Embed Size (px)
Citation preview
Availability, Affordability and Pricing of the Essential
Drugs: A Case Study of Bathinda City (Punjab)
Dissertation submitted to the Central University of Punjab
For the award of
Master of Philosophy
In
Economic Studies
By
Indu Bala
Supervisor
Dr. Sandeep Kaur Bhatia
Centre for Economic Studies
School of Social Science
Central University of Punjab, Bathinda
August, 2016

i
ABSTRACT
Availability, Affordability and Pricing of the Essential Drugs: A Case Study of
Bathinda city (Punjab)
Name of Student : Indu Bala
Registration Number : CUPB/MPH/SSS/CES/2014-2015/04
Degree for which submitted : Master of Philosophy
Name of Supervisor : Dr. Sandeep Kaur Bhatia
Centre : Centre for Economic Studies
School of Studies : School of Social Sciences
Key words : Drugs, Availability, Affordability, Prices
Differences, International Comparison of
Drugs Prices, Drug Price Control, Patent.
In recent times individual spending on health care is the common issue. This issue is
manifold as linked with the availability, affordability and pricing of drugs. The present
study evaluates these issues related to essential drugs in Bathinda city which is one
of the blocks of Malwa region. Availability, affordability and price differences are
examined across two types of drugs generic and, branded-generic at public and
private drug stores, using a primary survey of patients, drug retailers and wholesalers
mainly. The study also analyses the evolution of government drug pricing policies and
the impact of patents on drugs. Data on drug prices is collected of commonly used
essential drugs of different therapeutic classes. Affordability of the essential
medicines to the ordinary people is measured by comparing the treatment cost with
the wages earned by them. To compare the domestic prices with international
reference prices, median price ratios (MPR) are obtained by dividing the local public
and private sector median prices with international reference prices. The study
discovers that availability of essential drugs in the public sector is not sufficient to
meet the challenge of providing essential drugs to the entire population of the city.
The Private sector is dominating for providing drugs and better treatment which has
very less transparency in the pricing system and variations in the retail prices and
markups are very high. Affordability level of essential drugs for different treatments to
ii
the ordinary people is satisfactory but not for the people living below the poverty line.
Policies should be targeted to maintain a transparent pricing system and should be
affordable for all as well as making them more widely available. The drug price control
order should be properly implemented in fixing the MRP of branded-generic drugs.
(Indu Bala) (Dr. Sandeep Kaur Bhatia)
iii
ACKNOWLEDGEMENTS
First of all, I offer my humble thanks with folded hands and bowed head to the
almighty for his grace, kindness and blessing that gave me patience and motivation
during the course of my work.
I have the great honor to express my deep sense of gratitude and indebtedness to
my supervisor, Dr. Sandeep Kaur Bhatia, Assistant Professor, Center for Economic
studies, Central University of Punjab for her constant guidance, constant
encouragement, healthy criticism and generosity shown throughout the period of my
study and preparation of this manuscript.
I would like to give my special thanks to COC Dr. P.K Mishra, Dr. Naresh Singla, Dr.
J. K Parida, Centre for Economic Studies for their valuable suggestions pleasant
atmosphere of knowledge. I would also like to thanks Dr. R.K. Kohli, present Vice-
Chancellor of the university, Prof. Dr. P. Ramarao, Dean of academic affairs and Prof
A. K. Jain. Without their constant help, support and encouragement, this dissertation
would not have been possible.
I got immense pleasure to express my thanks to all my friends Jashanpreet Kaur
Jagdeep Kaur, Poonam Rani, Arif Gulzar Hajam, Zahoor Ahmad Paray, Harmeet
Kaur, Harpreet Kaur, Gagandeep Kaur, Sareena Goel for always supporting and
believing in me with enormous affection and valuable suggestions.
Finally, my family has supported and helped me along the course of this dissertation
by giving encouragement and providing the moral and emotional support I needed to
complete my dissertation. To them, I am eternally grateful.
Indu Bala
iv
Table of Contents
Sr. No. Contents Page No.
1 Chapter 1: Introduction 1-8
2 Chapter 2: Literature Review 9-18
3 Chapter 3: Data and Methodology 19-24
4 Chapter4: Availability, Affordability and Prices
Differences of Essential Drugs
25-55
5 Chapter 5: Evaluation of Indian Drug Pricing Policies
and TRIPS
56-67
6 Chapter 6: Conclusion 68-76
7 Bibliography 77-83
v
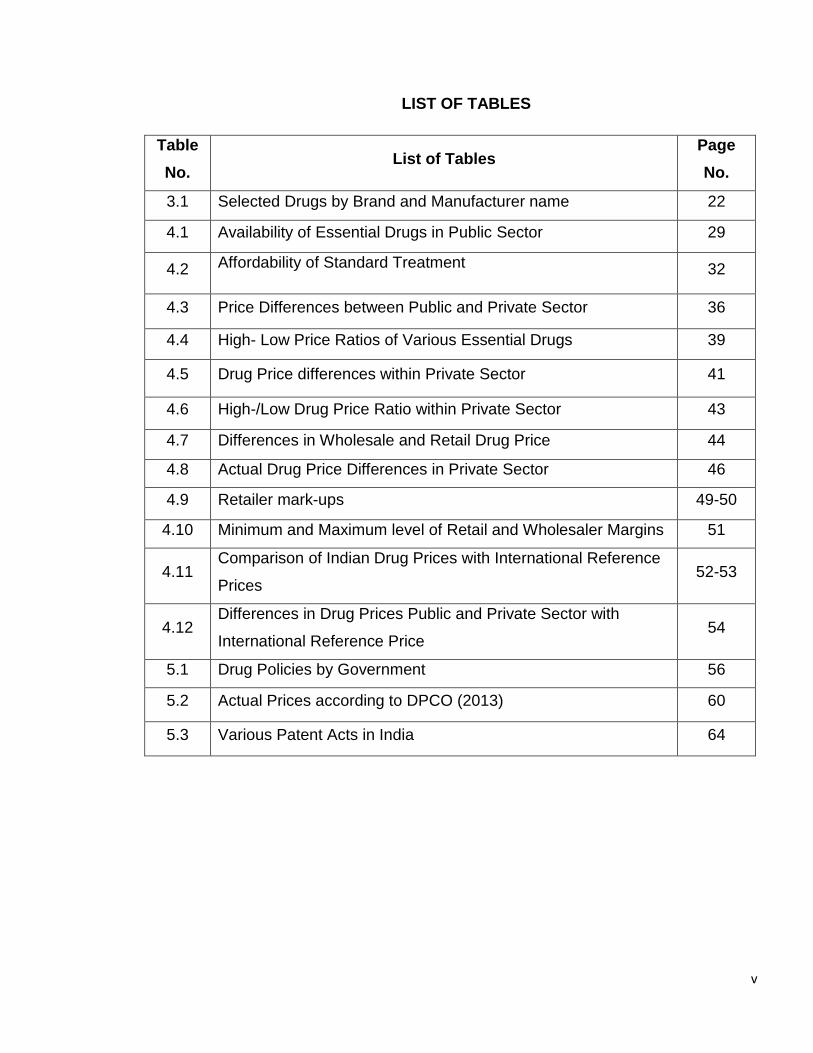
LIST OF TABLES
Table
No. List of Tables
Page
No.
3.1 Selected Drugs by Brand and Manufacturer name 22
4.1 Availability of Essential Drugs in Public Sector 29
4.2 Affordability of Standard Treatment 32
4.3 Price Differences between Public and Private Sector 36
4.4 High- Low Price Ratios of Various Essential Drugs 39
4.5 Drug Price differences within Private Sector 41
4.6 High-/Low Drug Price Ratio within Private Sector 43
4.7 Differences in Wholesale and Retail Drug Price 44
4.8 Actual Drug Price Differences in Private Sector 46
4.9 Retailer mark-ups 49-50
4.10 Minimum and Maximum level of Retail and Wholesaler Margins 51
4.11 Comparison of Indian Drug Prices with International Reference
Prices 52-53
4.12 Differences in Drug Prices Public and Private Sector with
International Reference Price 54
5.1 Drug Policies by Government 56
5.2 Actual Prices according to DPCO (2013) 60
5.3 Various Patent Acts in India 64
vi
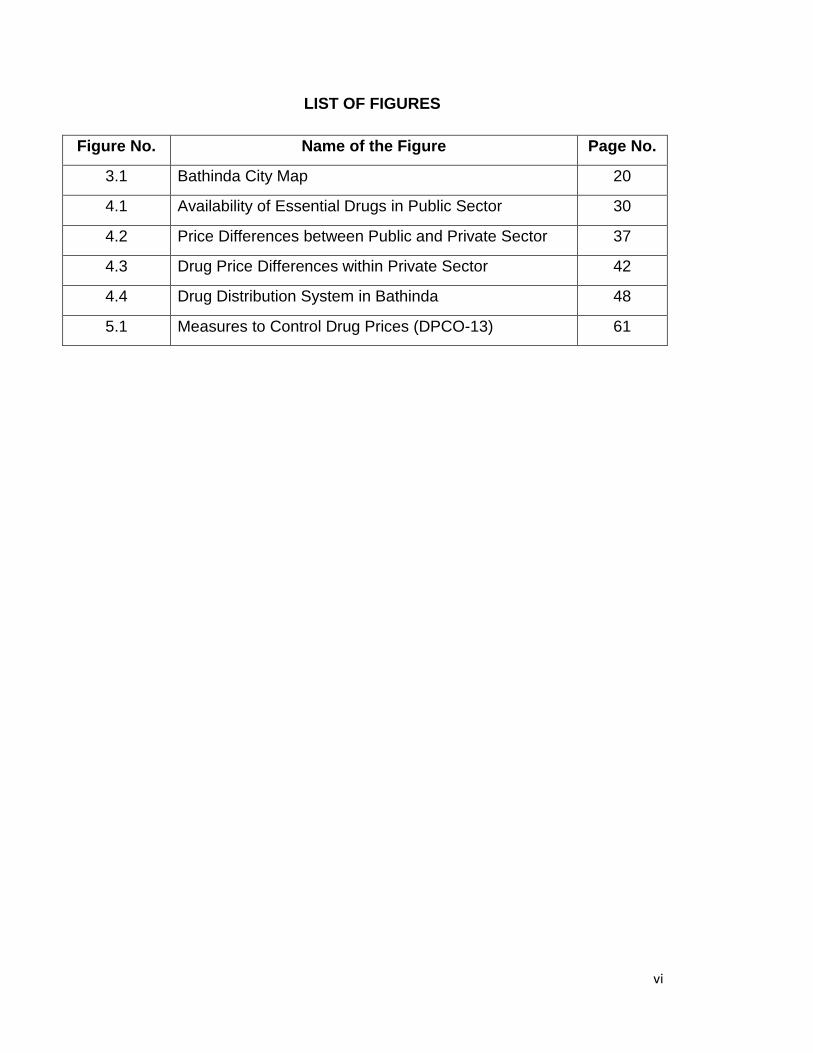
LIST OF FIGURES
Figure No. Name of the Figure Page No.
3.1 Bathinda City Map 20
4.1 Availability of Essential Drugs in Public Sector 30
4.2 Price Differences between Public and Private Sector 37
4.3 Drug Price Differences within Private Sector 42
4.4 Drug Distribution System in Bathinda 48
5.1 Measures to Control Drug Prices (DPCO-13) 61
vii
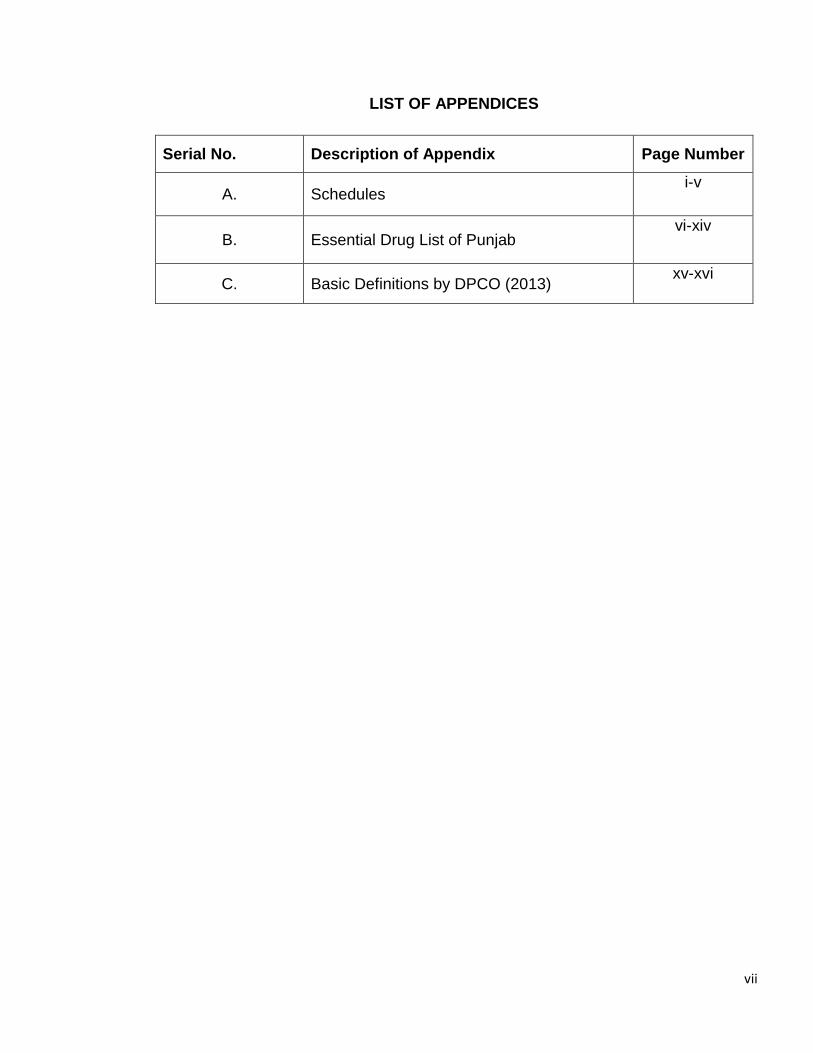
LIST OF APPENDICES
Serial No. Description of Appendix Page Number
A. Schedules i-v
B. Essential Drug List of Punjab vi-xiv
C. Basic Definitions by DPCO (2013) xv-xvi
viii
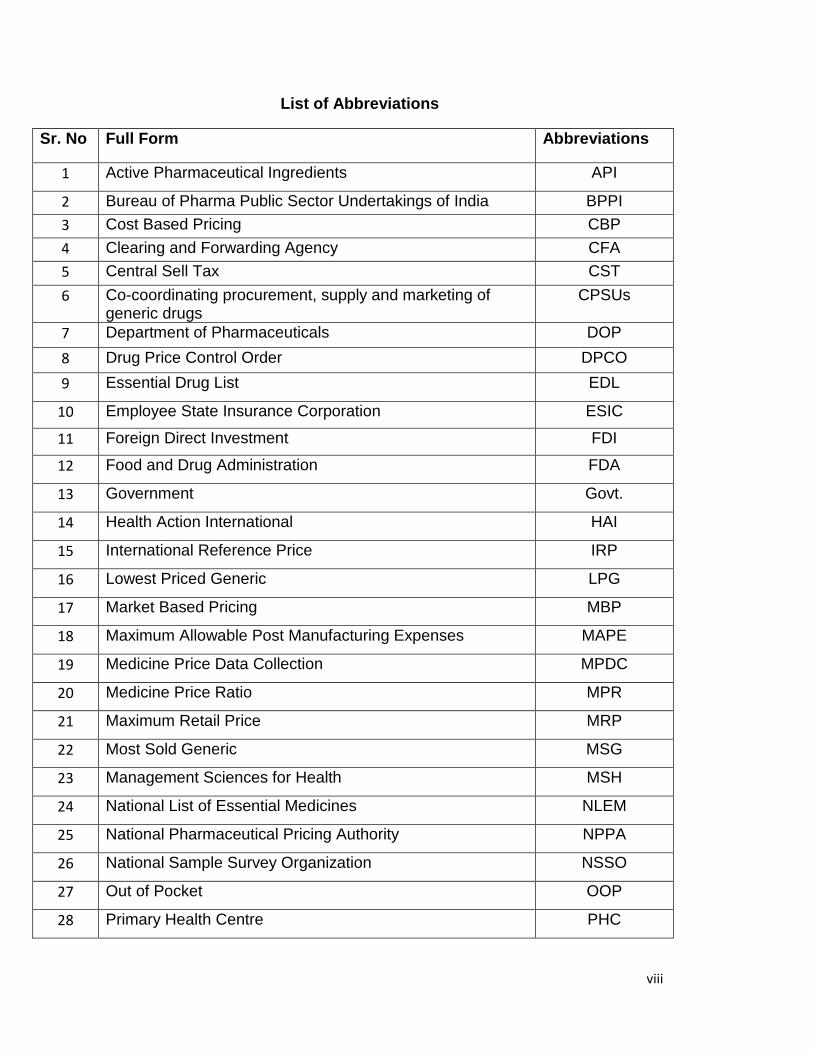
List of Abbreviations
Sr. No Full Form Abbreviations
1 Active Pharmaceutical Ingredients API
2 Bureau of Pharma Public Sector Undertakings of India BPPI
3 Cost Based Pricing CBP
4 Clearing and Forwarding Agency CFA
5 Central Sell Tax CST
6 Co-coordinating procurement, supply and marketing of generic drugs
CPSUs
7 Department of Pharmaceuticals DOP
8 Drug Price Control Order DPCO
9 Essential Drug List EDL
10 Employee State Insurance Corporation ESIC
11 Foreign Direct Investment FDI
12 Food and Drug Administration FDA
13 Government Govt.
14 Health Action International HAI
15 International Reference Price IRP
16 Lowest Priced Generic LPG
17 Market Based Pricing MBP
18 Maximum Allowable Post Manufacturing Expenses MAPE
19 Medicine Price Data Collection MPDC
20 Medicine Price Ratio MPR
21 Maximum Retail Price MRP
22 Most Sold Generic MSG
23 Management Sciences for Health MSH
24 National List of Essential Medicines NLEM
25 National Pharmaceutical Pricing Authority NPPA
26 National Sample Survey Organization NSSO
27 Out of Pocket OOP
28 Primary Health Centre PHC
ix
29 Price to Retailor PTR
30 Price to Patient PPP
31 Research And Development R&D
32 Trade Related Intellectual Property Rights TRIPS
33 Value Added Tax VAT
34 World Health Organization WHO
35 World Trade Organization WTO
1
CHAPTER - 1
INTRODUCTION
The large population in developing countries has been suffering from the health care
burden due to malnutrition, non-availability of facilities and lesser budget proposals
for health care in these countries. Indian Health Care Outlook (2015) reveals that in
developing countries, households usually have to purchase drugs and other health
facilities ‘Out of Pocket’ (OOP). The Indian health care system is also highly
dependent on personal spending as India is one of the world’s highest out-of-pocket
spending nations because of low government’s expenditures for health creating a
burden on patients and their families. World Health Organization (WHO) data reveals
that in 2012 only 33 percent of Indian health care expenditure originated from
government sources while remaining 86 percent was from private (Deloitte United
States, 2016).
Surveys conducted in six states during 2004–2005 sites involved Chennai (southern
India), Haryana (northern India), Karnataka (southern India), West Bengal (eastern
India), and two surveys sites in Maharashtra State (western India) through “World
Health Organization/ Health Action International” (WHO/HAI) a standardized
methodology exposes poor availability of drugs in public sector hospitals as only up
to 30 per cent . Therefore, low-income patients are enforced to buy more expensive
drugs from private sources or simply go without treatment. The main barrier to access
essential drugs makes health care unaffordable one is the low public sector
expenditure and other high medicine prices. In order to ensure availability at
reasonable prices, the Government of India (Ministry of Chemicals and Fertilizers)
has established an independent body of experts the National Pharmaceutical Pricing
Authority (NPPA) in 1997 which have the primary function of price determination,
revision, and related activities, such as updating the list of medicines under price
control by the inclusion and exclusion of drugs on the basis of established criteria and
guidelines. However, the NPPA monitors the prices of medicines sold in all sectors,
but still there are issues regarding the prices of drug (Kotwani et al., 2007).
2
Economic Health Care Scenario of Punjab State
According to a study by Chaudhuri (2012) examines that hospitalization and
outpatient services at public health facilities are quite low in Haryana (30 percent) and
in Punjab 20 percent. The specified reasons are the high cost of care including high
prices of drugs. In the Punjab, State the Health Systems Corporation includes public
hospitals and public clinics over which the poor people can access health facilities.
Two schemes were announced in 2008, to decrease out-of-pocket expenses for poor
families i.e. ‘Jan Aushadhi’ to provide inexpensive generic drugs through public health
care centers and ‘Rashtriya Swasthya Bima Yojna’ under which a family of five below
the poverty line would receive the cashless treatment maximum 30,000 annually.
PGRC Eighth Report (2013) viewed that health indicators in Punjab are slightly better
than many other states. It ranks third in the country in terms of birth rate (16.2 per
1000 population). The infant mortality rate of 30 per 1000 live births places it at fifth
rank. It has a maternal mortality ratio of 172 per 100,000 live births. Around 61
percent of deliveries are conducted in health institutions; the share of government and
private institutions stands at 22 percent and 39 percent respectively. A major concern
is the rising cost of medical care. The average expenditure for hospitalization in
Punjab is Rs. 15,431 which is one among the highest across the country. Even in
government health institutions, average out-of-pocket expenditure is Rs. 270/- per
OPD consultation and Rs. 7,700/- per hospitalization. User charges, inadequate
supply of medicines and other surgical supplies and lab reagents has led to an
escalation in the cost of medical care in government health institutions. The state
does not allocate adequate budget for medicines and supplies. At least 20 percent of
the health budget should be allocated for medical and surgical supplies. Clearly,
decreasing outlay on social sectors is responsible for a cut on soft items in the budget
such as medicines. A survey conducted by National Sample Survey Organization
(NSSO) in the first half of 2014, concluded that Punjab ranks top in terms of out-of-
pocket health expenditure because the people of Punjab spend a major portion of the
money income on medical treatment in the country. The out-of-pocket health
expenditure is any direct expenditure by households on drugs and health services
practitioners. It is a part of private health expenditure. According to head of School of
3
Public Health (PGIMER), people of Punjab bear the highest medical expenditure (in
terms of hospitalization), and in the area-wise break-up, the out-of-pocket health
expenditure in urban areas is Rs 29, 971 as compared to Rs 27,718 in rural areas of
the state. On an average in the Punjab state the expenditure of hospitalized per
person, Rs 28,539. In Haryana, Rs 24,000 against the national average of Rs 18,628.
Among union territories, Delhi and Chandigarh spend the highest with 34,604 and
34,658, respectively.
National Health Profile (2015) briefs Punjab’s per capita spending on health is Rs 728
and monthly per capita household out-of-pocket expenditure in the state is Rs 196.5.
In Haryana, it is Rs 131, Rs 95 in Jammu and Kashmir, Rs 134.5 in Himachal
Pradesh, Rs 103 in Chandigarh and Rs 132 in the national capital. The reason found
by experts of health expenditure burdens on common people that the lack of public
(government) expenditure. Punjab’s per capita spending on health is just Rs 728.The
state government is expensed on health are just 0.72 per cent of the gross state
domestic product. This profile of Punjab state shows the higher burden of health care
as compared to other states. (Bharti, 2016).
Role of Generic Drugs
India Pharmaceuticals position is well-known as ‘branded’ and ‘branded-generic and
most of the products are sold by a brand (trade) name. Till January 2005 all
medicines were the generic product when patents were not relevant in India. Branded
medicines were manufactured by multinational and good reputated manufacturers of
Indian. Branded medicines are promoted by manufacturers at higher prices while
almost all drugs easily available with trade-names. The public sector acquires drugs
as unbranded generics with the chemical or ‘International Nonproprietary Name’ on
the labeled product. The Indian pharmaceutical sector is communal under the
‘Ministries of Health and Family Welfare’ (Department of Chemicals and
Petrochemicals under the Ministry of Chemicals and Fertilizers) and the ‘Office of
Drugs Controller’. The government’s main thrust of pharmaceutical policies has been
on the manufacturing of the private sector and marketing of drugs and for the
common man there are not more improvements in accessibility of essential
medicines. The Indian health sector has been affected by structural adjustment,
4
economic liberalization reforms by the World Bank and increasing production cost in
pharmaceuticals (Roy et al., 2012).
Due to the high economic pressure on drug budgets the use of generic drugs is
progressively growing internationally because since they are usually substantially
lower in price than the innovative brands and these drugs provide the opportunity for
major savings in health care expenditure. However, physicians are apprehensive
regarding the quality of generic drugs and have concerns about their reliability as well
as interchange of certain drug categories. Although the generic medicines are bio-
equivalents of their innovator counterparts and are produced in similar facilities,
according to good manufacturing practices, these are widely believed as inferior in
their therapeutic efficacy and quality to branded products. Marketing practices
adopted by manufacturers of imported branded medicines also propagate the belief
that generics are inferior quality as reported from countries in Central and Eastern
Europe and independent countries emerged from the former Soviet Union. In India,
generic substitution is legally not allowed because of limited awareness about
generics to patents, and patients do not want pharmacist to change the trade name
written by doctor. Hence, consumer awareness for the generics, variety of trade
names available in the market and price variation is very limited. (Singal et al., 2011).
In developing countries, policymakers are confronted to increase the availability and
affordability of essential medicines. The government of India recently opened
‘Generic Drug Stores’ to make access to drugs, at some public channels of drug
distribution who sell generic drugs produced by the public sector. Their prices are
lower than market price. India also faces the task of equal access to affordable and
quality essential drugs for its own people despite pharmaceutical industry growth in
the last two decades, access to essential drugs remnants an issue of common
people. As for the poor population affordability remains to be the main barrier to
access to medicines. In April 2008, the ‘Department of Pharmaceuticals’ (DOP) under
the ‘Chairmanship of Minister of Chemicals and Fertilizer’ responsible for drug policy
and pricing launched a campaign to open generic drug stores called ‘Jan Aushadhi
stores’. Quality generic drugs are to be available at lower prices in these stores.
Opening generic drug stores and making essential medicines available at affordable
5
prices seems to be a step in the right direction. So far implementation of the policy
raises several concerns related to low availability (Kotwani, 2010).
Various drug policies are approved from time to time to manage the task of sustaining
balance between pharmaceutical, industrial growth and ensuring affordable and
reasonably priced medicines to the consumers at the same time, particularly the poor
common people. In India firstly control over the price of drugs was the outcome of the
Chinese aggression with the promulgation of the ‘Drugs Display of Prices Order’
(1962) and the Drugs Control of Prices Order, 1963. These were circulated under the
Act ‘Defenses of India’. With these orders, the prices of drugs were fixed from 1st
April, 1963. Consequently, arrangement of price control systems was notified through
various orders with different principles, in which the span of regulator of prices as well
as the nature of control of prices varied from order to order as per the respective drug
policies.
The latest Drug Price Control Order (DPCO-2013) was issued on 15.05.2013. All the
previous DPCOs, 1970, 1979, 1987 and 1995 were based on cost to manufacturers
with allowance for post manufacturing expenses. As per the provisions of DPCO
(2013) ceiling prices are now being fixed at the average retail price of the medicine,
produced by all those companies engaged in its production with a market share of ≥
1percent of the total market turnover, and adding 16percent margin to the
retailer. While most of the ‘Drug Pricing Policies’ in the past have been implemented
in light of various objectives, the 2012 National Pharmaceutical Policy is aimed mainly
at making drugs affordable. The main objective of the policy is to put in place a
regulatory basis to ensure the availability of essential drugs listed in the NLEM at
affordable prices (Arthapedia, 2016).
Availability and affordability of drugs is greatly affected by Intellectual Property Rights
(IPR) i.e. of India Patents Act (1970) and Amendments (2005). It has generated a
solid impression on the modern day life. These IPRs were encouraged in an ever
seen manner by the TRIPs agreement. The TRIPs agreement has directed its
member states to implement the requirements of the agreement in order to
encourage and protect IPRs. Members’ states are asked to provide protection to
different IPRs by making necessary amendments in their existing laws or enacting
6
new laws. India, being a member state of the TRIPs agreement brought changes in
its IPRs laws. The preceding fifteen years have seen many new IPR performances.
With globalization, liberalization and privatization, the field of IPR has grown multifold
and its importance has amplified, having a profound impact on commercial welfares
(Malik, 2013).
Although government increasing expending on public health facilities and managing
the drug prices polices to make drugs affordable, but the conditions of the health care
burden are not improving. A large part of the population depends upon the private
sector for heath treatment because of facilities available to patients, but the treatment
costs are mostly uncompromising for the ordinary people. As Indian’s generic drugs
are famous and demanded all over the world because of cheap prices. India can
achieve the highest level to provide availability of drugs for any health problem and
make them affordable to all.
Significance of the study
It is a matter of high concern that high prices of drugs directly make drugs beyond the
reach of million people in developing countries. Large numbers of the population in
India also do not have regular access to essential medicines. According to the
‘National Pharmaceutical Pricing Policy’ (NPPP) 2012 Indian Pharmaceutical industry
is producing drugs at 3rd position of by volume and 14th in terms of value at global
level. As India is very efficient in the pharmaceutical sector to produce drugs at very
cheap cost relative to world level and provide low price in the world, despite the fact
domestic consumers suffer from the high retail price of very cheap drugs. Commonly,
individuals have to bear the full cost of their drugs and health treatment, since drugs
are not fully subsidized through Indian government. To overcome this economic
burden of drugs the use of generic drugs is a good substitute but, consumer’s
awareness for the generics, variety of trade names available in the market, and price
variation is very limited. Hence, there is need to conduct a study that can analyze the
uses and price structure of pharma products manufactured in India. The study has
purposively selected Bathinda city situated in the Malwa region of Punjab, where the
health problem has major concern. High prices and price differences in the private
7
sector and low availability in the public sector are major barriers to the use of drugs
and better health. High prices of drugs is one of the issue, while as issues related to
the price differences within the same sector is another one. By keeping in view, the
present study is an attempt to discuss various issues related to h availability and
affordability of essential drugs Therefore the study has tried to examine the gap in
cost, wholesale, retail price and profit margin at different levels of distribution of drugs
from a manufacture unit to consumers of commonly demanded drugs in Bathinda city.
An attempt is also made to study the evaluation of drug policy and the impact of
TRIPS on drug prices. Therefore, keeping in view the above literature gap, the
present study attempts to carry out the following objectives to contribute the literature
and provide further knowledge about the subject.
Objectives of the Study
To evaluate the availability and affordability of essential drugs in a Bathinda
city.
To calculate the differences in drug prices at various stages of distribution in
different sectors i.e. public and private.
To evaluate the various Indian Drug Pricing Policies and TRIPS.
To give some policy suggestions for a sustainable and affordable health care
system.
Plan of the Present Study
The present study is scheduled into six chapters as:
The first chapter deals with the introduction about the problems related to the
essential drugs, health status of India and Punjab. Discussion about role of generic
drugs in the health care is also given. Objectives and significance of the present study
are explained.
The second chapter deals with a review of various studies related to the subject
matter of the study, which helps to deal with the research problem. By reviewing the
literature the research gap also given in this chapter.
8
The third chapter consists with the data and methodology used for analyzing the
objectives. In other words, it demonstrates source of data and different indices used
to know the facts related to different objectives of the study.
The fourth chapter deals with the analysis of the collected data related to the
availability, affordability, price differences and different markups of common essential
drugs. The international price comparisons are also taken into account.
The fifth chapter describes the evaluation of Indian drug price policies and current
drug price control order in detail also the impact of TRIPS on Indian pharmaceuticals.
The sixth chapter is an attempt to summarize the findings of the study. It also
includes some possible suggestions for policy building to access essential drugs for
ordinary people, stabilize the prices and to promote the generic affordable drugs.
9
CHAPTER - 2
LITERATURE REVIEW
The purpose of reviewing the literature is to study an overview of important literature
published on the subject of the study. Several studies have examined the Indian
pharmaceutical industry as per the availability of drugs, price differences and in a
different way as price mechanism, differences, and cost of production. In this context
an attempt has been made to review the related studies in a systematic order. First
section relates to availability, affordability and differences in drug prices and various
issues of usage of generic drugs in India. The second section deals with studies
related to drug control pricing policies and impacts of TRIPS.
Section I
Godwin and Varatharajan (2002) works on, differences in drug price across different
retail market settings in Thiruvananthapuram district of Kerala. The study determined
retail markup of 12 commonly used branded drugs with charged high drug prices is
estimated to capture the variability in mark-up across five different drug stores as
Government-owned drug stores, Private drug stores in a competitive setting, Society-
owned drug stores, Private drug stores in spatial monopoly setting, and Private drug
stores within hospitals. The sample was used as twelve Generic Name Paracetamol
,Ampicilin , Amoxycilin Mox, Ranitidine Rantac, Cetrizine Zetzine, Alprazolan Alprax ,
Penicillin G Voveran ,Atenolol Aten,Glyben Glamade Daoni,.Enaprel Envas,
Ciprofloxacilin. The results of study show there exists 32 percent price differential of
between different retail drug stores retailing the similar brand of the same drug; the
difference is huge as 120 percent of Amoxycilin. High difference in retail prices
attributable to the built-in markup in the MRP. However, retail margins in India are
estimated as near 32.7 percent (WHO/WTO, 2001). Studies also described a
difference of 150-200 percent between wholesale and retail prices. The formal and
informal factors as, Wholesale and retail markups, Import duties and taxes, can
double the price of a drug between manufacturers and consumer.
10
Kotwani (2003) works a report of medicine prices, availability, and affordability in the
state of Rajasthan on the basis of standardized methodology published by WHO/HAI
to analyses components of prices of a basket of essential medicines in the public,
private-for-profit and co-operative sectors. The results show that the government of
Rajasthan purchases medicines at a reasonable price for patients who are eligible for
free medicines at public health facilities. Almost half of medicines surveyed were
priced less than twice the international reference prices in private pharmacies. The
medicines such as albendazole, diazepam, diclofenace, amoxicilline, atenolol,
paracetamol, and hydrochlorothizide were expensive in the private sector. The prices
of albendazole, diazepam and diclofenac in the private was 8, 26 and 14 times the
procurement price in the public sector, including wholesale and retail margins are
very high or the manufacture prices are higher in the private sector than the public
sector. In case of public sector availability was low, so poor patients sometimes go
without treatment or buy medicines from private pharmacies forcefully. The availability
of medicines to treat HIV/AIDS was very low in all sectors.
Singal et al., (2011) examine the comparison between the quality and price of
generic (branded-generic) drug to their costly popular brand (branded) manufactured
by the same pharmaceutical company in India. The study considered materials and
methods on five medicines: alprazolam, cetirizine, ciprofloxacin, fluoxetine, and
pantoprazole which are commonly used and manufactured in branded and branded-
generic versions of the same company were selected. Price-to-patient and price-to-
retailers were found for five “pair” of medicines with results that retailer margin for
five branded medicines were in the range of 25-30percent, but for their branded-
generics version manufactured by the same company it was in the range of 201-1016
percent and price-to-patient for the branded version of cetirizine, fluoxetine,
ciprofloxacin, lansoprazole, and alprozolam was higher by 41percent, 33 percent, 20
percent, 14 percent, and 31percent than branded-generic. The study concludes that
the difference in price-to-patient was not as huge as it is expected for generics, but
the margins for retailer were very high for branded-generics. Quality of branded-
generics is same as for their branded version. It is suggested that there is a need to
modify the drug price policy, regulate the markups in the generic supply chain,

11
conduct and widely publicize the quality testing of generics for awareness of all
stakeholders.
Basak and Sathyanarayana (2012) depicts the evaluation of knowledge and
perceptions about generic medicines in community pharmacists' and drug retailers' in
two towns of Tamil Nadu, India, through a cross-sectional descriptive study, with a
questionnaire method, to survey community pharmacists and drug retailers working in
39 randomly selected private pharmacies from Among 66 respondents (pharmacists
and drug retailers), 39 (59.1percent) were drug retailers; 52 (78.8percent) were self-
employed; majority in the age group 31-40 (31.8percent); and mostly males
(83.3percent). Overall, 21 respondents (31.8percent) did not have knowledge about
generic drugs and 30 percent of the respondents believed that generic drugs are of
inferior quality compared to branded drugs. Only 63.6percent of the surveyed
pharmacists and drug retailers agreed that generic drugs can be considered
therapeutically equivalent with the branded ones. The majority of the respondents
(80percent) did not support generic substitution, even in case of approved drugs are
not available. Many community pharmacists and drug retailers have misconceptions
regarding generic medicines. It is concluded that lack of knowledge may negatively
affect the community pharmacists' support towards generic medicines in India and
this issue should be addressed by academicians and other relevant bodies.
Chaudhuri (2012) examines that hospitalization and outpatient services at public
health facilities are quite low as in Haryana (30percent) and in Punjab (20percent).
The specified reasons are the high cost of care including high prices of drugs. In the
Punjab, State the Health Systems Corporation includes public hospitals and public
clinics over which the poor people can access health facilities. Two schemes were
announced in 2008, to decrease out-of-pocket expenses for poor families. These two
schemes were ‘Jan Aushadhi’ where inexpensive generic drugs were made available
through public health care centers and ‘Rashtriya Swasthya Bima Yojna’ under which
a family of five below the poverty line would receive cashless treatment maximum
30,000 annually.
12
Roy et al., (2012) analysis the medicines cost and their affordability in private
pharmacies in Delhi (India), using a method of primary survey to measure the costs of
prescribed medicines and treatment of community acquired pneumonia (CAP), with
medicines purchased from 27 private pharmacies. Measurement of affordability is
taken by making a comparison of the monthly per capita expenditure, to the costs of
treatment (medicines). The results show observed costs of prescriptions (129.37+
217.99) in the cost of treatment of community acquired pneumonia varied huge
inconsistency from Rs. 34.50 to Rs.244.75 with azithromycin and Rs.72.20 to
Rs.277.30 with levofloxacin. The study finds show that there are large variations in
the costs of medicines are and economically not affordable for the poor in India.
Reforms in ‘National Pharmaceutical Policy’ are required immediately.
Eighth Report of PGRC (2013) observes that Punjab is somewhat better in health
indicators than many other states because of third rank in terms of birth rate (16.2 per
1000 population) in the country. The infant mortality rate of 30 per 1000 live births
places it at fifth rank. It has a maternal mortality ratio of 172 per 100,000 live births.
Around 61percent of deliveries are conducted in health institutions; the share of
government and private institutions stands at 22 percent and 39 percent respectively.
A major concern is the rising cost of medical care. The average expenditure for
hospitalization in Punjab is Rs. 15,431 which is one among the highest across the
country. Even in government health institutions, average out-of-pocket expenditure is
Rs. 270/- per OPD consultation and Rs. 7,700/- per hospitalization. User charges,
inadequate supply of medicines and other surgical supplies and lab reagents has led
to an escalation in the cost of medical care in government health institutions. The
state does not allocate adequate budget for medicines and supplies. At least
20percent of the health budget should be allocated for medical and surgical supplies.
Clearly, decreasing outlay on social sectors is responsible for a cut on soft items in
the budget such as medicines.
Hinsch et al., (2014) works on improving medicines price transparency and Price
information Mechanism through data collected during the course of a WHO project
focusing on the development of a vaccine price and procurement information

13
mechanism. The project collected information from six medicine price information
mechanisms and interviewed data managers and technical experts on key aspects as
well as observed market effects of these mechanisms. These include the uptake of
high quality medicines, more favorable results from contract negotiations, changes in
national pricing policies, and the decrease of prices in certain segments for countries
participating in or deriving data from the various mechanisms. In conclusion the
reviewed mechanisms avoid the methodological challenges observed
for medicine price comparisons that only use national price databases. It is suggested
that medicine price information mechanisms respond to the need for
increased medicine price transparency and have the potential to contribute to
improved access to medicines in developing countries.
Ahmad et al., (2015) examines that nearly half of India’s population has lack of
access to essential rugs in government hospitals due to the heavy dependency of
most of the patients in the private sector in spite of India’s greater exports in drugs to
more than 200 nations consisting of more than 20,000 manufacturers and with
3rd largest market by volume in the world. The main emphasis of in Indian
pharmaceutical, health policies is to focus on the progression of the industrial sector
rather than the issues of law availability, high pricing, and less affordability of drugs.
As it is a common view that drug prices in India are comparatively low, but studies
have reported that medications in India are costly and unaffordable. The margin on
drug sales across the same generic class is extremely high, often ranging from 1000
percent to 4000 percent. Since independence the objectives of the Indian
pharmaceutical industry have remained the same as the growth of domestic industry
and manufacture qualitative drugs. In India, more than 80 percent of healthcare
expenditure is borne by patients while the income of 70 percent of Indian population
is less than 2$. The most essential medications that are needed by the majority of the
Indian population should be reviewed for inclusion in the drug price control list. There
is a large difference in the prices of different branded drugs and generics that are
selling in the market even though they might characterize the same drug fragment.
Health experts should be advised to suggest cost-effective drugs in the attention of
the patients without being influenced by pharmaceutical companies. Consumer
14
knowledge about generics could be improved through effective educational
interferences. The issue of pricing needs an all-inclusive solution generated by the
coordinated efforts of stakeholders, pharmaceutical companies, and healthcare
professionals in order to catalyze equity in access to health care.
Rana and Roy (2015) examine the issues and relevance of generic drugs which are
bioequivalent to the innovator product in terms of dosage form, strength, and route of
administration, quality, safety, performance characteristics and intended use of global
health. Generic drugs are considered as a basis for providing affordable drugs to
patients. The major generic markets in the world include United States of America
(USA) followed by European Union (EU), Canada, Japan and Australia. The major
suppliers of generic medicines in China and India are showing fabulous growth in the
generic drugs sector. There are many legal and regulatory issues along with quality
concerns associated with the use of the generic products. Lately, bilateral
international agreements called Free Trade Agreements (FTA), delaying tactics by
originator companies like strategic patenting and litigations on generic manufacturers
have been a major setback for the generic medicine industry. These issues need to
be addressed to optimize use of generic Drugs. The sustainability of generic drugs in
public sector is crucial for improving access to essential medicines to the worldwide.
Section II
Lanjouw (1997) disclose the outcomes of a field survey conducted in order to
evaluate the impact of pharmaceutical product patents in India and her main
concludes that Indian firms, profit the level of generic drug production will decrease
for as they will possibly have to pay some of royals to the original innovators. An
increase in the incentives for investment in R & D in diseases relevant to developing
countries, as well as in the formation of innovations in general. However, this may be
basically due to the fact that the strategy of imitation is no longer available, rather
than being a direct incentive effect. Another impact can be that stronger IPR would
not enlarge the R & D activity of foreign firms in India, since in multinationals
pharmaceutical R & D is a highly centralized process, where cost is not the
paramount concern.
15
Lall (2003) reviews the case for uniform and strong IPR by developing country
groupings using various procedures of domestic technology imports and innovation.
This indicates that in India, "it is possible to argue, however, that India has now
reached a stage in pharmaceutical production where stronger IPRs would induce
greater innovation by local firms the benefits of which would have to be set off against
the closure of other firms.
Hoen (2003) examine that the causes for the shortage of access to essential
medicines are diverse, but in some cases of necessary treatments where drugs are
very costly are the major barrier. Unaffordability of drug prices can be the result of
strong intellectual property protection. While TRIPS does offer safeguards to remedy
the negative effects of patent protection or patent abuse, in practice it is unclear
whether and how countries can make use of these safeguards when patents
increasingly present barriers to medicine access. Public health supporters the Doha
Declaration as an important accomplishment because it gave dominance to public
health over private intellectual property on the other hand the Doha declaration did
not solve all of the problems associated with intellectual property protection and
public health. The recent failure of the WTO to resolve the outstanding issue to
ensure production and export of generic medicines to countries that do not produce
may even indicate that the optimism felt at Doha was premature.
Dhar and Gopakumar (2006) works to specify the performance of Indian
pharmaceutical firms by interacting the changes in the patent regime required by the
Agreement on TRIPS. In Post- TRIPS period the R & D spending of some of the top
firms as Ranbaxy and Dr Reddy’s has shown an increase which results, R&D
strengths of the firms have enhanced significantly.
Mani (2006) reveals a detailed mapping out of the sectoral system of innovation of
India’s pharmaceutical industry. The study shows that the TRIPS compliance of the
intellectual property right regime has not reduced the innovation capacity of the
domestic pharmaceutical industry, which has visualized an increase in both research
budget and patenting.
16
Chaturvedi and Chataway (2006) explain in the paper that Indian firms are investing
in R & D not only for innovative drug discovery also for developing capabilities to
assimilate and exploit knowledge available outside. Indian firms are acclimatizing to
the changing environments. R & D is predictable as the ‘survival kit’ in the post-TRIPs
scenario. They are also placing themselves as a partner of choice for technology
savvy national and multinational firms.
Birla and Gupta (2007) explain that Indian firms are increasing their innovative
capacity. The Indian Pharmaceutical Industry is moving, chances in Post- TRIPS
period. The participation of Indian generic companies are also growing their
participation in the progressive markets, particularly the US. R&D growth rate is also
increasing rapidly.
Manikandan and Gitanjali (2012) review the national list of essential medicines of
India. The Ministry of Health, Government of India revised the National List of
Essential Medicines of India (NLEMI 2011) in June 2011, eight years after the last
revision. The NLEMI 2011 contains 348 medicines and was prepared over one and a
half years by 87 experts. Though there are some positive aspects of the list such as
the documentation of a detailed description of the revision process, the inclusion of
many experts from various fields in the review committee, well written description of
the essential medicines concept and others, a critical review of the list reveals areas
of major and minor concerns. Improper medicine selection like the inclusion of a
nearly obsolete medicine such as ether, an anesthetic agent; non-inclusion of
pediatric formulations; spelling errors; and errors in the strengths of formulations
diminishes the significance of the NLEMI 2011. In its present form, the NLEMI 2011
did not align with the Indian Pharmacopoeia, and the National Health Programs as
well as the National Formulary of India 2010. Formatting errors, non-inclusion of an
index page, syntax and spelling errors may also undermine the usefulness of the
NLEMI 2011 as a reference material. An urgent revision of the NLEMI 2011 is
advised so as to avert misinforming the wider international and local readers.
17
Malik (2013) revises that TRIPs was one of the most contentious issues in the
Uruguay Round of multilateral trade negotiations, concluded in 1994 at Marrakesh.
India has decided to comply with all the instruments and annexes of GATT, including
Trade Related Aspects of Intellectual Property Rights (TRIPs) as a member of the
World Trade Organization (WTO), and having signed the General Agreement on
Tariff and Trade (GATT). Because of the WTO, India has to amend its intellectual
property laws. India was forced to comply with the TRIPs agreement. After the
formation of WTO in 1995, the India is being its member has to implement the TRIPs
agreement in to. The commitment under the TRIPs agreement compelled India to
amend its intellectual property laws.
Kumar (2014) view for comparison between old and latest systems in DPCO as
DPCO act 1995 and DPCO act 2013. The new pricing guideline, DPCO has come in
to effect from May 15, 2013. In past before implementing DPCO 2013, the prices of
74 bulk drugs are controlled by DPCO 1995, but when the DPCO 2013 has come into
effect, 652 new drugs are added to the list national list of essential medicines
(NLEM). It is required that the duty of government to make the lifesaving drugs
affordable to the common man. It is suggested for the implementation of new policies
that the government has to reduce the prices of the drug which is needful for common
man, to improve the research and development of new drugs, it has to be liberal in
fining the prices in such a way that the industries cannot be suffered and it has to
support the research in the nation. It controls the market prices of the drugs and it
supports research by exempting the price control of new drugs by giving the patent up
to 5 years.
Kanwar and Hall (2014) analyses the impacts of TRIPS Patents. TRIPS which are
the Agreement on Trade Related Aspect of Intellectual Property Rights attempt the
difficult assignment of balancing private and public rights. On one hand, it protects the
interest of the pharmaceutical companies that invest heavily in R and D of Drugs and,
on the other; it allows nations that belong to the WTO to promote public health in their
respective countries. However, patents on pharmaceutical products have adversely
affected industrially developing and least developed countries, hampering their ability
18
to formulate suitable public health policies that would enable their ailing citizen to
access medicines. For instance Pharmaceutical patents have raised the cost of life
saving drugs, effectively placing them out of the reach of the mainstream of the
World’s population.
Most of the studies are found which emphasized on availability, affordability and
prices in some states of India. Studies related to price differences are very few and
explained the only difference between the retail prices in different markets. Price
differences at different stages of distribution are not done in the earlier studies in India
and none of the study found in the Punjab. Therefore, the present study is an attempt
to examine the price differences at various stages from manufacture to consumer
along with the availability and affordability in the Bathinda city of Malwa region
(Punjab) known as health sensitive.
19
CHAPTER - 3
DATABASE AND METHODOLOGY
This chapter deals with the data collection and methodology used in the present study
for analyzing the availability, affordability and price differences of essential drugs in a
Bathinda city (Punjab).
Data Base
To achieve the different objectives of the present study, the study primarily relies on
the survey of the Bathinda city with the help of WHO/HAI methodology (2003),
described in the manual entitled ‘Medicine Prices – a new approach to measurement’
which has been designed to collect data, analyze and interpret the result in a
standardized way. To understand the methodology “International Drug Price indicator
Guide 2014” published by WHO is also used. This methodology helps in the present
study for selection of health facilities, the comparison of prices at international level
and to calculate affordability, and pricing components. The secondary data sources
have been used for:
1) The collection of Global Core and regional drug drugs lists, mentioned in the
WHO/HAI manual (2003) published for international price comparison.
2) To calculate the affordability minimum wages in the government sector of
Bathinda district is collected from ‘Labour Department of Punjab’ (Statistical
Section, 2013) and poverty estimates by (Tendulkar Method, 2011-12).
Selection of Area
Bathinda city is purposefully selected for primary survey. It is located in the Malwa
region in the state of Punjab which is known as health sensitive region. It is divided
into the 4 tehsils of Bathinda, Rampura Phul, Maur and Talwandi Sabo. These tehsils
are further divided into nine Blocks of Bathinda, Sangat, Nathana, Rampura, Phul,
Balianwali, Bhagta Bhaika, and Talwandi Sabo and there are total 21 cities and towns
in this district from which first Bathinda (Municipal Corporation) is selected
20
purposively because this is the only city of Malwa region where a government drug
store is established by central government.
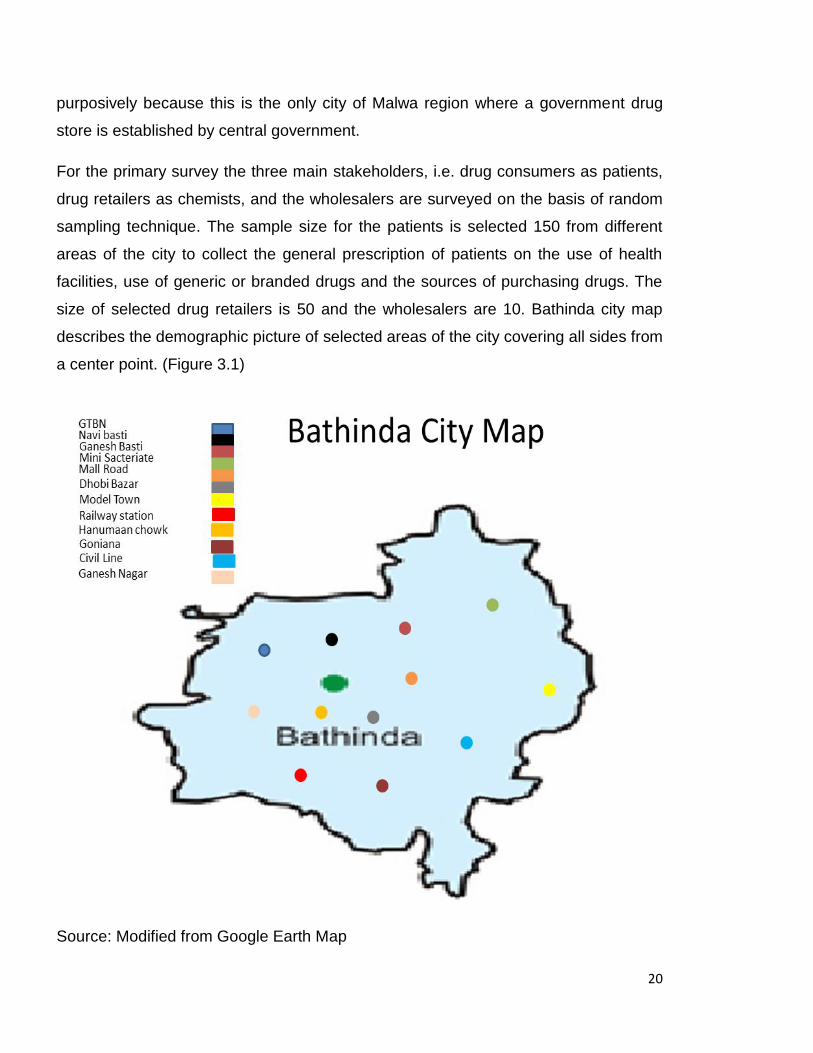
For the primary survey the three main stakeholders, i.e. drug consumers as patients,
drug retailers as chemists, and the wholesalers are surveyed on the basis of random
sampling technique. The sample size for the patients is selected 150 from different
areas of the city to collect the general prescription of patients on the use of health
facilities, use of generic or branded drugs and the sources of purchasing drugs. The
size of selected drug retailers is 50 and the wholesalers are 10. Bathinda city map
describes the demographic picture of selected areas of the city covering all sides from
a center point. (Figure 3.1)
Source: Modified from Google Earth Map
21
Two sectors are surveyed in the city for drug price comparison. The sectors are:
1) Public Sector Prices: Data for drug prices and drug availability are
collected from the public sector drug store in Bathinda city known as “Jan
Aushadhi” located in Civil Hospital Bathinda. This drug store works under a
Central government at very less price of essential medicines.
2) Private Sector Prices: Private sector drug prices are those, at which
patients pay for medicines to private retail drug stores. In this sector also
printed price, i.e. (MRP) maximum retail price is charged by retailers. So the
data on (MRP) prices in this sector are collected through printed price on the
strip.
In Public sector one drug store is available in the city “Jan Aushadhi drug” store and
profile of private drug distributors in the city is collected from the President of the
wholesalers and retailers of the Bathinda city. In private sector 50 retail drug stores
are randomly surveyed from the different areas such as retail drug stores near Civil
Hospital, Gandhi Market, Near Bus stand, Power house road, Ajit Road, Mall road,
Bibi wala road, Haji Rattan B.C.C road, Mati Das Nagar, Mini Sectriate, Guru Gobind
Singh Nagar. Famous wholesales who provide branded-generic drugs to different
private retail drug stores are also surveyed, because almost all the private retailers
buy medicines from local wholesalers and all the wholesalers provide the drugs at
the same prices to retailers.
Selection of Drugs
In the Bathinda city number of medicines are purchased from private drug stores, the
selection of medicines is very difficult on the basis of patients’ views, so the common
medicines are sorted out on the basis of views of doctors and retailors, final selection
is made by comparing these common medicines with Punjab Essential Drug List
(EDL) containing (235) name of all types of drugs including injections, (1 to 71), I.V
Fluids (72 to 82) Eye/Ear/Nasal Drops, (83 to 85), Tablets and capsules, (86 to 187),
Solution, Creams, Applications (188 to 204), Syrup/ Suspension (205 to 235) The
selected medicines are under the number (86 to 187) tablets and capsules.
(Annexure-B)
22
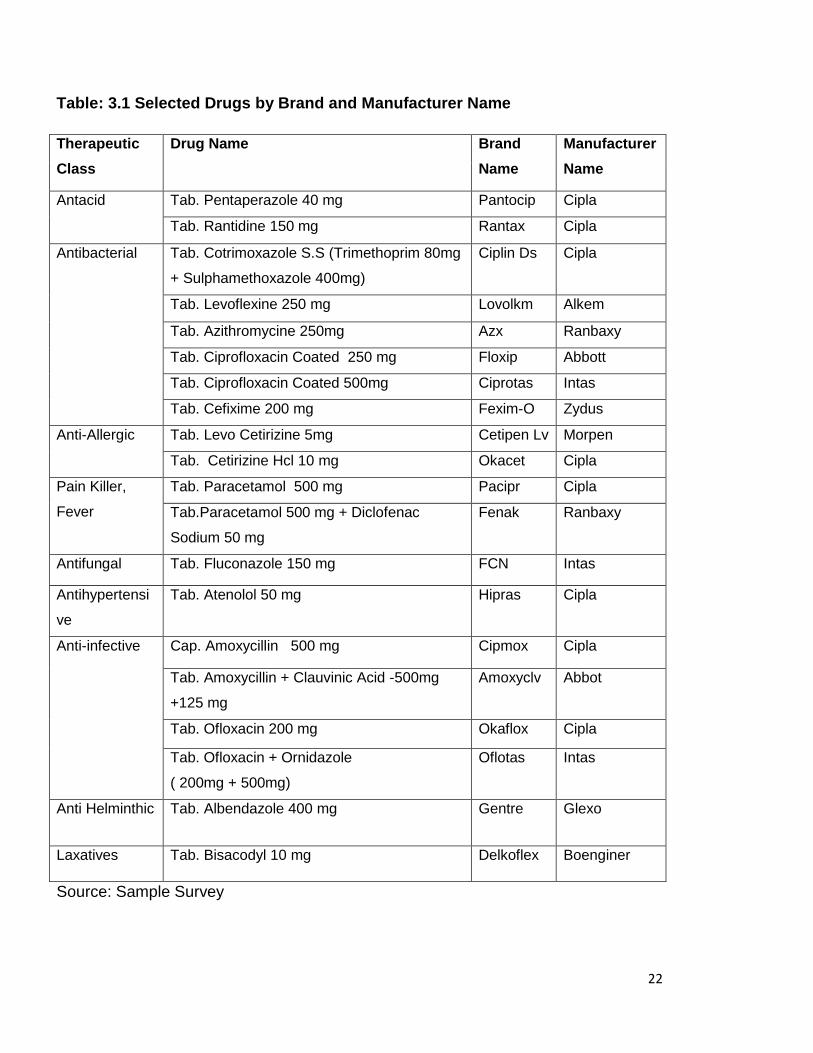
Table: 3.1 Selected Drugs by Brand and Manufacturer Name
Therapeutic
Class
Drug Name Brand
Name
Manufacturer
Name
Antacid Tab. Pentaperazole 40 mg Pantocip Cipla
Tab. Rantidine 150 mg Rantax Cipla
Antibacterial
Tab. Cotrimoxazole S.S (Trimethoprim 80mg
+ Sulphamethoxazole 400mg)
Ciplin Ds Cipla
Tab. Levoflexine 250 mg Lovolkm Alkem
Tab. Azithromycine 250mg Azx Ranbaxy
Tab. Ciprofloxacin Coated 250 mg Floxip Abbott
Tab. Ciprofloxacin Coated 500mg Ciprotas Intas
Tab. Cefixime 200 mg Fexim-O Zydus
Anti-Allergic Tab. Levo Cetirizine 5mg Cetipen Lv Morpen
Tab. Cetirizine Hcl 10 mg Okacet Cipla
Pain Killer,
Fever
Tab. Paracetamol 500 mg Pacipr Cipla
Tab.Paracetamol 500 mg + Diclofenac
Sodium 50 mg
Fenak Ranbaxy
Antifungal Tab. Fluconazole 150 mg FCN Intas
Antihypertensi
ve
Tab. Atenolol 50 mg Hipras Cipla
Anti-infective
Cap. Amoxycillin 500 mg Cipmox Cipla
Tab. Amoxycillin + Clauvinic Acid -500mg
+125 mg
Amoxyclv Abbot
Tab. Ofloxacin 200 mg Okaflox Cipla
Tab. Ofloxacin + Ornidazole
( 200mg + 500mg)
Oflotas Intas
Anti Helminthic Tab. Albendazole 400 mg Gentre Glexo
Laxatives Tab. Bisacodyl 10 mg Delkoflex Boenginer
Source: Sample Survey
23
For each drug two types of products are surveyed, generic without any brand name,
i.e. Lowest Price Generic, (LPG) and the Most Sold brand Generic (MSG). Generic
drugs with the lowest price are available in the public store. The wholesale prices are
only surveyed in the private sector because of wholesalers are the part of the drug
distribution chain in the private sector only.
In the public sector the drugs are directly supplied by center government and there is
no issue of whole and retail prices. In the private sector, which is dominating to
provide each type of drugs has many issues regarding the price differences within
sector and high markups mostly in generic-branded drugs. Thus, the brand and
manufacture name is also asked of most sold medicines to compare the different
prices and markups.
Drug Price distribution channel
With the help of the drug distribution chain in Bathinda, drug price components are
analyzed to establish that how the retail price of a medicine is determined and how
different markups and taxes are contributing in the price.
The manufacturer provides medicines to the wholesalers through Clearing and
Forwarding Agents (CFA), and central warehouse, then supplied to substockist or
wholesalers who distribute to different retail stores, lastly patients purchased from
chemists. Thus the chain internally within the city is started from wholesaler to
patients. So to find information about prices in an accurate way, wholesalers and
retailers are contacted and asked to provide information on price components of
selected medicines
Analysis of Data and Outcome Variables
Primary survey is followed by data analysis. Data collected in this study has been
analyzed through:
(i) Appropriate statistical tools are used in computerized excel, such as
averages, percentage, price ratios, sector wise unit prices, minimum and
maximum.
24
(ii) To explain the international comparison ‘Median Price Ratios’ are calculated.
These ratios are the median unit prices across the facilities surveyed in a
sector (in local currency) divided by the international reference price (also in
local currency) to compare the external standard price.
MPR= Median local unit price / Reference unit price (MSH).
The reference price serves as an external standard for evaluating local prices. WHO
and HAI recommend using the ‘Management Sciences for Health (MSH)
International Drug Price Indicator Guide 2014 as the reference source’.
Limitations of the Study
The study attempts to use the standardized methodology provided by WHO/HAI for
attaining the objectives, some guidelines of methodology cannot be satisfied.
According to WHO methodology originated brands of drugs are also surveyed, but in
the present study only commonly used brands are surveyed.
25
CHAPTER - 4
AVAILABILITY, AFFORDABILITY AND PRICING OF ESSENTIAL DRUGS
Introduction
This chapter is an attempt to examine the issues related to essential drugs, i.e.
availability, affordability and price differences, through the primary survey of Bathinda
city. The present survey is an amalgam of different respondents from various fields
suc h as doctors, druggists (wholesalers and retailers) and patients to verify and
examine the use of drugs from branded to generic and preference towards health
facilities. The present chapter is divided into two parts: first part explains the
availability and affordability of commonly used essential drugs in public and private
sector. The second part deals with the drug price differences between public and
private sectors, differences within the private sector and international price
differences i.e. international price comparison. Through prices differences, different
markups are also analyzed for reviewing the drug price policies to make them more
effective.
Overview of Respondents
The different respondents involved in the study are the first source to analyze the
issue of availability, affordability and price differences of common essential drugs by
surveying of doctors, patients and druggists in the city. Patient’s opinion towards
public sector health facilities is not adequate as the majority of the respondents about
68 percent are not interested to use the public sector health facilities and prefer to the
private sector health care facilities due to the availability of drugs and provision of
satisfactory treatment. The remaining respondents use the public facilities but not for
entire treatment and then go to private facilities because of they are not much
contented with the prevailing facilities due to low availability of drugs in the civil
hospital and then they have to purchase the drugs and health treatment from the
private sector out of pocket with a higher cost. The reason for the positive opinion
towards the private sector hospitals and drug stores instead of high cost is the
availability in a large number at any time this concludes that the majority of the
population in the city depends on private health care facilities with compensating the
26
higher cost of treatment for temporary and regular basis. Lack of knowledge of the
respondent’s about the public drug store ‘Jan Aushadhi’ for the drugs at very less
price is one of the reasons for preferring private drug stores while lack of availability
of all drugs is the second reason.
The patient’s perspective about prevailing drug prices indicates that nearly 30 percent
of the respondents are fully dissatisfied from prevailing prices of drugs, 27 percent are
somewhat satisfied, 16 percent are neutral, 22 percent are satisfied and only 7
percent are fully satisfied. It is observed that the fully satisfied respondents are with
higher income which is the main reason for not much burden of higher prices of drugs
to them and the around 30 percent respondents are dissatisfied bearing the health
care burden due to higher prices of drugs at private drug stores.
The results related to general prescription explain that patients do not have
knowledge about the generic drugs. Around 70 percent of the respondents do not
familiar with the term generic drugs, only distinguish that in generally known is, the
less cost of drugs in provided in the public sector. But because of low availability of
drugs in the hospital, doctors also prefer drugs from private retail shops. In this case,
it’s very difficult for any patient to substitute any type of generic which is less costly
than branded. Normally any individual cannot understand about the difference
between generic branded and branded medicines because of the same expression of
all drugs and patients have to choose the branded drugs as preferred by doctors
which results the high burden of drug prices is taken by the patients.
The perspective of doctors and druggists play a significant role for the prescription
about use of drugs because opinions of patients extremely depend upon these two for
use of any drug. Public sector doctors attempt to prefer generic drugs the most and
branded in very rare cases, on the other side private doctors favor to branded drugs
which are more expensive than generic drugs. The results of the present study depict
that 40 percent doctors in private sector favor only branded drugs because of their
quality and their belief generic drugs are less effective and not good in quality.
Remaining around 60 percent doctors have viewed that generics are good substitutes
for branded to make drugs more affordable and they prefer both types of drugs
27
according to the treatment for diseases. So doctors of different hospitals in the city
responses about the drug preference that, usually they prefer both branded and
generic, but ordinarily favor to the branded because of more effectiveness.
The perspective of the drug retailers (chemists) is also interrelated to the doctor’s
view. The patients make more demand of branded drugs from the druggist preferred
by the doctors to them. On the other side in public sector generic, drug store (Jan
Aushadhi) the generics without any brand name are sold. In private medical stores,
both branded and branded-generic are preferred to patient for both regular and
temporary basis. Around 60 percent retailers have viewed that there is a more
demand of branded drugs with a maximum 16 percent to 20 percent margin, but in
case of branded-generic drugs, there is a huge level of margin sometimes nearly
more than 100 percent. When retailers are asked about their views related to this
phenomenon of differences in margins, they expressed that we charge the prices with
a limit of margin according to patients can be minimum or maximum level of margins.
According to the drug wholesaler’s viewpoint, there is not much variation in the
demand of branded and branded generic drugs. The viewpoint of drug wholesalers is
that the print price of generic medicines is many times higher than the company price,
they contracted drugs from the company’s warehouses at very less price, then by
adding their profit margin maximum 10 percent according to drug’s price and drugs
distributed to the retailers in the city. Retailers have no link with wholesalers about
their margin levels, once the wholesalers distribute the drugs then its retailer’s own
choice of charge the price to patients.
The opinions of different respondents can be summed up that preference of branded
or generic drugs is not decided by patients because of lack of knowledge. It depends
upon the doctors or the chemists who suggests drugs. The reason for more
preference to branded drugs by doctor’s views is the better quality and the chemists
prefers to generic drugs because of two reasons, first the low price of generic and
patients can easily afford, secondly the margin level is many times higher than
branded. The differences in mark-up levels of branded generic drugs are the reason
of price difference in the markets. By considering the opinions of different
28
respondents discussed above the present study is an exertion to disclose the
differences in prices and markups charged by retailers which shows the non-
transparency and variations of drug prices in the market.
Availability of Essential Drugs
Availability of essential drugs is one major part of health care in the society. Essential
drugs availability is required in both public as well as in private sectors. By reviewing
the opinions of patients, it comes out that low availability of drugs is the issue of
public sector. As in private sector, there are number of sources available for the
patients to purchase drugs, i.e. medical stores in a large number almost in every
area, but they provide mainly very costly drugs and private doctors also prefer
branded drugs which are costlier than generics. Generics with different brand names
are available in the private sector, which are also sold at the printed price i.e.
maximum retail price (MRP). The generic drugs with lowest price are available in the
public sector drug store known as “Jan Aushadhi” within a civil hospital in Bathinda
city. This generic, drug store is working under the central government to provide
cheaper non-branded essential drugs. There is always issue of lower availability in
the public sector rather than the private sector because of profit- oriented strategy of
the private sector. The insufficient availability issue relates to the public sector is the
reason to select the public sector in the study.
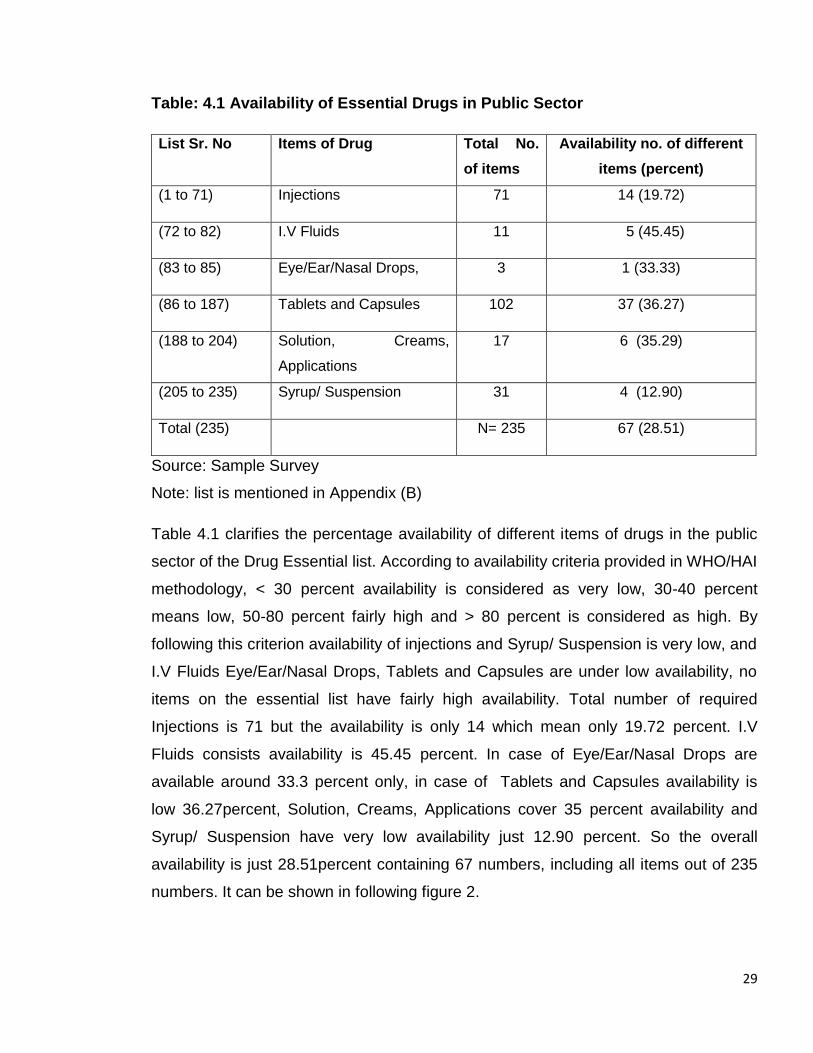
The availability of all essential drugs mentioned in survey is listed from “Drug
essential list of Punjab” (2011) including (235) number of different items of drugs,
which including injections, (1 to 71), I.V Fluids (72 to 82) Eye/Ear/Nasal Drops, (83 to
85), Tablets and capsules, (86 to 187), Solution, Creams, Applications (188 to 204),
Syrup/ Suspension (205 to 235) are surveyed. None of the brands are available in the
drug store. Only generics with salt name are provided there. The price which is
printed on the strip of drug is charged similarly. Overall availability of essential drugs
is found very less only 28.51percent. When patients found the low availability of drugs
in public sector facilities, they forcefully have to purchase drugs from the private drug
stores with high prices, which may also lead to excessive out-of-pocket spending.
29
Table: 4.1 Availability of Essential Drugs in Public Sector
List Sr. No Items of Drug Total No.
of items
Availability no. of different
items (percent)
(1 to 71) Injections 71 14 (19.72)
(72 to 82) I.V Fluids 11 5 (45.45)
(83 to 85) Eye/Ear/Nasal Drops, 3 1 (33.33)
(86 to 187) Tablets and Capsules 102 37 (36.27)
(188 to 204) Solution, Creams,
Applications
17 6 (35.29)
(205 to 235) Syrup/ Suspension 31 4 (12.90)
Total (235) N= 235 67 (28.51)
Source: Sample Survey
Note: list is mentioned in Appendix (B)
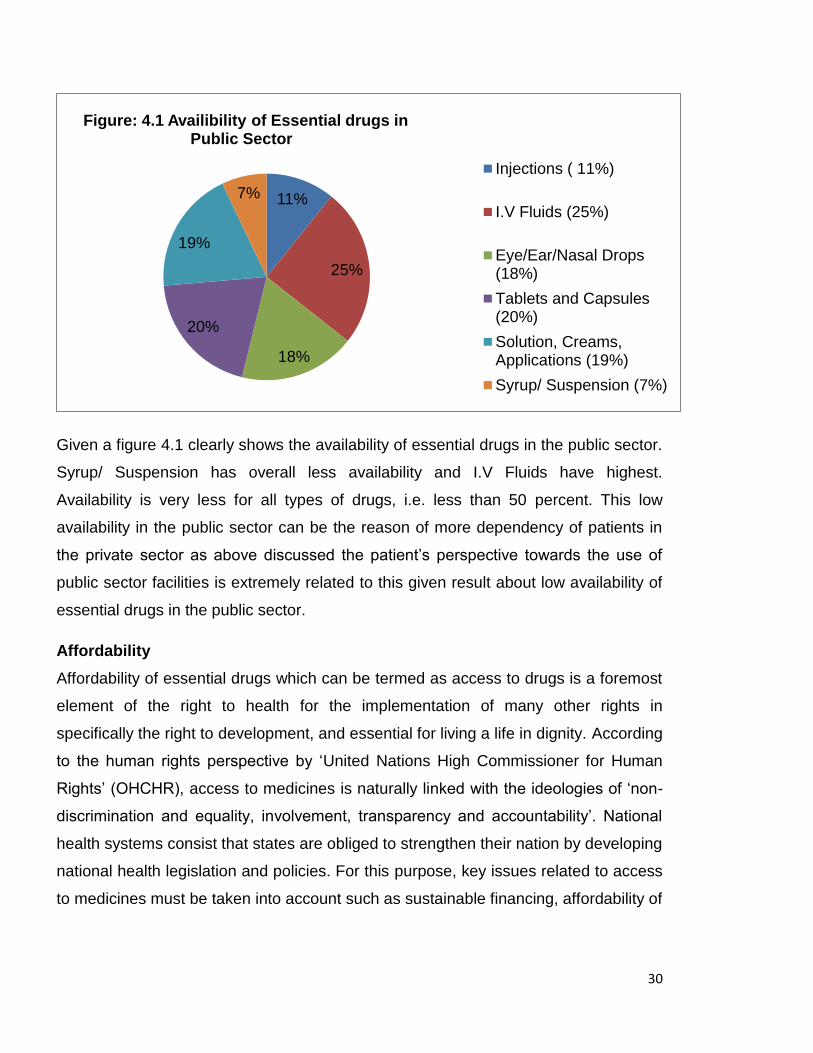
Table 4.1 clarifies the percentage availability of different items of drugs in the public
sector of the Drug Essential list. According to availability criteria provided in WHO/HAI
methodology, < 30 percent availability is considered as very low, 30-40 percent
means low, 50-80 percent fairly high and > 80 percent is considered as high. By
following this criterion availability of injections and Syrup/ Suspension is very low, and
I.V Fluids Eye/Ear/Nasal Drops, Tablets and Capsules are under low availability, no
items on the essential list have fairly high availability. Total number of required
Injections is 71 but the availability is only 14 which mean only 19.72 percent. I.V
Fluids consists availability is 45.45 percent. In case of Eye/Ear/Nasal Drops are
available around 33.3 percent only, in case of Tablets and Capsules availability is
low 36.27percent, Solution, Creams, Applications cover 35 percent availability and
Syrup/ Suspension have very low availability just 12.90 percent. So the overall
availability is just 28.51percent containing 67 numbers, including all items out of 235
numbers. It can be shown in following figure 2.
30
Given a figure 4.1 clearly shows the availability of essential drugs in the public sector.
Syrup/ Suspension has overall less availability and I.V Fluids have highest.
Availability is very less for all types of drugs, i.e. less than 50 percent. This low
availability in the public sector can be the reason of more dependency of patients in
the private sector as above discussed the patient’s perspective towards the use of
public sector facilities is extremely related to this given result about low availability of
essential drugs in the public sector.
Affordability
Affordability of essential drugs which can be termed as access to drugs is a foremost
element of the right to health for the implementation of many other rights in
specifically the right to development, and essential for living a life in dignity. According
to the human rights perspective by ‘United Nations High Commissioner for Human
Rights’ (OHCHR), access to medicines is naturally linked with the ideologies of ‘non-
discrimination and equality, involvement, transparency and accountability’. National
health systems consist that states are obliged to strengthen their nation by developing
national health legislation and policies. For this purpose, key issues related to access
to medicines must be taken into account such as sustainable financing, affordability of
11%
25%
18%
20%
19%
7%
Figure: 4.1 Availibility of Essential drugs in Public Sector
Injections ( 11%)
I.V Fluids (25%)
Eye/Ear/Nasal Drops(18%)
Tablets and Capsules(20%)
Solution, Creams,Applications (19%)
Syrup/ Suspension (7%)
31
essential drugs, price and quality control, dosage and efficacy of drugs, procurement
practices and procedures, supply chains, etc.
One method to measure the affordability is used given in the WHO/HAI methodology.
This comparison is given to the ordinary people, i.e. lowest paid unskilled government
worker. This is measured by comparing the treatment cost with the wages they earn.
The salary of the lowest paid government worker is identified by the government
source. It determines the number of days of wages required by this worker for
purchasing medicines for a standard duration of treatment for a common condition.
The wage rate in Bathinda of the lowest paid unskilled government worker is Rs.
219.20 on the daily basis. The lowest paid unskilled worker in the private sector or
unorganized sector could be earning more or less.
The second method is used to determine the affordability, by considering the number
of poor people. In Punjab, according to Tendulkar methodology (2011-12) the
population below poverty line is 7.66 percent in rural areas, 9.24 percent in urban
areas and 8.26percent overall which means no. of persons are 23.18 (lakhs). Punjab
state has poverty lines limit in monthly per capita (RS) 1,054 for rural and 1,155 for
urban. This means 35.13 Rs per day in rural and 38.5 in urban areas. So the
affordability of the essential medicines for 23.18 (lakhs) people is very low in Punjab.
The poverty status in the district Bathinda 32141 families are living below the poverty
line in addition to 6491 families in even more miserable conditions i.e. having an
income equal to half of the BPL families, thus making a total of 38632 families in all in
the BPL category. In the profile of city Bathinda 5177 families are living below the
poverty out of which 1093 families having the status of the poorest of the poor and
4084 families are poor who have less than Rs 47 per day spending.(2011-12) Even
the treatment cost of minor health problems is burden for these poor people. The
essential drugs surveyed have calculated the treatment cost both in public and private
sector by daily dose and duration of days for treatment.
32
Table: 4.2 Affordability of Standard Treatment
Therapeutic
class Drug Name
Daily Dose
Duration Days
Treatment Cost (Rs.)
Public
Sector
Private
Sector
Antacid Tab. Pentaperazole 40 mg OD 30 days 23.16 250.5
Tab. Rantidine 150 mg BD 30 days 20.31 30
Antibacterial
Tab. Cotrimoxazole S.S (Trimethoprim 80mg + Sulphamethoxazole 400mg)
BD 5 days 5 7
Tab. Levoflexine 250 mg BD 7 days 13.98 28
Tab. Azithromycine 250mg BD 5days 26.93 56.75
Tab. Ciprofloxacin Coated 250 mg
BD 1 day 1.654 3
Tab. Ciprofloxacin Coated 500mg
OD 1day 3.081 4.2
Tab. Cefixime 200 mg BD 5 days 28.92 62.5
Anti-Allergic Tab. Levo Cetirizine 5mg OD 5 days 1.63 17.5
Tab. Cetirizine Hcl 10 mg OD 5 days 1.35 10
Pain Killer Fever Tab. Paracetamol 500 mg BD 5 days 2.8 6
Tab.Paracetamol 500 mg + Diclofenac Sodium 50 mg
BD 5 days 2.66 8.5
Antifungal Tab. Fluconazole 150 mg OD 5days 20.62 119
Antihypertensive Tab. Atenolol 50 mg OD 30 days 12.9 68.7
Anti-infective
Cap. Amoxycillin 500 mg BD 7 days 25.9 49
Tab. Amoxycillin + Clauvinic Acid -500mg +125 mg
BD 3 days 20.61 45
Tab. Ofloxacin 200 mg BD 5 days 8.56 26
Tab. Ofloxacin + Ornidazole ( 200mg + 500mg)
BD 5 days 14.13 49
Anti Helminthic Tab. Albendazole 400 mg OD 7 days 14.21 70
Laxatives Tab. Bisacodyl 10 mg OD 1day 0.384 1
Source: Sample Survey
Note: OD- once a day, BD- twice a day
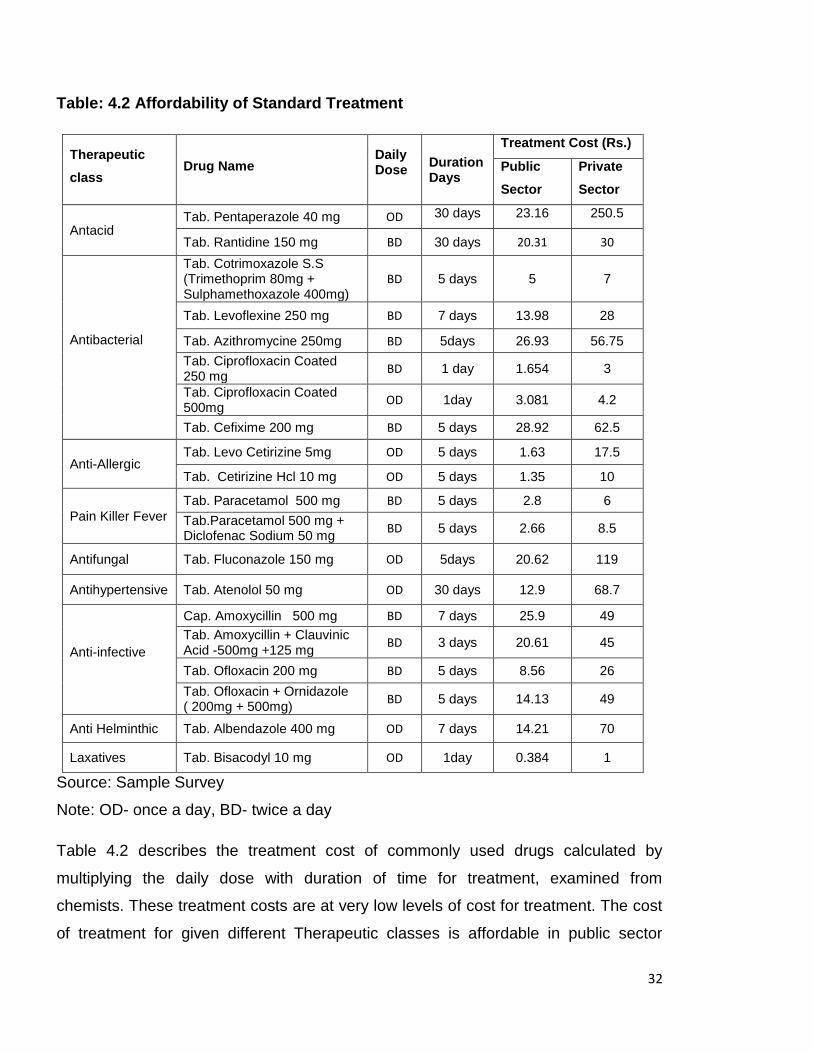
Table 4.2 describes the treatment cost of commonly used drugs calculated by
multiplying the daily dose with duration of time for treatment, examined from
chemists. These treatment costs are at very low levels of cost for treatment. The cost
of treatment for given different Therapeutic classes is affordable in public sector
33
comparing the private sector. It can be affordable to those who earn enough for the
surviving the basic needs but not affordable to those who lives the life with very low
income or below poverty line. These costs are also affordable for the ordinary people
defined in WHO/HAI methodology which are lowest unskilled government workers
because they earn wages Rs. 219.20 per day and the treatment cost of these
common drugs is slightly affordable, but the wages in unorganized sector of unskilled
workers are lower than the public sector and the 5177 families which are poor having
less than Rs. 47 per day spending has never afforded the treatment costs in the
private sector, and have difficulty to pay the treatment cost in the public sector. The
conclusion of the affordability issue is the treatment of these diseases are affordable
for only the higher income or slightly for the people employed in the government
sector, drugs are not affordable for the low income and or people because these
costs are only included drug costs, other costs as doctor’s consultation fees and
diagnostic tests will likely mean that the total cost to the patient may be considerably
higher.
Drug Prices
Price of any drug is known by MRP printed on the strip of the drug. MRP is the
maximum retail price, which a retailer can charge. Mostly in all of the retail shops the
drugs are sold on this printed price, according to the general phenomena of Indian
market this is identified to charge the printed price, which includes all the costs, such
as manufacturing, distributing, taxes etc. and the consumers also give the opinion
that they purchase the drugs at printed price. Indian Drugs are sold in two categories
as ‘branded’ and ‘branded-generic’ as almost all products carry a brand (trade) name.
All drugs were generics up to the January (2005), when product patents were not
applicable in India and the branded drugs are manufactured by a multinational or an
Indian manufacturer of good status. Branded medicines are promoted by
manufacturers. They are more popular and sell better at higher prices. Almost all
drugs carry trade-names and are available in private retail drugstore outlets. The
public sector attains drugs most often as generics with the product labeled using the
chemical name.
34
In a contemporary study it is found that in case of branded drugs, there is not much
difference between wholesale and retail price and markups, but in case of branded
generic drugs, huge difference between MRP and manufacturing price exist.
Wholesalers and some retailers also give their views about the gap in drug prices.
According to some retailers generic drugs are sold at reasonable prices and charged
less than MRP, because of the very less price charged by wholesalers. In this regard
different retailers charge different prices to different consumers, according to the
patient’s affordability, but mostly they charge the printed price on the drug strip i.e.
MRP. This difference makes the inadequate situation in the market and differences in
profit margins. So this is the issue that why the MRP is printed very high instead of
according to the actual cost which is very low.
The patient’s view on prevailing drug prices by survey shows the people who have
high income they bear the less burden of high drug prices and somewhat satisfied
with the prevailing prices, but the people who live their lives with very low income
even found difficulties in fulfillment of basic necessities they found higher burden of
health care because of very costly private treatments and high prices of drugs which
makes them dissatisfied to prevailing prices. The price variations from one to another
retailer are also make diversity in prices. People expect to lower these prices or any
financial help so that they can live a healthy life.
In the present study area of Bathinda city, both public and private sectors are
included in determining the price differences. In the public sector Department of
Pharmaceuticals in association with Central Pharma Public Sector Undertakings
(2008), launched ‘Jan Aushadhi stores’ to provide quality drugs at affordable prices to
the common people. Jan Aushadhi stores have been set up to provide generic drugs,
which are available at low prices, but are equivalent in quality and efficiency as
expensive branded drugs. On the other side in private sector generic-branded or
branded drugs which are much costlier than generics are preferred by doctors to
patients. The general opinion about generic drugs is not positive. It is opined that
generic drugs are less effective than branded so the demand of branded drugs is
more than generics. This opinion affects negative to the poor people, who cannot
35
afford very costly branded drugs and they also have to purchase the brand drugs. But
it is the wrong prescription about generic drugs because the prices of generic
medicines are much cheaper than their branded equivalent. It is proved that equally
safe and having the same efficacy as that of branded medicines in terms of their
therapeutic value. Bureau of Pharma Public Sector Undertakings of India (BPPI) has
been established under the Department of Pharmaceuticals, Government of India,
with the support of all the CPSUs for co-coordinating procurement, supply and
marketing of generic drugs through the Jan Aushadhi Stores. The quality, safety and
efficacy of medicines are ensured of getting each batch of medicines procured from
CPSUs as well as private suppliers tested from National Accreditation Board for
Testing and Calibration Laboratories, (NABL) approved laboratories and conforming
to the required standards before the same are supplied to Superstockists /Jan
Aushadhi Stores from the Warehouse of (BPPI). In the private sector retail drug
stores drugs are supplied by the wholesalers by drug distribution chain, in which the
price become varied from its wholesale to retail price (Janaushadhi, 2015).
Drug Price Differences between Public and Private sector
Prices of essential drugs are collected from the printed price on the drug strips
available in public and private sector. By comparing the prices, it is found that public
sector provides drugs at very reasonable prices as compared to the private sector.
Only generic drugs are found in the public sector drug store known as Jan Aushadhi
Drug store working under the Central Government Scheme on (2008), with the
objectives to promote awareness about cost effective drug prescribing, to make
available unbranded quality generic medicines at affordable prices through public-
private partnership. So the prices of the same name of drugs in private retail shops
which provide generic branded drugs are very different with same salt. Table 4.3
shows the price differences between the public and private sector of commonly used
drugs in Bathinda city.
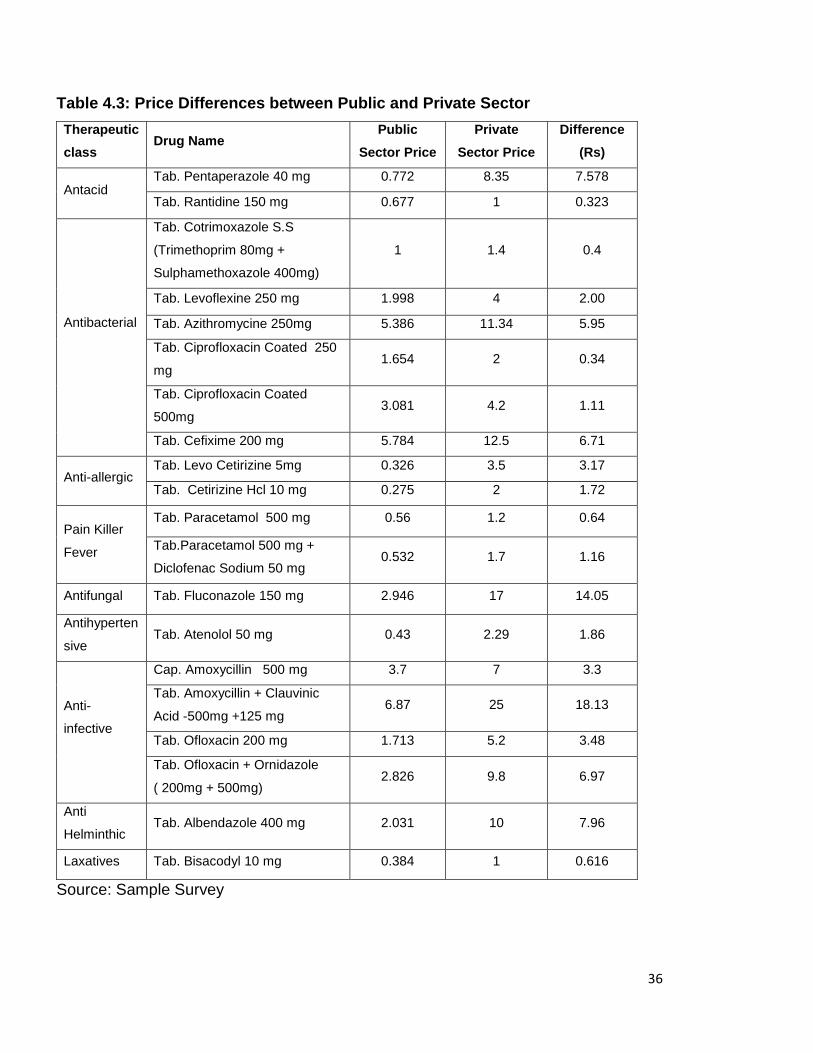
36
Table 4.3: Price Differences between Public and Private Sector
Therapeutic
class Drug Name
Public
Sector Price
Private
Sector Price
Difference
(Rs)
Antacid Tab. Pentaperazole 40 mg 0.772 8.35 7.578
Tab. Rantidine 150 mg 0.677 1 0.323
Antibacterial
Tab. Cotrimoxazole S.S
(Trimethoprim 80mg +
Sulphamethoxazole 400mg)
1 1.4 0.4
Tab. Levoflexine 250 mg 1.998 4 2.00
Tab. Azithromycine 250mg 5.386 11.34 5.95
Tab. Ciprofloxacin Coated 250
mg 1.654 2 0.34
Tab. Ciprofloxacin Coated
500mg 3.081 4.2 1.11
Tab. Cefixime 200 mg 5.784 12.5 6.71
Anti-allergic Tab. Levo Cetirizine 5mg 0.326 3.5 3.17
Tab. Cetirizine Hcl 10 mg 0.275 2 1.72
Pain Killer
Fever
Tab. Paracetamol 500 mg 0.56 1.2 0.64
Tab.Paracetamol 500 mg +
Diclofenac Sodium 50 mg 0.532 1.7 1.16
Antifungal Tab. Fluconazole 150 mg 2.946 17 14.05
Antihyperten
sive Tab. Atenolol 50 mg 0.43 2.29 1.86
Anti-
infective
Cap. Amoxycillin 500 mg 3.7 7 3.3
Tab. Amoxycillin + Clauvinic
Acid -500mg +125 mg 6.87 25 18.13
Tab. Ofloxacin 200 mg 1.713 5.2 3.48
Tab. Ofloxacin + Ornidazole
( 200mg + 500mg) 2.826 9.8 6.97
Anti
Helminthic Tab. Albendazole 400 mg 2.031 10 7.96
Laxatives Tab. Bisacodyl 10 mg 0.384 1 0.616
Source: Sample Survey
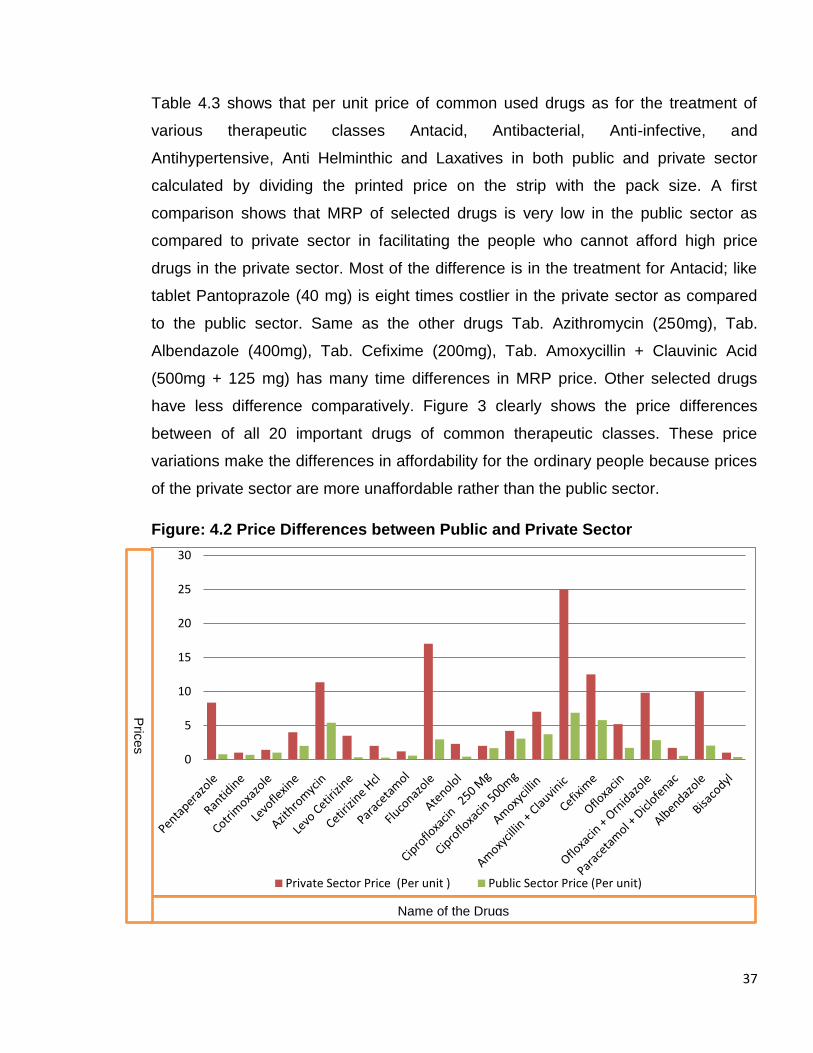
37
Table 4.3 shows that per unit price of common used drugs as for the treatment of
various therapeutic classes Antacid, Antibacterial, Anti-infective, and
Antihypertensive, Anti Helminthic and Laxatives in both public and private sector
calculated by dividing the printed price on the strip with the pack size. A first
comparison shows that MRP of selected drugs is very low in the public sector as
compared to private sector in facilitating the people who cannot afford high price
drugs in the private sector. Most of the difference is in the treatment for Antacid; like
tablet Pantoprazole (40 mg) is eight times costlier in the private sector as compared
to the public sector. Same as the other drugs Tab. Azithromycin (250mg), Tab.
Albendazole (400mg), Tab. Cefixime (200mg), Tab. Amoxycillin + Clauvinic Acid
(500mg + 125 mg) has many time differences in MRP price. Other selected drugs
have less difference comparatively. Figure 3 clearly shows the price differences
between of all 20 important drugs of common therapeutic classes. These price
variations make the differences in affordability for the ordinary people because prices
of the private sector are more unaffordable rather than the public sector.
Figure: 4.2 Price Differences between Public and Private Sector
0
5
10
15
20
25
30
Private Sector Price (Per unit ) Public Sector Price (Per unit)
Name of the Drugs
Prices
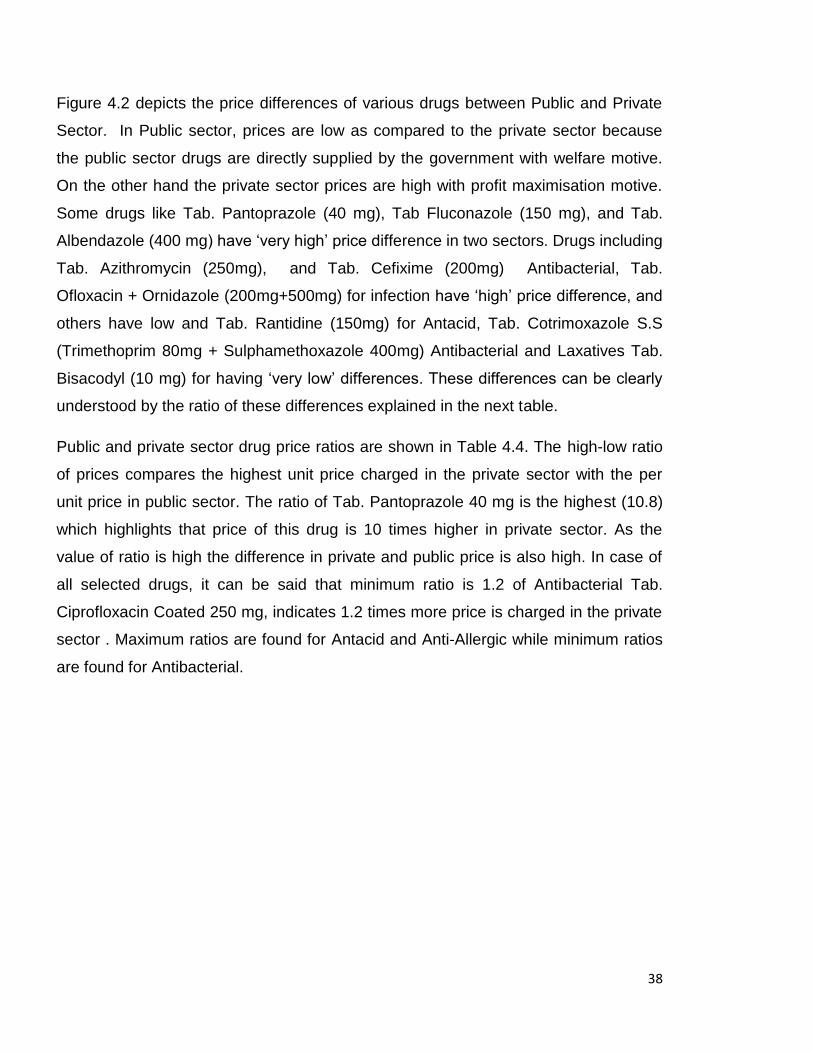
38
Figure 4.2 depicts the price differences of various drugs between Public and Private
Sector. In Public sector, prices are low as compared to the private sector because
the public sector drugs are directly supplied by the government with welfare motive.
On the other hand the private sector prices are high with profit maximisation motive.
Some drugs like Tab. Pantoprazole (40 mg), Tab Fluconazole (150 mg), and Tab.
Albendazole (400 mg) have ‘very high’ price difference in two sectors. Drugs including
Tab. Azithromycin (250mg), and Tab. Cefixime (200mg) Antibacterial, Tab.
Ofloxacin + Ornidazole (200mg+500mg) for infection have ‘high’ price difference, and
others have low and Tab. Rantidine (150mg) for Antacid, Tab. Cotrimoxazole S.S
(Trimethoprim 80mg + Sulphamethoxazole 400mg) Antibacterial and Laxatives Tab.
Bisacodyl (10 mg) for having ‘very low’ differences. These differences can be clearly
understood by the ratio of these differences explained in the next table.
Public and private sector drug price ratios are shown in Table 4.4. The high-low ratio
of prices compares the highest unit price charged in the private sector with the per
unit price in public sector. The ratio of Tab. Pantoprazole 40 mg is the highest (10.8)
which highlights that price of this drug is 10 times higher in private sector. As the
value of ratio is high the difference in private and public price is also high. In case of
all selected drugs, it can be said that minimum ratio is 1.2 of Antibacterial Tab.
Ciprofloxacin Coated 250 mg, indicates 1.2 times more price is charged in the private
sector . Maximum ratios are found for Antacid and Anti-Allergic while minimum ratios
are found for Antibacterial.
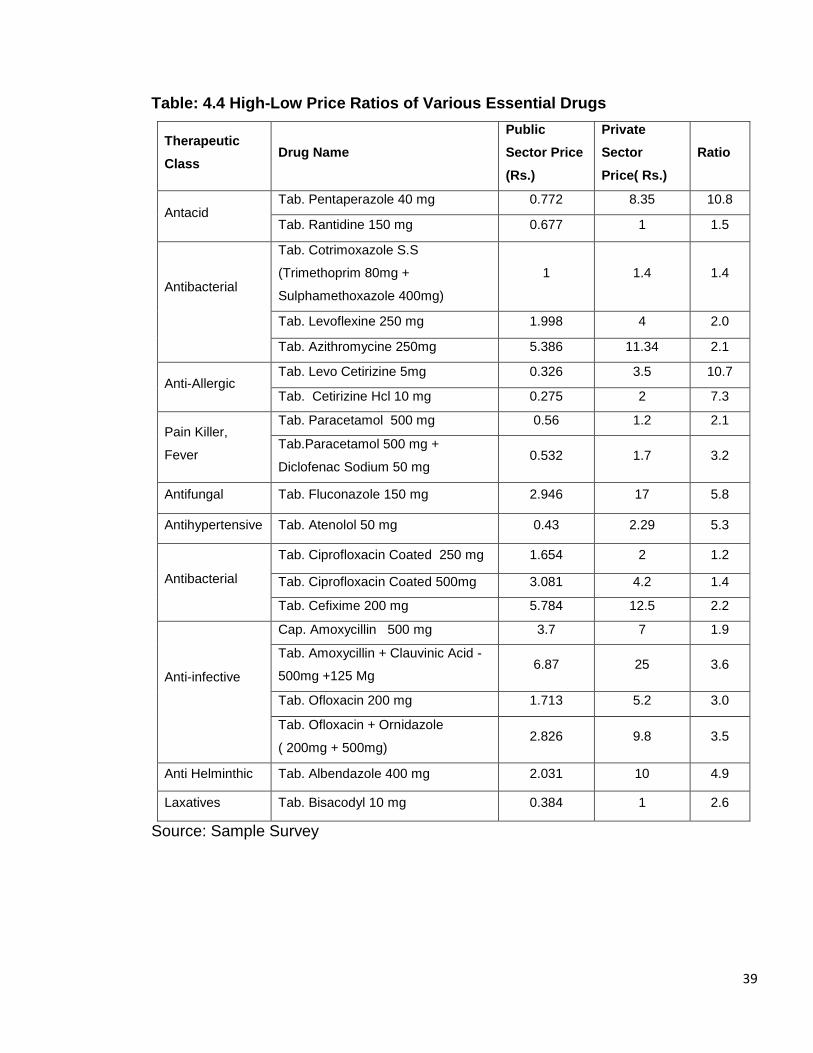
39
Table: 4.4 High-Low Price Ratios of Various Essential Drugs
Therapeutic
Class Drug Name
Public
Sector Price
(Rs.)
Private
Sector
Price( Rs.)
Ratio
Antacid Tab. Pentaperazole 40 mg 0.772 8.35 10.8
Tab. Rantidine 150 mg 0.677 1 1.5
Antibacterial
Tab. Cotrimoxazole S.S
(Trimethoprim 80mg +
Sulphamethoxazole 400mg)
1 1.4 1.4
Tab. Levoflexine 250 mg 1.998 4 2.0
Tab. Azithromycine 250mg 5.386 11.34 2.1
Anti-Allergic Tab. Levo Cetirizine 5mg 0.326 3.5 10.7
Tab. Cetirizine Hcl 10 mg 0.275 2 7.3
Pain Killer,
Fever
Tab. Paracetamol 500 mg 0.56 1.2 2.1
Tab.Paracetamol 500 mg +
Diclofenac Sodium 50 mg 0.532 1.7 3.2
Antifungal Tab. Fluconazole 150 mg 2.946 17 5.8
Antihypertensive Tab. Atenolol 50 mg 0.43 2.29 5.3
Antibacterial
Tab. Ciprofloxacin Coated 250 mg 1.654 2 1.2
Tab. Ciprofloxacin Coated 500mg 3.081 4.2 1.4
Tab. Cefixime 200 mg 5.784 12.5 2.2
Anti-infective
Cap. Amoxycillin 500 mg 3.7 7 1.9
Tab. Amoxycillin + Clauvinic Acid -
500mg +125 Mg 6.87 25 3.6
Tab. Ofloxacin 200 mg 1.713 5.2 3.0
Tab. Ofloxacin + Ornidazole
( 200mg + 500mg) 2.826 9.8 3.5
Anti Helminthic Tab. Albendazole 400 mg 2.031 10 4.9
Laxatives Tab. Bisacodyl 10 mg 0.384 1 2.6
Source: Sample Survey
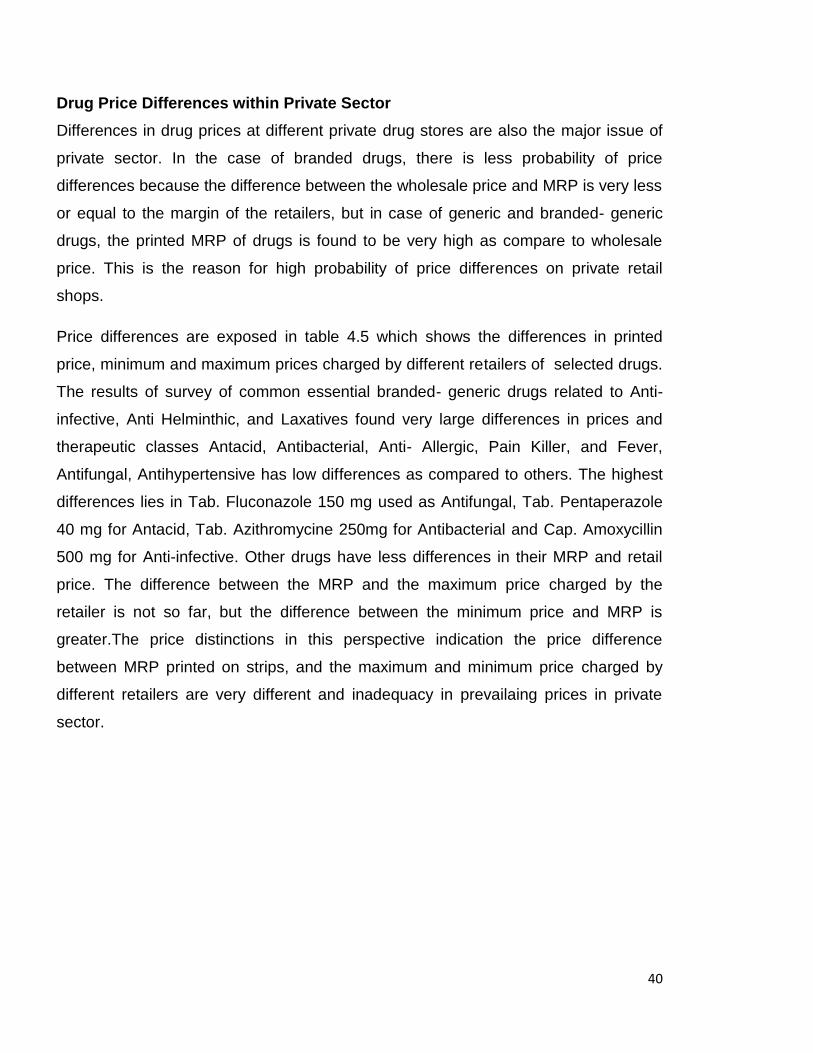
40
Drug Price Differences within Private Sector
Differences in drug prices at different private drug stores are also the major issue of
private sector. In the case of branded drugs, there is less probability of price
differences because the difference between the wholesale price and MRP is very less
or equal to the margin of the retailers, but in case of generic and branded- generic
drugs, the printed MRP of drugs is found to be very high as compare to wholesale
price. This is the reason for high probability of price differences on private retail
shops.
Price differences are exposed in table 4.5 which shows the differences in printed
price, minimum and maximum prices charged by different retailers of selected drugs.
The results of survey of common essential branded- generic drugs related to Anti-
infective, Anti Helminthic, and Laxatives found very large differences in prices and
therapeutic classes Antacid, Antibacterial, Anti- Allergic, Pain Killer, and Fever,
Antifungal, Antihypertensive has low differences as compared to others. The highest
differences lies in Tab. Fluconazole 150 mg used as Antifungal, Tab. Pentaperazole
40 mg for Antacid, Tab. Azithromycine 250mg for Antibacterial and Cap. Amoxycillin
500 mg for Anti-infective. Other drugs have less differences in their MRP and retail
price. The difference between the MRP and the maximum price charged by the
retailer is not so far, but the difference between the minimum price and MRP is
greater.The price distinctions in this perspective indication the price difference
between MRP printed on strips, and the maximum and minimum price charged by
different retailers are very different and inadequacy in prevailaing prices in private
sector.
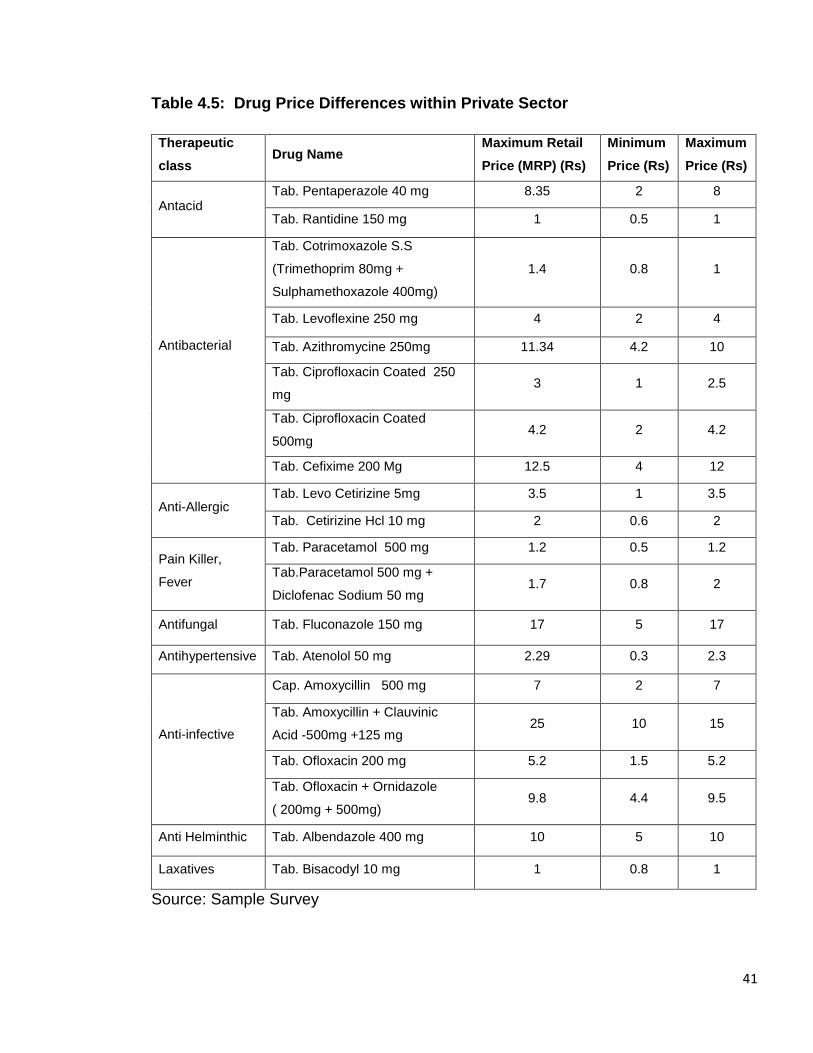
41
Table 4.5: Drug Price Differences within Private Sector
Therapeutic
class Drug Name
Maximum Retail
Price (MRP) (Rs)
Minimum
Price (Rs)
Maximum
Price (Rs)
Antacid Tab. Pentaperazole 40 mg 8.35 2 8
Tab. Rantidine 150 mg 1 0.5 1
Antibacterial
Tab. Cotrimoxazole S.S
(Trimethoprim 80mg +
Sulphamethoxazole 400mg)
1.4 0.8 1
Tab. Levoflexine 250 mg 4 2 4
Tab. Azithromycine 250mg 11.34 4.2 10
Tab. Ciprofloxacin Coated 250
mg 3 1 2.5
Tab. Ciprofloxacin Coated
500mg 4.2 2 4.2
Tab. Cefixime 200 Mg 12.5 4 12
Anti-Allergic Tab. Levo Cetirizine 5mg 3.5 1 3.5
Tab. Cetirizine Hcl 10 mg 2 0.6 2
Pain Killer,
Fever
Tab. Paracetamol 500 mg 1.2 0.5 1.2
Tab.Paracetamol 500 mg +
Diclofenac Sodium 50 mg 1.7 0.8 2
Antifungal Tab. Fluconazole 150 mg 17 5 17
Antihypertensive Tab. Atenolol 50 mg 2.29 0.3 2.3
Anti-infective
Cap. Amoxycillin 500 mg 7 2 7
Tab. Amoxycillin + Clauvinic
Acid -500mg +125 mg 25 10 15
Tab. Ofloxacin 200 mg 5.2 1.5 5.2
Tab. Ofloxacin + Ornidazole
( 200mg + 500mg) 9.8 4.4 9.5
Anti Helminthic Tab. Albendazole 400 mg 10 5 10
Laxatives Tab. Bisacodyl 10 mg 1 0.8 1
Source: Sample Survey
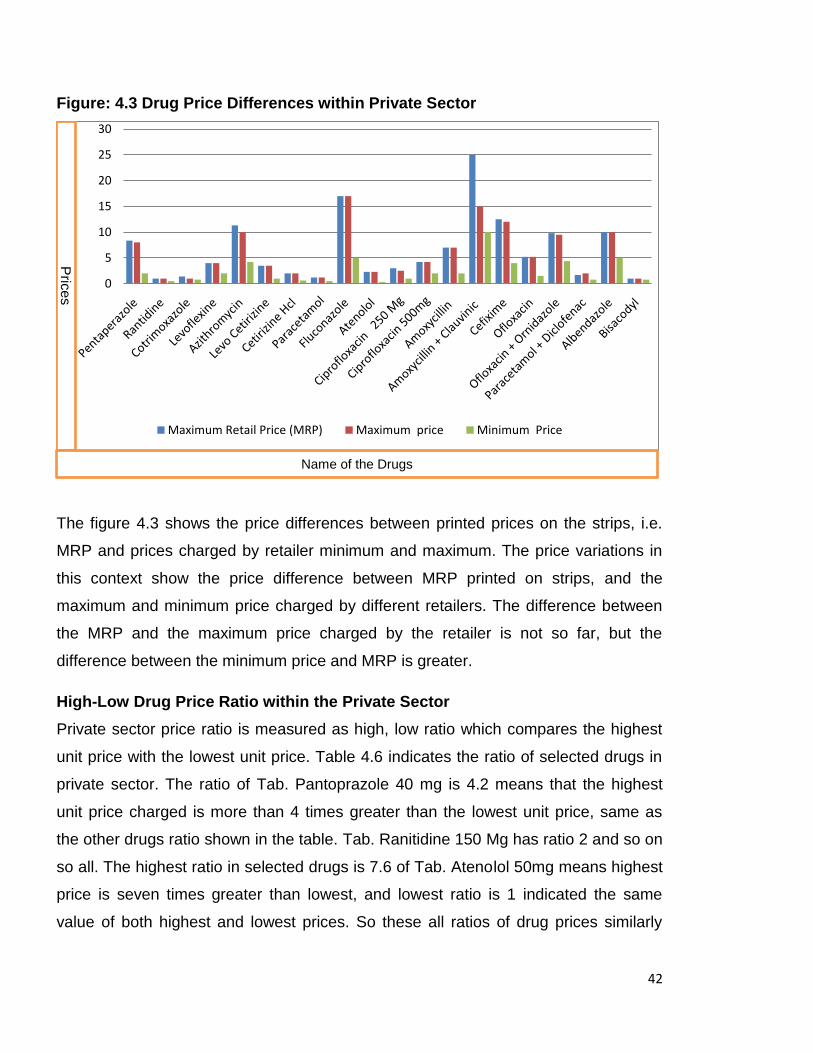
42
Figure: 4.3 Drug Price Differences within Private Sector
The figure 4.3 shows the price differences between printed prices on the strips, i.e.
MRP and prices charged by retailer minimum and maximum. The price variations in
this context show the price difference between MRP printed on strips, and the
maximum and minimum price charged by different retailers. The difference between
the MRP and the maximum price charged by the retailer is not so far, but the
difference between the minimum price and MRP is greater.
High-Low Drug Price Ratio within the Private Sector
Private sector price ratio is measured as high, low ratio which compares the highest
unit price with the lowest unit price. Table 4.6 indicates the ratio of selected drugs in
private sector. The ratio of Tab. Pantoprazole 40 mg is 4.2 means that the highest
unit price charged is more than 4 times greater than the lowest unit price, same as
the other drugs ratio shown in the table. Tab. Ranitidine 150 Mg has ratio 2 and so on
so all. The highest ratio in selected drugs is 7.6 of Tab. Atenolol 50mg means highest
price is seven times greater than lowest, and lowest ratio is 1 indicated the same
value of both highest and lowest prices. So these all ratios of drug prices similarly
0
5
10
15
20
25
30
Maximum Retail Price (MRP) Maximum price Minimum Price
Prices
Name of the Drugs
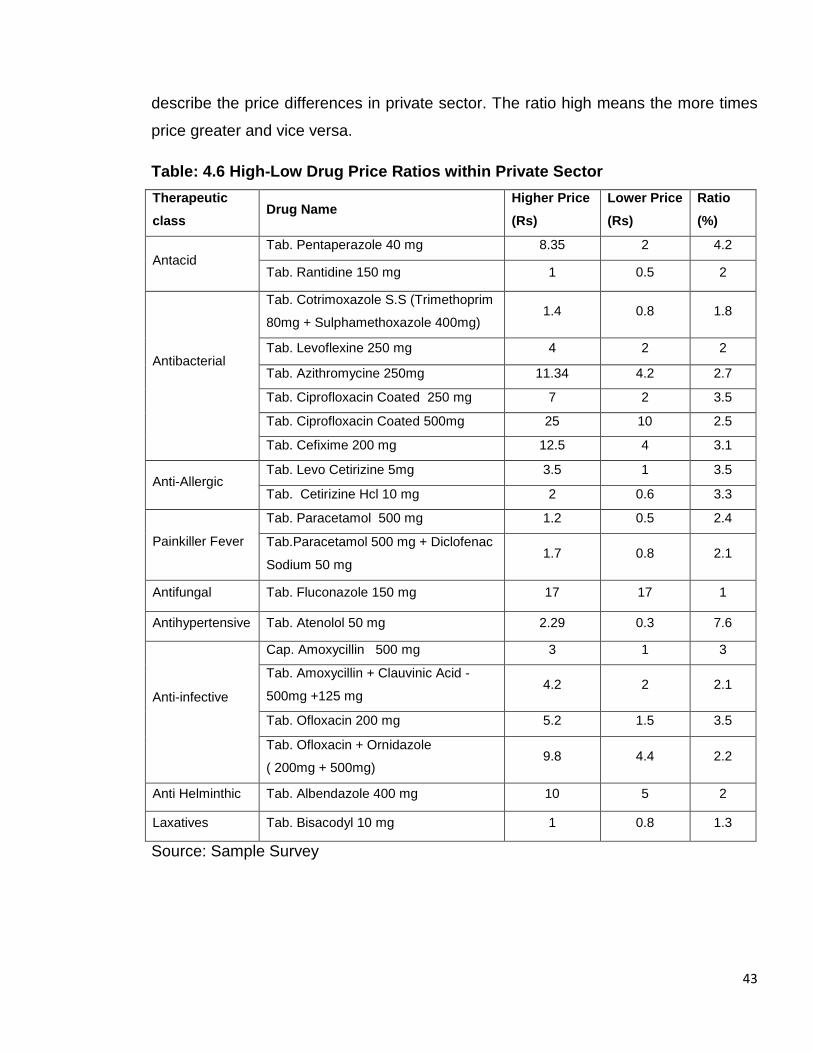
43
describe the price differences in private sector. The ratio high means the more times
price greater and vice versa.
Table: 4.6 High-Low Drug Price Ratios within Private Sector
Therapeutic
class Drug Name
Higher Price
(Rs)
Lower Price
(Rs)
Ratio
(%)
Antacid Tab. Pentaperazole 40 mg 8.35 2 4.2
Tab. Rantidine 150 mg 1 0.5 2
Antibacterial
Tab. Cotrimoxazole S.S (Trimethoprim
80mg + Sulphamethoxazole 400mg) 1.4 0.8 1.8
Tab. Levoflexine 250 mg 4 2 2
Tab. Azithromycine 250mg 11.34 4.2 2.7
Tab. Ciprofloxacin Coated 250 mg 7 2 3.5
Tab. Ciprofloxacin Coated 500mg 25 10 2.5
Tab. Cefixime 200 mg 12.5 4 3.1
Anti-Allergic Tab. Levo Cetirizine 5mg 3.5 1 3.5
Tab. Cetirizine Hcl 10 mg 2 0.6 3.3
Painkiller Fever
Tab. Paracetamol 500 mg 1.2 0.5 2.4
Tab.Paracetamol 500 mg + Diclofenac
Sodium 50 mg 1.7 0.8 2.1
Antifungal Tab. Fluconazole 150 mg 17 17 1
Antihypertensive Tab. Atenolol 50 mg 2.29 0.3 7.6
Anti-infective
Cap. Amoxycillin 500 mg 3 1 3
Tab. Amoxycillin + Clauvinic Acid -
500mg +125 mg 4.2 2 2.1
Tab. Ofloxacin 200 mg 5.2 1.5 3.5
Tab. Ofloxacin + Ornidazole
( 200mg + 500mg) 9.8 4.4 2.2
Anti Helminthic Tab. Albendazole 400 mg 10 5 2
Laxatives Tab. Bisacodyl 10 mg 1 0.8 1.3
Source: Sample Survey
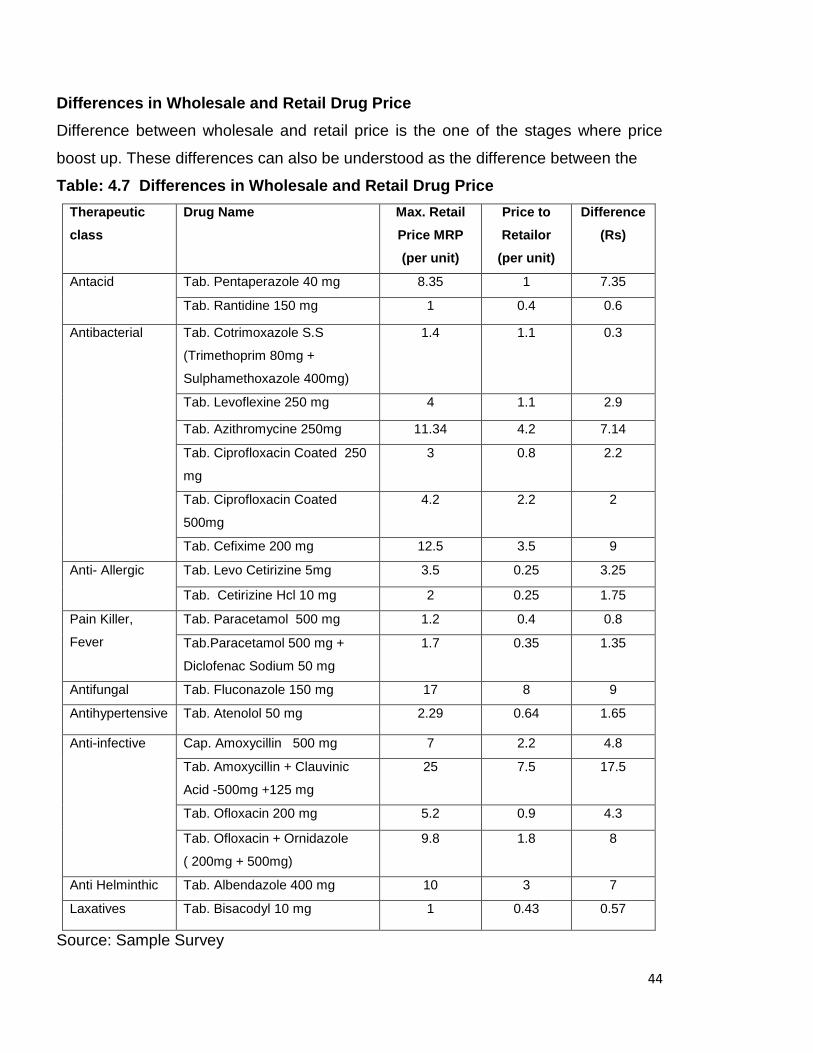
44
Differences in Wholesale and Retail Drug Price
Difference between wholesale and retail price is the one of the stages where price
boost up. These differences can also be understood as the difference between the
Table: 4.7 Differences in Wholesale and Retail Drug Price
Therapeutic
class
Drug Name Max. Retail
Price MRP
(per unit)
Price to
Retailor
(per unit)
Difference
(Rs)
Antacid Tab. Pentaperazole 40 mg 8.35 1 7.35
Tab. Rantidine 150 mg 1 0.4 0.6
Antibacterial
Tab. Cotrimoxazole S.S
(Trimethoprim 80mg +
Sulphamethoxazole 400mg)
1.4 1.1 0.3
Tab. Levoflexine 250 mg 4 1.1 2.9
Tab. Azithromycine 250mg 11.34 4.2 7.14
Tab. Ciprofloxacin Coated 250
mg
3 0.8 2.2
Tab. Ciprofloxacin Coated
500mg
4.2 2.2 2
Tab. Cefixime 200 mg 12.5 3.5 9
Anti- Allergic Tab. Levo Cetirizine 5mg 3.5 0.25 3.25
Tab. Cetirizine Hcl 10 mg 2 0.25 1.75
Pain Killer,
Fever
Tab. Paracetamol 500 mg 1.2 0.4 0.8
Tab.Paracetamol 500 mg +
Diclofenac Sodium 50 mg
1.7 0.35 1.35
Antifungal Tab. Fluconazole 150 mg 17 8 9
Antihypertensive Tab. Atenolol 50 mg 2.29 0.64 1.65
Anti-infective
Cap. Amoxycillin 500 mg 7 2.2 4.8
Tab. Amoxycillin + Clauvinic
Acid -500mg +125 mg
25 7.5 17.5
Tab. Ofloxacin 200 mg 5.2 0.9 4.3
Tab. Ofloxacin + Ornidazole
( 200mg + 500mg)
9.8 1.8 8
Anti Helminthic Tab. Albendazole 400 mg 10 3 7
Laxatives Tab. Bisacodyl 10 mg 1 0.43 0.57
Source: Sample Survey
45
price to the retailer (PTR) charged by the wholesaler and price to the patient (PTP)
charged by the retailer, is set up by considering the high mark-up of retailers, which
works as a source to promote generic drugs. The manufacturing cost of these drugs
is very low, as shown from the Table 4.8 that a wholesaler provides a drug Tab.
Pantoprazole 40 mg to the retailer 1 rupee of per unit by taking his profit of minimum
10percent, that means manufacture provides less than 1 rupee but the retailers have
permission to sell it at maximum Rs. 8.35 which means the difference in per unit of
Rs. 7.35 rupees and the patient affected by these differences.
Table 4.7 shows the difference between wholesale and retail price. Some drugs i.e.
Tab. Pentaperazole (40 mg), Tab. Azithromycin 250mg, Tab Fluconazole (150 mg),
Tab. Amoxycillin + Clauvinic Acid -500mg + 125 Mg, Tab. Cefixime (200 mg), Tab.
Ofloxacin + Ornidazole (200mg+500mg), Tab. Albendazole (400 mg) have very large
difference in two prices and others Tab. Cotrimoxazole S.S (Trimethoprim 80mg +
Sulphamethoxazole 400mg), Tab. Bisacodyl (10 mg), Tab. Paracetamol (500 mg),
Tab. Ciprofloxacin Coated (500mg) containing less difference as compare to others. It
can be concluded that Antacid, Antibacterial, Anti-Fungal, Anti-infective, Anti
Helminthic therapeutic category contain more price differences than others. So,
these classes have a high profit margin for retailers.
Table 4.8 describes that price difference have another aspect, i.e. difference between
MRP and median price charged by retailers. According to some retailers, they charge
less than the MRP. The large difference means retailers charge a reasonable price
because of low wholesale price. If the difference is very less or both prices are equal,
than the retailers take high markups. In selecting drugs only 5 drugs have the
supplementary difference between MRP and median price prevailing in different drug
stores, which means that the prices charged by the retailer is mostly near the MRP or
on MRP.
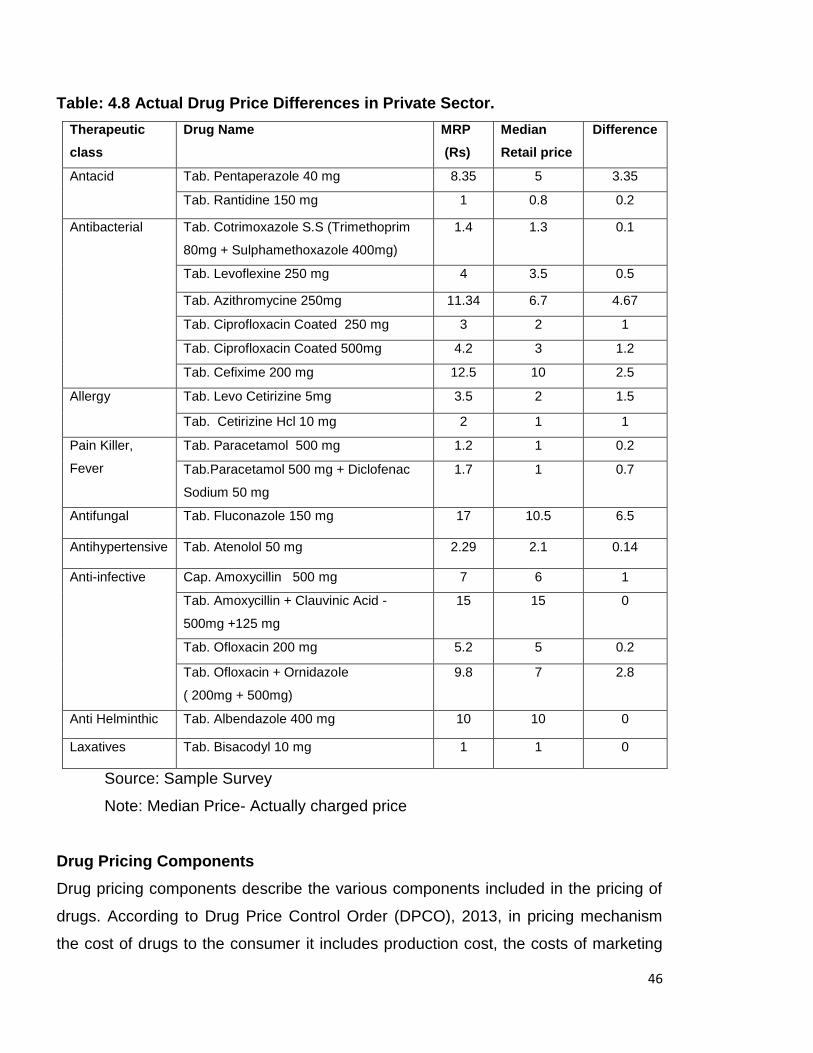
46
Table: 4.8 Actual Drug Price Differences in Private Sector.
Therapeutic
class
Drug Name MRP
(Rs)
Median
Retail price
Difference
Antacid Tab. Pentaperazole 40 mg 8.35 5 3.35
Tab. Rantidine 150 mg 1 0.8 0.2
Antibacterial
Tab. Cotrimoxazole S.S (Trimethoprim
80mg + Sulphamethoxazole 400mg)
1.4 1.3 0.1
Tab. Levoflexine 250 mg 4 3.5 0.5
Tab. Azithromycine 250mg 11.34 6.7 4.67
Tab. Ciprofloxacin Coated 250 mg 3 2 1
Tab. Ciprofloxacin Coated 500mg 4.2 3 1.2
Tab. Cefixime 200 mg 12.5 10 2.5
Allergy Tab. Levo Cetirizine 5mg 3.5 2 1.5
Tab. Cetirizine Hcl 10 mg 2 1 1
Pain Killer,
Fever
Tab. Paracetamol 500 mg 1.2 1 0.2
Tab.Paracetamol 500 mg + Diclofenac
Sodium 50 mg
1.7 1 0.7
Antifungal Tab. Fluconazole 150 mg 17 10.5 6.5
Antihypertensive Tab. Atenolol 50 mg 2.29 2.1 0.14
Anti-infective
Cap. Amoxycillin 500 mg 7 6 1
Tab. Amoxycillin + Clauvinic Acid -
500mg +125 mg
15 15 0
Tab. Ofloxacin 200 mg 5.2 5 0.2
Tab. Ofloxacin + Ornidazole
( 200mg + 500mg)
9.8 7 2.8
Anti Helminthic Tab. Albendazole 400 mg 10 10 0
Laxatives Tab. Bisacodyl 10 mg 1 1 0
Source: Sample Survey
Note: Median Price- Actually charged price
Drug Pricing Components
Drug pricing components describe the various components included in the pricing of
drugs. According to Drug Price Control Order (DPCO), 2013, in pricing mechanism
the cost of drugs to the consumer it includes production cost, the costs of marketing
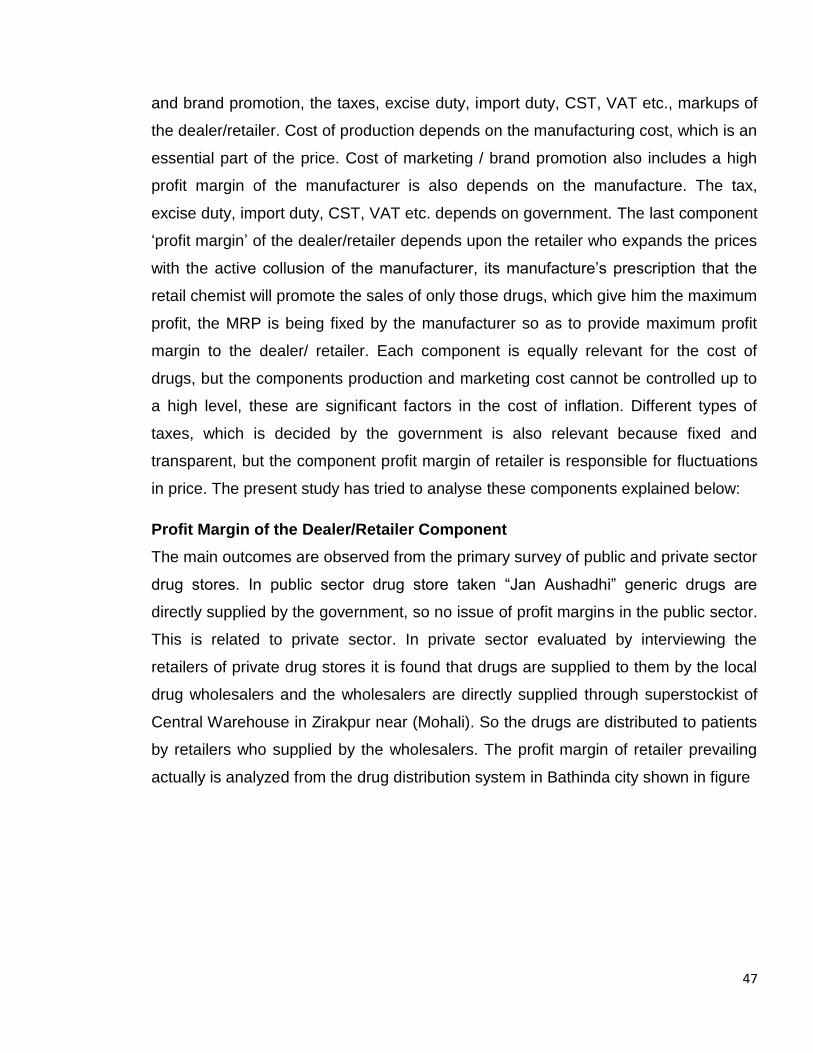
47
and brand promotion, the taxes, excise duty, import duty, CST, VAT etc., markups of
the dealer/retailer. Cost of production depends on the manufacturing cost, which is an
essential part of the price. Cost of marketing / brand promotion also includes a high
profit margin of the manufacturer is also depends on the manufacture. The tax,
excise duty, import duty, CST, VAT etc. depends on government. The last component
‘profit margin’ of the dealer/retailer depends upon the retailer who expands the prices
with the active collusion of the manufacturer, its manufacture’s prescription that the
retail chemist will promote the sales of only those drugs, which give him the maximum
profit, the MRP is being fixed by the manufacturer so as to provide maximum profit
margin to the dealer/ retailer. Each component is equally relevant for the cost of
drugs, but the components production and marketing cost cannot be controlled up to
a high level, these are significant factors in the cost of inflation. Different types of
taxes, which is decided by the government is also relevant because fixed and
transparent, but the component profit margin of retailer is responsible for fluctuations
in price. The present study has tried to analyse these components explained below:
Profit Margin of the Dealer/Retailer Component
The main outcomes are observed from the primary survey of public and private sector
drug stores. In public sector drug store taken “Jan Aushadhi” generic drugs are
directly supplied by the government, so no issue of profit margins in the public sector.
This is related to private sector. In private sector evaluated by interviewing the
retailers of private drug stores it is found that drugs are supplied to them by the local
drug wholesalers and the wholesalers are directly supplied through superstockist of
Central Warehouse in Zirakpur near (Mohali). So the drugs are distributed to patients
by retailers who supplied by the wholesalers. The profit margin of retailer prevailing
actually is analyzed from the drug distribution system in Bathinda city shown in figure
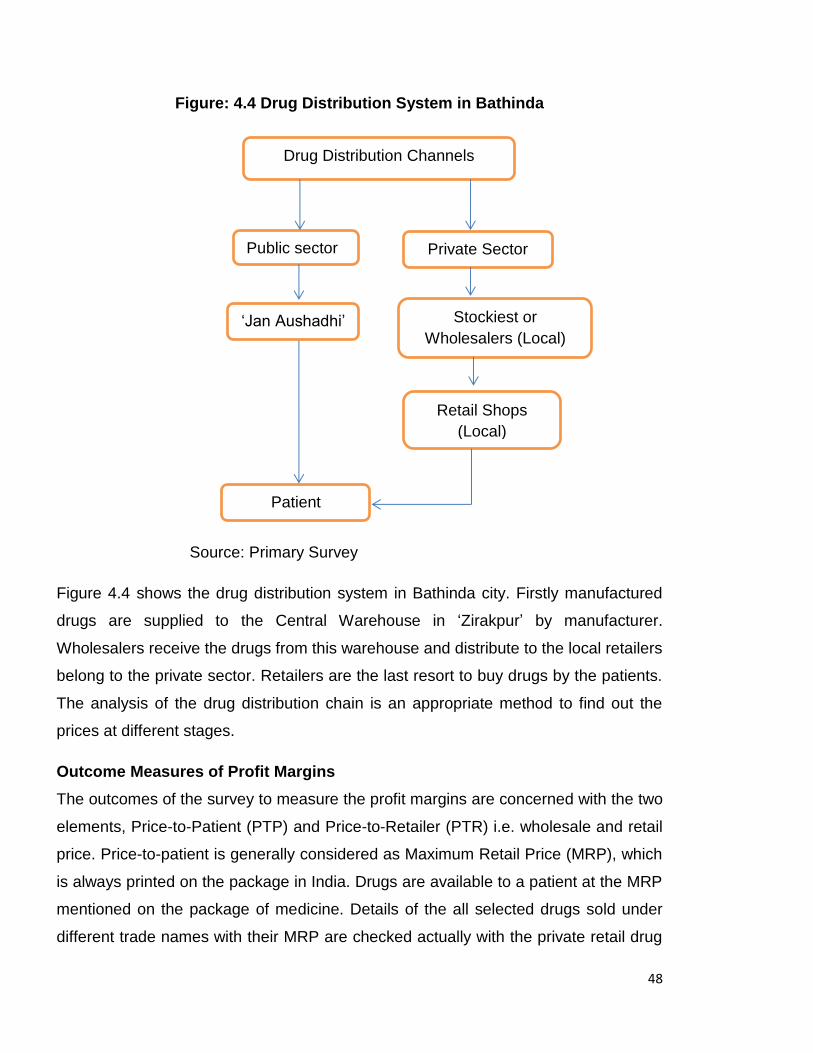
48
Figure: 4.4 Drug Distribution System in Bathinda
Source: Primary Survey
Figure 4.4 shows the drug distribution system in Bathinda city. Firstly manufactured
drugs are supplied to the Central Warehouse in ‘Zirakpur’ by manufacturer.
Wholesalers receive the drugs from this warehouse and distribute to the local retailers
belong to the private sector. Retailers are the last resort to buy drugs by the patients.
The analysis of the drug distribution chain is an appropriate method to find out the
prices at different stages.
Outcome Measures of Profit Margins
The outcomes of the survey to measure the profit margins are concerned with the two
elements, Price-to-Patient (PTP) and Price-to-Retailer (PTR) i.e. wholesale and retail
price. Price-to-patient is generally considered as Maximum Retail Price (MRP), which
is always printed on the package in India. Drugs are available to a patient at the MRP
mentioned on the package of medicine. Details of the all selected drugs sold under
different trade names with their MRP are checked actually with the private retail drug
Public sector Private Sector
Stockiest or Wholesalers (Local)
Retail Shops (Local)
Patient
Drug Distribution Channels
‘Jan Aushadhi’
49
stores (Chemist shop). On the other side ‘Price-to-Retailer’ (PTR) is the price at which
wholesaler (distributor) sells the product to the retailer this PTR this is asked from
wholesalers. The difference between these two is helpful for the calculation of retailer
mark-up of different drugs. These margins are calculated individually for all selected
drugs shown in the table:
In the public sector, just price to the patient is concerned because of at ‘Jan
Aushadhi’ drugs are directly supplied by government at the printed price, which is
very low as compared to branded-generic drugs of same name. There is no issue of
retail mark-up. The price to the patient is relevant at “Jan Aushadhi”. The issue
related to these two measures lies in private sector retail drug stores.
Table 4.9: Retailer Mark-Ups
Therapeutic class
Drug Name Brand Name
Manufacture Name
Price to
Ratiler MRP(Rs)
Mark-up
(Retail) (%)
Antacid
Tab. Pentaperazole 40 mg
Pantocip Cipla 1.16 8.35 619.83
Tab. Rantidine 150 mg
Rantax Cipla 0.4 1 150
Antibacterial
Tab. Cotrimoxazole S.S (Trimethoprim 80mg + Sulphamethoxazole 400mg)
Ciplin Ds Cipla 1.17 1.4 19.66
Tab. Levoflexine 250 mg
Lovolkem Alkem 1.45 4 175.86
Tab. Azithromycine 250mg
Azx 250 Ranbaxy 4.14 11.3 173.91
Tab. Ciprofloxacin Coated 250 mg
Floxip Abbott 0.9 3 233.33
Tab. Ciprofloxacin Coated 500mg
Ciprotas Intas 1.53 3.1 174.51
Tab. Cefixime 200 mg
Fexim-O Zydus 3.68 12.5 239.67
Contd…
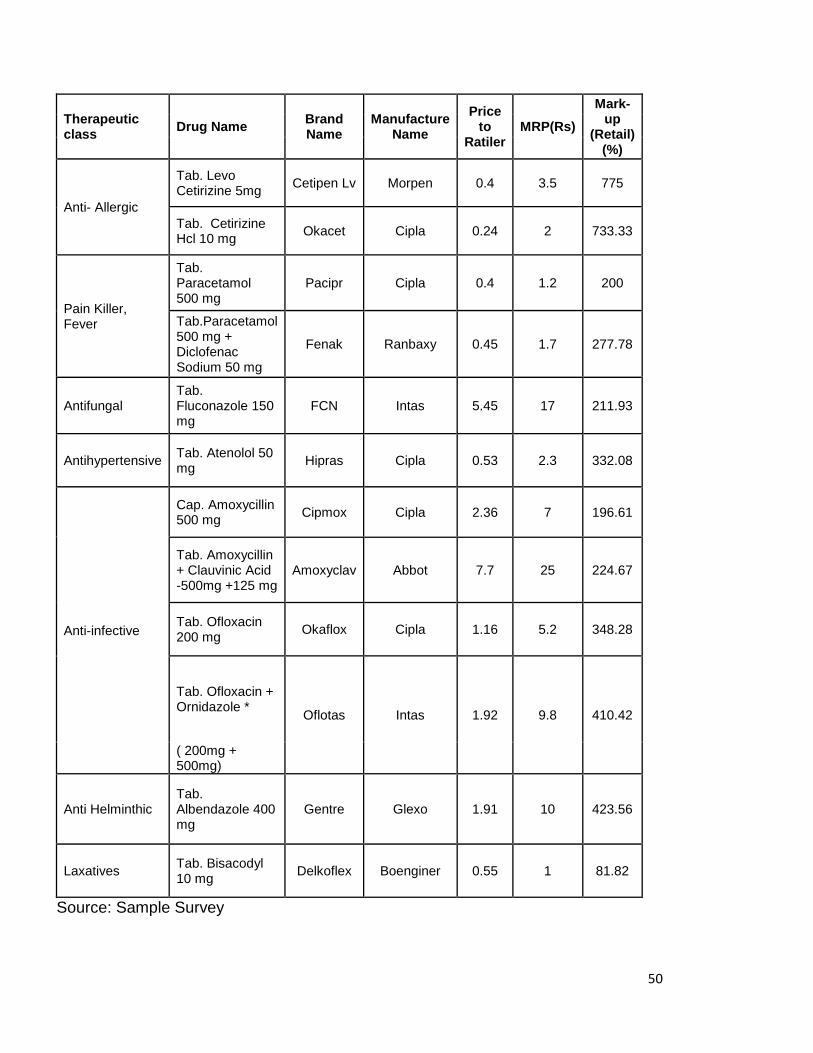
50
Therapeutic class
Drug Name Brand Name
Manufacture Name
Price to
Ratiler MRP(Rs)
Mark-up
(Retail) (%)
Anti- Allergic
Tab. Levo Cetirizine 5mg
Cetipen Lv Morpen 0.4 3.5 775
Tab. Cetirizine Hcl 10 mg
Okacet Cipla 0.24 2 733.33
Pain Killer, Fever
Tab. Paracetamol 500 mg
Pacipr Cipla 0.4 1.2 200
Tab.Paracetamol 500 mg + Diclofenac Sodium 50 mg
Fenak Ranbaxy 0.45 1.7 277.78
Antifungal Tab. Fluconazole 150 mg
FCN Intas 5.45 17 211.93
Antihypertensive Tab. Atenolol 50 mg
Hipras Cipla 0.53 2.3 332.08
Anti-infective
Cap. Amoxycillin 500 mg
Cipmox Cipla 2.36 7 196.61
Tab. Amoxycillin + Clauvinic Acid -500mg +125 mg
Amoxyclav Abbot 7.7 25 224.67
Tab. Ofloxacin 200 mg
Okaflox Cipla 1.16 5.2 348.28
Tab. Ofloxacin + Ornidazole *
Oflotas Intas 1.92 9.8 410.42
( 200mg + 500mg)
Anti Helminthic Tab. Albendazole 400 mg
Gentre Glexo 1.91 10 423.56
Laxatives Tab. Bisacodyl 10 mg
Delkoflex Boenginer 0.55 1 81.82
Source: Sample Survey
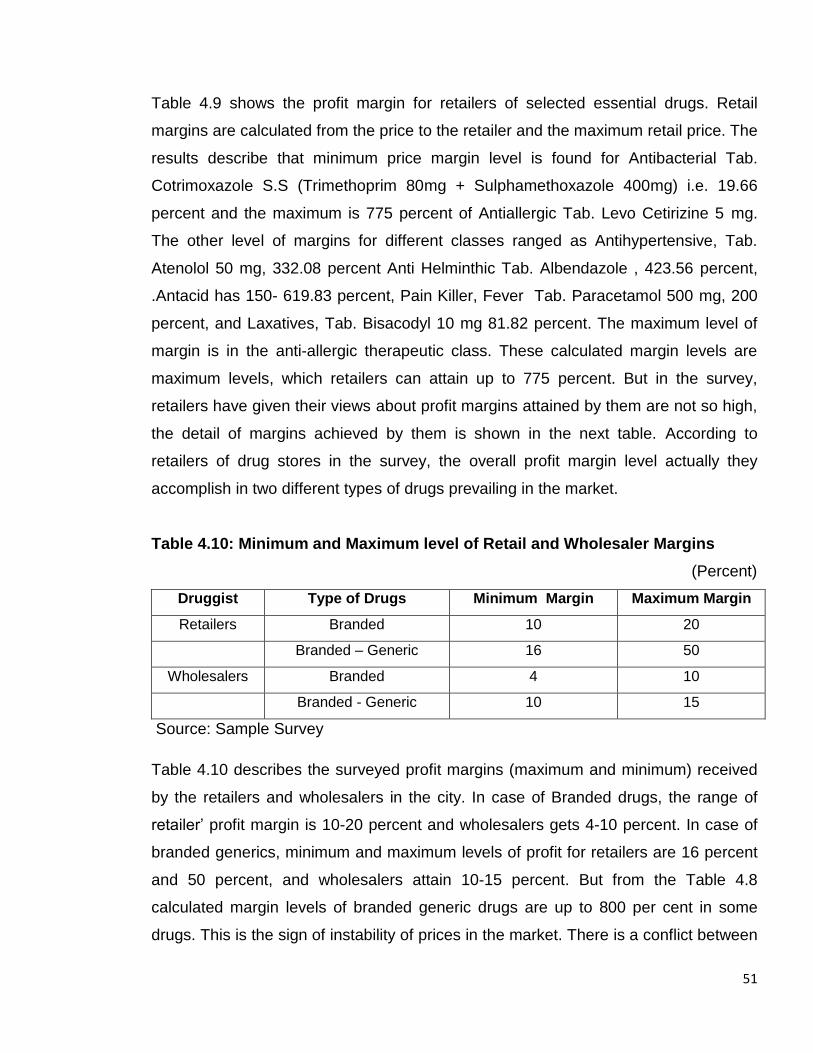
51
Table 4.9 shows the profit margin for retailers of selected essential drugs. Retail
margins are calculated from the price to the retailer and the maximum retail price. The
results describe that minimum price margin level is found for Antibacterial Tab.
Cotrimoxazole S.S (Trimethoprim 80mg + Sulphamethoxazole 400mg) i.e. 19.66
percent and the maximum is 775 percent of Antiallergic Tab. Levo Cetirizine 5 mg.
The other level of margins for different classes ranged as Antihypertensive, Tab.
Atenolol 50 mg, 332.08 percent Anti Helminthic Tab. Albendazole , 423.56 percent,
.Antacid has 150- 619.83 percent, Pain Killer, Fever Tab. Paracetamol 500 mg, 200
percent, and Laxatives, Tab. Bisacodyl 10 mg 81.82 percent. The maximum level of
margin is in the anti-allergic therapeutic class. These calculated margin levels are
maximum levels, which retailers can attain up to 775 percent. But in the survey,
retailers have given their views about profit margins attained by them are not so high,
the detail of margins achieved by them is shown in the next table. According to
retailers of drug stores in the survey, the overall profit margin level actually they
accomplish in two different types of drugs prevailing in the market.
Table 4.10: Minimum and Maximum level of Retail and Wholesaler Margins
(Percent)
Druggist Type of Drugs Minimum Margin Maximum Margin
Retailers Branded 10 20
Branded – Generic 16 50
Wholesalers Branded 4 10
Branded - Generic 10 15
Source: Sample Survey
Table 4.10 describes the surveyed profit margins (maximum and minimum) received
by the retailers and wholesalers in the city. In case of Branded drugs, the range of
retailer’ profit margin is 10-20 percent and wholesalers gets 4-10 percent. In case of
branded generics, minimum and maximum levels of profit for retailers are 16 percent
and 50 percent, and wholesalers attain 10-15 percent. But from the Table 4.8
calculated margin levels of branded generic drugs are up to 800 per cent in some
drugs. This is the sign of instability of prices in the market. There is a conflict between
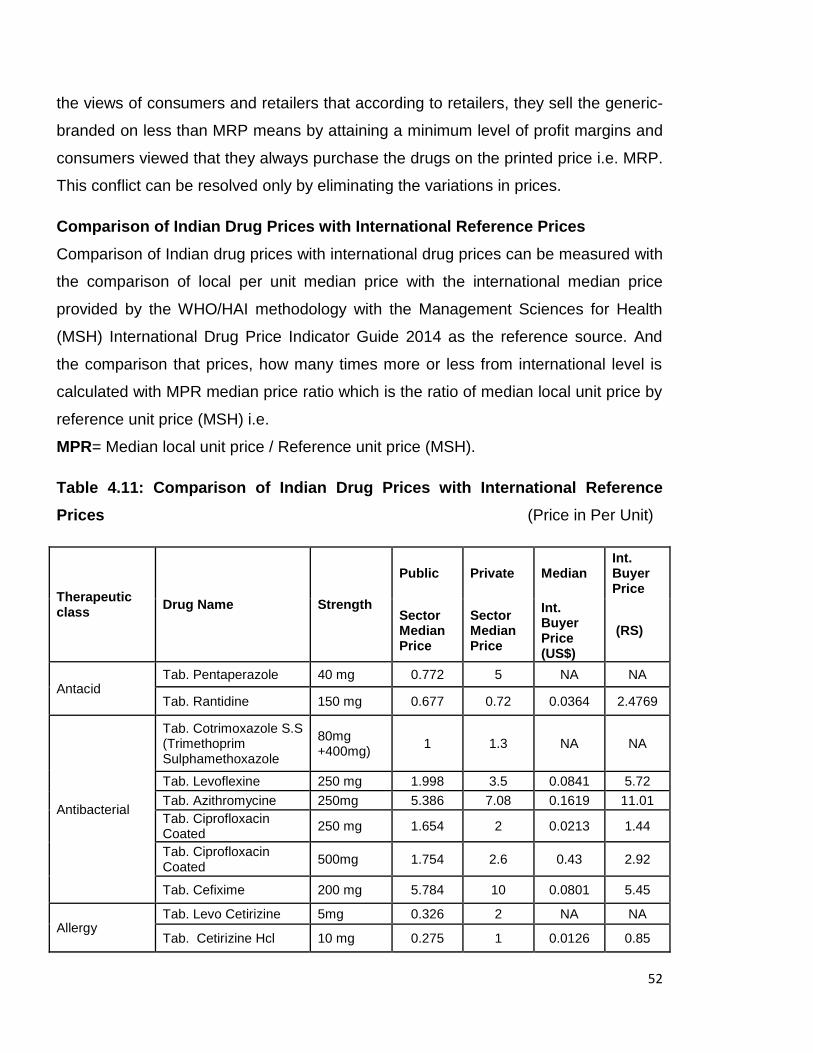
52
the views of consumers and retailers that according to retailers, they sell the generic-
branded on less than MRP means by attaining a minimum level of profit margins and
consumers viewed that they always purchase the drugs on the printed price i.e. MRP.
This conflict can be resolved only by eliminating the variations in prices.
Comparison of Indian Drug Prices with International Reference Prices
Comparison of Indian drug prices with international drug prices can be measured with
the comparison of local per unit median price with the international median price
provided by the WHO/HAI methodology with the Management Sciences for Health
(MSH) International Drug Price Indicator Guide 2014 as the reference source. And
the comparison that prices, how many times more or less from international level is
calculated with MPR median price ratio which is the ratio of median local unit price by
reference unit price (MSH) i.e.
MPR= Median local unit price / Reference unit price (MSH).
Table 4.11: Comparison of Indian Drug Prices with International Reference
Prices (Price in Per Unit)
Therapeutic class
Drug Name Strength
Public Private Median Int. Buyer Price
Sector Median Price
Sector Median Price
Int. Buyer Price (US$)
(RS)
Antacid Tab. Pentaperazole 40 mg 0.772 5 NA NA
Tab. Rantidine 150 mg 0.677 0.72 0.0364 2.4769
Antibacterial
Tab. Cotrimoxazole S.S (Trimethoprim Sulphamethoxazole
80mg +400mg)
1 1.3 NA NA
Tab. Levoflexine 250 mg 1.998 3.5 0.0841 5.72
Tab. Azithromycine 250mg 5.386 7.08 0.1619 11.01 Tab. Ciprofloxacin Coated
250 mg 1.654 2 0.0213 1.44
Tab. Ciprofloxacin Coated
500mg 1.754 2.6 0.43 2.92
Tab. Cefixime 200 mg 5.784 10 0.0801 5.45
Allergy Tab. Levo Cetirizine 5mg 0.326 2 NA NA
Tab. Cetirizine Hcl 10 mg 0.275 1 0.0126 0.85
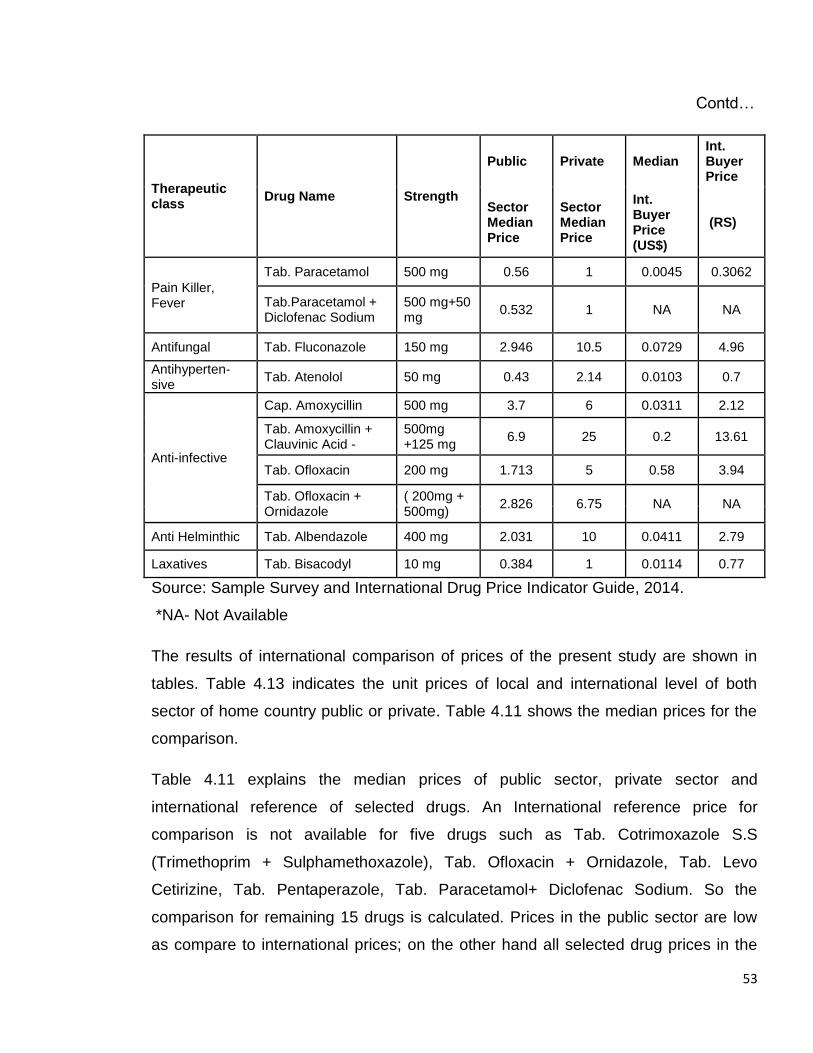
53
Contd…
Therapeutic class
Drug Name Strength
Public Private Median Int. Buyer Price
Sector Median Price
Sector Median Price
Int. Buyer Price (US$)
(RS)
Pain Killer, Fever
Tab. Paracetamol 500 mg 0.56 1 0.0045 0.3062
Tab.Paracetamol + Diclofenac Sodium
500 mg+50 mg
0.532 1 NA NA
Antifungal Tab. Fluconazole 150 mg 2.946 10.5 0.0729 4.96
Antihyperten-sive
Tab. Atenolol 50 mg 0.43 2.14 0.0103 0.7
Anti-infective
Cap. Amoxycillin 500 mg 3.7 6 0.0311 2.12
Tab. Amoxycillin + Clauvinic Acid -
500mg +125 mg
6.9 25 0.2 13.61
Tab. Ofloxacin 200 mg 1.713 5 0.58 3.94
Tab. Ofloxacin + Ornidazole
( 200mg + 500mg)
2.826 6.75 NA NA
Anti Helminthic Tab. Albendazole 400 mg 2.031 10 0.0411 2.79
Laxatives Tab. Bisacodyl 10 mg 0.384 1 0.0114 0.77
Source: Sample Survey and International Drug Price Indicator Guide, 2014.
*NA- Not Available
The results of international comparison of prices of the present study are shown in
tables. Table 4.13 indicates the unit prices of local and international level of both
sector of home country public or private. Table 4.11 shows the median prices for the
comparison.
Table 4.11 explains the median prices of public sector, private sector and
international reference of selected drugs. An International reference price for
comparison is not available for five drugs such as Tab. Cotrimoxazole S.S
(Trimethoprim + Sulphamethoxazole), Tab. Ofloxacin + Ornidazole, Tab. Levo
Cetirizine, Tab. Pentaperazole, Tab. Paracetamol+ Diclofenac Sodium. So the
comparison for remaining 15 drugs is calculated. Prices in the public sector are low
as compare to international prices; on the other hand all selected drug prices in the
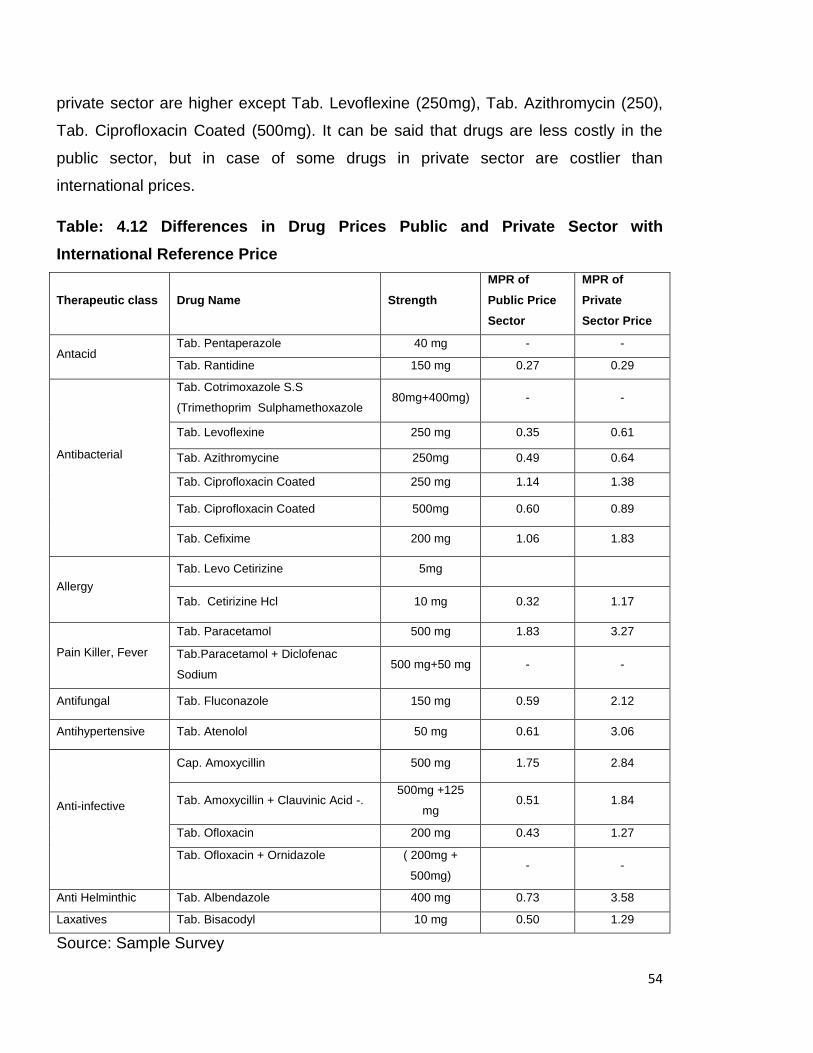
54
private sector are higher except Tab. Levoflexine (250mg), Tab. Azithromycin (250),
Tab. Ciprofloxacin Coated (500mg). It can be said that drugs are less costly in the
public sector, but in case of some drugs in private sector are costlier than
international prices.
Table: 4.12 Differences in Drug Prices Public and Private Sector with
International Reference Price
Therapeutic class Drug Name Strength
MPR of
Public Price
Sector
MPR of
Private
Sector Price
Antacid Tab. Pentaperazole 40 mg - -
Tab. Rantidine 150 mg 0.27 0.29
Antibacterial
Tab. Cotrimoxazole S.S
(Trimethoprim Sulphamethoxazole 80mg+400mg) - -
Tab. Levoflexine 250 mg 0.35 0.61
Tab. Azithromycine 250mg 0.49 0.64
Tab. Ciprofloxacin Coated 250 mg 1.14 1.38
Tab. Ciprofloxacin Coated 500mg 0.60 0.89
Tab. Cefixime 200 mg 1.06 1.83
Allergy
Tab. Levo Cetirizine 5mg
Tab. Cetirizine Hcl 10 mg 0.32 1.17
Pain Killer, Fever
Tab. Paracetamol 500 mg 1.83 3.27
Tab.Paracetamol + Diclofenac
Sodium 500 mg+50 mg - -
Antifungal Tab. Fluconazole 150 mg 0.59 2.12
Antihypertensive Tab. Atenolol 50 mg 0.61 3.06
Anti-infective
Cap. Amoxycillin 500 mg 1.75 2.84
Tab. Amoxycillin + Clauvinic Acid -. 500mg +125
mg 0.51 1.84
Tab. Ofloxacin 200 mg 0.43 1.27
Tab. Ofloxacin + Ornidazole
( 200mg +
500mg) - -
Anti Helminthic Tab. Albendazole 400 mg 0.73 3.58
Laxatives Tab. Bisacodyl 10 mg 0.50 1.29
Source: Sample Survey
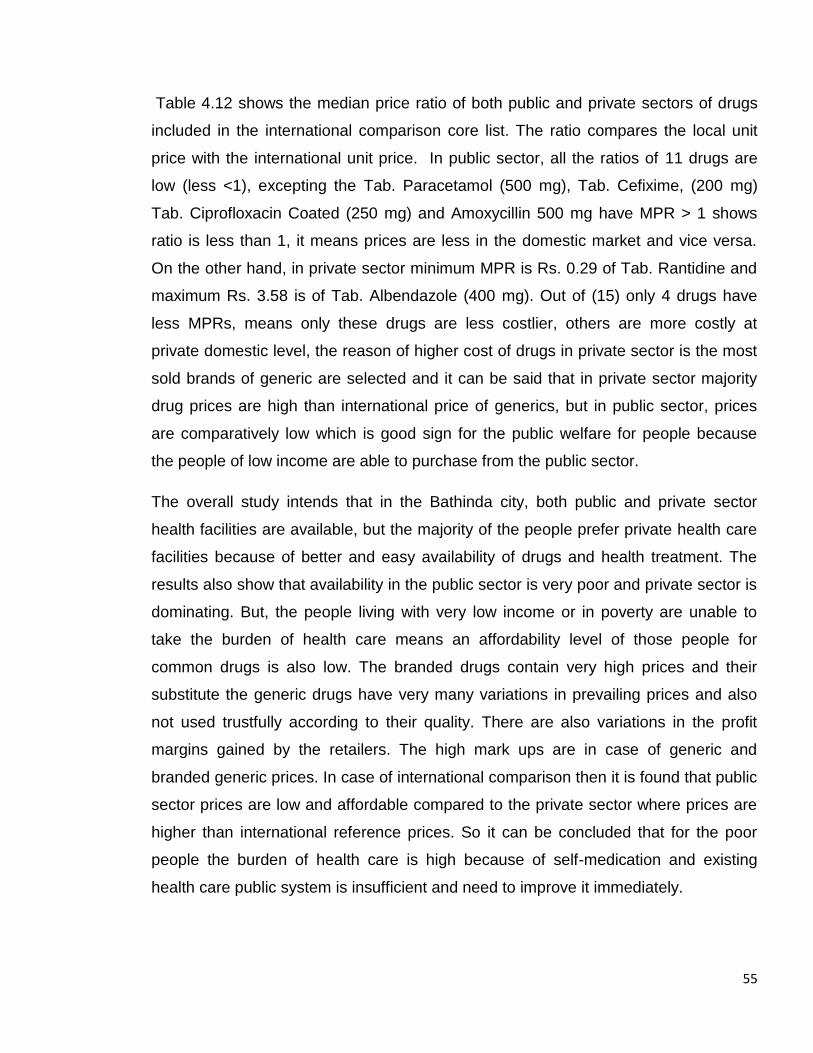
55
Table 4.12 shows the median price ratio of both public and private sectors of drugs
included in the international comparison core list. The ratio compares the local unit
price with the international unit price. In public sector, all the ratios of 11 drugs are
low (less <1), excepting the Tab. Paracetamol (500 mg), Tab. Cefixime, (200 mg)
Tab. Ciprofloxacin Coated (250 mg) and Amoxycillin 500 mg have MPR > 1 shows
ratio is less than 1, it means prices are less in the domestic market and vice versa.
On the other hand, in private sector minimum MPR is Rs. 0.29 of Tab. Rantidine and
maximum Rs. 3.58 is of Tab. Albendazole (400 mg). Out of (15) only 4 drugs have
less MPRs, means only these drugs are less costlier, others are more costly at
private domestic level, the reason of higher cost of drugs in private sector is the most
sold brands of generic are selected and it can be said that in private sector majority
drug prices are high than international price of generics, but in public sector, prices
are comparatively low which is good sign for the public welfare for people because
the people of low income are able to purchase from the public sector.
The overall study intends that in the Bathinda city, both public and private sector
health facilities are available, but the majority of the people prefer private health care
facilities because of better and easy availability of drugs and health treatment. The
results also show that availability in the public sector is very poor and private sector is
dominating. But, the people living with very low income or in poverty are unable to
take the burden of health care means an affordability level of those people for
common drugs is also low. The branded drugs contain very high prices and their
substitute the generic drugs have very many variations in prevailing prices and also
not used trustfully according to their quality. There are also variations in the profit
margins gained by the retailers. The high mark ups are in case of generic and
branded generic prices. In case of international comparison then it is found that public
sector prices are low and affordable compared to the private sector where prices are
higher than international reference prices. So it can be concluded that for the poor
people the burden of health care is high because of self-medication and existing
health care public system is insufficient and need to improve it immediately.
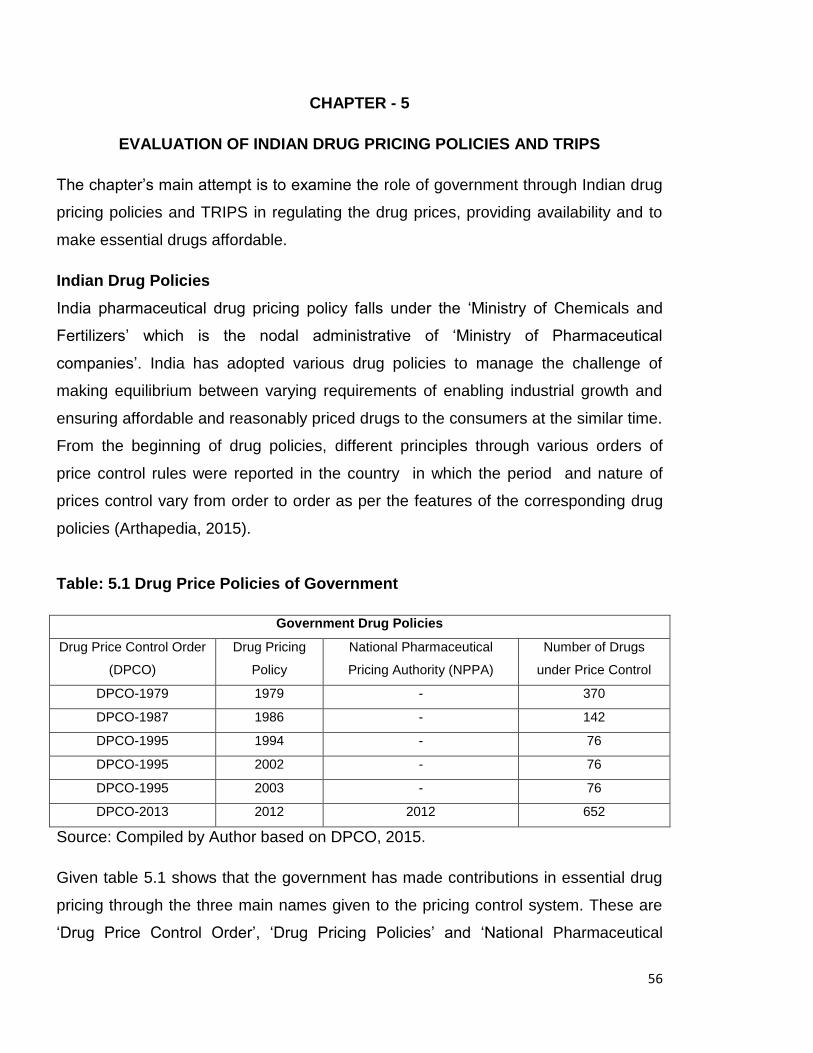
56
CHAPTER - 5
EVALUATION OF INDIAN DRUG PRICING POLICIES AND TRIPS
The chapter’s main attempt is to examine the role of government through Indian drug
pricing policies and TRIPS in regulating the drug prices, providing availability and to
make essential drugs affordable.
Indian Drug Policies
India pharmaceutical drug pricing policy falls under the ‘Ministry of Chemicals and
Fertilizers’ which is the nodal administrative of ‘Ministry of Pharmaceutical
companies’. India has adopted various drug policies to manage the challenge of
making equilibrium between varying requirements of enabling industrial growth and
ensuring affordable and reasonably priced drugs to the consumers at the similar time.
From the beginning of drug policies, different principles through various orders of
price control rules were reported in the country in which the period and nature of
prices control vary from order to order as per the features of the corresponding drug
policies (Arthapedia, 2015).
Table: 5.1 Drug Price Policies of Government
Government Drug Policies
Drug Price Control Order
(DPCO)
Drug Pricing
Policy
National Pharmaceutical
Pricing Authority (NPPA)
Number of Drugs
under Price Control
DPCO-1979 1979 - 370
DPCO-1987 1986 - 142
DPCO-1995 1994 - 76
DPCO-1995 2002 - 76
DPCO-1995 2003 - 76
DPCO-2013 2012 2012 652
Source: Compiled by Author based on DPCO, 2015.
Given table 5.1 shows that the government has made contributions in essential drug
pricing through the three main names given to the pricing control system. These are
‘Drug Price Control Order’, ‘Drug Pricing Policies’ and ‘National Pharmaceutical
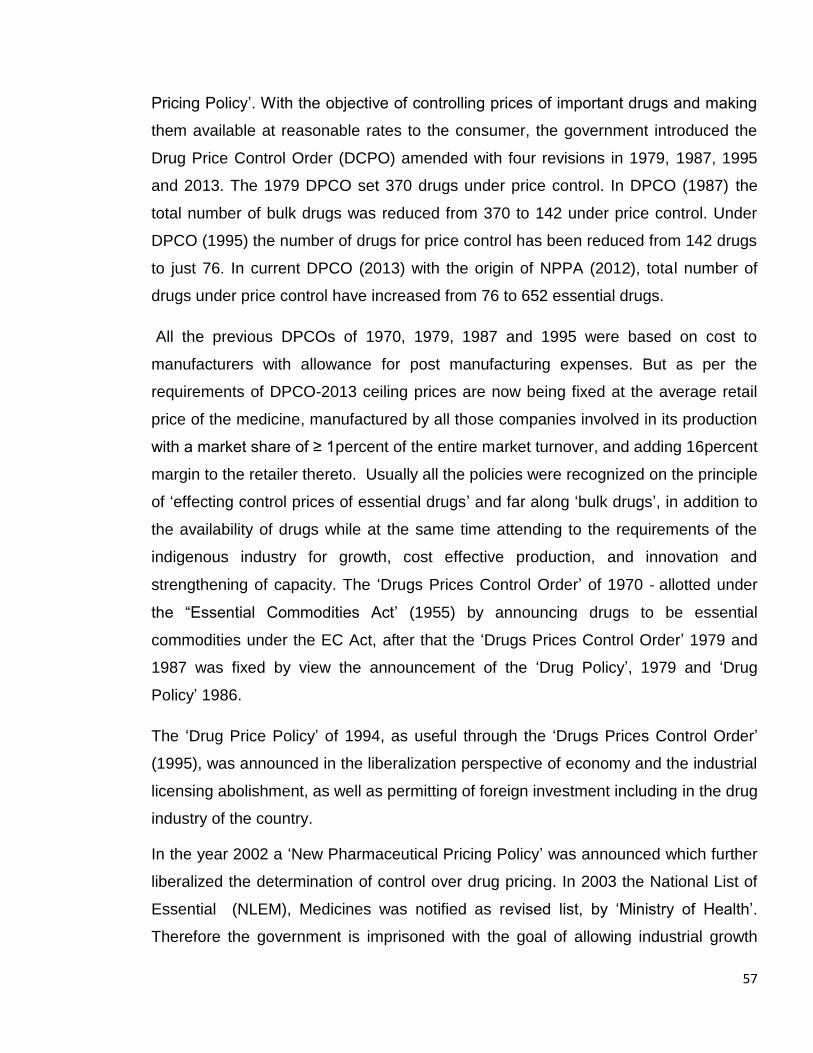
57
Pricing Policy’. With the objective of controlling prices of important drugs and making
them available at reasonable rates to the consumer, the government introduced the
Drug Price Control Order (DCPO) amended with four revisions in 1979, 1987, 1995
and 2013. The 1979 DPCO set 370 drugs under price control. In DPCO (1987) the
total number of bulk drugs was reduced from 370 to 142 under price control. Under
DPCO (1995) the number of drugs for price control has been reduced from 142 drugs
to just 76. In current DPCO (2013) with the origin of NPPA (2012), total number of
drugs under price control have increased from 76 to 652 essential drugs.
All the previous DPCOs of 1970, 1979, 1987 and 1995 were based on cost to
manufacturers with allowance for post manufacturing expenses. But as per the
requirements of DPCO-2013 ceiling prices are now being fixed at the average retail
price of the medicine, manufactured by all those companies involved in its production
with a market share of ≥ 1percent of the entire market turnover, and adding 16percent
margin to the retailer thereto. Usually all the policies were recognized on the principle
of ‘effecting control prices of essential drugs’ and far along ‘bulk drugs’, in addition to
the availability of drugs while at the same time attending to the requirements of the
indigenous industry for growth, cost effective production, and innovation and
strengthening of capacity. The ‘Drugs Prices Control Order’ of 1970 ‐ allotted under
the “Essential Commodities Act’ (1955) by announcing drugs to be essential
commodities under the EC Act, after that the ‘Drugs Prices Control Order’ 1979 and
1987 was fixed by view the announcement of the ‘Drug Policy’, 1979 and ‘Drug
Policy’ 1986.
The ‘Drug Price Policy’ of 1994, as useful through the ‘Drugs Prices Control Order’
(1995), was announced in the liberalization perspective of economy and the industrial
licensing abolishment, as well as permitting of foreign investment including in the drug
industry of the country.
In the year 2002 a ‘New Pharmaceutical Pricing Policy’ was announced which further
liberalized the determination of control over drug pricing. In 2003 the National List of
Essential (NLEM), Medicines was notified as revised list, by ‘Ministry of Health’.
Therefore the government is imprisoned with the goal of allowing industrial growth
58
with connected socio‐economic benefits along with balancing the declared objective
of making available essential medicines including providing better health care at
reasonable prices to all.
Consequently, the Government pronounced the National Pharmaceuticals Pricing
Policy, (NPPP 2012) by replacing the drug policy enunciated in September, 1994. To
come across the challenges about the country’s requirements for safe and quality
drugs at affordable prices. by the competitive international pharmaceutical industry in
a globalized economic environment. The ‘National Pharmaceuticals Pricing Policy’
(2012) has a new process for determining the ceiling price, termed as market-based
pricing mechanism as applied through the Drugs Prices Control Order 2013, its result
would be a reduction in prices of certain top brands.
National Pharmaceutical Pricing Authority (NPPA) – 2012
A very high ‘Out of Pocket Expenditure’ for drugs in India, measured at 85.88 in
2013 by the World Bank. The Government has to regulate the prices of at least the
essential medicines to ensure satisfactory access to affordable essential medicines
for the general public.Through the ‘National Pharmaceutical Pricing Authority’ (NPPA)
the Government tries to make insure the following objectives:
1) Adequate Availability of all essential drugs,
2) Reasonably Affordability for common man,
Therefore, while framing any drug pricing policy an equilibrium between ‘affordability’
and ‘availability’ of drugs is of critical importance,
Implemented provisions of ‘Drug Price Control Order’ (DPCO) 2013
Latest DPCO 2013 authorizes the National Pharmaceutical Pricing Authority (NPPA)
to control prices of essential drugs. According to new DPCO 2013, entirely dosages
and strengths identified in the National List of Essential Medicines (NLEM) will be
under price control.
Para 2(i) of the DPCO 2013 explains the term "Formulation as a drug processed out
of or containing one or more drugs with or without the use of any pharmaceutical aids,
for internal or external use for or in the diagnosis, treatment, mitigation or prevention
of disease".
59
"Scheduled formulation has been defined as any formulation, included in the First
Schedule whether referred to by generic versions or brand name".
"Nonscheduled formulation means a formulation, the strengths and dosage of which
are not specified in the First Schedule".
Pricing of scheduled formulation:
Para 4 of the DPCO 2013 provides a formula for the calculation of ceiling price of a
scheduled formulation as follows –
Step1. Calculation of Average Price to Retailer of the scheduled formulation i.e. P(s)
shall be calculated as below:
Average Price to retailer, P(S) = Sum*/ Total**
* “Sum of prices to retailer of all the brands and generic versions of the medicine
having market share more than or equal to one percent of the total market turnover
on the basis of moving annual turnover of that medicine” /
** “Total number of such brands and generic versions of the medicine having market
share more than or equal to one percent of total market turnover on the basis of
moving annual turnover for that medicine”.
Step2. Calculation of the ceiling price of the scheduled formulation, i.e. P(c) as below:
P(c) = P(s)* (1+M/100),
Where P(s) = Average Price to Retailer for the same strength and dosage of the
medicine as calculated in step1 above**.
M = percent Margin to retailers and its value =16.
Calculation of actual prices, according to DPCO, pricing of surveyed drugs:
MRP= Average Price to retailers, P(S) + 16 percent margin of retailer.
Table: 5.2 Actual Prices according to (DPCO 2013) ( Rs.)
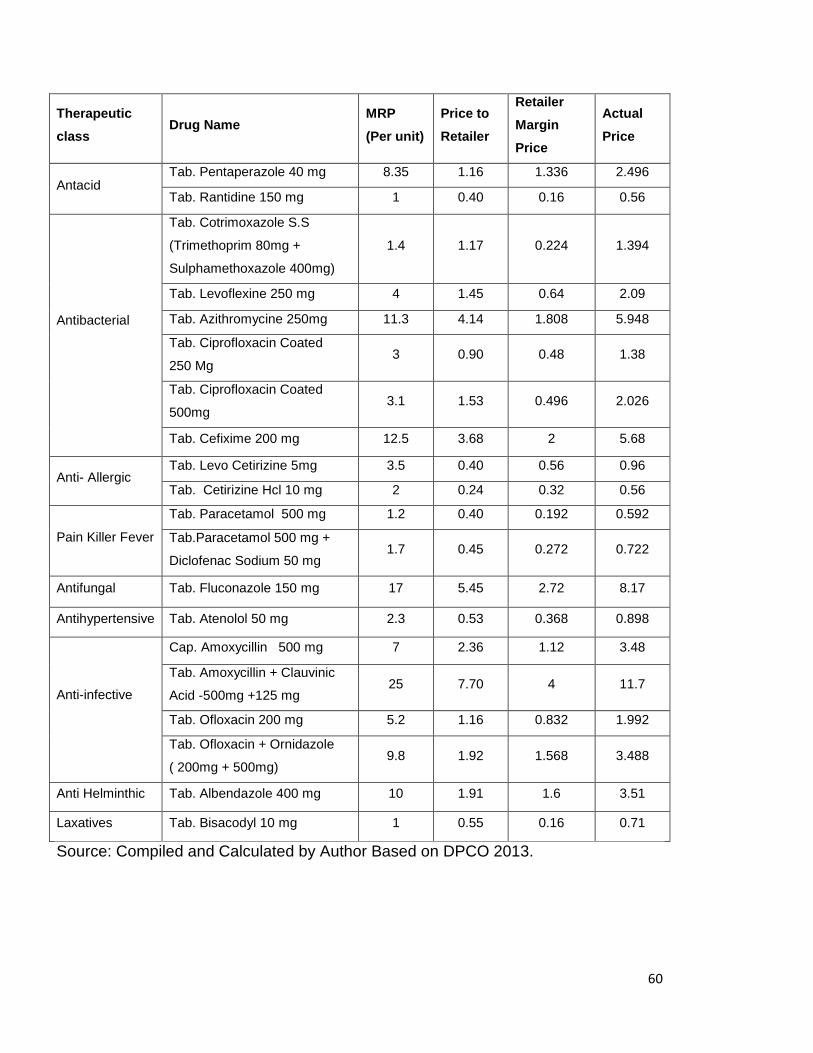
60
Therapeutic
class Drug Name
MRP
(Per unit)
Price to
Retailer
Retailer
Margin
Price
Actual
Price
Antacid Tab. Pentaperazole 40 mg 8.35 1.16 1.336 2.496
Tab. Rantidine 150 mg 1 0.40 0.16 0.56
Antibacterial
Tab. Cotrimoxazole S.S
(Trimethoprim 80mg +
Sulphamethoxazole 400mg)
1.4 1.17 0.224 1.394
Tab. Levoflexine 250 mg 4 1.45 0.64 2.09
Tab. Azithromycine 250mg 11.3 4.14 1.808 5.948
Tab. Ciprofloxacin Coated
250 Mg 3 0.90 0.48 1.38
Tab. Ciprofloxacin Coated
500mg 3.1 1.53 0.496 2.026
Tab. Cefixime 200 mg 12.5 3.68 2 5.68
Anti- Allergic Tab. Levo Cetirizine 5mg 3.5 0.40 0.56 0.96
Tab. Cetirizine Hcl 10 mg 2 0.24 0.32 0.56
Pain Killer Fever
Tab. Paracetamol 500 mg 1.2 0.40 0.192 0.592
Tab.Paracetamol 500 mg +
Diclofenac Sodium 50 mg 1.7 0.45 0.272 0.722
Antifungal Tab. Fluconazole 150 mg 17 5.45 2.72 8.17
Antihypertensive Tab. Atenolol 50 mg 2.3 0.53 0.368 0.898
Anti-infective
Cap. Amoxycillin 500 mg 7 2.36 1.12 3.48
Tab. Amoxycillin + Clauvinic
Acid -500mg +125 mg 25 7.70 4 11.7
Tab. Ofloxacin 200 mg 5.2 1.16 0.832 1.992
Tab. Ofloxacin + Ornidazole
( 200mg + 500mg) 9.8 1.92 1.568 3.488
Anti Helminthic Tab. Albendazole 400 mg 10 1.91 1.6 3.51
Laxatives Tab. Bisacodyl 10 mg 1 0.55 0.16 0.71
Source: Compiled and Calculated by Author Based on DPCO 2013.
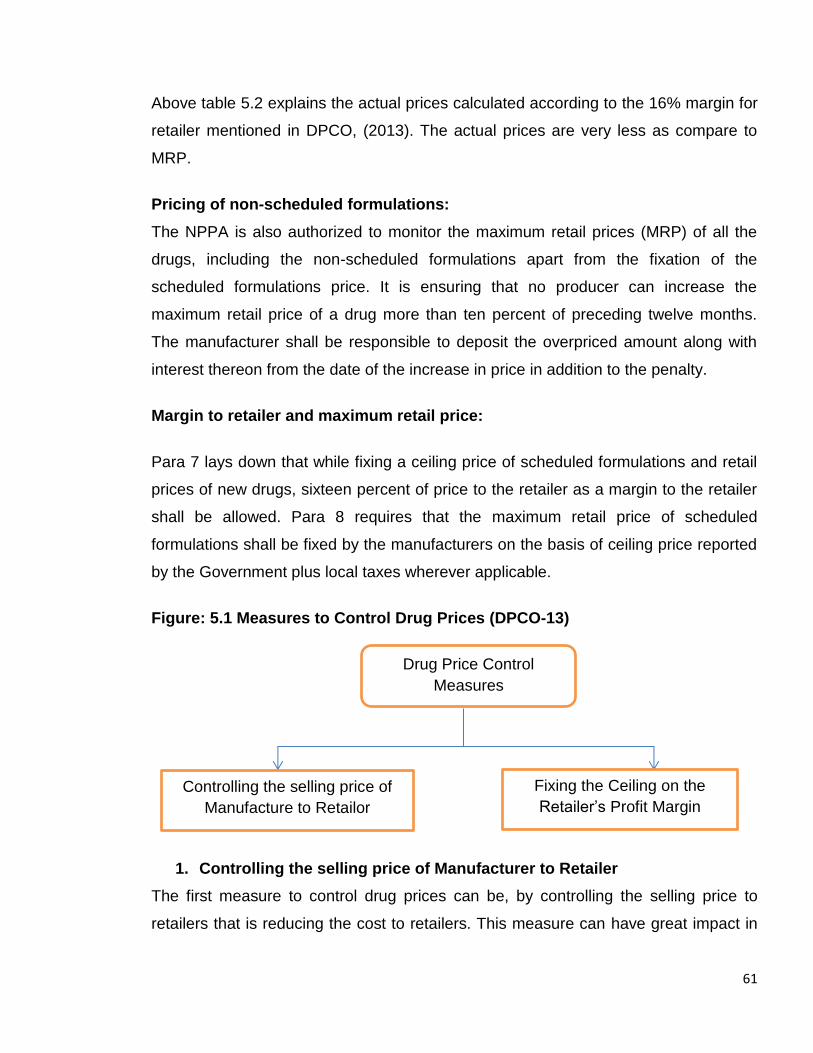
61
Above table 5.2 explains the actual prices calculated according to the 16% margin for
retailer mentioned in DPCO, (2013). The actual prices are very less as compare to
MRP.
Pricing of non-scheduled formulations:
The NPPA is also authorized to monitor the maximum retail prices (MRP) of all the
drugs, including the non-scheduled formulations apart from the fixation of the
scheduled formulations price. It is ensuring that no producer can increase the
maximum retail price of a drug more than ten percent of preceding twelve months.
The manufacturer shall be responsible to deposit the overpriced amount along with
interest thereon from the date of the increase in price in addition to the penalty.
Margin to retailer and maximum retail price:
Para 7 lays down that while fixing a ceiling price of scheduled formulations and retail
prices of new drugs, sixteen percent of price to the retailer as a margin to the retailer
shall be allowed. Para 8 requires that the maximum retail price of scheduled
formulations shall be fixed by the manufacturers on the basis of ceiling price reported
by the Government plus local taxes wherever applicable.
Figure: 5.1 Measures to Control Drug Prices (DPCO-13)
1. Controlling the selling price of Manufacturer to Retailer
The first measure to control drug prices can be, by controlling the selling price to
retailers that is reducing the cost to retailers. This measure can have great impact in
Drug Price Control Measures
(DPCO-2013)
Controlling the selling price of Manufacture to Retailor
Fixing the Ceiling on the Retailer’s Profit Margin
62
case of earlier cost based pricing. Now the drug price control policy is following the
Marke Based Pricing (MBP) by the government, which works out on the basis of
average of prices set by manufactures with 1percent or more of the market share.
That may turn out to be the average of the highest selling and costly brands rather
than the cheaper brands. In any case it does not force the manufacturer to reduce the
cost of production, overheads or his profits. This measure may not yield any
substantial benefits to consumers.
2. Fixing the Ceiling on the Retailer’s Profit Margin
Second price control measure, i.e. ceiling on retailer’s profit margin would be fixed.
Retail selling price is prospective to have a key impact. For excessive drug prices this
factor has been considered the single most significant factor responsible. Up to
nowadays the MRP was being fixed by the manufactures who were inflating the MRP
grossly up to 400-500percent in some cases. Capping on the MRP has the potential
to reduce the costs drastically.
TRIPS, Pharmaceuticals and India: An Overview
Generally, innovations can be protected through privacy, or through patents. In the
pharmaceutical sector, it is patent that are specifically crucial in appropriating the
returns to R & D. (Levin et al, 1987). The reason for the patent requirement is, once
the inventor, discovered a new drug produced through overlong and relatively
exclusive afford, R & D processes, capital, and the time involved is often negligible.
But, patents do not prevent competition from other substitutes of different therapeutic
that treat the same disease condition. Certainly, rare patented drugs have no
operative substitutes and this affects innovator firm’s strategies on initial prices. (Lu
and Comanor, 1998). Market size is well thought-out a significant factor of generic
entry that the patent system has been considered as a risk- device for risk smoothing,
the more effective a product is in terms of generating revenue to the original firm, the
more prospective it is to attract generic competition on expiry of the patent; equator,
the less successful products see profits sustained for a longer time (Hudson, 2000).
Patent system act as a social policy tool which provides the ‘legal patent owner to
prevent’ others from production, using or selling, importing or offering for sale the
63
new, patented drugs for a restricted period of time. Generally Trade Related
Intellectual Property Rights (TRIPS), constitutes 20-year period of a patent starts from
the time when application for patent has been filed, but in the case of pharmaceutical
products, which are exposed to lengthy procedures that verify safety and efficacy, the
effective patent lifetime might be only an average of 11 or 12 years.
According to the United Nations, a patent is a legally enforceable right, granted by a
country’s government to an inventor. A patent prevents others from producing, selling
or using a patented product or from utilizing a patented method or procedure. TRIPS
cover mainly seven different types of intellectual property rights as Trademarks,
Industrial designs, Geographical indications, Copyright, Integrated circuits, Trade
secrets, and Patents.
As of currently, India has a product patent regime regarding pharmaceutical products.
The first patent system was introduced in 1856, which gave special opportunity
entirely for the inventor was established which conferred the sole use and selling of
invention for 14 years. This act was substituted by Invention and Design Act, 1911. In
1930 and 1948 there were some major amendments in the similar act, a patents
enquiry committee appointed by the Government of India under Dr. Tek Chand, the
report submitted by the committee in 1953. In India patent system was governed by
the Patents Act 1970. The Indian Act 1970 has not shown efficacy for
pharmaceuticals as there are obligation of an artificially low royalty ceiling on
compulsory license and unavailability of product patent for pharmaceuticals. This act
recognizes only process patent in pharmaceutical and agro-chemicals, although in all
fields by the WTO agreement requires both process and product patents. (Agarwal,
2001).
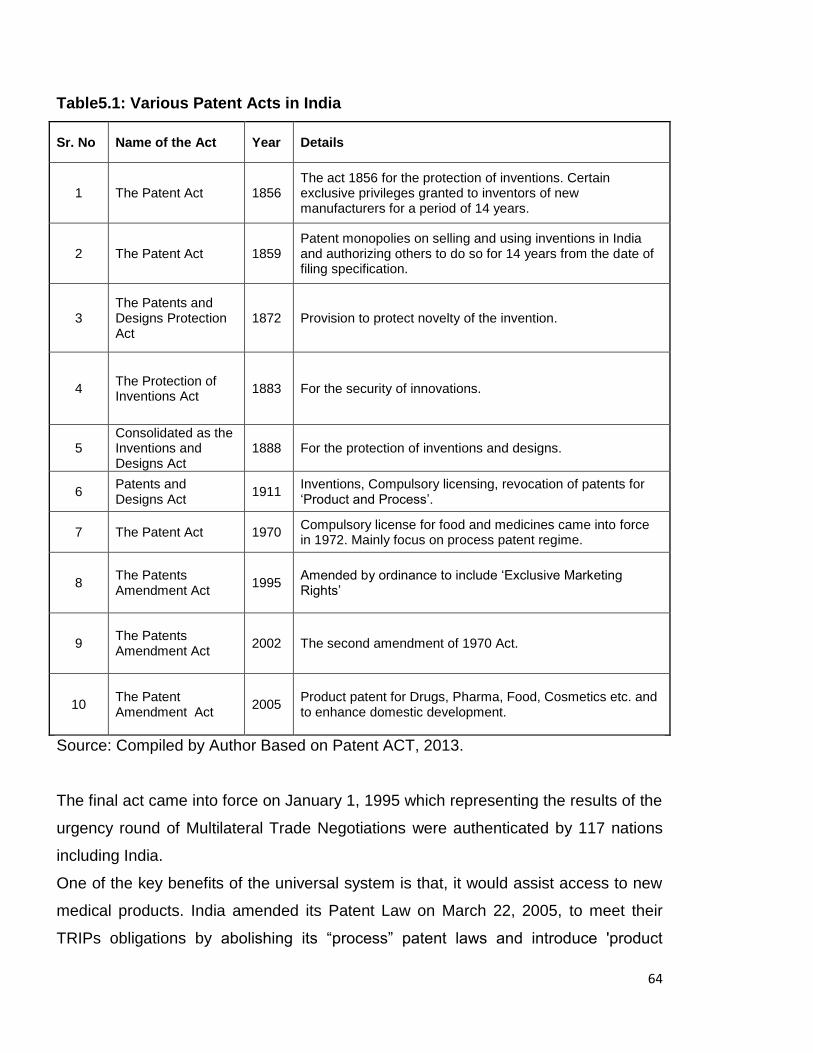
64
Table5.1: Various Patent Acts in India
Sr. No Name of the Act Year Details
1 The Patent Act 1856 The act 1856 for the protection of inventions. Certain exclusive privileges granted to inventors of new manufacturers for a period of 14 years.
2 The Patent Act 1859 Patent monopolies on selling and using inventions in India and authorizing others to do so for 14 years from the date of filing specification.
3 The Patents and Designs Protection Act
1872 Provision to protect novelty of the invention.
4 The Protection of Inventions Act
1883 For the security of innovations.
5 Consolidated as the Inventions and Designs Act
1888 For the protection of inventions and designs.
6 Patents and Designs Act
1911 Inventions, Compulsory licensing, revocation of patents for ‘Product and Process’.
7 The Patent Act 1970 Compulsory license for food and medicines came into force in 1972. Mainly focus on process patent regime.
8 The Patents Amendment Act
1995 Amended by ordinance to include ‘Exclusive Marketing Rights’
9 The Patents Amendment Act
2002 The second amendment of 1970 Act.
10 The Patent Amendment Act
2005 Product patent for Drugs, Pharma, Food, Cosmetics etc. and to enhance domestic development.
Source: Compiled by Author Based on Patent ACT, 2013.
The final act came into force on January 1, 1995 which representing the results of the
urgency round of Multilateral Trade Negotiations were authenticated by 117 nations
including India.
One of the key benefits of the universal system is that, it would assist access to new
medical products. India amended its Patent Law on March 22, 2005, to meet their
TRIPs obligations by abolishing its “process” patent laws and introduce 'product
65
patent’ for pharmaceuticals, food and chemicals (Agarwal and Saibaba, 2001). The
followers of TRIPS debated that the 2005 amendments will encourage foreign
investment, transfer of technology and increase investment in research and
development of neglected diseases.
The main subject concerns with the effect of patenting drugs would increase cost and
which may result that drugs will become out of one of the immediate consequences of
TRIPs agreement will be a sharp increase in the prices of invented drugs (Ramani,
and Maria, 2005). The positive impacts will be increasing the size of Indian
pharmaceutical industry and the growth rates. The product patenting will inspire the
introduction of new drugs, can be encouraging discovery directly or through newly
invented imports that are protected, or through foreign investment in production and
possibly in research (Chandran et al., 2004).
TRIPS implementation in India will effectively change the lifeline of affordable drugs
unless protection measures are implemented to prevent this. For compulsory
licensing one danger is that it will disappoint further the commercial R and D
necessary to new drugs to fight global epidemics. IPRs as monopoly power are a
critical fact which would affect the progress and enlargement of the health sector.
However, in the short run the monopoly power would inspire more innovation and
greater fervor in research and development which would be beneficial in the long run
but in the long run it would not be as beneficial. The patent is one of the IPRs which
gives the inventor sole right to produce his property or license it to other producers.
However misapplication of this right is not required and it is not expected that patent
holders would get into anti-competitive ways, such as ever-greening of patents,
patent pooling etc.
Unlike the other consumer items, in the case of drugs, the consumer goes with what
has been prescribed by the doctor. Hence, in the post WTO regime, the doctors will
play a central role in selecting between a patented drug and a generic drug, in cases
where alternatives are available and help the consumers from being exploited by the
market forces. The drug prices in India were brought under control based on the
recommendations of the Hathi committee (1975), which observed that since the drug
industry has a social responsibility it should operate much above the principles of
66
trade for profit. However, due to the repeated plea of the industry that the drug
production was becoming unprofitable, in 1986, the government reduced the number
of drugs under control from 347 to 166. Yet in spite of the price reductions in India,
over a period of 15 years from 1980, there has been a general rising trend in prices
especially of essential life-saving drugs (Rane, 1995). Whereas the finance ministry
under which the Drug Price Control Order (DPCO) is monitored has announced the
decision to reduce the number of drugs under the price control, the report on
pharmaceutical pricing set up by the government, after studying the scenario in
different countries where some form or the other of price control exists, has
recommended that drugs should be under the price control. The Pharmaceutical
Policy 2002 indicated a drastic reduction in the number of drugs under price control.
According to the industry sources, the new DPCO would cover about 34 bulk drugs
and their formulations under control (Lalitha, 2002).
Prior to the 2005 amendment, only processes were patentable and not the end
product itself. Therefore, if a company chose to manufacture the same product, but
used a different process, it could do so without violating Indian patent laws. This
regime naturally caused concerns to various companies, especially branded
manufacturers, as it did not protect their inventions fully and allowed others to
manufacture the same drug, which would have otherwise enjoyed patent protection in
other jurisdictions. With the 2005 amendment being enacted, product patents and
process patents have been permitted for a period of 20 years and special provisions
have been introduced to prevent ever-greening of patents.
Generic or off-patent drugs, manufactured by the Indian firms, are meeting the most
of the domestic demand. At that time, it is wrong to say that their therapeutic value
will be less than the new, on-patent drugs. Indian generic export prospects are very
high with the increasing concentration of Indian firms on generic drugs. Indian firms
are facing strong competition from even some developed and other developing
countries.Therefore, even under the new patent regime compatible with the TRIPs
agreement, the availability and prices of generic drugs will largely be unaffected.
From the above analysis of impacts of TRIPS shows that it have affected the prices,
availability and affordability of drugs. The TRIPS agreement has directed its member
67
states to implement the requirements of the agreement in order to encourage and
protect IPRs. India, being a member state of the TRIPs agreement has taken
changes in its IPRs laws (Malik 2013). The main reason for permitting patents is the
advantage to society as a whole by boosting innovation in exchange for a limited
monopoly. However, the situation is different with respect to new on-patent drugs.
There is no doubt that these drugs will be available in the Indian market either
through production or under license. From the survey, it is examined that strong
patent system under TRIPs has established a sort of monopoly. In condition of
monopoly, a high price can be charged, as these prices have no considerations with
the buying capacity of the consumers. With high prices prevailing in the market
makes drugs unaffordable to the poor people. Availability has been increased only in
the private sector with higher prices on the other hand problem of low availability in
the public sector is still there. The positive impact can be seen that growth in the
R & D expenditure and innovation of new drugs.
68
CHAPTER - 6
CONCLUSIONS
India is known to produce drugs at a cheaper cost, but we can’t deny this fact also
that Indian consumers suffer from the affordability of very cheap drugs. To overcome
this economic burden of drugs the use of generic drugs is a good substitute but
consumer’s awareness of the generic drugs is very limited. So the present study is an
attempt to examine the various issues related to health care, i.e. availability,
affordability and price differences of common essential drugs in two sectors, public
and private through the primary survey with the help of a standardized methodology
published by WHO/HAI in Bathinda city. The study covers various aspects like the
general prescription about the use of different type of drugs generic and generic
branded from different respondents of different fields. The study also evaluates the
government policies related to drug prices and the various impacts of TRIPS.
In order to achieve the envisaged objectives of the present study the study
comprehensively relies on primary survey along with secondary sources. The primary
data is mainly collected from various stakeholders, including patients, drug retailers,
drug wholesalers and few doctors on the basis of random sampling technique. By
considering the existing issues of health care and economic impact on the people,
both public and private sectors are selected for the survey. The secondary sources,
namely Report of ‘Labour department Punjab’ (Statistical Section, 2013) & poverty
estimates by (Tendulkar Method, 2011-12) are used to examine the affordability and
International Drug Price Indicator Guide, (2014 Edition) for international price
comparison. In the public sector availability of drugs is the major issue, but in the
private sector, there is no issue of availability because of various sources available in
the city. The major issues of private sector are the high prices of branded drugs and
the differences in price differences in generic-branded drugs.
69
Main Findings
The present study evaluates that both public and private sectors are equally important
in health care. The public sector provides generic drugs at reasonable prices to the
patients at ‘Jan Aushadhi Drug Store’ situated in the city civil hospital Bathinda. In
private pharmacies almost both branded and branded generic drugs are available at a
higher price as compared to the public sector. It is perceived that the private sector is
dominated for providing the health care facilities more effectively than public sector
with a higher cost of treatment even for a minor disease. The role of government is
appeared to be immoral. Public sector facilities are not providing satisfactory results
to the patients. The main reason of ineffectiveness of public health care facilities is
the lack of healthcare facilities. This is one of the reasons for the high rate of ‘Out of
Pocket’ expenditure on health care especially for branded drugs.
Firstly, the general prescription of different respondents about the use of drugs and
health care facilities, and drug prices are examined. According to doctor respondents
preference of drugs to patients indicates that almost 40 percent doctors in private
sector favor only branded drugs as they consider that generic drugs are less effective
and not good in quality. Remaining 60 percent doctors have viewed that generics are
good substitutes for branded drugs to make drugs more affordable so they prefer both
types of drugs according to the treatment for diseases.
According to patient respondents, nearly 68 percent of respondents of the study
prefer to the private sector health care facilities because of better facilities due to
sufficient availability, less time consuming and satisfactory treatment. The private
sector hospitals and drug stores are in a large number. The remaining respondents
which prefer public sector facilities they are not much contented with the prevailing
facilities because of low availability of drugs in the public sector and also they have to
purchase the drugs and health treatment ‘Out of Pocket’ with higher cost. About drug
prices nearly 30 percent of the respondents are fully dissatisfied from prevailing
prices of drugs while only 7 percent are fully satisfied. It is observed that the fully
satisfied respondents belong to higher income and dissatisfied belongs to lower
income groups which bear the health care burden due to higher prices of drugs at
private drug stores. Patients do not have knowledge about the generic drugs which
70
are the good substitute of branded drugs to reduce the financial burden of health.
About 70 percent of the respondents do not familiar with the term generic, only the
fact is generally known by them is that, less cost of drugs in provided in the public
sector.
Unavailability of essential drugs is issue in the public sector, so availability of 235
essential drugs mentioned in the Punjab essential drug list, containing different types
of drugs such as injections, I.V Fluids, Eye/Ear/Nasal Drops, Tablets and Capsules,
Solution, Creams, Applications and Syrup/ Suspension is evaluated by following the
availability criteria provided in WHO/HAI methodology. Availability of injections
(19.72) percent and Syrup/ Suspension (12.90) percent is very low, I.V Fluids
Eye/Ear/Nasal Drops (33.3) percent, Tablets and Capsules (36.2) percent, I.V Fluids
(45.45) percent are under low availability, no items on the essential list have fairly
high availability. So it can be concluded that the overall availability of all forms of
drugs is very low, i.e. 28.51 percent of i.e. less than 50 percent.
Drugs affordability to the ordinary and poor people is also measured by comparing
the treatment cost with the wages they earn. ‘Ordinary people’ are the lowest paid
unskilled government worker described in WHO/HAI methodology. The cost of
treatment for different therapeutic classes is affordable in the public sector as
compared to the private sector. The highest differences in treatment cost for Antacid
found in the public sector (Rs. 23.16) and in the private sector is (Rs. 250.5) similarly
Antifungal requires (Rs 20.62) in the public sector while (Rs. 119) in the private
sector. Antihypertensive require treatment cost in the private sector (Rs.12.9) and
(Rs. 68.7) in the private sector. The other therapeutic classes as Antibacterial,
requires (Rs. 28.92 to Rs. 62.5), Anti-Allergic (Rs 1.63 to Rs 17.5), Painkiller (Rs 2.66
to Rs 8.5) and Antihypertensive (Rs.12.9 to Rs. 68.7), Anti-infective Rs. (25.9 to Rs.
49) Anti Helminthic (Rs. 14.21- Rs.70) and Laxatives requires (Rs. 0.384 to Rs.1).
The result shows that affordable drugs in the public sector, but in private sector prices
are not affordable for poor families and affordable for ‘ordinary people’.
Differences in drug prices at different level in different sectors are also measured. The
differences are evaluated of commonly used drugs as for the treatment of Antacid,
Antibacterial, Anti-infective, Antihypertensive, Anthelminthic, Laxatives therapeutic
71
classes in public and private sector. Most of the difference in prices between two
sectors is for Tab. Pantoprazole has highest ratio (10.8) which highlights that price of
this drug is 10 times higher in the private sector and minimum ratio is (1.2) of Tab.
Ciprofloxacin Coated which indicates nearly two times more price is charged in the
private sector. As the value of the ratio is high the difference in private and public
price is also high. In case of other drugs, it can be said that ratios of other drugs as
Tab. Cefixime (6) Fluconazole which (5), Tab. Levo Cetirizine, Anti Helminthic Tab.
Albendazole have ratio (4), and Tab. Azithromycin, Tab Levoflexine, Tab.
Azithromycine, Tab. Ciprofloxacin, have ratio (2). These results show that in the
public sector drugs are very less as compare to the private sector.
Price differences within the private sector are also examined by calculating the high-
low ratio of drug prices, which compares the highest unit price with the lowest unit
price. A highest ratio is found 7.6 of Tab. Atenolol which indicates that the highest unit
price is more than 7 times greater than the lowest unit price, and the lowest ratio is 1
of Tab. Fluconazole means the same value of both highest and lowest prices. The
ratio of other drugs lies between these minimum and maximum ratios.
Differences in the wholesale price and retail prices are also collected to evaluate the
level of retail margins. The results describes that minimum price margin level is found
for Antibacterial Tab. Cotrimoxazole S.S (Trimethoprim 80mg + Sulphamethoxazole
400mg) i.e. 19.66 percent and the maximum is 775 percent for Antiallergic Tab. Levo
Cetirizine 5 mg. The other level of margins for different classes ranged as Laxatives,
Tab. Bisacodyl 10 mg 81.82 percent, Pain Killer, Fever Tab. Paracetamol 500 mg,
200 percent, Antihypertensive, Tab. Atenolol 50 mg, 332.08 percent Anti Helminthic
Tab. Albendazole , 423.56 percent, .Antacid has 619.83 percent, and The maximum
level of margin is in anti-allergic therapeutic class. These margin levels are very high
as near up to 800 percent. According to retailers, the actual level of margins attained
by them is minimum 16 percent and maximum 50 percent. These differences in level
of margins are also a reason of price differences in private retailers.
After determining the differences of local prices in public and private sector,
international comparison is also measured with the comparison of local per unit
72
median price with the international reference price provided by the WHO/HAI
methodology. The comparison indicates that how many times domestic prices are
more or less from international price level calculated by ‘Median Price Ratio’ (MPR)
which is the ratio of the median local unit price to reference unit price. In the public
sector the Median Price Ratio of selected drugs is low as (less <1) excepting the Tab.
Paracetamol Tab. Cefixime, Tab. Ciprofloxacin Coated and Amoxycillin which has
(MPR > 1). Low ratio value means prices are low in the domestic market and high
value means more prices. On the other hand, in private sector minimum MPR is Rs.
0.29 of Tab. Rantidine and Maximum Rs. 3.58 of Tab. Albendazole. Out of 15
selected drugs for international comparison only 4 drugs have less MPR, means only
these drugs are less costly others are more costly at private domestic level. The
reason of higher cost of drugs in this sector is more demand of generic popular
brands. The Indian pharmaceutical industry is very efficient in all over the world to
provide the drugs at very cheap prices as compared to other countries, but it is not as
much effective for the Indian population to make them affordable and available at
reasonable prices according to their financial conditions. It can be said that in the
private sector majority of drug prices are higher than the international price, but in
public sector case is reverse. So the private sector is unaffordable for the poor
people.
Evaluation of the existing Indian Drug Price Policy is required for understanding the
role of government in price control. India has adopted various drug policies from time
to time fall under the ‘Ministry of Chemicals and Fertilizers’. The main objective of the
drug price polices is to manage the challenge of making a balance between industrial
growth and ‘ensuring affordable and reasonably priced medicines to the consumers’
particularly the poorer masses at the times at the same time. The government has
made contributions in essential drug pricing through the three main names given to
the pricing control system. These are ‘Drug Price Control Order’, ‘Drug Pricing
Policies’ and ‘National Pharmaceutical Pricing Policy’ with the objective of controlling
prices of important drugs and making them available at reasonable rates to the
consumer. The Indian has introduced government introduced the Drug Price Control
Order (DPCO) amended with some revisions in DPCO as 1979, 1987, 1995 and
73
2013. The DPCO (1979) set 370 drugs under price control. In DPCO (1987) the total
number of bulk drugs was reduced from 370 to 142 under price control. Under DPCO
(1995) the number of drugs for price control has been reduced from 142 drugs to just
76. In current DPCO, (2013) with the origin of NPPA, (2012) total number of drugs in
control is increased from 76 to 652 essential drugs.
All the previous DPCOs of 1970, 1979, 1987 and 1995 were based on cost to
manufacturers cost. But as per the requirements of DPCO (2013) ceiling prices are
now being fixed at the average retail price of the medicine which is manufactured by
all those companies involved in its production with a market share of ≥ 1percent of the
entire market turnover, and adding 16 percent margin to the retailer. All the policies
were generally established on the principle of effecting control prices of essential
drugs, and far along bulk drugs, in addition to the availability of drugs while at the
same time attending to the requirements of the indigenous industry for growth, cost
effective production, and innovation and strengthening of capacity. The price control
principle adopted in this policy for broadly signified an important departure from the
previous policies. This imagined control over prices on the drugs basis related
economic criteria exemplified in the market share of different companies in the
context of total market sales turnover of various drugs.
Consequently, the Government pronounced the National Pharmaceuticals Pricing
Policy, (2012) by replacing the drug policy pronounced in September, 1994. To meet
the challenges brought about by the competitive international pharmaceutical industry
in a globalized economic environment and the country’s requirements for safe and
quality medicines at reasonable prices. The National Pharmaceuticals Pricing Policy
(2012) has a new process for determining the ceiling price, termed as market-based
pricing mechanism as applied through the Drugs Prices Control Order (2013), Its
result would be a reduction in prices of certain top brands, but not close potential
escape routes for good. It will also leave a lot of useful life-saving drugs used in
tertiary care outside the price control basket.
But the policy has not produced the satisfactory results. Currently NLEM (2011) does
not cover a wide range of ‘essential drugs’ as many combinations of TB drugs, a large
74
number of important drugs for diabetes and hypertension which are so important for
patients. Many other critical lifesaving medicines, such as, anti-cancer drugs,
expensive antibiotics and products needed for organ transplantation have been left
out of price control. The prices of a large number of drugs have reportedly gone up
after the notification of DPCO (2013) though NPPA.
The change in the criteria shows the changes in prices by changing the base and
price control methodology. When the comparison is made between the new drug
policies (2013) with previous (1995) the ‘Drug Price Control Order’ (DPCO 2013)
noticeably enunciates it is conveyed that after the implementation of the DPCO
(2013), apparently there has been a decrease in the stock of the medicines in the
market. In most of the states, hospitals and doctors are facing scarcity of the essential
medicines for the consumption of their patients. The results of the present study also
are also showing the same effect on the public sector.
After the independence ‘Patent Act’ has allowed for Indian manufacturers to produce
legally generic versions of medicines patented in other countries since (1970), An
important intense modification in ‘access to medicines’ in developing nations occurs
due to mark (2005). One side positive impacts of TRIPS are R & D intensities of the
firms have improved significantly and its expenditure has dramatically increased for a
segment of the Indian pharmaceutical industry. R & D expenditure has increased
along with a drastic shift in the structure of R & D activities of the Indian companies.
Before this Patent Indian drug manufacturers were mainly involved in the
enlargement of innovative procedures for manufacturing drugs.
On the other side TRIPS agreement has an opposing effect on prices and availability
of drugs which creates difficulty for nations to fulfill with their obligations to respect,
protect and fulfill the ‘right to health’ under the stronger patent system, TRIPS has
established a sort of monopoly. On condition of monopoly, high prices are charged by
innovator companies, as these prices have no considerations with the buying capacity
of the consumers. With high prices of branded drugs prevailing in the market makes
drugs affordable to the poor people. Availability has been increased only in the private
75
sector with higher prices of branded drugs. On the other hand problem of low
availability in the public sector is still there.
In view of the high drug prices, huge differences in price & markups in the private
sector and its poor availability in public sector suggest some policy implications for
effective drug distribution channel in India.
First, steps should be taken to improve the availability of medicines in the public
sector aiming to fulfill the target of hundred percent availability of the essential drugs.
For this, distribution of drugs should be maintained by ensuring adequate and timely
distribution of essential drugs.
Second, the demand for generic drugs in the market is required to be increased,
which would have a positive impact on prices. Although generic and generic branded
drugs are alternatives to originator brands, they are also mostly two to four times
more expensive in the private sector than international reference prices. So, the
prices of alternatives should be lowered as their manufacturing cost starts to diminish.
Therefore, overall evaluation of drug prices should be a key priority which would help
to increase the level of affordability of poor people.
Thirdly, it is necessary to expand the popular awareness programs about use and
information about generic drugs. The need of the hour is to increase the number of
facilities with the quantity and quality of drugs. Public sector facilities along with drug
stores at reasonable prices should be done in different rural areas on a priority basis.
Fourth, some commonly used drugs Antifungal Tab. Fluconazole (150 mg), Anti-
infective Tab. Amoxycillin + Clauvinic Acid (500mg +125 mg), Antacid Tablet
Pantoprazole and Anti-Allergic Anti Helminthic Tab. Albendazole (400 mg),
Antibacterial Tab. Cefixime (200mg), Azithromycin (250 mg) , Tab, Levoflexine (250
mg), Tab. Ofloxacin + Ornidazole (200mg + 500mg), are more expensive in the
private sector, with a high mark up to 775 percent so measures should be taken by
the pricing authority to decrease the prices of these drugs by the intervention of
regulatory authorities will likely be needed to regulate these markups.

76
Fifth, regulations in the supply chain of drugs can be maintained like fixation of the
markup level of retailers. The retail markup level given in the Drug Price Control
Order (2013), which is 16 percent, should be properly implemented. The survey
found variations in the margin attained by retailers for generic and generic branded.
More variations have found from retailer to consumer i.e. from 19 per cent to 775 per
cent. To reduce this gap between wholesale and retail prices, printed MRP on the
drug strips should be fixed rationally.
Sixth, in the prevailing drug pricing system, there is a lack of transparency of drug
prices. So these should be transparency in all types of drugs available in both public
and private sectors.
77
Bibliography
Agarwal, P. and Saibaba, P. (2001). TRIPS and India’s pharmaceutical
industry. Economic and Political Weekly 36 (39): 3787-3790.
Ahmad, A. Khan, M. U. And Patel, I. (2015). Drug pricing policies in one of the
largest drug manufacturing nations in the world: Are affordability and access a
cause for concern?. Journal of Research in Pharmacy Practice 4 (1): 1-3.
Basak, S. C. & Sathyanarayana, D. (2012). Exploring knowledge and perceptions of
generic medicines among drug retailers and community pharmacists. Indian
Journal of Pharmaceutical Sciences 74 (6), 571-582.
Basant, R. and Morris, S. (2000). Competition policy in India: Issues for a globalizing
economy. Economic and Political Weekly 35 (31): 2735-2747.
Bathinda city map, modified from Google Earth Map.
Bera, A. and Mukherjee, A. (2012). The production of generic drugs in India.
International Journal of Pharmaceutical, Chemical and Biological Science 2 (4):
575–587.
Bhargava, A. and Kalantri, S. P. (2013). The crisis in access to essential medicines
in India: key issues which call for action. Indian Journal of Medical Ethics 10 (2):
86-94.
Bharti, V. (2016). Punjab top state on out of pocket medical expenses. Retrieved
from http://www.tribuneindia.com/news/punjab/punjab-tops-states-on-out-of-
pocket-medical-expenses. on 14 March 2016.
Billa, G. Thakkar, K. Jaiswar, S. and Dhodi, D. (2014). A cross-sectional study to
evaluate the awareness and attitudes of physicians towards reducing the cost of
prescription drugs, Mumbai. Applied Health Economics and Health Policy 12
(2): 125-137.
Birla, D. Maheshwari, R. P. and Gupta, H. O. (2007). An approach to tackle the
threat of sympathy trips in directional overcurrent relay coordination.Power
Delivery, IEEE Transactions on 22 (2): 851-858.
Blier, P. (2003). Brand versus generic medications: the money, the patient and the
research. Journal of Psychiatry and Neuroscience: JPN 28 (3):167.
78
Chaturvedi, K. and Chataway, J. (2006). Strategic integration of knowledge in Indian
pharmaceutical firms: creating competencies for innovation.International Journal
of Business Innovation and Research 1 (2): 27-50.
Chaudhuri, A. (2012). Socio-economic inequity in health care utilization and
expenditures in richer states in India. The Indian Journal of Medical Research
136 (3): 368-369.
Chien, C. (2003). Cheap drugs at what price to innovation: does the compulsory
licensing of pharmaceuticals hurt innovation?. Berkeley Technology Law Journal
18 (3): 853-907.
Correa, C. M. (2000). Intellectual property rights, the WTO and developing countries:
the TRIPS agreement and policy options. Zed Books.
Deloitte United States, (2016). Indian health care outlook. Retrieved, from
https://www.deloitte.com.Health-Care/gx-lshc-2015 on April 2016.
Department of Pharmaceuticals-New Delhi. (2013). Drug price control order, 1940
(May), 1–67. Retrieved from http://www.idma-assn.org/pdf/drug-price-control-
order-2013.
Dhar, B. and Gopakumar, K. M. (2006). Post-2005 TRIPS scenario in patent
protection in the pharmaceutical sector: The case of the generic pharmaceutical
industry in India. online publication, UNCTAD-ICTSD Regional Research Paper,
Geneva.
Drug price control order (DPCO). Retrieved from www.arthapedia.in. on 3 Jaunary
2016.
Drug price control order. (1995). Ministry of Chemicals and Fertilizers (Department of
Chemicals and Petrochemicals) retrieved from www.dca.ap.nic.in.
Drug Price Control Order. (2013). An overview of drug price control. Retrieved from
www.mondaq.com. on September 2015.
Drug price control order. (2013). Ministry of Chemicals and Fertilizers (Department of
Pharmaceutical). Retrieved from www.nppaindia.nic.in.
Eight Status Report of PGRC (Punjab Government Reforms Commission). Retrieved
from www.pbrdp.gov.in. on March 2016.
79
Frank, R. G. (2001). Prescription drug prices: why do some pay more than others
do?. Health Affairs 20 (2): 115-128.
Godwin, S. K. and Varatharajan, D. (2002). Drug price differentials across different
retail market settings. Health Administrator 19 (1): 41–47.
Government of India. (2013). Press note on poverty estimates, 2011-12. Press
Information Bureau 1–10.
Hinsch, M. Kaddar, M. and Schmitt, S. (2014). Enhancing medicine price
transparency through price information mechanisms. Globalization and
Health 10 (1): 1.
Holloway, K. and Ivanovska, V. (2003). WHO’s database on rational use of
medicines. Essential Drug Monitor 33:12.
Hudson, J. (2000). Generic take-up in the pharmaceutical market following patent
expiry: a multi-country study. International Review of Law and Economics 20
(2): 205-221.
Human rights perspective of health. Retrived from http://www.ohchr.org. on
September.2015.
International, J. S. and Foundation, T. G. (2005). Using the WHO / HAI Medicine
price methodology to study a therapeutic group of medicines 3, 1–7.
Jain, D. (2013). Is the national pharmaceutical policy, 2012 really cheering the
pharma. Indian JL and Tech 9, 92-107.
Jan Aushudhi: An initiative. Retrieved from http://janaushadhi.gov.in. on 13 October
2015.
Kanwar, S., and Hall, B. H. (2015). The Market Value of R&D in Weak Innovation
Regimes: Evidence from India (No. 21196). National Bureau of Economic
Research.
Kapur, B. (2012). Analysis of health and health care services in Punjab.
Kiran, R. and Mishra, S. (2009). Performance of the Indian pharmaceutical industry
in Post-TRIPS Period: A firm level analysis. International Review of Business
Research Papers 5 (6): 148-160.
Kirtida, T. and M, Z. S. (2013). Retail Drug Prices : Need for strict drug price control
Policy 4 (4): 1394–1399.
80
Kotwani, A. (2003). Medicine prices in the state of Rajasthan, India : Report of a
survey of medicine prices, availability, affordability and price components.
Retrieved from
http://apps.who.int/medicinedocs/documents/s18026en/s18026en. on November
2015.
Kotwani, A. (2010). Commentary: Will generic Drug Stores improve access to
essential medicines for the poor in India? Journal of Public Health Policy 31 (2):
178–184.
Kotwani, A. Ewen, M. Dey, D. Iyer, S. Lakshmi, P. K., Patel, A. and Laing, R. (2007).
Prices and availability of common medicines at six sites in India using a
standard methodology. Indian journal of medical research 125 (5): 645.
Kumar, R. Tripathy, J. P. Singh, N. Kaur, M. Prinja, S. Lakshmi, P. V. M. and
Bhattacharya, S. (2015). Rapid Assessment of Health Services in Punjab using
a Mixed Method Approach. Indian Journal of Community Health 27 (2), 197-
203.
Kumar, V. Vishal Gupta, N. and Kumar, K. A. (2014). A comparision between old
and latest systems in DPCO. International Journal of Pharmacy and
Pharmaceutical Sciences 6 (2): 19–20.
Lalitha, N. (2002). Drug policy 2002: Prescription for symptoms. Economic and
political weekly 3102-3104.
Lalitha, N. (2011). Access to Indian generic drugs: emerging issues. Intellectual
property, pharmaceuticals and public health: access to drugs in developing
countries. Edward Elgar, London 225-252.
Lall, S. (2003). Indicators of the relative importance of IPRs in developing
countries. Research Policy, 32 (9): 1657-1680.
Lanjouw, J. O. Pakes, A. and Putnam, J. (1998). How to count patents and value
intellectual property: The uses of patent renewal and application data.The
Journal of Industrial Economics, 46 (4): 405-432.
Levin, R. C. Klevorick, A. K. Nelson, R. R. Winter, S. G. Gilbert, R. and Griliches, Z.
(1987). Appropriating the returns from industrial research and
development. Brookings Papers on Economic Activity 1987 (3): 783-831.
81
Lexchin, J. (2004). The effect of generic competition on the price of brand-name
drugs. Health Policy 68 (1): 47-54.
Lu, Z. J. and Comanor, W. S. (1998). Strategic pricing of new
pharmaceuticals. Review of Economics and Statistics 80 (1): 108-118.
Macdonald, S. (2004). When means become ends: considering the impact of patent
strategy on innovation. Information Economics and Policy 16 (1): 135-158.
Malik, P. (2013). Implications of TRIPs Agreement on India with special reference to
Pharmaceutical Sector. International Interdisciplinary Research Journal 3 (4):
531- 539.
Mani, Sunil (2006) The sectoral system of innovation of Indian pharmaceutical
industry. CDS working papers, no.382. Trivandrum: CDS.
Manikandan, S. and Gitanjali, B. (2012). National list of essential medicines of India:
the way forward. Journal of Postgraduate Medicine 58 (1): 68-72.
Mehta, S. P. (1998). TRIPS and Pharmaceuticals: Implications for
India.Schweizerisches Jahrbuch für Entwicklungspolitik 17: 97-106.
Ministry of Chemicals and Fertilizers. (2013). Retrieved from www.nppaindia.nic. on
November 2015.
Mohammad, A. and Kamaiah, B. (2014). The Indian pharmaceutical industry in post-
trips and post-product patent regime: a group-wise analysis of relative efficiency
using nonparametric approach. IUP Journal of Applied Economics 13 (1): 47.
Mojasola, A. Hernandez, M. Sansgiry, S. and Jones, L. (2012). Perception of generic
prescription drugs and utilization of generic drug discount programs. Ethnicity
and Disease 22 (4): 479.
Mudaliar, M. and Maheshwari, D. (2014). Comparing generic and innovator drugs : a
review of comparison of bioequivalence data of hydrocortisone conventional
tablet and hydrocortisone modified release tablet 3 (3): 1173–1183.
Nair, M. D. (2012). TRIPS and access to affordable drugs. Journal of Intellectual
Property Rights 17 (4): 305–314.
Phul, R. Sabo, T. Ka, B. B. Mandis, B. and Information, D. (1800). General
Description of the District 2.1, 1–4.
82
Punjab tops state on out of pocket medical expenses. Retrived from
http://www.tribuneindia.com/news/punjab/punjab-tops-states-on-out-of-pocket-
medical-expens1es/163513.html on 15 January 2016.
Ramani, S. V. and Maria, A. (2005). TRIPS: Its possible impact on biotech segment
of the Indian pharmaceutical industry. Economic and Political Weekly 40 (7):
675-683.
Rana, P. and Roy, V. (2015). Generic medicines: issues and relevance for global
health. Fundamental & Clinical Pharmacology, 29 (6): 529-542.
Report of the Core-Committee for Revision of National List of Essential Medicines
November (2015).
Report, I. (2016). 2015 Health care outlook industry chamber assocham estimates
that India ’ s medical tourism sector is, (March 2014). 2013–2016.
Roy, V. Gupta, U. and Agarwal, A. K. (2012). Cost of medicines and their affordability
in private pharmacies in Delhi (India). Indian Journal of Medical Research 136
(5): 827–835.
Selvaraj, S. (2007). How effective is India's drug price control regime. Harvard
School of Public Health.
Selvaraj, S. Hasan, H. Chokshi, M. Sengupta, A. Guha, A. Shiva, M. and
Menghaney, L. (2012). Pharmaceutical pricing policy: a critique. Economic and
Political Weekly 47 (4): 20-23.
Singal, G. L. Nanda, A. & Kotwani, A. (2011). A comparative evaluation of price and
quality of some branded versus branded-generic medicines of the same
manufacturer in India. Indian Journal of Pharmacology 43 (2): 131-136.
Srinivasan, S. and Phadke, A. (2013). Pharma policy 2012 and its
discontents. Economic and Political Weekly 48 (1): 38-42.
Wong, Z. Y. Hassali, M. A. Alrasheedy, A. A. Saleem, F. Yahaya, A. H. and Aljadhey,
H. (2014). Patients’ Beliefs about Generic Medicines in Malaysia. Pharmacy
Practice 12 (4): 474.
World Health Organization (2003). Medicine Prices-a New Approach to
Measurement. 1–152.
83
World Health Organization. (2006). Price, Availability and Affordability: An
International Comparison of Chronic Disease Medicines. EMRO Meeting
Reports, 1 (2006), Retrieved from http://www.who.int/iris/handle/10665/116493.
on 26 December 2015
World Health Organization. (2008). Measuring medicine prices, availability,
affordability and price components. Retrieved from
http://apps.who.int/iris/handle/10665/70013. on 13 February 2016.
World Health Organization. (2015). India: WHO Statistical Profile, 3. Retrieved from
http://www.who.int/gho/countries/ind. on April 2016.
World Health Organization. (2015). Part II: Global Health Indicators. World Health
Statistics (2015). 39–160.
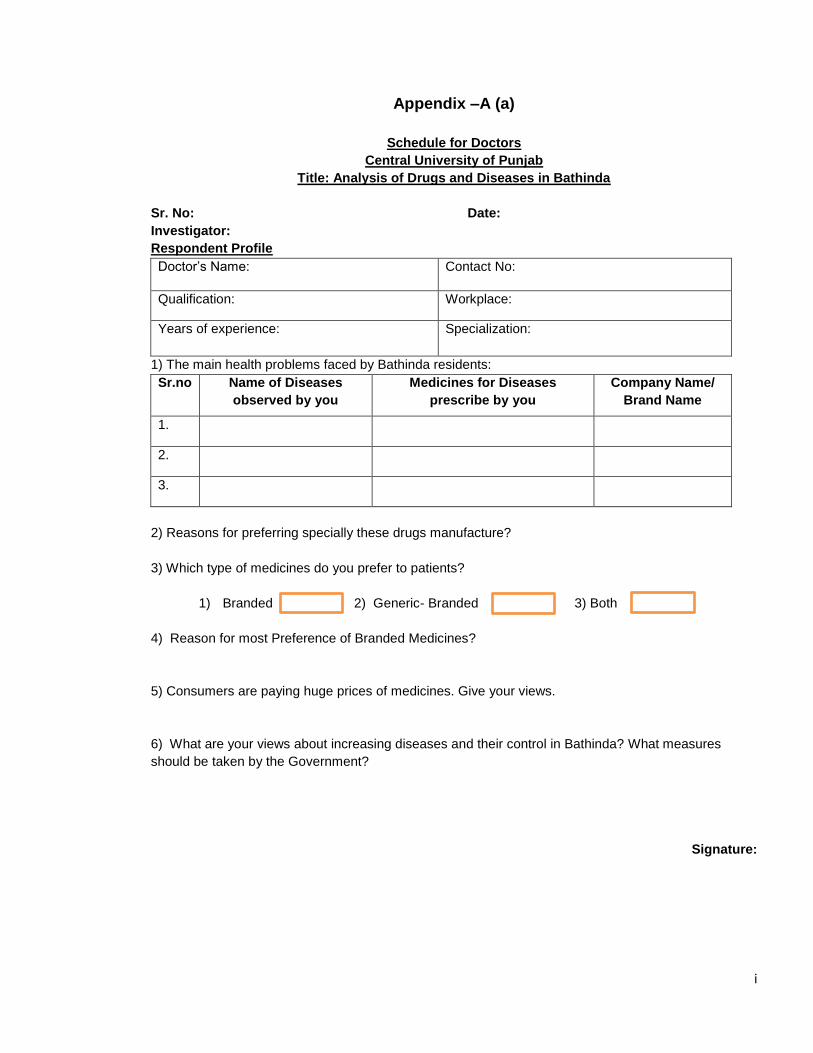
i
Appendix –A (a)
Schedule for Doctors
Central University of Punjab
Title: Analysis of Drugs and Diseases in Bathinda
Sr. No: Date:
Investigator:
Respondent Profile
Doctor’s Name: Contact No:
Qualification: Workplace:
Years of experience: Specialization:
1) The main health problems faced by Bathinda residents: Sr.no Name of Diseases
observed by you
Medicines for Diseases
prescribe by you
Company Name/
Brand Name
1.
2.
3.
2) Reasons for preferring specially these drugs manufacture? 3) Which type of medicines do you prefer to patients?
1) Branded 2) Generic- Branded 3) Both
4) Reason for most Preference of Branded Medicines?
5) Consumers are paying huge prices of medicines. Give your views.
6) What are your views about increasing diseases and their control in Bathinda? What measures should be taken by the Government?
Signature:
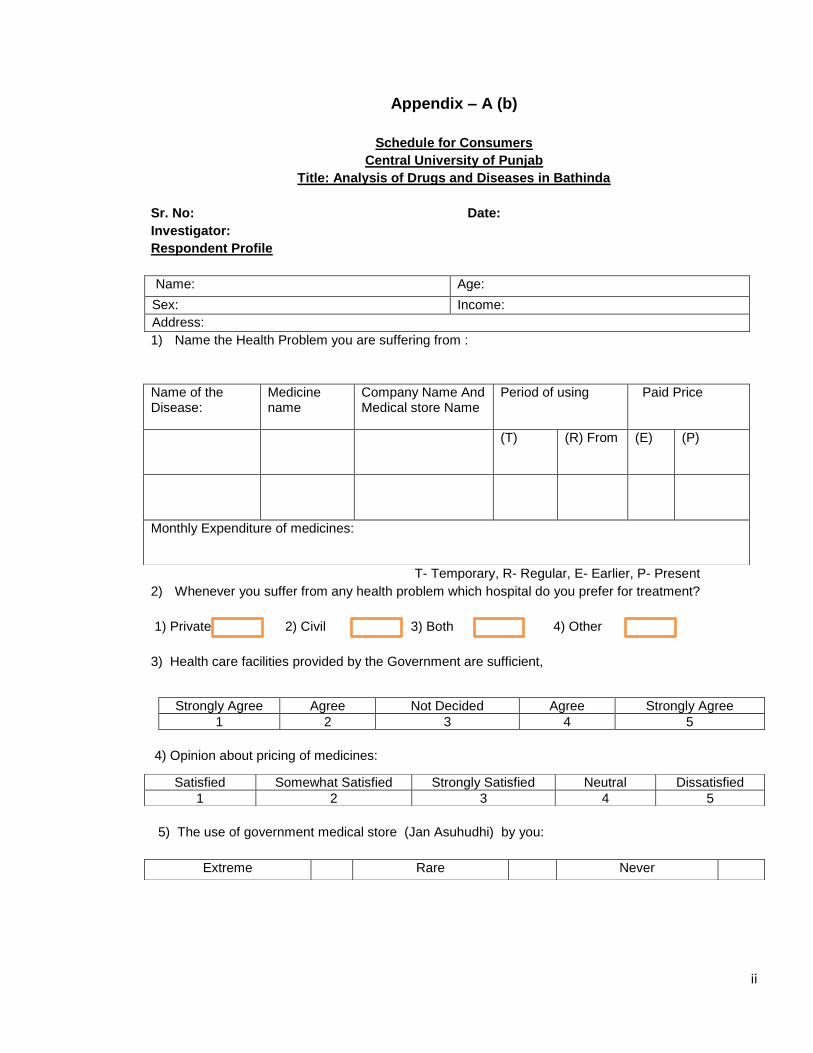
ii
Appendix – A (b)
Schedule for Consumers
Central University of Punjab
Title: Analysis of Drugs and Diseases in Bathinda
Sr. No: Date:
Investigator:
Respondent Profile
Name: Age:
Sex: Income: Address: 1) Name the Health Problem you are suffering from :
T- Temporary, R- Regular, E- Earlier, P- Present 2) Whenever you suffer from any health problem which hospital do you prefer for treatment?
1) Private 2) Civil 3) Both 4) Other 3) Health care facilities provided by the Government are sufficient,
4) Opinion about pricing of medicines:
5) The use of government medical store (Jan Asuhudhi) by you:
Name of the Disease:
Medicine name
Company Name And Medical store Name
Period of using Paid Price
(T) (R) From (E) (P)
Monthly Expenditure of medicines:
Strongly Agree Agree Not Decided Agree Strongly Agree 1 2 3 4 5
Satisfied Somewhat Satisfied Strongly Satisfied Neutral Dissatisfied 1 2 3 4 5
Extreme Rare Never
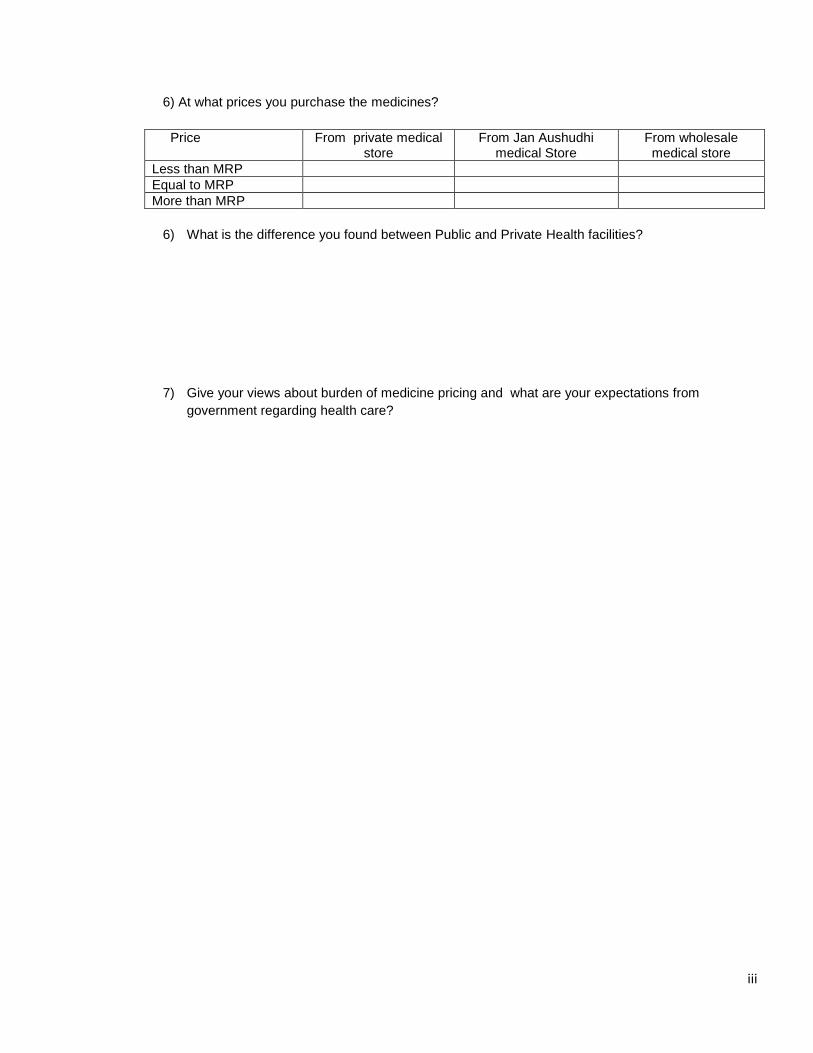
iii
6) At what prices you purchase the medicines?
Price From private medical store
From Jan Aushudhi medical Store
From wholesale medical store
Less than MRP Equal to MRP More than MRP
6) What is the difference you found between Public and Private Health facilities?
7) Give your views about burden of medicine pricing and what are your expectations from government regarding health care?
iv
Appendix – A (c)
Schedule for Retailer
Central University of Punjab
Title: - Analysis of Drugs Prices
Sr. No: Date:
Investigator: Name of the Area:
1) Respondent Profile
Respondent’s Name: Year of started Drug store: Age: Contact No: Qualification: E-Mail:
2) General Information
2.1 Identification of Drug Store:
2.2 Medicines Information
Type of Medicines (A) Branded (B) Branded-Generic (C) Both
Sold in Drug Store Most Demanded
3) Drugs Detail:
Mention the detail of commonly used essential drugs:
Sr.no Therapeutic
Class
Generic
Drug Name
Brand
Name
Company
Name
Unit MRP Retail
Price
4) Prices margins information
4.1 Specify the margins in (%) Percentage on different type of medicines:
1) Government 1) Private
2.1) Individual 2.2) Within Hospital 2) Society owned
3) Any Special Monopoly 4) Other:
Address of Drug Store:
Type of Drugs Level of Margins Branded Branded- Generic
v
4.2 Your opinion about Prices margins of medicines at which you sold:
Type of the medicines
1 Highly Satisfied
2 Somewhat Satisfied
3 Neutral
4 Less satisfied
5 Dissatisfied
Branded Branded- Generic
4.3 Views about increasing Prices on Branded and Branded-Generic:
5) Detail of Wholesalers:
Name and address the detail of wholesalers who provide medicines:
Sr.no Name of the Wholesaler Address
6) Availability Information
Tick the medicines name of Essential Generic Medicines available in the Drug Store:
*List is mentioned in (Appendix-B)
Signature
vi
Appendix – A (d)
Schedules for Wholesalers Central University of Punjab (Bathinda)
Title: - Drug Prices: A Case Study of Bathinda District
Sr. No: Date: Investigator: Name of the Area: 1 Respondent Profile
Respondent’s Name: Year Of Started Drug Store: Age: Contact No: Qualification: EMail:
2 General Information Medicines Information
Type of Medicines (A) Branded (B) Branded-Generic (C) Both
Sold In Drug Store Most Demanded
3) Drugs Prices Detail
3.1 Mention the Prices of the commonly used Essential Generic- Branded Drugs:
Sr.no Generic Drug Name Brand
Name
Company
Name
Wholesale
Price
MRP Company
Price
1 Tab. Pentaperazole 40 mg Pantocip Cipla
2 Tab. Rantidine 150 mg Rantax Cipla
3 Tab. Cotrimoxazole S.S
(Trimethoprim 80mg +
Sulphamethoxazole
400mg)
Ciplin Ds Cipla
4 Tab. Levoflexine 250 mg Lovolkem Alkem
5 Tab. Azithromycine 250mg Azx Ranbaxy
6 Tab. Levo Cetirizine 5mg Cetipen
Lv
Morpen
7 Tab. Cetirizine Hcl 10 mg Okacet Cipla
8 Tab. Paracetamol 500 mg Pacipr Cipla
9 Tab. Fluconazole 150 mg FCN Intas
10 Tab. Atenolol 50 mg Hipras Cipla
11 Tab. Ciprofloxacin Coated
250 Mg
Floxip Abbott
12 Tab. Ciprofloxacin Coated
500mg
Ciprotas Intas
13 Cap. Amoxycillin 500 Mg Cipmox Cipla
14 Tab. Amoxycillin + Amoxycla Abbot
vii
Clauvinic Acid -500mg
+125 Mg
v
15 Tab. Cefixime 200 mg Fexim-O Zydus
16 Tab. Ofloxacin 200 mg Okaflox Cipla
17 Tab. Ofloxacin +
Ornidazole ( 200mg +
500mg)
Oflotas Intas
18 Tab.Paracetamol 500 mg +
Diclofenac Sodium 50 mg
Fenak Ranbaxy
19 Tab. Albendazole 400 mg Gentre Glexo
20 Tab. Bisacodyl 10 mg Delkoflex Boenginer
3.2 Which type of drugs prices fluctuate more?
Generic Branded 3.3 Specify the Margins in (%) Percentage on different type of drugs:
4) Supply Detail:
1) Source of drugs availability:
Sr. no
Name of the source Detail
5) Views about the prices of Generic and Branded Drugs:
Type Of Drugs Level Of Margins Branded Branded- Generic
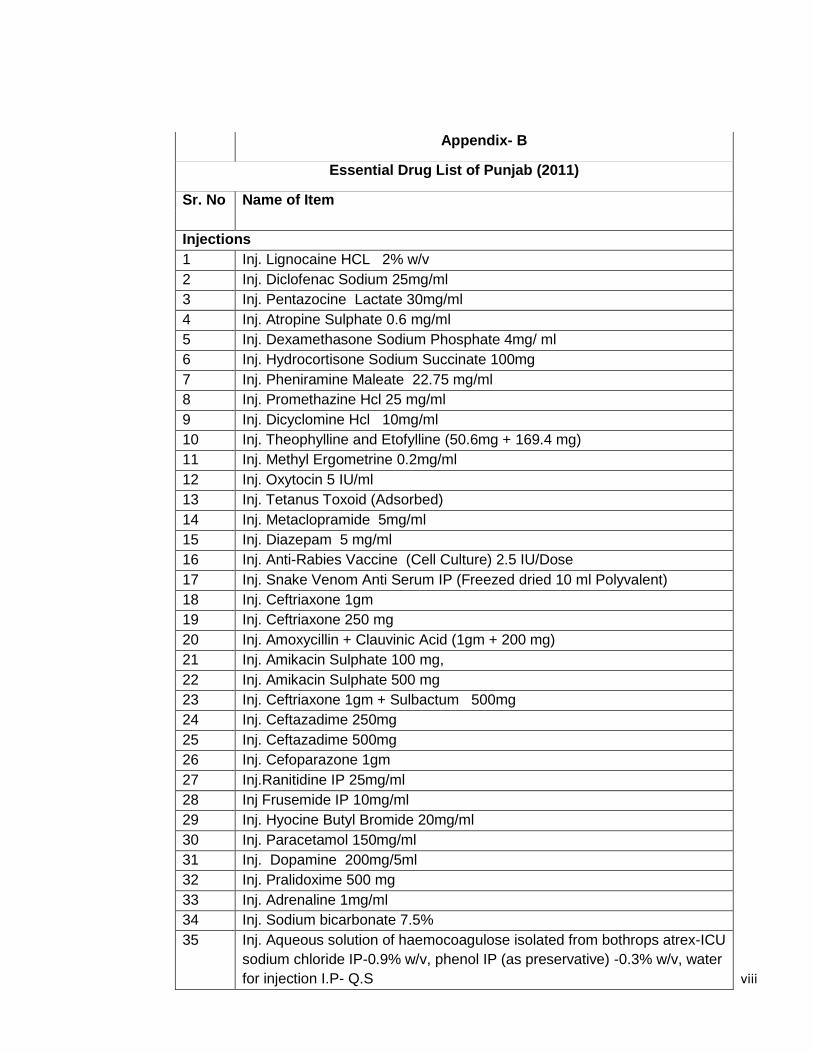
viii
Appendix- B
Essential Drug List of Punjab (2011)
Sr. No Name of Item
Injections
1 Inj. Lignocaine HCL 2% w/v 2 Inj. Diclofenac Sodium 25mg/ml 3 Inj. Pentazocine Lactate 30mg/ml 4 Inj. Atropine Sulphate 0.6 mg/ml 5 Inj. Dexamethasone Sodium Phosphate 4mg/ ml 6 Inj. Hydrocortisone Sodium Succinate 100mg 7 Inj. Pheniramine Maleate 22.75 mg/ml 8 Inj. Promethazine Hcl 25 mg/ml 9 Inj. Dicyclomine Hcl 10mg/ml 10 Inj. Theophylline and Etofylline (50.6mg + 169.4 mg) 11 Inj. Methyl Ergometrine 0.2mg/ml 12 Inj. Oxytocin 5 IU/ml 13 Inj. Tetanus Toxoid (Adsorbed) 14 Inj. Metaclopramide 5mg/ml 15 Inj. Diazepam 5 mg/ml 16 Inj. Anti-Rabies Vaccine (Cell Culture) 2.5 IU/Dose 17 Inj. Snake Venom Anti Serum IP (Freezed dried 10 ml Polyvalent) 18 Inj. Ceftriaxone 1gm 19 Inj. Ceftriaxone 250 mg 20 Inj. Amoxycillin + Clauvinic Acid (1gm + 200 mg) 21 Inj. Amikacin Sulphate 100 mg, 22 Inj. Amikacin Sulphate 500 mg 23 Inj. Ceftriaxone 1gm + Sulbactum 500mg 24 Inj. Ceftazadime 250mg 25 Inj. Ceftazadime 500mg 26 Inj. Cefoparazone 1gm 27 Inj.Ranitidine IP 25mg/ml 28 Inj Frusemide IP 10mg/ml 29 Inj. Hyocine Butyl Bromide 20mg/ml 30 Inj. Paracetamol 150mg/ml 31 Inj. Dopamine 200mg/5ml 32 Inj. Pralidoxime 500 mg 33 Inj. Adrenaline 1mg/ml 34 Inj. Sodium bicarbonate 7.5% 35 Inj. Aqueous solution of haemocoagulose isolated from bothrops atrex-ICU
sodium chloride IP-0.9% w/v, phenol IP (as preservative) -0.3% w/v, water for injection I.P- Q.S
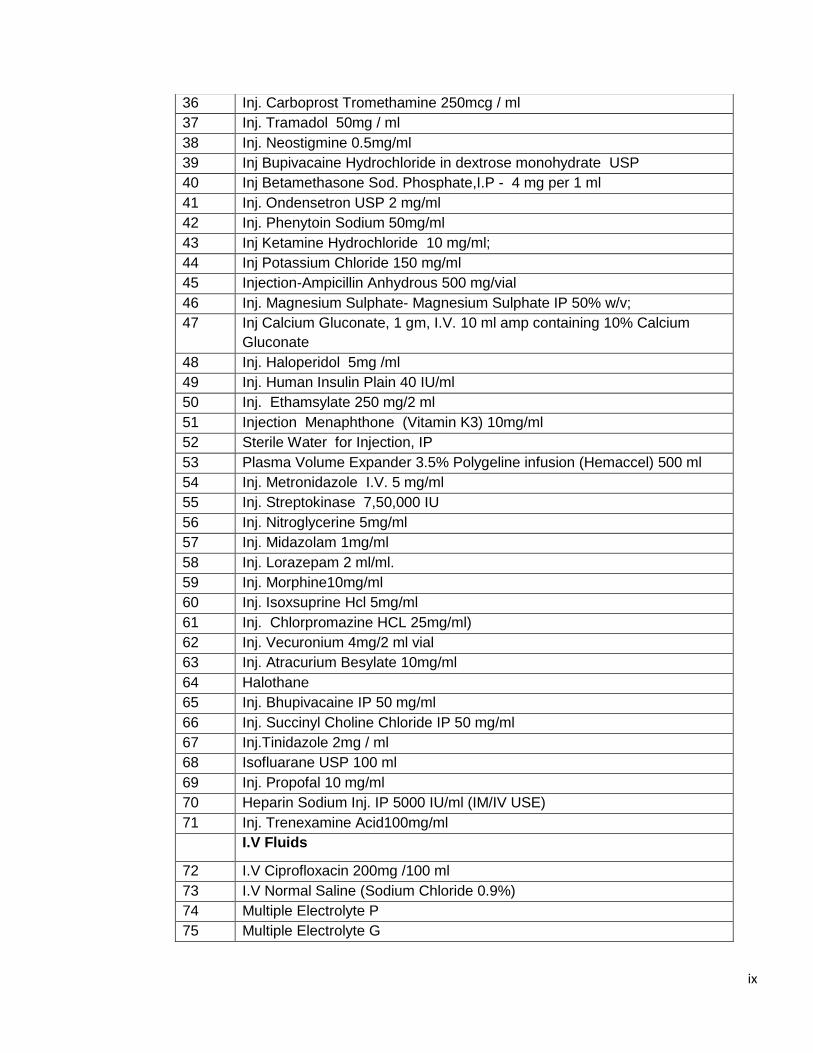
ix
36 Inj. Carboprost Tromethamine 250mcg / ml 37 Inj. Tramadol 50mg / ml 38 Inj. Neostigmine 0.5mg/ml 39 Inj Bupivacaine Hydrochloride in dextrose monohydrate USP 40 Inj Betamethasone Sod. Phosphate,I.P - 4 mg per 1 ml 41 Inj. Ondensetron USP 2 mg/ml 42 Inj. Phenytoin Sodium 50mg/ml 43 Inj Ketamine Hydrochloride 10 mg/ml; 44 Inj Potassium Chloride 150 mg/ml 45 Injection-Ampicillin Anhydrous 500 mg/vial 46 Inj. Magnesium Sulphate- Magnesium Sulphate IP 50% w/v; 47 Inj Calcium Gluconate, 1 gm, I.V. 10 ml amp containing 10% Calcium
Gluconate 48 Inj. Haloperidol 5mg /ml 49 Inj. Human Insulin Plain 40 IU/ml 50 Inj. Ethamsylate 250 mg/2 ml 51 Injection Menaphthone (Vitamin K3) 10mg/ml 52 Sterile Water for Injection, IP 53 Plasma Volume Expander 3.5% Polygeline infusion (Hemaccel) 500 ml 54 Inj. Metronidazole I.V. 5 mg/ml 55 Inj. Streptokinase 7,50,000 IU 56 Inj. Nitroglycerine 5mg/ml 57 Inj. Midazolam 1mg/ml 58 Inj. Lorazepam 2 ml/ml. 59 Inj. Morphine10mg/ml 60 Inj. Isoxsuprine Hcl 5mg/ml 61 Inj. Chlorpromazine HCL 25mg/ml) 62 Inj. Vecuronium 4mg/2 ml vial 63 Inj. Atracurium Besylate 10mg/ml 64 Halothane 65 Inj. Bhupivacaine IP 50 mg/ml 66 Inj. Succinyl Choline Chloride IP 50 mg/ml 67 Inj.Tinidazole 2mg / ml 68 Isofluarane USP 100 ml 69 Inj. Propofal 10 mg/ml 70 Heparin Sodium Inj. IP 5000 IU/ml (IM/IV USE) 71 Inj. Trenexamine Acid100mg/ml I.V Fluids
72 I.V Ciprofloxacin 200mg /100 ml 73 I.V Normal Saline (Sodium Chloride 0.9%) 74 Multiple Electrolyte P 75 Multiple Electrolyte G
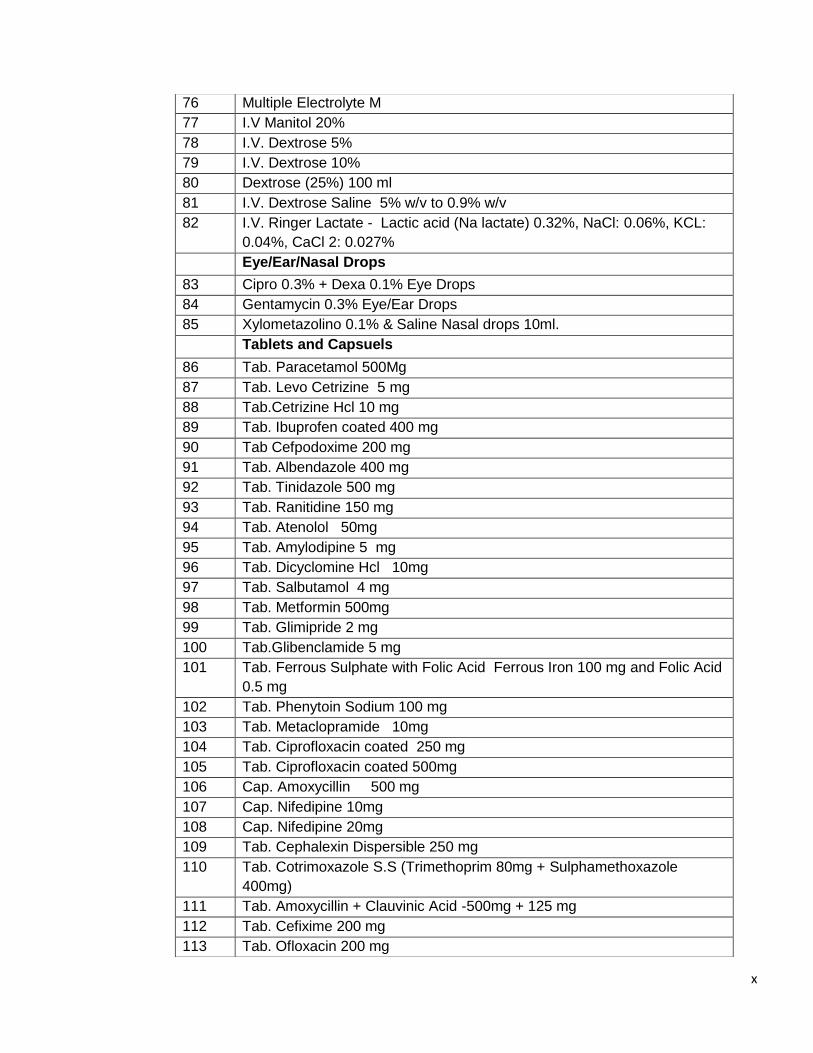
x
76 Multiple Electrolyte M 77 I.V Manitol 20% 78 I.V. Dextrose 5% 79 I.V. Dextrose 10% 80 Dextrose (25%) 100 ml 81 I.V. Dextrose Saline 5% w/v to 0.9% w/v 82 I.V. Ringer Lactate - Lactic acid (Na lactate) 0.32%, NaCl: 0.06%, KCL:
0.04%, CaCl 2: 0.027% Eye/Ear/Nasal Drops
83 Cipro 0.3% + Dexa 0.1% Eye Drops 84 Gentamycin 0.3% Eye/Ear Drops 85 Xylometazolino 0.1% & Saline Nasal drops 10ml. Tablets and Capsuels
86 Tab. Paracetamol 500Mg 87 Tab. Levo Cetrizine 5 mg 88 Tab.Cetrizine Hcl 10 mg 89 Tab. Ibuprofen coated 400 mg 90 Tab Cefpodoxime 200 mg 91 Tab. Albendazole 400 mg 92 Tab. Tinidazole 500 mg 93 Tab. Ranitidine 150 mg 94 Tab. Atenolol 50mg 95 Tab. Amylodipine 5 mg 96 Tab. Dicyclomine Hcl 10mg 97 Tab. Salbutamol 4 mg 98 Tab. Metformin 500mg 99 Tab. Glimipride 2 mg 100 Tab.Glibenclamide 5 mg 101 Tab. Ferrous Sulphate with Folic Acid Ferrous Iron 100 mg and Folic Acid
0.5 mg 102 Tab. Phenytoin Sodium 100 mg 103 Tab. Metaclopramide 10mg 104 Tab. Ciprofloxacin coated 250 mg 105 Tab. Ciprofloxacin coated 500mg 106 Cap. Amoxycillin 500 mg 107 Cap. Nifedipine 10mg 108 Cap. Nifedipine 20mg 109 Tab. Cephalexin Dispersible 250 mg 110 Tab. Cotrimoxazole S.S (Trimethoprim 80mg + Sulphamethoxazole
400mg) 111 Tab. Amoxycillin + Clauvinic Acid -500mg + 125 mg 112 Tab. Cefixime 200 mg 113 Tab. Ofloxacin 200 mg
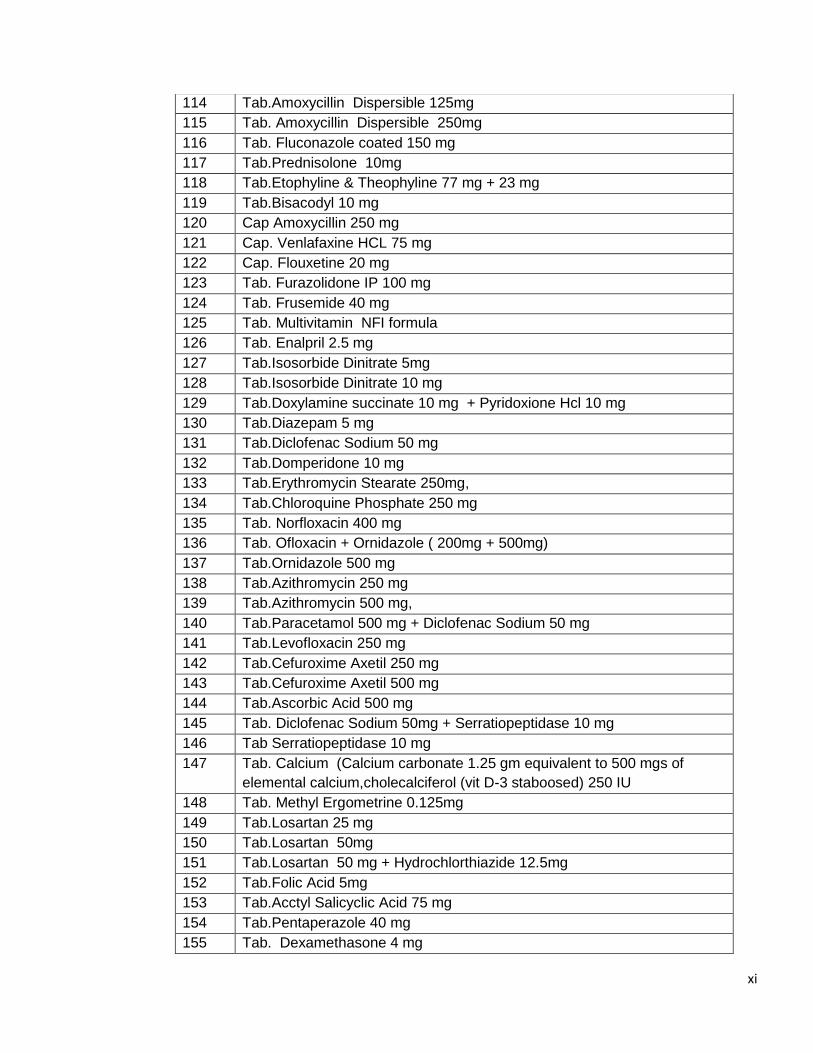
xi
114 Tab.Amoxycillin Dispersible 125mg 115 Tab. Amoxycillin Dispersible 250mg 116 Tab. Fluconazole coated 150 mg 117 Tab.Prednisolone 10mg 118 Tab.Etophyline & Theophyline 77 mg + 23 mg 119 Tab.Bisacodyl 10 mg 120 Cap Amoxycillin 250 mg 121 Cap. Venlafaxine HCL 75 mg 122 Cap. Flouxetine 20 mg 123 Tab. Furazolidone IP 100 mg 124 Tab. Frusemide 40 mg 125 Tab. Multivitamin NFI formula 126 Tab. Enalpril 2.5 mg 127 Tab.Isosorbide Dinitrate 5mg 128 Tab.Isosorbide Dinitrate 10 mg 129 Tab.Doxylamine succinate 10 mg + Pyridoxione Hcl 10 mg 130 Tab.Diazepam 5 mg 131 Tab.Diclofenac Sodium 50 mg 132 Tab.Domperidone 10 mg 133 Tab.Erythromycin Stearate 250mg, 134 Tab.Chloroquine Phosphate 250 mg 135 Tab. Norfloxacin 400 mg 136 Tab. Ofloxacin + Ornidazole ( 200mg + 500mg) 137 Tab.Ornidazole 500 mg 138 Tab.Azithromycin 250 mg 139 Tab.Azithromycin 500 mg, 140 Tab.Paracetamol 500 mg + Diclofenac Sodium 50 mg 141 Tab.Levofloxacin 250 mg 142 Tab.Cefuroxime Axetil 250 mg 143 Tab.Cefuroxime Axetil 500 mg 144 Tab.Ascorbic Acid 500 mg 145 Tab. Diclofenac Sodium 50mg + Serratiopeptidase 10 mg 146 Tab Serratiopeptidase 10 mg 147 Tab. Calcium (Calcium carbonate 1.25 gm equivalent to 500 mgs of
elemental calcium,cholecalciferol (vit D-3 staboosed) 250 IU 148 Tab. Methyl Ergometrine 0.125mg 149 Tab.Losartan 25 mg 150 Tab.Losartan 50mg 151 Tab.Losartan 50 mg + Hydrochlorthiazide 12.5mg 152 Tab.Folic Acid 5mg 153 Tab.Acctyl Salicyclic Acid 75 mg 154 Tab.Pentaperazole 40 mg 155 Tab. Dexamethasone 4 mg
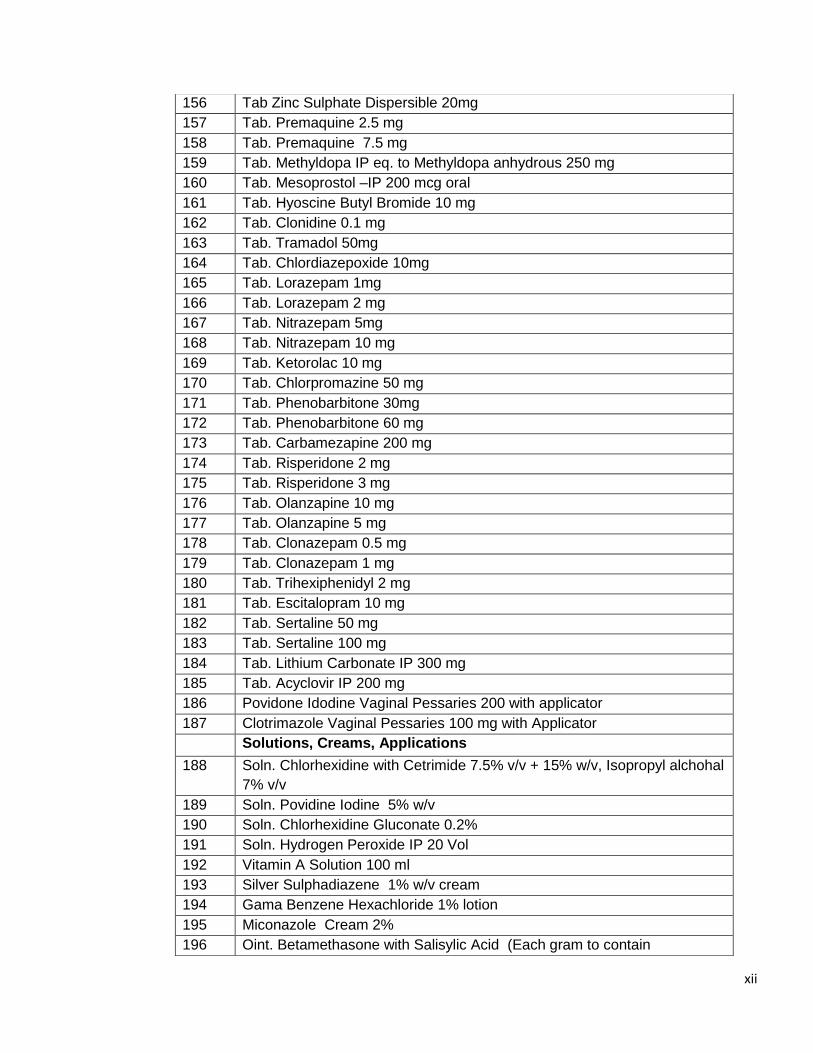
xii
156 Tab Zinc Sulphate Dispersible 20mg 157 Tab. Premaquine 2.5 mg 158 Tab. Premaquine 7.5 mg 159 Tab. Methyldopa IP eq. to Methyldopa anhydrous 250 mg 160 Tab. Mesoprostol –IP 200 mcg oral 161 Tab. Hyoscine Butyl Bromide 10 mg 162 Tab. Clonidine 0.1 mg 163 Tab. Tramadol 50mg 164 Tab. Chlordiazepoxide 10mg 165 Tab. Lorazepam 1mg 166 Tab. Lorazepam 2 mg 167 Tab. Nitrazepam 5mg 168 Tab. Nitrazepam 10 mg 169 Tab. Ketorolac 10 mg 170 Tab. Chlorpromazine 50 mg 171 Tab. Phenobarbitone 30mg 172 Tab. Phenobarbitone 60 mg 173 Tab. Carbamezapine 200 mg 174 Tab. Risperidone 2 mg 175 Tab. Risperidone 3 mg 176 Tab. Olanzapine 10 mg 177 Tab. Olanzapine 5 mg 178 Tab. Clonazepam 0.5 mg 179 Tab. Clonazepam 1 mg 180 Tab. Trihexiphenidyl 2 mg 181 Tab. Escitalopram 10 mg 182 Tab. Sertaline 50 mg 183 Tab. Sertaline 100 mg 184 Tab. Lithium Carbonate IP 300 mg 185 Tab. Acyclovir IP 200 mg 186 Povidone Idodine Vaginal Pessaries 200 with applicator 187 Clotrimazole Vaginal Pessaries 100 mg with Applicator Solutions, Creams, Applications
188 Soln. Chlorhexidine with Cetrimide 7.5% v/v + 15% w/v, Isopropyl alchohal 7% v/v
189 Soln. Povidine Iodine 5% w/v 190 Soln. Chlorhexidine Gluconate 0.2% 191 Soln. Hydrogen Peroxide IP 20 Vol 192 Vitamin A Solution 100 ml 193 Silver Sulphadiazene 1% w/v cream 194 Gama Benzene Hexachloride 1% lotion 195 Miconazole Cream 2% 196 Oint. Betamethasone with Salisylic Acid (Each gram to contain
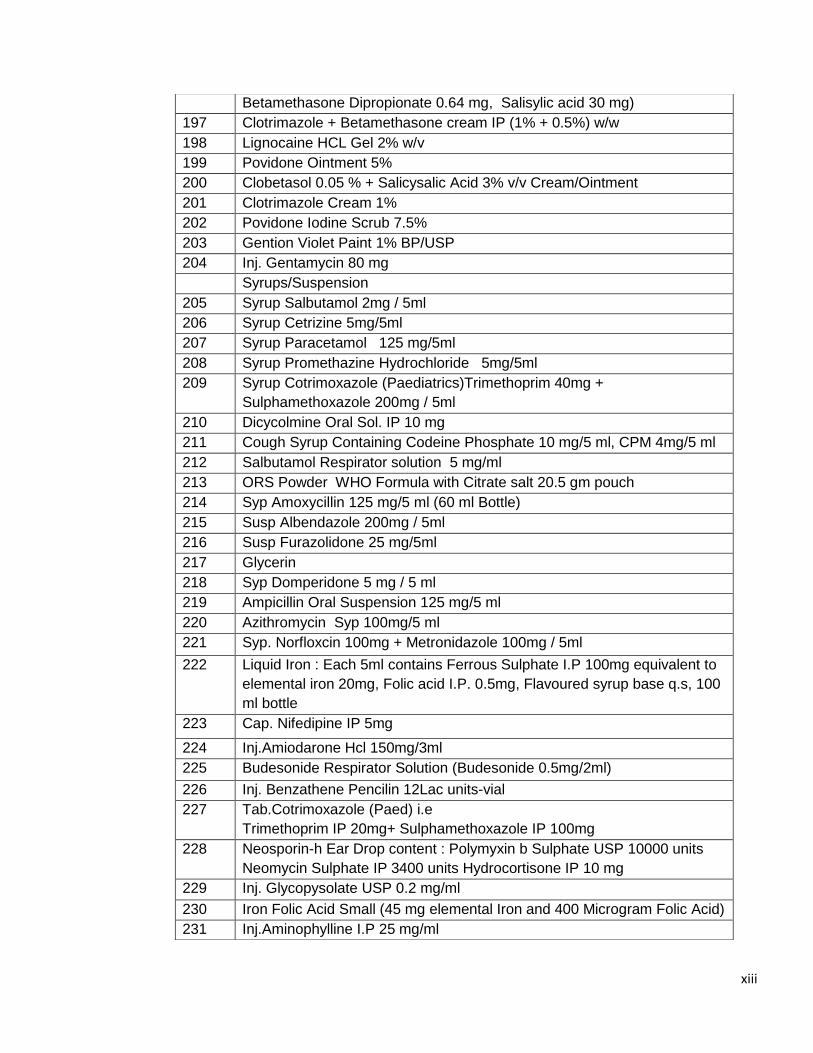
xiii
Betamethasone Dipropionate 0.64 mg, Salisylic acid 30 mg) 197 Clotrimazole + Betamethasone cream IP (1% + 0.5%) w/w 198 Lignocaine HCL Gel 2% w/v 199 Povidone Ointment 5% 200 Clobetasol 0.05 % + Salicysalic Acid 3% v/v Cream/Ointment 201 Clotrimazole Cream 1% 202 Povidone Iodine Scrub 7.5% 203 Gention Violet Paint 1% BP/USP 204 Inj. Gentamycin 80 mg Syrups/Suspension 205 Syrup Salbutamol 2mg / 5ml 206 Syrup Cetrizine 5mg/5ml 207 Syrup Paracetamol 125 mg/5ml 208 Syrup Promethazine Hydrochloride 5mg/5ml 209 Syrup Cotrimoxazole (Paediatrics)Trimethoprim 40mg +
Sulphamethoxazole 200mg / 5ml 210 Dicycolmine Oral Sol. IP 10 mg 211 Cough Syrup Containing Codeine Phosphate 10 mg/5 ml, CPM 4mg/5 ml 212 Salbutamol Respirator solution 5 mg/ml 213 ORS Powder WHO Formula with Citrate salt 20.5 gm pouch 214 Syp Amoxycillin 125 mg/5 ml (60 ml Bottle) 215 Susp Albendazole 200mg / 5ml 216 Susp Furazolidone 25 mg/5ml 217 Glycerin 218 Syp Domperidone 5 mg / 5 ml 219 Ampicillin Oral Suspension 125 mg/5 ml 220 Azithromycin Syp 100mg/5 ml 221 Syp. Norfloxcin 100mg + Metronidazole 100mg / 5ml
222 Liquid Iron : Each 5ml contains Ferrous Sulphate I.P 100mg equivalent to elemental iron 20mg, Folic acid I.P. 0.5mg, Flavoured syrup base q.s, 100 ml bottle
223 Cap. Nifedipine IP 5mg
224 Inj.Amiodarone Hcl 150mg/3ml 225 Budesonide Respirator Solution (Budesonide 0.5mg/2ml)
226 Inj. Benzathene Pencilin 12Lac units-vial 227 Tab.Cotrimoxazole (Paed) i.e
Trimethoprim IP 20mg+ Sulphamethoxazole IP 100mg 228 Neosporin-h Ear Drop content : Polymyxin b Sulphate USP 10000 units
Neomycin Sulphate IP 3400 units Hydrocortisone IP 10 mg 229 Inj. Glycopysolate USP 0.2 mg/ml
230 Iron Folic Acid Small (45 mg elemental Iron and 400 Microgram Folic Acid) 231 Inj.Aminophylline I.P 25 mg/ml
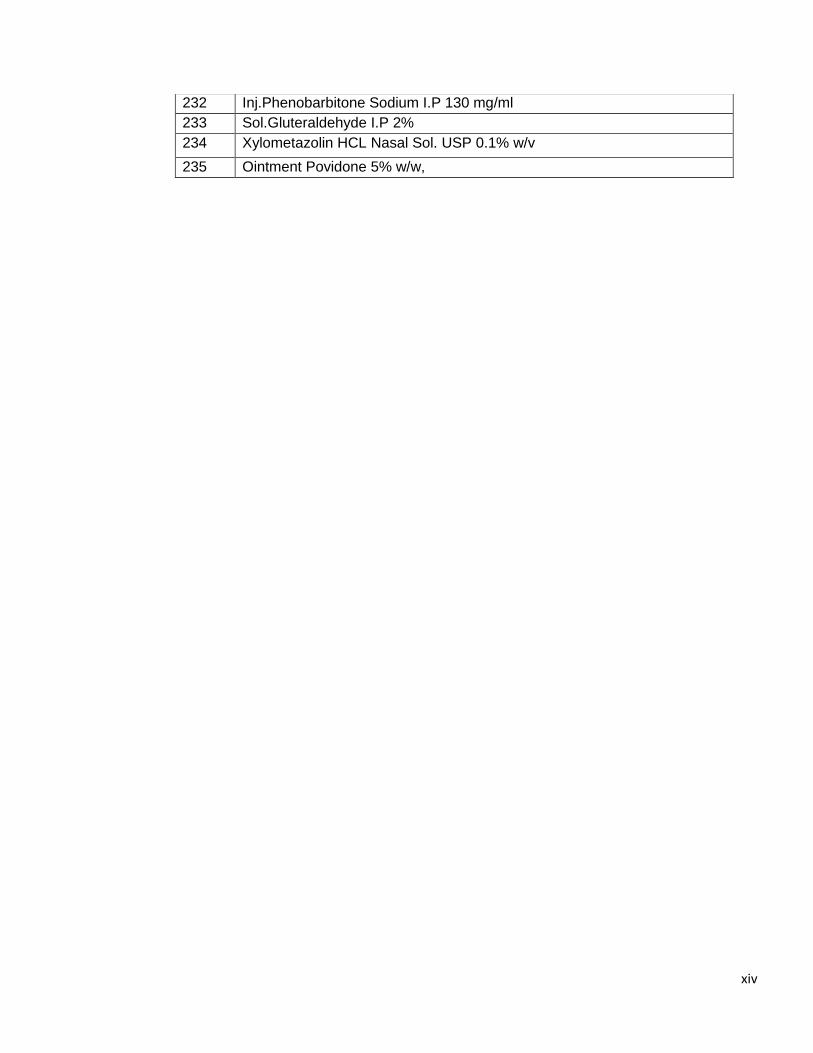
xiv
232 Inj.Phenobarbitone Sodium I.P 130 mg/ml 233 Sol.Gluteraldehyde I.P 2% 234 Xylometazolin HCL Nasal Sol. USP 0.1% w/v
235 Ointment Povidone 5% w/w,
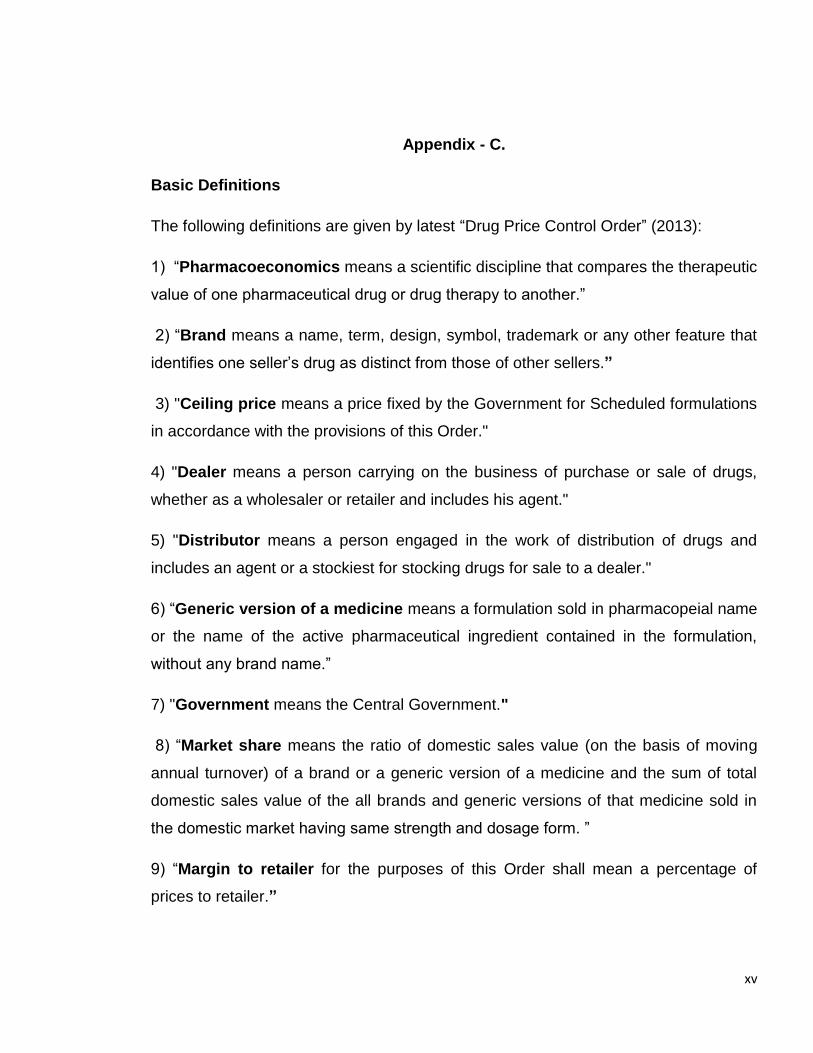
xv
Appendix - C.
Basic Definitions
The following definitions are given by latest “Drug Price Control Order” (2013):
1) “Pharmacoeconomics means a scientific discipline that compares the therapeutic
value of one pharmaceutical drug or drug therapy to another.”
2) “Brand means a name, term, design, symbol, trademark or any other feature that
identifies one seller’s drug as distinct from those of other sellers.”
3) "Ceiling price means a price fixed by the Government for Scheduled formulations
in accordance with the provisions of this Order."
4) "Dealer means a person carrying on the business of purchase or sale of drugs,
whether as a wholesaler or retailer and includes his agent."
5) "Distributor means a person engaged in the work of distribution of drugs and
includes an agent or a stockiest for stocking drugs for sale to a dealer."
6) “Generic version of a medicine means a formulation sold in pharmacopeial name
or the name of the active pharmaceutical ingredient contained in the formulation,
without any brand name.”
7) "Government means the Central Government."
8) “Market share means the ratio of domestic sales value (on the basis of moving
annual turnover) of a brand or a generic version of a medicine and the sum of total
domestic sales value of the all brands and generic versions of that medicine sold in
the domestic market having same strength and dosage form. ”
9) “Margin to retailer for the purposes of this Order shall mean a percentage of
prices to retailer.”
xvi
10) “Market based data means the data of sales related to a drug collected or
obtained by the Government as deemed fit, from time to time.”
11) “Maximum retail price means the ceiling price or the retail price plus local taxes
and duties as applicable, at which the drug shall be sold to the ultimate consumer and
where such price is mentioned on the pack.”
12) "Non-scheduled formulation means a formulation, the dosage and strengths of
which are not specified in the First Schedule."
13) “Price to retailer means the price of a drug at which it is sold to a retailer which
includes duties and does not include local taxes”
14) "Retail price means the price fixed by the Government for a new drug."
15) "Retailer means a dealer carrying on the retail business of sale of drugs to
customers."
16) "Wholesaler means a dealer or his agent or a stockist engaged in the sale of
drugs to a retailer, hospital, dispensary, medical, educational or research institution or
any other agency.





























