Embed Size (px)
Citation preview

DOI: 10.1542/peds.2009-2995; originally published online June 7, 2010; 2010;126;e124Pediatrics
Nicholas Hoque, Ela Chakkarapani, Xun Liu and Marianne ThoresenPerinatal Asphyxia
A Comparison of Cooling Methods Used in Therapeutic Hypothermia for
http://pediatrics.aappublications.org/content/126/1/e124.full.html
located on the World Wide Web at: The online version of this article, along with updated information and services, is
of Pediatrics. All rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Boulevard, Elk Grove Village, Illinois, 60007. Copyright © 2010 by the American Academy published, and trademarked by the American Academy of Pediatrics, 141 Northwest Pointpublication, it has been published continuously since 1948. PEDIATRICS is owned, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
at Universitetsbiblioteket I Oslo on August 9, 2013pediatrics.aappublications.orgDownloaded from

A Comparison of Cooling Methods Used inTherapeutic Hypothermia for Perinatal Asphyxia
WHAT’S KNOWN ON THIS SUBJECT: Large clinical trials haveshown the benefit of hypothermia for neonatal encephalopathy.A number of methods are used to cool infants, but it is unclearwhether there are differences in temperature and hemodynamicstability between methods.
WHAT THIS STUDY ADDS: Whole-body cooling by using a servo-controlled system virtually eliminated overshoot at the onset ofcooling and maintained core temperature within a narrow rangeduring treatment and rewarming. None of the methods studiedhad an adverse effect on hemodynamic parameters.
abstractOBJECTIVE: The objective of this study was to compare cooling meth-ods during therapeutic hypothermia (TH) for moderate or severe peri-natal asphyxia with regard to temperature and hemodynamic stability.
METHODS: A total of 73 newborns received TH in our center between1999 and 2009 by 4 methods: (1) selective head cooling with mild sys-temic hypothermia by using cap (SHC; n� 20); (2) whole-body coolingwith mattress manually controlled (WBCmc; n � 23); (3) whole-bodycooling with body wrap servo-controlled (WBCsc; n � 28); and (4)whole-body cooling with water-filled gloves (n� 2). Target rectal tem-peratures (Trec) were 34.5� 0.5°C (SHC) and 33.5� 0.5°C (WBC). Trec,mean arterial blood pressure, and heart rate were collected fromretrospective chart review.
RESULTS: Groups had similar baseline characteristics and conditionat birth. Trec waswithin target temperature�0.5°C for 97% of the timein infants with WBCsc, 81% in infants with WBCmc, 76% in infants withSHC, and 74% in infants who were cooled with gloves. Mean overshootwas 0.3°C for WBCsc, 1.3°C for WBCmc, and 0.8°C for SHC groups. Therewas no difference in mean arterial blood pressure or mean heartbetween groups during the maintenance of cooling. In infants whowere rewarmed at similar speed, there was greater variation in Trec inthe SHC compared with the WBCsc group.
CONCLUSIONS: Manually controlled cooling systems are associatedwith greater variability in Trec compared with servo-controlled sys-tems. Amanualmattress often causes initial overcooling. It is unknownwhether large variation in temperature adversely affects the neuro-protection of TH. Pediatrics 2010;126:e124–e130
AUTHORS: Nicholas Hoque, MBBS, Ela Chakkarapani,MBBS, Xun Liu, MD, PhD, and Marianne Thoresen, MD, PhD
Child Health, School of Clinical Sciences, University of Bristol, StMichael’s Hospital, Bristol, Avon, United Kingdom
KEY WORDSnewborn, perinatal asphyxia, therapeutic hypothermia, coolingmethod, rewarming, cardiovascular
ABBREVIATIONSTH—therapeutic hypothermiaTrec—rectal temperatureMABP—mean arterial blood pressureHR—heart rateSHC—selective head coolingWBCmc—manually controlled whole-body coolingWBCsc—servo-controlled whole-body coolingbpm—beats per minute
www.pediatrics.org/cgi/doi/10.1542/peds.2009-2995
doi:10.1542/peds.2009-2995
Accepted for publication Mar 29, 2010
Address correspondence to Marianne Thoresen, MD, PhD, ChildHealth, School of Clinical Sciences, University of Bristol, StMichael’s Hospital, Southwell St, Bristol, Avon, BS2 8EG, UnitedKingdom. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2010 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: The authors have indicated they haveno financial relationships relevant to this article to disclose.
e124 HOQUE et al at Universitetsbiblioteket I Oslo on August 9, 2013pediatrics.aappublications.orgDownloaded from

Therapeutic hypothermia (TH) has awide range of clinical applications thatinclude themanagement of cardiac ar-rest in adults, perinatal asphyxia, andtraumatic brain injury and during car-diac surgery. It has been shown to im-prove outcome after perinatal as-phyxia in 3 large clinical trials.1–3
Furthermore, hypothermia has be-come the standard of care for new-borns with asphyxiation in many cen-ters throughout the world. Althoughthe principles of cooling infants re-main the same, the method of coolinghas differed greatly both within andoutside the trial setting.1–10 Since thesetrials have been completed, newertechnologies that are currently in clin-ical use have emerged, yet many ques-tions regarding the differences be-tween themethods that are being usedremain to be answered. The CoolCaptrial used a water-filled cap (OlympicMedical Cool Care System [OlympicMedical, Seattle, WA]) applied to the in-fant’s head to induce selective headcooling combined with radiant heatingwhilemaintaining core temperature at34.5°C.1 The Total Body Hypothermiafor Neonatal Encephalopathy (TOBY)trial used a mattress circulated with acoolant fluid (Tecotherm, TS Med 200M[Tec-Com, Munich, Germany]) with man-ual adjustment of mattress tempera-ture to maintain core temperature at33.5°C.3 Following these trials, we havealso used a body wrap (CritiCool [MTRE,Yavne, Israel]) that allows servo-controlled, automated adjustment ofwater temperature. The variability oftemperature and hemodynamic pa-rameters among cooling methods hasnot previously been described in alarge number of infants.11,12 This is ofinterest because fluctuations in rectaltemperature (Trec) and consequentlybrain temperature may adversely af-fect the neuroprotective effect of TH.Changes in brain temperature may af-fect blood-brain barrier permeability,leading to edema, and allow passage
of neurotoxic substances into thebrain.13 In particular, the period of re-warming has been associated with he-modynamic problems and other com-plications, including seizures.14 In thisobservational study, we sought to com-pare various cooling methods with re-spect to variation in Trec, mean arte-rial blood pressure (MABP), and heartrate (HR).
METHODS
Between July 1999 and January 2009,73 infants received TH for perinatal as-phyxia in our center. All infants werehad either moderate or severe as-phyxia, fulfilling the clinical entry crite-ria that were used in the CoolCap andTOBY trials.1,3 Infants were sequentiallyrecruited to studies in which differentcooling methods were used as part ofthe protocol: 20 (27%) used selectivehead cooling (SHC), 23 (32%) usedmanually controlled whole-bodycooling (WBCmc), 28 (38%) usedservo-controlled whole-body cooling(WBCsc), and 2 (3%) used water-filledlatex gloves. We made a retrospectiveanalysis of case notes to calculatemean Trec, BP, and HR at hourly inter-vals; consequently, treatment was notrandomized. Other than TH and the useof air in delivery room resuscitation,there were no significant changes incare of infants during the study period.
We chose to examine 3 distinct periodsof cooling: (1) initiation of hypother-mia; (2) maintenance of hypothermia;and (3) rewarming. For rewarming, wepresent only infants who were re-warmed at a similar speed, over 6hours (47% of infants), the remainderbeing rewarmed at a variety of slowerspeeds. Initiation of hypothermia wasdefined as when the cooling devicewas activated until a stable (at least 15minutes) target Trec was achieved(34–35°C for SHC; 33–34°C for WBC).Achieving a stable target temperaturewas defined as the first time 2 consec-
utive hourly measurements within thetarget range were recorded. The pe-riod of maintenance of hypothermiawas defined as starting at the point ofachieving a stable target temperatureuntil the start of rewarming. The pe-riod of rewarming was defined as thepoint of initiation of rewarming untilcore temperature reached 36.0°C.
Cooling With Gloves
Two infants were cooled by using rub-ber gloves filled with cold water(�10°C) placed laterally along thetrunk, the axillae, the neck, and thehead. Infants were exposed, all heatingwas removed, and occasionally anelectric fan was used. Target Trec was33.0 to 34.0°C for 72 hours. Because ofthe small group size, these infantswere excluded from the statisticalanalysis.
SHC With Mild SystemicHypothermia by Using Cap
Infants in the SHC group were cooledby using a cap filled with water. A ther-mostatically controlled cooling unitand pump circulated water throughthe cap initially between 8 and 12°C.A radiant heater that was servo-controlled to keep the infant’s abdom-inal skin temperature �36.5°C wasswitched on shortly after the initiationof cooling, when Trec had fallen to35.5°C. The temperature of water cir-culating within the cap was manuallyadjusted to maintain Trec between 34and 35°C. During initiation and mainte-nance of cooling, the cap temperaturewas gradually raised to between 19and 23°C to maintain Trec within tar-get. Rewarming was achieved byremoving the cap and continuingoverhead heating to increase coretemperature gradually by up to 0.5°C/hour.
WBCmc With Mattress
Infants in the WBCmc group werecooled by using a mattress with cir-
ARTICLES
PEDIATRICS Volume 126, Number 1, July 2010 e125 at Universitetsbiblioteket I Oslo on August 9, 2013pediatrics.aappublications.orgDownloaded from

culating thermostatically controlledcoolant fluid. The fluid temperaturewas manually adjusted to maintainTrec between 33 and 34°C. The fluidtemperature would typically be 10 to20°C when cooling started and 30 to25°C at the end of the maintenance pe-riod of cooling.
WBCsc With Body Wrap
Infants in the WBCsc group werecooled by using a body wrap with cir-culating water applied to the chest,trunk, and lower limbs with a targetTrec of 33.5°C. Our practice is not touse the portion of the wrap that is in-tended to cover the head. Instead, weinsulate the head and neck from thewrap with a pillow by using 4r layersof bubble wrap.15 Water temperaturewas servo-controlled via an inbuiltalgorithm.
Written informed consent for studyparticipation was obtained from par-ents before treatment of infants whowere recruited for trials and pilotstudies. For infants who were treatedafter the trials ceased recruitment(November 31, 2006), consent was notroutinely obtained before the initiationof treatment, because TH was consid-ered the standard of care in our cen-ter. Ethical permission was obtainedfor retrospective analysis of anony-mized data from this patient group(09/H0106/64).
Statistical Analysis
Groups were compared by using 1-wayanalysis of variance, Kruskall-Wallistest, and Dunns posthoc test (SPSS15.0 [SPSS Inc, Chicago, IL]). P � .05was considered significant.
RESULTS
Baseline Characteristics
Baseline characteristics from 73 in-fants who received TH for perinatal as-phyxia and condition at birth were sim-ilar for the 3 larger groups (Table 1).
Eight infants did not complete treat-ment because they died.
Initiation of Hypothermia
During this period, Trec fell to amean � SD of 33.2 � 0.3°C forWBCsc, 32.2 � 0.7°C for WBCmc, and33.8 � 0.3°C for SHC groups (Fig 1,left). Only in the WBCsc group didTrec not fall below target tempera-ture range. When cooling with amanually controlled mattress, Trecwould often overshoot (ie, fall belowthe target range) during the initia-tion of hypothermia. The mean maxi-
mum overshoot was 0.3°C for WBCsc,1.3°C for WBCmc, and 0.8°C forSHC groups. There was significantlygreater overshoot in the manuallycontrolled groups compared withthe WBCsc group (SHC versus WBCsc,P � .05; WBCmc versus WBCsc, P �.001).
Maintenance of Hypothermia
Mean � SD Trec was maintainedwithin the target range in all 3 groups(33.4 � 0.2°C for WBCsc, 33.4 � 0.4°Cfor WBCmc, and 34.3 � 0.4°C for SHC;Fig 1, middle). Therewas a significantly
FIGURE 1Left, Individual infants’ Trec during initiation phase. Overshoot was greater in WBCmc versus WBCscgroup (P�.001). Middle, Mean� SD Trec during maintenance phase. Variation was greater in SHCand WBCmc groups versus WBCsc group (P�.001). Right, Mean� SD Trec during rewarming, over 4hours (SHC) and 6 hours (WBC) as a result of different starting temperatures.
TABLE 1 Baseline Characteristics
Characteristic Gloves(n� 2)
SHC(n� 20)
WBCmc(n� 23)
WBCsc(n� 28)
P
Gestational age, mean� SD, wk 39.5� 2.1 39.3� 1.7 40.1� 1.5 39.6� 1.3 .39Birth weight, mean� SD, g 3725� 884 3075� 653 3475� 843 3299� 554 .30Girls, n (%) 1 (50) 11 (58) 8 (35) 15 (54) .275-min Apgar score, median (IQR) 5 4 (2–5) 2 (0–5) 4 (1–6) .1910-min Apgar score, median (IQR) 5 5 (4–8) 4 (2–6) 5 (3–7) .19Worst pH within 60 min of birth,mean� SD
7.10 (0.10) 6.98 (0.10) 6.91 (0.20) 6.93 (0.20) .45
Worst base deficit within 60 minof birth, mean� SD
�15.5 (0.7) �17.9 (5.6) �17.6 (6.6) �18.3 (5.5) .99
Not completing treatment, n (%) 0 (0) 0 (0) 3 (13) 5 (18) .17
IQR indicates interquartile range.
e126 HOQUE et al at Universitetsbiblioteket I Oslo on August 9, 2013pediatrics.aappublications.orgDownloaded from

greater variability in Trec with eithermanually controlled group comparedwith theWBCsc group (P� .001). Therewas no difference in variation of Trecbetween the SHC and WBCmc groups.
There was no difference in MABP(mean� SD) during the maintenanceperiod of cooling between groups(49� 8mm Hg, for SHC, 51� 8mm Hg,for WBCmc, and 51 � 9 mm Hg, forWBCsc; Fig 2). Similarly, there was nodifference in mean� SD HR during themaintenance period of cooling be-tween groups (107 � 22 beats perminute [bpm] for WBCsc, 105 � 16bpm for WBCmc, and 103� 16 bpm forSHC; Fig 3). There was significantlygreater variation of both MABP (P �.01) and HR (P� .001) during themain-tenance period in the WBCsc groupwhen compared with the manuallycontrolled groups. Therewas no statis-tical difference between groups in thenumber of infants who received inotro-pic support among those who com-pleted treatment (�2 P� .08).
Rewarming
In the CoolCap trial protocol, rewarm-ing time from Trec 34.5 to 37.0°C was 4hours at a rate of �0.6°C/hour. In theTOBY protocol, rewarming time from33.5 to 36.5°C was 6 hours at a rate of0.5°C/hour. Since cooling was intro-duced to all infants with perinatalasphyxia (December 1, 2006), therewarming speed has been individual-ized and may be�0.5°C/hour depend-ing on BP and occurrence of seizures.In our infants, median (range) rate ofrewarming was 0.38 (0.30–0.80)°C/hour in SHC, 0.39 (0.20–0.80)°C/hourin WBCmc, and 0.25 (0.10–0.50)°C/hour in WBCsc groups. We comparedinfants who were rewarmed at a simi-lar rate with the 3 methods (Fig 1,right). Twelve infants in the SHC group,11 infants in the WBCmc group, and 7infants in the WBCsc group were re-warmed at a rate of 0.4°C. There was
significantly greater variation in Trecduring the rewarming period in theSHC group when compared with theWBCsc group (P� .01). The SD of Trecin the WBCmc group (0.4) was doublethat of the WBCsc group (0.2), but thisdifference was not statistically signifi-cant. There was also greater variationin MABP in the WBCmc group whencompared with the WBCsc group (Fig
2). There were no other statistical dif-ferences in MABP or HR between thegroups during rewarming.
Cooling With Gloves
One infant was inadvertently over-cooled, and Trec fell to a low of 31.6°C(Fig 4). This was accompanied by a fallin HR to a nadir of 70 bpm. Trec re-mained within target range 74% of the
FIGURE 2Left, Changes in mean� SDMABP during maintenance of cooling. Right, Changes in mean� SDMABPduring rewarming.
FIGURE 3Left, Changes inmean� SDHR duringmaintenance of cooling. Right, Changes inmean� SDHR duringrewarming.
ARTICLES
PEDIATRICS Volume 126, Number 1, July 2010 e127 at Universitetsbiblioteket I Oslo on August 9, 2013pediatrics.aappublications.orgDownloaded from
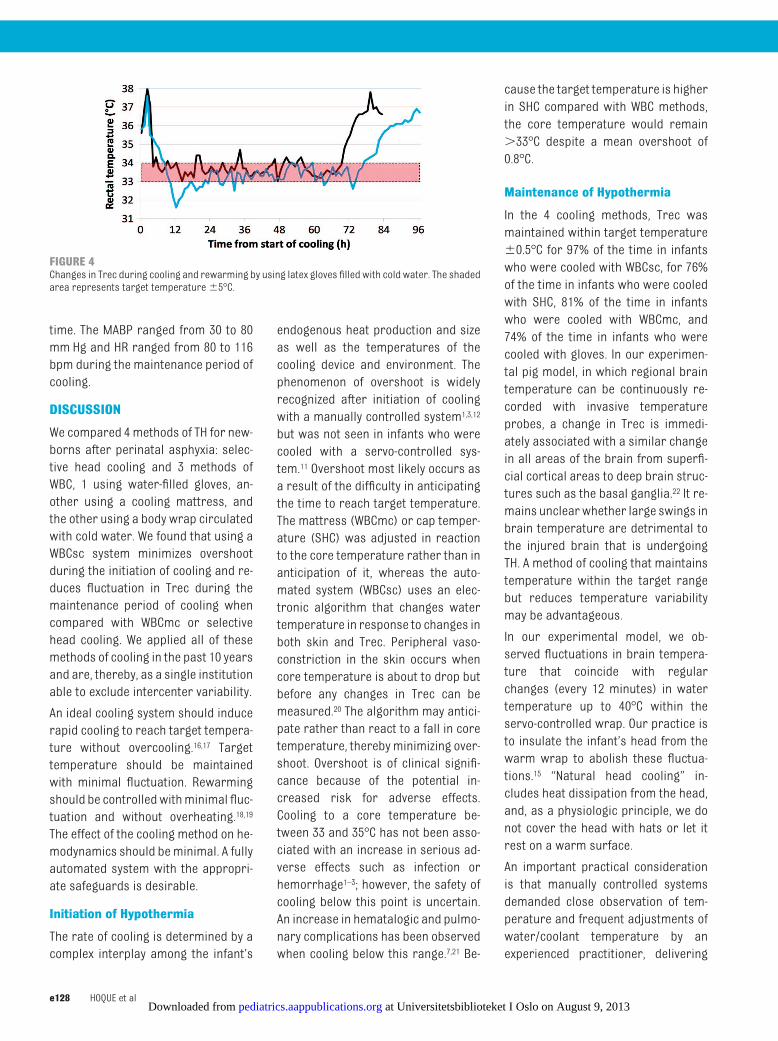
time. The MABP ranged from 30 to 80mm Hg and HR ranged from 80 to 116bpm during the maintenance period ofcooling.
DISCUSSION
We compared 4methods of TH for new-borns after perinatal asphyxia: selec-tive head cooling and 3 methods ofWBC, 1 using water-filled gloves, an-other using a cooling mattress, andthe other using a body wrap circulatedwith cold water. We found that using aWBCsc system minimizes overshootduring the initiation of cooling and re-duces fluctuation in Trec during themaintenance period of cooling whencompared with WBCmc or selectivehead cooling. We applied all of thesemethods of cooling in the past 10 yearsand are, thereby, as a single institutionable to exclude intercenter variability.
An ideal cooling system should inducerapid cooling to reach target tempera-ture without overcooling.16,17 Targettemperature should be maintainedwith minimal fluctuation. Rewarmingshould be controlledwithminimal fluc-tuation and without overheating.18,19
The effect of the cooling method on he-modynamics should beminimal. A fullyautomated system with the appropri-ate safeguards is desirable.
Initiation of Hypothermia
The rate of cooling is determined by acomplex interplay among the infant’s
endogenous heat production and sizeas well as the temperatures of thecooling device and environment. Thephenomenon of overshoot is widelyrecognized after initiation of coolingwith a manually controlled system1,3,12
but was not seen in infants who werecooled with a servo-controlled sys-tem.11 Overshoot most likely occurs asa result of the difficulty in anticipatingthe time to reach target temperature.The mattress (WBCmc) or cap temper-ature (SHC) was adjusted in reactionto the core temperature rather than inanticipation of it, whereas the auto-mated system (WBCsc) uses an elec-tronic algorithm that changes watertemperature in response to changes inboth skin and Trec. Peripheral vaso-constriction in the skin occurs whencore temperature is about to drop butbefore any changes in Trec can bemeasured.20 The algorithm may antici-pate rather than react to a fall in coretemperature, thereby minimizing over-shoot. Overshoot is of clinical signifi-cance because of the potential in-creased risk for adverse effects.Cooling to a core temperature be-tween 33 and 35°C has not been asso-ciated with an increase in serious ad-verse effects such as infection orhemorrhage1–3; however, the safety ofcooling below this point is uncertain.An increase in hematalogic and pulmo-nary complications has been observedwhen cooling below this range.7,21 Be-
cause the target temperature is higherin SHC compared with WBC methods,the core temperature would remain�33°C despite a mean overshoot of0.8°C.
Maintenance of Hypothermia
In the 4 cooling methods, Trec wasmaintained within target temperature�0.5°C for 97% of the time in infantswho were cooled with WBCsc, for 76%of the time in infants who were cooledwith SHC, 81% of the time in infantswho were cooled with WBCmc, and74% of the time in infants who werecooled with gloves. In our experimen-tal pig model, in which regional braintemperature can be continuously re-corded with invasive temperatureprobes, a change in Trec is immedi-ately associated with a similar changein all areas of the brain from superfi-cial cortical areas to deep brain struc-tures such as the basal ganglia.22 It re-mains unclearwhether large swings inbrain temperature are detrimental tothe injured brain that is undergoingTH. A method of cooling that maintainstemperature within the target rangebut reduces temperature variabilitymay be advantageous.
In our experimental model, we ob-served fluctuations in brain tempera-ture that coincide with regularchanges (every 12 minutes) in watertemperature up to 40°C within theservo-controlled wrap. Our practice isto insulate the infant’s head from thewarm wrap to abolish these fluctua-tions.15 “Natural head cooling” in-cludes heat dissipation from the head,and, as a physiologic principle, we donot cover the head with hats or let itrest on a warm surface.
An important practical considerationis that manually controlled systemsdemanded close observation of tem-perature and frequent adjustments ofwater/coolant temperature by anexperienced practitioner, delivering
FIGURE 4Changes in Trec during cooling and rewarming by using latex gloves filled with cold water. The shadedarea represents target temperature�5°C.
e128 HOQUE et al at Universitetsbiblioteket I Oslo on August 9, 2013pediatrics.aappublications.orgDownloaded from

1-to-1 care. In addition, overcooling isdifficult to avoid when endogenousheat production is attenuated by theadministration of muscle relaxants,sedatives, or anticonvulsants.11,23 Theservo-controlled system required noadjustment to maintain stable Trec. AsTH moves out of the trial setting andbecomes a standard of care through-out the world, it is desirable to use acooling method that is less labor-intensive and requires less specialistknowledge.
Although, the servo-controlled systemachieved better stability in tempera-ture with a much reduced propensityto overshoot, there was increasedvariability in both MABP and HR withthis method. Nevertheless, the meansof both parameters remained withinthe desired ranges for a term infant inthis clinical setting. Moreover, thismagnitude of variation is commonlyobserved in infants who received in-tensive care and was not greater dur-ing hypothermia.
Rewarming
Good temperature control during re-warming is an important part of TH.Rapid rewarming may cause periph-eral vasodilation and hypotension. Theability of the heart to maintain ade-quate cardiac output may already beimpaired by myocardial injury fromthe asphyxial insult. Furthermore, ithas been observed that cerebral met-abolic rate for oxygen is increased and
cerebral fractional oxygen extractionis decreased during rapid rewarmingafter cardiopulmonary bypass,24,25 andseizures have been observed duringrewarming both clinically and in ex-perimental models.14,26 Certainly post-hypoxic hyperthermia is associatedwith adverse outcome in noncooledinfants.18,19
The results presented are from a ret-rospective analysis of infants whowere sequentially recruited to studies,consequently, the treatment groupsare not randomized. A limitation ofsmall group sizes coupled with multi-ple confounders including occurrenceof seizures is the difficulty to draw con-clusions regarding the effect of vari-ous cooling methods on long-term out-come. Clearly, there are inherentdifferences between WBC and SHC,such as temperature gradients withinthe brain that may or may not be im-portant in neuroprotection.27,28 Resolu-tion of this question requires a largercohort of infants who ideally have beenrandomly assigned between methods.
Other Servo-controlled CoolingSystems
Infants in the Eunice Kennedy ShriverNational Institute of Child Health andHuman Development trial of WBC werecooled by using a servo-controlledblanket with circulatingwater (Blanke-trol II Hyper-Hypothermia System [Cin-cinnati Sub-Zero, Cincinnati, OH]).2
Core temperature was measured with
an esophageal probe and lowered tothen maintained at 33.5°C. This systemwas associated with an initial over-shoot to a mean of 32.7°C that is un-likely to be clinically significant. Thismethod achieved a mean core temper-ature of 33.4 � 0.9°C (25th and 75thpercentiles, 33.2 and 33.5°C); however,a second, larger blanket attached tothe cooling system was needed to at-tenuate the variation in esophagealtemperature.29
Recently described is a custom-madeservo-controlled fan used in conjunc-tion with a servo-controlled radiantwarmer.10 Three fans that normallyare used to cool desktop computersdirect room temperature air cephalo-caudally over the infant. They achieveda mean Trec of 33.6°C with an SD of 0.1to 0.2°C in a pilot study of 10 infants.
CONCLUSIONS
The 4methods of cooling that we exam-ined all maintained Trec within a nar-row target range; however, the over-shoot and variation in temperaturewere reduced when a servo-controlledsystem was used compared with amanually controlled system.
ACKNOWLEDGMENTSWe thank University Hospital Bristol,Olympic Medical US, MRC UK, and Lae-rdal Foundation for Acute MedicineNorway for supporting organizational,staff, and equipment costs that werenecessary for obtaining and analyzingdata.
REFERENCES
1. Gluckman PD, Wyatt JS, Azzopardi D, et al.Selective head cooling with mild sys-temic hypothermia after neonatalencephalopathy: multicentre randomisedtrial. Lancet. 2005;365(9460):663–670
2. Shankaran S, Laptook AR, Ehrenkranz RA,et al. National Institute of Child Health andHuman Development Neonatal ResearchNetwork. Whole-body hypothermia for ne-onates with hypoxic-ischemic encephalop-athy. N Engl J Med. 2005;353(15):1574–1584
3. Azzopardi DV, Strohm B, Edwards AD, et al.
Moderate hypothermia to treat perinatalasphyxial encephalopathy [published cor-rection appears in N Engl J Med. 2010;362(11):1056]. N Engl J Med. 2009;361(14):1349–1358
4. Simbruner G, Haberl C, Harrison V, Linley L,Willeitner AE. Induced brain hypothermia inasphyxiated human newborn infants: a ret-rospective chart analysis of physiologicaland adverse effects. Intensive Care Med.1999;25(10):1111–1117
5. Azzopardi D, Robertson NJ, Cowan FM, Ruth-
erford MA, Rampling M, Edwards AD. Pilotstudy of treatment with whole body hypo-thermia for neonatal encephalopathy. Pedi-atrics. 2000;106(4):684–694
6. Thoresen M, Whitelaw A. Cardiovascularchanges during mild therapeutic hypother-mia and rewarming in infants with hypoxic-ischemic encephalopathy. Pediatrics. 2000;106(1):92–99
7. Eicher DJ, Wagner CL, Katikaneni LP, et al.Moderate hypothermia in neonatalencephalopathy: efficacy outcomes and
ARTICLES
PEDIATRICS Volume 126, Number 1, July 2010 e129 at Universitetsbiblioteket I Oslo on August 9, 2013pediatrics.aappublications.orgDownloaded from

safety outcomes. Pediatr Neurol. 2005;32(1):11–24
8. Horn AR, Woods DL, Thompson C, Els I, KroonM. Selective cerebral hypothermia for post-hypoxic neuroprotection in neonates using asolid ice cap. S Afr Med J. 2006;96(9 pt 2):976–981. Available at: www.abstracts2view.com/pasall/search.php?adv�15155.5. Ac-cessed April 24, 2009
9. Robertson NJ, Nakakeeto M, Hagmann C, etal. Therapeutic hypothermia for birth as-phyxia in low-resource settings: a pilot ran-domised controlled trial. Lancet. 2008;372(9641):801–803
10. Horn A, Thompson C, Woods D, et al. Inducedhypothermia for infants with hypoxic- isch-emic encephalopathy using a servo-controlled fan: an exploratory pilot study.Pediatrics. 2009;123(6). Available at:www.pediatrics.org/cgi/content/full/123/6/e1090
11. Thoresen M. Supportive care during neuro-protective hypothermia in the termnewborn: adverse effects and their preven-tion. Clin Perinatol. 2008;35(4):749–763
12. Azzopardi D, StrohmB. Temperature controlduring therapeutic moderate whole bodyhypothermia for neonatal encephalopathy.Arch Dis Child Fetal Neonatal Ed. 2009;Aug13 [epub ahead of print]
13. Kiyatkin EA, Sharma HS. Permeability of theblood-brain barrier depends on brain tem-perature. Neuroscience. 2009;161(3):926–939
14. Battin M, Bennet L, Gunn AJ. Rebound sei-zures during rewarming. Pediatrics. 2004;114(5):1369
15. Liu X, Hoque N, Chakkarapani E, Thoresen M.Wearing a hat increases cortical brain tem-perature by 2°C during whole body coolingof piglets. E-PAS2009:5155.5 Available at:www .abs t r a c t s 2 v i ew . c om/pasa l l /search.php?adv�1 5155.5. Accessed April24, 2009
16. Gunn AJ, Gunn TR, Gunning MI, Williams CE,Gluckman PD. Neuroprotection with pro-longed head cooling started before post-ischemic seizures in fetal sheep. Pediatrics.1998;102(5):1098–1106
17. Laptook AR, Corbett RJ, Sterett R, Burns DK,Garcia D, Tollefsbol G. Modest hypothermiaprovides partial neuroprotection whenused for immediate resuscitation afterbrain ischemia. Pediatr Res. 1997;42(1):17–23
18. Laptook A, Tyson J, Shankaran S, et al. Ele-vated temperature after hypoxic-ischemicencephalopathy: risk factor for adverse out-comes. Pediatrics. 2008;122(3):491–499
19. Wyatt JS, Gluckman PD, Liu PY, et al. Deter-minants of outcomes after head cooling forneonatal encephalopathy. Pediatrics. 2007;119(5):912–921
20. Froese G, Burton A. Heat losses from thehuman head. J Appl Physiol. 1957; 10(2):235–241
21. Compagnoni G, Bottura C, Cavallaro G, Cris-tofori G, Lista G, Mosca F. Safety of deephypothermia in treating neonatal asphyxia.Neonatology. 2008;93(4):230–235
22. Thoresen M, Simmonds M, Satas S, Tooley J,Silver I. Effective selective head cooling dur-ing posthypoxic hypothermia in newbornpiglets. Pediatr Res. 2001;49(4):594–599
23. Thoresen M. Cooling the newborn afterasphyxia: physiological and experimentalbackground and its clinical use. Semin Neo-natol. 2000;5(1):61–73
24. Enomoto S, Hindman BJ, Dexter F, Smith T,Cutkomp J. Rapid rewarming causes an in-crease in the cerebral metabolic rate foroxygen that is temporarily unmatched bycerebral blood flow: a study during cardio-pulmonary bypass in rabbits. Anesthesiol-ogy. 1996;84(6):1392–1400
25. Wardle SP, Yoxall CW, Weindling AM. Cere-bral oxygenation during cardiopulmonarybypass. Arch Dis Child. 1998;78(1):26–32
26. Gerrits LC, Battin MR, Bennet L, Gonzalez H,Gunn AJ. Epileptiform activity during re-warming from moderate cerebral hypo-thermia in the near-term fetal sheep. Pedi-atr Res. 2005;57(3):342–346
27. Laptook AR, Shalak L, Corbett RJ. Differ-ences in brain temperature and cerebralblood flow during selective head versuswhole-body cooling. Pediatrics. 2001;108(5):1103–1110
28. Karlsson M, Tooley J, Satas S, et al. Delayedhypothermia as selective head cooling orwhole body cooling does not protect brainor body in newborn pig subjected tohypoxia-ischemia. Pediatr Res. 2008;64(1):74–80
29. Shankaran S, Laptook A, Wright LL, et al.Whole body hypothermia for neonatalencephalopathy: animal observations as abasis for a randomized, controlled pilotstudy in term infants. Pediatrics. 2002;110(2pt 1):377–385
e130 HOQUE et al at Universitetsbiblioteket I Oslo on August 9, 2013pediatrics.aappublications.orgDownloaded from

DOI: 10.1542/peds.2009-2995; originally published online June 7, 2010; 2010;126;e124Pediatrics
Nicholas Hoque, Ela Chakkarapani, Xun Liu and Marianne ThoresenPerinatal Asphyxia
A Comparison of Cooling Methods Used in Therapeutic Hypothermia for
ServicesUpdated Information &
tmlhttp://pediatrics.aappublications.org/content/126/1/e124.full.hincluding high resolution figures, can be found at:
References
tml#ref-list-1http://pediatrics.aappublications.org/content/126/1/e124.full.hat:This article cites 26 articles, 10 of which can be accessed free
Subspecialty Collections
orn_infant_subhttp://pediatrics.aappublications.org/cgi/collection/fetus:newbFetus/Newborn Infantthe following collection(s):This article, along with others on similar topics, appears in
Permissions & Licensing
mlhttp://pediatrics.aappublications.org/site/misc/Permissions.xhttables) or in its entirety can be found online at: Information about reproducing this article in parts (figures,
Reprints http://pediatrics.aappublications.org/site/misc/reprints.xhtml
Information about ordering reprints can be found online:
rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Grove Village, Illinois, 60007. Copyright © 2010 by the American Academy of Pediatrics. All and trademarked by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elkpublication, it has been published continuously since 1948. PEDIATRICS is owned, published, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
at Universitetsbiblioteket I Oslo on August 9, 2013pediatrics.aappublications.orgDownloaded from





























