Embed Size (px)
Citation preview

Community participation and attitudes ofdecision-makers towards community involvementin health development in Saudi ArabiaY. Al-Mazroal & S. Al-Shammari2
National policies and government strategies in Saudi Arabia are adequate for the promotion ofcommunity involvement in health development (CIH). The system of govemment is decentralized and hasample scope for intersectoral cooperation. In Ha'il and Qasim regions active efforts are being made torealize intersectoral coordination through regional committees in which community leaders are involved;unfortunately, however, such mechanisms are lacking at the central level. Decision-makers andcommunity leaders adequately recognized and interpreted the importance of CIH. Most of the respond-ents advocated community participation in planning and evaluation, while less than 50% thought thatcommunities could participate in the implementation of health services.
A survey in Ha'il and Qasim regions of 2417 residents indicated that community participation inhealth activities was in its infancy and that considerable effort is still needed at the central, regional, andperipheral levels to achieve meaningful community involvement in health.
IntroductionIn recent years community participation has as-sumed an increasingly important role in societies.This has been emphasized in the health sector,where, within the framework of primary health care(PHC), it has been asserted that communities haveboth the right and responsibility to be involved inthe planning, implementation and evaluation oftheir own health programmes.
Although there is general consensus aboutcommunity involvement for health development(CIH), there are differences in the approachesadopted, depending on the sociopolitical situation ina particular country and on the extent of communityorganization. Also, the perception of communityinvolvement by high-level decision-makers andhealth workers varies from one country to another.
WHO promotes community participation inPHC,a,b and the WHO Regional Office for Europehas reported the result of an analysis of variousforms of community participation in PHC in nine
' Director-General, Health Centres, Ministry of Health, SaudiArabia, and Assistant Secretary-General, Council of Health Min-isters of the Gulf Arab States.2 Assistant Professor, Department of Family and CommunityMedicine, College of Medicine 34, King Saud University, P.O.Box 2925, Riyadh 11461, Saudi Arabia. Requests for reprintsshould be sent to Dr Al-Shammari at this address.a Community involvement in health systems for primary healthcare. Unpublished WHO document SHS/83.6.b Activities for the World Health Organization in promotingcommunity involvement for health development. UnpublishedWHO document SHS/83.3.Reprint No. 5144
countries. c Also, the WHO Regional Office forAfrica has completed a study of the essentialfeatures of CIH in the African Region.d A similarstudy has also been carried out for the WHOSouth-East Asia Region.e
In Africa it has been reported that "passive"community participation was achieved but that"active" participation remains a challenge (1). Theresults of a study in rural India that involved existingpublic and private health systems demonstrated theimportance of socioeconomic and political factorsfor CIH (2). Finally, a study in Kenya of volunteerswho took part in a community-based health develop-ment programme addressed the issue of communityleadership and participation (3, 4). Because growthmonitoring has been recommended as an entry pointto PHC (5), community development has beenconsidered to be a starting point for communityparticipation in health programmes (6). Efforts toencourage community participation in health arebeing carried out in the Arab countries of the WHOEastern Mediterranean Region.f Saudi Arabia has
Analysis of the nine country study on forms of communityparticipation in PHC. WHO Regional Office of Europe. Unpub-lished document ICP/PHC 013-2.d Ben Atita, H. Major features of community involvement inhealth in the African Region. WHO Regional Office for Africa.Unpublished document.e Kutranon, S. Community involvement for health develop-ment-situation in the WHO South-East Asia Region. Unpub-lished document P 8/48/1.' Ginawi, A. A. Community participation in the Yemen ArabRepublic. Unpublished document.
Bulletin of the World Health Organization, 69 (1): 43-50 (1991) © World Health Organization 1991 43

Y. Al-Mazroa & S. Al-Shammari
adopted the strategy of Health for All by the Year2000 as well as the resolution taken in 1978 adoptingthe Declaration of Alma-Ata (7, 8). Supported by a5-year plan, the Saudi Ministry of Health embarkedin 1985 on nationwide implementation of PHC,including community participation. g,h
Objectives of the study
The objectives of the study were as follows:- to determine whether the current government
and Ministry of Health policy and strategy areoptimum, practical, and suit the situations inSaudi Arabia with respect to CIH;
- to appraise the present level of communitysupport at central and regional levels in dissemin-ating relevant information about PHC and in-teraction between health and other related sec-tors;
- to define the types, patterns, and level of com-munity participation that support the PHC team;and
- to elucidate the attitude of individuals aboutfuture community participation activities andtheir impact.
MethodThe national policies and government structureswere first reviewed. Discussions were then held withplanners and decision-makers at the central andregional levels and with community leaders at theregional level about the importance of CIH andintersectoral coordination. Using a structured inter-view format, the following 29 individuals wereinterviewed:- six senior decision-makers at the Ministry ofHealth (Directors-General of hospitals, interna-tional health, planning, preventive health, com-municable disease control and health institutes);
- the two Directors-General of health affairs inHa'il and Qasim regions;
- six senior decision-makers from the Ministries ofPlanning, Education, Labour and Social Welfare,Agriculture, and Municipalities and Rural Affairsat the central level, as well as the Presidency ofGirls Education; and
- a total of 15 similar officials and communityleaders at the regional level in Ha'il and Qasimregions.
9 Manual for PHC workers. Riyadh, Ministry of Health (Docu-ment 1406).h Fourth Five-Year Development Plan. Riyadh, Ministry of Plan-ning, 1985.
Those interviewed were selected to be repre-sentative of the decision-makers at various locationsdealing with primary health care in Saudi Arabia.Included was at least one authority to represent eachhealth delivery service or related governmentalsectors.
A questionnaire was also prepared in Arabic todetermine the views of individual community mem-bers about CIH and what action had been takentowards its implementation. The questionnaire waspre-tested in a pilot study in both rural and urbansettings and was subsequently used to carry out asurvey in Ha'il and Qasim regions, in the centre ofthe country. The total estimated population in thecatchment areas of the urban and rural healthcentres in both regions combined was 241 585 (46%)and 284 021 (54%), respectively (total, 525 606).
The sample for the study was selected using atwo-stage cluster sampling procedure. For this pur-pose, the first step was stratification into rural andurban localities. The health centres formed naturalclusters, and a 20% random sample (8 centres fromthe urban and 33 from the rural areas in bothregions) was selected in each stratum. Secondly, 138urban and 40 rural households from the catchmentarea of each selected health centre were selected.One adult member of each household (male orfemale) was asked to complete the questionnaire. Atotal of 2400 individuals (1104 (46%) from the urbanand 1296 (54%) from the rural communities) wereinterviewed. The study was completed over theperiod October 1988 to February 1989.
The data were analysed on an IBM PC micro-computer using dBASE III + software. Frequencydistribution tables and cross tabulations were ob-tained using SPSS software.
ResultsDecision-maker levelNational policies. These focused on the implementa-tion of a package of services that include thefollowing: the eight components of PHC and theenhancement and promotion of intrasectoral andintersectoral planning and action for communitydevelopment. In Ha'il and Qasim regions thesenational policies and strategies have been adoptedby the decision-makers and been implemented. Aregional development committee, consisting of deci-sion-makers and planners from various governmentsectors as well as community leaders and otherprominent individuals has been formed to promoteboth intersectoral activities and community involve-ment for regional socioeconomic development, in-cluding health. Similar committees have beenformed at the subregional and peripheral level.
44 WHO Bulletin OMS. Vol 69 1991.

Community involvement in health development in Saudi Arabia
Government structure. Government policy in SaudiArabia is to decentralize the decision-making pro-cess, particularly in areas concerned with develop-ment. Each region is autonomous in making deci-sions within the general frame of national policies.In 1982, the Council of Ministers issued a decree forthe formation of rural development committees.Each committee is responsible for a number ofvillages, and includes representatives from eightrelated ministries, including health, as well asprominent local individuals. The proposals made bythese committees are submitted to the regionaldevelopment committee for further discussions,integration, and approval. In 1986 the Council ofMinisters issued a further decree to establish andapprove the operating plans for social developmentcentres, whose main purpose is to encourage com-munity participation in local/rural socioeconomicdevelopment. Several of these centres have beenestablished in different parts of Saudi Arabia, andalmost all are adjacent to a PHC centre or have sucha centre within their premises.
Results of the interviews. The results of the inter-views of the 29 central and regional planners,decision-makers, and community leaders are out-lined below.
1) Interpretation and understanding of CIH. A totalof 28 (96%) of those interviewed understood CIH tobe the participation of communities in actionsrelated to the development of their health standards;these individuals considered CIH to comprise effect-ive cooperation between community members andhealth workers, leading to the appropriate use ofavailable health services, especially promotive andpreventive services. Altogether, 27 (93%) of therespondents considered CIH to be a means of usinglocally available community potentials and resourcesto support government activities for communityhealth and socioeconomic development.
2) Importance of CIH as a basic principle ofPHC. CIH was considered by 28 (96%) of therespondents to be an essential tool and basicprinciple for the success of PHC within the contextof overall socioeconomic development; in contrast,23 (79%) considered it to be a good starting pointfor PHC at the peripheral level. It was held by 27respondents (93%) that CIH helps planners, deci-sion-makers, and community leaders to identifycommunity needs and to make their plans morerealistic and responsive. Of these individuals, 25added that it generates a feeling of responsibilityamong individuals for their health, and thus prom-otes self-reliance. Altogether, 24 (83%) intervie-
wees believed that CIH will lead to improvements inhealth and in the delivery of health-related servicesbecause communities should become better able todefine critically the shortcomings in such servicesand assist in rectifying them; this group added thatCIH should make communities more aware of theimportance of following healthy attitudes, behavi-ours, and a life-style that should protect them fromdisease and injuries. In addition, 20 (69%) intervie-wees thought that realization of CIH will reduce thecost of health services, because people will rely moreon promotive and preventive activities to improvetheir own health.
3) Levels, depth, and dimensions of CIH. It washeld by 19 (65%) of the interviewees that communi-ties can be involved in planning health and health-related services, while 14 (48%) thought that com-munities can be involved in implementing PHCactivities. Overall, 25 interviewees (86%) believedthat communities can be involved in the evaluationof PHC activities or services.
4) Current standards of CIH at the central andregional levels. All the respondents at the centrallevel considered that CIH is in its infancy in SaudiArabia and needs more time to develop. Moreexposure to the PHC approach and the CIH conceptis still required before there will be participation atthe central level. Although the majority of respon-dents at the regional level believed that achieve-ments in CIH were satisfactory also at this level,more time is needed to make it more effective.5) Coordination between health and health-relatedsectors.
* At the central levelThis was discussed with the six Ministry of Healthofficials and six planners and decision-makers inrelated sectors. Nine thought that currently there issome coordination between these sectors, since allsectoral development plans are usually discussedtogether and compiled into a single national socio-economic plan. Half of those interviewed cited theexample of the rural development committees whereeight sectors discuss and coordinate their plans.
Five respondents cited the following examplesof successful coordination:- that between the Ministry of Health, municipali-
ties, and the agricultural sector to improveenvironmental health and sanitation;
- that between the Ministry of Health, municipali-ties, the agricultural sector, and emirates tocontrol zoonotic diseases, particularly brucellosis;
- that between Ministry of Health, Ministry ofEducation, the Presidency of Girls Education and
WHO Bulletin OMS. Vol 69 1991. 45

Y. Al-Mazroa & S. Al-Shammari
other ministries concerned with school health;-that between the Ministry of Health, industrial,
agricultural, and labour and social welfare sectorson workers' health; and
- that between the Ministry of Health and thelabour and social welfare sector on the care ofdisabled persons.
* At the regional levelThe 17 regional planners, decision-makers andcommunity leaders who where interviewed weresatisfied with the activities of the existent regionaldevelopment committees for strengthening intersec-toral coordination and community involvement. Ofthese, 16 stated that all sectoral development plansat the regional level are discussed by all regionaldecision-makers and planners and then compiled asa unified regional plan before being submitted to thecentral authorities. Twelve (70%) referred to thesupport given by related sectors and the regionalcommunity leaders to health authorities in imple-menting PHC. Ten (59%) cited the formation ofhealth committees at the peripheral level, whichinclude representatives of various sectors and com-munity members, to support the PHC teams. Eleven(65%) referred to peripheral rural developmentcommittees, where all sectors are represented aswell as community leaders. These committees repre-sent the lowest rung of the "bottom-up" system ofplanning that is responsive to the community'sneeds.
Among the other practical actions reported bythe respondents were the following:- the campaign for schistosomiasis control in Ha'il,
where all the sectors concerned and communityleaders as well as community members workedtogether under the supervision of the amir of theregion;
- the brucellosis control measures in Qasim region,where all the various sectors and communitiesparticipated; and
- the school health, environmental health, andsanitation activities in the Ha'il and Qasimregions.
6) Methods for improving intersectoral coordinationfor the promotion of CIH. Of the 12 respondentsfrom the Ministry of Health and centrally locatedsectors with whom this topic was discussed, 10(83%) suggested that a central intersectoral coordi-nation committee should be established and em-phasized that decision-makers and planners shouldpay greater attention to intersectoral planning andCIH. Nine of the interviewees (75%) believed thatthis could be achieved by drawing the attention ofthe community at large to the concept of intersec-toral coordination and CIH.
7) Means, methods, and mechanisms for promotingmore effective CIH. A total of 25 (86%) of the 29respondents believed that this could be attained bycontinuously educating and informing the commun-ity about the importance of their involvement insocioeconomic activities, including health. Twentyrespondents (69%) suggested that decision-makersshould accept the concept of CIH and regardcommunities as their partners, while 15 (48%) heldthat promotion of effective intersectoral coordina-tion was a prerequisite for promoting CIH. Al-together, 17 interviewees (58%) believed that im-provement of health services will encourage CIH.
Fourteen interviewees (48%) believed thatcommunities have to be made aware of theirpotentials and responsibilities in various areas ofsocioeconomic development, including health. Inaddition, 16 (55%) considered that recognition andinclusion in development plans of reasonabledemands of communities will motivate them toparticipate in CIH. To this, 12 (41%) intervieweesadded that shortcomings in services identified bycommunities should be taken seriously, in order toencourage their participation, and that good rela-tionships between communities and PHC workerswill promote CIH.
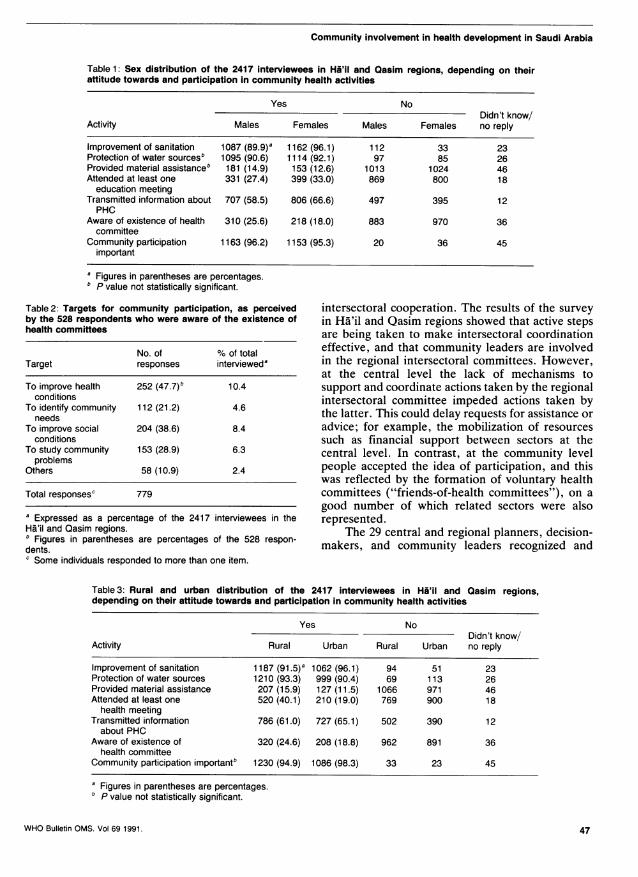
Community levelInterviews of 2417 persons (1208 males, 1209 fe-males) were carried out in 41 clusters in Ha'il (926people) and Qasim (1491 people) regions. Table 1shows the sex distribution of the respondents,depending on their attitude towards and participa-tion in community health activities. With the excep-tion of the responses for protection of water sourcesand material assistance, all the differences shown inTable 1 are statistically significant.
Table 2 shows the targets for communityparticipation, as perceived by the 528 individuals inthe Ha'il and Qasim regions who were aware of theexistence of health committees.
Table 3 shows the distribution in rural andurban areas of the 2417 interviewees in Ha'il andQasim regions in terms of their attitude towards andparticipation in community health activities. All thedifferences in Table 3 are statistically significant,except those for whether community participation isimportant.
DiscussionDecision-maker levelThe national policies and strategies for PHC inSaudi Arabia are adequate for the promotion ofcommunity participation. The government structureis decentralized and there is ample scope for
WHO Bulletin OMS. Vol 69 1991.46
Community involvement in health development in Saudi Arabia
Table 1: Sex distribution of the 2417 interviewees in Ha'il and Qasim regions, depending on theirattitude towards and participation in community health activities
Yes NoDidn't know/
Activity Males Females Males Females no reply
Improvement of sanitation 1087 (89.9)a 1162 (96.1) 112 33 23Protection of water sourcesb 1095 (90.6) 1114 (92.1) 97 85 26Provided material assistanceb 181 (14.9) 153 (12.6) 1013 1024 46Attended at least one 331 (27.4) 399 (33.0) 869 800 18
education meetingTransmitted information about 707 (58.5) 806 (66.6) 497 395 12PHC
Aware of existence of health 310 (25.6) 218 (18.0) 883 970 36committee
Community participation 1163 (96.2) 1153 (95.3) 20 36 45important
a Figures in parentheses are percentages.b P value not statistically significant.
Table 2: Targets for community participation, as perceivedby the 528 respondents who were aware of the existence ofhealth committees
No. of % of totalTarget responses intervieweda
To improve health 252 (47.7)b 10.4conditions
To identify community 112 (21.2) 4.6needs
To improve social 204 (38.6) 8.4conditions
To study community 153 (28.9) 6.3problems
Others 58 (10.9) 2.4
Total responsesc 779
a Expressed as a percentage of the 2417 interviewees in theHa'il and Qasim regions." Figures in parentheses are percentages of the 528 respon-dents.c Some individuals responded to more than one item.
intersectoral cooperation. The results of the surveyin Ha'il and Qasim regions showed that active stepsare being taken to make intersectoral coordinationeffective, and that community leaders are involvedin the regional intersectoral committees. However,at the central level the lack of mechanisms tosupport and coordinate actions taken by the regionalintersectoral committee impeded actions taken bythe latter. This could delay requests for assistance oradvice; for example, the mobilization of resourcessuch as financial support between sectors at thecentral level. In contrast, at the community levelpeople accepted the idea of participation, and thiswas reflected by the formation of voluntary healthcommittees ("friends-of-health committees"), on agood number of which related sectors were alsorepresented.
The 29 central and regional planners, decision-makers, and community leaders recognized and
Table 3: Rural and urban distribution of the 2417 interviewees in Hi'il and Qasim regions,depending on their attitude towards and participation in community health activities
Yes NoDidn't know/
Activity Rural Urban Rural Urban no reply
Improvement of sanitation 1187 (91.5)a 1062 (96.1) 94 51 23Protection of water sources 1210 (93.3) 999 (90.4) 69 113 26Provided material assistance 207 (15.9) 127 (11.5) 1066 971 46Attended at least one 520 (40.1) 210 (19.0) 769 900 18
health meetingTransmitted information 786 (61.0) 727 (65.1) 502 390 12
about PHCAware of existence of 320 (24.6) 208 (18.8) 962 891 36
health committeeCommunity participation importantb 1230 (94.9) 1086 (98.3) 33 23 45
a Figures in parentheses are percentages.P value not statistically significant.
WHO Bulletin OMS. Vol 691991. 47

Y. Al-Mazroa & S. Al-Shammari
interpreted the importance of CIH, probably be-cause the majority of them considered that itessentially involved intimate cooperation betweencommunity and health workers that would lead toappropriate use of services and of the community'spotential for health development. Furthermore,most of the respondents at this level believed thatcommunity participation would assist planners anddecision-makers to set realistic and responsive plansto tackle community health and associated prob-lems; and at the same time it should help to improveservices by defining their shortcomings and reducingtheir cost. Most of these respondents also advocatedcommunity participation in planning and evaluatingservices, but less than half believed that the commu-nities could participate in implementing the services.This difference arose because the decision-makersperceived implementation of CIH to be a technicalprocess that should be carried out by health work-ers, and not as part of the broader primary healthcare concept. The erroneous belief that curativeservices are more important than preventive mayhave influenced the thinking of the decision-makers;protection of water sources and environmentalsanitation are, however, also extremely importantelements of PHC, a fact which was acknowledged bythe responses of those interviewed at the communitylevel.
The information provided by the respondents atthe central level suggested that in the planningprocess intersectoral coordination was limited to thecompilation of sectoral plans into a national plan.Furthermore, the role of the community in thepreparation of these plans was not defined. Thisexplains why the majority of respondents (83.3%) atthis level suggested that an intersectoral coordina-tion committee for planning purposes be establishedfor orientation of decision-makers, planners, andcommunity leaders about intersectoral planning,and to give importance to the role of the communityin this respect.
There was nevertheless some coordination be-tween the eight sectors involved with those ruraldevelopment committees that were more account-able to regional than central levels. At the sametime, intersectoral coordination occurred in connec-tion with specific action on community healthdevelopment, e.g., improvement of environmentalhealth and sanitation, control of zoonotic diseases,improvement of workers' and schoolchildren'shealth, and care of the disabled.
Regional intersectoral coordination and com-munity participation were satisfactory. The regionaldevelopment committees, consisting of decision-makers, planners, and community representatives,prepared and discussed their plans before compiling
them; the success of PHC and the evolution ofcommunity participation in the two study regionswas greatly supported by these committees. At theperipheral and regional levels, representatives ofvarious sectors coordinate with each other and thehealth sector through the friends-of-health com-mittees. The process of bottom-up and intersectoralplanning was also emphasized by the rural develop-ment committees. Different sectors were thereforenot only coordinating with each other at the plan-ning stage but also in various actions related tocommunity health development, which promotedand motivated community participation at the re-gional and peripheral levels.
Community levelThe majority of respondents at the community levelwere highly motivated towards improving sanitationand protecting water resources. However, the extentto which they provided material assistance, attendededucation meetings, or transmitted informationabout PHC was unsatisfactorily low. The differencesbetween the two sexes in this respect may havearisen because the female respondents were moreexposed to education programmes at health centres,which they attended frequently with their children.In rural areas people have no alternative but to usethe free health centre services. The health and socialactivities provided there are a novelty for the localpopulations, who are more loyal to such centres thanare their urban counterparts. People in rural areaswere therefore more aware of health committeesand attended health centres more regularly thanthose who lived in cities. Both the urban-ruraldifferences and those between the sexes that arediscussed above can be narrowed through efficienthealth education programmes.
More than 95% of the community respondentswere in agreement about the importance of com-munity participation with the PHC teams, and gavegood reasons for their affirmative answers. How-ever, only one fourth or less of those interviewedknew about the friends-of-health committees in theirareas and could define the roles that such commit-tees played. This may be because the PHC conceptis relatively new in the community. Furthermore,the benefits derived from the availability of freehealth services may predispose some individuals tobehave only as recipients. Schemes to promotecommunity cooperation and participation shouldtherefore be adopted. In general, however, thecommunities did participate as indicated by theiractivities in refuse disposal, protection of watersources from pollution, dissemination of informa-tion, and admittedly to a lesser extent, in providing
WHO Bulletin OMS. Vol 69 1991.48

Community involvement in health development in Saudi Arabia
materials and financial support to the health centres.For more than 30 years various types of
community participation activities have existed inSaudi Arabia. These vary from area to area, andtheir income is mainly derived from private do-nations. Some support the needy or the disabled orboth, while others provide primary health servicesfree or at a minimal cost. At present the totalnumber of such voluntary welfare organizations is 93(Directorate of Social Development, private com-munication).
Initially, community participation in SaudiArabia involved only fund-raising, but with time, ithas evolved to cover other aspects, particularly afterthe adoption of the PHC approach and its im-plementation in different parts of the country. Thisrepresents a vital change from the original approach,where the community was seen as the passiverecipient of services planned and/or supplied by thecentral government. It cannot be expected that theswitch-over from centrally managed to community-based activities will happen immediately. In manycountries such a step will require significant changesin policy together with reorganization and reorienta-tion of health workers as well as of the community.
Below are some of the ways in which the resultsof the study have been used.* The outcome was widely distributed to relevant
decision-makers at central and regional levels inSaudi Arabia.
* Seminars on PHC in Saudi Arabia and Arabcountries of the Gulf discussed the findings andconsiderable interest was generated.
* In Saudi Arabia at least 200 PHC supervisorsattended training courses directed at planningactivities to promote PHC and motivate commun-ity participation.
* Several regions in Saudi Arabia shared theirexperiences on setting up health committees andthe procedures adopted for motivating the com-munity, and almost every health centre now has ahealth committee.
Recommendations* A wide national programme should be launched
in Saudi Arabia to orientate decision-makers andthe community towards CIH.
* An intersectoral coordination committee at thecentral level would facilitate action to achieveCIH.
* The two Council of Ministers' decrees on CIHshould be implemented properly.
* Bottom-up planning should be developed and
promoted through greater involvement of thedifferent sectors and community representatives.
* More studies are needed to identify the know-ledge, attitude, and practices of populationstowards community participation.
* Information about good examples and experi-ences of community participation in differentparts of Saudi Arabia should be disseminated.
* Active support for the friends-of-health com-mittees is needed, by setting clear plans thatdefine community roles.
AcknowledgementsThe study was supported financially by WHO (award of theJacques Parisot Foundation Fellowship to Y. Al-Mazroa) andby the Ministry of Health, Saudi Arabia.
ResumeParticipation de la communaute et attitudesdes decideurs a l'egard de I'engagementcommunautaire en faveur du developpementsanitaire en Arabie saoudite
Vingt-neuf decideurs, planificateurs et responsablescommunautaires aux niveaux central et r6gional onte interviewes en Arabie saoudite pour d6terminerd'appui fourni pour 1'engagement de la communauteen faveur du developpement sanitaire. Les politiquesnationales et le niveau d'integration dans les diverssecteurs publics pour la promotion de 1'engagementcommunautaire ont egalement fait l'objet d'une 6va-luation. Les politiques et les strategies nationales sesont aver6es adequates pour la promotion de 1'enga-gement communautaire, la structure decentralisee dugouvernement facilitant la cooperation intersecto-rielle. Dans les regions de Ha'il et Qasim, dans lecentre du pays, de gros efforts de coordination onte consentis par le biais de comit6s intersectorielsregionaux comprenant des responsables communau-taires. Malheureusement, un engagement equivalentfait defaut au niveau central. Les decideurs et lesresponsables communautaires ont e en mesure dereconna^itre et d'interpreter l'importance de 1'engage-ment communautaire en faveur du developpementsanitaire. La plupart des personnes interrogees a ceniveau se sont declarees favorables a la participationde la communaute a la planification et a 1'evaluation,
WHO Bulletin OMS. Vol 69 1991. 49

Y. Al-Mazroa & S. Al-Shammari
mais moins de 50% ont indique que les communau-t6s pourraient participer a la mise en place desservices de sante.
Une enquete sur le niveau de participation desmembres de la communaut6 au d6veloppement sani-taire a ete realisee aupres de 2417 habitants decommunautes rurales et urbaines dans les r6gionsde Qasim et Ha'il. Un nombre egal d'hommes et defemmes ont e interview6s. Les resultats ont montreque la participation des membres de la communauteaux activit6s sanitaires en est encore a ses debutsdans la region etudi6e. L'approche adopt6e en vuede la participation communautaire etait de former des"comites d'amis de la sante", dont le travail principalconsistait a diffuser des informations sanitaires et apromouvoir une meilleure utilisation des services desante, en particulier des activites de pr6vention et depromotion. Neanmoins, de gros efforts sont encorenecessaires aux niveaux central, regional et peri-pherique pour obtenir un engagement communau-taire significatif dans l'action de sante en Arabiesaoudite.
Les differences observees entre les reponses(sexe et lieu geographique) sont analysees et desexplications possibles sont donnees. Plusieurs fa-cons d'utiliser les resultats de ces etudes sont egale-ment proposees.
References1. Katzenellenbogen, J.M. et al. Community participation
in the Mamre Community Health Project. South Africanmedical journal, 74: 335-338 (1988).
2. Antia, N.H. The Mandwa Project: an experiment incommunity participation. International journal of healthservices, 18(1): 153-164 (1988).
3. Kaseje, D.C. et al. Characteristics and functions ofcommunity health workers in Saradidi, Kenya. Annals oftropical medicine and parasitology, 81(suppl. 1): 56-66(1987).
4. Kaseje, D.C. et al. Community leadership and participa-tion in the Saradidi, Kenya, Rural Health DevelopmentProgramme. Annals of tropical medicine and parasit-ology, 81(suppl. 1): 46-55 (1987).
5. Genece, E. & Rohde, H.J.E. Growth monitoring as entrypoint for primary health care. Indian journal of pediatrics,55(suppl. 1): S78-S83 (1988).
6. Charles, V. & Charles, S.X. Community development-an entry point for community participation in healthprogrammes. Indian journal of public health, 31(2):104-108 (1987).
7. Primary Health Care. Report of the International Confer-ence on Primary Health Care, Alma-Ata 1978. Geneva,World Health Organization, 1978 ("Health for All" SeriesNo. 1).
8. Global Strategy for Health for all by the Year 2000.Geneva, World Health Organization, 1981 ("Health forAll" Series No. 3).
50 WHO Bulletin OMS. Vol 69 1991.





























