Embed Size (px)
Citation preview

Docetaxel and Cisplatin With Granulocyte Colony-Stimulating Factor (G-CSF) Versus MVAC With G-CSFin Advanced Urothelial Carcinoma: A Multicenter,Randomized, Phase III Study From the HellenicCooperative Oncology GroupA. Bamias, G. Aravantinos, C. Deliveliotis, D. Bafaloukos, C. Kalofonos, N. Xiros, A. Zervas,D. Mitropoulos, E. Samantas, D. Pectasides, P. Papakostas, D. Gika, C. Kourousis, A. Koutras,C. Papadimitriou, C. Bamias, P. Kosmidis, and M.A. Dimopoulos
A B S T R A C T
PurposeThe combination of methotrexate, vinblastine, doxorubicin, and cisplatin (MVAC) represents thestandard regimen for inoperable or metastatic urothelial cancer, but its toxicity is significant. Wepreviously reported a 52% response rate (RR) using a docetaxel and cisplatin (DC) combination. Thetoxicity of this regimen compared favorably with that reported for MVAC. We thus designed arandomized phase III trial to compare DC with MVAC.
Patients and MethodsPatients with inoperable or metastatic urothelial carcinoma; adequate bone marrow, renal, liver, andcardiac function; and Eastern Cooperative Oncology Group performance status � 2 were randomlyassigned to receive MVAC at standard doses or docetaxel 75 mg/m2 and cisplatin 75 mg/m2 every 3weeks. All patients received prophylactic granulocyte colony-stimulating factor (G-CSF) support.
ResultsTwo hundred twenty patients were randomly assigned (MVAC, 109 patients; DC, 111 patients).Treatment with MVAC resulted in superior RR (54.2% v 37.4%; P � .017), median time to progression(TTP; 9.4 v 6.1 months; P � .003) and median survival (14.2 v 9.3 months; P � .026). After adjusting forprognostic factors, difference in TTP remained significant (hazard ratio [HR], 1.61; P � .005), whereassurvival difference was nonsignificant at the 5% level (HR, 1.31; P � .089). MVAC caused more frequentgrade 3 or 4 neutropenia (35.4% v 19.2%; P � .006), thrombocytopenia (5.7% v 0.9%; P � .046), andneutropenic sepsis (11.6% v 3.8%; P � .001). Toxicity of MVAC was considerably lower than thatpreviously reported for MVAC administered without G-CSF.
ConclusionMVAC is more effective than DC in advanced urothelial cancer. G-CSF–supported MVAC is well toleratedand could be used instead of classic MVAC as first-line treatment in advanced urothelial carcinoma.
J Clin Oncol 22:220-228. © 2004 by American Society of Clinical Oncology
INTRODUCTION
Urothelial cancer is a common malignancyworldwide. The crude incidence in the Eu-ropean Union is 23 cases per 100,000 per-sons per year, and the mortality is 10 casesper 100,000 persons per year. Urinary blad-der is the most common primary site, butthis cancer also originates from the renalpelvis, ureters, urethra, and prostatic ducts.
Prognosis of metastatic or inoperable dis-ease has been improved by the introductionof systemic combination chemotherapy, butit remains poor, with long-term disease-freesurvival less than 5% [1]. The combinationof methotrexate, vinblastine, doxorubicin,and cisplatin (MVAC), developed in 1983[2], is universally considered the standardtreatment, with response rates (RRs) morethan 50%, 3-year survival of 20% to 25%,
From the Departments of Clinical Ther-apeutics, Urology, Hygiene, and Epide-miology, University of Athens School ofMedicine; the Medical Oncology De-partment, Agii Anargyri; Hygia Hospital;the Second Department of InternalMedicine, Evangelismos Hospital; theOncology Department, Ippokration Hos-pital, Athens; the Department of Inter-nal Medicine, University of Patra, Patra;the School of Medicine, Rio; the De-partment of Medical Oncology, Herak-leion University Hospital, Herakleion;and Metaxa Hospital, Piraeus, Greece.
Submitted February 28, 2003; acceptedAugust 13, 2003.
Preliminary analysis presented at the39th American Society of ClinicalOncology Annual Meeting, May 29-June 3, 2003, Chicago, IL.
Authors’ disclosures of potential con-flicts of interest are found at the end ofthis article.
Address reprint requests toAristotle Bamias, MD, 31 Komninon St,Haidari 124 62 Athens, Greece; e-mail:[email protected].
© 2004 by American Society of ClinicalOncology
0732-183X/04/2202-220/$20.00
DOI: 10.1200/JCO.2004.02.152
JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E P O R T
VOLUME 22 � NUMBER 2 � JANUARY 15 2004
220
Downloaded from jco.ascopubs.org on June 2, 2013. For personal use only. No other uses without permission.Copyright © 2004 American Society of Clinical Oncology. All rights reserved.

and median survival past 1 year consistently reported [3-5].Furthermore, MVAC was shown to be superior to single-agent cisplatin [6] and the regimen of cisplatin, cyclophos-phamide, and doxorubicin [7].
Although MVAC has shown considerable efficacy inadvanced urothelial carcinoma, there is still room for im-provement: long-term survival is rare, whereas the toxicityof this combination is significant. Neutropenic sepsis hasbeen reported in more than 10% of patients treated withMVAC [4,6], and it has also been associated with a toxic-death rate of 3% to 4% [6,8]. Myelotoxicity has been shownto be reduced by the routine use of granulocyte colony-stimulating factor (G-CSF) [9] or granulocyte-macrophagecolony-stimulating factor [10]. The use of growth factorsalso allowed for the administration of MVAC in a moredose-dense fashion [11,12]. The results of these phase IIstudies suggested that the efficacy of MVAC might be im-proved by dose intensification. Newer agents, including thetaxanes paclitaxel and docetaxel, have shown promisingsingle-agent efficacy in advanced urothelial cancer [13-15],whereas the combination of paclitaxel with cisplatin andifosfamide produced encouraging efficacy results, withmanageable toxicity [16]. We have recently reported theresults of a phase II study of the combination of docetaxeland cisplatin (DC) as first-line treatment in 66 patients withadvanced urothelial carcinoma [17]. Both agents were ad-ministered at 75 mg/m2 every 3 weeks with G-CSF support.That study showed a 52% RR, with 12% of patients achiev-ing a complete response (CR). Median survival was 8months, which was somewhat inferior to that reported inprevious phase II studies using MVAC. Nevertheless, pa-tients with several adverse baseline characteristics had beenincluded in that study (performance status [PS] 3, age � 75years, administration of previous adjuvant or neoadjuvantchemotherapy), which could account for this result, giventhat median survival � 10 months has been reported forpatients with poor PS after MVAC treatment [6,18,19]. Thetoxicity profile compared favorably with that reported forMVAC, with grade 3 or 4 neutropenia encountered in 33%of patients, only 10 episodes of neutropenic fever in 293 ofcycles administered, and no toxic deaths. Encouraged bythese results, we initiated a randomized, phase III study tocompare directly the efficacy of DC with that of MVAC. Weroutinely used G-CSF with MVAC to decrease the myelo-toxicity of this regimen. We report the results of this study.
PATIENTS AND METHODS
Selection and Randomization
Patients with histologically confirmed inoperable, meta-static, or recurrent (after surgery and/or radiotherapy) carcinomaof the urothelial tract (renal pelvis, ureter, bladder, or urethra)were included in the study. Patients were to be no older than 75years, with adequate bone marrow and liver function (absoluteneutrophil count [ANC] � 1,500/�L, platelets � 100,000/�L,
bilirubin � 1.5� upper limit of normal, and aminotransferases �3� upper limit of normal), creatinine clearance (Cockroft for-mula) � 50 mL/min, Eastern Cooperative Oncology Group PS 0to 2, and the absence of moderate or severe heart failure or chronicobstructive airway disease. No previous chemotherapy for ad-vanced disease was allowed. Prior adjuvant or neoadjuvant treat-ment was allowed, provided that it had ended at least 12 monthsbefore randomization and the total doses of previously adminis-tered agents did not exceed the following levels: cisplatin 300mg/m2, epirubicin 400 mg/m2, and doxorubicin 300 mg/m2. Theprotocol of the study was approved by the Scientific Committee ofthe Hellenic Cooperative Oncology Group and the institutionalreview board of each participating center. Patients gave informedconsent before random assignment to treatment.
Baseline evaluation included full blood count (FBC), renaland liver function tests, calculation of creatinine clearance, elec-trolyte level tests, chest x-ray (computed tomography [CT] scan ofthe thorax if the chest x-ray was abnormal) and CT scan of thewhole abdomen. CT or magnetic resonance imaging of the brainand a bone scan were performed if clinically indicated.
Randomization was performed centrally after stratificationfor disease site (visceral metastases v locoregional disease [unre-sectable tumor and/or lymph node metastases at any site includingpelvis, retroperitoneum, mediastinum, and neck]) and prior ad-juvant or neoadjuvant chemotherapy (yes v no).
Treatment Schedule
Patients randomly assigned to MVAC (arm A) receivedmethotrexate 30 mg/m2 and vinblastine 3 mg/m2 on days 1, 15,and 22, and cisplatin 70 mg/m2 and doxorubicin 30 mg/m2 on day1, every 4 weeks. Patients randomly assigned to DC (arm B)received docetaxel 75 mg/m2 and cisplatin 75 mg/m2 every 3weeks. In both arms, cisplatin was administered as a 1-hour infu-sion with adequate pre- and posthydration. G-CSF was adminis-tered on days 7, 8, 9, 25, and 26 to patients who received MVACand on days 5 to 9 to patients who received DC. FBC and serumcreatinine tests were performed before each chemotherapy ad-ministration. Chemotherapy was administered on day 1 if ANCwas more than 1,500/�L and if platelets were more than 100,000/�L; otherwise, chemotherapy was delayed, and G-CSF was admin-istered until hematologic recovery. If hematologic recovery wasnot achieved by day 42 for MVAC or day 35 for DC, the patient wastaken off study. Chemotherapy on days 15 or 22 of the MVACregime was not administered if ANC was less than 1,000/�L orplatelets were less than 100,000/�L. FBC was performed on day 7in patients who received DC. If ANC was less than 500/�L, thedocetaxel dose was reduced to 50 mg/m2. The same reduction wasapplied if neutropenic fever occurred. If the calculated creatinineclearance was less than 50 mL/min, cisplatin was not administered,and serum creatinine was measured weekly. Cisplatin administra-tion was resumed if calculated creatinine clearance was increasedabove 50 mL/min; if this increase was not achieved by day 42 forMVAC or day 35 for DC, the patient was taken off study. Chemo-therapy was administered for a total of six cycles unless there wasdisease progression or unacceptable toxicity, or if the patient re-fused to continue. Treatment was allowed to continue beyond thesixth cycle if it was believed to benefit the patient. The decision offurther treatment was made by the responsible physician, but thestudy protocol suggested that patients with only locoregional dis-ease should be assessed for definitive local treatment (surgery orradiotherapy) after the completion of chemotherapy.
MVAC Versus DC in Urothelial Cancer
www.jco.org 221
Downloaded from jco.ascopubs.org on June 2, 2013. For personal use only. No other uses without permission.Copyright © 2004 American Society of Clinical Oncology. All rights reserved.

Efficacy and Toxicity Evaluation
The primary objective of the study was the comparison ofoverall survival in the two treatment arms. Survival was calculatedfrom the day of the initiation of treatment until date of death orlast contact for patients still alive at the time of follow-up. Second-ary end points were the comparison of RRs and time to pro-gression (TTP) across treatment arms. Tumor assessment wasperformed every three cycles of treatment. Patients with bidimen-sionally measurable disease who received protocol treatment andhad at least one follow-up tumor assessment were eligible forresponse evaluation. Standard WHO criteria [20] were used forclassifying response. TTP was calculated from the day of the initi-ation of treatment until the date of relapse, disease-related deathbefore response evaluation, or last contact for patients withoutrelapse at the time of analysis. Patients who did not receive proto-col treatment or suffered disease-unrelated death without progres-sion were considered censored at the time of the above-mentionedevents. Toxicity was evaluated at each chemotherapy visit accord-ing to National Cancer Institute Common Toxicity Criteria. Rel-ative dose-intensity (RDI) was defined as the percentage of theexpected dose administered to the patient (per unit of time ex-pressed in milligrams per square meters per week).
Statistical Considerations and Analysis
The objective of this trial was to detect a relative difference of20% in survival rates between the two treatment arms (hazardratio [HR], 1.66). With a two-sided log-rank test at the 5% levelof significance and an 80% power, this requires 182 patients intotal (91 patients per arm) [21]. Allowing for a 10% rate ofwithdrawals, 200 patients should be randomly assigned (100patients in each arm).
All analyses were performed using the SPSS statistical soft-ware (SPSS for Windows, version 10; SPSS Inc, Chicago, IL).Frequency distributions were used to describe the categoricvariables, whereas continuous variables were presented asmeans and standard deviations. Differences across treatmentarms regarding all categoric variables were examined with a �2
test; for continuous variables, the t test was used to test theequality of the appropriate means.
Survival curves for TTP and survival data were produced withthe Kaplan and Meier method [22] and compared between armswith the stratified log-rank test [22]. For univariate and multivar-iate analyses of TTP and survival, the Cox proportional hazardsmodel was used [23]. Throughout the analysis a level of 5% wasused to denote statistical significance except as indicated.
RESULTS
Patients
Between June 1997 and May 2002, 224 patients wereentered onto the study. Four patients were not randomlyassigned because they did not have inoperable disease.From the remaining 220 patients, 109 were randomly as-signed to arm A (MVAC) and 111 patients were assigned toarm B (DC). Characteristics of randomly assigned patients(Table 1) were well balanced across treatment arms exceptfor WHO PS: there were more patients with PS 0 and fewerwith PS 2 in the MVAC arm compared with the DC arm,and this difference was statistically significant (P � .040).Thirteen patients did not receive study treatment (MVAC
arm, six patients; DC arm, seven patients): three patientsdied before initiation of treatment and five patients haddeterioration of renal function before treatment initiation,whereas five patients refused to receive the allocated treat-ment. One hundred three patients had had their primarysite removed: 39 of these patients also received adjuvantradiotherapy, whereas 26 had chemotherapy before (n � 9)or after (n � 17) radical surgical removal of their primarytumor. One hundred ninety patients had transitional-cellcarcinomas. The other histologies included squamous car-cinoma (MVAC, five patients; DC, four patients), adeno-carcinoma (MVAC, three patients; DC, one patient), mixedcarcinomas (MVAC, six patients; DC, three patients), sar-comatoid carcinoma (DC, two patients), poorly differenti-ated carcinoma (DC, two patients), small-cell carcinoma(MVAC, one patient), large-cell carcinoma (MVAC, onepatient), giant cell carcinoma (MVAC, one patient) andplasmatocytoid carcinoma (MVAC, one patient).
Survival
All randomly assigned patients were included in sur-vival analysis on an intention-to-treat basis. Efficacy dataare shown in Table 2. At the time of analysis, 158 patients(MVAC, 74 patients [67.89%]; DC, 84 patients [75.68%])had died (150 disease-related deaths, three treatment-re-lated deaths, and five deaths resulting from other causes[myocardial infarctions in two patients, fulminant hepatitisin one patient, stroke in one patient, and one sudden deathresulting from unknown etiology]). Median follow-up forsurviving patients was 25.3 months (range, 3.2 to 51months). Survival curves for both arms are depicted inFigure 1. Median survival was statistically significantly bet-ter in patients who received MVAC compared with DCchemotherapy (14.2 v 9.3 months, respectively; P � .026).Two-year survival was also superior in patients receivingMVAC compared with patients receiving DC (28.6% v18.9%, respectively).
Univariate analysis, including the characteristics listedin Table 1 of all 220 randomly assigned patients, showedthat female sex (P � .041), no adjuvant chemotherapy (P �.002), neoadjuvant chemotherapy (P � .038), performancestatus of 0 or 1 (P � .004), and absence of visceral metasta-ses (P � .001) were associated with improved survival.Multivariate Cox regression analysis showed that only vis-ceral metastases (P � .004) and PS (P � .005) were inde-pendently associated with prognosis. When adjusted forthese factors (Table 3), the effect of treatment with MVACbecame nonsignificant compared with DC treatment (HR,1.31; P � .089). The survival curves for the two treatmentarms across categories of PS and metastatic sites are pre-sented in Figures 2 and 3. The relative effect on survival ofMVAC compared with DC did not vary across categories ofPS (P � .894 for interaction between treatment arm and PS)
Bamias et al
222 JOURNAL OF CLINICAL ONCOLOGY
Downloaded from jco.ascopubs.org on June 2, 2013. For personal use only. No other uses without permission.Copyright © 2004 American Society of Clinical Oncology. All rights reserved.

or metastatic site (P � .531 for interaction between treat-ment arm and presence of visceral metastases).
TTP
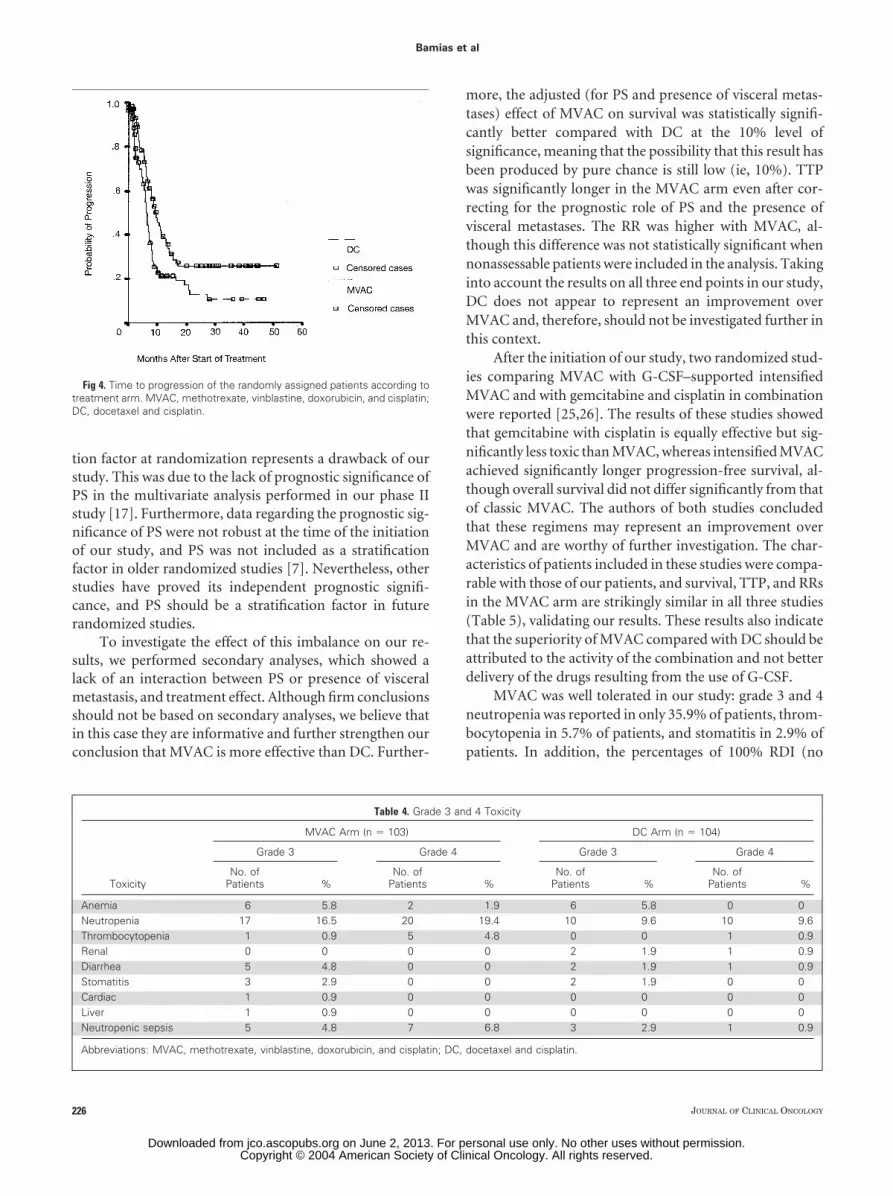
During follow-up there was disease relapse in 141 pa-tients: 65 patients in the MVAC arm and 76 patients in theDC arm. TTP curves for both treatment arms are depictedin Figure 4. Median TTP was statistically significantlybetter in patients who received MVAC chemotherapycompared with patients receiving DC (9.4 v 6.1 months,respectively; P � .003).
Univariate analysis showed that PS 0 or 1 (P � .029)and absence of visceral metastases (P � .001) were associ-ated with improved TTP. Multivariate analysis showed thatboth factors were independently associated with TTP (P �.052 and P � .001, respectively). When adjusted for thesefactors (Table 3), treatment with MVAC was still statisti-cally significantly better than treatment with DC (HR, 1.61;P � .005). The relative effect on TTP of MVAC comparedwith DC did not vary across categories of PS or metastaticsites (P � .412 for PS and TTP interaction; P � .449 formetastatic sites and TTP interaction).
Tumor Response
One hundred seventy-four patients were assessable fortumor response (MVAC, 83 patients; DC, 91 patients; Table2). There were 19 (22.9%) CRs with MVAC and 12 CRs(13.2%) with DC chemotherapy. The overall RR for MVACwas significantly higher than that of DC (54.2% v 37.4%,respectively; P � .017) when only patients assessable forresponse were considered. However, the difference in RRsbetween the randomized arms was not statistically signifi-cant when all randomly assigned patients were analyzed andnonassessable patients were considered nonresponders (in-tent-to-treat analysis 41.3% v 30.6%; P � .100).
Toxicity
All patients who received at least one cycle of chemo-therapy were analyzed for toxicity. A total of 456 cycles ofMVAC (median, five cycles; range, one to seven cycles) and480 cycles of DC (median, six cycles; range, one to ninecycles) were administered. Thirty-eight patients (37.6%) inthe MVAC arm and 64 patients (61.5%) in the DC armreceived full doses of the protocol treatment. Median RDIwas 92.3% for cisplatin, 94% for doxorubicin, 87% forvinblastine, and 87% for methotrexate in the MVAC arm,
Table 1. Baseline Patient Characteristics
Characteristic
MVAC Arm (n � 109) DC Arm (n � 111)
PNo. of
Patients %No. of
Patients %
Age, yearsMedian 65 65Range 32–75 44–75
Sex .519Male 100 91.7 99 89.2Female 9 8.3 12 10.8
Performance status� .040 60 55.6 45 42.51 35 32.4 35 332 13 12 26 24.5
Primary site of disease .763Bladder 93 85.3 91 81.8Renal pelvis 9 8.3 12 10.9Ureter 7 6.4 8 7.3
Histology .508Transitional 93 85.3 97 89Other 16 14.7 14 11
Visceral metastases† .251Yes 52 47.7 61 55.5No 57 52.3 49 45.5
Prior treatmentRemoval of primary site 51 46.8 52 48.6 .790Radiotherapy 19 17.4 20 18.7 .810Adjuvant chemotherapy 8 7.3 9 8.3 .801Neoadjuvant chemotherapy 6 5.5 3 2.8 .328
Abbreviations: MVAC, methotrecate, vinblastine, doxorubicin, and cisplatin; DC, docetaxel and cisplatin.�Data from 214 patients.†Data from 219 patients.
MVAC Versus DC in Urothelial Cancer
www.jco.org 223
Downloaded from jco.ascopubs.org on June 2, 2013. For personal use only. No other uses without permission.Copyright © 2004 American Society of Clinical Oncology. All rights reserved.

whereas RDI in the DC arm was 100% for both cisplatin anddocetaxel. All grade 3 and 4 toxicities (except for nausea orvomiting and alopecia) are shown in Table 4.
There were three toxic deaths (two in the MVAC armand one in the DC arm); all were due to neutropenic sepsis.Treatment with MVAC resulted in significantly more fre-quent grade 3 or 4 neutropenia than did treatment with DC
(35.9% v 19.2%, respectively; P � .006), thrombocytope-nia, (5.7% v 0.9%, respectively; P � .046) and episodes ofneutropenic sepsis (11.6% v 3.8%, respectively; P � .001).Nonhematologic toxicities were infrequent except for nau-sea and vomiting, which was encountered in 56 patients(51.4%) in the MVAC arm and 44 patients (39.6%) in theDC arm (P � .084). Nevertheless, grade 3 and 4 toxicity wasrare in both arms (occurring in three patients in the MVACarm and two patients in the DC arm). Renal toxicity wasequally distributed, with 14 patients (13.6% for the MVACarm and 14.5% for the DC arm) experiencing it in botharms, although grade 3 or 4 renal toxicity was encounteredonly in the DC arm. Neurotoxicity was the only othertoxicity (not shown in Table 4) that exceeded 2% of patientsin each arm: 18 patients who received MVAC (17.4%) and19 patients who received DC (18.2%) experienced grade 1or 2 neurotoxicity.
DISCUSSION
This multicenter, randomized, phase III trial showed thatMVAC with G-CSF support is more effective than DC inadvanced urothelial cancer. This study was based on ourprevious experience with DC, which showed promisingefficacy in 66 patients, many of whom had unfavorableprognostic characteristics [17]. These results confirmedthose of a previous, smaller study, which showed a 60%overall RR with 26% CR, and a median survival time of 13.6months in 25 patients with metastatic urothelial cancer
Table 2. Efficacy Outcomes
End Point
MVAC Arm DC Arm
HR 95% CI PNo. of
Patients %No. of
Patients %
Survival, monthsMedian 14.2 9.3 1.52 1.11 to 2.08 .025595% CI 12.5 to 15.9 7.9 to 10.7
TTP, monthsMedian 9.4 6.13 1.73 1.24 to 2.42 .002995% CI 7.4 to 11.3 5.6 to 6.6
2-year survival% of patients 28.6 18.995% CI 19.1 to 38.1 10.5 to 27.4
Response rates�
CR 19 22.9 12 13.2PR 26 31.3 22 24.2ORR 45 54.2† 34 37.4‡ .017SD 19 22.9 25 27.5PD 19 22.9 32 35.2
Abbreviations: MVAC, methotrexate, vinblastine, doxorubicin, and cisplatin; DC, docetaxel and cisplatin; HR, hazard ratio; TTP, time to progression; CR,complete response; PR, partial response; ORR, overall rate of response; SD, stable disease; PD, progressive disease.
�For assessable patients.†95% CI, 42.9 to 65.2.‡95% CI, 27.4 to 48.1.
Fig 1. Overall survival of the randomly assigned patients according totreatment arm. MVAC, methotrexate, vinblastine, doxorubicin, and cisplatin;DC, docetaxel and cisplatin.
Bamias et al
224 JOURNAL OF CLINICAL ONCOLOGY
Downloaded from jco.ascopubs.org on June 2, 2013. For personal use only. No other uses without permission.Copyright © 2004 American Society of Clinical Oncology. All rights reserved.

[24]. The baseline characteristics of the patients included inthe present study are similar to those of our previous study,and our results are similar regarding TTP and survival aftertreatment with DC. Despite confirmation of the activity ofDC in advanced urothelial cancer, our study showed thatDC was inferior to MVAC. Overall survival of patients
treated with MVAC was significantly longer than that ofpatients treated with DC, as shown by stratified log-ranktest (P � .025). Nevertheless, this difference was no longerstatistically significant when treatment effect was adjustedfor PS and presence or absence of visceral metastases (P �.089). This lack of significance most probably is due to animbalance in baseline PS. Not including PS as a stratifica-
Table 3. Multivariate Analysis for Cumulative OS and TTP
Factor
OS TTP
HR 95% CI P HR 95% CI P
WHO PS0 and 1 1.0 1.06 to 2.31 .038 1.0 .0972 1.57 1.42 0.93 to 2.17
Visceral metastasesYes 1.0 0.42 to 0.82 .003 1.0 .001No 0.59 0.55 0.39 to 0.77
Treatment armMVAC 1.0 0.94 to 1.81 .005 1.0 .005DC 1.31 1.61 1.15 to 2.26
Abbreviations: OS, overall survival; TTP, time to progression; HR, hazard ratio; PS, performance status; MVAC, methotrexate, vinblastine, doxorubicin, andcisplatin; DC, docetaxel and cisplatin.
Fig 2. Overall survival according to treatment arm in patients withperformance status (A) 0 or 1 and (B) 2. MVAC, methotrexate, vinblastine,doxorubicin, and cisplatin; DC, docetaxel and cisplatin.
Fig 3. Overall survival according to treatment arm in patients (A) with and(B) without visceral metastases. MVAC, methotrexate, vinblastine, doxoru-bicin, and cisplatin; DC, docetaxel and cisplatin.
MVAC Versus DC in Urothelial Cancer
www.jco.org 225
Downloaded from jco.ascopubs.org on June 2, 2013. For personal use only. No other uses without permission.Copyright © 2004 American Society of Clinical Oncology. All rights reserved.
tion factor at randomization represents a drawback of ourstudy. This was due to the lack of prognostic significance ofPS in the multivariate analysis performed in our phase IIstudy [17]. Furthermore, data regarding the prognostic sig-nificance of PS were not robust at the time of the initiationof our study, and PS was not included as a stratificationfactor in older randomized studies [7]. Nevertheless, otherstudies have proved its independent prognostic signifi-cance, and PS should be a stratification factor in futurerandomized studies.
To investigate the effect of this imbalance on our re-sults, we performed secondary analyses, which showed alack of an interaction between PS or presence of visceralmetastasis, and treatment effect. Although firm conclusionsshould not be based on secondary analyses, we believe thatin this case they are informative and further strengthen ourconclusion that MVAC is more effective than DC. Further-
more, the adjusted (for PS and presence of visceral metas-tases) effect of MVAC on survival was statistically signifi-cantly better compared with DC at the 10% level ofsignificance, meaning that the possibility that this result hasbeen produced by pure chance is still low (ie, 10%). TTPwas significantly longer in the MVAC arm even after cor-recting for the prognostic role of PS and the presence ofvisceral metastases. The RR was higher with MVAC, al-though this difference was not statistically significant whennonassessable patients were included in the analysis. Takinginto account the results on all three end points in our study,DC does not appear to represent an improvement overMVAC and, therefore, should not be investigated further inthis context.
After the initiation of our study, two randomized stud-ies comparing MVAC with G-CSF–supported intensifiedMVAC and with gemcitabine and cisplatin in combinationwere reported [25,26]. The results of these studies showedthat gemcitabine with cisplatin is equally effective but sig-nificantly less toxic than MVAC, whereas intensified MVACachieved significantly longer progression-free survival, al-though overall survival did not differ significantly from thatof classic MVAC. The authors of both studies concludedthat these regimens may represent an improvement overMVAC and are worthy of further investigation. The char-acteristics of patients included in these studies were compa-rable with those of our patients, and survival, TTP, and RRsin the MVAC arm are strikingly similar in all three studies(Table 5), validating our results. These results also indicatethat the superiority of MVAC compared with DC should beattributed to the activity of the combination and not betterdelivery of the drugs resulting from the use of G-CSF.
MVAC was well tolerated in our study: grade 3 and 4neutropenia was reported in only 35.9% of patients, throm-bocytopenia in 5.7% of patients, and stomatitis in 2.9% ofpatients. In addition, the percentages of 100% RDI (no
Table 4. Grade 3 and 4 Toxicity
Toxicity
MVAC Arm (n � 103) DC Arm (n � 104)
Grade 3 Grade 4 Grade 3 Grade 4
No. ofPatients %
No. ofPatients %
No. ofPatients %
No. ofPatients %
Anemia 6 5.8 2 1.9 6 5.8 0 0Neutropenia 17 16.5 20 19.4 10 9.6 10 9.6Thrombocytopenia 1 0.9 5 4.8 0 0 1 0.9Renal 0 0 0 0 2 1.9 1 0.9Diarrhea 5 4.8 0 0 2 1.9 1 0.9Stomatitis 3 2.9 0 0 2 1.9 0 0Cardiac 1 0.9 0 0 0 0 0 0Liver 1 0.9 0 0 0 0 0 0Neutropenic sepsis 5 4.8 7 6.8 3 2.9 1 0.9
Abbreviations: MVAC, methotrexate, vinblastine, doxorubicin, and cisplatin; DC, docetaxel and cisplatin.
Fig 4. Time to progression of the randomly assigned patients according totreatment arm. MVAC, methotrexate, vinblastine, doxorubicin, and cisplatin;DC, docetaxel and cisplatin.
Bamias et al
226 JOURNAL OF CLINICAL ONCOLOGY
Downloaded from jco.ascopubs.org on June 2, 2013. For personal use only. No other uses without permission.Copyright © 2004 American Society of Clinical Oncology. All rights reserved.

reductions or delays) were 41.6% for cisplatin, 44.6% fordoxorubicin, and 37.6% for vinblastine and methotrexate.These data show that toxicity and drug delivery were morefavorable in our study than reported in earlier and morerecent trials for classic MVAC [6,25-27], as shown in Table5. Lower incidence of neutropenia, neutropenic sepsis, andstomatitis can be attributed to the routine use of G-CSF.Lower incidence of thrombocytopenia is more difficult toexplain, but it could be because days 15 and 22 were omittedif the platelet count was less than 100,000/�L, which ishigher than the threshold used in previous studies. In addi-tion, some cases of grade 3 or 4 thrombocytopenia may havebeen undetected because weekly FBC was not obligatory inour study. Our results indicate that G-CSF–supportedMVAC is better tolerated than classic MVAC. Furthermore,the toxicity profile of MVAC, administered in our study,compares favorably with that of both combination gemcit-abine plus cisplatin and intensified MVAC (Table 5), withthe exception of neutropenic sepsis in patients who receivedcombination gemcitabine and cisplatin. We therefore be-
lieve that G-CSF–supported MVAC could be considered asa reference regime for advanced urothelial cancer instead ofthe more toxic classic MVAC. Admittedly, this should beviewed in the context of the possible changes that may resultfrom the publication of the two aforementioned random-ized studies regarding the choice of first-line chemotherapyin advanced urothelial cancer.
In the last decade, research has been focused on theimprovement of treatment of advanced urothelial cancer.Our study has shown that DC cannot substitute for MVACbecause of the lower efficacy of DC. Nevertheless, the addi-tion of G-CSF significantly ameliorates the toxicity ofMVAC, and G-CSF–supported MVAC could be consideredas a substitute for classic MVAC if this regimen is to be usedin patients with advanced urothelial cancer.
� � �
Authors’ Disclosures of Potential
Conflicts of Interest
The authors indicated no potential conflicts of interest.
REFERENCES
1. Saxman SB, Propert KJ, Einhorn LH, et al:Long-term follow-up of a phase III Intergroup studyof cisplatin alone or in combination with methotrex-ate, vinblastine, and doxorubicin in patients withmetastatic urothelial carcinoma: A CooperativeGroup Study. J Clin Oncol 15:2564-2569, 1997
2. Sternberg C, Yagoda A, Scher HI, et al:Preliminary results of M-VAC (methotrexate, vin-blastine, doxorubicin, and cisplatin) for transi-tional cell carcinoma of the urothelium. J Urol133:403-407, 1985
3. Sternberg C, Yakoda A, Scher HI, et al:M-VAC (methotrexate, vinblastine, doxorubicin,and cisplatin) for advanced transitional cell carci-noma of the urothelium. J Urol 139:461-469,1988
4. Roth BJ, Bajorin DF: Advanced bladdercancer: The need to identify new agents in the
post-M-VAC (methotrexate, vinblastine, doxoru-bicin and cisplatin) world. J Urol 153:894-900,1995
5. Sternberg CN: The treatment of advancedbladder cancer. Ann Oncol 6:113-126, 1995
6. Loehler PJ, Einhorn LH, Elson PJ, et al: Arandomized comparison of cisplatin alone or incombination with methotrexate, vinblastine, anddoxorubicin in patients with metastatic urothelialcarcinoma. J Clin Oncol 10:1066-1073, 1992
7. Logothetis CJ, Dexeus FH, Finn L, et al: Aprospective randomized trial comparing MVACand CISCA chemotherapy for patients with met-astatic urothelial tumors. J Clin Oncol 8:1050-1055, 1990
8. Sternberg C, Yakoda A, Scher HI, et al:Methotrexate, vinblastine, doxorubicin, andcisplatin for advanced transitional cell carci-noma of the urothelium: Efficacy and patternsof response and relapse. Cancer 64:2448-2458, 1989
9. Gabrilove JL, Jakubowski A, Scher H, et al:Effect of granulocyte-colony stimulating factor onneutropenia and associated morbidity due to che-motherapy for transitional-cell carcinoma of theurothelium. N Engl J Med 318:1414-1422, 1988
10. Moore MJ, Iscoe N, Tannock IF, et al: Aphase II study of methotrexate, vinblastine,doxorubicin and cisplatin plus recombinant hu-man granulocyte-macrophage colony stimulatingfactors in patients with advanced transitional cellcarcinoma. J Urol 150:1131-1134, 1993
11. Sternberg CN, de Mulder PH, van Oost-erom AT, et al: Escalated M-VAC chemotherapyand recombinant human granulocyte-macroph-age colony stimulating factor (rhGM-CSF) in pa-tients with advanced urothelial tract tumors. AnnOncol 4:403-407, 1993
12. Seidman AD, Scher HI, Gabrilove JL, et al:Dose-intensification of methotrexate, vinblas-tine, doxorubicin, and cisplatin with recombinanthuman granulocyte-colony stimulating factor as
Table 5. Efficacy and Toxicity (grade 3 and 4) of This Study and Two More Recent Randomized Studies Using MVAC in Advanced Urothelial Cancer
Efficacy and Toxicity
von der Maase et al Study [26] Sternberg et al Study [25] Present Study
GC(n � 203)
MVAC(n � 202)
HDMVAC(n � 134)
MVAC(n � 129)
MVAC � G-CSF(n � 109)
Median survival, months 13.8 14.8 15.5 14.1 14.2Median TTP, months 7.4 7.4 11.1 9.6 9.41Response rate, % of patients 54.3 55 72 58 54.2Neutropenia, % of patients 81.1 82 20 62� 35.9Thrombocytopenia, % of patients 57 20.6 22 23 5.7Neutropenic fever, % of patients 1 14 10 26† 11.6Stomatitis, % of patients 1 22 10 17 2.9Toxic deaths, % of patients 1 3 3 4 1.8
Abbreviations: MVAC, methotrexate, vinblastine, doxorubicin, cisplatin; GC, gemcitabine and cisplatin; HDMVAC, high-dose MVAC; G-CSF, granulocytecolony-stimulating factor; TTP, time to progression.
�Grade 3 or 4 leucopenia.†Neutropenic fever.
MVAC Versus DC in Urothelial Cancer
www.jco.org 227
Downloaded from jco.ascopubs.org on June 2, 2013. For personal use only. No other uses without permission.Copyright © 2004 American Society of Clinical Oncology. All rights reserved.

initial therapy in advanced urothelial cancer.J Clin Oncol 11:408-414, 1993
13. Roth BJ, Dreicer R, Einhorn LH, et al:Significant activity of paclitaxel in advanced tran-sitional-cell carcinoma of the urothelium: Aphase II trial of the Eastern Cooperative Oncol-ogy Group. J Clin Oncol 12:2264-2270, 1994
14. McCaffrey JA, Hilton S, Mazumdar M, etal: Phase II trial of docetaxel in patients withadvanced or metastatic transitional-cell carci-noma. J Clin Oncol 15:1853-1857, 1997
15. Dimopoulos MA, Deliveliotis C, Moulopou-los LA, et al: Treatment of patients with meta-static urothelial carcinoma and impaired renalfunction with single-agent docetaxel. Urology52:56-60, 1998
16. Bajorin DF, McCaffrey JA, Hilton S, et al:Treatment of patients with transitional-cell carci-noma of the urothelial tract with ifosfamide,paclitaxel, and cisplatin: A phase II trial. J ClinOncol 16:2722-2727, 1998
17. Dimopoulos MA, Bakoyiannis C, Geor-goulias V, et al: Docetaxel and cisplatin combina-tion chemotherapy in advanced carcinoma of theurothelium: A multicenter phase II study of the
Hellenic Cooperative Oncology Group. Ann On-col 10:1385-1388, 1999
18. Bajorin DF, Dodd PM, Mazudmar M, et al:Long-term survival in metastatic transitional-cellcarcinoma and prognostic factors predicting out-come of treatment. J Clin Oncol 17:3173-3181,1999
19. Geller NL, Sternberg CN, Penenberg D, etal: Prognostic factors for survival of patients withadvanced urothelial tumors treated with metho-trexate, vinblastine, doxorubicin, and cisplatinchemotherapy. Cancer 67:1525-1531, 1991
20. Miller AB, Hoogstraten B, Staquet M, et al:Reporting results of cancer treatment. Cancer47:207-214, 1981
21. Machin D, Campbell M, Fayers P, et al:Sample Size Tables for Clinical Studies (ed 2).London, United Kingdom, Blackwell Science, 1997
22. Cox DR, Oakes D. Analysis of SurvivalData. London, United Kingdom, Chapman andHall, 1984
23. Kaplan EL, Meier P: Non-parametric esti-mation for incomplete observations. J Am StatAssoc 53:457-481, 1958
24. Sengelov L, Kamby C, Lund B, et al:Docetaxel and cisplatin in metastatic urothelialcancer: A phase II study. J Clin Oncol 16:3392-3397, 1998
25. Sternberg CN, de Mulder PHM, Schorna-gel JH, et al: Randomized phase III trial ofhigh-dose-intensity methotrexate, vinblastine,doxorubicin, and cisplatin (MVAC) chemother-apy and recombinant human granulocyte colo-ny-stimulating factor versus classic MVAC inadvanced urothelial tract tumors: EuropeanOrganization for Research and Treatment ofCancer protocol No. 30924. J Clin Oncol 19:2638-2646, 2001
26. Von der Maase H, Hansen SW, RobertsJT, et al: Gemcitabine and cisplatin versusmethotrexate, vinblastine, doxorubicin, andcisplatin in advanced metastatic bladder can-cer: Results of a large, randomized, multina-tional, multicenter, phase III study. J Clin On-col 18:3068-3077, 2000
27. Scher HI, Geller NL, Curley T, et al: Effectof relative cumulative dose-intensity on survivalof patients with urothelial cancer treated withM-VAC. J Clin Oncol 11:400-407, 1993
Bamias et al
228 JOURNAL OF CLINICAL ONCOLOGY
Downloaded from jco.ascopubs.org on June 2, 2013. For personal use only. No other uses without permission.Copyright © 2004 American Society of Clinical Oncology. All rights reserved.

ERRATUM
The January 15, 2004 article by Bamias et al entitled, “Docetaxel and Cisplatin WithGranulocyte Colony-Stimulating Factor (G-CSF) Versus MVAC With G-CSF in Ad-vanced Urothelial Carcinoma: A Multicenter, Randomized, Phase III Study From theHellenic Cooperative Oncology Group” (J Clin Oncol 22:220-228, 2004) contained incor-rect information in Table 3.
The corrected table is reprinted below in its entirety.
Table 3. Multivariate analysis for Cumulative OS and TTP
Factor
OS TTP
HR 95% CI P HR 95% CI P
WHO PS .038 .0970 and 1 1.0 1.02 1.57 1.06 to 2.31 1.42 0.93 to 2.17
Visceral metastases .003 .001Yes 1.0 1.0No 0.59 0.42 to 0.82 0.55 0.39 to 0.77
Treatment arm .089 .005MVAC 1.0 1.0DC 1.31 0.94 to 1.81 1.61 1.15 to 2.26
Abbreviations: OS, overall survival; TTP, time to progression; HR, hazard ratio; PS, performance status; MVAC,methotrexate, vinblastine, doxorubicin, and cisplatin; DC, docetaxel and cisplatin.
DOI: 10.1200/JCO.2004.03.906
1771
Downloaded from jco.ascopubs.org on June 2, 2013. For personal use only. No other uses without permission.Copyright © 2004 American Society of Clinical Oncology. All rights reserved.





























