Embed Size (px)
Citation preview

JAP-00368-2002.R2
Time course of hemorheological alterations following heavy
anaerobic exercise in untrained human subjects
1Ozlem Yalcın, 2Alpaslan Erman, 2Sedat Muratli, 1Melek Bor-Kucukatay and
1Oguz K. Baskurt
1Department of Physiology, Akdeniz University School of Medicine, Antalya, Turkey
and 2School of Physical Education and Sports, Akdeniz University, Antalya, Turkey
Running head
Time course of hemorheology after heavy exercise
Contact information
Oguz K. Baskurt
Department of Physiology
Akdeniz University School of Medicine
Antalya Turkey
E mail: [email protected]
Keywords
Hemorheology, anaerobic exercise, Wingate test
Copyright 2002 by the American Physiological Society.
J Appl Physiol Articles in PresS. Published on October 18, 2002 as DOI 10.1152/japplphysiol.00368.2002

JAP-00368-2002.R2
ABSTRACT
The time course of hemorheological alterations was investigated following
heavy anaerobic exercise in untrained male human subjects. The Wingate protocol
was performed by each subject, and blood lactate, red blood cell (RBC) deformability
and aggregation, white blood cell (WBC) activation, and several hematological
parameters were investigated during 24 hours following the exercise and compared
with pre-exercise values. Compared to the pre-exercise value, blood lactate level was
found to be ~10 fold higher immediately after the exercise. There was a transient,
significant increment of RBC and WBC counts immediately after exercise that was
followed by a decrement of RBC count. There was a second increase of WBC count,
accompanied with increased percentages of granulocytes and granulocyte activation,
starting 45 minutes after exercise. RBC deformability was found to be impaired
immediately after exercise and remained reduced for at least 12 hours; RBC
aggregation was also found to be decreased following exercise, with the onset of this
decrease delayed by 30 minutes. The results of this study indicate that a single bout
of heavy anaerobic exercise may induce significant hemorheological deterioration
lasting for up to 12 hours, and thus suggest the need to consider such effects in
individuals with impaired cardiovascular function.

JAP-00368-2002.R2
INTRODUCTION
Exercise may induce sudden death in both sportsman and sedentary people
(1,17,23,26), and such events have been reported among all age groups (e.g.,
children, young adults, mid-age groups, elderly) (1,23,33). Sudden deaths have
been reported during both early and late stages of exercise or after exercise
(1,2,21,23), and Albert et al. accepted sudden death events that occurred within 30
minutes after exercise as “exercise-related” (1). Some of these events could be
related to underlying diseases (e.g., cardiovascular), yet in some situations post-
mortem examinations failed to reveal findings specific to the cause of such deaths
(15,23,29). Nevertheless, exercise-related sudden deaths are usually reported as
cardiovascular events (23,33,39), with arrhythmias, myocardial ischemia and/or
infarction, and other vascular problems (e.g., atherosclerotic blood vessels,
microcirculatory problems) the most frequent manifestations of these events
(29,32,39).
Tissue perfusion problems might be encountered, even without total occlusion
of blood vessels, if blood flow to a given tissue cannot balance tissue demands. For
example, hemodynamic and cardiac alterations during strenuous exercise may
enormously increase the oxygen demand of myocardium, yet the magnitude of blood
flow that can be supplied by a given vessel geometry cannot match this demand
despite the increased blood pressure; impaired perfusion even though the same
coronaries can easily satisfy the circulatory demand at rest. Note that during

JAP-00368-2002.R2
strenuous exercise, it can be assumed that the autoregulatory reserve of the
coronary circulation is fully utilized (i.e., resistance vessels are maximally dilated due
to metabolic vasodilators) and that any increment in blood viscosity may further
decrease blood flow.
Heavy exercise has been reported to induce acute significant alterations in
blood composition and rheology (8,31,38), with the effects of exercise on blood
rheology dependent on the type, duration and intensity of exercise, and the athletic
capacity of the individual also plays a significant role. In most studies on untrained
individuals the acute effect of exercise was found to be decreased blood fluidity
(8,31,41). The fluidity of blood is determined by its composition (plasma protein
levels, hematocrit) and the rheological properties of blood cells, especially RBC;
since it is a shear-thinning, non-Newtonian fluid, blood fluidity is also affected by flow
conditions. Hence increased blood pressure and the resulting increase of flow and
shear forces during strenuous exercise may compensate for any deterioration in
blood fluidity. However, immediately after the cessation of exercise hemodynamic
factors return to resting levels, thereby normalizing the shear forces; hemorheological
alterations that continue to exist after this hemodynamic normalization may contribute
to tissue perfusion problems.
Although hemorheological alterations induced by various exercise models
have been reported, the time course of these alterations has not been investigated in
detail. In particular, most studies have focused upon the immediate effects noted
following cessation of exercise. However, it can be hypothesized that
hemorheological alterations may continue for prolonged periods after exercise, and

JAP-00368-2002.R2
may thus could have adverse effects well-past the acute event. This study was thus
designed to test this hypothesis by investigating the time course of hemorheological
and related hematological alterations following heavy anaerobic exercise in
sedentary male adults.
MATERIALS AND METHODS
Subjects
Ten apparently healthy male volunteers, 20-36 years of age, were included in
the study; the subjects were non-smokers and were not exercising regularly. The
experimental procedures were explained to all subjects and their written consents to
participate in the study were obtained. The subjects were asked to have a light,
standard breakfast in the morning of the day of the experiment, then to report to the
exercise laboratory at 9.00 AM. Their body fat was estimated by bio-impedance
method using TANITA Body Composition Analyzer (TANITA Corporation of America,
Inc., Illinois, USA), following which they carried out the exercise protocol described
below.
Exercise protocol
A standard period of anaerobic exercise, based on the Wingate Anaerobic
Power Test (24), was performed by the subjects at the Akdeniz University Sports
Sciences Research and Application Center. The test was performed on a bicycle
ergometer equipped with an optical sensor enabling computerized monitoring of the
cycling speed. The subjects were asked to warm up for a period of 3 minutes, at 60
rpm speed with a load of 1.5 kg. After the warm up period, the subjects were asked

JAP-00368-2002.R2
to cycle at their maximum speed and to maintain this speed for 30 sec after 75 g/kg
extra loading. The computerized system calculated the maximum speed, the
equivalent distance cycled during the 30 sec period, and power outputs at various
intervals of the test. A fatigue index was also calculated based on the differences in
power output at the start and end of the test period.
Blood sampling
Blood samples were obtained before the start of exercise and repeated at 15
min intervals during the first hour, than at 2, 4, 8, 12 and 24 hours following exercise.
Blood samples were anticoagulated with ethylendiaminetetra- acetic acid (EDTA, 1.5
mg/ml), and all analyses were performed within four hours after blood sampling.
RBC and WBC counts, as well as differential WBC counts, were obtained using an
electronic hematology analyzer (Cell-Dyn 3500R, Abbott Diagnostic Division, USA).
Blood lactate concentration was measured by a lactate analyzer using BM-Lactate
test strips (Accusport, Boehringer Mannheim, Diagnostics & Biochemicals,
Germany).
RBC deformability measurements
RBC deformability (i.e., the ability of the entire cell to adopt a new
configuration when subjected to mechanical forces) was determined, at 37 °C and at
a fluid shear stress of 1.58 Pa, by laser diffraction analysis using an ektacytometer
(LORCA, RR Mechatronics, Hoorn, The Netherlands). This system calculates an
average RBC elongation index (EI), where a higher EI indicates greater cell
deformability (19).
JAP-00368-2002.R2
RBC aggregation measurements
RBC aggregation was assessed using a photometric aggregometer interfaced
to a digital computer (5); this system is based upon the increase of light transmission
through a RBC suspension consequent to aggregation. The system reports a
dimensionless index that increases with increased extent of aggregation.
RBC aggregation was measured for cells in autologous plasma and for cells
re-suspended in isotonic phosphate buffered saline (PBS, 290 mOsm/kg, pH=7.4)
containing 1% dextran 500 (molecular mass 500 kDa, Sigma Chemical Co, St.
Louis, MO, USA). The measurements made using this standard dextran solution
reflect the intrinsic tendency of RBC to aggregate (3). The hematocrit of the samples
used for aggregation measurements was adjusted to 0.4 l/l, with all measurements
done at room temperature (20±2 °C).
Quantitation of granulocyte respiratory burst
Granulocytes were isolated from whole blood using polysucrose density
gradients (Histopaque 1119; Sigma Chemical Co, St. Louis, MO, USA) as described
elsewhere (11). Isolated granulocytes were washed with and then suspended in
PBS at a cell count of of 2.5 x 106 per ml. The granulocyte suspension was then
incubated in the dark, at 37 ºC for 25 min, in the presence of 10-6 mol/L 2′,7′-
Dicholoro-fluorescrein Diacetate (DCF, D-6883; Sigma Chemical Co, St. Louis, MO,
USA). The fluorescence of DCF was determined in granulocyte suspensions (106 per
ml Krebs phosphate buffer) by a spectrofluorometer (Schimadzu RF-5000,
Schimadzu Corporation, Tokyo, Japan) at 485 nm excitation and 510 nm emission

JAP-00368-2002.R2
wavelengths (22), with the intensity of the fluoroscence directly related to the degree
of activation of granulocytes (i.e., granulocyte respiratory burst).
Statistics
Results are expressed as mean ± standard error (SE). Statistical comparisons
between groups were done by "repeated measures ANOVA" followed by "Newman-
Keuls post-hoc test", with p values <0.05 accepted as statistically significant.
RESULTS
The anthropometric parameters of the study group are presented in Table 1.
Body mass index, body fat and lean body mass were within normal limits. During the
performance of the Wingate protocol the average power output was 7.8±0.8 W/kg
and the fatigue index was 45.4±13.1 %.
At the end of the Wingate anaerobic test, blood lactate concentration
increased to a mean value of 10 mmol/L from a pre-exercise value of 0.9 mmol/L
(Table 2). The blood lactate concentration then returned to the pre-exercise level at
120 minutes. The anaerobic exercise period immediately induced a significant, 8-
10% increment in RBC counts which then returned to control at 15 minutes post-
exercise (Figure 1). However, during the later portion of the monitoring period there
was a drop in RBC counts: starting at the second hour after the end of exercise
significant decrements in RBC counts were observed (Figure 1). Mean corpuscular
volume was 87.7±1.2 fL before the exercise and no significant alterations were
observed during the followup period.

JAP-00368-2002.R2
RBC deformability was found to be significantly reduced immediately after the
anaerobic exercise episode and for 12 hours following exercise, then to return to
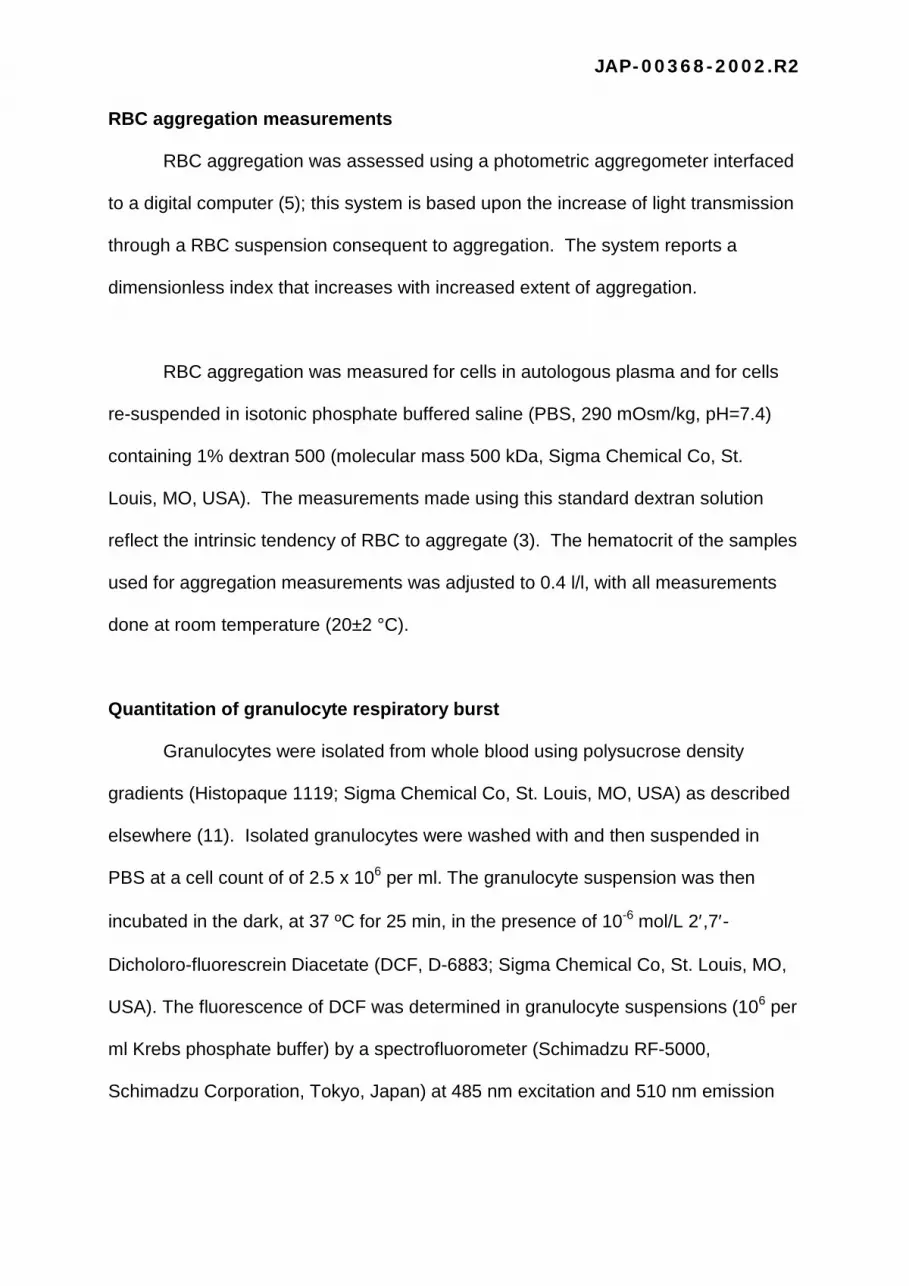
control levels at 24 hours (Figure 2). RBC aggregation in plasma was also
significantly reduced after the exercise, with the onset of this reduction delayed until
30 minutes; reduced aggregation was observed during the first 12 hours (Figure 3).
A similar pattern of reduced RBC aggregation was observed for RBC re-suspended
in the 1% dextran 500 solution, although the significant onset was delayed until 45
minutes and was observed only up to 8 hours (Figure 4).
WBC counts increased significantly immediately after cessation of anaerobic
exercise, then fell to control levels for the first hour (Figure 5). However, there was a
second phase of increase that started at 120 minutes after the end of exercise and
persisted until 4 hours. The composition of the WBC population was also affected by
exercise, such that the percentage of granulocytes increased starting at 45 minutes
after the anaerobic test and lasted for more than three hours (Figure 6). Additionally,
the respiratory burst of the granulocyte population was found to be enhanced during
the first 4 hours with the increase above control significant at the 60 minute time point
(Figure 7).

JAP-00368-2002.R2
DISCUSSION
The Wingate protocol used in this study is a well known model of heavy
anaerobic exercise (24), and it was observed that all ten subjects perceived the
performed exercise experience as strenuous and barely tolerable. Blood lactate
concentrations increased more than 10- fold, thus clearly indicating the high level of
metabolic load induced by this exercise protocol. Other groups have also reported
similar increments in lactate levels after Wingate protocol in untrained adults (18).
This strenuous anaerobic period of exercise performed by untrained individuals can
therefore be accepted as a model of unexpected, forced heavy physical exercise that
might be encountered by any person under demanding conditions.
Strenuous exercise was followed by a series of changes in RBC and WBC
counts which may partly be explained by altered hemodynamic conditions. That is,
increased flow and shear forces within the circulation would be expected to lead to
recruitment of sequestered RBC in various circulatory beds (3,25,41) and of WBC
from the marginal pool (40), plasma volume alterations (8,31,38), and increased
damage and/or removal of circulating RBC (4,25,37). At present, we are unable to
determine which of these factors contributed importantly to the observed changes
(Figures 1, 5 and 6).
The results of this study also indicate mechanical deterioration of RBC as
indicated by decreased elongation indexes (Figure 2), with the significant impairment
of RBC deformability noted immediately after the strenuous exercise. The increased
blood lactate concentration at the 5 minute time point might be an explanation for this

JAP-00368-2002.R2
immediate impairment of RBC deformability inasmuch as Brun et al. demonstrated a
significant correlation between blood lactate and RBC rigidification after exercise (8).
However, the mechanical impairment of RBC continued long after blood lactate
concentrations returned to normal values (Figure 2, Table 2).
Significant decrements in RBC aggregation in both autologous plasma and in
the standard dextran aggregating medium were slightly delayed and were then
observed for up to 8-12 hours (Figures 3 and 4). Decreased aggregation in plasma
may result from alterations of both plasma composition and RBC properties (28,35),
and thus a decreased fibrinogen concentration related to plasma volume expansion
after exercise might be responsible for such an alteration (35). However, RBC
aggregation measurements in a standard aggregating medium (1% Dextran 500)
also revealed a similar pattern of alteration, suggesting that cellular alterations also
play role in decreased aggregation after heavy exercise. Impaired RBC deformability
would also be expected to reduce red blood cell aggregability since rigid cells exhibit
lower levels of aggregation (35). Alternatively, RBC surface properties that play role
in aggregation might be altered by oxidation and/or proteolytic enzymes released by
activated granulocytes (6).
Our results for RBC deformability are consistent with other literature data
indicating impaired RBC deformability after strenuous exercise (9,10,16,30,41,42).
However, literature data on alterations of RBC aggregation is not consistent:
increased (8,10), unaltered (16) or decreased (41) RBC aggregation have been
reported to be occur following exercise. This inconsistency does not seem to be

JAP-00368-2002.R2
surprising, since the exercise models, the properties of subjects (e.g., the degree of
training) and the hemorheological methods used in these prior studies vary widely.
Granulocyte activation may play role in the hemorheological effects of
strenuous exercise. Published literature reports also support the role of an
inflammatory response to strenuous exercise as contributing to hemorheological
deteriorations, and the inflammatory effects of strenuous exercise have been
compared with those occurring in sepsis (13,36). The most likely cause of the
inflammatory response after strenuous exercise is generalized muscle damage (34)
and the existence of such a response has been reported by a large number of
publications (e.g., 27,34). Since an inflammatory response has been associated with
RBC mechanical alterations (6), granulocyte activation can thus be considered to be
at least one of the factors responsible for the hemorheological alterations observed in
this study. Note, however, that the data obtained in the present study do not directly
identify a causal relationship between WBC and RBC alterations; possible
pathophysiological mechanisms underlying RBC-WBC interactions are discussed in
detail elsewhere (6). Note also that in addition to inducing RBC mechanical
alterations, activated granulocytes may directly influence microcirculatory
hemodynamics (20) since granulocyte activation is associated with significant
rigidification of these cells (12) and activated granulocytes may block microcirculatory
circuits (20). Together with their increased number, activated and rigid granulocytes
may be among the factors that contribute to post-exercise circulatory problems.
In overview, this study demonstrates that impaired RBC deformability may
continue up to 12 hours after a single period of strenuous exercise. RBC

JAP-00368-2002.R2
deformability is one of the factors determining the fluidity of blood and hence the
hydrodynamic resistance in blood vessels (14). Furthermore, it is a major rheological
factor affecting microcirculatory and capillary blood flow, and thus reduced
deformability may limit tissue perfusion, especially in individuals with geometrically-
challenged vascular systems and diminished local perfusion pressures (7). During
heavy exercise, the circulation and local perfusion pressures are markedly enhanced,
easily balancing any extra hemorheological load related to RBC mechanical
deterioration. However, after hemodynamic activity and perfusion pressures return to
pre-exercise levels, this hemorheological extra load may not be well tolerated and
tissue perfusion problems might be encountered. Therefore, this prolonged effect of
heavy exercise on RBC deformability may well explain the cardiovascular problems
encountered during the early and late recovery periods after heavy exercise episodes
(1,17,23,26).
ACKNOWLEDGEMENTS
This study is part of MS Degree thesis of Ozlem Yalcin, presented to the Health
Sciences Institute, Akdeniz University, Antalya, Turkey. This study was supported by
Akdeniz University Research Fund (99.02.0122.02).

JAP-00368-2002.R2
REFERENCES
1- Albert CM, Mittleman MA, Chae CU, Lee IM, Hennekens CH and Manson JE.
Triggering of sudden death from cardiac causes by vigorous exertion. New Engl J
Med 343: 1355-1361, 2000.
2- Amsterdam EA. Sudden death during exercise. Cardiol 77: 411-417, 1990.
3- Baskurt OK, Bor-Küçükatay M, Yalçın O, Meiselman HJ and Armstrong JK.
Standard aggregating media to test the “aggregability” of rat red blood cells. Clin
Hemorheol Microcirc. 22: 161-166, 2000.
4- Baskurt OK. The role of spleen in suppressing the rheological alterations in
circulation blood. Clin Hemorheol Microcirc 20:181-1188, 1999.
5- Baskurt OK, Meiselman HJ and Kayar E. Measurement of red blood cell
aggregation in a "plate-plate" shearing system by analysis of light transmission. Clin
Hemorheol 19: 307-314, 1998.
6- Baskurt OK and Meiselman HJ. Activated polymorphonuclear leukocytes affect
red blood cell aggregability. J Leukoc Biol 63: 89-93, 1998.
7- Baskurt OK, Levi E, Caglayan S, Dikmenoglu N, Ucer O, Guner R and
Yorukan S. The role of hemorheologic factors in the coronary circulation. Clin
Hemorheol 11:121-127, 1991.

JAP-00368-2002.R2
8- Brun JF, Khaled S, Ranaud E, Bouix D, Micallef JP and Orsetti A. The
triphasic effects of exercise on blood rheology: Which relevance to physiology and
pathophysiology? Clin Hemorheol Microcirc 19: 89-104, 1998.
9- Brun JF, Micallef JP and Orsetti A. Hemorheologic effects of light prolonged
exercise. Clin Hemorheol Microcirc 14: 807-818,1994.
10- Bouix, D., C. Peyreigne, E. Raynaud, J. P. Micallef, and J. F. Brun.
Relationships among body composition, hemorheology and exercise performance.
Clin Hemorheol Microcirc 19: 245-254, 1998.
11- Boyum A. Separation of leukocytes from blood and bone marrow. Scand Clin
Lab Invest 21: 97-77, 1968.
12- Buttrum, S.M., Drost, E.M., Macnee, W., Goffin, E., Lockwood, C.M., Hatton,
R. and Nash, G.B. Rheological response of neutrophils to different types of
stimulation. J Appl Physiol 77: 1801-1810, 1994.
13- Camus G, Deby-Dupont G, Duchateau J, Deby C, Pincemail J and Larny M.
Are similar inflammatory factors involved in strenuous exercise and sepsis?
Intensive Care Med 20: 602-610, 1994.
14- Chien S. Red cell deformability and its relevance to blood flow. Annu Rev Physiol
49: 177-192, 1987.

JAP-00368-2002.R2
15- Drory Y, Kramer MR and Lev B. Exertional sudden death in soldiers. Med Sci
Sports Exerc 23: 147-151, 1991.
16- Ernst E, Daburger L, Saradeth T. The kinetics of blood rheology during and
after prolonged standardized exercise. Clin Hemorheol 11: 429-439, 1991.
17- Futterman LG and Myerburg R. Sudden death in athletes: an update. Sports
Med 26: 335-350, 1998.
18- Gokbel H and Dolek C. Serum lactic acid and total testosterone levels after the
Wingate test. Turkish J Sport Med 30: 145-152, 1995.
19- Hardeman M. R., Goedhart P. T., Dobbe J.G.G and Lettinga K.P. Laser-
assisted optical rotational cell analyzer (LORCA): 1. A new instrument for
measurement of various structural hemorheological parameters. Clin Hemorheol 14:
605-618, 1994.
20- Harris AG and Skalak TC. Leukocyte cytoskeletal structure determines capillary
plugging and network resistance. Am J Physiol 265: H1670-H1675, 1993.
21- Hautala A, Tulppo MP, Makikallio TH, Laukkanen R, Nissila S and Huikuri
HV. Changes in cardiac autonomic regulation after prolonged maximal exercise. Clin
Physiol 21: 238-245, 2001.

JAP-00368-2002.R2
22- Hofstra TC, Vijay KK, Meiselman HJ and Coates TD. Sickle erythrocytes
adhere to polymorphonuclear neutrophils and activate the neutrophil respiratory.
Blood 87: 4440-4447, 1996.
23- Hoshi A and Inaba Y. Sudden cardiac deaths during exercise in school (1986-
1995). Jap J Phys Fitness Sports Med 49: 503-511, 2000.
24- Inbar O, Bar-Or O, Skinner JS. The Wingate anaerobic test. Illinois: Human
Kinetics, 1996, 110 pp.
25- Ji LL. Exercise, oxidative stress, and antioxidant. Am J Sports Exerc 24: S20-24,
1996.
26- Kohl HW, Powel KE, Gordon NF, Blair SN and Paffenbarger RS. Physical
activity, physical fitness and sudden cardiac death. Epidemiol Rev 14: 37-57, 1992.
27- Konig D, Wagner KH, Elmadfa I and Berg A. Exercise and oxidative stress:
significance of antioxidants with reference to inflammatory, muscular and systemic
stress. Exerc Immunol Rev 7: 108-133, 2001.
28- Meiselman HJ. Red blood cell role in RBC aggregation: 1963-1993 and beyond.
Clin Hemorheol 13: 575-592, 1993.
29- Morentin B, Suarez-Mier MP and Aguilera B. Sudden death due to
atheromatous coronary disease in the young. Rev Esp Cardiol 54: 1167-1174, 2001.

JAP-00368-2002.R2
30- Nageswari K, Banerjee R, Gupte RV and Puniyani RR. Effects of exercise on
rheological and microcirculatory parameters. Clin Hemorheol Microcirc 23: 243-247,
2000.
31- Neuhaus D and P. Gaehtgens. Haemorheology and long term exercise. Sports
Med 18: 10-21, 1994.
32- Neuhauser KM, Neuhauser TS, Drehner D and Blackwood GV. Death among
US air force basic trainees, 1956 to 1996. Mil Med 164: 841-847, 1999.
33- Pescatello LS. Physical activity, cardiometabolic health and older adults – recent
findings. Sports Med 28: 315-323, 1999.
34- Pyne DB. Exercise-induced muscle damaged and inflammation: a review. Aust J
Sci Med Sport 26:49-52, 1994.
35- Rampling M W. Red cell aggregation and yield stress. In: Clinical Blood
Rheology, edited by Lowe G D O. Florida: CRC Press, Inc, 1988, p. 45-64.
36- Shephard RJ. Sepsis and mechanisms of inflammatory response: is exercise a
good model. Br J Sports Med 35: 223-230, 2001.
37- Smith JA. Exercise, training and red blood cell turnover. Sports Med 19: 9-31,
1995.

JAP-00368-2002.R2
38- Szygula Z. Erythrocytic system under the influence of physical exercise and
training. Sports Med 10: 181-197, 1990.
39- Virmani R, Burke AP and Farb A. Sudden cardiac death. Cardiovasc Pathol 10:
275-282, 2001.
40- Wiik P, Opstad A and Boyum A. Granulocyte chemiluminescence response
toserum opsonized particles ex vivo during long-term strenuous exercise, energy and
sleep depletion in humans. Eur J Appl Physiol 73: 251-258, 1996.
41- Yalcin O, Bor-Kucukatay M, Senturk UK and Baskurt OK. Effects of swimming
exercise on red blood cell rheology in trained and untrained rats; J Appl Physiol 88:
2074-2080, 2000.
42- Yang RF, Zhao CJ, Wu YP, Wu X. Deformability of erythrocytes after exercise.
Biorheology 32: 250, 1995 (abstract).

JAP-00368-2002.R2
FIGURE LEGENDS
Figure 1. Red blood cell counts (RBC) before and after the anaerobic exercise bout
(mean±SE; n=10; Difference from the value measured before the exercise;
*: 0.05; †: p<0.01; ‡: p<0.001).
Figure 2. Red blood cell elongation indexes (EI) measured at 1.58 Pascal shear
stress before and after the anaerobic exercise bout (mean±SE; n=10;
Difference from the value measured before the exercise; ‡: p<0.001).
Figure 3. Red blood cell aggregation indexes (M) measured in autologous plasma
before and after the anaerobic exercise bout (mean±SE; n=10; Difference
from the value measured before the exercise; †: p<0.01; ‡: p<0.001).
Figure 4. Red blood cell aggregation indexes (M) measured in 1% solution of Dextran
500 (MW: 500.000) before and after the anaerobic exercise bout
(mean±SE; n=10; Difference from the value measured before the exercise;
*: p<0.05).
Figure 5. White blood cell counts (WBC) before and after the anaerobic exercise bout
(mean±SE; n=10; Difference from the value measured before the exercise;
†: p<0.01).
Figure 6. Percentage of granulocytes in total white blood cell count before and after
the anaerobic exercise bout (mean±SE; n=10; Difference from the value
measured before the exercise; *: 0.05; †: p<0.01; ‡: p<0.001).
Figure7. Granulocyte respiratory burst measured as fluoroscence of DCF (mean±SE;
n=10; Difference from the value measured before the exercise; *: 0.05).

JAP-00368-2002.R2
Table 1. Antropometric measures of the subjects (n=10; mean±SE).
Age
(Year)
Weight
(kg)
Height
(m)
BMI
(kg/m2)
% Fat
LBM
(kg)
20-36
70.5±7.3
1.79±4.3
21.9±1.5
14.1±3.1
60.4±4.6
(BMI: Body mass index; LBM: Lean body mass)
Table 2. Blood lactate concentrations before and after the Wingate anaerobic test
(n=10; mean±SE ).
After exercise
(mmol/L)
Before
exercise
-15 minute
5 minute
15 minute
30 minute
45 minute
60 minute
0.9±0.3
10.0±3.0‡
8.6±2.7‡
4.9±1.9‡
2.7±0.8†
1.6±0.6*
(Difference from the value measured before the exercise; *: 0.05; †: p<0.01; ‡: p<0.001)

JAP-00368-2002.R2
-50 0 50 100 1504.50
4.75
5.00
5.25
5.50
4 8 12 24
Minute Hour
‡
** † *
Exercise
†
RBC
(1012
/L)
Figure 1.

JAP-00368-2002.R2
-50 0 50 100 1500.23
0.25
0.27
0.29
4 8 12 24
Minute Hour
‡ ‡‡‡‡‡ ‡ ‡‡
Exercise
EI (1
.58
Pa)
Figure 2.
JAP-00368-2002.R2
-50 0 50 100 1500
5
10
15
20
4 8 12 24
Minute Hour
†‡‡†
† †
M in
dex
(pla
sma)
Exercise
Figure 3.

JAP-00368-2002.R2
-50 0 50 100 15015
20
25
30
35
4 8 12 24
Minute Hour
* * *
Exercise
M In
dex
(1%
Dex
500
)
Figure 4.

JAP-00368-2002.R2
-50 0 50 100 1504
6
8
10
12
4 8 12 24
Minute Hour
†
††
WBC
(109 /L
)
Exercise
Figure 5.

JAP-00368-2002.R2
-50 0 50 100 15040
50
60
70
80
90
4 8 12 24
Minute Hour
*
‡†
‡
Exercise
% G
ranu
locy
te
Figure 6.

JAP-00368-2002.R2
-50 0 50 100 1500
50
100
150
200
250
4 8 12 24
Minute Hour
*
Exercise
Mea
n flu
oros
cenc
e
Figure 7.





























