Embed Size (px)
Citation preview

This article appeared in a journal published by Elsevier. The attachedcopy is furnished to the author for internal non-commercial researchand education use, including for instruction at the authors institution
and sharing with colleagues.
Other uses, including reproduction and distribution, or selling orlicensing copies, or posting to personal, institutional or third party
websites are prohibited.
In most cases authors are permitted to post their version of thearticle (e.g. in Word or Tex form) to their personal website orinstitutional repository. Authors requiring further information
regarding Elsevier’s archiving and manuscript policies areencouraged to visit:
http://www.elsevier.com/copyright

Author's personal copy
Invited papers presented at the EPNS 2011 Cavtat meeting
Cardiac arrest and post resuscitation of the brain
Fenella Kirkhama,b,*aUCL Institute of Child Health, UKb Southampton General hospital, London WCIN 2AP, UK
a r t i c l e i n f o
Article history:
Received 28 March 2011
Accepted 17 April 2011
Keywords:
Hypoxic-ischaemic encephalopathy
Out-of-hospital cardiac arrest
In-hospital cardiac arrest
Near drowning
Electroencephalography
Evoked potentials
Prognosis
Hypothermia
Extracorporeal membrane
oxygenation
a b s t r a c t
Primary out-of-hospital cardiac arrest in childhood is rare but survival is a little better for
children than for adults, although the prognosis for infants is very poor. Hypoxic-
ischaemic encephalopathy after in-hospital cardiac arrest in children undergoing
complicated treatment for previously untreatable conditions is now a common problem
and is probably increasing. An additional ischaemic insult worsens the prognosis for other
encephalopathies, such as that occurring after accidental or non-accidental head injury.
For near-drowning, the prognosis is often good, provided that cardiopulmonary resusci-
tation (CPR) is commenced immediately, and the child gasps within 40 minutes of rescue
and regains consciousness soon afterwards. The prognosis is much worse for the nearly
drowned child admitted to casualty or the emergency room deeply unconscious with fixed
dilated pupils, requiring continuing CPR and with an arterial pH <7, especially if there is
little recovery by the time of admission to the intensive care unit. The use of adrenaline,
sodium bicarbonate and calcium appears to worsen prognosis. Neurophysiology, specifi-
cally serial electroencephalography and evoked potentials, is the most useful tool prog-
nostically, although neuroimaging and biomarkers may play a role. In a series of 89
patients studied after cardiac arrest in three London centres between 1982 and 1985, 39%
recovered consciousness within one month. Twenty seven percent died a cardiac death
whilst in coma, and the outcome in the remainder was either brain death or vegetative
state. EEG and initial pH were the best predictors of outcome in this study. Seizures
affected one third and were associated with deterioration and worse outcome. The advent
of extracorporeal membrane oxygenation (ECMO) and the positive results of hypothermia
trials in neonates and adults have rekindled interest in timely management of this
important group of patients.
ª 2011 European Paediatric Neurology Society. Published by Elsevier Ltd. All rights
reserved.
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3802. Specific causes of hypoxic-ischaemic encephalopathy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 380
2.1. Trauma . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3802.2. Near drowning . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 380
* Corresponding author. UCL Institute of Child Health, UKE-mail address: [email protected].
Official Journal of the European Paediatric Neurology Society
e u r o p e a n j o u r n a l o f p a e d i a t r i c n e u r o l o g y 1 5 ( 2 0 1 1 ) 3 7 9e3 8 9
1090-3798/$ e see front matter ª 2011 European Paediatric Neurology Society. Published by Elsevier Ltd. All rights reserved.doi:10.1016/j.ejpn.2011.04.009

Author's personal copy
2.3. Sudden infant death . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3812.4. Electrocution injuries . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3812.5. Lightning . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 381
3. Management . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3813.1. Resuscitation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3813.2. Prevention of secondary brain damage . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 382
3.2.1. Management of intracranial hypertension . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3823.2.2. Management of seizures . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3823.2.3. Hypothermia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 383
4. Outcome . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3834.1. Patterns of neurological damage in survivors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 383
4.1.1. Persistent vegetative state . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3834.1.2. Visual problems . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3834.1.3. Motor disorders . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 383
5. Prediction of outcome . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3845.1. General information . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 384
5.1.1. Age . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3845.1.2. Underlying aetiology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3845.1.3. Nature of arrest . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3845.1.4. Duration of arrest . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 384
5.2. Clinical signs . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3845.3. Neurophysiology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 384
5.3.1. Conventional electrophysiology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3845.3.2. Monitoring EEG . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3855.3.3. Evoked potentials . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 385
5.4. Neuroradiology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3855.5. Biochemistry . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 385
6. Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 386Acknowledgements . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 386References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 386
1. Introduction
Unexpected cardiac arrest in a previously well child is
uncommon,1e4 but occurs in infants (sudden infant death
syndrome),5 occasionally during exercise or as a consequence
of accidents such as trauma, near drowning, electrocution and
strangulation. In a North American study, the incidence of
paediatric out-of-hospital cardiac arrest was 8.04 per 100,000
person-years (72.71 in infants, 3.73 in children, and 6.37 in
adolescents) versus 126.52 per 100,000 person-years for adults.
Survival for all pediatric out-of-hospital cardiac arrest was
6.4% (3.3% for infants, 9.1% for children, and 8.9% for adoles-
cents) versus 4.5% for adults (P ¼ 0.03). In a Korean study, the
incidence of paediatric out-of-hospital cardiac arrest was 4.2
per 100,000 person-years (67.1 in infants, 2.5 in children, and
3.5 in adolescents).4 The improvement in the management of
complex conditions in children means that in-hospital
paediatric cardiopulmonary resuscitation is now common-
place in casualty, on the ward, in theatre and in intensive
care.6,7 Kirkham10 studied 89 children with HIE presenting to
three London hospitals between 1982 and 1985, only 4% of
whom had suffered an out-of-hospital arrest. The underlying
aetiology was cardiological in 72%, respiratory in 15% and
neurological in 6%. If ventilation is available, the prognosis for
in-patient paediatric cardiac arrest is better than for out-of-
hospital resuscitations, with an overall hospital survival of
20.9% and 16.1% having favorable neurological outcomes in
one study.8 However, survival is unusual without ventilation.9
2. Specific causes of hypoxic-ischaemicencephalopathy
2.1. Trauma
Accidental and non-accidental traumatic brain injury is
common; cardiorespiratory arrest may be secondary to the
severity of the head injury, to haemorrhage from associated
injuries or to brain stem or spinal cord damage and is a very
poorprognostic sign.11e15 In a recent series, 3/28 (11%) survived
to hospital discharge, 2 with respiratory arrest neurologically
intact; none survived if CPR was required for > 20 mins.11
2.2. Near drowning
Even in water-oriented societies, immersion accidents are
relatively rare (incidence 3e6 per 100,000,16 but over half the
children admitted to hospital survive17,18 and they often
require intensive management. The prognosis for the child
pulled from the water apparently dead is excellent, provided
e u r o p e a n j o u r n a l o f p a e d i a t r i c n e u r o l o g y 1 5 ( 2 0 1 1 ) 3 7 9e3 8 9380

Author's personal copy
that cardiopulmonary resuscitation is commenced immedi-
ately, that the child gasps within 40 min of rescue and regains
consciousness soon afterwards. The prognosis is much worse
for the child admitted to casualty or the emergency room
deeply unconscious (Glasgow coma score less than 519) with
fixed dilated pupils and apnoea,20 without a detectable pulse21
and therefore requiring continuing cardiopulmonary resusci-
tation, especially if there is little recovery by the time of
admission to the intensive care unit.22 In a meta-analysis,5 for
this group, 23% survived and 6% had good neurological
outcome. Laboratory measures suggesting poor outcome
include an arterial pH of less than 7.0023,24 and hyper-
glycaemia.25,26 Persistent seizures are a poor prognostic
sign.18 Several authors have found EEG to be a useful predictor
of outcome, particularly if there is deterioration compared
with the record performed at 24 h.27e29 Evoked potentials may
also be useful.30,31 None of these poor prognostic indicators
precludes a good outcome,18 although a combination makes
severe handicap or vegetative survival likely, since moderate
handicap is rare after near-drowning.32 Apparently miracu-
lous recoveries have occurred, mainly of children who have
been submerged in very cold water for long periods18 and
present to Casualty with a temperature of less than 33 �C.21
2.3. Sudden infant death
The risk factors for sudden infant death syndrome include
sleeping in the prone position, bed-sharing,maternal smoking
and alcohol use and infection or other illness. Childrenmay be
found to have died of presumed prolonged QT syndrome
secondary to cardiac ion channel mutations (diagnosable on
DNA from Guthrie) metabolic disease such as medium chain
acyl-coA deficiency carnitine palmitoyltransferase 1A vari-
ants or to be the victims of child abuse. Compared with the
extensive literature on the epidemiology and aetiology of
sudden infant death (SID), there is very little data available on
the prognosis for those infants who are resuscitated at the
scene or in hospital (“near-miss”SID). Infants presenting in
status epilepticus may have been the victims of hypoxic-
ischaemic events akin to “near-miss” episodes. Con-
stantinou33 described the clinical course in 14 patients. Half
were deeply unconscious on admission and succumbed
within 3 days. Five appeared conscious initially but later
deterioratedwith persistent status epilepticus, deep coma and
signs of brain stem dysfunction; the other two survivors were
unconscious on admission but also developed status epi-
lepticus. Overall the prognosis was extremely poor; only one
child survived without severe brain damage.
2.4. Electrocution injuries
These are unusual events in childhood, but can be devastating
in their consequences. Small children are most at risk of
electrocution in the home, while older boys are more
commonly involved in high tension electrical injuries.
Neurological problems can be directly caused by the electrical
injury or are secondary to the associated cardiac arrest.34
There is also evidence for late demyelination, particularly in
the spinal cord, and late extrapyramidal disorders.35 Atonic
and myoclonic seizures are not uncommon in the longterm,
and there is a very high incidence of emotional disorders in
adults. Children may occasionally recover after prolonged
coma.36
2.5. Lightning
Lightning injuries can occur at any age, but there are few
published data in children. Again, the pathology, which may
include haemorrhage, results either directly from the injury or
as a consequence of cardiac arrest.37 The prognosis is poor
with a 30% mortality and sequelae (not necessarily neuro-
logical) in the majority of survivors; cardiopulmonary arrest,
loss of consciousness at the scene and leg or cranial burns
suggest a poor prognosis. Acutely, the neurological manifes-
tations in children can include coma, seizures and ataxia;
changes in memory and mood can persist for long periods of
time.38
3. Management
3.1. Resuscitation
The prime aims of emergency resuscitation attempts are to
restore spontaneous circulation whilst maintaining suffi-
cient myocardial and cerebral blood flow to prevent irre-
versible ischaemic damage. Most studies of CPR have been
conducted in adults, in whom spontaneous circulation is
often successfully restored after cardioversion of ventricular
fibrillation or tachycardia. External cardiac massage (ECM),
introduced in the early 1960s, almost completely replaced
the previously standard open cardiac massage (OCM), as it
was less invasive and could be performed by anybody
anywhere. For children who have out-of-hospital cardiac
arrests from non-cardiac causes, conventional CPR (with
rescue breathing) by bystander is the preferable approach to
resuscitation, while for arrests of cardiac causes, either
conventional or compression-only CPR is similarly effec-
tive.39 As there is evidence for better outcome after in-
patient resuscitation by a paediatric trainee,6 Paediatric
Advanced Life Support (PALS) training should be mandatory
for doctors looking after children.40 For in-hospital arrests, it
is possible to generate higher mean arterial, coronary and
cerebral perfusion pressures with OCM41,42 and it may be
possible to institute emergency cardiopulmonary bypass or
extracorporeal membrane oxygenation,43e50 but this tech-
niques is invasive, requiring a highly experienced team and
there is currently little evidence for benefit.
Hyperoxia and hypocapnia51 should be avoided. The
drugs commonly used during cardiac arrest include the
inotrope adrenaline (epinephrine), sodium bicarbonate and
calcium but there are concerns that all three worsen
outcome. The prognosis is poor for children requiring
adrenaline for drowning and other causes of out-of-hospital
cardiac arrest.6,52 In Moler’s recent multicentre series,
receiving more than three doses of adrenaline was associ-
ated with poor outcome in 96% (44 of 46) of cases.52 Terli-
pressin may be an alternative.53 In addition to longstanding
concerns over the use of calcium,54 the use of sodium
e u r o p e a n j o u r n a l o f p a e d i a t r i c n e u r o l o g y 1 5 ( 2 0 1 1 ) 3 7 9e3 8 9 381

Author's personal copy
bicarbonate/tromethamine also appears to be a predictor of
death.49,55
3.2. Prevention of secondary brain damage
Some patients recover consciousness very soon after a brief
episode of cardiac arrest and usually make a full recovery. In
others, the brainmay be severely and irreversibly damaged by
the initial insult; most of these patients either fulfil the clinical
criteria for brain stem death or have neurophysiological
evidence of a poor prognosis within 24 h of the event. It is the
management of the intermediate group, who remain uncon-
scious but with some evidence of brain stem function clini-
cally and cortical function neurophysiologically, which
remains extremely controversial, particularly as some
patients appear to deteriorate secondarily. Whilst awaiting
results of further studies, there are a few management strat-
egies which can be recommended as being probably safe but
of unproven efficacy; these should preferably be reserved for
the intermediate group who remain unconscious but without
evidence of irreversible damage.
3.2.1. Management of intracranial hypertension
3.2.1.1. Cardiac arrest. There are very few published data,
and many groups have given up monitoring and aggressively
managing intracranial hypertension in children with HIE for
fear of increasing the number of children left severely hand-
icapped or in a persistent vegetative state.56 However, as good
outcome has been reported in some cases in whom intracra-
nial hypertension has been vigorously prevented or managed,
e.g. with surgical decompression,57 monitoring should be
considered for the individual child. Intracranial pressure was
monitored in 18 of the patients in the Guy’s paediatric study57
andwas persistently raised (mean ICP greater than 10mmHg)
in 10 of these. The two children with good outcome and the
child who made a cognitive recovery but was left with
a spastic quadriparesis (probably due to a posterior fossa
haematoma) all had mean ICP between 9 and 15 mm Hg and
maximum ICP up to 35 mm Hg (i.e. above the normal range,
but mean CPP was maintained above 60 mmHg and CPP never
fell below 37 mm Hg. In the other 15 children, either the EEG
prior to ICP monitoring suggested a poor outcome58 or mean
CPP could not be maintained above 60 mm Hg and minimum
CPP above 40 mm Hg because of poor cardiac function or
persistent intracranial hypertension. Opening, maximum and
mean ICP did not predict outcome, but minimum and mean
CPP did.
Appropriate candidates have been well-resuscitated using
modern cardiopulmonary resuscitation techniques, so that
the EEG has recovered to diffuse slowing or better, despite
continuing unconsciousness or sedation for ventilation.
Cerebral perfusion pressure (CPP)must be frequently recorded
and managed appropriately.
3.2.1.2. Near drowning. Intracranial hypertension is
a common but not universal feature of the encephalopathy
which follows serious near-drowning incidents,59,60 although
again, whether or not treatment prevents secondary deterio-
ration is much more controversial.22,61 Intracranial
hypertension,59 low cerebral perfusion pressure,60 and low
cerebral blood flow25 are all predictors of death but do not
distinguish between intact and vegetative survival.Criteria for
ICP monitoring should be the same as for HIE.
3.2.2. Management of seizuresSeizures are not uncommon after cardiac arrest in children.
After near miss sudden infant death, a brief seizure may be
compatible with good outcome but status epilepticus carries
a very poor prognosis62 even if the child had recovered
consciousness between the event and the onset of
seizures.33,63 Many children are sedated and paralysed for
ventilation after cardiac arrest and so observation of seizures
may be impossible. There are very few data on the prevalence
of non-convulsive seizures (NCS) or non-convulsive status
epilepticus (NCSE) in childhood hypoxic-ischaemic encepha-
lopathy. NCSE is common in neonates after asphyxia, and in
comatose adults, and appears to predict death and poor
outcome. One third of the children in the Guy’s study10 had
a clinical fit or an EEG seizure discharge at some stage post-
arrest. Short seizures did not preclude good outcome, but
seizures or electrical discharges lasting longer than 20 min
were associated with secondary deterioration. It is becoming
widespread practice that unconscious children have an EEG to
determine establish whether clinically recognised seizures
have terminated or to distinguish subtle seizures from
movement disorders secondary to drug withdrawal.64e66
Routine or continuous EEG (cEEG) with or without video
recording seems to diagnose non-convulsive seizures or non-
convulsive status epilepticus (NCS or NCSE) and there is some
evidence for an association with outcome.66
There is a good case for giving therapeutic doses of
conventional anticonvulsants, e.g. benzodiazepines,
phenobarbitone, phenytoin, to children after global ischae-
mic insults either prophylactically or as treatment for clin-
ical seizures or electroencephalographic discharges,
particularly if the EEG background is compatible with good
prognosis. Continuous infusion of short-acting benzodiaz-
epines, such as midazolam, may be of benefit in certain
selected patients with status epilepticus. Chlormethiazole is
not recommended for the control of seizures after cardiac
arrest since the fluid volume is substantial and there is
a significant risk of volume overload if the patient has
a degree of acute renal failure. Although there are concerns
about the drug’s effect on the cardiac conducting system, it
is probably safe to use phenytoin (loading dose 20 mg/kg,
then 5 mg/kg/day in 2 divided doses with regular drug
levels) in patients who do not have ongoing cardiac
dysrhythmias provided that the drug is infused over at least
45 min. Phenobarbitone may also be effective in controlling
seizures in unconscious patients and again, it may be worth
pushing the drug dose towards the top end of the thera-
peutic range as additional sedation is not usually a problem.
Thiopentone coma is contraindicated because there are
significant problems with cardiac depression67,68 and with
diagnosing irreversible brain damage and this management
strategy has now been largely abandoned. Other anaes-
thetics such as ethomidate and althesin either do not have
a significant protective effect after ischaemia or are associ-
ated with unacceptable side effects.
e u r o p e a n j o u r n a l o f p a e d i a t r i c n e u r o l o g y 1 5 ( 2 0 1 1 ) 3 7 9e3 8 9382

Author's personal copy
3.2.3. HypothermiaThepublicationof randomisedcontrolled trials showingbenefit
in terms of survival and neurological outcome for hypothermia
in adults69e73 and neonates74e79 with hypoxia-ischaemia has
reopened the question of whether children who have had
a cardiac arrest would benefit from maintenance of hypo-
thermia, e.g. after near drowning, or immediate cooling, e.g.
after in- or out-of-hospital cardiac arrest of other aetiologies.
Although return of consciousness was commoner after resus-
citationduring thecoldseason inoneseries79 andhyperthermia
in the first 24 hours post-arrest predicts poor neurological
outcome,7 mortality was not related to hyperthermia7 and
return-of-circulation is more likely with a higher lowest
temperature recorded.52 Clinical experience with the use of
hypothermia in children with near-drowning suggested that
moderate hypothermia of 30e33� centigrade is associated with
a very significant risk of neutropaenia and infection.67 Mild
hypothermia has been used after cardiac arrest in children, but
typically in those predicted to do worse80; at present the avail-
able data do not make the case for benefit but it is clear that
randomisedtrialsareneeded.81e83Arecentsurveryofpaediatric
intensivists in theUnitedKingdomfound that abouthalfdiduse
cooling for children who had had a cardiac arrest for a median
durationof24e48h (range4e72h)atmediantarget temperature
of 34 �Ce35 �C (range 32 �Ce37 �C).More that two thirds of those
using hypothermia for children targetted a temperature range
higher than that applied in the published adult and neonatal
studies (33 � 1 �C), perhaps because of the previous negative
experience with lower temperatures in children.There may be
a case for selective cooling of the head or a reduction of the core
temperature to 32e34 �C after cardiac arrest in some children
despite the lack of controlled trials.82,83 If a cooling turban or
blanket is available, hypothermia may be initiated quickly
during in-hospital cardiac arrest and may be discontinued
equally rapidly for clinical examinations or if there are
unwanted effects. It will be interesting to see if xenon has
a synergystic effect.
4. Outcome
The outcome for cardiac arrest varies greatly from series to
series, depending on the selection of patients. For in-patients,
up to 64% are successfully resuscitated in paediatric series.
Survival drops rapidly so that longterm mortality reaches
60e90% even in children. In a recent series, 27% of children
survived and 18% had good neurological outcome, percent-
ages which were better than adults despite a lower proportion
with ventricular fibrillation as the first rhythm.84 The
proportion of those resuscitated from out-of-hospital arrest
tends to be lower,5 but in some series more awaken and
survive to discharge.
Overall, the prognosis for hypoxic-ischaemic encephalop-
athy in childhood is poor.33,85 In our series of 89 patients,10
only 35% recovered consciousness within one month and
just over a third of these had good outcome at follow up at
least 2 years later. Twenty seven percent died a cardiac death
whilst in coma, and the outcome in the remainder was either
brain death or vegetative state. In another paediatric series of
patients resuscitated in the emergency room, only 5 of 91
patients were discharged from hospital and only 2 of these
were normal.86 There was a higher survival rate (20%) in
O’Rourke’s series but none were normal.87
4.1. Patterns of neurological damage in survivors
There are few longterm follow-up data on children who have
suffered a cardiac arrest. It may be very difficult to document
specific neurological handicaps in a young child and these
may change with time in the developing brain. Occasionally,
considerable recovery takes place in the first year after injury
although this is more likely in the cognitive and visual
spheres; a severe mixed motor disorder apparent soon after
an ischaemic event usually persists andmay sometimesmask
improvement in intellectual function.
Survivors of near-drowning in childhood either make an
excellent recovery, sometimes withminormotor problems, or
are left in a vegetative state.32 However, for other causes of
cardiac arrest in the Guy’s study of paediatric cardiac arrest,10
moderate (n ¼ 3) and severe (n ¼ 7) handicap were seen at the
one month follow-up as well as vegetative state (n ¼ 3), but
good outcome (n ¼ 21) with no obvious deficit was also
common. Some of these children had died of their underlying
disease by the time of the more detailed two year follow-up,
but again in the survivors, good outcome or moderate hand-
icap were much commoner than severe handicap.
4.1.1. Persistent vegetative statePersistent vegetative state (PVS) may be defined as a state of
consciousness without awareness and is well recognised in
children after severe ischaemic insults.88 Although PVS is
a common outcome after intensive therapy for paediatric
near-drowning,25 the overall incidence appears to be lower in
children with HIE than in adults.89 For example in the Guy’s
study10 none of the 3 in a PVS at one month survived for more
than a year.
4.1.2. Visual problemsBlindness is a common consequence of coma due to cardiac
arrest in children.33,90 The occipital cortex is particularly
vulnerable to ischaemic damage either because the posterior
cerebral circulation is compromised directly or when there is
border zone ischaemia between the posterior and middle
cerebral arteries. In addition there is some evidence for
a retinopathy after cardiac arrest in childhood.91 Vision
recovers to some extent in many patients and some children
who are apparently blind for 2e3months after hypotension or
cardiac arrest eventually make a good recovery.90
4.1.3. Motor disordersQuadriparesis (often mixed dystonic and spastic) is a rela-
tively common consequence of HIE in infants and young
children.33 Dystonia with a delay in onset (mean delay 12.9
years) has been well described after hypoxic-ischaemic
insults in children and may respond to treatment with anti-
cholinergics or L-Dopa.35 A transient dystonic syndrome with
onset a few days after the insult has also been recognised and
may be related to changes in the balance of neurotransmit-
ters. Action myoclonus may occasionally develop and
e u r o p e a n j o u r n a l o f p a e d i a t r i c n e u r o l o g y 1 5 ( 2 0 1 1 ) 3 7 9e3 8 9 383

Author's personal copy
sometimes responds to sodium valproate or clonezepam.
Spinal cord damage has been described.
5. Prediction of outcome
A number of papers have been published addressing the
problems of whether survival and neurological outcome can
be predicted after cardiac arrest and if so, which variables give
the best prediction and how soon after cardiac arrest a reliable
picture can be obtained. Authors have looked at general
information about the patient available at the time of the
arrest or soon afterwards, at clinical examination and at the
results of additional investigations such as EEG, biochemical
markers and neuroradiology.
5.1. General information
5.1.1. AgeBell and Hodgson92 found that coma was commoner in those
aged less than 10 years than in adults, but overall outcome
was not worse in the younger patients. In the Guy’s study,10
those who recovered conciousness by one month were
significantly younger (median 5 months) than those who did
not (median 2 years).
5.1.2. Underlying aetiologyThe range of conditions underlying cardiac arrest in childhood
is very wide and aetiology does not appear to be predictive of
outcome.10 Coma before cardiopulmonary resuscitation is
predictive of poor outcome, however. In Von Seggern’s
series,93 76% of those who were alert before cardiac arrest
survived more than 24 h whereas only 30% of those who were
unconscious survived more than 24 h. The outcome for
cardiac (rather than respiratory) arrest in the context of
trauma is poor.5,11 Prognosis is less good for obese children.94
5.1.3. Nature of arrestThere is no doubt that mortality and morbidity are lower for
respiratory than for cardiac or cardiorespiratory arrests. In
adults, the prognosis for survival and/or good neurological
outcome appears to be better if cardiac arrest is due to
ventricular fibrillation, which is less common in paediatric
arrests,86 than if it is due to asystole.
5.1.4. Duration of arrestFor arrests occurring in the emergency room86 or on the
general ward6 those who survive neurologically intact are
promptly resuscitated and respond rapidly. The situation
may be different for those who arrest in theatre or on ITU
and who receive prompt and effective resuscitation. Von
Seggern93 found that 26% of those requiring more than an
hour for stabilisation were alive and awake at 24 h. In the
Guy’s study,10 duration of cardiac arrest (asystole or rarely
VF) and of hypotension were both highly significantly related
to the one month outcome, but an occasional patient with an
arrest time of up to an hour made a good recovery. The
results were not affected by the time to resuscitation in this
study.
5.2. Clinical signs
There is no doubt that survival and good neurological
outcome are less common for those in coma after cardiac
arrest and that duration of coma is predictive of outcome.92
The timing of the clinical examination is very important
and there is a lot of evidence that serial testing is preferable to
a single examination. Although some isolated clinical signs
and combinations of signs appear to be highly predictive of
good or poor outcome, it may be impossible to predict
outcome accurately at an early enough stage to influence
management. In the Guy’s study,10 18 of the 43 children who
recovered consciousness within the first month apparently
had a modified Glasgow coma score less than 9 at 24 h, and 12
remained in this condition at 72 h. The problem with this
study of mainly in-patient arrest was that the children were
sedated and often also paralysed for ventilation, and
although efforts were made to withold drugs prior to exami-
nations, clinical signs may have been obscured. EEG added
a great deal of information, particularly within the first 24 h
(see below).
Clinical deterioration after initial improvement is well
recognised after paediatric cardiac arrest33,85 and is associated
with poorer outcome. In our paediatric series of 89 patients,10
23 showed partial recovery of consciousness and of brain stem
function, and recovery of the EEG to diffuse slowing or better,
and then deteriorated with poor eventual neurological
outcome. Factors associatedwith this secondary deterioration
included prolonged seizures (longer than 20 min), a positive
fluid balance of more than 7%, and a mean arterial pressure,
averaged over the first 24 h, of less than 50 mm Hg.
Absent pupillary response to light is common immediately
after cardiac arrest and may be compatible with recovery. It is
important to exclude drug effects, particularly atropine.
However, only one patient in the Guy’s paediatric series,10
with an absent pupillary response to light at 6 h regained
consciousness within the first month. In Moler’s recent mul-
ticentre series, bilaterally reactive pupils at 12 h were associ-
ated with lower mortality.52
5.3. Neurophysiology
Most children arrest in the context of another illness. As part
of their management, they are often already paralysed on the
intensive care unit, and are thus not accessible for clinical
examination. There is therefore a considerable literature
about the prediction of outcome using neurophysiological
techniques after paediatric cardiac arrest.95
5.3.1. Conventional electrophysiology
5.3.1.1. Background EEG. Several authors have described
grading systems for looking at EEGs after cardiac arrest.95,96 It
is clear that, in the absence of sedating drugs, EEGs which are
isoelectric or show only burst suppression are associated with
poor outcome,95 particularly if these patterns persist for more
than 24 h after cardiac arrest. A normal EEGwithin the first few
hours after cardiac arrest is usually predictive of goodoutcome
provided that no other insult supervenes. Intermediate grad-
ings, such as diffuse slowing with or without some faster
e u r o p e a n j o u r n a l o f p a e d i a t r i c n e u r o l o g y 1 5 ( 2 0 1 1 ) 3 7 9e3 8 9384
Author's personal copy
frequencies present, have less predictive power but combi-
nations of features in EEGs undertaken within the first week
after cardiac arrest often allow accurate prognosis.97 Serial
EEGs appear to be useful prognostically in non-traumatic
coma including hypoxic-ischaemic encephalopathy.58,62
Few authors have compared the predictive power of EEG
with clinical signs. Tardieu62 found EEG to be less useful than
clinical signs in distinguishing survivors with and without
handicap after mainly out-of-hospital cardiac arrest in
infancy; the EEG often deteriorated in those who were not
fully awake by 8 h. In contrast, in the Guy’s series of 89 mainly
in-patient paediatric arrests, the EEG pattern at 6 h, recorded
on either a three channel system (Oxford Medilog) or a cere-
bral function monitor (Medaid Ltd), was more powerful in the
prediction of outcome in a discriminant analysis than 6 h
Glasgow coma score, 6 h brain stem score or immediate
arterial pH,10 although again the EEG often deteriorated in
those initially predicted to do well.
5.3.1.2. Discharges. Electroencephalographic status epi-
lepticus may occur without obvious motor manifestations.
The appearance of intermittent spikes and sharp waves or
frank discharges is associated with the likelihood of a poor
final outcome but is not uniformly fatal if the background EEG
is continuous.
5.3.2. Monitoring EEGSeveral centres have used either the original cerebral
function monitor, which records an amplitude trace only, or
the cerebral function analysing monitor (CFAM),66,98 or the
compressed spectral array (CSA),98,99 both of which display
amplitude and frequency. Using the CFAM, the traces may
be graded although subtle features may not be recognised.
For the CSA, an unchanging trace is usually associated with
poor outcome. Deterioration of the pattern is also a poor
prognostic sign, but this may be more distressing for rela-
tives and nursing staff than serial EEGs. EEG monitoring
may be useful in the management of status epilepticus, but
should assist the interpretation of, rather than replacing,
serial EEGs.100
5.3.3. Evoked potentialsVisual, auditory brain stem and somatosensory evoked
potentials have been elicited in several studies of chil-
dren28,101-107 in non-traumatic coma including HIE. Brain stem
and somatosensory evoked potential have a role in the
prediction of outcome, particularly if the EEG is in an inter-
mediate group. Somatosensory evoked potentials appear to be
the most useful, while visual evoked potentials may be
misleading90 but predictive value is greater if the data from all
three modalities are combined.
5.4. Neuroradiology
Neuroimaging performed soon after cardiac arrest may show
cerebral swelling with effacement of the sulci or widespread
loss of grey-white differentiation or low density in the basal
ganglia or in the watershed regions. The “reversal sign” with
low density in the cerebral hemispheres and relatively higher
densities in the basal ganglia on computed tomography is not
uncommon.108 All these patterns are associated with poor
prognosis, but a normal CT scan does not guarantee a good
outcome.62 Several series have found this modality to be
useful prognostically109,110 T2-weighted, diffusion (Fig. 1) and
perfusion magnetic resonance imaging and proton spectros-
copy may be useful but must be interpreted with caution by
experts.106,111e118
5.5. Biochemistry
High blood glucose predicts poor outcome on admission after
out-of-hospital cardiac arrest and near-drowning25 although
the effect may be due to the duration of cardiopulmonary
resuscitation or the dose of adrenaline. In the Guy’s study of
mainly in-patient arrests, the first glucose after the arrest was
higher in those who did not recover consciousness than in
those who did (median 10.0 vs 7.7) but this did not reach
statistical significance (p ¼ 0.08).10
Acidosis on admission is associated with poor outcome
after paediatric near-drowning and the pH of the first gas was
highly significantly lower in those who did not recover
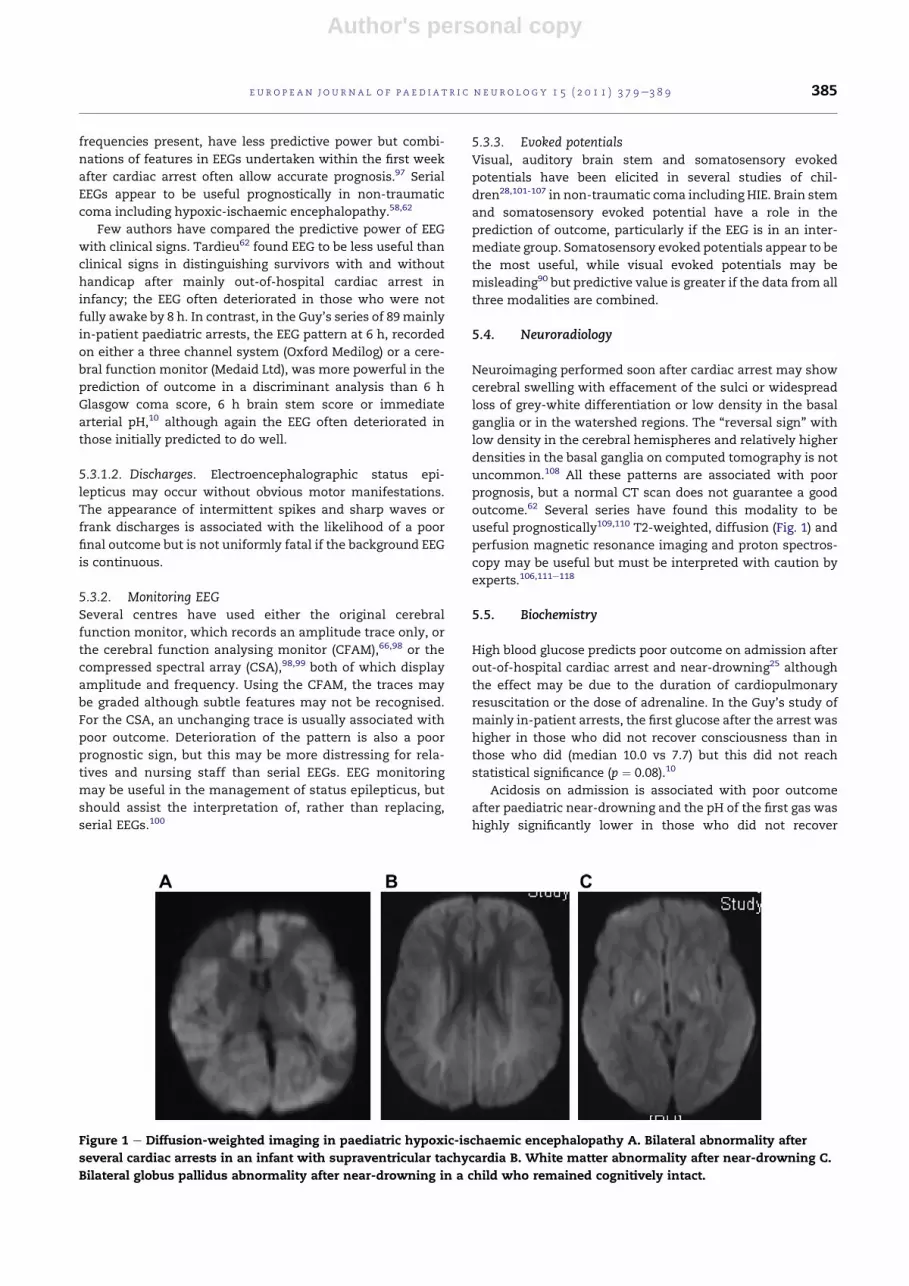
Figure 1 e Diffusion-weighted imaging in paediatric hypoxic-ischaemic encephalopathy A. Bilateral abnormality after
several cardiac arrests in an infant with supraventricular tachycardia B. White matter abnormality after near-drowning C.
Bilateral globus pallidus abnormality after near-drowning in a child who remained cognitively intact.
e u r o p e a n j o u r n a l o f p a e d i a t r i c n e u r o l o g y 1 5 ( 2 0 1 1 ) 3 7 9e3 8 9 385

Author's personal copy
consciousness compared with those who did (mean 7.058 vs.
7.238) in the Guy’s paediatric study,10 and this variable was an
important discriminant in the prediction of outcome.
A number of authors have looked at the prediction of
outcome using serummarkers such as procalcitonin,119 S-100
and neuron specific enolase120,121 but there are not enough
data currently to determine whether they sufficiently sensi-
tive or specific to be used clinically.
6. Summary
Cardiac arrest in childhood is a different clinical problem from
that in adulthood as myocardial infarction is rare, but out-of-
hospital arrest does occur for a variety of reasons andwith the
increasing number of therapeutic options for serious but not
necessarily fatal disease, in-patient cardiac arrest and
hypoxic-ischaemic encephalopathy are not uncommon. The
prognosis for patients who are unconscious on admission
after out-of-hospital arrest (including sudden infant death
and near-drowning) is poor, and can usually be predicted by
clinical signs and general information about the arrest. The
outcome for children who suffer an in-patient cardiac or
respiratory arrest or profound hypotension is often deter-
mined by underlying illness. Since clinical signs are often
obscured, additional prognostic information from investiga-
tions such as EEG, evoked potentials and neuroimaging may
be very useful. In both groups, there are patients who would
be predicted to survive intact but who deteriorate secondarily
and either die or survive in a vegetative state. Neurophysi-
ology may also useful in identifying this group, who may
benefit from hypothermia and control of intracranial hyper-
tension and status epilepticus. Randomised controlled trials
of therapeutic hypothermia for paediatric cardiac arrest are
urgently needed. Other treatments proposed on the basis of
basic science research into pathogenesis of ischaemic damage
cannot be recommended at the present time.
Acknowledgements
Dr Kirkham was supported by the British Heart Foundation.
r e f e r e n c e s
1. de Mos N, van Litsenburg RR, McCrindle B, Bohn DJ,Parshuram CS. Pediatric in-intensive-care-unit cardiacarrest: incidence, survival, and predictive factors. Crit CareMed 2006;34(4):1209e15.
2. Zideman DA, Hazinski MF. Background and epidemiology ofpediatric cardiac arrest. Pediatr Clin North Am 2008;55(4):847e59 [ix].
3. Atkins DL, Everson-Stewart S, Sears GK, Daya M,Osmond MH, Warden CR, et al. Epidemiology and outcomesfrom out-of-hospital cardiac arrest in children: theResuscitation Outcomes Consortium Epistry-Cardiac Arrest.Circulation 2009;119(11):1484e91.
4. Park CB, Shin SD, Suh GJ, Ahn KO, Cha WC, Song KJ, et al.Pediatric out-of-hospital cardiac arrest in Korea:
a nationwide population-based study. Resuscitation 2010;81(5):512e7.
5. Donoghue AJ, Nadkarni V, Berg RA, Osmond MH, Wells G,Nesbitt L, et al. CanAm Pediatric Cardiac Arrest Investigators.Out-of-hospital pediatric cardiac arrest: an epidemiologicreview and assessment of current knowledge. Ann Emerg Med2005;46(6):512e22.
6. Donoghue AJ, Nadkarni VM, Elliott M, Durbin D. AmericanHeart Assocation National Registry of CardiopulmonaryResuscitation Investigators. Effect of hospital characteristicson outcomes from pediatric cardiopulmonary resuscitation:a report from the national registry of cardiopulmonaryresuscitation. Pediatrics 2006;118(3):995e1001.
7. Bembea MM, Nadkarni VM, Diener-West M, Venugopal V,Carey SM, Berg RA, et al. Temperature patterns in the earlypostresuscitation period after pediatric inhospital cardiacarrest. Pediatr Crit Care Med 2010;11(6):723e30.
8. Wu ET, Li MJ, Huang SC, Wang CC, Liu YP, Lu FL, et al.Survey of outcome of CPR in pediatric in-hospital cardiacarrest in a medical center in Taiwan. Resuscitation 2009;80(4):443e8.
9. Olotu A, Ndiritu M, Ismael M, Mohammed S, Mithwani S,Maitland K, et al. Characteristics and outcome ofcardiopulmonary resuscitation in hospitalised Africanchildren. Resuscitation 2009;80(1):69e72.
10. Kirkham FJ. Coma after cardiac arrest. In: Eyre JA, editor.Coma in childhood. Bailliere Tindall; 1994. p. 1e40.
11. Lopez-Herce J, Domınguez P, Carrillo A. Spanish Study Groupof Cardiopulmonary Arrest in Children. Factors associatedwith survival in children with traumatic cardiopulmonaryarrest. Resuscitation 2008;76:314.
12. Calkins CM, Bensard DD, Partrick DA, Karrer FM. A criticalanalysis of outcome for children sustaining cardiac arrestafter blunt trauma. J Pediatr Surg 2002;37(2):180e4.
13. Meyer PG, Meyer F, Orliaguet G, Blanot S, Renier D, Carli P.Combined high cervical spine and brain stem injuries:a complex and devastating injury in children. J Pediatr Surg2005;40(10):1637e42.
14. Bennett M, Kissoon N. Is cardiopulmonary resuscitationwarranted in children who suffer cardiac arrest posttrauma? Pediatr Emerg Care 2007;23(4):267e72.
15. Crewdson K, Lockey D, Davies G. Outcome from paediatriccardiac arrest associated with trauma. Resuscitation 2007;75(1):29e34.
16. Nixon J, Pearn J, Wilkey I, Corcoran A. Fifteen years of childdrowningea 1967-1981 analysis of all fatal cases from theBrisbane Drowning Study and an 11 year study ofconsecutive near-drowning cases. Accid Anal Prev 1986;18(3):199e203.
17. Pearn JH, Wong RY, Brown III J, Ching YC, Bart Jr R,Hammar S. Drowning and near-drowning involvingchildren: a five-year total population study from the City andCounty of Honolulu. Am J Public Health 1979;69(5):450e4.
18. Kemp AM, Sibert JR. Outcome in children who nearly drown:a British Isles study. BMJ 1991;302(6782):931e3.
19. Dean JM, Kaufman ND. Prognostic indicators in pediatricnear-drowning: the Glasgow coma scale. Crit Care Med 1981;9(7):536e9.
20. Jacobsen WK, Mason LJ, Briggs BA, Schneider S,Thompson JC. Correlation of spontaneous respiration andneurologic damage in near-drowning. Crit Care Med 1983;11(7):487e9.
21. Biggart MJ, Bohn DJ. Effect of hypothermia and cardiac arreston outcome of near-drowning accidents in children. J Pediatr1990;117(2 Pt 1):179e83.
22. Allman FD, Nelson WB, Pacentine GA, McComb G. Outcomefollowing cardiopulmonary resuscitation in severe pediatricnear-drowning. Am J Dis Child 1986;140(6):571e5.
e u r o p e a n j o u r n a l o f p a e d i a t r i c n e u r o l o g y 1 5 ( 2 0 1 1 ) 3 7 9e3 8 9386

Author's personal copy
23. Frates Jr RC. Analysis of predictive factors in the assessmentof warm-water near-drowning in children. Am J Dis Child1981;135(11):1006e8.
24. Oakes DD, Sherck JP, Maloney JR, Charters III AC. Prognosisand management of victims of near-drowning. J Trauma1982;22(7):544e9.
25. Ashwal S, Schneider S, Tomasi L, Thompson J. Prognosticimplications of hyperglycemia and reduced cerebral bloodflow in childhood near-drowning.Neurology 1990;40(5):820e3.
26. Graf WD, Cummings P, Quan L, Brutocao D. Predictingoutcome in pediatric submersion victims. Ann Emerg Med1995;26(3):312e9.
27. Kruus S, Bergstrom L, Suutarinen T, Hyvonen R. Theprognosis of near-drowned children. Acta Paediatr Scand1979;68(3):315e22.
28. Cheliout-Heraut F, Rubinsztajn R, Ioos C, Estournet B.Prognostic value of evoked potentials and sleep recordingsin the prolonged comatose state of children. Preliminarydata. Neurophysiol Clin 2001;31(5):283e92.
29. Janati A, Erba G. Electroencephalographic correlates of near-drowning encephalopathy in children. Electroencephalogr ClinNeurophysiol 1982;53(2):182e91.
30. Rappaport M, Maloney JR, Ortega H, Fetzer D, Hall K. Survivalin young children after drowning: brain evoked potentials asoutcome predictors. Clin Electroencephalogr 1985;16(4):183e91.
31. Niu YW, Cherng WS, Lin MT, Tsao LY. An analysis ofprognostic factors for submersion accidents in children.Zhonghua Min Guo Xiao Er Ke Yi Xue Hui Za Zhi 1992;33(2):81e8.
32. Bell TS, Ellenberg L, McComb JG. Neuropsychologicaloutcome after severe pediatric near-drowning. Neurosurgery1985;17(4):604e8.
33. Constantinou JE, Gillis J, Ouvrier RA, Rahilly PM. Hypoxic-ischaemic encephalopathy after near miss sudden infantdeath syndrome. Arch Dis Child 1989;64(5):703e8.
34. Haim A, Zucker N, Levitas A, Sofer S, Katz A, Zalzstein E.Cardiac manifestations following electrocution in children.Cardiol Young 2008;18(5):458e60.
35. Glatstein M, Scolnik D, Mari E, Penazzi M, Ruiz G,Waisburg C. Levodopa treatment of late onsetextrapyramidal movements in a child after high Voltageelectrocution. Am J Ther; 2011.
36. Horsfield P, Williams AJ. Recovery after electrical injury. DevMed Child Neurol 1977;19(2):224e6.
37. Cherington M, Yarnell PR, London SF. Neurologiccomplications of lightning injuries. West J Med 1995;162(5):413e7.
38. Kotagal S, Rawlings CA, Chen SC, Burris G, Npuriouri S.Neurologic, psychiatric, and cardiovascular complications inchildren struck by lightning. Pediatrics 1982;70(2):190e2.
39. Kitamura T, Iwami T, Kawamura T, Nagao K, Tanaka H,Nadkarni VM, et al. Conventional and chest-compression-only cardiopulmonary resuscitation by bystanders forchildren who have out-of-hospital cardiac arrests:a prospective, nationwide, population-based cohort study.Lancet 2010;375(9723):1347e54.
40. Baker TW, King W, Soto W, Asher C, Stolfi A, Rowin ME. Theefficacy of pediatric advanced life support training inemergency medical service providers. Pediatr Emerg Care2009;25(8):508e12.
41. Sheikh A, Brogan T. Outcome and cost of open- and closed-chest cardiopulmonary resuscitation in pediatric cardiacarrests. Pediatrics 1994;93(3):392e8.
42. Fialka C, Sebok C, Kemetzhofer P, Kwasny O, Sterz F,Vecsei V. Open-chest cardiopulmonary resuscitation aftercardiac arrest in cases of blunt chest or abdominal trauma:a consecutive series of 38 cases. J Trauma 2004;57(4):809e14.
43. Cochran JB, Tecklenburg FW, Lau YR, Habib DM. Emergencycardiopulmonary bypass for cardiac arrest refractory to
pediatric advanced life support. Pediatr Emerg Care 1999;15(1):30e2.
44. Coskun KO, Popov AF, Schmitto JD, Hinz J, Kriebel T,Schoendube FA, et al. Extracorporeal circulation forrewarming in drowning and near-drowning pediatricpatients. Artif Organs 2010;34(11):1026e30.
45. Eich C, Brauer A, Timmermann A, Schwarz SK, Russo SG,Neubert K, et al. Outcome of 12 drowned children withattempted resuscitation on cardiopulmonary bypass: ananalysis of variables based on the "Utstein Style forDrowning. Resuscitation 2007;75(1):42e52.
46. Suominen PK, Vallila NH, Hartikainen LM, Sairanen HI,Korpela RE. Outcome of drowned hypothermic children withcardiac arrest treated with cardiopulmonary bypass. ActaAnaesthesiol Scand 2010;54(10):1276e81.
47. Wollenek G, Honarwar N, Golej J, Marx M. Cold watersubmersion and cardiac arrest in treatment of severehypothermia with cardiopulmonary bypass. Resuscitation2002;52(3):255e63.
48. Alsoufi B, Al-Radi OO, Nazer RI, Gruenwald C, Foreman C,Williams WG, et al. Survival outcomes after rescueextracorporeal cardiopulmonary resuscitation in pediatricpatients with refractory cardiac arrest. J Thorac CardiovascSurg 2007;134(4):952e9.
49. Raymond TT, Cunnyngham CB, Thompson MT, Thomas JA,Dalton HJ, Nadkarni VM. Outcomes among neonates, infants,and children after extracorporeal cardiopulmonaryresuscitation for refractory inhospital pediatric cardiacarrest:a report from the National Registry of CardiopulmonaryResuscitation. Pediatr Crit Care Med 2010;11(3):362e71.
50. Prodhan P, Fiser RT, Dyamenahalli U, Gossett J, Imamura M,Jaquiss RD, et al. Outcomes after extracorporealcardiopulmonary resuscitation (ECPR) following refractorypediatric cardiac arrest in the intensive care unit.Resuscitation 2009;80(10):1124e9.
51. Duff JP, Joffe AR, Sevcik W, deCaen A. Autoresuscitationafter pediatric cardiac arrest: is hyperventilation a cause?Pediatr Emerg Care 2011;27:208e9.
52. Moler FW, Donaldson AE, Meert K, Brilli RJ, Nadkarni V,Shaffner DH, et al. Multicenter cohort study of out-of-hospital pediatric cardiac arrest. Crit Care Med 2011;39(1):141e9.
53. Gil-Anton J, Lopez-Herce J, Morteruel E, Carrillo A,Rodriguez-Nunez A. Pediatric cardiac arrest refractory toadvanced life support: is there a role for terlipressin? PediatrCrit Care Med 2010;11(1):139e41.
54. Srinivasan V, Morris MC, Helfaer MA, Berg RA, Nadkarni VM.Calcium use during in-hospital pediatric cardiopulmonaryresuscitation: a report from the National Registry ofCardiopulmonary Resuscitation. Pediatrics 2008;121(5):e1144e51.
55. Meert KL, Donaldson A, Nadkarni V, Tieves KS, Schleien CL,Brilli RJ, et al. Multicenter cohort study of in-hospitalpediatric cardiac arrest. Pediatr Crit Care Med 2009;10(5):544e53.
56. Le Roux PD, Jardine DS, Kanev PM, Loeser JD. Pediatricintracranial pressure monitoring in hypoxic and nonhypoxicbrain injury. Childs Nerv Syst 1991;7(1):34e9.
57. Kirkham FJ. Intracranial pressure and cerebral blood flow innon-traumatic coma in childhood. In: Minns RA, editor.Measurement of intracranial pressure and cerebral blood flow inchildren. MacKeith Press; 1991. p. 283e338.
58. Tasker RC, Boyd S, Harden A, Matthew DJ. Monitoring innon-traumatic coma. Part II: electroencephalography. ArchDis Child 1988;63(8):895e9.
59. Dean JM, McComb JG. Intracranial pressure monitoring insevere pediatric near-drowning. Neurosurgery 1981;9(6):627e30.
e u r o p e a n j o u r n a l o f p a e d i a t r i c n e u r o l o g y 1 5 ( 2 0 1 1 ) 3 7 9e3 8 9 387

Author's personal copy
60. Nussbaum E, Galant SP. Intracranial pressure monitoring asa guide to prognosis in the nearly drowned, severelycomatose child. J Pediatr 1983;102(2):215e8.
61. Sarnaik AP, Preston G, Lieh-Lai M, Eisenbrey AB. Intracranialpressure and cerebral perfusion pressure in near-drowning.Crit Care Med 1985;13(4):224e7.
62. Tardieu M, Devictor D, Wood C, Navelet Y, Pariente D,Huault G, et al. Prognostic factors in cerebral hypoxic-ischemias in infants less than a year old. Arch Fr Pediatr 1987;44(10):833e8.
63. Aubourg P, Dulac O, Plouin P, Diebler C. Infantile statusepilepticus as a complication of ‘near-miss’ sudden infantdeath. Dev Med Child Neurol 1985;27(1):40e8.
64. Saengpattrachai M, Sharma R, Hunjan A, Shroff M, Ochi A,Otsubo H, et al. Nonconvulsive seizures in the pediatricintensive care unit: etiology, EEG, and brain imagingfindings. Epilepsia 2006;47(9):1510e8.
65. Jette N, Claassen J, Emerson RG, Hirsch LJ. Frequency andpredictors of nonconvulsive seizures during continuouselectroencephalographic monitoring in critically ill children.Arch Neurol 2006;63(12):1750e5.
66. Murdoch-Eaton D, Darowski M, Livingston J. Cerebralfunction monitoring in paediatric intensive care: usefulfeatures for predicting outcome. Dev Med Child Neurol 2001;43(2):91e6.
67. Bohn DJ, Biggar WD, Smith CR, Conn AW, Barker GA.Influence of hypothermia, barbiturate therapy, andintracranial pressure monitoring on morbidity and mortalityafter near-drowning. Crit Care Med 1986;14(6):529e34.
68. Hildebrand CA, Hartmann AG, Arcinue EL, Gomez RJ, Bing RJ.Cardiac performance in pediatric near-drowning. Crit CareMed 1988;16(4):331e5.
69. Bernard SA, Gray TW, Buist MD, Jones BM, Silvester W,Gutteridge G, et al. Treatment of comatose survivors ofout-of-hospital cardiac arrest with induced hypothermia.N Engl J Med 2002;346(8):557e63.
70. Mild therapeutic hypothermia to improve the neurologicoutcome after cardiac arrest. N Engl J Med 2002;346(8):549e56.
71. Kamarainen A, Virkkunen I, Tenhunen J, Yli-Hankala A,Silfvast T. Prehospital therapeutic hypothermia forcomatose survivors of cardiac arrest: a randomizedcontrolled trial. Acta Anaesthesiol Scand 2009;53(7):900e7.
72. Hassani H, Meyer S. Hypothermia for neuroprotection inadults after cardiopulmonary resuscitation. Am FamPhysician 2010;82(5):477.
73. Nielsen N, Friberg H, Gluud C, Herlitz J, Wetterslev J.Hypothermia after cardiac arrest should be further evaluated-A systematic review of randomised trials with meta-analysisand trial sequential analysis. Int J Cardiol; 2010.
74. Shankaran S, Laptook AR, Ehrenkranz RA, Tyson JE,McDonald SA, Donovan EF, et al. Whole-body hypothermiafor neonates with hypoxic-ischemic encephalopathy. N EnglJ Med 2005;353(15):1574e84.
75. Azzopardi DV, Strohm B, Edwards AD, Dyet L, Halliday HL,Juszczak E, et al. Moderate hypothermia to treat perinatalasphyxial encephalopathy. N Engl J Med 2009;361(14):1349e58.
76. Zhou WH, Cheng GQ, Shao XM, Liu XZ, Shan RB, Zhuang DY,et al. Selective head cooling with mild systemic hypothermiaafter neonatal hypoxic-ischemic encephalopathy:a multicenter randomized controlled trial in China. J Pediatr2010;157(3):367e72. 372.
77. Simbruner G, Mittal RA, Rohlmann F, Muche R. Systemichypothermia after neonatal encephalopathy: outcomes ofneo.nEURO.network RCT. Pediatrics 2010;126(4):e771e8.
78. Edwards AD, Brocklehurst P, Gunn AJ, Halliday H, Juszczak E,Levene M, et al. Neurological outcomes at 18 months of age
after moderate hypothermia for perinatal hypoxic ischaemicencephalopathy: synthesis and meta-analysis of trial data.BMJ 2010;340:c363.
79. Sugita M, Okamoto K, Terasaki H. Effect of the season on theneurological outcome in children with cardiac arrest. ActaPaediatr Jpn 1998;40(1):20e5.
80. Doherty DR, Parshuram CS, Gaboury I, Hoskote A, Lacroix J,Tucci M, et al. Hypothermia therapy after pediatric cardiacarrest. Circulation 2009;119(11):1492e500.
81. Hutchison JS, Doherty DR, Orlowski JP, Kissoon N.Hypothermia therapy for cardiac arrest in pediatric patients.Pediatr Clin North Am 2008;55(3):529e544,. ix.
82. Fink EL, Clark RS, Kochanek PM, Bell MJ, Watson RS. Atertiary care center’s experience with therapeutichypothermia after pediatric cardiac arrest. Pediatr Crit CareMed 2010;11(1):66e74.
83. de Caen AR, Kleinman ME, Chameides L, Atkins DL, Berg RA,Berg MD, et al. Paediatric Basic and Advanced Life SupportChapter Collaborators. Part 10: Paediatric basic andadvanced life support: 2010 International Consensus onCardiopulmonary Resuscitation and EmergencyCardiovascular Care Science with TreatmentRecommendations. Resuscitation 2010;81(Suppl 1):e213e259.
84. Nadkarni VM, Larkin GL, Peberdy MA, Carey SM, Kaye W,Mancini ME, et al. National Registry of CardiopulmonaryResuscitation Investigators. First documented rhythm andclinical outcome from in-hospital cardiac arrest amongchildren and adults. JAMA. 2006;295(1):50e7.
85. Seshia SS, Johnston B, Kasian G. Non-traumatic coma inchildhood: clinical variables in prediction of outcome. DevMed Child Neurol 1983;25(4):493e501.
86. Torphy DE, Minter MG, Thompson BM. Cardiorespiratoryarrest and resuscitation of children. Am J Dis Child 1984;138(12):1099e102.
87. O’Rourke PP. Outcome of children who are apneic andpulseless in the emergency room. Crit Care Med 1986;14(5):466e8.
88. Gillies JD, Seshia SS. Vegetative state following coma inchildhood: evolution and outcome. Dev Med Child Neurol1980;22(5):642e8.
89. Cole G, Boyd S, Kendall B, Dinwiddie R, Matthew D. Childrenin a persistent vegetative state. Br Med J (Clin Res Ed) 1984;289(6458):1620e1.
90. Wong VC. Cortical blindness in children: a study of etiologyand prognosis. Pediatr Neurol 1991;7(3):178e85.
91. Nickel BL, Hoyt CS. The hypoxic retinopathy syndrome. Am JOphthalmol 1982;93(5):589e93.
92. Bell JA, Hodgson HJ. Coma after cardiac arrest. Brain 1974;97(2):361e72.
93. Von Seggern K, Egar M, Fuhrman BP. Cardiopulmonaryresuscitation in a pediatric ICU. Crit Care Med 1986;14(4):275e7.
94. Srinivasan V, Nadkarni VM, Helfaer MA, Carey SM, Berg RA.Childhood obesity and survival after in-hospital pediatriccardiopulmonary resuscitation. Pediatrics 2010;125(3):e481e8.
95. Pampiglione G, Harden A. Resuscitation aftercardiocirculatory arrest. Prognostic evaluation of earlyelectroencephalographic findings. Lancet 1968;1(7555):1261e5.
96. Binnie CD, Prior PF, Lloyd DS, Scott DF, Margerison JH.Electroencephalographic prediction of fatal anoxic braindamage after resuscitation from cardiac arrest. Br Med J 1970;4(5730):265e8.
97. Nishisaki A, Sullivan III J, Steger B, Bayer CR, Dlugos D, Lin R,et al. Retrospective analysis of the prognostic value ofelectroencephalography patterns obtained in pediatric in-hospital cardiac arrest survivors during three years. PediatrCrit Care Med 2007;8(1):10e7.
e u r o p e a n j o u r n a l o f p a e d i a t r i c n e u r o l o g y 1 5 ( 2 0 1 1 ) 3 7 9e3 8 9388

Author's personal copy
98. Altafullah I, Asaikar S, Torres F. Status epilepticus: clinicalexperience with two special devices for continuous cerebralmonitoring. Acta Neurol Scand 1991;84(5):374e81.
99. Talwar D, Torres F. Continuous electrophysiologic monitoringof cerebral function in the pediatric intensive care unit.Pediatr Neurol 1988;4(3):137e47.
100. Tasker RC, Boyd SG, Harden A, Matthew DJ. The cerebralfunction analysing monitor in paediatric medical intensivecare: applications and limitations. Intensive Care Med 1990;16(1):60e8.
101. Lutschg J, Pfenninger J, Ludin HP, Vassella F. Brain-stemauditory evoked potentials and early somatosensory evokedpotentials in neurointensively treated comatose children.Am J Dis Child 1983;137(5):421e6.
102. Fisher B, Peterson B, Hicks G. Use of brainstem auditory-evoked response testing to assess neurologic outcomefollowing near drowning in children. Crit Care Med 1992;20(5):578e85.
103. Sandroni C, Barelli A, Piazza O, Proietti R, Mastria D,Boninsegna R. What is the best test to predict outcome afterprolonged cardiac arrest? Eur J Emerg Med 1995;2(1):33e7.
104. Mandel R, Martinot A, Delepoulle F, Lamblin MD, Laureau E,Vallee L, et al. Prediction of outcome after hypoxic-ischemicencephalopathy: a prospective clinical andelectrophysiologic study. J Pediatr 2002;141(1):45e50.
105. Robinson LR, Micklesen PJ, Tirschwell DL, Lew HL. Predictivevalue of somatosensory evoked potentials for awakeningfrom coma. Crit Care Med 2003;31(3):960e7.
106. Abend NS, Licht DJ. Predicting outcome in children withhypoxic ischemic encephalopathy. Pediatr Crit Care Med 2008;9(1):32e9.
107. Suppiej A, Cappellari A, Cogo PE. Prognostic role ofsomatosensory and auditory evoked potentials in paediatrichypoxic-ischemic encephalopathy managed withhypothermia: an illustrative case. Neurophysiol Clin 2009;39(2):101e5.
108. Han BK, Towbin RB, De Court G, McLaurin RL, Ball Jr WS.Reversal sign on CT: effect of anoxic/ischemic cerebralinjury in children. AJR Am J Roentgenol 1990;154(2):361e8.
109. Romano C, Brown T, Frewen TC. Assessment of pediatricnear-drowning victims: is there a role for cranial CT? PediatrRadiol 1993;23(4):261e3.
110. Rafaat KT, Spear RM, Kuelbs C, Parsapour K, Peterson B.Cranial computed tomographic findings in a large group ofchildren with drowning: diagnostic, prognostic, and forensicimplications. Pediatr Crit Care Med 2008;9(6):567e72.
111. Kreis R, Arcinue E, Ernst T, Shonk TK, Flores R, Ross BD.Hypoxic encephalopathy after near-drowning studied byquantitative 1H-magnetic resonance spectroscopy. J ClinInvest 1996;97(5):1142e54.
112. Ashwal S, Holshouser BA, Tomasi LG, Shu S, Perkin RM,Nystrom GA, et al. 1H-magnetic resonance spectroscopy-determined cerebral lactate and poor neurological outcomesin children with central nervous system disease. Ann Neurol1997;41(4):470e81.
113. Dubowitz DJ, Bluml S, Arcinue E, Dietrich RB. MR ofhypoxic encephalopathy in children after near drowning:correlation with quantitative proton MR spectroscopyand clinical outcome. AJNR Am J Neuroradiol 1998;19(9):1617e27.
114. Christophe C, Fonteyne C, Ziereisen F, Christiaens F,Deltenre P, De Maertelaer V, et al. Value of MR imaging of thebrain in children with hypoxic coma. AJNR Am J Neuroradiol2002;23(4):716e23.
115. Nogami K, Fujii M, Kato S, Nishizaki T, Suzuki M,Yamashita S, et al. Analysis of magnetic resonance imaging(MRI) morphometry and cerebral blood flow in patients withhypoxic-ischemic encephalopathy. J Clin Neurosci 2004;11(4):376e80.
116. Finelli PF, DiMario Jr FJ. MR imaging and prognosis ofhypoxic-ischemic leukoencephalopathy. Neurocrit Care 2006;4(2):119e26.
117. Pollock JM, Whitlow CT, Deibler AR, Tan H, Burdette JH,Kraft RA, et al. Anoxic injury-associated cerebralhyperperfusion identified with arterial spin-labeled MRimaging. AJNR Am J Neuroradiol 2008;29(7):1302e7.
118. Aragao MF, Law M, Netto JP, Valenca MM, Naidich T.Prognostic value of proton magnetic resonance spectroscopyfindings in near drowning patients: reversibility of the earlymetabolite abnormalities relates with a good outcome. ArqNeuropsiquiatr 2009;67(1):55e7.
119. Los AM, Rey C, Concha A, Medina A, Prieto B. Acute-phasereactants after paediatric cardiac arrest. Procalcitonin asmarker of immediate outcome. BMC Pediatr 2008;8:18.
120. Topjian AA, Lin R, Morris MC, Ichord R, Drott H, Bayer CR,et al. Neuron-specific enolase and S-100B are associatedwith neurologic outcome after pediatric cardiac arrest.Pediatr Crit Care Med 2009;10(4):479e90.
121. Rundgren M, Karlsson T, Nielsen N, Cronberg T, Johnsson P,Friberg H. Neuron specific enolase and S-100B as predictorsof outcome after cardiac arrest and induced hypothermia.Resuscitation 2009;80(7):784e9.
e u r o p e a n j o u r n a l o f p a e d i a t r i c n e u r o l o g y 1 5 ( 2 0 1 1 ) 3 7 9e3 8 9 389





























