Embed Size (px)
Citation preview

Reg Num: 115554 Gluteal Activation Warm Up 1
Gluteal Activation Warm Up Increases Subsequent Ground Reaction Force, Gluteal, Bilateral
Hamstring and Quadriceps Force Whilst Simultaneously reducing Gluteus Medius
Recruitment During the Hang High Pull in Elite Male Rugby Union Players.
Matthew Thomas Parr
Dr Daniel Cleather
June 2015
St Mary’s University, Twickenham, London.
School of Human Sciences
MSc Strength & Conditioning

Reg Num: 115554 Gluteal Activation Warm Up 2
Acknowledgments
Thank you to my wife Jemima and my children Maisie and Freya for sacrificing their time
with me in order for me to complete this research, further thanks must go to my supervisor Dr
Daniel Cleather and Phil Price for their insight and patience.

Reg Num: 115554 Gluteal Activation Warm Up 3
Abstract
Gluteal Activation Warm Up Increases Subsequent Ground Reaction Force, Gluteal, Bilateral
Hamstring and Quadriceps Force Whilst Simultaneously Reducing Gluteus Medius
Recruitment During the Hang High Pull in Elite Male Rugby Union Players.
The gluteal muscles play a material role in athletic performance and injury prevention thus
the purpose of this research was to identify the effect of a gluteal activation warm up on
gluteal motor unit (MU) recruitment and force output within the hang high pull (HHP),
endeavouring to increase athletic performance and reduce injury risk. Seventeen elite male
rugby union players undertook two separate warm ups, control and activation, prior to
executing three HHP. Electromyography (EMG) was employed to measure gluteus maximus
(GMAX) and gluteus medius (GMED) recruitment levels. The FreeBody Beta
musculoskeletal model (FBB) was used to measure the force output of the bilateral
hamstring, GMAX, GMED and quadriceps with a force plate measuring ground reaction
force (GRF). EMG results showed a statistically significant (p < 0.048) decrease in GMED
recruitment following the activation warm up with FBB data showing a strong trend of
increased force output following the activation warm up. This research concludes that the
implementation of a gluteal activation warm up may increase athletic performance and reduce
injury risk due to the increased gluteal and lower limb force output despite decreased GMED
motor unit recruitment.
Keywords: Isometric Contraction, Nervous System, Force, Preferential Recruitment

Reg Num: 115554 Gluteal Activation Warm Up 4
Table of Contents
Abstract p.3
Chapter One: Introduction
1.1 Introduction p.8
Chapter Two: Literature Review
2.1 Importance of the gluteal musculature within sports performance p.9
2.2 Importance of Gluteal Musculature in Injury Prevention p.11
2.3 Activation research p.12
2.4 Gluteal activation research p.14
2.5 Musculoskeletal modelling review p.16
2.6 Summary p.17
Chapter Three: Method
3.1 Introduction p.18
3.2 Research strategy p.19
3.3 Data Collection p.24
Chapter Four: Results

Reg Num: 115554 Gluteal Activation Warm Up 5
4.1 Results p.26
Chapter 5: Discussion
5.1 Introduction p.30
5.2 Research Objectives p.31
5.3 Recommendations and practical applications p.40
5.4 Contribution to knowledge p.41
5.5 Self Reflection p.41
Chapter 6
References p.42
Appendix p.66

Reg Num: 115554 Gluteal Activation Warm Up 6
List of Figures
Figure 1. Most effective GMAX and GMED recruitment exercises p.15
Figure 2. Research structure info graphic p.20
Figure 3. Control trial non-specific warm up. p.22
Figure 4. Intervention trial GMAX and GMED specific warm up. p.23
Figure 5. Peak motor unit recruitment rate in control and intervention trials p.29

Reg Num: 115554 Gluteal Activation Warm Up 7
List of Tables
Table 1. Cohort Anthropometrics Data Table p.19
Table 2. EMG Pilot Data in μν as a Percentage of MVIC p.26
Table 3. Group Mean Peak Recruitment as MVIC Percentage and p.27
Multiples of Body Mass
Table 4. FBB GMED, GMAX and GRF RFD as xBW/ms and EMGGMED p.28
and GMAX RFD as MVIC% μv/ms

Reg Num: 115554 Gluteal Activation Warm Up 8
Chapter One
2. Introduction
1.1 Introduction
Warm up protocols frequently endeavour to enhance force output (De Villarreal, Gonzalez-
Badillo & Izquierdo, 2007) especially as explosive movements are a key characteristic of
elite performance (Izquierdo, Hakkinen, Gonzalez-Badillo, Ibanez & Gorostiaga, 2002).
Activation warm ups are one such method, potential increases are believed to result from
increased axon potential discharge rate enabling a high coding rate to recruit high threshold
motor units (HTMU) (Aagaard et al., 2007) in turn producing powerful movements.
Increasing the coding rate and preferential recruitment of HTMU within musculature material
to athletic performance such as the gluteal musculature appears vital to increasing
performance and as such will be investigated. Within this research the gluteus maximus
(GMAX) and gluteus medius (GMED) will be targeted, as hip extension force has been cited
as a material factor in sporting performance (Nagano, Komura, Fukashiro & Himeno, 2005:
Newton & Kraemer, 1994: Mero & Komi, 1994), thus developing methods of increasing
sporting performance via increased gluteal force offers a rationale for the undertaking of this
research.
Considering the importance of HTMU activation and the impact of the gluteal musculature
on sporting performance, further research on the optimisation of these factors appears prudent
as the effects of gluteal activation warm ups on peak force output are currently unclear
(Buttifant, Crow, Kearney & Hrysomallis, 2011). Therefore further investigation of this
subject is required to provide an insight as to the efficacy of gluteal activation warm ups on

Reg Num: 115554 Gluteal Activation Warm Up 9
subsequent recruitment and force output. Within this literature review a rationale will be
given for the need of this research to investigate the effect of GMAX and GMED activation
warm up on recruitment and force output.
Chapter Two
2.1 Importance of Gluteal Musculature in Sporting Performance
Increased acceleration (Murphy, Lockie & Coutts, 2003: Kyrolainen, Avela & Komi, 2005:
Reilly & Borrie, 1992: Reilly, 1997), maximum velocity running (MVR) (Kyrolainen et al.,
2005: Meir, Colla & Milligan, 2001: Deutsch, Maw, Jenkins & Reaburn, 1998), change of
direction (CoD) (Young & Farrow, 2006: Holmberg, 2009) and jump performance have been
proposed as key sports performance indicators (KPI) (Izquierdo et al., 2002: Hoffman,
Cooper, Wendell & Kanf, 2004: Murphy et al., 2003: Penfold & Jenkins, 1996). All of these
are actions with high GMAX and GMED involvement (Nagano et al. 2005: Newton &
Kraemer, 1994: Mero & Komi, 1994), therefore it could be extrapolated that identifying
methods of improving GMAX and GMED recruitment and force output, such as activation
warm ups, may in turn increase performance and thus merits investigation. As previously
stated the GMAX and GMED play a material role in MVR (Kyrolainen et al., 2005: Meir et
al. 2001: Deutsch, 1998) and acceleration (Reily, 1996: Rienzi et al., 2000: Meir et al., 2001);
with the GMED stabilising the pelvis and femur (Gottschalck, Kourush & Leveau, 1989) and
abducts the hip (Boudreau et al., 2009), whilst the GMAX extends the hip, abducts and
external rotates the femur (Souza & Powers, 2009. Understanding the biomechanical
functions of GMAX and GMED is vital to performance enhancement as it enables greater
specificity of gluteal activation exercise selection.
Reg Num: 115554 Gluteal Activation Warm Up 10
Analysis of hip extension during running highlights that hip extension force correlates with
high stride frequency, with Schroter (1998) and Brown, Ferrigno and Santana (2000)
suggesting high stride frequency as vital during the crucial initial accelerative steps (Penfold
& Jenkins, 1996). Murphy et al. (2003) explored kinematic deviations between fast and slow
accelerators. Faster accelerators displayed a 9% greater stride frequency potentially due to
greater horizontal hip velocity, with Guskiewicz, Lephart and Burkholder (1993) proposing a
similar correlation between superior sprint performance and hip extensor power. Hip
extension torque produced by GMAX affects thigh velocity, with increased GMAX force
production increasing hip extension velocity thus reducing the thigh swing to stance duration
(Lieberman, 2006: Blazevich, 2000) enabling increased stride frequency and in turn running
velocity, thus investigation of the methods of enhancing hip extension force such as a gluteal
activation warm up appears valid. Similarly ground reaction force (GRF) is influenced by
hip extension force, Weyand, Sternlight, Bellizzi and Wright (2000) established that faster
runners apply greater GRF, GRF is the product of lower limb triple extension force, initiated
proximally by GMAX hip extension, thus GMAX contractile force greatly influences GRF
and thus running speed (Weyand et al., 2000), with Mann (1986) finding acceleration
velocity also related to horizontal force production of the hip extensors during ground
contact. This highlights the vital role GMAX plays in hip extension; increasing stride
frequency and in turn GRF resulting in increased running velocity, due to this association
identifying methods of optimally strengthening the GMAX such as a gluteal activation warm
up may facilitate improved running velocity within the sporting environment.
In addition to increased limb velocity and vertical GRF production, GMAX and GMED play
a vital role in femur and pelvic stability (Cutter & Kervorkain, 1999: Earle, 2005), as
insufficient GMAX strength reduces the hip’s ability to resist flexion (Lieberman et al., 2006)

Reg Num: 115554 Gluteal Activation Warm Up 11
with insufficient GMED strength reducing pelvic stability during stance (Gottschalck, 1989:
Lieberman et al., 2006) causing Trendelenburg hip drop and force leakage (Cutteret &
Kervorkain, 1999: Earle, 2005), consequently reducing ground contact force, reducing
vertical GRF thus decreased running velocity (Blazevich, 2000). Thus further highlighting
the importance of elevated GMAX and GMED force and recruitment on running velocity,
ergo by improving GMED force via increased recruitment in compound movements such as
the HHP may enable greater pelvic stability resulting in increased acceleration and MVR,
therefore providing further rationale for the investigation of the effect of a gluteal activation
warm up on GMAX and GMED force in the pursuit of increased athletic performance.
The GMAX and GMED function similarly within CoD (Neumann, 2010: Neptune, Wright &
Van Der Bogert, 1999) as within MVR and acceleration, with Neptune et al. (1999) finding
that the GMED displayed a constant EMG output during cutting movements and side
shuffling, highlighting GMED’s role in isometrically stabilizing the pelvis proximally,
creating a foundation for GMAX to produce and transfer force during CoD (Oliver & Keeley,
2010). The GMAX and GMED functional similarly in the counter movement jump (CMJ)
with Nagano et al. (2005) finding the GMAX to be maximally activated during take-off,
highlighting the differing functions of the gluteal muscles with GMAX as a force producer
and the GMED acting as a stabiliser (Bobbert & Van Ingen Schenau, 1988). The functions of
the GMAX and GMED in crucial performance measures discussed above provide a mandate
for this research in identifying methods of increasing gluteal force output to enable increased
sporting performance.
Reg Num: 115554 Gluteal Activation Warm Up 12
2.2 Importance of Gluteal Musculature in Injury Prevention
Further to the role of the GMAX and GMED in performance, decreased GMED strength has
been cited to increase Anterior Cruciate Ligament (ACL) injury risk (McLean et al., 2005:
Earle 2005), ACL injuries often occur during deceleration, landing and CoD (Powell &
Barber-Foss, 2000: Griffin et al. 2000: Griffin et al. 2006: Ireland, 1999: Olsen, Myklebust,
Engerbertsen & Bahr, 2004: Boden, Dean, Feagin & Garrett, 2000), due to decreased GMED
strength reducing frontal and transverse plane pelvic stability during gate and increasing hip
external rotation during cutting movements (Schmitz Riemann & Thompson, 2002: Earle,
2005: Heller, 2003: McLean, Huang & Van Den Bogert, 2004), insufficient GMED and hip
abductor strength creates a lack of frontal plane pelvic stability leading to Trendelenburg sign
(Cutter & KerVorkain, 1999: Earle, 2005). The Trendelenburg sign occurs when insufficient
GMED strength causes the GRF vector to shift laterally (Neumann, 2010) resulting in
increased knee valgus angle (Powers, 2010), increased knee valgus angle causes the
tibiofemoral joint stress within the frontal plane contributing to the relative ACL strain
(Withrow, Huston, Wojtys & Ashton Miller, 2006). Therefore considering these findings it
could be hypothesised that increasing GMED force via a gluteal activation warm up may
reduce the risk of increased knee valgus angle and in turn the risk of ACL injury. Therefore
investigation into methods of strengthening the GMED therapeutically such as within
activation warm ups, or via heavy resistance training which has been shown to produce high
levels of neuromuscular activation (Escamilla et al., 1998) and neural drive (Aagaard et al.,
2002: Hakkinen, Alen & Komi, 1985: Higbie, Cureton, Warren & Prior, 1996), appears a
valid rationale for the completion of this research.

Reg Num: 115554 Gluteal Activation Warm Up 13
Heavy resistance training has been shown as a stimulus which periodically will increase
hypertrophy (Aagaard et al., 2001: Andersen et al., 2005: Narici et al., 1996) and strength
gain (Aagaard et al., 2000: Andersen et al., 2005: Hakkinen & Komi, 1985). As GMED
strength has been associated with knee valgus angle and in turn ACL injury, increasing the
level of GMED neuromuscular stimuli within an a commonly used athletic training exercise
like the HHP, enabling increased cross sectional area and in turn strength via the use of a
therapeutic gluteal activation warm up appears advantageous.
2.3 Activation Research
Muscle activation describes the recruitment of individual motor units, governed by motor
neuron coding rate and the Henneman size principle (Zatsiorsky & Prilutsky, 2012), powerful
movements require a high coding rate recruiting high HTMU (Cormie, McGuigan & Newton,
2011), therefore establishing methods of innervating HTMU and increasing coding rate prior
to the requirement for powerful movement may facilitate decreased motor unit innervation
lag-time and accelerate recruitment of HTMU (Tsao & Hodges, 2008), subsequently
improving task performance. Within a therapeutic setting repeated activation of muscles with
delayed innervation patterns has been utilised to treat musculoskeletal dysfunctions
(Richardson, Jull, Hodges & Hides, 1999); the mechanism responsible for increasing the
excitation of the innervation afferent is believed to be plastic changes in the nervous system
modifying automatic muscle functions during tasks (Tsao & Hodges, 2008) and increased
efferent neural drive (Aagaard et al., 2002). Tsao & Hodges (2007) found that one session of
low intensity voluntary transverse abdominus (TA) activation training enabled the earlier
onset of TA EMG activity during subsequent trunk and upper limb movement, evidencing the
acceleration of feedforward motor patterns and the plasticity of automatic postural control

Reg Num: 115554 Gluteal Activation Warm Up 14
(Tsao & Hodges, 2008) in low velocity actions. Despite these findings in low velocity
movement, it is unclear if such mechanisms will result in increased force output within
explosive movements; the effect of low-level gluteal activation exercise on power output was
investigated by Crow, Buttifant, Kearny and Hrysomallis (2012), who discovered a 4.2%
increase in CMJ height after a therapeutic gluteal activation warm up in elite AFL players,
increases are believed to occur via increased efferent neural drive, preferential recruitment of
HTMU, affrent excitability and increased v-wave response (Aagaard et al., 2002: Milner-
Brown, Stein & Yemm, 1973) mechanisms described by Tsao and Hodges (2007). However
Crow et al (2012) reported no data suggesting the underlying mechanism for this increase;
CMJ height increased following a gluteal activation warm up but it is still unclear if increased
gluteal force production caused said increase. Therefore this window in the literature
provides a rationale for the use of EMG and MM to analyse the effects of a gluteal activation
warm up on GMAX and GMED recruitment and force output specifically, potentially
enabling a mechanical rationale for the cause and effect of any increase CMJ or force.
Minimal findings support the efficacy of low-level activation exercise at increasing the power
output of subsequent dynamic exercise (Crow et al. 2012) as such the effects of activation
exercise remain ambiguous, consequently the primary objective of this research is to establish
the effect of low-level therapeutic gluteal activation exercise on GMAX and GMED
recruitment and force output in the HHP.
2.4 Gluteal Activation Research
A number of studies (Ekstrom, Donatelli & Carp, 2007: DiStefano et al., 2009: Boren et al.,
2011) and literature reviews (Reiman, Bolgla & Loudon, 2012) have investigated the effect
of therapeutic GMAX and GMED exercise on motor unit recruitment, the research of

Reg Num: 115554 Gluteal Activation Warm Up 15
Ekstrom et al. (2007), DiStefano et al. (2009), Ayotte et al. (2007) and Bolgla (2005) and the
review of Reiman et al. (2012) highlighted the four exercises with the highest GMAX
activation MVIC% were compound exercises activating a large number of lower limb
muscles (Figure 1). Similarly these GMED exercises showed that the second and third
greatest activating exercises were also compound movements, however the highest GMED
activating exercise was the side bridge to neutral, a more isolated exercise exhibiting lateral
hip extension and thus qualifying for consideration of use within this research. Due to the
compound nature of the top ranked exercises evaluating the efficacy of the exercises based
solely on MVIC % may be ill-considered; as there is insufficient isolation of the GMAX and
GMED, which may potentially activate additional lower limb muscles therefore the
requirement for further review of activation literature is appropriate.
The following figure is adapted from the review of Riemann et al (2012)
Figure 1. Most effective GMAX and GMED recruitment exercises
0
10
20
30
40
50
60
70
80
Forward step up SL Deadlift SL Squat Wall Squat Side Bridge toNeutral
MV
IC %
Exercise
4 Most Effective GMAX & GMED EXERCISES (Reiman et al (2012)
GMAX
GMED

Reg Num: 115554 Gluteal Activation Warm Up 16
To this end Boren et al (2011) conducted cross comparisons research of the highest-ranking
gluteal musculature activation exercise from the work of DiStefano et al. (2009), Ayotte et al.
(2007) and Bolgla (2005), enabling improved testing protocol and cohort standardisation.
Standardising protocols and cohort offered a uniformity thus increasing validity, providing an
accurate comparison of targeted GMAX and GMED activation and their efficacy of
recruitment. Boren et al. (2011) found the side plank with hip abduction to be the most
effective GMED recruitment exercise with a 103% MVIC% and the Front plank with
unilateral hip extension as the most effective for GMAX recruitment at 106% MVIC
respectively, both are exercises with limited impact on the global musculature (…) and are
therefore appropriate for use within this research which endeavours to specifically target the
gluteal musculature. However when MVIC % exceeds 100% further scrutiny of the testing
protocol is required, Boren et al. (2011) offered two reasons for this; a lack of motivation and
an issue within the testing causing subjects the inability to exert maximal contraction. The
issue of incorrect electrode placement and ‘noise’ must also be examined; although it appears
the testing protocols appear in accordance with the other literature.
The side plank with hip abduction corresponds biomechanically with the function of the
GMED, GMED stabilises the pelvis and femur (Gottschalck et al., 1989), abducts the hip and
has elevated recruitment when combined with a minimal base of support (Boudreau et al.,
2009), and thus the relationship between anatomy, function and recruitment are apparent.
This relationship is also true of the actions of the GMAX within the front plank with
unilateral hip extension, GMAX is responsible for hip extension, abduction and femoral
external rotation (Souza & Powers, 2009), thus the biomechanics of these plank variation

Reg Num: 115554 Gluteal Activation Warm Up 17
correlates closely with the functions of the gluteal muscles during locomotion. Boren et al.
(2011) suggests that the increased MVIC % could be due to the high levels of trunk
musculature co-contraction resulting from the limited base of support, requiring the hip
musculature to contract to a greater extent to compensate for this increased demand.
The most appropriate GMAX and GMED exercises arising from this literature for the GMAX
and GMED activation warm up are; the side plank with hip abduction for the GMED
activation and the front plank with unilateral hip extension for the GMAX, these exercises
whilst being effective as GMAX and GMED activation exercises have the advantage of
having minimal impact upon the remaining lower limb musculature an important
consideration of this research, isolating the gluteal muscles provides a more accurate analysis
of the effect of gluteal activation upon recruitment and force output.
2.5 Musculoskeletal Modelling Research
MM is a growing field of research, particularly within medicine, much of this research
focuses on everyday activities such as sitting and standing exercises, activities performed at
slow velocities and as such differ from the high velocities of elite sporting actions, MM
provides a method of non-invasive measurement of muscular forces and as such is fitting for
this research as the evaluation of muscular forces within an elite population requires accurate
but non-invasive procedures. Considering this difference, the findings of the clinical MM
research has limited application within an elite performance population (Cleather, Goodwin
& Bull, 2013), however a small body of research has explored movements such as the squat
and push jerk (Cleather & Bull 2010). Considering the critical differences between clinical

Reg Num: 115554 Gluteal Activation Warm Up 18
and sports science research within MM the researcher believes further high velocity MM
research is required when estimating musculoskeletal forces, within elite population dynamic
exercises. A further review of MM literature can be found in Appendix 1.
2.6 Summary
The GMAX and GMED have been highlighted as muscles vital to athletic performance
(Kyrolainen et al., 2005: Meir et al., 2001: Deutsch, 1998: Reily, 1996: Rienzi et al., 2000:
Nagano et al., 2005: Newton & Kraemer, 1994: Mero & Komi, 1994), generating hip
extension force during locomotion (Murphy et al., 2003: Kyrolainen et al., 2005: Guskiewicz
et al., 1993: Lieberman, 2006: Blazevich, 2000) and maintaining a rigid and stable pelvis
during multi directional movement (Oliver & Keeley, 2010), GMAX and GMED
strengthening therefore demands substantial focus in the strive for improved performance.
One proposed method of increasing GMAX and GMED recruitment and thus strength gain
(Ayotte et al., 2007) is an activation warm up; providing feedforward motor programmes
(Tsao & Hodges, 2007), exciting the motor neurons and recruiting motor units (Aagaard et
al., 2002). Enabling decreased motor unit recruitment lag-time (Tsao & Hodges, 2008),
increased HTMU recruitment (Aagaard et al., 2007) in turn optimising the stimuli required
for strength gain (Ayotte et al., 2007). Therefore considering the issues emerging from this
reading the following research objectives will be investigated;
Identify the effect of the independent variable, a GMAX and GMED activation warm
up’s effect on the dependant variables GMAX and GMED recruitment and GMAX,
GMED and lower limb force output during the HHP.

Reg Num: 115554 Gluteal Activation Warm Up 19
Discover if GMAX and GMED recruitment and GMAX, GMED and lower limb force
output impacted total ground reaction force (GRF).
Investigate the effect of the gluteal activation warm up on GMAX, GMED and GRF
RFD.
Formulate recommendations for the application of this GMAX and GMED activation
warm up.
Chapter Three
Method
3.1 Introduction
The primary aim of this study was to identify the effect of the independent variable a GMAX
and GMED activation warm up’s effect, on the dependant variables GMAX and GMED
recruitment and force output during the Hang High Pull (HHP) within elite rugby union
players, the cohort comprised of Premiership and International players from London Irish
Rugby Club. The secondary objectives were to discover if GMAX and GMED recruitment
and force output impacted total ground reaction force (GRF) and the effect of the gluteal
activation warm up on GMAX, GMED and GRF rate of force development (RFD). GMAX
and GMED recruitment data was collected using EMG (Biopac MP150, Delsys monitor iv
wireless transmission and data logging system, Worcestershire, UK), with force output data
collected via a combination of kinematic data using Vicon motion capture (Vicon MX
system, Vicon Motion Systems Ltd, Oxford, UK) and kinetic force plate data (Kistler Type
9286AA, Kistler Instrumente AG, Winterthur, Switzerland), then amalgamated to within
FreeBody Beta MM (FBB) to run optimizations. The GMAX and GMED have been shown
to influence athletic KPI (Murphy et al. 2003), highlighting efficient methods of increasing
GMAX and GMED contractile force, as material to increasing athletic performance. Within

Reg Num: 115554 Gluteal Activation Warm Up 20
this research methods chapter the research strategy, data collection methods and data analysis
will be discussed.
3.2 Research Strategy
Table 1
Cohort Anthropometrics Data Table
EMG FBB Pilot
Subjects 17 10 4
Age (years) 26.0 (±3.8) 25.0 (±3.4) 26.2 (±5.4)
Height (cm) 181 (±25.1) 185.5 (±6.6) 186.5 (±6.4)
Body Mass (kg) 103.3 (±10.1) 102.8 (±9.6) 104.3 (±11.9)
Load (kg) 86.9 (±9.0) 88.2(±9.6) 87.5 (±12.6)
Prior to the primary crossover trial an EMG pilot study was undertaken to establish if any
activation carryover was elicited by the control warm up and HHP that could affect the
dependent variables prior to the activation warm up and HHP, thus invalidating the effect of
the activation warm up. The pilot consisted of 4 subjects with mean age 26.2 (±5.4), height
186.5 (±6.4) and body mass 104.3 (±11.9) (Table 1), participating in identical testing
procedures as the primary study (as described below), however only EMG data was analysed
to establish any increase in MU recruitment, pilot study EMG data can be found in Appendix
2. If any activation carryover was present a subsequent whole cohort pre-test would have
been undertaken to gather data on the level of EMG MU recruitment and FBB force output,
enabling the results of the primary study to be individually adjusted to account for increases

Reg Num: 115554 Gluteal Activation Warm Up 21
in dependant variables within subjects. Completion of the pilot tests reduced any inaccuracy
within study design and thus increased the research’s validity.
Figure 2. Research structure info graphic
A randomised crossover design was chosen to reduce bias related to confounding variables
(Mills, Kelly & Guyatt, 1984), allowing each subject to act as their own control, enabling
advantageous between and within group comparison (Elbourne et al., 2002: MacLure. 1991).
The minimal washout period of the independent variable removed the potential issue of
carryover, increasing statistical efficiency enabling a reduced cohort size, thus highlighting
the use of a crossover design as valid (Cleophas, 1990: Mills et al., 2009: Hopkins, 2000).
Conducting both control and intervention testing within one testing session removed issues of
inexact recreation of EMG electrode and Vicon marker placement and also reduced the time
demands on the cohort (minimal time demands were a significant consideration as it was
Pilot Test
Carryover Present
Full Cohort Pilot Study
No Carryover present
Main Control and Intervention Study

Reg Num: 115554 Gluteal Activation Warm Up 22
imperative the time and energy expenditure of the elite population was at a minimum during
the competitive season). Inexact EMG electrode placement can alter readings as the distance
from signal origin to detection site has been shown to alter EMG trace and thus negate
accurate EMG comparison (Mesin, Merletti & Rainoldi, 2009: Konrad, 2005). Similarly
EMG signal can be influenced by external factors such as depth of subcutaneous adipose
tissue and hydration levels; these factors affect EMG magnitude with an inverse relationship
between subcutaneous tissue depth and EMG magnitude (Kuiken, Lowery & Stoyokov,
2003: Nordander et al., 2003), therefore by minimising the time frame between data
collections negated these potential issues, enabling accurate peak EMG collection and MVIC
normalisation.
On arrival subjects were prepared for EMG electrode (Appendix 3) (Biopac MP150, Delsys
monitor iv wireless transmission and data logging system) and Vicon reflective marker
placement (Appendix 4), subjects wore tight fitting garments, with the skin beneath the EMG
electrode site prepared by shaving and cleaning the area with alcohol wipes, enabling better
skin contact resulting in increased amplitude characteristics, reduced electrical interference,
noise and signal disturbance (Hermens, Freriks, Disselhorst-Klug & Rau, 2000). Vicon
markers were attached using double sided adhesive tape and adhesive spray; the placements
on the right lower limb are shown in Appendix 4, the markers and electrodes remained in situ
until the completion of the final test thus preventing any previously mentioned inaccuracy
arising from repeated EMG electrode (Mesin et al., 2009) and Vicon Marker placement.
EMG electrodes were placed 2cm apart half way between and in the line of the second sacral
vertebrae to the greater trochanter of the femur in parallel with the muscle fibres of the
GMAX and half way between and in line from the crista iliac and the greater trochanter for
the GMED (Seniam.0rg) (Appendix 3).

Reg Num: 115554 Gluteal Activation Warm Up 23
Following electrode and marker placement individual subjects began the testing regime
(shown in Figure 2) initially undertaking the control warm up shown in Figure 3, subjects
performed the control warm up followed by a 1-minute rest period, post rest period subjects
performed 3 HHP at 80% 1RM, on a force plate within the Vicon testing area collecting
kinematic and kinetic data for use in the FBB, whilst synchronised GMAX and GMED EMG
was collected. HHP loads were tailored to the individual subject via extrapolation of
individual training loads, increasing the consistency of individual intensity. 80% 1RM was
selected as 70-80% 1RM to maximise force production and GMAX and GMED involvement,
as 70-80% 1RM is stated as the optimal range for lower body power production, activation
and hip extensor moment (Cormie et al., 2007: Kawamori et al., 2005: Haff et al., 1997:
Hakkinen et al., 1985: Beardsley & Contreras, 2014).
Exercise Reps Sets
Stationary Bike 3 minutes 1
Inch Worm 8
2
Bodyweight Squat 8
Leg Swing 5 E/L
Lunge 8
Press up 8
Figure 3. Control trial non-specific warm up.

Reg Num: 115554 Gluteal Activation Warm Up 24
Following the HHP subjects underwent 20 minutes of down time allowing any post activation
potentiating (PAP) from the activation warm up or HHP to subside, conjecture exists over the
evidence for PAP (Behm, Button, Barbour, Butt & Young, 2004), despite said debate PAP is
believed to dissipate from 1 to 16 minutes and thus sufficient time was prescribed to nullify
any PAP (Corrie & Hardin, 1964: Gullich & Schmidtbleicher, 1996: Trimble & Harp, 1998:
Kitago et al., 2004: Kilduf et al., 2007: Hodgson, Docherty & Robbins, 2005). Succeeding
the 20 minute down period, subjects completed the GMAX and GMED activation warm up
shown in Figure 4, following 1-minute rest subjects again performed 3 HHP at 80% 1RM on
a force plate within the Vicon MX motion capture area with synchronised EMG data
collection.
Exercise Reps Sets
Stationary Bike 3 minutes 1
Inch Worm 6 1
Bodyweight Squat 6
Leg Swing 6 E/L
Prone Plank with Hip Extension (Right Side) 6 (2 sec hold at top)
Prone Plank with Hip Extension (Left Side) 6 (2 sec hold at top)
Side Plank with Hip Extension (Dominant leg down) 6 (2 sec hold at top)
Side Plank with Hip Extension (Non-dominant leg down) 6 (2 sec hold at top)
Single Leg Squat 3 E/L
Reg Num: 115554 Gluteal Activation Warm Up 25
Figure 4. Intervention trial GMAX and GMED specific warm up.
Following the HHP subjects again underwent 20 minutes down time enabling any PAP
effects of the activation warm up or HHP to subside prior to the completion of Maximum
Voluntary Isometric Contraction (MVIC) testing (Corrie & Hardin, 1964: Gullich &
Schmidtbleicher, 1996: Trimble & Harp, 1998: Kitago et al., 2004: Kilduf et al., 2007:
Hodgson, Docherty & Robbins, 2005). MVIC testing enabled normalization and accurate
analysis of GMAX and GMED EMG data, elevating the result validity (Kellis &
Baltzopoulos, 1996). MVIC testing utilised the prone with 90 degree knee flexion exercise to
measure GMAX hip extension MVIC and side-lying with the test leg upper most hip
abduction to measure GMED MVIC, following the testing guidelines of Hislop and
Montgomery (2007) and was completed post HHP reducing the impact of issues of accurate
recreation of EMG test conditions such as; electrode placement, hydration and body
composition (DeLuca, 1997: Rainoldi, Melchiorri, Caruso, 2004: Mesin et al., 2009: Kuiken
et al , 2003: Nordander et al., 2003) and potential GMAX and GMED activation occurring if
MVIC testing had preceded the control warm up procedure.
2.3 Data collection
The subjects were recruited from London Irish Rugby club for this study; their mean age,
height and body mass are displayed in Table 1. Subjects were divided into 3 testing dates due
to the cohort’s size and the time constraints of the test and subjects. Ethical approval was
obtained from St Mary’s University Twickenham School of Sport, Human and Applied
Sciences (Appendix 5).

Reg Num: 115554 Gluteal Activation Warm Up 26
Data collection of GMAX and GMED occurred in synchronicity; recruitment was measured
via Electromyography (EMG), kinematic analysis data collected via Vicon motion capture
(Vicon MX system, Vicon Motion Systems Ltd, Oxford, UK) in conjunction with kinetic
GRF data via the FP (Kistler Type 9286AA, Kistler Instrumente AG, Winterthur,
Switzerland). The FBB data was utilised to identify peak hip extension angle, GMAX,
GMED, bilateral hamstring, quadriceps force and GRF, a more in depth description of the
data collection process is available in Appendix 6. Kinematic or position data of the markers
and kinetic GRF data was filtered from 1000Hz to 200Hz in Microsoft Excel and inputted to
FBB in line with the work of Cleather and Bull (2010).
Peak EMG amplitude data was collected and rectified and smoothed to an EPOCH of 50ms
via the average over samples algorithm; this time window is appropriate for high velocity
movements (Muthuraman, Govindan, Deuschl, Heute & Raethjen, 2008: Mustard & Lee,
1987) such as the HHP, as a reduced time window reduces the risk of phase shift in
contractions and thus increase accuracy of data capture (Konrad, 2005: Muthuraman et al.,
2008). Once smoothed the peak EMG data was normalised against MVIC, normalisation
provides a standard value against which subjects and muscle groups can be compared,
enabling accurate comparison of subject’s GMAX and GMED pre and post intervention
(Knutson, Soderberg, Ballantyne & Clarke, 1994). However one issue surrounding MVIC is
subjects’ inconsistency in achieving maximum contraction, despite this issue MVIC is a
robust method of normalising EMG data and thus an appropriate method within this research
(Westing, Seger & Thorstensson, 1990). Further discussion of MVIC can be found in
Appendix 3.

Reg Num: 115554 Gluteal Activation Warm Up 27
MM analysis offers a method of calculating individual muscle force and data, via
combination of kinetic and kinematic data collected from Vicon and force plate data. The
FBB model of Cleather and Bull (2010) is a comprehensive model building on the model of
Horsman et al., (2007), utilising muscle lines and linked rigid segments model of the foot,
shank, thigh and pelvis to calculate the inter-segmental moments during the HHP (Cleather &
Bull, 2010). FBB facilitates accurate estimation of lower limb muscle forces and total GRF
allowing the researcher to examine of the effect of the gluteal activation warm up on MU
recruitment and force output. Further discussion of MM is discussed in Appendix 1.
The utilisation of multiple methods of data collection enabled the triangulation of two data
sets, facilitating a global picture of the impact of the independent variables on the research
objectives. The use of simultaneous EMG and FBB data collection enabled comparison of
data; EMG data providing an insight into the level of motor recruitment, which reflects
contractile force (Konrad, 2005) in conjunction with FBB, which provided a mathematical
estimation of contraction force, thus offering two differing modalities of measuring the same
independent variable.
Once collected the data was statistically analysed within SPSS using separate dependant t-
tests to compare the means of HHP GMAX and GMED control and intervention peak EMG
amplitudes and FBB peak hip extension angle, GMAX, GMED, bilateral hamstring,
quadriceps peak force and GRF outputs. Dependant t-test’s enabled intra subject comparison,
appropriate for this research due to the crossover design, offering increased interpretation
accuracy of the independent variable’s effect by removing inter cohort base level variance
Reg Num: 115554 Gluteal Activation Warm Up 28
(Mills et al., 2009), with linear regressions employed to investigate the relationships between
GMAX, GMED and GRF rate of force development (RFD).
Chapter Four
Results
The EMG pilot results showed no significant effect from the control warm up, although a
decrease was visible within the second control HHP’s (Table 2) and thus was no requirement
to adjust the primary research results.
Table 2
EMG Pilot Data in μν as a Percentage of MVIC
Control 1 Control 2
GMAX 29.531 (±40.67) 0.745 (±0.22)
GMED
17.473 (±28.16)
1.131 (±0.20)
Mean (±SD)
Statistically Significant (p < 0.05) *
As denoted in the method, peak EMG amplitude results were normalised against MVIC to
provide a percentage and standardise recruitment level within the cohort, whilst MU
Recruitment rate was quantified by microvolts over milliseconds μv/ms.
Reg Num: 115554 Gluteal Activation Warm Up 29
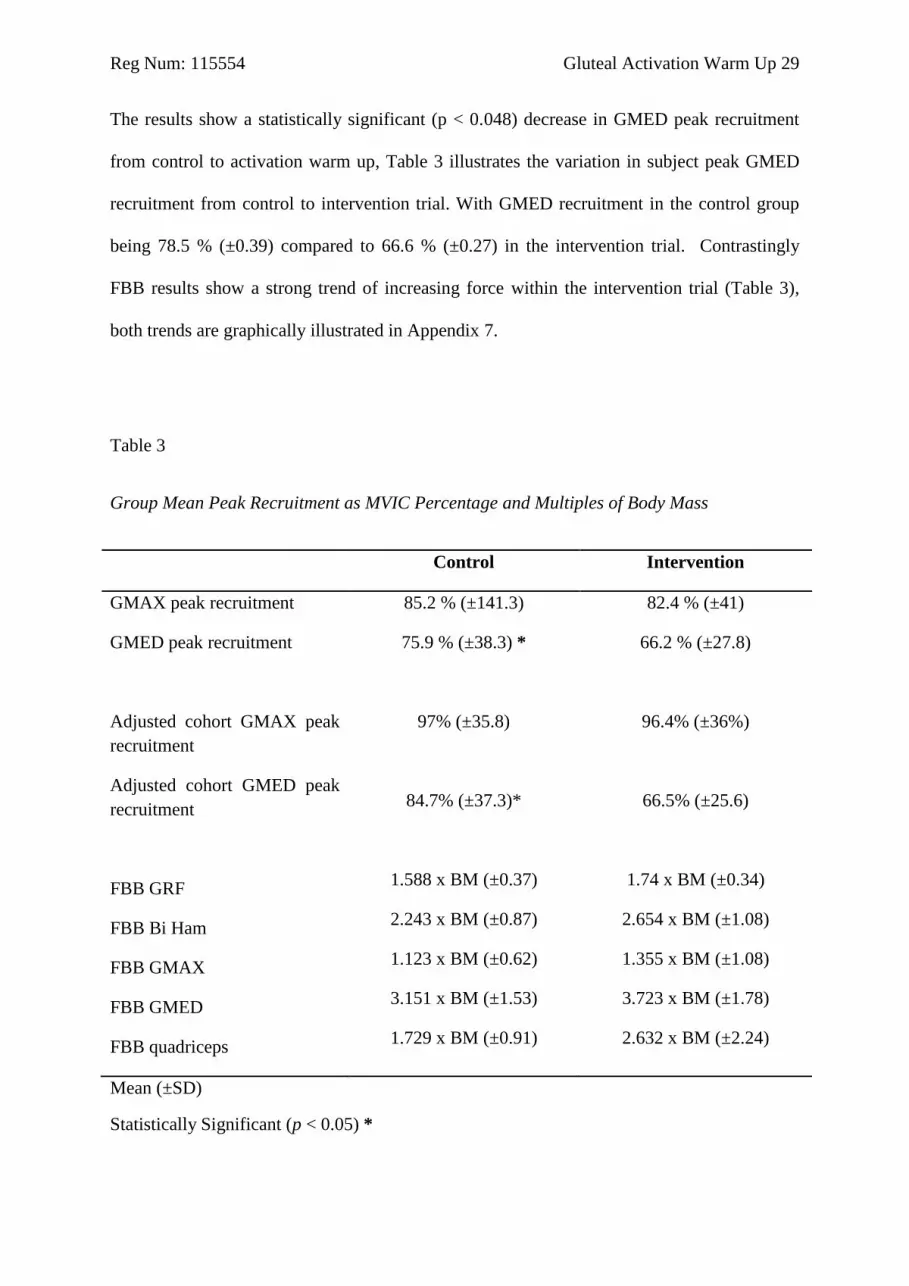
The results show a statistically significant (p < 0.048) decrease in GMED peak recruitment
from control to activation warm up, Table 3 illustrates the variation in subject peak GMED
recruitment from control to intervention trial. With GMED recruitment in the control group
being 78.5 % (±0.39) compared to 66.6 % (±0.27) in the intervention trial. Contrastingly
FBB results show a strong trend of increasing force within the intervention trial (Table 3),
both trends are graphically illustrated in Appendix 7.
Table 3
Group Mean Peak Recruitment as MVIC Percentage and Multiples of Body Mass
Control Intervention
GMAX peak recruitment 85.2 % (±141.3) 82.4 % (±41)
GMED peak recruitment 75.9 % (±38.3) * 66.2 % (±27.8)
Adjusted cohort GMAX peak
recruitment
Adjusted cohort GMED peak
recruitment
FBB GRF
FBB Bi Ham
FBB GMAX
FBB GMED
FBB quadriceps
97% (±35.8)
84.7% (±37.3)*
1.588 x BM (±0.37)
2.243 x BM (±0.87)
1.123 x BM (±0.62)
3.151 x BM (±1.53)
1.729 x BM (±0.91)
96.4% (±36%)
66.5% (±25.6)
1.74 x BM (±0.34)
2.654 x BM (±1.08)
1.355 x BM (±1.08)
3.723 x BM (±1.78)
2.632 x BM (±2.24)
Mean (±SD)
Statistically Significant (p < 0.05) *

Reg Num: 115554 Gluteal Activation Warm Up 30
The GMED had a greater significance (p < 0.006) when the EMG cohort was reduced to
identically match the FBB cohort, thus offering increased comparison accuracy. Table 3
shows both full and adjusted EMG cohort data.
Table 4
FBB GMED, GMAX and GRF RFD as xBW/ms and EMGGMED and GMAX RFD as
MVIC% μv/ms
Control Intervention
FBB GMED RFD 0.219 xBW/ms (±0.33) 0.189 xBW/ms (±0.18)
FBB GMAX RFD 0.066 xBW/ms (±0.04) 0.267 xBW/ms (±0.56)
FBB GRF RFD 0.098 xBW/ms (±0.11) 0.201 xBW/ms (±0.21)
FBB GMAX & GRF RFD
regression p values
0.272 0.349
FBB GMED & GRF RFD
regression p values
0.059 0.267
Mean (±SD)
Statistically Significant (p < 0.05) *
Once being filtered and run through the FBB RFD the results were statistically analysed via
dependent t-tests and linear regressions in SPSS, no statistically significant results (p ≤ 0.05)
were found via t-test (Table 4), however GMED RFD and GRF RFD showed a near

Reg Num: 115554 Gluteal Activation Warm Up 31
significant result (p < 0.059) using linear regression (Table 4). No statistically significant
results (p ≤ 0.05) or trends were found in the EMG data (Figure 5).
Figure 5. Peak motor unit recruitment rate in control and intervention trials
Chapter Five
Discussion
5.1 Introduction
The primary aim of this research was to further the understanding of the effects of gluteal
activation warm ups on the subsequent gluteal MU recruitment and force output, the specific
research objectives were to:
0
0.000005
0.00001
0.000015
0.00002
0.000025
0.00003
0.000035
0.00004
0.000045
0.00005
GMAX GMED
μv/
ms
Peak MU Recruitment Rate
control
Intervention

Reg Num: 115554 Gluteal Activation Warm Up 32
Identify the effect of the independent variable, a GMAX and GMED activation warm
up’s effect on the dependant variables GMAX and GMED recruitment and GMAX,
GMED and lower limb force output during the HHP.
Discover if GMAX and GMED recruitment and GMAX, GMED and lower limb force
output impacted total ground reaction force (GRF).
Investigate the effect of the gluteal activation warm up on GMAX, GMED and GRF
RFD.
Formulate recommendations for the application of this GMAX and GMED activation
warm up.
Within this chapter a discussion of the research findings in relation to the research
hypothesis, overall aim and specific research objectives will occur, resulting in practical
applications for the use of gluteal activation warm ups, a discussion of the possible rationale
behind the statistically significant decreased (p < 0.048) EMG peak GMED MU following
the activation warm. Following this discussion there will be a similar critique of why despite
this statistically significant (p < 0.048) decrease in MU recruitment during the intervention
HHP the FBB results show a non-significant but clear trend of increased force output in;
bilateral hamstring, GMAX, GMED, quadriceps and GRF following the intervention warm
up (Table 3 & Appendix 7). The next research objective regards the exploration of the
relationship between GRF and GMAX and GMED recruitment and force output, the FBB
results (Table 3 & Appendix 7) highlight a non-significant (p > 0.05) trend of increased GRF
following the gluteal activation warm up, this trend and the potential rationale will be
investigated along with the potential causes of increased force and GRF within the FBB data
(Table 3). Following the GRF debate a discussion of the differing trends within EMG and
FBB RFD (Figure 5 & Table 4) will occur, resulting in practical recommendation for the

Reg Num: 115554 Gluteal Activation Warm Up 33
application of this gluteal activation warm up will be given in light these findings and
previous research.
5.2 Research Objectives
As identified within the discussion introduction the primary research objective was to identify
the effect of the gluteal activation warm up on GMAX and GMED MU recruitment and force
output, lower limb force and GRF within the HHP. The peak GMED EMG amplitude results
(Table 3) of this research show a statistically significant (p < 0.048) decrease during the HHP
following the gluteal activation warm up, with a greater decrease in GMED MU recruitment
of p < 0.006 (Table 3) found when the EMG cohort was adjusted to identically match the 10
subjects employed within the FBB research, further supporting the relationship between
EMG and FBB results. These results initially suggest this gluteal activation warm up is
detrimental to MU recruitment and muscular force, a result contrary to the theory that
activation exercise increases the muscular innervation pattern via plastic changes in nervous
system (Tsao & Hodges, 2007), enabling greater firing rate and frequency (Van Cutsem,
Duchateau & Hainaut, 1998). However this may be simplistic as MU firing rates fluctuate
within different contraction types and do not always follow a linear correlation of increased
MU recruitment resulting in increased muscular force; as within high force isometric
contraction MU recruitment can reduce during high levels of force generation (Milner-Brown
et al., 1973).
Previous research investigating the effect of therapeutic activation exercise has resulted in
mixed conclusions; however Tsao and Hodges (2008) discovered that a specific TA
activation exercises facilitated faster activation of the TA within subsequent upper limb

Reg Num: 115554 Gluteal Activation Warm Up 34
exercise after only one session and over a 4 week training programme, similarly Crow et al.
(2012) identified an immediate 4.2% increase in CMJ height post gluteal activation warm up.
However despite the 4.2% increase in CMJ height the findings of Crow et al. (2012) did not
identify any specific increase in MU recruitment or force output of the lower limb muscles as
no data regarding increased muscle force and GRF was available to quantify the mechanism
of CMJ height increase, thus providing no rationale for CMJ height increase. The increase
was solely described in terms of a cause and effect relationship, that the activation warm up
resulted in increased CMJ height with no insight into the contributing factors of this increase,
thus this research attempted to fill said void. Despite the lack of explanation of their findings,
Crow et al. (2012) did find a statistically significant increase in CMJ height, which could be
extrapolated to have occurred due to increased GRF resulting from increased muscle force
and thus potentially facilitating increased CMJ height (Hammer, Seth & Delp, 2010), results
equivalent to those within the FBB data (Table 3) despite the statistically significant (p <
0.048) decrease in GMED MU recruitment following the gluteal activation warm up (Table
3).
These opposing trends in EMG and FBB data (Table 3) whilst initially puzzling provide an
interesting discussion surrounding the differing parameters measured within this research and
their relationship during dynamic actions. Peak EMG amplitude describes MU activity
during muscular contractions, in particular peak EMG amplitude describes the number of MU
recruited, with the number of MU being cited as modulating muscle force, with the firing rate
of recruited MU regulated by the higher centers of the central nervous system (CNS)
controlling the extent of force produced by each motor unit (DeLuca & Erim, 1994) and as
such makes quantifying these opposing findings challenging. However the behavior of MU
during high force isometric contractions may provide a rationale for these opposing findings,
Reg Num: 115554 Gluteal Activation Warm Up 35
Milner-Brown et al. (1973) states that at high levels of voluntary force generation during
isometric contractions a sharp decline occurs in the number of MU’s recruited whilst high
levels of force are generated, postulating that HTMU can generate increasing force despite
reduced MU recruitment and thus increased MU recruitment has reduced attribution to the
high generation of muscular force during high threshold isometric contractions. The ability
of the HTMU to generate increased force whilst the lower threshold MU (LTMU) have
reduced recruitment resulting in reduced total MU recruitment is hypothesized to be due to
the increased firing rate of the HTMU (Kernell, 1966: Granit et al., 1957: Kernell, 1965), a
theory appearing contrary to Henenman’s size principle, however this modulation of MU
recruitment is unique to isometric contractions with the strongest evidence for the
maintenance or increase in muscular force whilst MU recruitment decreases occurring in
contractions above 50% MVC in small muscles where MU recruitment has reached
completion (Kukulka & Clamann, 1981: De Luca et al., 1982) and 70-80% MVC in large
muscles (Kukulka & Clamann, 1981: De Luca et al., 1982), highlighting that high force
isometric contractions can be maintained despite decreasing firing rates with no additional
MU recruitment (De Luca, Foley & Erim, 1996). Therefore considering the rationale
provided by the previously discussed research and the results of this research, it could be
speculated that the activation warm up (Figure 4) facilitated increased GMED contraction
intensity to above 50% (Kukulka & Clamann, 1981: De Luca et al., 1982), thus breaching the
threshold required to trigger the cascade of plastic changes within the CNS resulting in
altered MU recruitment patterns and a statistically significantly (p < 0.048) decrease in
GMED MU recruitment despite increased force output.
This pattern of MU recruitment is unique to isometric contractions and despite the dynamic
nature of the HHP it is believed that the primary function of the GMED during the HHP is to

Reg Num: 115554 Gluteal Activation Warm Up 36
isometrically stabilize the pelvis. Considering the function of the GMED during the HHP in
conjunction with the research in isometric contractions and the trends discovered within this
research, it is speculated that the activation warm up elicited plastic changes within the motor
neuron pool, altering the firing patterns of the afferents from the central centers, thus
streamlining the neural circuitry required to preferentially activated the HTMU (De Luca &
Erim, 1994) enhancing contraction intensity to above 50% (Kukulka & Clamann, 1981: De
Luca et al., 1982), thus triggering the cascade of events in the CNS reduced the number of
LTMU recruited, resulting in the reduce requirement for total GMED MU recruitment. These
findings and extrapolations are specifically relevant to this research as the primary function
of the GMED during the HHP is isometric contraction to stabilize the pelvis, similar to its
function during the CMJ (Nagano et al., 2005), creating a stable platform for the GMAX and
lower limb muscles to produce force during concentric and eccentric contractions. Thus the
GMED EMG results (Table 3) suggest the gluteal activation warm up elicited plastic changes
in the CNS, facilitating preferential activation of the HTMU reducing the requirement of the
LTMU recruitment enabling greater force generation despite the reduction in total MU
recruitment (Table 3 & Appendix 7). This theory is further supported by virtually unchanged
GMAX MU recruitment of the matched FBB and EMG cohort (Table 3), as the function of
the GMAX is to act dynamically during the HHP to create hip extension and as such GMAX
function differs to the GMED.
The mechanisms believed to increase muscle force output in dynamic contractions of the
GMAX, bilateral hamstring and quadriceps is believed to center around; increasing coding
rate via increased afferent excitability, decreased MU innervation lag-time and increasing
HTMU recruitment. These mechanisms appear to increase the force output of the GMAX,
bilateral hamstring and Quadriceps during dynamic contractions resulting in increased GRF

Reg Num: 115554 Gluteal Activation Warm Up 37
(Hammer et al., 2010), increasing coding rate increases firing frequency, potentially
increasing the efficiency of the innervating axon, which carries the impulse to the MU
(Person & Kudina, 1971), enabling the greater firing rate of MU and thus increasing force.
Increasing muscle activation also increases the recruitment of HTMU (Tsao & Hodges, 2008)
via increasing the excitability of the afferent nerves potentially priming the innervating axon
of the HTMU’s, enabling increased HTMU recruitment efficiency during periods requiring
high levels of muscular force (Van Cutsem et al., 1998). These physiological processes
appear to be potential mechanisms of increasing force output and GRF elicited via the gluteal
activation warm up (Table 3 & Appendix 7) and as such provide a mandate for the utilization
of this gluteal activation warm up to increase performance KPI.
The FBB results highlight a trend of increased GRF, bilateral hamstring, GMAX, GMED and
quadriceps force (Table 3) following the activation warm up (Figure 4), despite statistical
analysis not find any statistically significant results (p ≤ 0.05) a strong trend is visible in
Appendix 7, suggesting that the gluteal activation warm up (Figure 4) elicited a positive and
relevant effect on force output. This trend mirrors the findings of Tsao & Hodges (2008) due
to the FBB results showing increased GRF following one activation intervention similar to
the extrapolation of the mechanisms responsible for the 4.2% increase in CMJ height found
by Crow et al. (2012). CMJ height is heavily influenced by GRF (Hori, Newton, Nosaka &
McGuigan 2006) as GRF is the result of lower limb muscular force (Hammer et al., 2010), it
could be extrapolated that despite no empirical evidence being provided for the increase in
CMJ height exhibited within the work of Crow et al. (2012), the increase may be the result of
similar physiological mechanisms as discussed within this research resulting in increased
lower limb force (Table 3) manifested as increased GRF (Hammer et al. 2010).

Reg Num: 115554 Gluteal Activation Warm Up 38
The statistically significant reduction (p < 0.048) in GMED MU recruitment resulting from
the activation warm up in Figure 4 could initially be view as having a detrimental effect on
both performance (Murphy et al., 2003) and injury risk (Presswood et al., 2008), however
when analysed in conjunction with the increased force outputs found in the FBB results this
conclusion appears limited, as the plastic changes in the CNS resulting in preferential HTMU
recruitment elicited by the gluteal activation warm up suggest that despite decreased GMED
MU recruitment the increased force facilitated by the activation warm up (Figure 4) enable
increased performance as a result of increased GRF and increased GMED and GMAX force
output which may potentially reduce ACL injury risk by reducing Trendelenburg sign (Cutter
& KerVorkain, 1999: Earle, 2005) and in turn knee valgus angle (Powers, 2010 Reiman et al.,
2009) and hip and tibial internal rotation moments within the transverse plane (Krosshaug et
al., 2007: Besier et al., 2001: Besier et al., 2001: McLean et al., 2005: Earle 2005). A similar
improvement in performance appears to be visible as a result of the gluteal activation warm
up due to the increased lower limb force and resultant increase in GRF and thus on sporting
KPI (Weyand et al., 2000: Murphy et al., 2003: Blazevich, 2000) discussed within the
literature review.
Further evidence for the improvement in athletic performance resulting from the activation
warm up in Figure 4 is increased pelvic stability during stance, resulting from elevated
GMED strength (Gottschalck, 1989: Lieberman et al., 2006) consequently reducing
Trendelenburg sign and in turn force leakage (Oliver & Keeley, 2010: Neptune et al., 1999
Cutteret al., 1999: Earle, 2005), resulting in increased GRF (Gottschalck, 1989: Lieberman et
al., 2006: Cutteret & Kervorkain, 1999: Earle, 2005) which has been previously cited as
Reg Num: 115554 Gluteal Activation Warm Up 39
increasing sporting KPI (Weyand et al., 2000: Murphy et al., 2003). As well as reducing
force leakage a stable pelvis enhances the ability of the GMAX and other hip extensors to
create proximal to distal force, resulting in increased GRF (Lieberman et al., 2006:
Blazevich, 2000: Weyand et al., 2000) and thus sporting KPI (Weyand et al., 2000: Murphy
et al., 2003).
Considering that FBB GMED and GMAX force output showed a non-significant trend of
increase following the gluteal activation warm up, despite the statistically significant (p <
0.048) decrease in EMG GMED peak MU recruitment (Table 3) which appears to arise from
the plastic changes in the CNS leading to preferential recruitment of the HTMU, it appears
the gluteal activation warm up (Figure 4) is an effective method of increasing lower limb
force and GRF during the HHP. Therefore the use of this activation warm up may increase
pelvic stability resulting in enhanced athletic performance (Murphy et al., 2003) and reduced
injury risk (Presswood et al., 2008).
The second research objective; exploring the relationship between GMAX and GMED
recruitment and force output and their relationship with GRF will now be discussed, the
relationship of GRF and GMAX and GMED recruitment and force output is relevant due to
the importance of GRF on athletic performance KPI (Murphy et al., 2003: Blazevich, 2000:
Weyand et al., 2000). Similarly to the previous discussion regarding on GMAX and GMED
recruitment and force output, the two methods of data collection show differing results and as
such create a challenging critique. Peak GRF was calculated using FBB and did not yield a
significant (p ≤ 0.05) increase; however despite this, a strong trend of increase is visible in
(Appendix 7) highlighting the positive impact of the gluteal activation protocol (Figure 4),

Reg Num: 115554 Gluteal Activation Warm Up 40
the previously discussed mechanisms of increased contractile force occurring in concert with
reduced MU recruitment (Milner-Brown et al., 1973) is also relevant to this discussion and as
despite the statistically significant decrease (p < 0.048) in GMED recruitment following the
activation warm up, the gluteal activation warm up in Figure 4 appears to have a positive
effect on GRF. This positive increase in GRF resulting from the activation warm up appears
to be the result of the trend of increased lower limb muscle force, the relationship between
GRF and lower limb force, which show increase following the activation warm up (Table 3),
has been established by Hammer et al. (2010) who states the accumulation of increased lower
limb forces results in increased GRF, thus there appears to be a strong relationship between
GMAX and GMED force and the resultant GRF. Therefore considering the positive impact
of the gluteal activation warm up on GRF, the relationship between increased lower limb
forces and GRF (Hammer et al. 2010) in conjunction with the 4.2% increase in CMJ height
found by Crow et al. (2012) following the activation warm up found in Appendix 8, provides
a rationale for the efficacy of activation warm up protocols at increasing athletic performance
via increased GRF (Weyand et al., 2000: Blavevich, 2000: Murphy et al., 2003).
The penultimate research objective was to investigate the effect of the gluteal activation
warm up on GMAX, GMED and GRF RFD; RFD describes the rate at which force is
produced (Δ force/Δ time), a quality cited as vital in explosive sports performance (Aagaard
et al., 2002: Hakkinen & Komi, 1986: Schmidtbleicher & Buehrle, 1987: Sleivert & Wenger,
1994: Thorstensson, Karlsson, Viitasalo, Luthanen & Komi, 1976). Within this research
RFD is defined as Δ force/Δ time from the onset of the contraction at which the peak
contraction occurred within the FBB and EMG data respectively. RFD data for both EMG
and FBB is shown in Figure 5 and Table 3 respectively, no significant change in means was

Reg Num: 115554 Gluteal Activation Warm Up 41
identified via dependent t-test across measurements in either FBB or EMG respectively,
however a linear regression highlighted FBB GMED RFD as having a near significant (p <
0.059) relationship with FBB GRF RFD (Table 3), as such any resultant increase in FBB
GMED RFD arising from the gluteal activation warm up may have a positive impact on FBB
GRF RFD. EMG RFD highlighted a trend of decreased RFD following the activation warm
up a trend correlating with the Peak EMG MU recruitment findings, which also show a
decreased peak following the activation warm up, both of these sets of results appearing to
follow a logical trend due to RFD being influenced by peak force, as increased absolute force
increases the ability to express force at a greater rate (Andersen & Aagaard, 2006). Therefore
both peak EMG MU recruitment and MU rate of recruitment show a decrease as a result of
the gluteal activation warm up (Figure 5) with only a limited trend being apparent within the
FBB data despite the near significant (p < 0.059) relationship between FBB GMAX RFD and
GRF RFD (Table 3), illustrating that the implementation of this gluteal activation warm up
(Figure 4) has no significant benefit on RFD within both FBB and EMG data collection
methods respectively, however due to the near significant (p < 0.059) relationship between
FBB GMED RFD and FBB GRF RFD and the statistically significant decrease (p < 0.048) in
GMED and increased FBB force output due to the isometric contraction of the GMED, the
implementation of the warm up in Figure 4 may warrant further investigation, as the
potentially greater GMED contraction of >50% (Kukulka & Clamann, 1981: De Luca et al.,
1982) eliciting the previously discussed plastic changes in the CNS and MU recruitment
could potentially facilitate a strong relationship between GMED RFD and GRF RFD, with
greater GMED isometric force output influencing increased GRF via the previously discussed
increases in pelvic stability. Despite maximum force output being important to sporting
performance, RFD is of greater importance (Aagaard et al., 2002) as high velocity
movements such as sprint ground contact times have a limited duration of 50-250ms

Reg Num: 115554 Gluteal Activation Warm Up 42
compared to ≥ 300ms for time to maximum force (Thorstensson et al., 1976), therefore the
minimal time window may be insufficient to exert maximal force and as such increased RFD
is important in facilitating a greater proportion of maximum force to be exerted during the
early phase of muscle contraction (Aagaard et al., 2002). Due to the importance of RFD on
sporting performance the implementation of the gluteal activation warm up show in Figure 4
may be advantageous to performance as, despite no significant improvements in RFD being
established the strong trend of increased lower limb force within the FBB results may
increase the total amount of force available for expression as GRF. Therefore despite this
gluteal activation warm up having a no statistically significant (p ≤ 0.05) effect on RFD, the
relationship between total force and RFD and the importance of RFD on sporting
performance (Aagaard et al., 2002) means further investigation of gluteal activation warm
ups on RFD appears warranted.
5.3 Recommendations and Practical application
The conclusion of the primary research objective is that the gluteal activation protocol
employed within this research (Figure 4) resulted in a significant reduction in GMED MU
recruitment, evidenced by a p < 0.048 decrease in GMED MU recruitment (Table 3),
however the strong trend of increase in the FBB muscular forces data highlights an
interesting occurrence unique to isometric contractions, thus speculation suggests the
implementation of this gluteal activation warm up appears beneficial in increasing lower limb
muscle forces and GRF. The secondary research objective investigating the effect GMAX
and GMED had on GRF discovered that despite the statistically significant reduction (p ≤
0.05) in GMED MU recruitment FBB GRF showed a non-significant increase, further
reinforced by the relationship between FBB GRF, GMAX and GMED force output showing

Reg Num: 115554 Gluteal Activation Warm Up 43
increase. Therefore considering these findings, the practical implementation of this protocol
could be prior to athletic performance; this performance could be gym based prior to a HHP
or similar compound exercises resulting in increased muscle strength and RFD over a training
cycle (Beachle & Earle, 2008). Further to this application, this protocol could be employed
prior to competitive performance similar to the practical application of Crow et al. (2012),
increasing GRF and thus potentially facilitating increased sporting KPI and sports
performance (Murphy et al., 2003: Blazevich, 2000: Weyand et al., 2000).
When evaluating this research it is imperative to understand its limitations, in particular those
concerning data collection, the use of both EMG and FBB enabled triangulation of results
and thus greater analysis of the gluteal activation warm up, however by limiting EMG
analysis to GMED and GMAX rather than aligning EMG muscle analysis with FBB
comparison was limited. EMG analysis was limited to the GMAX and GMED due to the
time constraints of the population, as one requirement of employing this elite population was
limiting the energy and time cost to a minimum during the competitive season, also the
potential for the increased EMG paraphernalia creating ghost markers within the kinematic
data was considered.
5.4 Contributions to knowledge
This research may have contributed to the knowledge of the use of therapeutic gluteal
activation as a method of increasing athletic performance in elite athletes, showing that an
extensive gluteal activation warm up (Figure 4) could enhance lower limb force output and
GRF despite a statistically significant decrease in GMED MU recruitment (p < 0.048); a

Reg Num: 115554 Gluteal Activation Warm Up 44
scenario believed to be due to plastic changes in the CNS enhancing preferential HTMU
recruitment and reducing the requirement for increased total MU recruitment during high
force isometric contractions (Milner-Brown et al., 1973). Further to the contribution of
knowledge to the field of gluteal activation this research broadens the scope of MM research,
due to the intervention based analysis of high velocity weightlifting movements, other
dynamic MM research exists, Cleather and Bull (2010) utilised the push jerk to investigate
inter-segmental moments of the foot, calf, thigh and pelvis, with Pandy and Zajac (1991) and
Anderson and Pandy (1999) investigating the CMJ and squat jump respectively, however this
was not interventionist research and therefore, it is the researcher’s belief that a minor
contribution to MM field has been made.
5.5 Self Reflection
On reflection the researcher incurred some problems during data collection; issues
surrounding data storage leading to differing FBB and EMG cohort numbers (Table 1),
resulting in the FBB data carrying reduced statistical power (Hopkins, 2009: Knudson, 2011),
however when the EMG cohort was limited to the identical 10 subjects utilised in the FBB
cohort the results showed a comparative if not a amplified effect. Therefore considering this
the researcher’s advice for future students would be to gain an increased proficiency using the
kinematic and kinetic data collection methods required for FBB to negate any potential issue,
building on the testing procedure shown in Appendix 6.

Reg Num: 115554 Gluteal Activation Warm Up 45
Despite this issue, the primary research objective found a statistically significant (p < 0.048)
decrease in GMED MU recruitment (Table 3) following this gluteal activation warm up, an
effect believed to be due to the previously discussed plastic changes in the CNS during
isometric contractions, elicited by the gluteal activation warm up, these changes contributed
to a strong trend of increase in GMAX, GMED, bilateral hamstring, quadriceps force and
GRF. Thus in conclusion the implementation of the activation warm in Figure 4 could
improve the force generation of the lower limb musculature, facilitating increased GRF, as
such in a research field yielding limited practical applications, these research findings
contribute to the body of evidence supporting the use of a therapeutic gluteal activation warm
ups to improve force generation in elite male rugby union players and wider elite populations.
References
Aagaard, P., Simonsen, E. B., Andersen, J. L., Magnusson, P., & Dyhre-Poulsen, P. (2002). Increased
rate of force development and neural drive of human skeletal muscle following resistance
training. Journal of applied physiology, 93(4), 1318-1326.
Andersen, L. L., & Aagaard, P. (2006). Influence of maximal muscle strength and intrinsic muscle
contractile properties on contractile rate of force development. European journal of applied
physiology, 96(1), 46-52.
Andersen, L. L., Magnusson, S. P., Nielsen, M., Haleem, J., Poulsen, K., & Aagaard, P. (2006).
Neuromuscular activation in conventional therapeutic exercises and heavy resistance
exercises: implications for rehabilitation. Physical therapy, 86(5), 683-697.

Reg Num: 115554 Gluteal Activation Warm Up 46
Anderson, F. C., & Pandy, M. G. (1999). A dynamic optimization solution for vertical jumping in
three dimensions. Computer methods in biomechanics and biomedical engineering, 2(3), 201-
231.
Anderson, F. C., & Pandy, M. G. (2003). Individual muscle contributions to support in normal
walking. Gait & posture, 17(2), 159-169.
Ayotte, N. W., Stetts, D. M., Keenan, G., & Greenway, E. H. (2007). Electromyographical analysis of
selected lower extremity muscles during 5 unilateral weight-bearing exercises. Journal of
Orthopaedic & Sports Physical Therapy, 37(2), 48-55.
Baker, D., & Nance, S. (1999). The relation between running speed and measures of strength and
power in professional rugby league players. The Journal of Strength & Conditioning
Research, 13(3), 230-235.
Beachle, T. R., & Earle, R. W. Essentials of strength training and conditioning. Vol. 7. Champaign,
IL: Human kinetics, 2008.
Beardsley, C., & Contreras, B. (2014). The Increasing Role of the Hip Extensor Musculature With
Heavier Compound Lower-Body Movements and More Explosive Sport Actions. Strength &
Conditioning Journal, 36(2), 49-55.

Reg Num: 115554 Gluteal Activation Warm Up 47
Behm, D. G., Bambury, A., Cahill, F., & Power, K. (2004). Effect of acute static stretching on force,
balance, reaction time, and movement time. Medicine and Science in Sports and Exercise, 36,
1397-1402.
Berns, G. S., Hull, M. L., & Patterson, H. A. (1992). Strain in the anteromedial bundle of the anterior
cruciate ligament under combination loading. Journal of Orthopaedic Research, 10(2), 167-
176.
Besier, T. F., Lloyd, D. G., Cochrane, J. L., & Ackland, T. R. (2001). External loading of the knee
joint during running and cutting maneuvers. Medicine and Science in Sports and Exercise,
33(7), 1168-1175.
Blazevich, A. J. (2000). Optimizing Hip Musculature For Greater Sprint Running Speed. Strength &
Conditioning Journal, 22(2), 22.
Bobbert, M. F., & van Ingen Schenau, G. J. (1988). Coordination in vertical jumping. Journal of
biomechanics, 21(3), 249-262.
Boden, B. P., Feagin Jr, J. A., & Garrett Jr, W. E. (2000). Mechanisms of anterior cruciate ligament
injury. Orthopedics, 23(6), 573.

Reg Num: 115554 Gluteal Activation Warm Up 48
Boudreau, S. N., Dwyer, M. K., Mattacola, C. G., Lattermann, C., Uhl, T. L., & McKeon, J. M.
(2009). Hip-muscle activation during the lunge, single-leg squat, and step-up-and-over
exercises. Journal of sport rehabilitation, 18(1), 91.
Boren, K., Conrey, C., Le Coguic, J., Paprocki, L., Voight, M., & Robinson, T. K. (2011).
Electromyographic analysis of gluteus medius and gluteus maximus during rehabilitation
exercises. International journal of sports physical therapy, 6(3), 206.
Brown, L., & Ferrigno, V. (Eds.). (2014). Training for Speed, Agility, and Quickness, 3E. Human
Kinetics.
Buttifant, D., Crow, J., Kearney, S., & Hrysomallis, C. (2011). Whole Body Vibration vs. Gluteal
Muscle Activation: What are the Acute Effects on Explosive Power?. The Journal of Strength
& Conditioning Research, 25, S14-S15.
Carlock, J. M., Smith, S. L., Hartman, M. J., Morris, R. T., Ciroslan, D. A., Pierce, K. C., ... & Stone,
M. H. (2004). The relationship between vertical jump power estimates and weightlifting
ability: a field-test approach. The Journal of Strength & Conditioning Research, 18(3), 534-
539.
Cleather, D. J., & Bull, A. M. (2010). Lower-extremity musculoskeletal geometry affects the
calculation of patellofemoral forces in vertical jumping and weightlifting. Proceedings of the
Institution of Mechanical Engineers, Part H: Journal of Engineering in Medicine, 224(9),
1073-1083.

Reg Num: 115554 Gluteal Activation Warm Up 49
Cleather, D. J., & Bull, A. M. (2010). Influence of inverse dynamics methods on the calculation of
inter-segmental moments in vertical jumping and weightlifting. Biomedical engineering
online, 9(1), 74.
Cleophas, T. J. (1990). A simple method for the estimation of interaction bias in crossover studies.
The Journal of Clinical Pharmacology, 30(11), 1036-1040.
Čoh, M., Tomain, K., & Štuhec, S. (2006). The biomechanical model of the sprint start and block
acceleration. Facta Universitatis: Series Physical Education and Sport, 4, 103-114.
Cormie, P., McBride, J. M., & McCaulley, G. O. (2009). Power-time, force-time, and velocity-time
curve analysis of the countermovement jump: impact of training. The Journal of Strength &
Conditioning Research, 23(1), 177-186.
Cormie, P., McGuigan, M. R., & Newton, R. U. (2011). Developing maximal neuromuscular power.
Sports medicine, 41(1), 17-38.
Cormie, P., McCaulley, G. O., Triplett, N. T., & McBride, J. M. (2007). Optimal loading for maximal
power output during lower-body resistance exercises. Medicine and Science in Sports and
Exercise, 39(2), 340.

Reg Num: 115554 Gluteal Activation Warm Up 50
Corrie, W. S., & Hardin, W. B. (1964). Post-tetanic potentiation of H reflex in normal man:
quantitative study. Archives of neurology, 11(3), 317-323.
Crow, J. F., Buttifant, D., Kearny, S. G., & Hrysomallis, C. (2012). Low load exercises targeting the
gluteal muscle group acutely enhance explosive power output in elite athletes. The Journal of
Strength & Conditioning Research, 26(2), 438-442.
Cutsem, M., Duchateau, J., & Hainaut, K. (1998). Changes in single motor unit behaviour contribute
to the increase in contraction speed after dynamic training in humans. The Journal of
Physiology, 513(1), 295-305.
Cutter, N. C., & Kevorkian, C. G. (Eds.). (1999). Handbook of manual muscle testing. McGraw-
Hill/Appleton & Lange.
De Luca, C. J., LeFever, R. S., McCue, M. P., & Xenakis, A. P. (1982). Behaviour of human motor
units in different muscles during linearly varying contractions. The Journal of Physiology,
329(1), 113-128.
De Luca, C. J., & Erim, Z. (1994). Common drive of motor units in regulation of muscle force.
Trends in neurosciences, 17(7), 299-305.
De Luca, C. J., Foley, P. J., & Erim, Z. (1996). Motor unit control properties in constant-force
isometric contractions. Journal of Neurophysiology, 76(3), 1503-1516.

Reg Num: 115554 Gluteal Activation Warm Up 51
De Luca, C. J. (1997). The use of surface electromyography in biomechanics. Journal of applied
biomechanics, 13, 135-163.
Deutsch, M. U., Maw, G. J., Jenkins, D., & Reaburn, P. (1998). Heart rate, blood lactate and
kinematic data of elite colts (under-19) rugby union players during competition. Journal of
sports sciences, 16(6), 561-570.
Distefano, L. J., Blackburn, J. T., Marshall, S. W., & Padua, D. A. (2009). Gluteal muscle activation
during common therapeutic exercises. Journal of Orthopaedic & Sports Physical Therapy,
39(7), 532-540.
Ekstrom, R. A., Donatelli, R. A., & Carp, K. C. (2007). Electromyographic analysis of core trunk, hip,
and thigh muscles during 9 rehabilitation exercises. journal of orthopaedic & sports physical
therapy, 37(12), 754-762.
Elbourne, D. R., Altman, D. G., Higgins, J. P., Curtin, F., Worthington, H. V., & Vail, A. (2002).
Meta-analyses involving cross-over trials: methodological issues. International journal of
epidemiology, 31(1), 140-149.
Escamilla, R. F., Fleisig, G. S., Zheng, N., Barrentine, S. W., Wilk, K. E., & Andrews, J. R. (1998).
Biomechanics of the knee during closed kinetic chain and open kinetic chain exercises.
Medicine and science in sports and exercise, 30(4), 556-569.

Reg Num: 115554 Gluteal Activation Warm Up 52
Farina, D., Merletti, R., & Enoka, R. M. (2004). The extraction of neural strategies from the surface
EMG. Journal of Applied Physiology, 96(4), 1486-1495.
Fleming, B. C., Renstrom, P. A., Beynnon, B. D., Engstrom, B., Peura, G. D., Badger, G. J., &
Johnson, R. J. (2001). The effect of weightbearing and external loading on anterior cruciate
ligament strain. Journal of biomechanics, 34(2), 163-170.
Fukunaga, T., Miyatani, M., Tachi, M., Kouzaki, M., Kawakami, Y., & Kanehisa, H. (2001). Muscle
volume is a major determinant of joint torque in humans. Acta Physiologica Scandinavica,
172(4), 249-255.
Garhammer, J. (1993). A review of power output studies of Olympic and powerlifting: Methodology,
performance prediction, and evaluation tests. The Journal of Strength & Conditioning
Research, 7(2), 76-89.
Gentil, P., Oliveira, E., Junior, V. D. A. R., do Carmo, J., & Bottaro, M. (2007). Effects of exercise
order on upper-body muscle activation and exercise performance. The Journal of Strength &
Conditioning Research, 21(4), 1082-1086.
Gottschalk, F, Kourosh, S., & Leveau, B. (1989). The functional anatomy of tensor fasciae latae and
gluteus medius and minimus. Journal of anatomy, 166, 179.

Reg Num: 115554 Gluteal Activation Warm Up 53
Granit, R., Phillips, C. G., Skoglund, S., & Steg, G. (1957). Differentiation of tonic from phasic alpha
ventral horn cells by stretch, pinna and crossed extensor reflexes. Journal of neurophysiology,
20(5), 470-481.
Gravel, D., Bélanger, A. Y., & Richards, C. L. (1987). Study of human muscle contraction using
electrically evoked twitch responses during passive shortening and lengthening movements.
European journal of applied physiology and occupational physiology, 56(6), 623-627.
Griffin, L. Y., Agel, J., Albohm, M. J., Arendt, E. A., Dick, R. W., Garrett, W. E., ... & Wojtys, E. M.
(2000). Noncontact anterior cruciate ligament injuries: risk factors and prevention strategies.
Journal of the American Academy of Orthopaedic Surgeons, 8(3), 141-150.
Griffin, L. Y., Albohm, M. J., Arendt, E. A., Bahr, R., Beynnon, B. D., DeMaio, M., & Yu, B.
(2006). Understanding and Preventing Noncontact Anterior Cruciate Ligament Injuries A
Review of the Hunt Valley II Meeting, January 2005. The American journal of sports
medicine, 34(9), 1512-1532.
Grimaldi, A. (2011). Assessing lateral stability of the hip and pelvis. Manual therapy, 16(1), 26-32.
Güllich, A., & Schmidtbleicher, D. (1996). MVC-induced short-term potentiation of explosive force.
Guskiewicz, K., Lephart, S., Burkholder, R., 1993. The relationship between sprint speed and hip
flexion/extension strength in collegiate athletes. Isokinetics and Exercise Science 3, 111–116.

Reg Num: 115554 Gluteal Activation Warm Up 54
Häkkinen, K., Alen, M., & Komi, P. V. (1985). Changes in isometric force‐ and relaxation‐ time,
electromyographic and muscle fibre characteristics of human skeletal muscle during strength
training and detraining. Acta physiologica scandinavica, 125(4), 573-585.
Häkkinen, K., & Komi, P. V. (1986). Training-induced changes in neuromuscular performance under
voluntary and reflex conditions. European journal of applied physiology and occupational
physiology, 55(2), 147-155.
Hakkinen, K., Pakarinen, A., Alen, M., Kauhanen, H., & Komi, P. V. (1988). Neuromuscular and
hormonal adaptations in athletes to strength training in two years. Journal of Applied
Physiology, 65(6), 2406-2412.
Haff, G. G., Stone, M. H., O’Bryant, H.S., Harman, C. N,. Dinan, R.. Johnson., & HAN, K. H.
(1997). Force-time dependent characteristics of dynamic and isometric muscle actions.
Journal of Strength and Conditioning Research, 11(4), 269-72
Heller, B. M., & Pincivero, D. M. (2003). The effects of ACL injury on lower extremity activation
during closed kinetic chain exercise. Journal of sports medicine and physical fitness, 43(2),
180.
Hermens, H. J., Freriks, B., Disselhorst-Klug, C., & Rau, G. (2000). Development of
recommendations for SEMG sensors and sensor placement procedures. Journal of
electromyography and Kinesiology, 10(5), 361-374.

Reg Num: 115554 Gluteal Activation Warm Up 55
Hewett, T. E., Myer, G. D., Ford, K. R., Heidt, R. S., Colosimo, A. J., McLean, S. G., ... & Succop, P.
(2005). Biomechanical measures of neuromuscular control and valgus loading of the knee
predict anterior cruciate ligament injury risk in female athletes A prospective study. The
American journal of sports medicine, 33(4), 492-501.
Hislop, H. J., & Daniels, M. J. (2007). Worthingham's Muscle Testing: Techniques of Manual
Examination. St Louis, MO: Saunders.
Hodgson, M., Docherty, D., & Robbins, D. (2005). Post-activation potentiation. Sports Medicine,
35(7), 585-595.
Hoffman, J. R., Cooper, J., Wendell, M., & Kang, J. (2004). Comparison of Olympic vs. traditional
power lifting training programs in football players. The Journal of Strength & Conditioning
Research, 18(1), 129-135.
Holmberg, P. M. (2009). Agility training for experienced athletes: A dynamical systems approach.
Strength & Conditioning Journal, 31(5), 73-78.
Hopkins, W. G. (2000). Measures of reliability in sports medicine and science. Sports medicine,
30(1), 1-15.

Reg Num: 115554 Gluteal Activation Warm Up 56
Hopkins, W. G. (2008). Research designs: choosing and fine-tuning a design for your study.
Sportscience, 12(1), 1-3.
Hopkins, W., Marshall, S., Batterham, A., & Hanin, J. (2009). Progressive statistics for studies in
sports medicine and exercise science. Medicine+ Science in Sports+ Exercise, 41(1), 3.
Hori, N., Newton, R. U., Nosaka, K., & McGuigan, M. R. (2006). Comparison of Different Methods
of Determining Power Output in Weightlifting Exercises. Strength & Conditioning Journal,
28(2), 34-40.
Horsman, M. K., Koopman, H. F. J. M., Van der Helm, F. C. T., Prosé, L. P., & Veeger, H. E. J.
(2007). Morphological muscle and joint parameters for musculoskeletal modelling of the
lower extremity. Clinical biomechanics, 22(2), 239-247.
Hunter, J. P., Marshall, R. N., & McNair, P. J. (2005). Relationships between ground reaction force
impulse and kinematics of sprint-running acceleration. J Appl Biomech, 21(1), 31-43.
Ikai, M., & Fukunaga, T. (1968). Calculation of muscle strength per unit cross-sectional area of
human muscle by means of ultrasonic measurement. Internationale Zeitschrift fuer
Angewandte Physiologie Einschliesslich Arbeitsphysiologie, 26(1), 26-32.
Ireland, M. L. (1999). Anterior cruciate ligament injury in female athletes: epidemiology. Journal of
Athletic Training, 34(2), 150.

Reg Num: 115554 Gluteal Activation Warm Up 57
Izquierdo, M., Häkkinen, K., Gonzalez-Badillo, J. J., Ibanez, J., & Gorostiaga, E. M. (2002). Effects
of long-term training specificity on maximal strength and power of the upper and lower
extremities in athletes from different sports. European Journal of Applied Physiology, 87(3),
264-271.
Jan, S. V. S. (2005). Introducing anatomical and physiological accuracy in computerized
anthropometry for increasing the clinical usefulness of modeling systems. Critical Reviews™
in Physical and Rehabilitation Medicine, 17(4).
Jull, G., Hodges, P., Hides, J., & Panjabi, M. M. (1999). Therapeutic exercise for spinal segmental
stabilization in low back pain: scientific basis and clinical approach (pp. 61-76). Edinburgh:
Churchill Livingstone.
Júnior, R., Valdinar, A., Bottaro, M., Pereira, M. C., Andrade, M. M., Júnior, P., ... & Carmo, J. C.
(2010). Electromyographic analyses of muscle pre-activation induced by single joint exercise.
Brazilian Journal of Physical Therapy, 14(2), 158-165.
Kankaanpää, M., Taimela, S., Laaksonen, D., Hänninen, O., & Airaksinen, O. (1998). Back and hip
extensor fatigability in chronic low back pain patients and controls. Archives of physical
medicine and rehabilitation, 79(4), 412-417.

Reg Num: 115554 Gluteal Activation Warm Up 58
Kawamori, N., Crum A. J., Blumert, P. A., Kulik, J. R., Childers, J. T., Wood, J. A., & Haff, G. G.
(2005). Influence of different relative intensities on power output during the hang power
clean: identification of the optimal load. The Journal of Strength & Conditioning Research,
19(3), 698-708.
Kellis, E., & Baltzopoulos, V. (1996). The effects of normalization method on antagonistic activity
patterns during eccentric and concentric isokinetic knee extension and flexion. Journal of
Electromyography and Kinesiology, 6(4), 235-245.
Kernell, D. (1965). The limits of firing frequency in cat lumbosacral motoneurones possessing
different time course of after hyper polarization. Acta Physiologica Scandinavica, 65(1‐ 2),
87-100.
Kernell, D. (1966). Input resistance, electrical excitability, and size of ventral horn cells in cat spinal
cord. Science, 152(3729), 1637-1639.
Kilduff, L. P., Bevan, H. R., Kingsley, M. I., Owen, N. J., Bennett, M. A., Bunce, P. J., ... &
Cunningham, D. J. (2007). Postactivation potentiation in professional rugby players: optimal
recovery. The Journal of Strength & Conditioning Research, 21(4), 1134-1138.
Kitago, T., Mazzocchio, R., Liuzzi, G., & Cohen, L. G. (2004). Modulation of H-reflex excitability by
tetanic stimulation. Clinical neurophysiology, 115(4), 858-861.

Reg Num: 115554 Gluteal Activation Warm Up 59
Knudson, D. V. (2011). Authorship, and sampling practice in selected biomechanics and sports
science journals. Perceptual and motor skills, 112(3), 838-844.
Knutson, L. M., Soderberg, G. L., Ballantyne, B. T., & Clarke, W. R. (1994). A study of various
normalization procedures for within day electromyographic data. Journal of
Electromyography and Kinesiology, 4(1), 47-59.
Konrad, P. (2005). The abc of emg. A practical introduction to kinesiological electromyography, 1
Krosshaug, T., Slauterbeck, J. R., Engebretsen, L., & Bahr, R. (2007). Biomechanical analysis of
anterior cruciate ligament injury mechanisms: three‐ dimensional motion reconstruction
from video sequences. Scandinavian journal of medicine & science in sports, 17(5), 508-519.
Kukulka, C. G., & Clamann, H. P. (1981). Comparison of the recruitment and discharge properties of
motor units in human brachial biceps and adductor pollicis during isometric contractions.
Brain research, 219(1), 45-55.
Kunz, H., Kauffman, D.A., (1981). Biomechanical analysis of sprinting: decathletes versus
champions. British Journal of Sports Medicine 15, 177–181.

Reg Num: 115554 Gluteal Activation Warm Up 60
Kuiken, T. A., Lowery, M. M., & Stoykov, N. S. (2003). The effect of subcutaneous fat on
myoelectric signal amplitude and cross-talk. Prosthetics and orthotics international, 27(1),
48-54.
Kyröläinen, H., Avela, J., & Komi, P. V. (2005). Changes in muscle activity with increasing running
speed. Journal of sports sciences, 23(10), 1101-1109.
Leinonen, V., Kankaanpää, M., Airaksinen, O., & Hänninen, O. (2000). Back and hip extensor
activities during trunk flexion/extension: effects of low back pain and rehabilitation. Archives
of physical medicine and rehabilitation, 81(1), 32-37.
Lieberman, D. E., Raichlen, D. A., Pontzer, H., Bramble, D. M., & Cutright-Smith, E. (2006). The
human gluteus maximus and its role in running. Journal of Experimental Biology, 209(11),
2143-2155.
Mann, R. (1986). The biomechanical analysis of sprinters. Track Technique, 94, 3000-3003.
Maclure, M. (1991). The case-crossover design: a method for studying transient effects on the risk of
acute events. American journal of epidemiology, 133(2), 144-153.
Markolf, K. L., Burchfield, D. M., Shapiro, M. M., Shepard, M. F., Finerman, G. A., Slauterbeck, J.
L. (1995). Combined knee loading states that generate high anterior cruciate ligament forces.
Journal of Orthopedic Research, (13), 930-935.

Reg Num: 115554 Gluteal Activation Warm Up 61
McLean, S. G., Huang, X., Su, A., & Van Den Bogert, A. J. (2004). Sagittal plane biomechanics
cannot injure the ACL during sidestep cutting. Clinical biomechanics, 19(8), 828-838.
McLean, S. G., Walker, K. B., & Van Den Bogert, A. J. (2005). Effect of gender on lower extremity
kinematics during rapid direction changes: an integrated analysis of three sports movements.
Journal of Science and Medicine in Sport, 8(4), 411-422.
McNair, P. J., Marshall, R. N., & Matheson, J. A. (1990). Important features associated with acute
anterior cruciate ligament injury. The New Zealand medical journal, 103(901), 537-539.
Meir, R., Colla, P., & Milligan, C. (2001). Impact of the 10-meter rule change on professional rugby
league: Implications for training. Strength & Conditioning Journal, 23(6), 42-46.
Mero, A., & Komi, P. V. (1994). EMG, force, and power analysis of sprint-specific strength exercises.
Journal of Applied Biomechanics, 10, 1-1.
Mesin, L., Merletti, R., & Rainoldi, A. (2009). Surface EMG: the issue of electrode location. Journal
of Electromyography and Kinesiology, 19(5), 719-726.
Mills, E. J., Chan, A. W., Wu, P., Vail, A., Guyatt, G. H., & Altman, D. G. (2009). Design, analysis,
and presentation of crossover trials. Trials, 10(1), 27.

Reg Num: 115554 Gluteal Activation Warm Up 62
Milner Brown, H. S., Stein, R. B., & Yemm, R. (1973). The contractile properties of human motor
units during voluntary isometric contractions. The Journal of physiology, 228(2), 285-306.
Moss, B. M., Refsnes, P. E., Abildgaard, A., Nicolaysen, K., & Jensen, J. (1997). Effects of maximal
effort strength training with different loads on dynamic strength, cross-sectional area, load-
power and load-velocity relationships. European journal of applied physiology and
occupational physiology, 75(3), 193-199.
Murphy, A. J., Lockie, R. G., & Coutts, A. J. (2003). Kinematic determinants of early acceleration in
field sport athletes. Journal of sports science & medicine, 2(4), 144.
Mustard, B. E., & Lee, R. G. (1987). Relationship between EMG patterns and kinematic properties for
flexion movements at the human wrist. Experimental Brain Research, 66(2), 247-256.
Muthuraman, M., Raethjen, J., Hellriegel, H., Deuschl, G., & Heute, U. (2008, August). Imaging
coherent sources of tremor related EEG activity in patients with Parkinson's disease. In
Engineering in Medicine and Biology Society, 2008. EMBS 2008. 30th Annual International
Conference of the IEEE (pp. 4716-4719). IEEE.
Nagano, A., Komura, T., Fukashiro, S., & Himeno, R. (2005). Force, work and power output of lower
limb muscles during human maximal-effort countermovement jumping. Journal of
Electromyography and Kinesiology, 15(4), 367-376.

Reg Num: 115554 Gluteal Activation Warm Up 63
Narici, M. V., Binzoni, T., Hiltbrand, E., Fasel, J., Terrier, F., & Cerretelli, P. (1996). In vivo human
gastrocnemius architecture with changing joint angle at rest and during graded isometric
contraction. The Journal of Physiology, 496(1), 287-297.
Nelson-Wong, E., Gregory, D. E., Winter, D. A., & Callaghan, J. P. (2008). Gluteus medius muscle
activation patterns as a predictor of low back pain during standing. Clinical Biomechanics,
23(5), 545-553.
Nelson-Wong, E., Flynn, T., & Callaghan, J. P. (2009). Development of active hip abduction as a
screening test for identifying occupational low back pain. journal of orthopaedic & sports
physical therapy, 39(9), 649-657.
Neumann, D. A. (2010). Kinesiology of the hip: a focus on muscular actions. journal of orthopaedic
& sports physical therapy, 40(2), 82-94.
Newton, R. U., & Kraemer, W. J. (1994). Developing explosive muscular power: Implications for a
mixed methods training strategy. Strength & Conditioning Journal, 16(5), 20-31.
Neptune, R. R. (1999). Optimization algorithm performance in determining optimal controls in human
movement analyses. Journal of biomechanical engineering, 121(2), 249-252.

Reg Num: 115554 Gluteal Activation Warm Up 64
Nordander, C., Willner, J., Hansson, G. Å., Larsson, B., Unge, J., Granquist, L., & Skerfving, S.
(2003). Influence of the subcutaneous fat layer, as measured by ultrasound, skinfold calipers
and BMI, on the EMG amplitude. European journal of applied physiology, 89(6), 514-519.
Oliver, G. D., & Keeley, D. W. (2010). Gluteal muscle group activation and its relationship with
pelvis and torso kinematics in high-school baseball pitchers. The Journal of Strength &
Conditioning Research, 24(11), 3015-3022.
Olsen, O. E., Myklebust, G., Engebretsen, L., & Bahr, R. (2004). Injury mechanisms for anterior
cruciate ligament injuries in team handball a systematic video analysis. The American journal
of sports medicine, 32(4), 1002-1012.
Pandy, M. G., & Zajac, F. E. (1991). Optimal muscular coordination strategies for jumping. Journal
of biomechanics, 24(1), 1-10.
Penfold, L., & Jenkins, D. (1996). Training for speed. Training for speed and endurance, 24-41.
Person, R. S., & Kudina, L. P. (1972). Discharge frequency and discharge pattern of human motor
units during voluntary contraction of muscle. Electroencephalography and clinical
neurophysiology, 32(5), 471-483.
Petering, R. C., & Webb, C. (2011). Treatment options for low back pain in athletes. Sports Health: A
Multidisciplinary Approach, 3(6), 550-555.

Reg Num: 115554 Gluteal Activation Warm Up 65
Pick, J., & Becque, M. D. (2000). The relationship between training status and intensity on muscle
activation and relative submaximal lifting capacity during the back squat. The Journal of
Strength & Conditioning Research, 14(2), 175-181.
Powell, J. W., & Barber-Foss, K. D. (2000). Sex-related injury patterns among selected high school
sports. The American journal of sports medicine, 28(3), 385-391.
Powers, C. M. (2010). The influence of abnormal hip mechanics on knee injury: a biomechanical
perspective. journal of orthopaedic & sports physical therapy, 40(2), 42-51.
Rainoldi, A., Melchiorri, G., & Caruso, I. (2004). A method for positioning electrodes during surface
EMG recordings in lower limb muscles. Journal of neuroscience methods, 134(1), 37-43.
Reilly, T. (1996) Motion analysis and physiological demands. In: Science and Soccer. Ed: Reilly, T.
E & F.N. Spon, London, 65-81.
Reilly, T. (1997). Energetics of high-intensity exercise (soccer) with particular reference to fatigue.
Journal of sports sciences, 15(3), 257-263.
Reiman, M. P., Bolgla, L. A., & Lorenz, D. (2009). Hip function's influence on knee dysfunction: a
proximal link to a distal problem. Journal of sport rehabilitation, 18(1), 33.
Reg Num: 115554 Gluteal Activation Warm Up 66
Reiman, M. P., Bolgla, L. A., & Loudon, J. K. (2012). A literature review of studies evaluating
gluteus maximus and gluteus medius activation during rehabilitation exercises. Physiotherapy
theory and practice, 28(4), 257-268.
Rienzi, E., Drust, B., Reilly, T., Carter, J. E. L. & Martin, A. (2000). Investigation of anthropometric
and work-rate profiles of elite South American international soccer players. Journal of Sports
Medicine and Physical Fitness 40, 162-169.
Schmidtbleicher, D., & Buehrle, M. (1987). Neuronal adaptation and increase of cross-sectional area
studying different strength training methods. Biomechanics XB, 6, 615-620.
Schmitz, R. J., Riemann, B. L., & Thompson, T. (2002). Gluteus medius activity during isometric
closed-chain hip rotation. Journal of Sport Rehabilitation, 11(3), 179-189.
Schroter, G. (1998). For Schools and Beginners-Basics of the Sprint Start. Modern Athlete and Coach,
36, 23-26.
Sforzo, G. A., & Touey, P. R. (1996). Manipulating exercise order affects muscular performance
during a resistance exercise training session. The Journal of Strength & Conditioning
Research, 10(1), 20-24.

Reg Num: 115554 Gluteal Activation Warm Up 67
Sleivert, G. G., & Wenger, H. A. (1994). Reliability of measuring isometric and isokinetic peak
torque, rate of torque development, integrated electromyography, and tibial nerve conduction
velocity. Archives of physical medicine and rehabilitation, 75(12), 1315-1321.
Souza, R. B., & Powers, C. M. (2009). Predictors of hip internal rotation during running an
Evaluation of hip strength and femoral structure in women with and without patellofemoral
pain. The American journal of sports medicine, 37(3), 579-587.
Suresh, K. P. (2011). An overview of randomization techniques: An unbiased assessment of outcome
in clinical research. Journal of human reproductive sciences, 4(1), 8.
Thorstensson, A., Karlsson, J., Viitasalo, J. H. T., Luhtanen, P., & Komi, P. V. (1976). Effect of
strength training on EMG of human skeletal muscle. Acta Physiologica Scandinavica, 98(2),
232-236.
Tricoli, V., Lamas, L., Carnevale, R., & Ugrinowitsch, C. (2005). Short-term effects on lower-body
functional power development: weightlifting vs. vertical jump training programs. The Journal
of Strength & Conditioning Research, 19(2), 433-437.
Trimble, M. H., & Harp, S. S. (1998). Postexercise potentiation of the H-reflex in humans. Medicine
and science in sports and exercise, 30(6), 933-941.

Reg Num: 115554 Gluteal Activation Warm Up 68
Tsao, H., & Hodges, P. W. (2007). Immediate changes in feedforward postural adjustments following
voluntary motor training. Experimental brain research, 181(4), 537-546.
Tsao, H., & Hodges, P. W. (2008). Persistence of improvements in postural strategies following motor
control training in people with recurrent low back pain. Journal of Electromyography and
Kinesiology, 18(4), 559-567.
Cutsem, M., Duchateau, J., & Hainaut, K. (1998). Changes in single motor unit behaviour contribute
to the increase in contraction speed after dynamic training in humans. The Journal of
physiology, 513(1), 295-305.
Van Sint Jan, S., & Della Croce, U. (2005). Accurate palpation of skeletal landmark locations: why
standardized definitions are necessary. A proposal. Clinical biomechanics, 20, 659-660.
de Villarreal, E. S. S., González-Badillo, J. J., & Izquierdo, M. (2007). Optimal warm-up stimuli of
muscle activation to enhance short and long-term acute jumping performance. European
journal of applied physiology, 100(4), 393-401.
Westing, S. H., Seger, J. Y., & Thorstensson, A. (1990). Effects of electrical stimulation on eccentric
and concentric torque‐ velocity relationships during knee extension in man. Acta physiologica
scandinavica, 140(1), 17-22.

Reg Num: 115554 Gluteal Activation Warm Up 69
Weyand, P. G., Sternlight, D. B., Bellizzi, M. J., & Wright, S. (2000). Faster top running speeds are
achieved with greater ground forces not more rapid leg movements. Journal of applied
physiology, 89(5), 1991-1999.
Winter, D. A., Prince, F., Frank, J. S., Powell, C., & Zabjek, K. F. (1996). Unified theory regarding
A/P and M/L balance in quiet stance. Journal of neurophysiology, 75(6), 2334-2343.
Withrow, T. J., Huston, L. J., Wojtys, E. M., & Ashton-Miller, J. A. (2006). The effect of an
impulsive knee valgus moment on in vitro relative ACL strain during a simulated jump
landing. Clinical Biomechanics, 21(9), 977-983.
Young, W., & Farrow, D. (2006). A review of agility: Practical applications for strength and
conditioning. Strength & Conditioning Journal, 28(5), 24-29.
Zatsiorsky, V., & Prilutsky, B. (2012). Biomechanics of skeletal muscles. Human Kinetics.
Champaigne, IL.
Reg Num: 115554 Gluteal Activation Warm Up 70
Appendix
Appendix
Appendix 1
Musculoskeletal Modelling Literature Review
Musculoskeletal modelling (MM) systems were first developed by Williams and Seireg,
(1977) and have advanced over the past decades to computer simulations and MM that are
now available in commercial formats, with MM now becoming an integral method of product
design and biomechanics research, an advance greatly due to advances in computer
capabilities and speeds (Delp et al, 1990: Lund, de Zee, Andersen & Rasmussen, 2012).
MM is a biomechanical analysis tool that enables analysis in situations where direct
measurements are inaccessible (Cleather & Bull, 2010), such as collecting in vivo measures
of muscular torque would be inappropriate for an elite population. MM utilises lines of
muscle action, inverse dynamics (ID) and optimization techniques (OT) to estimate
mechanical loading in the form of; joint moments, muscle forces, joint forces for specific
movements or tasks (Horsman et al, 2007: Nagano et al, 2005: Bryanton et al, 2012).
Offering an innovative method of understanding the mechanical loads of individual muscles
within weightlifting, enabling diagnosis of joint moments and muscular forces and the
limiting factors in completion of the exercises (Chiu & Salem, 2006: Flanagan and Salem,
2008). Complete calculation of these variables within a multibody system can establish the
relationship between bone motion and the inter-muscular forces, enabling mechanical

Reg Num: 115554 Gluteal Activation Warm Up 71
dynamic formulation (Erberhard & Schielon, 2006: Unda de Jalon, Losantos & Emparantza,
1987). These formulations produce descriptions of the functions of the musculoskeletal
system (Veeger, Van der Helm, Pronk & Rozendal, 1991), an advantageous tool for a
strength and conditioning coach when striving to maximise muscle torque and subsequent
force output. However a challenge to these MM’s is the complexity of human geometry and
systems, a relevant issue as the geometry of the musculoskeletal system determines the
moment arm of the muscle and therefore joint moment and muscular force in any given
position (Delp et al, 1990), therefore accurate measurement of tendon length and muscle size
and geometry are vital (Horsman et al, 2007), as musculotendon length determines
musculotendon force (Zajac, 1989). Variation in musculoskeletal geometry results in
complication surrounding reliable experimental data collection (Lund et al, 2012).
Complications regarding data collection and specifically the choice of MM pose questions of
best accuracy; the Delp MM (Delph, 1990: Delp et al, 1990: Delp & Loan, 1995) is a widely
used an amalgamation of previous work, this model contains 43 musculotendonous actuators
describing the musculoskeletal geometry and the musculotendonous parameters and lines of
action (Delp et al, 1990). However despite the greater number of muscle lines within the
Delp model, the Horsman model is believed to be a more comprehensive model (Cleather &
Bull, 2010).
Whereas Horsman’s data set is based upon cadaver evidence, employing a complete set of
muscle attachment sites and actuation parameters, joint properties, geometric information and
38 lines of muscle action (Horsman et al, 2007). Due to this, this model offers increased
detail of muscle lines of action (Cleather & Bull, 2010) over the Delp model. Lines of
muscle action represent each individual musculotendinous unit consisting of; origin and
insertion, underlying structures, cross-sectional area and a special awareness of proximity to

Reg Num: 115554 Gluteal Activation Warm Up 72
bone. This increased detail offers a more accurate analysis of the lower extremity (which as
previously mentioned is vital for accurate calculation), as this model was developed from one
consistent dataset no scaling of anatomical variations was needed (Horsman et al, 2007). The
Model developed by Cleather (2010) utilised within this research uses the Horsman model,
chosen due to the increased accuracy and consistency provided by the number of lines of
action and the exact replication of one cadaver.
The use of computers to conduct these calculations have grown in interest from the
development of the first MM software SIMM in the 1990’s to the more complex MM of
today, with three dimensional (3D) MM offering greater accuracy in mapping lines of muscle
actions and movement vectors as the 3D approach accounts for rotation and movements
outside of the sagittal plane (Nagano et al, 2005), considering this methodological feedback a
Vicon MX 3D motion capture device has been chosen. The MM FBB (Cleather & Bull,
2010) the MM is used within this research, FBB interprets the Kinematic data provided by
Vicon MX, EMG and the kinetic data provided by a portable force plate.
One commonly used method of inter-segmental force calculation within MM’s is the
Newton-Euler method (NE) (Nikravesh, 1988), the NE treats the segments of the skeleton as
individual bodies, allowing for all possible translations and rotations, following these
calculation the joint constraints are included in the calculation to allow only the relevant
muscular degrees of freedom, therefore tailoring the geometry and thus results to the
individual subject.

Reg Num: 115554 Gluteal Activation Warm Up 73
The validity of MM results have a high reliance on musculoskeletal geometry, mapping and
uniformity of subject, Dao et al, 2012 highlight the necessity for minimal subject movement
variation to reduce the parameter width of the cohort to enable greater accuracy of
comparison, however this research was conducted on polio patents who have large gait
discrepancies and thus this critique may not be applicable to an elite sporting population, who
despite varying anthropometrics possess similar gaits’. Thus accurate mapping of anatomical
structure and geometry is a material factor in the accuracy of the MM product (Pandy, 2001:
Herzog, 1992: Brand et al, 1994), therefore the use of generic MM for differing populations
may not always be optimal (Blankevoort & Huiskes, 1996). However despite these
limitations, alternative measurements such as computer tomography and magnetic resonance
imaging may be inadequate at capturing data at the frequencies required to capture muscle
contraction velocity and muscle activation, thus the use of ever more accurate MM powered
by faster computers indicates that the use of MM maybe optimal when studying high velocity
movement (Pandy, 2001).
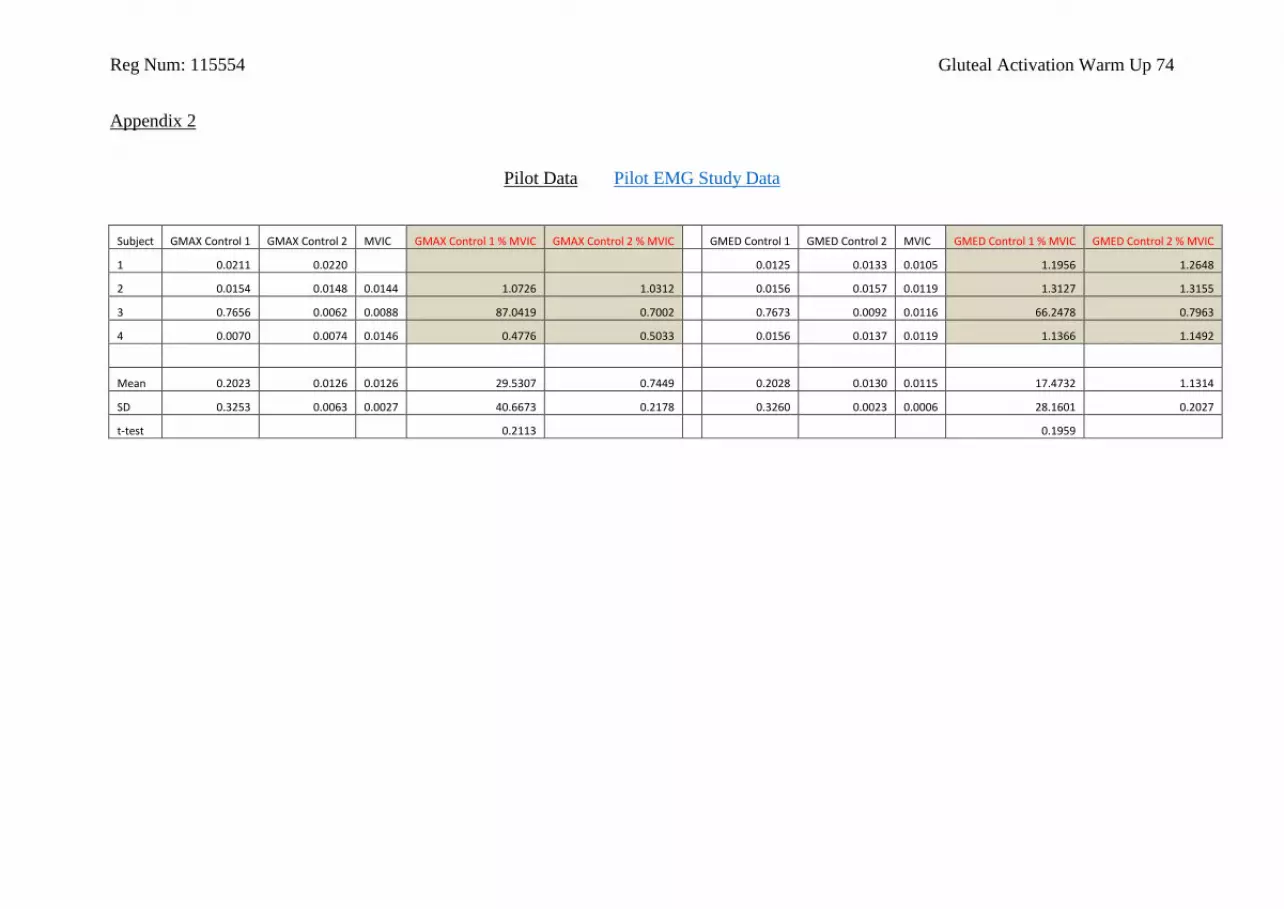
Reg Num: 115554 Gluteal Activation Warm Up 74
Appendix 2
Pilot Data Pilot EMG Study Data
Subject GMAX Control 1 GMAX Control 2 MVIC GMAX Control 1 % MVIC GMAX Control 2 % MVIC GMED Control 1 GMED Control 2 MVIC GMED Control 1 % MVIC GMED Control 2 % MVIC
1 0.0211 0.0220 0.0125 0.0133 0.0105 1.1956 1.2648
2 0.0154 0.0148 0.0144 1.0726 1.0312 0.0156 0.0157 0.0119 1.3127 1.3155
3 0.7656 0.0062 0.0088 87.0419 0.7002 0.7673 0.0092 0.0116 66.2478 0.7963
4 0.0070 0.0074 0.0146 0.4776 0.5033 0.0156 0.0137 0.0119 1.1366 1.1492
Mean 0.2023 0.0126 0.0126 29.5307 0.7449 0.2028 0.0130 0.0115 17.4732 1.1314
SD 0.3253 0.0063 0.0027 40.6673 0.2178 0.3260 0.0023 0.0006 28.1601 0.2027
t-test 0.2113 0.1959

Reg Num: 115554 Gluteal Activation Warm Up 75
Appendix 3
EMG Electrode Placement
GMAX GMED

Reg Num: 115554 Gluteal Activation Warm Up 76
Appendix 4
Vicon Marker Placement
Marker positions used for data capture.
Marker Location
FCC Calcaneus
FMT Tuberosity of the fifth metatarsal
FM2 Head of the second metatarsal
TF Additional marker placed on the foot
FAM Apex of the lateral malleolus
TAM Apex of the medial malleolus
C1, C2, C3 Additional markers placed on the calf segment
FLE Lateral femoral epicondyle
FME Medial femoral epicondyle
T1, T2, T3 Additional markers placed on the thigh segment
RASIS Right anterior superior iliac spine
LASIS Left anterior superior iliac spine
RPSIS Right posterior superior iliac spine
LPSIS Left posterior superior iliac spine

Reg Num: 115554 Gluteal Activation Warm Up 77
Appendix 5
Ethics Forms Ethics Documents

Reg Num: 115554 Gluteal Activation Warm Up 78
Reg Num: 115554 Gluteal Activation Warm Up 79
SCHOOL OF SPORT, HEALTH AND APPLIED SCIENCES (SHAS)
G) RESEARCH / DISSERTATION / PROJECT DECLARATION
In undertaking my Dissertation/ Research Project, I agree to adhere to the approved guidelines and procedures for the protocol I am using
and, inform my supervisor of any necessary changes to my protocol, which may require a revised Dissertation/ Research/ Project Form
DECLARATION SIGNATURE:
Individual undertaing the relevan Research/ Dissertation or Project activity
DATE: 13/01/15

Reg Num: 115554 Gluteal Activation Warm Up 80
School of Sport, Health and Applied Science (SHAS)
PRACTICAL HEALTH AND SAFETY RISK ASSESSMENT FORM (PRA1)
Name of Assessor(s):Matt Parr
Signature(s):Date Signed:
Total number of pages: 7Review date / notes:
15/01/2016 / or immediately in the event of a compulsory update.
SECTION 1: Identify Hazard types - Consider the activity or work area and identify if any of the hazards listed below are significant.
1 Fall of objects 7Heating, ventilation and humidity
13Pressure vessels - autoclave
19Biological hazards – micro-organisms, human samples or non-lab fieldwork
25 Working at heights
2Spillages, slips, Trips & Falls
8Layout , storage, space, obstructions
14 Noise or Vibration 20Fire hazards, flammable materials and explosion
26 Occupational stress
3Manual handling operations including repetitive movements
9 Electrical Equipment 15 Sharps – syringes, blades 21 Handling food 27Violence to staff / verbal assault
4 Display screen equipment 10Physical hazards –electrical, temperature
16Ergometers – rower, treadmill, bikes
22 Vehicles and driving 28Lone working / work out of hours
5 Work in public areas 11 Contractors 17 Ionising and non-ionising radiation
23 Physical Activity 29 Confined spaces
6 Lighting levels 12Mechanical (machinery) and use of portable tools / equipment
18Chemical hazards – toxic, corrosive, flammables
24 Outdoor work 30 Other(s) - specify
Assessment Reference No. 115554Activity assessed:
EMG, Vicon and force plate are used to assess the gluteal
activation levels and force output during the hang high pullAssessment date 15/01/2015Persons who may be affected by the activity (i.e. are at risk)
User and Users of activity assessed
Brief description of activity/procedure
Use of EMG, Vicon and a force plate to assess glutealmuscle activation during the hang high pull.Subjects will undergo a controlled warm up consisting of a general heart rate raising warm up and anintervention warm up specifically targeting the gluteal musculature. Following each warm up subjects will perform 3 hang high pulls at 80%1RM.Finally subjects will undergo GMAX and GMED MVIC testing to provide a comparison measure to assess gluteal activation.
Description of work to be done:
Please tick ( ) the following which applies:
Work to be done in designated areas
Work to be done under close supervision
Work to be done in the presence of at least 2 other workers
Work to be done within normal hours
Work not to be left unattended
15/01/2015

Reg Num: 115554 Gluteal Activation Warm Up 81
Health and Safety Risk Assessments – continuation sheetAssessment Reference No. 115554
Page 2
Name of Assessor(s):Matt Parr
Signature(s):Date Signed:
Total number of pages: 7Review date / notes:
15/01/2016 / or immediately in the event of a compulsory update.
SECTION 2: Risk Controls - For each hazard identified in Section 1, complete Section 2. Please refer to the Risk Assessment Guidance notes on simmsCAPital folder for Risk Matrix. Please note that L refers to Likelihood; S refers to Severity and RS refers to Risk Score (L times S equals RS)
Hazard No.
Outcome due to Hazard description (Substance / equipment / procedure)
L SL X S
= RS
Initial risk Level (tick one)
Refer to the risk matrix Controls needed to eliminate or adequately reduce risks
L SL X S
= RS
Remaining Risk Level
(tick one)
0-5 0-5 0-25High
(13-25)Med
(5-12)Low(0-4)
0-5 0-5 0-25High
(13-25)Med
(5-12)Low(0-4)
1 Fall of objects 4 3 12
Ensure users have received adequatetraining to use equipment.Ensure units are securely connectedto the tripod head and the legs of thetripod provide an adequate base ofsupport for the unit attached. Ensurethe tripod weight is appropriate for theweight of the unit attached.Ensure set up is stable prior tocommencing.
1 3 3
2 Spillages, slips, Trips & Falls 4 3 12Use wire covering and tape to fix wireto floor or suitable safe positioning
1 3 3
3Manual handling operations incl uding repetitive movements
3 3 6
Ensure user is aware of correct handling protocol to set up the system.Provide and refer to Manual Handling Operations guide (HSPG 11).
1 3 3
4 Display screen equipment 2 2 4
Ensure users have received adequatetraining to use the equipment.Ensure the equipment is not adistraction for subjects.Equipment regularly checked toensure correct functioning
1 2 2
6 Lighting levels 4 4 16
Testing area inspected for additionalhazards.Ensure lighting is not too bright ordirectly in participant’s line of vision.Lighting only low when necessary.
2 4 8
15/01/2015
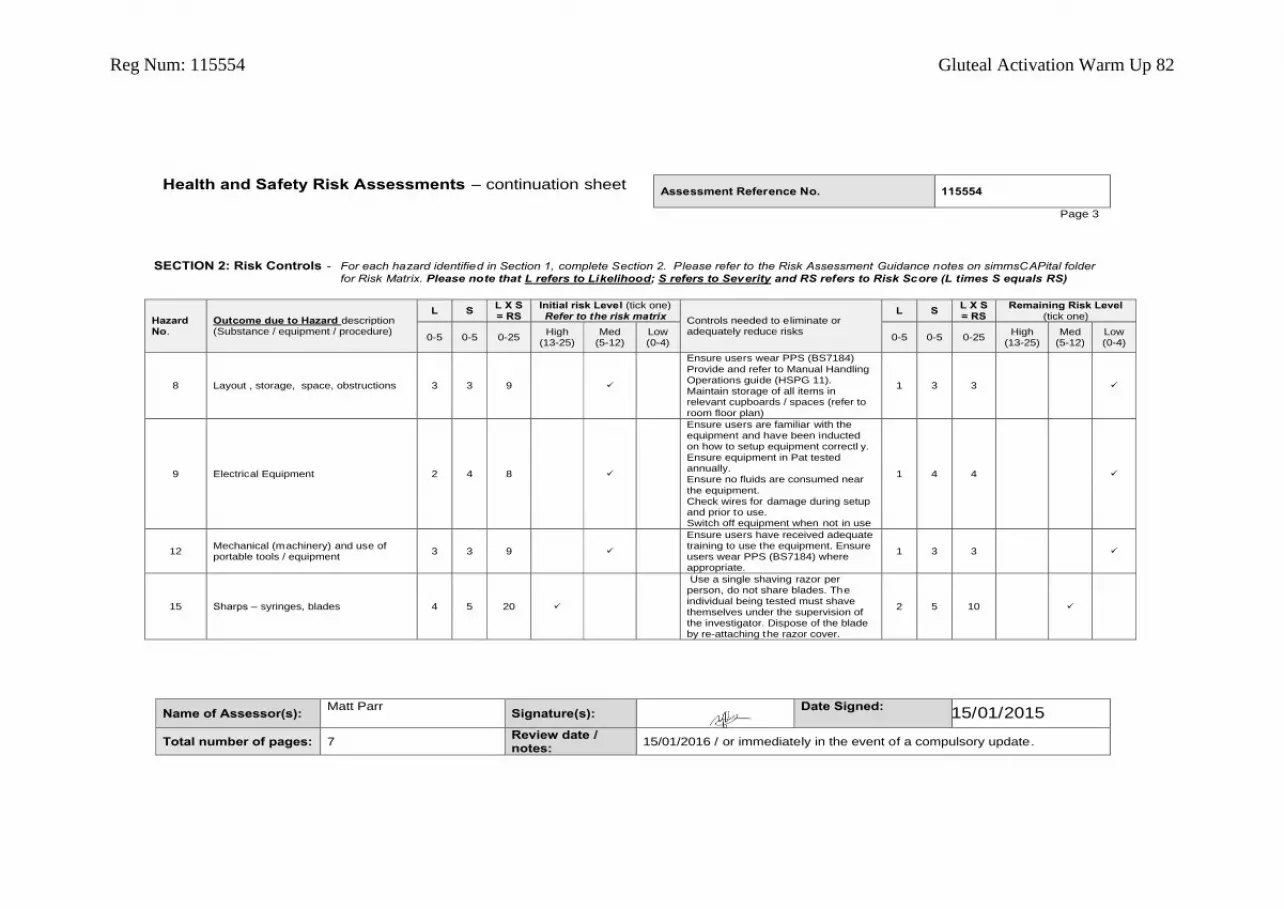
Reg Num: 115554 Gluteal Activation Warm Up 82
Health and Safety Risk Assessments – continuation sheetAssessment Reference No. 115554
Page 3
Name of Assessor(s):Matt Parr
Signature(s):Date Signed:
Total number of pages: 7Review date / notes:
15/01/2016 / or immediately in the event of a compulsory update.
SECTION 2: Risk Controls - For each hazard identified in Section 1, complete Section 2. Please refer to the Risk Assessment Guidance notes on simmsCAPital folder
for Risk Matrix. Please note that L refers to Likelihood; S refers to Severity and RS refers to Risk Score (L times S equals RS)
Hazard No.
Outcome due to Hazard description (Substance / equipment / procedure)
L SL X S = RS
Initial risk Level (tick one)Refer to the risk matrix Controls needed to eliminate or
adequately reduce risks
L SL X S = RS
Remaining Risk Level(tick one)
0-5 0-5 0-25High
(13-25)Med
(5-12)Low(0-4)
0-5 0-5 0-25High
(13-25)Med
(5-12)Low(0-4)
8 Layout , storage, space, obstructions 3 3 9
Ensure users wear PPS (BS7184)
Provide and refer to Manual HandlingOperations guide (HSPG 11).Maintain storage of all items inrelevant cupboards / spaces (refer toroom floor plan)
1 3 3
9 Electrical Equipment 2 4 8
Ensure users are familiar with theequipment and have been inductedon how to setup equipment correctl y.Ensure equipment in Pat testedannually.Ensure no fluids are consumed nearthe equipment.Check wires for damage during setupand prior to use.Switch off equipment when not in use
1 4 4
12Mechanical (machinery) and use of portable tools / equipment
3 3 9
Ensure users have received adequatetraining to use the equipment. Ensureusers wear PPS (BS7184) whereappropriate.
1 3 3
15 Sharps – syringes, blades 4 5 20
Use a single shaving razor perperson, do not share blades. Theindividual being tested must shavethemselves under the supervision ofthe investigator. Dispose of the bladeby re-attaching the razor cover.
2 5 10
15/01/2015

Reg Num: 115554 Gluteal Activation Warm Up 83
Health and Safety Risk Assessments – continuation sheetAssessment Reference No. 115554
Page 4
Name of Assessor(s):Matt Parr
Signature(s):Date Signed:
Total number of pages: 7Review date / notes:
15/01/2016 / or immediately in the event of a compulsory update.
SECTION 2: Risk Controls - For each hazard identified in Section 1, complete Section 2. Please refer to the Risk Assessment Guidance notes on simmsCAPital folder
for Risk Matrix. Please note that L refers to Likelihood; S refers to Severity and RS refers to Risk Score (L times S equals RS)
Hazard No.
Outcome due to Hazard description (Substance / equipment / procedure)
L SL X S = RS
Initial risk Level (tick one)Refer to the risk matrix Controls needed to eliminate or
adequately reduce risks
L SL X S = RS
Remaining Risk Level(tick one)
0-5 0-5 0-25High
(13-25)Med
(5-12)Low(0-4)
0-5 0-5 0-25High
(13-25)Med
(5-12)Low(0-4)
23 Physical Activity 3 4 12
All relevant equipment inspectedand calibrated before the start o fthe testing session. Any faults ormaintenance issues reported to a
member of technical services staff.Ensure the participant is aware ofthe testing protocol and theassociated risks (a wri tten protocolshould be provided).Ensure participant (s) hascompleted and signed an Informedconsent form (refer to Ethics Sub-Committee Suggested Format for aParticipant Consent Form) and(Physical Activity ReadinessQuestionnaire (PARQ)) prior tocommencing any procedure.Ensure students are supervised bya trained member of staff duringmaximal exercise protocols.Ensure student(s) has receivedappropriate training to administerthe protocols.Ensure user performs an adequatewarm-up and cool-down.
1 4 4
15/01/2015

Reg Num: 115554 Gluteal Activation Warm Up 84
Health and Safety Risk Assessments – continuation sheetAssessment Reference No. 115554
Page 5
Name of Assessor(s):Matt Parr
Signature(s):Date Signed:
Total number of pages: 7Review date / notes:
15/01/2016 / or immediately in the event of a compulsory update.
SECTION 3: Action Plan in the event of an emergency - For each hazard identified in Section 2, complete Section 3.
- Please refer to the Risk Assessment Guidance.
Hazard Number
Hazard Description –Substance / equipment /procedure
Action required (describe)
All hazards identified in section 1 Apply relevant First Aid and seek Medical Assistance where appropriate
SECTION 4: Arrangement for supervision and/or monitoring effectivenes s of control- For each hazard identified in Sections 2/3, complete Section 4.
- Please refer to the Risk Assessment Guidance notes.
Hazard No.
Hazard Description –Substance/equipment/procedure
Comments
All hazards identified in section 1Monitoring achieved through pre and post checks, continual supervision by test coordinator and/or separately recruited individual where further supervision is required.
15/05/2015

Reg Num: 115554 Gluteal Activation Warm Up 85
Health and Safety Risk Assessments – continuation sheetAssessment Reference No. 115554
Page 6
Name of Assessor(s):Matt Parr
Signature(s):Date Signed:
Total number of pages: 7Review date / notes:
15/01/2016 / or immediately in the event of a compulsory update.
SECTION 5: Further comments – If a more complex assessment is required, continue below:
IMPORTANT CONTACT DETAILS (including where activities are undertaken off campus):
St Mary’s University Security – 0208 240 4335 (advise in the event of calling the emergency services) Health and Safety Executive (HSE) Information line – 0845 345 0055 / www.HSE.gov.ukBASES (British Association of Sport & Exercise Science) – www.bases.org.ukCroner’s - 0208 547 2637 / www.croner.co.ukCLEAPPS - (0)1895 251496 / http://www.cleapss.org.uk/secfr.htm
GUIDELINES FOR REFFERAL (as a hard copy attachment, listed web link or other source):
(Examples of supporting information could be a Material Safety Data Sheet (MSDS) or a Qualification/Accreditation guideline).
Manual Handling Operations guide (HSPG 11) – see Health and Safety home page on Simms Space (students) or Staff Net (staff)Suggested Format for a Participant Consent Form – see Ethics Sub-Committee home page on Simms Space (students) or Staff Net (staff)Subject Information Sheet – see attachedSchool of SHAS Medical History and-or PARQ Form – see attachedR26 floor plan – See simmsCAPital biomechanics informationGeneral Risk Assessment information and guidance – see Ethics Sub-Committee home page on Simms Space (students) or Staff Net (staff)
15/01/2015

Reg Num: 115554 Gluteal Activation Warm Up 86
Health and Safety Risk Assessments – continuation sheetAssessment Reference No. 115554
Page 7
Name of Assessor(s):Matt Parr
Signature(s):Date Signed:
Total number of pages: 7Review date / notes:
15/01/2016 / or immediately in the event of a compulsory update.
SECTION 6: Period of cover – If a more complex assessment is required, continue below:
By signing this risk assessment I confirm that I have read and understood all of the risks associated with the activity specified on sheet 1, and that I will follow all of the specified controls to reduce the risks identified with the activity.
PERIOD OF COVER FOR TASK/EVENT
PRINT NAME OF TASK/EVENT LEADER SIGNATURE DATE SIGNED HAZARDS IDENTIFIED (mark with a tick or a cross)
FROM TO
15/01/2015

Reg Num: 115554 Gluteal Activation Warm Up 87
Participant Information Sheet
Waldegrave Rd
Twickenham
Greater London
TW1 4SX
Phone: 020 8240 4000
Participant Information Sheet
Research Title:
The Effect of Gluteal Activation Exercise on Gluteus Maximus and Gluteus Medius Recruitment and Force
Output During the Hang High Pull in Elite Rugby Union Players.
Purpose
The purpose of this study is to identify if gluteal muscle activation increases gluteal recruitment and force
output during subsequent exercise, this information will be valuable when designing training programmes
targeting gluteal adaptation.
Invite
You are invited to participate in this research, you do so in the knowledge that you are free to withdraw from
this research at any time and that your details will remain confidential, your anonymity will be respected and
that your legal rights will not be compromised in the event of incident.

Reg Num: 115554 Gluteal Activation Warm Up 88
Funding
Solely the organiser, Matt Parr, funds this research.
Why you
You have been invited to participate in this research, as you are an elite rugby union player at London Irish
Rugby Club, you have the right to refuse participation and can withdraw from this research at any time by
signing the bottom of your consent form “I wish to withdraw from this study”.
Research Method:
You will be asked to perform a control warm up followed by 3 hang high pulls, an intervention warm up
followed by 3 hang high pulls and maximum voluntary isometric contraction testing. During the hang high
pulls and maximum voluntary isometric contraction testing you will be asked to wear electromyography
electrodes and Vicon motion capture markers. Minimal risks are associated with this testing procedure and
everything will be done to minimise any associated risk, you will be performing weightlifting movements
which carry a small risk of injury, however due to a comprehensive warm up the risks have been reduced.
Clothing
Please bring with you tight fitting clothing to make data collection as accurate as possible.
Time demands
The research has been design to take no longer than 4 hours during 1 day of testing.
Print Name:

Reg Num: 115554 Gluteal Activation Warm Up 89
Signed: Date:
Organiser:
Contact Matt Parr for any further details: mobile 07737415422 and Email [email protected]

Reg Num: 115554 Gluteal Activation Warm Up 90
Institution Consent Letter

Reg Num: 115554 Gluteal Activation Warm Up 91
Appendix 6
Actual Testing Protocol Notes
Finding equipment
- Things like synch box, cables, tape, EMG electrodes are in Room 25 (equipment store)
Prepare area
- Arrange lifting boxes, bar and plates
- Put EMG units on floor against the wall
- Connect long Ethernet cable to computer (back bottom right and into the back of the
Biopac boxes
- Set up Physio bed near computers for electrode placement
- Stick all Vicon markers on to sticky tape and cut up
Turn on both computers (Vicon & EMG)
- Turn on all 3 Vicon boxes & other small box (on top and back)
- Turn on EMG Biopac units – check the sliding scale on top correlates to channels
Connect the synch box cables from splitter to EMG units and to Vicon Desktop
- Connect the cables from splitter to the correct ports
- Screw aerial into synch box
Vicon
- Load “Vicon Nexus”
- In “system” select “the pricep”
Cameras
- Highlight all cameras by clicking on press shift and highlight them all
- Now select each camera individually
- Click Paintbrush to get blue screen
- Remove any marks on screen by clicking on the cross icon, then click each mark which
should disappear.
Calibration
- Click “calibrate cameras”
- Move immediately to stand on FP with wand, wave wand around smoothly and at
different height – I must move around as well until all cameras show green lights
- Click stop to stop calibration or look at progress bar at bottom right corner
- Now place triangle marker at the Rear Right corner (when sitting at computer), ensuring
the metal guides are in the groove and its level
- Press “Set volume origin” and then “Set origin”

Reg Num: 115554 Gluteal Activation Warm Up 92
Data storage
- Create name titled folders with Your folder on the D drive
- Press F2 to bring up files
- Select “new database’ & save to the correct folder you created in the D drive
- Find and open the newly created file
- Create new ‘top level’, patient & session for each person with a new session for each trial
- Go back to main Vicon tab
- Click “subjects”
- Click create new subject from model template
- Select Freebody
EMG
On EMG computer load Acqknowledge
- Select the tab “MP150” from toolbar
Choose “setup acquisition”
- Set sample rate at 1000 & acquisition rate at 20,000,000 or 20 seconds
Back to MP150 and select “set up channel”
- Setup 1 channel per muscle and 1 for the synch
- Select analogue and select each tick box
- Label the channels
- Repeat for digital
- Now select “calculations”
- Highlight each channel individually and choose setup
- Ensure the channels match up to the analogue channels
- Choose source, select Average over samples, sample rate = 200, select “rectify”
- Once completed close box to save settings
EMG electrode placement
- Shave areas and clean with alcohol wipes
- Find correct placement (see attached image)
- Use RED electrodes
- Stick on straightaway once off strip
- Place overlapping so that only the metal nipples are 2cm apart - - 2 on GMED and 2 on
GMAX plus 1 on shin as an earth wire.
- Leave on for 5-10 mins before activity begins to allow good connection
Vicon marker placement (see attached image)
- May need to shave some of the marker positions
- Spray marker areas with adhesive spray
- Label markers
Vicon Orientation
- Select the capture button that looks like a “take clapper” (top right)
- Select session and then choose the correct ‘session’ to use as the profile
- Select “Dynamic trail with force”
- Right click on FP & select “zero level” DO THIS FOR EACH SUBJECT
- Subject stands still on FP

Reg Num: 115554 Gluteal Activation Warm Up 93
- Press start and collect 5 sec of data then click stop
Data Collection
- Zero FP
- Select “freebody’ in subject drop down for each subject
- Click start on both EMG (Green button) and Vicon (start)
- Press Red button on small portable black box (looks like a car remote) close before the
start of the lifts.
- Press stop after lifts
Vicon post activity
- On Vicon press F2 to bring the last trial forward
- Select the appropriate session and double click, it will then open in main Vicon tab
- Click on cog wheel (top right) or “pipeline’
- Select reconstruct label
- Click the play button (triangle)
- Select “Tools” then “Pipeline” then Phil March 2012
- Press Play and it is saved
- To find data Select D drive find file then copy and paste it to own storage device
- To begin next dynamic trail click “Go Live”
EMG post activity
- Select “Save As” for every trial one batch of lifts = 1 file
- Save as subjects name or number (uniform)
- Always as 2 separate Acqknowledge and excel files.
MVIC
- Use manual testing protocol (lying)
- Save as both text file and Acqknowledge file
Vicon marker labelling
- Label markers post testing to speed process up.
- Click the labels tag
- Click on each marker and label according to marker map

Reg Num: 115554 Gluteal Activation Warm Up 94
Appendix 7
Graphic illustration of the contrasting FBB and EMG trends
Figure 6. FBB muscular force outputs and EMG recruitment in control and intervention trials
0
0.5
1
1.5
2
2.5
3
3.5
4
GRF Bi Ham GMAX GMED Quad
Fo
rce
(xB
W)
FBB Combined Peak Force Means
Control Intervention
0
10
20
30
40
50
60
70
80
90
100
% M
VIC
GMAX GMED
EMG Peak MU Recruitment
Control Intervention
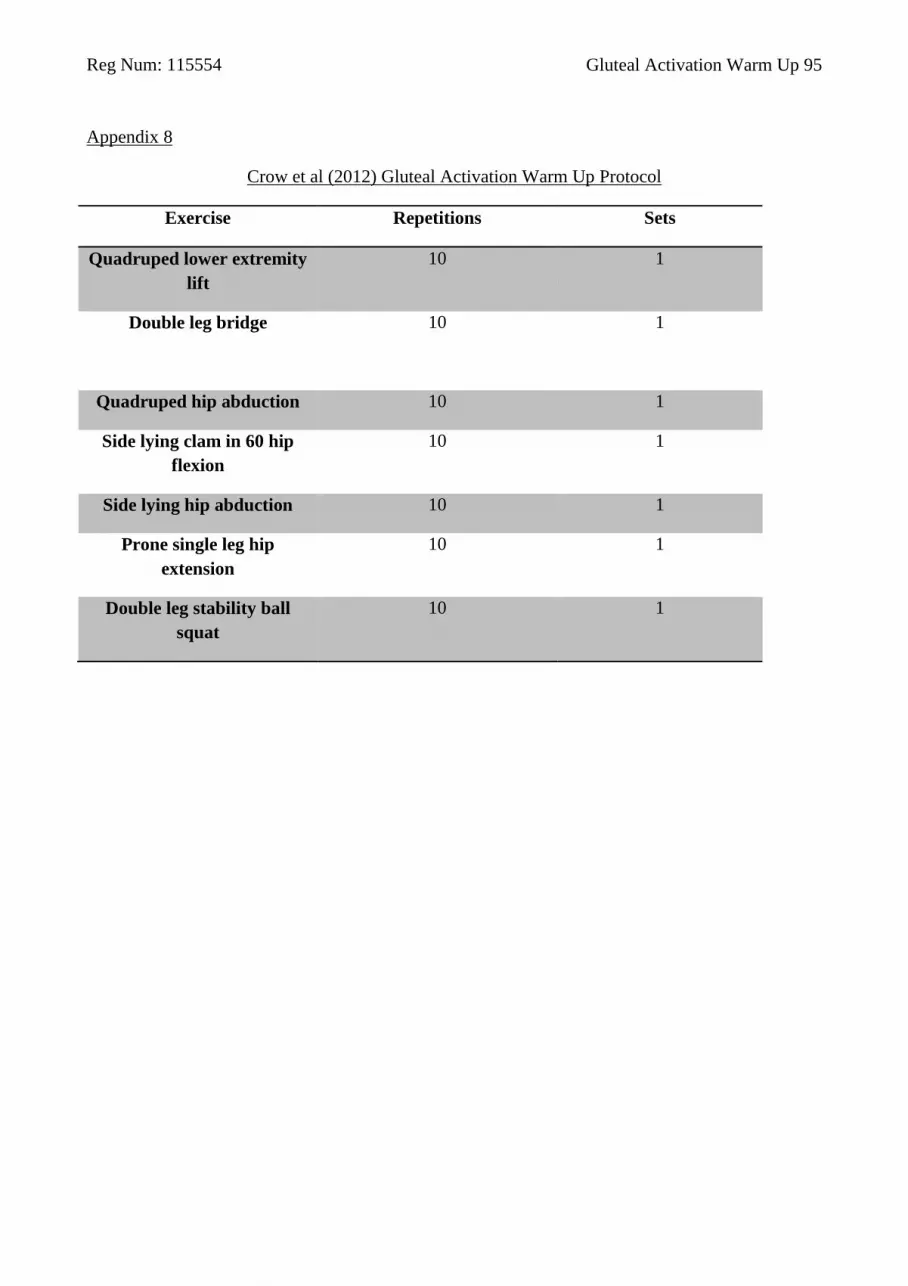
Reg Num: 115554 Gluteal Activation Warm Up 95
Appendix 8
Crow et al (2012) Gluteal Activation Warm Up Protocol
Exercise Repetitions Sets
Quadruped lower extremity
lift
10 1
Double leg bridge
10 1
Quadruped hip abduction 10 1
Side lying clam in 60 hip
flexion
10 1
Side lying hip abduction 10 1
Prone single leg hip
extension
10 1
Double leg stability ball
squat
10 1

Reg Num: 115554 Gluteal Activation Warm Up 96
Raw Data
EMG Cohort Data Part 1 of 4 Dropbox EMG Data
Function Subject Age Height (cm) Bodyweight (kg) Playing Position HHP 1RM HHP 1RM HHP 80%
1 30 195 114 Lock Elite 112.5 90
2 29 183 99 Wing Elite 115 92.5
3 19 185 103 Centre Elite 112.5 90
4 28 178 91 Fly half Int 95 75
5 22 188 101 Flanker Elite 105 85
6 30 193 110 Number 8 Int 105 85
7 24 178 96 Fullback Elite 112.5 90
8 23 185 95 Wing Elite 95 70
9 24 198 113.5 Flanker Int 112.5 90
10 28 185 112 Hooker Elite 125 100
11 28 183 93 Centre Elite 112.5 90
12 29 84 84 Fly half Elite 87.5 70
13 33 196 115 Lock Elite 112.5 90
14 25 194 110 Centre Elite 112.5 90
15 28 193 115.7 Flanker Int 120 95
16 21 182 114.2 Prop Elite 125 100
17 21 178 90.1 Scrum half Elite 95 75
Mean 26 181.0588235 103.3235294 #DIV/0! #DIV/0! 109.1176471 86.91176471
Median 28 185 103 #NUM! #NUM! 112.5 90
SD 3.819454843 25.09856004 10.12745421 #DIV/0! #DIV/0! 10.39446885 8.974203707

Reg Num: 115554 Gluteal Activation Warm Up 97
Part 2 of 4
GMAX MVIC GMED MVIC C Peak GMAX EMG C GMAX % MVIC C GMAX RFD % MVIC Int Peak GMAX EMG
0.00807312 0.024674683 0.01063446 1.31726771 0.000334996 0.010611572
0.019618835 0.03836731 0.008048401 0.410238462 1.72105E-05 0.02385437
0.0257483 0.0303476 0.0160657 0.623951873 3.67198E-05 0.0154276
0.007324219 0.01979126 0.006805725 0.929208333 1.85031E-05 0.006860046
0.017630005 0.035736694 0.015258789 0.865501125 2.71658E-05 0.013472595
0.010074768 0.021425476 0.009997559 0.992336352 2.33647E-05 0.008742371
0.014936829 0.0268307 0.00936798 0.627173294 8.54338E-06 0.00813049
0.014984741 0.040608215 0.013991699 0.933729787 2.49131E-05 0.01340332
0.011097717 0.021717529 0.010538635 0.949621889 3.98283E-05 0.008991394
0.016900024 0.015534363 0.01442749 0.853696414 1.11294E-05 0.010879211
0.0186362 0.0192331 0.0201373 1.080547537 3.06613E-05 0.0158847
0.0141653 0.0161777 0.0147937 1.044361927 1.1823E-05 0.0100766
0.029758606 0.014637756 0.007072754 0.237670874 1.46706E-05 0.007165222
0.015566406 0.034088745 0.010554504 0.678030897 5.35415E-05 0.009526367
0.009766235 0.017823792 0.009041748 0.925817136 2.56894E-05 0.008218079
0.007582703 0.160213013 0.005927734 0.781744275 1.79311E-05 0.006198425
0.005688477 0.009104004 0.010551147 1.854828326 3.4386E-05 0.010723572
0.014561911 0.032135996 0.011365607 0.88857213 4.30045E-05 0.011068584
0.014936829 0.021717529 0.010551147 0.925817136 2.49131E-05 0.0100766
0.006378651 0.033194651 0.003724412 0.346956932 7.3877E-05 0.004227216

Reg Num: 115554 Gluteal Activation Warm Up 98
Part 3 of 4
Int GMAX % MVIC Int GMAX RFD % MVIC C Peak GMED EMG C GMED % MVIC C GMED RFD % MVIC
1.3144326 4.14705E-05 0.018570557 0.752615826 7.77218E-05
1.215891232 1.74301E-05 0.02385437 0.621736848 7.62313E-05
0.599169654 2.56853E-05 0.0268582 0.885018914 4.01982E-05
0.936625 1.57789E-05 0.01340271 0.677203479 3.30985E-05
0.764185563 3.6336E-05 0.026880798 0.752190398 0.000115709
0.867749069 1.6043E-05 0.015126953 0.706026465 4.59408E-05
0.544325051 8.7191E-06 0.0161728 0.602772198 1.57731E-05
0.894464584 2.46234E-05 0.053282166 1.312103108 2.96323E-05
0.810202117 1.81729E-05 0.018608398 0.856837727 5.11359E-05
0.643739391 1.0777E-05 0.023111572 1.487770858 1.04162E-05
0.85235724 3.06633E-05 0.0191083 0.993511186 2.94914E-05
0.711358037 1.16123E-05 0.015387 0.951124078 1.16123E-05
0.240778152 1.34437E-05 0.009720764 0.664088398 5.10794E-05
0.611982434 3.82567E-05 0.013739014 0.403036651 4.54157E-05
0.841478658 3.77356E-05 0.013009644 0.729903262 7.60634E-05
0.81744275 1.77199E-05 0.008578491 0.053544285 4.24347E-05
1.885139485 2.09051E-05 0.010697632 1.175046929 3.92265E-05
0.85596006 2.2669E-05 0.019182904 0.801442977 4.654E-05
0.81744275 1.81729E-05 0.0161728 0.752190398 4.24347E-05
0.350318154 1.02816E-05 0.010099379 0.323939545 2.6449E-05

Reg Num: 115554 Gluteal Activation Warm Up 99
Part 4 of 4
Int Peak GMED EMG Int GMed % MVIC Int GMED RFD % MVIC
0.018527527 0.750871942 4.28621E-05
0.014719849 0.383656003 5.21964E-05
0.024826 0.818054805 4.9055E-05
0.015030212 0.759436872 4.23255E-05
0.021847229 0.611338833 0.000110918
0.014016418 0.654194026 3.93959E-05
0.0155298 0.578807113 1.29292E-05
0.036048279 0.887709014 3.5397E-05
0.016217957 0.746768029 5.7554E-05
0.014848938 0.955876864 2.206E-05
0.0139713 0.726419558 2.46187E-05
0.0145651 0.900319576 7.38129E-05
0.011072998 0.756468258 3.28218E-05
0.020202026 0.592630392 3.31192E-05
0.012684937 0.711685643 6.26335E-05
0.007224731 0.045094536 2.00206E-05
0.008859253 0.973116117 4.85321E-05
0.016481915 0.697202799 4.47207E-05
0.014848938 0.746768029 4.23255E-05
0.00647012 0.217838675 2.2677E-05

Reg Num: 115554 Gluteal Activation Warm Up 100
Adjusted EMG Cohort Dropbox EMG Data
Part 1 of 4
Subject Age Height (cm) Bodyweight (kg) Playing Position HHP 1RM HHP 1RM HHP 80%
Cox 30 195 114 Lock Elite 112.5 90
Fenby 29 183 99 Wing Elite 115 92.5
Gillsennsn 22 188 101 Flanker Elite 105 85
Guest 30 193 110 Number 8 Int 105 85
Homer 24 178 96 Fullback Elite 112.5 90
Lewington 23 185 95 Wing Elite 95 70
Low 24 198 113.5 Flanker Int 112.5 90
Mayhew 28 185 112 Hooker Elite 125 100
Mulchrone 28 183 93 Centre Elite 112.5 90
Smallbone 21 182 114.2 Prop Elite 125 100
Steele 21 178 90.1 Scrum half Elite 95 75
Mean 25.45454545 186.1818182 103.4363636 #DIV/0! #DIV/0! 110.4545455 87.95454545
Median 24 185 101 #NUM! #NUM! 112.5 90
SD 3.420888677 6.336304943 8.96460441 #DIV/0! #DIV/0! 9.523784927 8.71376796

Reg Num: 115554 Gluteal Activation Warm Up 101
Part 2 of 4
GMAX MVIC GMED MVIC C Peak GMAX EMG C GMAX % MVIC C GMAX RFD % MVIC Int Peak GMAX EMG
0.00807312 0.024674683 0.01063446 1.31726771 0.000334996 0.010611572
0.019618835 0.03836731 0.008048401 0.410238462 1.72105E-05 0.02385437
0.017630005 0.035736694 0.015258789 0.865501125 2.71658E-05 0.013472595
0.010074768 0.021425476 0.009997559 0.992336352 2.33647E-05 0.008742371
0.014936829 0.0268307 0.00936798 0.627173294 8.54338E-06 0.00813049
0.014984741 0.040608215 0.013991699 0.933729787 2.49131E-05 0.01340332
0.011097717 0.021717529 0.010538635 0.949621889 3.98283E-05 0.008991394
0.016900024 0.015534363 0.01442749 0.853696414 1.11294E-05 0.010879211
0.0186362 0.0192331 0.0201373 1.080547537 3.06613E-05 0.0158847
0.007582703 0.160213013 0.005927734 0.781744275 1.79311E-05 0.006198425
0.005688477 0.009104004 0.010551147 1.854828326 3.4386E-05 0.010723572
0.013202129 0.037585917 0.011716472 0.969698652 5.18299E-05 0.011899275
0.014936829 0.024674683 0.010551147 0.933729787 2.49131E-05 0.010723572
0.004658514 0.03986366 0.00375784 0.357861754 9.00001E-05 0.004599917

Reg Num: 115554 Gluteal Activation Warm Up 102
Part 3 of 4
Int GMAX % MVIC Int GMAX RFD % MVIC C Peak GMED EMG C GMED % MVIC C GMED RFD % MVIC
1.3144326 4.14705E-05 0.018570557 0.752615826 7.77218E-05
1.215891232 1.74301E-05 0.02385437 0.621736848 7.62313E-05
0.764185563 3.6336E-05 0.026880798 0.752190398 0.000115709
0.867749069 1.6043E-05 0.015126953 0.706026465 4.59408E-05
0.544325051 8.7191E-06 0.0161728 0.602772198 1.57731E-05
0.894464584 2.46234E-05 0.053282166 1.312103108 2.96323E-05
0.810202117 1.81729E-05 0.018608398 0.856837727 5.11359E-05
0.643739391 1.0777E-05 0.023111572 1.487770858 1.04162E-05
0.85235724 3.06633E-05 0.0191083 0.993511186 2.94914E-05
0.81744275 1.77199E-05 0.008578491 0.053544285 4.24347E-05
1.885139485 2.09051E-05 0.010697632 1.175046929 3.92265E-05
0.964539007 2.20782E-05 0.021272003 0.846741439 4.85193E-05
0.85235724 1.81729E-05 0.018608398 0.752615826 4.24347E-05
0.359932193 9.81354E-06 0.011369585 0.37341398 2.94108E-05

Reg Num: 115554 Gluteal Activation Warm Up 103
Part 4 of 4
Int Peak GMED EMG Int GMed % MVIC Int GMED RFD % MVIC
0.018527527 0.750871942 4.28621E-05
0.014719849 0.383656003 5.21964E-05
0.021847229 0.611338833 0.000110918
0.014016418 0.654194026 3.93959E-05
0.0155298 0.578807113 1.29292E-05
0.036048279 0.887709014 3.5397E-05
0.016217957 0.746768029 5.7554E-05
0.014848938 0.955876864 2.206E-05
0.0139713 0.726419558 2.46187E-05
0.007224731 0.045094536 2.00206E-05
0.008859253 0.973116117 4.85321E-05
0.016528298 0.664895639 4.24076E-05
0.014848938 0.726419558 3.93959E-05
0.007253338 0.25598991 2.56115E-05

Reg Num: 115554 Gluteal Activation Warm Up 104
FBB Data Dropbox FBB Data
Part 1 of 3
Function Subject Age Height (cm) Bodyweight (kg) Playing Position HHP 1RM HHP 1RM HHP 80%
1 30 195 114 Lock Elite 112.5 90
2 29 183 99 Wing Elite 115 92.5
3 22 188 101 Flanker Elite 105 85
4 24 178 96 Fullback Elite 112.5 90
5 23 185 95 Wing Elite 95 70
6 24 198 113.5 Flanker Int 112.5 90
7 28 185 112 Hooker Elite 125 100
8 28 183 93 Centre Elite 112.5 90
9 21 182 114.2 Prop Elite 125 100
10 21 178 90.1 Scrum half Elite 95 75
Mean 25 185.5 102.78 111 88.25
Median 24 184 100 112.5 90
SD 3.255764119 6.24899992 9.146671526 9.823441352 9.086390923

Reg Num: 115554 Gluteal Activation Warm Up 105
Part 2 of 3
C GRF C GRF RFD Int GRF Int GRF RFD C Bi Ham Int Bi Ham C GMAX C GMAX RFD
1.7604737 0.026513 9.17E-01 3.06E-01 2.7218488 8.71E-01 1.105637 0.12188
2.00E+00 0.0462876 2.00E+00 4.63E-02 3.1825462 2.72E+00 1.2335675 0.035185
1.46E+00 0.13275 1.46E+00 1.33E-01 1.75E+00 0.30094827 5.53E-01 0.042573
1.7496304 0.034329 2.1719277 0.187166 2.0343548 3.9264207 1.3806079 0.036334
1.62E+00 0.0199 1.84E+00 7.52E-02 3.03E+00 1.93E+00 1.28E+00 0.05265
1.67E+00 0.026513 1.86E+00 7.66E-02 3.27E+00 3.32E+00 2.63E+00 0.1064115
6.45E-01 0.322645 1.79E+00 1.18E-01 9.23E-01 3.28E+00 6.57E-01 0.0127775
1.91E+00 0.314295 1.82E+00 2.98E-02 9.23E-01 4.05E+00 6.99E-01 0.15406
1.77E+00 0.027915 1.53E+00 7.66E-01 2.99E+00 2.40E+00 1.36E+00 0.048075
1.28E+00 0.03050813 2.01E+00 2.76E-01 1.60E+00 3.74E+00 3.29E-01 0.0516694
1.587873283 0.098165573 1.739966194 0.201372815 2.24251863 2.653908085 1.123005025 0.06616154
1.7089494 0.032418565 1.8273488 0.12562 2.3781018 2.9997783 1.16960225 0.0498722
0.370409769 0.114442917 0.340000652 0.207885471 0.867689247 1.220840269 0.61561214 0.042925465

Reg Num: 115554 Gluteal Activation Warm Up 106
Part 3 of 3
Int GMAX Int GMAX RFD C GMED C GMED RFD Int GMED Int GMED RFD C Quad Int Quad
9.23E-01 2.96E-02 5.4672882 0.05958 3.00E+00 1.24E-02 0.40567547 6.59E-03
5.53E-01 3.52E-02 5.68E+00 0.07069 5.47E+00 7.07E-02 2.27E+00 4.06E-01
0.13938573 0.027877 3.43E+00 1.142197 0.25429196 0.082122 1.41E-02 0.33648865
2.3343267 0.214625 2.669167 0.027964 2.1565423 0.076287 2.3840857 2.7966903
1.89E-01 2.76E-02 2.89E+00 0.114313 2.98E+00 5.80E-01 2.38E+00 4.42E+00
1.61E+00 7.62E-02 3.90E+00 0.059579 4.86E+00 1.10E-01 2.38E+00 6.96E-01
8.61E-01 1.23E-01 8.97E-01 0.019726 3.11E+00 3.83E-02 1.76E+00 4.40E+00
3.86E+00 1.93E+00 1.37E+00 0.188527 5.02E+00 3.34E-01 2.91E+00 7.34E+00
1.11E+00 1.38E-01 3.57E+00 0.093726 3.54E+00 4.42E-01 1.89E+00 3.55E+00
1.98E+00 7.26E-02 1.64E+00 0.41004 6.85E+00 1.41E-01 8.94E-01 2.37E+00
1.355423888 0.26733464 3.151090724 0.2186342 3.723376396 0.18872876 1.728946377 2.63226972
1.01503332 0.074419 3.159800005 0.082208 3.3220944 0.095961 2.07978075 2.5825671
1.07916491 0.556596958 1.529502093 0.326404614 1.782347466 0.184086093 0.915338818 2.242945308

Reg Num: 115554 Gluteal Activation Warm Up 107
SPSS Data
SPSS Data
SPSS Outputs
SPSS Outputs
EMG t-tests
GMAX
Paired Samples Test
Paired Differences t df Sig.
(2-
taile
d)
Mean Std.
Deviation
Std. Error
Mean
95% Confidence Interval
of the Difference
Lower Upper
Pai
r 1
Pre
-
Po
st
2.7811437
77
23.7709779
12
5.7653089
86
-
9.4407652
93
15.0030528
47
.48
2
1
6
.636
GMAX Matched EMG Cohort
Paired Samples Test
Paired Differences t df Sig. (2-tailed)
Mean Std. Deviation
Std. Error Mean
95% Confidence Interval of the Difference
Lower Upper
Pair 1
GMAXPre - GMAXPost
.0051596445 .2829784069 .0853211999 -.1849478360
.1952671249 .060 10 .953

Reg Num: 115554 Gluteal Activation Warm Up 108
GMED
Paired Samples Test
Paired Differences t df Sig.
(2-
taile
d)
Mean Std.
Deviation
Std. Error
Mean
95% Confidence
Interval of the
Difference
Lower Upper
Pai
r 1
Pre
-
Po
st
9.6250884
33
18.5142083
87
4.4903551
03
.1059608
55
19.1442160
12
2.14
4
1
6
.048
GMED Matched EMG Cohort
Paired Samples Test
Paired Differences t df Sig. (2-
tailed) Mean Std.
Deviation
Std.
Error
Mean
95% Confidence
Interval of the
Difference
Lower Upper
Pair
1
GMEDPre -
GMEDPost
.18185 .17417 .05252 .06484 .29886 3.463 10 .006

Reg Num: 115554 Gluteal Activation Warm Up 109
RFD
Paired Samples Test
Paired Differences t df Sig. (2-
tailed) Mean Std.
Deviation
Std. Error
Mean
95% Confidence Interval of
the Difference
Lower Upper
Pair
1
PreGRF - GRF RFD
Pre
1.488344837 .457457535 .144660774 1.161099430 1.815590244 10.289 9 .000
Pair
2
PostGRF - GRF
RFD Post
1.538519955 .483807894 .152993490 1.192424637 1.884615273 10.056 9 .000
Pair
3
GRF RFD Pre -
GMED RFD Pre
-.120468627 .356143850 .112622574 -.375238589 .134301335 -1.070 9 .313
Pair
4
GRF RFD Post -
GMED RFD Post
.012644055 .253567966 .080185231 -.168747541 .194035651 .158 9 .878
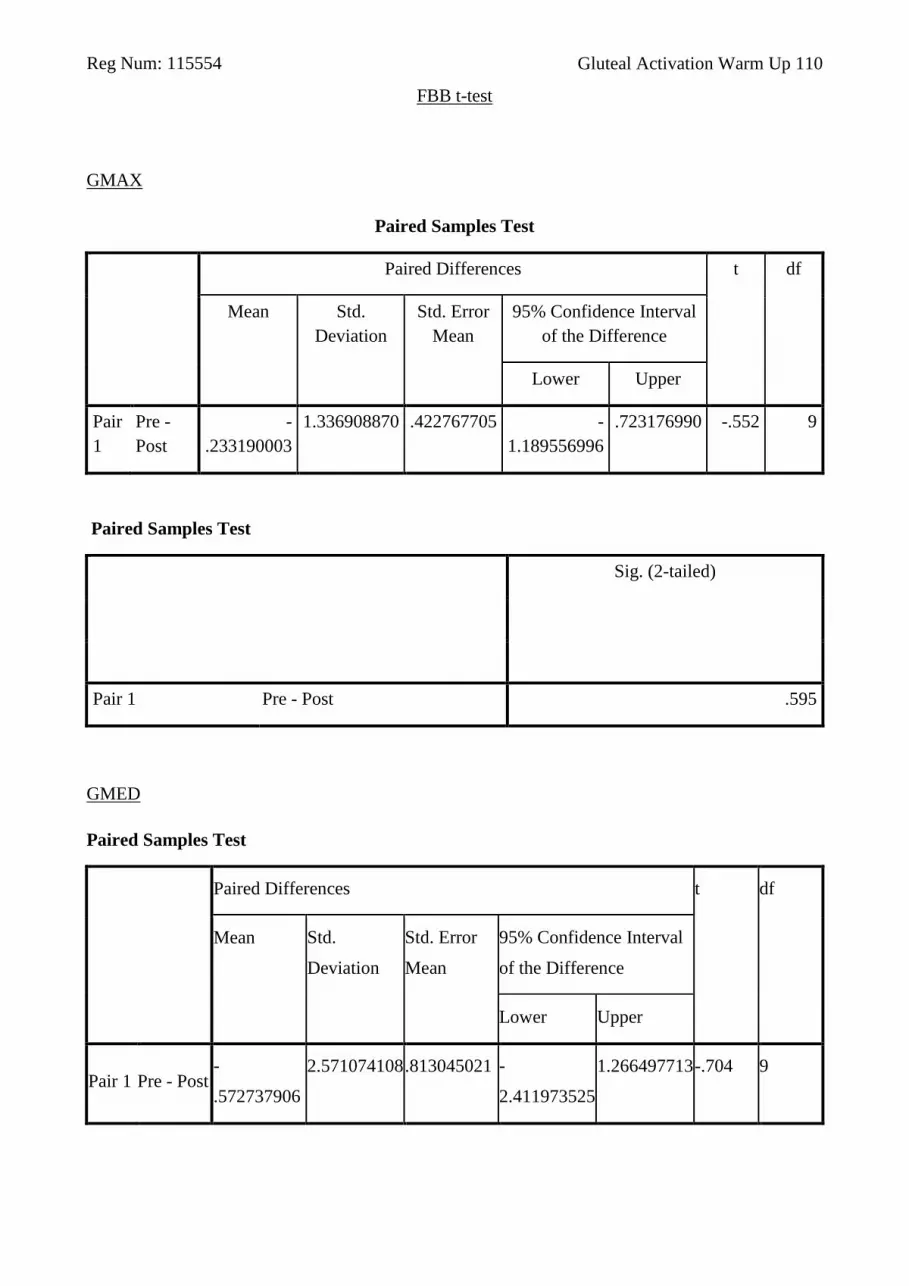
Reg Num: 115554 Gluteal Activation Warm Up 110
FBB t-test
GMAX
Paired Samples Test
Paired Differences t df
Mean Std.
Deviation
Std. Error
Mean
95% Confidence Interval
of the Difference
Lower Upper
Pair
1
Pre -
Post
-
.233190003
1.336908870 .422767705 -
1.189556996
.723176990 -.552 9
Paired Samples Test
Sig. (2-tailed)
Pair 1 Pre - Post .595
GMED
Paired Samples Test
Paired Differences t df
Mean Std.
Deviation
Std. Error
Mean
95% Confidence Interval
of the Difference
Lower Upper
Pair 1 Pre - Post -
.572737906
2.571074108 .813045021 -
2.411973525
1.266497713 -.704 9

Reg Num: 115554 Gluteal Activation Warm Up 111
Paired Samples Test
Sig. (2-tailed)
Pair 1 Pre - Post .499
Bilateral Hamstring
Paired Samples Test
Paired Differences t df
Mean Std.
Deviation
Std. Error
Mean
95% Confidence Interval
of the Difference
Lower Upper
Pair
1
Pre -
Post
-
.411361917
1.798173341 .568632339 -
1.697697635
.874973801 -.723 9
Paired Samples Test
Sig. (2-tailed)
Pair 1 Pre - Post .488

Reg Num: 115554 Gluteal Activation Warm Up 112
Quadriceps
Paired Differences t df
Mean Std.
Deviation
Std. Error
Mean
95% Confidence Interval
of the Difference
Lower Upper
Pair 1 Pre - Post -
.903390778
1.951436087 .617098274 -
2.299364060
.492582504 -1.464 9
Paired Samples Test
Sig. (2-tailed)
Pair 1 Pre - Post .177
GRF
Paired Samples Test
Paired Differences t df
Mean Std.
Deviation
Std. Error
Mean
95% Confidence Interval
of the Difference
Lower Upper
Pair
1
Pre -
Post
-
.153382360
.542488751 .171550006 -
.541455435
.234690715 -.894 9

Reg Num: 115554 Gluteal Activation Warm Up 113
Paired Samples Test
Sig. (2-tailed)
Pair 1 Pre - Post .395
Hip Extension Angle
Paired Samples Test
Paired Differences t df
Mean Std.
Deviation
Std. Error
Mean
95% Confidence Interval
of the Difference
Lower Upper
Pair
1
Pre -
Post
-
.101294000
9.966962062 3.151830147 -
7.231229142
7.028641142 -.032 9
Paired Samples Test
Sig. (2-tailed)
Pair 1 Pre - Post .975
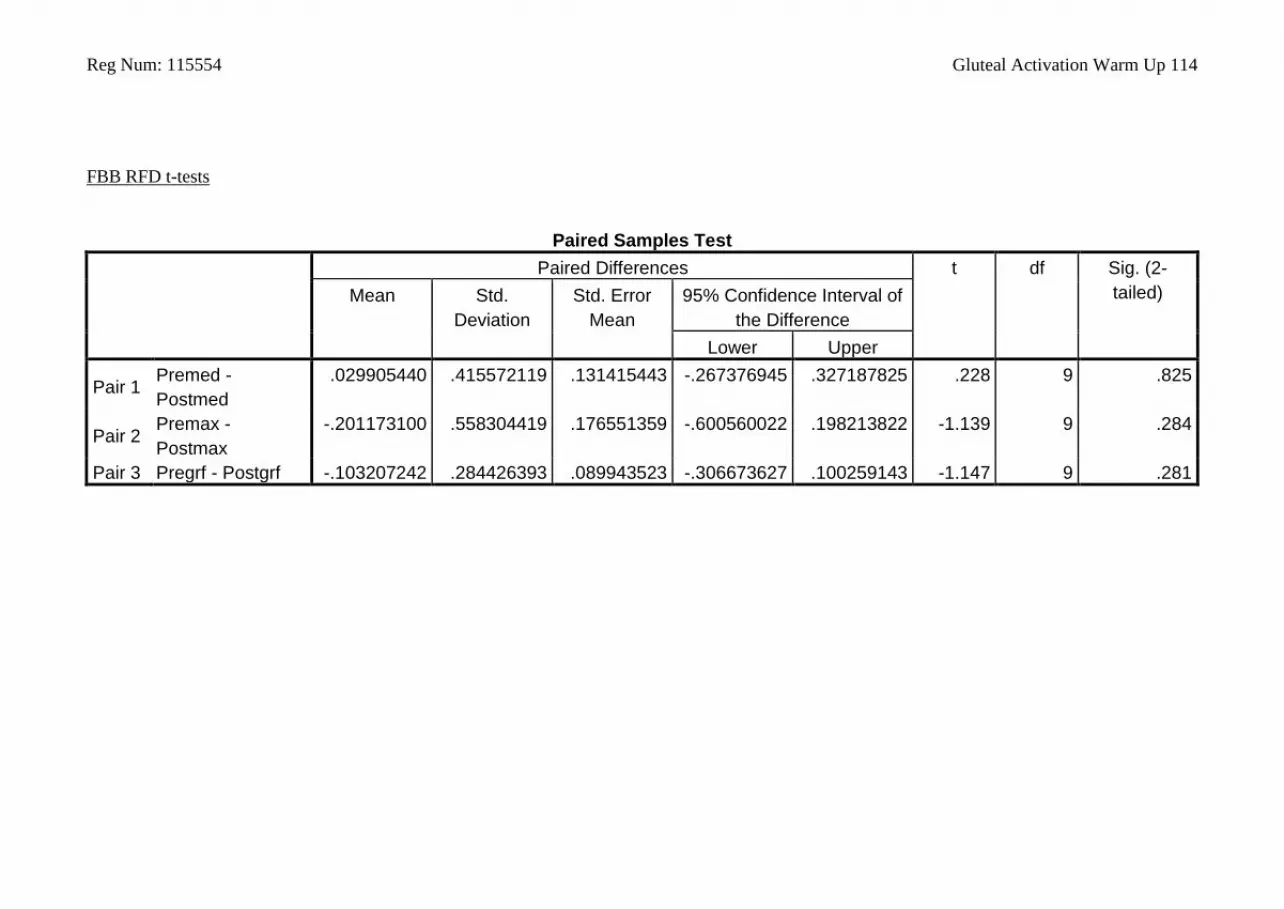
Reg Num: 115554 Gluteal Activation Warm Up 114
FBB RFD t-tests
Paired Samples Test
Paired Differences t df Sig. (2-
tailed) Mean Std.
Deviation
Std. Error
Mean
95% Confidence Interval of
the Difference
Lower Upper
Pair 1 Premed -
Postmed
.029905440 .415572119 .131415443 -.267376945 .327187825 .228 9 .825
Pair 2 Premax -
Postmax
-.201173100 .558304419 .176551359 -.600560022 .198213822 -1.139 9 .284
Pair 3 Pregrf - Postgrf -.103207242 .284426393 .089943523 -.306673627 .100259143 -1.147 9 .281
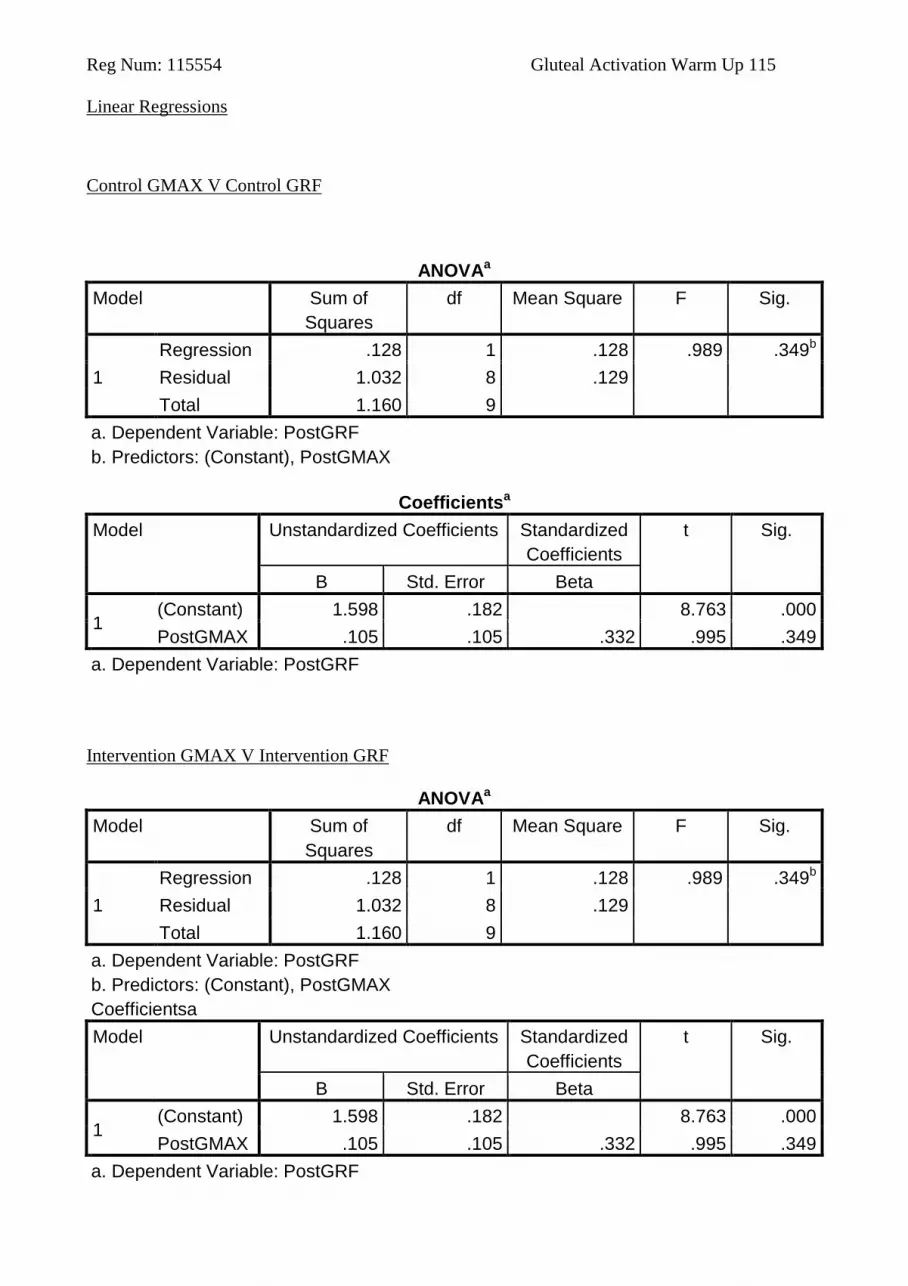
Reg Num: 115554 Gluteal Activation Warm Up 115
Linear Regressions
Control GMAX V Control GRF
ANOVAa
Model Sum of
Squares
df Mean Square F Sig.
1
Regression .128 1 .128 .989 .349b
Residual 1.032 8 .129
Total 1.160 9
a. Dependent Variable: PostGRF
b. Predictors: (Constant), PostGMAX
Coefficientsa
Model Unstandardized Coefficients Standardized
Coefficients
t Sig.
B Std. Error Beta
1 (Constant) 1.598 .182 8.763 .000
PostGMAX .105 .105 .332 .995 .349
a. Dependent Variable: PostGRF
Intervention GMAX V Intervention GRF
ANOVAa
Model Sum of
Squares
df Mean Square F Sig.
1
Regression .128 1 .128 .989 .349b
Residual 1.032 8 .129
Total 1.160 9
a. Dependent Variable: PostGRF
b. Predictors: (Constant), PostGMAX
Coefficientsa
Model Unstandardized Coefficients Standardized
Coefficients
t Sig.
B Std. Error Beta
1 (Constant) 1.598 .182 8.763 .000
PostGMAX .105 .105 .332 .995 .349
a. Dependent Variable: PostGRF

Reg Num: 115554 Gluteal Activation Warm Up 116
Control GMAX RFD V Control GRF RFD
ANOVAa
Model Sum of
Squares
df Mean Square F Sig.
1
Regression .002 1 .002 .127 .731b
Residual .129 8 .016
Total .131 9
a. Dependent Variable: GRF RFD Pre
b. Predictors: (Constant), GMAX RFD Pre
Coefficientsa
Model Unstandardized
Coefficients
Standardized
Coefficients
t Sig.
B Std. Error Beta
1
(Constant) .076 .074 1.032 .332
GMAX RFD
Pre
.333 .935 .125 .356 .731
a. Dependent Variable: GRF RFD Pre
Intervention GMAX RFD V Intervention GRF RFD
ANOVAa
Model Sum of
Squares
df Mean Square F Sig.
1
Regression .025 1 .025 .489 .504b
Residual .407 8 .051
Total .432 9
a. Dependent Variable: GRF RFD Post
b. Predictors: (Constant), GMAX RFD Post
Coefficientsa
Model Unstandardized
Coefficients
Standardized
Coefficients
t Sig.
B Std. Error Beta
1 (Constant) .225 .079 2.847 .022

Reg Num: 115554 Gluteal Activation Warm Up 117
GMAX RFD
Post
-.090 .128 -.240 -.700 .504
a. Dependent Variable: GRF RFD Post
Control GMED V Control GRF
ANOVAa
Model Sum of
Squares
df Mean Square F Sig.
1
Regression .516 1 .516 4.825 .059b
Residual .855 8 .107
Total 1.371 9
a. Dependent Variable: PreGRF
b. Predictors: (Constant), PreGMED
Coefficientsa
Model Unstandardized Coefficients Standardized
Coefficients
t Sig.
B Std. Error Beta
1 (Constant) 1.119 .237 4.727 .001
PreGMED .148 .068 .613 2.197 .059
a. Dependent Variable: PreGRF
Intervention GMED V Intervention GRF
ANOVAa
Model Sum of
Squares
df Mean Square F Sig.
1
Regression .176 1 .176 1.426 .267b
Residual .985 8 .123
Total 1.160 9
a. Dependent Variable: PostGRF
b. Predictors: (Constant), PostGMED
Coefficientsa
Model Unstandardized Coefficients Standardized
Coefficients
t Sig.
B Std. Error Beta

Reg Num: 115554 Gluteal Activation Warm Up 118
1 (Constant) 1.463 .257 5.694 .000
PostGMED .074 .062 .389 1.194 .267
a. Dependent Variable: PostGRF
Control GMED RFD V Control GRF RFD
ANOVAa
Model Sum of
Squares
df Mean Square F Sig.
1
Regression .001 1 .001 .043 .840b
Residual .130 8 .016
Total .131 9
a. Dependent Variable: GRF RFD Pre
b. Predictors: (Constant), GMED RFD Pre
Coefficientsa
Model Unstandardized
Coefficients
Standardized
Coefficients
t Sig.
B Std. Error Beta
1
(Constant) .093 .049 1.905 .093
GMED RFD
Pre
.026 .124 .073 .208 .840
a. Dependent Variable: GRF RFD Pre
Intervention GMED RFD V Intervention GRF RFD
ANOVAa
Model Sum of
Squares
df Mean Square F Sig.
1
Regression .027 1 .027 .539 .484b
Residual .405 8 .051
Total .432 9
a. Dependent Variable: GRF RFD Post
b. Predictors: (Constant), GMED RFD Post
Coefficientsa
Model Unstandardized
Coefficients
Standardized
Coefficients
t Sig.
B Std. Error Beta

Reg Num: 115554 Gluteal Activation Warm Up 119
1
(Constant) .148 .102 1.451 .185
GMED RFD
Post
.284 .386 .251 .734 .484
a. Dependent Variable: GRF RFD Post





























