Embed Size (px)
Citation preview
Anesthesiology
Clinical evaluation of transcntaneous electronic nerve stimulation forpain control during tooth preparation
Nurhan Oztaç*/Ayçegul Ölmez**/Banu Yel***
Abstract The purpose of this study was to evaluate the effectiveness of a transcutaneouselectrical tien-e stimulation unit. The effects of electronic dental anesthesia andlocal anesthesia for deep cavity preparations in primar}- molars were compared Inchildren aged 7 to 9 years by using the Eland Color Scale. The patients hadsymmetric teeth requiring Class I cavit}- preparation. One ofthe teeth was treatedwith electronic anesthesia and the other with local anesthesia. The tooth andmethod svere selected randomly. Both restorations were finished at the same visit.There was no statistically significant difference between ¡he groups in the perceptionof pain. Fifty-six percent ofthe children preferred ¡ranscutaneous electrical nervestimulation, while 36% of them preferred local anesthesia.(Quintessence Im 1997.-28:603-608.)
Clinical reievance
Electronic anesthesia can be effective during opera-tive procedures involving deep dentinal cavities andcan be an alternative to local anesthesia in children.
Introduction
Electronic anesthesia in dentistry was popular up tothe early 190ÛS; interest subsided, but a rebirth wasinitiated by Wall and Sweet,' who described the gatecontrol theory of pain transmission. Various electronicdental anesthesia (EDA) devices are currently available.Shealy et al- introduced transcutaneous electricalnerve stimulation (TENS) for the control of chronic
* Associate Professor. Faculty of Deiitislr>'. Oazi Umversily, Depart-ment of Pedodonlics, Ankara. Turkey.
" Assistant Professor. FacuHy of Denlistry, Gazi Universily, Dcpart-manl of Pedodüiilics. Ankara. Turkey.
" * Research Assistant, Faculty of Dentistry, Gaii University. Depart-ment of Ped Oil ont ics, Ankara. Turkey.
Reprint requests: Dr Nurhan Oztas. Gazi Üniversitesi, Di^hekimligiFakiiltesi. Pedodonti Anabilim Dali. 8, Cadde. 82. Sokak. Emek.Ankara. 06510 Türkiye. Faïi 90-312-2239226.
pain. In recent years, modifications have been made tomake TENS useful in dentistry. The terms ££14 andTENShavs been used interchangeably in the literature,'All EDA units are classified as TENS units by theADA Council on Dental Materials. Instruments, andEquipment, although most manufacturers of EDAunits differentiate their units from TENS units.**
The concept of EDA has gained widespread accep-tance in dentistry. •''̂ The clinical uses of EDA orTENS for restorative dentistr>' demonstrate varioussuccess rates. Hochman* reported that more than 76%of the patients in dental procedures including sub-gingival scaling, endodontic treatment, and dentalrestorations had 90% or greater success with the use ofTENS as dental anesthesia. Clark et al'" reported theresults ofa double-biind study on the use of EDA forrestorative, periodontal, and endodontic proceduresas well as for extractions; they tbund an overall successrate of 80% in the test group and 15% in the placebogroup. Donaldson et al'' treated 124 adult patients witha high-frequency (58 Hz), low-voltage 23 V unitsimilar to EDA in conjunction with nitrous oxide-oxygen and obtained an 81% success rate. Theirsuccess rates were only 33% with EDA alone and 36%with nitrous oxide-oxygen alone.
Bishop" conducted a double-blind study of 50patients undergoing TENS for restorative procedures.
Quintessence Internationai Voiume 28, Number 9/1997 603
periodontal scaling, endodontic therapy, myofacialpain disorder therapy, and tooth extractions. TlieTENS experimental group had a success rate of 92.8%with the restorative proeedures, whereas the placebogroup responded favorably in only 15% of the restora-tive procedures.
Electronic anesthesia, although still in its infancy,promises to be increasingly effective in pédiatriedentistry,'"" Jedrychowski and Duperon''* determinedthe efficiency and acceptance of EDA for pédiatriepatients and found that EDA was effective for 95% ofthe patients receiving restorative eare. They concludedthat EDA rrught offer many safety and psychologicaladvantages over injeetable local anesthesia, Quarn-strom'^ utilized three different h-wave and square-wave TENS units in conjunction with four differentnitrous oxide delivery systems and reported a 97%success rate for children aged 13 years and younger,
Croll"' documented the placement of a Class Iresin-modified glass-ionomer restoration in a severelycarious maxillary primary first molar of a 27-month-old girl with a combination of EDA and nitrousoxide-oxygen inhalation. He stated that the benefits ofEDA were applicable to some infants as well as olderchildren, Harvey and Elliott'' evaluated the painperceptions of 20 children aged 8 to 14 years duringClass I amalgam preparations in mandibular permanentfirst molars. They found a statistically significantdifference in pain perception between the EDA groupand the control group.
Te Duits et al'^ compared the effectiveness of localanesthesia ( LA) with that of TENS via electronic dentalanesthesia for restorative dental procedures in children.No statistically significant difference was found be-tween the groups, and 78% of the patients preferredEDA, A previous study'' compared the effectivenessof EDA to that of LA for deep Class 1 cavity prep-arations in primary molars. The results of that studysupport the results obtained by te Duits et al,'^
Children are usually unable to describe their paineffectively, and their expression of pain can be affectedby age, developmental stage, verbal competency, bodylanguage, and emotional maturity, McGrath et al-''recommended simple, self-reporting measures forchildren older than 6 years of age. including a VisualAnalog Scale (VAS), Several authors-'"--* have rec-otnmended self reporting scales, including a VAS. forassessing pain in children, Spirito and Stark'"* reportedthat one major criticism of self reporting measures inyoung children was their lack of cognitive ability andlanguage skills to evaluate themselves with common
self reporting measurement techniques. According toStewart,-- the most reliable measurement of pain is acomparison between ihe patient's subjective assess-ment of pain and an objective interpretation of theperson's behavior. Stewart used the Stewart Pain ColorScale to measure pain in adults, Eland-^ later modifiedthe Stewart Color Scale for use in children between 4and 10 years of age.
The purpose of this study was to compare theeffectiveness of traditional LA and TENS for deepClass I cavity preparations in primary second molars inchildren aged 7 to 9 by using ihe Eland Color Scale,
Method and materialsHealthy, cooperative children who were aged 7 to 9years and not color blind were included in this study.Twenty-five children who reported pain on enamel anddentin during preparations were selected. They hadsymmetric primary mandibular second molars withlesions of a similar size, requiring a preventiverestoration that extended deep into the dentin on theocelusal surface. Each tooth was free of restorations,vital, nonmobiie, free of trauma, and objectively andsubjectively asymptomatic and exhibited no radio-graphic root résorption. Participants were randomlydivided into two groups. Group 1 had the firstrestoration with LA and the second with TENS.Group 2 had the treatment in the reverse order. Both ofthe restorations were completed at the same visit.
The effectiveness of TENS (V-TENS plus, Aqua-dent), which controls pain via electronic dentalanesthesia, and LA (Ultracaine D-S. Hoechst) wasevaluated using the Eland Color Scale, Before thecolor scale was used, each child was interviewed aboutthe events that had hurt in the past. The investigatorpresented eight squares in a row in the exact sameorder to each child (yellow, orange, red, green, blue,purple, brown, and black) across the top of a white feltboard and asked the child which square he or shewould choose when he or she had been hurt the most.The investigator placed the color square in the middleof the felt board away from the others, and itrepresented severe pain (numerical value of 3). Thenthe investigator asked the child which color he or shewould choose when he or she had been hurt less thanthe most painful event and placed the color squarebelow the square chosen to represent severe pain; itrepresented moderate pain (numerical value of 2).Again the investigator asked the child which color heor she would choose when hurt just a little and placed
604 Quintessence International Volume 28, Number 9/1997
Oztas et al
the color square below the colors representing severeand moderate pain. This square represented mild pain(numerical value of I ). Finally, each child was askedwhich color he or she would prefer when not hurt. Theinvestigator placed the color square at the bottom ofthe board, and it represented no pain {numerical valueofO).
After the procedure was explained to the parent andconsent was obtained for the treatment, a photographofa patient with the electronic anesthesia system wasshown to the child. A brief and simple explanation wasperformed about how the pictured person had theelectrode on her hand, which made the skin tinglewhen the battery was turned on.
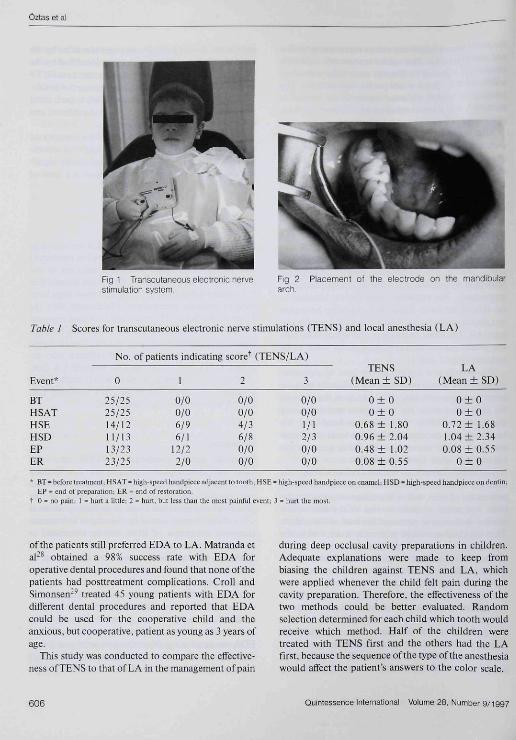
Explanations were made to keep the children frombeing biased against TENS and LA. Local anesthesiawas introduced as a sleepy water, and TENS wasexplained as a sensation "like when your foot fallsasleep, but it will be in your mouth." Electronicanesthesia was applied according to the manufacturer'sinstructions. The extraoral electrode was attached tothe skin ofthe hand. Intraoral ring silicon hose-pipewas placed on the buccal sulcus of both the maxilla andmandible. The metal electrode on the silicon hose-pipewas placed on the buccal surface of the tooth to berestored (Figs 1 and 2).
The investigator controlled the level of electronicanesthesia by slowly increasing the amplitude until thelower lip began twitching. If, at any time, the childrenfelt discomfort while the investigator was increasingthe level of TENS, they raised a hand and theamplitude was decreased. When the local anesthesiawas used, there was a 5-minute delay prior to thetreatment to allow for adequate effect.
The Eland Color Scale was used before, during, andafter the restorative procedures to assess the child'sperception of pain. Before the treatment (step I), thechild was asked to point to one of the four colorspreviously chosen to represent the level of discomfort.Then the child was asked to point to a color while thehigh-speed handpiece was running near, but not incontact with, the tooth (step 2). During the prepara-tion, the child was asked to point to a color representingthe level of discomfort when he or she felt pain onenamel or dentin (step 3). At that time. LA or TENSwas applied to the patient. After the carious lesion wascompletely removed, the child was again asked to pickthe color (step 4). The teeth were restored withamalgam. After that, the child selected the last color Sminutes postoperatively (step 5). The child's colorselection was recorded corresponding to the following
pain levels; 0 = no pain; I = an event identified by thechild as hurting a little; 2 = an event identified by thechild as a hurt but less than the most painful event; 3 =an event identified by the child as hurting the most.
After the restorations were completed, each childwas asked which method he or she had preferred andthe investigator recorded the results.
The recorded values for each step ofthe restorationscompleted with TENS and LA were analyzed via chi-square analysis to determine any statistically signif-icant difference between two techniques at a level ofP<.05.
Results
The treatment scores for TENS and LA are shown inTabfe 1. The mean scores of step I (before treatment)and step 2 (high-speed handpiece adjacent to thetooth) were 0 for both groups. That result showed thatthe patients did not feel any pain, and these steps wereused to compare pain control effectiveness with theEland Color Scale. The mean levels of pain reportedfor steps 3 to 5 were low. and the differences betweengroups were not statistically significant. There was alsono significant difference between children who re-ceived TENS first and those who received LA first.
When the children were asked which method theypreferred. 56% preferred TENS, 36% preferred LA,and 8% preferred both LA and TENS.
DiscussionElectronic dental anesthesia, or TENS, may offersafety and psychofogicai advantages over LA. Toxicityand sensitivity reactions to local anesthetic solutionsand needle phobias are eliminated. One of thepostanesthesia problems found in pédiatrie patients isself-inflicted trauma caused by chewing of soft tissues.However, symptoms of EDA can be eliminated assoon as the current is turned off. With the cessation ofEDA, the patient's tactife senses are not altered bynumbness, and ocelusal adjustment of new restora-tions may be more accurate.'''
Yap and Ho-' evaluated the comfort on administra-tion and effectiveness of electronic and local anesthe-sia for operative procedures, as perceived by cliniciansand patients. They reported that administration ofEDA was rated as significantly more comfortable thanthat of LA, by both clinicians and patients. AlthoughLA was significantly more effective than EDA, 93.3%
Quintessence Internationai Voiume 28, Number 9/1997 605
Ûztas et al
Fig 1 Transcutaneous electronic nervestimulation system.
Fig 2arch.
Placement ot the electrode on the mandibular
Table ! Scores for transcutaneous electronic nerve stimulations (TENS) and local atiesthesia (LA)
Event*
BTH SATHSEHSDEPER
No,
0
25/2525/2514/1211/1313/2323/25
of patients indicating score"̂
1
0/00/06/96/1
12/22/0
2
0/00/04/36/80/00/0
(TENS/LA)
3
0/00/01/12/30/00/0
TENS(Mean ± SD)
0 + 00 ± 0
0,68+ 1.800,96+ 2,040,48 ± 1,020,08 ±0,55
LA{Mean±SD)
0 + 00 ± 0
0.72 ± 1,681.04+2,340,08 ±0-55
0 ± 0
' BT = before treatment: HSAT = high-speed bandpieceadjacent to tooth;EP = end of preparation; ER - end of restoration,
t 0 = no pain, ! = burt a litlle: 2 = hurt, but less tban tbe most painful ev
SE = bigh-speedhandpiece on enamel; HSD = high-speed handpiece on dentin:
ent; 3 = hurt the most.
of the patients still preferred EDA to LA. Matranda etal-^ obtained a 98% success rate with EDA foroperative dental procedures and found that none of thepatients had posttreatment complications, Croll andSimonsen'^ treated 45 young patients with EDA fordifferent dental procedures and reported that EDAcould be used for the cooperative child and theanxious, butcooperative. patient as young as 3 years ofage-
This study was conducted to compare the efTective-nessofTENSto that ofLA in the management of pain
during deep occlusal cavity preparations in children.Adequate explanations were made to keep frombiasing the children against TENS and LA. whichwere applied whenever the child felt pain during thecavity preparation- Therefore, the effectiveness of thetwo methods could be better evaluated. Randomselection determined for each child which tooth wouldreceive which method- Half of the children weretreated with TENS first and the others had the LAfirst, because the sequence of the type of the anesthesiawould afFect the patient's answers to the color scale.
606 Quintessence International Volume 28, Number 9/1997
Oztas et al
As mentioned earlier, high sueeess rates have alsobeen reported for restorative procedures carried out inchildren. Until now. electronic anesthesia has onlyheen indicated for cavities that are small to moderate insize. Malamed et al-"̂ studied the use of EDA for ClassI. II. Ill, iy and V carious lesions and found an 85%success rate in shallow-to-moderate lesions and a59.5% success rate for deep ones. Te Duils et al''̂reported that EDA could control pain as etfectively asLA for lesions relatively shallow into dentin. Yap andHo-' found that EDA appears to he a viable method ofpain management during operative procedures involv-ing small-to-moderate-sized cavities. However, Estefanet aJ-'' reported that pain control under EDA does notseem to be affected by the depth of preparation or thelocation ofthe lesion.
A previous study'" used the Eland Color Scale tocompare the effectiveness of EDA to that of LA fordeep Class I cavity preparations in primary molars inchildren aged 7 to 9 years. That study followed thesame procedures as this one. except that the devicetjsed for EDA was manufactured by 3M Dental. In thepresent study, a TENS device (V-Tens Plus) thatcontrols pain via electronic dental anesthesia was used.In both ofthe studies. EDA was as successful as LA.although deep dentinal cavities were included. In theprevious study, 84% ofthe children preferred EDA and8% LA. while in the present study, 56% ofthe childrenpreferred EDA and 36/È preferred LA, The lower rateof preference for TENS (V-Tens Plus) in this study canbe attributed to the fact that the children were troubledby the numbness of their hands while the electrode wasattached to their hands.
The Eland Color Scale is the only method used toevaluate discomfort levels in children, allowing themto draw û:om their own past painful experiences.Hammond and Eull'- used the Eland Color Scale toevaluate nitrous oxide analgesia and children's percep-tion of pain and found thai the scale was effective inmeasuring pain in children. Te Duits et al'^ comparedthe effectiveness of LA with that of TENS via EDA forrestorative dental procedures in children using theEland Color Scale. They also found that the scale waseffective in measuring pain in children.
In this study, the colors ofthe Eland Color Scalewere reviewed before each restoration to ensure thatthe child was familiar with the four colors selected.Therefore, the child's initial color selection wasretested. The validity of this method was tested byevaltiating the response before treatment and torunning of the high-speed handpiece adjacent to the
tooth, two steps that should cause no discomfort. Onehundred percent of patients reported no pain for bothof these steps.
Summary
No significant differences were found between TENSand LA in their effectiveness in controlling painperception. Eifty-six percent ofthe children preferredTENS and 36% preferred LA.
References
1. Wall PD, Sweet WH. Temporary abolition of pain in man Science1967:155:108-109.
2. Shealy CN, Monimer JT, Reswick JD. Electrical inhibition of painby stimulation of the dorsal columns; Preliminary clinical reports.AnesthAnalB I967;46;489-491.
3. Malamed SF, Quinn CL. Torgersen RT, Thompson W. Electronicdental anesthesia for restorative dentistry. Anesth Prog i9S9:36:195-198.
4. Council on Dental Materials, Instruments and Equipment. Statusreport: Transctitaneous electrical nerve stimulation (TENS) in thetherapy of pain control. J Am Dent Assoc 1988:116:540.
5. Allgood JP. Trans cutaneous electrical nerval stimulation (TENS I indental practice. Compend Ccntin Educ Dem l9a6:7:6'lÜ-644.
6. Donaldson D, Quarnstrom F. lastak JT. The combined effect ofnitrous oxide and oxygen and electrical stimulation during restora-tive dental treatment. J Am Dent Assoc 1989; 118:733-7.16.
7. Malamed SF, Joseph C. Electronic anesthesia: Electricity indentistry. Compend Contin Educ Dent 1987;15:12-14.
8. Yap AUJ, Ong G. An introduction to dental electronic anesthesia.Quintessence Int 1996:27:325-331.
9. Hochman R. Neurotransmitter modutator (TENS) for control ofdental operative pain. J Am Dent Assoc 1988;! 16:208-212.
10. Clark MM, Siiverstone LM. Lindermuth J. Hicks MJ, et al. Anevaluation ofthe chnical analgesia/anesthesia elTicacy on acute painusing the high frequency neurat modulator in various dentai settings.Oral Surg Orai Med Oral Pathol 1987:63:501-505.
11. Bishop TS. High-frequency neural modulation iti dentistry. J AmDent Assoc t9S6:i t2:176-l77.
12. AbdulhameedSM.FeigalRJ. RudneyJD, etal Effect of peripheralelectrical stimulation on measures of tooth pain threshold and Uralsoft tisstie comfon in children. Anesth Prog 1989:36:52-59.
13. Segura A, Kanetlis M, Doniy KJ. Extraoral electronic dentalanesthesia for moderate procedures in pédiatrie patients [abstract!23¡. J Dent Res I995;74;27.
14. Jedrychowsb JR. Duperon DF. Effectiveness and acceptance ofelectronic dental anesthesia by pédiatrie patients. J Dent Child1993;60;186-l!)2.
15. Quarnstrom FC. Electrical anesthesia. J Cahf Dent Assoc 1988:16;J5-40.
16. Croll TP. Electrotiic anesthesia for primary molar restoration in aî7-montli-old child: A case report. Quintessence Int 1995;26;549-551.
17. Harvey M, Elliott M. Transe uta neo us electrical nerve stimulation(TENS) for pain management during cavity preparations in pédiatriepatients. J Dent Child 1995;62:49-5I.
18. te Duits E. Gocpferd S, Donly K, PinkhamJ, etal. The effectivenessof electronic dental anesthesia m children. Pediatr Dent 1993;15:191-196.
Quintessence International Volume 28, Number 9/1997 607
Oztas et ai
19, ÖitasN.ÖlmezA, YclB, TliccífeclivenessoftDA m desp denlincavities of children Pedod Clin Res iy96;.l; 19-24,
20, McGratli PJ. Beyer J. Cleeland C. Eland J. et al. Repon of thesubconiitiiltee on assessment and méthodologie issues in the manage-ment of pain in childhood cancer. Pediatrics 1996;86:814-817,
21, Carpenter PJ. New method for measuring young children's selfreport of lear and pain. J Pain Symptom ManEige 199O;5:233-24Ü,
22, Erickson CJ, Pain measurement in children: Problems and direc-üons, JDtv Bchuv Pediatr igfON h I.Î5-1.17.
23, Lavigne SV. Schulein M l . Hahn YS, Psychological aspects of painfijlmiidical conditions in ehildren. I, Developmental aspects andassessment. Pain I986;27:133-I46,
24, Spitito A, Stark JS. Childhood pain; Assessment and sisnificance ofself-repon Behav Med AbsL 1987:8:1-4.
25, StewanML, Measurement of clinical pain. In: Jacox AK led). PainA Source Book for Nurses and Other Health Professionals, Boston;Little. Brown. I977:1O7-IÍ7.
26, Eland JM. Minimising Pain Associated With PrekjniJerfeartIntramuscular Irueetions Ithesis]. Iowa City, lA: UiuvcriUy ot towa,1980,
27, Yap AUJ, Ho HCW. Electronic and local anesthesia; A ':li"''^3l "'»Icomparison for operative procedures. Quintessence Int 1996;27:549-55.1.
28, Malraiida LF. Thurmond SW. Barkmeier WW. Clinical evaluation ofan electronic anesthesia system. Gen Dent 1994:42 .14-38,
29, Croll TP. Simonsen RJ, Dental electronic anesthesia for children,J Dent Child I994;6I ;97-104.
30, Maiamcd SF. Quinn CL. Tongersen RT, Electronic dental anesthesiafor restorative dentistry, Anesth Prog 1989:36:192-200,
,i I, Estefan D, Calamia J, Calamia S, A clinical evaluation of electronicanesthesia for pain control during tooth preparation [abstract I23|.J Dent Res 1995;74:I9J,
32, Hammond Nl, Full CA. Nitrous oxide analgesia and children'sperception of pain, Pediatr Dent 1984:6:238-242. D
HARVARDsurvivesthe testof time
'Please ask for brochures
Schncllliärtcnd
Mmwm
JWII IWiCIilll Ulk* W MA
Richter & Hoffmann • Harvard Dental-GesellschaftJohannisbcrgcr Straße 24. 14197 Berlin, Germany
608 Quintessence international Volutne 28, Number 9/1997





























