Embed Size (px)
Citation preview

Allogeneic bone marrow transplantation for agnogenic myeloidmetaplasia
PHILIPPE GUARDIOLA,1 HELENE ESPEROU,1 DOMINIQUE CAZALS-HATE M,2 NORBERT IFRAH,3 JEAN-PIERRE JOUET,4
AGNES BUZYN,5 LAURE NT SUTTON,6 NICO LE GRAT ECOS,7 HERVE TIL LY,8 BRUNO LIOURE9
AND ELIANE GLUCKMAN,1
for the French Society of Bone Marrow Transplantation 1Bone Marrow Transplantation Unit, and 2HistopathologyDepartment, Saint-Louis Hospital, Paris, 3Centre Hospitalier Universitaire, Angers, 4Centre Hospitalier Huriez, Lille,5Necker Hospital, Paris, 6La Pitie-Salpetriere Hospital, Paris, 7Cimiez Hospital, Nice, 8Becquerel Centre, Rouen,and 9Hautepierre Hospital, Strasbourg, France
Received 16 April 1997; accepted for publication 19 June 1997
Summary. Agnogenic myeloid metaplasia is a rare indicationfor allogeneic bone marrow transplantation (BMT). We haveretrospectively studied 12 patients allografted for this diseasewithin the French BMT group. Prior to BMT, the mean agewas 40 years (range 14–49). Diagnosis was based on thePolycythaemia Vera Study Group criteria. Before BMT, 10patients had been splenectomized, eight required transfu-sions, and four had received at least two lines of chemother-apy. Cyclophosphamide and total body irradiation was themain conditioning regimen used (n¼8). The donor was anHLA-identical sibling except in one case where there was oneHLA-DR mismatch. Acute graft-versus-host disease (GVHD)prophylaxis consisted of methotrexate and cyclosporine A.11 patients engrafted with median times to achieve absoluteneutrophil count >0.5 × 109/l and platelet count >50 ×109/l of 17 (range 12–44) and 29 (range 12–196) days
respectively. One primary graft failure occurred. 10 patientsdeveloped grade II–IV acute GVHD, four developed extensivechronic GVHD. One patient relapsed 16 months post-BMTand was untreated and well 14 months later. Three patientsdied from the BMT procedure. In May 1996 the medianfollow-up was 25 months and the 4-year overall and event-free survivals were 71% and 59%, respectively. Thus, weconclude that extensive myelofibrosis is not associated withdelayed engraftment, and that HLA-identical sibling allo-geneic BMT can be considered in a small proportion ofpatients with agnogenic myeloid metaplasia.
Keywords: agnogenic myeloid metaplasia, primary myelo-fibrosis, myeloproliferative disorder, allogeneic bone marrowtransplantation.
Agnogenic myeloid metaplasia (AMM) is a myeloproliferativedisorder characterized by marrow fibrosis, myeloid meta-plasia, splenomegaly and leucoerythroblastic blood picture(Dameshek, 1951; Laszlo, 1975). Despite the fact thatDupriez et al (1996) have recently reasserted that AMM waspreferentially a pathology of elderly patients (median age 65years), approximatively 10% of their 195 patients were <50years old. Furthermore, although the course of the disease isusually chronic, the median survival has been evaluated at 5years (Nakai et al, 1962; Pitcock et al, 1962; Ward & Block,1971; Varki et al, 1983; Hasselbalch, 1990; Visani et al,1990; Thiele et al, 1992; Dupriez et al, 1996). Although lessfrequent than during chronic myelogenous leukaemia,blastic transformation, which occurs in 4–28% of AMM, isone of the major causes of death (Cehrelli et al, 1976;
Rosenthal & Molony, 1977; Marcus et al, 1986; Garcia et al,1989; Barosi et al, 1995; Kimura et al, 1995). This is ofparticular concern since no current treatment has shown anability to cure or even to prolong survival of these patients.In order to delineate the high-risk patients, Dupriez et al(1996) have proposed a simple prognostic score whichdefines three subgroups of patients according to theirhaemoglobin level and leucocyte count. The high-risksubgroup was defined by haemoglobin <10 g/dl andleucocytes <4 or >30 × 109/l, with a life expectancy of 1year. Here, in this retrospective study, carried out with theFrench Society of Bone Marrow Transplantation, we reportthe results of allogeneic BMT for AMM.
PATIENTS AND METHODS
Definition. Criteria retained by the Polycythaemia VeraStudy Group to define AMM were used for the inclusion of
British Journal of Haematology, 1997, 98, 1004–1009
1004 q 1997 Blackwell Science Ltd
Correspondence: Professor E. Gluckman, Bone Marrow Transplan-tation Unit, Saint-Louis Hospital, 1 avenue Claude Vellefaux,F 75475 Paris cedex 10, France.

1005Allogeneic BMT for AMM
q 1997 Blackwell Science Ltd, British Journal of Haematology 98: 1004–1009
the patients in the study (Laszlo, 1975). Thus, splenomegaly,red cell poikilocytosis and leucoerythroblastosis wererequired in addition to the absence of monocytosis andPhiladelphia chromosome. Patients were not included if theyhad a previous history of polycythaemia vera or myelodys-plastic syndrome, and if marrow/peripheral blood blastosiswas >15%. All bone marrow biopsies were reviewed in thehistopathologic laboratory of the Saint-Louis Hospital inorder to exclude other causes of marrow fibrosis such asacute myelofibrosis, myelodysplastic syndromes, hairy cellleukaemia or acute megakaryoblastic leukaemia. At thesame time, according to Sultan et al (1991), reticulin andcollagen contents were assessed by special histologic stains,as well as the cellularity and the blast percentage of eachbone marrow biopsy. Briefly, marrow fibrosis was grade I ifincreased cellularity and reticulinic marrow fibrosis wereobserved, grade II if the overall cellularity was decreasedwith mutilating fibrosis, or grade III when osteomyelo-sclerosis was diagnosed.
Patients’ characteristics (Table I). Between 1979 and1995, 12 patients (seven males and five females) fromeight centres in France were allografted for AMM. At thetime of diagnosis, mean age was 35 years. Four patientshad hepatomegaly. Median haemoglobin level, leucocyteand platelet counts were 10.7 g/dl (range 6.9–14.0), 12.6 ×109/l (range 7.3–69) and 215 × 109/l (range 15–1800)respectively. A search for myeloid metaplasia was investi-gated in 11 cases and confirmed the diagnosis in all caseseither by histopathologic analysis of splenectomies (n¼10)and liver biopsies (n¼4) or ferrokinetic studies (n¼5).Among the 10 cytogenetic analysis available, three wereabnormal, showing trisomy 8, monosomy 19 and trans-location (7;12). At that time, seven patients, according toDupriez et al (1996), had a low-risk score 0 (haemoglobin>10.0 g/dl and leucocytes >4 and <30 × 109/l, lifeexpectancy 93 months). Hydroxyurea was the mostfrequent chemotherapy used before BMT (n¼6). Five
patients required at least two different lines of treatmentsto control their disease, and one patient (UPN10) wasallografted without any previous treatment.
Besides the age of the patient and the presence of an HLA-identical sibling donor, the timing of the graft was based onthe presence of anaemia requiring multiple transfusions(n¼7), hepatosplenomegaly (>5 cm below costal margin)(n¼3), cytogenetic abnormalities (n¼3), or worsening ofmarrow fibrosis on repeat biopsies (n¼1).
At time of BMT, the mean age was 40 years (range 14–49)and the median time from diagnosis to BMT 45 months(range 2–120), with two patients allografted within a year ofdiagnosis. Prior to BMT, median haemoglobin level, leuco-cyte and platelet counts were 8.5 g/dl (range 5.7–13.3),11.3 × 109/l (range 1.3–40) and 327 × 109/l (range 26–1100) respectively. According to the score of Dupriez et al(1996), the majority of patients (n¼9) had an intermediatescore 1 (life expectancy 26 months). Bone marrowexamination showed osteomyelosclerosis in seven cases,grade II marrow fibrosis in three cases, and grade I in three.Bone marrow cellularity was <50% in four cases which hadgrade III marrow fibrosis. There was no sign of acutetransformation on biopsies. Recipient and donor serologicalstatus for cytomegalovirus are summarized in Table I.Elective splenectomy was performed in 10 patients prior toBMT. Eight patients required red blood cell transfusions; twoalso needed platelet transfusions.
Conditioning regimens. As presented in Table II, thecombination of cyclophosphamide, 120 mg/kg, and single-dose or fractionated total body irradiation (TBI) was mainlyused as conditioning regimen (n¼8). Three other patientsreceived an intensified preparative regimen with the additionof etoposide. UPN9 did not receive TBI, and was conditionedby cyclophosphamide 120 mg/kg and thiotepa 10 mg/kg.Cells were always harvested from bone marrow ; peripheralblood stem cells and CD34 positive selection were never used.The median dose of nucleated cells infused per kilogram body
Table I. Patients’ characteristics at diagnosis and prior to BMT.
Dupriez score Myelofibrosis Splenectomy RBC units Platelet units ABO CMV status HLA statusUPN Sex prior to BMT prior to BMT prior to BMT prior to BMT prior to BMT incompatibility (donor/recipient) (donor/recipient)
1 M 2 II Yes No No Major Unknown / Neg Matched2 F 0 I Yes > 10 < 10 Minor Neg / Neg Matched3 F 1 III Yes > 10 No None Pos / Pos Matched4 M 1 III Yes No No Major Pos / Pos Matched5 M 1 II Yes > 10 No Minor Neg / Neg Matched6 M 1 III Yes No No None Neg / Pos Matched7 M 1 III Yes No No None Neg / Neg Matched8 F 1 III Yes >10 No None Neg / Pos Matched9 M 1 I No > 10 < 10 None Pos / Neg DR mismatched
10 M 1 III No < 10 No None Neg / Neg Matched11 F 1 III Yes > 10 No Major Pos / Pos Matched12 F 0 II Yes < 10 No None Pos / Pos Matched
Dupriez score 0: haemoglobin >10 g/dl and WBC >4 × 109/l and <30 × 109/l (expected median survival: 93 months); score 1: haemoglobin<10 g/dl or WBC <4 × 109/l or WBC >30 × 109/l (expected median survival: 26 months); score 2: haemoglobin <10 g/dl and WBC <4 × 109/lor >30 × 109/l (expected median survival: 13 months).
weight was 2.5 × 108 (range 0.56–5.8). Five patientsreceived <2 × 108 nucleated cells per kilogram.
Engraftment. The day of marrow infusion was designatedas day 0. Myeloid engraftment endpoint was the first daywith an absolute neutrophil count (ANC) of at least 0.5 ×109/l. Platelet engraftment endpoint was defined as the firstday with a minimal platelet count of 50 × 109 /l withoutplatelet transfusion. Chimaerism was determined by stan-dard procedures depending on the donor–recipient combi-nation. Primary graft failure was diagnosed if myeloidengraftment endpoint was not reached until day 30.Sustained engraftment was defined by haemoglobin level>10.0 g/dl, platelet count >100 × 109/l, and white bloodcell count >4 × 109/l, with full donor chimaerism at 1 yearpost-BMT.
HLA status and graft-versus-host disease (GVHD). Amongthe 12 donor/recipient pairs, 11 were HLA-A, -B, -DRidentical, and one was HLA-DR mismatched (Table I).Prophylaxis of acute GVHD consisted of methotrexate andcyclosporine A. Acute and chronic GVHD were gradedaccording to the Seattle criteria (Glucksberg et al, 1974;Thomas et al, 1975). Analysis involving chronic GVHD wasbased upon patients who survived longer than 100 d fromBMT.
Outcome and statistical analysis. Survival was assessed onthe date of last patient contact and analysed on 1 May 1996.The median duration of follow-up was 25 months (range 1–173). Complete remission was defined by disappearance offibrosis on marrow biopsy, total haemopoietic chimaerism,and normal karyotype if abnormalities were present prior toBMT. Diagnosis of disease recurrence followed haematologi-cal, histopathological or cytogenetic criteria. The duration ofevent-free survival was calculated from the date of BMT tothe date of progression of disease, relapse, death, or the datethe patient was last known to be alive. The overall survivaland event-free survival were analysed by the Kaplan & Meier(1958) method.
RESULTS
EngraftmentEleven patients engrafted; only one primary graft failureoccurred (UPN3). The median times to reach myeloid andplatelet engraftment endpoints were 17 d (range 12–44) and29 d (range 12–196) respectively (Table II). UPN9 andUPN10, the patients who were not splenectomized prior toBMT, were the only ones who did not reach the plateletengraftment endpoint before day 100 post-BMT. For theoverall group, in comparison to myeloid engraftment,platelet recovery was delayed (P ¼ 0.004, Wilcoxon signedrank test). The difference was still significant even if UPN9and UPN10 were not included in the analysis (P ¼ 0.016,Wilcoxon signed rank test). Sustained engraftment occurredin eight patients, the others could not be analysed because ofinsufficient follow-up (n¼3) or death occurring within 1 yearpost-transplantation (n¼1). One patient (UPN10) receivedG-CSF after BMT because of neutropenia induced byanti-thymocyte globulin therapy.
q 1997 Blackwell Science Ltd, British Journal of Haematology 98: 1004–1009
1006 Philippe Guardiola et al
Tabl
eII
.Con
diti
onin
gre
gim
ens,
don
orce
lldo
sein
fuse
d,an
dre
sult
s.
Nu
clea
ted
AN
CP
late
lets
Age
atY
ear
cell
dose
>0
. 5×
19
9/l
>5
0×
10
9/l
Acu
teC
hro
nic
Follo
w-u
pU
PN
BM
T(y
r)of
BM
TC
ondi
tion
ing
regi
men
s(×
10
8/k
g)(d
)(d
)G
VH
DG
VH
Dfr
omB
MT
Cau
seof
deat
h
11
41
97
9C
Y1
20
mg/
kg,T
BI
10
Gy
5. 8
01
56
8IV
Exte
nsi
ve1
73
mon
ths
–2
38
19
86
CY
12
0m
g/kg
,FT
BI
12
Gy
0. 5
61
61
9II
Lim
ited
10
8m
onth
s–
33
91
98
9C
Y1
20
mg/
kg,F
TB
I1
1G
y2
. 98
Not
ach
ieve
dN
otac
hie
ved
IIN
otev
alu
able
32
days
Ren
alfa
ilure
43
71
99
1C
Y1
20
mg/
kg,F
TB
I1
2G
y0
. 88
16
15
IILi
mit
ed5
8m
onth
s–
54
51
99
1C
Y1
20
mg/
kg,F
TB
I1
2G
y3
. 20
17
20
IN
one
40
mon
ths
–6
49
19
93
CY
12
0m
g/kg
,TB
I1
0G
y1
. 92
20
34
Non
eN
one
29
mon
ths
–7
44
19
93
CY
12
0m
g/kg
,FT
BI
12
Gy
2. 9
81
51
9IV
Non
e5
mon
ths
Inva
sive
aspe
rgill
osis
83
61
99
4C
Y1
20
mg/
kg,V
P1
63
0m
g/kg
,FT
BI
12
Gy
1. 4
22
93
3IV
Exte
nsi
ve1
6m
onth
sB
ron
chio
litis
oblit
eran
s9
46
19
94
CY
12
0m
g/kg
,TH
IOT
EPA
10
mg/
kg2
. 10
44
19
6II
ILi
mit
ed2
0m
onth
s–
10
38
19
95
CY
12
0m
g/kg
,FT
BI
12
Gy
3. 4
02
31
14
IVEx
ten
sive
6m
onth
s–
11
44
19
95
CY
12
0m
g/kg
,VP
16
20
mg/
kg,F
TB
I1
2G
y1
. 38
19
29
IIEx
ten
sive
14
mon
ths
–1
24
41
99
5C
Y1
20
mg/
kg,V
P1
62
0m
g/kg
,FT
BI
12
Gy
2. 9
81
21
2II
Lim
ited
5m
onth
s–
AN
C:a
bsol
ute
neu
trop
hil
cou
nt;
CY:
cycl
oph
osph
amid
e;V
P1
6:et
opos
ide.
1007Allogeneic BMT for AMM
q 1997 Blackwell Science Ltd, British Journal of Haematology 98: 1004–1009
Graft-versus-host diseaseAs presented in Table II, grade II–IV acute GVHD occurred in10 cases, of whom five were severe grade III–IV. Corticoster-oids and anti-thymocyte globulins were used to treat patientswith severe acute GVHD. Two patients, UPN3 and UPN7,died of acute GVHD. Eight patients developed chronic GVHDwhich was extensive in four cases, and responsible for a fatalbronchiolitis obliterans 16 months post-BMT (UPN8).
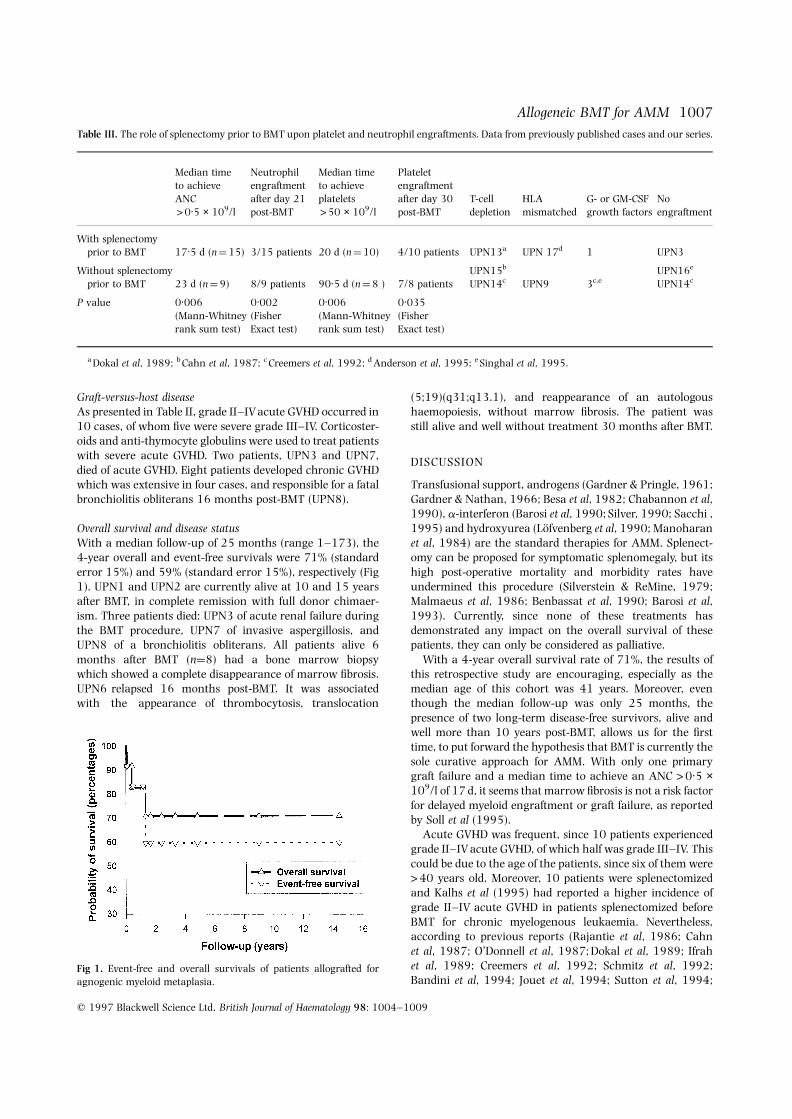
Overall survival and disease statusWith a median follow-up of 25 months (range 1–173), the4-year overall and event-free survivals were 71% (standarderror 15%) and 59% (standard error 15%), respectively (Fig1). UPN1 and UPN2 are currently alive at 10 and 15 yearsafter BMT, in complete remission with full donor chimaer-ism. Three patients died: UPN3 of acute renal failure duringthe BMT procedure, UPN7 of invasive aspergillosis, andUPN8 of a bronchiolitis obliterans. All patients alive 6months after BMT (n¼8) had a bone marrow biopsywhich showed a complete disappearance of marrow fibrosis.UPN6 relapsed 16 months post-BMT. It was associatedwith the appearance of thrombocytosis, translocation
(5;19)(q31;q13.1), and reappearance of an autologoushaemopoiesis, without marrow fibrosis. The patient wasstill alive and well without treatment 30 months after BMT.
DISCUSSION
Transfusional support, androgens (Gardner & Pringle, 1961;Gardner & Nathan, 1966; Besa et al, 1982; Chabannon et al,1990), a-interferon (Barosi et al, 1990; Silver, 1990; Sacchi ,1995) and hydroxyurea (Lofvenberg et al, 1990; Manoharanet al, 1984) are the standard therapies for AMM. Splenect-omy can be proposed for symptomatic splenomegaly, but itshigh post-operative mortality and morbidity rates haveundermined this procedure (Silverstein & ReMine, 1979;Malmaeus et al, 1986; Benbassat et al, 1990; Barosi et al,1993). Currently, since none of these treatments hasdemonstrated any impact on the overall survival of thesepatients, they can only be considered as palliative.
With a 4-year overall survival rate of 71%, the results ofthis retrospective study are encouraging, especially as themedian age of this cohort was 41 years. Moreover, eventhough the median follow-up was only 25 months, thepresence of two long-term disease-free survivors, alive andwell more than 10 years post-BMT, allows us for the firsttime, to put forward the hypothesis that BMT is currently thesole curative approach for AMM. With only one primarygraft failure and a median time to achieve an ANC >0.5 ×109/l of 17 d, it seems that marrow fibrosis is not a risk factorfor delayed myeloid engraftment or graft failure, as reportedby Soll et al (1995).
Acute GVHD was frequent, since 10 patients experiencedgrade II–IV acute GVHD, of which half was grade III–IV. Thiscould be due to the age of the patients, since six of them were>40 years old. Moreover, 10 patients were splenectomizedand Kalhs et al (1995) had reported a higher incidence ofgrade II–IV acute GVHD in patients splenectomized beforeBMT for chronic myelogenous leukaemia. Nevertheless,according to previous reports (Rajantie et al, 1986; Cahnet al, 1987; O’Donnell et al, 1987; Dokal et al, 1989; Ifrahet al, 1989; Creemers et al, 1992; Schmitz et al, 1992;Bandini et al, 1994; Jouet et al, 1994; Sutton et al, 1994;
Fig 1. Event-free and overall survivals of patients allografted foragnogenic myeloid metaplasia.
Table III. The role of splenectomy prior to BMT upon platelet and neutrophil engraftments. Data from previously published cases and our series.
Median time Neutrophil Median time Plateletto achieve engraftment to achieve engraftmentANC after day 21 platelets after day 30 T-cell HLA G- or GM-CSF No>0.5 × 109/l post-BMT >50 × 109/l post-BMT depletion mismatched growth factors engraftment
With splenectomyprior to BMT 17.5 d (n ¼ 15) 3/15 patients 20 d (n ¼ 10) 4/10 patients UPN13a UPN 17d 1 UPN3
Without splenectomy UPN15b UPN16e
prior to BMT 23 d (n ¼ 9) 8/9 patients 90.5 d (n ¼ 8 ) 7/8 patients UPN14c UPN9 3c,e UPN14c
P value 0.006 0.002 0.006 0.035(Mann-Whitney (Fisher (Mann-Whitney (Fisherrank sum test) Exact test) rank sum test) Exact test)
a Dokal et al, 1989; b Cahn et al, 1987; c Creemers et al, 1992; d Anderson et al, 1995; e Singhal et al, 1995.

Anderson et al, 1995; Singhal et al, 1996) and our data, itseems that splenectomy performed prior to BMT couldenhance platelet and granulocyte engraftments in patientswith AMM (Table III). Furthermore, Schmitz et al (1992)detected persistent malignant cells of recipient origin in thespleen as long as 10 months after BMT, arguing also infavour of splenectomy performed prior to BMT, even if therisk of acute GVHD is increased.
With our series, a total of 33 patients allografted for AMMhas been reported with a median age at BMT of 34 years(median time from diagnosis to BMT 14 months). All thedonors were relatives, three couples of donors/recipientsbeing HLA mismatched, and five patients receiving a T-cell-depleted graft. Engraftment was observed in 29 patients andfour primary graft failures occurred. With a median follow-up of 21 months, 19 patients were in complete remission(relapses n¼4) and 12 patients have died (36%, 95% CI 8%),mainly from the BMT procedure. Finally, even thoughtransplant-related mortality is of major concern for BMT,this unconventional approach, which offers a potential cure,should certainly be considered for occasional patients under50 years when a HLA geno-identical donor exists. Obviously,with such a small series we could not be definite as to whenbone marrow transplantation should be considered in thisdisease. Nevertheless, the use of the prognostic scoreproposed by Dupriez et al will certainly be of importance(Morel et al, 1997), serving as a guideline to choose the besttreatment strategy.
REFERENCES
Anderson, J.E., Appelbaum, F.R., Chauncey, T.R. & Storb, R. (1995)Allogeneic bone marrow transplantation for polycythemia vera,agnogenic myeloid metaplasia, and essential thrombocytosis: aseries of 13 patients. Blood, 86, (Suppl. 1), 388a (abstract 1540).
Bandini, G., Ljungman, P., Arcese, G., Van Rhee, F., Corbett, R. &Patton, W.N., on behalf of the Chronic Leukaemia Working Partyof the EBMT (1994) Allogeneic bone marrow transplantation forprimary myelofibrosis. Bone Marrow Transplantation, 13, 105(abstract 41).
Barosi, G., Ambrosetti, A., Buratti, A., Finelli, C., Liberato, N.L.,Quaglini, S., Ricetti, M.M., Visani, G., Tura, S. & Ascari, E. (1993)Splenectomy for patients with myelofibrosis with myeloid meta-plasia: pretreatment variables and outcome prediction. Leukemia,7, 200–206.
Barosi, G., Liberato, L.N., Costa, A., Buratti, A., Di Dio, F., Salvatore,S. & Ascari, E. (1990) Induction and maintenance alpha-interferon therapy in myelofibrosis with myeloid metaplasia.European Journal of Haematology, 45, (Suppl. 52), 12–14.
Barosi, G., Quaglini, S., Petti, C., Grossi, A., Pogliani, E., Leoni, P.,Rotoli, B., Finelli, C., Foa, P., Ambrosetti, A., Rodeghiero, F.,Centra, A., Gaurnone, R. & Liberato, N.L. (1995) Risk factors forblastic transformation in myelofibrosis with myeloid metaplasia(MMM). Blood, 86, (Suppl. 1), 790a (abstract 3147).
Benbassat, J., Gilon, D. & Penchas, S. (1990) The choice betweensplenectomy and medical treatment in patients with advancedprimary myelofibrosis. American Journal of Haematology, 33, 128–135.
Besa, E.C., Nowell, P.C., Geller, N.L. & Gardner, F.H. (1982) Analysisof the androgen response of 23 patients with primarymyelofibrosis. Cancer, 49, 308–313.
Cahn, J.Y., Plouvier, E., Flesch, M., Carbillet, J.P. & Herve, P. (1987)T-cell-depleted allogeneic bone marrow transplantation in a caseof childhood idiopathic myelofibrosis. Bone Marrow Transplantation,2, 209–211.
Cehrelli, C., Ezdinli, E.Z., Li, C.Y. & Krmpotic, E. (1976) Blastic phaseof primary myelofibrosis simulating malignant lymphoma. Cancer,38, 1297–1305.
Chabannon, C., Pegourie, B., Sotto, J.J. & Hollard, D. (1990) Clinicaland hematological improvement in a patient receiving danazoltherapy for myelofibrosis with myeloid metaplasia. Nouvelle RevueFrancaise d’Hematologie, 32, 165–167.
Creemers, G.J., Lowenberg, B. & Hagenbeek, A. (1992) Allogeneicbone marrow transplantation for primary myelofibrosis. BritishJournal of Haematology, 82, 772–773.
Dameshek, W. (1951) Some speculations on the myeloproliferativesyndromes. Blood, 6, 372–375.
Dokal, I., Jones, L., Deenmamode, M., Lewis, S.M. & Goldman, J.M.(1989) Allogeneic bone marrow transplantation for primarymyelofibrosis. British Journal of Haematology, 71, 158–160.
Dupriez, B., Morel, P., Demory, J.L., Lai, J.L., Simon, M., Plantier, I. &Bauters, F. (1996) Prognostic factors in agnogenic myeloidmetaplasia: a report on 195 cases with a new scoring system.Blood, 88, 1013–1018.
Garcia, S., Miguel, A., Linares, M., Navarro, M. & Colomina, P.(1989) Idiopathic myelofibrosis terminating in erythroleukemia.American Journal of Hematology, 32, 70–71.
Gardner, F.H. & Nathan, D.G. (1966) Androgens and erythropoiesis.III. Further evaluation of testosterone treatment of myelofibrosis.New England Journal of Medicine, 274, 420–426.
Gardner, F.H. & Pringle, J.C., Jr (1961) Androgens and erythropoi-esis. II. Treatment of myeloid metaplasia. New England Journal ofMedicine, 264, 103–111.
Glucksberg, H., Storb, R., Fefer, A., Buckner, C.D., Neiman, P.E., Clift,R.A., Lerner, K.G. & Thomas, E.D. (1974) Clinical manifestationsof graft-versus-host disease in human recipient of marrow fromHLA-matched sibling donors. Transplantation, 18, 295–304.
Hasselbalch, H. (1990) Primary myelofibrosis: a clinical study of 80patients. American Journal of Hematology, 34, 291–300.
Ifrah, N., Gardembas-Pain, M., Hunault, M., Saint-Andre, J.P.,Foussard, C. & Boasson, M. (1989) Allogeneic bone marrowtransplantation for primary myelofibrosis. British Journal ofHaematology, 73, 575–576.
Jouet, J.P., Noel, M.P., Facon, T., Caulier, M.T., Dupriez, B., Gosselin, B.,Clincea, R. & Bauters, F. (1994) BMT in a case of primarymyelofibrosis (PMF). Bone Marrow Transplantation, 13, 105(abstract 42).
Kalhs, P., Schwarzinger, I., Anderson, G., Mori, M., Clift, R.A., Storb,R., Buckner, C.D., Appelbaum, F.R., Hansen, J.A. & Sullivan, K.M.(1995) A retrospective analysis of the long-term effect ofsplenectomy on late infections, graft-versus-host disease, relapse,and survival after allogeneic marrow transplantation for chronicmyelogenous leukemia. Blood, 86, 2028–2032.
Kaplan, E.L. & Meier, P. (1958) Nonparametric estimation fromincomplete observations. Journal of the American StatisticalAssociation, 53, 457–481.
Kimura, A., Kawaishi, K., Nakata, Y., Hyodo, H., Kuramoto, A. &Satow, Y. (1995) Leukemic transformation of primary myelo-fibrosis: immunophenotype, genotype and growth characteristicsof blast cells. Leukemia and Lymphoma, 19, 493–498.
Laszlo, J. (1975) Myeloproliferative disorders (MPD): myelofibrosis,myelosclerosis, extramedullary hematopoiesis, undifferentiatedMPD, and hemorrhagic thrombocythemia. Seminars inHematology, 12, 409–432.
Lofvenberg, E., Wahlin, A., Roos, G. & Ost, A. (1990) Reversal of
q 1997 Blackwell Science Ltd, British Journal of Haematology 98: 1004–1009
1008 Philippe Guardiola et al

1009Allogeneic BMT for AMM
q 1997 Blackwell Science Ltd, British Journal of Haematology 98: 1004–1009
myelofibrosis by hydroxyurea. European Journal of Haematology, 44,33–38.
Malmaeus, J., Akre, T., Adami, H.O. & Hagberg, H. (1986) Earlypostoperative course following elective splenectomy in haemato-logical diseases: a high complication rate in patients withmyeloproliferative disorders. British Journal of Surgery, 73, 720–723.
Manoharan, A. & Pitney, W.R. (1984) Chemotherapy resolvessymptoms and reverses marrow fibrosis in myelofibrosis. Scandi-navian Journal of Haematology, 33, 453–459.
Marcus, R.E., Hibbin, J.A., Matutes, E., Whittle, N., Waterfield, M.D.& Goldman, J.M. (1986) Megakaryoblastic transformation ofmyelofibrosis with expression of the c-sis oncogene. ScandinavianJournal of Haematology, 36, 186–193.
Morel, P., Demory, J.L. & Dupriez, B. (1997) Relevance of prognosticfeatures in myeloid metaplasia to selection of patients for bonemarrow transplantation. Blood, 89, 2219–2220.
Nakai, G.S., Craddock, C.G. & Figueroa, W.G. (1962) Primarymyelofibrosis: a survey of twenty-nine cases and a review of theliterature. Annals of Internal Medicine, 57, 419–440.
O’Donnell, M.R., Nademanee, A.P., Snyder, D.S., Schmidt, G.M.,Parker, P.M., Bierman, P.J., Fahey, J.L., Stein, A.S., Krance, R.A.,Stock, A.D., Forman, S.J. & Blume, K.G. (1987) Bone marrowtransplantation for myelodysplastic and myeloproliferativesyndromes. Journal of Clinical Oncology, 5, 1822–1826.
Pitcock, J.A., Reinhard, E.H., Justus, B.W. & Mendelsohn, R.S. (1962)A clinical and pathological study of seventy cases of myelofibrosis.Annals of Internal Medicine, 57, 73–85.
Rajantie, J., Sale, G.E., Deeg, H.J., Amos, D., Appelbaum, F., Storb, R.,Clift, R.A. & Buckner, C.D. (1986) Adverse effect of severe marrowfibrosis on hematologic recovery after chemoradiotherapy andallogeneic bone marrow transplantation. Blood, 67, 1693–1697.
Rosenthal, D.S. & Moloney, W.C. (1977) Occurrence of acuteleukaemia in myeloproliferative disorders. British Journal ofHaematology, 36, 373–382.
Sacchi, S. (1995) The role of a-interferon in essential thrombo-cythaemia, polycythaemia vera and myelofibrosis with myeloidmetaplasia (MMM): a concise update. Leukemia and Lymphoma, 19,13–20.
Schmitz, N., Suttorp, M., Schlegelberger, B., Weber-Matthiesen, K.,Tiemann, M. & Sonnen, R. (1992) The role of the spleen after bone
marrow transplantation for primary myelofibrosis. British Journalof Haematology, 81, 616–618.
Silver, R.T. (1990) Interferons in the treatment of myeloproliferativediseases. Seminars in Hematology, 27, (Suppl. 4), 6–14.
Silverstein, M.N. & ReMine, W.H. (1979) Splenectomy in myeloidmetaplasia. Blood, 53, 515–518.
Singhal, S., Powles, R., Treleaven, J., Pollard, C., Lumley, H. &Mehta, J. (1995) Allogeneic bone marrow transplantation forprimary myelofibrosis. Bone Marrow Transplantation, 16, 743–746.
Soll, E., Massumoto, C., Clift, R.A., Buckner, C.D., Appelbaum, F.R.,Storb, R., Sale, G., Hackman, R. & Martin, P. (1995) Relevance ofmarrow fibrosis in bone marrow transplantation: a retrospectiveanalysis of engraftment. Blood, 86, 4667–4673.
Sultan, C., Scoazec, J.Y. & Imbert, M. (1991) Histopathologie de laMoelle Osseuse, pp. 74–78. Masson, Paris.
Sutton, L., Soussain, S., Travade, P., Binet, J.L. & Leblond, V. (1994)Unusual rise of peripheral blood erythroblasts, preceding neu-trophil recovery after allogeneic BMT for primitive myelofibrosiswith myeloid metaplasia. Bone Marrow Transplantation, 13, 104.
Thiele, J., Kvasnicka, H.M., Steinberg, T., Zankovich, R., Fischer, R. &Diehl, V. (1992) Survival in primary (primary) osteomyelofibrosis,so-called primary myelofibrosis. Leukemia and Lymphoma, 6, 389–399.
Thomas, E.D., Storb, R., Clift, R.A., Fefer, A., Johnson, F.L., Neimann,P.E., Lerner, K.G., Glucksberg, H. & Buckner, C.D. (1975) Bone-marrow transplantation. New England Journal of Medicine, 292,832–843.
Varki, A., Lottenberg, R., Griffith, R. & Reinhard, E. (1983) Thesyndrome of primary myelofibrosis: a clinicopathologic reviewwith emphasis on the prognostic variables predicting survival.Medicine, 62, 353–371.
Visani, G., Finelli, G., Castelli, U., Petti, M.C., Ricci, N., Vianelli, N.,Gianni, L., Zuffa, E., Aloe Spiriti, M.A., Latagliata, R., Pileri, S.,Magrini, U., Gugliota, L., Morra, E., Bernasconi, C., Mandelli, F. &Tura, S. (1990) Myelofibrosis with myeloid metaplasia: clinicaland haematological parameters predicting survival in a series of133 patients. British Journal of Haematology, 75, 4–9.
Ward, H.P. & Block, M.H. (1971) The natural history of primarymyelofibrosis (AMM) and a critical evaluation of its relationshipwith the myeloproliferative syndrome. Medicine, 50, 357–420.





























