Embed Size (px)
Citation preview

This article appeared in a journal published by Elsevier. The attachedcopy is furnished to the author for internal non-commercial researchand education use, including for instruction at the authors institution
and sharing with colleagues.
Other uses, including reproduction and distribution, or selling orlicensing copies, or posting to personal, institutional or third party
websites are prohibited.
In most cases authors are permitted to post their version of thearticle (e.g. in Word or Tex form) to their personal website orinstitutional repository. Authors requiring further information
regarding Elsevier’s archiving and manuscript policies areencouraged to visit:
http://www.elsevier.com/copyright

Author's personal copy
Review
A unique emotional processing profile of euthymic bipolar disorder?A critical review
L. Mercer, R. Becerra n
Faculty of Computing, Health and Science, Edith Cowan University, Perth, Western Australia, Australia
a r t i c l e i n f o
Article history:
Received 5 June 2012
Received in revised form
24 October 2012
Accepted 24 October 2012Available online 6 December 2012
Keywords:
Bipolar
Euthymia
Remission
Emotional processing
Emotion
a b s t r a c t
Objectives: To undertake a critical review of the literature on emotional processing (EP) in bipolar
patients in remission. This literature review focuses on a number of dimensions of EP including facial
emotion recognition, emotional memory, affective theory of mind (ToM), affective attention and
affective auditory information processing.
Methods: A systematic search was conducted through PsychINFO and Medline databases to obtain
relevant literature. Studies that include behavioural measures of EP were included.
Results: The findings from this review demonstrate that bipolar disorder (BD) patients continue to
exhibit some EP deficits during euthymic phases. A number of factors believed to contribute to such
findings have been highlighted.
Conclusions: This review has shed light on some of the conflicting findings reported in the literature and
thus offers a more comprehensive profile of euthymic bipolar patients’ EP abilities. This information
could enrich clinicians’ therapeutic efforts to minimise relapse by attending to euthymic bipolar
patients’ specific emotional processing difficulties.
& 2012 Elsevier B.V. All rights reserved.
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 296
2. Methods . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 296
3. Results . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 296
3.1. Affective attention . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 296
3.2. Emotional memory. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 300
3.3. Facial emotion recognition . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 300
3.4. Mood induction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 301
3.5. Auditory processing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 302
3.5.1. Prosody . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 302
3.5.2. Criticism . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 302
3.5.3. Emotional sentences . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 302
3.6. Theory of mind. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 302
3.7. Other . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 302
4. Discussion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 303
4.1. Facial emotion recognition . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 303
4.2. Mood induction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 303
4.3. Affective attention . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 304
4.4. Auditory processing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 304
4.5. Memory . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 304
4.6. Theory of mind. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 304
4.7. Methodological issues . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 305
4.8. Limitations and recommendations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 306
Role of funding source . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 307
Conflict of interest. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 307
Acknowledgements . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 307
Contents lists available at SciVerse ScienceDirect
journal homepage: www.elsevier.com/locate/jad
Journal of Affective Disorders
0165-0327/$ - see front matter & 2012 Elsevier B.V. All rights reserved.
http://dx.doi.org/10.1016/j.jad.2012.10.030
n Correspondence to: Edith Cowan University, 270 Joondalup Drive, Joondalup, Perth, Western Australia 6027, Australia. Tel.: þ61 422 013245.
E-mail address: [email protected] (R. Becerra).
Journal of Affective Disorders 146 (2013) 295–309

Author's personal copy
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 307
Further reading . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 308
1. Introduction
BD is a common and debilitating illness. It is characterised bycyclic episodes of depression and mania, interspersed withperiods of recovery or euthymia (Robinson et al., 2008;American Psychiatric Association, 2000). Characterised by mooddisturbances, BD is classified as a Mood Disorder in the Diagnosticand Statistical Manual (American Psychiatric Association, 2000).There are three distinct types of BD; type I, type II and BD nototherwise specified (American Psychiatric Association, 2000).Bipolar I disorder (BDI) is characterised by the occurrence ofone or more manic episodes with or without episodes of depres-sion, whilst bipolar II disorder (BDII) is characterised by one ormore episodes of both hypomania and depression (Summerset al., 2006).
Research investigating the prognosis of BD has indicated thatdespite observed gains credited to pharmacological treatment(Goldberg, 2004) 50% of patients have been reported to relapsewithin the first year (Tohen et al., 1990), with these statisticsincreasing to 70% within 5 years (Gitlin et al., 1995). With relapsestatistics reported to be substantially high, it is important toinvestigate factors that may contribute to such relapse rates. Onepotential factor that could influence bipolar patients’ ability toeffectively participate in therapy and consequently contribute toreducing relapse rates is their ability to process emotionalinformation. Euthymic bipolar disorder (EBD) patients have beenreported to be more thought disordered when disclosing informa-tion of an emotional nature (Shimkunas, 1972; Tai, Haddock &Bentall, 2004) have difficulties comprehending facial emotionexpressions (Vaskinn et al., 2007) and understanding verbalaffective expressions (Bozikas et al., 2007). Consequently, aber-rant EP can lead to misunderstandings, confusion and problems insocial and therapeutic interactions (Vaskinn et al., 2007).
EP involves the identification, appraisal, understanding andregulation of generated emotions (Phillips, 2009). It requires theability to discriminate between and make sense of externalemotional stimuli and entails regulation of one’s own affectiveresponses (Phillips, 2003; Mayer and Cobb, 2000). Review of theliterature on EP has revealed inconsistent findings with evidenceboth supporting (Lex et al., 2008; Vaskinn et al., 2007) andcontradicting (Kerr et al., 2005; Bozikas et al., 2007) the presenceof emotional deficits in EBD patients. Such studies have onlyfocused their attention on one subsection of EP such as recogni-tion of facially expressed emotions, but have not included othertypes of EP (i.e. attention bias for emotional stimuli). Thus, thereappears to be a gap in the literature with no study to date havingconducted a comprehensive review on EBD patients’ EP abilities.It has also been speculated that bipolar patients may return tonormal levels of functioning during euthymia (de Almeida Rocca,van den Heuvel, Caaetano & Lafer, 2009). A comprehensive reviewof euthymic patients’ abilities to process emotional informationwill help to elucidate such speculation and assist to establish aclearer picture of the emotional profile of EBD.
The purpose of this literature review is to characterise theemotional profiles of EBD patients by conducting a critical reviewof EP in euthymic patients. One important aim is to generateinformation for clinicians who work with EBD patients to helpimprove clinical outcomes. Hence the focus of this review will beon the behavioural measures of EP only and will not includestudies that employed brain imaging measures of EP. Investigation
of the BD literature on EP has highlighted a number of majorsubcategories of EP which are as follows: facial emotion recogni-tion, emotional memory, affective ToM, affective attention andaffective auditory information processing. These subcategories ofEP will be included and critically reviewed.
2. Methods
A systematic search was conducted through PsychINFO andMedline databases to obtain relevant literature, for the period1975–2011 (15 March 2011) in peer reviewed journals in Englishlanguage only. Keywords used in the search were separated intofour groups and joined by ‘‘AND’’ operators. The first group ofwords identified BD patients; ‘‘Bipolar’’ or ‘‘Manic Depression’’.The second group identified remitted populations; ‘‘Remission’’,‘‘Remitted’’ or ‘‘Euthymic*’’. The next group consisted of thefollowing text strings: ‘‘Emotion*’’ or ‘‘Affect’’. The final groupconsisted of the following text strings and joined by ‘OR’ opera-tors; ‘‘Facial’’, ‘‘Processing’’, ‘‘Expression’’, ‘‘Stroop’’, ‘‘Perception’’,‘‘Competence’’, ‘‘Recognition’’, ‘‘Information Processing’’, ‘‘ Atten-tion’’, ‘‘Memory’’, ‘‘Intonation’’, ‘‘Auditory’’, ‘‘Tonality’’ and ‘‘ToM’’.
Selection criteria for papers were: (i) include EBD patients anda control group, (ii) present results separately for EBD patients toother BD patients, (iii) include adult population only, (iv) includea behavioural measure of EP (physiological and neurological datanot included in review).
3. Results
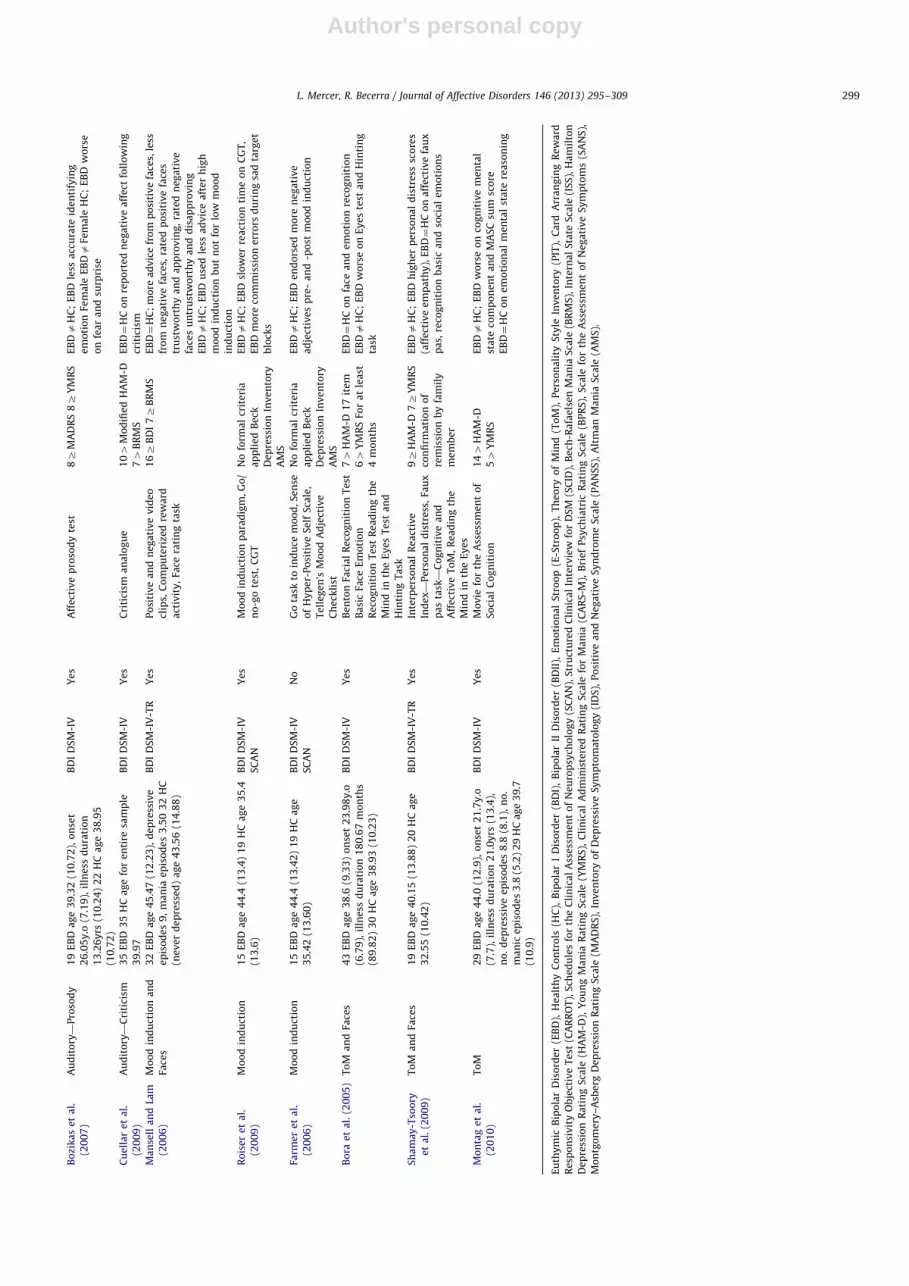
Thirty-four articles were confirmed to meet the inclusioncriteria. See Table 1. for an overview.
3.1. Affective attention
Attention for emotional stimuli has been examined in EBDpopulations using emotional Stroop, affective go/no-go and dot-probe tasks (i.e. Lex et al., 2008; Jongen et al., 2007). Researchersare interested in examining whether the inclusion of emotionalstimuli potentially places additional demands on participant’sprocessing abilities and thus may compromise their speed andaccuracy performance. Commonly affective go/no-go tasks consistof three conditions (positive, negative and neutral), whereby theparticipants are instructed to indicate when the identifiedvalenced word is viewed; i.e. in a positive affective conditionthe participant would indicate when a positive valenced wordappeared in the context of negatively valenced distracters (i.e.Jongen et al., 2007).
Emotional Stroop tasks have been used to demonstrate thatperformance can be modified by selective attention to emotionalstimuli by implicitly inducing affect through exposure to emo-tionally valent words (Malhi et al., 2005). In this task, participantsare required to selectively pay attention to the colour of thewords and thus inhibit or suppress responses to the content of thewords presented. A slower response rate to emotional words isindicative that the emotional content is interfering with one’sinformation processing abilities (Compton et al., 2003).
Three studies utilised emotional Stroop tasks to examine EP inEBD patients (Lex et al., 2008; Kerr et al., 2005; Malhi et al., 2005).
L. Mercer, R. Becerra / Journal of Affective Disorders 146 (2013) 295–309296

Author's personal copy
Ta
ble
1S
tud
ies
de
mo
gra
ph
icch
ara
cte
rist
ics,
ass
ess
me
nt
too
ls,
ap
pli
ed
crit
eri
aa
nd
resu
lts.
Re
fere
nce
Cla
ssifi
cati
on
Su
bje
cts
Dia
gn
osi
sa
nd
Dia
gn
ost
icC
rite
ria
Me
dic
ati
on
Re
po
rte
dP
rim
ary
Ass
ess
me
nt
To
ols
Re
mis
sio
nC
rite
ria
Re
sult
s
Ke
rre
ta
l.(2
00
5)
Att
en
tio
n1
5E
BD
ag
e4
7.6
6(9
.10
)il
lne
ss
du
rati
on
11
.2y
rs
18
HC
ag
e4
1.8
3(1
3.0
7)
No
cla
ssifi
cati
on
DS
M-I
II-R
Ye
sE
-Str
oo
pta
sk,C
ard
Str
oo
pta
sk74
Be
ckD
ep
ress
ion
Inv
en
tory
54
BR
MS
12
5r
ISS
we
llb
ein
g
20
0Z
ISS
act
iva
tio
n
For
at
lea
st8
we
ek
s
EB
Da
HC
;E
BD
slo
we
rn
eu
tra
l,p
osi
tiv
e,
ne
ga
tiv
eco
nd
itio
ns
Jon
ge
ne
ta
l.
(20
07
)
Att
en
tio
n1
3E
BD
ag
e4
3(8
.0)
HC
toE
BD
ag
e4
4(1
1.0
)
No
oth
er
info
rma
tio
np
rov
ide
d
No
cla
ssifi
cati
on
Op
era
tio
na
l
Cri
teri
aC
he
ckli
st
Ye
sC
om
bin
ed
Do
t-P
rob
eT
ask
an
d
Sp
ati
al
Cu
ein
gP
ara
dig
m
104
Be
ckD
ep
ress
ion
Inv
en
tory
EB
Da
HC
;E
BD
bia
sto
wa
rdd
ep
ress
ive
wo
rds
an
da
wa
yfr
om
po
siti
ve
wo
rds,
HC
bia
s
tow
ard
sp
osi
tiv
ew
ord
so
nly
,E
BD
slo
we
r
rea
ctio
nti
me
s
Ma
lhi
et
al.
(20
05
)
Att
en
tio
n1
2E
BD
ag
e3
4.9
(9.1
)il
lne
ssd
ura
tio
n
11
.9y
rs(7
.1),
no
.d
ep
ress
ive
ep
iso
de
s
10
.7(7
.9),
no
.m
an
ice
pis
od
es
4.3
(3.2
)
12
HC
ag
e3
3.7
(6.3
)
BD
ID
SM
-IV
-
(SC
ID-P
)
Ye
sE
-Str
oo
pta
sk64
HA
M-D
64
YM
RS
For
at
lea
st3
mo
nth
s
EB
Da
HC
;E
BD
rate
dn
eg
ati
ve
wo
rds
sig
nifi
can
tly
mo
ren
eg
ati
ve
We
ssa
et
al.
(20
07
)
Att
en
tio
n1
7E
BD
(10
BD
I,7
BD
II)
ag
e4
4.9
4
(12
.70
)il
lne
sso
nse
t2
2.6
y.o
(10
.5),
illn
ess
du
rati
on
21
.9y
rs(1
2.7
)1
7H
C
ag
e4
4.9
4(1
1.3
6)
BD
Ia
nd
BD
II
(co
mb
ine
d)
Dia
gn
ost
ic
Inte
rvie
wfo
r
Ge
ne
tic
Stu
die
s
Ye
sfM
RI
go
/no
-go
task
–p
ictu
res
of
faci
al
aff
ect
(fe
arf
ul,
ha
pp
y,
ne
utr
al)
54
HA
M-D
84
YM
RS
For
at
lea
st8
we
ek
s
EB
D¼
HC
on
go
/no
-go
task
Go
pin
et
al.
(20
11
)
Att
en
tio
n5
9E
BD
ag
e4
0.9
1(1
1.9
8)
14
4H
Ca
ge
37
.38
(12
.88
)
BD
ID
SM
-IV
(SC
ID-P
)
No
Go
/no
-go
task
—p
osi
tiv
e,
ne
ga
tiv
ea
nd
ne
utr
al
wo
rds
12Z
HA
M-D
12Z
CA
RS
-MB
PR
S
(72
)S
AN
S
EB
Da
HC
;E
BD
less
acc
ura
tep
osi
tiv
e
con
dit
ion
,sl
ow
er
po
siti
ve
an
dn
eu
tra
lst
imu
li
EB
D¼
HC
on
acc
ura
cyn
eg
ati
ve
an
dn
eu
tra
l
con
dit
ion
,n
od
iffe
ren
cere
act
ion
tim
efo
r
ne
ga
tiv
est
imu
li
Lex
et
al.
(20
08
)A
tte
nti
on
an
d
Me
mo
ry
19
EB
Da
ge
39
.7(1
0.6
)il
lne
ssd
ura
tio
n
19
.87
yrs
(9.4
7)
19
HC
ag
e4
8.1
(15
.2)
BD
ID
SM
-IV
Ye
sE
-Str
oo
pta
skIn
cid
en
tal
reca
ll
task
DS
M-I
VFo
ra
tle
ast
2m
on
ths
EB
D¼
HC
pe
rfo
rma
nce
e-S
tro
op
an
dm
em
ory
task
s
Ka
ue
r-S
an
t’A
nn
a
et
al.
,(2
00
8)
Me
mo
ry2
0E
BD
ag
e4
4.5
,il
lne
ssd
ura
tio
n1
8.8
20
HC
ag
e4
2.9
BD
Ia
nd
BD
II
(co
mb
ine
d)
DS
M-I
V
Ye
sH
eu
er
an
dR
eis
bu
rg
test
—n
eu
tra
la
nd
em
oti
on
al
sto
rie
s
DS
M-I
Vli
fech
art
ing
For
at
lea
st1
mo
nth
EB
Da
HC
;E
BD
no
en
ha
nce
me
nt
of
me
mo
ryfo
r
em
oti
on
al
con
ten
t,E
BD
rate
dn
eu
tra
lst
imu
li
as
mo
ree
mo
tio
na
lim
pa
ctin
g
Ma
lhi
et
al.
(20
07
a)
Me
mo
ry1
0E
BD
ag
e3
2.4
(10
.8)
illn
ess
du
rati
on
8.8
yrs
(5.8
),n
o.d
ep
ress
ive
ep
iso
de
s4
.9
(4.1
),n
o.
ma
nic
ep
iso
de
s3
.2(2
.6)
10
HC
ag
e3
1.7
(11
.9)
BD
ID
SM
-IV
(SC
ID-P
)
Ye
sW
ord
-ba
sed
me
mo
ryta
sk64
HA
M-D
64
YM
RS
For
at
lea
st3
mo
nth
s
EB
Da
HC
;E
BD
rate
dn
eg
ati
ve
wo
rds
mo
re
ne
ga
tiv
e,
EB
Dtr
en
dd
iffe
ren
cesl
ow
er
rea
ctio
n
tim
es
Va
nd
er
Gu
cht
et
al.
(20
09
)
Me
mo
rya
nd
Re
wa
rd
Re
spo
nsi
vit
y
43
EB
D4
1H
CN
oo
the
rin
form
ati
on
giv
en
No
cla
ssifi
cati
on
DS
M-I
V
No
Au
tob
iog
rap
hic
al
Me
mo
ry,
PIT
,C
AR
RO
T,
Mo
difi
ed
Re
spo
nse
Sty
leQ
ue
stio
nn
air
e
8Z
HA
M-D
3Z
BR
MS
For
at
lea
st2
mo
nth
s
EB
D¼
HC
on
PIT
,C
AR
RO
T,
reca
llp
osi
tiv
ea
nd
ne
ga
tiv
em
em
ori
es,
EB
Da
HC
;E
BD
mo
re
rum
ina
tio
nin
resp
on
seto
ne
ga
tiv
em
oo
d
De
rntl
et
al.
(20
09
)
Me
mo
rya
nd
Face
s2
6E
BD
Ia
ge
43
.15
(8.8
8),
on
set
38
.35
y.o
(8.8
6),
no
.o
fe
pis
od
es
4.7
7
(4.7
1)
36
EB
DII
ag
e4
2.6
7(1
0.1
2),
on
set
39
.74
y.o
(10
.12
),n
o.
of
ep
iso
de
s3
.31
(4.0
2)
62
HC
ag
e4
2.8
9(1
0.1
9)
BD
Ia
nd
BD
II
DS
M-I
V
Ye
sV
ien
na
Em
oti
on
Re
cog
nit
ion
Ta
skV
ien
na
Me
mo
ryo
f
Em
oti
on
Re
cog
nit
ion
No
form
al
crit
eri
a
ap
pli
ed
18Z
MA
DR
S
84
YM
RS
ex
cep
tfo
r
two
pa
tie
nts
(YM
RS¼
12
,1
3)
EB
DIa
HC
;E
BD
Isi
gn
ifica
nt
de
fici
tin
ge
ne
ral
em
oti
on
reco
gn
itio
n,
EB
DI
mis
too
ksa
dfa
ces
for
fea
rE
BD
II¼
HC
on
em
oti
on
reco
gn
itio
n
EB
DI
an
dE
BD
II¼
HC
me
mo
ryta
sk
Ro
bin
son
et
al.
(20
08
)
Face
s1
5E
BD
ag
e3
8.5
3(1
2.9
7)
16
HC
ag
e
36
.31
(10
.53
)
BD
ID
SM
-IV
Ye
sFa
cem
atc
hin
ga
nd
lab
ell
ing
task
fea
rfu
la
nd
an
gry
face
s
No
form
al
crit
eri
a
ap
pli
ed
4.0
77
2.9
9
HA
M-D
1.8
07
2.0
8
YM
RS
EB
D¼
HC
on
acc
ura
cya
nd
rea
ctio
nti
me
sfo
r
task
con
dit
ion
s
Ve
nn
et
al.
(20
04
)
Face
s1
7E
BD
(14
BD
I,3
BD
II)
ag
e4
4.3
5(3
.20
)
17
HC
ag
e4
3.7
6(3
.36
)
BD
I&
BD
II
(co
mb
ine
d)
DS
M-I
V
Ye
sIn
tera
ctiv
efa
cia
la
nd
em
oti
on
reco
gn
itio
nco
mp
ute
r
pro
gra
m—
5%
incr
em
en
tso
f
em
oti
on
84
HA
M-D
84
YM
RS
EB
D¼
HC
acr
oss
all
em
oti
on
reco
gn
itio
n
Ha
sse
le
ta
l.
(20
08
)
Face
s1
9E
BD
ag
e3
2.4
7(8
.8),
on
set
22
.47
y.o
(8.0
1),
illn
ess
du
rati
on
10
.6y
rs(6
.61
)
24
HC
ag
e2
7.7
8(8
.7)
BD
ID
SM
-IV
(SC
ID-I
)
Ye
sE
ve
nt-
rela
ted
pa
rad
igm
s—
mil
da
nd
inte
nse
ha
pp
y,
fea
rfu
la
nd
ne
utr
al
face
s,O
ve
rt
SC
IDa
nd
clin
ica
l
inte
rvie
wFo
ra
tle
ast
2m
on
ths
EB
D¼
HC
on
faci
al
em
oti
on
an
dg
en
de
r-
lab
ell
ing
acc
ura
cy
L. Mercer, R. Becerra / Journal of Affective Disorders 146 (2013) 295–309 297

Author's personal copy
Ta
ble
1(c
on
tin
ued
)
Re
fere
nce
Cla
ssifi
cati
on
Su
bje
cts
Dia
gn
osi
sa
nd
Dia
gn
ost
icC
rite
ria
Me
dic
ati
on
Re
po
rte
dP
rim
ary
Ass
ess
me
nt
To
ols
Re
mis
sio
nC
rite
ria
Re
sult
s
em
oti
on
lab
ell
ing
,Im
pli
cit
em
oti
on
task
—ju
dg
eg
en
de
r
Ha
sse
le
ta
l.
(20
09
)
Face
s1
4E
BD
ag
e3
2.6
4(9
.92
),o
nse
t2
2.0
0y
.o
(8.9
9),
illn
ess
du
rati
on
11
.69
yrs
(6.3
2)
16
HC
ag
e2
8.5
0(9
.28
)
BD
ID
SM
-IV
(SC
ID-I
)
Ye
sE
ve
nt-
rela
ted
pa
rad
igm
s—m
ild
an
din
ten
se
ha
pp
y,
fea
rfu
la
nd
ne
utr
al
face
s,O
ve
rte
mo
tio
nla
be
llin
g,
Imp
lici
te
mo
tio
nta
sk—
jud
ge
ge
nd
er
SC
IDa
nd
clin
ica
l
inte
rvie
wFo
ra
tle
ast
2m
on
ths
EB
D¼
HC
on
faci
al
em
oti
on
an
dg
en
de
r
lab
ell
ing
acc
ura
cy
Alm
eid
ae
ta
l.
(20
10
)
Face
s1
5E
BD
ag
e3
3.2
8(7
.83
),o
nse
t1
8.8
0y
.o
(6.8
2),
illn
ess
du
rati
on
14
.67
yrs
(5.4
8)
15
HC
ag
e3
2.6
9(8
.00
)
BD
ID
SM
-IV
(SC
ID-P
)
Ye
sM
ild
an
din
ten
see
mo
tio
na
l
(fe
ar,
sad
,h
ap
py
)a
nd
ne
utr
al
face
s
No
form
al
crit
eri
a
ap
pli
ed
EB
D¼
HC
on
aff
ect
reco
gn
itio
n,
bo
thre
du
ced
acc
ura
cyo
nla
be
llin
gsa
dfa
ces
Lem
bk
ea
nd
Ke
tte
r(2
00
2)
Face
s8
EB
DI,
EB
DII
10
HC
No
oth
er
info
rma
tio
ng
ive
n
BD
Ia
nd
BD
II
DS
M-I
V
No
Faci
al
ex
pre
ssio
nre
cog
nit
ion
task
—6
pri
ma
rye
mo
tio
ns
104
HA
M-D
104
YM
RS
EB
DI
an
dE
BD
II¼
HC
acr
oss
all
em
oti
on
sE
BD
II
be
tte
rfe
ar
reco
gn
itio
nth
an
EB
DI
Lan
ge
ne
cke
r
et
al.
(20
10
)
Face
s6
6E
BD
ag
e4
0.4
8(1
2.3
9),
no
.
de
pre
ssiv
ee
pis
od
es
21
.31
(59
.29
),n
o.
ma
nic
ep
iso
de
s7
.62
(9.9
2)
34
HC
ag
e
36
.85
(16
.60
)
BD
Ia
nd
BD
II
(co
mb
ine
d)
Dia
gn
ost
ic
Inte
rvie
wfo
r
Ge
ne
tic
Stu
die
s
Ye
sE
mo
tio
np
erc
ep
tio
nte
st,F
aci
al
em
oti
on
pe
rce
pti
on
test
No
form
al
crit
eri
a
ap
pli
ed
4.3
6
(2.9
0)¼
HA
M-D
1.4
4
(2.0
4)¼
YM
RS
EB
D¼
HC
on
em
oti
on
pro
cess
ing
test
Ad
din
gto
na
nd
Ad
din
gto
n
(19
98
)
Face
s4
0E
BD
ag
e3
8.5
(11
.0),
on
set
26
y.o
(9.2
)4
0H
Ca
ge
32
.6(1
1.3
)
No
cla
ssifi
cati
on
DS
M-I
II-R
Ye
sFa
cia
la
ffe
ctm
atc
hin
g
(dis
crim
ina
tio
nta
sk,)
Faci
al
aff
ect
lab
ell
ing
(id
en
tifi
cati
on
task
,)B
en
ton
Faci
al
Re
cog
nit
ion
Te
st
No
form
al
crit
eri
a
ap
pli
ed
‘‘All
BD
me
t
crit
eri
afo
rB
Din
rem
issi
on
’’e
xce
pt
on
e—
BD
de
pre
ssiv
e
typ
e
EB
D¼
HC
on
lab
ell
ing
faci
al
aff
ect
,fa
cia
l
reco
gn
itio
nE
BDa
HC
;E
BD
sho
we
dd
efi
cits
in
faci
al
aff
ect
ma
tch
ing
Bo
zik
as
et
al.
(20
06
)
Face
s1
9E
BD
ag
e3
9(1
1),
on
set
26
(7),
illn
ess
du
rati
on
13
(10
)3
0H
Ca
ge
38
(10
)
BD
ID
SM
-IV
Ye
sK
inn
ey
’sId
en
tity
an
dA
ffe
ct
Ma
tch
ing
Te
st
8Z
MA
DR
S8Z
YM
RS
EB
Da
HC
;E
BD
sig
nifi
can
tly
wo
rse
on
aff
ect
ma
tch
ing
EB
D¼
HC
on
ide
nti
tym
atc
hin
g
Kim
et
al.
(20
09
)Fa
ces
14
EB
Da
ge
30
.4(5
.9),
illn
ess
du
rati
on
4.3
yrs
(4.4
),n
o.d
ep
ress
ive
ep
iso
de
s1
.2
(1.3
),n
o.
ma
nic
ep
iso
de
s2
.2(1
.9)
14
HC
ag
e2
7.5
(3.3
)
BD
ID
SM
-IV
-TR
Ye
sV
irtu
al
av
ata
rsth
at
dis
pla
ye
d
em
oti
on
(an
gry
,h
ap
py
or
ne
utr
al)
7Z
HA
M-D
5Z
YM
RS
For
at
lea
st2
mo
nth
s
EB
D¼
HC
resp
on
sea
ccu
racy
EB
Da
HC
;E
BD
slo
we
rre
act
ion
tim
es
for
ex
pe
rim
en
tal
blo
cks
bu
tn
ot
con
tro
l
Ma
lhi
et
al.
(20
07
b)
Face
s1
0E
BD
ag
e3
3.5
(8.7
)il
lne
ssd
ura
tio
n
12
yrs
(7.7
),n
o.
de
pre
ssiv
ee
pis
od
es
10
.4(8
.7),
no
,m
an
ice
pis
od
es
4.7
(3.4
)
10
HC
ag
e3
3.6
(6.4
)
BD
ID
SM
-IV
(SC
ID-P
)
Ye
sFa
cia
le
mo
tio
nre
cog
nit
ion
task
—fe
ar,
dis
gu
st,
ne
utr
al
ex
pre
ssio
ns
6Z
HA
M-D
(17
ite
m)
6Z
YM
RS
For
at
lea
st
3m
on
ths
EB
D¼
HC
on
acc
ura
cyfa
cia
le
xp
ress
ion
sa
nd
tota
le
rro
rra
tes
EB
Da
HC
;E
BD
slo
we
rre
act
ion
tim
es
for
ne
utr
al
face
s
Ve
rsa
cee
ta
l.
(20
10
)
Face
s1
7E
BD
ag
e3
4.2
(8.4
),o
nse
t2
5.4
y.o
(10
.8),
illn
ess
du
rati
on
12
.3y
rs(9
.8)
24
HC
ag
e2
9.5
(9.6
)
BD
ID
SM
-IV
(SC
ID-P
)
Ye
sE
xp
lici
te
mo
tio
nla
be
llin
g
task
—h
ap
py
,sa
d,
ne
utr
al
ex
pre
ssio
ns
(mil
da
nd
inte
nse
)
7Z
HA
M-D
10Z
YM
RS
For
at
lea
st
2m
on
ths
EB
Da
HC
;E
BD
less
acc
ura
teh
ap
py
face
s
EB
D¼
HC
on
lab
ell
ing
sad
face
s
Yu
rge
lun
-To
dd
et
al.
(20
00
)
Face
s1
4E
BD
10
HC
no
furt
he
rin
form
ati
on
giv
en
No
cla
ssifi
cati
on
DS
M-I
V(S
CID
-P)
Ye
sFa
cia
le
mo
tio
nd
iscr
imin
ati
on
an
dla
be
lta
sk—
fea
rfu
la
nd
ha
pp
yfa
ces
No
form
al
crit
eri
a
ap
pli
ed
ran
ge
so
f
sco
res;
4–
24
HA
M-D
2–
29
YM
RS
EB
D¼
HC
on
ide
nti
fica
tio
nh
ap
py
face
s
EB
Da
HC
;E
BD
less
acc
ura
tefo
rfe
arf
ul
face
s
Ha
rme
re
ta
l.
(20
02
a)
Face
s2
0E
BD
ag
e3
7.8
(2.5
)2
0H
Ca
ge
37
.7
(3.8
)
No
cla
ssifi
cati
on
DS
M-I
V
Ye
sFa
cia
le
xp
ress
ion
reco
gn
itio
n
task
—1
0%
incr
em
en
tsFa
mo
us
face
cla
ssifi
cati
on
8Z
HA
M-D
8Z
YM
RS
For
at
lea
st6
mo
nth
s
EB
D¼
HC
aff
ect
reco
gn
itio
nE
BDa
HC
;E
BD
sma
llim
pa
irm
en
tin
fam
ou
sfa
cecl
ass
ifica
tio
n,
EB
Dfa
cili
tate
dre
cog
nit
ion
of
dis
gu
st
Ta
ie
ta
l.(2
00
4)
Au
dit
ory
—E
mo
tio
na
l
sen
ten
ces
16
EB
Da
ge
45
.5(1
1.2
7),
on
set
24
.6y
.o
(8.7
)2
0H
Ca
ge
33
.9(9
.51
)
No
cla
ssifi
cati
on
DS
M-I
V
Ye
sE
mo
tio
na
la
nd
no
n-e
mo
tio
na
l
inte
rvie
wq
ue
stio
ns
Sca
lefo
r
the
Ass
ess
me
nt
of
Th
ou
gh
t,
Lan
gu
ag
ea
nd
Co
mm
un
ica
tio
n
No
form
al
crit
eri
a
ap
pli
ed
For
at
lea
st
8w
ee
ks
EB
Da
HC
;sh
ow
ed
hig
he
rle
ve
lso
fth
ou
gh
t
dis
ord
er
inth
ee
mo
tio
na
lly
sali
en
tco
nd
itio
n
Va
skin
ne
ta
l.
(20
07
)
Au
dit
ory
—E
mo
tio
na
l
Se
nte
nce
sa
nd
Face
s
21
BD
ag
e3
8.1
(9.3
),il
lne
ssd
ura
tio
n
11
.5y
rs(1
0.9
)3
1H
Ca
ge
30
.7(9
.6)
BD
ID
SM
-IV
(SC
ID-P
)
Ye
sFa
ce/V
oic
eE
mo
tio
n
Ide
nti
fica
tio
na
nd
Dis
crim
ina
tio
nT
est
304
IDS
124
YM
RS
6Z
PA
NS
S
EB
D¼
HC
bo
thsh
ow
ed
no
de
fici
tso
na
ud
ito
ry
or
faci
al
em
oti
on
ide
nti
fica
tio
no
r
dis
crim
ina
tio
n
L. Mercer, R. Becerra / Journal of Affective Disorders 146 (2013) 295–309298
Author's personal copy
Bo
zik
as
et
al.
(20
07
)
Au
dit
ory
—P
roso
dy
19
EB
Da
ge
39
.32
(10
.72
),o
nse
t
26
.05
y.o
(7.1
9),
illn
ess
du
rati
on
13
.26
yrs
(10
.24
)2
2H
Ca
ge
38
.95
(10
.72
)
BD
ID
SM
-IV
Ye
sA
ffe
ctiv
ep
roso
dy
test
8Z
MA
DR
S8Z
YM
RS
EB
Da
HC
;E
BD
less
acc
ura
teid
en
tify
ing
em
oti
on
Fem
ale
EB
Da
Fem
ale
HC
;E
BD
wo
rse
on
fea
ra
nd
surp
rise
Cu
ell
ar
et
al.
(20
09
)
Au
dit
ory
—C
riti
cism
35
EB
D3
5H
Ca
ge
for
en
tire
sam
ple
39
.97
BD
ID
SM
-IV
Ye
sC
riti
cism
an
alo
gu
e1
04
Mo
difi
ed
HA
M-D
74
BR
MS
EB
D¼
HC
on
rep
ort
ed
ne
ga
tiv
ea
ffe
ctfo
llo
win
g
crit
icis
m
Ma
nse
lla
nd
Lam
(20
06
)
Mo
od
ind
uct
ion
an
d
Face
s
32
EB
Da
ge
45
.47
(12
.23
),d
ep
ress
ive
ep
iso
de
s9
,m
an
iae
pis
od
es
3.5
03
2H
C
(ne
ve
rd
ep
ress
ed
)a
ge
43
.56
(14
.88
)
BD
ID
SM
-IV
-TR
Ye
sP
osi
tiv
ea
nd
ne
ga
tiv
ev
ide
o
clip
s,C
om
pu
teri
zed
rew
ard
act
ivit
y,
Face
rati
ng
task
16Z
BD
I7Z
BR
MS
EB
D¼
HC
;m
ore
ad
vic
efr
om
po
siti
ve
face
s,le
ss
fro
mn
eg
ati
ve
face
s,ra
ted
po
siti
ve
face
s
tru
stw
ort
hy
an
da
pp
rov
ing
,ra
ted
ne
ga
tiv
e
face
su
ntr
ust
wo
rth
ya
nd
dis
ap
pro
vin
g
EB
Da
HC
;E
BD
use
dle
ssa
dv
ice
aft
er
hig
h
mo
od
ind
uct
ion
bu
tn
ot
for
low
mo
od
ind
uct
ion
Ro
ise
re
ta
l.
(20
09
)
Mo
od
ind
uct
ion
15
EB
Da
ge
44
.4(1
3.4
)1
9H
Ca
ge
35
.4
(13
.6)
BD
ID
SM
-IV
SC
AN
Ye
sM
oo
din
du
ctio
np
ara
dig
m,G
o/
no
-go
test
,C
GT
No
form
al
crit
eri
a
ap
pli
ed
Be
ck
De
pre
ssio
nIn
ve
nto
ry
AM
S
EB
Da
HC
;E
BD
slo
we
rre
act
ion
tim
eo
nC
GT
,
EB
Dm
ore
com
mis
sio
ne
rro
rsd
uri
ng
sad
targ
et
blo
cks
Farm
er
et
al.
(20
06
)
Mo
od
ind
uct
ion
15
EB
Da
ge
44
.4(1
3.4
2)
19
HC
ag
e
35
.42
(13
.60
)
BD
ID
SM
-IV
SC
AN
No
Go
task
toin
du
cem
oo
d,
Se
nse
of
Hy
pe
r-P
osi
tiv
eS
elf
Sca
le,
Te
lle
ge
n’s
Mo
od
Ad
ject
ive
Ch
eck
list
No
form
al
crit
eri
a
ap
pli
ed
Be
ck
De
pre
ssio
nIn
ve
nto
ry
AM
S
EB
Da
HC
;E
BD
en
do
rse
dm
ore
ne
ga
tiv
e
ad
ject
ive
sp
re-
an
d-p
ost
mo
od
ind
uct
ion
Bo
rae
ta
l.(2
00
5)
To
Ma
nd
Face
s4
3E
BD
ag
e3
8.6
(9.3
3)
on
set
23
.98
y.o
(6.7
9),
illn
ess
du
rati
on
18
0.6
7m
on
ths
(89
.82
)3
0H
Ca
ge
38
.93
(10
.23
)
BD
ID
SM
-IV
Ye
sB
en
ton
Faci
al
Re
cog
nit
ion
Te
st
Ba
sic
Face
Em
oti
on
Re
cog
nit
ion
Te
stR
ea
din
gth
e
Min
din
the
Ey
es
Te
sta
nd
Hin
tin
gT
ask
74
HA
M-D
17
ite
m
64
YM
RS
For
at
lea
st
4m
on
ths
EB
D¼
HC
on
face
an
de
mo
tio
nre
cog
nit
ion
EB
Da
HC
;E
BD
wo
rse
on
Ey
es
test
an
dH
inti
ng
task
Sh
am
ay
-Tso
ory
et
al.
(20
09
)
To
Ma
nd
Face
s1
9E
BD
ag
e4
0.1
5(1
3.8
8)
20
HC
ag
e
32
.55
(10
.42
)
BD
ID
SM
-IV
-TR
Ye
sIn
terp
ers
on
al
Re
act
ive
Ind
ex
—P
ers
on
al
dis
tre
ss,
Fau
x
pa
sta
sk—
Co
gn
itiv
ea
nd
Aff
ect
ive
To
M,
Re
ad
ing
the
Min
din
the
Ey
es
9Z
HA
M-D
7Z
YM
RS
con
firm
ati
on
of
rem
issi
on
by
fam
ily
me
mb
er
EB
Da
HC
;E
BD
hig
he
rp
ers
on
al
dis
tre
sssc
ore
s
(aff
ect
ive
em
pa
thy
),E
BD¼
HC
on
aff
ect
ive
fau
x
pa
s,re
cog
nit
ion
ba
sic
an
dso
cia
le
mo
tio
ns
Mo
nta
ge
ta
l.
(20
10
)
To
M2
9E
BD
ag
e4
4.0
(12
.9),
on
set
21
.7y
.o
(7.7
),il
lne
ssd
ura
tio
n2
1.0
yrs
(13
.4),
no
.d
ep
ress
ive
ep
iso
de
s8
.8(8
.1),
no
.
ma
nic
ep
iso
de
s3
.8(5
.2)
29
HC
ag
e3
9.7
(10
.9)
BD
ID
SM
-IV
Ye
sM
ov
iefo
rth
eA
sse
ssm
en
to
f
So
cia
lC
og
nit
ion
144
HA
M-D
54
YM
RS
EB
Da
HC
;E
BD
wo
rse
on
cog
nit
ive
me
nta
l
sta
teco
mp
on
en
ta
nd
MA
SC
sum
sco
re
EB
D¼
HC
on
em
oti
on
al
me
nta
lst
ate
rea
son
ing
Eu
thy
mic
Bip
ola
rD
iso
rde
r(E
BD
),H
ea
lth
yC
on
tro
ls(H
C),
Bip
ola
rI
Dis
ord
er
(BD
I),
Bip
ola
rII
Dis
ord
er
(BD
II),
Em
oti
on
al
Str
oo
p(E
-Str
oo
p),
Th
eo
ryo
fM
ind
(To
M),
Pe
rso
na
lity
Sty
leIn
ve
nto
ry(P
IT),
Ca
rdA
rra
ng
ing
Re
wa
rd
Re
spo
nsi
vit
yO
bje
ctiv
eT
est
(CA
RR
OT
),S
che
du
les
for
the
Cli
nic
al
Ass
ess
me
nt
of
Ne
uro
psy
cho
log
y(S
CA
N),
Str
uct
ure
dC
lin
ica
lIn
terv
iew
for
DS
M(S
CID
),B
ech
-Ra
fae
lse
nM
an
iaS
cale
(BR
MS
),In
tern
al
Sta
teS
cale
(IS
S),
Ha
mil
ton
De
pre
ssio
nR
ati
ng
Sca
le(H
AM
-D),
Yo
un
gM
an
iaR
ati
ng
Sca
le(Y
MR
S),
Cli
nic
al
Ad
min
iste
red
Ra
tin
gS
cale
for
Ma
nia
(CA
RS
-M),
Bri
ef
Psy
chia
tric
Ra
tin
gS
cale
(BP
RS
),S
cale
for
the
Ass
ess
me
nt
of
Ne
ga
tiv
eS
ym
pto
ms
(SA
NS
),
Mo
ntg
om
ery
–A
sbe
rgD
ep
ress
ion
Ra
tin
gS
cale
(MA
DR
S),
Inv
en
tory
of
De
pre
ssiv
eS
ym
pto
ma
tolo
gy
(ID
S),
Po
siti
ve
an
dN
eg
ati
ve
Sy
nd
rom
eS
cale
(PA
NS
S),
Alt
ma
nM
an
iaS
cale
(AM
S).
L. Mercer, R. Becerra / Journal of Affective Disorders 146 (2013) 295–309 299

Author's personal copy
Lex et al. (2008) found that patients and healthy controls (HC)required significantly less time to respond to neutral than positiveand negative words. Reaction times between negative and posi-tive words were not significantly different within groups. Malhiet al. (2005) found no significant difference between EBD patientsand HC speed or ability to correctly rate the emotional valence ofpresented word stimuli. Patients rated negative words as signifi-cantly more negative than HC. In contrast, after controlling for IQKerr et al. (2005) found that EBD patients were significantlyslower than HC on neutral, positive and negative conditions. Nosignificant differences in reaction times were found amongst thepatient groups (depressed, manic and euthymic BD and majordepressive disorder patients).
Two studies utilized affective go/no-go tasks (Wessa et al.,2007; Gopin et al., 2011) and one study employed a modified dot-probe task to assess EBD patients’ attention biases (Jongen et al.,2007). Gopin et al. (2011) found that EBD patients were signifi-cantly less accurate than HC on the positive affective condition.No significant differences were found on accuracy rates for thenegative and neutral conditions between the two groups.Response biases differed between HC and patients in the affectivenegative condition but not in the positive or neutral conditions;patients appeared to be more engaged and responsive to thepresentation of negative stimuli. EBD patients were significantlyslower than HC to respond to neutral and positive stimuli,however no differences were found for response times to negativestimuli (Gopin et al., 2011). Wessa et al. (2007) reported no globalattention deficits in EBD patients. No significant differencesbetween EBD patients and HC performance was found withrespect to reaction times, omission or false alarm errors acrossthe emotional and non-emotional tasks. Increased neural activitywas demonstrated by EBD patients specifically to emotionalstimuli however this did not result in observed deficits at abehavioural level.
In Jongen et al. (2007) EBD patients showed a bias towardsdepression-related words and a bias away from positive words,while HC showed a bias towards positive words and no bias fordepression words. A significant difference was found for attentionbias for depressed words between euthymic and depressed BDgroups. No difference was observed for positive words betweenpatient groups (Jongen et al., 2007).
Overall, results indicate that EBD patients abilities to processemotional material was compromised in three of the six affectiveattention studies (Kerr et al., 2005; Gopin et al., 2011; Jongenet al., 2007). It is noteworthy that although EBD patients in Malhiet al. (2005) displayed comparable speed and accuracy rates totheir HC comparisons, EBD patients displayed differentialresponding to negative words having rated them as significantlymore negative than HC.
3.2. Emotional memory
It has been argued that bipolar patients may display anenhanced perception of emotional stimuli and consequently anenhanced memory for emotionally charged events (Kauer-Sant’Anna et al., 2008). This hypothesis is based on previousfindings that suggest memory for emotional salient stimuli mayutilise specific neuro-anatomical circuitries, including the amyg-dala, which has been found to show increased activity in bipolarpatients (Kauer-Sant’Anna et al., 2008).
Five studies have examined memory for emotional stimuli inEBD patients (Lex et al., 2008; Kauer-Sant’Anna et al., 2008;Derntl et al., 2009; Malhi et al., 2007a; Van der Gucht et al.,2009) of which four studies suggest that EBD patients do notdisplay such deficits (Lex et al., 2008; Derntl et al., 2009; Malhiet al., 2007a; Van der Gucht et al., 2009). Statistically equal
numbers of positive, negative and neutral words were recalledby patients and HC, and no differences were found for positive,negative or neutral intrusions (Lex et al., 2008). No significantdifferences between groups were found on the emotional mem-ory task employed by Derntl et al. (2009) and Malhi et al. (2007a)Patients’ recall for positive and negative memories was compar-able to HC performance in Van der Gucht et al. (2009).
Kauer-Sant’Anna et al. (2008) presented neutral and emotionalstories (via narrated slides) to examine EBD patients’ emotionalmemory capacities. HC demonstrated better memory recall foremotional material over neutral material, while no difference wasfound between the percentage of correct answers for EBD patientson recall of emotional or neutral information. EBD patients weremore likely to rate neutral stimuli as having a greater emotionalimpact than controls.
3.3. Facial emotion recognition
Facial expressions provide channels in which crucial informa-tion regarding ones’ emotional state can be transmitted helping toenrich another’s understanding of their physical and socialsurroundings (Bourke et al., 2010; Venn et al., 2004). Theobservation of facially expressed emotions can signal a personto regulate their own affective state and behaviour (Phillips et al.,2003). Consequently, the ability to accurately interpret anddiscriminate facial expressions of emotion is essential for effec-tive social functioning (Venn et al., 2004) and thus an importantaspect of EP. The ability to process facially expressed emotionsmay be referred to as facial EP.
Nineteen studies have utilised facially expressed emotions toexamine EBD patients’ EP abilities (Robinson et al., 2008; Vaskinnet al., 2007; Derntl et al., 2009; Venn et al., 2004; Bora et al., 2005;Hassel et al., 2008, 2009; Shamay-Tsoory et al., 2009; Mansell andLam, 2006; Almeida et al., 2010; Versace et al., 2010; Lembke andKetter, 2002; Langenecker et al., 2010; Addington and Addington,1998; Bozikas et al., 2006; Kim et al., 2009; Malhi et al., 2007b;Yurgelun-Todd et al., 2000; Harmer et al., 2002a). A literaturereview of facial EP in BD patients in all mood states has also beenundertaken (de Almeida Rocca et al., 2009) which included 32papers published between 1990 and 2008, of which seven studiesmet the criteria of the current literature review.
Results from the facial EP literature show mixed results.Twelve of the nineteen studies report no deficits in EBD patients’facial EP abilities. (Bora et al., 2005) found no significant differ-ence between controls and euthymic bipolar I disorder (EBDI)patients’ performance on an emotion recognition test (Adolphset al., 2002) or Benton Facial Recognition Test (Akdemir et al.,2001). No significant differences in accuracy or reaction timeswere found for EBDI patients and HC ability to match or labelfacial expressions (Robinson et al., 2008). Hassel et al. (2008,2009) found that EBDI patients and HC did not significantly differin correctly labelling facial emotion expressions (sadness, anger,fear, happiness, disgust or neutral expression). Similarly, nosignificant differences were found on the Face Emotion Identifica-tion and Discrimination Test (Kerr and Neale, 1993) by EBD,schizophrenic or HC groups (Vaskinn et al., 2007). Shamay-Tsooryet al. (2009) reported no significant differences between patientsand HC on identification of either basic or social (interested,worried, confident, fantasizing, preoccupied, friendly and suspi-cious) emotions. Highest approval and trust ratings were givenfor positive faces, and negative faces were rated as the leasttrustworthy and given the lowest approval ratings by EBD,unipolar and HC groups (Mansell and Lam, 2006). All participantswere also more likely to take advice from positive faces and lessadvice from negative faces (Mansell and Lam, 2006). Almeidaet al. (2010) utilized an explicit labelling task consisting of mild
L. Mercer, R. Becerra / Journal of Affective Disorders 146 (2013) 295–309300

Author's personal copy
(50% emotional intensity) and intense (100% emotional intensity)happy, sad, fearful and neutral facial expressions. No significantdifferences were found in EBDI patients and HC performanceabilities, and both groups demonstrated a reduced accuracy inlabelling sad expressions. Participants in Versace et al. (2010)completed two event-related fMRI experiments; one displayedintense happy, mild happy and neutral facial expressions, and theother consisted of intense sad, mild sad and neutral facialexpressions. No significant difference in task performance wasfound between EBD patients and HC on either of the emotionallabelling tasks.
Three of the four studies that included both EBDI and euthy-mic bipolar II disorder (EBDII) patients reported no deficits intheir performance (Venn et al., 2004; Lembke and Ketter, 2002;Langenecker et al., 2010). Lembke and Ketter (2002) found thatEBDI and EBDII patients performed comparably to HC on match-ing emotion labels to facial expressions of the six primaryemotions (surprise, happy, fear, sad, anger, disgust; Ekman andFriesen, 1976). EBDII patients displayed better accuracy on fearrecognition than EBDI patients and HC however results were onlysignificant for the EBDI patients. In Venn et al. (2004) patients’recognition of the six primary emotions (Ekman and Friesen,1976) was not impaired. No significant differences on accuracy,response times or errors were found on the Facial EmotionPerception Test or Emotion Perception Test (Langenecker et al.,2010) for patients or HC. It is important to note that two studiesthat included both EBDI and EBDII patients did not conductseparate analyses for each patient group (Venn et al., 2004;Langenecker et al., 2010).
Six studies reported deficits in EBD patients’ facial EP abilities.Addington and Addington (1998) reported no deficits in patients’ability to label emotional faces however deficits in facial affectdiscrimination of the six primary emotions (Ekman and Friesen,1976) was found. Employment of Kinney’s Affect Matching andIdentity Matching Tests (Kinney, 1995; Kinney et al., 1995)required participants to identify and match affective photographsof children’s facial expressions (Bozikas et al., 2006). EBDI patientsperformed comparatively to HC on identity matching howeverpatients performed significantly worse on affect matching(Bozikas et al., 2006). On a virtual reality task whereby partici-pants observed and listened to human avatars give angry, happyor neutral verbal and nonverbal (facial) expressions (Kim et al.,2009), no difference was found between EBDI patients and HCperformance accuracy scores. Patients’ reaction times were sig-nificantly slower across the three experimental (angry, happy orneutral) conditions, and comparable to HC for the neutral avatarcontrol condition. Both groups were significantly faster at com-pleting the happy condition than the angry or neutral conditions(Kim et al., 2009).
Whilst undergoing fMRI, participants completed a facial emo-tion recognition task which included fear, disgust and neutralfacial expressions (Malhi et al., 2007b). EBD patients and HCaccurately identified the presented facial expressions. Patientswere significantly slower to respond to neutral facial expressionsthan HC and they showed a trend difference of slower responsetimes to expressions of fear and disgust. Yurgelun-Todd et al.(2000) fMRI study of fearful and happy facial expressions revealedthat EBD patients and HC correctly identified happy facialexpressions, however only 71.4% of patients correctly identifiedexpressions of fear. It was not reported whether the two groupsresponses to fearful facial expression were significantly differentor not. No gender differences were found for patients whoincorrectly identified fearful stimuli.
Out-patients diagnosed with EBDI or EBDII and matched HCcompleted a facial emotion recognition task in Derntl et al.(2009). EBDII patients and HC correctly identified the emotional
facial expressions. In contrast, EBDI patients showed significantlyworse performance in labelling emotional expressions comparedto HC. EBDI patients incorrectly identified sad expressions asfearful expressions. No significant gender differences were foundwithin the groups.
Two studies reported enhanced abilities in EBD patients’ facialEP (Lembke and Ketter, 2002; Harmer et al., 2002a). EBDIIpatients displayed better fear recognition than EBDI patientsand HC though results were only significant between the patientgroups (Lembke and Ketter, 2002). EBD patients also demon-strated facilitated recognition of disgust which was significantlydifferent to HC for facial expressions featuring 70–100% levels ofdisgust (Harmer et al., 2002a). Patients made significantly fewererrors at labelling other facial expressions as disgust (Harmeret al., 2002a).
In summary, results from the facial EP literature providesvaried results with twelve studies reporting no deficits, sixstudies finding EP deficits and two studies having found enhancedfacial emotion recognition abilities by EBD patients. These resultsleave an overall impression that EP deficits exist in EBD patientswhen processing facial expressions.
3.4. Mood induction
Another method by which EP has been examined is byinducing positive or negative moods implicitly (unbeknown tothe participant) and investigating the effect this has on patients’EP abilities (Roiser et al., 2009). Three studies have examinedmood induction in EBD patients (Mansell and Lam, 2006; Roiseret al., 2009; Farmer et al., 2006).
Roiser et al. (2009) results are indicative of a qualitativedifference between EBD patients and HC response to positivemood induction. Following mood induction both groups displayedequivalent increases in mood however EBD patients displayed aslower decision making process on the Cambridge Gamble Task(CGT; Rogers et al., 1999). Patients’ reaction times increasedparticularly when more difficult decisions had to be made onthe CGT (Rogers et al., 1999). On the affective go/no-go task, EBDpatients made significantly more commission errors during ‘sad’target blocks than ‘happy’ blocks, thus patients displayed a biastowards positive words having made more inappropriateresponses to positive distracters than negative ones (Roiseret al., 2009). Such bias was not demonstrated by HC.
Significantly more negative adjectives were endorsed by EBDpatients to be true about themselves than HC before and afterFarmer et al. (2006) mood induction task. Following positivemood induction, participants indicated being happier; no differ-ence was found for endorsement of positive adjectives whilstendorsements of negative adjectives were reduced. EBD patientsand HC were faster and more accurate at completing the Global-Local processing task (Witkin et al., 1971) following moodinduction (Farmer et al., 2006).
After high mood induction, EBD patients in Mansell and Lam(2006) study were found to use less advice than controls. Similarresults were not found following low mood induction. Patientsand HC took more advice from positive faces than negative ones.No effect of mood was found for participants’ ratings of the levelof approval or trustworthiness of faces. Correlational analysisrevealed that larger increases in mood were negatively associatedwith use of advice for EBD patients and no association was foundfor HC (Mansell and Lam, 2006).
Overall, results from the mood induction literature examiningEP in EBD patients suggest differences between EBD patients andHC processing of emotional material following mood inductiontasks.
L. Mercer, R. Becerra / Journal of Affective Disorders 146 (2013) 295–309 301

Author's personal copy
3.5. Auditory processing
3.5.1. Prosody
Affective prosody is the nonlexical component of speech whichindicates the emotional state of others (Bozikas et al., 2007). Onestudy has examined affective prosody in EBD patients wherebyemotionally neutral audiorecorded sentences were presentedwith one of the five (happiness, sadness, surprise, fear and anger)emotional prosodic intonation or neutral intonation i.e. ‘‘Today isWednesday’’ expressed in an angry voice (Bozikas et al., 2007).Results indicated that EBD patients were found to be less accurateat identifying expressions of emotion through intonation than HC.A significant main effect for emotion categories was found withboth groups displaying similar rank orders of the emotions theyfound easy and difficult to identify. For patients, the rank orderfrom easiest to hardest emotion to identify was; neutral, happy,surprise, anger, fear and sadness. For HC, the rank order was;neutral, happy, fear, surprise and anger/sadness. Female EBDpatients performed significantly worse than healthy females onidentification of fear and surprise. Male patients performedcomparatively to male HC (Bozikas et al., 2007).
3.5.2. Criticism
It has been suggested that criticism may evoke more emotiondue to being more personally engaging and interpersonal innature than other static forms (i.e. pictures) employed to assessEP (Butzlaff and Hooley, 1998). Consequently, one study (Cuellaret al., 2009) delivered a standardized criticism analogue toexamine participants’ reaction and recovery. Participants weretold they were partaking in an experiment which was examininghow people provide and receive emotional support. Participantswere asked to describe a difficulty they had experienced.A confederate would interrupt the participant two minutes intotheir description to provide the standardized criticism analogue‘‘I see this is a difficult situation for you, but I think you’reoverreacting. Maybe you need to focus on what you’ve have doneto help create this problemy’’(p. 929, Cuellar et al., 2009). EBDpatients reported higher levels of negative affect than HC prior toexposure to criticism. A trend difference (po0.08) was foundwith patients indicating greater negative affect in reaction tocriticism than HC. Predictors of reactivity to criticism for patientsincluded interpreting the criticism as more critical, being female,having more familial support and receiving disability payments(Cuellar et al., 2009).
3.5.3. Emotional sentences
Responses to emotionally salient and non-salient interviewquestions were examined to determine whether the presence ofemotional content impacts on BD patients’ thought and commu-nication abilities (Tai et al., 2004). Questions such as ‘‘Tell meabout any big arguments you had in your family’’ or ‘‘Tell meabout the things you regret most in your life?’’ are examples ofemotionally salient questions, whereas ‘‘Tell me about any hob-bies you have’’ is an example of a non-salient question (Tai et al.,2004). Higher levels of thought and communication disorder inthe emotionally salient condition was found in comparison to thenon-emotional condition for manic, EBD patients and HC. Manicpatients displayed the largest amount of thought disorder whilstHC demonstrated the least. EBD patients displayed a significantincrease in thought disorder in the emotional compared to non-emotional condition, whilst depressed patients and HC did not(Tai et al., 2004).
Vaskinn et al. (2007) examined visual (facial expressions) andauditory (sentence) emotion perception in EBD and schizophrenicpopulations. The auditory emotion perception identification task
required participants to identify what emotion was being verballyexpressed, while the discrimination task required participants todistinguish whether to verbalised sentences expressed the sameemotion or not. EBD patients did not display visual or auditoryemotion perception deficits. A non-significant gender differencewas observed; female EBD patients were less accurate than maleEBD patients on the facial and auditory emotion identification anddiscrimination tasks. This observed pattern deviated from theschizophrenic and HC performance, with females outperformingtheir male comparisons on both the auditory emotion tasks andvisual identification task, albeit this difference was not significant(Vaskinn et al., 2007).
Examining the results of the above studies, Tai et al. (2004)provide support for the existence of auditory EP deficits EBDpatients, whilst Vaskinn et al. (2007) results contradict suchdeficits having found no deficits displayed in patients abilityto identify and discriminate emotional auditory (and visual)material.
3.6. Theory of mind
ToM is defined as the ability to recognize the feelings, inten-tions and motivations of others (Premack and Woodruff, 1978).ToM can be divided into cognitive and affective components.Cognitive ToM refers to the ability to adopt another’s point ofview or make inferences about their beliefs, while affective ToMrefers to the ability to make inferences about other’s emotions(Shamay-Tsoory et al., 2009). It is the affective component of ToMthat is of interest in the present review.
All three studies that examined affective ToM in EBD patientsreported affective ToM deficits in EBD patients (Bora et al., 2005;Shamay-Tsoory et al., 2009; Montag et al., 2010). Significantdifferences in patients and HC performance for cognitive andaffective was found by Shamay-Tsoory et al. (2009). EBD patientsscored significantly higher on the affective scale (personal distressscale) of the Interpersonal Reactive Index (Davis, 1980) but not onthe perspective taking, fantasy or empathetic concern subscales.No significant differences for recognition of affective faux pas(appreciation of the emotional impact that a statement may haveon an individual) was reported (Shamay-Tsoory et al., 2009).
EBD patients displayed mindreading difficulties as evaluatedby the Movie for Assessment of Social Cognition (MASC; Dziobeket al., 2006; Montag et al., 2010), a video-based test of subtlemindreading difficulties. However, patients’ performance wascomparable to HC on emotional mental state reasoning (Montaget al., 2010). Bora et al. (2005) found no significant differencebetween EBD and HC groups on face or gender recognition on theEyes Test (Baron-Cohen et al., 1997). However, patients per-formed significantly worse on social emotion recognition andToM task.
3.7. Other
One study examined reward responsivity in BD patients invarious mood states (euthymic, depressed and manic/hypomanicor mixed state) (Van der Gucht et al., 2009). Reward responsivitywas measured by the amount participants increased their speedon each trial of Card Arranging Reward Responsivity ObjectiveTest (CARROT; Powell et al., 1996) with monetary rewardsreceived for their increase in speed. No significant differenceswere found for participants’ attributional styles as measured byinternality scores for positive or negative events on the PragmaticInference Task (Winters and Neale, 1985).
Similarly, no differences were found on the speed participantscompleted the CARROT (Powell et al., 1996). All three BD patientgroups reported more rumination when in a negative mood state
L. Mercer, R. Becerra / Journal of Affective Disorders 146 (2013) 295–309302

Author's personal copy
than HC as assessed by the modified Response Style Question-naire (Knowles et al., 2005).
4. Discussion
Review of the existing literature indicates that some BDpatients do retain their EP deficits during euthymia. Overall,22 out of 34 studies reviewed reported some form of EP deficitsdisplayed by EBD patients. With evidence for and against thepresence of EP deficits in EBD patients it is important to addresswhy such discrepancies exist and what clinical implications thishas for treatment of EBD patients.
4.1. Facial emotion recognition
Examination of the facial EP literature provides mixed resultswith twelve studies reporting no deficits, six finding deficits andtwo studies reporting enhanced facial emotion recognition abil-ities by EBD patients. The remission criteria applied by three ofthe six studies that reported facial EP deficits is questionable andlikely to contribute to discrepancies found. Derntl et al. (2009)applied a liberal remission criterion. Two studies did not applyspecific remission criteria and also did not classify patients’ typeof BD diagnosis (Addington and Addington, 1998; Yurgelun-Toddet al., 2000). Results may also be confounded by the presence ofmanic and depressive symptomatology with one study failing toapply any formal assessment of patients’ symptoms (Addingtonand Addington, 1998), another study showed a large distributionof scores across Hamilton Rating Scale for Depression (HAM-D;Hamilton, 1960) and Young Mania Rating Scale (YMRS; Younget al., 1978), and patients obtained high scores on both theaforementioned measures (Yurgelun-Todd et al., 2000). In addi-tion, the generalisation of Bozikas et al. (2006) findings arelimited as they utilised photographs of children’s facial expres-sions, caution must be taken when comparing these findings toother studies that employed adult facial stimuli.
Across the studies which reported no facial EP deficits,a greater variety of measures were employed to assess sympto-matology and remission criteria applied was generally moreliberal than the literature supporting EP deficits. These findingswere unexpected as it appears more logical that studies thatapply liberal remission criterion would have their results con-founded by undetected mania and depression symptomatologyand consequently their results would reflect similar deficitsdisplayed by manic and depressed BD patients.
Three of the four studies which included both EBDI and EBDIIpatients reported no deficits in patients’ perception of facialemotions (Derntl et al., 2009; Lembke and Ketter, 2002;Langenecker et al., 2010). Only two studies separated EBDI andEBDII patients into separate groups when conducting their ana-lysis and of these only one study reported EP deficits (EBDIpatients only) (Derntl et al., 2009). Twice as many EBDII thanEBDI patients reported taking anti-depressant medication whichthe authors argued may have resulted in a positive influence onEBDII patients’ performance (Derntl et al., 2009). Lembke andKetter (2002) found that EBDI and EBDII patients performedcomparatively to HC however they did not report participants’demographic information or medication status making it difficultto disentangle potential reasons for discrepancies found.
Overall, studies that reported no EP deficits included slightlyolder EBD patients than those that reported deficits (see Table 1).EBD patients who displayed facial emotion deficits were older atage of onset of BD and showed shorter mean illness durations.These finding are based on a limited number of studies thatreported age of illness onset or illness duration. Although these
findings are contradictory to our expectations, patients’ denial orlack of awareness of their disorder may have resulted in laterdiagnosis and thus greater deficits due to delayed treatment.Further investigation is needed to clarify these findings.
The ability to accurately identify facial emotion requires theextraction of visuospatial and figural information, attention,concentration, memory and labelling of the emotional expression(Morrison et al., 1988). Consequently integration of cognitive andemotional processes are required to successfully complete such atask (Yurgelun-Todd et al., 2000). Due to this complex process it isdifficult to discern at a behavioural level whether a disruption inthe affective or cognitive processing system results in incorrectfacial affect labelling. Consequently, researchers have turned theirattention to examining EP at a neural level to help gain moreclarity on this matter. Findings from a fMRI study suggest thatEBD patients may differ to HC in their EP abilities at a neural butnot a behavioural level (Wessa et al., 2007).
4.2. Mood induction
The literature shows that induction of positive mood statesimpacts on EBD patients’ EP abilities. Following positive moodinduction, EBD patients displayed a positive emotional bias andslower decision making processes than HC (Roiser et al., 2009).In Farmer et al. (2006), HC and EBD patients responded similarly topositive mood induction; both reporting to be happier, endorsingless negative adjectives about themselves, enhanced accuracy andfaster response times.
Manic BD patients have displayed mood-congruent positivebiases, such that manic patients demonstrate a preference forpositive stimuli which is consistent with their current heightenedemotional state (Lembke and Ketter, 2002; Murphy et al., 1999).Roiser et al. (2009) findings support the argument that positivemood induction biases EBD patients towards positive emotionalstimuli. Farmer et al. (2006) findings give inconclusive support tosuch argument. Although patients endorsed more positive adjec-tives than controls following mood induction they also endorsedsignificantly more negative adjectives to be true about them-selves prior to and following positive mood induction (Farmeret al., 2006). These results taken together do not provide convin-cing evidence to support or disprove that inducing a positivemood state result in a mood-congruent positive bias in EBDpatients. Questions are also raised about what impact negativemood induction would have on EBD patients’ EP abilities.
One study included positive and negative mood induction withEBD patients (Mansell and Lam, 2006). Contrary to HC, EBDpatients were less likely to take advice from others when in ahigh mood but not in a low mood state (Mansell and Lam, 2006).These findings postulate that in a high mood state EBD patientsuse less feedback from others and are less likely to modify theirbehaviour according to the social context. Participants were alsomore likely to take advice from positive faces and less likely totrust a person displaying a negative facial expression (Manselland Lam, 2006).
Results from the mood induction studies must be interpretedwith caution as they employed different tasks to assess EP,included only EBDI patients and lacked strict remission criteria.Significantly higher depression scores were obtained by EBDpatients than HC in two of the studies (Roiser et al., 2009;Farmer et al., 2006), whilst the third study applied lenientdepression symptomatology criteria (Mansell and Lam, 2006).EBD patients’ depression scores increased from one week prior totesting to the day of testing (Farmer et al., 2006) which mayindicate patients were becoming increasingly depressed. EBDpatients also reported higher mania scores than HC in Manselland Lam (2006). Overall, results from mood induction studies
L. Mercer, R. Becerra / Journal of Affective Disorders 146 (2013) 295–309 303

Author's personal copy
provide preliminary evidence to suggest that EBD patients mayhave a differential pattern of responding when in different moodstates but does not provide categorical assurance as to whether amood-congruent bias exists in EBD patients.
4.3. Affective attention
Examination of EBD patients’ performance on emotionalStroop tasks provides mixed results regarding EBD patients’ability to inhibit attention biases to emotional stimuli. One study(Kerr et al., 2005) found that EBD patients were slower than HC intheir reaction times across positive and negative conditions,whilst two studies found that EBD patients’ reaction times whenexposed to emotional stimuli were slower than HC but thedifference was not significant (Lex et al., 2008; Malhi et al.,2005). Obtainment of longer response latencies is suggestive thatthe presence of emotional stimuli has interfered with patients’information processing abilities thus reducing their performancespeed (Compton et al., 2003). However, EBD patients were alsoslower than HC on the neutral non-emotional condition (Lexet al., 2008; Kerr et al., 2005). This raises the question as towhether the processing of emotional material did impede EBDpatients’ performance or whether their reduced speed of proces-sing for emotional and non-emotional stimulus can be explainedby more global cognitive weaknesses.
Emotional Stroop tasks are known to engage executive func-tioning abilities (Malhi et al., 2005). Thus, deficits in EBD patients’executive functioning may account for their compromised per-formance rather than EP difficulties. Kerr and colleagues (2005)inclusion of a card Stroop task indicated that EBD patientsdisplayed attention impairments which could not be accountedfor by the presence of emotional stimuli. Consequently, the onlystudy which found a significant difference between patients andHC speed of performance also reported attention deficits in EBDpatients which could not be attributed to the presence of emo-tional stimuli. Based on these findings EBD patients have not beenconclusively found to display attention biases to emotionalstimuli using emotional Stroop tasks. This area of research wouldbenefit from controlling for other potential confounds such ascognitive dysfunction. Unfortunately the research available onneuropsychological functioning in BD and EBD tends to assesscognitive functioning without including EP as a controlledvariable.
Results from two of the three studies that employed go/no-goand dot probe tasks indicate EBD patients’ abilities are compro-mised (Jongen et al., 2007; Gopin et al., 2011). Compared to HC,patients showed reduced accuracy rates and slower reactiontimes (with the exception being for negative stimuli wherebypatients performed as well as HC Gopin et al., 2011). Both studiesreported that EBD patients displayed a bias towards negativestimuli (Jongen et al., 2007; Gopin et al., 2011) and away frompositive emotional stimuli (Jongen et al., 2007).
Wessa et al. (2007) found at a behavioural level EBD patientsperformed similarly to HC on a go/no-go exercise of emotionalfaces. However, patients activated different neural substrates toHC. These findings are suggestive of different neural processing inEBD patients to facial emotional stimuli that go undetected on ago/no-go task. The authors proposed that emotion recognition,response inhibition and selective attention are mediated by anoveractivation of brain structures (Wessa et al., 2007). Otherstudies support the suggestion that EBD patients can preservetheir behavioural performance by overactivation at a neural level(Chang et al., 2004; Strakowski et al., 2005). More sensitivebehavioural measures such as film clips or real life exposuremay have allowed for a behavioural expression of neural proces-sing differences.
4.4. Auditory processing
Not being able to effectively identify auditory expressions ofemotions has been linked to impaired communication, interper-sonal and occupational difficulties in schizophrenic patients(Hooker and Park, 2002; Mueser et al., 1996; Poole et al., 2000).With high rates of psychosocial difficulties also reported in EBDpatients (Dickerson et al., 2001; Abbod, Sharkey, Webb, Kelly, &Gill, 2002) it is important to conclusively determine whether EBDpatients’ identification of auditory EP is impaired as this wouldhave important implications for treatment focus.
Two of the four auditory affective studies have demonstrateddeficits in EBD patients’ abilities to process emotional material.EBD patients indicated vuneraliblity to communication, languageand thought difficulties when discussing emotional topics (Taiet al., 2004) and they demonstrated difficulties with identificationof emotion through intonation (Bozikas et al., 2007). In contrast,EBD patients displayed intact auditory emotion perception(Vaskinn et al., 2007) and their reaction to criticism did not differfrom HC (Cuellar et al., 2009).
Possible reasons for conflicting results include; a variety ofmeasurement tools and remission criterion applied to assesssymptomatology, and application of different tasks used acrossthe studies. Alike manic patients, EBD patients showed increasedthought disorder when discussing emotional topics, thus con-cerns are raised about whether patients were euthymic at thetime of testing (Tai et al., 2004). Without relevant informationpertaining to depression and mania symptomatology reported, itis impossible to clarify whether this confounded results (Tai et al.,2004).
4.5. Memory
Four of the five studies examining emotional memory reportedcomparable performance between EBD patients and HC (Lex et al.,2008; Derntl et al., 2009; Malhi et al., 2007a; Van der Gucht et al.,2009). In contrast, Kauer-Sant’Anna et al. (2008) found thatpatients recalled significantly less emotional material and ratedneutral stimuli as having a greater emotional impact than HC.These differences may be explained by the complexity of the tasksemployed with EBD patients performing as well as HC on basicmemory tasks (Lex et al., 2008; Derntl et al., 2009; Malhi et al.,2007a; Van der Gucht et al., 2009), but performing worse thancontrols when the emotional stimuli was embedded in a story.The emotional story may have closely simulated the difficultiesthat EBD patients experience in everyday life (Kauer-Sant’Annaet al., 2008); namely impaired social skills (Vaskinn et al., 2007)and facial emotion recognition difficulties (Addington andAddington, 1998). The authors proposed that patients may haverated neutral stimuli as having a greater emotional impactbecause they may have an ‘‘oversensitive emotional reaction tofacts’’ (Kauer-Sant’Anna et al., 2008, p. 461). Based on the abovefindings it was concluded that EBD patients do not displayemotional memory deficits however further research is neededto examine EBD patients’ performance in complex situations.
4.6. Theory of mind
Results from ToM studies support an altered pattern ofcognitive functioning in EBD patients and give partial support tothe presence of some affective ToM impairment in EBD popula-tions. While EBD patients in Bora et al. (2005) demonstratedimpairment on cognitive and affective ToM, patients in Montaget al. (2010) only displayed impairment on cognitive ToM proces-sing. Shamay-Tsoory et al. (2009) reported a significant differencebetween HC and EBD patients’ performance on the affective and
L. Mercer, R. Becerra / Journal of Affective Disorders 146 (2013) 295–309304

Author's personal copy
cognitive ToM tasks. It would be beneficial to determine whetherEBD patients continue to display affective ToM deficits aftercognitive ToM scores are controlled for.
4.7. Methodological issues
It is assumed that diminished or reduced symptoms overa defined period of time equates to being euthymic (Malhi et al.,2005). Thus, a measurement tool and rating scale cut-off score areusually applied in the studies reviewed to determine euthymia.Examination of the literature indicates that measures used andscale rating cut-off criteria vary substantially across the literature.Four different measures were utilised across the studies to mea-sure mania symptomatology; YMRS (Young et al., 1978 n¼22),Mania Rating Scale (Bech et al., 1978; n¼5), Clinician AdministeredRating Scale for Mania (Altman et al., 1994; n¼1) and AltmanSelf-Rating Mania Scale (Altman et al., 1997; n¼1). Four differentmeasures were employed to measure depression symptomatology;HAM-D (Hamilton, 1960; n¼22), Beck Depression Inventory (Becket al., 1961; n¼4) and Montgomery Asberg Depression Rating Scale(Montgomery and Asberg, 1979; n¼3) and Inventory of DepressiveSymptomatology (Rush et al., 1996; n¼1). Variation in rating scalecut-off scores ranged from five to fourteen across the studies thatemployed HAM-D Hamilton (1960) and six to twelve for YMRS(Young et al., 1978). The largest remission criterion variation wasfound in studies that employed the Beck Depression Inventory(Beck et al., 1961) where scores ranged from seven to sixteen.
The lack of a standardised measure to determine euthymia hassignificant implications for existing research findings. If a studyapplies strict remission criteria and reports the presence ofemotional deficits (i.e. Malhi et al., 2005) then this providesstrong support for the existence of such deficits with resultsbeing less likely to be confounded by the presence of mania ordepression symptomatology. Studies that have applied moreliberal remission criteria need to consider that EBD patientsmay display deficits which pertain to existing symptomatology(i.e. Gopin et al., 2011; Derntl et al., 2009). If rating scale cut-offsare a true indicator of euthymia then the measures used and cut-offs applied are vital. Consequently, it is imperative that agree-ment upon the standardised measures for euthymia (one mea-surement tool for depression and one for mania symptomatology)and rating scale cut-offs are established. In the absence ofcategorical psychometric reasons and based on convention, it isrecommended that future studies adopt the YMRS (Young et al.,1978) and HAM-D (Hamilton, 1960) as acceptable respectivemeasures of mania and depression symptomatology and applythe respective rating scale cut-off scores of equal to or beloweight and seven to determine euthymia.
Assessment of manic and depressive symptomatology is stan-dard procedure in BD studies. However, it is less common toassess patients’ emotional state (i.e. happy, anxious etc.) at timeof testing. Patients’ current emotional state could arguably impacton their test performance and particularly their ability to processemotional material. Mood induction studies have demonstratedsome evidence to suggest that the current mood state of anindividual can impact on their performance (i.e. Roiser et al.,2009). Of the limited studies that have examined EBD patients’emotional states, the majority fail to examine how such stateimpacts on their EP performance (Wessa et al., 2007; Van derGucht et al., 2009; Cuellar et al., 2009). Such investigation wouldilluminate the uncertainties about the impact patients’ emotionalstate has on their EP abilities.
As BDI and BDII are categorically different (Summers et al.,2006) it is important to examine whether the EP abilities of bothpatient groups differ. The majority of the studies included EBDIpatients only and seven did not classify patients BD diagnosis.
Only two (Derntl et al., 2009; Lembke and Ketter, 2002) of the sixstudies that included EBDI and EBDII patients (Wessa et al., 2007;Kauer-Sant’Anna et al., 2008; Venn et al., 2004; Langenecker et al.,2010) conducted separate analysis for these patients. Derntl et al.(2009) found no significant difference between EBDI and EBDIIpatients’ ability to recognize facially expressed emotions. Lembkeand Ketter (2002) found that EBDI and EBDII patients’ facialemotion recognition skills were comparable across the primaryemotions (Ekman and Friesen, 1976). However, EBDII patientsdisplayed significantly better recognition of fear than EBDIpatients. Based on these findings one may be guided to concludethat EBDI and EBDII patients do not appear to differ greatly intheir EP abilities. However, a limited number of studies haveexamined potential differences between EBDI and EBDII patients’EP abilities and these studies have only employed facial emotionrecognition tasks. To gain a more comprehensive picture ofpatients’ EP abilities, EBDI and EBDII patients’ performance needsto be compared in other EP modalities.
Two (Bozikas et al., 2007; Cuellar et al., 2009) of the six studies(Vaskinn et al., 2007; Derntl et al., 2009; Addington andAddington, 1998; Yurgelun-Todd et al., 2000) that have examinedpotential gender differences support differential EP profiles formale and female EBD patients. Female patients were found to bemore reactive to criticism than their male counterparts (Cuellaret al., 2009). Male patients performed as well as male HC inidentification of the six primary emotional expressions (Ekmanand Friesen, 1976), whereas female patients displayed deficits intheir identification of fear and surprise compared to female HC(Bozikas et al., 2007). Vaskinn et al. (2007) examination of facialand auditory emotion recognition revealed no gender differencesin EBD patients and no gender difference were found on twostudies of facial affect recognition (Derntl et al., 2009; Addingtonand Addington, 1998; Yurgelun-Todd et al., 2000). Evidentlyfurther investigation is needed to qualify whether gender differ-ences exist in EBD patients’ EP abilities.
The existing literature suggests that EBD patients displayspecific deficits to negative valence emotions with 13 studiesrevealing that patients displayed differential responding to HC onnegative emotional stimuli (Kerr et al., 2005; Jongen et al., 2007;Malhi et al., 2005; Gopin et al., 2011; Malhi et al., 2007a; Derntlet al., 2009; Almeida et al., 2010; Lembke and Ketter, 2002;Bozikas et al., 2006; Yurgelun-Todd et al., 2000; Harmer et al.,2002a; Roiser et al., 2009; Farmer et al., 2006). Two studiesreported EBD patients displayed a response bias to negativeemotions with patients appearing to be more engaged and willingto respond to negative stimuli (Jongen et al., 2007; Gopin et al.,2011) whilst showing reduced accuracy (Gopin et al., 2011) and abias away from positive words (Jongen et al., 2007). Patients ratednegative words as significantly more negative than HC on anemotional Stroop (Malhi et al., 2005) and memory task (Malhiet al., 2007a) and were found to endorse more negative adjectives(Farmer et al., 2006). Patients also performed significantly sloweron the negative condition of an emotional Stroop task (Kerr et al.,2005).
There is also evidence to indicate that EBD patients displayspecific EP deficits for fear and sad emotional stimuli. Female EBDpatients performed worse on fear recognition from emotionalintonation (Bozikas et al., 2007). EBDI patients were found tomistake sad faces for fearful expressions (Derntl et al., 2009) andpatients were less accurate on identification of fearful facialexpressions (Yurgelun-Todd et al., 2000). Patients made moreerrors on the sad target blocks of a go/no-go task (Roiser et al.,2009) and demonstrated reduced accuracy in labelling sad facialexpressions (Almeida et al., 2010). Contrary to these findings,EBDII patients displayed better fear recognition than EBDI and HCon a facial emotion recognition task (results were only significant
L. Mercer, R. Becerra / Journal of Affective Disorders 146 (2013) 295–309 305

Author's personal copy
between patient groups) (Lembke and Ketter, 2002). EBD patientsalso displayed facilitated recognition of disgust compared to HC(Harmer et al., 2002a).
Five studies reported differential responding between EBDpatients and HC to positive valence stimuli (Bozikas et al., 2007;Kerr et al., 2005; Jongen et al., 2007; Gopin et al., 2011; Versaceet al., 2010). The types of deficits EBD patients displayed topositive stimuli included slower response times on an emotionalStroop task (Kerr et al., 2005), reduced performance for thepositive affective condition of a go/no-go task (Gopin et al.,2011), and reduced accuracy on identification of surprise byintonation (Bozikas et al., 2007) and intense happy facial expres-sions (Versace et al., 2010). EBD patients moved their attentionaway from positive words while HC directed their attentiontowards positive stimuli (Jongen et al., 2007).
Overall the results indicate that EBD patients displayed greaterdifficulty with negative EP, specifically identification of fear andsadness. Researchers commonly employ Ekman and Friesen(1976) primary emotions which consist of two positive emotions(happy and surprise) and four negative emotions (sad, fear,disgust, and anger). Thus, EBD patients greater differentialresponding to negative emotions due to the larger set of negativeemotions included in researchers’ analysis. Future studies wouldbenefit from including equal amounts of positive and negativeemotions to clarify whether valence and emotion specific deficitexists in EBD populations.
Medication is the treatment of choice for BD and for the largemajority of patients adherence to a medication regime will berequired to achieve euthymia (Frangou et al., 2005). It was out ofthe scope of this review to make sense of the impact that differentmedications had on research findings. It is plausible that phar-macological treatment impacts on EBD patients’ abilities toprocess emotional material. It has been suggested that medicationmay be accountable for the observed blunting effects in EBDpatients’ physiological response to emotionally salient material(Kauer-Sant’Anna et al., 2008). Impaired neurocognition has beenassociated with antipsychotic medication in BD patients (Blairand Curran, 1999). Administration of medication in healthyparticipants has been shown to impact on their performance onemotional tasks including recognition of anger (Harmer et al.,2002b) and negative expressions (Harmer et al., 2001) andshowed longer reaction times for identification of sad expressions(Lawrence et al., 2004). In contrast, antidepressant medicationand lithium have been linked to normalising affective disorderpatients’ neural responses to fearful, sad and happy faces(Bhagwagar et al., 2004; Miklowitz, 2006). Thus, it is plausiblethat pharmacological treatments are associated with changes inEBD patients’ performance and EP capabilities. Further investiga-tion is needed to discriminate the specifics of such influence onpatients’ performance. One common problem in the literature isthe inclusion of small sample sizes which impedes analysis of theeffects of medication status on task performance. The currentliterature would benefit from examination of EP in BD popula-tions before and after medication.
4.8. Limitations and recommendations
A number of limitations were observed across the majority ofthe articles. Small sample sizes were generally included whichreduces the power of the studies and generalisation of conclu-sions drawn. All but one study (Langenecker et al., 2010) werecross-sectional in nature. The majority of the studies did notinclude a psychiatric control group for comparison and conse-quently the reported weaknesses cannot be confirmed to bespecific to BD as they might also be present in psychopathologyin general. The inclusion of other psychiatric diagnoses would
help clarify whether these weaknesses in EP are specific to BDor not.
An important factor that has not been examined in thereviewed literature is the potential influence that static (e.g.,photographs) versus dynamic (e.g., video-based, real-life interac-tion) presentations of emotional stimuli have on patients’ EPabilities. Such analysis may reveal that EBD patients’ performanceis better on static (more basic) presentations of emotional stimulithan complex interactions (dynamic), or perhaps exposure tomore dynamic everyday interactions that are richer in detailresult in patients being more accurate on dynamic presentationsof emotional stimuli. Preliminary evidence suggests that BDpatients’ EP abilities may be influenced by the format in whichstimuli is presented (Mansell and Lam, 2006).
From a clinical point of view the findings of the current reviewencourage the authors to postulate recommendations for theclinician. However, it is important to note that such recommen-dations are based on trends observed and that further research isrequired to draw more conclusive findings and thus clinicalrecommendations. Acknowledgement that EBD patients may bevulnerable to thought, language and communication difficultieswhen discussing emotional topics (Tai et al., 2004) may helpincrease patients’ awareness of their EP deficits, allowing them toadjust and accommodate for such difficulties. Time spent onassisting the client to become more familiar with various emo-tional presentations is likely to increase their identification anddiscrimination accuracy of emotional expressions thus potentiallyimproving their social interactions and more importantly dimin-ishing relapses by promoting better preparation in coping withtriggering factors. Facilitating clients to be aware of potentialmood-specific biases is likely to result in them having betterinsight and capable of engaging in better decision makingprocesses. Therapeutic time can also be dedicated to reducingEBD patients’ potential difficulty with negative stimuli. CognitiveBehaviour Therapy (CBT), as adjunct therapy to psychopharma-cology, has been found to improve outcomes (120). We postulatethat psychological therapy like CBT, or any other psychologicalapproach, would be more effective when dealing with EBD if thispopulations’ EP were to be considered. This postulate warrantstesting in rigorous clinical trials.
In conclusion, the issue of EP in BD during remission remains acomplex phenomenon. The current literature indicates that EBDpatients do display EP deficits within the areas of attention(slower response times, bias towards negative words and awayfrom positive words and reduced accuracy for positive stimuli)facial emotion recognition (affect matching, emotion recognitionand slower response times), auditory processing (higher levels ofthought disorder displayed in the emotional condition and pooreremotion recognition skills) and ToM (poorer performance andhigher personal distress scores). Following mood induction, EBDpatients displayed slower reaction times, made more errors in thesad target condition and took less advice from others after highmood induction. There is also evidence to show that EBD patientsdisplay specific deficits to negative valence emotions and to alesser degree positive valence emotions. The area of EP researchthat provided that most conclusive findings by way of mostagreement amongst studies was emotional memory. Four of thefive studies did not find EBD patients’ to display any deficits intheir memory for emotional material (Kauer-Sant’Anna et al.,2008).
The main conclusion of the current literature review is thatfurther investigation within this area of research is needed toelucidate whether a unique EP profile in EBD patients exists. Oneinterpretation of the current findings observed is that perhaps aunique EP profile for EBD patients does not exist. However, giventhe serious methodological irregularities that characterise this
L. Mercer, R. Becerra / Journal of Affective Disorders 146 (2013) 295–309306

Author's personal copy
research arena, it is recommended that more research with morerigorous methodology is conducted. In particular, research in thisarea needs to; utilise more precise inclusion criteria to determineremission, differentiate between BDI and BDII diagnosis, assesspotential gender differences, include not only affective stimuli butmake explicit the valence and type of affective phenomena,control for type and amount of medication of subjects and assessthe participants’ mood at the time of assessment. The presentreview has highlighted the areas in need of improvement to beable to generate a clear EP profile of this population.
Role of funding sourceNothing declared.
Conflict of interestThe authors of this paper do not have any commercial associations that might
pose a conflict of interest in connection with this manuscript.
AcknowledgementsThe authors would like to thank Dr Elizabeth Kaczmarek and Dr Craig Harms
for their helpful comments.
References
Abbod, Z., Sharkey, A., Webb, M., Kelly, A., Gill, M., 2002. Are patients with bipolaraffective disorder socially disadvantaged? A comparison with a control group.Bipolar Disorder 2, 243–248.
Addington, J., Addington, D., 1998. Facial affect recognition and informationprocessing in schizophrenia and bipolar disorder. Schizophrenia Research 32,171–181.
Adolphs, R., Baron-Cohen, S., Tranel, D., 2002. Impaired recognition of socialemotions following amygdale damage. Journal of Cognitive Neuroscience 14,1264–1274.
Akdemir, A., Turkcapar, M.H., Orsel, S.D., Demirergi, N., Dag, I., Ozbay, M.H., 2001.Reliability and validity of the Turkish version of Hamilton depression ratingscale. Comprehensive Psychiatry 42, 161–165.
Almeida, J.R.C., Versace, A., Hassel, S., Kupfer, D.J., Phillips, M.L., 2010. Elevatedamygdala activity to sad facial expressions: a state marker of bipolar but notunipolar depression. Society of Biological Psychiatry 67, 414–421.
Altman, E.G., Hedeker, D.R., Janicak, P.G., Peterson, J.L., Davis, J.M., 1994. Theclinician-administered rating scale for mania (CARS-M); Development, relia-bility and validity. Biological Psychiatry 36, 24–134.
Altman, E.G., Hedeker, D.R., Peterson, J.L., Davis, J.M., 1997. The Altman self-ratingmania scale. Biological Psychiatry 42, 948–955.
American Psychiatric Association, 2000. Diagnostic and Statistical Manual ofMental Disorders-IV-Text Revision, 4th ed APA, Washington, DC.
Baron-Cohen, S., Jolliffe, T., Mortimore, C., Robertson, M., 1997. Another advancedtest of theory of mind: evidence from very high functioning adults with autismor asperger syndrome. Journal of Child Psychological Psychiatry 38, 813–822.
Bech, P., Rafaelsen, O.J., Kramp, P., Bolwig, T.G., 1978. The mania rating scale: scaleconstruct and inter-observer agreement. Neuropharmacology 17, 430–431.
Beck, A.T., Ward, C.H., Mendelson, M., Mock, J., Erbaugh, J., 1961. An inventory formeasuring depression. Archives of General Psychiatry 41, 53–63.
Bhagwagar, Z., Cowen, P.J., Goodwin, G.M., Harmer, C.J., 2004. Normalisation ofenhanced fear recognition by acute SSRI treatment in subjects with previoushistory of depression. American Journal of Psychiatry 161, 166–168.
Blair, R.J.R., Curran, V., 1999. Selective impairment in the recognition of angerinduced by diazepam. Psychopharmacology 147, 335–338.
Bora, E., Vahip, S., Gonul, A.S., Akdeniz, F., Alkan, M., Ogut, M., Eryavuz, A., 2005.Evidence for theory of mind deficits in euthymic patients with bipolardisorder. Acta Psychiatrica Scandinavica 112, 110–116.
Bourke, C., Douglas, K., Porter, R., 2010. Processing of facial emotion expression inmajor depression: a review. The Royal Australian and New Zealand College ofPsychiatrists 44, 681–696.
Bozikas, V.P., Kosmidis, M.H., Tonia, T., Andreou, C., Focas, K., Karavatos, A., 2007.Impaired perception of affective prosody in remitted patients with bipolardisorder. The Journal of Neuropsychiatry and Clinical Neurosciences 19, 436–440.
Bozikas, V.P., Tonia, T., Fokas, K., Karavatos, A., Kosmidis, M.H., 2006. Impairedemotion processing in remitted patients with bipolar disorder. Journal ofAffective Disorders 91, 53–56.
Butzlaff, R.L., Hooley, J.M., 1998. Expressed emotion and psychiatric relapse.Archives of General Psychiatry 55, 547–552.
Chang, K., Adleman, N.E., Dienes, K., Simeonova, D.I., Menon, V., Reiss, A., 2004.Anomalous prefrontal-subcortical activation in familial pediatric bipolar dis-order. Archives of General Psychiatry 61, 781–792.
Compton, R.J., Banich, M.T., Mohanty, A., Milham, M.P., Herrington, J., Miller, G.A.,Scale, P.E., Webb, A., Heller, W., 2003. Paying attention to emotion: an fMRI
investigation of cognitive and emotional Stroop tasks. Cognitive, Affective, &Behavioral Neuroscience 3, 81–96.
Cuellar, A.K., Johnson, S.L., Ruggero, C.J., 2009. Affective reactivity in response tocriticism in remitted bipolar disorder: a laboratory analog of expressedemotion. Journal of Clinical Psychology 65, 925–941.
Davis, M.H., 1980. Measuring individual differences in empathy: evidence for amultidimensional approach. Journal of Personality and Social Psychology 44,113–126.
de Almeida Rocca, C.C., van den Heuvel, E., Caaetano, S.C., Lafer, B., 2009. Facialemotion recognition in bipolar disorder: a critical review. Revista Brasileira DePsiquiatria 31, 171–180.
Derntl, B., Seidel, E.-M., Kryspin-Exner, I., Hasmann, A., Dobmeier, M., 2009. Facialemotion recognition in patients with bipolar I and bipolar II disorder. BritishJournal of Clinical Psychology 48, 363–375.
Dickerson, F.B., Sommerville, J., Origoni, A.E., Ringel, N.B., Parente, F., 2001.Outpatients with schizophrenia and bipolar disorder I: do they differ in theircognitive and social functioning? Psychiatry Research 102, 21–27.
Dziobek, I., Fleck, S., Kalbe, E., Rogers, K., Hassenstab, J., Brand, M., Kessler, J.,Woike, J., Wolf, O., Convit, A., 2006. Introducing the MASC: a movie for theassessment of social cognition. Journal of Autism and Developmental Dis-orders 36, 623–636.
Ekman, P., Friesen, W.V., 1976. Pictures of Facial Affect. CA: Consulting Psychol-ogist Press, Pato Alto.
Farmer, A., Lam, D., Sahakian, B., Roiser, J., Burke, A., O’Neill, N., Keating, S., Smith, G.P.,McGuffin, P., 2006. A pilot study of positive mood induction in euthymic bipolarsubjects compared with healthy controls. Psychological Medicine 36, 1213–1218.
Frangou, S., Donaldson, S., Hadjulis, M., Landau, S., Goldstein, L.H., 2005. TheMaudsley bipolar disorder project: executive dysfunction in bipolar disorder Iand its clinical correlates. Biological Psychiatry 58, 859–864.
Gitlin, M.J., Swendsen, J., Heller, T.L., Hammen, C., 1995. Relapse and impairmentin bipolar disorder. The American Journal of Psychiatry 152, 1635–1640.
Goldberg, J.E., 2004. The Changing Landscape of Psychopharmacology. GuildfordPress, New York, pp. 109–138.
Gopin, C.B., Burdick, K.E., DeRosse, P., Goldberg, T.E., Malhotra, A.K., 2011.Emotional modulation of response inhibition in stable patients with bipolarI disorder: a comparison with healthy and schizophrenia subjects. BipolarDisorders 13, 164–172.
Hamilton, M., 1960. A rating scale for depression. Journal of NeurologicalNeurosurgical Psychiatry 23, 56–62.
Harmer, C.J., Grayson, L., Goodwin, G.M., 2002a. Enhanced recognition of disgust inbipolar illness. Society of Biological Psychiatry 51, 298–304.
Harmer, C.J., Perrett, D.I., Cowen, P.J., Goodwin, G.M., 2001. Administration of thebeta-adrenoceptor blocker propranolol impairs the processing of facial expres-sions of sadness. Psychopharmacology 154, 383–389.
Harmer, C.J., Shelley, N.C., McTavish, S.F.B., Cowen, P.J., Goodwin, G.M., 2002b.Repeated administration of citalopram or reboxetine reduces the perception ofnegative emotions from facial expressions. Journal of PsychopharmacologySupplementary A, 70.
Hassel, S., Almeida, J.R., Frank, E., Versace, A., Nau, S.A., Klein, C.R., Kupfer, D.J.,Phillips, M.L., 2009. Prefrontal cortical and striatal activity to happy and fearfaces in bipolar disorder is associated with comorbid substance abuse andeating disorder. Journal of Affective Disorder 118, 19–27.
Hassel, S., Almeida, J.R., Kerr, N., Nau, S., Ladouceur, C.D., Fissell, K., Kupfer, D.J., Phillips,M.L., 2008. Elevated striatal and creased dosolateral prefrontal cortical activity inresponse to emotional stimuli in euthymic bipolar disorder: no associations withpsychotrophic medication load. Bipolar Disorders 10, 916–927.
Hooker, C., Park, S., 2002. Emotion processing and its relationship to socialfunctioning in schizophrenia patients. Psychiatry Research 112, 41–50.
Jongen, E.M.E., Smulders, F.T.Y., Ranson, S.M.G., Arts, B.M.G., Krabbendam, L., 2007.Attentional bias and general orientating processes in bipolar disorder. Journalof Behaviour Therapy and Experimental Psychiatry 38, 168–183.
Kauer-Sant’Anna, M., Yatham, L.N., Tramontina, J., Weyne, F., Cereser, K.M.,Gazalle, F.K., Andreazza, A.C., Santin, A., Quevedo, J., Izquierdo, I., Kapczinski,F., 2008. Emotional memory in bipolar disorder. The British Journal ofPsychiatry 192, 458–463.
Kerr, S.L., Neale, J.M., 1993. Emotion perception in schizophrenia—specific deficitor further evidence of generalized poor performance. Journal of AbnormalPsychology 102, 312–318.
Kerr, N., Scott, J., Phillips, M.L., 2005. Patterns of attentional deficits and emotionalbias in bipolar and major depressive disorder. British Journal of ClinicalPsychology 44, 343–356.
Kim, E., Jung, Y.-C., Ku, J., Kim, J.-J., Lee, H., Kim, S.Y., Kim, S.I., Cho, H.-S., 2009.Reduced activation in the mirror neuron system during a virtual socialcognition task in euthymic bipolar disorder. Progress in Neuro-Psychopharmacology & Biological Psychiatry 33, 1409–1416.
Kinney, J.M., 1995. Comprehension of Affect in Children with Pervasive Develop-mental Disorders: Specific Deficits in Perceptual Matching Tasks. UnpublishedDoctoral Dissertation. American University, Washington, DC. Human Neurop-sychology Laboratory.
Kinney, J.M., Fantie, B.D., Pascualvaca, D.M., Rodriguez, D., Mirsky, A.F., 1995.Comprehension of affect in children with pervasive developmental disorders:deficits in matching faces to cartoon situations. Journal of InternationalNeuropsychology in Society 1, 156–157.
Knowles, R., Tai, S., Christensen, I., Bentall, R., 2005. Coping with depression andvulnerability to mania: a factor analytic study of Nolen-Hoeksema (1991)response style questionnaire. British Journal of Clinical Psychology 44, 99–112.
L. Mercer, R. Becerra / Journal of Affective Disorders 146 (2013) 295–309 307

Author's personal copy
Langenecker, S.A., Saunder, E.F.H., Kade, A.M., Ransom, M.T., McInnis, M.G., 2010.Intermediate: cognitive phenotypes in bipolar disorder. Journal of AffectiveDisorders 122, 285–293.
Lawrence, N.S., Williams, A.M., Surguladze, S., Giampietro, V., Brammer, M.J.,Andrew, C., Frangou, S., Ecker, C., Phillips, M.L., 2004. Subcortical and ventralprefrontal cortical neural responses to facial expressions distinguish patientswith bipolar disorder and major depression. Society of Biological Psychiatry55, 578–587.
Lembke, A., Ketter, T.A., 2002. Impaired recognition of facial emotion in mania. TheAmerican Journal of Psychiatry 159, 302–304.
Lex, C., Meyer, T.D., Marquart, B., Thau, K., 2008. No strong evidence for abnormallevels of dysfunctional attitudes, automatic thoughts, and emotionalinformation-processing biases in remitted bipolar I affective disorder. Psy-chology and Psychotherapy: Theory, Research and Practice 81, 1–13.
Malhi, G.S., Lagopoulos, J., Owen, A.M., Ivanovski, B., Shnier, R., Sachdev, P., 2007a.Reduced activation to implicit affect induction in euthymic bipolar patients:an fMRI study. Journal of Affective Disorders 97, 109–122.
Malhi, G.S., Lagopoulos, J., Sachdev, P.S., Ivanovski, B., Shnier, R., 2005. Anemotional stroop functional MRI study of euthymic bipolar disorder. BipolarDisorders 7, 58–69.
Malhi, G.S., Lagopoulos, J., Sachdev, P.S., Ivanovski, B., Shnier, R., Ketter, T., 2007b.Is a lack of disgust something to fear? A functional magnetic resonanceimaging facial emotion recognition study in euthymic bipolar disorderpatients. Bipolar Disorders 9, 345–357.
Mansell, W., Lam, D., 2006. ‘‘I won’t do what you tell me!’’ Elevated mood and theassessment of advice-taking in euthymic bipolar I disorder. BehaviourResearch and Therapy 44, 1787–1801.
Mayer, J.D., Cobb, C.D., 2000. Educational policy on emotional intelligence: does itmake sense? Educational Psychology Review 12, 163–183.
Miklowitz, D.J., 2006. A review of evidence-based psychosocial intervention forbipolar disorder. Journal of Clinical Psychiatry 67, 28–33.
Montag, C., Ehrlich, A., Neuhaus, K., Dziobek, I., Heekeren, H.R., Heinz, A., Gallinat,J., 2010. Theory of mind impairments in euthymic bipolar patients. Journal ofAffective Disorder 123, 264–269.
Montgomery, S.A., Asberg, M., 1979. A new depression scale designed to besensitive to change. British Journal of Psychiatry 134, 382–389.
Morrison, R.L., Bellack, A.S., Bashore, T.R., 1988. Perception of emotion amongschizophrenic patients. Journal of Psychopathology and Behavioural Assess-ment 10, 319–332.
Mueser, K.T., Doonan, R., Penn, D.L., Blanchard, J.J., Bellack, A.S., Nishith, P., DeLeon,J., 1996. Emotional recognition and social competence in chronic schizophre-nia. Journal of Abnormal Psychology 105, 271–275.
Murphy, F.C., Sahakian, B.J., Rubinsztein, J.S., Michael, A., Rogers, R.D., Robbins,T.W., Paykel, E.S., 1999. Emotional bias and inhibitory control processes inmania and depression. Psychological Medicine 29, 1307–1321.
Phillips, M.L., 2003. Understanding the neurobiology of emotion perception:implications for psychiatry. British Journal of Psychiatry 182, 190–192.
Phillips, M.L., 2009. Prefrontal cortical and striatal activity to happy and fear facesin bipolar disorder is associated with comorbid substance abuse and eatingdisorder. Journal of Affective Disorder 118, 19–27.
Phillips, M.L., Drevets, W.C., Rauch, S.L., Lane, R., 2003. Neurobiology of emotionperception I: the neural basis of normal emotion perception. BiologicalPsychiatry 54, 504–514.
Poole, J.H., Tobias, F.C., Vinogradov, S., 2000. The functional relevance of affectrecognition errors in schizophrenia. Journal of International NeuropsychologySociety 6, 649–658.
Powell, J., Al-Adawi, S., Morgan, J., 1996. Motivational deficits after brain injury:effects of bromocriptine in 11 patients. Journal of Neurological NeurosurgicalPsychiatry 60, 416–421.
Premack, D., Woodruff, G., 1978. Does the chimpanzee have a ‘‘theory-of-mind’’?Behavioural Brain Science 4, 515–526.
Robinson, J.L., Monkul, E.S., Tordesillas-Gutierrez, D., Franklin, C., Bearden, C.E.,Fox, P.T., Glahn, D.C., 2008. Fronto-limbic circuitry in euthymic bipolardisorder: evidence for prefrontal hyperactivation. Psychiatry Research: Neu-roimaging 164, 106–113.
Rogers, R.D., Everitt, B.J., Baldacchino, A., Blackshaw, A.J., Swainson, R., Wynne, K.,Baker, N.B., Hunter, J., Carthy, T., Booker, E., London, M., Deakin, J.F., Sahakian, B.J.,Robbins, T.W., 1999. Dissociable deficits in the decision-making cognition ofchronic amphetamine abusers, opiate abusers, patients with focal damage toprefrontal cortex, and tryptophan-depleted normal volunteers: evidence formonoaminergic mechanisms. Neuropsychopharmacology 20, 322–339.
Roiser, J., Farmer, A., Lam, D., Burke, A., O’Neill, N., Keating, S., Powell Smith, G.,Shakian, B., McGuffin, P., 2009. The effect of positive mood induction onemotional processing in euthymic individuals with bipolar disorder andcontrols. Psychological Medicine 39, 785–791.
Rush, A.J., Gullion, C.M., Basco, M.R., Jarrett, R.B., Trivedi, M.H., 1996. The inventoryof depressive symptomatology (IDS): psychometric properties. PsychologicalMedicine 26, 477–486.
Shamay-Tsoory, S., Harari, H., Szepsenwol, O., Levkovitz, Y., 2009. Neuropsycho-logical evidence of impaired cognitive empathy in euthymic bipolar disorder.The Journal of Neuropsychiatry and Clinical Neurosciences 21, 59–67.
Shimkunas, A., 1972. Demand for intimate self-disclosure and pathologicalverbalisations in schizophrenia. Journal of Abnormal Psychology 80, 197–205.
Strakowski, S.M., Adler, C.M., Holland, S.K., Mills, N.P., Del Bello, M.P., Eliassen, J.C.,2005. Abnormal fMRI brain activation in patients with bipolar disorderduring performance of a working memory task. Bipolar Disorder 162, 1697–1705.
Summers, M., Papadopoulou, K., Bruno, S., Cipolotti, L., Ron, M.A., 2006. Bipolar Iand bipolar II disorder: cognition and emotion processing. PsychologicalMedicine 36, 1799–1809.
Tai, S., Haddock, G., Bentall, R., 2004. The effects of emotional salience on thoughtdisorder in patients with bipolar affective disorder. Psychological Medicine 34,803–809.
Tohen, M., Waternaux, C.M., Tsuang, M.T., 1990. Outcome in mania: a 4-yearprospective follow-up of 75 patients utilizing survival analysis. Archives ofGeneral Psychiatry 47, 1106–1111.
Van der Gucht, E., Morriss, R., Lancaster, G., Kinderman, P., Bentall, R.P., 2009.Psychological processes in bipolar affective disorder: negative cognitive styleand reward processing. The British Journal of Psychiatry 194, 146–151.
Vaskinn, A., Sundet, K., Friis, S., Simonsen, C., Birkenæs, A.B., Engh, J.A., Jonsdottir, H.,Ringen, P.A., Opjordsmoen, S., Andreassen, O.A., 2007. The effect of gender onemotion perception in schizophrenia and bipolar disorder. Acta PsychiatricaScandinavica 116, 263–270.
Venn, H.R., Gray, J.M., Montagne, B., Murray, L.K., Burt, D.M., Frigerio, E., Perrett, D.I.,Young, A.H., 2004. Perception of facial expressions of emotion in bipolardisorder. Bipolar Disorder 6, 286–293.
Versace, A., Thompson, W.K., Zhou, D., Almeida, J.R.C., Hassel, S., Klein, C.R., Kupfer, D.J.,Phillips, M.L., 2010. Abnormal left and right amygdale-orbitofrontal corticalfunctional connectivity to emotional faces: state versus trait vulnerability markersof depression in bipolar disorder. Society of Biological Psychiatry 67, 422–431.
Wessa, M., Houenous, J., Paill�ere-Martinot, M., Berthoz, S., Artigues, E., Leboyer, M.,Martinot, J., 2007. Fronto-striatal overactivation in euthymic bipolar patientsduring an emotional go/nogo task. American Journal of Psychiatry 164,638–646.
Winters, K.C., Neale, J.M., 1985. Mania and low self-esteem. Journal of AbnormalPsychology 94, 282–290.
Witkin, H.A., Ottman, P.K., Raskin, E., Karp, S., 1971. A Manual for the EmbeddedFigure Test. Consulting Psychologists Press, Mountain View, CA.
Young, R.C., Biggs, J.T., Ziegler, V.E., Meyer, D.A., 1978. A rating scale formania: reliability, validity and sensitivity. British Journal of Psychiatry 133,429–435.
Yurgelun-Todd, D.A., Gruber, S.A., Kanayama, G., Killgore, W.D., Baird, A.A., Young, A.D.,2000. fMRI during affect discrimination in bipolar affective disorder. BipolarDisorder 2, 237–248.
Further reading
American Psychiatric Association, 1994. Diagnostic and Statistical Manual ofMental Disorders, 4th ed. American Psychiatric Association, Washington, DC.
Andreasen, N.C., 1983. Scale for the Assessment of Negative Symptoms (SANS).University of Iowa, Iowa City.
Andreasen, N.C., 1979. Thought, language and communication disorders: I. Clinicalassessment, definition of terms and evaluation of their reliability. Archives ofGeneral Psychiatry 36, 1315–1321.
Baron-Cohen, S., O’Riordan, M., Stone, V., Jones, R., Plaisted, K., 1999. Recognitionof faux pas by normally developing children and children with aspergersyndrome or high-functioning autism. Journal of Autism DevelopmentalDisorder 29, 407–418.
Bauer, M.S., Critis-Cristoph, P., Ball, W.A., Dewess, E., McAllister, T., Alahi, P.,Cacciola, J., Whybrow, P.C., 1991. Independent assessment of manic anddepressive symptoms by self-rating: scale characteristics and implicationsfor the study of mania. Archives of General Psychiatry 48, 807–812.
Bentall, R.P., Thompson, M., 1990. Emotional stroop performance and the manicdefence. British Journal of Psychiatry 29, 235–237.
Derntl, B., Kryspin-Exner, I., Fernbach, E., Moser, E., Habel, U., 2008. Emotionrecognition accuracy in healthy young females in associated with cycle phase.Hormones and Behavior 53, 90–95.
First, M.B., Gibbon, M., Spitzer, R.L., Williams, J.B.W., 1995a. Structured ClinicalInterview for DSM-IV (SCID-I): User’s Guide and Interview, Research Version.Biometrics Research Department, New York Psychiatric Institute, New York.
First, M.B., Spitzer, R.L., Gibbon, M., Williams, J.B.W., 1995b. Structured ClinicalInterview for DSM-IV Axis I & Axis II Disorders (Version 20). BiometricsResearch, New York State Psychiatric Institute, New York.
First, M., Spitzer, R.L., Gibbon, M., Williams, J.B.W., 2002. Structured ClinicalInterview for DSM-IV-TR Axis I Disorders, Research Version, Patient Edition.New York State Psychiatric Institute, New York.
Golden, C.J., 1978. Stroop, Colour and Word Test. Stoelting, Chicago.Haddock, G., Wolfenden, M., Lowens, I., Tarrier, N., Bentall, R., 1995. Effect of
emotional salience on thought disorder in patients with schizophrenia. BritishJournal of Psychiatry 167, 618–620.
Hariri, A.R., Tessitore, A., Mattay, V.S., Fera, F., Weinberger, D.R., 2002. Theamygdala response to emotional stimuli: a comparison of faces and scenes.NeuroImage 17, 317–323.
Hedlund, S., Rude, S.S., 1995. Evidence of latent depressive schemas in formerlydepressed individuals. Journal of Abnormal Psychology 104, 517–525.
Heuer, F., Reisberg, D., 1990. Vivid memories of emotional events: accuracy ofremembered minutiae. Memory & Cognition 18, 496–506.
Hiou, K., Vagia, A., Haritidou, E., Karakostas, D., Kosmidis, M.H., 2004. Affectperception as a cognitive function: validity and clinical application of a
L. Mercer, R. Becerra / Journal of Affective Disorders 146 (2013) 295–309308

Author's personal copy
neuropsychological test battery in healthy individuals and patients with brainlesions. Psychology 11, 388–401. (in Greek).
Kay, S.R., Fiszbein, A., Opler, L.A., 1987. The positive and negative syndrome scale(PANSS) for schizophrenia. Schizophrenia Bulletin 13, 261–276.
Lam, D.H., Wright, K., Sham, P., 2005. Sense of hyper-positive self and res-ponse to cognitive therapy in bipolar disorder. Psychological Medicine 35,69–77.
Lyon, H.M., Startup, M., Bentall, R.P., 1999. Social cognition and the manic defense:attributions, selective attention, and self-schema in bipolar affective disorder.Journal of Abnormal Psychology 108 (2), 273–282.
McGuffin, P., Farmer, A., Harvey, I., 1991. A polydiagnostic application of theoperational criteria in studies of psychotic illness. Development and reliabilityof the OPCRIT system. Archives of General Psychiatry 48, 764–770.
Murray, L.M., 1999. Facial Expression Perception in Different Psychiatric Groups.Unpublished Doctoral Dissertation, University of St Andrews.
Nurnberger Jr., J.I., Blehar, M.C., Kaufmann, C.A., York-Cooler, C., Simpson, S.G.,Harkavy-Friedman, J., Severe, J.B., Malaspina, D., Reich, T., 1994. Diagnosticinterview for genetic studies. Rational, unique features, and training NIMHgenetics initiative. Archives of General Psychiatry 51, 849–859.
Overall, J., Gorham, D., 1962. The brief psychiatric rating scale. PsychologicalReports 10, 799–812.
Spitzer, R.L., Endicott, J., Robins, E., 1975. Research and Diagnostic Criteria. NewYork State Psychiatric Institute, New York.
Spitzer, R.L., Williams, J.B., Gibbon, M., First, M.B, 1990. User’s Guide for theStructured Clinical Interview for DSM-III-R SCID. American Psychiatric Press,Washington DC.
Sternberg, S., 1969. Memory-scanning: mental processes revealed by reaction-time experiments. American Scientist 57, 421–457.
Surguladze, S., Brammer, M.J., Keedwell, P., Giampietro, V., Young, A.W., Travis,M.J., Williams, S.C.R., 2005. A differential pattern of neural response towardsad versus happy facial expressions in major depressive disorder. BiologicalPsychiatry 57, 201–209.
Watson, D., Clark, L.A., Tellegen, A., 1988. Development and validation of briefmeasures of positive and negative affect: the PANAS scale. Journal ofPersonality and Social Psychology 54, 1063–1070.
Williams, J.M.G., Broadbent, K., 1986. Autobiographical memory in attemptedsuicide patients. Journal of Abnormal Psychology 95, 144–149.
Wing, J.K., Babor, T., Brugha, T., Burke, J., Cooper, J.E., Giel, R., Jablenski, A., Reiger, D.,Sartorius, N., 1990. SCAN. Schedules for clinical assessment in neuropsychiatry.Archives of General Psychiatry 47, 589–593.
Wright, K., Lam, D.H., Newsom-Davis, I., 2005. Induced mood change anddysfunctional attitudes in remitted bipolar I affective disorder. Journal ofAbnormal Psychology 114, 689–696.
Young, A.W., Rowland, D., Calder, A.J., Etcoff, N.L., Seth, A., Perret, D.I., 1997. Facialexpression megamix: tests of dimensional and category accounts of emotionrecognition. Cognition 63, 271–313.
L. Mercer, R. Becerra / Journal of Affective Disorders 146 (2013) 295–309 309





























