Embed Size (px)
Citation preview

ASSESSMENT AND RESPONSE TO INTIMATE PARTNER VIOLENCE IN A
STATEWIDE HOME VISITATION PROGRAM:
A QUALITATIVE DESCRIPTIVE STUDYDanielle M. Davidov PhD,
Jessica Coffman MA, Christiaan Abildso PhD MPH,Angela Dyer MSPH, Alfgeir Kristjansson PhD,
Michael Mann PhD, Thomas K Bias PhD,Emily Vasile, MPAff, Louise Moore RN

FUNDING• HRSA Maternal, Infant, and Early Childhood Home Visiting
Program Evaluation Grant– West Virginia University, School of Public Health, Health
Research Center
• WV Clinical and Translational Science Institute (WVCTSI)– Research was supported by the National Institute Of General
Medical Sciences of the National Institutes of Health under Award Number U54GM104942. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health

HOME VISITATION PROGRAMS
• Offered to the most vulnerable pregnant women and young families
• Benefits in improving prenatal, child health & development, maternal outcomes
• Evidence for prevention of child maltreatment (CM)

HOME VISITATION & IPV
• Intimate partner violence (IPV) attenuates positive effects of home visitation
• CM & IPV – Shared risk factors– Overlap in rates of perpetration (30% - 60%)– IPV in home visitation (~48%)
• Home visitation might be an appropriate mechanism to detect and address IPV

HOME VISITATION & IPV• Affordable Care Act
– $1.5 billion over 5 years
• Unique context requires new strategies– Very few interventions
• Formative research randomized trials– DV Enhanced Home Visitation (DOVE) – Nurse-Family Partnership IPV Study

HOME VISITATION & IPV
• Little is known about how home visitors assess and respond to IPV, especially in rural and underserved areas with unique social and geographic challenges
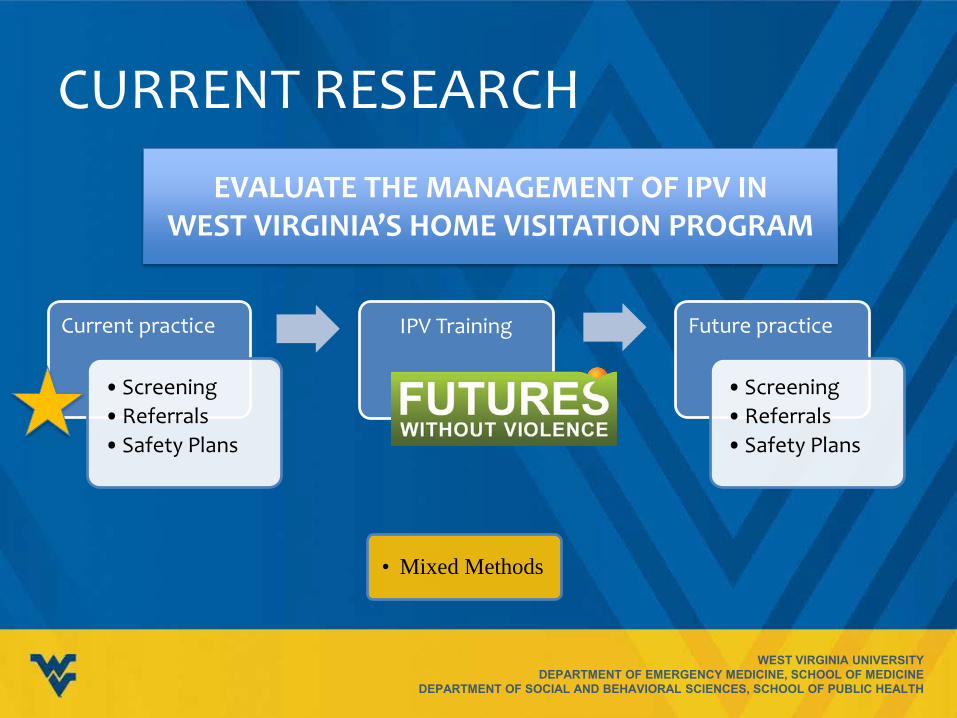
CURRENT RESEARCH
Current practice
• Screening• Referrals• Safety Plans
IPV Training
• Mixed Methods
Future practice
• Screening• Referrals • Safety Plans
EVALUATE THE MANAGEMENT OF IPV IN WEST VIRGINIA’S HOME VISITATION PROGRAM
QUALITATIVE APPROACH
• Qualitative Description (QD)– Useful for clinical and mixed methods research
– Rich, straight description of experience or event
– Describe informants’ experiences in their own language
• vs highly theoretical or abstract rendering of data

SETTING WVHVP
R R I
R E
R P
R
R P E
R E H
R
R P
R P
R M E
R
R
R M P
R
R PE
R
R I E
R
R E
R P
R
R ME
R
R I E
R EP
R EH
R E P
R
R ME
R I E P
R E P
R E
R P
R E H
R E
R M E
R M P R P
RR
R IR
R I
R E P
R PE I
R
R P
RR P
R E I P
R
R EP
R E P
R E M
Parents As Teachers = PHealthy Families America = HMIHOW = MRight From The Start = REarly Head Start = EHAPI = I

SAMPLING
• All HVs were eligible
• Invited to an optional focus group breakfast prior to mandatory IPV training session– Convenience– Maximum variation– Snowball

DATA COLLECTION
• Focus groups before IPV trainings– 3 sessions; 1 individual interview – 45 min – 1 hour
• 1 moderator • 1 note taker • Audio recorded

PARTICIPANTS
• 16 home visitors @ 3 training sites – 3–7 HVs per group – 14 women; 2 men– 12 White, 4 African American– Avg age: 41 yrs (range: 26-60) – Avg years as HV: 6 yrs (range: new-22)
• 3 HV models represented

GUIDING RESEARCH QUESTIONSScreening, Referrals, and Safety Planning
• Current protocol
• General Experiences
• Barriers
• Facilitators

What We Found Out About IPV Screening
SCREENING: CURRENT PROTOCOL
• HITS screening tool is used
– Primarily with moms, but some programs have both partners fill out the tool
– Often given on the 1st visit, but usually by the 3rd visit
– HVs feel that clients are more honest when they can ask the HITS questions verbally vs. having the client fill out the paper; paper form is useful when partner is present
– Consensus that the HITS is not a good name for the tool and that it does not elicit honest answers from clients


SCREENING: BARRIERS
• Using HITS tool makes screening challenging
• Partner being present is a barrier to screening
• Some clients feel comfortable disclosing only emotional IPV, but many do not view this as a form of abuse or control

BARRIERS: SCREENING TOOL
I’ve had moms tell me what’s going on and then when I give them the screen they mark never, never, never, never…they just say well I trust you to tell you this information but I’m not giving it. Who is that paper going to and what’s going on?
Usually at the first visit they won’t give you as much information because they don’t know you. They don’t know if they can trust you yet. And so they will typically answer all negatives so that their score comes out to where there’s no issues in the home.

BARRIERS: PARTNER’S PRESENCE
It [screening] can have the potential to be dangerous at times….I don’t feel like you get accurate answers with it because if you’re in the room with your partner or whoever and they are abusing you it’s very hard for them to mark if they scream or curse at you or if they are physically abusing you.

SCREENING: FACILITATORS
• Being able to discuss the HITS as “just a piece of paperwork” was a facilitator for new HVs
• Having flexibility about when to screen is critical – If partner is present or the HV senses tension, they
do not feel pressured to screen
• Having the time to build a trusting relationship

FACILITATORS: TRUST I mean I think that’s important, you know, to have the relationship before you give the form…I don’t think it’s accurate…what they answer on the form. You know in all my years I’ve only had one mom that answered and got a high score on her form…
I feel as if true disclosure is going to come through relationship and not from a screening tool, and so really the critical thing is to develop the relationship to the point where they trust you and can be honest with you…
What We Found Out About Referring to IPV
Services

REFERRING• Some HVs have had positive experiences referring
clients to local shelters; others have faced challenges – High turnover, lack of training and compassion
fatigue/burnout
• Transportation and long travel times to get to shelters = significant barriers
• Some HVs had never referred a client to IPV services and were unsure about the appropriate course of action after a disclosure or positive screen

REFERRING TO IPV SHELTERS
We’ve had a lot of turnover a lot in the shelter and we don’t always have a favorable experience there. I guess sometimes the people aren’t just trained in it as they should be and they’re just there doing a job. I’ve had several clients who are just like 'the advice they give me I know I’m going to get killed.' They didn’t feel safe. They really did not feel safer there…

FACILITATORS: TRUST & GUIDANCE
I think our families, with that trust, they expect you to advocate for them, and I think that’s one of the biggest things that I do tell my families: don't worry—this is what's going to go on.
I don’t feel comfortable going to [shelter] on behalf of my family let alone sending them out there on their own. I’m not going to do that.

BARRIERS: TRANSPORTATION
Obviously there is a need for a shelter….because there’s definitely a transportation barrier….we’re talking for some of these people an hour-and-a-half to get to a shelter, and that’s if they’re close to the main roads.
It’s [the shelter] not where they need, you know, close. And that’s actually a hang-up with a lot of people I’m sure because they don’t want to leave, if they do have kids they don’t want to take their kids outside of [County Name] or take them out of the school system and put them into a new school system or something.

What We Found Out About Safety Planning

SAFETY PLANNING• Safety planning may be necessary for clients in
potentially dangerous situations – Some avoidance of the term “safety plan”– Creative, indirect ways of discussing safety with
clients (eg, doing a “universal safety assessment”)
• Some HVs have never discussed or created safety plans with clients—several wanted more training and education

SAFETY PLANNING
Especially if somebody is not being honest with you I’ll add in like well what do you do if there’s a fire? So I added in to like safety for everybody and everything—well what if there’s a tornado?
I come up with a lot of clients who are kind of resistant once you start using terminology like safety plan…So I try to like dance around it a little bit… without like saying safety plan, cause a lot of times then they’re like okay now she’s going to have this in her notes, and we’ve done a safety plan, and people are going to know, and they get really resistant.

OTHER ISSUES
• Male victims or bilateral abuse – Screening & disclosure – Perceived few or no resources for male victims
• Safety plans for the HV – Feel supported by HV program, supervisors and
colleagues – Would like more information about what to do
when violence escalates when HV is present

SCREENING: IMPLICATIONS FOR PRACTICE
• Investigate screening ‘best practices’– Timing, mode, framing the issue
• HITS name
• HITS + Relationship Assessment Tool (RAT)?– From Futures Without Violence Curriculum

REFERRING: IMPLICATIONS FOR PRACTICE
• How can organizations work together to support clients experiencing DV? – Improving collaborations, building rapport and trust
• Local cross-trainings (shelters, police, legal aid, CPS)
• HVs can serve as advocates and liaisons – Provide clients with “anticipatory guidance” about what
to expect

SAFETY PLANNING: IMPLICATIONS FOR PRACTICE
• “Universal safety assessment” – Discuss safety within context of safety for all– Safety plan for DV should be explicit
• Other HV programs have adopted this approach
• More training and education – Trainings w/ WV Coalition Against DV

RIGOR & TRUSTWORTHINESS
• Member checking– Throughout data collection – After data collection
• With HVs & their supervisors
• Does this “ring true” to you?• Are we “way off” on anything?
• Are there any issues that we’ve missed?

THANK YOU!

DANIELLE M DAVIDOV, PHD
West Virginia UniversityDepartment of Emergency Medicine
Morgantown, WV304-293-4083





























