Embed Size (px)
Citation preview

rdiology 30 (2014) 647e652
Canadian Journal of CaClinical Research
Antihypertensive Drug Prescribing and Persistence AmongNew Elderly Users: Implications for Persistence
Improvement InterventionsKaren Tu, MD, MSc,a,b,c Laura N. Anderson, PhD, MSc,a Debra A. Butt, MD, MSc,a,b
Hude Quan, MD, PhD,d Brenda R. Hemmelgarn, MD, PhD,d,e Norm R. Campbell, MD,d and
Finlay A. McAlister, MD, MScf; on behalf of the Hypertension Outcome and Surveillance Teama Institute for Clinical Evaluative Sciences (ICES), Toronto, Ontario, Canada
bDepartment of Family and Community Medicine, University of Toronto, Toronto, Ontario, CanadacUniversity Health NetworkeToronto Western Hospital Family Health Team, Toronto, Ontario, Canada
dDepartment of Community Health Sciences, University of Calgary, Calgary, Alberta, CanadaeDepartment of Medicine, University of Calgary, Calgary, Alberta, Canada
fDivision of General Internal Medicine, University of Alberta, Edmonton, Canada
ABSTRACTBackground: The objective of this study was to examine persistencerates and factors influencing persistence for new elderly users ofantihypertensive drugs.Methods: We conducted a population-based cohort study in Ontario ofadults aged 66 years or older to identify new users of antihypertensivemedications between 1999 and 2010. Two-year therapy and classpersistence were defined as persistence on any antihypertensivemedication and persistence only on the same antihypertensive medi-cation class, respectively.Results: From 1999-2010, the prevalence of antihypertensive druguse increased from 47.8%-60.5% (P < 0.0001). Persistence wasevaluated in 420,148 new users of antihypertensive drugs. After 2years, therapy persistence was 58.9% and varied according to initialclass prescribed, from 52.3% for diuretics to 64.1% for angiotensin-converting enzyme inhibitors. Class persistence ranged from 25.3%
Received for publication October 31, 2013. Accepted March 9, 2014.
Corresponding author: Dr Karen Tu, ICES Central, 2075 BayviewAvenue, Toronto, Ontario M4N 3M5, Canada. Tel.: þ1-416-480-4055 �3871; fax: þ1-416-480-6048.
E-mail: [email protected] page 651 for disclosure information.
0828-282X/$ - see front matter � 2014 Canadian Cardiovascular Society. Publishehttp://dx.doi.org/10.1016/j.cjca.2014.03.017
R�ESUM�EIntroduction : L’objectif de cette �etude �etait d’examiner les taux depersistance et les facteurs influençant la persistance au traitementantihypertenseur chez les nouveaux utilisateurs âg�es.M�ethodes : Nous avons r�ealis�e une �etude de cohorte sur une popu-lation d’adultes de 66 ans ou plus de l’Ontario pour d�eterminer lesnouveaux utilisateurs d’antihypertenseurs de 1999 à 2010. La per-sistance au traitement de 2 ans et la persistance à la classe ont�et�e d�efinies comme �etant respectivement la persistance à toutantihypertenseur et la persistance seule à la même classed’antihypertenseurs.R�esultats : De 1999 à 2010, la fr�equence d’utilisation des anti-hypertenseurs est pass�ee de 47,8 % à 60,5 % (P < 0,0001). Lapersistance a �et�e �evalu�ee chez 420 148 nouveaux utilisateurs d’anti-hypertenseurs. Après 2 ans, la persistance au traitement �etait de 58,9% et variait en fonction de la classe initialement prescrite, de 52,3 %
Hypertension is a leading cause of cardiovascular disease andmortality,1 and uncontrolled blood pressure is associated withcardiac, cerebrovascular, and renal diseases and death.2 Bloodpressure lowering medications are among the most commonlyprescribed medications in Canada, with a total of 104.3million prescriptions in 2003.3 Antihypertensive drug use isassociated with a significant reduction in both blood pressure
and cardiovascular events, including myocardial infarction(MI), stroke, and death.3-5
Higher adherence to antihypertensive drug therapy isassociated with lower risk of congestive heart failure (CHF),6
coronary artery disease,7 cerebrovascular events,8 and cardio-vascular outcomes in general and all-cause mortality.9
Furthermore, previous research has shown that better adher-ence to antihypertensive agents and other cardiovascular drugsare associated with lower costs of care.10-14 Despite the ben-efits of higher adherence, 2 recent meta-analyses using pre-scription refill data found relatively poor antihypertensivedrug adherence, with fewer than two-thirds of patientsadhering to their medications over a median of 1 or 2 years offollow-up after initiating an antihypertensive drug.15,16
d by Elsevier Inc. All rights reserved.

for diuretics to 35.8% for angiotensin II receptor blockers. Therapypersistence rates were greater in new users from more recent years(adjusted odds ratio [aOR], 1.24; 95% confidence interval [CI], 1.21-1.27). Subgroups that demonstrated poorer persistence included pa-tients older than 75 years (aOR, 0.95; 95% CI, 0.94-0.96), those withlowest neighbourhood income quintile (aOR, 0.81; 95% CI, 0.80-0.83compared with the highest quintile), those from urban vs rural areas(aOR, 0.83; 95% CI, 0.81-0.84), and those who started on diuretics asinitial monotherapy compared with all other drug classes.Conclusions: Although 2-year therapy and class persistence were lowfor new users of antihypertensive drugs, improvements have occurredover the past decade. Our data highlight subgroups to target for futurepersistence improvement interventions.
pour les diur�etiques à 64,1 % pour les inhibiteurs de l’enzyme deconversion de l’angiotensine. La persistance à la classe allait de 25,3% pour les diur�etiques à 35,8 % pour les antagonistes des r�ecepteursde l’angiotensine II. Les taux de persistance au traitement �etaient plus�elev�es chez les nouveaux utilisateurs au cours des dernières ann�ees(ratio d’incidence approch�e ajust�e [RIAa], 1,24; intervalle de confiance[IC] à 95 %, 1,21-1,27). Les sous-groupes qui d�emontraient une moinsbonne persistance incluaient les patients de plus de 75 ans (RIAa,0,95; IC à 95 %, 0,94-0,96), ceux ayant un quintile de revenu duquartier plus faible (RIAa, 0,81; IC à 95 %, 0,80-0,83 comparativementau quintile plus �elev�e), ceux des zones urbaines vs ceux des zonesrurales (RIAa, 0,83; IC à 95 %, 0,81-0,84) et ceux qui commençaientles diur�etiques en monoth�erapie initiale comparativement aux autresclasses de m�edicaments.Conclusions : Bien que la persistance au traitement de 2 ans et que lapersistance à la classe �etaient faibles chez les nouveaux utilisateursd’antihypertenseurs, des am�eliorations ont �et�e constat�ees au cours dela dernière d�ecennie. Nos donn�ees mettent en �evidence les sous-groupes à cibler lors de futures interventions pour am�eliorer lapersistance.
648 Canadian Journal of CardiologyVolume 30 2014
Although both studies reported poor long-term adherencerates, they differed in their conclusions about whether therewere class-specific differences or not. The studies included inthese meta-analyses used various definitions of adherence andwere performed in developed countries with/without universalhealth care access. In contrast, self-reported findings from theCanadian Community Health Study found that only 5% ofpatients initiating antihypertensive therapy self-reportedstopping within 1 year and only 10% self-reported occasion-ally missing a dose.17
With the increasing experience with newer drug classes,such as angiotensin II receptor blockers (ARBs), and thecontradictory findings regarding the impact of drug class onpersistence in the existing literature, we set out to assessantihypertensive drug prescribing patterns and persistencefrom 1999-2010 among new elderly users of antihypertensivedrugs in Ontario, Canada and to evaluate characteristicsassociated with persistence.
Methods
Study design
A retrospective population-based cohort study was con-ducted using Ontario administrative data housed at the Insti-tute for Clinical Evaluative Sciences (ICES). Universal healthcare access is available to residents of Ontario through thepublicly funded Ontario Health Insurance Plan (OHIP), thesingle payer for all medically necessary services. Service detailsfor residents, providers, and hospitals are captured in healthadministrative databases, which can be linked on an individuallevel to provide a comprehensive health services profile for eachresident. This study received ethics approval from the Sunny-brook Health Sciences Centre Research Ethics Board.
Data sources
We used the Ontario Drug Benefit database (ODB), theRegistered Persons Database (RPDB), OHIP, and the
Canadian Institute for Health Information Discharge AbstractDatabase. These data sets were held securely in a linked dei-dentified form and analyzed at ICES.
The ODB database contains comprehensive records ofprescription medication dispensations from a minimallyrestricted formulary, including antihypertensive medicationsfor residents in Ontario aged 65 years and older. The RPDB isa roster of all Ontarians eligible for OHIP and contains in-formation on sex, date of birth, date of death, and postalcode.18 Neighbourhood income quintiles and rurality weredefined through linkage of postal codes to Canadian censusdata.19 Data on pre-existing cardiovascular-related comorbidconditions (CHF, MI, and stroke) were obtained using theCanadian Institute for Health Information Discharge AbstractDatabase hospitalization database back to 1988 using Inter-national Classification of Diseases, Ninth Revision and In-ternational Classification of Diseases, Tenth Revisiondiagnostic codes in all possible coding fields.20-22 The pres-ence of diabetes was defined using the Ontario DiabetesDatabase,23 which uses a validated administrative data defi-nition (including both OHIP and Canadian Institute forHealth Information data) to define diabetes cases in Ontario.Additionally, for a more general assessment of the potentialimpact of comorbidities on persistence, we examined (1) thenumber of ambulatory diagnostic groups,24 a common co-morbidity measure applied to patients in the primary caresetting, and (2) the number of different drug prescriptions inthe year preceding initiation of an antihypertensive agent.Ambulatory diagnostic groups are based on diagnosis codesand take into consideration duration, severity, and causeof the condition; diagnostic certainty; and specialty careinvolvement.
Study population
Cohorts of Ontarians older than 66 years in each fiscal yearfrom 1999-2010 were evaluated to calculate the incidence andprevalence of antihypertensive drug use, and new users in eachfiscal year were pooled to report results in 2-year groups. The

Tu et al. 649Antihypertensive Drug Prescribing and Persistence
study population consisted of all adults included in theRPDB aged 66 years or older at the start of each fiscalyear. The cohort accumulation was started at age 66 yearsbecause patients only become eligible for ODB at age65 years, thus allowing for a 1-year “washout period” toensure that new prescriptions were truly for new users and notsimply appearing as new prescriptions because the patient justbecame eligible for ODB. Residents were excluded if theywere younger than 66 years or older than 100 years of age,were missing data on sex, were not alive before April 1 of eachfiscal year, or had no contact with the health care system inthe 5 years preceding the beginning of each fiscal year to avoidincluding patients new to the province who would likely haveincomplete historical administrative data information in theOntario databases.
Outcome variable
Incident antihypertensive drug use was defined using a1-year “look-back” period; adults using an antihypertensivedrug in the previous year were classified as prevalent. Thecohort of patients initiating antihypertensive drug therapybetween April 1, 1999 and March 31, 2011 was identified forthe following classes of drugs: angiotensin-converting enzyme(ACE) inhibitors, ARBs, calcium channel blockers (CCBs), b-blockers (BBs), thiazide, and thiazide-like diuretics andcombination agents (see Supplemental Table S1 for drug list).Class and therapy persistence was evaluated among newantihypertensive users who had a minimum of 2 prescriptionsdispensed; patients were followed for 2 years from the initialprescription to evaluate therapy and class persistence. Therapypersistence (continuation with any antihypertensive medica-tion) and class persistence (continuation with the same drugclass) were defined as a repeated prescription filled within aninterval defined by the duration of the previous prescriptionplus a 50% grace period (ie, 1.5 times the number of days ofthe previous prescription).25,26 Patients initiating treatmentwith combination agents were considered class persistent onlyif they continued taking any combination agent. Study par-ticipants were defined as persistent if they reached the end ofthe 2-year follow-up or died without a gap in prescriptionrefills.
Statistical analysis
All statistical analyses were conducted using SAS, version9.3 (SAS Institute, Cary, NC). The rate of new antihyper-tensive drug use was calculated by dividing the number of newusers by the rest of the populationdexcluding prevalent usersfrom the denominator. Logistic regression was used to eval-uate characteristics associated with both class and therapypersistence, defined as persistent or not at the end of 2 years.Unadjusted odds ratios (ORs) were obtained from simplelogistic regression models for each variable, and adjusted ORs(aORs) were obtained from an adjusted multivariate modelthat included all the following variables simultaneously: agegroup, sex, neighbourhood income quintile, rural/urbanresidence, and cohort year over the follow-up period. Sensi-tivity analyses were conducted to evaluate the impact ofremoving patients with a history of any cardiovascular co-morbid condition at baseline (ie, time of new prescription fill).
ResultsFrom 1999/2000-2009/10, there was a significant decrease
in the overall incidence of new antihypertensive drug use from10.6% to 7.9% (P < 0.0001) and over the same period,prevalence of use increased from 47.8% to 60.5% (P <0.0001 (Supplemental Table S2). Among the entire popula-tion, the proportion of new users of antihypertensive drugsdecreased significantly within all age groups from 1999/2000-2009/2010 (Supplemental Table S2). Similar decreases overtime were observed among both men and women, all neigh-bourhood income quintiles, rural and urban dwellers, and forall comorbid conditions; however, within any given year, theproportion of new users was greatest among patients previ-ously diagnosed with MI, CHF, stroke, or diabetes.
From 1999/2000-2009/2010, a significant increase wasobserved in the proportion of new users initiating therapywith ARBs (from 1.3% to 14.2%) and combination drugs(from 0.8% to 5.0%) (Fig. 1). Over the same period, theproportion of new users significantly decreased for patientsinitiating treatment with ACE inhibitors (41.5% to 36.7%),BBs (19.0% to 17.7%), CCBs (14.4% to 10.1%) and di-uretics (23.1% to 16.5%) (Fig. 1).
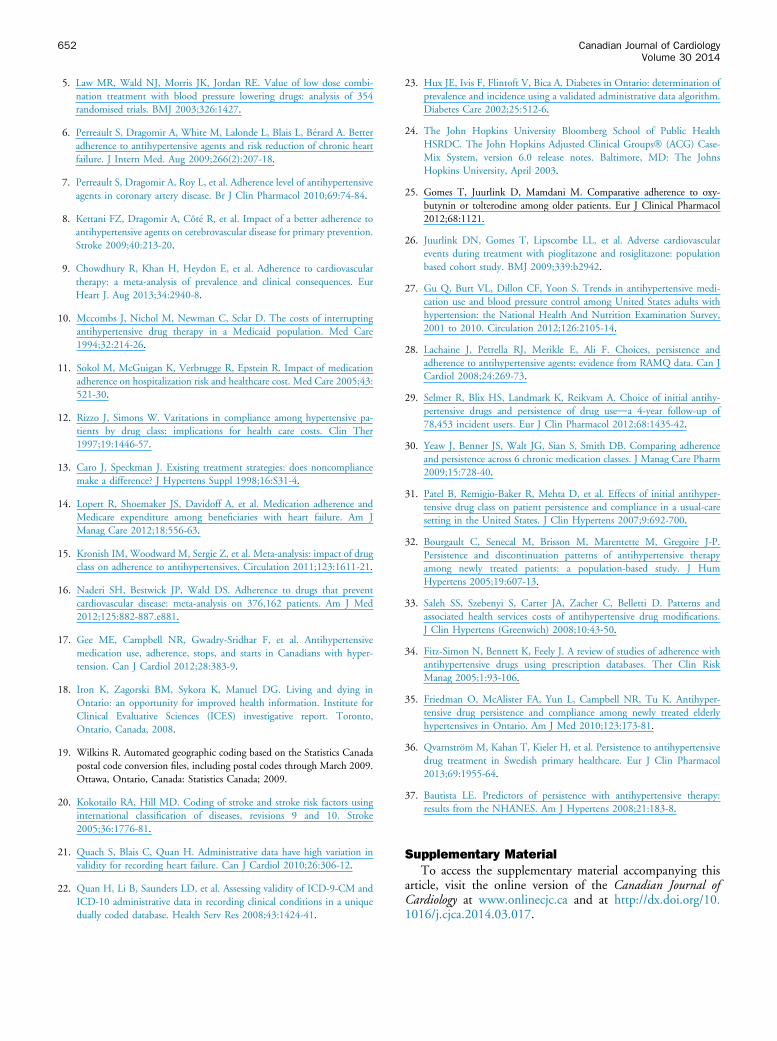
Over the first year of treatment, therapy persistence was64.6% and class persistence was 42.6%. By the end of thesecond year, therapy and class persistence decreased to 58.9%and 30.5%, respectively (Fig. 2). Two-year class persistencewas higher for patients who started on ACEs, ARBs, CCBs,combination drugs, or BBs compared with patients whoinitiated therapy with diuretics (Supplemental Table S3).
Therapy and class persistence increased over time duringthe study period (Supplemental Table S3). Although patientsfirst treated in 1999/2000 exhibited 2-year therapy persistenceof 55.8%, 60.9% of the cohort first treated in 2007/2008 stillhad persistent therapy at 2 years (aOR, 1.23; 95% CI, 1.20-1.26), and class persistence increased from 29.2% to 33.6%(aOR, 1.24; 95% CI, 1.21-1.27) (Supplemental Table S3).Class and therapy persistence were lower for individuals olderthan 75 years, those living in urban areas, those with lowerhousehold incomes, and for patients without diabetes, CHF,MI, or stroke (Supplemental Table S3). Therapy persistencewas also lower for patients with more comorbidities and forthose taking greater numbers of drugs in the year beforeantihypertensive treatment initiation.
The aORs for all characteristics and both class and therapypersistence were not appreciably different in the sensitivityanalysis when individuals with cardiovascular-related comorbid-ities (diabetes, CHF, stroke, MI) were removed (SupplementalTable S4).
DiscussionUsing a large population-based cohort from Ontario, we
found that the frequency of new users of antihypertensive drugsamong adults 66 years of age and older decreased slightly from1999-2010, whereas prevalence of use increased substantially.This suggests that a greater number of patients are beinginitiated on antihypertensive therapy before age 66 years, whichimplies that patients are being diagnosed with hypertension atearlier ages. The rates of antihypertensive persistence we foundare similar to those reported in other studies using medicationdispensation databases and substantially lower than those
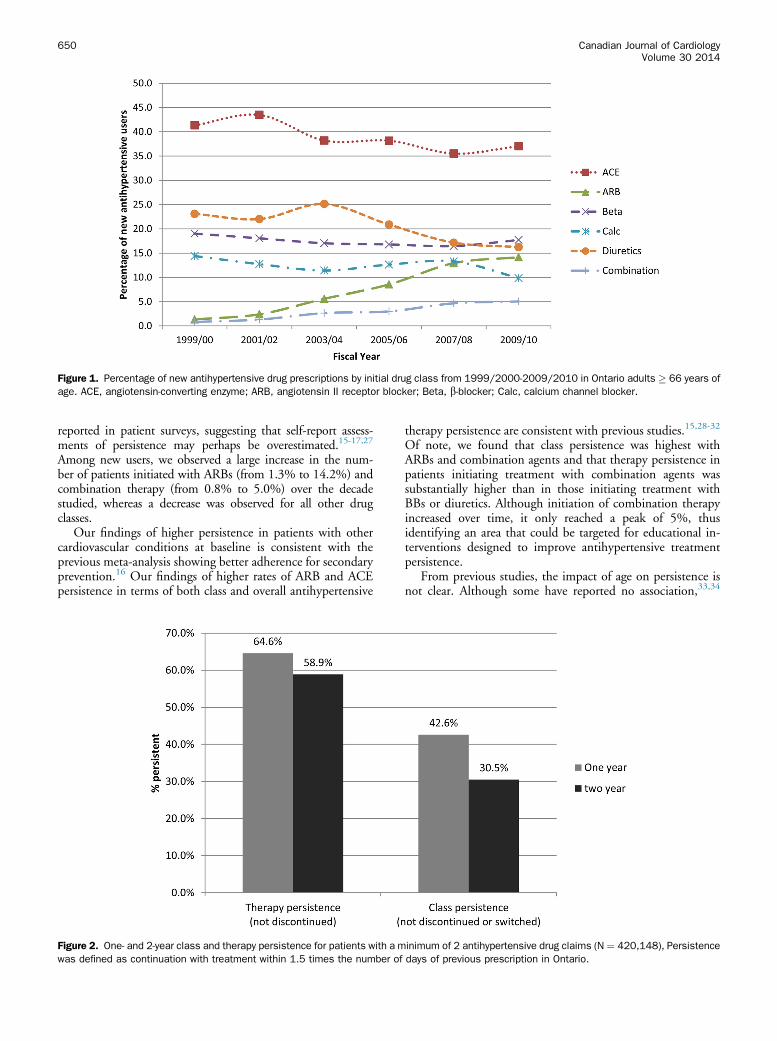
Figure 1. Percentage of new antihypertensive drug prescriptions by initial drug class from 1999/2000-2009/2010 in Ontario adults � 66 years ofage. ACE, angiotensin-converting enzyme; ARB, angiotensin II receptor blocker; Beta, b-blocker; Calc, calcium channel blocker.
650 Canadian Journal of CardiologyVolume 30 2014
reported in patient surveys, suggesting that self-report assess-ments of persistence may perhaps be overestimated.15-17,27
Among new users, we observed a large increase in the num-ber of patients initiated with ARBs (from 1.3% to 14.2%) andcombination therapy (from 0.8% to 5.0%) over the decadestudied, whereas a decrease was observed for all other drugclasses.
Our findings of higher persistence in patients with othercardiovascular conditions at baseline is consistent with theprevious meta-analysis showing better adherence for secondaryprevention.16 Our findings of higher rates of ARB and ACEpersistence in terms of both class and overall antihypertensive
Figure 2. One- and 2-year class and therapy persistence for patients with a mwas defined as continuation with treatment within 1.5 times the number of
therapy persistence are consistent with previous studies.15,28-32
Of note, we found that class persistence was highest withARBs and combination agents and that therapy persistence inpatients initiating treatment with combination agents wassubstantially higher than in those initiating treatment withBBs or diuretics. Although initiation of combination therapyincreased over time, it only reached a peak of 5%, thusidentifying an area that could be targeted for educational in-terventions designed to improve antihypertensive treatmentpersistence.
From previous studies, the impact of age on persistence isnot clear. Although some have reported no association,33,34
inimum of 2 antihypertensive drug claims (N ¼ 420,148), Persistencedays of previous prescription in Ontario.

Tu et al. 651Antihypertensive Drug Prescribing and Persistence
others report higher persistence in older users.35-37 However,most studies reporting on the impact of age on persistencehave defined older as 65þ years compared with youngeradults. We have further refined this by examining differencesacross age strata in a cohort in which all patients are older than65 years. We found increased class persistence with increasingage, but therapy persistence was lower in the older age groups.Similarly we found higher class persistence and lower therapypersistence with more comorbidities and a greater number ofmedications in the year before antihypertensive treatmentinitiation. It is possible that this lower persistence withincreasing age and higher complexity are related to the pres-ence of other more pressing medical conditions that requireattention, and the preventive nature of controlling hyperten-sion is viewed to be less important closer to the end of life. Aprevious study also found poorer persistence with urban-dwelling users. It may be possible that individuals living inurban settings are more likely to see multiple providers, havemore comorbidities, or take more multiple medications (or acombination of these factors), which all could lead to poorerpersistence.
A strength of our study is the data source, which consistedof population-based administrative databases with universaldrug coverage representative of all Ontario adults age 66 yearsand older; however, some limitations of this study should beconsidered. First, drug data were not available for the entirepopulation younger than 65 years of age, and thus we couldonly examine persistence rates in older new users of antihy-pertensive therapy. Additionally, patients younger than age 66years who had previously started on an antihypertensive drugand stopped for more than a year and then restarted wouldhave erroneously been considered new users in our study.Second, we were unable to determine the indication for thedrugs dispensed, and thus our study is of new users of anti-hypertensive therapy rather than patients with newly diag-nosed hypertension; however, our results were consistent evenafter excluding patients with other indications for antihyper-tensive agents such as diabetes, CHF, MI, and stroke. Third,it was unknown if patients were advised to stop taking theirantihypertensive medication, because no data were availableon blood pressure control. Fourth, our results were based on amedication dispensed from a pharmacy, and therefore wewere unable to assess medication prescription rates; we werealso unable to determine if the patient took the medication.Fifth, our calculation of persistence may have been under-estimated if patients received medication samples from theirphysicians; however, the newer medications (ARBs, combi-nation agents) are more likely to be given to patients assamples than are older medications like diuretics, and thismay have led to bias in favour of better persistence for thenewer medications because patients would likely not havethen filled a prescription that they tried initially through asample and had side effects. Sixth, our study was not able todetermine if those who were not persistent during the 2-yearfollow-up time frame were restarted on antihypertensivemedications in a later year. Last, a full economic analysis ofthe potential population-level impact of poorer persistencerelated to first-line use of the cheaper subclasses of medication(diuretics, BBs) or the impact of ethnicity was beyond thescope of this study but would be useful to analyze in futurestudies.
ConclusionsWe found that despite improvements over the decade we
studied, 2-year class and therapy persistence for antihyper-tensive drugs remains suboptimal. The differences weobserved in class persistence with choice of first-line therapymay be useful for physician decision making about initiatingantihypertensive therapy. More efforts are needed to improvepersistence for all patients starting antihypertensive therapy,and in particular those from urban and low-income settings.
AcknowledgementsThe following are members of the Hypertension and
Outcomes Surveillance Team of the Canadian HypertensionEducation Program: Oliver Baclic, Gillian Bartlett, DebraButt, Norm Campbell, Guanmin Chen, Sulan Dai, BrendaHemmelgarn, Michael Hill, Helen Johansen, Nadia Khan,Lisa Lix, Finlay McAlister, Jay Onysko, Hude Quan, MarkSmith, Larry Svenson, Gary Teare, Karen Tu, Robin Walker,and Andy Wielgosz. We thank Brogan Inc, Ottawa for use oftheir Drug Product and Therapeutic Class Database.
Funding SourcesThis project was funded by the Canadian Institutes of
Health Research (grant number: MOP97823). This study wassupported by the Institute for Clinical Evaluative Sciences(ICES), which is funded by an annual grant from the OntarioMinistry of Health and Long-Term Care (MOHLTC). Theopinions, results and conclusions reported in this article arethose of the authors and are independent from the fundingsources. No endorsement by ICES or the Ontario MOHLTCis intended or should be inferred. K.T. is supported by aCanadian Institutes of Health Research Fellowship Award inPrimary Care, and K.T. and D.A.B. are supported by Inves-tigator Awards from the Department of Family and Com-munity Medicine, University of Toronto. F.A.M. and H.Q.are supported by salary awards from Alberta Innovates: HealthSolutions, and F.A.M. is also supported by a salary awardfrom the University of Alberta Chair in Cardiovascular Out-comes Research.
DisclosuresN.R.C. has received funding for travel to a meeting in
2012 from Novartis.
References
1. Global Health Risks. Mortality and Burden of Disease Attributable toMajor Risks. Geneva, Switzerland: World Health Organization, 2009.
2. Cushman WC. The burden of uncontrolled hypertension: morbidity andmortality associated with disease progression. J Clin Hypertens (Green-wich) 2003;5(3 suppl 2):14-22.
3. Campbell NR, Brant R, Johansen H, et al. Increases in antihypertensiveprescriptions and reductions in cardiovascular events in Canada. Hy-pertension 2009;53:128-34.
4. Law MR, Morris JK, Wald NJ. Use of blood pressure lowering drugs inthe prevention of cardiovascular disease: meta-analysis of 147 randomisedtrials in the context of expectations from prospective epidemiologicalstudies. BMJ 2009;338:b1665.
652 Canadian Journal of CardiologyVolume 30 2014
5. Law MR, Wald NJ, Morris JK, Jordan RE. Value of low dose combi-nation treatment with blood pressure lowering drugs: analysis of 354randomised trials. BMJ 2003;326:1427.
6. Perreault S, Dragomir A, White M, Lalonde L, Blais L, B�erard A. Betteradherence to antihypertensive agents and risk reduction of chronic heartfailure. J Intern Med. Aug 2009;266(2):207-18.
7. Perreault S, Dragomir A, Roy L, et al. Adherence level of antihypertensiveagents in coronary artery disease. Br J Clin Pharmacol 2010;69:74-84.
8. Kettani FZ, Dragomir A, Côt�e R, et al. Impact of a better adherence toantihypertensive agents on cerebrovascular disease for primary prevention.Stroke 2009;40:213-20.
9. Chowdhury R, Khan H, Heydon E, et al. Adherence to cardiovasculartherapy: a meta-analysis of prevalence and clinical consequences. EurHeart J. Aug 2013;34:2940-8.
10. Mccombs J, Nichol M, Newman C, Sclar D. The costs of interruptingantihypertensive drug therapy in a Medicaid population. Med Care1994;32:214-26.
11. Sokol M, McGuigan K, Verbrugge R, Epstein R. Impact of medicationadherence on hospitalization risk and healthcare cost. Med Care 2005;43:521-30.
12. Rizzo J, Simons W. Varitations in compliance among hypertensive pa-tients by drug class: implications for health care costs. Clin Ther1997;19:1446-57.
13. Caro J, Speckman J. Existing treatment strategies: does noncompliancemake a difference? J Hypertens Suppl 1998;16:S31-4.
14. Lopert R, Shoemaker JS, Davidoff A, et al. Medication adherence andMedicare expenditure among beneficiaries with heart failure. Am JManag Care 2012;18:556-63.
15. Kronish IM, Woodward M, Sergie Z, et al. Meta-analysis: impact of drugclass on adherence to antihypertensives. Circulation 2011;123:1611-21.
16. Naderi SH, Bestwick JP, Wald DS. Adherence to drugs that preventcardiovascular disease: meta-analysis on 376,162 patients. Am J Med2012;125:882-887.e881.
17. Gee ME, Campbell NR, Gwadry-Sridhar F, et al. Antihypertensivemedication use, adherence, stops, and starts in Canadians with hyper-tension. Can J Cardiol 2012;28:383-9.
18. Iron K, Zagorski BM, Sykora K, Manuel DG. Living and dying inOntario: an opportunity for improved health information. Institute forClinical Evaluative Sciences (ICES) investigative report. Toronto,Ontario, Canada, 2008.
19. Wilkins R. Automated geographic coding based on the Statistics Canadapostal code conversion files, including postal codes through March 2009.Ottawa, Ontario, Canada: Statistics Canada; 2009.
20. Kokotailo RA, Hill MD. Coding of stroke and stroke risk factors usinginternational classification of diseases, revisions 9 and 10. Stroke2005;36:1776-81.
21. Quach S, Blais C, Quan H. Administrative data have high variation invalidity for recording heart failure. Can J Cardiol 2010;26:306-12.
22. Quan H, Li B, Saunders LD, et al. Assessing validity of ICD-9-CM andICD-10 administrative data in recording clinical conditions in a uniquedually coded database. Health Serv Res 2008;43:1424-41.
23. Hux JE, Ivis F, Flintoft V, Bica A. Diabetes in Ontario: determination ofprevalence and incidence using a validated administrative data algorithm.Diabetes Care 2002;25:512-6.
24. The John Hopkins University Bloomberg School of Public HealthHSRDC. The John Hopkins Adjusted Clinical Groups� (ACG) Case-Mix System, version 6.0 release notes. Baltimore, MD: The JohnsHopkins University, April 2003.
25. Gomes T, Juurlink D, Mamdani M. Comparative adherence to oxy-butynin or tolterodine among older patients. Eur J Clinical Pharmacol2012;68:1121.
26. Juurlink DN, Gomes T, Lipscombe LL, et al. Adverse cardiovascularevents during treatment with pioglitazone and rosiglitazone: populationbased cohort study. BMJ 2009;339:b2942.
27. Gu Q, Burt VL, Dillon CF, Yoon S. Trends in antihypertensive medi-cation use and blood pressure control among United States adults withhypertension: the National Health And Nutrition Examination Survey,2001 to 2010. Circulation 2012;126:2105-14.
28. Lachaine J, Petrella RJ, Merikle E, Ali F. Choices, persistence andadherence to antihypertensive agents: evidence from RAMQ data. Can JCardiol 2008;24:269-73.
29. Selmer R, Blix HS, Landmark K, Reikvam A. Choice of initial antihy-pertensive drugs and persistence of drug useda 4-year follow-up of78,453 incident users. Eur J Clin Pharmacol 2012;68:1435-42.
30. Yeaw J, Benner JS, Walt JG, Sian S, Smith DB. Comparing adherenceand persistence across 6 chronic medication classes. J Manag Care Pharm2009;15:728-40.
31. Patel B, Remigio-Baker R, Mehta D, et al. Effects of initial antihyper-tensive drug class on patient persistence and compliance in a usual-caresetting in the United States. J Clin Hypertens 2007;9:692-700.
32. Bourgault C, Senecal M, Brisson M, Marentette M, Gregoire J-P.Persistence and discontinuation patterns of antihypertensive therapyamong newly treated patients: a population-based study. J HumHypertens 2005;19:607-13.
33. Saleh SS, Szebenyi S, Carter JA, Zacher C, Belletti D. Patterns andassociated health services costs of antihypertensive drug modifications.J Clin Hypertens (Greenwich) 2008;10:43-50.
34. Fitz-Simon N, Bennett K, Feely J. A review of studies of adherence withantihypertensive drugs using prescription databases. Ther Clin RiskManag 2005;1:93-106.
35. Friedman O, McAlister FA, Yun L, Campbell NR, Tu K. Antihyper-tensive drug persistence and compliance among newly treated elderlyhypertensives in Ontario. Am J Med 2010;123:173-81.
36. Qvarnström M, Kahan T, Kieler H, et al. Persistence to antihypertensivedrug treatment in Swedish primary healthcare. Eur J Clin Pharmacol2013;69:1955-64.
37. Bautista LE. Predictors of persistence with antihypertensive therapy:results from the NHANES. Am J Hypertens 2008;21:183-8.
Supplementary MaterialTo access the supplementary material accompanying this
article, visit the online version of the Canadian Journal ofCardiology at www.onlinecjc.ca and at http://dx.doi.org/10.1016/j.cjca.2014.03.017.





























