection of sodium nitrite over othermethaemoglobin formers is that, in the more rapidmethaemoglobin formers, the animals were able tosurvive the initial acute cyanide challenge; however ,they subsequently succumbed to the cyanide releasedfrom the cyanmethaemoglobin pool: A protractedmethaemoglobinemia is therefore presumed to offersustained protection against cyanide poisoning. Hence,the efficacy of sustained methaemoglobinemia wasstudied as a result of co-administration of sodium nitrite(a slow ~ethaemoglobin former)and DMAP (a rapidmethaemoglobin former) in the ratio of 1:3. Thisregimen resulted in a persistent methaemoglobinemiawith a corresponding sustained protection againstcyanide over a prolonged period32. Moreover, in vitroresults showed a prolonged persistence ofmethaemoglobinemia at higher levels in humanerythrocytes as col:npared with those of the fats becauseof the low activity of methae~oglobin reductase inhumans33. It may therefore be speculated that a morejudicious dose of DMAP in combination with sodiumnitrite be envisaged to offer a substantial prophylaxisagainst cyanide poisoning in humans.
The toxicity of DMAP is yet another factor whichlimits its clinical applications34. The co-administrationof sodium nitrite with DMAP, however, takes care ofthe problems associated with the toxicity ofDMAP also,as the regimen contains a very small amount of it whichis just sufficient to counter the initial threat of cyanide
poisoning.Besides the nitrites and DMAP, other
met haemoglobin formers are used in limited cases arep-aminopropiophenone (P APP) (IV) andhydroxylamine (HA) (V in Fig. 1)35.36.
~( = 0+
CN
I
Fe3+
ICyt Ox
Fe3+
ICyt Ox
( ACTIVE )(INACTIVE)
( CY ANOHYDRIN )
Mecbanlsm of detoxification with cyanobydrin rormen.Scheme 2.
115
DEF SCI i, VOL 44, NO 4, OcrOBER 1994
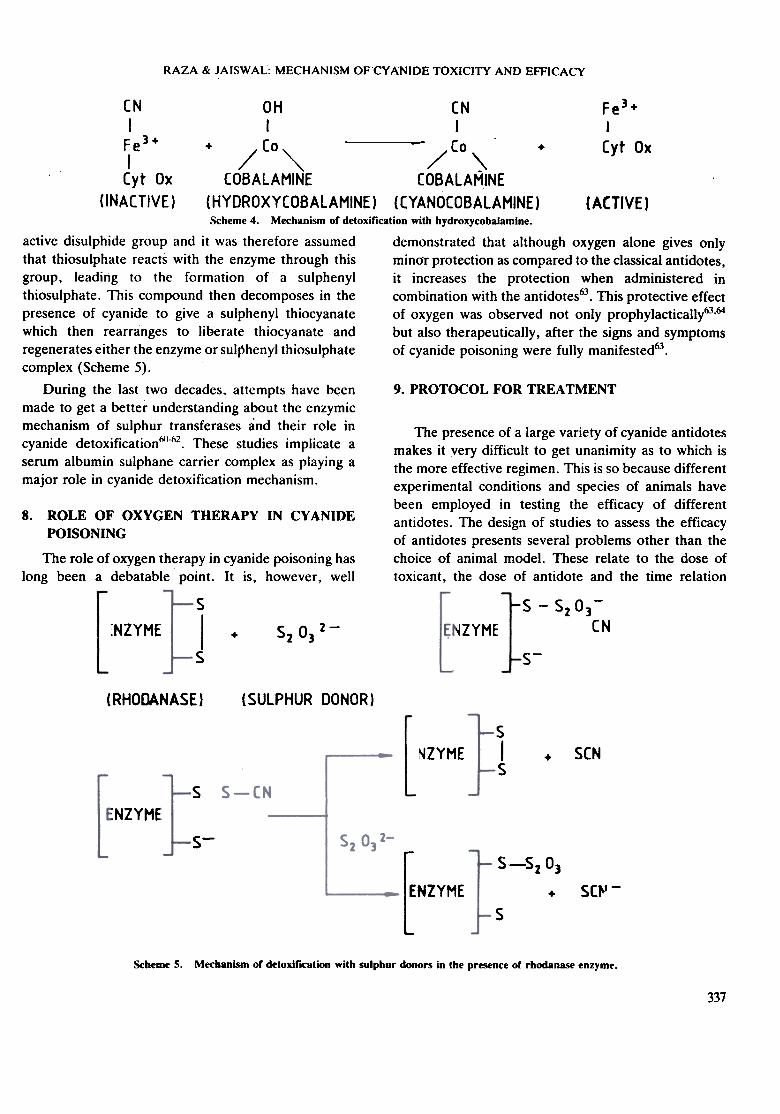
Hydroxycobalamine detoxifies cyanide by giving upits hydroxyl group and binding a cyanyl group, forming
cyanocobalamine (Scheme 4) which is excreted in theurine45. The cobalt compounds have a greater affinity
for cyanide than cytochrome oxidase and thus free the
enzyme to resume its role in cellular resplration54.
Co2EDT A can cause hypertension, cardiac
arrhythmia and 'ardiac insufficiency if administered in
the absence of cyanide poisoning. It is perhaps in this
context that some workers have recommended the use
of Co2EDT A for comatose patients who do not recover
with classical therapy and for patients lapsing into
unconsciousness despite treatment51.
6.3 Cobalt Compounds
Cobalt ion is known to form a stable complex withcyanide and has been used in the treatment of cyanidepoisoning43.44, but its use could not receive generalsupport mainly because of the toxicity of cobalt ions.However, since the discovery of the antidotal effects ofhydroxycobalamine (IX in Fig. i) in experimentalcyanide poisoning45, the interest in such compounds hasbeen revived and has led to the testing of many saltsand chelates of cobalt as antidotes to cyanide46-50. Of
these, dicobaltethylenediaminetetracetic acid(Co2EDTA) (X in Fig. 1) was found to be a moreeffective antidote than sodium nitrite51. This led to theuse of Co2 EDT A as the main compound in antidotaltherapy for cyanide poisoning in many Europeancountries. The selection of Co2EDT A as the preferredcobalt compound is reasonable, since it was hoped thatmany of the toxic effects of cobalt ion would beminimised by administering its compoWlds as chelates.
It is generally assumed that most cobalt compoundsreact directly with free cyanide ion to trap it as a stablewater soluble chelate or as an insoluble precipitate.Some cobalt compounds, however, may have aconcdmitant effect, namely, methaemoglobinformation. Cobaltous chloride, for example, is said ~ogenerate methaemoglobin in human blood by virtue ofits ability to inhibit the methaemoglobin reductase
activity52.Sodium cobaltinitrite (XI in Fig. 1) generates
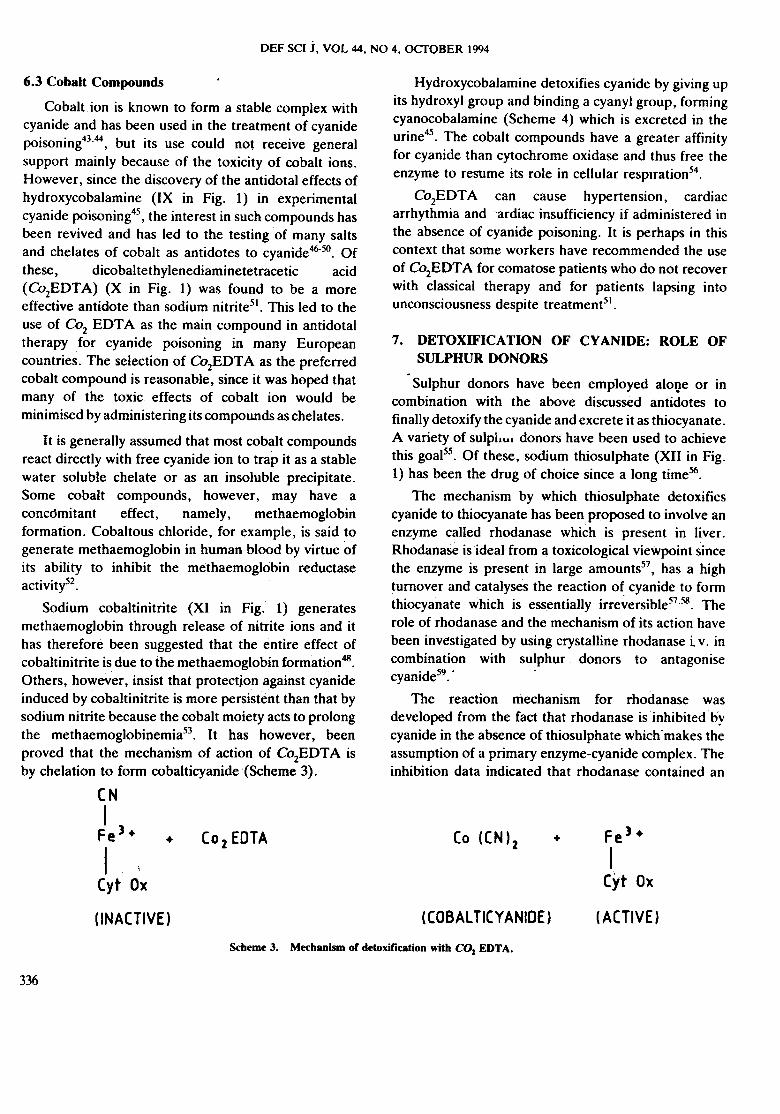
methaemoglobin through release of nitrite ions and ithas therefore been suggested that the entire effect ofcobaltinitrite is due to the methaemoglobin formation48.Others, however, insist that protectjon against cyanideinduced by cobaltinitrite is more persistent than that bysodium nitrite because the cobalt moiety acts to prolongthe methaemoglobinemia53. It has however, beenproved that the mechanism of action of Co2EDTA isby chelation to form cobalticyanide '(Scheme 3).
CN
7. DETOXIFICATION OF CY ANIDE: ROLE OFSULPHUR DONORS
Sulphur donors have been employed alol}e or incombination with the above discussed antidotes tofinally detoxify the cyanide and excrete it as thiocyanate.A variety of sulpllui donors have been used to achievethis goal55. Of these, sodium thiosulphate (XII in Fig.1) has been the drug of choice since a long time56.
The mechanism by which thiosulphate detoxifiescyanide to thiocyanate has been proposed to involve anenzyme called rhodanase which is present in liver .Rhodanase is ideal from a toxicological viewpoint sincethe enzyme is present in large amounts57, has a highturnover and catalyses the reaction of cyanide to formthiocyanate which is essentially irreversible57.58. Therole of rhodanase and the mechanism of its action havebeen inve-stigated by using crystalline rhodanase i v. incombination with sulphur donors to antagonisecyanide59. ..
The reaction mechanism for rhodanase wasdeveloped from the fact that rhodanase is inhibited bycyanide in the absence of thiosulphate which "makes theassumption of a primary enzyme-cyanide complex. Theinhibition data indicated that rhodanase contained an
I
Fe3+
I
Cyt Ox
Fe3+
I,Cyt Ox
(o2EDTA (0 ((N)2 ++
(COBAL TICYANIDE) ( ACTIVE )( INACTIVE )
Scheme 3. MechanIsm or detoxification with CO1 EDT A.
336
RAZA & JAISWAL: MECHANISM OF"CYANIDE TOXICITY AND EFFICACY
CN
I
Fe3+
I
OH
I
tN
I~e3 + + / Co """ / Co \ + Cyt Ox
Cyt Ox COBALAMINE COBALAMINE
(INACTIVE) (HYDROXYCOBALAMINE} (CYANOCOBALAMINE} (ACTIVE}Scheme 4. Mechanism or detoxification with hydroxycobalamine.
active disulphide group and it was therefore assumed demonstrated that although oxygen alone gives only
that thiosulphate reacts with the enzyme through this min(jr protection as compared to the classical antidotes,
group, leading to the formation of a sulphenyl it increases the protection when administered in
thiosulphate. This compound then decomposes in the combination with the antidotes63. This protective effect
presence of cyanide to give a sulphenyl thiocyanate of oxygen was observed not only prophylactically63.64
which then rearranges to liberate thiocyanate and but also therapeutically, after the signs and symptoms
regenerates either the enzyme or sulphenyJ thiosulphate of cyanide poisoning were fully manifested63.
complex (Scheme 5).
During the last two decades, attempts have b~en 9. PROTOCOL FOR TREA TMENT
made to get a better understanding about the enzymic
mechanism of sulphur transferases and their role in
cyanide detoxificationN'-h2. These studies implicate a
serum albumin sulphane carrier complex as playing a
major role in cyanide detoxification mechanism.
The presence of a large variety of cyanide antidotesmakes it very difficult to get unanimity as to which isthe more effective regimen. This is so because differentexperimental conditions and species of animals havebeen employed in testing the efficacy of differentantidotes. The design of studies to assess the efficacyof antidotes presents several problems other than thechoice of animal model. These relate to the dose oftoxicant, the dose of antidote and the time relation
8. ROLE OF OXYGEN THERAPY IN CY ANIDEPOISONING
The role of oxygen therapy in cyanide poisoning has
long been a debatable point. It is, however, well
s
Is
$ -$203-
CNs 0 2-
2 3ENZYME '~NZYME+
s-
(RHODANASE) (SULPHUR DONOR)
sIs
SCNENZYME +
sENZYME
s-
S-S2 03
ENZYMEsc"' -
+
s
Scheme s. Mechanism or detoxification with sulphur donors in the presence or rhodanase enzyme.
337
DEF SCI J, VOL 44, NO 4, OCTOBER 1994
between them. While the United States of Americaremains faithful to the combination of sodium nitriteand sodium thiosulphate (Lilly's Cyanide Antidote Kit)in the treatment of cyanide poisoning, some Europeancountries, such as Germany use DMAP, whereas otherssuch as UK and France favour Co2EDTA.The Lilly'sKit available in the USA is not without inherentlimitations. The toxicity of sodium nitrite and its slowformation of methaemoglobin are the two main factorswhich have always been advocated against this regimen.It should be possible to make a rational choice betweenDMAP and Co2EDTA by comparing their efficaciesagainst experimental poisoning in animals and bycomparing their relative toxicities. In fact, not manysuch comparisons have been carrie.d out. There is onlyone reporf7 which showed better survival with DMAPthan with Co2EDT A. A recent report employing theco-administration of sodium nitrite and DMAP se:emsto be encouraging as it not only redqces the toxicity ofthese chemicals due to reduced dosage but also givessustained protection against cyanide threat which isfurther augmented by sodium thiosulphate32.
7.
8.
9.
10.
12
ACKNOWLEDGEMENTS
The authors thank Dr R V Swamy, Director ,
Defence Research & Development Establishment, for
providing necessary facilities and useful suggestions.
REFERENCES 13
14.2
315
4
16.
5.
17
in perfused rat livers by glucagon and metabolicinhibitor. Biochim. Biophys. Acta, 1974, 362,.469-79.
Ballantyne, B. Toxicology of cyanides. In Clinicaland exRerimental toxicology of cyanides, editedby B. Ballantyne & T.M. Marrs. Wright, Bristol,1987. pp 41-126.
Antonini, E.; Brunori, M.; Greenwood, C.;Malstrom, B.G. & Rotilio, G.C. The interactionof cyanide with cytochrome oxidase. Eur. JBiochem., 1971, 23, 396-400.
Buuren, K.J. Van; Nicholis, P. & Gelder, B.F.Van. Biochemical and biophysical studies oncytochrome aa3. Binding of cyanide to cytochromeaa3. Biochim. Biophys. Acta, 1972,256,243-57.
Buuren, K.J. Van; Nicholis, P & Gelder, B.F.Van. Biochemical and biophysical studies oncytochrome aa3. Reaction of cyanide with oxidizedand reduced enzyme. Biochim. Biophys. Acta,1972,256, 258-76.
Marsho, T. V. & Kung, S.D. Oxygenase propertiesof crystallized fraction I protein from tobacco.Arch. Biochem. Biophys., 1976, 173, 341-46.
Hansen, B.A & Dekker, E.E. Inactivation ofbovine liver by 2-keto-4-hydroxyglutarate aldolaseby cyanide in the presence of aldehydes;
Biochemistry, 1976,15,2912-17.Heymans, C; Bouckaret, J .J .& Dautrebande, L.Au sujet du mecanisme de la stimulation respiratorpar le sulfure de sodium. Compt. Rend. Soc. Bioi. ,1931, 106, 52-54.Weger, N .P .Treatment of cyanide poisoning with
4-dimethylaminophenol (DMAP): Experimentaland clinical overview. Fund. Appl. Toxicol. 1983,3, 387-96.
Christel, D; Eyer, P; Hegemann, M; Kiese, M;Lorcher, W. & Weger, N. Pharmacokinetics ofcyanide in poisoning of dogs and effect of4-dimethylaminophenol or thiosulphate. Arch.
Toxicol, 1977, 38, J77-89.Graham, D.L.; Laman, D.; Theodore, J. & RobinE.D. Acute cyanide poisoning complicated bylactic acidosis and pulmonary edema. Arch. Intern.Med., 1977,137, 1051-55.
Vogel, S.N.; Sultan, T.R. & Ten Eyck, R.P.Cyanide poisoning. Clin. Toxicol., 1981, 18,367.83. ,6.
Vennesland, B; Conn, E.E.; Knowles, C.J.;Westlay , J. & Wissing, F. Cyanide in biology.Academic Press, London, 1982. p. 548.
Way, J .L. Cyanide intoxication and its mechanismof antagonism. Ann. Rev. Pharmaca[. Taxical.,1984,24, 451-81.
Keilin, D. The history of cell respiration and
cytochrome. Cambridge University Press,Cambridge, 1966. p. 416.
Schuber~, J. & Brill, W .A. Antagonism ofexperimental cyanide toxicity in relation to the Inviva activity of cytochrome oxidase.l. Pharmaca[.Exp. Ther., 1968, 162, 352-59.
Isome, G.E.&Way, J,L. Effect of oxygen on theantagobism of cyanide intoxication, cytochromeoxidase in viva. Taxica[. App[. Pharmaca[., 1982,
65,250-56.
Jacob, A. & Diem, S. Activation ofglycogenolysis
338
RAZA & JAISWAL: MECHANISM OF CYANIDE TOXICITY AND-EFFICACY
18
30
19
31
20.
32.
21
33
22 34
3523
24. 36.
3725
2638
n39
40.
and sodium thiosulphate as a cyanide antidote. J.
Emerg. Med., 1987, 5,115-21.
Smith, R.P. The nitrite methaemoglobin complex-its significance in methaemoglobin analyses andits possible role in methaemoglobinemia.Biochem. Pharmacol. , 1967, 16, 1655-64.
.Kruszyna, R.; Kruszyna, H. & Smith, R.P.Comparison of hydroxylamine, 4-dimethylamino-phenol and nitrite protection against cyanidepoisoning in mice. Arch. Toxicol., 1982, 49,191-202.
Bhattacharya, R.; leevaratnam, K.: Raza, S.K.& Das Gupta, S. Cyanide antagonism in rodentmodels. Arch Toxicol. (Suppl.), 1991, 14,231-35.
Agar N.S. & Hardy, J.D. Erythrocytemethaemoglobin reductase of various mammalianspecies. Experientia, 1972, 28, 1248-49.
Szinicz, L.; Weger, N.; Schneideman, L. & Kiese,M. Nephrotoxicity of amino phenols: Effect of 4-dimethylaminophenol on isolated rat kidneytubules. Arch. Toxicol. 1979, 42, 63-73.
Kiese, M. & Munch, W. Kinetic derhamiglobinbildung, VI. Mitteilunghamiglobinbildung durch hydroxylamine. Arch.Exp. Pathol. Pharmacol., 1950,211, 115-20.
Bhattacharya, R. ; Jeevaratnam, K. ; Raza, S.K.& Das Gupta, S. Protection against cyanidepoisoning by the co-administration of sodiumnitrite and hydroxylamine in rats. Human Exp.Toxicdl., 1993, 12, 33-36.
Marcf1, l. Advanced organic chemistry: Reactions,mechanisms and structure, Ed. 3. John Wiley,New York, 1985. p. 854.
Cittadini, A. ; Caprino, L. & Terranova, T. Theeffect of pyruvate on cyanide inhibited respirationin intact ascites tumor cells. Experientia, 1971, 27,633-35.
Schwartz, C.; Morgan, R.L.; Way, L.M. & Way,l.L. Antagonism of cyanide intoxication withsodium pyruvate. Toxicol. Appl. Pharmacol. ,
1979, 50,437-41.
Moore, S.l.; Norris, l.C.; Ho, I.K. & Hume, A.S.The efficacy of alpha-ketoglutaric acid in theantagonism of cyanide intoxication. Toxicol. Appl.Pharmacol., 1986, 82, 40-44.
Norris, .l.C.; Utley, W.A. & Hume, A.S.
28
4129.
Hall, A.H; Rumack, B.H; Schaffer, M.I. &Linden, C.H. Clinical toxicology of cyanide: NorthAmerican clinical experiences. In Ref. 7. pp.312-33.
Klaussen, C.D. Nonmetallic environmental1oxic-ants: Air pollutants, solvents and vapours andpesticides. In The pharmacological basis oftherapeutics, edited by Oilman, A.O; Rall, T. W.;Nies, A.S. & Taylor, P., Edn. 8. Pergamon Press,New York, 1990. pp. 1615-39.
Chen, K.K.; Rose, C.L. & Clowes, O.H.A. Amylnitrite and cyanide poisoning. J. Am. Med. Assoc.,1933, 100, 1920-22.
Chen, K.K. ; Rose, C.L. & .Clowes, O.H.A.Methylene blue, nitrites and sodium thiosulphateagainst cyanide poisoning. Proc. Soc. Exp. Bioi.Med., 1933,31, 250-51.
Jandorf, B.J. & Bodansky, 0. Therapeutic andprophylactic effect of methaemoglobinemia ininhalation poisoning by hydrogen cyanide andcyanogen chloride. J. Ind. Hyg. Toxicol., 1946,28, 124-32.
Offterdinger, H. Wirkung verschiedenerblausaure-antidote auf den herzmuskel, NaunnynSchmiedebergs. Arch. Pharmacol. , 1970,266,416.
Weber, H.D.; Friedberg, K.D. & Lendle, L.Beurteilung therapeutischer massnahmen beiderblausaurcurevergiftlung unter constantercyanidinfusion. Arch. Exp. Pothol. Pharmacol. ,1962,244, 1-16.
Weger, N. Aminophenole als Blauf~ -e-Antidote. Arch. Toxicol., 1968, 49, 50.
Kiese, M. & Weger, N. Formation offerrlhaemoglobin with amino phenols in humansfor the treatment of cyanide poisoning. Eur. J.
Pharmacol., 1969,7,97-105.
Klimmek, R.; Fladerer, H. & Weger, N.Circulation, respiration and blood homeostasis incyanide poisoned dogs after treatment with4-dimethylaminophenol or cobaltous compounds.Arch. Toxicol., 1979, 43, 121-33.
Kiese, M.; Szinicz, L. Thiel, N. & Weger, N.Ferrihaemoglobin and kidney lesion in ratsproduced by 4-amino phenol or dimethylamino-phenol. Arch. Toxicol., 1975, 34, 337-40.
Hall, A.H. & Rumack, B. Hydroxycobalamine
339
DEF SCI J, VOL 44, NO 4, OcrOBER 1994
52.
42. 53.
54.43.
55
44
56
45.
57
46. 58.
59.
60.47.
48.
Mechanism of antagonizing cyanide inducedlethality by alpha-ketoglutaric acid. Toxicology,1~, 62, 275-83.
Keniston, R.C.; Cabellon, S. (Jr) & Yarbrough,K.S. pyridoxal-5-phosphate as an antidote forcyanide, spermine, gentamicin and dopaminetoxicity: An in vivo rat study. Toxicol. Appl.
Pha,macol., 1987,88,433-41.
Halpem, J.; Guastalla, G & Bercaw, J. Someaspects of the chemistry of cobalt (I) cyanide andrelated complexes. Coord. Chem. Rev., 1972, 8,167-84.
Meurice, J. Intoxication et disintoxication dedifferents nitriles par l' hy~sulfite de soude etles sels metalliques. Arch. Intern. Pharmacodyn.,1900, 7, 12-53.
Machete, C.W.; Kelley, K.L.; Boxer, G.E. &Rickards, J. C. Antidotal efficacy of vitamin B12(hydr'..v,!cobalamine) in experimental cyanidepoisoning. Proc. Soc. Exp. Bioi. Med., 1952, 81,234-37.
Friedberg, K.D. & Shukla, U.R. The efficacy ofaquocobalamine as an antidote in cyanidepoisoning when given alone or combined withsodium thiosulphate. Arch. Toxicol, 1975, 33,103-13.
Evans, C.L. Cobalt compounds as antidotes forhydrocyanic acid. Brit. I. Pharmacol. Chemother,
1964, 23,455-75.
Burrows, G.E. & Way, J.L. Cyanide intoxicationin sheep: Antagonism with sodium nitrite cobaltchloride and sodium thiosulphate. Am. I. Vet.
Res., 1979, 40,613-17.
61
62,
49. Isom, G. & Way, J.L. Cyanide intoxication:
Protection with cobaltous chloride. Toxicol. Appl.
Pharmacol., 1972,24,449-56.
63.Frankenberg, L. & Sorbo, B. Effect of cyanideantidotes on metabolic conversion of cyanide tothiocyanate. Arch. Toxicol., 1975, 33, 81-89.
50.
64.
Shen, S.C.; Ley, A.B. & Grant, V.M.Methaemoglobin formation in human blood bycobalt in vitro. I. Clin.lnvest., 1954, 33,1560-66.
Goldenberg, M.M. & Mann, D.E. Jr. Theantidotal effectiveness of sodium cobaltinitrite inantagonizing cyanide poisoning in albino mice. I.Am. Pharm. Assoc., 1960, 49,210-12.
DeGarbino, J.P. & Bismuth, C. Propositionstherapeutiques actuallesen cas d' intoxication parles cyanures., Toxicol. Eur. Res., 1981, 3,69-76.
Sorbo, B.H. Crystalline rhodanase II. The enzymecatalyzed reactions., Acta Chem. Scand., 1953, 7,1137-45.
Hug, E. Accion del nitrite de sodiyl delhyposulphite de sodio en el tratomiento de laintoxication provocado por el cianura de potassioen el Conejo. Revta. Soc. Argent. Bioi., 1933, 9,91-97.
Himwich, W.A. & Saunders, J.P. Enzymaticconversion of cyanide to thiocyanate. Am. I.Physiol., 1948, 153, 348-54.
Sorbo, B.H. On the substrate specificity ofrhodanase. Acta Chem. Scand., 1953, 7,1129-36.
Westley, J. Rhodanase. Adv. Enzymol., 1973, 39,327-368.
Westley, J. Sulfur transfer catalysis by enzymes.In Bio-organic chemistry, edited by E.E. VanTame Len. Academic Press, New York, 1977. pp.371-90.
Westley, J. ; Alder, A. ; Westley, L & Nishida, C.The sulfur transferase. Fund. Appl. Toxical.,1983, 3, 377-82.
Westley, J. Rhodanase and the sulphane pool. InEnzymatic basis of detoxication, Vol. II, editedby W.B. Jacoby. Academic Press, New York,1980. pp. 245-62.
Burrows, G.E. & Way, J.L: Cyanide intoxicationin sheep: Therapeutic value of oxygen or cobalt.Am. I. Vet. Res., 1977, 38,328-30.
Burrows, G.E; Liu D.H.W. & Way, J.L. Effectof oxygen on cyanide intoxication v: Physiologiceffects. I. Pharmacal. Exp. Ther., 1973, 184,739-48.
Niggler, J.; Provoost, R.A. & Parizel, G.Hydrogen cyanide poisoning: Treatment withcobalt-EDTA.J. Occup. Med., 1978,20,414-16.
51
340





























