Embed Size (px)
Citation preview

Complexity and health – yesterday’s traditions,tomorrow’s futurejep_1163 543..548
Joachim P. Sturmberg MBBS DORACOG MFM PhD FRACGP1 andCarmel M. Martin MBBS MSc PhD FRACGP2
1Associate Professor, Monash University, Melbourne, and The Newcastle University, Newcastle, Australia2Associate Professor, Northern Ontario School of Medicine, Sudbury, Ontario, Canada
Keywords
complexity, health, health experience, healthsystems, philosopy of medicine
Correspondence
Joachim P. SturmbergPO Box 3010WamberalNSW 2260AustraliaE-mail: [email protected]
Accepted for publication: 9 February 2009
doi:10.1111/j.1365-2753.2009.01163.x
Introduction‘If it is complex it means we don’t really understand it,and the way forward is to break the problem down into its partsto make sense of it’. This thought reflects the way we havebeen taught, and the way we largely practise in clinical care everyday.
But are we really functioning on this basis? Or is it the only waywe know how to live? We all experience situations every daywhere the evidence does not really fit our understanding of aproblem – the familiar reductionist approach limits our ability tofully explore new problems and to gain new insight. An increas-ingly persistent question has emerged in relation to what consti-tutes the knowledge we need for effective and efficient clinicalcare, an issue taken up by this new Forum on Systems and Com-plexity in Medicine and Healthcare.
The world will not evolve past itscurrent state of crisis by using thesame thinking that created thesituation (Albert Einstein)The biomedical approach to medicine has given us a mostdetailed understanding of the anatomy and physiology of thenormal and abnormal functioning of our bodies. Nevertheless, ormaybe simply because of this success, is the ‘biomedical taking itapart method of medicine’ starting to fail our patients [1]? Ourunderstanding of health as absence of disease has furtherstrengthened a longstanding dichotomous medical world view, aview that is strangely, though not unsurprisingly, foreign to ourpatients [2].
Historically, health care emerged in hunter and gatherer societ-ies in response to the experience that caring for the sick and injuredimproved their own survival. As caring for the sick became moresophisticated, the role of the shaman/medicine man evolved toinclude three functions – curing the sick, directing communalsacrifice and escorting the dead to another world. In today’ssociety, we have separated these roles into three professions: thedoctor, the priest and the undertaker [3].
Although these functions are separated in modern society, theyare still important functions expected by society and remainexceedingly important for the patients’ healing. The word ‘health’arose from the old English ‘hal’ meaning ‘whole’ – healing is‘becoming whole’.
From its beginnings medicine had an important social function;restoring the health of the sick and injured enabled them to onceagain become fully functioning members of the community. Inrecognition of the importance of the healer, society granted him, atthat time healers were almost always male, the privilege of nothaving to hunt; besides being fed, he often also received gifts.These social perspectives remain fundamental to our understand-ings of health, illness and care [4,5].
If our reductionist approach to medicine is the cause of the crisisin patient care, can more of the same lead to its solution [1,6–9]?In Albert Einstein’s view the answer is an unequivocal ‘no’. Abetter understanding of more of the parts will further remove usfrom understanding the whole; or using system philosophical lan-guage ‘the whole is different to and more than the sum of its parts’.
Engel, in 1977, already recognized the deficiencies of the reduc-tionist project on medicine and proposed a system-based model ofhealth care to counterbalance and complement the prevailingworldview – the now widely acknowledged but rarely practisedbiopsychosocial model of health care [10,11].
Journal of Evaluation in Clinical Practice ISSN 1356-1294
© 2009 The Authors. Journal compilation © 2009 Blackwell Publishing Ltd, Journal of Evaluation in Clinical Practice 15 (2009) 543–548 543

The best interest of the patient is theonly interest to be considered, and inorder that the sick may have thebenefit of advancing knowledge, unionof forces is necessary (William J. Mayo,MD, Rush Medical CollegeCommencement, 1910)The notion of complexity, meaning that something is ‘complex’ ifit is made of (usually several) closely connected parts, is not reallynew. William Osler already remarked in the late 19th century that‘It is much more important to know what sort of a patient has adisease than to know what kind of a disease a patient has’ [12]. Herecognized the importance that factors other than identifiablepathologies were interconnected to the patient’s health and healthexperience.
The importance of the patient’s health experience was thedriving force for the Mayo Brothers too, not only in terms of thecare needs for the patient, but also in regards to education, researchand health care organization. It is this core value that reverberatedthrough the clinic and helped it to emerge as one of the most highlyregarded institutions in the world.
Though neither Osler nor Mayo explicitly used systems or com-plexity language, they both clearly articulated the interconnectednature of the patient with his environment and the collaborationamong highly qualified and motivated health care workers in an afully integrated organization.
Despite rapidly increasing biomedical knowledge about dis-eases and technological advances for treating those neither Oslernor the Mayo Brothers saw the need to separate the disease fromthe patient, the Cnidian approach. They embraced the well-proven Hippocratic traditions of the Greek School of Cos thatsaw the disease as inseparable from the patient [2]. The bestdoctors have always tried to find the balance between thesetwo ideas. The development of the patient-centred clinicalmethod [13–15] and relationship-centered care [16] are yet othermoves in the same direction. Medicine needs well-rounded prac-titioners who are comfortable with and conscious about makingdecisions in a particular context, and aware that variationsin practice in any given situation is natural and to be expected[17].
How may systems and complexityscience contribute to ourunderstanding of health andhealth care?A key aim of the new Forum on Systems and Complexity inMedicine and Healthcare is to reinvigorate our traditional connec-tions with the ‘complex messy world of health and disease’ asexperienced by our patients and to strengthen the interconnectednature of thinking, knowing and acting in the field of health andhealth care. Knowing is complex [18]; every issue we seem toknow in medicine – and for that matter in general – is contextsensitive and can be seen through another prism providing us withadditional ‘frames’ of understanding. These ‘frames’ provide newmental structures that shape the way we see the world [19];systems and complexity science therefore offers an extension tounderstanding, rather than a panacea, to the current intellectual,
therapeutic, organizational and educational crisis in medicine[8,9,18,20,21].
Before exploring complex issues in health care, we need torevisit the lay term perceptions of the term complexity (Table 1).
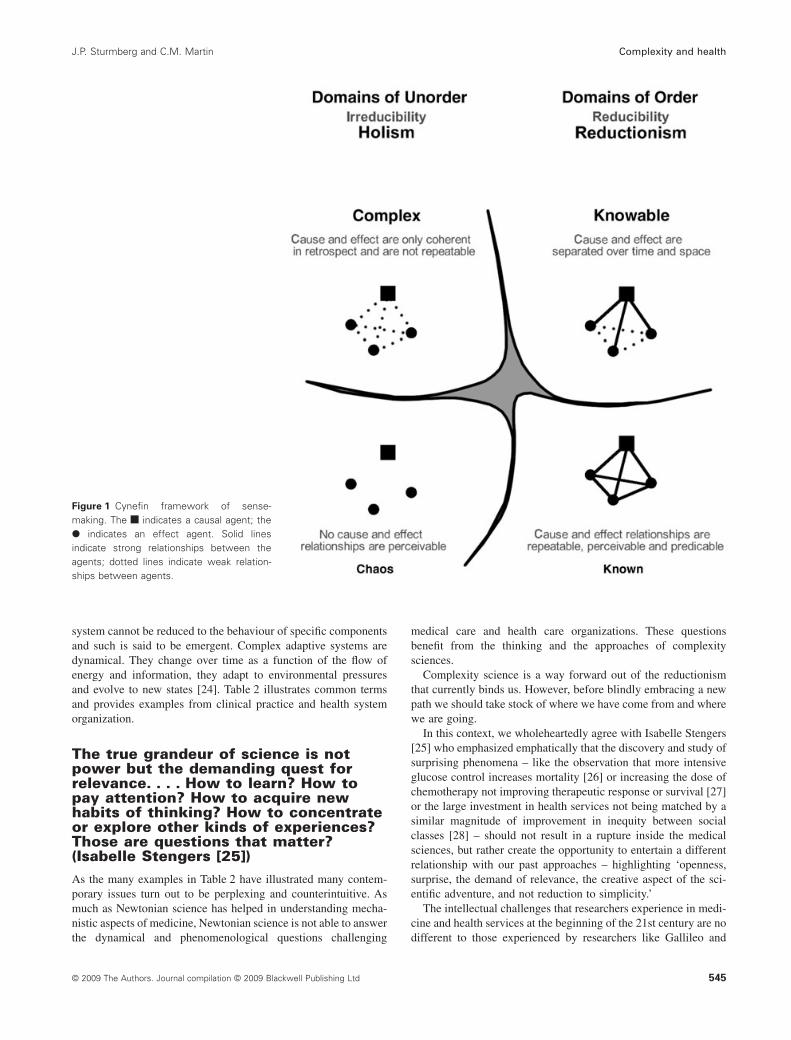
An essential concept of ‘understanding things’ arises from‘seeing things’ in the context resulting from a number of individualcomponents and their interactions. Kurtz and Snowden describedfour different states of relationships, three of the four we identifywith easily – the ‘known’, where cause and effect relations arerepeatable, perceivable and predictable; the ‘knowable’ wherecause and effect are separated over time and space and ‘chaos’where no cause and effect relationships are perceivable. The fourthstate of relationships is ‘complexity’ where cause and effect areonly coherent in retrospect and are not repeatable. We find thismore difficult to comprehend [22] (Fig 1). In part, this may relateto the psychology of certainty and uncertainty. As Dörner hasshown, when confronted with a complex problem we feel to not befully in control as it is exceedingly difficult to hold all the relevantinformation about the problem in mind and to foresee the conse-quences of a particular decision for the whole. He demonstratedthat this phenomenon is fairly universal and independent of subjectmatter knowledge or general level of education [23]. The insighthas emerged that complex problems can only be understood ‘afterthe event’, which can be infuriating particularly when we have torealize that we may have made the wrong judgements or decisions(Fig 1).
Complex systems have been described in detail by Paul Cilliersin his book Complexity and Postmodernism – UnderstandingComplex Systems [24]. Living and social systems, including indi-vidual animals and humans, ecologies, economies and socialinstitutions, are inherently complex. As much as each systemfunctions in a specific context, they also share a number of generalcharacteristics.
Complex systems consist of many different components thatinteract in non-linear ways. They are open to their environment, andinteractions occur at many different levels and influence each otherthrough recursive feedback loops. Complex systems are self-organizing; pattern and organization develop iteratively throughinteractions among the system’s components in the absence of anyexternal supervisory influence, as is seen, for example, in theflocking behaviour of birds. Some simple rules for self-organizationin human systems include shared values and principles, connectiv-ity and feedback, dialogue, memory and interdependency.
Importantly a complex system is not defined by its constituentcomponents but rather by its relationships or patterns of interac-tion. As a consequence the behaviour of a complex adaptive
Table 1 Complexity – can be understood as either or both
• a phenomenological sense of the ‘complex’ multifacetedunpredictable world we live in, which is behind the lay definitionand/or
• in the epistemological sense of complexity science and theories[32]
• Complexity Science and Complexity Theories represent aconvergence of different types of ideas and theories to address thenon-linearity and dynamics of the real world systems, often knownas complex adaptive systems [33].
Complexity and health J.P. Sturmberg and C.M. Martin
© 2009 The Authors. Journal compilation © 2009 Blackwell Publishing Ltd544
system cannot be reduced to the behaviour of specific componentsand such is said to be emergent. Complex adaptive systems aredynamical. They change over time as a function of the flow ofenergy and information, they adapt to environmental pressuresand evolve to new states [24]. Table 2 illustrates common termsand provides examples from clinical practice and health systemorganization.
The true grandeur of science is notpower but the demanding quest forrelevance. . . . How to learn? How topay attention? How to acquire newhabits of thinking? How to concentrateor explore other kinds of experiences?Those are questions that matter?(Isabelle Stengers [25])As the many examples in Table 2 have illustrated many contem-porary issues turn out to be perplexing and counterintuitive. Asmuch as Newtonian science has helped in understanding mecha-nistic aspects of medicine, Newtonian science is not able to answerthe dynamical and phenomenological questions challenging
medical care and health care organizations. These questionsbenefit from the thinking and the approaches of complexitysciences.
Complexity science is a way forward out of the reductionismthat currently binds us. However, before blindly embracing a newpath we should take stock of where we have come from and wherewe are going.
In this context, we wholeheartedly agree with Isabelle Stengers[25] who emphasized emphatically that the discovery and study ofsurprising phenomena – like the observation that more intensiveglucose control increases mortality [26] or increasing the dose ofchemotherapy not improving therapeutic response or survival [27]or the large investment in health services not being matched by asimilar magnitude of improvement in inequity between socialclasses [28] – should not result in a rupture inside the medicalsciences, but rather create the opportunity to entertain a differentrelationship with our past approaches – highlighting ‘openness,surprise, the demand of relevance, the creative aspect of the sci-entific adventure, and not reduction to simplicity.’
The intellectual challenges that researchers experience in medi-cine and health services at the beginning of the 21st century are nodifferent to those experienced by researchers like Gallileo and
Figure 1 Cynefin framework of sense-making. The indicates a causal agent; the� indicates an effect agent. Solid linesindicate strong relationships between theagents; dotted lines indicate weak relation-ships between agents.
J.P. Sturmberg and C.M. Martin Complexity and health
© 2009 The Authors. Journal compilation © 2009 Blackwell Publishing Ltd 545
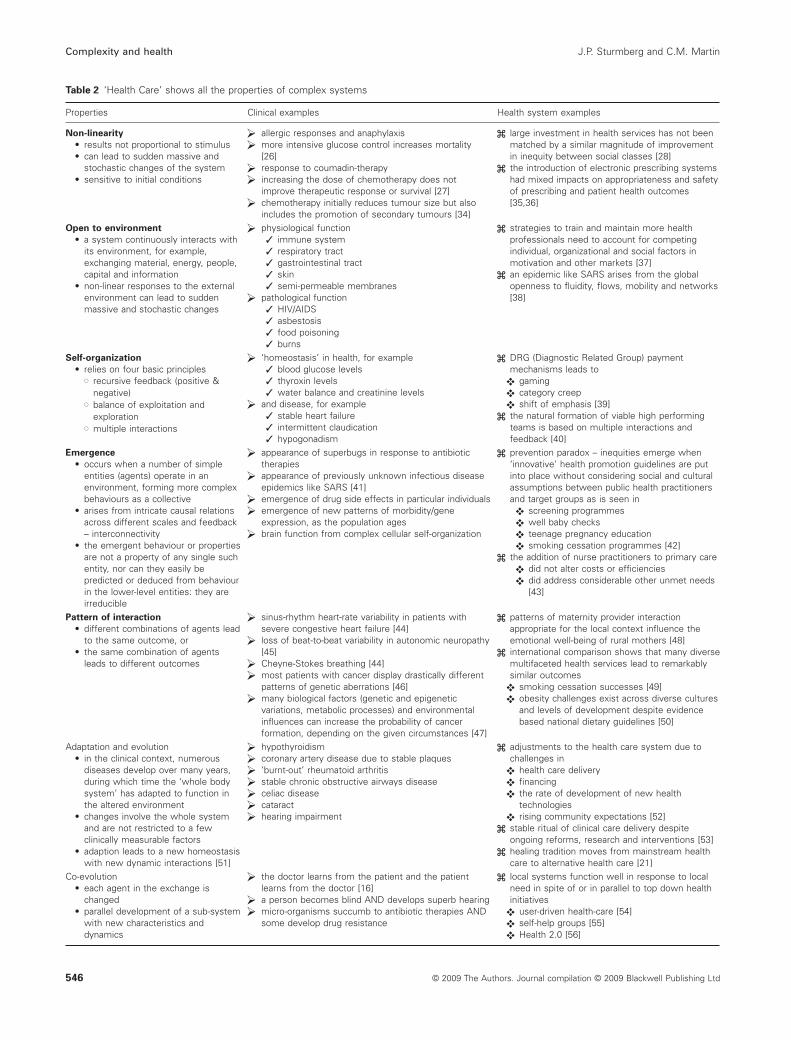
Table 2 ‘Health Care’ shows all the properties of complex systems
Properties Clinical examples Health system examples
Non-linearity
• results not proportional to stimulus• can lead to sudden massive and
stochastic changes of the system• sensitive to initial conditions
allergic responses and anaphylaxismore intensive glucose control increases mortality[26]response to coumadin-therapyincreasing the dose of chemotherapy does notimprove therapeutic response or survival [27]chemotherapy initially reduces tumour size but alsoincludes the promotion of secondary tumours [34]
large investment in health services has not beenmatched by a similar magnitude of improvementin inequity between social classes [28]the introduction of electronic prescribing systemshad mixed impacts on appropriateness and safetyof prescribing and patient health outcomes[35,36]
Open to environment
• a system continuously interacts withits environment, for example,exchanging material, energy, people,capital and information
• non-linear responses to the externalenvironment can lead to suddenmassive and stochastic changes
physiological function✓ immune system✓ respiratory tract✓ gastrointestinal tract✓ skin✓ semi-permeable membranes
pathological function✓ HIV/AIDS✓ asbestosis✓ food poisoning✓ burns
strategies to train and maintain more healthprofessionals need to account for competingindividual, organizational and social factors inmotivation and other markets [37]an epidemic like SARS arises from the globalopenness to fluidity, flows, mobility and networks[38]
Self-organization
• relies on four basic principles� recursive feedback (positive &
negative)� balance of exploitation and
exploration� multiple interactions
‘homeostasis’ in health, for example✓ blood glucose levels✓ thyroxin levels✓ water balance and creatinine levels
and disease, for example✓ stable heart failure✓ intermittent claudication✓ hypogonadism
DRG (Diagnostic Related Group) paymentmechanisms leads to
gamingcategory creepshift of emphasis [39]
the natural formation of viable high performingteams is based on multiple interactions andfeedback [40]
Emergence
• occurs when a number of simpleentities (agents) operate in anenvironment, forming more complexbehaviours as a collective
• arises from intricate causal relationsacross different scales and feedback– interconnectivity
• the emergent behaviour or propertiesare not a property of any single suchentity, nor can they easily bepredicted or deduced from behaviourin the lower-level entities: they areirreducible
appearance of superbugs in response to antibiotictherapiesappearance of previously unknown infectious diseaseepidemics like SARS [41]emergence of drug side effects in particular individualsemergence of new patterns of morbidity/geneexpression, as the population agesbrain function from complex cellular self-organization
prevention paradox – inequities emerge when‘innovative’ health promotion guidelines are putinto place without considering social and culturalassumptions between public health practitionersand target groups as is seen in
screening programmeswell baby checksteenage pregnancy educationsmoking cessation programmes [42]
the addition of nurse practitioners to primary caredid not alter costs or efficienciesdid address considerable other unmet needs[43]
Pattern of interaction
• different combinations of agents leadto the same outcome, or
• the same combination of agentsleads to different outcomes
sinus-rhythm heart-rate variability in patients withsevere congestive heart failure [44]loss of beat-to-beat variability in autonomic neuropathy[45]Cheyne-Stokes breathing [44]most patients with cancer display drastically differentpatterns of genetic aberrations [46]many biological factors (genetic and epigeneticvariations, metabolic processes) and environmentalinfluences can increase the probability of cancerformation, depending on the given circumstances [47]
patterns of maternity provider interactionappropriate for the local context influence theemotional well-being of rural mothers [48]international comparison shows that many diversemultifaceted health services lead to remarkablysimilar outcomes
smoking cessation successes [49]obesity challenges exist across diverse culturesand levels of development despite evidencebased national dietary guidelines [50]
Adaptation and evolution• in the clinical context, numerous
diseases develop over many years,during which time the ‘whole bodysystem’ has adapted to function inthe altered environment
• changes involve the whole systemand are not restricted to a fewclinically measurable factors
• adaption leads to a new homeostasiswith new dynamic interactions [51]
hypothyroidismcoronary artery disease due to stable plaques‘burnt-out’ rheumatoid arthritisstable chronic obstructive airways diseaseceliac diseasecataracthearing impairment
adjustments to the health care system due tochallenges in
health care deliveryfinancingthe rate of development of new healthtechnologiesrising community expectations [52]
stable ritual of clinical care delivery despiteongoing reforms, research and interventions [53]healing tradition moves from mainstream healthcare to alternative health care [21]
Co-evolution• each agent in the exchange is
changed• parallel development of a sub-system
with new characteristics anddynamics
the doctor learns from the patient and the patientlearns from the doctor [16]a person becomes blind AND develops superb hearingmicro-organisms succumb to antibiotic therapies ANDsome develop drug resistance
local systems function well in response to localneed in spite of or in parallel to top down healthinitiatives
user-driven health-care [54]self-help groups [55]Health 2.0 [56]
Complexity and health J.P. Sturmberg and C.M. Martin
© 2009 The Authors. Journal compilation © 2009 Blackwell Publishing Ltd546

Newton, Heisenberg, Currie and Einstein, and Weiner and Prigog-ine when trying to address the pressing new questions arising fromthe inconsistencies observed in their respected fields.
The crisis in health care is probably better understood as theinstability in the health care system. This provides an opportu-nity to study and understand the historical patterns and interac-tions of the current system and to apply that knowledge togetherwith the workings of complex adaptive systems in order toexplore meaningful ways forward for those we serve, as clini-cians, health service planners, researchers into pathologies andteachers.
To succeed in this endeavour, we need to explore how complex-ity approaches can provide different solutions to the problems inhealth care than the prevailing Newtonian ones. To this end, thenew Forum on Systems and Complexity in Medicine and Health-care provides a place for scientific debate and promulgation ofresearch findings. It also offers a means to engage with those whostruggle at the margins of the current system and who are lookingfor new ideas.
The interactions in complex adaptive systems occur within theirhistorical constraints that live on into the future. In terms of thehealth care system, our patients’ elementary needs for care andunderstanding have not changed. We may have a better under-standing of the tissue reactions that are associated with clinicallydefined disease entities; still, each disease entity occurs in a uniqueindividual who experiences it in her unique personal way in herunique social context [2,14,29–31].
References1. Feinstein, A. R. (1999) Statistical reductionism and clinicians’ delin-
quencies in humanistic research. Clinical Pharmacology and Thera-peutics, 66 (3), 211–217.
2. Sturmberg, J. P. & with a contribution by Martin, C. M. (2007) TheFoundations of Primary Care. Daring to be Different. Oxford, SanFrancisco, CA: Radcliffe Medical Press.
3. May, W. (1983) The Physician’s Covenant: Images of the Healer inMedical Ethics. Philadelphia, PA: The Westminster Press.
4. Rosenberg, C. E. (1989) Disease in history: frames and framers. TheMilbank Quarterly, 67 (Supp. l), 1–15.
5. McCormick, J. (1993) The contribution of science to medicine. Per-spectives in Biology and Medicine, 36 (3), 315–322.
6. Polanyi, M. (1958) Personal Knowledge. Towards a Post-Critical Phi-losophy. London: Routledge.
7. Upshur, R. E. G. (2002) If not evidence, then what? Or does medicinereally need a base? Journal of Evaluation in Clinical Practice, 8 (2),113–119.
8. Rawlins, M. (2008) De testimonio: on the evidence for decisions aboutthe use of therapeutic interventions. Lancet, 372 (9656), 2152–2161.
9. Feinstein, A. R. (2002) Will clinicians’ challenges be solved byanother theoretical model? Commentary. Journal of Evaluation inClinical Practice, 8 (2), 139–141.
10. Engel, G. L. (1977) The need for a new medical model: a challenge forbiomedicine. Science, 196, 129–136.
11. Borrell-Carrió, F., Suchman, A. & Epstein, R. (2004) The biopsycho-social model 25 years later: principles, practice, and scientific inquiry.Annals of Family Medicine, 2 (6), 576–582.
12. Bean, B. W. (1961) Sir William Osler Aphorisms. Springfield, IL:Charles C Thomas.
13. McWhinney, I. R. (1989) A Textbook of Family Medicine. New York,Oxford: Oxford University Press.
14. Stewart, M., Brown, J. B., Weston, W. W., McWhinney, I. R., Mc-William, C. L. & Freeman, T. H. (1995) Patient-Centered Medicine.London: Sage Publications.
15. McWhinney, I. R. (1996) The importance of being different. WilliamPickles Lecture 1996. The British Journal of General Practice, 46 (7),433–436.
16. Suchman, A. L. (2006) A new theoretical foundation for relationship-centered care. Complex responsive processes of relating. Journal ofGeneral Internal Medicine, 21 (Suppl. 1), S40–S44.
17. Loughlin, M. (2006) The future for medical epistemology? Commen-tary on Tonelli (2006) Integrating evidence into clinical practice: analternative to evidence-based approaches. Journal of Evaluation inClinical Practice, 12 (3), 289–291.
18. Sturmberg, J. P. & Martin, C. M. (2008) Knowing – in medicine.Journal of Evaluation in Clinical Practice, 14 (5), 767–770.
19. Lakoff, G. & Johnsen, M. (2003) Metaphors We Live by. London: TheUniversity of Chicago Press.
20. Kolbe, R. J. (1996) The crisis in medicine – a response. South AfricanMedical Journal, 86 (3), 231–235.
21. Snyderman, R. & Weil, A. T. (2002) Integrative medicine: bringingmedicine back to its roots. Archives of Internal Medicine, 162 (4),395–397.
22. Kurtz, C. F. & Snowden, D. J. (2003) The new dynamics of strategy:sense-making in a complex and complicated world. IBM SystemsJournal, 42 (3), 462–483.
23. Dörner, D. (1996) The Logic of Failure: Recognizing and AvoidingError in Complex Situations. New York: Metropolitan Books.
24. Cilliers, P. (1998) Complexity and Postmodernism. UnderstandingComplex Systems. London: Routledge.
25. Stengers, I. (2004) The challenge of complexity: unfolding the ethicsof science. In Memoriam Ilya Prigogine. Emergency: Complexity &Organization, 6 (1–2), 92–99.
26. The Action to Control Cardiovascular Risk in Diabetes Study Group(2008) Effects of intensive glucose lowering in type 2 diabetes. TheNew England Journal of Medicine, 358 (24), 2545–2559.
27. Leyvraz, S., Pampallona, S., Martinelli, G., et al. (2008) A threefolddose intensity treatment with ifosfamide, carboplatin, and etoposidefor patients with small cell lung cancer: a randomized trial. Journal ofthe National Cancer Institute, 100 (8), 533–541.
28. Blas, E., Gilson, L., Kelly, M. P., et al. (2008) Addressing socialdeterminants of health inequities: what can the state and civil societydo? Lancet, 372 (9650), 1684–1689.
29. Balint, M. (1957) The Doctor, His Patient and the Illness. Edinburgh,London, Melbourne and New York: Churchill Livingstone.
30. Greenhalgh, T. (2006) What Seems to be the Trouble? Oxford, SanFrancisco, CA: Radcliffe Medical Press.
31. Fugelli, P. (2008) The healing dance. Why society and medicineneed the general practitioner. Available from: http://www.racgp.org.au/Content/NavigationMenu/News/Conferencesandevents/asc20071/Abstracts07/Specialpresentations/ASC07Fugelli.pdf (accessed 23April 2009).
32. Martin, C. M. & Kaufman, T. (2007) Addressing unfinished businessin primary health care (PHC). A shared framework across Canadais needed to implement PAHO/WHO ‘new orientations’ for adap-tive PHC-based health systems. Ottawa: A Commissioned Reportfor the Canadian Alliance of Community Health Centre Associa-tions; Primary Health Care Transition Fund (PHCTF) NationalEvaluation.
33. Leykum, L. K., Pugh, J., Lawrence, V., Parchman, M., Noël, P. H.,Cornell, J. & Mcdaniel, R. R. J. (2007) Organizational interventionsemploying principles of complexity science have improved outcomesfor patients with type II diabetes. Implementation Science, 2 (1), 28.
34. Mittra, I. (2007) The disconnection between tumor response and sur-vival. Nature Clinical Practice. Oncology, 4 (4), 203.
J.P. Sturmberg and C.M. Martin Complexity and health
© 2009 The Authors. Journal compilation © 2009 Blackwell Publishing Ltd 547

35. Hider, P. (2002) Electronic prescribing: a critical appraisal ofthe literature. New Zealand Health Technology Assessment, 5 (2).http://nzhta.chmeds.ac.nz/publications/elpresc.pdf (accessed 23 April2009).
36. Ammenwerth, E., Schnell-Inderst, P., Machan, C. & Siebert, U. (2008)The effect of electronic prescribing on medication errors and adversedrug events: a systematic review. Journal of the American MedicalInformatics Association, 15 (5), 585–600.
37. Zurn, P., Dolea, C. & Stilwell, B. (2005) Nurse Retention andRecruitment: Developing a Motivated Workforce. Geneva: WorldHealth Organization, Department of Human Resources for Health.http://www.icn.ch/global/Issue4Retention.pdf (accessed 23 April2009).
38. Ali, S. (2008) Infectious disease, global cities and complexity. Paperpresented at the Annual Meeting of the American Sociological Asso-ciation Annual Meeting, Sheraton Boston and the Boston MarriottCopley Place, Boston, MA, July 31, 2008. http://www.allacademic.com/meta/p_mla_apa_research_citation/2/3/7/3/0/p237304_index.html (accessed 23 April 2009).
39. Kuhn, M. & Siciliani, L. (2008) Upcoding and Optimal Auditing inHealth Care (or the Economics of DRG Creep). SSRN.
40. Grumbach, K. & Bodenheimer, T. (2004) Can health care teamsimprove primary care practice? Journal of the American MedicalAssociation, 291 (10), 1246–1251.
41. Smith, R. D. (2006) Responding to global infectious disease out-breaks: Lessons from SARS on the role of risk perception, communi-cation and management. Social Science & Medicine, 63 (12), 3113–3123.
42. Frohlich, K. L. & Potvin, L. (2008) Transcending the known in publichealth practice: the inequality paradox: the population approach andvulnerable populations. American Journal of Public Health, 98 (2),216–221.
43. Laurant, M., Reeves, D., Hermens, R., Braspenning, J., Grol, R. &Sibbald, B. (2005) Substitution of doctors by nurses in primary care.Cochrane Database of Systematic Reviews, 18 (2), CD001271.
44. Goldberger, A. (1996) Non-linear dynamics for clinicians: chaostheory, fractals, and complexity at the bedside. Lancet, 347, 1312–1314.
45. Stella, P., Ellis, D., Maser, R. E. & Orchard, T. J. (2000) Cardiovas-cular autonomic neuropathy (expiration and inspiration ratio) in type 1diabetes. Incidence and predictors. Journal of Diabetes and Its Com-plications, 14 (1), 1–6.
46. Wood, L. D., Parsons, D. W., Jones, S., et al. (2007) The genomiclandscapes of human breast and colorectal cancers. Science, 318(5853), 1108–1113.
47. Henry, H. Q. H. (2007) Cancer genome sequencing: the challengesahead. Bioessays, 29 (8), 783–794.
48. Sutherns, R. (2004) Adding women’s voices to the call for sustainablerural maternity care. Canadian Journal of Rural Medicine, 9 (4),239–244.
49. US Public Health Service. (2000) Treating Tobacco Use and Depen-dence – A Systems Approach. A Guide for Health Care Administrators,Insurers, Managed Care Organizations, and Purchasers. WashingtonDC: US Public Health Service. http://www.uams.edu/coph/reports/SmokeFree_Toolkit/Media/Objective%206%20Supporting%20Ongoing%20Implementation/Systems%20for%20Treating%20Tobacco%20Use%20and%20Dependence.pdf (accessed 23 April2009).
50. Nishida, C., Uauy, R., Kumanyika, S. & Shetty, P. (2004) The jointwho/fao expert consultation on diet, nutrition and the prevention ofchronic diseases: process, product and policy implications. PublicHealth Nutrition, 007 (01A), 245–250.
51. Heng, H. H. Q. (2008) The conflict between complex systems andreductionism. Journal of the American Medical Association, 300 (13),1580–1581.
52. House of Representatives Standing Committee on Health and Ageing(2006) The blame game. Report on the inquiry into health funding.Canberra: Commonwealth of Australia.
53. Plamping, D. (1998) Looking forward: change and resistance tochange in the NHS. British Medical Journal, 317 (7150), 69–71.
54. Biswas, R., Martin, C. M., Sturmberg, J. S., Mukherji, K. J., Lee, E. W.H., Umakanth, S. & Kasthuri, A. S. (2009) Social cognitive ontologyand user driven health care. In Handbook of Research on SocialSoftware and Developing Community Ontologies (eds S. Hatzipana-gos & S. Warburton), pp. 68–89. London: IGI Global.
55. Martin, C. M., Peterson, C., Robinson, R. & Sturmberg, J. P. (2009)Care for chronic illness in australian general practice – focus groups ofchronic disease self-help groups over 10 years. Implications forchronic care systems reforms. Asia Pacific Journal of Family Medi-cine, 8 (1), 1.
56. Eysenbach, G. (2008) Medicine 2.0: Social networking, collaboration,participation, apomediation, and openness. Journal of Medical Inter-net Research, 10 (3), e22. Available at: http://www.jmir.org/2008/3/e22/ (accessed 23 April 2009).
Complexity and health J.P. Sturmberg and C.M. Martin
© 2009 The Authors. Journal compilation © 2009 Blackwell Publishing Ltd548





























