Embed Size (px)
Citation preview

This article was downloaded by: [UVA Universiteitsbibliotheek SZ]On: 12 June 2015, At: 06:52Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registeredoffice: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK
Anxiety, Stress, & Coping: AnInternational JournalPublication details, including instructions for authors andsubscription information:http://www.tandfonline.com/loi/gasc20
Assessment of dental anxiety: A facetapproachMarlies E. A. Stouthard a , Gideon J. Mellenbergh a & JohanHoogstraten ba University of Amsterdam , The Netherlandsb Department of Social Densitry , Dental Health Education AcademicCentre for Dentistry Amsterdam , The NetherlandsPublished online: 29 May 2007.
To cite this article: Marlies E. A. Stouthard , Gideon J. Mellenbergh & Johan Hoogstraten (1993)Assessment of dental anxiety: A facet approach, Anxiety, Stress, & Coping: An International Journal,6:2, 89-105, DOI: 10.1080/10615809308248372
To link to this article: http://dx.doi.org/10.1080/10615809308248372
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all the information (the“Content”) contained in the publications on our platform. However, Taylor & Francis,our agents, and our licensors make no representations or warranties whatsoever as tothe accuracy, completeness, or suitability for any purpose of the Content. Any opinionsand views expressed in this publication are the opinions and views of the authors,and are not the views of or endorsed by Taylor & Francis. The accuracy of the Contentshould not be relied upon and should be independently verified with primary sourcesof information. Taylor and Francis shall not be liable for any losses, actions, claims,proceedings, demands, costs, expenses, damages, and other liabilities whatsoever orhowsoever caused arising directly or indirectly in connection with, in relation to or arisingout of the use of the Content.
This article may be used for research, teaching, and private study purposes. Anysubstantial or systematic reproduction, redistribution, reselling, loan, sub-licensing,systematic supply, or distribution in any form to anyone is expressly forbidden. Terms &Conditions of access and use can be found at http://www.tandfonline.com/page/terms-and-conditions

Anxiety, Stress, and Coping, 1993, Vol. 6, pp. 89-105 Reprints available directly from the publisher Photocopying permitted by license only
0 1993 Harwood Academic Publishers GmbH Printed in Malaysia
ASSESSMENT OF DENTAL ANXIETY: A FACET APPROACH
MARLIES E. A. STOUTHARD, GIDEON J. MELLENBERGH University ofAmsterdam, The Netherlands
JOHAN HOOGSTRATEN Department of Social Densitry and Dental Health Education Academic Centre for Dentistry Amsterdam, The Netherland
(Received I9 March 1993)
Dental anxiety is a complicated phenomenon, and its multicomponent nature is often not acknow- ledged in existing measurement instruments. Using a facet design, a new Dental Anxiety Inventory (DAI) was constructed. Facets chosen were: time(made up of four elements: at home, on your way to the denstist, in the denstist’s waiting room, in the dental chair), situation (three elements: introductory aspects, dentist-patient interaction, actual dental treatment), and reaction (three elements: subjective feelings, physical reactions, cognitive reactions). Psychometric qualities of the DAI are good. The internal structure of the DAI was studied by linear and nonlinear techniques, and was partially recovered from the data. The construct and criterion validity of the DAI was supported in several studies.
KEY WORDS test construction, facet design, dental anxiety, LISREL, multidimensional scaling, construct and criterion validity.
Just as the general term anxiety may have diverse meanings (Edelmann, 1992), dental anxiety is not a clear-cut concept. In lay terms, being anxious when at the denstist might refer to a relatively mild feeling of apprehension as well as to extreme dental anxiety. Also in the dental literature, different definitions are found, if any at all. Dental anxiety is used alternately to cover a general feeling of fear and apprehension (Emphasis, 1983), extreme or disproportionate anxiety (Molin & Seeman, 1969) and dental phobia (hutch, 1971). Its range varies with each definition. Another quality of dental anxiety often not acknowledged is its multi- component nature, both with regard to the stimulus situations and the response systems. Fear for dental procedures and pain anticipation on the one hand, and physical reactions on the other hand have been stressed too much (Glanzmann, 1989). This is surprising since the importance of other stimulus situations has repeatedly been shown. Gale (1 972) found that perceived negative comments by the dentist on the patient’s oral state was rated almost as high as dental procedures like drilling and extraction. Stouthard and Hoogstraten (1987) confirmed this result in a paired comparison study. Seeman and Molin (1 976) showed that feelings of helplessness and confinement to the dental chair are important aspects of dental anxiety. Also, the multidimensionality of dental anxiety reactions has been stressed (Berggren, 1984; Ingersoll, 1982; Melamed, 1979). Analogous to anxiety in general
Address correspondence to: Dr. M. E. A. Stouthard, Department of Methodology, Faculty of Psycho- logy, University of Amsterdam, Roetersstraat 13, 101 8 WB Amsterdam, The Netherlands
89
Dow
nloa
ded
by [
UV
A U
nive
rsite
itsbi
blio
thee
k SZ
] at
06:
52 1
2 Ju
ne 2
015

90 M. E. A. STOUTHARD et al.
(Edelmann, 1992; Schwarzer, Van der Ploeg, & Spielberger, 1987), emotional, cognitive, physiological, and behavioral aspects may be discerned. It might there- fore be concluded that dental anxiety is no simple phobia e.g., coinciding with blood-injury fear (Edelmann, 1992), but rather that it is a complex phenomenon which also has to do with threat of self-respect, loss of control and social anxiety (Glanzmann, 1989). The dentist-patient relationship plays an important role in addition to pain anticipation and dental procedures. And multiple response systems should be taken into account.
This lack of consensus about its domain and range is reflected in the assessment of dental anxiety. None of the dental anxiety instruments known to us satisfy the above-mentioned theoretical points. Moreover, a critical appraisal of the fear- instruments available at present (Stouthard, 1989) showed they do not comply with the APA norms for test construction (adjusted Dutch version; Evers, Vliet- Mulder, & Ter Laak, 1992). The two most frequently used dental anxiety measures are Corah’s four-item Dental Anxiety Scale (DAS; Corah, 1969) and the 20-item Dental Fear Survey (Kleinknecht, Klepac, & Alexander, 1973). Serious criticism applies to both, although their reliability is satisfactory and their validity is widely supported.
First, with regard to the DAS, Corah (1969) claimed that its aim is the assessment of dental anxiety, but no theoretical definition of the construct is given, which leaves the validity of this claim in the dark. The multicomponent nature of dental anxiety is not reflected in the items. As a result, the DAS was not able to detect the effect of the dentist-patient relations on dental anxiety (Rouse & Hamilton, 1990). Second, the DAS does not contain a standardized instruction. Furthermore, the response alternatives of the last three items of the DAS do not form a rating scale, but instead the two reaction modes: affective feelings (“re- laxed”, “anxious”) and physical reactions (“tense”, “break in a sweat or feel physically sick”) are used intermingled. Thus, the scale is not unidimensional with regard to its content. Also, the DAS is not balanced with respect to item syntax and content. The fourth item is deviant in form (not of the “If. . ., then . . .” type) and more detailed (“. . . scrape your teeth around the gums . . .”) than the other three items. As a result, the item does not contribute to the scale’s internal consistency (Stouthard, 1986). And finally, no clear-cut norm scores for men and women are available, but only an incomplete guideline for the interpretation is given (Corah, Gale, & Wig, 1978).
The criticism on the DFS concentrates mainly on its unbalanced structure (Glanzmann, 1989). The questionnaire contains two items on behavioral reactions (dental avoidance) and five on physiological reactions, but none on the cognitive and affective reaction modes. Furthermore, although items on fear for different aspects of the dental treatment are included, items on the dentist’s comments and the dentist-patient relationship are omitted. And again, a standardized instruction is lacking and no norm scores are available.
Other measures of dental anxiety have also been published. Single-item mea- sures like Schuurs’ (1 98 l) self-report measure about time-related physiological reactions (DPFR) and Neverlien’s (1990) Dental Anxiety Question (DAQ) might seem to serve as practicable approximations of the intensity of dental anxiety. However, the criterion validity of such global ratings is questionable (Paulonen & Jackson, 1985). And from the nature of things, they can only capture an overall impression of dental anxiety or, alternatively, one single aspect. Consequently,
Dow
nloa
ded
by [
UV
A U
nive
rsite
itsbi
blio
thee
k SZ
] at
06:
52 1
2 Ju
ne 2
015

DENTAL ANXIETY: A FACET APPROACH 91
respondents might interpret the situation to which they respond differently. Results based on such idiosyncratic interpretations would be of little use (Kleinknecht, Thorndike, McGlynn, & Harkavy, 1984).
In our view, at least some of the above-mentioned shortcomings of these scales are irreparable. To overcome the criticisms, it was decided to develop a new Dental Anxiety Inventory (DAI). Dental anxiety was defined as situation-specific trait anxiety, as the disposition to experience anxiety in dental situations. Its assessment should reflect the relatively stable individual differences in anxiety proneness to dental situations, and as such be a predictor of differential state anxiety increases in high and low trait-anxious persons (Laux & Glanzmann, 1987; Spielberger, 1972). Dental anxiety seems to be situation-specific so that operationalization separately from related concepts like general anxiety and neuroticism seems warranted.
The facet theory (Canter, 1985) offers a useful heuristic for test construction for complex concepts. It allows the test constructor to specify an exhaustive and systematic definition and operationalization. The DAI was constructed using such a facet approach. An attempt to map the whole domain of dental anxiety was made. All relevant aspects of the concept-to-be-measured were distinguished and com- bined in order to give a systematic description as completely as possible. The aim of this new instrument was not only to identify extremely anxious dental patients, but also to assess anxiety proneness to regular dental patients and the prevalence of dental anxiety in the general (Dutch) population. Thus it should cover the whole range of dental anxiety, from no anxiety at all to extreme anxiety.
Materials To analyze the concept of dental anxiety, a literature study and interviews with experts on dental anxiety were carried out. We found that a distinction should be made between the kinds of dental situations that may evoke anxiety, the types of reactions dental patients may experience, and in the duration of the state anxiety. First, fear-evoking stimuli not only evolve from the actual dental treatment, but also from the dentist-patient relationship (Gale, 1972; Stouthard & Hoogstraten, 1987). Patients may respond differentially to different dental situations. The actual dental treatment refers to invasive operations on the patient’s teeth and includes dental procedures such as drilling and extraction, oral inspection with the probe and giving an anaesthetic injection. The introductory aspects of the dental treat- ment refer to what precedes the dental treatment, ranging from making the appointment to the smell, sight and sound of the dental instruments. Interaction between dentist and patient includes the dentist’s comments on the patient’s oral health, communication about the dental treatment and the position of the patient.
Second, common reactions include affective, behavioral, cognitive and physical responses (Berggren, 198% Glanzrnann, 1989). Distinct anxiety reactions may refer to different aspects of dental anxiety and people tend to express their anxiety in different ways (Schuurs et al., 1985). Affective responses such as feeling nervous, anxious and insecure were labelled emotional feelings. Physical reactions include physiological responses such as sweating and heart palpitations as well as physical/ motor-behavioral responses like sleeplessness and clenching fists. Although total avoidance of dentistry is regarded as a manifestation of extreme dental anxiety (Schuurs, Duivenvoorden, Thoden van Velzen, & Verhage, 1984), the behavioral reaction mode was not included as a separate element of the reaction facet. Overt
Dow
nloa
ded
by [
UV
A U
nive
rsite
itsbi
blio
thee
k SZ
] at
06:
52 1
2 Ju
ne 2
015
92 M. E. A, STOUTHARD et al.
behavioral reactions appeared to occur too infrequently in the adult population (Kleinknecht & Bernstein, 1978) to justifjl inclusion of this category on psychomet- ric grounds. The aim of the inventory was not to differentiate between extremely anxious and other dental patients, but to cover the whole range of dental anxiety. Cognitive responses, finally, refer to thought and intentions to perform certain behaviors such as thinking about something else, or of cancelling or delaying the appointment, and wishing for withdrawal. In a previous version of the facet design, this category was labelled defense- and coping reactions. This description signified the purpose of the reactions rather than the reaction mode, which is primarily cognitive. Therefore, the label of this facet element was more adequately rephrased as cognitive reactions. The “worry” component of anxiety was also incorporated in the general part of the construct definition.
And finally, it was hypothesized that the onset of the state anxiety pertaining to the time of dental treatment signified its strength and nature (Hall & Edmondson, 1983; Schuurs, 1981). After all, fear in the dental chair may be common and conceivable, but fear at home long before the dental treatment may be qualitatively different.
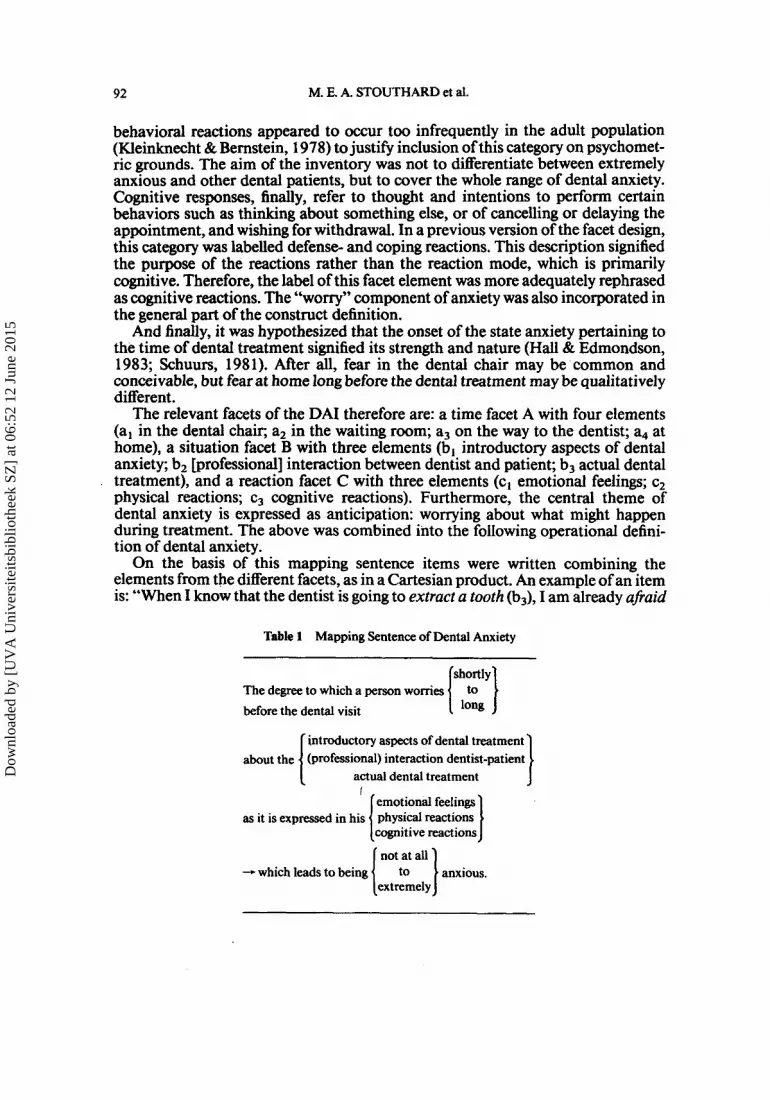
The relevant facets of the DAI therefore are: a time facet A with four elements (a, in the dental chair; a2 in the waiting room; a3 on the way to the dentist; a4 at home), a situation facet B with three elements (b, introductory aspects of dental anxiety; b2 [professional] interaction between dentist and patient; b3 actual dental treatment), and a reaction facet C with three elements (c, emotional feelings; c2 physical reactions; c3 cognitive reactions). Furthermore, the central theme of dental anxiety is expressed as anticipation: worrying about what might happen during treatment. The above was combined into the following operational defini- tion of dental anxiety.
On the basis of this mapping sentence items were written combining the elements from the different facets, as in a Cartesian product. An example of an item is: “When I know that the dentist is going to extract a tooth (b3), I am already ufi.aid
Table 1 Mapping Sentence of Dental Anxiety
The degree to which a person womes before the dental visit
introductory aspects of dental treatment
actual dental treatment
emotional feelings
cognitive reactions as it is expressed in his physical reactions
-.which leads to being [
(professional) interaction dentist-patient
‘ I I 1 anxious. extremely
Dow
nloa
ded
by [
UV
A U
nive
rsite
itsbi
blio
thee
k SZ
] at
06:
52 1
2 Ju
ne 2
015

DENTAL ANXIETY: A FACET APPROACH 93
(c,) in the waiting room (a2)”. In this way, 4 x 3 x 3 = 36 unique combinations could be formed. Each item was made up of specific examples of the constituting facet elements. Answer were given on a 5-point Likert-type scale, ranging from complete disagreement (1) to complete agreement (5). Scores may range from 36 to 180. The DAI contains a comprehensive instruction.
Method In several studies, the construct and criterion validity of the DAI was studied. These studies are described below in separate method and results sections. First, some psychometric characteristics of the DAI will be given.
STUDY 1
Procedure and subjects The psychometric characteristics of the DAI were studied in four different samples. The I986 cohort of psychology freshmen (n = 38 1 , 68% females, mean age was 23.8 years) completed the DAI as part of a compulsory course. This study was repeated with the 1988 cohort of psychology freshmen (n = 372,67% females, mean age was 23.1 years). To assess the test-retest reliability, these students completed the DAI again after five weeks.
Also, the DAI was administered to a nationwide sample (n = 648). The respon- dents were randomly drawn from a panel which was surveyed on a weekly basis. More information on the panel may be found elsewhere (Bon & Van Doorn, 1987). The sample proved representative with respect to oral health status, sex, age, educational level, income and geographic dispersion. The DAI was administered by means of a homecomputer (Stouthard & Hoogstraten, 1990).
And finally, the DAI was administrated to a sample of dental patients scheduled for a periodic check-up in two consecutive weeks in one general dental practice. All subjects (n = 89,37% men, mean age 34.9 years) were regular dental patients who visited the dentist twice a year. A second administration after two weeks allows for the assessment of the test-retest reliability.
Results The mean scores, standard deviations, score range, and reliability for all four samples are given in Table 2. Results indicate that the students on average scored higher than the dental patients and the nationwide sample. Furthermore, women consistently obtained higher scores than men. Subjects used the whole range of the DAI, except for the regular dental patients who tended to be not extremely anxious. The internal consistency (Cronbach’s a) and the test-retest reliability of the DAI were high. The results proved stable over the different samples.
Dow
nloa
ded
by [
UV
A U
nive
rsite
itsbi
blio
thee
k SZ
] at
06:
52 1
2 Ju
ne 2
015

94 M. E. A. STOUTHARD et al.
Table 2 Mean, Standard Deviation and Reliability of the DAI for Several Samples
M SD range a rxx n
Nationwide sample
Psychology students 1986
Psychology students 1988
Dental patients
Total Men
Women
Total Men
Women
Total Men
Women
Total Men
Women
66.9 32.3 61.1 30.5 72.5 33.1
77.2 24.4 72.4 22.1 79.7 25.0
75.1 26.9 68.9 22.4 78.0 28.3
63.6 29.1 61.9 31.2 65.4 28.2
36-1 78 36- 178 36-172
37- 179 37-133 37- 179
36-179 37- 164 36- 179
36-1 57 36- 150 36-157
.98
.98
.98
.96
.95
.96
.96
.95
.97
.97
.97
.97
648 320 328
38 1 123 258
.87 372
.81 123
.90 249
.84 89
.77 33
.9 1 56
STUDY 2
Procedure It was studied whether the chosen facets and their consisting elements could be recovered from the data. This was done by both linear (analysis of variance, confirmative factor analysis) and nonlinear (multidimensional scaling analysis) techniques.
On the basis of the facet design, we proposed a number of specific hypotheses about subscores of the DAI. The time facet may result in increasing scores over its elements: anxiety will be lowest at home, and highest in the dental chair (a, > a2 > a3 > a4). In other words, the nearer the dental treatment, the higher the mean anxiety score (Lamb & Plant, 1972; Schuurs, 1981; Tullman, Tullman, Rogers, & Rosen, 1979). With regard to the situation facet, we hypothesized that anxiety for actual dental treatment is stronger than for the other elements of this facet (b3 > b,,b2) (Gale, 1972; Stouthard & Hoogstraten, 1987). And finally, anxiety will be manifested more clearly in a person’s emotional feelings as compared to physical and behavioral reactions (c, > cz,c3) (Kleinknecht et al., 1984). An analysis of variance with repeated measurements aimed at studying these hypotheses.
The theoretical facet structure of the DAI was represented in a factor analytical model as follows: (a) The four elements of facet A and the three elements of facet B and facet C constitute ten factors, with loadings from only those items in which these factors were represented. For example, an item representing the elements a2, b3 and c, had factor loadings on only these three factors. (b) Furthermore, a general factor “dental anxiety” was assumed, on which all items loaded.
Dow
nloa
ded
by [
UV
A U
nive
rsite
itsbi
blio
thee
k SZ
] at
06:
52 1
2 Ju
ne 2
015

DENTAL ANXIETY: A FACET APPROACH 95
(c) Both the elements per facet and the facets themselves could be intercorrelated. However, some restrictions had to be made for the identifiability of the model. In order to keep the number of restrictions as small as possible, independence of the elements within facets but not between the facets was assumed. The general factor was uncorrelated with all specific factors. (d) All items also had loadings on a unique factor, which represented the variance not covered for by the common factors. The unique factors were uncorrelated. The factor analytical model of the facet design was analyzed by means of LISREL (Joreskog & Srbom, 1986). ULS-estimators were used and the goodness of fit was assessed by AGFI (adjusted goodness of fit) and RMR (root mean square residual). The multidimensional scaling was done using MINISSA (Roskam, 1975). It was assumed that items with common facet-elements would be located closer together in a multidimensional Euclidian space than items without common facetelements. Thus, per facet regions of items containing the same facet-elements should be identifiable.
Subjects The psychometric characteristics of the DAI wete studied in a nationwide sample (n = 648). The study was repeated with the 1986 cohort of psychology freshmen (n = 38 1).
Results
Internal structure of the DAI Mean subscores of the elements per facet (see Table 3) showed the expected
Table 3 Mean Subscores of Elements per Facet
Time facet
a1 a2 a3 a4 M 18.2 16.4 16.1 16.0 SD 8.7 8.1 8.3 6.3
Situation facet
M SD
b, b2 b3 22.3 20.3 24.0 11.3 10.1 11.8
Reaction facet
CI c2 c3 M 22.7 21.9 22.2 SD 11.4 10.8 10.7
Note. n - 648.
Dow
nloa
ded
by [
UV
A U
nive
rsite
itsbi
blio
thee
k SZ
] at
06:
52 1
2 Ju
ne 2
015

96 M. E. A. STOUTHARD et al.
tendency. Results of the analysis of variance showed a significant difference between subscores on the time facet (F= 127.53 with df= 3,1941, p < .Ol), the situation facet (F = 174.22 with df = 2,1294, p < .Ol), and the reaction facet (F = 12.19 with df = 2,1294, p < .05). Contrast analyses showed that all differences were in the hypothesized direction (tested contrasts: a, > a,; a, > a3; a3 > a4; b3 > b,; b3 > b,; c, > c2; c, > c3). They were, however, small compared to their standard deviations.
The results of the confirmatory factor analysis using LISREL showed that the model did not fit the data well (AGFI = .86 1 and RMR = .182). Successive adjust- ments of the model resulted in some improvemment, but not in a good fit of the model (Stouthard, 1989).
After concluding that confirmative factor analysis would not lead to a model fitting the data, an exploratory factor analysis was conducted in order to study the internal structure further. The results formed the basis of a new confirmatory factor analysis. A model with three factors (general dental anxiety; fear for dentist’s comments on the teeth; fear for drilling, extraction and anaesthesia) showed good fit (AGFI = 0.996 and RMR = 0.034). Moreover, this model proved stable over different samples (Stouthard, 1989). The general factor was orthogonal to the other two, and the two specific factors were oblique. Factor loadings on the general factor were substantial (greater than .56), those on the specific factors somewhat lower.
The configuration resulting from the MINISSA analysis showed only partial congruency with the facet design. The two-dimensional solution represented the data best, although still with a moderate level of stress (SFORMI = .21 for the national sample). Only the situation facet B was clearly recognizable in this configuration (see Figure 1). Regions with items containing the same element of this facet could be identified. For example, the items representing facet element b,: dentist-patient interaction (denoted by middle digit 2 in data label) are located together at the left side of the two-dimensional Euclidian space. In the three- dimensional solution, that would perhaps be expected on theoretical grounds, both the situation and the time facet could be partially recognized (Stouthard, 1989). All analyses were repeated with a more homogeneous sample of psychology freshmen (1986 cohort; see Table 2). Similar results were found.
STUDY 3a
Procedure and subjects The relation of the DAI to other measures of dental anxiety was studied in two different samples in order to get some insight in the construct validity of the DAI. First, Corah’s DAS (1 969) was administered to the 1988 cohort of psychology freshmen (n = 372) several weeks after they completed the DAI, both as part of a compulsory course.
Results Mean DAS score for the psychology freshmen was 10.0 with standard deviation 3.0. Mean DAI score and standard deviation were 75.1 and 26.9 (see Table 2).
Dow
nloa
ded
by [
UV
A U
nive
rsite
itsbi
blio
thee
k SZ
] at
06:
52 1
2 Ju
ne 2
015

DENTAL ANXIETY: A FACET APPROACH 97
Figure 1. Two-dimensional MINNISA-solution of the internal structure of the DAI. Note. The digits denote the items by their combinations of facet elements (e.g., 213 refers to the item with elements a,b,c,)
Pearson's product moment correlation coefficient between DAS and' DAI was r = 0.82 ( n = 370).
STUDY 3b
Procedure and subjects The relation of DAI with DAS was also investigated in a random sample of 21 patients from a dental school (10 men and 1 I women, mean age was 38.2 years, two thirds were public health insurance patients). They were selected on socio- demographic characteristics to match a sample of extremely anxious dental patients. The subjects were visited at home and completed both questionnaires in the same session.
Results For the group of dental school patients, the mean scores and standard deviations were 6.8 and 2.0 for the DAS, and 56.9 and 16.6 for the DAI, respectively. The correlation between DAS and DAI was r = 0.69 ( n = 20).
Dow
nloa
ded
by [
UV
A U
nive
rsite
itsbi
blio
thee
k SZ
] at
06:
52 1
2 Ju
ne 2
015

98 M. E. A. STOUTHARD et al.
STUDY 3c
Procedure and subjects To further study the construct validity of the DAI, the relation between the DAI and the dentist’s judgement of his patient’s anxiety was studied as a multimethod comparison. The sample consisted of 43 patients from one general dental practice, 12 men and 31 women, mean age was 33.3 years. All patients scheduled for a periodic check-up in two consecutive weeks were invited to participate in the waiting room before dental treatment or after treatment. They completed the DAI individually as a paper-and-pencil test. The two dentists who participated in this study were asked to rate their patients individually after the control visit on a 5-point behavior rating scale indicating patient’s tension, anxiety and susceptibil- ity to treatment (Carlsson, Linde, & ohman, 1980).
Results The results of the dentists’s judgement indicated that no patients were rated extremely anxious, and most patients were rated relaxed and not anxious (55.8%) or a Iittle anxious and tense (27.9%). Mean DAI score was 62.7 with standard deviation 28.9. The correlation between the DAI and the dentist’s judgement was moderate (r = 0.38). The restriction of range of the dentists’ judgement scores and the relatively small sample might have confined this result.
STUDY 4
Procedure and subjects The concurrent validity and the sensitivity of the DAI were studied quasi- experimentally. The DAI-scores of patients known to be extremely dentally anx- ious were compared to the DAI-scores of patients presumed not anxious. The external criterium used for selecting extremely anxious dental patients was accep- tation for treatment in a special Dental Health Clinic. The patients of this clinic were extremely anxious, often to the extent that they had avoided regular dental care for many years (Makkes, Schuurs, Thoden van Velzen, Duivenvoorden, & Verhage, 1986). All waiting list patients admitted for treatment (n = 21) partici- pated in this study. Patients presumed not anxious were Dental School patients treated by dental students. Green and Green (1 987) showed that among a similar group of patients the average level of anxiety is relatively low. The two groups of patients were matched on sex and age. Educational level, occupational level and health insurance were controlled for statistically. The mean DAS scores of the groups were 15.5 and 6.8, respectively, indicating a successful quasi-experimental manipulation.
Resu Its DAI scores of both groups are presented in Table 4. The differences between these two groups were large as expected (t-test for dependent samples; t = 10.41 with
Dow
nloa
ded
by [
UV
A U
nive
rsite
itsbi
blio
thee
k SZ
] at
06:
52 1
2 Ju
ne 2
015

DENTAL ANXIETY: A FACET APPROACH 99
Table 4 Diffrence Betwen Anxious and Nonanxious Patients
Group' Anxious Nonanxious
DAI M 130.5 57.9 SD 23.6 17.1
Note. "n - 19 for each group.
df = 18, p < .01). By means of discriminant analysis, with the DAI as discriminat- ing variable, it was examined whether the DAI could accurately predict dental anxiety. Results showed that 95.2% of the respondents were correctly classified as either belonging to the extremely anxious group or to the low-anxious group.
STUDY 5
Procedure and subjects The claim that the DAI should measure specific dental trait anxiety was studied. The DAI scores should reflect the relatively stable dental anxiety proneness, independent of the situation. If this claim is correct, the moment of administration of the DAI with regard to the dental visit should not influence its results. If the DAI should essentially measure dental state anxiety, the scores should be higher just before and during dental treatment than afterwards (Eijkman & Orlebeke, 1975; Lamb & Plant, 1972; Tullman et al., 1979).
We studied the effect of moment of administration on dental anxiety quasi- experimentally, with overall dental trait anxiety level as a covariate. All partici- pants (n = 89) were regular dental patients (33 men and 56 women) who visited the dental office twice a year for a periodical check-up. The DAI was administered to dental patients in one of three conditions. The moment of administration was the manipulated variable: just before the dental visit in the waiting room (Condition l), just after the dental visit in the waiting room (Condition 2), or three months after the last dental visit at home (Condition 3). Patients visiting the dental office in three consecutive weeks were randomly assigned to Conditions 1 or 2. For Condition 3, patients were randomly drawn from the group that visited the dentist about three months ago. All patients were asked in advance by mail to participate, and about 50% agreed. We hypothesized that no differences in DAI scores would exist. To control for overall dental trait anxiety level, all patients were asked to complete the DAI a second time two weeks after the first administration at home. After a reminder by phone, 80% responded to this request (n = 7 1). To control for the quasi-experimental manipulation, in Conditions 1 and 2 dental state anxiety was measured retrospectively just after the dental visit, using three simple ques- tions ("How anxious were you in the waiting room / . . . during treatment / . . . now?'). Scores may range from 1 to 5.
Results Dental state anxiety increased somewhat from waiting room to treatment, and dropped considerably after treatment, as was to be expected (see Figure 2). T-tests
Dow
nloa
ded
by [
UV
A U
nive
rsite
itsbi
blio
thee
k SZ
] at
06:
52 1
2 Ju
ne 2
015

100
2.0 -
1.8 -
1.6 -
1.4 -
1.2 -
M. E. A. STOUTHARD et al.
Q)
m c c ? a
1.0 1, before during after
moment Figure 2. Dental state anxiety before, during and after treatment. Note. Conditions 1 and 2 combined. n = 51.
showed that the differences were significant. State anxiety was indeed higher before than after the dental visit.
The results of the DAI for the three conditions and two administrations are given in Table 5. Analyses of variance showed no effect of condition for either the first or the second administration of the DAI (F= 1.35, p = .26 and F = 1.29, p = .28, respectively, both with 2 and 68 degrees of freedom). Analysis of variance
Table 5 Results of Both Administrations of the DAI for Three Conditions
Condition 18 IIb I I I C
First X 69.4 56.9 64.0 administration SD 32.1 24.7 29.3
n 30 28 31
Second X 68.9 54.5 65.0 Administration SD 32.3 26.1 30.9 after 2 weeks n 26 19 62
Note. 'Just before treatment. bJust after treatment. Three months after dental visit
Dow
nloa
ded
by [
UV
A U
nive
rsite
itsbi
blio
thee
k SZ
] at
06:
52 1
2 Ju
ne 2
015

DENTAL ANXIETY: A FACET APPROACH I01
of the DAI scores for the first administration with the results of the second administration as covariates also revealed no effect of condition (F-0.85 with df = 2,67 andp = .43). This finding was not contaminated by overall dental anxiety level in the three groups, since no differences between conditions were found for the second administration. Also, the DAI scores for the first and second adminis- tration showed no significant differences in each condition. And finally, the correlation between the DAI and state anxiety was high in Condition 1 (r = 0.87) as well as in Condition 2 (r = 0.83).
DISCUSSION
The surplus value of the facet approach for the measurement of dental anxiety was obvious on the level of operationalization. It suggested the inclusion of the time facet and the interaction between dentist and patient in the concept of dental anxiety. Inclusion was indicated by literature, but nevertheless until now not explicitly realized in other measures of dental anxiety. The use of the facet design in the construction of the DAI strongly supported its content validity. The facet structure of the DAI could not be completely recovered empirically, however. A possible explanation might be that the general component in the concept of dental anxiety is so dominant it overshadows all other facets. Alternatively, the respon- dents may not have employed the facet structure in their responses. The empirical structure of the DAI appeared to contain a strong general dental anxiety factor and two factors about specific dental situations. These two factors referred to the dentist-patient relations and fear for physical injury and pain, and were indicated as elements of the situation facet in the facet design. This suggests that a visit to the dentist may be perceived as a stressful situation characterized by both ego threat and physical danger.
A general drawback of the facet design is that the questionnaires constructed using this approach tend to be rather long. Therefore, the DAI is not primarily suitable to field situations. For the screening of dental anxiety in the dental practice, a shortened version of the DAI is available (SDAI, Stouthard, Groen, & Mellenbergh, 1992; See Appendix). In this nine-item version, the facet elements were combined in a Latin square instead of a Cartesian product, so that the facet structure was not lost (the time facet was reduced to three levels). With this restriction, nine items from the DAI were selected on psychometric grounds. The correlation between DAI and SDAI was high (r = .90) (Stouthard, 1989).
The reliability of the DAI is very high. This result might be due to the number of items. The reliability of the shortened nine-item version SDAI also proved to be high (Cronbach’s a of .91 and higher in different samples of students or patients; Stouthard, 1989). Both the internal consistency and the stability of the DAI are very satisfactory.
The validity of the DAI is supported in several studies. The correlation between DAI and DAS indicated a strong correspondence. Remarkably, it was somewhat lower in dental school patients, who filled in both in one session, than in psychology students, who completed both with a lapse of several weeks between them. This is possibly due to restriction of range in the former group. The relation of self- reported dental anxiety with a dentist’s judgement of the patient’s anxiety indi- cated reasonable agreement, especially since restriction of range appeared here too.
Dow
nloa
ded
by [
UV
A U
nive
rsite
itsbi
blio
thee
k SZ
] at
06:
52 1
2 Ju
ne 2
015

102 M. E. A. STOUTHARD et al.
The DAI differentiated between high-anxious and low-anxious dental patients, and its sensitivity and specificity were good. Finally, the authors’ claim that the DAI should measure situation specific trait anxiety was sustained. Although the DAI scores varied at different moments of administration, these differences did not reach significance in situations apart from the dental treatment, or even in situations related to the dental treatment. Moreover, trait anxiety as measured by the DAI seemed to predict differential increases in dental state anxiety accurately. The present results seem to support the DAI as a suitable measure of dental trait anxiety. Indeed, it was not intended to be a measure of dental state anxiety. It should refer to anxiety proneness, indicating and predicting the degree of dental anxiety a person usually experiences before and during dental treatment. State anxiety calls for an independent assessment using an appropriate measurement instrument (Corah, 1986; Laux & Glanzmann, 1987).
The DAI contains a standardized instruction. Lack of it is stressed as an important methodological shortcoming in other existing instruments. The effect of change in instruction on responses should not be underestimated. The use of an extended instruction with the DAI led to different results: mentioning the facet structure in the instruction resulted in lower overall DAI scores (Stouthard, 1989). This result was interpreted as support for the alternative explanation that respon- dents did not respond to the facet design. The fit of the confirmatory factor model did not improve, however, nor did the multidimensional scaling technique solu- tion.
It may be concluded that the DAI is a suitable instrument for measuring dental anxiety. It is highly reliable and its validity is satisfactory so far. Norms for the DAI in the Dutch version are available (Stouthard, 1990). The DAI complies with APA norms of test design and construction, reliability and validity (Evers et al., 1992). The use of the facet design in test construction has offered the opportunity for a thorough analysis of the construct and its assessment.
REFERENCES
Berggren, U. (1984). Dental fear and avoidance. A study of etiology consequences and treatment. Unpublished doctoral dissertation. Goteborg: University of Goteborg, Faculty of Odontology.
Bon, E.P.M., & Doom, L. van (1 987). Some results and experiences of a new consumer panel technique: Tefe interview. Paper presented at the FSOMAR Seminar in Dusseldorf June 10-12. Amsterdam, NIm.
Canter, D. (1 985). Facet theory. New York Springer Verlag. Carlsson, S.G., Linde, A., & Ohman, A,( 1980). Reduction of tension in fearful dental patients. Journal
Corah, N.L. (1 969). Development of a dental anxiety scale. Journal of Dental Research. 48.596. Corah, N.L (1 986). Methodological needs and behavioral research with adult dental patients. Anaesthe-
Corah, N.L, Gale, E.N., & Illig, S. J. (1978). Assessment of a dental anxiety scale. Journal ofthe
Edelmann, RJ. (1992). Anxiety. Theory, research and intewention in clinical and health psychology.
Emphasis (1 983). Overcoming dental fear: Strategies for its prevention and management. Journaf ofthe
Eijkman, M.A.J., & Orlebeke, J.F. (1975). De faktor ‘angst’ in de tandheelkundige behandeling [The
of theAmerican DentalAssociation, 101,638-641.
sia Progress, 33,46119.
American Dental Association, 97,8 16-81 9.
Chichester: John Wiley and Sons Ltd.
American Dental Association, 107, 18-27.
factor ‘anxiety’ in dental treatment]. Nederlands Tijakchriji voor Tandheelkunde, 82, 1 14-1 23.
Dow
nloa
ded
by [
UV
A U
nive
rsite
itsbi
blio
thee
k SZ
] at
06:
52 1
2 Ju
ne 2
015

DENTAL ANXIETY: A FACET APPROACH 103
Even, A., vliet-Mulder, 3.C. van, & Laak, 3. ter (1992). Documenfatie van tests en testresearch in
Gale, E.N. (1972). Fears of the dental situation. Journal ofDentalResearch, 51,964-966. Glanzmann, P.G. (1989). Methoden zur Messung von Angst and Angstlichkeit. In H.G. Sergl. & H.
Miiller-Fahlbusch (Eds.) Angst undAngstabbau in der Zahnmedizin (pp. 17-28). Berlin: Quintessenz Verlag.
Green, RM., & Green, A. (1987). Patient’s perceptions of their overall level of anxiety of dental care. British Dental Journal, 162, 55-156.
Hall, N., & Edmondson, H.D. (1983). The aetiology and psychology of dental fear. British Dental Journal, 154,247-252.
Ingersoll, B.D. ( 1982). Behavioral aspects of dentistry. Norwalk, C T Appleton-Century-Croft. Joreskog, KG., & Sorbom, D. (1986). WSREL VI. Analysis of linear structural relationships by
maximum likelihood, instrumental variables and least square m e t h d . 4th Ed. Uppsala, Sweden: University of Uppsala.
Kleinknecht, R.A., & Bernstein, D.A. (1978). The assessment of dental fear. Behavioral Therapy, 9,
Kleinknecht, R.A., Klepac, R.K, & Alexander, L.D. (1973). Origins and characteristics of dental fear.
Kleinknecht, R.A., Thorndike, R.M., McGlynn, F.D., & Harkavy, J. (1984). Factor analysis of the
Lamb, D.H., & Plant, R. (1972). Patient anxiety in the dental office. Journal of Denfal Research, 51,
hutch, H. (1971). Dental phobia. British JournalofPsychiatry, 119, 151-158. Laux, L., & Glanzmann, P. (1987). A self-presentational view of test anxiety. In Schwarzer, R., Ploeg, H.
M. van der, & Spielberger, C.D. (Eds.) Advances in test anxiety research, Vol. 5, (pp. 31-37). Lisse: Swets and Zeitlinger.
Makkes, P.C., Schuurs, A.H.B., Thoden van Velzen, S.K., Duivenvoorden, H. J., & Verhage, F. (1 986). Criteria voor selectie van volwassenen met extreme angst voor de tandheelkundige behandeling [Criteria for the selection of patients wth extreme dental anxiety]. Nederfands Tijhchrift voor Tandheelkunde, 93,3 17-32 1.
Melamed, B.G. (1979). Behavioral approaches to fear in dental settings. In M. Hersen, R.M. Eider, & P.M. Miller (Eds.) Progress in behavior modification Vol. 7(pp. 17 1-203). New York: Academic Press.
Molin, C., & Seeman, K. (1969). Disproportionate dental anxiety: Clinical and nosological consider- ations. Acta Odontologica Scandinavica, 28, 191-2 12.
Neverlien, P.O. (1990). Assessment of a single item Dental Anxiety Question. Acfa Odontologica Scandinavica, 48,365-369.
Paulonen, S.V., & Jackson, D.N. (1985). The validity of formal and informal personality assessments. Journal of Research in Personality, 19, 33 1-342.
Roskam, EE Ch. I. (1975). A documentation of MINISSA (N), Report 75. Nijmegen: Katholieke Universiteit Nijmegen.
Rouse, RA., & Hamilton, M.A. (1 990). Dentists’ technical competence, communication and personal- ity as predictors of dental patient anxiety. Journal of Behavioral Medicine, 13,307-3 19.
Schuurs, A.H.B. (1981). Factors associated with regularity of dental attendance. Unpublished doctoral dissertation, Amsterdam, ACTA.
Schuurs, A.H.B., Duivenvoorden, H.J., Thoden van Velzen, S.K., & Verhage, F. (1984). Dental anxiety, the parental family and regularity of dental attendance. Community Dentistry and Oral Epidemiol-
Schuurs, A.H.B., Duivenvoorden, H.J., Thoden van Velzen, S.K., Verhage, F., Makkes, P., & Eijkman, M.A.J. (1 985). Dimensionality of dental anxiety measurements. Community Dentistry and Oral Epidemiology, 13, 152-155.
Schwarzer, R., Ploeg, H.M. van der, & Spielberger, C.D. (Eds.) (1987). Advances in Test Anxiety Research. (Vol. 5 ) Lisse: Swets and Zeitlinger.
Seeman, K , & Molin, C. (1976). Psychopathology, feelings of confinement and helplessness in the dental chair, and relationship to the dentist in patients with disproportionate dental anxiety (DDA). Acta Psychiatrica Scandinavica, 54, 8 1-9 1.
Spielberger C.D. (1972). Conceptual and methodological issues in anxiety research. In C.D. Spielberger (Ed.), Anxiety, current trends in theory andresearch Vol. II(pp. 48 1-493). New York Academic Press.
Stouthard, M.E.A. (1 986). Corah’s Dental Anxiety Scale. Unpublished report. Amsterdam: ACTA.
Nederland [Documentation of tests and test research in the Netherlands]. Assen: Van Gorcum.
626-634.
Journal of the American Dental Associaton, 86,842-848.
dental fear survey. Journal of the American Dental Association, 108, 59-6 1.
986-989.
O ~ Y , 12,89-95. Dow
nloa
ded
by [
UV
A U
nive
rsite
itsbi
blio
thee
k SZ
] at
06:
52 1
2 Ju
ne 2
015

104 M. E. A. STOUTHARD et al.
Stouthard, M.E.A. (1989). Angst voor de tandheefhndige behandefing [Dental anxiety]. Unpublished
Stouthard, M.E.A. (1990). Voorlopige handleidingbddeATB [Manual of the DAI]. Amsterdam: ACTA. Stouthard, M.E.A., Groen, H., & Mellenbergh, G.J. (1992). Constructing a shortened version of the
Stouthard, M.E.A., & Hoogstraten, J. (1 987). Fears associated with twelve dental situations. Journal of
Stouthard, M.E.A., & Hoogstraten, Joh. (1990). Prevalence of dental anxiety in the Netherlands.
Tullman, G.M., Tullman, M.J., Rogers, B.J., & Rosen, J.B. (1 979). Anxiety in dental patients: A study of
doctoral dissertation, Amsterdam, ACTA.
Dental Anxiety Inventory. (Manuscript submitted for publication).
DentdResearch, 66,1175-1 178.
Community Dentistry and Oral Epidemiology, 18, 139-142.
three phases of state anxiety in three treatment groups. Psychological Reports, 45,407-4 12.
Author’s Note The DAI and SDAI were translated in six different languages (English, German, French, Spanish, Italian and Norwegian) in order to enable an international and crosscultural comparison. Publications of the results of some translations are in preparation, whereas research with others is in progress. Requests for reprints of these translations will be honoured.
Dow
nloa
ded
by [
UV
A U
nive
rsite
itsbi
blio
thee
k SZ
] at
06:
52 1
2 Ju
ne 2
015

DENTAL ANXIETY: A FACET APPROACH 105
Dental Anxiety Inventory - short form (DM.EA Stouthard, ACTA
APPENDIX
SDAI
Instructions This questionnaire consists of nine statements that are related to the dentist. Would you please indicate for each statement to what extent it applies to you personally? You may not have been in the given situation before. In that case, please try to imagine the situation as best as you can and indicate *hat your reaction would be. Indicate for each statement the number belonging to the answer which matches your feelings best.
1--2---3 -I-I 4-- 5 totally hardly Partly quite completely untrue true true true true
1.
2.
3.
4.
5.
6.
7.
8.
9.
I become nervous when the dentist invites me to sit down in the chair. When I know the dentist is going to extract a tooth I am already afraid in the waiting room. When I think of tKe sound of the drilling machine on my way to the dentist, I would rather go back. I want to walk out of the waiting room the moment I think the dentist will not explain what s h e is going to do in my mouth. As soon as the dentist gets hidher needle ready for the anaesthetic, I shut my eyes tight. In the waiting room, I sweat or freeze when I think of sitting down in the dentist’s chair. On my way to the dentist, I get anxious at the thought that s h e will have to drill. When I am sitting in the dentist’s chair not knowing what is going on in my mouth, I break in a cold sweat. On my way to the dentist, the idea of being in the chair already makes me nervous.
1 -2-3--65
1-2-3-4-5
1--2-3--4-5
1-2-3-4-5
1 ---2-3-65
1 --2-3-4-5
1 --2--3--4--5
1 ---2-3-4-5
1--2-3---4-5
Dow
nloa
ded
by [
UV
A U
nive
rsite
itsbi
blio
thee
k SZ
] at
06:
52 1
2 Ju
ne 2
015





























