Embed Size (px)
Citation preview

Original Article With Video Illustration
L
fuB
pL
Arthroscopic Treatment of Mild to Moderate Deformity AfterSlipped Capital Femoral Epiphysis: Intra-Operative Findings
and Functional OutcomesJames D. Wylie, M.D., James T. Beckmann, M.D., M.S., Travis G. Maak, M.D., and
Stephen K. Aoki, M.D.
Purpose: To identify intra-articular pathology during arthroscopic osteochondroplasty for slipped capital femoralepiphysis (SCFE)erelated femoroacetabular impingement and determine functional outcomes after treatment.Methods: Nine hips in 9 patients (6 male and 3 female patients; mean age, 17.5 years; age range, 13.5 to 26.9 years)underwent hip arthroscopy for femoroacetabular impingement after in situ pinning of the SCFE. Medical records, ra-diographs, and intraoperative images were reviewed to determine the severity of disease and damage to the hip joints. Forall patients, we obtained the modified Harris Hip Score and Hip Outcome Score (HOS) preoperatively and at a minimum of12 months postoperatively, as well as a Likert scale of perceived change in physical activity. Results: All 9 treated patientshad some degree of labral or acetabular cartilage injury at the time of arthroscopy, which was a mean of 58.6 months(range, 18 to 169 months) after in situ pinning. The alpha angle improved from 75� preoperatively to 46� postoperatively(P < .001). The mean follow-up period was 28.6 months (range, 12.6 to 55.6 months). The mean modified Harris HipScore improved from 63.6 preoperatively to 91.4 postoperatively (P ¼ .005). Similarly, the mean HOS activitieseofedailyliving scale improved from 70.2 to 93.3 (P ¼ .010), and the HOS sports scale improved from 53.4 to 88.9 (P ¼ .004). Mostpatients reported significant improvement on a physical-activity Likert scale, with 4 reporting much improved, 3 reportingimproved, and 1 reporting slightly improved physical activity. One patient reported an unchanged activity level. No pa-tients reported a worse activity level after surgery. Conclusions: Post-SCFE cartilage and/or labral damage develops inpatients with symptomatic mild to moderate SCFE deformity, and arthroscopic treatment improved functional outcomesin a small cohort of patients at short-term follow-up. Level of Evidence: Level IV, therapeutic case series.
lipped capital femoral epiphysis (SCFE) is a devas-
Stating hip problem in the adolescent populationthat can lead to femoral neck deformity, chondrolysis,and avascular necrosis of the femoral head. SCFE willdevelop in approximately 11 in 100,000 children.1 Theprevalence is hypothesized to be increasing because ofthe increased rates of obesityd80% of SCFEs occur inpatients with a body mass index greater than the 95thpercentile.2 Also contributing to this pathology is anFrom the Department of Orthopaedic Surgery, University of Utah, Saltake City, Utah, U.S.A.The authors report the following potential conflict of interest or source ofnding: S.K.A. receives support from ArthroCare, Pivot Medical, Arthrex,iomet, Musculoskeletal Transplant Foundation.Received February 5, 2014; accepted August 15, 2014.Address correspondence to Stephen K. Aoki, M.D., Department of Ortho-
aedic Surgery, University of Utah Orthopedic Center, 590 Wakara Way, Saltake City, UT, U.S.A. E-mail: [email protected]� 2014 by the Arthroscopy Association of North America0749-8063/1492/$36.00http://dx.doi.org/10.1016/j.arthro.2014.08.019
Arthroscopy: The Journal of Arthroscopic and Related
earlier maturation of the population.3 Lower extremityfunction is commonly compromised after in situ fixa-tion with the potential need for early hip replacement.4
In long-term studies, all degrees of SCFE led to somefunctional loss, with worse results in the setting ofcomplications and attempted realignment.5
The most common treatment for SCFE is in situpinning of the slipped epiphysis that, by definition, re-sults in an apex anterosuperior deformity of the femoralhead-neck junction.3 Despite the fact that the meta-physis then undergoes some remodeling over time,functional loss results from residual deformity thatimpinges with the acetabular rim in flexion and inter-nal rotation.6 Similar to other causes of femo-roacetabular impingement (FAI), the repetitive traumafrom impingement leads to labral tears and injury to thearticular cartilage.7 However, the anatomic angle ofthe physis is distinctly different between the post-SCFEdeformity and cam-type FAI, suggesting differing cau-ses of these 2 conditions.8 Three groups have reportedthat most patients undergoing open surgery for SCFE
Surgery, Vol -, No - (Month), 2014: pp 1-7 1

2 J. D. WYLIE ET AL.
had acetabular labral and/or cartilage injury at the timeof surgery.9-11 A preliminary report of arthroscopicosteochondroplasty at the time of in situ pinning showedchondrolabral injury and that the 3 patients had a pain-free return to full activities after this technique.12
The purpose of the study was to identify intra-articularpathology during arthroscopic osteochondroplasty forSCFE-related FAI and determine functional outcomesafter treatment. We hypothesized that patients with apost-SCFE deformity would present with acetabulararticular cartilage and labral pathology at the time ofarthroscopy. We also hypothesized that patients whounderwent arthroscopy with osteochondroplasty forproximal femoral deformity after in situ pinning forSCFE would have significantly decreased pain withincreased hip function and improved physical activitycompared with preoperatively.
Methods
Study DesignPatients selected retrospectively for inclusion in this
series included both adult and pediatric patients from 2separate registries that are both approved by the insti-tutional review board at our institution. As part of theseregistries, all patients fill out a worksheet including themodified Harris Hip Score (mHHS) and Hip OutcomeScore (HOS) during their initial patient evaluation. Pa-tients who underwent surgical intervention were askedto complete the mHHS, the HOS, and a Likert scale ofactivity level at all postoperative visits. Postoperativevisits include visits at 1 month, 3 months, 6 months, and1 year, as well as yearly thereafter. If patients do notreturn for their yearly visits, then outcomes question-naires are mailed to them. All patients in this studyunderwent hip arthroscopy by the principal investigator(S.K.A.) between 2008 and 2013. The principal investi-gator has performed hip arthroscopy in 1,100 patients. Aquery of his database for a primary diagnosis for SCFEidentified 30 cases, and there were 9 cases in whicharthroscopy had been performed more than 1 yearearlier. The inclusion criteria included a primary diag-nosis of post-SCFE deformity and surgery greater than1 year ago. The exclusion criteria were the lack ofoutcome scores at a minimum of 12 months of follow-up and surgery performed within the past 12 months.Follow-up was obtained for all 9 patients. The meanfollow-up period was 28.6 months (minimum, 12.6months; maximum, 55.6 months). There were no casesof treatment of the original slip by the principal inves-tigator; all patients were referred for treatment of ahealed post-SCFE deformity.
Patient EvaluationAll patients presented with symptoms consistent
with hip pathology. They described groin or anterior
thigh pain that was worse with activity or had painthat limited activity. On examination, patients hadreproducible pain with deep flexion; in some casesthey had obligate external rotation with flexion.Flexioneadductioneinternal rotation impingementtesting provoked groin pain. Radiographic imagingshowed healed SCFE deformities with lack of femoralhead-neck offset. In all patients conservative man-agement including anti-inflammatories and activitymodification had failed.The patient’s sex, age, surgical history, and intra-
operative findings were obtained from the medicalrecords. Operative reports were reviewed, and intra-articular pathology was recorded and classified aspreviously described by Beck et al.13 In brief, theacetabular cartilage was defined as follows: normal,malacia, debonding, cleavage, or defect. The acetabularlabrum was defined as follows: normal, degeneration,full-thickness tear, detachment, or ossification. The dateof in situ pinning was recorded from the medical records,and the time from in situ pinning to hip arthroscopywas determined. Patients also underwent preoperativeradiographic analysis with anteroposterior, frog-leg lateral,and false-profile views of the hip. Anteroposterior andfalse-profile views were completed weight bearing. Theradiographic parameters measured were the preop-erative alpha angle on the frog-leg lateral film toquantify proximal femoral deformity and the originalslip angle on the lateral film to define the severity ofthe original SCFE. Alpha angles were also measuredpostoperatively. The radiographs were reviewed andquantified by the authors of the study (J.D.W., J.T.B.,S.K.A.). As mentioned previously, patient-reportedoutcomes including the mHHS and HOS arecollected preoperatively and at 3, 6, and 12 monthspostoperatively and at any visit thereafter. The mHHSis a subjective hip-specific quality-of-life measure thatis commonly used in assessing hip outcomes.14-16 Onthis scale, higher scores represent better hip qualityof life. The HOS is another commonly used hip-specific quality-of-life measure; it has 2 subscales,the activitieseofedaily living scale and the sportsscale. Scoring for the HOS has been previouslydescribed with higher values corresponding to betterhip quality of life.17 All patients also filled out a7-level Likert scale of physical activity with potentialanswers being much worse, worse, slightly worse,unchanged, slightly improved, improved, and muchimproved.
Surgical Technique and RehabilitationThe patient is placed supine on the traction table
(Smith & Nephew, Memphis, TN). The patient is pre-pared and draped in normal fashion, and access to thehip is obtained as previously described.18 C-arm fluo-roscopy is positioned on the opposite side of the table.
HIP ARTHROSCOPY FOR POST-SCFE DEFORMITY 3
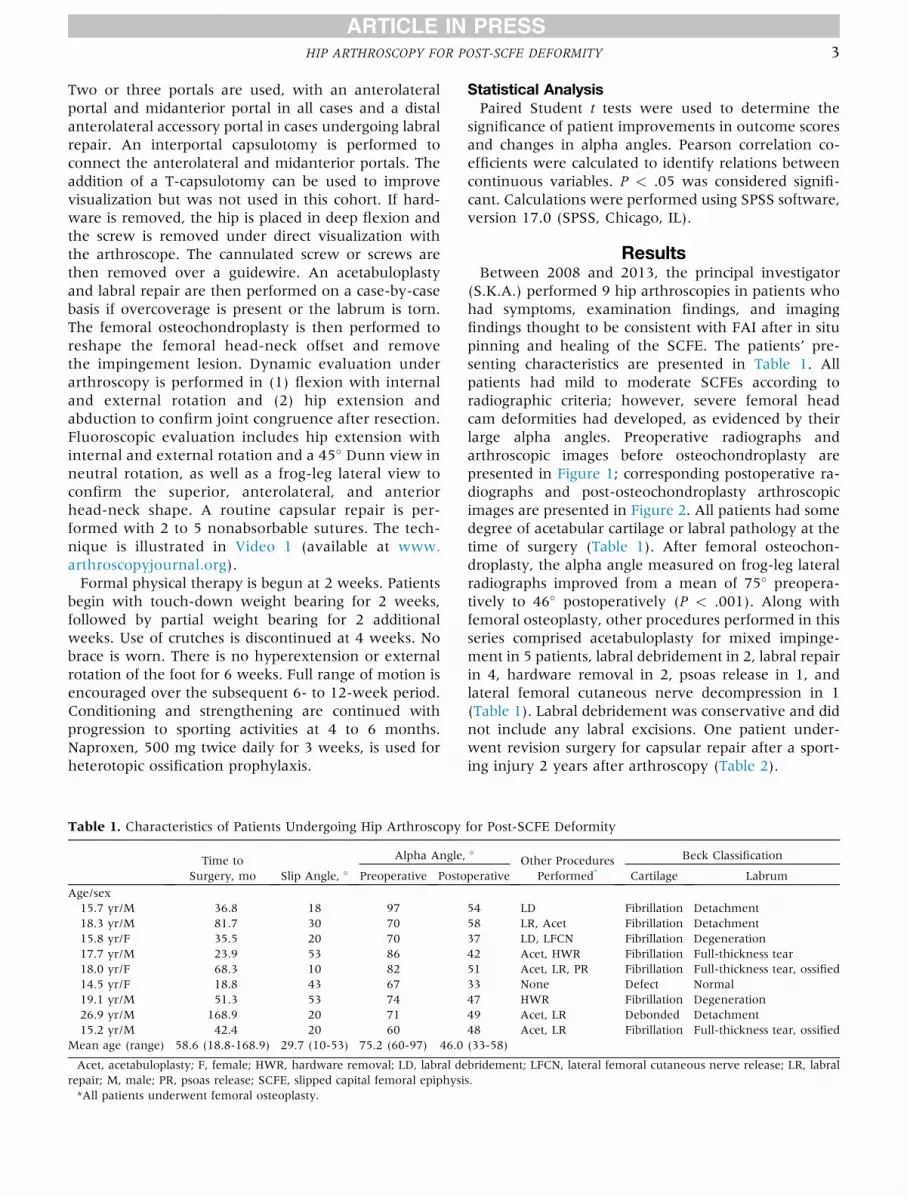
Two or three portals are used, with an anterolateralportal and midanterior portal in all cases and a distalanterolateral accessory portal in cases undergoing labralrepair. An interportal capsulotomy is performed toconnect the anterolateral and midanterior portals. Theaddition of a T-capsulotomy can be used to improvevisualization but was not used in this cohort. If hard-ware is removed, the hip is placed in deep flexion andthe screw is removed under direct visualization withthe arthroscope. The cannulated screw or screws arethen removed over a guidewire. An acetabuloplastyand labral repair are then performed on a case-by-casebasis if overcoverage is present or the labrum is torn.The femoral osteochondroplasty is then performed toreshape the femoral head-neck offset and removethe impingement lesion. Dynamic evaluation underarthroscopy is performed in (1) flexion with internaland external rotation and (2) hip extension andabduction to confirm joint congruence after resection.Fluoroscopic evaluation includes hip extension withinternal and external rotation and a 45� Dunn view inneutral rotation, as well as a frog-leg lateral view toconfirm the superior, anterolateral, and anteriorhead-neck shape. A routine capsular repair is per-formed with 2 to 5 nonabsorbable sutures. The tech-nique is illustrated in Video 1 (available at www.arthroscopyjournal.org).Formal physical therapy is begun at 2 weeks. Patients
begin with touch-down weight bearing for 2 weeks,followed by partial weight bearing for 2 additionalweeks. Use of crutches is discontinued at 4 weeks. Nobrace is worn. There is no hyperextension or externalrotation of the foot for 6 weeks. Full range of motion isencouraged over the subsequent 6- to 12-week period.Conditioning and strengthening are continued withprogression to sporting activities at 4 to 6 months.Naproxen, 500 mg twice daily for 3 weeks, is used forheterotopic ossification prophylaxis.
Table 1. Characteristics of Patients Undergoing Hip Arthroscopy
Time toSurgery, mo Slip Angle, �
Alpha Angle,
Preoperative Posto
Age/sex15.7 yr/M 36.8 18 9718.3 yr/M 81.7 30 7015.8 yr/F 35.5 20 7017.7 yr/M 23.9 53 8618.0 yr/F 68.3 10 8214.5 yr/F 18.8 43 6719.1 yr/M 51.3 53 7426.9 yr/M 168.9 20 7115.2 yr/M 42.4 20 60
Mean age (range) 58.6 (18.8-168.9) 29.7 (10-53) 75.2 (60-97) 46.0
Acet, acetabuloplasty; F, female; HWR, hardware removal; LD, labral derepair; M, male; PR, psoas release; SCFE, slipped capital femoral epiphysi*All patients underwent femoral osteoplasty.
Statistical AnalysisPaired Student t tests were used to determine the
significance of patient improvements in outcome scoresand changes in alpha angles. Pearson correlation co-efficients were calculated to identify relations betweencontinuous variables. P < .05 was considered signifi-cant. Calculations were performed using SPSS software,version 17.0 (SPSS, Chicago, IL).
ResultsBetween 2008 and 2013, the principal investigator
(S.K.A.) performed 9 hip arthroscopies in patients whohad symptoms, examination findings, and imagingfindings thought to be consistent with FAI after in situpinning and healing of the SCFE. The patients’ pre-senting characteristics are presented in Table 1. Allpatients had mild to moderate SCFEs according toradiographic criteria; however, severe femoral headcam deformities had developed, as evidenced by theirlarge alpha angles. Preoperative radiographs andarthroscopic images before osteochondroplasty arepresented in Figure 1; corresponding postoperative ra-diographs and post-osteochondroplasty arthroscopicimages are presented in Figure 2. All patients had somedegree of acetabular cartilage or labral pathology at thetime of surgery (Table 1). After femoral osteochon-droplasty, the alpha angle measured on frog-leg lateralradiographs improved from a mean of 75� preopera-tively to 46� postoperatively (P < .001). Along withfemoral osteoplasty, other procedures performed in thisseries comprised acetabuloplasty for mixed impinge-ment in 5 patients, labral debridement in 2, labral repairin 4, hardware removal in 2, psoas release in 1, andlateral femoral cutaneous nerve decompression in 1(Table 1). Labral debridement was conservative and didnot include any labral excisions. One patient under-went revision surgery for capsular repair after a sport-ing injury 2 years after arthroscopy (Table 2).
for Post-SCFE Deformity
�Other Procedures
Performed*Beck Classification
perative Cartilage Labrum
54 LD Fibrillation Detachment58 LR, Acet Fibrillation Detachment37 LD, LFCN Fibrillation Degeneration42 Acet, HWR Fibrillation Full-thickness tear51 Acet, LR, PR Fibrillation Full-thickness tear, ossified33 None Defect Normal47 HWR Fibrillation Degeneration49 Acet, LR Debonded Detachment48 Acet, LR Fibrillation Full-thickness tear, ossified(33-58)
bridement; LFCN, lateral femoral cutaneous nerve release; LR, labrals.

Fig 1. (A) Preoperativeanteroposterior pelvis radio-graph in a 17-year-oldpatient showing retainedhardware and proximalfemoral deformity. (B) Cor-responding preoperativefrog-leg lateral radiograph.(C) Arthroscopic image ofcam deformity (c) inter-facing with labrum (L).
4 J. D. WYLIE ET AL.
All 9 patients had a minimum of 12 months’ follow-up. Their individual outcomes are reported in Table 2.Among these patients, the mean follow-up period was28.6 months (range, 12.6 to 55.6 months). The mHHSimproved from a mean of 63.6 preoperatively to 91.4at latest follow-up (P ¼ .005). Similarly, the HOSactivitieseofedaily living scale improved from 70.2 to93.3 at latest follow-up (P ¼ .010), and the HOS sportsscale improved from 53.4 to 88.9 at latest follow-up(P ¼ .004) (Fig 3). Regarding physical activity, 8 ofthe 9 patients reported improvement. The ninth patientreported that the activity level was unchanged. Nopatients reported worsening of the activity level afterarthroscopy (Table 2). There were 4 complications inthese 9 patients: 1 patient needed revision surgery forcapsular laxity, 1 patient had transient perinealnumbness, 1 patient had transient lateral femoralcutaneous nerve numbness, and heterotopic ossifica-tion developed in 1 patient (Table 2).
DiscussionSCFE treated with in situ pinning, by definition, fixes
the femoral neck in a position of deformity even aftermild slips. The residual SCFE deformity can cause hippain, functional impairment, and progression to joint
degeneration due to impingement of the anterosuperiordeformity with the acetabulum. Accordingly, all patientsin this study had some degree of acetabular cartilage orlabral pathology at the time of surgery. Arthroscopicosteochondroplasty normalized alpha angles and signifi-cantly improved outcome scores on average in this series.Acetabular cartilage and labral injury after SCFE have
been widely reported both at initial presentation andduring deformity correction. Leunig et al.11,12 describeduniversal hip pathology at the time of fixation of theSCFE, through both open surgery and arthroscopy.Similarly, Ziebarth et al.10 found a high incidence ofacetabular cartilage and labral lesions visualized onsurgical dislocation at the time of index surgery thatwere not correlated with slip severity. In this case series,the slip angle also was not correlated with acetabularand labral injury severity. Joint damage at the time ofpresentation could be explained by an average 8-weekdelay in diagnosis reported in a review of 196 patientsby Kocher et al.19 Most patients with unstable SCFEs(88%) have antecedent pain lasting on average 42 daysbefore presentation.20 These delays suggest that jointdamage from impingement may be ongoing before theSCFE diagnosis and treatment and presumably con-tinues as long as deformity persists.
Fig 2. (A) Postoperativeanteroposterior pelvis radio-graph in same patient as inFigure 1 showing hardwareremoval and osteochon-droplasty. (B) Correspondingpostoperative frog-leg lateral(LAT) radiograph. (C)Arthroscopic image showingosteochondroplasty of camdeformity (c).

Tab
le2.
Outcomes
ofPatients
Undergo
ingHip
ArthroscopyforPost-SCFEDeform
ity
Follow-up,mo
mHHS
HOS-A
DL
HOS-Sports
LikertActivityLev
elComplications
Preoperative
Postoperative
Preoperative
Postoperative
Preoperative
Postoperative
Age
/sex
15.7
yr/M
55.6
52.8
100
70.6
100
27.8
97.2
Much
improve
dNone
18.3
yr/M
50.3
33.0
100
69.1
100
58.3
94.4
Much
improve
dPerinea
lnumbn
ess,resolved
by6-w
kfollow-up
15.8
yr/F
*34.8
63.8
61.6
72.1
57.4
50.0
47.2
Sligh
tlyim
prove
dCap
sularinstab
ility
requiringrevision
17.7
yr/M
21.5
67.1
84.7
63.2
94.1
25.0
88.9
Improve
dNone
18.0
yr/F
24.7
64.9
100
42.6
100
44.4
94.4
Much
improve
dNone
14.5
yr/F
22.6
68.2
95.7
79.4
91.2
77.8
83.3
Improve
dLFCN
numbn
ess,resolved
by3-m
ofollow-up
19.1
yr/M
20.2
64.9
100
66.2
98.5
38.9
94.4
Much
improve
dnone
26.9
yr/M
15.0
95.7
95.7
97.0
100
94.4
100
Unch
anged
none
15.2
yr/M
12.6
61.6
84.7
72.0
98.5
63.8
100
Improve
dHeterotopic
ossification
Meanag
e(ran
ge)
28.6
(12.6-55.6)
63.6
(33.0-95.7)
91.4
(61.6-100)
70.2
(42.6-97.0)
93.3
(57.4-100)
53.4
(25.0-94.4)
88.9
(47.2-100)
ADL,activities
ofdaily
living;
F,female;
HOS,Hip
OutcomeScore;LFCN,lateralfemoralcu
taneo
usnerve
release;
M,male;
mHHS,modified
HarrisHip
Score;SCFE,slipped
capital
femoral
epiphysis.
*Thepatientunderwen
trevisionsurgeryforcapsularrepairbe
cause
ofperceived
anteriorcapsularinstab
ilityafterasportinginjury
postoperatively.
HIP ARTHROSCOPY FOR POST-SCFE DEFORMITY 5
Joint injury has also been found ubiquitously duringdelayed deformity correction. Three groups have re-ported that all patients undergoing a surgical dislocationto treat a post-SCFE deformity had some degree ofarticular cartilage or labral injury.9-11 Interestingly, theabsence of hip pain may not preclude the possibility ofarticular damage. A recent case report of 5 asymp-tomatic patients with mild SCFE deformity showed thatall patients had acetabular damage within 18 monthsof in situ pinning.21 Similarly, gadolinium-enhancedmagnetic resonance imaging of hips after in situfixation of SCFE showed cartilage abnormalities in post-SCFE hips that did not correlate with subjective symp-toms.22 These studies suggest that SCFE deformitycommonly results in early articular damage that persistsafter in situ pinning, can be present even in the absenceof symptoms, and may lead to early total hip arthro-plasty in this population.3 In our cohort all 9 patientshad acetabular and/or labral pathology visualized at amean of 52.8 months after in situ pinning duringarthroscopic osteochondroplasty. Pathology was pri-marily located in the anterosuperior region of the jointand the corresponding labral tissue, as has been pri-marily described with cam-type FAI.7
Treatment of the residual SCFE deformity is per-formed to reduce pain, improve function, and reduceprogression of joint degeneration.12 It is difficult todetermine whether the timing of deformity correctionplays a role in joint degeneration; however, severalreports have raised the concern that premature arthritismay develop from FAI associated with even minorslips.23 Consequently, reduction of the SCFE acutely orreorientation of the proximal femur after healing in situhas been advised in an attempt to prevent long-termsequelae including early hip arthritis.24 Retrospectivedata support a possible link between residual SCFEdeformity and premature hip arthritis. A recent studyfound subclinical SCFE morphology in over 60% ofcases of early hip arthritis.25 The potential for futuredevelopment of hip arthritis after SCFE in our series isconcerning because joint injury was found in all pa-tients at the time of treatment that did not seem to bedependent on the time from pinning to arthroscopy.We were unable to determine whether time to osteo-chondroplasty was associated with worsened hip pa-thology; however, without correction of the SCFEdeformity, the possibility of repetitive impingement islikely. Resultant joint degradation from post-SCFEimpingement could justify aggressive correction tohopefully prevent compounded articular injury andpreserve the hip joint. However, in the setting oftraditional cam, pincer, or mixed FAI, there is no evi-dence to suggest that prophylactic surgery to preservethe hip joint is indicated.26
Arthroscopic osteochondroplasty is a low-morbidityprocedure that may be capable of correcting post-

Fig 3. Improvement at mean of 28.6 months postoperativelyin modified Harris Hip Score (mHHS), Hip Outcome Scoreactivitieseofedaily living scale (HOS ADL), and Hip OutcomeScore sports scale (HOS Sports) after arthroscopy for posteslipped capital femoral epiphysis deformity. The asterisksindicate P < .05.
6 J. D. WYLIE ET AL.
SCFE deformity. Historically, staged intertrochantericosteotomy was performed after in situ SCFE pinning,with good long-term outcomes reported.27 Morerecently, some authors have advocated techniques thataddress the SCFE deformity concomitantly with treat-ment of the acute slip. Open surgical dislocation of thehip while monitoring blood flow to the femoral headhas been described for reduction of the acute slip withconcomitant osteochondroplasty for correction of re-sidual femoral neck deformity.24,27 A recent reportshowed good short-term outcomes in 3 patients whounderwent hip arthroscopy with osteochondroplasty atthe time of in situ fixation for SCFE.12 These patientswere reported to have no pain and a return to full ac-tivities at final follow-up; however, there were nofunctional outcomes reported. Our study found thatpatients who underwent arthroscopic osteochon-droplasty also had improved pain and function at aminimum 1-year follow-up. Although comparisonamong procedures is difficult because this is the firststudy to report preoperative and postoperative vali-dated outcome measures after arthroscopy, functionalimprovements were observed to be statistically signifi-cant in all outcome scores in this series. Hip arthroscopyhas the added advantage of less morbidity when
compared with open hip surgery and has been shownto be equivalent to open surgery for similar proceduresincluding the treatment of FAI.28,29 In this series thealpha angle was corrected, on average, from 75� pre-operatively to 46� postoperatively, showing the tech-nical feasibility of arthroscopic osteochondroplasty torestore a more normal femoral anatomy.This report shows that hip arthroscopy with femoral
osteochondroplasty is a viable option to treat symp-tomatic SCFE patients previously treated with in situpinning at the time of the slip. This study is the first toreport functional outcomes in this cohort of patients.
LimitationsThere are limitations to this study. It included a small
number of patients with limited follow-up, and therewas no control group of patients who underwent con-servative or open treatment. There was no a prioripower analysis performed. Larger groups of patientswith longer follow-up periods will be needed to un-derstand the durability of hip arthroscopy for SCFEdeformity. Comparisons with open treatment will needto be made to understand how best to care for thesepatients. However, this study does show the describedtechnique to be effective at least in the short-termfor symptomatic deformity after SCFE. Further studiesare needed to determine whether this procedure pre-serves the hip joint and prevents degenerative changeover time.
ConclusionsCartilage and/or labral damage caused by SCFE
develops in patients with symptomatic mild to mod-erate SCFE deformity and that arthroscopic treatmentimproved functional outcomes and physical activitylevels in a small cohort of patients at short-termfollow-up.
References1. Lehmann CL, Arons RR, Loder RT, Vitale MG. The
epidemiology of slipped capital femoral epiphysis: Anupdate. J Pediatr Orthop 2006;26:286-290.
2. Manoff EM, Banffy MB, Winell JJ. Relationship betweenbody mass index and slipped capital femoral epiphysis.J Pediatr Orthop 2005;25:744-746.
3. Novais EN, Millis MB. Slipped capital femoral epiphysis:Prevalence, pathogenesis, and natural history. Clin OrthopRelat Res 2012;470:3432-3438.
4. Larson AN, McIntosh AL, Trousdale RT, Lewallen DG.Avascular necrosis most common indication for hiparthroplasty in patients with slipped capital femoralepiphysis. J Pediatr Orthop 2010;30:767-773.
5. Carney BT, Weinstein SL, Noble J. Long-term follow-upof slipped capital femoral epiphysis. J Bone Joint Surg Am1991;73:667-674.
6. Mamisch TC, Kim YJ, Richolt JA, Millis MB, Kordelle J.Femoral morphology due to impingement influences the

HIP ARTHROSCOPY FOR POST-SCFE DEFORMITY 7
range of motion in slipped capital femoral epiphysis. ClinOrthop Relat Res 2009;467:692-698.
7. Ganz R, Parvizi J, Beck M, Leunig M, Notzli H,Siebenrock KA. Femoroacetabular impingement: A causefor osteoarthritis of the hip. Clin Orthop Relat Res2003;(417):112-120.
8. Monazzam S, Bomar JD, Pennock AT. Idiopathic cammorphology is not caused by subclinical slipped capitalfemoral epiphysis. An MRI and CT study. Orthop J SportsMed 2013;1:1-6.
9. Sink EL, Zaltz I, Heare T, Dayton M. Acetabular cartilageand labral damage observed during surgical hip disloca-tion for stable slipped capital femoral epiphysis. J PediatrOrthop 2010;30:26-30.
10. Ziebarth K, Leunig M, Slongo T, Kim YJ, Ganz R. Slippedcapital femoral epiphysis: Relevant pathophysiologicalfindings with open surgery. Clin Orthop Relat Res 2013;471:2156-2162.
11. Leunig M, Casillas MM, Hamlet M, et al. Slipped capitalfemoral epiphysis: Early mechanical damage to theacetabular cartilage by a prominent femoral metaphysis.Acta Orthop Scand 2000;71:370-375.
12. Leunig M, Horowitz K, Manner H, Ganz R. In situ pinningwith arthroscopic osteoplasty for mild SCFE: A pre-liminary technical report. Clin Orthop Relat Res 2010;468:3160-3167.
13. Beck M, Kalhor M, Leunig M, Ganz R. Hip morphologyinfluences the pattern of damage to the acetabular carti-lage: Femoroacetabular impingement as a cause of earlyosteoarthritis of the hip. J Bone Joint Surg Br 2005;87:1012-1018.
14. Byrd JW, Jones KS. Prospective analysis of hip arthros-copy with 2-year follow-up. Arthroscopy 2000;16:578-587.
15. Byrd JW, Jones KS. Primary repair of the acetabularlabrum: Outcomes with 2 years’ follow-up. Arthroscopy2014;30:588-592.
16. Larsen CM, Giveans MR, Samuelson KM, Stone RM,Bedi A. Arthroscopic hip revision surgery for residualfemoroacetabular impingement (FAI): Surgical outcomescompared with a matched cohort after primary arthro-scopic FAI correction. Am J Sports Med 2014;42:1785-1790.
17. Martin RL, Philippon MJ. Evidence of validity for the hipoutcome score in hip arthroscopy. Arthroscopy 2007;23:822-826.
18. Aoki SK, Beckmann JT, Wylie JD. Hip arthroscopy andthe anterolateral portal: Avoiding labral penetration andfemoral articular injuries. Arthrosc Tech 2012;1:e155-e160.
19. Kocher MS, Bishop JA, Weed B, et al. Delay in diagnosisof slipped capital femoral epiphysis. Pediatrics 2004;113:e322-e325.
20. McPartland TG, Sankar WN, Kim YJ, Millis MB. Patientswith unstable slipped capital femoral epiphysis haveantecedent symptoms. Clin Orthop Relat Res 2013;471:2132-2136.
21. Lee CB, Matheney T, Yen YM. Case reports: Acetabulardamage after mild slipped capital femoral epiphysis. ClinOrthop Relat Res 2013;471:2163-2172.
22. Zilkens C, Miese F, Bittersohl B, et al. Delayedgadolinium-enhanced magnetic resonance imaging ofcartilage (dGEMRIC), after slipped capital femoral epiph-ysis. Eur J Radiol 2011;79:400-406.
23. Fraitzl CR, Kafer W, Nelitz M, Reichel H. Radiologicalevidence of femoroacetabular impingement in mild slip-ped capital femoral epiphysis: A mean follow-up of 14.4years after pinning in situ. J Bone Joint Surg Br 2007;89:1592-1596.
24. Kuzyk PR, Kim YJ, Millis MB. Surgical management ofhealed slipped capital femoral epiphysis. J Am Acad OrthopSurg 2011;19:667-677.
25. Giles AE, Corneman NA, Bhachu S, et al. Sharedmorphology of slipped capital femoral epiphysis andfemoroacetabular impingement in early-onset arthritis.Orthopedics 2013;36:e1365-e1370.
26. Collins JA, Ward JP, Youm T. Is prophylactic surgery forfemoroacetabular impingement indicated?: A systematicreview. Am J Sports Med in press, available online 21 August,2013. doi: 10.1177/0363546513499227.
27. Masse A, Aprato A, Grappiolo G, Turchetto L,Campacci A, Ganz R. Surgical hip dislocation for anatomicreorientation of slipped capital femoral epiphysis: Pre-liminary results. Hip Int 2012;22:137-144.
28. Botser IB, Smith TW Jr, Nasser R, Domb BG. Open sur-gical dislocation versus arthroscopy for femoroacetabularimpingement: A comparison of clinical outcomes.Arthroscopy 2011;27:270-278.
29. Domb BG, Stake CE, Botser IB, Jackson TJ. Surgicaldislocation of the hip versus arthroscopic treatment offemoroacetabular impingement: A prospective matched-pair study with average 2-year follow-up. Arthroscopy2013;29:1506-1513.





























