Embed Size (px)
Citation preview

This article was downloaded by: [Aristotle University of Thessaloniki]On: 21 March 2014, At: 05:47Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House,37-41 Mortimer Street, London W1T 3JH, UK
Women & HealthPublication details, including instructions for authors and subscription information:http://www.tandfonline.com/loi/wwah20
Changing Help-Seeking Rates for Intimate PartnerViolence in CanadaJanice Du Mont EdD a , Tanira Forte MSc b , Marsha M. Cohen MD and MHSc c , Ilene HymanPhD d & Sarah Romans MB and MD ea Centre for Research in Women's Health, Sunnybrook and Women's Health Sciences Centre,University of Toronto , 790 Bay Street, 7th Floor, Toronto, ON, Canada , M5G 1N8 E-mail:b Centre for Research in Women's Health, Sunnybrook and Women's Health Sciences Centre,University of Toronto , 790 Bay Street, 7th Floor, Toronto, ON, Canada , M5G 1N8 E-mail:c Centre for Research in Women's Health, Sunnybrook and Women's Health Sciences Centre,University of Toronto , 790 Bay Street, 7th Floor, Toronto, ON, Canada , M5G 1N8 E-mail:d Centre for Research in Women's Health, Sunnybrook and Women's Health Sciences Centre,University of Toronto , 790 Bay Street, 7th Floor, Toronto, ON, Canada , M5G 1N8 E-mail:e Centre for Research in Women's Health, Sunnybrook and Women's Health Sciences Centre,University of Toronto , 790 Bay Street, 7th Floor, Toronto, ON, Canada , M5G 1N8 E-mail:Published online: 17 Oct 2008.
To cite this article: Janice Du Mont EdD , Tanira Forte MSc , Marsha M. Cohen MD and MHSc , Ilene Hyman PhD & SarahRomans MB and MD (2005) Changing Help-Seeking Rates for Intimate Partner Violence in Canada, Women & Health, 41:1, 1-19,DOI: 10.1300/J013v41n01_01
To link to this article: http://dx.doi.org/10.1300/J013v41n01_01
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all the information (the “Content”) containedin the publications on our platform. However, Taylor & Francis, our agents, and our licensors make norepresentations or warranties whatsoever as to the accuracy, completeness, or suitability for any purpose of theContent. Any opinions and views expressed in this publication are the opinions and views of the authors, andare not the views of or endorsed by Taylor & Francis. The accuracy of the Content should not be relied upon andshould be independently verified with primary sources of information. Taylor and Francis shall not be liable forany losses, actions, claims, proceedings, demands, costs, expenses, damages, and other liabilities whatsoeveror howsoever caused arising directly or indirectly in connection with, in relation to or arising out of the use ofthe Content.
This article may be used for research, teaching, and private study purposes. Any substantial or systematicreproduction, redistribution, reselling, loan, sub-licensing, systematic supply, or distribution in anyform to anyone is expressly forbidden. Terms & Conditions of access and use can be found at http://www.tandfonline.com/page/terms-and-conditions

Changing Help-Seeking Rates for IntimatePartner Violence in Canada
Janice Du Mont, EdDTonia Forte, MSc
Marsha M. Cohen, MD, MHScIlene Hyman, PhD
Sarah Romans, MB, MD
ABSTRACT. The adverse physical and psychological sequelae of inti-mate partner violence (IPV) are well documented, as are governmentinitiatives in Canada since the early 1990s to address the problemthrough public awareness campaigns and service enhancement pro-grams. While these initiatives have been designed to encourage abusedwomen to come forward, there has been little research examining changesover time in help-seeking rates among this group. To fill this void, wecompared data from two large Canadian population-based, cross-sec-tional telephone surveys: the 1993 Violence Against Women Survey(1993-VAWS) and the 1999 General Social Survey (1999-GSS). Amongwomen who reported physical and/or sexual violence by a current or pre-vious partner, we examined differences in rates of disclosure of abuse,
Janice Du Mont (E-mail: [email protected]), Tonia Forte (E-mail: [email protected]), Marsha M. Cohen (E-mail: [email protected]), Ilene Hyman (E-mail: [email protected]) and Sarah Romans (E-mail: [email protected]) are all affiliatedwith the Centre for Research in Women’s Health, Sunnybrook and Women’s HealthSciences Centre, University of Toronto, 790 Bay Street, 7th Floor, Toronto, ON, Can-ada M5G 1N8.
This research was supported by a grant from the Canadian Institutes of Health Re-search, Institute of Gender and Health, and the Atkinson Foundation. Dr. Du Mont isthe recipient of a New Investigator Award in Gender and Health from the Canadian In-stitutes of Health Research. Dr. Romans is the Shirley Brown Chair in Women’s Men-tal Health at the Centre for Research in Women’s Health. The authors thank RobinMason for her helpful comments on an earlier draft of this article.
Women & Health, Vol. 41(1) 2005Available online at http://www.haworthpress.com/web/WH
2005 by The Haworth Press, Inc. All rights reserved.Digital Object Identifier: 10.1300/J013v41n01_01 1
Dow
nloa
ded
by [
Ari
stot
le U
nive
rsity
of
The
ssal
onik
i] a
t 05:
47 2
1 M
arch
201
4

help-seeking by type of service, and barriers to service use. Abusedwomen in the 1999-GSS were significantly more likely than those in the1993-VAWS to have reported disclosing a violent incident(s) to a familymember (66.4% vs. 43.9%), friend or neighbor (67.4% vs. 45.4%), doc-tor or nurse (31.9% vs. 23.0%), and/or minister, priest, or cleric (11.5%vs. 7.3%). The 1999-GSS cohort was also more likely to have presentedto a shelter or transition house (11.0% vs. 7.8%), a crisis center (17.3%vs. 4.2%), a counselor or psychologist (39.1% vs. 14.7%), a women’scenter (11.2% vs. 3.4%), and/or a community or family center (15.4%vs. 4.7%). Among those women who did not seek help, fewer in the1999-GSS reported that they did not know of any services (6.4% vs.17.0%), or that services were not available (0.8% vs. 14.5%). Althoughwe found a demonstrable increase in the numbers of abused womenseeking help, overall, rates of service utilization were still low as late as1999, highlighting the importance of continued government com-mitment to funding IPV initiatives. [Article copies available for a fee fromThe Haworth Document Delivery Service: 1-800-HAWORTH. E-mail address:<[email protected]> Website: <http://www.HaworthPress.com> 2005 by The Haworth Press, Inc. All rights reserved.]
KEYWORDS. Woman abuse, wife assault, domestic violence, intimatepartner violence, help-seeking, disclosure, service utilization, barriers toservice utilization
INTRODUCTION
The United Nation(UN)s’ (1993) definition of violence against womenincludes any act “that results in, or is likely to result in, physical, sexualor psychological harm or suffering to women, including threats of suchacts, coercion or arbitrary deprivations of liberty, whether occurring inpublic or private life.” Worldwide, it is estimated that one in every threewomen “has been beaten, coerced into sex, or otherwise abused in herlifetime” (Heise, Ellsberg, & Gottemoeller, 1999, p. 1). Intimate partnerviolence (IPV), or abuse perpetrated by husbands, boyfriends, dates, orother male intimates, is one of the most universal and widespread formsof violence against women (Heise et al., 1999). According to the 1993Violence Against Women Survey (Statistics Canada 1993), the esti-mated lifetime prevalence of male-to-female IPV in Canada is 29%(Rodgers, 1994).
IPV often leads to the marginalization and isolation of women byconstraining their ability to make autonomous decisions regarding their
2 WOMEN & HEALTH
Dow
nloa
ded
by [
Ari
stot
le U
nive
rsity
of
The
ssal
onik
i] a
t 05:
47 2
1 M
arch
201
4
own lives and undermining their full participation in society (Carillo, 1992;Macleod & Kinnon, 1997). It contributes to women’s social and economicinequality by establishing barriers in homes, schools, workplaces, andother public spaces (Carillo, 1992; MacLeod & Kinnon, 1997). Abusivemen may deny their partners the opportunity to acquire the knowledgeand skills needed for employment or prevent them from working out-side the home. For those who do pursue education or take on paid jobs,the effects of violence may result in poor grades or work performance,high absenteeism, and eventual withdrawal or dismissal (Carillo, 1992;Macleod & Kinnon, 1997). Exclusion from or limited access to educa-tion and employment increases women’s financial dependence on theirmale partners, placing them in the difficult position of having to riskloss of income, food, and housing in order to leave the abusive relation-ship. Many women find themselves inadequately housed or homeless asresult of IPV (Miller & Du Mont, 2000).
Women abused by their intimate male partners may also experience avast array of health problems. Injuries, which tend to be the most visibleand immediate consequence, range from cuts, scratches, and bruises tobroken bones, dislocated joints, head or spinal cord injuries, knifewounds, internal bleeding, and miscarriages (Dal Grande, Hickling,Taylor, & Woollacott, 2003; Krug, Dahlberg, Mercy, Zwi, & Lozano,2002; Kyriacou, Anglin, Taliaferro, Stone, Tubb, Linden, Muelleman,Barton, & Kraus, 1999; Tjaden & Thoennes, 2000). Abused women areat increased risk for HIV and other sexually transmitted infections(Dunkle, Jewkes, Brown, Gray, McIntryre, & Harlow, 2004; Wingood,DiClemente, & Raj, 2000). The psychological sequelae of IPV includeclinical depression, anxiety disorders, substance abuse problems, andeating disorders (Coker, Davis, Arias, Desai, Sanderson, Brandt, &Smith, 2002a; Coker, Smith, Thompson, McKeown, Bethea, & Davis,2002c; Golding, 1999; Koss, 1990; Krug et al., 2002). According toKoss (1990), many women who have experienced violence exhibit animmediate post-victimization distress response, which, if not resolved,can develop into posttraumatic stress disorder. As well, abused womenoften feel anger, fear, guilt, and shame and report lowered self-esteemand difficulties relating to men (Rodgers, 1994). For some, the burdenof abuse is so great that they attempt to or take their own lives (Carillo,1992; Coker et al., 2002c; Golding, 1999).
Despite the ubiquity of IPV and its serious adverse impact on women’swell-being, studies show that many abused women do not seek helpfrom community and health services. Henning and Klesges (2002)found that only 15% of women exposed to IPV in Shelby County, Ten-
Du Mont et al. 3
Dow
nloa
ded
by [
Ari
stot
le U
nive
rsity
of
The
ssal
onik
i] a
t 05:
47 2
1 M
arch
201
4

nessee had sought formal counseling or support services. Gondolf’s(1998) four city investigation of court ordered batterers and Coker, Der-rick, Lumpkin, Aldrick, and Oldendick’s (2000b) cross sectional sur-vey of females and males in South Carolina revealed that only 7% and11% of abused women, respectively, had sought help from a shelter.The Centers for Disease Control and Prevention (2000) reported that39% of women experiencing IPV in Massachusetts in the five years pre-ceding 1996-97 reported to police, 34% obtained a restraining order,and 29% sought medical care. Most women abused by a partner in DalGrande and colleagues (2003) representative sample of South Austra-lian adults did not contact police (77%), a non-health service (69%), or ahealth service (71%). Kershner and Anderson’s (2002) survey of abusedrural women found that only 32% had discussed the abuse with a healthcare provider. Similarly, Coker and colleagues (2000b), and Hegartyand Taft (2001) who randomly sampled Brisbane General Practices,found rates of disclosure to health care providers at only slightly morethan one third (35% and 37%, respectively).
It may not be surprising then that IPV victims report numerous barri-ers to using services. Dal Grande and colleagues (2003) found thatamong abused women and men the most common reasons given for notusing services were that the respondent did not want or need help, therespondent was unaware of any health related services that dealt withthe issue, the violent incident was perceived as too minor, and too muchtime had elapsed since the violent incident. Other reasons women do notdisclose or seek help subsequent to being abused identified in the re-search literature include: fears for safety, lack of knowledge about ap-propriate sources of support, concerns about losing custody of theirchildren (De Voe & Smith, 2003; Peckover, 2003); fear of retaliation bythe abuser, reluctance to involve police, prohibitive costs, long waitingtimes, lack of trust in health care provider (Rodriquez, Quiroga, &Bauer, 1996); lack of privacy, time constraints, continuity of care (Bac-chus, Mezey, & Bewley, 2003); self-reliance, having left the abusivepartner, shame and embarrassment, the perception that doctors can nothelp or are there to deal only with physical problems, and the inability totalk to a male doctor (Hegarty & Taft, 2001). Among abused immigrantwomen specifically, social isolation, language barriers, discrimination,and fears of deportation were among the most common reasons givenfor not using services (Abu-Ras, 2003; Bauer, Rodriquez, Quiroga, &Flores-Oritz, 2000).
Globally, violence against women is increasingly understood as a hu-man rights violation and a major public health issue (Krug et al., 2002;
4 WOMEN & HEALTH
Dow
nloa
ded
by [
Ari
stot
le U
nive
rsity
of
The
ssal
onik
i] a
t 05:
47 2
1 M
arch
201
4
Velzeboer, Ellsberg, Arcas, & Garcia-Moreno, 2003). Canada has beenin the vanguard with initiatives resulting in the adoption of the Decla-ration on the Elimination of Violence Against Women in 1993 bythe UNs’ General Assembly and the appointment of a Special Rap-porteur on Violence Against Women in 1994 by the UNs’ Commis-sion on Human Rights (Status of Women Canada, 2000, 1995).Much work has been done to address the issue nationally (Status ofWomen Canada, 1995). In 1993, Statistics Canada launched the firstever population-based study of violence against women worldwide.In its wake were a plethora of federal, territorial, provincial, and mu-nicipal government initiatives aimed at addressing violence againstwomen including IPV, through, for example, public awareness andeducation campaigns, service enhancement and implementation pro-grams, the establishment of domestic violence courts, pro-chargingpolice policies, law enforcement training initiatives (Status ofWomen Canada, 1998, 2003), and the expansion of hospital-basedsexual assault centers to serve women assaulted by their intimatemale partners (Du Mont, Macdonald, & Badgley, 1997; Du Mont &Parnis, 2002).
The 2003 Status of Women Canada address to the UN Committee onthe Elimination of All Forms of Discrimination Against Women (CEDAW)stated that Canadian efforts to address violence against women between1994 and 1998 had had some positive effect, citing lower reported ratesof male-to-female IPV in 1999 compared to 1993 (Status of WomenCanada, 2003). It attributed the improved situation, in part, to increasednumbers of community-based supports and shelters across the countryworking to address the issue. While the number of shelters for abusedwomen grew nationally from 371 in 1993 to 470 in 1998 and the num-ber of women using shelters from 45,777 in 1992-93 to 47,962 in1997-98 (Federal-Provincial-Territorial Ministers Responsible for theStatus of Women, 2002), information, generally, about changes overtime in abused women’s help-seeking subsequent to IPV is very lim-ited.
Preliminary analyses by Statistics Canada of “trends” in social ser-vice use by women abused by their intimate partners in Canada havebeen reported in an in-house publication, Family Violence in Canada:A Statistical Profile 2001 (Johnson & Hotton, 2001). Johnson andHotton’s comparisons of the 1993 Violence Against Women Survey(VAWS) with the 1999 General Social Survey (GSS) revealed signifi-cant increases in the use of any social service across 8 provinces of Can-ada. However, differences between the two surveys in terms of the use
Du Mont et al. 5
Dow
nloa
ded
by [
Ari
stot
le U
nive
rsity
of
The
ssal
onik
i] a
t 05:
47 2
1 M
arch
201
4

of specific services, reasons for not using services, and disclosure to in-formal and formal sources of support were not examined. To increaseknowledge in these areas, we undertook to further analyse data from the1993-VAWS and 1999-GSS.
METHODS
Data Sources
VAWS. In 1993, Statistics Canada conducted a national, voluntarytelephone survey on violence against women by male partners, ac-quaintances, and strangers. The target population was all Englishand French speaking women 18 years of age and older living in pri-vate households in the ten Canadian provinces. The ten provinceswere divided into geographical areas and the sample was selectedusing a method of Random Digit Dialing (RDD) called the Elimina-tion of Non-working Banks (Norris & Paton, 1991). After a house-hold was successfully contacted, one eligible woman within thehousehold was randomly selected to be interviewed. Interviewerswere trained to assess whether the woman was able to answer ques-tions freely; if not, the interview was rescheduled. Interviews wereconducted from February to June 1993. The overall response ratefor the survey was 63.7%. The total sample consisted of 12,300women.
GSS. The GSS is a recurring national, voluntary telephone surveyconducted by Statistics Canada since 1985. It is designed to monitorthe attitudes and experiences of Canadians on a wide range of socialand well-being issues. In 1999, it focused on violence and victimiza-tion, including IPV. The target population included men and womenaged 15 years and older living in private households in the ten prov-inces. The provinces were divided into geographical strata and thesample was selected using a method of RDD called the Eliminationof Non-working Banks (Norris & Paton, 1991). After a householdwas successfully contacted, one eligible individual within the house-hold was randomly selected to be interviewed. Interviews were con-ducted from February to December 1999 and administered in Englishor French. The overall response rate for the survey was 81.3%. The to-tal sample consisted of 25,876 respondents, of which 14,269 werewomen.
6 WOMEN & HEALTH
Dow
nloa
ded
by [
Ari
stot
le U
nive
rsity
of
The
ssal
onik
i] a
t 05:
47 2
1 M
arch
201
4

Sample
The present study assessed rates of disclosure and service use, and bar-riers to service use among women respondents in the 1993-VAWS and1999-GSS who reported physical and/or sexual violence by a current orprevious partner (N = 2019 and N = 922, respectively). Both surveys as-sessed IPV using a modified version of the Conflicts Tactics Scale(Straus, 1989). The 1993-VAWS assessed partner violence since the ageof 16. The 1999-GSS collected information on experiences of partner vio-lence in the five years preceding the survey. While both surveys collectedinformation on violence by a current or previous partner, the 1999-GSS re-quired contact with the previous partner in the preceding five years.
Respondents who disclosed physical and/or sexual violence byan intimate partner were asked to provide details about the victim-ization. Women in the 1993-VAWS who had experienced IPV byboth a current and a previous partner were asked to describe oneviolent relationship randomly selected by the interviewer (Thomp-son, Saltzman, & Johnson, 2001). In the 1999-GSS, women who re-ported physical and/or sexual violence by both a current and aprevious partner (n = 10) were asked the series of questions twice,once for each partner. To attain comparability between the two sur-veys, we selected randomly responses pertaining to one partneronly. We then deleted 153 and 23 cases, respectively, from the1993-VAWS and 1999-GSS for which there was no information ondisclosure and service utilization. Our final sample was comprisedof 1,866 women from the 1993-VAWS and 899 women from the1999-GSS (see Table 1 for a description of the samples).
Variables
Variables examined in this study were grouped into three catego-ries: (1) disclosure of IPV to informal and formal sources of support,(2) use of social services subsequent to IPV, and (3) reasons for not us-ing social services subsequent to IPV. Only responses to questions ineach category that were similar in manner in both surveys were com-pared (see Table 2). Informal and formal supports to who IPV was dis-closed included family members, friends or neighbors, doctors ornurses, and ministers, priests or clerics. Services used included shel-ters or transition houses, crisis centers or crisis lines, counselors or psy-chologists, women’s centers, and community or family centers. Reasonsgiven by respondents for not using services included not knowing of
Du Mont et al. 7
Dow
nloa
ded
by [
Ari
stot
le U
nive
rsity
of
The
ssal
onik
i] a
t 05:
47 2
1 M
arch
201
4
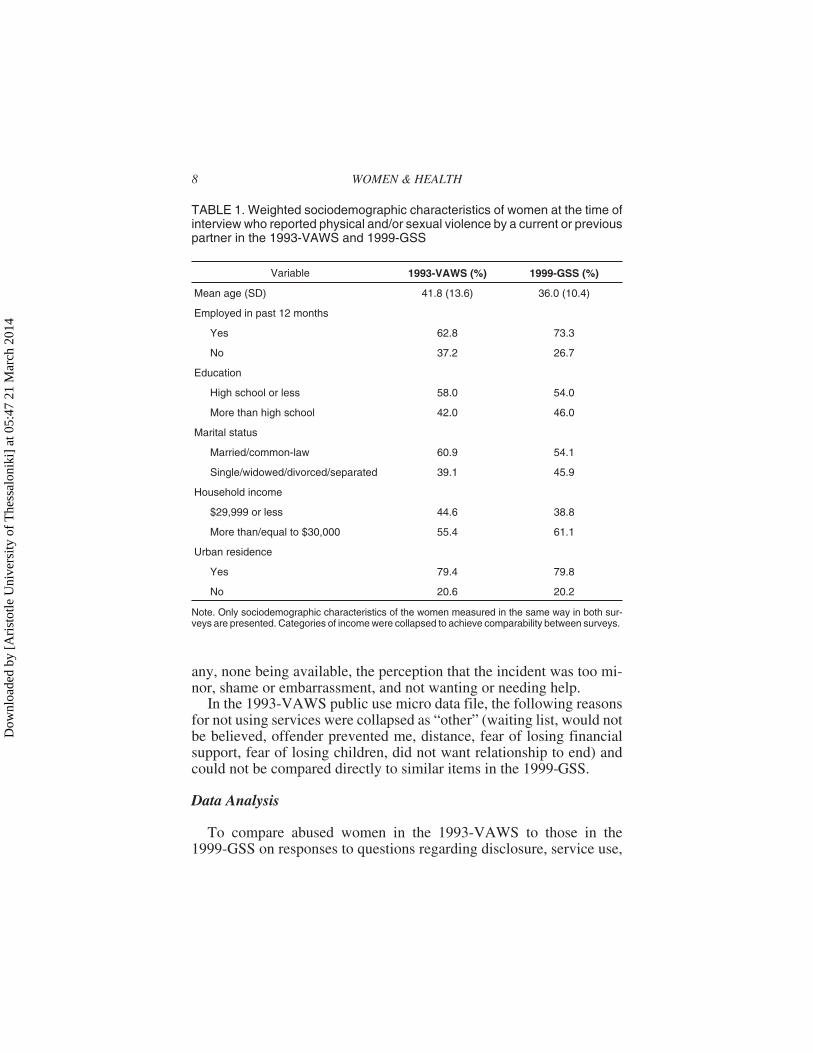
any, none being available, the perception that the incident was too mi-nor, shame or embarrassment, and not wanting or needing help.
In the 1993-VAWS public use micro data file, the following reasonsfor not using services were collapsed as “other” (waiting list, would notbe believed, offender prevented me, distance, fear of losing financialsupport, fear of losing children, did not want relationship to end) andcould not be compared directly to similar items in the 1999-GSS.
Data Analysis
To compare abused women in the 1993-VAWS to those in the1999-GSS on responses to questions regarding disclosure, service use,
8 WOMEN & HEALTH
TABLE 1. Weighted sociodemographic characteristics of women at the time ofinterview who reported physical and/or sexual violence by a current or previouspartner in the 1993-VAWS and 1999-GSS
Variable 1993-VAWS (%) 1999-GSS (%)
Mean age (SD) 41.8 (13.6) 36.0 (10.4)
Employed in past 12 months
Yes 62.8 73.3
No 37.2 26.7
Education
High school or less 58.0 54.0
More than high school 42.0 46.0
Marital status
Married/common-law 60.9 54.1
Single/widowed/divorced/separated 39.1 45.9
Household income
$29,999 or less 44.6 38.8
More than/equal to $30,000 55.4 61.1
Urban residence
Yes 79.4 79.8
No 20.6 20.2
Note. Only sociodemographic characteristics of the women measured in the same way in both sur-veys are presented. Categories of income were collapsed to achieve comparability between surveys.
Dow
nloa
ded
by [
Ari
stot
le U
nive
rsity
of
The
ssal
onik
i] a
t 05:
47 2
1 M
arch
201
4

and reasons for not using services, frequencies were calculated for cate-gorical data and then compared across the two surveys using the z test.All analyses were weighted according to Statistics Canada’s guidelinesto represent the population of women living in Canada (Statistics Can-ada, 2000). Cases with variables that had missing data were not ana-lyzed. Analyses were conducted using Stata, Version 7.0. A p value of.05 was considered statistically significant. All tests of significancewere two-tailed.
RESULTS
Disclosure
As reported in Table 3, abused women in the 1999-GSS were signifi-cantly more likely to disclose the violent incident(s) to another person
Du Mont et al. 9
TABLE 2. Comparable questions assessing disclosure, service use, and rea-sons for not using services in the 1993-VAWS and the 1999-GSS
1993-VAWS 1999-GSS
Did you ever talk to anyone about whathappened, such as…
Family?Friend/neighbor?Doctor?Minister, priest or clergy?
Other than to the police, did you ever talk toanyone about (these) this incident(s), such as:
Family?Friend or neighbor?Doctor or nurse?Minister, priest, clergy or another spiritualadvisor?
Did you ever contact any of the followingservices for help?
Crisis center/crisis line?Another counselor?Community/family center?Shelter or transition house?Women’s center?
During the past 5 years, did you ever contactor use any of the following services for helpbecause of the violence, such as
Crisis center or crisis line?Another counselor or psychologist?Community center or family center?Shelter or transition house?Centre for women or women's support group?
Is there any reason why you didn’t usethese services?
Didn’t know of any servicesNone availableToo minorShame/embarrassmentDidn’t want/need help
Is there any reason that you didn’t use any ofthese services?
Didn’t know of any servicesNone availableToo minorShame/embarrassmentDidn’t want/need help
Dow
nloa
ded
by [
Ari
stot
le U
nive
rsity
of
The
ssal
onik
i] a
t 05:
47 2
1 M
arch
201
4
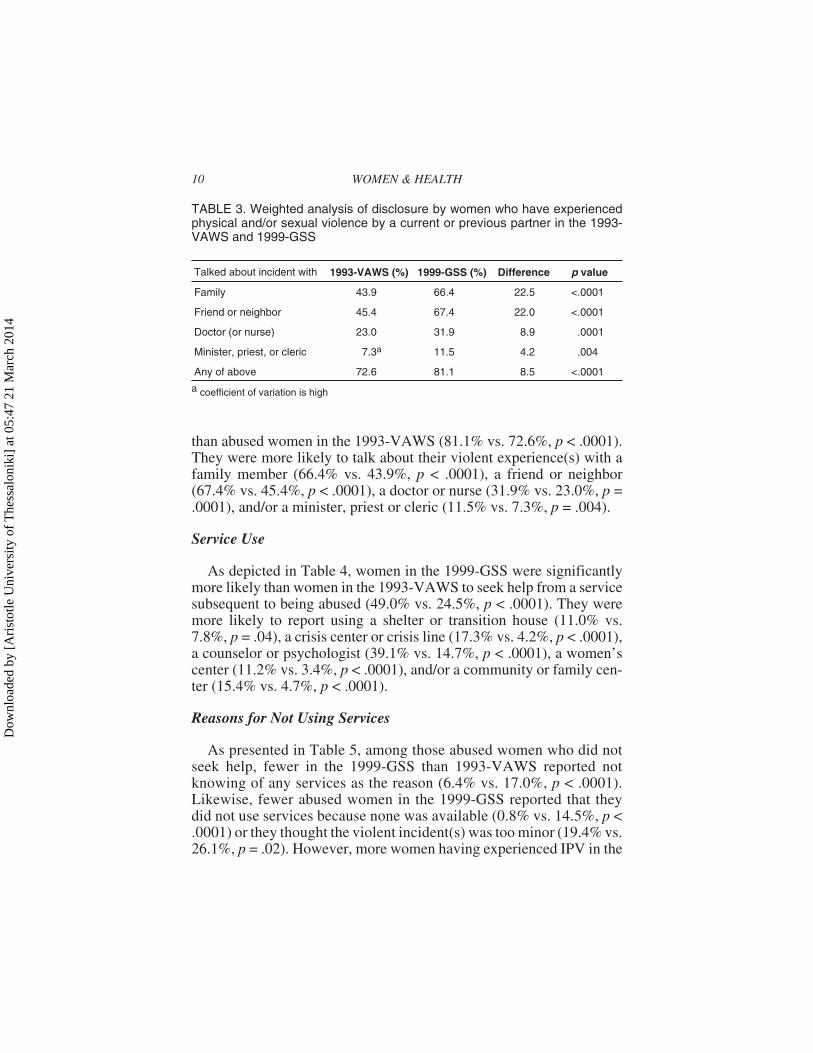
than abused women in the 1993-VAWS (81.1% vs. 72.6%, p < .0001).They were more likely to talk about their violent experience(s) with afamily member (66.4% vs. 43.9%, p < .0001), a friend or neighbor(67.4% vs. 45.4%, p < .0001), a doctor or nurse (31.9% vs. 23.0%, p =.0001), and/or a minister, priest or cleric (11.5% vs. 7.3%, p = .004).
Service Use
As depicted in Table 4, women in the 1999-GSS were significantlymore likely than women in the 1993-VAWS to seek help from a servicesubsequent to being abused (49.0% vs. 24.5%, p < .0001). They weremore likely to report using a shelter or transition house (11.0% vs.7.8%, p = .04), a crisis center or crisis line (17.3% vs. 4.2%, p < .0001),a counselor or psychologist (39.1% vs. 14.7%, p < .0001), a women’scenter (11.2% vs. 3.4%, p < .0001), and/or a community or family cen-ter (15.4% vs. 4.7%, p < .0001).
Reasons for Not Using Services
As presented in Table 5, among those abused women who did notseek help, fewer in the 1999-GSS than 1993-VAWS reported notknowing of any services as the reason (6.4% vs. 17.0%, p < .0001).Likewise, fewer abused women in the 1999-GSS reported that theydid not use services because none was available (0.8% vs. 14.5%, p <.0001) or they thought the violent incident(s) was too minor (19.4% vs.26.1%, p = .02). However, more women having experienced IPV in the
10 WOMEN & HEALTH
TABLE 3. Weighted analysis of disclosure by women who have experiencedphysical and/or sexual violence by a current or previous partner in the 1993-VAWS and 1999-GSS
Talked about incident with 1993-VAWS (%) 1999-GSS (%) Difference p value
Family 43.9 66.4 22.5 <.0001
Friend or neighbor 45.4 67.4 22.0 <.0001
Doctor (or nurse) 23.0 31.9 8.9 .0001
Minister, priest, or cleric 7.3a 11.5 4.2 .004
Any of above 72.6 81.1 8.5 <.0001
a coefficient of variation is high
Dow
nloa
ded
by [
Ari
stot
le U
nive
rsity
of
The
ssal
onik
i] a
t 05:
47 2
1 M
arch
201
4
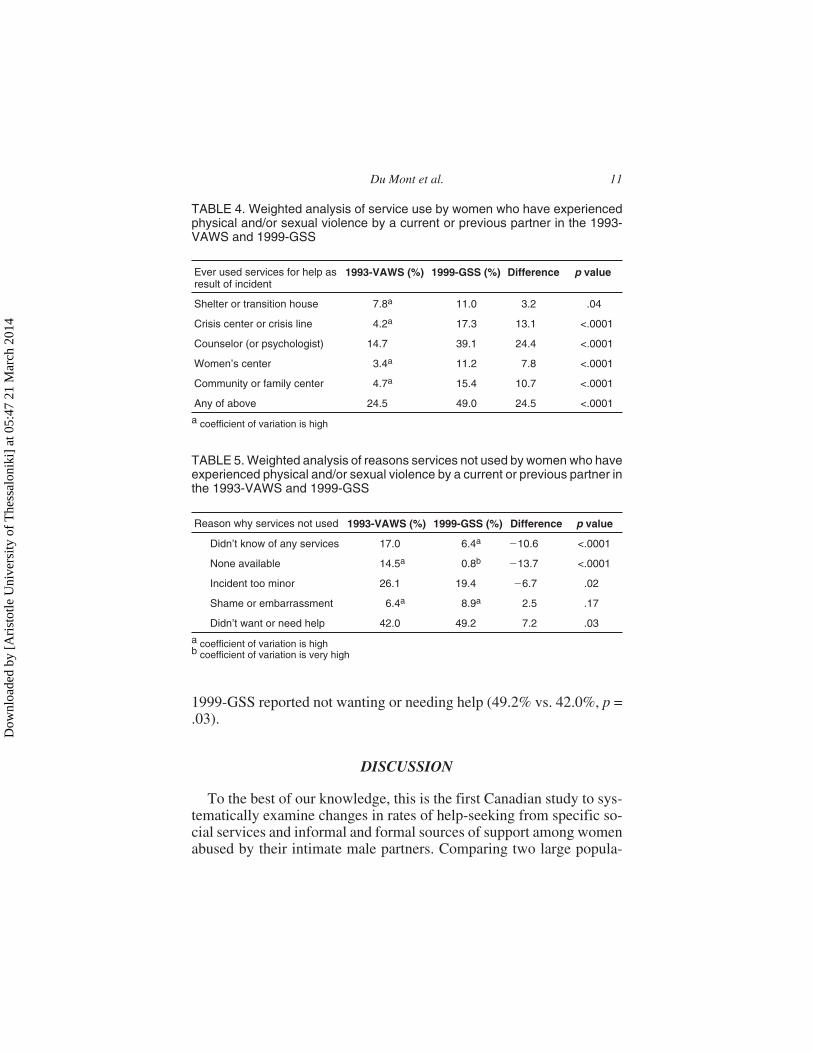
1999-GSS reported not wanting or needing help (49.2% vs. 42.0%, p =.03).
DISCUSSION
To the best of our knowledge, this is the first Canadian study to sys-tematically examine changes in rates of help-seeking from specific so-cial services and informal and formal sources of support among womenabused by their intimate male partners. Comparing two large popula-
Du Mont et al. 11
TABLE 4. Weighted analysis of service use by women who have experiencedphysical and/or sexual violence by a current or previous partner in the 1993-VAWS and 1999-GSS
Ever used services for help asresult of incident
1993-VAWS (%) 1999-GSS (%) Difference p value
Shelter or transition house 7.8a 11.0 3.2 .04
Crisis center or crisis line 4.2a 17.3 13.1 <.0001
Counselor (or psychologist) 14.7 39.1 24.4 <.0001
Women’s center 3.4a 11.2 7.8 <.0001
Community or family center 4.7a 15.4 10.7 <.0001
Any of above 24.5 49.0 24.5 <.0001
a coefficient of variation is high
TABLE 5. Weighted analysis of reasons services not used by women who haveexperienced physical and/or sexual violence by a current or previous partner inthe 1993-VAWS and 1999-GSS
Reason why services not used 1993-VAWS (%) 1999-GSS (%) Difference p value
Didn’t know of any services 17.0 6.4a �10.6 <.0001
None available 14.5a 0.8b �13.7 <.0001
Incident too minor 26.1 19.4 �6.7 .02
Shame or embarrassment 6.4a 8.9a 2.5 .17
Didn’t want or need help 42.0 49.2 7.2 .03
a coefficient of variation is highb coefficient of variation is very high
Dow
nloa
ded
by [
Ari
stot
le U
nive
rsity
of
The
ssal
onik
i] a
t 05:
47 2
1 M
arch
201
4

tion-based surveys, we found statistically significant differences inrates of disclosure and service utilization. Almost one-quarter morewomen in the 1999-GSS than 1993-VAWS disclosed to family, friendsor neighbors, and counselors or psychologists subsequent to beingabused (23%, 22%, 24%, respectively). There were also smaller but sig-nificant increases in the number of abused women in the 1999-GSS co-hort disclosing to a health care provider (9%) and spiritual advisor(4%), and using all types of social services including shelters or transi-tion houses (3%), crisis centers or crisis lines (13%), women’s centersor support groups (8%), and community or family centers (11%).
Although there could be other influences over the decade that led tothese changes, such as women’s increased independence from abusivepartners because of gradual improvements in their economic status(Federal-Provincial-Territorial Ministers Responsible for the Status ofWomen, 2002), the start of several large-scale Canadian federal initia-tives targeting violence against women may account for increaseddisclosure and service use in 1999. For example, in 1991, the govern-ment launched a second five-year Family Violence Initiative, whichwas focused in part on increasing public awareness about family vio-lence strengthening and intervention and treatment services for abusedwomen and children (Health Canada, 2002; Status of Women Canada,1998). The Federal Plan for Gender Equality, a program involving 24federal departments and agencies, was subsequently initiated in 1995(Status of Women Canada, 1995). One of its key objectives was “reduc-ing violence in society, particularly violence against women and chil-dren” (Status of Women Canada, 1995). Strategies to be implementedunder its auspices included developing and disseminating informationon models and guidelines that address the needs of abused womenliving in poverty and in rural communities, supporting informationexchange and education to improve interventions and resource mate-rials for public education, enhancing the capacity of the health ser-vice sector to recognize and respond to the needs of vulnerable orhigh risk groups, increasing media awareness of abuse and involvingthe media in prevention efforts, and supporting shelters for batteredwomen and children (Status of Women, Canada, 1995). Implemen-tation of the Plan was followed quickly in 1997 by a third phase ofthe Family Violence Initiative, also intended to promote publicawareness about and reduce abuse in the family by strengthening thecriminal justice and community-based responses to the problem, in-cluding improving and enhancing existing emergency shelters and sec-ond stage housing (Health Canada, 2002).
12 WOMEN & HEALTH
Dow
nloa
ded
by [
Ari
stot
le U
nive
rsity
of
The
ssal
onik
i] a
t 05:
47 2
1 M
arch
201
4
Differences found between the 1999-GSS and 1993-VAWS cohortson reasons for not using services might also be explained by these 1990seducational campaigns and service enhancement programs. A muchsmaller proportion of abused women in the 1999-GSS than in the1993-VAWS reported that no services were available (1% vs. 15%). Aswell, in 1999, the proportion of abused women stating that they did notknow of any services or that the violent incident(s) was too minor toseek help decreased by 11% and 7%, respectively. As noted earlier, Sta-tus of Women Canada in its 2003 address to CEDAW stated that in-creases in community-based supports and shelters might be partiallyresponsible for the decrease in reported IPV between 1993 and 1999(Status of Women Canada, 2003). However, while it is true that thenumber of shelters increased between 1993 and 1998 (Federal-Provin-cial-Territorial Ministers Responsible for the Status of Women, 2002)and has continued to increase through 2002/03 (Government of Canada,2002), CEDAW, nonetheless, responded that it was “particularly con-cerned about the inadequate funding for women’s crisis services andshelters” and urged Canada to step up its efforts to address violenceagainst women and increase its funding to such agencies (CEDAW,2003, item 369, 370).
The most common reason given for not using services in both sur-veys was not wanting or needing help, with the proportion of womenendorsing this item being significantly higher in the 1999-GSS than1993-VAWS cohort (49% vs. 42%). While it is difficult to know how tointerpret this finding, there is evidence to suggest generally that thesources of support upon which abused women rely most heavily are in-formal (e.g., Kershner & Anderson, 2002). Our data certainly supportthis assertion with far more women disclosing to family and friends orneighbors than using social services. In fact, in the 1993-VAWS whenwomen were asked what they found especially helpful in dealing withthe abuse, more stated support from family or friends than individualcounseling, support groups, doctors, and ministers, priests or clerics(Statistics Canada, 1994). Overall, the reasons given by abused womenfor not using services in the 1993-VAWS and 1999-GSS are similar tothose given in previous studies. Recall that Dal Grande and colleagues(2003) found that three of the most common reasons IPV respondents inSouth Australia did not use services were they did not want or needhelp, they were unaware of any health services that could help, and theviolent incident(s) was perceived as too minor.
Despite the increases we found in disclosure and service utilizationbetween the two surveys, it is disheartening to note that as late as 1999 a
Du Mont et al. 13
Dow
nloa
ded
by [
Ari
stot
le U
nive
rsity
of
The
ssal
onik
i] a
t 05:
47 2
1 M
arch
201
4

substantial proportion of abused women still failed to seek help fromfamily (34%), friends or neighbors (33%), spiritual advisors (88%), andhealth care providers (68%). That so few women disclosed to a doctoror nurse is unfortunate given the potentially serious health sequelae ofIPV (e.g., Koss, 1990; Krug et al., 2002; Kyriacou et al., 1999). It is adisappointing finding in that national associations such as the CanadianPsychiatric Association (1992), Canadian Public Health Association(1994), Society of Obstetricians and Gynaecologists of Canada (1996),and Canadian Nursing Association (1992, 1996) had developed policystatements and practice guidelines for early detection and treatment ofIPV just prior to and following the 1993-VAWS. Our finding is verysimilar to those from American and Australian studies with proportionsof IPV victims having disclosed to a health care professional in those ju-risdictions reported between 29% and 37% (Coker et al., 2000b; DalGrande et al., 2003; Hegarty & Taft, 2001; Kershner & Anderson,2002). To rectify this under-reporting, Petersen, Moracco, Goldstein,and Clark (2003) call for more screening to identify and assist abusedwomen in health care settings and to refer them to appropriate agenciesin the community that deal with the issue. While the issue of screeningremains contentious, and it is true that the benefit to abused women ofsocial service contact needs more rigorous evaluation (MacMillan &Wathen, 2003; Wathen & MacMillan, 2003a, 2003b), we agree that un-til then, health care providers should be sensitive to the issue of IPV andits impact on health and have protocols to refer affected women to com-munity-based services (Caralis & Musialowski, 1997).
Given the well-documented social consequences of IPV (e.g., Macleod &Kinnon, 1997; Miller & Du Mont, 2000), it is also noteworthy that aslate as 1999 more than half (51%) of abused women had never soughthelp from a social service. Despite government initiatives to enhanceservices in this sector following the 1993-VAWS, only 11% of the1999-GSS cohort used a shelter, 17% a crisis center or line, 11% awomen’s center or support group, and 15% a community or family cen-ter. These findings, which are very similar to those from the extant liter-ature, with reported shelter use ranging from 7% to 11% (Coker et al.,2000b; Gondolf, 1998) and use of formal counseling or support servicesreported at 15% (Henning & Klesges, 2002), should not necessarily because for concern as the needs of women exposed to IPV appear to bebeing addressed foremost by family and friends (Kaukinen, 2002). Suchinformal sources of support have been reported to help women copewith the violence and move toward ending it and may provide pathways
14 WOMEN & HEALTH
Dow
nloa
ded
by [
Ari
stot
le U
nive
rsity
of
The
ssal
onik
i] a
t 05:
47 2
1 M
arch
201
4

for obtaining subsequent professional care (Dunbar & Jeannechild,1996; Kaukinen, 2002).
Although the 1993-VAWS and 1999-GSS differed somewhat intheir methodology, issues surrounding the different target popula-tion and reference period are not likely to have impacted our results.For while the 1993-VAWS included women aged 18 years and olderand the 1999-GSS women aged 15 years and older, only five women inthe latter sample we examined were aged 15 to 17. Moreover, the1993-VAWS asked respondents if they had ever used services whereasthe 1999-GSS limited information to the preceding five years from thedate of the survey. Given this difference, we would have expected ratesof service use to have been higher in the 1993-VAWS, but instead,found rates of service use to have been higher in the 1999-GSS.
However, there are some limitations to this research that must be ac-knowledged. First, between surveys, there were slight variations in thewording of questions assessing disclosure and service use. For example,women in the 1993-VAWS were asked if they ever talked to a doctorabout their violent experience(s) whereas respondents in the 1999-GSSwere asked if they ever spoke with a doctor or nurse, which may par-tially account for the higher number of positive responses to this item inthe GSS cohort. Second, we were not able to assess true trends over timein help-seeking as abused women were not asked in either survey onwhich dates they had disclosed IPV and/or used services. Finally, wecould not adjust for demographic characteristics that may have influ-enced help-seeking for IPV because respondents were asked about theirage, marital status, household income, etc., at the time of the surveyinterview and not at the time of disclosure or service use.
These limitations highlight the need for additional population-basedstudies to assess whether increases in disclosure and service use subse-quent to IPV have continued. Researchers could compare the 1999-GSSwith the next cycle that examines victimizations. Future studies shouldcollect information on the demographics of women having experiencedIPV at the time of abuse so that interventions might target those who areless likely to seek help. In-depth interviews with women who have ex-perienced IPV could also shed light on what “not wanting” or “notneeding” help really means. Finally, there is a need for research that ex-amines the capacity of social services to address IPV and the effect oftheir interventions on abused women’s health and well-being (Wathen &MacMillan, 2003a, 2003b).
In the meantime, we found that our comparison of independent datasets shed light on secular changes in disclosure and service use in an in-
Du Mont et al. 15
Dow
nloa
ded
by [
Ari
stot
le U
nive
rsity
of
The
ssal
onik
i] a
t 05:
47 2
1 M
arch
201
4

formative manner. Our analyses suggest that there have been positiveshifts in IPV victims help-seeking, with more surveyed women in 1999than 1993 having recognized and articulated their experiences of abuseto individuals and support services. These shifts highlight the impor-tance of continued government commitment to funding IPV initiatives.As Macleod and Kinnon (1997) found in their evaluation of 30 HealthCanada funded projects aimed at reducing violence against women, in-formal and formal social support networks reduce “the isolation thatcontributes to violence . . . [and are an] essential part of creating healthyindividuals, families and communities” (p. 21).
REFERENCES
Abu-Ras, W. M. (2003). Barriers to services for Arab immigrant battered women in aDetroit suburb. Journal of Social Work Research and Evaluation, 4(1), 49-66.
Bacchus, L., Mezey, G., & Bewley, S. (2003). Experiences of seeking help from healthprofessionals in a sample of women who experienced violence. Health and SocialCare in the Community, 11(1), 10-18.
Bauer, H. M., Rodriguez, M. A., Quiroga, S. S., & Flores-Ortiz, Y. G. (2000). Barriersto health care for abused Latina and Asian immigrant women. Journal of HealthCare for the Poor and Underserved, 11(1), 33-44.
Bishop J., & Patterson, P. G. R. (1992, April 12). Guidelines for the Evaluation andManagement of Family Violence. (Position Paper). Canadian Psychiatric Associa-tion. Retrieved September 28, 2004, from http://www.cpa-apc.org/Publications/Po-sition_ Papers/Violence.asp
Canadian Nurses Association. (1992). Family Violence: Clinical Guidelines for Nurses.Ottawa: National Clearinghouse on Violence.
Canadian Nurses Association. (1996, March). Policy Statement: Interpersonal Violence.http://www.cna-nurses.ca/pages/policies/old policy statements out of circulation/interpersonal_violence.html
Canadian Public Health Association. (1994, November). Violence in Society: A PublicHealth Perspective. http://www.cpha.ca/english/policy/pstatem/violenc/page1.htm
Caralis, P. V., Musialowski, R. (1997). Women’s experiences with domestic violenceand their attitudes and expectations regarding medical care of abuse victims. SouthernMedical Journal, 90(11), 1075-1080.
Carrillo, R. (1992). Battered Dreams: Violence Against Women as an Obstacle to De-velopment. New York: United Nations Development Fund for Women.
Centers for Disease Control and Prevention. (2000, June 9). Use of medical care, policeassistance, and restraining orders by women reporting intimate partner violence–Massachusetts, 1996-1997. Morbidity and Mortality Weekly Report, 49(22), 486-488.
Coker, A. L., Davis, K. E., Arias, I., Desai, S., Sanderson, M., Brandt H. M., &Smith, P. H. (2002a). Physical and mental health effects of intimate partner vio-lence for men and women. American Journal of Preventive Medicine, 23(4),260-268.
16 WOMEN & HEALTH
Dow
nloa
ded
by [
Ari
stot
le U
nive
rsity
of
The
ssal
onik
i] a
t 05:
47 2
1 M
arch
201
4

Coker, A. L., Derrick, C., Lumpkin, J. L., Aldrick, T. E., & Oldendick, R. (2000b).Help-seeking for intimate partner violence and forced sex in South Carolina. AmericanJournal of Preventive Medicine, 19(4), 316-320.
Coker, A. L., Smith, P. H., Thompson, M. P., McKeown, R. E., Bethea, L., Davis, K. E.(2002c). Social support protects against the negative effects of partner violence onmental health. Journal of Women’s Health and Gender-Based Medicine, 11(5),465-476.
Committee on the Elimination of All Forms of Discrimination against Women. (2003,January). Consideration of Reports submitted by States Parties Under Article 18 ofthe Convention. New York: United Nations, Convention of the Elimination of allForms of Discrimination against Women.
Dal Grande, E., Hickling, J., Taylor, A., & Woollacott, T. (2003). Domestic violence inSouth Australia: A population survey of males and females. Australian and NewZealand Journal of Public Health, 27(5), 543-550.
De Voe, E. R., & Smith, E. L. (2003). Don’t take my kids: Barriers to service use deliv-ery for battered mothers and their young children. Journal of Emotional Abuse,3(3-4), 277-294.
Du Mont, J., & Parnis, D. (2002, September). An Overview of the Sexual Assault Careand Treatment Centres of Ontario [Revised and Expanded]. Prepared for the WorldHealth Organization, Geneva.
Du Mont, J., Macdonald, S., & Badgley, R. (1997, May). An Overview of the Sexual As-sault Care and Treatment Centres of Ontario. Prepared for the Ontario Network ofSexual Assault Care and Treatment Centres.
Dunbar, D., & Jeannechild, N. (1996). The stories and strengths of women who leavebattering relationships. Journal of Couples Therapy, 6(1-2), 149-173.
Dunkle, K. L., Jewkes, R., Brown, H. C., Gray, G. E., McIntryre, J. A., & Harlow, S. D.(2004). Gender-based violence, relationship power, and risk of HIV in women at-tending antenatal clinics in South Africa. The Lancet, 363, 1415-1421.
Federal-Provincial-Territorial Ministers Responsible for the Status of Women. (2002, De-cember). Assessing Violence Against Women: A Statistical Profile. Ottawa: Author.
Golding, J. M. (1999). Intimate partner violence as a risk factor for mental disorders: Ameta-analysis. Journal of Family Violence, 14(2), 99-132.
Gondolf, E. W. (1998). The victims of court-ordered batterers: Their victimization,help seeking, and perceptions. Violence Against Women, 4(6), 659-676.
Government of Canada. (2002, December). Report submitted to the Committee onthe Elimination of Discrimination Against Women for consideration in its reviewof Canada’s Fifth Report on the Convention on the Elimination of All FormsDiscrimination Against Women. Ottawa: Minister of Public Works and GovernmentServices Canada.
Health Canada. (2002, December). Family Violence Research Initiative. Year Five Re-port. Author.
Heise, L., Ellsberg, M., & Gottemoeller, M. (1999). Ending Violence Against Women.Population Reports, Series No. 11. Baltimore: John’s Hopkins University.
Hegarty, K. L., & Taft, A. J. (2001). Overcoming the barriers to disclosure and inquiryof partner abuse for women attending general practice. Australian and New ZealandJournal of Public Health, 25(5), 433-437.
Du Mont et al. 17
Dow
nloa
ded
by [
Ari
stot
le U
nive
rsity
of
The
ssal
onik
i] a
t 05:
47 2
1 M
arch
201
4

Henning, K. R. & Klesges, L. M. (2002). Utilization of counseling and supportive ser-vices by female victims of domestic abuse. Violence and Victims, 17(5), 623-636.
Ilkkaracan, P. (1998). Exploring the context of women’s sexuality in eastern Turkey.Reproductive Health Matters, 6(12), 66-75.
Johnson, H., & Hotton, T. (2001, June). Spousal violence. In C. Trainor & K. Mihorean(Eds.), Family Violence in Canada: A Statistical Profile 2001 (pp. 26-41). Ottawa:Statistics Canada.
Kaukinen, C. (2002). The help-seeking of women violent crime victims: Findings fromthe Canadian Violence Against Women Survey. The International Journal of Soci-ology and Social Policy, 22(7/8), 5-44.
Kershner, M., & Anderson, J. E. (2002). Barriers to disclosure of abuse among ruralwomen. Minnesota Medicine, 85(3), 32-37.
Koss, M. P. (1990). The women’s mental health research agenda: Violence againstwomen. American Psychologist, 45, 374-380.
Krug, E. G., Dahlberg, L. L., Mercy, J. A., Zwi, A. B., & Lozano, R. (Eds). (2002).World Report on Violence and Health. Geneva: World Health Organization.
Kyriacou, D. N., Anglin, D., Taliaferro, E., Stone, S., Tubb, T., Linden, J. A., Muelleman,R., Barton, E., & Kraus, J. F. (1999). Risk factors for injury to women from domesticviolence. The New England Journal of Medicine, 341(25), 1892-1898.
MacLeod, L., & Kinnon, D. (1997). Taking the Next Step to Stop Woman Abuse: FromViolence Prevention to Individual, Family, Community and Societal Health. Ottawa:National Clearing House on Family Violence.
MacMillan, H. L., & Wathen, C. N. (2003). Violence against women: Integrating theevidence into clinical practice. Canadian Medical Association Journal, 169(6),570-571.
Miller, K-L., & Du Mont, J. (2000). Countless abused women: Homeless and inade-quately housed. Canadian Woman Studies, 20(3), 115-122.
Norris, D. A., & Paton, D. G. (1991). Canada’s General Social Survey: Five years ofexperience. Survey Methodology, 17, 227-240.
Peckover, S. (2003). ‘I could have just done with a little more help’: An analysis ofwomen’s help-seeking from health visitors in the context of domestic violence.Health and Social Care in the Community, 11(3), 275-282.
Petersen, R., Moracco, K. E., Goldstein, K. M., & Clark, K. A. (2003). Women’s per-spective on intimate partner violence services: The hope in Pandora’s box. Journalof the American Medical Women’s Association, 58(3), 185-190.
Rodgers, K. (1994, March). Wife Assault: The Findings of a National Survey. JuristatService Bulletin. Ottawa: Statistics Canada, Canadian Centre for Justice Statistics.
Rodriguez, M. A., Quiroga, S.S., & Bauer, H. M. (1996). Breaking the silence: Bat-tered women’s perspectives on medical care. Archives of Family Medicine, 5(3),153-158.
Society of Obstetricians and Gynaecologists of Canada. (1996). Violence AgainstWomen. Policy Statement 46. Ottawa: Author.
Statistics Canada. (2000). The 1999 General Social Survey. Cycle 13 Victimization.12M0013GPE. Ottawa: Author.
Statistics Canada. (1993). Violence Against Women Survey. 11-001E. Ottawa: Author.Statistics Canada. (1994). Violence Against Women Survey. Microdata file. Ottawa.
18 WOMEN & HEALTH
Dow
nloa
ded
by [
Ari
stot
le U
nive
rsity
of
The
ssal
onik
i] a
t 05:
47 2
1 M
arch
201
4

Status of Women Canada. (2003, January 23). Address on the Presentation of Can-ada’s Fifth Report to the Committee on the Elimination of all Forms of Discrimina-tion Against Women. New York, United Nations.
Status of Women Canada. (2000, June). Canada and the United Nations General As-sembly Special Session Beijing 5 Fact Sheets: Women and Health. http://www.swc-cfc.gc.ca/pubs/b5_factsheets/b5_factsheets_13_e.html
Status of Women Canada. (1998, December). Report by the Government of Canada tothe United Nations Commission on Human Rights. Special Rapporteur on ViolenceAgainst Women. http://www.swc-cfc.gc.ca/pubs/unreport/unreport_e.pdf
Status of Women Canada. (1995, August). Setting the Stage for the Next Century: TheFederal Plan for Gender Equality. SW21-15/1995. Ottawa: Author.
Straus, M. (1989). Measuring intrafamily conflict and violence: The Conflicts TacticsScale. Journal of Marriage and Family, 41, 75-88.
Thompson, M. P., Saltzman, L. E., & Johnson, H. (2001). Risk factors for physical in-jury among women assaulted by current or former spouses. Violence AgainstWomen, 7(8), 886-899.
Tjaden, P., & Thoennes, N. (2000, July). Extent, Nature, and Consequences of IntimatePartner Violence: Findings from the National Violence Against Women Survey.Washington: U.S. Department of Justice, Office of Justice Programs.
United Nations General Assembly. (1993, December 20). Declaration of the Elimina-tion of Violence Against Women. Geneva: Proceedings of the 85th Plenary Meeting.
Velzeboer, M., Ellsberg, M., Arcas, C. C., & Garcia-Moreno, C. (2003). ViolenceAgainst Women: The Health Sector Responds. Washington, DC: Pan AmericanHealth Organization.
Wathen, C. N., & MacMillan, H. L. (2003a). Interventions for violence against women.Journal of the American Medical Association, 289(5), 589-600.
Wathen, C. N., & MacMillan, H. L. (2003b). Prevention of violence against women.Recommendation statement from the Canadian Task Force on Preventive HealthCare. Canadian Medical Association Journal, 169(6), 582-584.
Wingood, G. M., DiClemente, R. J., & Raj, A. (2000). Adverse consequences of intimatepartner abuse among women in non-urban domestic violence shelters. American Jour-nal of Preventive Medicine, 19 (4), 270-275.
Du Mont et al. 19
Dow
nloa
ded
by [
Ari
stot
le U
nive
rsity
of
The
ssal
onik
i] a
t 05:
47 2
1 M
arch
201
4





























