Embed Size (px)
Citation preview
026 Antiviral treatment for Bell's palsy (idiopathic facial paralysis)
1 / 40
Antiviral treatment for Bell's palsy (idiopathic facial paralysis)Review information
Review type: InterventionReview number: 026AuthorsIldiko Gagyor1, Vishnu B Madhok2, Fergus Daly3, Dhruvashree Somasundara2, Michael Sullivan4, Fiona Gammie2, FrankSullivan5
1Department of General Practice/Family Medicine, University of Göttingen, Göttingen, Germany2Centre for Primary Care and Population Research, Division of Clinical and Population Sciences and Education,University of Dundee, Dundee, UK3Frontier Science (Scotland) Ltd, Kingussie, UK4School of Clinical Sciences, University of Edinburgh, Edinburgh, UK5Department of Family and Community Medicine, North York General Hospital, University of Toronto, Toronto, CanadaCitation example: Gagyor I, Madhok VB, Daly F, Somasundara D, Sullivan M, Gammie F, Sullivan F. Antiviral treatmentfor Bell's palsy (idiopathic facial paralysis). Cochrane Database of Systematic Reviews 2009 , Issue 4 . Art. No.:CD001869. DOI: 10.1002/14651858.CD001869.pub4 .
Contact personIldiko GagyorAcademic GPDepartment of General Practice/Family MedicineUniversity of GöttingenHumboldtalle 38GöttingenLower Saxony37073Germany
E-mail: [email protected]
DatesAssessed as Up-to-date:7 October 2014Date of Search: 7 October 2014Next Stage Expected: 7 October 2016Protocol First Published: Issue 3 , 1999Review First Published: Issue 2 , 2001Last Citation Issue: Issue 4 , 2009
What's newDate Event Description28 February 2014 New citation: conclusions not
changedReview updated with no change to conclusions. Newauthors: Ildiko Gagyor, Vishnu B Madhok, DhruvashreeSomasundara, Michael Sullivan, and Fiona Gammie.Previous authors Pauline Lockhart, Marie Pitkethly, andNatalia Comerford withdrew.
22 January 2014 Updated New trials added, text rewritten, new calculations,references updated.
History
026 Antiviral treatment for Bell's palsy (idiopathic facial paralysis)
2 / 40
Date Event Description12 May 2010 Amended Correction to reference
10 November 2009 Amended Correction of minor error in Discussion.
25 February 2009 New citation: conclusions changed This is a substantive update to the previous edition of the
review with a new review team. Five new studies added tothe analysis with changes made to Results and Discussionsections as necessary.
5 February 2009 Updated Substantive update to previous edition of review.Abstract and background information re-written. Modificationof outcomes: all data from trials, whatever the trial length asopposed to 6 month outcomes. Five new studies added tothe analysis with necessary changes made to Results andDiscussion sections. One study removed from the previousreview as no data contributed and none forthcoming toprevious authors when approached.
1 November 2007 Amended Two trials, one with 551 participants comparingprednisolone with aciclovir with both and with neither,another with 221 participants comparing prednisolone andvalaciclovir with prednisolone and placebo have just beenpublished and will be included in an update of this review.
1 March 2004 New citation: conclusions changed Substantive amendment
1 January 2004 Updated The review was updated in January 2004. Searches wereupdated as follows: Neuromuscular Disease Group TrialsRegister (searched April 2003), MEDLINE (searchedJanuary 1966 to April 2003), EMBASE (searched January1980 to April 2003), and LILACS (searched January 1982 toApril 2003).
AbstractBackgroundCorticosteroids are widely used in the treatment of idiopathic facial paralysis (Bell’s palsy), but the effectiveness of additionaltreatment with an antiviral agent is uncertain. Significant morbidity can be associated with severe cases of Bell's palsy.
ObjectivesTo assess the effects of antiviral treatments alone or in combination with any other therapy for Bell’s palsy.
Search methodsOn 7 October 2014 we searched the Cochrane Neuromuscular Disease Group Specialized Register, CENTRAL, MEDLINE,EMBASE, LILACS, DARE, NHS EED, and HTA. We also reviewed the bibliographies of the identified trials and contactedtrial authors and known experts in the field and relevant drug companies to identify additional published or unpublished data.We searched clinical trials registries for ongoing studies.
Selection criteriaWe considered randomised controlled trials or quasi-randomised controlled trials of antivirals with and without corticosteroidsversus control therapies for the treatment of Bell's palsy. We excluded trials that had a high risk of bias in several domains.
Data collection and analysisPairs of authors independently assessed trials for relevance, eligibility, and risk of bias, using standard Cochraneprocedures.
Main resultsEleven trials, including 2883 participants, met the inclusion criteria and are included in the final analysis. We added fourstudies to the previous review for this update. Some of the trials were small, and a number were at high or unclear risk ofbias. Other trials did not meet current best standards in allocation concealment and blinding.
026 Antiviral treatment for Bell's palsy (idiopathic facial paralysis)
3 / 40
Incomplete recoveryWe found no significant benefit from adding antivirals to corticosteroids in comparison with corticosteroids alone for peoplewith Bell’s palsy (risk ratio (RR) 0.69, 95% confidence interval (CI) 0.47 to 1.02, n = 1715). For people with severe Bell’spalsy (House-Brackmann scores of 5 and 6 or the equivalent in other scales), we found a reduction in the rate of incompleterecovery at month six when antivirals plus corticosteroids were used (RR 0.64, 95% CI 0.41 to 0.99, n = 478). The outcomefor the participants receiving corticosteroids alone was significantly better than for those receiving antivirals alone (RR 2.09,95% CI 1.36 to 3.20, n = 1169). The treatment effect of placebo was significantly lower than that of antivirals pluscorticosteroids (RR 0.56, 95% CI 0.41 to 0.76, n = 658). Antivirals alone had a non-significant detrimental effect on theoutcome compared with placebo (RR 1.10, 95% CI 0.87 to 1.40, n = 658).Motor synkinesis or crocodile tearsIn three trials comparing antivirals and corticosteroids with corticosteroids and placebo that assessed this outcome, we founda significant difference in long-term sequelae in favour or antivirals plus corticosteroids (RR 0.73, 95% CI 0.54 to 0.99, n =869). Three trials comparing antivirals alone with corticosteroids alone investigating this outcome showed fewer sequelaewith corticosteroids (RR 1.44, 95% CI 1.11 to 1.85, n = 873). We found no data on long-term sequelae for othercomparisons.Adverse events Adverse event data were available in three studies giving comparison data on 1528 participants. None of the fourcomparisons (antivirals plus corticosteroids versus corticosteroids plus placebo or no treatment; antivirals versuscorticosteroids; antivirals plus corticosteroids versus placebo; antivirals versus placebo) showed significant differences inadverse events between treatment and control arms. We could find no correlation with specific treatment within these results.
Authors' conclusionsModerate-quality evidence from randomised controlled trials showed no additional benefit from the combination of antiviralswith corticosteroids compared to corticosteroids alone or with placebo, and no benefit from antivirals alone compared toplacebo, for the treatment of Bell's palsy. Moderate-quality evidence showed a small but just significant benefit ofcombination therapy compared with corticosteroids alone in severe Bell’s palsy. We found no significant increase in adverseevents from the use of antivirals compared with either placebo or corticosteroids.
Plain language summaryAntiviral treatment for Bell's palsyReview questionWe reviewed the evidence about the effect of antiviral therapy alone or in combination with any other therapy, on Bell's palsy.BackgroundBell's palsy is a disease of the facial nerve that causes one side of the face to be paralysed. Some studies have suggestedthat it is caused by the same viral infections that cause cold sores (herpes simplex) or shingles (varicella zoster). If this iscorrect, antiviral drugs would be likely to help recovery. The paralysis is usually temporary even when left untreated, althoughwithout treatment about one person in five is left with permanent facial disfigurement or pain. A Cochrane review has alreadyconfirmed the effectiveness of corticosteroids in Bell’s palsy.Study characteristicsWe identified 11 trials, which included 2883 participants with mild, moderate, or severe one-sided Bell’s palsy of unknowncause. Participants were aged from 14 to 84 years. The trials compared antivirals in combination with corticosteroids tocorticosteroid treatment alone or in combination with placebo; antiviral treatment alone or in combination with placebo toplacebo or no treatment only; antiviral treatment alone or in combination with placebo to corticosteroid treatment alone or incombination with placebo; and antiviral treatment in combination with corticosteroids to placebo or no treatment only. Theduration of the included studies ranged from three months to 12 months.Key results and quality of the evidenceThis updated review provides moderate-quality evidence for no benefit for people with Bell's palsy from the combination ofantivirals with corticosteroids compared to corticosteroids alone or with placebo, based on data from 1715 trial participants.The combination of corticosteroids with antivirals is probably more effective than corticosteroids alone in the treatment ofpeople with severe Bell’s palsy.Antivirals alone (or combined with placebo) were not as effective as corticosteroids alone or corticosteroids in combinationwith antivirals.Moderate-quality evidence showed a significant benefit with antivirals plus corticosteroids compared with corticosteroidsalone in people with severe Bell’s palsy.In three trials considerably more long-term after-effects of Bell's palsy were seen in people treated with corticosteroids alonethan in people treated with antivirals and corticosteroids combined (moderate-quality evidence). There were also fewer long-term after-effects with corticosteroids alone than with antivirals alone (three trials).Based on the evidence from three trials, none of the different treatments showed significant differences in adverse events,
026 Antiviral treatment for Bell's palsy (idiopathic facial paralysis)
4 / 40
taking into account the moderate quality of data for this outcome.The evidence in this review is current to October 2014.
Background Description of the conditionBell's palsy is an acute, generally unilateral paralysis or weakness of facial musculature consistent with peripheral facialnerve dysfunction, of no detectable cause (Niparko 1993). Additional symptoms frequently include pain around or behind theear on the affected side, sometimes extending into the occipital or cervical regions. Impaired tolerance to ordinary levels ofnoise and disturbed sense of taste on the affected side may also be present (Burgess 1984).Epidemiological studies have reported an annual incidence of 23 to 25 per 100,000 per year, but a recent study using ageneral-practice database suggests it may be even higher, at 37 per 100,000 per year (Victor 1994 ; Martyn 1997 ; Morales2013). The condition affects men and women more or less equally, and was once thought to be most common in the 30- to45-year age group (Peitersen 1982 ; Katusic 1986 ; Yanagihara 1988 ; Bateman 1992 ; Brandenberg 1993 ; Peitersen2002). However, a recent primary-care database study suggests a second peak in the over-70s (Morales 2013). Bell's palsypresents disproportionately amongst pregnant women and people who have diabetes, influenza, a cold, or some other upperrespiratory ailment. On average, a British general practitioner will see one person who has developed the condition every 12to 18 months. Both sides of the face are affected equally often (Prescott 1988).The aetiology of Bell's palsy is still debated. A viral infection, vascular ischaemia, autoimmune inflammatory disorders, andheredity have been proposed as underlying causes (Adour 1982 ; Burgess 1984 ; Lorber 1996 ; Lackner 2010). A viralaetiology has gained popularity since the isolation of herpes simplex virus type 1 genome from the saliva and facial nerveendoneurial fluid of people with this condition (Murakami 1996 ; Lackner 2010). On the whole, the prognosis is favourable,though a significant proportion of people who are left untreated have residual symptoms. One of the largest series of peoplewith Bell's palsy, which included people receiving no treatment, showed that 85% of people began to recover within threeweeks after onset (Peitersen 1982). Partial recovery usually occurred within three to six months for the remaining 15%. Thesame series showed that normal facial expression reappeared in 71% of cases, 13% had insignificant sequelae (long-termafter-effects), and the final 16% had permanently diminished function with aberrant innervation (expressed as motorsynkinesis or autonomic dysfunction), and postparalytic spasms.
Description of the interventionThe treatment of Bell's palsy was highly controversial until 2008, at which time corticosteroids alone were shown to beeffective in treating the condition (Salinas 2010). Previous Cochrane reviews on the treatment of Bell’s palsy examined theeffectiveness of oral prednisolone and aciclovir or valaciclovir (Allen 2004; Lockhart 2009). Several studies excluded from theanalysis in these reviews either failed to randomise participants or, when correctly randomised, results were erroneouslyinterpreted in a favourable light (May 1976 ; Wolf 1978). High-dose corticosteroid therapy has several potential side effects,including peptic ulceration, hypertension, and confusional states. Antiviral therapy was considered expensive, and treatmentwas reserved for circumstances in which a clear benefit appeared likely.Previous recommendations suggested that antiviralsneeded to be started within 48 hours, although a study of viral replication in participants with Bell’s palsy suggests that thewindow might be extended (Abiko 2002).
Why it is important to do this reviewThe previous update of this Cochrane review included large-scale randomised controlled trials (RCTs) of antivirals (A) andcorticosteroids (S) that had been published in the years before the review. The authors stated that, compared to placebo, Ado not contribute to a significant improvement in the rate or extent of recovery of trial participants (Lockhart 2009). Thecurrent review updates these findings based on four additional studies.
Objectives To assess the effects of antiviral treatments alone or in combination with any other therapy for Bell’s palsy.
Methods Criteria for considering studies for this review Types of studies We searched for all randomised controlled trials (RCTs) or quasi-RCTs (which are trials that employ alternate or othersystematic allocation) involving aciclovir, valaciclovir, or famciclovir alone or in combination with any other therapy in thetreatment of Bell's palsy, published in any language. The duration of studies included in this review ranges from 3 to 12months; the minimum study duration was 3 months. As in previous versions of the review, we used study quality as anexclusion criterion, excluding trials with a high risk of bias in several domains.
Types of participants We considered all trials where participants had a diagnosis of unilateral facial paralysis of unknown cause and satisfied thetrial authors’ requirements for eligibility and inclusion.
Types of interventions We considered all trials of treatment with any oral antiviral licensed for the treatment of herpes simplex infections in
026 Antiviral treatment for Bell's palsy (idiopathic facial paralysis)
5 / 40
immunocompetent participants. The list comprised aciclovir; valaciclovir, which is a prodrug of aciclovir; and famciclovir,which is a prodrug of penciclovir. We considered trials where participants received antiviral therapy versus placebo or anyother treatment.
Types of outcome measures We have described changes to outcome measures in this and previous versions of the review in Differences betweenprotocol and review.
Primary outcomesIncomplete recovery of facial function at the end of study measured using a validated rating scale.
Secondary outcomesMotor synkinesis or crocodile tears at the end of the study.1.Complete facial paralysis at the end of the study.2.Adverse events.3.Incomplete recovery at month six in severe cases.4.
Some trials have reported other symptoms (pain, discomfort, and embarrassment) as outcomes, but we did not considerthem in this review.
Search methods for identification of studies Electronic searches On 7 October 2014, we searched the Cochrane Neuromuscular Disease Group Specialized Register, the Cochrane CentralRegister of Controlled Trials (CENTRAL; 2014, Issue 9), MEDLINE (January 1966 to September 2014), EMBASE (January1980 to September 2014), and LILACS (January 1982 to September 2014). On the same date we also searched the NationalInstitute for Health Research Database of Abstracts and Reviews of Effects (DARE), Health Technology Assessment (HTA)database, and the National Health Service Economic Evaluation Database (NHS EED). We searched for registered trials inClinicalTrials.gov (www.clinicaltrials.gov) and in the World Health Organization International Clinical Trials Registry Platform (www.who.int/ictrp/en/).We have provided detailed search strategies in the appendices: Cochrane Neuromuscular Disease Group SpecializedRegister (Appendix 1), CENTRAL (Appendix 2), MEDLINE (Appendix 3), EMBASE (Appendix 4), and LILACS (Appendix 5).
Searching other resources We also reviewed the bibliographies of the identified trials and contacted trial authors and known experts in the field andrelevant drug companies to identify additional published or unpublished data.
Data collection and analysis Since a significant benefit of S for the early management of Bell’s palsy has been previously demonstrated (Lockhart 2009;Salinas 2010), the main focus of this review was to determine the effect of A in combination with S.Throughout we utilised the following notation:
AO: antiviral treatment alone or in combination with placeboAS: antiviral treatment in combination with corticosteroidsOO: placebo or no treatment onlyOS: corticosteroid treatment alone or in combination with placebo
Using these notations we conducted four comparisons altogether:AS versus OSAO versus OOAO versus OSAS versus OO
For an overall comparison of treatment with and without A we used the following notations:A: antiviral treatment in any combination (i.e. AO or AS);not-A: treatment not including antiviral treatment (i.e. OS or OO).
Selection of studies Six review authors working in pairs (FG and VM, DS and MS, IG and FS) scrutinised titles and abstracts to determineeligibility for review of the full-text article. At least two review authors independently assessed each full-text paper forrelevance, eligibility, and quality. We had no disagreements about inclusion. Two review authors independently analysedeach full-text report and selected studies for inclusion.
Data extraction and management Two review authors extracted data onto a data extraction form and double-checked data extraction in pairs. Two reviewauthors (IG and VM) agreed data input into the Cochrane authoring and statistical software, Review Manager 5 (RevMan2014). Any disagreements were discussed with FD to reach a resolution. We arranged translation of any papers wherenecessary.
026 Antiviral treatment for Bell's palsy (idiopathic facial paralysis)
6 / 40
Assessment of risk of bias in included studiesTwo review authors (IG and VM) independently assessed the risk of bias in included studies using the 'Risk of bias'methodology described in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011). FD reviewed the'Risk of bias' assessments. The review authors considered methods of randomisation and allocation concealment, blinding(of treatment administrator, participants, and outcome assessors), selective outcome reporting (for example failure to reportadverse events), and incomplete outcome data (that is dropouts). We assessed each trial as at high, low, or unclear risk ofbias for each of these criteria.
Measures of treatment effectAll our outcomes were dichotomous. We analysed the data as risk ratios (RRs) with corresponding 95% confidence interval(CI).When comparing studies that used differing symptom scores to assess outcome, we used the House-Brackmann scale whenavailable, as this was used most widely and could be compared with other scales.When assessing adverse events, we used the number of participants affected as opposed to the number of events, tofacilitate data comparison.
'Summary of findings' tableWe created a 'Summary of findings' table for the comparison 'Antivirals plus corticosteroids versus corticosteroids plusplacebo or no treatment' using the following outcomes.
Incomplete recovery at the end of the study (House-Brackmann scale)1.Motor synkinesis or crocodile tears at the end of the study (House-Brackmann scale)2.Adverse events3.
We used the five GRADE considerations (risk of bias, inconsistency of effect, imprecision, indirectness, and publication bias)to assess the quality of a body of evidence (studies that contribute data for the prespecified outcomes). We employedmethods and recommendations described in Section 8.5 and Chapter 12 of the Cochrane Handbook for Systematic Reviewsof Interventions (Higgins 2011) using GRADEpro software (GRADEpro 2008). We justified all decisions to down- or upgradethe quality of studies using footnotes.
Unit of analysis issues Each of the included studies carried out randomisation at the participant level. Nine trials used a simple parallel-group design(Adour 1996; Li 1997; De Diego 1998; Hato 2007 ; Kawaguchi 2007; Vázquez 2008; Yeo 2008; Lee 2013 ; Abdelghany 2013)and two trials used a factorial design (Sullivan 2007; Engström 2008).For studies with a factorial design, we aggregated groups according to whether or not antivirals were administered. Wedescribed details in the Results.
Dealing with missing dataWe contacted authors of two studies (Kawaguchi and Engström) for additional data that were required for analysis but whichwere not provided in their papers, and one (Engström) responded with data. We contacted a previous review author(Lockhart) for information on other studies and we received a response. We used the Kawaguchi 2007 data provided inprevious versions of this review.
Assessment of heterogeneity We used the I2 statistic to assess heterogeneity among the included studies in each analysis. If we found substantialunexplained heterogeneity, we reported it and explored possible causes.
Assessment of reporting biasesAs a result of the small number of included trials, we were not able to produce meaningful funnel plots to assess thelikelihood of publication bias (Egger 1997).
Data synthesisWe calculated a treatment effect using the Mantel-Haenszel method (Egger 2007). We used the random-effects modelwhere we found marked heterogeneity (I2 greater than 40%) between studies. If we had found little or no heterogeneity, wewould have used a fixed-effect analysis. The main outcome in all trials was complete recovery. For this review, the reviewauthors calculated the number of participants with incomplete recovery by subtracting the number of participants withcomplete recovery from the number of participants in the reference group.
Subgroup analysis and investigation of heterogeneity We calculated a subgroup analysis for incomplete recovery of people with severe Bell’s palsy at baseline using data fromfour trials (Hato 2007; Sullivan 2007; Engström 2008; Lee 2013). We excluded Abdelghany 2013 from this analysis sinceonly 12-month data were available. Severe Bell’s palsy was defined as severe to complete facial paralysis, graded as equalto or greater than V in the House-Brackmann grading system (Table 1), equal to or less than 20 in the Sunnybrook score (Table 2), and equal to or less than 20 in the Yanagihara score (Table 3).
Sensitivity analysis
026 Antiviral treatment for Bell's palsy (idiopathic facial paralysis)
7 / 40
We used sensitivity analyses to assess the effects of combining trials with and without additional treatments in an analysis ofA versus S and to assess the impact of length of follow-up on the results of the meta-analysis. We performed sensitivityanalyses to assess the potential difference in participant response to aciclovir versus valaciclovir and further sensitivityanalyses to investigate whether the exclusion of trials not meeting current best standards (that is those that had a high orunclear risk of bias in more than five categories or trials with less than 200 participants) would influence the results. Ananalysis investigated whether our conclusions were altered when we excluded the study with a follow-up of less than sixmonths (Adour 1996). Furthermore, in the analysis of AS versus OS in severe cases, we performed a sensitivity analysis toassess differences between trials in which only a subgroup of participants had severe Bell’s palsy versus the trials wherealmost all participants had severe Bell’s palsy.
Results Description of studies Results of the searchFor this review, we found 375 references in MEDLINE, 102 in EMBASE, 4 in LILACS, 28 in the Cochrane NeuromuscularDisease Group Specialized Register, and 39 in CENTRAL. We also found 12 additional trials in the Database of Abstracts ofReviews of Effects (DARE), one in the Health Technology Assessments (HTA), one in the Economic Evaluation Database(EED) and two by hand searching. We found two ongoing studies in the World Health Organization International ClinicalTrials Registry Platform (IRCT201109187575N1; IRCT2012062210087N1). See Figure 1 for a flow chart of the studyselection process.
Included studiesWe added four RCTs with 896 participants in total to the previous version of this review, which had seven trials and 1987participants.The 11 studies in the current review included 2883 participants (see Characteristics of included studies).Engström 2008 recruited 829 participants who were treated within 72 hours of onset and randomised by a computerisedmechanism in a two-stage process into four treatment groups: valaciclovir with prednisolone or valaciclovir with placebo orplacebo with prednisolone or double placebo in a factorial design. The trial was double blind (administrator and participant)for assessment of recovery status until the end of follow-up. Participants were assessed at onset, after 2 weeks (11 to 17days), and after 1, 2, 3, 6, and 12 months. Disease status was measured using the House-Brackmann grading system andthe Sunnybrook scale. Complete recovery status was defined by a Sunnybrook score of 100 and a House-Brackmann gradeof 1. Time to recovery was estimated. Data analysis included an assessment of treatment interaction.For this review, we aggregated groups and analysed AS plus AO versus OS plus OO as A versus not-A in order to achievethe most powerful comparison for the effect of treatment with valaciclovir on recovery rates at 12 months. We analysed therecovery rates 12 months after the onset of facial palsy using the Sunnybrook definition and defined complete recovery as aHouse-Brackmann grade of I.Hato 2007 randomised 296 participants within seven days of onset using sealed envelopes into two treatment groups:valaciclovir with prednisolone or placebo with prednisolone, to provide a comparison AS versus OS. The final analysisincluded 221 participants. Administrators were not blinded to the treatment allocation, but participants were blinded totreatment received. Those assessing recovery status were not blinded to treatment. Participants’ disease severity wasassessed using the Yanagihara 40-point scoring system; participants were considered completely recovered if attaining ascore greater than 36. Participants were assessed at onset and monthly thereafter for six months or until completelyrecovered if recovery occurred before six months.Sullivan 2007 recruited 551 participants who were treated within 72 hours of onset and randomised by a dedicated remotetelephone-computerised mechanism in a two-stage process into four treatment groups: aciclovir with prednisolone oraciclovir with placebo or placebo with prednisolone or double placebo in a factorial design. The trial was blinded foradministrator, participant, and assessment of recovery status until the end of follow-up. Participants were assessed at onset,after three months, and if still unwell at three months, after nine months. Recovery status was measured using the House-Brackmann scale, with complete recovery defined by House-Brackmann grade I. Data analysis included an assessment oftreatment interaction. Sullivan 2007 reported final outcomes on 496 completed participants at three months and nine monthsin treatment groups that were aggregated as for Engstrom.Yeo 2008 recruited 91 participants who were randomised to receive either aciclovir and prednisolone or prednisolone alone,to provide a comparison AS versus OS. Participants also received physical therapy and plasma volume expanders asadjuncts. The trial was double blind and investigators followed up participants for six months or until complete recovery.Recovery was assessed using the House-Brackmann scale and defined as a House-Brackmann score of II or less.Li 1997 recruited 51 participants within four days of onset of Bell's palsy. Participants were randomly assigned into twogroups, receiving either aciclovir plus prednisolone or prednisolone. Good recovery was defined as a House-Brackmannscore of II or I at month six. Li 1997 reported outcomes for 46 participants; five were lost to follow-up.Lee 2013 was a RCT in participants with severe to complete Bell’s palsy that used the House-Brackmann score forassessment. The trial included 201 participants with a score of V or more. After randomisation into two groups, participantsreceived either famciclovir plus prednisolone simultaneously or prednisolone alone. Recovery rate was designated as scoresof I or II on the House-Brackmann scale at month six.Vázquez 2008 included 42 participants and reported outcomes at 6 and 12 months using the Sunnybrook Facial Grading
026 Antiviral treatment for Bell's palsy (idiopathic facial paralysis)
8 / 40
System. Scores of greater than 90 were defined as a satisfactory recovery. Participants in the intervention group weretreated with prednisone and valaciclovir and in the control group with prednisone and placebo. The main study outcome wasrate of participants with total recovery at six months’ follow-up in each group and average time to recovery in each group.Adour 1996 recruited 119 participants, of whom 99 were included in the published analysis. The study was double blind andplacebo controlled. Participants were recruited within three or days or less of onset of paralysis and received either aciclovirand prednisolone or placebo and prednisolone. The study duration was four months; participants were reviewed at twoweeks, two months, and four months. This was a single-centre study. The Facial Paralysis Recovery Index (FPRI) was usedto measure facial function; the primary trial outcome was incomplete recovery defined by a FPRI of 7 or less.De Diego 1998 recruited 113 participants, including 101 in the final analysis. Participants were randomly assigned totreatment. Baseline assessment was carried out within 48 hours of onset of symptoms. Participants received either aciclovirfor 10 days or prednisolone for 16 days (reducing dose). Reviews were scheduled for 1, 3, 6, and 12 weeks after initialcontact, with further contact if persistent incomplete recovery was noted. The primary study outcome was recovery asdefined by a House-Brackmann score of II or less or a Facial Paralysis Recovery Profile of 8 or more. The report did not givethe final length of follow-up but stated that it continued "until complete recovery or stabilization of the paralysis".Abdelghany 2013 conducted a three-armed RCT, including 625 participants within 72 hours of onset of Bell's palsy.Randomisation was carried out using a sealed-envelope method. Participants were randomly assigned into three treatmentgroups: aciclovir and prednisolone, prednisolone and placebo, or aciclovir and placebo. Follow-up visits were performed atday 14 and at 1, 2, 3, 6, and 12 months. Disease status was measured using the Sunnybrook scale. Complete recovery wasdefined as a Sunnybrook score of 100. Data analysis included an analysis for treatment interaction. The authors reportedfinal outcomes for 603 participants at 12 months; 22 participants were lost to follow-up.Kawaguchi 2007 recruited 150 participants who were treated within seven days of onset and randomised using sealedenvelopes into two treatment groups: valaciclovir plus prednisolone or prednisolone alone. There was inadequate blinding ofthe clinician. Kawaguchi et al. provided unpublished data on incomplete recovery for the previous update. Participants wereassessed at 1, 2, 3, 4, 5, and 6 months after inclusion using the Yanagihara scale. We could not contact the authors to obtaindata for this review, but we have included the data previously published in this review.
Excluded studiesAuthors of the previous version of this review excluded Antunes 2000 because of incomplete data in 44 participants. Despiteour attempts to contact the authors, there was still insufficient information for the data to be usefully included in the analyses.The authors of a previous version of this review reassessed the inclusion of the two studies that were awaiting assessment (de Aquino 2001; Roy 2005). Dr. D. Allen, the author of a previous version of this review, attempted to contact the lead authorof the former paper for clarification of the data, but this was not forthcoming and so we have excluded this trial because of alack of adequate information. The latter study recruited 82 participants, of whom 18 dropped out, and compared aciclovir plusmethylprednisolone to methylprednisolone alone, reporting no benefit from the addition of aciclovir. The authors did notprovide outcome data in the abstract, which appeared in a journal supplement, and according to the search strategiesemployed, the trial has not been published as a full paper to date. We excluded this trial due to a lack of adequateinformation.A further study was classified as awaiting assessment in the previous version of this review (Inanli 2001). This paper wasincluded in a systematic review and a meta-analysis (de Almeida 2009; Goudakos 2009). We excluded the paper from thecurrent review because we could not find it in print or electronic form. See Characteristics of excluded studies.Overall, we excluded five studies for not being RCTs (Ibarrondo 1999; Axelsson 2003; Hato 2003; Hultcrantz 2005; Ahangar2006); two for having a very short follow-up (Zhou 1999; Chen 2005); three because reports provided insufficient informationto assess methods or outcomes (Antunes 2000; de Aquino 2001; Roy 2005); four because of high risk of bias in severaldomains: Minnerop 2008 (inadequate randomisation, unblinded, 50 of 167 participants lost to follow-up), Ramos Macias1992 (only abstract available, 15 of 45 participants had Ramsay Hunt syndrome and were given intravenous therapy), Roy2005 (lack of outcome data, as described above), Shahidullah 2011 (inadequate randomisation, unblinded, 39 of 107participants lost to follow-up); and one paper was not available (Inanli 2001).
Ongoing studiesWe identified two trial reports in a search of ClinicalTrials.gov just prior to completion of the review. The current status ofthese trials is unknown; we will assess them fully in a future update of the review. See Ongoing studies.
Risk of bias in included studies We have summarised our 'Risk of bias' assessments in Figure 2.
Allocation (selection bias)Three studies were at low risk of selection bias, being adequately randomised with allocation concealment (Adour 1996;Sullivan 2007; Engström 2008). Two other studies were at low risk of bias from randomisation but at high risk of bias frominadequate allocation concealment (Kawaguchi 2007; Lee 2013). In the remaining studies, the risk of bias from the method ofrandomisation was unclear, and the risk of bias for allocation concealment was either unclear, in Li 1997; Hato 2007;Vázquez 2008; Yeo 2008; Abdelghany 2013, or, high, in De Diego 1998.
Blinding (performance bias and detection bias)Adour 1996, Li 1997, Sullivan 2007, Engström 2008, and Vázquez 2008 were described as double blind and placebo
026 Antiviral treatment for Bell's palsy (idiopathic facial paralysis)
9 / 40
controlled. Lee 2013 did not use a placebo to ensure blinding. Abdelghany 2013 was blinded using a placebo, but the reviewauthors considered blinding possibly inadequate, as the method of ensuring independence of research data collection fromclinical care was unclear. De Diego 1998, Hato 2007, and Kawaguchi 2007 did not describe blinding or placebo use. TheYeo 2008 report stated that the study was double blind, however, the text does not describe this, so we assessed the risk ofbias for blinding as unclear.
Incomplete outcome data (attrition bias)All studies except Yeo 2008 reported frequencies, and often reasons, for failure to complete follow-up.Most trials reported a dropout rate of 10% or less (Li 1997; De Diego 1998; Kawaguchi 2007; Sullivan 2007; Engström 2008;Vázquez 2008; Yeo 2008; Abdelghany 2013). Exceptions were Lee 2013 with a dropout rate of 13.1%, Adour 1996 with adropout rate of 17%, and Hato 2007 with a dropout rate of 25%.
Selective reporting (reporting bias)All studies except Adour 1996 and Kawaguchi 2007 reported all their intended primary outcomes. Adour 1996 failed to reporton audiometry and stapedial reflex testing. Engström 2008 reported all primary outcomes; secondary outcomes werereported in later published papers (Axelsson 2012; Berg 2012).Six studies did not report adverse events (Li 1997; De Diego 1998; Kawaguchi 2007; Yeo 2008; Abdelghany 2013; Lee 2013).
Other potential sources of biasDiagnostic criteriaNine studies gave adequate information (Li 1997; De Diego 1998; Hato 2007; Kawaguchi 2007; Sullivan 2007; Engström2008; Vázquez 2008; Yeo 2008; Lee 2013). All studies explicitly mentioned a diagnosis of Bell's palsy and stated that theyhad considered and excluded other causes of facial palsy. Two trials, Hato 2007 and Kawaguchi 2007, retrospectivelyexcluded participants on the basis of positive serology for herpes simplex or varicella zoster viruses. Lee 2013 excludedparticipants who did not fulfil inclusion criteria, without specifying the reasons. Two studies mentioned referral to specialistsfor diagnostic confirmation (Sullivan 2007; Engström 2008). The remaining study, Adour 1996, stated participants werediagnosed with Bell's palsy but did not give any further information.
Outcome criteriaAll studies used referenced facial function scoring systems to grade recovery from facial paralysis. Adour 1996 and De Diego1998 used the Facial Paralysis Recovery Profile and Adour 1996 also used the Facial Paralysis Recovery Index. Hato 2007and Kawaguchi 2007 used the Yanagihara scoring system (Yanagihara 2003), which has a validated system for conversionto the House-Brackmann scale (House 1985). Li 1997, Sullivan 2007, Engström 2008, Yeo 2008, and Lee 2013 presentedresults using the House-Brackmann scale (House 1985). Engström 2008 supplemented this with use of the Sunnybrookscale to minimise the effects of interrater variability (Ross 1996). Abdelghany 2013 used the Sunnybrook scale forassessment of facial paralysis. Vázquez 2008 used a facial grading scale related to Sunnybrook (Ross 1996).
Statistical analysisTen of the 11 studies analysed gave adequate detail; they clearly stated and then used appropriate statistical tests. OnlyHato 2007 scored 'unclear' in this category, as it did not state the tests used.
Baseline differences between groupsEight of the eleven trials were adequate in this category. De Diego 1998 found a significant difference in rates ofhypertension between the two groups, but further analysis revealed that there was no significant difference in trial outcomesas a result. Kawaguchi 2007 reported a significant difference between mean ages of the treatment groups, but furtheranalysis of the age distribution using Chi2 test revealed no significant difference. Lee 2013 reported a later onset of thetreatment in the combination treatment without significance. Abdelghany 2013 reported later initiation of treatment inparticipants with severe Bell's palsy than with moderate or mild Bell's palsy.
Effects of interventions As the included trials reported different intervals and lengths of follow-up, we performed the analyses on data reported atthree months (De Diego 1998), six months (Li 1997; Hato 2007; Kawaguchi 2007; Vázquez 2008; Yeo 2008; Lee 2013), ninemonths (Sullivan 2007), or 12 months (Engström 2008; Abdelghany 2013) after the start of treatment.For the subgroup analysis of incomplete recovery in participants with severe Bell’s palsy at onset, we either extracted data atmonth six, in Hato 2007 and Lee 2013, or imputed data to month six, in Sullivan 2007 and Engström 2008.
Antivirals plus corticosteroids versus corticosteroids plus placebo or no treatment (AS versus OS)Incomplete recoveryThis comparison contained nine studies with 1715 participants in total (Adour 1996; Li 1997; Hato 2007; Kawaguchi 2007;Sullivan 2007; Engström 2008; Vázquez 2008; Yeo 2008; Abdelghany 2013). We excluded Lee 2013 from this analysis dueto its selected participants (severe cases only).The risk ratio (RR) of incomplete recovery at the end of the study showed a statistically significant difference between ASand OS treatments, favouring AS over OS. The RR of incomplete recovery was 0.80 (95% confidence interval (CI) 0.65 to
026 Antiviral treatment for Bell's palsy (idiopathic facial paralysis)
10 / 40
0.98). Heterogeneity was substantial when we used the fixed-effect model (Chi2 = 16.83, df = 8 (P value = 0.03), I2 = 52%);we used the random-effects model to partially correct for this (RR 0.69, 95% CI 0.47 to 1.02) (Analysis 1.1, Figure 3).
Motor synkinesis or crocodile tearsAdour 1996, Engström 2008, and Abdelghany 2013 provided data for the outcome motor synkinesis or crocodile tears at theend of the study (Analysis 1.2). The analysis included 869 participants and showed a significant difference between AS andOS (RR 0.73, 95% CI 0.54 to 0.99).
Adverse eventsAdverse events were not significantly less likely in AS versus OS (RR 1.18, 95% CI 0.83 to 1.69). This analysis included datafrom 877 participants in three studies (Hato 2007; Sullivan 2007; Engström 2008) (Analysis 1.3).
Antivirals versus corticosteroids (A versus S)Incomplete recoveryThis comparison contained four studies (De Diego 1998; Sullivan 2007; Engström 2008; Abdelghany 2013).All studies (1169 participants) provided data for our primary outcome of incomplete recovery at the end of the study.Incomplete recovery was significantly less common in the participants treated with A versus those treated with S. Initialcalculations using the fixed-effect model showed a RR of 1.85 (95% CI 1.52 to 2.26), but with a high degree of heterogeneity(Chi2 = 8.60, P value = 0.04, I2 = 65%). We repeated the analysis using the random-effects model to partially correct for this,and the RR was 2.09 (95% CI 1.36 to 3.20) (Analysis 2.1, Figure 4).
Motor synkinesis or crocodile tearsDe Diego 1998, Engström 2008, and Abdelghany 2013 provided data for the outcome motor synkinesis or crocodile tears atthe end of the study (Analysis 2.2). The analysis included 873 participants and showed significantly fewer sequelae in S thanin A (RR 1.44, 95% CI 1.11 to 1.85).
Adverse eventsFewer participants experienced adverse events in the antiviral group than the corticosteroids group (RR 0.85, 95% CI 0.57 to1.28, Analysis 2.3), but the CIs included the possibility of the opposite effect.
Antivirals plus corticosteroids versus placebo (AS versus OO)Incomplete recoveryThis comparison contained two studies and outcome data on 658 participants (Sullivan 2007; Engström 2008).Incomplete recovery at the end of the study was significantly much less common with AS versus OO (RR 0.56, 95% CI 0.41to 0.76) (Analysis 3.1, Figure 5).
Motor synkinesis or crocodile tearsNot reported
Adverse eventsAdverse events (among 649 participants) were slightly but not significantly more common with AS than with OO (RR 1.14,95% CI 0.79 to 1.65) (Analysis 3.2).
Antivirals versus placebo (AO versus OO)Incomplete recoveryFor two trials (658 participants) that compared antivirals versus placebo without any complicating additional treatment, theRR of incomplete recovery was non-significant (RR 1.10, 95% CI 0.87 to 1.40) (Sullivan 2007; Engström 2008). Theheterogeneity was moderate (Chi2 = 0.63, P value = 0.20, I2 = 39%) (Analysis 4.1).
Motor synkinesis or crocodile tearsNot reported
Adverse eventsAdverse events (among 651 participants) were not significantly more common in OO (RR 0.83, 95% CI 0.56 to 1.24) (Analysis 4.2).
Antivirals plus corticosteroids versus corticosteroids plus placebo or no treatment (AS versus OS) in severecasesIncomplete recoveryFor this comparison, we extracted data from four studies with 478 participants (Hato 2007; Sullivan 2007; Engström 2008;Lee 2013). The RR of incomplete recovery in this subgroup was just significantly less in AS versus OS (RR 0.64, 95% CI0.41 to 0.99, random-effects model). The heterogeneity was moderate (Chi2 = 5.2, P value = 0.16, I2 = 42%) (see Analysis5.1, Figure 6).
026 Antiviral treatment for Bell's palsy (idiopathic facial paralysis)
11 / 40
Sensitivity analysesWe investigated the effect of using the comparison AS versus OS by performing further analysis to investigate whetherexcluding the study with a follow-up of less than six months altered our conclusions (Adour 1996). We performed furthersensitivity analyses to assess the potential difference in participant response to aciclovir, in Adour 1996, Li 1997, Sullivan2007, Yeo 2008, and Abdelghany 2013, versus valaciclovir, in Hato 2007, Engström 2008, and Vázquez 2008.We performed sensitivity analyses to investigate whether the exclusion of trials not meeting current best standards (that is ahigh or unclear risk of bias in more than five categories or trials with less than 200 participants) would influence the results.
Antivirals plus corticosteroids versus corticosteroids plus placebo or no treatment (AS versus OS)When we excluded Adour 1996, the RR of incomplete recovery was 0.76 (95% CI 0.52 to 1.10, n = 1616). This representsno significant changes referring to the main analysis (RR 0.69, 95% CI 0.47 to 1.02, n = 1715, Analysis 1.1) with the removalof outcomes that reported follow-up at six months or less.When we performed sensitivity analyses to assess the potential difference in participant response to aciclovir versusvalaciclovir, we found no significant difference from the results of the main analysis (Analysis 1.1). When we excluded Adour1996, Li 1997, Kawaguchi 2007, Sullivan 2007, Yeo 2008, and Abdelghany 2013, the RR of incomplete recovery was 0.74(95% CI 0.42 to 1.31, n = 678). When we excluded trials using aciclovir, the RR was 0.65 (95% CI 0.36 to 1.16, n = 678).Exclusion of trials with fewer than 200 participants (Adour 1996; Li 1997; Vázquez 2008; Yeo 2008), and trials not meetingcurrent best standards (Li 1997; Hato 2007; Kawaguchi 2007; Vázquez 2008; Yeo 2008; Abdelghany 2013), did notsignificantly change the results of Analysis 1.1 (RR 0.90, 95% CI 0.66 to 1.24, n = 1438 and RR 0.81, 95% CI 0.38 to 1.74, n= 766, respectively).
Antivirals plus corticosteroids versus corticosteroids plus placebo or no treatment (AS versus OS) in severecasesWe performed a sensitivity analysis to assess differences between Sullivan 2007 and Engström 2008, where only asubgroup of participants had severe Bell’s palsy, versus Hato 2007 and Lee 2013, where almost all participants had severeBell’s palsy. The results showed a remarkable difference between the analyses: RR 0.47 (95% CI 0.30 to 0.75) versus RR0.82 (95% CI 0.57 to 1.17).
Discussion Summary of main resultsThe results of this updated review do not show a clear benefit from combining antivirals with steroids in comparison withsteroids alone for people with Bell’s palsy. This is based on the moderate but non-significant reduction of incompleterecovery (RR 0.69, 95% CI 0.47 to 1.02, n = 1715). Negative results are supported by heterogeneity and inconsistency ofoutcomes across studies. Comparing the data of participants with severe Bell’s palsy, we demonstrated a smaller but justsignificant reduction in the rate of incomplete recovery for the combination treatment at month six.Remarkably, the data of Sullivan 2007, Vázquez 2008, and Abdelghany 2013 showed a non-significant detrimental effect onrecovery compared with Hato 2007, Engström 2008, and Lee 2013 (Analysis 1.1). Possible reasons for this are that the trialswere heterogeneous in ways that we discuss below.The reduction in incomplete recovery was significantly better in participants receiving corticosteroids compared withantivirals. The treatment effect of placebo was significantly lower than for antivirals plus corticosteroids.
Overall completeness and applicability of evidenceWhen antivirals were compared to placebo, there was a slight but non-significant difference in the recovery of participants infavour of placebo. This result was influenced by the Sullivan 2007 trial, which suggested that antiviral treatment had a non-significant detrimental effect on recovery.Heterogeneity may be due to clinical variation, for example in study participant characteristics, disease severity at baseline,and delay in receiving treatment or different type of antiviral agent used and the small numbers in the subgroups. Equally,variation may be due to methodological considerations such as method of randomisation, the use of blinding, the choice ofoutcome assessment measures and recovery cut-off points or the trial duration. In particular, Li 1997, Hato 2007, Kawaguchi2007, and Abdelghany 2013 had methodological weaknesses in baseline group assessment, completeness of follow-up, andadequacy of blinding. Any of these factors could result in bias and introduce inaccuracy. The heterogeneity was exacerbatedin many studies by keeping the inclusion criteria fairly broad; this maximises data inclusion and therefore power, but resultsmust be interpreted with this in mind. The sensitivity analysis of participants with severe Bell’s palsy showed a remarkabledifference between the studies with data from subgroups and trials with a complete dataset. The different definitions ofsevere Bell’s palsy depending on the symptom scores used in the trial should also be considered a potential source ofheterogeneity.Sensitivity analysis of trials with data with less than a six-month endpoint showed results similar to those achieved with thewhole-group analysis, that is it detected no significant effect of shortened time of follow-up.Similarly, subgroup analysis of the relative treatment difference with different antivirals showed no significant changes in theoutcomes for combined treatment versus treatment with steroids alone. Given this finding, it is unlikely that different antiviralcompounds will have a significant effect on the outcome 'Incomplete recovery at the end of the study', despite the differencein bio-availability (Sullivan 2007).
026 Antiviral treatment for Bell's palsy (idiopathic facial paralysis)
12 / 40
We found insufficient data to examine any of the other variables reported in the studies, such as pain, quality of life, andvariation in response due to time to treatment and severity at onset. These variables may be useful for hypothesis generationfor future work in this area.From the data available for comparison of motor synkinesis or crocodile tears at the end of the study, the results of fourstudies with a total of 1358 participants (Adour 1996; De Diego 1998; Engström 2008; Abdelghany 2013), were significant intwo comparisons. De Diego 1998, Engström 2008, and Abdelghany 2013 compared antivirals with corticosteroids and foundfewer episodes of these long-term sequelae in the corticosteroid-treated participants, while Adour 1996, Engström 2008, andAbdelghany 2013 compared antivirals plus corticosteroids with corticosteroids alone and found fewer episodes of thesesequelae in the antiviral treatment group. A degree of clinical heterogeneity (different clinical assessment scales used) andmethodological heterogeneity (different treatment regimens and follow-up plans) limit the interpretation of these data.Adverse event data were available in three studies giving comparison data for 1528 participants (Hato 2007; Sullivan 2007;Engström 2008). None of the comparisons showed significant differences in adverse events between arms. We could find nocorrelation with specific treatment within these results.We found variation in the clinical endpoints chosen as defining recovery: Sullivan 2007 and Engström 2008 used House-Brackmann Grade 1, while Yeo 2008 used House-Brackmann Grade 2. The other studies used a variety of different scalesthat show more or less equivalence to these. We have provided details of the symptoms scales and comparison whereavailable (Table 1, Table 2, Table 3).Neither Kawaguchi 2007 nor Yeo 2008 found a significant association between time to treatment and final recovery status.We found differences in severity at recruitment: Li 1997, Hato 2007, Vázquez 2008, Yeo 2008, and Lee 2013 included amore severe spectrum of palsy than Engström 2008 and Abdelghany 2013. Hato 2007, Engström 2008, and Abdelghany2013 stratified participants by severity-of-disease status at onset. Hato 2007 found that in cases of complete or severe palsy,the recovery rate for the combination treatment was significantly greater than for participants treated with steroids only. Lee2013 included only severe cases and found a significantly higher rate of recovery in the group receiving a combinationtreatment using famciclovir. In contrast, Engström 2008 and Abdelghany 2013 could not confirm these findings in treatmentof participants with severe Bell's palsy, whereas Sullivan 2007 showed a non-significant detrimental effect on completerecovery.The primary-outcome result raises another important consideration, that is the health economic issues: a 10-day course ofaciclovir 400 mg 5 times per day costs GBP 5.33 (USD 8.75, EUR 6.47); an equivalent course of valaciclovir costs GBP 8.50(USD 13.96, EUR 10.31). Famciclovir is significantly more expensive at GBP 138.79 (USD 227.89, EUR 168.42). A 10-daycourse of prednisolone (two 25 mg tablets daily) costs about GBP 7.14 (USD 11.72, EUR 8.66) (BNF 2013). These cost dataare specific to the UK market (2013); costs vary significantly in other countries (Hernández 2008).
Quality of the evidenceWe assessed the quality of evidence for the treatment of Bell’s palsy with antivirals combined with corticosteroids comparedto corticosteroids alone or with placebo to be high. However, due to the heterogeneity of the results of included RCTs, wedowngraded the evidence from high to moderate. High-quality evidence was available for other outcomes such as motorsynkinesis and crocodile tears. We found the quality of the evidence for adverse events to be moderate because only threeof the included trials reported this outcome.
Potential biases in the review processTo help ensure that decisions about which studies to include in this review were reproducible, two review authors repeatedthe review process (we divided the studies into three groups). We made no distinction on the experience and expertise ofeach review author in the reviewing pairs. Regarding applying the eligibility criteria and assessing the relevance of studies,review authors were aware of the names of the study authors, institutions, journal of publication, and results. FS and FDwere excluded from the assessment of their own trial (Sullivan 2007). We had no final disagreements about which studiesshould be included.According to previous practice in this review, we excluded several studies and a published abstract that provided insufficientinformation. As a result there could be some risk of publication and selective reporting bias due to data from some studiesbeing unavailable.
Agreements and disagreements with other studies or reviewsWe have included studies conducted in Asia, North and Middle America, and Europe. It is possible that genetic differences indrug metabolism or response or even different aetiological processes may account for some of the observed variation inresponse.We found two systematic reviews and two meta-analyses comparing steroids and antivirals for the treatment of Bell’s palsy (de Almeida 2009; Goudakos 2009; Quant 2009; Numthavaj 2011). De Almeida et al. compared any corticosteroid treatmentwith antivirals and included 18 trials in the meta-analysis. Most of the trials did not meet the inclusion criteria for this review.De Almeida states a benefit of corticosteroids for people with Bell’s palsy and the probability of an additional benefit whencorticosteroids are combined with antivirals. A systematic review and meta-analysis by Goudakos et al. comparedcorticosteroids with corticosteroids plus antivirals for the treatment of Bell’s palsy. This review included only four trials andomitted other important studies, for example Engström 2008, which is the largest trial conducted on this topic. Goudakos didnot find an additional benefit from combining corticosteroids with antivirals. The meta-analyses by Numthavaj and Quanteach included six trials for analysis, with a great overlap. In both papers the authors reported higher rates of recovery when
026 Antiviral treatment for Bell's palsy (idiopathic facial paralysis)
13 / 40
steroids were combined with antivirals compared to steroids alone, but the difference was non-significant.
Authors' conclusions Implications for practice Moderate-quality evidence showed a significant benefit of the combination of corticosteroids with antivirals compared withcorticosteroids alone in severe Bell’s palsy. Moderate-quality evidence from RCTs showed a potentially meaningful clinicalbenefit from combination therapy compared to corticosteroids alone or with placebo and no significant benefit from antiviralscompared to placebo, for the treatment of Bell's palsy. We found no significant increase in adverse events from the use ofantivirals compared with either placebo or corticosteroids.
Implications for research The novel finding in this analysis of a small, just significant benefit in terms of incomplete recovery of severe cases of Bell'spalsy through the combination of antivirals with corticosteroids may merit further investigation. Additional work in this areacould address the question of the best treatment for severe Bell’s palsy raised by the possible causes of heterogeneity insome of the comparisons in this review. This may be achieved through a meta-analysis of individual participant data.Depending upon the results of this analysis, an adequately powered randomised controlled trial in people with severe Bell’spalsy comparing different potential treatment options such as antiviral agents or immune modulators may be indicated.More work is needed to assess the likelihood of long-term cosmetic sequelae, which should be reported in each further trial.There is no further need to conduct trials with a placebo group on this topic, as a clear benefit from steroid therapy is evident.Moreover, antivirals should be tested in combination with steroids and not alone in future studies. Subgroup analysis ofexisting data and future studies should be done to assess the impact on the outcome of variables such as time fromdiagnosis until treatment, severity of palsy at baseline, and age of participants at presentation. Work assessing a wider rangeof endpoints, such as quality of life and perceived disability, should be undertaken with the goal of developing a betterunderstanding of Bell's palsy for the affected person.
Acknowledgements Dr J Sipe, Mrs L Dunn, Dr D Allen, Dr P Lockhart, Ms N Comerford, and Ms M Pitkethly authored the previous editions of thisreview; we are very grateful for their hard work and enthusiasm. We also extend our thanks to Ruth Brassington for hervaluable assistance with the writing process; to Angela Gunn, who provided search results; and to the CochraneNeuromuscular Disease Group for their extensive technical assistance and support.This project was supported by the National Institute for Health Research via Cochrane Infrastructure funding to the CochraneNeuromuscular Disease Group. The views and opinions expressed therein are those of the review authors and do notnecessarily reflect those of the Systematic Reviews Programme, NIHR, NHS, or the Department of Health. The CochraneNeuromuscular Disease Group is also supported by the MRC Centre for Neuromuscular Diseases.
Contributions of authors All review authors contributed to the review and data extraction process. Dr I Gagyor wrote the first draft of the report withadditional clinical input from Professor F Sullivan, Dr V Madhok, Dr F Daly, Dr D Somasundara, and Dr M Sullivan. Dr IGagyor incorporated the work into the existing review and was responsible for the 'Risk of bias' assessment, data analysis,and use of the RevMan 5 software.
Declarations of interest Ildiko Gagyor: None knownVishnu B Madhok: I have received payment for reviewing a review prepared by BMJ Evidence.Fergus Daly: The fact that I am a named author on one of the included articles (Sullivan 2007) did not influence in any waymy thinking, presentation or contribution to this review.Dhruvashree Somasundara: None knownMichael Sullivan: None knownFiona Gammie: None knownFrank Sullivan: I am the author of one of the included studies (Sullivan 2007). I have no other known conflicts of interest.
Differences between protocol and review There were several differences between the published review protocol and the previous update of the review. These mainlyreflected changes over time to treatment options and Cochrane methodology. As for the previous update, the search forstudies now includes treatment with valaciclovir and famciclovir, either alone or in combination with any other therapy, toreflect the treatment options now available for Bell's palsy. We undertook the methodological assessment according toChapter 8 of the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011).As implemented in previous versions of the review, we documented in this update the selection criteria relating to high risk ofbias and study duration. The minimum study duration was three months. As in previous updates, we used study quality as anexclusion criterion, especially in trials with a high risk of bias in several domains.For this update, seven review authors read a selection of papers, reviewed them for quality, and extracted data. The review
026 Antiviral treatment for Bell's palsy (idiopathic facial paralysis)
14 / 40
authors distributed the work so that at least two review authors reviewed each paper. IG performed the final 'Risk of bias'assessment, which FS and VM independently reviewed.We focused this search on people who were immunocompetent, which we did not stipulate in the original protocol. We didthis as treatment protocols for immunocompromised individuals and treatment response may differ significantly from otherindividuals and, as such, could not be fully explored in this analysis.The authors of the previous update widened the outcome criteria to include outcomes at the end of the study, as opposed toone year or six months after treatment, in order to allow for the inclusion of a maximal number of published studies. Thisprevious update included studies with durations of three to 12 months, which allowed for maximum data inclusion. As it wasunderstood that this method might introduce significant heterogeneity to the results, the review authors included a sensitivityanalysis looking at outcomes in participants in studies reporting at 12 weeks or less and 6 months or less in order to assessthe influence this had on the robustness of published results. The authors of the current review accepted these changes. Forthe subgroup analysis of incomplete recovery, we extracted data on the severity Bell’s palsy at month six or imputed usingthe last measure carried forward.We have added in this update the outcome 'incomplete recovery in severe cases', measured at month six or imputed usingthe last measure carried forward. We defined severe cases as a severe-to-complete facial paralysis, graded as equal to orgreater than V in the House-Brackmann grading system, equal to or less than 20 in the Sunnybrook score, and equal to orless than 20 in the Yanagihara score. We did not include the data of Abdelghany 2013 in this analysis, as only 12-monthsdata were available.We have modified the outcome measures since the previous review to take into account the heterogeneity of this group ofstudies.We have altered incomplete recovery to include the range of definitions used by the included studies in order to allow formaximum data capture: As opposed to the previous definition of moderate dysfunction, the term now includes participantswith a lack of full function. By this definition, more participants will be classified as 'incomplete recovery'.The previous update replaced 'adverse events attributable to antiviral treatment' with 'adverse events'; in studies where bothagents are administered, it is difficult to assess which agent is causing the adverse event. Similarly, even when only anantiviral is being prescribed, it is difficult to know whether a specific event should be attributed to the medication or to anotherintercurrent cause. The level of detailed analysis of adverse events in studies did not permit such a judgement to be made.This review reported adverse events for each analysis separately.The review authors added a 'Summary of findings' table and additional sections to the methods to comply with currentCochrane standards.We performed sensitivity analyses to investigate whether the exclusion of trials not meeting current best standards (that is ahigh or unclear risk of bias in more than five categories or trials with less than 200 participants) would influence the results.
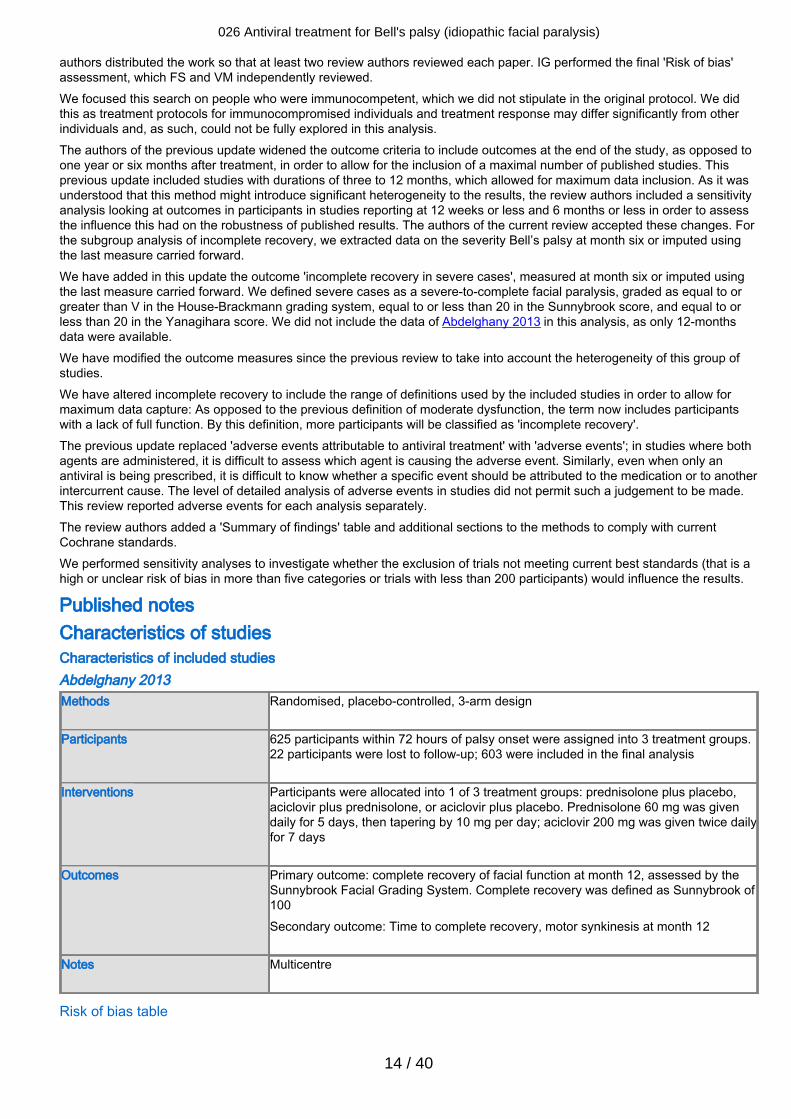
Published notes Characteristics of studiesCharacteristics of included studies Abdelghany 2013Methods Randomised, placebo-controlled, 3-arm design
Participants 625 participants within 72 hours of palsy onset were assigned into 3 treatment groups.
22 participants were lost to follow-up; 603 were included in the final analysis
Interventions Participants were allocated into 1 of 3 treatment groups: prednisolone plus placebo,aciclovir plus prednisolone, or aciclovir plus placebo. Prednisolone 60 mg was givendaily for 5 days, then tapering by 10 mg per day; aciclovir 200 mg was given twice dailyfor 7 days
Outcomes Primary outcome: complete recovery of facial function at month 12, assessed by theSunnybrook Facial Grading System. Complete recovery was defined as Sunnybrook of100Secondary outcome: Time to complete recovery, motor synkinesis at month 12
Notes Multicentre
Risk of bias table
026 Antiviral treatment for Bell's palsy (idiopathic facial paralysis)
15 / 40
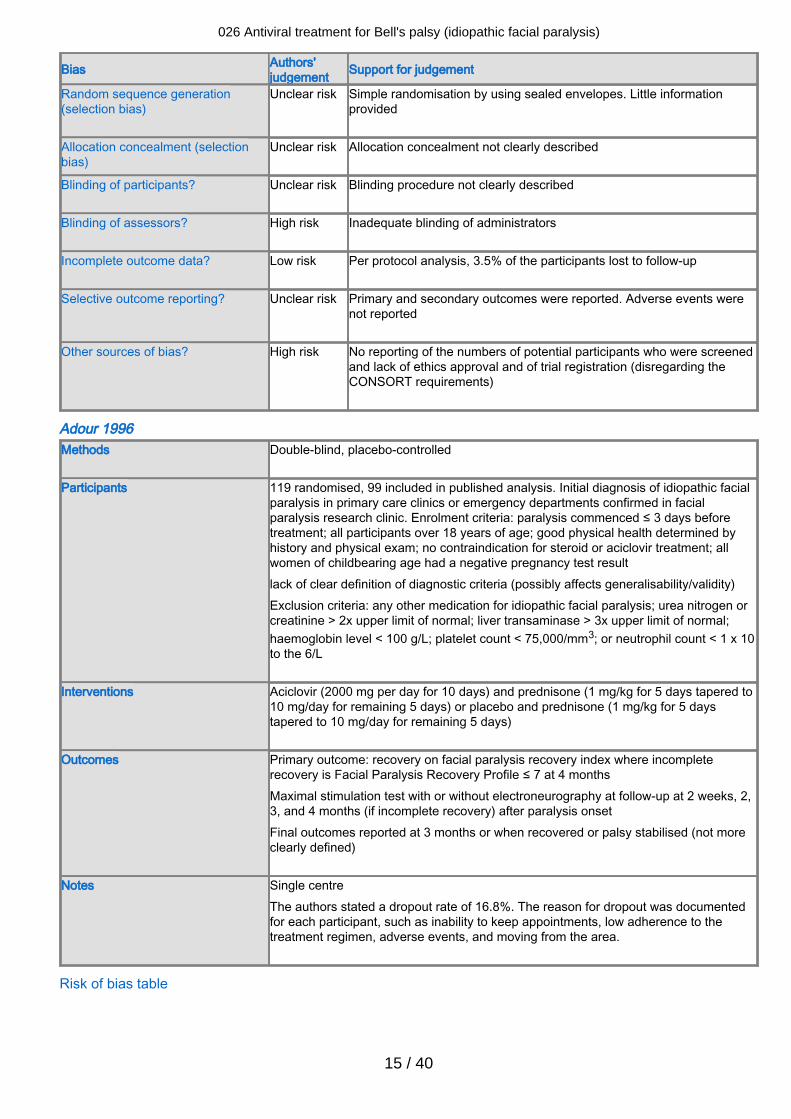
Bias Authors'judgement Support for judgement
Random sequence generation(selection bias)
Unclear risk Simple randomisation by using sealed envelopes. Little informationprovided
Allocation concealment (selectionbias)
Unclear risk Allocation concealment not clearly described
Blinding of participants? Unclear risk Blinding procedure not clearly described
Blinding of assessors? High risk Inadequate blinding of administrators
Incomplete outcome data? Low risk Per protocol analysis, 3.5% of the participants lost to follow-up
Selective outcome reporting? Unclear risk Primary and secondary outcomes were reported. Adverse events werenot reported
Other sources of bias? High risk No reporting of the numbers of potential participants who were screenedand lack of ethics approval and of trial registration (disregarding theCONSORT requirements)
Adour 1996Methods Double-blind, placebo-controlled
Participants 119 randomised, 99 included in published analysis. Initial diagnosis of idiopathic facial
paralysis in primary care clinics or emergency departments confirmed in facialparalysis research clinic. Enrolment criteria: paralysis commenced ≤ 3 days beforetreatment; all participants over 18 years of age; good physical health determined byhistory and physical exam; no contraindication for steroid or aciclovir treatment; allwomen of childbearing age had a negative pregnancy test resultlack of clear definition of diagnostic criteria (possibly affects generalisability/validity)Exclusion criteria: any other medication for idiopathic facial paralysis; urea nitrogen orcreatinine > 2x upper limit of normal; liver transaminase > 3x upper limit of normal;haemoglobin level < 100 g/L; platelet count < 75,000/mm3; or neutrophil count < 1 x 10to the 6/L
Interventions Aciclovir (2000 mg per day for 10 days) and prednisone (1 mg/kg for 5 days tapered to10 mg/day for remaining 5 days) or placebo and prednisone (1 mg/kg for 5 daystapered to 10 mg/day for remaining 5 days)
Outcomes Primary outcome: recovery on facial paralysis recovery index where incompleterecovery is Facial Paralysis Recovery Profile ≤ 7 at 4 monthsMaximal stimulation test with or without electroneurography at follow-up at 2 weeks, 2,3, and 4 months (if incomplete recovery) after paralysis onsetFinal outcomes reported at 3 months or when recovered or palsy stabilised (not moreclearly defined)
Notes Single centreThe authors stated a dropout rate of 16.8%. The reason for dropout was documentedfor each participant, such as inability to keep appointments, low adherence to thetreatment regimen, adverse events, and moving from the area.
Risk of bias table
026 Antiviral treatment for Bell's palsy (idiopathic facial paralysis)
16 / 40
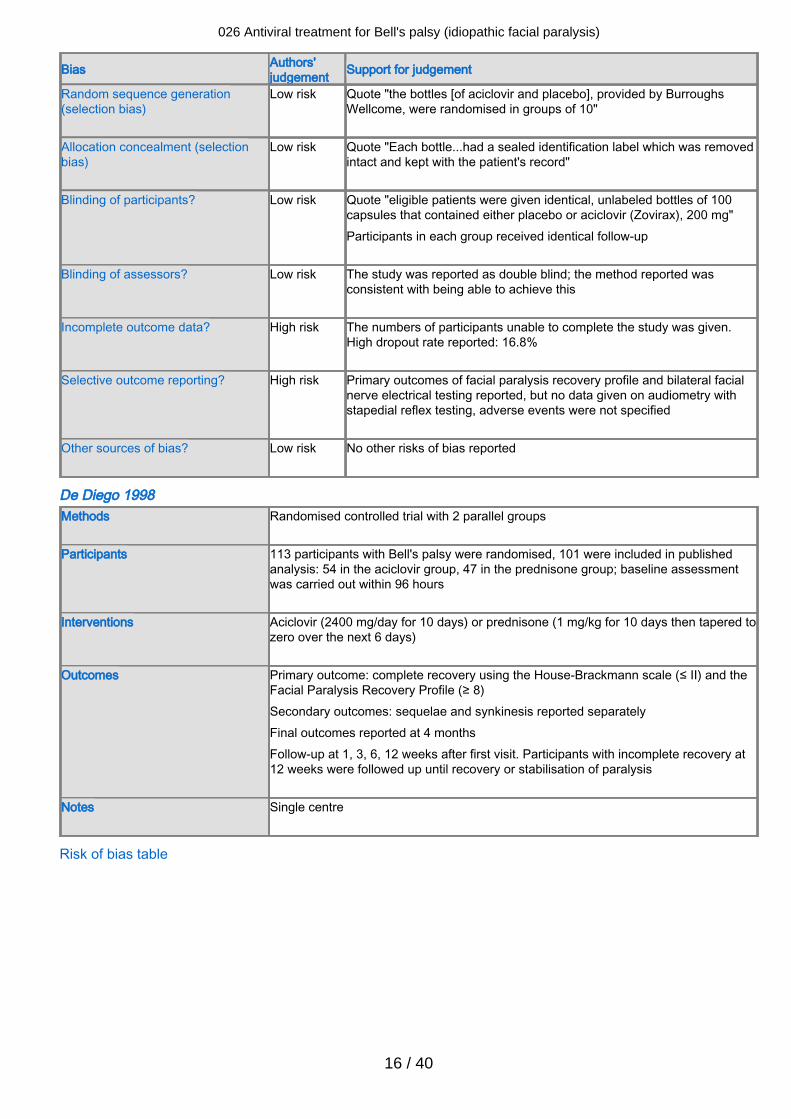
Bias Authors'judgement Support for judgement
Random sequence generation(selection bias)
Low risk Quote "the bottles [of aciclovir and placebo], provided by BurroughsWellcome, were randomised in groups of 10"
Allocation concealment (selectionbias)
Low risk Quote "Each bottle...had a sealed identification label which was removedintact and kept with the patient's record"
Blinding of participants? Low risk Quote "eligible patients were given identical, unlabeled bottles of 100capsules that contained either placebo or aciclovir (Zovirax), 200 mg"Participants in each group received identical follow-up
Blinding of assessors? Low risk The study was reported as double blind; the method reported wasconsistent with being able to achieve this
Incomplete outcome data? High risk The numbers of participants unable to complete the study was given.High dropout rate reported: 16.8%
Selective outcome reporting? High risk Primary outcomes of facial paralysis recovery profile and bilateral facialnerve electrical testing reported, but no data given on audiometry withstapedial reflex testing, adverse events were not specified
Other sources of bias? Low risk No other risks of bias reported
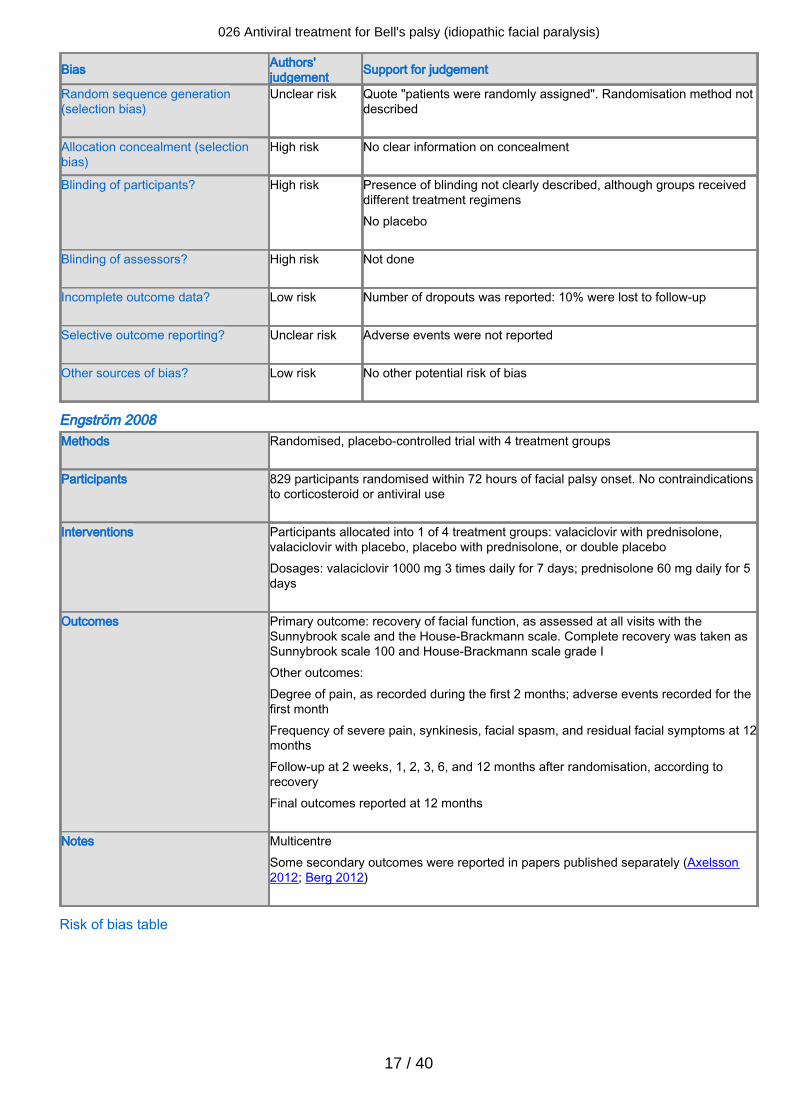
De Diego 1998Methods Randomised controlled trial with 2 parallel groups
Participants 113 participants with Bell's palsy were randomised, 101 were included in published
analysis: 54 in the aciclovir group, 47 in the prednisone group; baseline assessmentwas carried out within 96 hours
Interventions Aciclovir (2400 mg/day for 10 days) or prednisone (1 mg/kg for 10 days then tapered tozero over the next 6 days)
Outcomes Primary outcome: complete recovery using the House-Brackmann scale (≤ II) and theFacial Paralysis Recovery Profile (≥ 8)Secondary outcomes: sequelae and synkinesis reported separatelyFinal outcomes reported at 4 monthsFollow-up at 1, 3, 6, 12 weeks after first visit. Participants with incomplete recovery at12 weeks were followed up until recovery or stabilisation of paralysis
Notes Single centre
Risk of bias table
026 Antiviral treatment for Bell's palsy (idiopathic facial paralysis)
17 / 40
Bias Authors'judgement Support for judgement
Random sequence generation(selection bias)
Unclear risk Quote "patients were randomly assigned". Randomisation method notdescribed
Allocation concealment (selectionbias)
High risk No clear information on concealment
Blinding of participants? High risk Presence of blinding not clearly described, although groups receiveddifferent treatment regimensNo placebo
Blinding of assessors? High risk Not done
Incomplete outcome data? Low risk Number of dropouts was reported: 10% were lost to follow-up
Selective outcome reporting? Unclear risk Adverse events were not reported
Other sources of bias? Low risk No other potential risk of bias
Engström 2008Methods Randomised, placebo-controlled trial with 4 treatment groups
Participants 829 participants randomised within 72 hours of facial palsy onset. No contraindications
to corticosteroid or antiviral use
Interventions Participants allocated into 1 of 4 treatment groups: valaciclovir with prednisolone,valaciclovir with placebo, placebo with prednisolone, or double placeboDosages: valaciclovir 1000 mg 3 times daily for 7 days; prednisolone 60 mg daily for 5days
Outcomes Primary outcome: recovery of facial function, as assessed at all visits with theSunnybrook scale and the House-Brackmann scale. Complete recovery was taken asSunnybrook scale 100 and House-Brackmann scale grade IOther outcomes:Degree of pain, as recorded during the first 2 months; adverse events recorded for thefirst monthFrequency of severe pain, synkinesis, facial spasm, and residual facial symptoms at 12monthsFollow-up at 2 weeks, 1, 2, 3, 6, and 12 months after randomisation, according torecoveryFinal outcomes reported at 12 months
Notes MulticentreSome secondary outcomes were reported in papers published separately (Axelsson2012; Berg 2012)
Risk of bias table
026 Antiviral treatment for Bell's palsy (idiopathic facial paralysis)
18 / 40
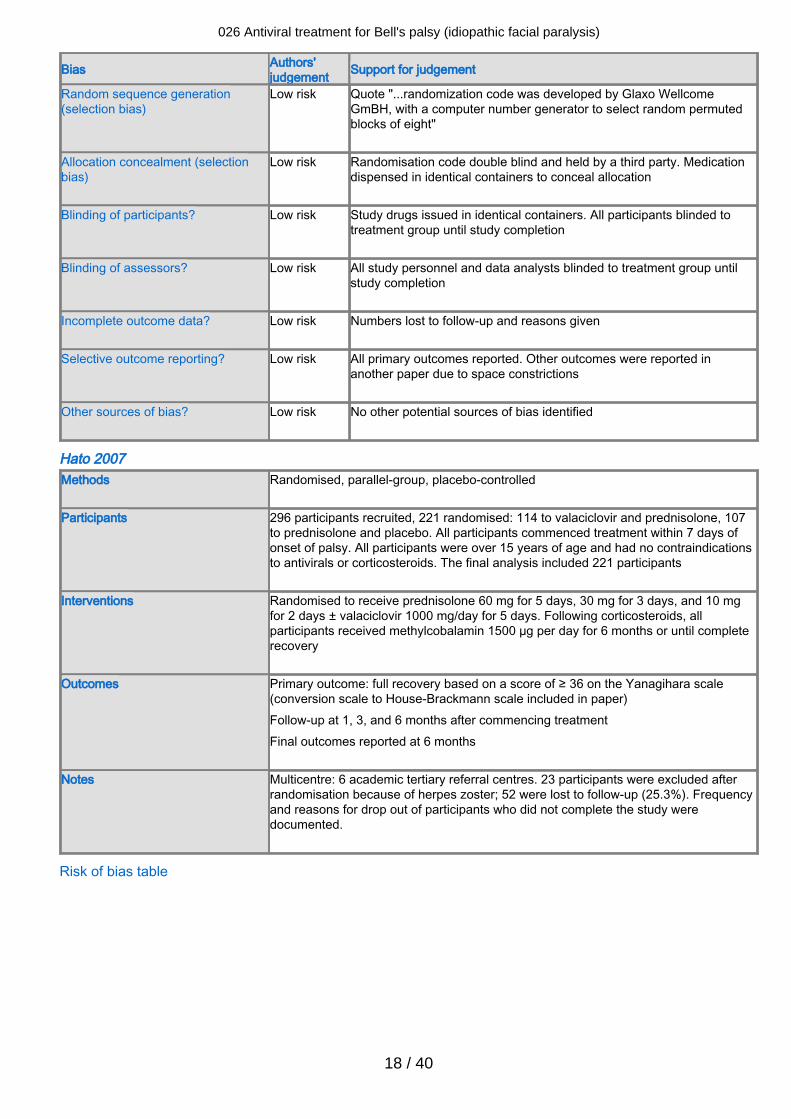
Bias Authors'judgement Support for judgement
Random sequence generation(selection bias)
Low risk Quote "...randomization code was developed by Glaxo WellcomeGmBH, with a computer number generator to select random permutedblocks of eight"
Allocation concealment (selectionbias)
Low risk Randomisation code double blind and held by a third party. Medicationdispensed in identical containers to conceal allocation
Blinding of participants? Low risk Study drugs issued in identical containers. All participants blinded totreatment group until study completion
Blinding of assessors? Low risk All study personnel and data analysts blinded to treatment group untilstudy completion
Incomplete outcome data? Low risk Numbers lost to follow-up and reasons given
Selective outcome reporting? Low risk All primary outcomes reported. Other outcomes were reported inanother paper due to space constrictions
Other sources of bias? Low risk No other potential sources of bias identified
Hato 2007Methods Randomised, parallel-group, placebo-controlled
Participants 296 participants recruited, 221 randomised: 114 to valaciclovir and prednisolone, 107
to prednisolone and placebo. All participants commenced treatment within 7 days ofonset of palsy. All participants were over 15 years of age and had no contraindicationsto antivirals or corticosteroids. The final analysis included 221 participants
Interventions Randomised to receive prednisolone 60 mg for 5 days, 30 mg for 3 days, and 10 mgfor 2 days ± valaciclovir 1000 mg/day for 5 days. Following corticosteroids, allparticipants received methylcobalamin 1500 µg per day for 6 months or until completerecovery
Outcomes Primary outcome: full recovery based on a score of ≥ 36 on the Yanagihara scale(conversion scale to House-Brackmann scale included in paper)Follow-up at 1, 3, and 6 months after commencing treatmentFinal outcomes reported at 6 months
Notes Multicentre: 6 academic tertiary referral centres. 23 participants were excluded afterrandomisation because of herpes zoster; 52 were lost to follow-up (25.3%). Frequencyand reasons for drop out of participants who did not complete the study weredocumented.
Risk of bias table
026 Antiviral treatment for Bell's palsy (idiopathic facial paralysis)
19 / 40
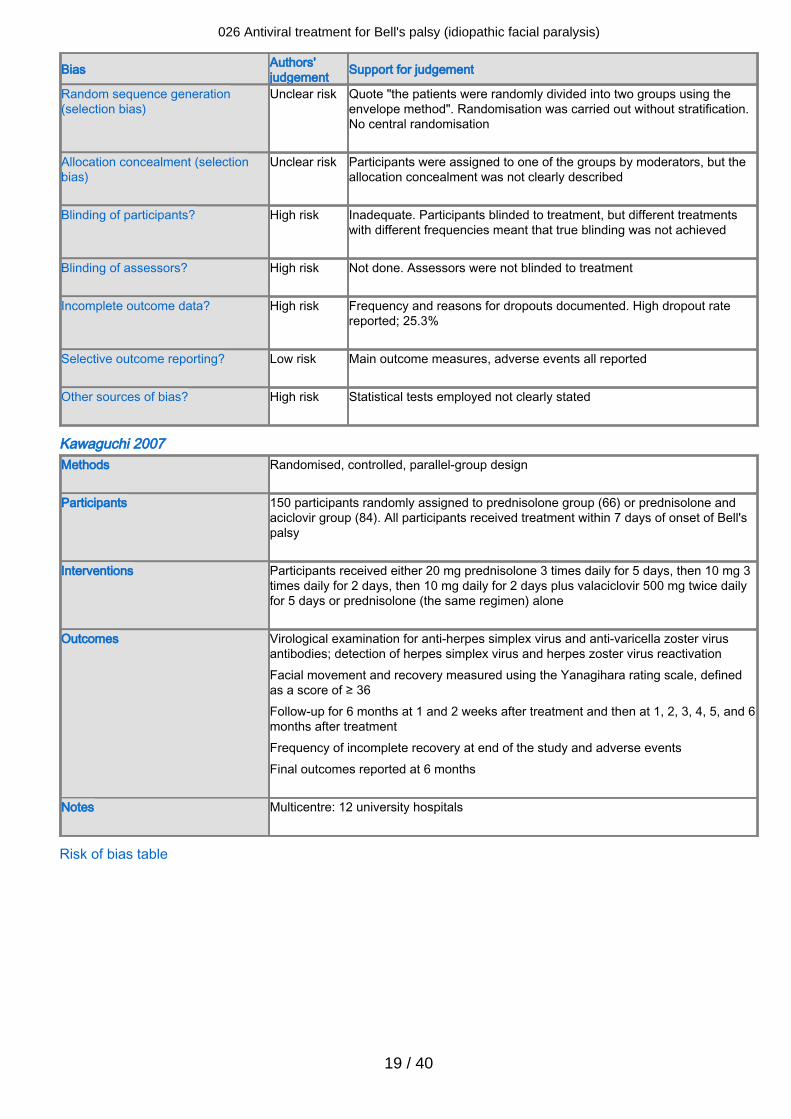
Bias Authors'judgement Support for judgement
Random sequence generation(selection bias)
Unclear risk Quote "the patients were randomly divided into two groups using theenvelope method". Randomisation was carried out without stratification.No central randomisation
Allocation concealment (selectionbias)
Unclear risk Participants were assigned to one of the groups by moderators, but theallocation concealment was not clearly described
Blinding of participants? High risk Inadequate. Participants blinded to treatment, but different treatmentswith different frequencies meant that true blinding was not achieved
Blinding of assessors? High risk Not done. Assessors were not blinded to treatment
Incomplete outcome data? High risk Frequency and reasons for dropouts documented. High dropout ratereported; 25.3%
Selective outcome reporting? Low risk Main outcome measures, adverse events all reported
Other sources of bias? High risk Statistical tests employed not clearly stated
Kawaguchi 2007Methods Randomised, controlled, parallel-group design
Participants 150 participants randomly assigned to prednisolone group (66) or prednisolone and
aciclovir group (84). All participants received treatment within 7 days of onset of Bell'spalsy
Interventions Participants received either 20 mg prednisolone 3 times daily for 5 days, then 10 mg 3times daily for 2 days, then 10 mg daily for 2 days plus valaciclovir 500 mg twice dailyfor 5 days or prednisolone (the same regimen) alone
Outcomes Virological examination for anti-herpes simplex virus and anti-varicella zoster virusantibodies; detection of herpes simplex virus and herpes zoster virus reactivationFacial movement and recovery measured using the Yanagihara rating scale, definedas a score of ≥ 36Follow-up for 6 months at 1 and 2 weeks after treatment and then at 1, 2, 3, 4, 5, and 6months after treatmentFrequency of incomplete recovery at end of the study and adverse eventsFinal outcomes reported at 6 months
Notes Multicentre: 12 university hospitals
Risk of bias table
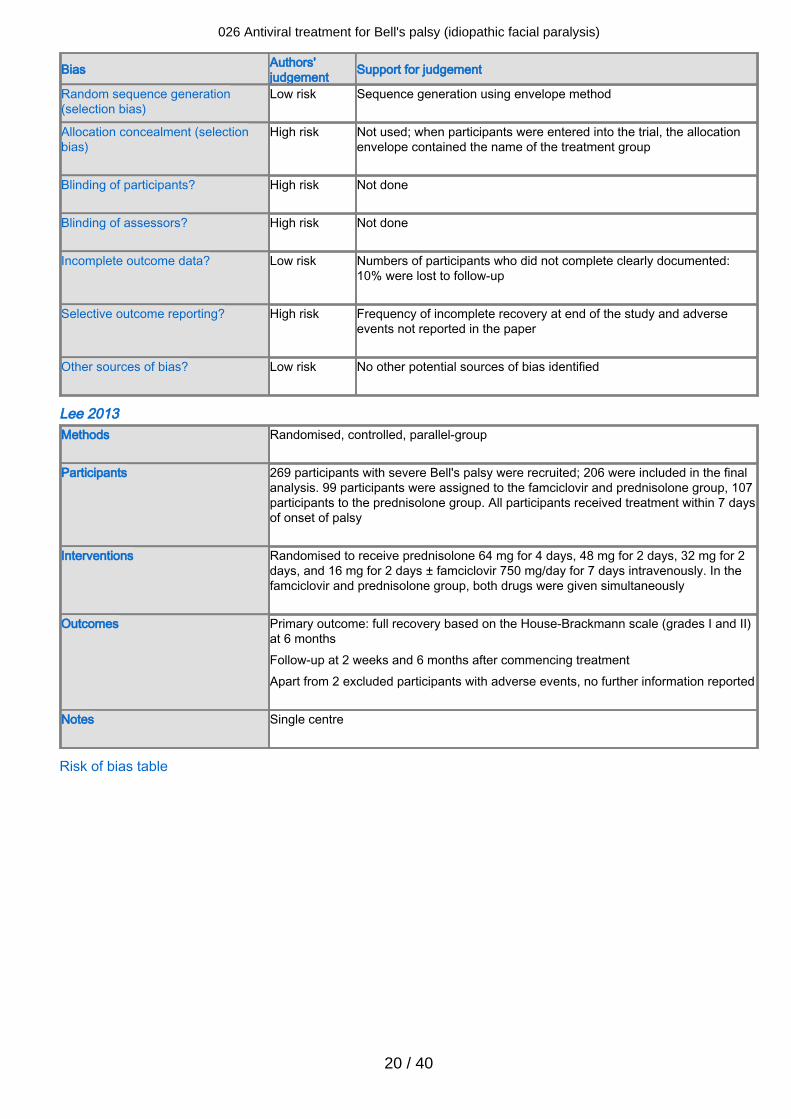
026 Antiviral treatment for Bell's palsy (idiopathic facial paralysis)
20 / 40
Bias Authors'judgement Support for judgement
Random sequence generation(selection bias)
Low risk Sequence generation using envelope method
Allocation concealment (selectionbias)
High risk Not used; when participants were entered into the trial, the allocationenvelope contained the name of the treatment group
Blinding of participants? High risk Not done
Blinding of assessors? High risk Not done
Incomplete outcome data? Low risk Numbers of participants who did not complete clearly documented:10% were lost to follow-up
Selective outcome reporting? High risk Frequency of incomplete recovery at end of the study and adverseevents not reported in the paper
Other sources of bias? Low risk No other potential sources of bias identified
Lee 2013Methods Randomised, controlled, parallel-group
Participants 269 participants with severe Bell's palsy were recruited; 206 were included in the final
analysis. 99 participants were assigned to the famciclovir and prednisolone group, 107participants to the prednisolone group. All participants received treatment within 7 daysof onset of palsy
Interventions Randomised to receive prednisolone 64 mg for 4 days, 48 mg for 2 days, 32 mg for 2days, and 16 mg for 2 days ± famciclovir 750 mg/day for 7 days intravenously. In thefamciclovir and prednisolone group, both drugs were given simultaneously
Outcomes Primary outcome: full recovery based on the House-Brackmann scale (grades I and II)at 6 monthsFollow-up at 2 weeks and 6 months after commencing treatmentApart from 2 excluded participants with adverse events, no further information reported
Notes Single centre
Risk of bias table
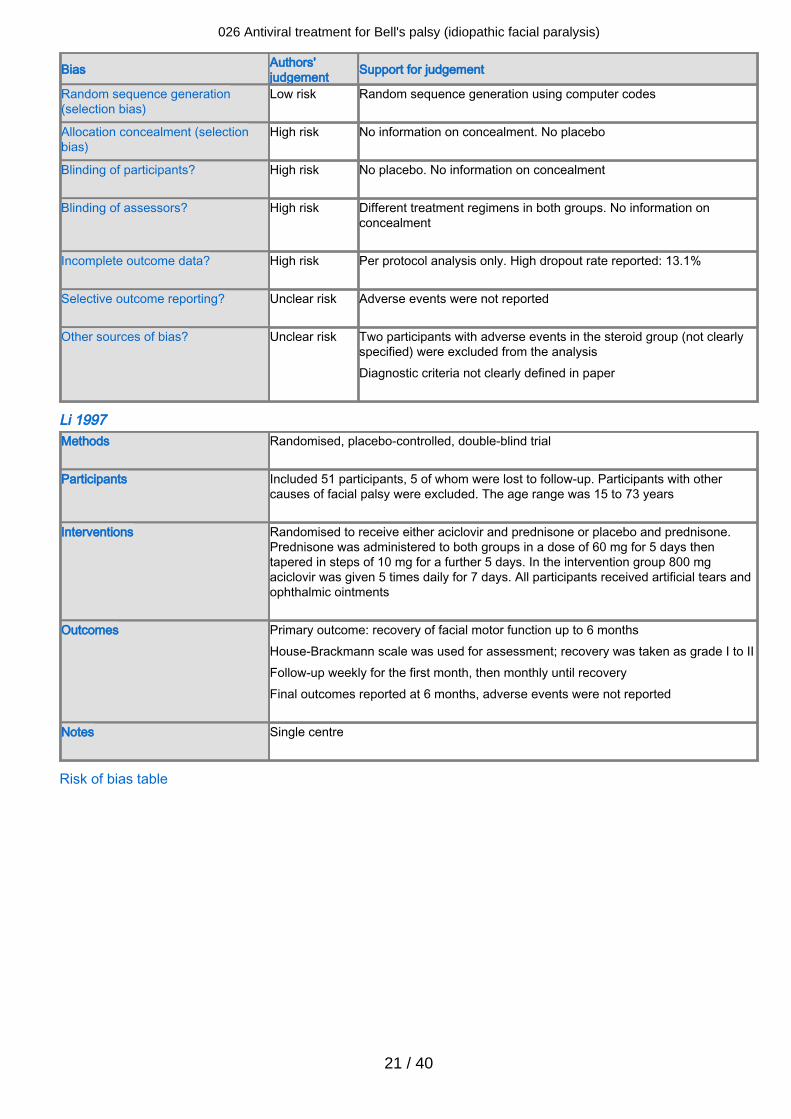
026 Antiviral treatment for Bell's palsy (idiopathic facial paralysis)
21 / 40
Bias Authors'judgement Support for judgement
Random sequence generation(selection bias)
Low risk Random sequence generation using computer codes
Allocation concealment (selectionbias)
High risk No information on concealment. No placebo
Blinding of participants? High risk No placebo. No information on concealment
Blinding of assessors? High risk Different treatment regimens in both groups. No information onconcealment
Incomplete outcome data? High risk Per protocol analysis only. High dropout rate reported: 13.1%
Selective outcome reporting? Unclear risk Adverse events were not reported
Other sources of bias? Unclear risk Two participants with adverse events in the steroid group (not clearlyspecified) were excluded from the analysisDiagnostic criteria not clearly defined in paper
Li 1997Methods Randomised, placebo-controlled, double-blind trial
Participants Included 51 participants, 5 of whom were lost to follow-up. Participants with other
causes of facial palsy were excluded. The age range was 15 to 73 years
Interventions Randomised to receive either aciclovir and prednisone or placebo and prednisone.Prednisone was administered to both groups in a dose of 60 mg for 5 days thentapered in steps of 10 mg for a further 5 days. In the intervention group 800 mgaciclovir was given 5 times daily for 7 days. All participants received artificial tears andophthalmic ointments
Outcomes Primary outcome: recovery of facial motor function up to 6 monthsHouse-Brackmann scale was used for assessment; recovery was taken as grade I to IIFollow-up weekly for the first month, then monthly until recoveryFinal outcomes reported at 6 months, adverse events were not reported
Notes Single centre
Risk of bias table
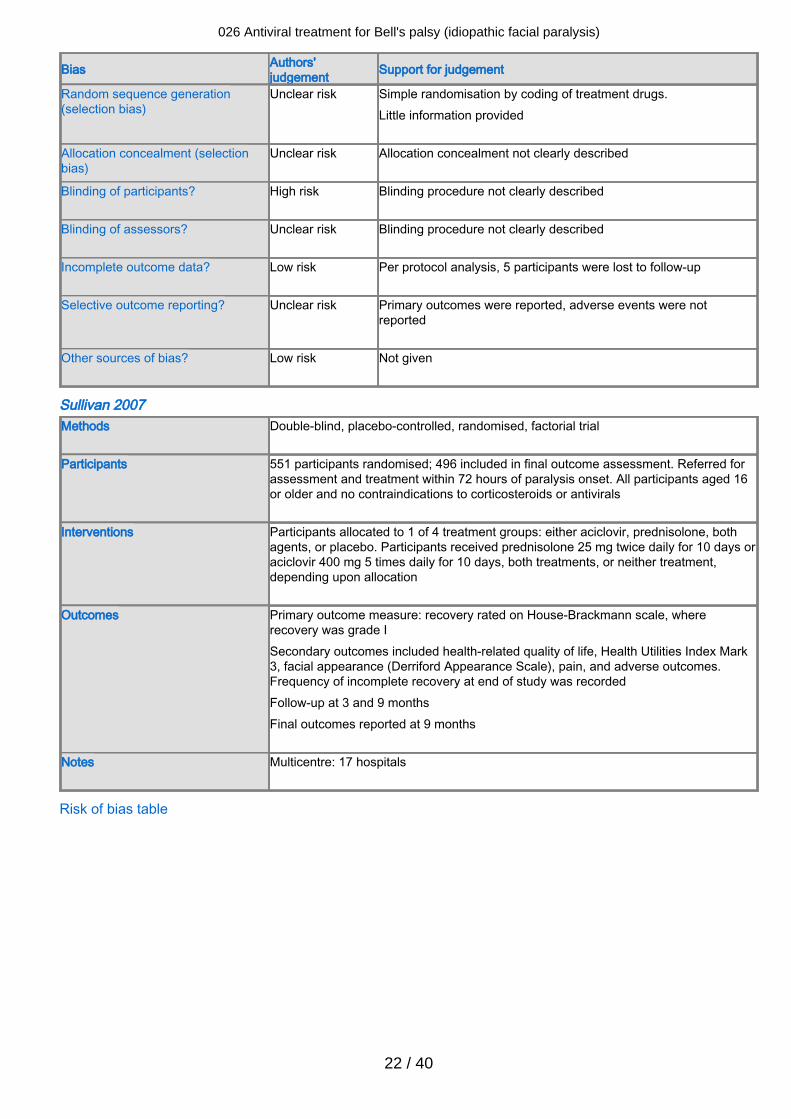
026 Antiviral treatment for Bell's palsy (idiopathic facial paralysis)
22 / 40
Bias Authors'judgement Support for judgement
Random sequence generation(selection bias)
Unclear risk Simple randomisation by coding of treatment drugs.Little information provided
Allocation concealment (selectionbias)
Unclear risk Allocation concealment not clearly described
Blinding of participants? High risk Blinding procedure not clearly described
Blinding of assessors? Unclear risk Blinding procedure not clearly described
Incomplete outcome data? Low risk Per protocol analysis, 5 participants were lost to follow-up
Selective outcome reporting? Unclear risk Primary outcomes were reported, adverse events were notreported
Other sources of bias? Low risk Not given
Sullivan 2007Methods Double-blind, placebo-controlled, randomised, factorial trial
Participants 551 participants randomised; 496 included in final outcome assessment. Referred for
assessment and treatment within 72 hours of paralysis onset. All participants aged 16or older and no contraindications to corticosteroids or antivirals
Interventions Participants allocated to 1 of 4 treatment groups: either aciclovir, prednisolone, bothagents, or placebo. Participants received prednisolone 25 mg twice daily for 10 days oraciclovir 400 mg 5 times daily for 10 days, both treatments, or neither treatment,depending upon allocation
Outcomes Primary outcome measure: recovery rated on House-Brackmann scale, whererecovery was grade ISecondary outcomes included health-related quality of life, Health Utilities Index Mark3, facial appearance (Derriford Appearance Scale), pain, and adverse outcomes.Frequency of incomplete recovery at end of study was recordedFollow-up at 3 and 9 monthsFinal outcomes reported at 9 months
Notes Multicentre: 17 hospitals
Risk of bias table
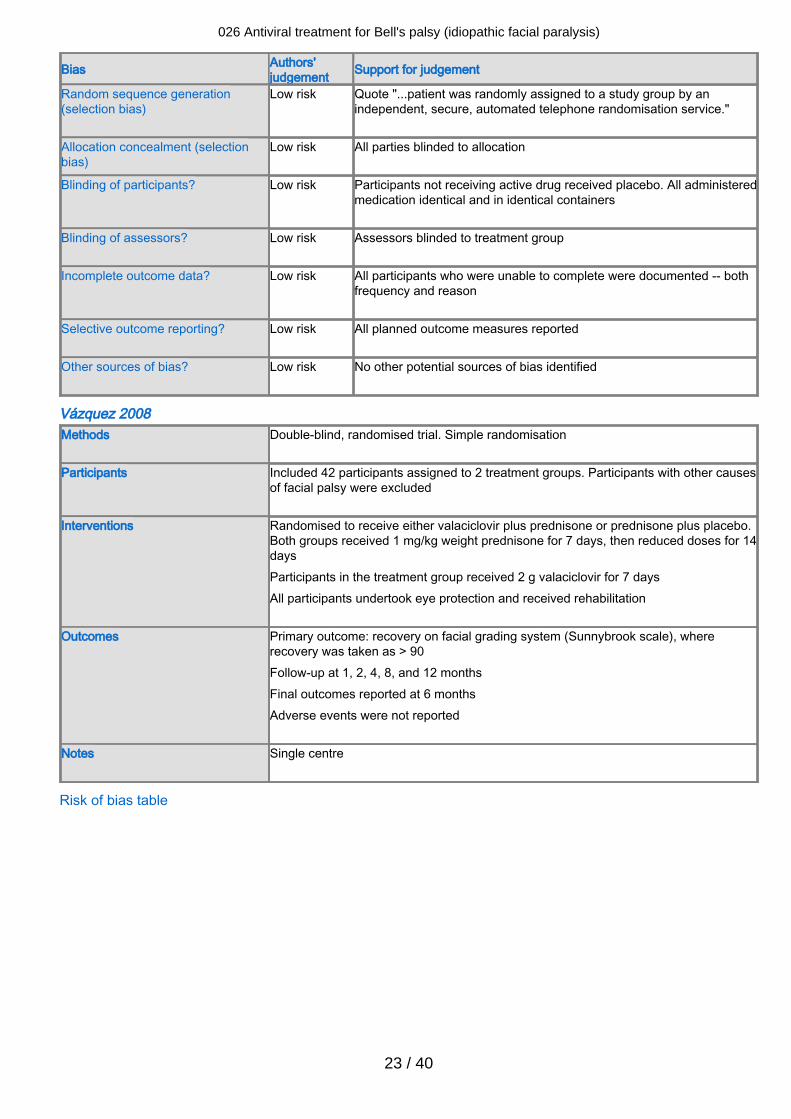
026 Antiviral treatment for Bell's palsy (idiopathic facial paralysis)
23 / 40
Bias Authors'judgement Support for judgement
Random sequence generation(selection bias)
Low risk Quote "...patient was randomly assigned to a study group by anindependent, secure, automated telephone randomisation service."
Allocation concealment (selectionbias)
Low risk All parties blinded to allocation
Blinding of participants? Low risk Participants not receiving active drug received placebo. All administeredmedication identical and in identical containers
Blinding of assessors? Low risk Assessors blinded to treatment group
Incomplete outcome data? Low risk All participants who were unable to complete were documented -- bothfrequency and reason
Selective outcome reporting? Low risk All planned outcome measures reported
Other sources of bias? Low risk No other potential sources of bias identified
Vázquez 2008Methods Double-blind, randomised trial. Simple randomisation
Participants Included 42 participants assigned to 2 treatment groups. Participants with other causes
of facial palsy were excluded
Interventions Randomised to receive either valaciclovir plus prednisone or prednisone plus placebo.Both groups received 1 mg/kg weight prednisone for 7 days, then reduced doses for 14daysParticipants in the treatment group received 2 g valaciclovir for 7 daysAll participants undertook eye protection and received rehabilitation
Outcomes Primary outcome: recovery on facial grading system (Sunnybrook scale), whererecovery was taken as > 90Follow-up at 1, 2, 4, 8, and 12 monthsFinal outcomes reported at 6 monthsAdverse events were not reported
Notes Single centre
Risk of bias table
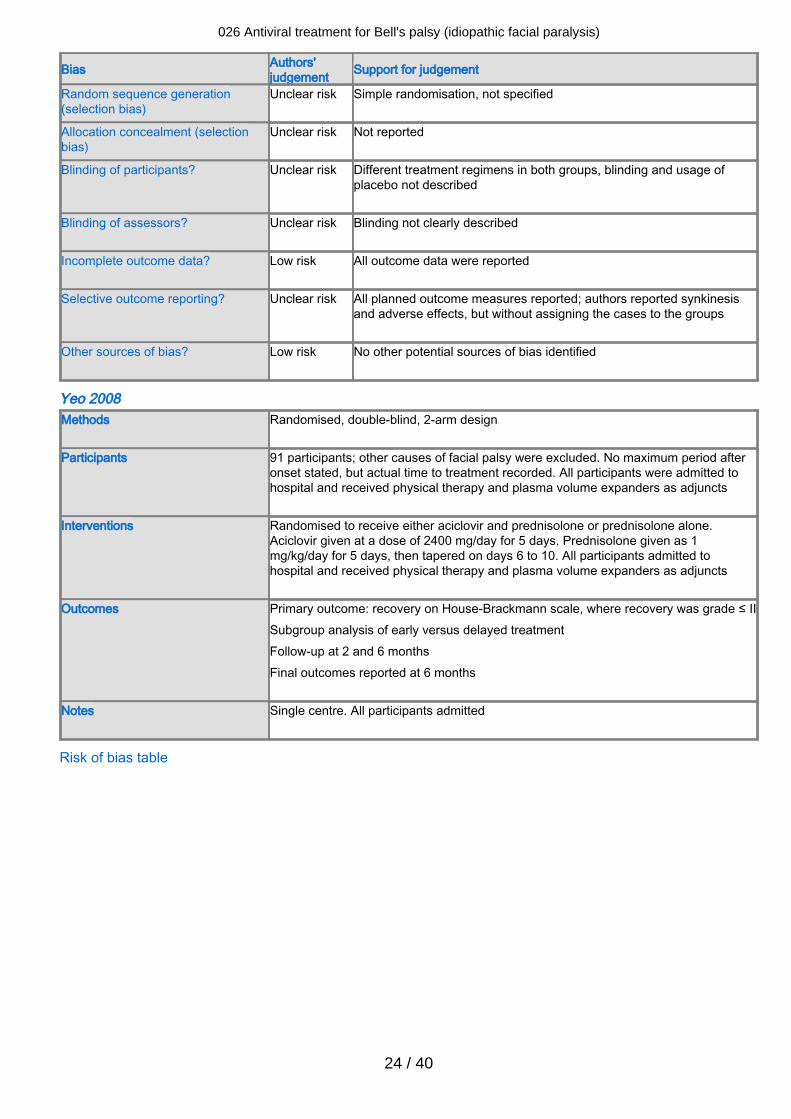
026 Antiviral treatment for Bell's palsy (idiopathic facial paralysis)
24 / 40
Bias Authors'judgement Support for judgement
Random sequence generation(selection bias)
Unclear risk Simple randomisation, not specified
Allocation concealment (selectionbias)
Unclear risk Not reported
Blinding of participants? Unclear risk Different treatment regimens in both groups, blinding and usage ofplacebo not described
Blinding of assessors? Unclear risk Blinding not clearly described
Incomplete outcome data? Low risk All outcome data were reported
Selective outcome reporting? Unclear risk All planned outcome measures reported; authors reported synkinesisand adverse effects, but without assigning the cases to the groups
Other sources of bias? Low risk No other potential sources of bias identified
Yeo 2008Methods Randomised, double-blind, 2-arm design
Participants 91 participants; other causes of facial palsy were excluded. No maximum period after
onset stated, but actual time to treatment recorded. All participants were admitted tohospital and received physical therapy and plasma volume expanders as adjuncts
Interventions Randomised to receive either aciclovir and prednisolone or prednisolone alone.Aciclovir given at a dose of 2400 mg/day for 5 days. Prednisolone given as 1mg/kg/day for 5 days, then tapered on days 6 to 10. All participants admitted tohospital and received physical therapy and plasma volume expanders as adjuncts
Outcomes Primary outcome: recovery on House-Brackmann scale, where recovery was grade ≤ IISubgroup analysis of early versus delayed treatmentFollow-up at 2 and 6 monthsFinal outcomes reported at 6 months
Notes Single centre. All participants admitted
Risk of bias table
026 Antiviral treatment for Bell's palsy (idiopathic facial paralysis)
25 / 40
Bias Authors'judgement Support for judgement
Random sequence generation(selection bias)
Unclear risk States 'randomised' in study title, but no description of this in thearticle
Allocation concealment (selectionbias)
Unclear risk No clear statement of this in the study
Blinding of participants? Unclear risk States 'double-blind' in study title, but no description of methodsemployed for this in text
Blinding of assessors? Unclear risk States 'double-blind' in study title, but no description of methodsemployed for this in text
Incomplete outcome data? Unclear risk Incomplete follow-up data not mentioned in the study
Selective outcome reporting? Unclear risk Stated primary outcome measure reported, no adverse eventsreported
Other sources of bias? Low risk No further potential risks
Footnotes
Characteristics of excluded studies Ahangar 2006Reason for exclusion Allocation was not randomised
Antunes 2000Reason for exclusion Small study numbers and insufficient information in original paper to assign a
participant with incomplete recovery to the correct control group. Author contacted byDr D Allen, but no response received
Axelsson 2003Reason for exclusion Use of a historical control group
Chen 2005Reason for exclusion Follow-up data for only 4 weeks from palsy onset
de Aquino 2001Reason for exclusion Methodology not clear from original paper. An author of a previous version of this
review (D Allen) attempted to obtain further information but obtained no response
Hato 2003Reason for exclusion Retrospective analysis of treatment
Hultcrantz 2005Reason for exclusion Allocation was not randomised
Ibarrondo 1999
026 Antiviral treatment for Bell's palsy (idiopathic facial paralysis)
26 / 40
Reason for exclusion Retrospective study. 100 participants collected between 1983 and 1989 receivedcorticotherapy. 100 participants treated after 1989 received aciclovir
Inanli 2001Reason for exclusion The paper was not available
Minnerop 2008Reason for exclusion Inadequate random allocation to treatment group, no blinding, 30% lost to follow-up,
intervention group and control group of unequal size
Ramos Macias 1992Reason for exclusion Inadequate allocation concealment. No information reported about methods of
randomisation, diagnostic criteria used, length of follow-up, or number of participantslost to follow-up. Thirty-three percent had Ramsay Hunt syndrome, abstract onlyavailable
Roy 2005Reason for exclusion Inadequate information on outcome data, 22% lost to follow-up, abstract only published
in journal supplement and not traced as a full publication
Shahidullah 2011Reason for exclusion Inadequate random allocation to treatment group, no blinding, 36% lost to follow-up
Zhou 1999Reason for exclusion Prospective study. 69 participants with Bell's palsy followed up for only 2 weeks. Not
double blind, and allocation concealment not described. Used own scale for palsygrading, outcome measures not met. Did report adverse events. Four participantsreceiving aciclovir treatment had gastric malaise
Footnotes
Characteristics of studies awaiting classification Footnotes
Characteristics of ongoing studies IRCT201109187575N1
026 Antiviral treatment for Bell's palsy (idiopathic facial paralysis)
27 / 40
Study name Comparison of therapeutic effects of prednisolone, aciclovir, and combination of thesedrugs in Bell's palsy
Methods Randomised, parallel assignment
Participants People with Bell's palsy over 10 years of age, less than 7 days from the onset ofparalysis
Interventions Group 1: prednisone 1 mg/kg body weight daily for 3 days. The treatment was taperedover the next 12 daysGroup 2: aciclovir, 400 mg every 5 hours per day for 10 daysGroup 3: combination of aciclovir and prednisone
Outcomes Primary: House-Brackmann score every 15 daysTreatment failure (no reduction of House-Brackmann score) at the end of month 3
Starting date 22 May 2010
Contact information Dr Alireza Rezaei AshtianiDepartment of Internal Medicine,Valie-Asr Hospital, ArakIslamic Republic of [email protected]
Notes
IRCT2012062210087N1Study name Efficacy of corticosteroid and aciclovir in Bell's palsy
Methods Randomised, parallel group
Participants Children 2 to 18 years old with Bell's palsy less than 3 days after the start of symptoms
Interventions Combination therapy with prednisolone 2 mg/kg of body weight for 7 days and aciclovir
or prednisolone alone 20 mg/kg of body weight for 7 days
Outcomes Severity of Bell's palsy at House-Brackmann score 1 and 2 months after treatment
Starting date Recruitment completed
Contact information Ali KhwajaImam Ali Hospital in ZahedanZahedanSistan and Baluchestandrkhajehneuro@gmail
Notes
Footnotes
Summary of findings tables1 Antivirals plus corticosteroids compared to corticosteroids plus placebo or no treatment for Bell's palsy(idiopathic facial paralysis)
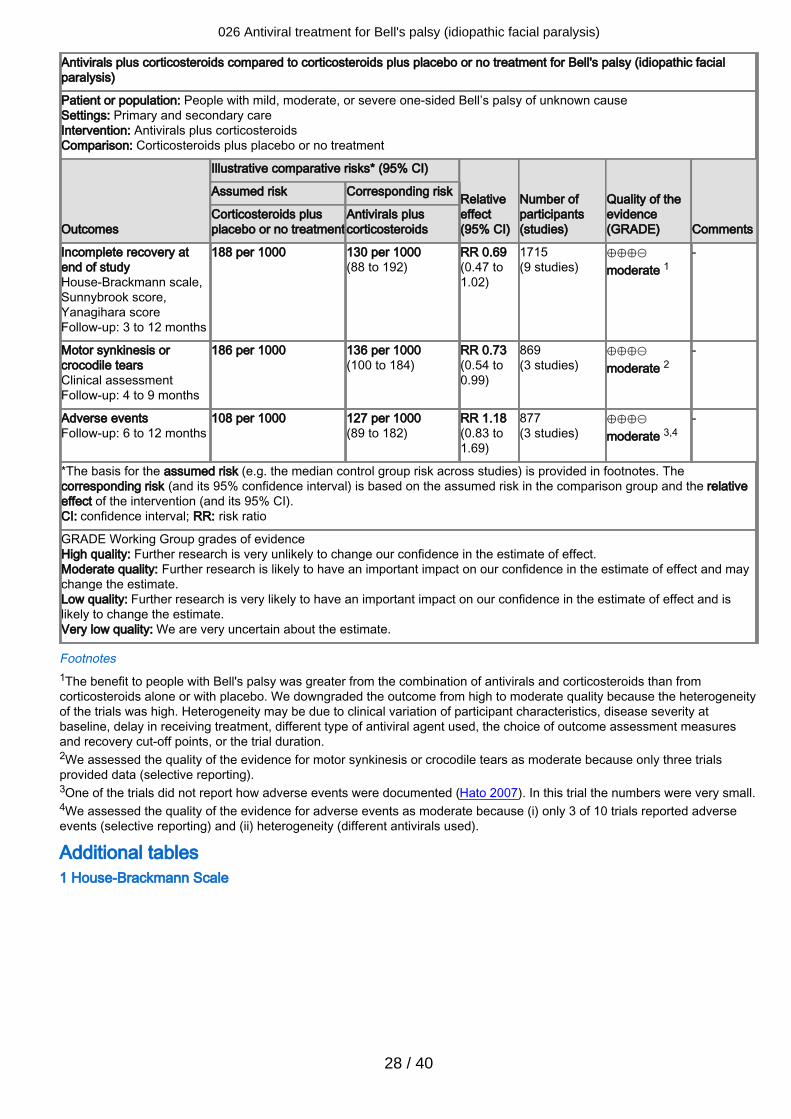
026 Antiviral treatment for Bell's palsy (idiopathic facial paralysis)
28 / 40
Antivirals plus corticosteroids compared to corticosteroids plus placebo or no treatment for Bell's palsy (idiopathic facialparalysis)
Patient or population: People with mild, moderate, or severe one-sided Bell’s palsy of unknown causeSettings: Primary and secondary careIntervention: Antivirals plus corticosteroidsComparison: Corticosteroids plus placebo or no treatment
Outcomes
Illustrative comparative risks* (95% CI)
Relativeeffect(95% CI)
Number ofparticipants(studies)
Quality of theevidence(GRADE) Comments
Assumed risk Corresponding risk
Corticosteroids plusplacebo or no treatment
Antivirals pluscorticosteroids
Incomplete recovery atend of studyHouse-Brackmann scale,Sunnybrook score,Yanagihara scoreFollow-up: 3 to 12 months
188 per 1000 130 per 1000(88 to 192)
RR 0.69 (0.47 to1.02)
1715(9 studies)
⊕⊕⊕⊝moderate 1
-
Motor synkinesis orcrocodile tearsClinical assessmentFollow-up: 4 to 9 months
186 per 1000 136 per 1000(100 to 184)
RR 0.73 (0.54 to0.99)
869(3 studies)
⊕⊕⊕⊝moderate 2
-
Adverse eventsFollow-up: 6 to 12 months
108 per 1000 127 per 1000(89 to 182)
RR 1.18 (0.83 to1.69)
877(3 studies)
⊕⊕⊕⊝moderate 3,4
-
*The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. Thecorresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relativeeffect of the intervention (and its 95% CI).CI: confidence interval; RR: risk ratio
GRADE Working Group grades of evidenceHigh quality: Further research is very unlikely to change our confidence in the estimate of effect.Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and maychange the estimate.Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and islikely to change the estimate.Very low quality: We are very uncertain about the estimate.
Footnotes1The benefit to people with Bell's palsy was greater from the combination of antivirals and corticosteroids than fromcorticosteroids alone or with placebo. We downgraded the outcome from high to moderate quality because the heterogeneityof the trials was high. Heterogeneity may be due to clinical variation of participant characteristics, disease severity atbaseline, delay in receiving treatment, different type of antiviral agent used, the choice of outcome assessment measuresand recovery cut-off points, or the trial duration.2We assessed the quality of the evidence for motor synkinesis or crocodile tears as moderate because only three trialsprovided data (selective reporting).3One of the trials did not report how adverse events were documented (Hato 2007). In this trial the numbers were very small.4We assessed the quality of the evidence for adverse events as moderate because (i) only 3 of 10 trials reported adverseevents (selective reporting) and (ii) heterogeneity (different antivirals used).
Additional tables 1 House-Brackmann Scale
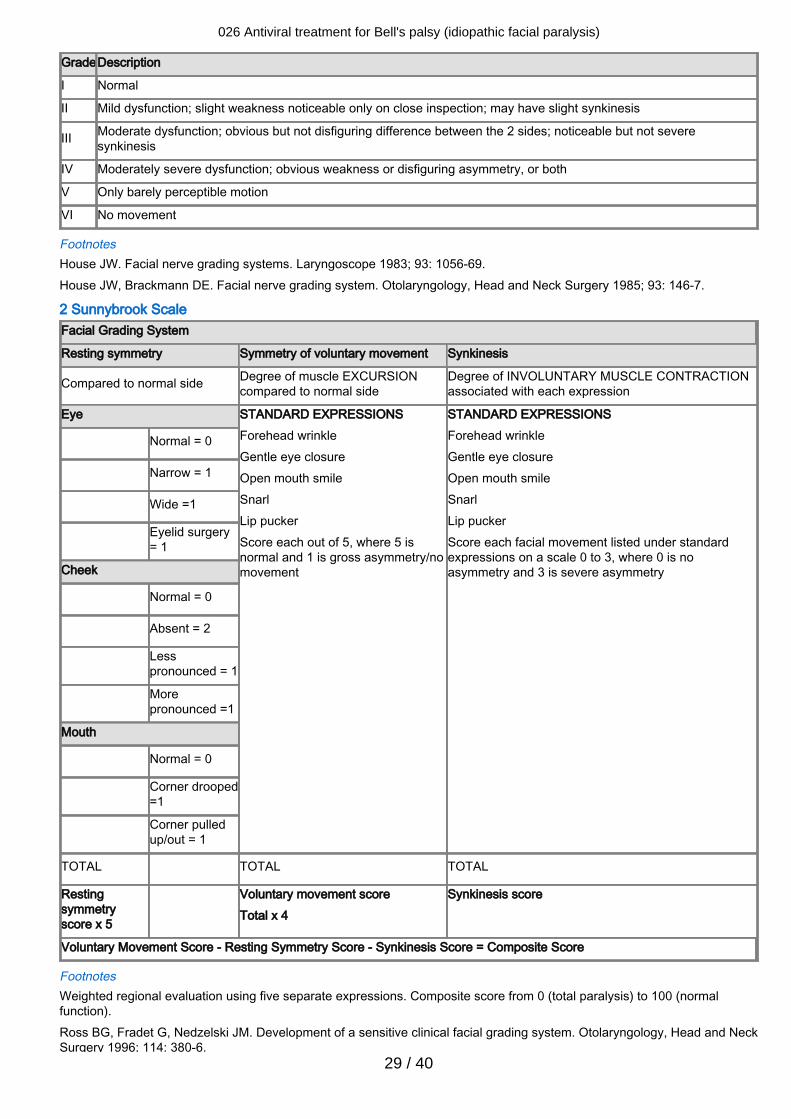
026 Antiviral treatment for Bell's palsy (idiopathic facial paralysis)
29 / 40
GradeDescription
I Normal
II Mild dysfunction; slight weakness noticeable only on close inspection; may have slight synkinesis
III Moderate dysfunction; obvious but not disfiguring difference between the 2 sides; noticeable but not severesynkinesis
IV Moderately severe dysfunction; obvious weakness or disfiguring asymmetry, or both
V Only barely perceptible motion
VI No movement
FootnotesHouse JW. Facial nerve grading systems. Laryngoscope 1983; 93: 1056-69.House JW, Brackmann DE. Facial nerve grading system. Otolaryngology, Head and Neck Surgery 1985; 93: 146-7.
2 Sunnybrook ScaleFacial Grading System
Resting symmetry Symmetry of voluntary movement Synkinesis
Compared to normal side Degree of muscle EXCURSIONcompared to normal side
Degree of INVOLUNTARY MUSCLE CONTRACTIONassociated with each expression
Eye STANDARD EXPRESSIONSForehead wrinkleGentle eye closureOpen mouth smileSnarlLip puckerScore each out of 5, where 5 isnormal and 1 is gross asymmetry/nomovement
STANDARD EXPRESSIONSForehead wrinkleGentle eye closureOpen mouth smileSnarlLip puckerScore each facial movement listed under standardexpressions on a scale 0 to 3, where 0 is noasymmetry and 3 is severe asymmetry
Normal = 0
Narrow = 1
Wide =1
Eyelid surgery= 1
Cheek
Normal = 0
Absent = 2
Lesspronounced = 1
Morepronounced =1
Mouth
Normal = 0
Corner drooped=1
Corner pulledup/out = 1
TOTAL TOTAL TOTAL
Restingsymmetryscore x 5
Voluntary movement scoreTotal x 4
Synkinesis score
Voluntary Movement Score - Resting Symmetry Score - Synkinesis Score = Composite Score
FootnotesWeighted regional evaluation using five separate expressions. Composite score from 0 (total paralysis) to 100 (normalfunction).Ross BG, Fradet G, Nedzelski JM. Development of a sensitive clinical facial grading system. Otolaryngology, Head and NeckSurgery 1996; 114: 380-6.
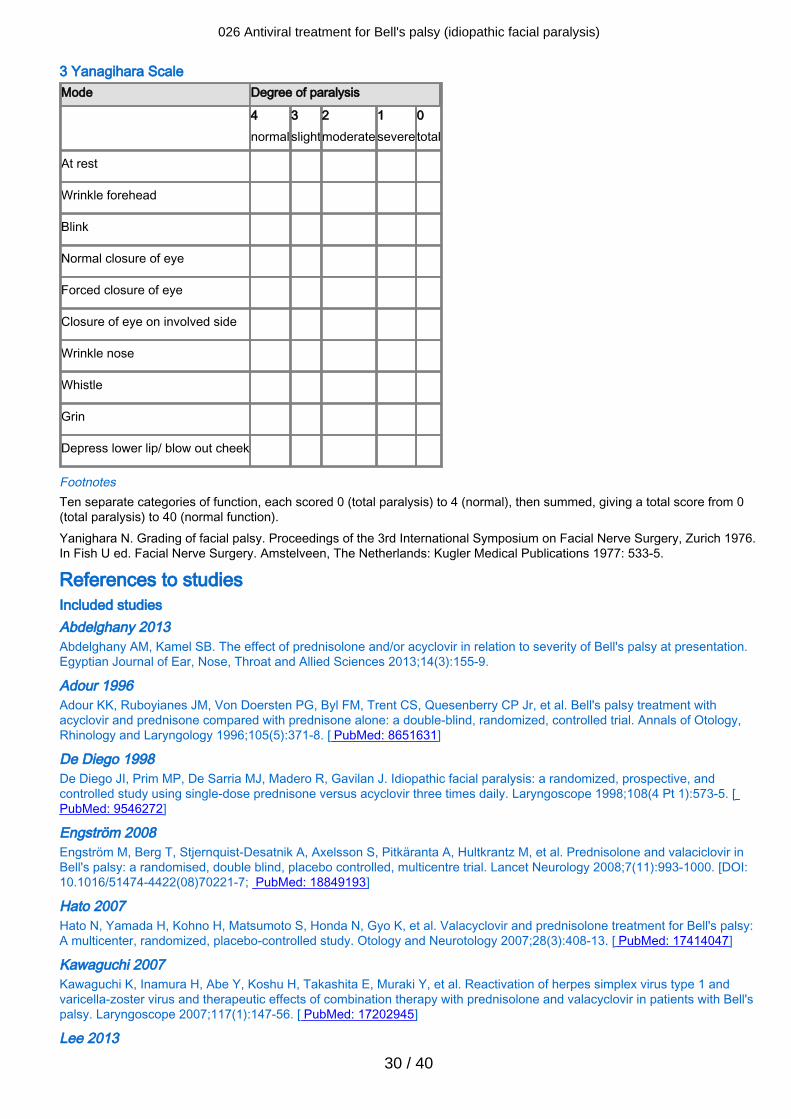
026 Antiviral treatment for Bell's palsy (idiopathic facial paralysis)
30 / 40
3 Yanagihara ScaleMode Degree of paralysis
4normal
3slight
2moderate
1severe
0total
At rest
Wrinkle forehead
Blink
Normal closure of eye
Forced closure of eye
Closure of eye on involved side
Wrinkle nose
Whistle
Grin
Depress lower lip/ blow out cheek
FootnotesTen separate categories of function, each scored 0 (total paralysis) to 4 (normal), then summed, giving a total score from 0(total paralysis) to 40 (normal function).Yanighara N. Grading of facial palsy. Proceedings of the 3rd International Symposium on Facial Nerve Surgery, Zurich 1976.In Fish U ed. Facial Nerve Surgery. Amstelveen, The Netherlands: Kugler Medical Publications 1977: 533-5.
References to studiesIncluded studies Abdelghany 2013Abdelghany AM, Kamel SB. The effect of prednisolone and/or acyclovir in relation to severity of Bell's palsy at presentation.Egyptian Journal of Ear, Nose, Throat and Allied Sciences 2013;14(3):155-9.
Adour 1996Adour KK, Ruboyianes JM, Von Doersten PG, Byl FM, Trent CS, Quesenberry CP Jr, et al. Bell's palsy treatment withacyclovir and prednisone compared with prednisone alone: a double-blind, randomized, controlled trial. Annals of Otology,Rhinology and Laryngology 1996;105(5):371-8. [ PubMed: 8651631]
De Diego 1998De Diego JI, Prim MP, De Sarria MJ, Madero R, Gavilan J. Idiopathic facial paralysis: a randomized, prospective, andcontrolled study using single-dose prednisone versus acyclovir three times daily. Laryngoscope 1998;108(4 Pt 1):573-5. [PubMed: 9546272]
Engström 2008Engström M, Berg T, Stjernquist-Desatnik A, Axelsson S, Pitkäranta A, Hultkrantz M, et al. Prednisolone and valaciclovir inBell's palsy: a randomised, double blind, placebo controlled, multicentre trial. Lancet Neurology 2008;7(11):993-1000. [DOI:10.1016/51474-4422(08)70221-7; PubMed: 18849193]
Hato 2007Hato N, Yamada H, Kohno H, Matsumoto S, Honda N, Gyo K, et al. Valacyclovir and prednisolone treatment for Bell's palsy:A multicenter, randomized, placebo-controlled study. Otology and Neurotology 2007;28(3):408-13. [ PubMed: 17414047]
Kawaguchi 2007Kawaguchi K, Inamura H, Abe Y, Koshu H, Takashita E, Muraki Y, et al. Reactivation of herpes simplex virus type 1 andvaricella-zoster virus and therapeutic effects of combination therapy with prednisolone and valacyclovir in patients with Bell'spalsy. Laryngoscope 2007;117(1):147-56. [ PubMed: 17202945]
Lee 2013
026 Antiviral treatment for Bell's palsy (idiopathic facial paralysis)
31 / 40
Lee HY, Byun JY, Park MS, Yeo SG. Steroid-antiviral treatment improves the recovery rate in patients with severe Bell'spalsy. American Journal of Medicine 2013;126(4):336-41. [ PubMed: 23394867]
Li 1997Li Y, Gao P, Mao X, Cao P. Randomized clinical trial of acyclovir plus prednisone versus prednisone alone in Bell's palsy.Ceylon Journal of Medical Science 1997;40(2):37-41.
Sullivan 2007Published and unpublished data [ISRCTN: 71548196]Sullivan FM, Swan IRC, Donnan PT, Morrison JM, Smith BH, McKinstry B, et al. Early treatment with prednisolone oracyclovir in Bell's palsy. New England Journal of Medicine 2007;357(16):1598-607. [ PubMed: 17942873]
Vázquez 2008[Other: NCT00561106]Vázquez MC, Sánchez N, Calvo J, Perna A. Efficacy of antiviral in treatment of Bell's palsy [Eficacia de los antivirales en laparálisis de Bell]. Revista Medica del Uruguay 2008;24(3):167-74. [Other: LILACS 501670]
Yeo 2008Yeo SG, Lee YC, Park DC, Cha CI. Acyclovir plus steroid versus steroid alone in the treatment of Bell's palsy. AmericanJournal of Otolaryngology - Head and Neck Medicine and Surgery 2008;29(3):163-6. [ PubMed: 18439948]
Excluded studies Ahangar 2006Ahangar AA, Hosseini S, Saghebi R. Comparison of the efficacy of prednisolone versus prednisolone and acyclovir in thetreatment of Bell's palsy. Neurosciences 2006;11(4):256-9.
Antunes 2000Published data only (unpublished sought but not used)Antunes ML, Fukuda Y, Testa JRG. Clinical treatment of Bell's palsy: comparative study among valaciclovir plus deflazacort,deflazacort and placebo [Tratamento clinico da paralisia de Bell: estudo comparativo com o uso de valaciclovir maisdeflazacort versus deflazacort versus placebo]. Acta Associação William House de Otologia 2000;19(2):68-75.
Axelsson 2003Axelsson S, Lindberg S, Stjernquist-Desatnik A. Outcome of treatment with valacyclovir and prednisone in patients with Bell'spalsy. Annals of Otology, Rhinology and Laryngology 2003;112(3):197-201.
Chen 2005Chen WL, Yang ZH, Huang ZQ. Outcome of treatment of 46 patients with Bell's palsy with aciclovir and prednisone.Shanghai Kou Qiang Yi Xue [Shanghai Journal of Stomatology] 2005;14(6):590-2.
de Aquino 2001Published data only (unpublished sought but not used)de Aquino JEAP, Cruz Filho AN. Comparative study of three types of treatment of idiopathic facial palsy (Bell) [Estudocomparativo com tres tipos de tratamento clinico na paralisa facial idiopatica (Bell)]. Acta Associação William House deOtologia 2001;20(4):195-200.
Hato 2003Hato N, Matsumoto S, Kisaki H, Takahashi H, Wakisaka H, Honda N, et al. Efficacy of early treatment of Bell's palsy with oralacyclovir and prednisolone. Otology and Neurotology 2003;24(6):948-51.
Hultcrantz 2005Hultcrantz M. Treatment of facial paralysis - evidence-based recommendations. Lakartidningen 2005;102(10):744-75.
Ibarrondo 1999Ibarrondo J, Navarrete ML, Encarnación LF, Quesada P, Crespo F, García M, et al. Treatment of idiopathic facial paralysis:corticoids versus acyclovir versus empirical treatment [Tratamiento de la paralisis facial idiopatica: corticoides versusaciclovir versus empirico]. Acta Otorrinolaringologica Espanola 1999;50(2):118-20.
Inanli 2001Inanli S, Tutkun A, Ozturk O. Idiopathic facial nerve paralysis treatment with acyclovir and prednisolone alone. TurkishArchives of Otolaryngology 2001;39:19-24.
Minnerop 2008Minnerop M, Herbst M, Fimmers R, Kaabar P, Matz B, Klockgether T, et al. Bell's palsy: combined treatment of famciclovirand prednisone is superior to prednisone alone. Journal of Neurology 2008;255:1726-30.
Ramos Macias 1992
026 Antiviral treatment for Bell's palsy (idiopathic facial paralysis)
32 / 40
Ramos Macías A, De Miguel Martínez I, Martín Sánchez AM, Gómez González JL, Martín Galán A. Incorporation of acyclovirin the treatment of peripheral paralysis. A study of 45 cases [Incorporación del aciclovir en el tratamiento de la parálisisperiférica. Un estudio en 45 casos]. Acta Otorrinolaringológica Espanola 1992;43(2):117-20.
Roy 2005Roy A, Jose J, Kamath V, Matthew T. Efficacy of aciclovir and methylprednisolone versus methylprednisolone alone in thetreatment of Bell's palsy. Journal of the Neurological Sciences 2005;238(Suppl 1):S207.
Shahidullah 2011Shahidullah M, Haque A, Islam MR, Rizvi AN, Sultana N, Mia BA. Comparative study between combination of famciclovirand prednisolone with prednisolone alone in acute Bell's palsy. Mymensingh Medical Journal 2011;20(4):605-13. [CRS:8300125000010514; EMBASE: EMBASE 22081178; Other: CN-00857180]
Zhou 1999Zhou P. Aciclovir in treating Bell's palsy. Chinese Journal of New Drugs and Clinical Remedies 1999;18(1):13-4.
Studies awaiting classification Ongoing studies IRCT201109187575N1IRCT201109187575N1. Comparison of therapeutic effects of prednisolone, acyclovir, and combination of these drugs inBell's palsy. http://www.irct.ir/searchresult.php?id=7575&number=1 (accessed 14.October 2014).
IRCT2012062210087N1IRCT2012062210087N1. Efficacy of corticosteroid and acyclovir in Bell's palsy.http://www.irct.ir/searchresult.php?id=10087&number=1 (accessed 14.October 2014).
Other referencesAdditional references Abiko 2002Abiko Y, Ikeda M, Hondo R. Secretion and dynamics of herpes simplex virus in tears and saliva of patients with Bell's Palsy.Otology and Neurology 2002;23(5):779-83.
Adour 1982Adour KK. Current concepts in neurology: diagnosis and management of facial paralysis. New England Journal of Medicine1982;307(6):348-51.
Axelsson 2012Axelsson S, Berg T, Jonsson L, Engström M, Kanerva M, Stjernquist-Desatnik A. Bell's palsy - the effect of prednisoloneand/or valaciclovir versus placebo in relation to baseline severity in a randomised controlled trial. Clinical Otolaryngology2012;37(4):283-90.
Bateman 1992Bateman DE. Facial palsy. British Journal of Hospital Medicine 1992;47(6):430-1.
Berg 2012Berg T, Bylund N, Marsk E, Jonsson L, Kanerva M, Hultcrantz M, et al. The effect of prednisolone on sequelae in Bell'spalsy. Archives of Otolaryngology - Head & Neck Surgery 2012;138(5):445-9.
BNF 2013British Medical Association and Royal Pharmaceutical Society of Great Britain. British National Formulary. 66th edition.London: British Medical Association and the Royal Pharmaceutical Society of Great Britain, 2013.
Brandenberg 1993Brandenberg NA, Annegers JF. Incidence and risk factors for Bell's Palsy in Laredo, Texas: 1974-1982. Neuroepidemiology1993;12(6):313-25.
Burgess 1984Burgess LP, Yim DW, Lepore ML. Bell's palsy: the steroid controversy revisited. Laryngoscope 2000;94(11 Pt 1):1472-6.
de Almeida 2009de Almeida JR, Al Khabori M, Guyatt GH, Witterick IJ, Lin VY, Nedzelski JM, et al. Combined corticosteroid and antiviraltreatment for Bell palsy: a systematic review and meta-analysis. JAMA 2009;302(9):985-93.
Egger 1997Egger M, Smith GD, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997;315:629-
026 Antiviral treatment for Bell's palsy (idiopathic facial paralysis)
33 / 40
34.
Egger 2007Egger M, Davey Smith G, Altman DG. Systematic Reviews in Health Care: Meta-Analysis in Context. 6th edition. London:BMJ Books, 2007. [ISBN: 978-0-7279-1488-0]
Goudakos 2009Goudakos JK, Markou KD. Corticosteroids versus corticosteroids plus antiviral agents in the treatment of Bell Palsy: asystematic review and meta-analysis. Archives of Otolaryngology - Head & Neck Surgery 2009;135(6):558-64.
GRADEpro 2008GRADEpro [Computer program]. Version 3.2 for Windows. Jan Brozek, Andrew Oxman, Holger Schünemann, 2008.
Hernández 2008Hernández RA, Sullivan F, Donnan P, Swan I, Vale L; BELLS Trial Group. Economic evaluation of early administration ofprednisolone and/or aciclovir for the treatment of Bell's palsy. Family Practice 2009;26(2):137-44.
Higgins 2011Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March2011]. The Cochrane Collaboration, 2011. Available from www.cochrane-handbook.org.
House 1985House JW, Brackmann DE. Facial nerve grading system. Otolarnygology - Head & Neck Surgery 1985;93(2):146-7.
Katusic 1986Katusic SK, Beard CM, Wiederholt WC, Bergstralh EJ, Kurland LT. Incidence, clinical features and prognosis in Bell's Palsy,Rochester, Minnesota, 1968-1982. Annals of Neurology 1986;20(5):622-7.
Lackner 2010Lackner A, Kessler HH, Walch C, Quasthoff S, Raggam RB. Early and reliable detection of herpes simplex virus type 1 andvaricella zoster virus DNAs in oral fluid of patients with idiopathic peripheral facial nerve palsy: Decision support regardingantiviral treatment? Journal of Medical Virology 2010;82(9):1582-5.
Lorber 1996Lorber B. Are all diseases infectious? Annals of Internal Medicine 1996;125(10):844-51.
Martyn 1997Martyn CN, Hughes RA. Epidemiology of peripheral neuropathy. Journal of Neurology, Neurosurgery & Psychiatry1997;62(4):310-8.
May 1976May M, Wette R, Hardin WB Jr, Sullivan J. The use of steroids in Bell's palsy: a prospective controlled study. Laryngoscope1976;86(8):1111-22.
Morales 2013Morales DR, Donnan PT, Daly F, Staa TV, Sullivan FM. Impact of clinical trial findings on Bell's palsy management in generalpractice in the UK 2001-2012: interrupted time series regression analysis. BMJ Open 2013;3(7):1-8.
Murakami 1996Murakami S, Mizobuchi M, Nakashiro Y, Doi T, Hato N, Yanagihara N. Bell palsy and herpes simpex virus: identification ofviral DNA in endoneurial fluid and muscle. Annals of Internal Medicine 1996;124(1 Pt 1):27-30.
Niparko 1993Niparko JK, Mattox DE. Bell's palsy and herpes zoster oticus. In: Johnson RT, Griffin JW, editors(s). Current Therapy inNeurologic Disease. 4th edition. St Louis, Missouri: BC Decker, 1993:355-61. [Other: ISBN: 0801677300]
Numthavaj 2011Numthavaj P, Thakkinstian A, Dejthevaporn C, Attia J. Corticosteroid and antiviral therapy for Bell's palsy: a network meta-analysis. BMC Neurology 2011;11(1). [DOI: 10.1186/1471-2377-11-1]
Peitersen 1982Peitersen E. The natural history of Bell's Palsy. American Journal of Otology 1982;4(2):107-11.
Peitersen 2002Peitersen E. Bell's palsy: the spontaneous course of 2,500 peripheral facial nerve palsies of different etiologies. Acta Oto-Laryngologica 2002;122(Suppl 549):4-30.
Prescott 1988
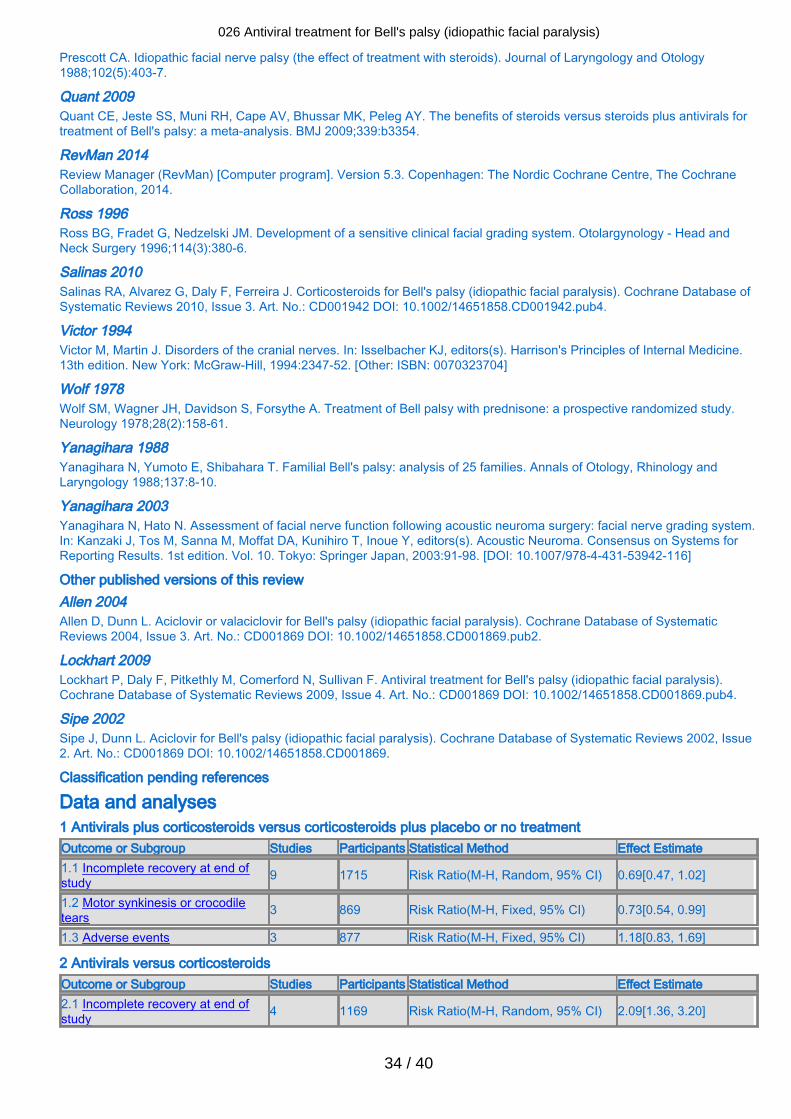
026 Antiviral treatment for Bell's palsy (idiopathic facial paralysis)
34 / 40
Prescott CA. Idiopathic facial nerve palsy (the effect of treatment with steroids). Journal of Laryngology and Otology1988;102(5):403-7.
Quant 2009Quant CE, Jeste SS, Muni RH, Cape AV, Bhussar MK, Peleg AY. The benefits of steroids versus steroids plus antivirals fortreatment of Bell's palsy: a meta-analysis. BMJ 2009;339:b3354.
RevMan 2014Review Manager (RevMan) [Computer program]. Version 5.3. Copenhagen: The Nordic Cochrane Centre, The CochraneCollaboration, 2014.
Ross 1996Ross BG, Fradet G, Nedzelski JM. Development of a sensitive clinical facial grading system. Otolargynology - Head andNeck Surgery 1996;114(3):380-6.
Salinas 2010Salinas RA, Alvarez G, Daly F, Ferreira J. Corticosteroids for Bell's palsy (idiopathic facial paralysis). Cochrane Database ofSystematic Reviews 2010, Issue 3. Art. No.: CD001942 DOI: 10.1002/14651858.CD001942.pub4.
Victor 1994Victor M, Martin J. Disorders of the cranial nerves. In: Isselbacher KJ, editors(s). Harrison's Principles of Internal Medicine.13th edition. New York: McGraw-Hill, 1994:2347-52. [Other: ISBN: 0070323704]
Wolf 1978Wolf SM, Wagner JH, Davidson S, Forsythe A. Treatment of Bell palsy with prednisone: a prospective randomized study.Neurology 1978;28(2):158-61.
Yanagihara 1988Yanagihara N, Yumoto E, Shibahara T. Familial Bell's palsy: analysis of 25 families. Annals of Otology, Rhinology andLaryngology 1988;137:8-10.
Yanagihara 2003Yanagihara N, Hato N. Assessment of facial nerve function following acoustic neuroma surgery: facial nerve grading system.In: Kanzaki J, Tos M, Sanna M, Moffat DA, Kunihiro T, Inoue Y, editors(s). Acoustic Neuroma. Consensus on Systems forReporting Results. 1st edition. Vol. 10. Tokyo: Springer Japan, 2003:91-98. [DOI: 10.1007/978-4-431-53942-116]
Other published versions of this review Allen 2004Allen D, Dunn L. Aciclovir or valaciclovir for Bell's palsy (idiopathic facial paralysis). Cochrane Database of SystematicReviews 2004, Issue 3. Art. No.: CD001869 DOI: 10.1002/14651858.CD001869.pub2.
Lockhart 2009Lockhart P, Daly F, Pitkethly M, Comerford N, Sullivan F. Antiviral treatment for Bell's palsy (idiopathic facial paralysis).Cochrane Database of Systematic Reviews 2009, Issue 4. Art. No.: CD001869 DOI: 10.1002/14651858.CD001869.pub4.
Sipe 2002Sipe J, Dunn L. Aciclovir for Bell's palsy (idiopathic facial paralysis). Cochrane Database of Systematic Reviews 2002, Issue2. Art. No.: CD001869 DOI: 10.1002/14651858.CD001869.
Classification pending references
Data and analyses 1 Antivirals plus corticosteroids versus corticosteroids plus placebo or no treatmentOutcome or Subgroup Studies Participants Statistical Method Effect Estimate1.1 Incomplete recovery at end ofstudy 9 1715 Risk Ratio(M-H, Random, 95% CI) 0.69[0.47, 1.02]
1.2 Motor synkinesis or crocodiletears 3 869 Risk Ratio(M-H, Fixed, 95% CI) 0.73[0.54, 0.99]
1.3 Adverse events 3 877 Risk Ratio(M-H, Fixed, 95% CI) 1.18[0.83, 1.69]
2 Antivirals versus corticosteroidsOutcome or Subgroup Studies Participants Statistical Method Effect Estimate2.1 Incomplete recovery at end ofstudy 4 1169 Risk Ratio(M-H, Random, 95% CI) 2.09[1.36, 3.20]
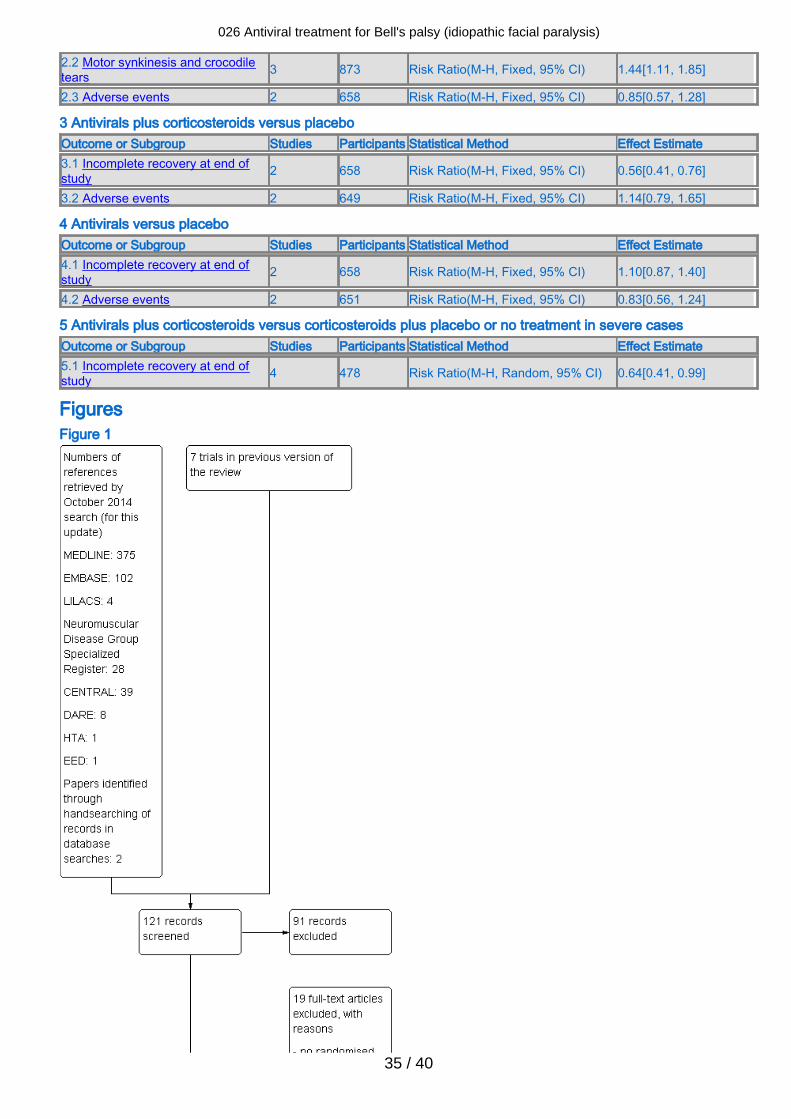
026 Antiviral treatment for Bell's palsy (idiopathic facial paralysis)
35 / 40
2.2 Motor synkinesis and crocodiletears 3 873 Risk Ratio(M-H, Fixed, 95% CI) 1.44[1.11, 1.85]
2.3 Adverse events 2 658 Risk Ratio(M-H, Fixed, 95% CI) 0.85[0.57, 1.28]
3 Antivirals plus corticosteroids versus placeboOutcome or Subgroup Studies Participants Statistical Method Effect Estimate3.1 Incomplete recovery at end ofstudy 2 658 Risk Ratio(M-H, Fixed, 95% CI) 0.56[0.41, 0.76]
3.2 Adverse events 2 649 Risk Ratio(M-H, Fixed, 95% CI) 1.14[0.79, 1.65]
4 Antivirals versus placeboOutcome or Subgroup Studies Participants Statistical Method Effect Estimate4.1 Incomplete recovery at end ofstudy 2 658 Risk Ratio(M-H, Fixed, 95% CI) 1.10[0.87, 1.40]
4.2 Adverse events 2 651 Risk Ratio(M-H, Fixed, 95% CI) 0.83[0.56, 1.24]
5 Antivirals plus corticosteroids versus corticosteroids plus placebo or no treatment in severe casesOutcome or Subgroup Studies Participants Statistical Method Effect Estimate5.1 Incomplete recovery at end ofstudy 4 478 Risk Ratio(M-H, Random, 95% CI) 0.64[0.41, 0.99]
FiguresFigure 1
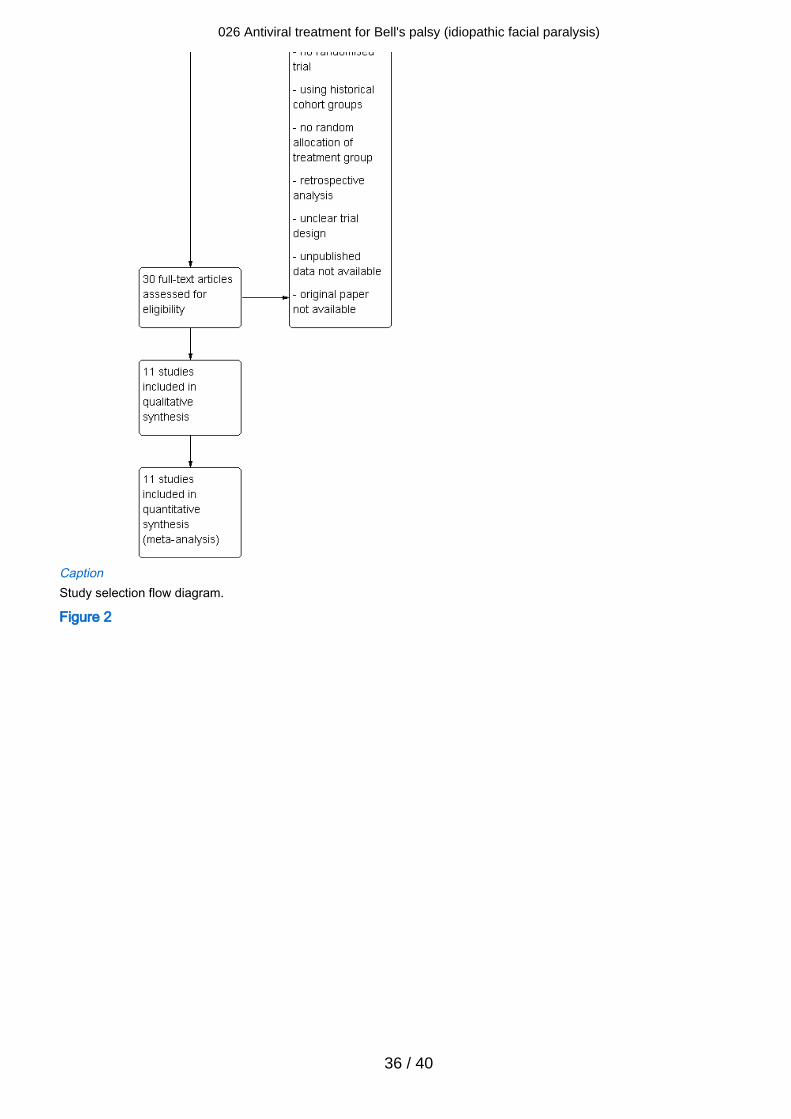
026 Antiviral treatment for Bell's palsy (idiopathic facial paralysis)
36 / 40
CaptionStudy selection flow diagram.
Figure 2
026 Antiviral treatment for Bell's palsy (idiopathic facial paralysis)
37 / 40
CaptionA summary of review authors' 'Risk of bias' assessments for included studies. Red = high risk of bias; yellow = unclear risk ofbias; green = low risk of bias.
Figure 3 (Analysis 1.1)
CaptionForest plot of comparison: 1 Antivirals plus corticosteroids versus corticosteroids plus placebo or no treatment, outcome: 1.1Incomplete recovery at end of study.
Figure 4 (Analysis 2.1)
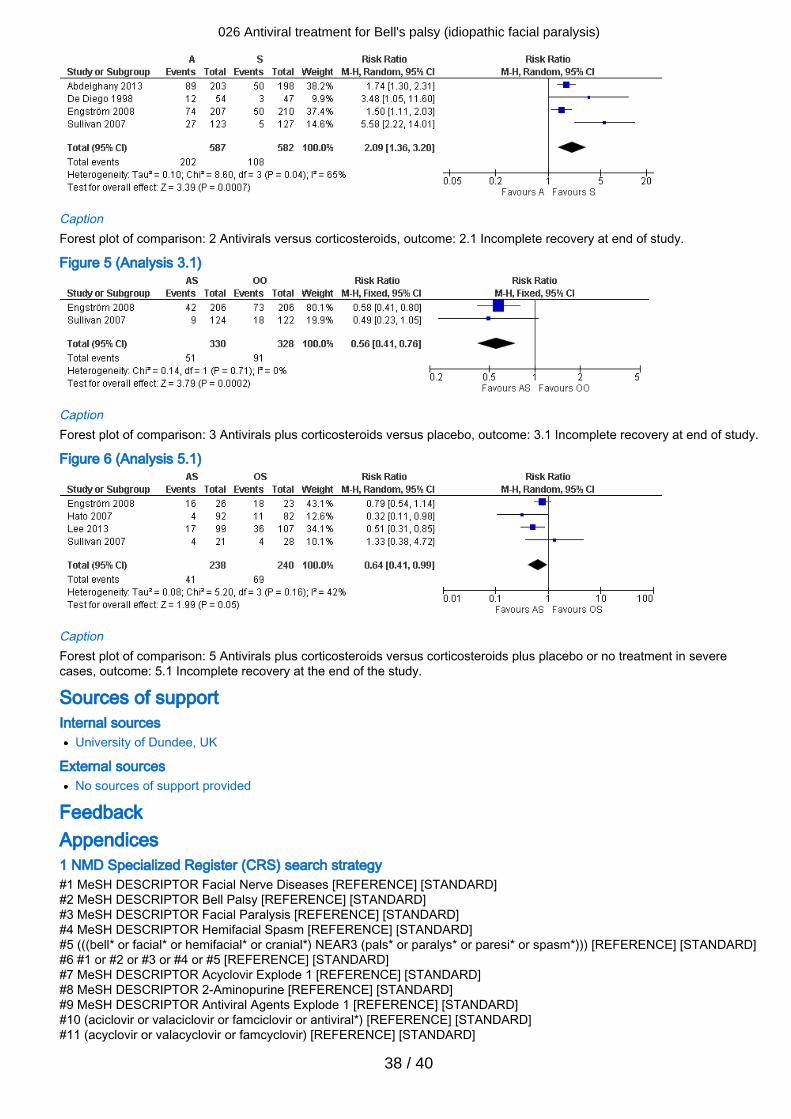
026 Antiviral treatment for Bell's palsy (idiopathic facial paralysis)
38 / 40
CaptionForest plot of comparison: 2 Antivirals versus corticosteroids, outcome: 2.1 Incomplete recovery at end of study.
Figure 5 (Analysis 3.1)
CaptionForest plot of comparison: 3 Antivirals plus corticosteroids versus placebo, outcome: 3.1 Incomplete recovery at end of study.
Figure 6 (Analysis 5.1)
CaptionForest plot of comparison: 5 Antivirals plus corticosteroids versus corticosteroids plus placebo or no treatment in severecases, outcome: 5.1 Incomplete recovery at the end of the study.
Sources of support Internal sources
University of Dundee, UK
External sourcesNo sources of support provided
Feedback Appendices 1 NMD Specialized Register (CRS) search strategy#1 MeSH DESCRIPTOR Facial Nerve Diseases [REFERENCE] [STANDARD]#2 MeSH DESCRIPTOR Bell Palsy [REFERENCE] [STANDARD]#3 MeSH DESCRIPTOR Facial Paralysis [REFERENCE] [STANDARD]#4 MeSH DESCRIPTOR Hemifacial Spasm [REFERENCE] [STANDARD]#5 (((bell* or facial* or hemifacial* or cranial*) NEAR3 (pals* or paralys* or paresi* or spasm*))) [REFERENCE] [STANDARD]#6 #1 or #2 or #3 or #4 or #5 [REFERENCE] [STANDARD]#7 MeSH DESCRIPTOR Acyclovir Explode 1 [REFERENCE] [STANDARD]#8 MeSH DESCRIPTOR 2-Aminopurine [REFERENCE] [STANDARD]#9 MeSH DESCRIPTOR Antiviral Agents Explode 1 [REFERENCE] [STANDARD]#10 (aciclovir or valaciclovir or famciclovir or antiviral*) [REFERENCE] [STANDARD]#11 (acyclovir or valacyclovir or famcyclovir) [REFERENCE] [STANDARD]
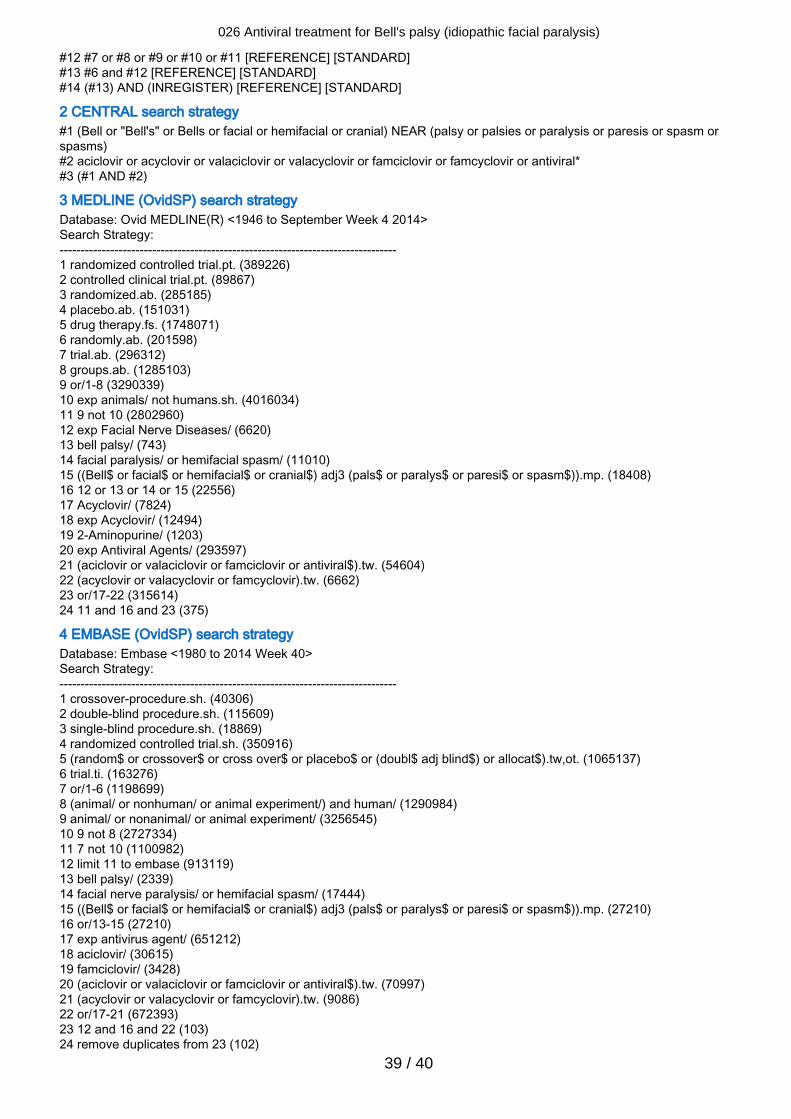
026 Antiviral treatment for Bell's palsy (idiopathic facial paralysis)
39 / 40
#12 #7 or #8 or #9 or #10 or #11 [REFERENCE] [STANDARD]#13 #6 and #12 [REFERENCE] [STANDARD]#14 (#13) AND (INREGISTER) [REFERENCE] [STANDARD]
2 CENTRAL search strategy#1 (Bell or "Bell's" or Bells or facial or hemifacial or cranial) NEAR (palsy or palsies or paralysis or paresis or spasm orspasms)#2 aciclovir or acyclovir or valaciclovir or valacyclovir or famciclovir or famcyclovir or antiviral*#3 (#1 AND #2)
3 MEDLINE (OvidSP) search strategyDatabase: Ovid MEDLINE(R) <1946 to September Week 4 2014>Search Strategy:--------------------------------------------------------------------------------1 randomized controlled trial.pt. (389226)2 controlled clinical trial.pt. (89867)3 randomized.ab. (285185)4 placebo.ab. (151031)5 drug therapy.fs. (1748071)6 randomly.ab. (201598)7 trial.ab. (296312)8 groups.ab. (1285103)9 or/1-8 (3290339)10 exp animals/ not humans.sh. (4016034)11 9 not 10 (2802960)12 exp Facial Nerve Diseases/ (6620)13 bell palsy/ (743)14 facial paralysis/ or hemifacial spasm/ (11010)15 ((Bell$ or facial$ or hemifacial$ or cranial$) adj3 (pals$ or paralys$ or paresi$ or spasm$)).mp. (18408)16 12 or 13 or 14 or 15 (22556)17 Acyclovir/ (7824)18 exp Acyclovir/ (12494)19 2-Aminopurine/ (1203)20 exp Antiviral Agents/ (293597)21 (aciclovir or valaciclovir or famciclovir or antiviral$).tw. (54604)22 (acyclovir or valacyclovir or famcyclovir).tw. (6662)23 or/17-22 (315614)24 11 and 16 and 23 (375)
4 EMBASE (OvidSP) search strategyDatabase: Embase <1980 to 2014 Week 40>Search Strategy:--------------------------------------------------------------------------------1 crossover-procedure.sh. (40306)2 double-blind procedure.sh. (115609)3 single-blind procedure.sh. (18869)4 randomized controlled trial.sh. (350916)5 (random$ or crossover$ or cross over$ or placebo$ or (doubl$ adj blind$) or allocat$).tw,ot. (1065137)6 trial.ti. (163276)7 or/1-6 (1198699)8 (animal/ or nonhuman/ or animal experiment/) and human/ (1290984)9 animal/ or nonanimal/ or animal experiment/ (3256545)10 9 not 8 (2727334)11 7 not 10 (1100982)12 limit 11 to embase (913119)13 bell palsy/ (2339)14 facial nerve paralysis/ or hemifacial spasm/ (17444)15 ((Bell$ or facial$ or hemifacial$ or cranial$) adj3 (pals$ or paralys$ or paresi$ or spasm$)).mp. (27210)16 or/13-15 (27210)17 exp antivirus agent/ (651212)18 aciclovir/ (30615)19 famciclovir/ (3428)20 (aciclovir or valaciclovir or famciclovir or antiviral$).tw. (70997)21 (acyclovir or valacyclovir or famcyclovir).tw. (9086)22 or/17-21 (672393)23 12 and 16 and 22 (103)24 remove duplicates from 23 (102)
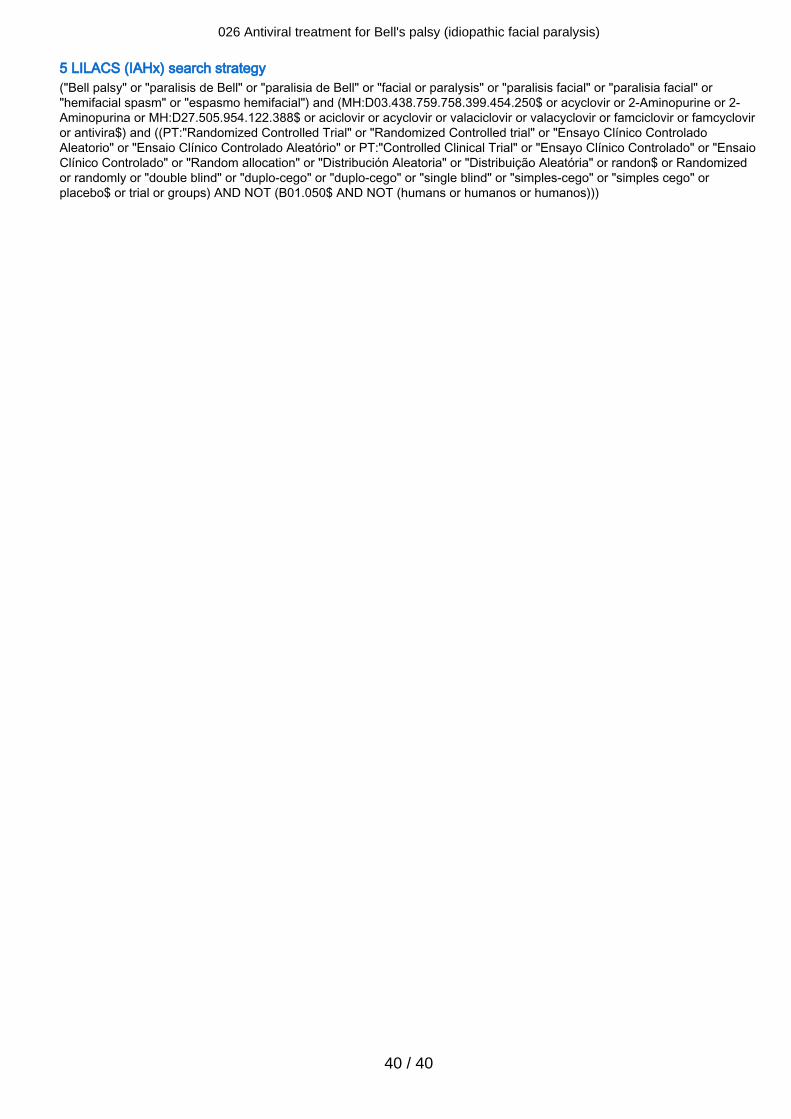
026 Antiviral treatment for Bell's palsy (idiopathic facial paralysis)
40 / 40
5 LILACS (IAHx) search strategy("Bell palsy" or "paralisis de Bell" or "paralisia de Bell" or "facial or paralysis" or "paralisis facial" or "paralisia facial" or"hemifacial spasm" or "espasmo hemifacial") and (MH:D03.438.759.758.399.454.250$ or acyclovir or 2-Aminopurine or 2-Aminopurina or MH:D27.505.954.122.388$ or aciclovir or acyclovir or valaciclovir or valacyclovir or famciclovir or famcycloviror antivira$) and ((PT:"Randomized Controlled Trial" or "Randomized Controlled trial" or "Ensayo Clínico ControladoAleatorio" or "Ensaio Clínico Controlado Aleatório" or PT:"Controlled Clinical Trial" or "Ensayo Clínico Controlado" or "EnsaioClínico Controlado" or "Random allocation" or "Distribución Aleatoria" or "Distribuição Aleatória" or randon$ or Randomizedor randomly or "double blind" or "duplo-cego" or "duplo-cego" or "single blind" or "simples-cego" or "simples cego" orplacebo$ or trial or groups) AND NOT (B01.050$ AND NOT (humans or humanos or humanos)))





























