Embed Size (px)
Citation preview

www.elsevier.com/locate/clinbiomech
Clinical Biomechanics 19 (2004) 44–49
Alterations in lower extremity movement and muscleactivation patterns in individuals with knee osteoarthritis
John D. Childs *, Patrick J. Sparto, G. Kelley Fitzgerald, Mario Bizzini, James J. Irrgang
Department of Physical Therapy, School of Health and Rehabilitation Sciences, University of Pittsburgh, Pittsburgh PA, USA
Received 24 February 2003; accepted 15 August 2003
Abstract
Objective. The purpose of this study was to investigate lower extremity movement and muscle activation patterns in individuals
with knee osteoarthritis and healthy age- and gender-matched control subjects.
Design. This study utilized a non-randomized case-control design to compare 24 subjects with unilateral symptomatic knee
osteoarthritis to 24 age- and gender-matched control subjects without knee osteoarthritis.
Background. It is hypothesized that knee osteoarthritis is associated with altered lower extremity movement and muscle acti-
vation patterns.
Methods. A gait analysis was performed to determine the lower extremity movement and muscle activation patterns when
walking on a level surface at 1.12 to 1.34 m/s and while descending a 20 cm step. Paired t-tests were used to compare the average offive trials between the groups.
Results. Subjects with knee osteoarthritis demonstrated less excursion of the knee in the sagittal plane from heelstrike to peak
flexion before midstance (i.e. during loading). Subjects with knee osteoarthritis also demonstrated reduced peak vertical ground
reaction forces relative to body weight. The muscle activity patterns were also different between the groups. The vastus lateralis,
medial hamstrings, tibialis anterior and medial gastrocnemius were on approximately 1.5 times longer than the same muscles in the
control subjects. Additionally, significant increases in muscle co-activation were also observed in individuals with knee osteoarthritis
during walking. Similar findings were observed when the subject descended a 20 cm step.
Relevance
Individuals with knee osteoarthritis utilize different movement and muscle activation patterns when walking and descending a
step. The alterations may interfere with the knee’s ability to dissipate loads, which could lead to progression of the disease.
Published by Elsevier Ltd.
Keywords: Kinematics; Loading; Knee; Osteoarthritis; Gait
1. Introduction
Knee osteoarthritis (OA) is a prevalent condition that
contributes significantly to functional limitations and
disability (van Baar et al., 1998). Common alterations in
gait observed in individuals with knee OA have been
described and include decreased knee excursion (Messier
et al., 1992), altered ground reaction force (Gyory et al.,
1976), and altered muscle activity patterns of key lower
extremity muscles involved in gait (Benedetti et al., 1999;
* Corresponding author. Address: 508 Thurber Drive, Schertz, TX
78154-1146, USA.
E-mail address: [email protected] (J.D. Childs).
0268-0033/$ - see front matter Published by Elsevier Ltd.
doi:10.1016/j.clinbiomech.2003.08.007
Suzuki and Takahama, 1979). While these alterations
are believed to be attempts to reduce pain and protectthe knee from further degeneration, over the long term,
they may have adverse effects on the knee joint.
In general, studies assessing kinematics during gait in
individuals with knee OA have demonstrated decreased
excursion of the knee during the stance and swing
phases of gait (Messier et al., 1992). However, these
results must be interpreted cautiously. Brinkmann and
Perry (1985) compared individuals with knee OA toyounger controls who walked at a much faster velocity.
Gyory et al. (1976) allowed some subjects to use assistive
devices, and they did not control velocity. Messier et al.
(1992) controlled gait velocity and found only a 3� dif-ference in total excursion of the knee. Studies investigating

J.D. Childs et al. / Clinical Biomechanics 19 (2004) 44–49 45
the kinetics of gait are also conflicting. Some have re-ported increased ground reaction forces (Radin et al.,
1991), while others have reported similar (Messier et al.,
1992) or decreased (Gyory et al., 1976) ground reactions
forces in patients with knee OA compared to healthy
control subjects.
To facilitate interpretation of these findings, it would
be helpful to understand the muscle activity of key lower
extremity muscles during gait. However, there is limiteddata in the literature that suggests there is altered muscle
activity during gait in individuals with knee OA
(Benedetti et al., 1999). Suzuki and Takahama (1979)
demonstrated increased activity of the quadriceps and
hamstrings during the stance phase of gait. There is also
data to suggest that individuals with knee OA may
utilize increased co-activation patterns (i.e. ‘‘co-con-
traction’’) between antagonistic muscle pairs duringweight bearing (Benedetti et al., 1999). Additional re-
search is needed to clarify the timing and magnitude of
lower extremity muscle activity during gait in this pop-
ulation. To date, this information has not been reported
in the literature for individuals with unilateral symp-
tomatic knee OA compared to age- and gender-matched
control subjects that do not have symptomatic or ra-
diographic evidence of OA.Research related to gait in individuals with knee OA
has been conducted under a variety of conditions that
frequently do not control for potential confounding
factors such as age (Brinkmann and Perry, 1985), gait
velocity (Brinkmann and Perry, 1985), and the use of
assistive devices (Gyory et al., 1976). For example,
controlling for gait velocity has been recommended and
utilized by researchers to account for potential differ-ences in range of motion and vertical ground reaction
forces that could simply be attributed to differences in
self-selected velocity between those with knee OA and
those without (Messier et al., 1992). The variety of
testing conditions makes comparisons between studies
problematic and likely contributes to the conflicting
findings between studies. Therefore the purpose of this
study was to concomitantly investigate lower extremitysagittal kinematics, kinetics and muscle activation pat-
terns in individuals with knee OA and healthy age- and
gender-matched control subjects during two functional
activities, walking on a level surface and negotiating a
step 20 cm in height. An improved understanding of the
alterations during gait in individuals with knee OA may
lead to the development of more effective rehabilitation
strategies.
2. Methods
This study utilized a non-randomized case-control
design to compare the gait characteristics of 24 subjects
with unilateral symptomatic knee OA to 24 age- and
gender-matched control subjects without knee OA. Thedata were collected as part of a pilot study to determine
important sagittal kinematic, kinetic and electromyog-
raphy variables that distinguish subjects with OA from
healthy controls when walking at a controlled speed on
a level surface and when descending a 20 cm step.
3. Subjects
Subjects with OA consisted of volunteers, 62 (47–78)
years of age (56% female). Subjects were previously di-
agnosed with unilateral knee OA involving the tibio-
femoral and/or patellofemoral compartments. All subjects
signed an informed consent document approved by the
University of Pittsburgh Institutional Review Board for
Biomedical Research prior to participating in the study.Subjects were included if they were at least 40 years of
age, met the 1986 American College of Rheumatology
clinical and radiographic criteria for knee OA (Altman
et al., 1986), and had grade II or greater Kellgren and
Lawrence radiographic changes on the symptomatic side
(Kellgren and Lawrence, 1957). Subjects with knee OA
were allowed to have bilateral radiographic evidence of
knee OA so long as their symptoms were unilateral.Subjects with knee OA were excluded if they: (1) were
unable to safely walk distances greater than 200 feet
without the use of assistive devices; (2) had a history of a
ligament injury of the involved knee, (3) had symp-
tomatic knee OA of the uninvolved knee or (4) had
undergone total knee arthroplasty.
Control subjects consisted of healthy age- and gen-
der-matched individuals, 62 (47–78) years of age (56%female), who: (1) had no history of knee OA or other
pathology involving the knees or other joints of the
lower extremity; and (2) did not have greater than Grade
I Kellgren and Lawrence radiographic changes of either
knee. Subjects in either group who had uncontrolled
hypertension, a history of cardiovascular disease, were
pregnant, or were cognitively impaired to the extent they
could not understand the instructions for the testingprocedures were also excluded. Demographic charac-
teristics, key clinical findings, and self-report measures
of function for both groups are listed in Table 1. These
include range of motion of the knee, quadriceps strength
expressed as a percentage of body mass index, an 11-
point numeric pain rating scale (Downie et al., 1978),
the Activities of Daily Scale (ADLS) of the Knee Out-
comes Survey score (Irrgang et al., 1998), and theWestern Ontario and McMaster Universities (WO-
MAC) Osteoarthritis Index score (Bellamy et al., 1988).
Subjects with knee OA had greater mass and body mass
index and significantly less range of motion and quad-
riceps strength. In addition, they had significantly
greater pain and WOMAC scores and lower ADLS
scores. The number of subjects with medial, lateral, and

Table 1
Descriptive statistics (mean (SD)) of knee OA and control subjects
Knee OA ðn ¼ 24Þ Controls ðn ¼ 24Þ p-value
Age (years) 62 (10) 62 (10) 0.366
Gender (percent female) 56% 56% n/a
Height (cm) 167 (14) 166 (8) 0.372
Mass (kg) 84 (24) 74 (16) 0.046
Body Mass Index (kg/m2) 30 (7) 27 (6) 0.033
Knee extension (degree): A negative sign corresponds to hyperextension. 6 (4.4) )1.7 (3) <0.001
Knee flexion (degree) 125 (10) 138 (6) <0.001
Total knee range of motion (degree) 119 (13) 139 (8) <0.001
Knee extensor strength (Nm/BMI) 5.2 (1.9) 7.0 (1.9) <0.001
NPRSa (average of best, worst, and current levels of pain over a 24-hour period) 2.1 (1.3) 0 (0) <0.001
ADLSb 70.1 (16) 99.8 (1) <0.001
WOMACc 24.6 (15) 0.3 (1) <0.001
aNumeric pain rating scale.bActivities of daily living scale of knee outcome survey (higher scores indicate higher levels of function).cWestern Ontario and McMasters University Osteoarthritis Index (lower scores indicate lower levels of disability).
Table 2
Summary of radiographic findings in subjects with knee OA
No. of
subjects
ðn ¼ 24ÞIsolated medial compartment knee OA 12
Medial and patellofemoral compartment knee OA 9
Lateral and patellofemoral compartment knee OA 2
Tri-compartmental knee OA 1
46 J.D. Childs et al. / Clinical Biomechanics 19 (2004) 44–49
patellofemoral compartment knee OA is summarized in
Table 2.
4. Equipment
A gait analysis was performed to determine the knee
excursion range of motion, ground reaction force, andmuscle activity patterns when walking on a level surface
and while descending a step 20 cm in height. A 20 cm
step was chosen because it is the height of a normal step
in the United States. Knee excursion was measured us-
ing an electromagnetic motion analysis system (Motion
Monitor, Innovative Sports Training Inc., Chicago, IL,
USA). Ground reaction force data were obtained using
a six degrees-of-freedom force platform (AdvancedMechanical Technology Inc., Newton, MA, USA). A
surface electromyography (sEMG) recording system
(Bagnoli-2 EMG, Delsys Inc., Boston, MA, USA) was
used to measure activity of the vastus lateralis, medial
hamstrings, tibialis anterior, and medial gastrocnemius.
Angular position of the knee was sampled at 50 Hz and
ground reaction force and surface electromyography
data were sampled at 1000 Hz.
5. Testing procedures
Subjects wore comfortable walking shoes, with the
restriction that the shoes did not have a heel height
greater than 1 in. Electromagnetic sensors were placed
using neoprene cuffs around the shanks and thighs. The
cuffs have connectors that firmly attach the sensor to the
body segment and are designed to minimize movementbetween the sensor and body segment. The primary axis
of the electromagnetic sensor was aligned with the long
axis of the respective body segment. Prior to application
of the sEMG electrodes, the hair underlying the elec-
trodes was removed using a standard disposable safety
razor, and the skin was cleansed with rubbing alcohol.
Surface electromyography electrodes were placed over
the vastus lateralis, medial hamstrings, tibialis anterior,and medial gastrocnemius muscles. The electrodes were
oriented on the center of the muscle belly in a longitu-
dinal fashion in the direction of the muscle fibers.
Placement of the electrode was facilitated by palpat-
ing the muscle as the subject contracted the muscle
against resistance. Additionally accurate placement of
the electrode was verified during the normalization
process. If a good signal was not obtained when theindividual performed a maximal isometric contraction
of the muscle, then the electrode was repositioned.
A reference electrode was placed over the head of the
fibula.
Subjects were required to walk along a level surface
approximately 3.7 m in length at a velocity ranging from
1.12 to 1.34 m/s, which is considered to be the normal
walking velocity for individuals in the age group thatwas enrolled in this study (Murray et al., 1970). Gait
velocity was controlled by the use of two infrared sig-
nals, one placed before and after the force platform.
Subjects were instructed to strike the force platform with
their involved side. For control subjects, the side used
for comparison was determined a priori by the involved
side of the subject with knee OA with whom the control
subject was matched. Data were collected over five validtrials. A valid trial was defined as one in which the
subject struck the force platform with the involved ex-
tremity at the required velocity without adjusting his/her
J.D. Childs et al. / Clinical Biomechanics 19 (2004) 44–49 47
stride length. With practice, subjects rarely had tocomplete more than 2–3 additional trials.
Subjects also descended a step 20 cm in height. From
a level surface standing next to the step, the subject was
asked to step up on the step with the asymptomatic
extremity and then step down onto the force platform
with the symptomatic extremity. After stepping down,
the subject continued to walk forward several steps.
Subjects performed five repetitions of this activity anddid not use a handrail or any other device to assist ne-
gotiation of the stair. Subjects were permitted to per-
form 1–2 practice trials to insure they understood the
instructions and initiated the task with the appropriate
foot.
6. Data management and analysis
The knee flexion/extension angle, and ground reac-
tion force data were smoothed using a zero-lag Butter-
worth lowpass filter. The magnitude of the ground
reaction forces was normalized by body weight. The
sEMG were smoothed using a moving root-mean-
square (RMS) filter with a 25 ms window. To facilitate
comparison between groups, the sEMG was normalizedto the mean of the RMS values obtained during three 3-s
maximum voluntary isometric contractions of each of
the muscles (Rudolph et al., 2000).
The data from each of the five valid trials were nor-
malized in time to the duration of stance phase. Fur-
thermore, onset and offset times of the muscle activity
were determined without normalization to time by vi-
sually identifying the time when the sEMG had a phasicincrease in activation above baseline. The amount of
muscle co-activation between antagonistic muscle pairs
in the lower extremity (vastus lateralis vs. medial ham-
strings and anterior tibialis vs. gastrocnemius muscles)
Table 3
Summary of the alterations in knee kinematics and vertical ground reaction
Walking task
OA C
Kinematic parameters (units)
Knee angle at initial contact (degree) 4.5 (4.5) 1
Knee flexion excursion during loading response phase
(heelstrike to peak flexion before midstance) (degree)
15.7 (5.7) 1
Time to peak during loading response phase (%stance) 27.9 (4.9) 2
Kinetic parameters (units)
Loading rate to 1st peak of vertical ground reaction
force (%/s)
650 (170) 7
Maximum vertical ground reaction force during loading
(% body weight)
106 (12) 1
Maximum vertical ground reaction force during pushoff
(% body weight)
104 (7) 1
All values represent parameters during the stance phase of gait––mean (SD)
was determined using the method of Rudolph et al.(2000)
ðEMGL þ EMGMÞ � EMGL=EMGM;
where EMGL is the level of activity in the less active
muscle and EMGM is the level of activity in the moreactive muscle. Muscle co-activation was averaged over
the stance phase, and the mean value from the five trials
was calculated. For all dependent measures, paired t-tests were used to compare the average of five trials
between the involved limb of the knee OA subject and
the same side limb of the matched control subject
(Portney and Watkins, 2000). Because this study was
exploratory in nature, the alpha-level was not adjusteddownwards to control for the Type-I error rate.
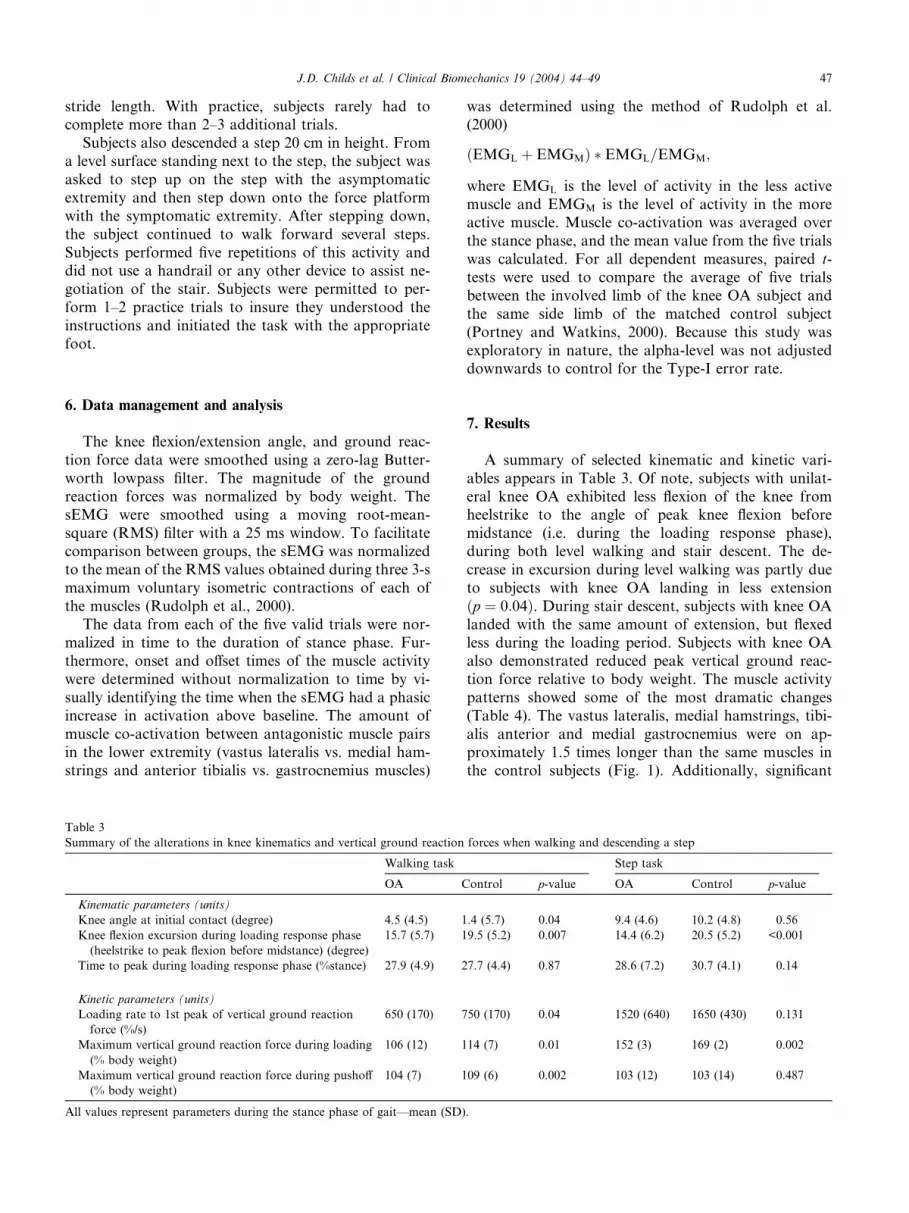
7. Results
A summary of selected kinematic and kinetic vari-
ables appears in Table 3. Of note, subjects with unilat-
eral knee OA exhibited less flexion of the knee fromheelstrike to the angle of peak knee flexion before
midstance (i.e. during the loading response phase),
during both level walking and stair descent. The de-
crease in excursion during level walking was partly due
to subjects with knee OA landing in less extension
ðp ¼ 0:04Þ. During stair descent, subjects with knee OAlanded with the same amount of extension, but flexed
less during the loading period. Subjects with knee OAalso demonstrated reduced peak vertical ground reac-
tion force relative to body weight. The muscle activity
patterns showed some of the most dramatic changes
(Table 4). The vastus lateralis, medial hamstrings, tibi-
alis anterior and medial gastrocnemius were on ap-
proximately 1.5 times longer than the same muscles in
the control subjects (Fig. 1). Additionally, significant
forces when walking and descending a step
Step task
ontrol p-value OA Control p-value
.4 (5.7) 0.04 9.4 (4.6) 10.2 (4.8) 0.56
9.5 (5.2) 0.007 14.4 (6.2) 20.5 (5.2) <0.001
7.7 (4.4) 0.87 28.6 (7.2) 30.7 (4.1) 0.14
50 (170) 0.04 1520 (640) 1650 (430) 0.131
14 (7) 0.01 152 (3) 169 (2) 0.002
09 (6) 0.002 103 (12) 103 (14) 0.487
.

Table 4
Summary of the alterations in muscle activation patterns when walking and negotiating a step
Walking task Step task
OA Control p-value OA Control p-value
Duration of muscle activity
Vastus lateralis (ms) 447 (187) 282 (84) <0.001 469 (202) 299 (95) <0.001
Hamstrings (ms) 417 (130) 250 (106) <0.001 343 (134) 182 (53) <0.001
Tibialis anterior (ms) 382 (107) 224 (60) <0.001 407 (181) 174 (79) <0.001
Gastrocnemius (ms) 502 (156) 362 (128) <0.001 492 (122) 319 (90) <0.001
Muscle co-activation
Vastus lateralis-hamstrings (%) 28 (25) 15 (9) 0.03 24 (22) 15 (12) 0.07
Tibialis anterior-gastrocnemius (%) 20 (11) 11 (5) <0.01 20 (15) 12 (5) 0.05
All values represent parameters during the stance phase of gait––mean (SD).
Muscle coactivation¼ (EMGL +EMGM) *EMGL/EMGM, where EMGL is the average level of activity in the less active muscle during stance phase
and EMGM is the average level of activity in the more active muscle during stance phase.
-400 -200 0 200 400 600 800Time (ms), where 0 = Heelstrike
Vastus lateralis
Hamstrings
Tibialis anterior
Gastrocnemius
Control
Knee OA
Fig. 1. Duration of muscle activity in subjects with knee OA vs. con-
trols during walking task.
48 J.D. Childs et al. / Clinical Biomechanics 19 (2004) 44–49
increases in muscle co-activation were also observed in
individuals with knee OA during walking. Similar find-
ings were observed during the step task.
8. Discussion
These results indicate that individuals with knee OA
utilize different movement and muscle activation pat-
terns when walking and negotiating a step compared to
healthy age- and gender-matched control subjects
without knee OA. Our results confirm and clarify someof the previous research that has assessed gait parame-
ters in individuals with knee OA. Compared to healthy
control subjects, individuals with knee OA exhibit a
decreased excursion of flexion of the knee during the
loading response phase of gait (Messier et al., 1992). In
our study, during the loading response phase of gait,
individuals with knee OA exhibited approximately 4–6�less flexion of the knee compared to age- and gender-matched control subjects (Table 3). During level walk-
ing, the decrease in excursion could be explained by
subjects with knee OA landing with the knee flexed.
These changes are consistent with the decreased knee
extension range of motion that is observed clinically inthe subjects with knee OA (Table 1). Future work will be
directed at more fully exploring the relationships be-
tween impairments and function of the knee during gait.
Reduced knee flexion excursion combined with in-
creased muscle co-activation during the loading re-
sponse phase of gait may represent a stiffening of the
joint. The combination of these two factors may lead to
increased compressive loading and reduce the potentialfemoral contact area over which the force can be dis-
tributed, which may in turn contribute to increased cu-
mulative loading in localized areas.
Subjects with knee OA in our study demonstrated an
increased duration of muscle activity during stance for
all four lower extremity muscles that were assessed dur-
ing both the walking and step tasks. Fig. 1 illustrates this
finding during the walking task for all muscle groups. Weobserved that the muscles of the subjects with knee OA
turn on sooner and turn off later than the same muscles
of the control subjects. In addition, significant increased
co-activation of antagonistic muscle pairs in the lower
extremity was observed between the vastus lateralis and
hamstrings and between the anterior tibialis and gas-
trocnemius muscles during walking. The results of our
study support the findings of previous studies thatdemonstrated increased muscle activity and the possi-
bility of increased co-activation of antagonistic muscle
pairs in key lower extremity muscles during gait in in-
dividuals with knee OA (Benedetti et al., 1999). Future
studies should concomitantly investigate movement and
muscle activation patterns in the frontal and transverse
planes and address the mechanism for the increased
muscle activity observed in the subjects with knee OA.Additionally, it is possible that a different step height
could alter the amount of knee motion needed to ne-
gotiate a step depending on the subject’s height, which
could in turn alter muscle activity patterns and perhaps
loading upon landing. However, a 20 cm step is the
height of a normal step in the United States, and no

J.D. Childs et al. / Clinical Biomechanics 19 (2004) 44–49 49
differences in height of the subjects were observed be-tween the groups ðp ¼ 0:37Þ (Table 1).Decreased excursion of the knee combined with in-
creased muscle co-activation and duration of muscle
activity may represent an attempt to avoid pain and/or
stabilize the knee during the loading response phase of
gait. Although we did not have a measure of load dis-
tribution (which is difficult to measure experimentally), it
is possible these alterations may act to stiffen the knee,thus increasing compressive loads across the knee. This
may make the knee less capable of dissipating potentially
harmful loads, increasing susceptibility of the knee to the
development and progression of the disease. If this is the
case, rehabilitation strategies that increase knee excur-
sion and decrease muscle co-activation patterns may
need to be developed to maximize the effectiveness of
rehabilitation that is traditionally focused on quadricepsstrengthening. Although the preliminary results of this
study are encouraging, future work is currently being
conducted to investigate the implications of our findings
on the rehabilitation of patients with knee OA.
Acknowledgements
The authors would like to acknowledge Dr. Chris
Harner from the University of Pittsburgh Medical
Center (UPMC) Health System’s Center for Sports
Medicine for referring patients as potential subjects for
this study. The authors would also like to acknowledgeDr. Chester W. Oddis from the UPMC Department of
Rheumatology for interpreting the radiographs that
were performed in this study.
This study was supported in part by a grant from the
Orthopaedic Physical Therapy Section of the American
Physical Therapy Association, Inc. and by a scholarship
from the Foundation for Physical Therapy, Inc.
The opinions or assertions contained herein are theprivate views of the authors and are not to be construed
as official or as reflecting the views of the U.S. Air Force
or Department of Defense.
References
Altman, R., Asch, E., Bloch, D., et al., 1986. Development of criteria
for the classification and reporting of osteoarthritis. Classification
of osteoarthritis of the knee. Diagnostic and Therapeutic Criteria
Committee of the American Rheumatism Association. Arthritis
Rheum 29, 1039–1049.
Bellamy, N., Buchanan, W.W., Goldsmith, C.H., et al., 1988.
Validation study of WOMAC: a health status instrument for
measuring clinically important patient relevant outcomes to
antirheumatic drug therapy in patients with osteoarthritis of the
hip or knee. J. Rheumatol. 15, 1833–1840.
Benedetti, M.G., Bonato, P., Catani, F., et al., 1999. Myoelectric
activation pattern during gait in total knee replacement: relation-
ship with kinematics, kinetics, and clinical outcome. IEEE Trans.
Rehabil. Eng. 7, 140–149.
Brinkmann, J.R., Perry, J., 1985. Rate and range of knee motion
during ambulation in healthy and arthritic subjects. Phys. Ther. 65,
1055–1060.
Downie, W.W., Leatham, P.A., Rhind, V.M., et al., 1978. Studies with
pain rating scales. Ann. Rheum. Dis. 37, 378–381.
Gyory, A.N., Chao, E.Y., Stauffer, R.N., 1976. Functional evaluation
of normal and pathologic knees during gait. Arch. Phys. Med.
Rehabil. 57, 571–577.
Irrgang, J.J., Snyder-Mackler, L., Wainner, R.S., et al., 1998.
Development of a patient-reported measure of function of the
knee. J. Bone Joint Surg. Am. 80, 1132–1145.
Kellgren, J.H., Lawrence, J.S., 1957. Radiological assessment of osteo-
arthrosis. Ann. Rheum. Diseases 16, 494–502.
Messier, S.P., Loeser, R.F., Hoover, J.L., et al., 1992. Osteoarthritis of
the knee: effects on gait, strength, and flexibility. Arch. Phys. Med.
Rehabil. 73, 29–36.
Murray, M.P., Kory, R.C., Sepic, S.B., 1970. Walking patterns of
normal women. Arch. Phys. Med. Rehabil. 51, 637–650.
Portney, L.G., Watkins, M.P., 2000. Foundations of Clinical Re-
search: Applications to Practice, second ed. Prentice Hall Health,
Upper Saddle, NJ.
Radin, E.L., Yang, K.H., Riegger, C., et al., 1991. Relationship
between lower limb dynamics and knee joint pain. J. Orthop. Res.
9, 398–405.
Rudolph, K.S., Axe, M.J., Snyder-Mackler, L., 2000. Dynamic
stability after ACL injury: who can hop? Knee. Surg. Sports
Traumatol. Arthrosc. 8, 262–269.
Suzuki, K., Takahama, M., 1979. Gait patterns of the diseased knee
joint. Nippon Seikeigeka Gakkai Zasshi 53, 847–853.
van Baar, M.E., Dekker, J., Lemmens, J.A., et al., 1998. Pain and
disability in patients with osteoarthritis of hip or knee: the
relationship with articular, kinesiological, and psychological char-
acteristics. J. Rheumatol. 25, 125–133.





























