Embed Size (px)
Citation preview
MASARYK UNIVERSITY
Faculty of Social Studies
Department of Psychology
DOCTORAL THESIS
Brno 2017 Violeta Zefi, MA

ii
MASARYK UNIVERSITY
Faculty of Social Studies
Department of Psychology
Violeta Zefi, MA
Adolescents’ and emerging adults’ attitudes towards people living
with HIV and AIDS and their risk perception of HIV
Doctoral Thesis
Supervisor: Prof. PhDr. Petr Macek, CSc.
Brno, 2017
iii
I declare that I have worked on this thesis independently, using only the primary and
secondary sources listed in the bibliography.
In Brno, date: Violeta Zefi, MA
Name Surname
4
ABSTRACT
AIDS is considered as one of the most dangerous and incurable diseases of the modern
society. Except health issues, HIV implicates social, cultural and psychological causes and
consequences as well. According to World Health Organization (WHO) it is estimated that half of
the world’s HIV infection is found among the adolescents and emerging adults between 15 and 24
years of age. This study aims to fill the lack of the existing data by examining the Kosovar
adolescents and emerging adults regarding HIV and AIDS, especially on issues of their attitudes
towards people living with HIV and AIDS, knowledge and risk perception of HIV. Kosovo has
one of the youngest populations in Europe. The young men and women younger than 25 years old
represent 49% of the whole population in Kosovo, while 19.1% of young people are under the age
of 15-24 (Ministry of Culture, Youth and Sports, 2013). Although the prevalence of HIV is low,
if not prevented at early stages, Kosovo has specific elements that may lead to the incensement of
the scale of the epidemic of HIV. As an economically underdeveloped country with the highest
unemployment rate in Europe and with few opportunities for development in many aspects, young
people aged 18-25 years increasingly face particular challenges that can lead to increased exposure
and susceptibility to HIV. Thus, the aim of this study is to examine the level of knowledge of HIV
and AIDS, attitudes towards people living with HIV and risk perception of HIV in correlation with
socio-cultural aspects among adolescents and emerging adults in Kosovo.
To collect data, the sequential explanatory mixed method design was used, where the quantitative
phase was used for collecting data on the level of knowledge of HIV and AIDS, attitudes towards
people living with HIV and risk perception of HIV. Whereas, focus group discussions were used
to deeply analyze socio-cultural correlations with level of knowledge, risk perception of HIV and
attitudes towards people living with HIV and AIDS, in order to get a better understanding of the
issue. In addition, the idea is to confront these data (qualitative data) with the data obtained from
the quantitative analysis among adolescents and emerging adults.
In total 1234 (N=1234) subjects were part of a self-administered and self-reporting questionnaire.
Adolescents from 13 to 18 (N= 384 or 31.0%) years old and emerging adults from 19 to 25 (N=850
or 68.7%) years old were part of the questionnaire. In terms of gender distribution, 67.1% (N=828)
were females and 32.9% (N=406) were males, while, residing in urban areas were 60.3% (N=744)
of subjects, and in the rural areas were 39.6% (N=489) of subjects. Although, there were four focus

5
group discussions organized from two target groups: adolescents and emerging adults. In addition,
between seven to eight subjects were part of each of the focus group discussions.
Results from quantitative and qualitative analysis show a satisfactory level of knowledge about
HIV and AIDS among the adolescents and emerging adults in Kosovo. In addition, there are still
misconceptions about HIV and AIDS. For instance, 20.9% of subjects agree that you can get
infected with HIV through social contacts that you have in everyday life (handshakes, hugs etc.).
Emerging adults and female subjects have a higher level of knowledge of HIV and AIDS compared
with adolescents and male subjects. In addition, other socio-demographic characteristics of
subjects such as: age group, monthly income, educational level of subjects and urban residence
were found to be significant predictors of knowledge about HIV and AIDS.
Attitudes of subjects towards people living with HIV and AIDS were tolerant and positive.
Findings show that emerging adults and female subjects have more positive attitudes towards
people living with HIV and AIDS compared with adolescents and male subjects. Other socio-
demographic characteristics of subjects such as age group, mothers’ level of education and
subjects’ educational level was found as a significant predictor of positive attitudes towards people
living with HIV and AIDS. However, stigmatizing attitudes have also been reported towards
people living with HIV and AIDS. In this regard, 56.3% of all subjects are not ready to eat from
the same plate with a person who lives with HIV and AIDS and 48.6 % of all subjects disagree
with the idea that a health worker who is infected with HIV and AIDS should be allowed to
continue to work with patients.
Result showed that male perceive more the risk of getting infected with HIV compared with
female, while between emerging adults and adolescents there is no statistically significant
difference on perceiving risk of getting infected with HIV.
Furthermore, 46.5% of female and male subjects declared that “there is no risk at all” of getting
infected with HIV; 29.9% declared that there is a “small risk”; 11.9% declared that there is an
“average risk” and 4.7% declared a “high risk” of getting infected with HIV. Therefore, the
perception of risk towards HIV and AIDS in both target groups, adolescent and emerging adults,
is low.
Keywords: adolescents, emerging adults, HIV and AIDS, knowledge, attitudes, risk perception,
Kosovo.
6
ACKNOWLEDGMENTS
First and foremost, I would like to express my sincere gratitude to my supervisor Prof. PhDr. Petr
Macek, CSc. for the continuous support of my PhD studies and related research, for his patience,
motivation and immense knowledge. His guidance helped me during the whole time of researching
and writing this thesis. I could not have imagined having a better advisor and supervisor for my
PhD studies. I was honored to work with him during this hard but wonderful PhD journey.
Secondly, I would like to express my appreciation to Masaryk University as an institution,
respectfully to the Faculty of Social Studies and Department of Psychology, for giving me the
opportunity to be a part of such a prestigious University. I appraise the opportunity given by MU
that changed my life forever. In addition, a special thanks also goes to Ing. Dagmar Habova, who
works at the Office for International Relations, for her continues support and readiness to always
provide me with necessary information.
This dissertation would not be completed without the people who participated in the research
process, by filling out the questionnaires and those who participated in focus group discussions
too. For this reason, I would also like to thank everyone who helped me share the questionnaires
and collect the required data among the respondents.
A special thanks goes to my friends and colleagues, whose moral and professional comments and
suggestions made me work harder and also improve the quality of this dissertation. I am sure that
this dissertation would have not been the same without their support.
I am thankful to my uncle, Dr. Pashk Buzhala, for encouraging me all the time and especially in
this difficult and challenging endeavor. His professional advice was very useful, whereas his
personal consultations very inspiring.
Not only this PhD thesis but my entire education would have not been possible without the support
of my beloved family. Thus, a special thanks goes to my beautiful mother, Flore, for understanding,
supporting and guiding me; to my big brother, Zef, who is the best example of a brother and of a
7
friend and to his wonderful wife, Vilma, and a soon to come daughter; their princess. A special
thanks to my beautiful sister and her wonderful son, Gabriel, who gave me joy with their phone
calls, care and support. A special appreciation to my one and only “little” brother Ndrec, for the
tremendous support that he has always given me but especially during this period of time. A huge
thanks to his wonderful girlfriend, Aferdita, too. I love you all.
In life there are special people who touch our lives with words and actions that change us forever.
These are people who extend our vision and inspire us to higher levels of personal and professional
achievement. So, a big thanks goes to Alfred for being there for me every day and giving me hope,
support and what is more important, love. Thank you and I love you.

8
This doctoral dissertation is dedicated to Alfred, who has been a constant source of support and encouragement during
this hard but wonderful PhD journey. I’m truly thankful for having you in my life.
9
LIST OF ABBREVIATIONS
AIDS Acquired Immunodeficiency Syndrome
APA American Psychological Association
CDC Center for Disease Control and Prevention
EU European Union
FHC Family Health Centres
HBM Health Belief Model
HIV Human Immunodeficiency Virus
KABP Knowledge, Attitude, Belief, and Practice
MH Ministry of Health
MSM Men Who Have Sex with Man
NIPH National Institute of Public Health
PLWHA People Living with HIV and AIDS
PWID People Who Inject Drugs
SEE South Eastern Europe
SPSS Statistical Package for the Social Sciences
STD’s Sexually Transmitted Diseases
UNAIDS The Joint United Nations Programme on HIV and AIDS
UNICEF United Nations International Children's Emergency Fund
UNKT United Nation Kosovo Team
10
UNMIK United Nations Mission in Kosovo
WB World Bank
WHO World Health Organization
11
TABLE OF CONTENTS
ABSTRACT................................................................................................................................... 4
ACKNOWLEDGMENTS ............................................................................................................ 6
LIST OF ABBREVIATIONS ...................................................................................................... 9
LIST OF TABLES ...................................................................................................................... 14
LIST OF FIGURES .................................................................................................................... 16
CHAPTER I ................................................................................................................................ 18
INTRODUCTION....................................................................................................................... 18
1.1 Setting the problem ...................................................................................................... 18
1.2 Organization of the study............................................................................................. 21
1.3 Kosovo: short cultural and historical context .............................................................. 23
CHAPTER II............................................................................................................................... 27
LITERATURE REVIEW .......................................................................................................... 27
2.1 Health Belief Model..................................................................................................... 27
2.2 Key definition and terminology ................................................................................... 31
2.3 Adolescence and emerging adulthood as developmental stages.................................. 34
2.3.1 Why emerging adulthood is not “late adolescence”.............................................. 40
2.4 Attitudes: the concept and formation ........................................................................... 41
2.5 Adolescents, emerging adults and HIV and AIDS ...................................................... 43
2.5.1 Knowledge of HIV and AIDS among adolescents and emerging adults .............. 43
2.5.2 Attitudes of adolescents and emerging adults towards people with HIV and AIDS........................................................................................................................................ 45
2.5.3 HIV and AIDS-related stigma and its associated prejudice and discrimination ... 47
2.5.4 Risk perception of HIV among adolescents and emerging adults ........................ 53
2.6 Background studies in Kosovo – a brief description ................................................... 56
2.6.1 Research analysis of HIV knowledge, attitudes towards PLWHA and riskperception in Kosovo among adolescents and emerging adults..................................... 56
12
2.7 Research questions and hypotheses ............................................................................. 58
CHAPTER III ............................................................................................................................. 63
STUDY ONE ............................................................................................................................... 63
Quantitative Research ........................................................................................................ 63
3.1 Methodology ................................................................................................................ 63
3.1.1 Sample................................................................................................................... 63
3.2 Instrument .................................................................................................................... 69
3.2.1 Questionnaire ........................................................................................................ 69
3.3 Procedure ..................................................................................................................... 73
3.4 Ethical issues................................................................................................................ 75
3.5 Results from quantitative research............................................................................... 75
3.5.1 Level of knowledge to HIV and AIDS, attitudes towards PLWHA and riskperception to HIV (addressing H1-H7).......................................................................... 75
3.5.2 Correlation analysis between level of knowledge, risk perception of HIV andattitudes towards people living with HIV and AIDS ................................................... 107
CHAPTER IV............................................................................................................................ 115
STUDY TWO ............................................................................................................................ 115
Qualitative Research ........................................................................................................ 115
4.1 Methodology .............................................................................................................. 115
4.1.1 Participants .......................................................................................................... 115
4.1.2 Information about focus groups and thematic analysis ....................................... 116
4.2 Ethical issues.............................................................................................................. 121
4.3 Results from the qualitative research (focus groups)................................................. 121
4.3.1 Knowledge and perception of HIV and AIDS .................................................... 122
4.3.2 Attitudes towards people with HIV and AIDS.................................................... 128
4.3.3 Risk perception of HIV and AIDS ...................................................................... 133
CHAPTER V ............................................................................................................................. 136
5.1 Discussion of quantitative and qualitative results...................................................... 136
13
5.1.1 Knowledge regarding HIV and AIDS................................................................. 136
5.1.2 Attitudes towards people with HIV and AIDS......................................................... 141
5.1.3 Risk perception of HIV and AIDS ........................................................................... 145
CHAPTER VI............................................................................................................................ 150
GENERAL CONCLUSIONS .................................................................................................. 150
6.1 Contributions, implications for future studies and limitations................................... 154
BIBLIOGRAPHY..................................................................................................................... 156
ANNEX 1: Finalized questionnaire ............................................................................................ 171
ANNEX 2: Internal consistency (Cronbach α) reported for each gender for all subjects .......... 180
ANNEX 3: Table 20 a. The Cross tabulation results (HIV is really not my problem; it's
somebody else’s. * What are the chances that you personally be infected with HIV?) ............. 181
ANNEX 4: Interview protocol for focus group discussion ........................................................ 182
ANNEX 5: Consent to participate in focus group ...................................................................... 185
14
LIST OF TABLES
Table 1. Socio - demographic characteristics of subjects........................................................................... 63
Table 2. Number and Percentages of Level of Knowledge to HIV and AIDS............................................. 76
Table 3. Results of Chi-Square Test of Association on level of knowledge of HIV and AIDS, by gender and
age group .................................................................................................................................................... 77
Table 4. Number and Percentages of Attitudes to PLWHA ........................................................................ 79
Table 5. Attitudes towards PLWHA, according to gender and age group.................................................. 81
Table 6. Relationship between gender & age groups within attitudes towards PLWHA ........................... 83
Table 7. Level of knowledge of HIV and AIDS, by monthly income ........................................................... 85
Table 8. Results of Chi-Square Test of Association, by permanent residence (urban vs. rural) ................ 86
Table 9. Attitudes towards PLWHA, by mothers’ level of education (N=1200) ......................................... 88
Table 10. Attitudes towards PLWHA, by fathers’ level of education (N=1200)......................................... 90
Table 11. Level of knowledge of HIV and AIDS, by the educational status of all subjects (N=1224) ....... 92
Table 12. Results of Chi-Square Test of Association by the education level of subjects ............................ 95
Table 13. Attitudes towards PLWHA, by the educational status of subjects (N=1224) ............................. 97
Table 14. Results of Chi-Square Test of Association by subject’s education level ..................................... 99
Table 15. The Cross tabulation results (civil status & gender * Why do you think you are at risk of becoming
with HIV?)................................................................................................................................................. 100
Table 16. The Cross tabulation results (civil status & gender * Why do you think are at low risk of becoming
with HIV?)................................................................................................................................................. 101
Table 17. Mean and SD values for interest variable by age group, gender, permanent residence, civil status
and parents’ incomes ................................................................................................................................ 103
Table 18. Kruskal-Wallis H Results by age group, gender and permanent residence .............................. 104
Table 19. Kruskal-Wallis H results by civil status, parents’ incomes and education level ...................... 105
15
Table 20. The Cross tabulation results (group age & gender * What are the chances that you personally be
infected with HIV?) ................................................................................................................................... 106
Table 21. Spearman correlation results between level of HIV knowledge (K1-K8) and attitudes towards
PLWHA (A1-A10) ..................................................................................................................................... 107
Table 22. Kendall correlation results between level of knowledge (K1-K8) and risk perception of HIV 110
Table 23. Kendall correlation results between attitudes (A1-A10) towards people with HIV and AIDS and
risk perception of HIV............................................................................................................................... 111
Table 24. Socio demographic details of subjects in focus group discussions........................................... 115
Table 25. Codes and themes derived from the focus group discussions ................................................... 125

16
LIST OF FIGURES
Figure 1. Population pyramid of Kosovo .................................................................................................... 24
Figure 2. Health Belief Model..................................................................................................................... 30
Figure 3. Parents’ level of education .......................................................................................................... 65
Figure 4. Who do you live with? ................................................................................................................. 66
Figure 5. The employment status by gender................................................................................................ 67
Figure 6. The success in school/faculty, by gender..................................................................................... 68
Figure 7. Parents’ income ........................................................................................................................... 69
17
~Chapter One~Introduction
18
CHAPTER I
INTRODUCTION
1.1 Setting the problem
Even though HIV and AIDS are considered as the worst health crises in recorded history in the
world, they have moved beyond being primarily and only health issues (Gile, 2013). Today, HIV
implicates other social, cultural and psychological causes and consequences as well. In the
globalized world in which people are living today, HIV and AIDS have become an issue which
concerns not only specific persons or states, but the international community as well. For this
reason, today, HIV and AIDS are considered international issues.
AIDS is the late stage of the HIV infection when a person’s immune system is severely damaged
and has difficulty fighting diseases (Colman, 2015). Before the development of certain
medications, people with HIV could progress to AIDS in just a few years. Currently, people can
live much longer – years and even decades – with HIV before they develop AIDS. This is because
of “highly active” combinations of medications that were introduced in the mid. 90’s (Center for
Disease Control and Prevention, 2012).
Since the HIV and AIDS epidemic has emerged as a global problem with a disastrous impact on
survival and human development, it has created fear, social anxiety and feelings against humanity.
Besides, negative attitudes towards HIV-infected persons and AIDS patients today are widespread
and have greatly hindered the overall control of the epidemic (Mghase, 2010). Furthermore, in the
absence of a cure for HIV, the only existing means of controlling the AIDS epidemic is by
changing the high-risk behaviors that transmit the virus. In this respect, AIDS is considered much
more of a psychological issue than a medical problem.
Kosovo has one of the youngest populations in Europe (UNICEF, 2015). In addition, it has a
growing population with dominant younger age groups. The young men and women aged younger
than 25 years represent 49% of the whole population in Kosovo, while 19.1% of young people are
19
under the age of 15-24 (Ministry of Culture, Youth and Sports, 2013). Young people in Kosovo
have lived through a period of tremendous instability, change and transformation. It is a generation
that was mostly educated in the parallel system in the past, with little expectation of future jobs
and opportunities.
HIV as a worldwide pandemic is increasingly being spread in Kosovo. Starting from the first
reported case in 1986, the year 2016 has marked the largest number of HIV cases reported per year
in Kosovo. Modes of transmission for the cases registered in Kosovo between the years 1986-2016
are as follows: heterosexuals – 52%, MSM (men who have sex with men) – 18%, PWID (people
who inject drugs) – 2%, and vertical transmission (mother to child transmission) – 2% and
unknown – 26% (National Institute of Public Health, 2017). Lately, more transmissions have been
reported among men who have sex with men. The possibility of a high proportion of undiagnosed
infections makes it difficult to estimate the overall HIV prevalence accurately and to confirm
whether the HIV incidence has remained stable. It is important to emphasize that the HIV epidemic
in Kosovo remains, most likely, a small epidemic with the potential for growth, particularly among
men who have sex with men and people who inject drugs (National Institute of Public Health of
Kosovo, 2016).
In the HIV and AIDS classification system of the UNAIDS, Kosovo is considered a low level
epidemic country. However, the country is located in the region of South East Europe (SEE), which
is recognized as one of the regions with the fastest speed of spreading of HIV epidemic in the
world. The increase of risk factors faced by people in Kosovo, including changes in economic and
social conditions, suggest the need for strengthening surveillance, prevention and efforts to control
HIV and AIDS.
Although the prevalence of HIV is low, if not prevented at early stages, Kosovo has specific
elements that may lead to the expansion of the scale of the epidemic of HIV. As an economically
underdeveloped country with the highest unemployment rate in Europe and with few opportunities
for development in many aspects, young people aged 18-25 increasingly face particular challenges
that can lead to increased exposure and susceptibility to HIV. Kosovo possesses identifiable factors
that put people at risk for infection with HIV, such as: young population, high unemployment,
20
rapid social changes within the family and society, the growing problem of the narcotics industry,
booming of the sex industry, a stigmatized homosexual community, and high rate of population
migration, both within and outside Kosovo (Ministry of Health, 2003).
Kosovo’s young people face a world that is undergoing rapid change too. Social changes have a
direct impact on their attitudes and behavior, particularly in the sphere of sexual behavior and drug
use. Studies in Kosovo have shown that the age of sexual debut is declining rapidly among young
people, as well as the beginning of drug use (United Nations Kosovo Team, 2008). High level of
unemployment, especially among young people, has resulted migration to the Western European
countries. Unemployed young people mainly travel abroad on their own and without their partners,
which increases their vulnerability to HIV infection. Their limited knowledge and awareness on
HIV and other sexually transmitted diseases are major risk factors.
As mentioned above, adolescents and young adults constitute a considerable proportion of
Kosovo’s population. Factors like lack of information about HIV and AIDS, misconceptions,
stigma and discrimination, age of sexual debut that is declining rapidly, lack of voluntary testing
etc., increase the vulnerability to HIV and AIDS infection among adolescents and young adults.
There are only few researches on HIV and AIDS among adolescents and young adults in Kosovo.
Comprehensive and up-to-date studies on the knowledge, attitudes and risk perception are quite
limited. It is assumed that adolescents and young adults are probably going to be faced with
situations and circumstances that require informed decisions on how to live a sexually and
responsible life. Although Kosovo is still in an early stage of HIV infection, the rising rates of
infection in other central and eastern European countries suggest the need to understand HIV
knowledge, risk perception and attitudes towards people living with HIV and AIDS among
adolescents and emerging adults in Kosovo.
21
1.2 Organization of the study
This study is composed of six main chapters and several sub-chapters separated and designed
based on the American Psychological Association (APA) publication manual. The first chapter,
introduction, is composed of three sections. The first section is the introduction of the thesis where
the main problem of analysis is treated and properly framed. In addition, in the first chapter are
included key definitions and terminology that are used in this study include the following:
adolescence, emerging adulthood, HIV, AIDS, attitudes, risk perception, prevention, stigma,
prejudice etc. The third section of the first chapter is focused in a short summary of Kosovo cultural
and historical context.
Literature review is treated in the chapter two. This chapter is divided into several sub-chapters
which treat different aspects of the subject. In addition to the description of the main theoretical
considerations and main concepts used, in this section the health belief model is described as well.
This psychological model aims to explain and predict health behaviors of the subjects’ part in this
research project. Furthermore, the described model is focused on individual beliefs and attitudes
that determine the search for health solutions in response to the long-term illnesses such as HIV
and AIDS.
Moreover, adolescence is considered a period of life when a lot of psychological and physical
changes occur to an individual. This affects, among others, their attitudes, believes and values
towards others. On the other hand, emerging adult is a concept developed in recent decades in
industrialized societies which includes the period of life from 18-25 years old. Also, another
section is a summary of all the relevant reports, analysis and research documents that were
conducted in Kosovo from 2000 until 2017 regarding the HIV knowledge, risk perception of HIV
and attitudes towards people living with HIV and AIDS among adolescents and younger adults. In
the last part of this chapter the research questions and hypotheses of this thesis are described. In
total, there are four research questions and seven hypotheses examined and tested in this study.
It is important to emphasize that this study is divided in two main parts: study one and study two,
quantitative and qualitative research. Both these studies are presented in chapter three and chapter
22
four. The quantitative analysis (study one) is included in the chapter three. The first part of it
includes the methodological approach which is used to gather the necessary data. Questionnaires
were used as part of quantitative methods. For the purpose of this study, there were 1234 subjects,
in total, who participated in the survey. In addition to this, in the chapter three are included the
data analysis of the results derived from the questionnaire which were processed and analyzed by
using SPSS software. All the relevant data gathered from the questionnaires are presented in tables.
These are accompanied by a short but very concise and analytical description of the tables and the
respective correlations between variables.
On the other hand, the qualitative analysis (study two) is included in the chapter four. This is
conducted by using focus groups as the qualitative methodological approach. There were four
focus groups conducted (two with adolescents and two with emerging adults) with a participation
of 30 subjects. Thematic analysis was used as a method for the analysis of focus group transcripts.
This was done by using the qualitative software NVivo.
This part of the study was developed for two main aims: first, to deeply analyze socio-cultural
correlations with attitudes towards PLWHA, and level of knowledge and risk perception of HIV
among adolescents and emerging adults. Whereas, the second aim is to get a better understanding
on the subject and to confront these data with the data obtained from the quantitative analysis.
Also, the hypotheses raised in this study were analyzed in both chapters in relation to the findings
derived from the quantitative and qualitative analysis.
The chapter five, discussion, covered both analysis: qualitative and quantitative. In addition to this,
these findings then were compared and confronted with the studies, reports and academic papers
of other scholars around the world. Thus, this process – the discussion of the obtained data
compared and contrasted with data from other studies – created the opportunity to identify relevant
contextual factors which influence adolescents and emerging adults in Kosovo to have that
particular HIV knowledge, attitudes towards PLWHA and HIV risk perception.
Chapter six, which is the final chapter of this study, consists of a presentation of some concluding
remarks with regard to the issues that have been addressed during the course of this study. It
23
presents: implications for the theoretical areas that have been explored; implications for practical
programs of actions; a reflection of the difficulties and limitations encountered in this study; and
last, but certainly not least, a call for further researches concerning the knowledge, attitudes and
risk perception of adolescents and emerging adults in Kosovo regarding HIV in Kosovo.
1.3 Kosovo: short cultural and historical context
Kosovo is located in South Eastern Europe (SEE) and during the past years was part of political
unrest and military intervention. From 1989 to 1999, Kosovo was still part of the Federal Republic
of Yugoslavia, but extreme discrimination against the Kosovo Albanian population existed (Judah,
2008). In 1998, a war between the Kosovo Liberation Army and the Serbian military started. In
March 1999, NATO intervened and bombing continued until June 1999 when the Serbian military
retreated (Central Intellegence Agency: The World Factbook, 2017). During the conflict over
1.200.000 Kosovars were internally displaced or left Kosovo and most of the refugees went to the
neighboring countries. From the end of the war until 2008 Kosovo has been protectorate of the
United Nations (UNMIK) (Kosovar AIDS Committee, 2008). With a strong support of the
international community, Kosovo declared its independence on 17 of February 2008 and since
then was recognized by a considerable number of states worldwide.
The World Bank (WB) categorizes Kosovo as a lower-middle-income country with a solid
economic growth since the end of conflict. However, Kosovo continues to be the poorest area in
Europe with a per-capita domestic product of about $3,900 and with one-third of population living
below poverty line and nearly one-eighth in extreme poverty with regional disparities. The poorest
live in rural areas (65%). Furthermore, Kosovo has the highest unemployment rate in Europe of
around 30 per cent (39% women, and 27%) with nearly 70% long-term unemployed. The
unemployment rate among young people aged 15-24 is about 56% (68% women and 51% men)
(UNAIDS: Kosovo Narrative Report , 2017).
According to the report from the Agency for Statistics, Kosovo has a population of approximately
1.8 million people, of whom the majority are Albanians (92%), followed by Serbs (4%), Bosnians
and Gorans (2%), Turks (1%), and Roma, Ashkali and Egyptians (1%). About 96% of the
24
population are Muslim, while the Christian population is estimated at 3.69% (Catholic 2.2% and
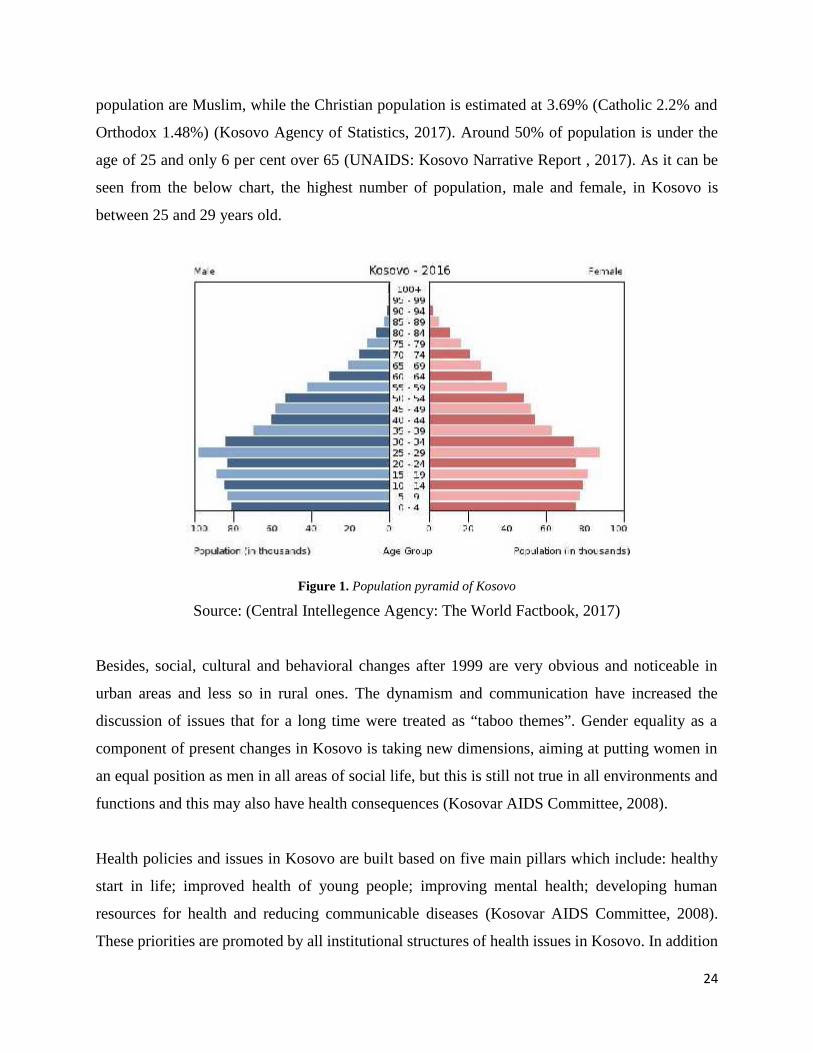
Orthodox 1.48%) (Kosovo Agency of Statistics, 2017). Around 50% of population is under the
age of 25 and only 6 per cent over 65 (UNAIDS: Kosovo Narrative Report , 2017). As it can be
seen from the below chart, the highest number of population, male and female, in Kosovo is
between 25 and 29 years old.
Figure 1. Population pyramid of Kosovo
Source: (Central Intellegence Agency: The World Factbook, 2017)
Besides, social, cultural and behavioral changes after 1999 are very obvious and noticeable in
urban areas and less so in rural ones. The dynamism and communication have increased the
discussion of issues that for a long time were treated as “taboo themes”. Gender equality as a
component of present changes in Kosovo is taking new dimensions, aiming at putting women in
an equal position as men in all areas of social life, but this is still not true in all environments and
functions and this may also have health consequences (Kosovar AIDS Committee, 2008).
Health policies and issues in Kosovo are built based on five main pillars which include: healthy
start in life; improved health of young people; improving mental health; developing human
resources for health and reducing communicable diseases (Kosovar AIDS Committee, 2008).
These priorities are promoted by all institutional structures of health issues in Kosovo. In addition

25
to this, the primary health care system in Kosovo is based in the Family Medicine concept which
provides decentralized primary health care in Family Health Centres (FHC). These FHC are
complemented by secondary regional hospitals and the only tertiary care institution the “Kosovo
University Clinical Centre” at the Pristina (Kosovar AIDS Committee, 2008). On the other hand,
the National Institute of Public Health is the main institution in Kosovo which is directly in charge
of developing the health strategy in the field of epidemiology, health education and promotion,
disease prevention and health information (National Institute of Public Health, 2017). Strategies
and policies developed and implemented by the Institute are approved by the Ministry of Health
(MH) of Kosovo.
26
~Chapter Two~Literature Review
27
CHAPTER II
LITERATURE REVIEW
2.1 Health Belief Model
Several theories and models have been developed and used to understand health seeking behavior
and health outcomes. The common general model used for analysis of health behavior is the Health
Belief Model (HBM), which has been used as one size fits all in health related studies. There are
several other models and theories used for studying health behavior of individuals such as the
social cognitive theory; theory of reasoned action and planned behavior; risk reduction model etc.
(Majelantle, Keetile, Bainame, & Nkawana, 2014).
The Health Belief Model was developed in the 1950’s. The model is based on the theory of Kurt
Lewin, himself a social psychologist (Odhiambo, 2012). This is a psychological model whose aim
is to explain and predict health behaviors (Green & Murphy, 2014). The model is focused on
individual beliefs and attitudes that determine the search for health solutions in response to the
long-term illnesses such as HIV and AIDS (Nakakuwa, 2015).
Taken together, the HBM suggests that individuals will take appropriate AIDS preventive action
if they have high levels of perceived susceptibility to, and high levels of perceived severity of
AIDS. Individuals also will take appropriate action if they believe that recommended action (such
as limiting sex to one regular partner) will be beneficial in reducing either their susceptibility to
AIDS, or the severity of the disease, and if they believe that the anticipated barriers to taking the
recommended action are outweighed by its benefits. The model also assumes that if the perceived
threat of the disease is high and perceived barriers to the recommended action is low, a cue to
action can prompt or trigger an individual to adopt and maintain AIDS preventive behavior
(Odhiambo, 2012).
According to Hochbaum, Rosenstock & Kegels (1952) the Health Belief Model states that the
perception of a personal health behavior threat is itself influenced by at least three factors:
28
1. General health values which include interest and concern about health;
2. Specific health beliefs about vulnerability to a particular health threat and
3. Beliefs about the consequences of the health problem (Hochbaum, Rosenstock, & Kegels,
1952).
In addition, according to this model, high perceived risk of harm should encourage people to take
action to reduce their risk. Although this implied positive relation between perceived risk and
subsequent protective behavior is observed in many empirical studies, it is often weaker than
expected (Noroozinejad, et al., 2013).
The Health Belief Model spells out four perceptions as the main constructs of the model: perceived
susceptibility, perceived severity, perceived benefits, and perceived barriers (Courtenay, 2000). It
is accordingly proposed that these concepts account for people’s “readiness to act” (Nakakuwa,
2015). Also, other constructs have been added to the Health Belief Model over time, such as: cues
to action that will activate that readiness and stimulate overt behavior; and self-efficacy or one’s
confidence in the ability to successfully perform an action (Glanz, Rimer, & Viswanath, 2008).
Perceived susceptibility or vulnerability (1) - to disease may be described as the subjective
perceived risk of contracting a disease (Nakakuwa, 2015). Individuals vary widely in their
perception of susceptibility to a disease or condition. Those at low end of the extreme deny the
possibility of contracting an adverse condition. Whereas, individuals in a moderate category admit
to a statistical possibility of disease susceptibility (Hochbaum, Rosenstock, & Kegels, 1952) as
well, those individuals at the high extreme of susceptibility feel there is real danger that they will
experience an adverse condition or contract a given disease. However, the perception of
susceptibility is not always linked to the adoption of healthier behaviors (Courtenay, 2000). For
example, adolescents and emerging adults who perceive themselves to be susceptible to HIV and
AIDS would more likely use condoms to protect themselves from the sexual transmission of the
disease (or have sex to one regular partner). On the other hand, the negative attitudes towards
people living with HIV and AIDS might be explained by the perceived chances to acquire HIV.
29
Perceived severity (2) - speaks to an individual’s beliefs about the seriousness or severity of a
disease (Hochbaum, Rosenstock, & Kegels, 1952). According to McCormick-Brown (1999), as
quoted by Nakakuwa (2015), the perception of seriousness is often based on medical information
or knowledge, it may also come from the beliefs a person has about the difficulties a disease will
create or the effect it will have on his or her life in general (Nakakuwa, 2015). For example, the
opinions of the subjects can be based on the perception that HIV infection is a serious condition
and the consequences of the disease are expected to be very severe.
Furthermore, the perceived susceptibility and severity of the disease are components of the theory
of Instrumentalism and symbolism largely consumed by Herek (1985) and Pryor et al (1989),
which state that personal attitudes towards HIV-infected people reflect the needs of the individuals
to avoid a threat by rejecting those affected by the disease (Perrin, 2010).
A perceived barrier (3) - however, action may not take place, even though an individual may
believe that the benefits to taking action are effective (Glanz, Rimer, & Viswanath, 2008). This
may be due to barriers. In fact, barriers relate to the characteristics of a treatment or preventive
measure may be inconvenient, expensive, unpleasant, painful or upsetting (Hochbaum,
Rosenstock, & Kegels, 1952). For example, adolescents and emerging adults may identify their
personal barriers with regard to using protective measures and explore ways to eliminate or reduce
these barriers.
The four major constructs or perceptions, as found in the HBM, are modified by other variables
such as: gender, age-group, educational level, employment status, permanent residence, parent’s
income etc. These socio-demographic characteristics are considered modifying factors of
knowledge and risk perception of HIV and personal attitudes towards HIV and AIDS people (See
Figure 2).
30
Figure 2. Health Belief Model
Source: Glanz, K., Rimer, B.K., & Lewis. F.M (2002)
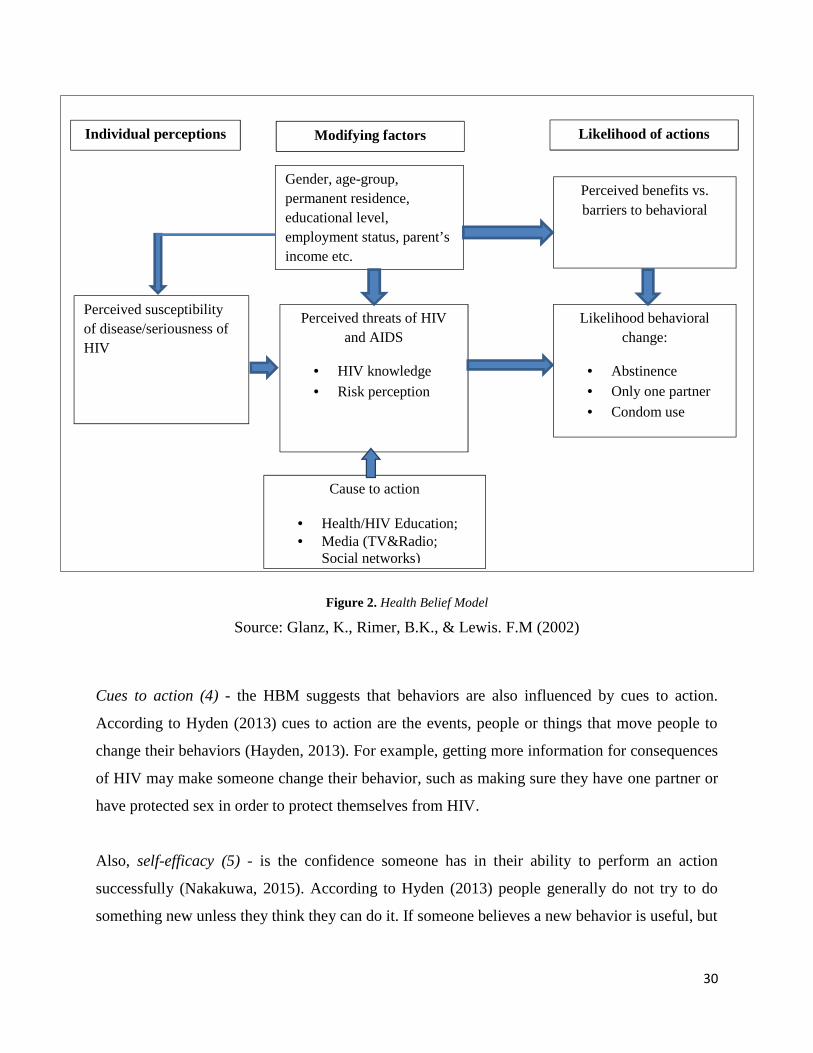
Cues to action (4) - the HBM suggests that behaviors are also influenced by cues to action.
According to Hyden (2013) cues to action are the events, people or things that move people to
change their behaviors (Hayden, 2013). For example, getting more information for consequences
of HIV may make someone change their behavior, such as making sure they have one partner or
have protected sex in order to protect themselves from HIV.
Also, self-efficacy (5) - is the confidence someone has in their ability to perform an action
successfully (Nakakuwa, 2015). According to Hyden (2013) people generally do not try to do
something new unless they think they can do it. If someone believes a new behavior is useful, but
Individual perceptions Modifying factors Likelihood of actions
Gender, age-group,permanent residence,educational level,employment status, parent’sincome etc.
Perceived threats of HIVand AIDS
HIV knowledge
Risk perception
Cause to action
Health/HIV Education; Media (TV&Radio;
Social networks)
Perceived benefits vs.barriers to behavioral
Likelihood behavioralchange:
Abstinence Only one partner
Condom use
Perceived susceptibilityof disease/seriousness ofHIV
31
does not think he or she is capable of doing it, the chances are that they will not try to perform that
action (Hayden, 2013).
The HBM has been applied to a broad range of health behaviors and subject populations.
According to Conner & Norman (1996) three broad areas of health behavior can be identified and
may include, 1) preventive health behaviors, which involve health-promoting (e.g. diet, exercise
and condom use), 2) health-risk (e.g. smoking, concurrent sexual partnerships) behaviors, and 3)
vaccination and contraceptive practices (Conner & Norman, 2005). Therefore, using some of the
main constructs of the Health Belief Model as a guide, this current study tried to provide valuable
information about a certain individual, relationship, and sociocultural correlates that should be
targeted when designing prevention programs on HIV and AIDS related knowledge, risk
perception and attitudes towards people living with HIV among adolescents and emerging adults
in Kosovo.
2.2 Key definition and terminology
According to Tuckman (1999) an operational definition must define the exact manner in which a
variable or a phenomenon is measured (Tuckman, 1999). Main concepts used in this current study
include, but are not limited to: adolescents, emerging adults, HIV, AIDS, attitudes, behaviors, risk
perception, stigma etc. The definition of these terms is based on three main sources, which by
academic community are considered as relevant for the field: A Oxford Dictionary of Psychology
published by Oxford University Press (Colman, 2015), APA Dictionary of Psychology published
by American Psychological Association (VandenBos, 2015) and other specific explanations
provided by other relevant authors and scholars. Scientific definitions of concepts used in the study
are given as follows:
Adolescence: The period of development from the onset of puberty to the attainment of adulthood,
beginning with the appearance of secondary sexual characteristics, usually between 11 and 13
years of age, continuing through the teenage years, and terminating legally at the age of majority,
usually 18 years of age (Colman, 2015). Currently there are a lot of misunderstandings and
disagreements among scholars in the field of psychology regarding the beginning and the end of
32
this time period in a life of a person. For the purpose of this study adolescence is defined between
13-18 years of age.
Emerging adulthood: A development stage that is neither adolescence nor young adulthood but is
theoretically and empirically distinct from them both, spanning the late teens through the twenties.
Emerging adulthood is a period of life that has developed in recent decades in industrialized
societies, lasting from about the age of 18 to 25. Arnett, coined the term in his book “Emerging
Adulthood: The Winding Road from the Late Teens Though the Twenties” (2014), where she
described emerging adulthood as the time from the end of adolescence to the young-adult
responsibilities of a stable job, marriage and parenthood. This developmental period, varies in
length depending in the certain cultures and certain times (Arnett, 2014).
The task of defining emerging adulthood still remains a confusing one due to the various factors
which mostly are cultural. For the purpose of this study, emerging adulthoods include persons
between 19-25 years of age.
HIV: Human immunodeficiency virus, a retrovirus that is transmitted through sexual contact,
infected blood or blood products, and from mother to child via the placenta and that breaks down
the human body’s immune system (Colman, 2015).
AIDS: Acquired immune (or immune-) deficiency syndrome, a disorder caused by the HIV
retrovirus and transmitted by infected blood entering the body. AIDS is a clinical condition in
which the immune system is so severely damaged from infection with human immunodeficiency
virus (HIV) as to allow serious opportunistic infections and diseases (Colman, 2015).
Knowledge: the state of being familiar with something or aware of its existence, usually resulting
from experience or study (VandenBos, 2015). As well, Kartz (1960) defines knowledge as a
function of attitude (Katz, 1960). For the purpose of this study subjects were considered to be
knowledgeable about ways of transmission or non-transmission of HIV, HIV prevention etc.
33
Attitudes: An enduring pattern of evaluative responses towards a person, object, or issue.
According to a frequently quoted classical definition, it is a more or less consistent pattern of
affective, cognitive, and conative or behavioral responses (or of feeling, thinking, and behaving)
towards a psychological object, but the consistency implied by this definition is a supposition that
is frequently unmatched by reality, and it is possible to have an attitude towards something without
ever having the opportunity to express it in behavior (VandenBos, 2015).
Risk perception: Risk has been defined in a number of ways, but is often seen as the likelihood
that an individual will experience the effect of danger (Short, 1984). Risk perception is the
subjective judgement that people make about the characteristics and severity of a risk. In relation
to HIV, risk perception is an indicator of perceived vulnerability to infection, a measure of one’s
understanding of HIV transmission as well as willingness to consider behavioral changes
(Breakwell, 2014). Risk perceptions vary according to factors such as past experiences, age,
gender, and culture.
Prevention: Behavioral, biological, or social interventions intended to reduce the risk of disorders,
diseases, or social problems for both individuals and entire populations (VandenBos, 2015).
Stigma: A mark or disgrace associated with a person, a personal quality, or personal circumstances
(Colman, 2015). Also, stigma is defined as behavior that unfairly and negatively impact upon the
rights, life and opportunities of a person actually living with HIV or ill with AIDS; or a person
associated (affected) with someone living with HIV or AIDS.
Stigmatization: Is defined as the act or process of stigmatizing a person or a group of people
(Colman, 2015).
Prejudice: a negative attitude towards another person or group formed in advance of any
experience with that person or group (VandenBos, 2015). Prejudice is typically conceptualized as
an attitude that, like other attitudes, has a cognitive component (e.g., beliefs about a target group),
an affective component (e.g., dislike), and a conative component (e.g., a behavioral predisposition
to behave negatively towards the target group).

34
Discrimination: Discrimination refers to unjustifiable negative behavior towards a group or its
members, where behavior is adjudged to include both actions towards, and judgements/decisions
about, group members. Correll et al. (2010, p. 46) provide a very useful definition of discrimination
as “behavior directed towards category members that is consequential for their outcomes and that
is directed towards them not because of any particular deservingness or reciprocity, but simply
because they happen to be members of that category” (Correll, Judd, Park, & Wittenbrink, 2010).
2.3 Adolescence and emerging adulthood as developmental stages
Adolescence, known as well as the second decade of life, is a time of great change. In this period
physical changes occur. Except physical changes – they also experience cognitive, emotional,
social and interpersonal changes as well. As they grow and develop, adolescents are influenced by
outside factors such as: parents, peers, community, culture, religion, school, technology, media,
social networks etc.
The process of adolescence is a period of preparation for adulthood during which time several key
developmental experiences occur. Besides physical and sexual maturation, these experiences
include movement towards social and economic independence, development of identity, the
acquisition of skills needed to carry out adult relationships and roles, and the capacity for abstract
reasoning (World Health Organization, 2017). While adolescence is a time of tremendous growth
and potential, it is also a time of considerable risk during which social contexts exert powerful
influences. This is a particular stage of social, emotional and intellectual development which
influences a young individual towards an adult individual. This is mainly a social and cultural
phenomenon. Currently there are also a lot of misunderstandings and disagreements also among
scholars in the field of psychology regarding the beginning and the end of this time period in a life
of a person.
The beginning and the end of adolescence is different and, at the same time, can be and is
influenced by the particular country and, to be more accurate, culture and, on the other hand, is
depended by special features of an individual. However, it is defined as intermediate ages through
35
which everyone must pass in order to reach the necessary maturity and to gain the status of the
adult.
The term adolescence is commonly understood to define the period of life between childhood and
adulthood. This time frame of a certain individual, however, not only describes a very diverse
reality, but adolescence varies considerably across cultures, over time, and within individuals too.
Just as cultures differ qualitatively from one another in terms of identifying and defining their
adolescents, so the term adolescence differs qualitatively across time and history (Kaplan, 2004).
It is generally known that the scientific study of adolescence began with the publication of G.
Stanley Hall's (Hall, 1904). Hall’s adolescence was one of the seminal works of the early history
of psychology, and in Hall's view, adolescence extended from age 14 to age 24 (Arnett, 2007).
Contrary, contemporary scholars generally consider adolescence to begin at age of 10 or 11 and to
end by the age of 18 or 19. The task of defining adolescence remains a confusing one due to the
fact that adolescents themselves are influenced by various factors that determine when childhood
ends and adulthood begins (Degner, 2006).
The meaning of adolescence has changed during the last 12 centuries as education; social
relationships and the importance of peer relations have undergone a considerable change over a
period of generations (Hurrelmann, 1987). Some authors argued that development in technology
too had impact in adolescence. Young people in this age group have in common: living with their
parents, experiencing the physical changes of puberty, they are attending secondary school, and
are part of a school-based peer culture. Therefore, for the needs of the study we will refer to the
age of 10-18, as a general acceptable definition for adolescents.
According to many authors, adolescence is characterized by several developmental characteristics
which include aspects such as: physical (1), cognitive (2), moral (3), spiritual (4), psychological
(5), social-emotional (6), (Caskey & Anfara, 2014). In order to describe them better, for each of
these developmental characteristics of adolescence, a short, but very concise, analysis is provided.
Adolescent Physical Development: the early stage of adolescence is a time of great physical
development. Despite the fact that sometimes it seems that adolescents’ bodies change overnight,

36
the process of sexual maturation actually occurs over a period of several years. The sequence of
physical changes is largely predictable, but there is great variability in the age of onset of puberty
and the pace at which changes occur (Kipke, 1999).
Physical development refers to bodily changes which include: growth, fine motor skills, biological
maturity etc. Developmental growth includes significant increases in height, weight, and internal
organ size as well as changes in skeletal and muscular systems (Kellough & Kellough, 2008), with
growth spurts occurring about two years earlier in girls than boys (Brighton, 2007).
For most adolescents, sexual maturation involves achieving fertility and the physical changes that
support fertility. For girls, these changes involve breast budding, which may begin around age 10
or earlier, and menstruation, which typically begins at age 12 or 13.9 (Archibald, Graber, &
Brooks-Gunn, 1999). On the other hand, for boys, the onset of puberty involves enlargement of
the testes at around age 11 or 12 and first ejaculation, which typically occurs between the ages of
12 and 14. The development of secondary sexual characteristics, such as body hair and (for boys)
voice changes, occurs later in puberty (Archibald, Graber, & Brooks-Gunn, 1999).
Adolescent cognitive development: refers to the increased ability of people to understand, think
and reason. During early adolescence, youth exhibit a wide range of individual intellectual
development including meta-cognition and independent thought (Caskey & Anfara, 2007). They
tend to be curious and display wide-ranging interests (Kellough & Kellough, 2008). Although few
significant differences have been identified in the cognitive development of adolescent boys and
girls, it appears that adolescent boys and girls do differ in their confidence in certain cognitive
abilities and skills. Adolescent girls tend to feel more confident about their reading and social skills
than boys, and adolescent boys tend to feel more confident about their athletic and math skills
(Eccles, Bonnie, Deborah, Oksana, & Vida, 1999).
Adolescent moral development: is generally defined as an individuals' ability to make principled
choices and how to treat one another. During early adolescence, many of the attitudes, beliefs, and
values that young adolescents develop remain with them for life (Caskey & Anfara, 2007).Thus,
37
adults can help facilitate moral development in adolescents by modeling altruistic behaviors
towards other people.
Adolescent spiritual development: is defined as a developmental process for making meaning of
one's life (Lingley, 2013). Young adolescents often want to explore spiritual matters, develop
connections between self and others, and gain a sense of themselves and the world (Caskey &
Anfara, 2014).
Adolescent psychological development: is characterized by identity formation and the search for
independence. During adolescence individuals seek their own sense of individuality and
uniqueness. They may experience an increased awareness of their ethnic identity as well (Caskey
& Anfara, 2014). As young adolescents search for an adult identity and adult acceptance, they
strive to maintain peer approval (Kellough & Kellough, 2008). Also, adolescents want greater
independence and responsibility. They increasingly want to assert more autonomy over their
decisions, emotions and actions and to disengage from parental control. Their social and cultural
environment importantly affects how adolescents express this desire for autonomy (Montgomery,
2005).
Adolescent social-emotional development: concerns a person's capacity for mature interactions
with people. Emotional development occurs uniquely for each adolescent. Emotional development
during adolescence involves establishing a realistic and coherent sense of identity in the context
of relating to others and learning to cope with stress and manage emotions, processes that are life-
long issues for most people (Santrock, 2016).
Young adolescents have a strong need to belong to a group—with peer approval becoming more
important and adult approval decreasing in importance (Caskey & Anfara, 2007). Adolescents
experience a variety of peer association: positive and negative as well. During early adolescence,
individuals typically widen their circle of friends (Brighton, 2007) and may experience feelings of
romantic or sexual attraction (Caskey & Anfara, 2014). On the other hand, family serve a number
of important functions throughout adolescence. Strong sense of closeness, and attachment to
family has been found to be associated with better emotional development, better school
38
performance, and engagement in fewer high-risk activities, such as drug use (Gentry & Campbell,
2002).
In summary, adolescence is a multi-factorial and complex maturational phase; with great variation
across individuals and cultures around the world. Six developmental characteristics of adolescence
are interrelated and each affects another characteristic. Each of them is influenced by different
factors, like race, ethnicity, gender, culture, family, community, and environment.
On the other hand, emerging adulthood is a period of life that has developed in recent decades in
industrialized societies, lasting from about the age of 18 to 25. Arnett, coined the term in his book
“Emerging Adulthood: The Winding Road from the Late Teens Though the Twenties” (2014),
where he described emerging adulthood as the time from the end of adolescence to the young-
adult responsibilities of a stable job, marriage and parenthood (Arnett, 2000). This developmental
period, varies in length depending in the certain cultures and certain times.
During the period, late teens to mid-20s, emerging adults attain a subjective sense that they have
reached adulthood and are ready to take on the full range of adult responsibilities (Arnett, 2014).
As a result, emerging adults share the five characteristics as the age of identity exploration (1), the
age of instability (2), the self-focused age (3), the age of feeling in between (4), and the age of
possibilities (5), (Trible, 2015). These features have received empirical support (Reifman, Jensen.,
& Colwell, 2003).
All of these five features of emerging adulthood are different. Identity of exploration is perhaps
the most central features of emerging adulthood (Arnett, 1997); is the time when young people
explore possibilities in areas of life, in particular love and work. Another feature of emerging
adulthood is instability (Trible, 2015). For example, the best illustration of the instability of
emerging adulthood is in how often they move from one residence to another. Self-focused is
another feature of this period. Children and adolescents are self-focused in their own way, but they
always have parents and teachers to answer to, and usually siblings as well. Another feature of this
period-emerging adulthood-is also, feeling in between (Arnett, 1997), when most people live in
their parents’ home and are required to attend secondary school, and young adulthood, when
39
people have entered marriage and parenthood and have settled into a stable occupational path. The
last feature is age of possibilities, when many different futures remain open; when little about a
person’s direction in life has been decided for certain (Trible, 2015).
There have been a number of important theoretical contributions to the understanding of
development from the late teens through the twenties. One of the earliest theoretical contributions
was made by Erik Erikson (1950, 1968). Erikson wrote of development in adolescence and of
development in young adulthood (Arnett, 2000). He also commented on the prolonged
adolescence typical of industrialized societies and on the psychosocial moratorium granted to
young people in such societies “during which the young adult through free role experimentation
may find a niche in some section of his society” (Erikson, 1994, p. 156). Hence, Eric Erikson
seems to have distinguished a period that is in some ways adolescence and in some ways young
adulthood, a period in which an adult’s commitments and responsibilities are delayed while the
role of experimentation that began in adolescence continues (Arnett, 2000).
One more theoretical contribution to understand development from the late teens through the
twenties can be found in the work of Daniel Levinson (1978). Levinson developed a theory that
included development in the late teens and the twenties; he called ages 17-33 the novice phase of
development and argued that the overriding task of this phase is to move into the adult world and
build a stable life structure (Arnett, 2000). During this process, according to Levinson, the young
person experiences a considerable amount of change and instability while sorting through various
possibilities in love and work in the course of establishing a life structure (Levinson, 1978).
Also, perhaps the best-known theory of development in the late teens and the twenties is Kenneth
Keniston's theory. Keniston’s term youth was the period between adolescence and young adult,
conceptualized by the idea of change, movement, freedom and ambivalence towards society as a
whole (Keniston, 1962). This period was a time of experimentation and a time to wrestle with the
questions of vocation, social role and lifestyle (Arnett, 2000). However, as we saw in description
above, there is good empirical support for conceiving this period, known as the emerging
adulthood period.
40
While Erikson (1968), Levinson (1978), and Keniston (1971) all contributed to the theoretical
groundwork for emerging adulthood, the nature of the period has changed considerably since the
time of their writings, too many years ago (Stewart, 2016). But, demographic changes in the timing
of marriage and parenthood in recent decades have made a period of emerging adulthood typical
for young people in industrialized societies (Arnett, 2000).
Emerging adulthood is a period characterized by change and exploration for most people
(Rindfuss, 1991). It is in many aspects the age of possibilities, a period in which many different
potential futures remain possible and personal freedom and exploration are higher for most people
than at any other time. Not all young people experience their late teens and twenties as years of
change and exploration (Arnett, 2000). Some lack the opportunities to use those years as a
volitional period; others may be inclined by personality or circumstances to limit their explorations
or to seek a relatively early resolution to them. However, we can characterize emerging adulthood
as a period when change and exploration are common for most of people.
2.3.1 Why emerging adulthood is not “late adolescence”
Adolescence, even “late adolescence” is an entirely inadequate term for college students or anyone
else who is in the age period from the late teen through the mid-twenties (Arnett, 2014). True,
adolescents and most adults have in common not yet entering marriage and parenthood. According
to Arnett, adolescents and emerging adults differ in some ways; some of them we will discuss
below.
Virtually all adolescents (ages 10–18) live at home with one or both parents. Contrary, most
emerging adults have moved out of their parents’ homes, and their living situations are diverse.
Almost all adolescents experience dramatic physical and in contrast, emerging adults have reached
full reproductive maturity (Larson, Wilson, Brown, Furstenberg, & Verma, 2002). As well,
virtually all adolescents attend secondary school, and, many emerging adults are enrolled in
college, but nowhere near all of them.
41
According to Arnett, adolescents also have in common that they have the legal status of minors,
not adults. They cannot vote, they cannot sign legal documents, and they are legally under the
authority and responsibility of their parents in a variety of ways (Arnett, 2014). In contrast, from
age 18 emerging adults have all the legal rights of adults (Larson, Wilson, Brown, Furstenberg, &
Verma, 2002). Through the above-mentioned and other aspects, emerging adults are different from
adolescents.
As a result, “late adolescence’’ is an inadequate term for describing them. The term emerging
adulthood is preferable because it distinguishes them from adolescents while recognizing that they
are not yet fully adults (Arnett, 2006).
In this particular part of second chapter, we outlined what adolescence is and which the
developmental characteristics of adolescence are. As well, we outlined what emerging adulthood
is and what the distinguishing features of emerging adulthood are. Special attention was dedicated
to the theoretical contributions to the understanding of the development from the late teens through
the twenties and as well as the different stages of adolescence and emerging adulthood.
2.4 Attitudes: the concept and formation
Attitudes have long been considered an essential concept of social psychology. At the same time,
attitudes have been an interest of researchers in the past ten years and hundreds of studies covering
almost every conceivable topic about which attitudes might be expressed. Because attitudes are an
important influence on people, they take up a central place in social psychology. In fact, early
researches have defined social psychology as the scientific study of attitudes (Fiske, Gilbert, &
Lindzey, 2010) and in 1954 Gordon Allport noted, “This concept is probably the most distinctive
and indispensable concept in contemporary American social psychology” (Droba, 1933). As one
may expect of any concept that has received decades of attention, the concept of attitudes has
changed over the years and has also involved extensive debates and controversies.
According to Pickens (2006), when we refer to a person’s attitudes, we are trying to explain his or
her behavior. Attitudes are a complex combination of things we tend to call personality, beliefs,
42
values, behaviors, and motivations (Pickens, 2005). As well, attitudes help us define how we see
situations, as well as define how we behave towards the situation or object. The initial definitions
of attitudes were broad and included some components like cognitive, affective, motivational, and
behavioral components. For example, Allport (1935) defined an attitude as “a mental and neural
state of readiness, organized through experience, exerting a directive and dynamic influence upon
the individual’s response to all objects and situations with which it is related”. A decade later,
Krech and Crutchfield (1948) wrote, “An attitude can be defined as an enduring organization of
motivational, emotional, perceptual, and cognitive processes with respect to some aspect of the
individual’s world” (Hogg & Tindal, 2008).
As stated above, the concept of attitude occupies a very favored position in social psychology and
examination of the various definitions and discussions of attitude offered by social psychologists,
reveal that there is an amazing diversity of conceptions of what the term denotes. But, we consider
that definition of attitudes that is more related to the research is: “a favorable or unfavorable
evaluative reaction towards something or someone exhibited in one’s beliefs, feelings, or intended
behavior” (Myers, Psychology, 2011).
Attitudes’ structure can be described in terms of three components. Affective component: this
involves a person’s feelings or emotions about the attitude object. Behavioral component: is the
intention to behave in a certain way towards an object or a person, and cognitive component: this
involves a person’s belief or knowledge about an attitude object. This model is known as the ABC
model of attitudes (McLeod, 2014).
Attitudes involve what people think, feel and how they would like to behave towards an attitude
object: are developed over a period of time and are usually based on principles that on the other
hand are influenced by the surrounding social environment. In addition to this, attitudes can be
influenced by personal experiences, religious, cultural, legal and specific environmental factors.
Furthermore, attitudes differ not only among racial, national, and occupational groups, but change
over a period of time within any given group or section of society.
43
2.5 Adolescents, emerging adults and HIV and AIDS
2.5.1 Knowledge of HIV and AIDS among adolescents and emerging adults
HIV has become one of the most serious health problems in the world with unforeseen
consequences. It is universally agreed that this disease is a global challenge that has threatened the
very existence of the human race. Presently, there is no country in the world without HIV and
AIDS cases.
HIV knowledge during adolescence has been projected to be a possible predictor of engagement
in current and future risky sexual behaviors (Kline, 2014). Globally it is known that there is a lack
of HIV knowledge among individuals between the ages of 15-24 (Maimaiti, Shamsuddin,
Abdurahim, Tohti, & Maimaiti, 2010). In many parts of the world, the age-group of 15-24 are at
particularly high risk of HIV infection from unprotected sex between men and intravenous drug-
use because of the very high prevalence rates often found amongst people who engage in these
behaviors. They are also often especially vulnerable to exploitation that may increase their
vulnerability to HIV infection.
Below we will discuss and analyze some of the research studies conducted in many parts of the
world regarding knowledge towards HIV. We will be focused in studies that treated adolescents
and emerging adults’ knowledge towards HIV.
Knowledge of how HIV is transmitted is one of many factors that enable individuals to protect
themselves from the infection. Accurate and sufficient knowledge can also reduce stigma and
discrimination against people living with HIV and AIDS. HIV knowledge among age-groups of
15-24 globally constitutes a major challenge to control the infection. Most people become sexually
active in adolescence. The need to admit that adolescents are having sex, but lack the proper
knowledge to protect themselves is important in the fight against HIV and AIDS. Young people
are now the epicenter and bear a disproportionate burden of this pandemic (Nambatya, 2010).
In sub-Saharan Africa, surveys continue to indicate that young people between 15-24 years of age
harbor serious misconceptions about HIV and how it is transmitted (Wodi B. E., 2005). Even
44
though it is considered now a common knowledge that HIV cannot be transmitted through
mosquito bites, many young people still believe that mosquitoes are a good vehicle for HIV
transmission (Nambatya, 2010). Another common misconception about AIDS includes the idea
that all HIV-infected people appear ill and are easily identifiable. Studies conducted in Ethiopia
among young people highlight decreased usage of condoms and the lack of HIV and AIDS
transmission knowledge (Paul, 2011). Furthermore, a cross-sectional study among high school
students revealed that only 41% of female students and 44% of male students were educated on
the various modes of HIV transmission (Alene, Wheeler, & Grosskurth, 2004). Likewise, the
national survey of Ethiopia reported a similar trend, whereby 28.7% of young men and only 15.8%
of young women were knowledgeable on the varied modes of horizontal HIV and AIDS
transmission (Paul, 2011).
Studies among African American adolescents as, Inungu, Langford, Mumford, and Younis (2009)
found out that misconceptions regarding HIV transmission are common among age group of 18-
30. For example, 35% of college students stated that they did not know whether or not mosquitoes
could transmit HIV. Similarly, studies conducted on African American adolescents have shown
low levels of HIV and AIDS knowledge (Kline, 2014). Another study conducted among African
Americans found out that only 50% of participants answered correctly in HIV knowledge and were
at least accurate concerning effective condom use and HIV testing. In the search for associated
socio-demographic and psychological factors, greater knowledge was associated with sexual
experience and, among experienced adolescents, with sexually transmitted infection/HIV testing
and-unexpectedly-less condom use (Swenson, et al., 2010).
Countless studies are conducted in Europe regarding HIV knowledge among the group age 11-25.
Goodwin, Kozlova, Nizharadze, and Polyakova (2004) conducted research in three different
countries: Russia, Georgia and the Ukraine (Goodwin, Kozlova, Nizharadze, & Polyakova, 2004).
Among the age group of 14-17 they found out that this age group is less knowledgeable about the
ways of HIV transmission. Contrary to the studies above, good knowledge of HIV among
adolescents was shown in a study conducted in Finland (Potsonen & Kontula, 1999). Both young
men and young women showed good level of knowledge concerning HIV.
45
Also, a study conducted among the age group 17-23 in Turkey (2005) showed that 95% of students
were aware of AIDS by its definition and its causation. More than 88% had knowledge that HIV
could be detected through blood test (Koksal, Namal, Vehid, & Yurtsever, 2005). A study
conducted in Germany among the age group 12-20 showed that HIV and AIDS was the infection
most participants had heard of (Samkange-Zeeb, 2013). Study conducted by six European Union
(EU) countries- Austria, Germany, Italy, Poland, Slovak Republic, Slovenia (2007) among the age
group 18-25 found that 76% of the participants answered correctly that AIDS can be treated, but
not completely cured. There are still 15.9% who believe that AIDS cannot be treated at all, and
further 2.4% who suggest that AIDS can be completely cured. Despite inconsistencies, the study
showed that participants have high level of basic knowledge about HIV. In addition, this study
showed that there are no striking differences according to the country of living. Nevertheless the
Austrians with 96.7% have most representatives in the high knowledge category, and the Italians,
with 85.6% - least (Netzelmann, et al., 2007).
Likewise, data from an empirical research in Czech Republic shows that adolescents have solid
knowledge about the channels of HIV transmission. However, they do not consistently apply this
knowledge to their sex lives (Rabu, 2003). This fact proves that providing information about HIV
along with instructions for safe behavior can aware people about the dangers involved, but this is
insufficient to encourage behavioral change.
AIDS is an important public health problem because of the complex, emotional, behavioral, and
psychosocial complications that accompany the physical illness. The only way to combat a disease
that has no cure is to prevent it. On the other hand, the best single way to prevent the disease is
through education therefore knowledge towards HIV and AIDS is very important for prevention,
care and support for people living with HIV and AIDS.
2.5.2 Attitudes of adolescents and emerging adults towards people with HIV and AIDS
The issue of stigmatizing attitudes constitutes another barrier to HIV infection prevention. Still
there is a great deal of stigma in the world today about HIV and AIDS. The stigma associated with
HIV and AIDS has threatened the physical and psychological well-being of the people infected.

46
This assumption is supported by many scholars. People with HIV seem as being responsible for
their infection especially in the places where a high stigma towards AIDS exists. These persistent
negative societal responses play a critical role in the experiences of people with HIV and AIDS.
However, some studies in different countries of the world have shown negative attitudes towards
HIV and AIDS, on the other hand, a significant part of the studies have shown tolerant and positive
attitudes towards people living with HIV and AIDS.
The stigmatizing attitudes are reported in a lot of international empirical studies in the world. A
study carried out in India, South Africa and United States on the attitudes towards PLWHA,
observed that stigmatizing attitudes towards them may reduce people’s willingness to have
themselves tested for HIV, thereby increasing the risk of transmission (Ndifon, 2005).
Stigmatizing attitudes are reported in the research conducted in Turkey by Koksal et al. (2005). In
this study, there were identified a substantial negative and intolerant attitudes towards people with
HIV and AIDS (Koksal, Namal, Vehid, & Yurtsever, 2005). Their attitudes towards infected
workers were unfavorable. In addition, it is reported that, 61.6% of the participants believed that
HIV-infected persons should not be allowed to work anymore. Whereas, a study conducted in Indi,
an age group of 14-16 showed that one third of participants would not allow HIV people to enter
school (Brook, 1993). Nineteen percent of students in a study in Israel declared that HIV-positive
students should not be allowed to continue their studies because they can endanger their fellow
students (Agrawal, Rao, Chandrashekar, & Coulter, 1999). The level of discriminatory attitudes
towards HIV-infected persons was high among Korean adolescents too (Sohn & Park, 2012). They
displayed a high level of discrimination against people with HIV and AIDS in some situations,
particularly in making him/her feel disgusted, avoiding sitting with people living with HIV, and
blaming those infected with HIV.
These negative attitudes will lead to discrimination. In addition, the negative approach can
significantly influence the infected person not to ask for medical treatment in time. As a
consequence, this will worsen their health too. These kind of attitudes influence the creation of
prejudice against those living with HIV and AIDS as well as marginalizing and excluding
individuals. Ultimately, such attitudes allow societies to excuse themselves from the responsibility
of caring for and looking after those who are infected with HIV.
47
Contrary to the findings above, there are different empirical researches that showed some
supportive attitudes towards people living with HIV and AIDS. For example, a study conducted
in Turkey, among high school students, found out that about half of the participants believed that
people with HIV and AIDS should be able to attend school and should not have to stop working
(Savaser, 2003). On the other hand, in a survey done with adolescents in Jamaica found a very
strong empathy and an overall supportive attitude for people with HIV and AIDS (Robillard,
2001). Almost the same conclusions are found in a research done in China. According to these
data generally the respondents’ attitudes towards people living with HIV and AIDS in China
were found to be accepting and quite positive (Tan, Pan, Zhou, Wang, & Xie, 2007).
Additionally, they showed strong willingness and supporting approaches to live in the same
community with people infected by HIV and AIDS.
Furthermore, a study conducted in India showed as well supportive attitudes towards people living
with HIV. Among the respondents about 93% were of the opinion that AIDS patients should not
be isolated from the society, 26% felt sympathetic towards people living with HIV and AIDS; 70%
of participants responded that they would not hesitate to sit next to a PLWHA in the bus. About
23% stated that they would be uneasy and apprehensive if their child’s classmate had HIV and
AIDS, whereas 13% opined that infected children should attend regular schools (Malleshappa &
Krishna, 2012).
2.5.3 HIV and AIDS-related stigma and its associated prejudice and discrimination
Stigma, as a social phenomenon, is not new to the infected individuals, health communities and
the wider public. In addition, this is not something that occurs only and exclusively to the HIV
infected individuals. Stigma is a frequent reaction to various diseases. Throughout history, many
diseases have brought stigma, including: tuberculosis, cancer, mental illnesses and many different
sexually transmitted infections (Catalán, 2002).
Stigma is considered as a very complicated issue that has deep roots in the complicated domains
of gender, race, ethnicity, religion, class, sexuality, and culture. As such, stigma cannot be
understood very easily, nor is it readily addressed, and above all it is such a complex phenomenon.
48
In this regard, stigma usually makes the disease more complex, difficult to discuss and harder to
deal with (Valdiserri, 2002).
Even though it is perceived that stigma is new as a social phenomenon, in fact it is not. The term
stigma dates back to the Greeks who cut or burned marks onto the skin of criminals, slaves, and
traitors in order to identify them as tainted or immoral people that should be avoided (Goffman E.
, 1980). However, as we know it today, stigma is not simply a physical mark, but rather an attribute
that results in widespread social disapproval. Stigma attached to HIV and AIDS is still a global
problem.
The concept of stigma has undergone important changes in definition and characterization since
its initial articulation by the Erving Goffman in the 1960. In the meantime, studies on stigma have
grown dramatically over the past two decades, particularly in social psychology (Link and Phelan,
2001). Based on APA Dictionary of Psychology (2015), stigma is defined as the negative social
attitude attached to a characteristic of an individual that may be regarded as a mental, physical, or
social deficiency. A stigma implies social disapproval and can lead unfairly to the discrimination
against and exclusion of the individual.
One of the curious aspects of literature concerning stigma is the variability that exists in the
definition of the concept (Link & Phelan, 2001). In many situations, investigators provide no
explicit definition and seem to refer to something like the dictionary definition (“a mark of
disgrace”), or to some related aspect like stereotyping or rejection. When stigma is explicitly
defined, many authors quote Goffman’s definition of stigma as an “attribute that is deeply
discrediting” and that reduces the bearer “from a whole and usual person to a tainted, discounted
one” (Goffman E. , 1980, p. 3). Stigmatization is also defined as an intertwined mix of perspective
(perceiver vs. target), identity (group-based vs. personal) and cognitive-affective-behavioral
response (Beaulieu, Adrien, Potvin, & Dassa, 2014).
Since Goffman, alternative or differently elaborated definitions have varied considerably. For
example, Stafford & Scott (1986) propose that stigma “is a characteristic of persons that is contrary
to a norm of a social unit” where a “norm” is defined as a “shared belief that a person ought to
49
behave in a certain way at a certain time” (Link & Phelan, 2001, p. 386). The modern idea of
stigma owes a great deal to Goffman, who viewed stigma as a process based on the social
construction of identity (Kleinman & Hall-Clifford, 2009). Persons who become associated with
a stigmatized condition thus pass from a “normal” to a “discredited” or “discreditable” social status
(Goffman, 2009). In his original discussion of stigma, Goffman included both psychological and
social elements, but his ideas have primarily been used in the analysis of the psychological impact
of stigma on individuals. This has created an understanding of the psychology of the stigmatized,
focusing on the processes by which stigma is internalized and shapes individual behavior. Yet, this
has been to the exclusion of considerations of how social life and relationships are changed by
stigma (Kleinman & Hall-Clifford, 2009).
Lately, Pryor and Reeder developed a taxonomy that seeks to bring greater conceptual clarity to
the current term, but diverse literature on stigma. According to them there are four types of stigma.
The first type of stigma is public stigma. Their model represents people’s social and psychological
reactions to someone they perceive to have a stigmatizing condition (Stutterheim S. E., 2011). This
type of stigma comprises cognitive (stereotypes), affective (prejudice), and behavioral
(discrimination) components and reflects the perspective of the perceiver (Stutterheim, et al.,
2009). The second type of stigma according to the Pryor and Reeder’s model is self-stigma. This
type of stigma reflects the social and psychological impact of possessing a stigma (Bos, Pryor,
Reeder, & Stutterheim, 2013). Further, the third type of stigma is stigma-by-association. This
model entails social and psychological reactions to people associated with a stigmatized person.
Authors also include the impact of being connected to a stigmatized person in the concept of
stigma-by-association (Stutterheim S. E., 2011). The final type of stigma mentioned by Pryor and
Reeder is institutional stigma. This type of stigma is denied as the legitimatization and perpetuation
of a stigmatized status by society’s institutions and ideological systems (Bos, Pryor, Reeder, &
Stutterheim, 2013). Furthermore, it reflects the previously mentioned growing trend towards
acknowledging structural factors and the role of power and dominance in stigmatization processes.
Some modern illnesses have been as extensively stigmatized as HIV (Black & Miles, 2002) and
also particular cultures or communities stigmatize certain behaviors in different ways. In addition
to this, because HIV is a condition that is often acquired through volitional behavior (Stutterheim
50
S. E., 2011; Bos, Dijker, & Koomen, 2007), many consider people living with HIV personally
responsible for having HIV or associate HIV with certain behaviors viewed by many people as
socially unacceptable such as homosexuality, intravenous drug use and commercial sex work (Bos,
Kok, & Dijker, 2001). All these perceptions contribute, in one way or another, to HIV being a
powerfully stigmatizing condition. It is unfortunately a well-established fact that many people
living with HIV and AIDS (PLWHA) suffer from stigma and discrimination, especially those
already marginalized by gender, race and socio-economic status (Kippax, Aggleton, Moatti, &
Delfraissy, 2007).
HIV-related stigma affects care and treatment of people living with HIV in a number of ways and
across a broad range of settings. Manifestations of stigma include, but are not limited to: avoidance,
exclusion, rejection, isolation, social ostracism, blaming, violence, service denial, physical
distance, indifference, awkward social interaction and being advised to conceal one’s status
(Catalán, 2002). Related settings in which stigmatization can occur are with families, in
communities, among friends, with sexual partners, health care settings, the housing sector, in the
in financial services sector, within religious institutions, at work, while travelling or migrating,
and in educational settings (Stutterheim, et al., 2009; Simbayi, et al., 2007; Carr & Gramling,
2004). As a consequence, stigma prevents people infected with HIV from seeking advice,
receiving proper health and psychosocial care, and taking prevention measures to avoid infecting
others (Patnerships in health, 2008).
For people living with HIV and AIDS (PLWHA), stigma has important negative consequences,
such as physical and social isolation, violence, loss of livelihood and housing, differential
treatment in educational and health institutions, limitation of travel opportunities, limitation of the
sexual life, disruption of social identity, and loss of agency (Öktem, 2015). Also, consequences of
HIV negatively impacts social interactions between people with HIV and others, and can result in
decreased social network size, limited social support, and social isolation (Stutterheim S. E., 2011).
Also, it can impact not only people living with HIV but also their family members and
communities as well. Psychologically reasoning HIV-related stigma can generate significant
distress in the form of depression, anxiety, and lowered self-esteem (Lee, Kochman, & Sikkema,

51
2002; Stutterheim S. E., 2011). Obviously, the negative consequences of stigmatization towards
people living with HIV and their family members are substantial.
Throughout psychology’s history, researchers have evinced strong interest in understanding
prejudice and discrimination (Dovidio, Hewstone, Glick, & Esses, 2010). The concept of prejudice
as a subject of social psychological inquiry emerged around the 1920s (Samelson, 1978).
Prejudice, however, is a complex construct, and its definition involves several awkward problems.
As a result, a large number of different definitions have been proposed.
Prejudice is a preconceived negative judgment of a group and its individual members. Some
prejudice definitions include positive judgments, but nearly all uses of “prejudice” refer to negative
ones-what Gordon Allport termed in his classic book, The Nature of Prejudice, “an antipathy based
upon a faulty and inflexible generalization” (Allport, 1979, p. 9). In his seminal volume, Allport
(1954) defined prejudice as ‘an antipathy based on faulty and inflexible generalization. It may be
felt or expressed. It may be directed towards a group as a whole or towards an individual because
he is a member of that group (Dovidio, Hewstone, Glick, & Esses, 2010). Most researchers have
continued to define prejudice as a negative attitude. Recent definitions of prejudice, bridge the
individual-level emphasis of psychology and the group-level focus of sociology by concentrating
on the dynamic nature of prejudice. Eagly and Diekman (2005), for example, view prejudice as a
mechanism that maintains status and role differences between groups (Eagly & Diekman, 2005).
Like many attitudes, prejudice is complex. For example, it may include a component of patronizing
affection that serves to keep the target disadvantaged. Prejudice is an attitude. An attitude is a
distinct combination of feelings, inclinations to act, and beliefs. It can be easily remembered as the
ABCs of attitudes: affect (feelings), behavior tendency (inclination to act), and cognition (beliefs),
(Myers, 2012). A prejudiced person may dislike those self-differences and behave in a
discriminatory manner, believing them as ignorant and dangerous.
On the other hand, discrimination refers to unjustifiable negative behavior towards a group or its
members, where behavior is adjudged to include both actions towards, and judgements/decisions
about group members. Correll et al. (2010, p. 46) provides a very useful definition of
discrimination as “behavior directed towards category members that is consequential for their
52
outcomes and that is directed towards them not because of any particular deservingness or
reciprocity, but simply because they happen to be members of that category” (Correll, Judd, Park,
& Wittenbrink, 2010).
Prejudice and discrimination against people infected, or presumed to be infected, with HIV has
occurred since the disease was first identified in the early 1980s (Kinniburgh, Scott, Gottlieb, &
Power, 2001). AIDS related stigma and its attendant prejudice and discrimination are significantly
related shaped by misunderstanding and fear of HIV and AIDS disease, coupled with social
attitudes towards the people who contract it and the conditions under which it is transmitted
(Herek, Thinking about AIDS and stigma: A psychologist's perspective, 2002). As well, many
authors have stressed that HIV and AIDS prejudice can largely be explained by the fears,
sometimes irrational, that surround the disease: fear of catching it, its incurable nature, and its
potentially lethal consequences (Beaulieu, Adrien, Potvin, & Dassa, 2014).
When we look at the interrelated determinants of HIV-related stigma, we see that HIV and AIDS
is associated with behaviors that are already stigmatized or considered “deviant,” (Öktem, 2015)
such as: homosexuality, injection drug use, and sex work. Second, PLWHA are thought to be
“responsible” for being infected with HIV (Lugova, Mon, Daher, & Suleiman, 2015). As well,
HIV and AIDS are considered as a life-threatening disease; therefore, people are afraid of
acquiring HIV. Finally, religious and/or moral beliefs lead people to conclude that having HIV is
the result of a moral fault, such as promiscuous or deviant sex, that deserves punishment (De
Bruyn, 1998).
There are also individual and socioeconomic factors affecting stigmatizing attitudes towards
people living with HIV and AIDS (Öktem, 2015). For example, lower levels of stigmatizing
attitudes are documented in younger individuals, in persons having personal contact with someone
living with HIV and having “more favorable attitudes” towards homosexuals (Herek, 1999). The
role of socioeconomic factors, mainly education, class, and rural–urban residency, at individual
and/or community levels has also been discussed in the literature as determinants of stigmatizing
attitudes. According to Aggleton et al., (2011) lower educational and income levels are found to
53
be related with higher levels of discrimination against PLWHA, while varying across settings,
cultures, and forms of stigma (Aggleton, Yankah, & Crewe, 2011).
Ignorance and fear about HIV and AIDS and bias against people infected by HIV continue to fuel
stigma and discrimination around the world. So, there is a substantial body of literature that shows
that PLWH do face a dilemma when it comes to disclosure (Pachankis, 2007). Sharing their HIV
status could provoke anxiety and cause perceived threats to their personal well-being because HIV
is still associated with stigma and prejudice (Rodkjaer, Sodemann, Ostergaard, & Lomborg, 2011).
As well, psychologically, HIV-related stigma can generate significant distress in the form of
depression, anxiety, and lowered self esteem (Stutterheim S. E., 2011; Vanable, Carey, Blair, &
Littlewood, 2006). Clearly, the negative consequences of stigmatization towards people living
with HIV and AIDS are substantial.
2.5.4 Risk perception of HIV among adolescents and emerging adults
HIV and AIDS risk behavior and prevalence still remain critical health concerns around the world.
In many regions of the world, new HIV infections are heavily concentrated among individuals
between 15-24 years of age (Kibombo, Nemma, & Ahmed, 2007). Influenced by many factors
such as poverty, gender inequality, lack of information and proper prevention services, adolescents
are mostly exposed to the risks of getting infected by HIV.
Risk perception has been theorized to be an important antecedent for adopting protective behavior.
It is a key construct of research applying the behavior change models (Macintyre, Rutenberg, &
Karim, 2004). In relation to HIV, risk perception is an indicator of perceived vulnerability to
infection, a measure of one’s understanding of HIV and AIDS transmission as well as willingness
to consider behavioral changes (Breakwell, 2014).
A review of various studies show that individuals are more likely to underestimate than to
overestimate their risk for HIV infection, regardless of the nature of their sexual behavior (Jeffers,
2012). So, in general, very low perception of HIV risk has been reported even in relatively high
prevalence rates. On the other hand, low perception has been reported to individuals who were
54
engaged in HIV risk behaviors or to those individuals who are knowledgeable about the HIV. For
instance, in a survey conducted in Zambia, it is reported that although 52% of the individuals
interviewed in a cross-sectional study knew someone with AIDS, most of the younger group of
adolescents did not think they were at risk of getting HIV (Magnani, et al., 2002). Furthermore,
another survey conducted among African Americans argued that individuals engaged in high risk
behaviors, including, low rates of condom use, substance abuse, and exchanging money for drugs,
typically did not perceive themselves at risk for contracting HIV. In addition, individuals who
reported more than five partners were more likely to perceive their HIV risk as zero or low, and
less likely using condoms (Nunn, et al., 2011).
According to a study conducted with students in the United States of America, Turkey and South
Africa, the perception of HIV risk was low among US and Turkish students, and high among South
African students (Adefuye, et al., 2011). High risk perception of HIV among South African
students can be explained with the fact that this country has the biggest and highest profile
of HIV epidemic in the world. In addition, in 2006, the survey conducted in Mozambique (15–24
age groups) found out that 32% of females considered themselves at no or low risk of contracting
HIV, 22% thought they were at moderate or high risk, and 46% did not know how to assess their
HIV risk. According to these findings, 27% of females who considered themselves at no or low
risk, and 23% who reported not knowing how to assess their risk, were at moderate or high risk of
HIV infection. On the other hand, 88% of males declared that they had no or low risk of acquiring
HIV, 46% that they had a moderate or high risk, and 17% that they did not know. However, 80%
of those who considered themselves at no or low risk, and 92% of those who did not know how to
assess their risk, were classified as having a moderate or high risk of HIV infection (Prata, Morris,
Mazive, Vahidnia, & Stehr, 2006).
Gender differentials on perceived HIV risk and sexual behavior have been studied, with some
studies indicating males to be at more risk while others show females were more at risk (Kibombo,
Nemma, & Ahmed, 2007). Research seems to show that being personally affected by HIV and
AIDS, especially having seen a close person die of AIDS, may be associated with higher perceived
risk of HIV infection (Kayiki & Forste, 2011). Therefore, this condition – knowing someone who
died of AIDS – is expected to influence condom use as a protective measure against HIV infection.
55
Besides, Kibombo, Neema, and Ahmed (2007) identified no strong association between knowing
someone with HIV and engaging in high risk behaviors among adolescents in Uganda. It is, still,
expected that the perception of HIV and AIDS risk will be associated with increased condom use,
even if it is not associated with other high risk behaviors (Kibombo, Nemma, & Ahmed, 2007).
By exploring both quantitative and qualitative research studies on HIV risk assessment and the
management of risk, it has been discovered that there are a variety of factors that influence risk
perception. Psychological factors, such as optimistic bias and psychological maintenance, social
factors such as gender, ethnicity, social networks, cultural norms, policies and religion have been
noted to shape perception of risk. Prevalence of HIV within a network may also play a major role
in decision making, a topic which has not been greatly explored as of yet (Jeffers, 2012).
The relationship between perception of risk and sexual behavior is complex and poorly understood
(Akwara, Madise, & Hinde, 2003). Studies conducted in different cultures have associated HIV
risk perception with a wide range of variables: number of sexual partners, knowledge of sexual
partners, past sexual behavior, fear of AIDS, shame associated with having AIDS, community
perception of AIDS risk, knowing someone with AIDS, discussing AIDS at home, closeness of
parent-child relationships and religious affiliation (Prata, Morris, Mazive, Vahidnia, & Stehr,
2006).
The global HIV and AIDS situation for youths is extremely serious. On the other hand, the need
for stronger focused response is also urgent. Young people are particularly vulnerable to HIV
infection because of risky sexual behaviors (Guindo, Liu, & Haba, 2014). Therefore,
understanding HIV-related risky sexual behaviors and perception of risk among young people is
critical to designing interventions to stem the tide of new infection among the population (Adefuye,
et al., 2011).

56
2.6 Background studies in Kosovo – a brief description
2.6.1 Research analysis of HIV knowledge, attitudes towards PLWHA and risk perception inKosovo among adolescents and emerging adults
There are only few researches in Kosovo on the problem of HIV and AIDS, as consequence data
about the sexual behavior of Kosovar adolescents and emerging adults is relatively poor today. In
addition to this, there is a lack of researches regarding the attitudes towards people living with HIV
and AIDS as well as regarding knowledge and risk perception among young people towards HIV.
Academics and scholars of this field started to pay attention on this issue only after the war in
Kosovo (1999). Knowledge, attitudes and risk perception of HIV have been studied in Kosovo in
graduate thesis and with small samples. However, this has supported the policy makers to properly
orient the strategy for prevention of HIV as well for reducing the stigma and discrimination
towards HIV infected people.
No matter how unreal the HIV and AIDS risk might currently seem in the Kosovo, where the
numbers of registered HIV and AIDS cases have so far been relatively low, the situation cannot
be underestimated. Unfortunately, as it is well known, even very low number in the beginning can
have significant influence in spreading the disease in a relatively short period of time.
According to research studies conducted after the war (1999), there is a high degree of stigma
towards people living with HIV and AIDS in Kosovo. The research “Knowledge, attitude and
habits of youngsters to sexual and reproductive health” (2001) showed that among Kosovars aged
14–19, knowledge of HIV and AIDS is insufficient and that HIV positive people are highly
stigmatized. The survey shows that in 43.7% of respondent families never talk about intimate
topics and issues of sexual and reproductive health. Such kind of topics are considered shameful
in these families and therefore are not discussed at all (National Public Health Institute, 2001).
On the other hand, according to the research “Knowledge of school youth on AIDS” (2001),
conducted by the Ministry of Health in Kosovo, it is argued that there are many prejudices among
students about people living with HIV and AIDS. Based on these findings, most of the students
prefer to distance themselves from their peers living with HIV and AIDS and think that these
57
people should be treated in special institutions and separated from the rest of society. According
to the research more than 90% of students know that HIV is not transmitted through the use of
shared toilets, only 10% of them would have used the same toilet as a person infected with HIV
(Ministry of Health, 2001).
People living with HIV and AIDS are usually blamed by their families, friends and community for
their condition, especially if they are infected with HIV through sexual intercourse or through the
drug injection. This observation is also confirmed by the research “Knowledge, attitudes, practices
and behavior of young people in Kosovo on HIV and AIDS” (2008), where HIV is described as
“a disease of shame” (National Public Health Institute, 2008). Furthermore, research on
“Behavioral and biological aspects of HIV and sexually transmitted diseases” in Kosovo has
shown that people living with HIV and AIDS and those affected by HIV, are stigmatized by
society. Due to the fear of rejection by their families, friends or community, according to this
research, the majority of HIV positive people do not disclose their condition even to their close
friends or family members (United Nation Kosovo Team, 2006).
Compared to the early post-war years in Kosovo, the level of information on HIV and AIDS among
young people has increased significantly. The research mentioned above, “Knowledge, attitudes,
practices and behavior of young people in Kosovo in relation to HIV and AIDS” (2008), has found
that young people are highly informed about HIV and AIDS where 90% of them have heard about
HIV and AIDS at least once. However, less than half of respondents (47%) are aware of the
difference between these two expressions: “HIV” and “AIDS”. What is more concerning in this
regard, are the attitudes of young people towards the disease itself and towards the infected people.
AIDS is still considered a taboo topic for many reasons but the main reason is because it is related
to sex. There also dominates a strong bias among the general public on the nature of this disease,
which is described as “a shameful disease” gained from unrestrained sex, drug addiction, by
homosexuals and by people who do not care enough about personal hygiene (National Public
Health Institute, 2008).
Another research, conducted in 2014, showed that one in four sexually active adolescents in
Kosovo declare that they do not use any kind of protection against pregnancy or sexually
58
transmitted infections during their sexual activities. These findings emphasize the need for a more
comprehensive sexual education in elementary and secondary schools. A representative sample of
4,531 adolescents in the sixth (age 11), eighth (age 13) and tenth (age 15) grade participated in the
survey regarding the various health behaviors, including those related to sexual and reproductive
health. Tenth-grade students were asked whether they were sexually active, with 13.3% saying
they were; the most common ages for first sexual intercourse were 14 and 15. Condoms were the
most popular contraceptive, used by 33.2% of sexually active respondents, though 26.5% declared
that they did not use any kind of protective measures. Additionally, more than half of sexually
active students declared they did not use a condom during their last sexual intercourse. This finding
demonstrates a low awareness level amongst adolescents about the risk of contracting HIV, STI
transmission and pregnancy (World Health Organization & United Nations Population, 2014).
This part summarized all the relevant researches conducted in Kosovo from 2000 till 2016
regarding the knowledge and risk perception of HIV and also the attitudes towards people with
HIV and AIDS. Based on the above mentioned findings, it can be concluded that despite the fact
that AIDS is considered as a taboo topic among families in Kosovo, the level of knowledge among
young people is satisfying. On the other hand, perception of risk to HIV and AIDS is very low,
which makes young people more vulnerable towards the disease. Furthermore, a substantial
proportion of the research findings (conducted before 2010) in Kosovo appear to be unsympathetic
to people who are infected with HIV, especially towards those who got infected through using
drugs and through unprotected sex. But, on the other hand, those findings also showed that most
common accepting attitude is the willingness to care for a family member who is infected with
AIDS in their own home and not using regular medical facilities.
2.7 Research questions and hypotheses
The study addresses several research questions and raises some other hypotheses. The combination
of research questions with hypotheses has been intentional and related to the methodological
approaches used: survey with adolescents and emerging adults and focus groups.
59
The research questions (RQ) which are examined in this study are listed in the following section.
Their aim is:
RQ1: To understand the level of knowledge among the adolescents and emerging adults
towards HIV and AIDS (quantitative research).
RQ2: To understand attitudes of adolescents and emerging adults towards people with HIV
and AIDS (quantitative research).
RQ3: To understand if adolescents and emerging adults perceive risk of infection from
HIV and AIDS (quantitative research).
RQ4: To analyze attitudes towards people living with HIV and AIDS, level of knowledge
and risk perception of HIV in correlation with socio-cultural aspects among adolescents and
emerging adults (qualitative research).
In addition to this, there are seven hypotheses that were raised in the current study.
H1: Emerging adults have more knowledge about HIV and as a result they have more
positive attitudes towards people with HIV compared with adolescents.
Considering previous studies (Maswanya, et al., 2000), it is hypothesized that there would be
differences among emerging adults vs. adolescents regarding level of knowledge of HIV as well
regarding attitudes towards people with HIV and AIDS.
H2: Female adolescents and emerging adults have more positive attitudes towards people
with HIV compared with male from both groups.
The second hypothesis is concerned with the gender differences related to the attitudes towards
people with HIV among adolescents and emerging adults. Taking into consideration previous
studies in the field (Nyawose, 2001; Štulhofer, Graham, Božičević, Kufrin, & Ajduković, 2007)
and referring to the previous research studies and different reports conducted in Kosovo (United
Nations Kosovo Team, 2008), it will be expected that there will be differences regarding gender
as a variable and its correlation to attitudes towards people with HIV and AIDS.
H3: Male and emerging adults perceive to be more at risk to getting infected with HIV
compared with female and adolescents.
60
Considering previous studies (Nunn, et al., 2011; United Nations Kosovo Team, 2008; Darteh,
Kyereme, & Asare, 2016), it is hypothesized that there would be differences among males and
females and adolescents and emerging adults, regarding risk perceptions towards HIV.
H4: Adolescents and emerging adults with higher monthly income of their parents have
more and much accurate knowledge about HIV compared to those with a lower monthly income
of their parents.
Considering previous studies (Othman, 2015; Huda & Amanullah, 2013), it is hypothesized that
there would be differences among adolescents and emerging adults with higher and lower income
of their parents regarding HIV knowledge.
H5: Adolescents and emerging adults with permanent residence in urban areas have more
knowledge about HIV than those with permanent residence in rural areas.
Considering previous studies and as well as previous research reports conducted in Kosovo (Lal,
Vasan, Sarma, & Thankappan, 2000; Agyemang, Buor, & Tagoe-Darko, 2012; United Nations
Kosovo Team, 2008), it is hypothesized that there would be gender differences among the subjects
with permanent residence in urban vs. rural areas regarding HIV knowledge.
H6: Adolescents and emerging adults with parents who have a higher level of education,
have more positive attitudes towards people with HIV than adolescents and emerging adults with
parents who have a lower level of education.
Considering previous studies (Huda & Amanullah, 2013), it is hypothesized that there would be
differences among the adolescents and emerging adults regarding parents who have a higher level
of education compared with both targeted group with parents who have a lower level of education.
H7: Adolescents and emerging adults with a higher level of education have more
knowledge about HIV as well as more positive attitudes towards people with HIV, compared with
adolescents and emerging adults with a lower level of education.
Considering previous studies (Agyemang, Buor, & Tagoe-Darko, 2012), it is hypothesized that
there would be differences among adolescents and emerging adults with a higher level of education

61
compared with both targeted groups with a lower education regarding the level of knowledge about
HIV and their attitudes towards PLWHA.

62
~Chapter Three~Study 1
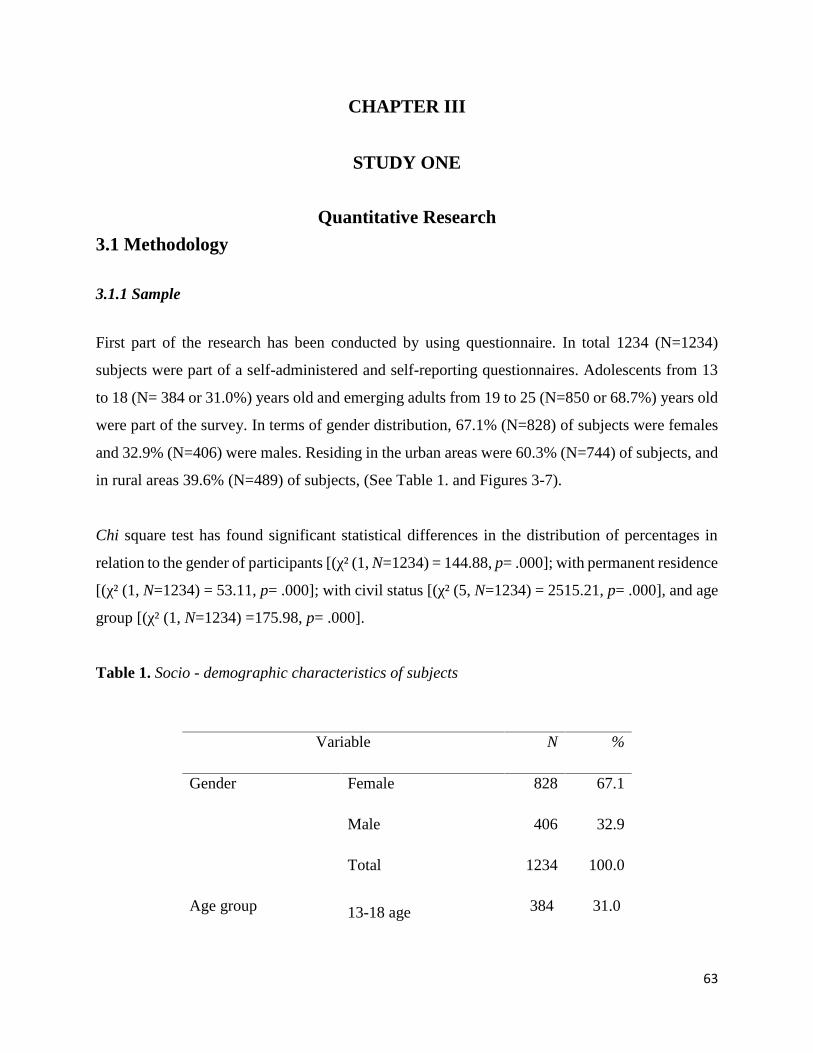
63
CHAPTER III
STUDY ONE
Quantitative Research
3.1 Methodology
3.1.1 Sample
First part of the research has been conducted by using questionnaire. In total 1234 (N=1234)
subjects were part of a self-administered and self-reporting questionnaires. Adolescents from 13
to 18 (N= 384 or 31.0%) years old and emerging adults from 19 to 25 (N=850 or 68.7%) years old
were part of the survey. In terms of gender distribution, 67.1% (N=828) of subjects were females
and 32.9% (N=406) were males. Residing in the urban areas were 60.3% (N=744) of subjects, and
in rural areas 39.6% (N=489) of subjects, (See Table 1. and Figures 3-7).
Chi square test has found significant statistical differences in the distribution of percentages in
relation to the gender of participants [(χ² (1, N=1234) = 144.88, p= .000]; with permanent residence
[(χ² (1, N=1234) = 53.11, p= .000]; with civil status [(χ² (5, N=1234) = 2515.21, p= .000], and age
group [(χ² (1, N=1234) =175.98, p= .000].
Table 1. Socio - demographic characteristics of subjects
Variable N %
Gender Female 828 67.1
Male 406 32.9
Total 1234 100.0
Age group 13-18 age 384 31.0
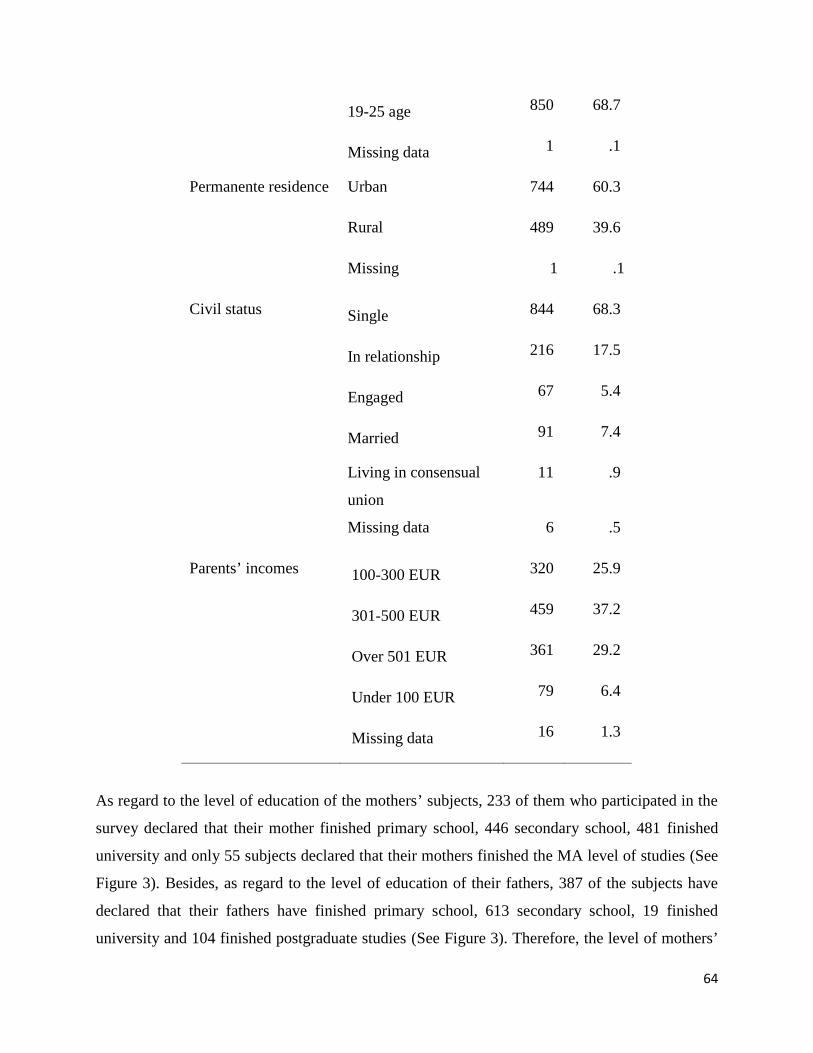
64
19-25 age 850 68.7
Missing data 1 .1
Permanente residence Urban 744 60.3
Rural 489 39.6
Missing 1 .1
Civil status Single 844 68.3
In relationship 216 17.5
Engaged 67 5.4
Married 91 7.4
Living in consensual
union
11 .9
Missing data 6 .5
Parents’ incomes 100-300 EUR 320 25.9
301-500 EUR 459 37.2
Over 501 EUR 361 29.2
Under 100 EUR 79 6.4
Missing data 16 1.3
As regard to the level of education of the mothers’ subjects, 233 of them who participated in the
survey declared that their mother finished primary school, 446 secondary school, 481 finished
university and only 55 subjects declared that their mothers finished the MA level of studies (See
Figure 3). Besides, as regard to the level of education of their fathers, 387 of the subjects have
declared that their fathers have finished primary school, 613 secondary school, 19 finished
university and 104 finished postgraduate studies (See Figure 3). Therefore, the level of mothers’
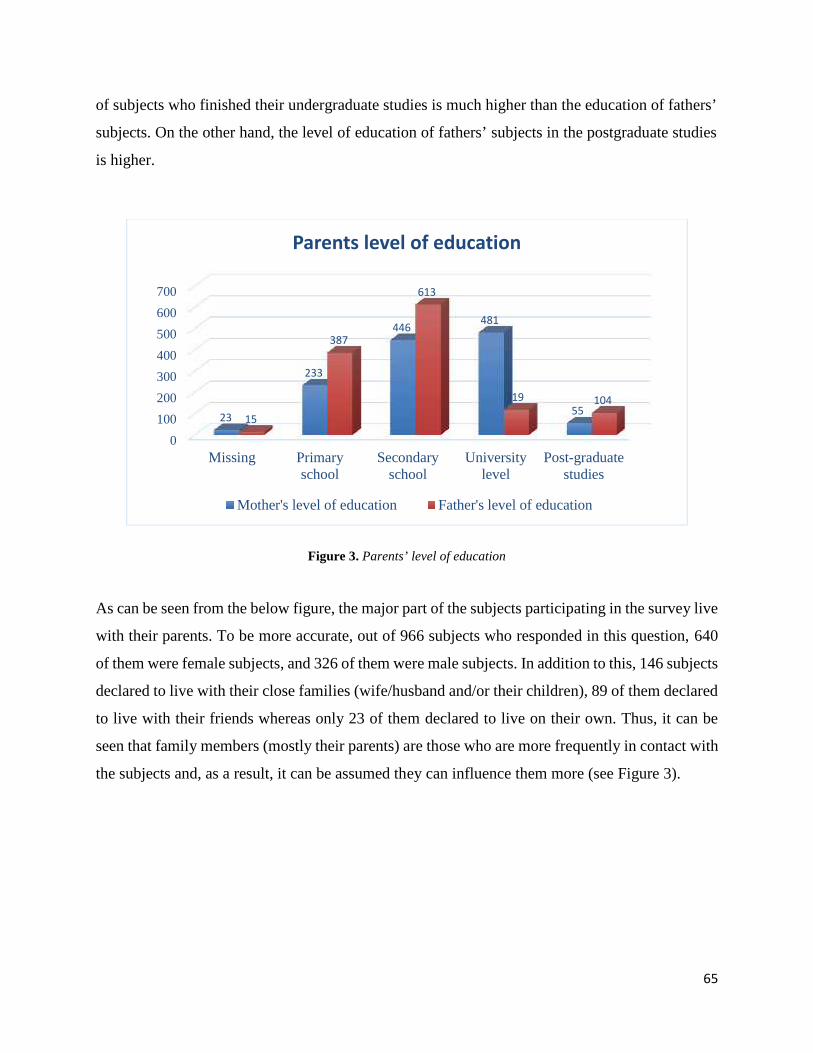
65
of subjects who finished their undergraduate studies is much higher than the education of fathers’
subjects. On the other hand, the level of education of fathers’ subjects in the postgraduate studies
is higher.
Figure 3. Parents’ level of education
As can be seen from the below figure, the major part of the subjects participating in the survey live
with their parents. To be more accurate, out of 966 subjects who responded in this question, 640
of them were female subjects, and 326 of them were male subjects. In addition to this, 146 subjects
declared to live with their close families (wife/husband and/or their children), 89 of them declared
to live with their friends whereas only 23 of them declared to live on their own. Thus, it can be
seen that family members (mostly their parents) are those who are more frequently in contact with
the subjects and, as a result, it can be assumed they can influence them more (see Figure 3).
0
100
200
300
400
500
600
700
Missing Primaryschool
Secondaryschool
Universitylevel
Post-graduatestudies
23
233
446 481
5515
387
613
119 104
Parents level of education
Mother's level of education Father's level of education
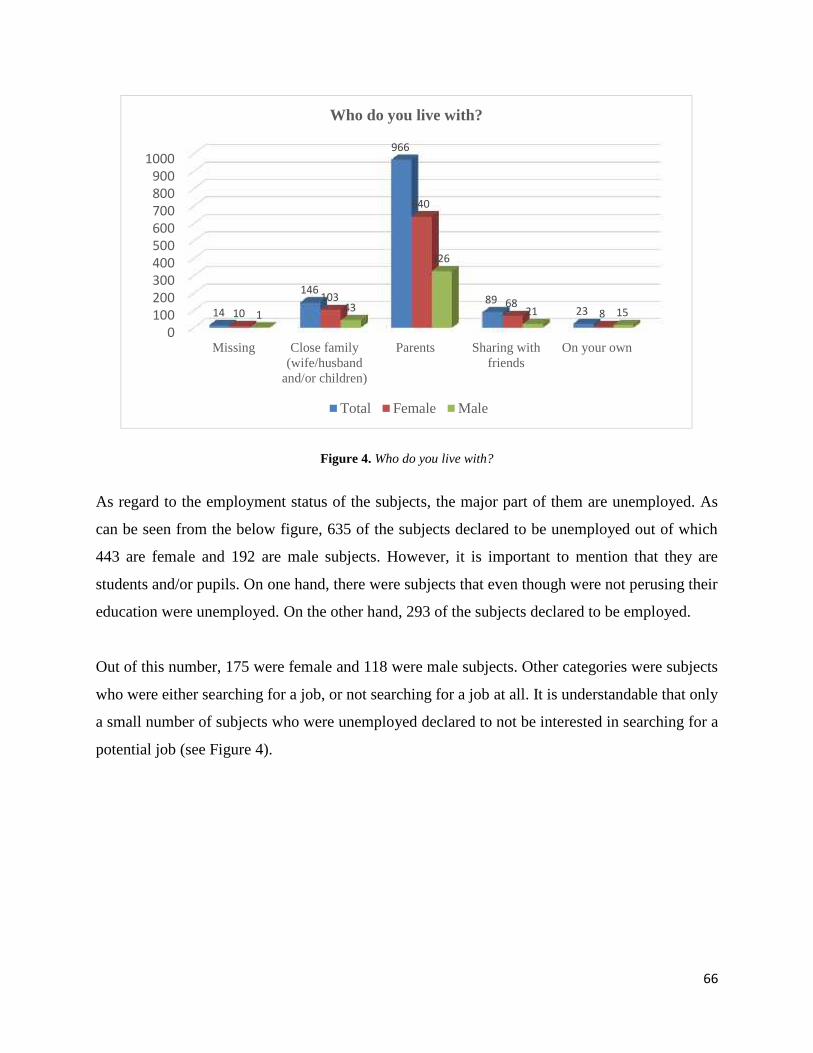
66
Figure 4. Who do you live with?
As regard to the employment status of the subjects, the major part of them are unemployed. As
can be seen from the below figure, 635 of the subjects declared to be unemployed out of which
443 are female and 192 are male subjects. However, it is important to mention that they are
students and/or pupils. On one hand, there were subjects that even though were not perusing their
education were unemployed. On the other hand, 293 of the subjects declared to be employed.
Out of this number, 175 were female and 118 were male subjects. Other categories were subjects
who were either searching for a job, or not searching for a job at all. It is understandable that only
a small number of subjects who were unemployed declared to not be interested in searching for a
potential job (see Figure 4).
0100200300400500600700800900
1000
Missing Close family(wife/husband
and/or children)
Parents Sharing withfriends
On your own
14
146
966
892310
103
640
6881 43
326
21 15
Who do you live with?
Total Female Male
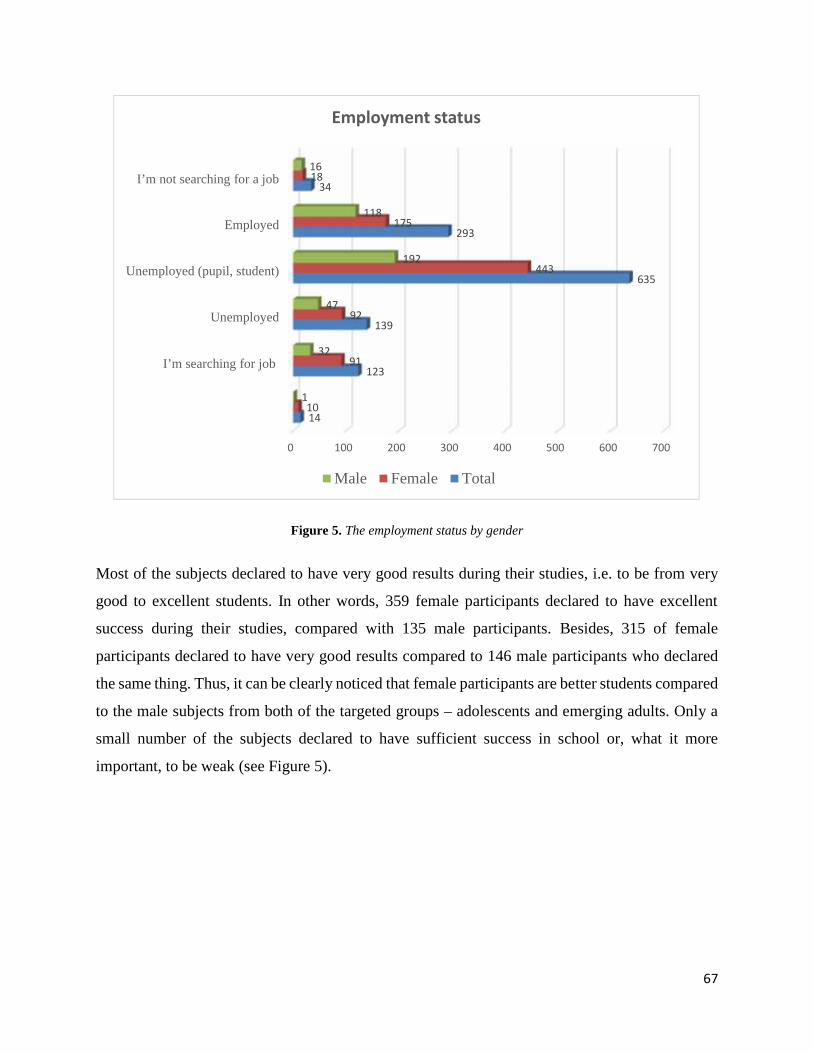
67
Figure 5. The employment status by gender
Most of the subjects declared to have very good results during their studies, i.e. to be from very
good to excellent students. In other words, 359 female participants declared to have excellent
success during their studies, compared with 135 male participants. Besides, 315 of female
participants declared to have very good results compared to 146 male participants who declared
the same thing. Thus, it can be clearly noticed that female participants are better students compared
to the male subjects from both of the targeted groups – adolescents and emerging adults. Only a
small number of the subjects declared to have sufficient success in school or, what it more
important, to be weak (see Figure 5).
0 100 200 300 400 500 600 700
I’m searching for job
Unemployed
Unemployed (pupil, student)
Employed
I’m not searching for a job
14
123
139
635
293
34
10
91
92
443
175
18
1
32
47
192
118
16
Employment status
Male Female Total
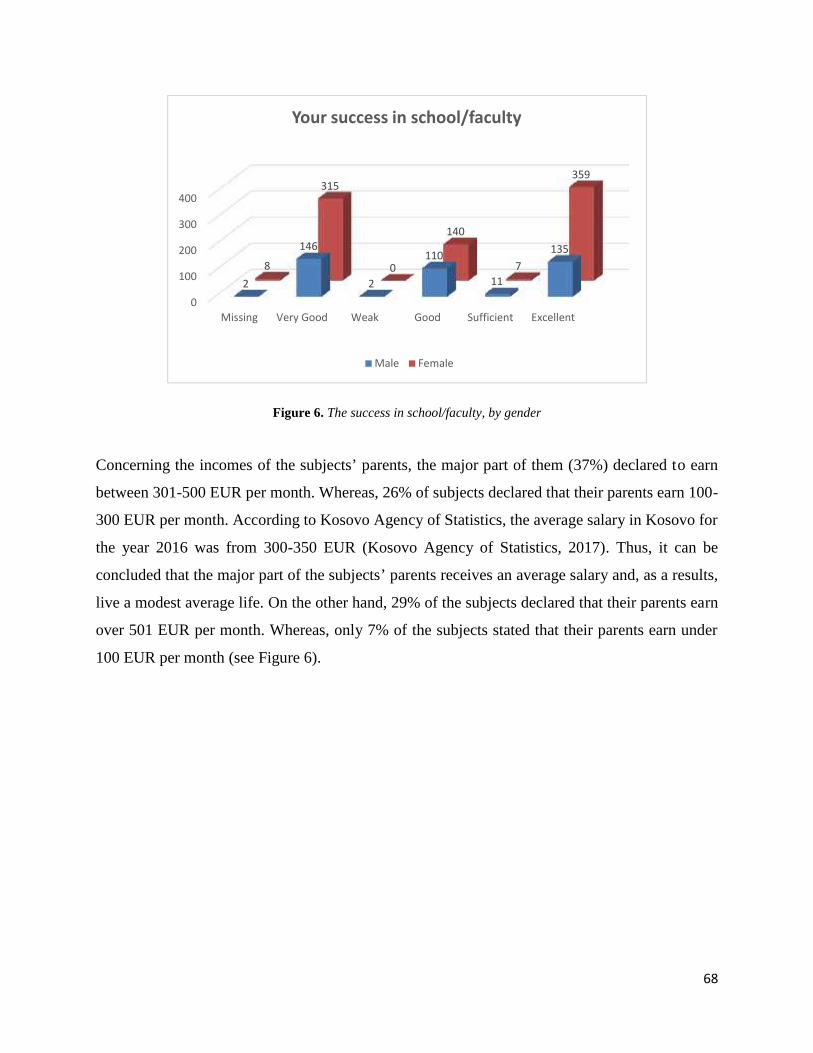
68
Figure 6. The success in school/faculty, by gender
Concerning the incomes of the subjects’ parents, the major part of them (37%) declared to earn
between 301-500 EUR per month. Whereas, 26% of subjects declared that their parents earn 100-
300 EUR per month. According to Kosovo Agency of Statistics, the average salary in Kosovo for
the year 2016 was from 300-350 EUR (Kosovo Agency of Statistics, 2017). Thus, it can be
concluded that the major part of the subjects’ parents receives an average salary and, as a results,
live a modest average life. On the other hand, 29% of the subjects declared that their parents earn
over 501 EUR per month. Whereas, only 7% of the subjects stated that their parents earn under
100 EUR per month (see Figure 6).
0
100
200
300
400
Missing Very Good Weak Good Sufficient Excellent
2
146
2
110
11
1358
315
0
140
7
359
Your success in school/faculty
Male Female
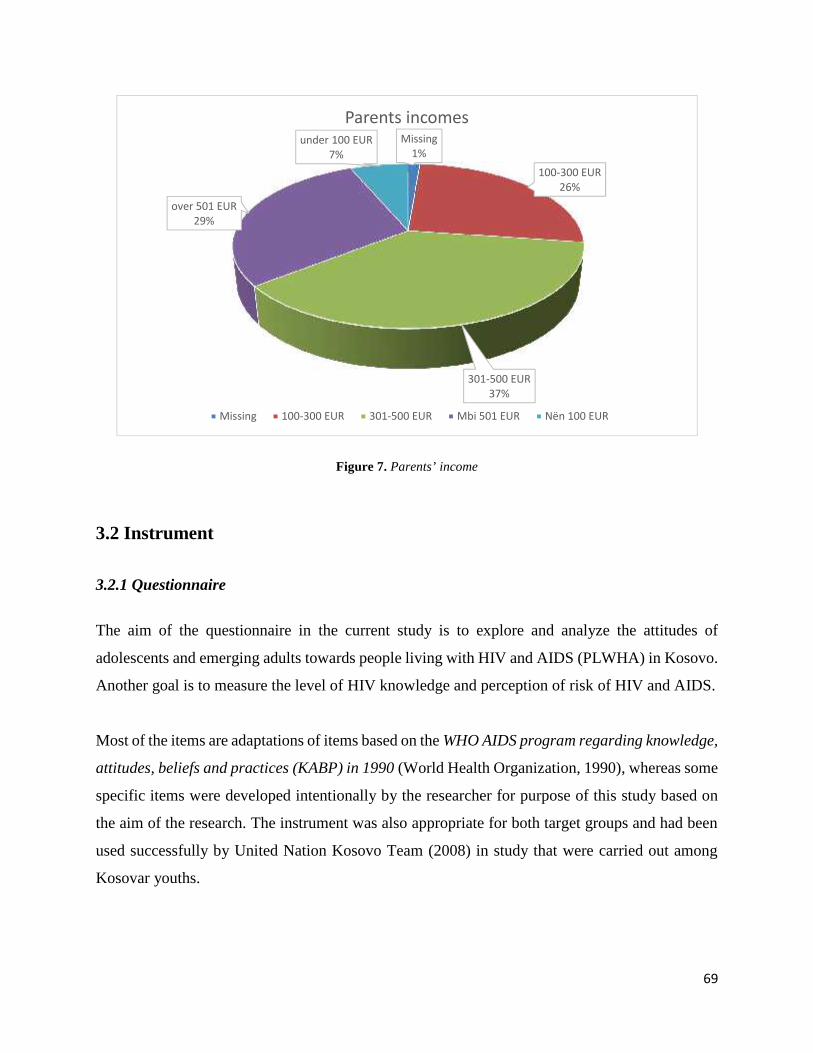
69
Figure 7. Parents’ income
3.2 Instrument
3.2.1 Questionnaire
The aim of the questionnaire in the current study is to explore and analyze the attitudes of
adolescents and emerging adults towards people living with HIV and AIDS (PLWHA) in Kosovo.
Another goal is to measure the level of HIV knowledge and perception of risk of HIV and AIDS.
Most of the items are adaptations of items based on the WHO AIDS program regarding knowledge,
attitudes, beliefs and practices (KABP) in 1990 (World Health Organization, 1990), whereas some
specific items were developed intentionally by the researcher for purpose of this study based on
the aim of the research. The instrument was also appropriate for both target groups and had been
used successfully by United Nation Kosovo Team (2008) in study that were carried out among
Kosovar youths.
Missing1%
100-300 EUR26%
301-500 EUR37%
over 501 EUR29%
under 100 EUR7%
Parents incomes
Missing 100-300 EUR 301-500 EUR Mbi 501 EUR Nën 100 EUR
70
For the purpose of designing the questionnaire, there were also measuring instruments examined
which aimed at identifying factors which were similar in different countries of the world. The final
questionnaire included questions related to: HIV knowledge, attitudes towards PLWHA and risk
perception of HIV and AIDS, in addition to socio-demographic information. The questionnaire
was divided into four parts.
Part I was focused on the socio-demographic characteristics of the subjects. Data on demographic
variables included the following questions: (1) age, (2) gender, (3) permanent residence (urban or
rural), (4) municipality, (5) religion, (6) civil status, (7) level of study, (8) success in school/faculty,
(9) employment status, (10) living status, (11) education level of the mothers, (12) education level
of fathers, (13) parents’ income. These socio-demographic characteristics were chosen based on
existing literature suggesting their importance in studying HIV knowledge and risk perception of
HIV and attitudes towards people living with HIV and AIDS.
Part II of the questionnaire contained nine HIV knowledge-related items, with questions about
knowledge of HIV infection, transmission patterns and opinions about the adequacy of their own
knowledge regarding HIV, meaning of HIV and AIDS and their differences etc. The items were
adapted from WHO AIDS program regarding knowledge, attitudes, beliefs and practices (KABP)
and only one specific item was developed intentionally by the researcher for purpose of this part
of questionnaire. In addition, there were both included positively and negatively framed questions
to assess their knowledge, as well as their misconceptions about HIV and AIDS. The following
were the addressed statements of misconceptions: HIV can be spread by every day contacts;
through swimming pools etc.
Part III of the questionnaire is comprised by ten questions which are focused on attitudes towards
PLWHA. It is important to mention that in this part of the questionnaire are included both,
positively and negatively framed questions. The items were adapted from WHO AIDS program
regarding knowledge, attitudes, beliefs and practices (KABP). Questions in this session aimed to
identify attitudes and viewpoints of adolescents and emerging adults regarding people who live
with HIV and AIDS. The attitudes section inquires the feelings of subjects towards being

71
comfortable talking, working, sharing a class with PLWHA; feeling empathy towards people with
HIV etc.
Finally, part IV is comprised by four questions about the risk perception of HIV. Questions in this
session aimed to identify risk perceptions towards HIV and why subjects consider themselves of
being at the low risk or eventually at high risk of getting infected with HIV. The items were also
adapted from WHO AIDS program regarding knowledge, attitudes, beliefs and practices (KABP).
The responses categories for most of the scales are: (1) strongly agree; (2) agree; (3) I have no
opinion; (4) disagree and (5) strongly disagree, and some others had 3 to 8 responses (depending
on questions).
As mentioned above, one of the methodological approaches which has been used to gather data
from the targeted population is the survey through a questionnaire. This approach – questionnaire
– is considered by many scholars as one of the most usual way of gathering data from respondents
participating in the research. It is worth mentioning that this was not always a very popular
approach among the researchers. However, the use of questionnaires as one of the tools for
gathering social data increased significantly during the twentieth century. A very important factor
which influenced this process was the incensement of using statistical techniques. This created an
opportunity to the scholars to work easily with a very large number of cases and with bigger
amount of data which, at the same time, were much more complex (Matthews & Ross, 2010).
Nevertheless, the idea of the early surveys was focused mostly and exclusively in collecting data
about people and their experiences, without entering deeper in their understanding about a
particular issue. In this regard, scholars who were concerned in working in social research were
intrigued to explore in more detail the opinions and values of people. For this reason, they started
to develop particular techniques on how to measure these opinions and values in order to make
them more quantifiable and, at the same time, more useful in science. One of the most prominent
scholars who contributed significantly in this regard is the well-known American psychologist
Rensis Likert (Maurer & Pierce, 1998). First and foremost, he was interested in the human
organization and, for this reason; he developed the so called “Likert scale”. The core idea and
function of the Likert scale is to make it possible for the respondents to evaluate ideas or one

72
particular attitude statement along a five point scale from “strongly agree” to “strongly disagree”
(Matthews & Ross, 2010, pp. 200-201).
It is important to mention that in the contemporary social science, in general, and of psychology,
in particular, questionnaires are used in many cases when a researcher aims to find out about all
sorts of social issues, problems and phenomena. Questionnaires are good and practical tools to
gather and analyze not only, the so called, factual data where included are demographic data such
as: people’s age, gender, location, level of income, religion etc., but, they are quite effective in
gathering people’s opinions, ideas, attitudes, knowledge, experiences and judgments too. These
categories in science are known as latent constructs. In this case, a researcher needs to ask the
respondents if they agree, have no opinion or, in contrary, disagree with the statement you have
formulated (Howitt & Cramer, 2007). Having in mind that one of main aims of the study, the
author considered that the best tool to gather data is to use questionnaires designed carefully by
applying the Likert scale. This has been done for many reasons. First of all, because the Likert
scale offers the respondents the opportunity to show how strongly they feel about the factors that
have been raised in the statement and can helpfully distinguish people between (Matthews & Ross,
2010). When these data are correlated with the demographic data of the respondents, then this
creates a solid ground for the researcher to conduct a solid analysis. Another advantage of using
Likert scale, according to Matthes & Ross (2010), is because this approach does not limit
respondents to give a yes/no answer. Moreover, it allows a degree of opinions and alternatives by
offering them the opportunity to have no opinion at all if they see reasonable.
It is understandable that any methodological approach has its advantages and its disadvantages.
This, naturally, depends in many actors and factors. Some of them can be influenced by the
research, but some are and cannot.
Some of the disadvantages that researches face in their research activities by using questionnaires
as the main method of gathering data include, but are not limited to, the following:
According to phenomenologists the usage of quantitative research as a method of
gathering data is simply an artificial creation by the researcher. This occurs due to the fact
73
that through the questionnaire the researcher can gather only a limited amount of
information without explanation (Matthews & Ross, Research methods, 2014).
Another significant disadvantage that researchers face by using questionnaires is that there
is no way to tell how truthful a respondent/subject is being, or how much thought a
respondent has put in prior to answer the question.
Some scholars argued that another disadvantage of using questionnaires can happen
because people may read differently question and therefore reply based on their own
understanding and interpretation of the question.
I addition, it is assumed that in any questionnaire there is a level of researcher imposition.
This means that when developing the questionnaire, the researcher is making their own
decisions and assumptions as to what is and is not important to include or to leave out of
the questionnaire (Popper, 2004; Ackroyd, 1992).
3.3 Procedure
In the first phase, the survey instrument was designed in the English language. Further, in the
second phase, questionnaire was translated into the Albanian language. This has been done due to
better understanding of questions by the subjects because Albanian is the official language of the
subjects who participated in the study. The questionnaire provided in the Albanian language was
translated back to the English language. The translation has been done by two different
professionals, including one psychologist and one professional translator of the English-Albanian
language. In order for the translation to be more valid, understandable and comprehensive, after
the first version of the document, a meeting was conducted with the two professionals. During the
meeting they discussed the questions one by one and came up with the more adequate Albanian
version of questionnaire.
After the finalization of the translation a questionnaire was piloted with 100 subjects (N=100).
This was done with the aim of testing the validity and reliability of the questionnaires. In order to
ensure that the items of the questionnaire were culturally acceptable and easily understood for the
74
subjects participating in the study the pilot study was conducted. Also, participating subjects in the
pilot study were asked to report if they have found any difficulty with the items of the questionnaire
and if they found any items that is not understandable or incomprehensible. Based on the subjects’
comments, final changes were made to the translated version of the questionnaire and the last
version of the questionnaire for the purpose of the study was defined.
Internal consistency of the scale Alpha coefficients for reliability and internal consistency of the
items were found to be 0.74 for HIV knowledge and 0.74 for attitudes towards PLWHA (See
Annex 2). On the other hand, we could not find the internal consistency of the alpha coefficients
for reliability and internal consistency, for risk perception items due to the small number of items
and answers (multiple answers) in each item. Regarding internal consistency coefficient, research
evidence suggests that good internal consistency is indicated when is more than 0.70 (Nunnally &
Bernstein, 1994). While, it should be noted that some of the used scales have only a few items and
are affected by the number of items (Cortina, 1993).
To analyze all the collected data in this research, the SPSS statistical package for Windows
software version 21 was used. For processing the statistical data descriptive and conclusive
statistical analyses were used. The totality of the collected data were analyzed through descriptive
analysis through which were found basic statistical parameters and distributions of the obtained
data. The present variables are presented through the percentage values (%), number of individuals
for respective percentage, arithmetic mean (AM), standard deviation (SD), in the confidence
interval of 95% (95% CI). During the analysis a specific code is used to identify necessary
information for every participant in the research.
The presented analyses are:
The internal consistency of questionnaire scale is analyzed by using Cronbach alpha (α);
Presentation in percentages of the gained values of variables for each part of the
questionnaire;
To identify the difference between the received responses, the chi-square goodness-of-fit
test was used. Chi-square (goodness-of-fit) which is a non-parametric test for the single
variable. Also, in this analysis the expectation follows the pattern of null hypothesis (zero),
thus, there are not expected differences in responses to the respective variable;
75
To identify potential correlations between demographic variables and received responses,
the Pearson’s chi-square of association was used;
Differences between groups were identified through Mann-Whitney U and Kruskal-Wallis
H etc.
3.4 Ethical issues
Special attention has been given to the ethical issues. Participation of the subjects was on voluntary
bases and subjects were informed on their rights to interrupt and withdraw from the questionnaire
at any time during the study process.
3.5 Results from quantitative research
3.5.1 Level of knowledge to HIV and AIDS, attitudes towards PLWHA and risk perception to
HIV (addressing H1-H7)
Results of this study have shown a satisfactory level of knowledge about HIV and AIDS among
adolescents and emerging adults. The analysis of data below, indicated that in most items subjects
had a satisfactory knowledge about HIV and AIDS. The percentages of “true” responses for all the
HIV knowledge items were slightly higher than “false” and “I have no opinion” responses for most
of the items. The exception was the response for items second (2) and sixth (6), where the subjects
showed very correct knowledge of HIV and AIDS (70.4%, 64.2%), (See Table 2). For instance,
53.9% of all subject declared that they cannot notice a person infected with HIV and they look
completely normal.
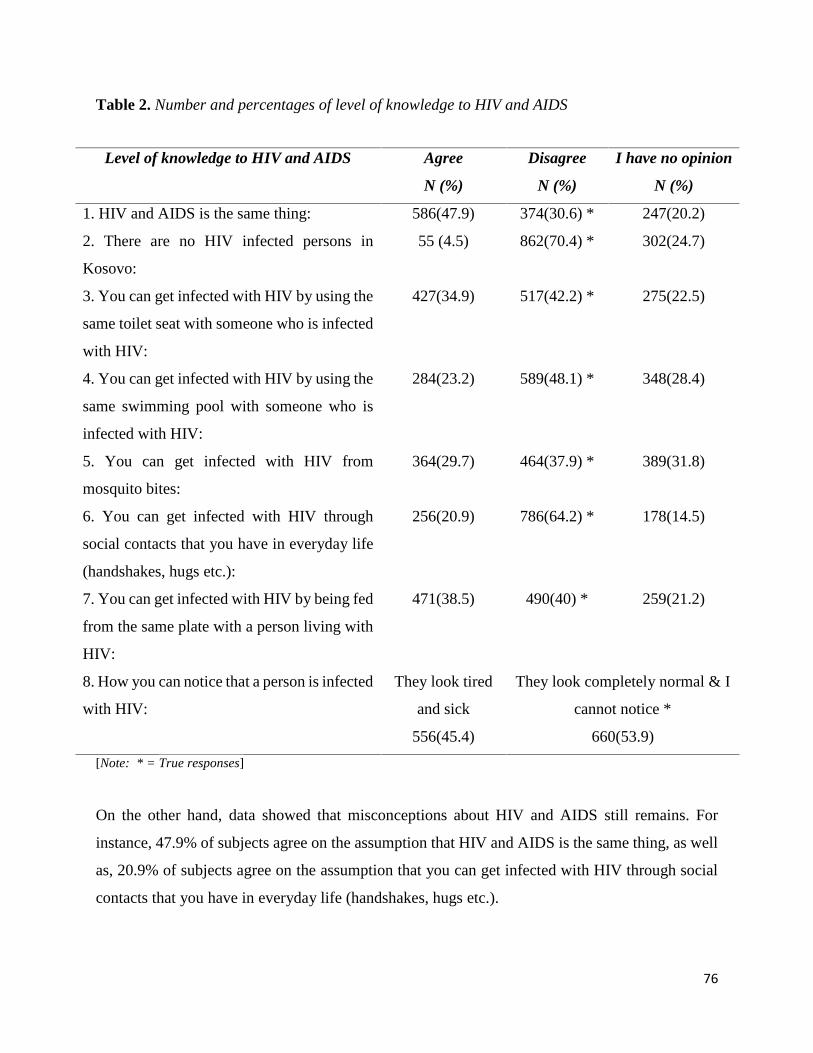
76
Table 2. Number and percentages of level of knowledge to HIV and AIDS
Level of knowledge to HIV and AIDS Agree
N (%)
Disagree
N (%)
I have no opinion
N (%)
1. HIV and AIDS is the same thing: 586(47.9) 374(30.6) * 247(20.2)
2. There are no HIV infected persons in
Kosovo:
55 (4.5) 862(70.4) * 302(24.7)
3. You can get infected with HIV by using the
same toilet seat with someone who is infected
with HIV:
427(34.9) 517(42.2) * 275(22.5)
4. You can get infected with HIV by using the
same swimming pool with someone who is
infected with HIV:
284(23.2) 589(48.1) * 348(28.4)
5. You can get infected with HIV from
mosquito bites:
364(29.7) 464(37.9) * 389(31.8)
6. You can get infected with HIV through
social contacts that you have in everyday life
(handshakes, hugs etc.):
256(20.9) 786(64.2) * 178(14.5)
7. You can get infected with HIV by being fed
from the same plate with a person living with
HIV:
471(38.5) 490(40) * 259(21.2)
8. How you can notice that a person is infected
with HIV:
They look tired
and sick
They look completely normal & I
cannot notice *
556(45.4) 660(53.9)
[Note: * = True responses]
On the other hand, data showed that misconceptions about HIV and AIDS still remains. For
instance, 47.9% of subjects agree on the assumption that HIV and AIDS is the same thing, as well
as, 20.9% of subjects agree on the assumption that you can get infected with HIV through social
contacts that you have in everyday life (handshakes, hugs etc.).
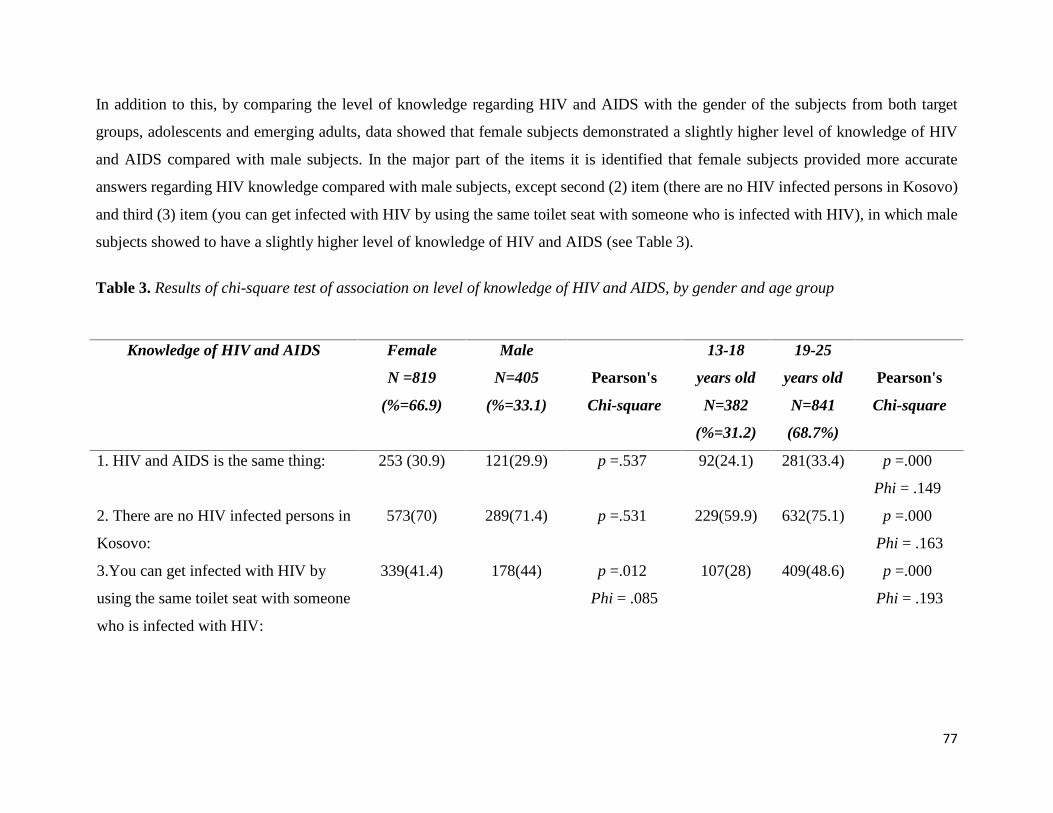
77
In addition to this, by comparing the level of knowledge regarding HIV and AIDS with the gender of the subjects from both target
groups, adolescents and emerging adults, data showed that female subjects demonstrated a slightly higher level of knowledge of HIV
and AIDS compared with male subjects. In the major part of the items it is identified that female subjects provided more accurate
answers regarding HIV knowledge compared with male subjects, except second (2) item (there are no HIV infected persons in Kosovo)
and third (3) item (you can get infected with HIV by using the same toilet seat with someone who is infected with HIV), in which male
subjects showed to have a slightly higher level of knowledge of HIV and AIDS (see Table 3).
Table 3. Results of chi-square test of association on level of knowledge of HIV and AIDS, by gender and age group
Knowledge of HIV and AIDS Female
N =819
(%=66.9)
Male
N=405
(%=33.1)
Pearson's
Chi-square
13-18
years old
N=382
(%=31.2)
19-25
years old
N=841
(68.7%)
Pearson's
Chi-square
1. HIV and AIDS is the same thing: 253 (30.9) 121(29.9) p =.537 92(24.1) 281(33.4) p =.000
Phi = .149
2. There are no HIV infected persons in
Kosovo:
573(70) 289(71.4) p =.531 229(59.9) 632(75.1) p =.000
Phi = .163
3.You can get infected with HIV by
using the same toilet seat with someone
who is infected with HIV:
339(41.4) 178(44) p =.012
Phi = .085
107(28) 409(48.6) p =.000
Phi = .193
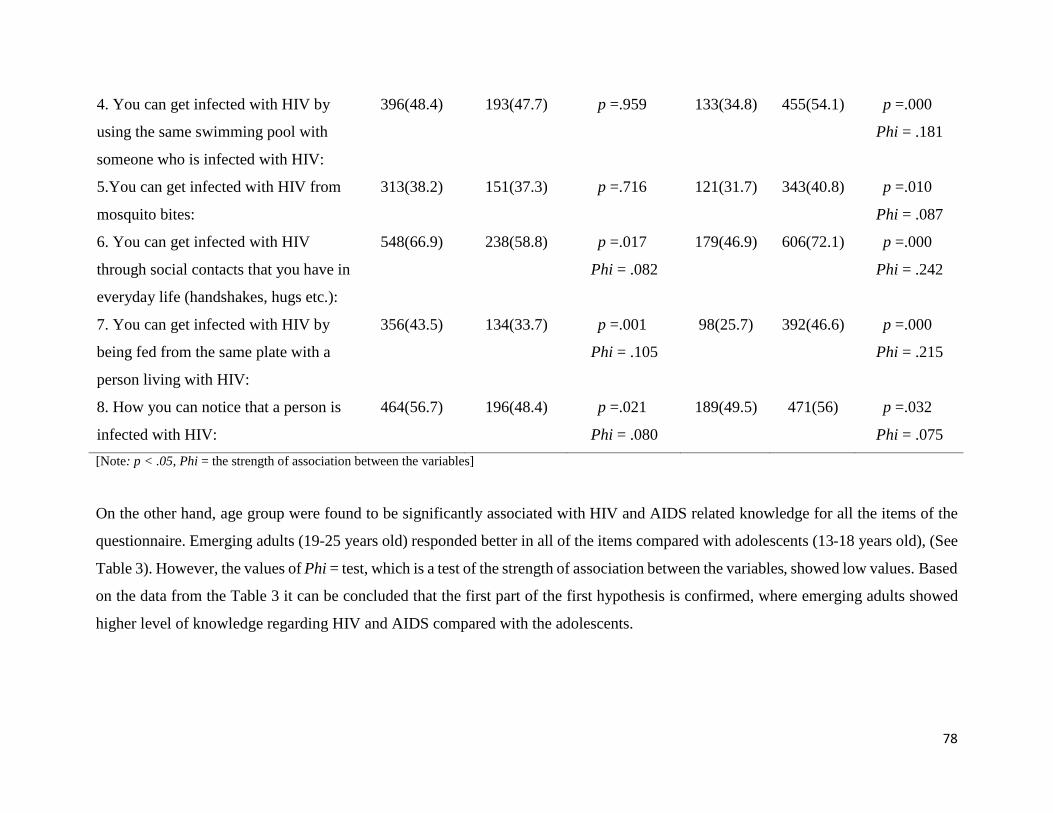
78
4. You can get infected with HIV by
using the same swimming pool with
someone who is infected with HIV:
396(48.4) 193(47.7) p =.959 133(34.8) 455(54.1) p =.000
Phi = .181
5.You can get infected with HIV from
mosquito bites:
313(38.2) 151(37.3) p =.716 121(31.7) 343(40.8) p =.010
Phi = .087
6. You can get infected with HIV
through social contacts that you have in
everyday life (handshakes, hugs etc.):
548(66.9) 238(58.8) p =.017
Phi = .082
179(46.9) 606(72.1) p =.000
Phi = .242
7. You can get infected with HIV by
being fed from the same plate with a
person living with HIV:
356(43.5) 134(33.7) p =.001
Phi = .105
98(25.7) 392(46.6) p =.000
Phi = .215
8. How you can notice that a person is
infected with HIV:
464(56.7) 196(48.4) p =.021
Phi = .080
189(49.5) 471(56) p =.032
Phi = .075
[Note: p < .05, Phi = the strength of association between the variables]
On the other hand, age group were found to be significantly associated with HIV and AIDS related knowledge for all the items of the
questionnaire. Emerging adults (19-25 years old) responded better in all of the items compared with adolescents (13-18 years old), (See
Table 3). However, the values of Phi = test, which is a test of the strength of association between the variables, showed low values. Based
on the data from the Table 3 it can be concluded that the first part of the first hypothesis is confirmed, where emerging adults showed
higher level of knowledge regarding HIV and AIDS compared with the adolescents.
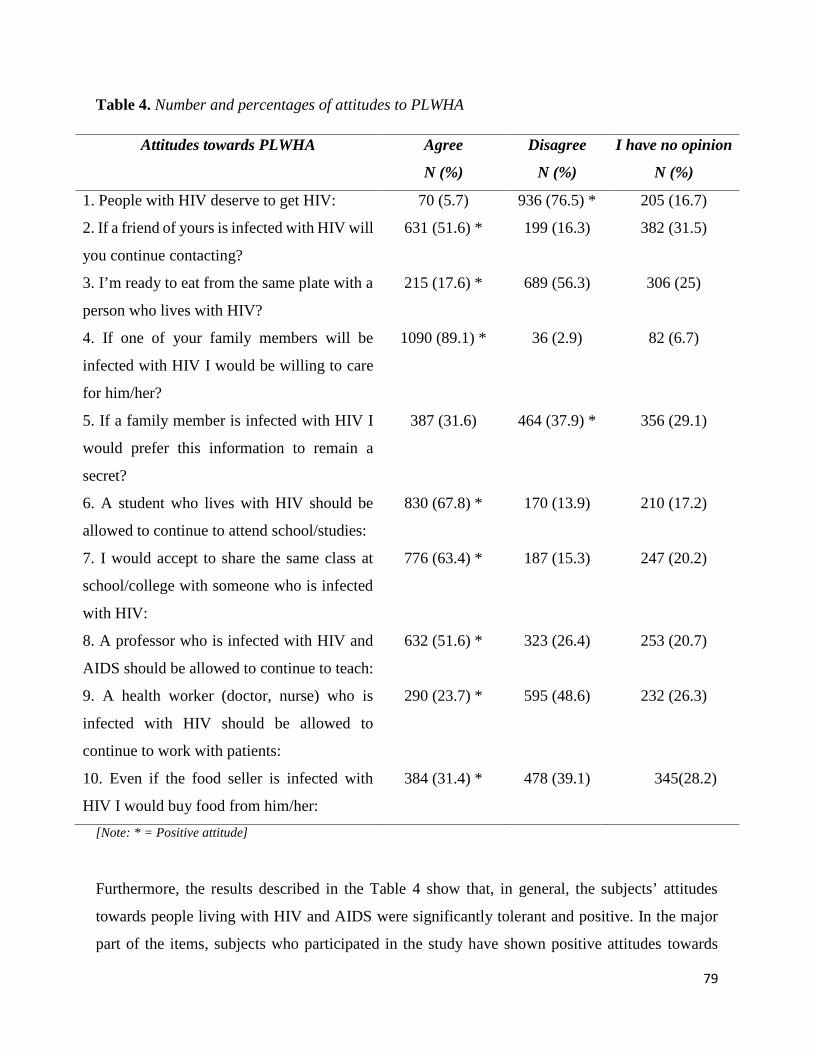
79
Table 4. Number and percentages of attitudes to PLWHA
Attitudes towards PLWHA Agree
N (%)
Disagree
N (%)
I have no opinion
N (%)
1. People with HIV deserve to get HIV: 70 (5.7) 936 (76.5) * 205 (16.7)
2. If a friend of yours is infected with HIV will
you continue contacting?
631 (51.6) * 199 (16.3) 382 (31.5)
3. I’m ready to eat from the same plate with a
person who lives with HIV?
215 (17.6) * 689 (56.3) 306 (25)
4. If one of your family members will be
infected with HIV I would be willing to care
for him/her?
1090 (89.1) * 36 (2.9) 82 (6.7)
5. If a family member is infected with HIV I
would prefer this information to remain a
secret?
387 (31.6) 464 (37.9) * 356 (29.1)
6. A student who lives with HIV should be
allowed to continue to attend school/studies:
830 (67.8) * 170 (13.9) 210 (17.2)
7. I would accept to share the same class at
school/college with someone who is infected
with HIV:
776 (63.4) * 187 (15.3) 247 (20.2)
8. A professor who is infected with HIV and
AIDS should be allowed to continue to teach:
632 (51.6) * 323 (26.4) 253 (20.7)
9. A health worker (doctor, nurse) who is
infected with HIV should be allowed to
continue to work with patients:
290 (23.7) * 595 (48.6) 232 (26.3)
10. Even if the food seller is infected with
HIV I would buy food from him/her:
384 (31.4) * 478 (39.1) 345(28.2)
[Note: * = Positive attitude]
Furthermore, the results described in the Table 4 show that, in general, the subjects’ attitudes
towards people living with HIV and AIDS were significantly tolerant and positive. In the major
part of the items, subjects who participated in the study have shown positive attitudes towards
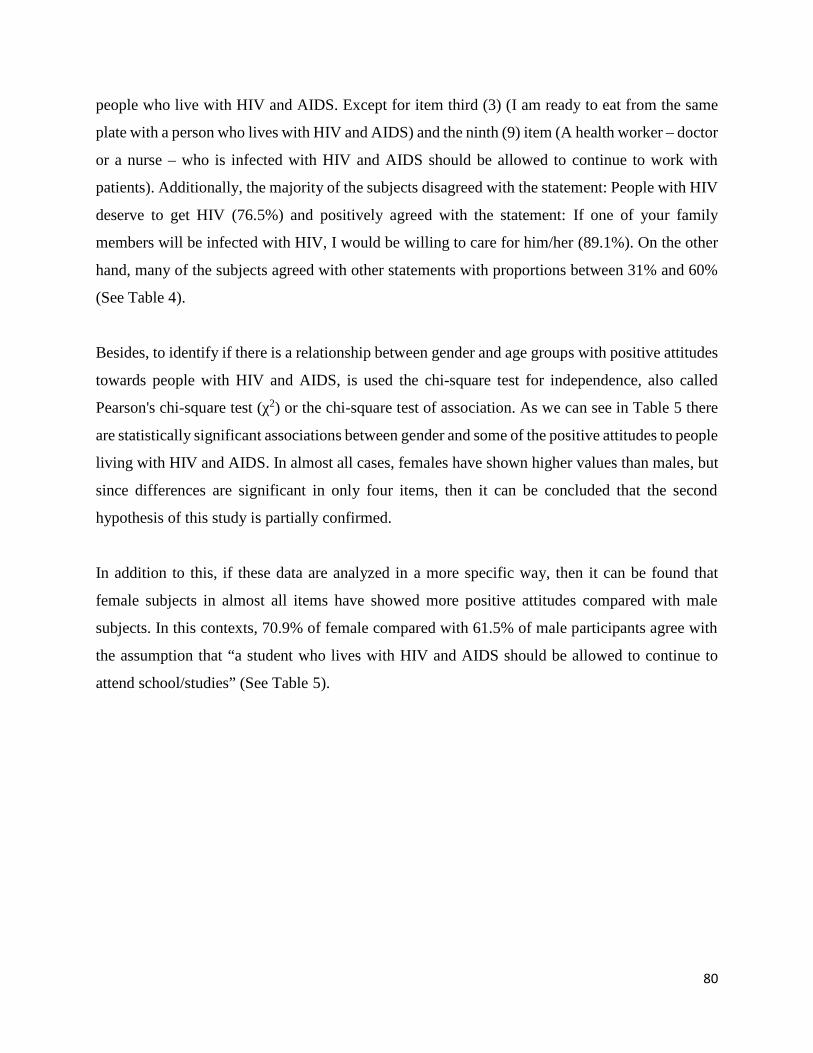
80
people who live with HIV and AIDS. Except for item third (3) (I am ready to eat from the same
plate with a person who lives with HIV and AIDS) and the ninth (9) item (A health worker – doctor
or a nurse – who is infected with HIV and AIDS should be allowed to continue to work with
patients). Additionally, the majority of the subjects disagreed with the statement: People with HIV
deserve to get HIV (76.5%) and positively agreed with the statement: If one of your family
members will be infected with HIV, I would be willing to care for him/her (89.1%). On the other
hand, many of the subjects agreed with other statements with proportions between 31% and 60%
(See Table 4).
Besides, to identify if there is a relationship between gender and age groups with positive attitudes
towards people with HIV and AIDS, is used the chi-square test for independence, also called
Pearson's chi-square test (χ2) or the chi-square test of association. As we can see in Table 5 there
are statistically significant associations between gender and some of the positive attitudes to people
living with HIV and AIDS. In almost all cases, females have shown higher values than males, but
since differences are significant in only four items, then it can be concluded that the second
hypothesis of this study is partially confirmed.
In addition to this, if these data are analyzed in a more specific way, then it can be found that
female subjects in almost all items have showed more positive attitudes compared with male
subjects. In this contexts, 70.9% of female compared with 61.5% of male participants agree with
the assumption that “a student who lives with HIV and AIDS should be allowed to continue to
attend school/studies” (See Table 5).
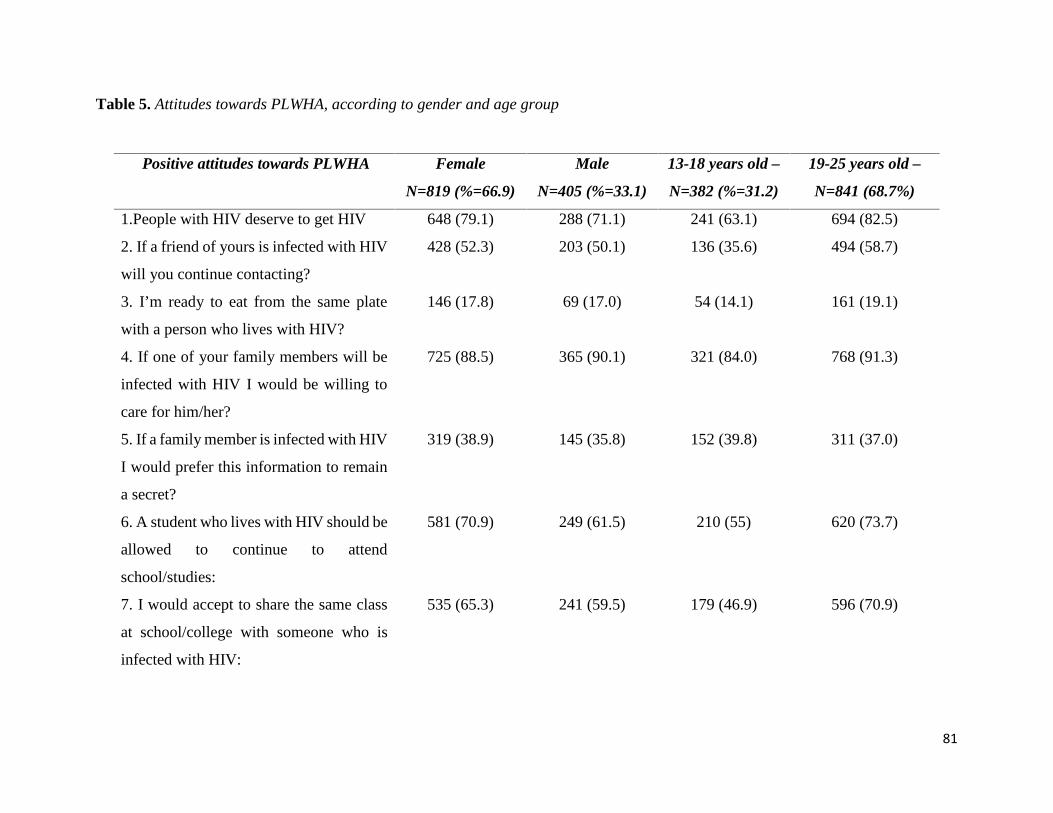
81
Table 5. Attitudes towards PLWHA, according to gender and age group
Positive attitudes towards PLWHA Female
N=819 (%=66.9)
Male
N=405 (%=33.1)
13-18 years old –
N=382 (%=31.2)
19-25 years old –
N=841 (68.7%)
1.People with HIV deserve to get HIV 648 (79.1) 288 (71.1) 241 (63.1) 694 (82.5)
2. If a friend of yours is infected with HIV
will you continue contacting?
428 (52.3) 203 (50.1) 136 (35.6) 494 (58.7)
3. I’m ready to eat from the same plate
with a person who lives with HIV?
146 (17.8) 69 (17.0) 54 (14.1) 161 (19.1)
4. If one of your family members will be
infected with HIV I would be willing to
care for him/her?
725 (88.5) 365 (90.1) 321 (84.0) 768 (91.3)
5. If a family member is infected with HIV
I would prefer this information to remain
a secret?
319 (38.9) 145 (35.8) 152 (39.8) 311 (37.0)
6. A student who lives with HIV should be
allowed to continue to attend
school/studies:
581 (70.9) 249 (61.5) 210 (55) 620 (73.7)
7. I would accept to share the same class
at school/college with someone who is
infected with HIV:
535 (65.3) 241 (59.5) 179 (46.9) 596 (70.9)
82
8. A professor who is infected with HIV
and AIDS should be allowed to continue
to teach:
442 (54.0) 190 (46.9) 140 (36.6) 491 (58.4)
9. A health worker (doctor, nurse) who is
infected with HIV should be allowed to
continue to work with patients:
203 (24.8) 87 (21.5) 66 (17.3) 224 (26.6)
10. Even if the food seller is infected with
HIV I would buy food from him/her:
266 (32.5) 118 (29.1) 91 (23.8) 293 (34.8)
Furthermore, by analyzing both of the targeted groups, adolescents and the emerging adults, as regard to the attitudes towards people
living with HIV and AIDS, the data has shown that emerging adults have demonstrated to have more positive attitudes towards people
living with HIV, compared with the subjects from the group of adolescents. This conclusion in fact confirms the second part of the first
hypothesis of this current study, more precisely emerging adults resulted to have more positive and tolerant attitudes towards people
living with HIV and AIDS. In addition to this, if these data are analyzed in more specific way, then it can be found that in only one
statement (If a family member is infected with HIV I would prefer this information to remain a secret), where subjects of both age
groups (adolescents and emerging adults), almost equally prefer this information to remain a secret (39.0% for adolescents vs. 37.0%
for emerging adults), (see Table 5 and 6).
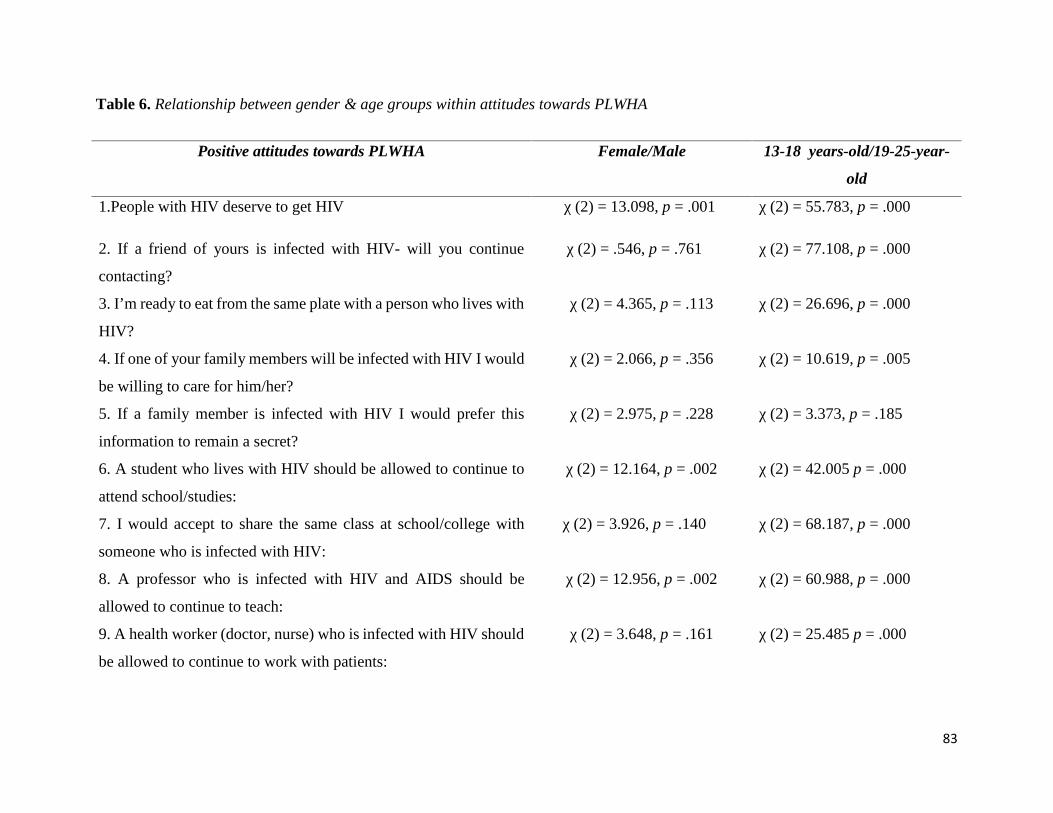
83
Table 6. Relationship between gender & age groups within attitudes towards PLWHA
Positive attitudes towards PLWHA Female/Male 13-18 years-old/19-25-year-
old
1.People with HIV deserve to get HIV χ (2) = 13.098, p = .001 χ (2) = 55.783, p = .000
2. If a friend of yours is infected with HIV- will you continue
contacting?
χ (2) = .546, p = .761 χ (2) = 77.108, p = .000
3. I’m ready to eat from the same plate with a person who lives with
HIV?
χ (2) = 4.365, p = .113 χ (2) = 26.696, p = .000
4. If one of your family members will be infected with HIV I would
be willing to care for him/her?
χ (2) = 2.066, p = .356 χ (2) = 10.619, p = .005
5. If a family member is infected with HIV I would prefer this
information to remain a secret?
χ (2) = 2.975, p = .228 χ (2) = 3.373, p = .185
6. A student who lives with HIV should be allowed to continue to
attend school/studies:
χ (2) = 12.164, p = .002 χ (2) = 42.005 p = .000
7. I would accept to share the same class at school/college with
someone who is infected with HIV:
χ (2) = 3.926, p = .140 χ (2) = 68.187, p = .000
8. A professor who is infected with HIV and AIDS should be
allowed to continue to teach:
χ (2) = 12.956, p = .002 χ (2) = 60.988, p = .000
9. A health worker (doctor, nurse) who is infected with HIV should
be allowed to continue to work with patients:
χ (2) = 3.648, p = .161 χ (2) = 25.485 p = .000
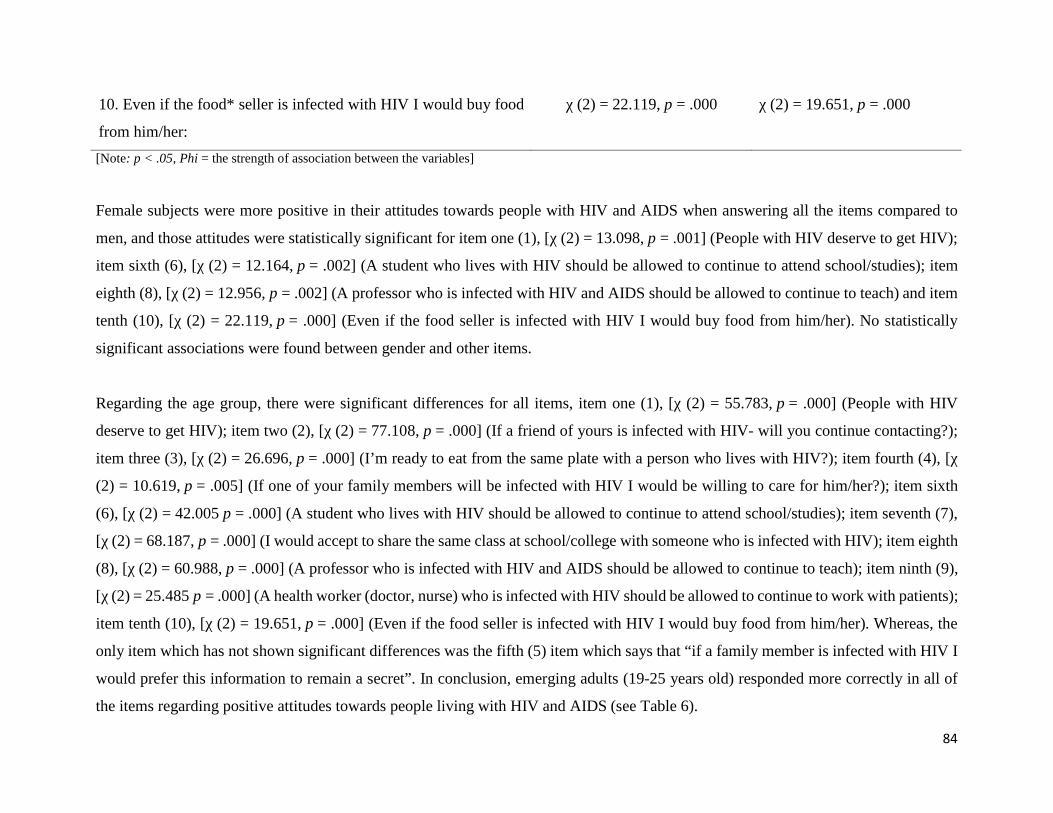
84
10. Even if the food* seller is infected with HIV I would buy food
from him/her:
χ (2) = 22.119, p = .000 χ (2) = 19.651, p = .000
[Note: p < .05, Phi = the strength of association between the variables]
Female subjects were more positive in their attitudes towards people with HIV and AIDS when answering all the items compared to
men, and those attitudes were statistically significant for item one (1), [χ (2) = 13.098, p = .001] (People with HIV deserve to get HIV);
item sixth (6), [χ (2) = 12.164, p = .002] (A student who lives with HIV should be allowed to continue to attend school/studies); item
eighth (8), [χ (2) = 12.956, p = .002] (A professor who is infected with HIV and AIDS should be allowed to continue to teach) and item
tenth (10), [χ (2) = 22.119, p = .000] (Even if the food seller is infected with HIV I would buy food from him/her). No statistically
significant associations were found between gender and other items.
Regarding the age group, there were significant differences for all items, item one (1), [χ (2) = 55.783, p = .000] (People with HIV
deserve to get HIV); item two (2), [χ (2) = 77.108, p = .000] (If a friend of yours is infected with HIV- will you continue contacting?);
item three (3), [χ (2) = 26.696, p = .000] (I’m ready to eat from the same plate with a person who lives with HIV?); item fourth (4), [χ
(2) = 10.619, p = .005] (If one of your family members will be infected with HIV I would be willing to care for him/her?); item sixth
(6), [χ (2) = 42.005 p = .000] (A student who lives with HIV should be allowed to continue to attend school/studies); item seventh (7),
[χ (2) = 68.187, p = .000] (I would accept to share the same class at school/college with someone who is infected with HIV); item eighth
(8), [χ (2) = 60.988, p = .000] (A professor who is infected with HIV and AIDS should be allowed to continue to teach); item ninth (9),
[χ (2) = 25.485 p = .000] (A health worker (doctor, nurse) who is infected with HIV should be allowed to continue to work with patients);
item tenth (10), [χ (2) = 19.651, p = .000] (Even if the food seller is infected with HIV I would buy food from him/her). Whereas, the
only item which has not shown significant differences was the fifth (5) item which says that “if a family member is infected with HIV I
would prefer this information to remain a secret”. In conclusion, emerging adults (19-25 years old) responded more correctly in all of
the items regarding positive attitudes towards people living with HIV and AIDS (see Table 6).
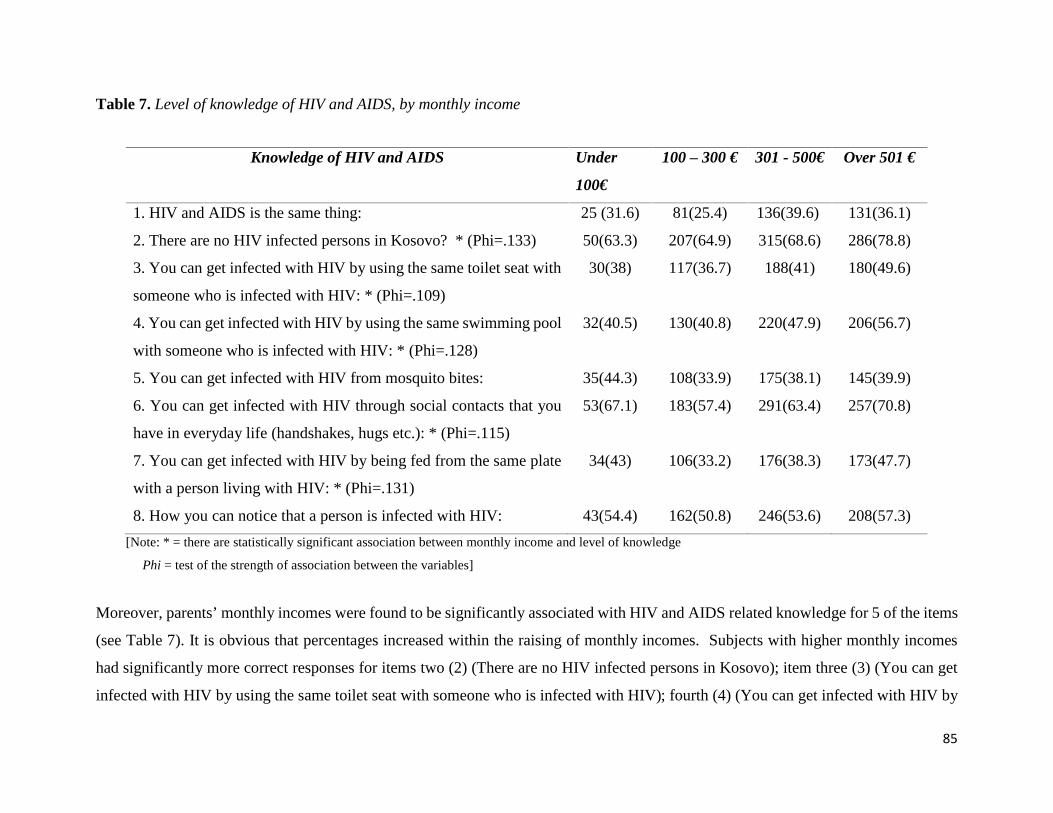
85
Table 7. Level of knowledge of HIV and AIDS, by monthly income
Knowledge of HIV and AIDS Under
100€
100 – 300 € 301 - 500€ Over 501 €
1. HIV and AIDS is the same thing: 25 (31.6) 81(25.4) 136(39.6) 131(36.1)
2. There are no HIV infected persons in Kosovo? * (Phi=.133) 50(63.3) 207(64.9) 315(68.6) 286(78.8)
3. You can get infected with HIV by using the same toilet seat with
someone who is infected with HIV: * (Phi=.109)
30(38) 117(36.7) 188(41) 180(49.6)
4. You can get infected with HIV by using the same swimming pool
with someone who is infected with HIV: * (Phi=.128)
32(40.5) 130(40.8) 220(47.9) 206(56.7)
5. You can get infected with HIV from mosquito bites: 35(44.3) 108(33.9) 175(38.1) 145(39.9)
6. You can get infected with HIV through social contacts that you
have in everyday life (handshakes, hugs etc.): * (Phi=.115)
53(67.1) 183(57.4) 291(63.4) 257(70.8)
7. You can get infected with HIV by being fed from the same plate
with a person living with HIV: * (Phi=.131)
34(43) 106(33.2) 176(38.3) 173(47.7)
8. How you can notice that a person is infected with HIV: 43(54.4) 162(50.8) 246(53.6) 208(57.3)
[Note: * = there are statistically significant association between monthly income and level of knowledge
Phi = test of the strength of association between the variables]
Moreover, parents’ monthly incomes were found to be significantly associated with HIV and AIDS related knowledge for 5 of the items
(see Table 7). It is obvious that percentages increased within the raising of monthly incomes. Subjects with higher monthly incomes
had significantly more correct responses for items two (2) (There are no HIV infected persons in Kosovo); item three (3) (You can get
infected with HIV by using the same toilet seat with someone who is infected with HIV); fourth (4) (You can get infected with HIV by
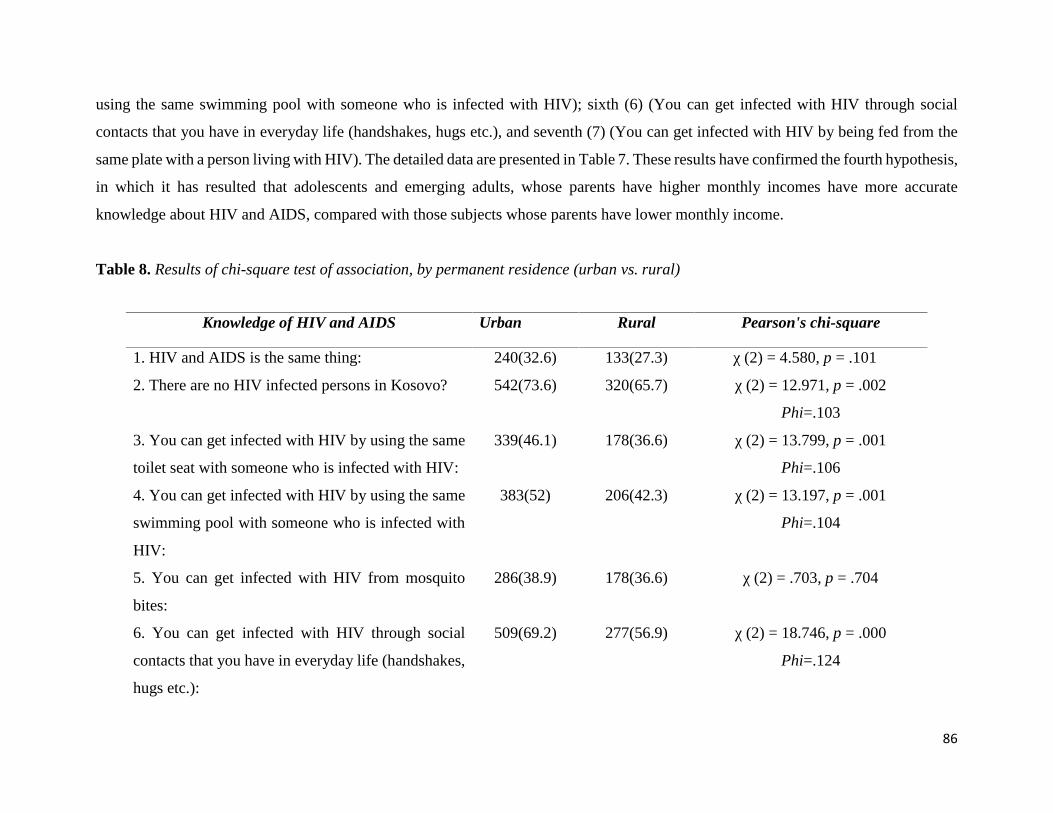
86
using the same swimming pool with someone who is infected with HIV); sixth (6) (You can get infected with HIV through social
contacts that you have in everyday life (handshakes, hugs etc.), and seventh (7) (You can get infected with HIV by being fed from the
same plate with a person living with HIV). The detailed data are presented in Table 7. These results have confirmed the fourth hypothesis,
in which it has resulted that adolescents and emerging adults, whose parents have higher monthly incomes have more accurate
knowledge about HIV and AIDS, compared with those subjects whose parents have lower monthly income.
Table 8. Results of chi-square test of association, by permanent residence (urban vs. rural)
Knowledge of HIV and AIDS Urban Rural Pearson's chi-square
1. HIV and AIDS is the same thing: 240(32.6) 133(27.3) χ (2) = 4.580, p = .101
2. There are no HIV infected persons in Kosovo? 542(73.6) 320(65.7) χ (2) = 12.971, p = .002
Phi=.103
3. You can get infected with HIV by using the same
toilet seat with someone who is infected with HIV:
339(46.1) 178(36.6) χ (2) = 13.799, p = .001
Phi=.106
4. You can get infected with HIV by using the same
swimming pool with someone who is infected with
HIV:
383(52) 206(42.3) χ (2) = 13.197, p = .001
Phi=.104
5. You can get infected with HIV from mosquito
bites:
286(38.9) 178(36.6) χ (2) = .703, p = .704
6. You can get infected with HIV through social
contacts that you have in everyday life (handshakes,
hugs etc.):
509(69.2) 277(56.9) χ (2) = 18.746, p = .000
Phi=.124
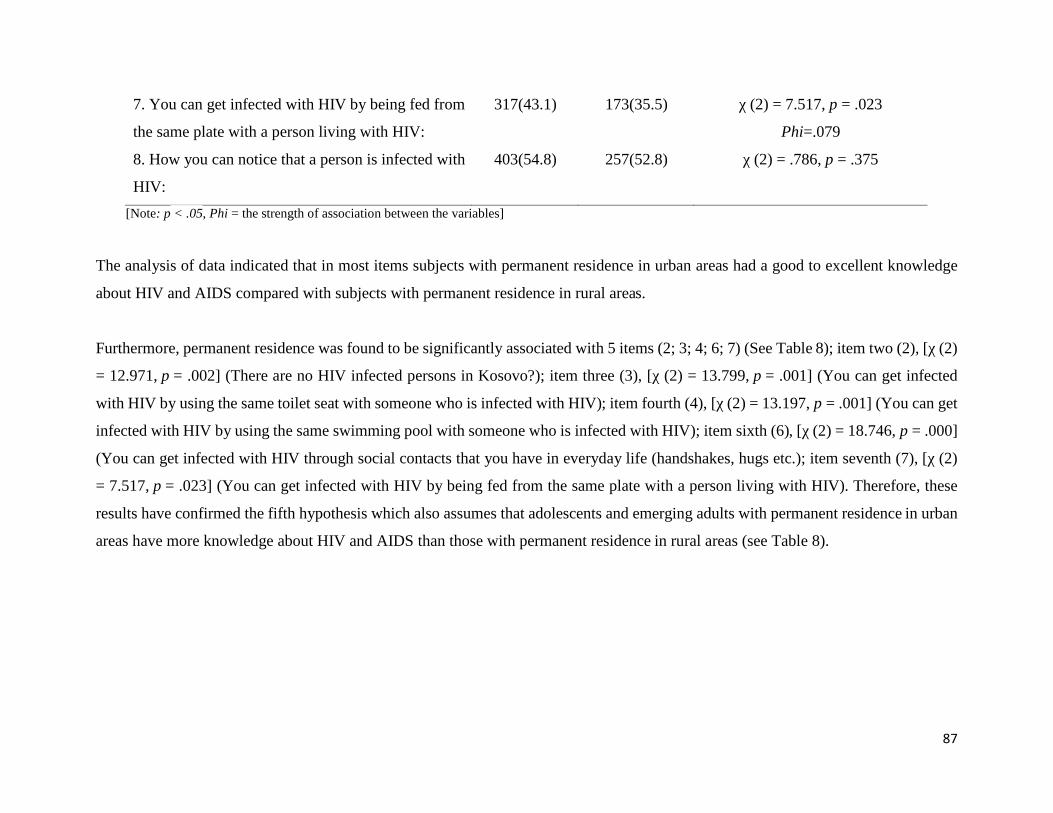
87
7. You can get infected with HIV by being fed from
the same plate with a person living with HIV:
317(43.1) 173(35.5) χ (2) = 7.517, p = .023
Phi=.079
8. How you can notice that a person is infected with
HIV:
403(54.8) 257(52.8) χ (2) = .786, p = .375
[Note: p < .05, Phi = the strength of association between the variables]
The analysis of data indicated that in most items subjects with permanent residence in urban areas had a good to excellent knowledge
about HIV and AIDS compared with subjects with permanent residence in rural areas.
Furthermore, permanent residence was found to be significantly associated with 5 items (2; 3; 4; 6; 7) (See Table 8); item two (2), [χ (2)
= 12.971, p = .002] (There are no HIV infected persons in Kosovo?); item three (3), [χ (2) = 13.799, p = .001] (You can get infected
with HIV by using the same toilet seat with someone who is infected with HIV); item fourth (4), [χ (2) = 13.197, p = .001] (You can get
infected with HIV by using the same swimming pool with someone who is infected with HIV); item sixth (6), [χ (2) = 18.746, p = .000]
(You can get infected with HIV through social contacts that you have in everyday life (handshakes, hugs etc.); item seventh (7), [χ (2)
= 7.517, p = .023] (You can get infected with HIV by being fed from the same plate with a person living with HIV). Therefore, these
results have confirmed the fifth hypothesis which also assumes that adolescents and emerging adults with permanent residence in urban
areas have more knowledge about HIV and AIDS than those with permanent residence in rural areas (see Table 8).
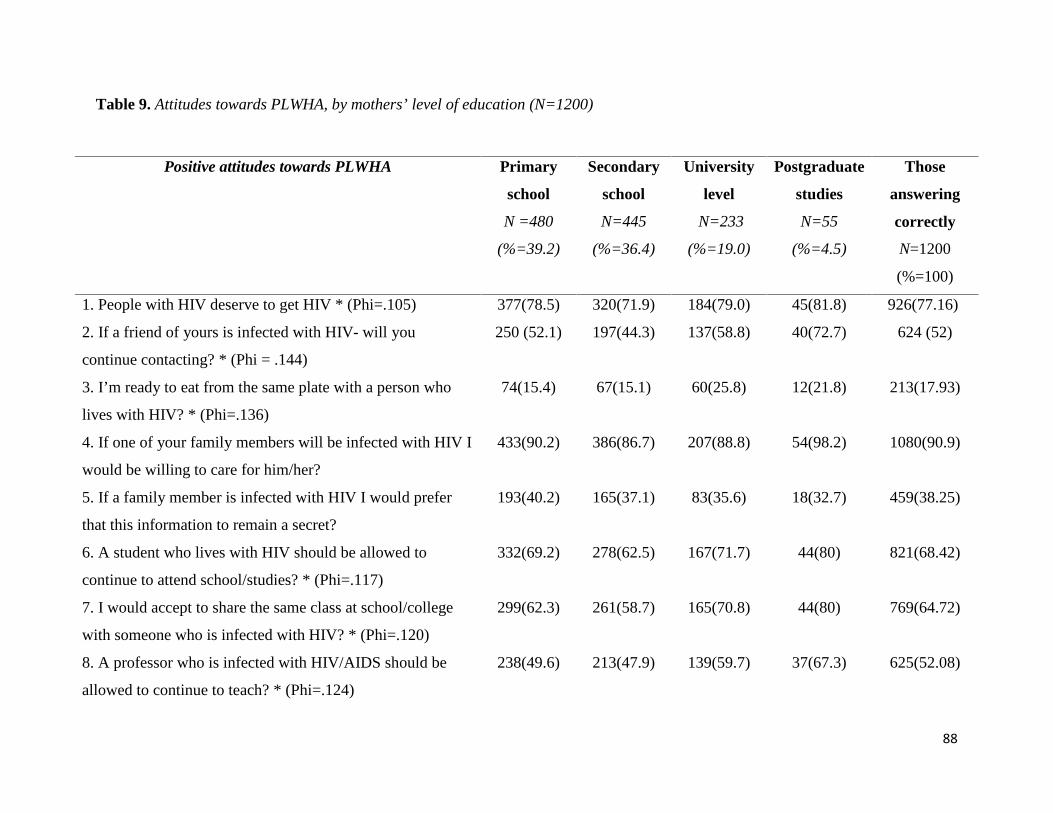
88
Table 9. Attitudes towards PLWHA, by mothers’ level of education (N=1200)
Positive attitudes towards PLWHA Primary
school
N =480
(%=39.2)
Secondary
school
N=445
(%=36.4)
University
level
N=233
(%=19.0)
Postgraduate
studies
N=55
(%=4.5)
Those
answering
correctly
N=1200
(%=100)
1. People with HIV deserve to get HIV * (Phi=.105) 377(78.5) 320(71.9) 184(79.0) 45(81.8) 926(77.16)
2. If a friend of yours is infected with HIV- will you
continue contacting? * (Phi = .144)
250 (52.1) 197(44.3) 137(58.8) 40(72.7) 624 (52)
3. I’m ready to eat from the same plate with a person who
lives with HIV? * (Phi=.136)
74(15.4) 67(15.1) 60(25.8) 12(21.8) 213(17.93)
4. If one of your family members will be infected with HIV I
would be willing to care for him/her?
433(90.2) 386(86.7) 207(88.8) 54(98.2) 1080(90.9)
5. If a family member is infected with HIV I would prefer
that this information to remain a secret?
193(40.2) 165(37.1) 83(35.6) 18(32.7) 459(38.25)
6. A student who lives with HIV should be allowed to
continue to attend school/studies? * (Phi=.117)
332(69.2) 278(62.5) 167(71.7) 44(80) 821(68.42)
7. I would accept to share the same class at school/college
with someone who is infected with HIV? * (Phi=.120)
299(62.3) 261(58.7) 165(70.8) 44(80) 769(64.72)
8. A professor who is infected with HIV/AIDS should be
allowed to continue to teach? * (Phi=.124)
238(49.6) 213(47.9) 139(59.7) 37(67.3) 625(52.08)
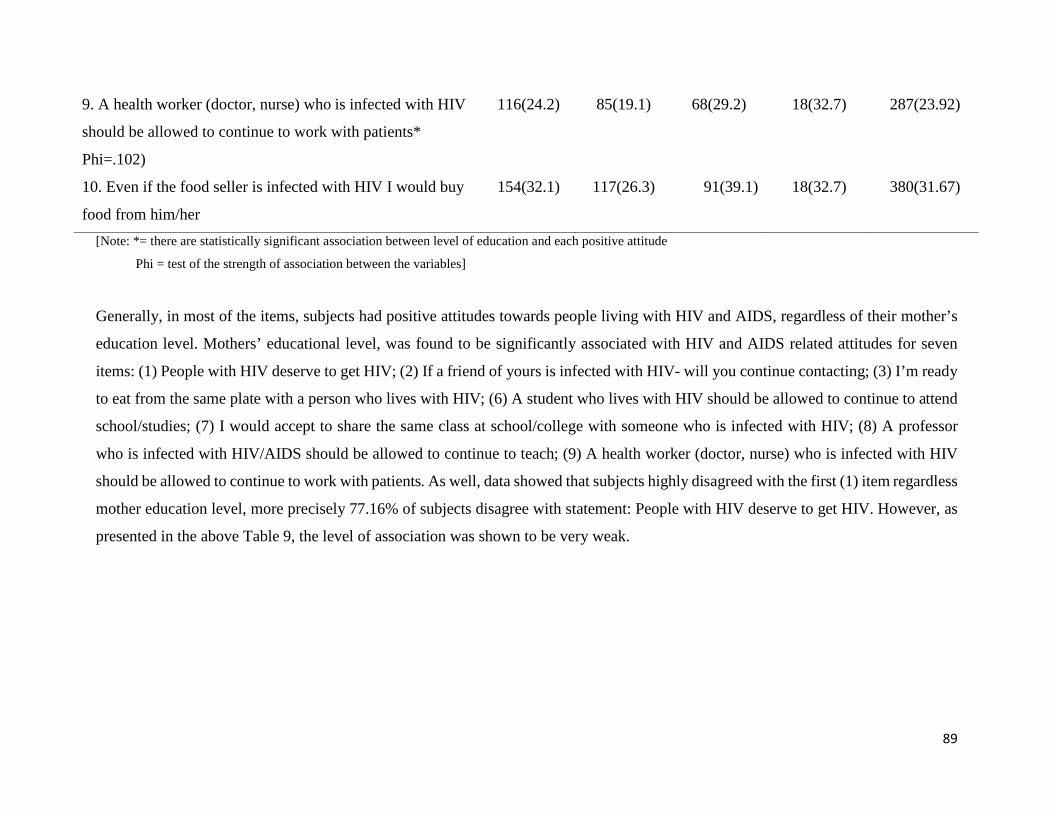
89
9. A health worker (doctor, nurse) who is infected with HIV
should be allowed to continue to work with patients*
Phi=.102)
116(24.2) 85(19.1) 68(29.2) 18(32.7) 287(23.92)
10. Even if the food seller is infected with HIV I would buy
food from him/her
154(32.1) 117(26.3) 91(39.1) 18(32.7) 380(31.67)
[Note: *= there are statistically significant association between level of education and each positive attitude
Phi = test of the strength of association between the variables]
Generally, in most of the items, subjects had positive attitudes towards people living with HIV and AIDS, regardless of their mother’s
education level. Mothers’ educational level, was found to be significantly associated with HIV and AIDS related attitudes for seven
items: (1) People with HIV deserve to get HIV; (2) If a friend of yours is infected with HIV- will you continue contacting; (3) I’m ready
to eat from the same plate with a person who lives with HIV; (6) A student who lives with HIV should be allowed to continue to attend
school/studies; (7) I would accept to share the same class at school/college with someone who is infected with HIV; (8) A professor
who is infected with HIV/AIDS should be allowed to continue to teach; (9) A health worker (doctor, nurse) who is infected with HIV
should be allowed to continue to work with patients. As well, data showed that subjects highly disagreed with the first (1) item regardless
mother education level, more precisely 77.16% of subjects disagree with statement: People with HIV deserve to get HIV. However, as
presented in the above Table 9, the level of association was shown to be very weak.
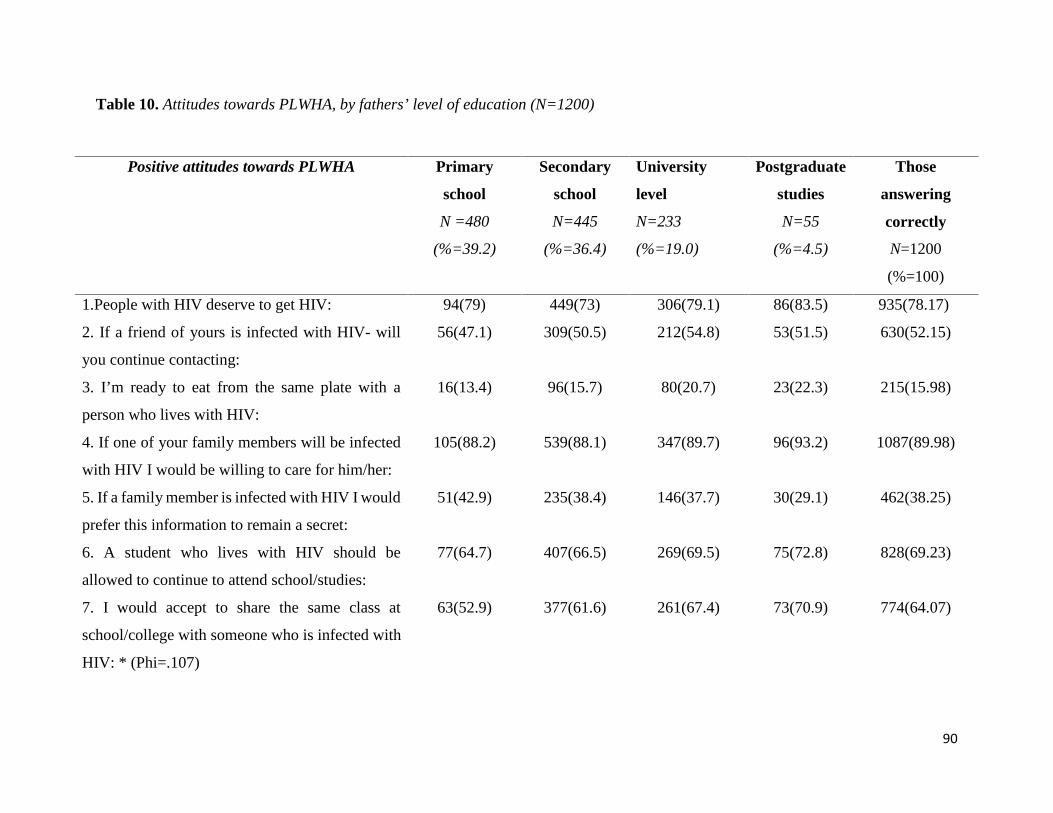
90
Table 10. Attitudes towards PLWHA, by fathers’ level of education (N=1200)
Positive attitudes towards PLWHA Primary
school
N =480
(%=39.2)
Secondary
school
N=445
(%=36.4)
University
level
N=233
(%=19.0)
Postgraduate
studies
N=55
(%=4.5)
Those
answering
correctly
N=1200
(%=100)
1.People with HIV deserve to get HIV: 94(79) 449(73) 306(79.1) 86(83.5) 935(78.17)
2. If a friend of yours is infected with HIV- will
you continue contacting:
56(47.1) 309(50.5) 212(54.8) 53(51.5) 630(52.15)
3. I’m ready to eat from the same plate with a
person who lives with HIV:
16(13.4) 96(15.7) 80(20.7) 23(22.3) 215(15.98)
4. If one of your family members will be infected
with HIV I would be willing to care for him/her:
105(88.2) 539(88.1) 347(89.7) 96(93.2) 1087(89.98)
5. If a family member is infected with HIV I would
prefer this information to remain a secret:
51(42.9) 235(38.4) 146(37.7) 30(29.1) 462(38.25)
6. A student who lives with HIV should be
allowed to continue to attend school/studies:
77(64.7) 407(66.5) 269(69.5) 75(72.8) 828(69.23)
7. I would accept to share the same class at
school/college with someone who is infected with
HIV: * (Phi=.107)
63(52.9) 377(61.6) 261(67.4) 73(70.9) 774(64.07)
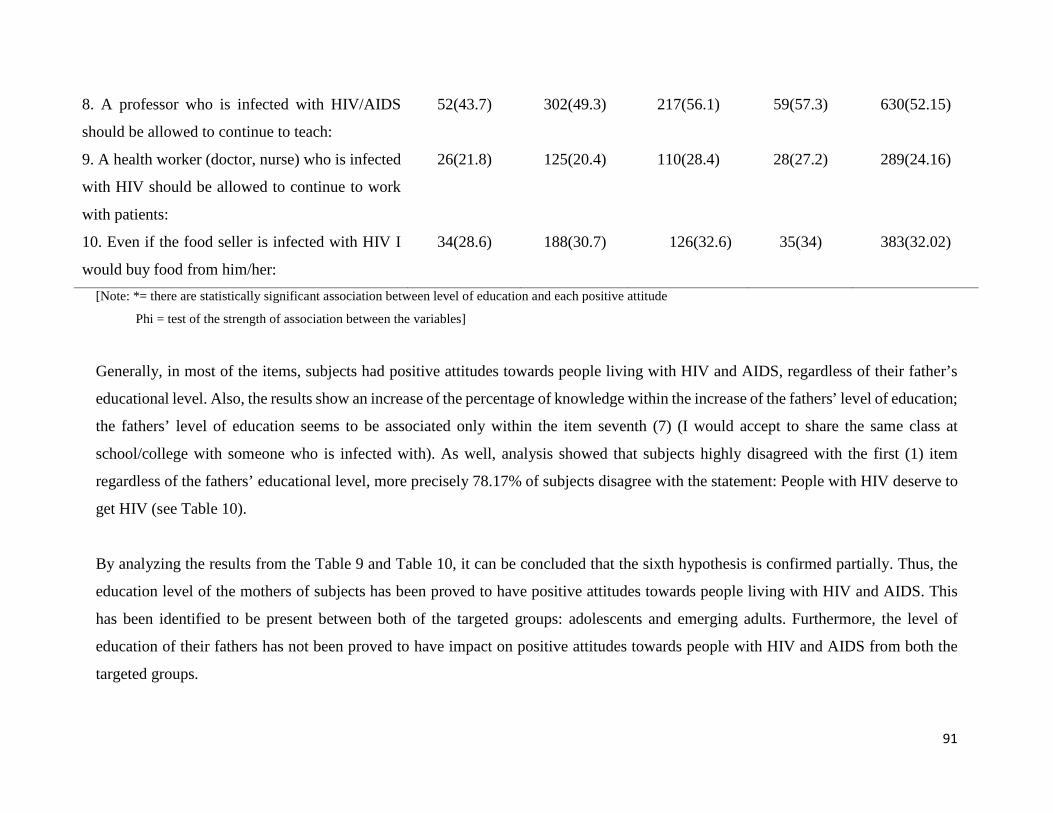
91
8. A professor who is infected with HIV/AIDS
should be allowed to continue to teach:
52(43.7) 302(49.3) 217(56.1) 59(57.3) 630(52.15)
9. A health worker (doctor, nurse) who is infected
with HIV should be allowed to continue to work
with patients:
26(21.8) 125(20.4) 110(28.4) 28(27.2) 289(24.16)
10. Even if the food seller is infected with HIV I
would buy food from him/her:
34(28.6) 188(30.7) 126(32.6) 35(34) 383(32.02)
[Note: *= there are statistically significant association between level of education and each positive attitude
Phi = test of the strength of association between the variables]
Generally, in most of the items, subjects had positive attitudes towards people living with HIV and AIDS, regardless of their father’s
educational level. Also, the results show an increase of the percentage of knowledge within the increase of the fathers’ level of education;
the fathers’ level of education seems to be associated only within the item seventh (7) (I would accept to share the same class at
school/college with someone who is infected with). As well, analysis showed that subjects highly disagreed with the first (1) item
regardless of the fathers’ educational level, more precisely 78.17% of subjects disagree with the statement: People with HIV deserve to
get HIV (see Table 10).
By analyzing the results from the Table 9 and Table 10, it can be concluded that the sixth hypothesis is confirmed partially. Thus, the
education level of the mothers of subjects has been proved to have positive attitudes towards people living with HIV and AIDS. This
has been identified to be present between both of the targeted groups: adolescents and emerging adults. Furthermore, the level of
education of their fathers has not been proved to have impact on positive attitudes towards people with HIV and AIDS from both the
targeted groups.
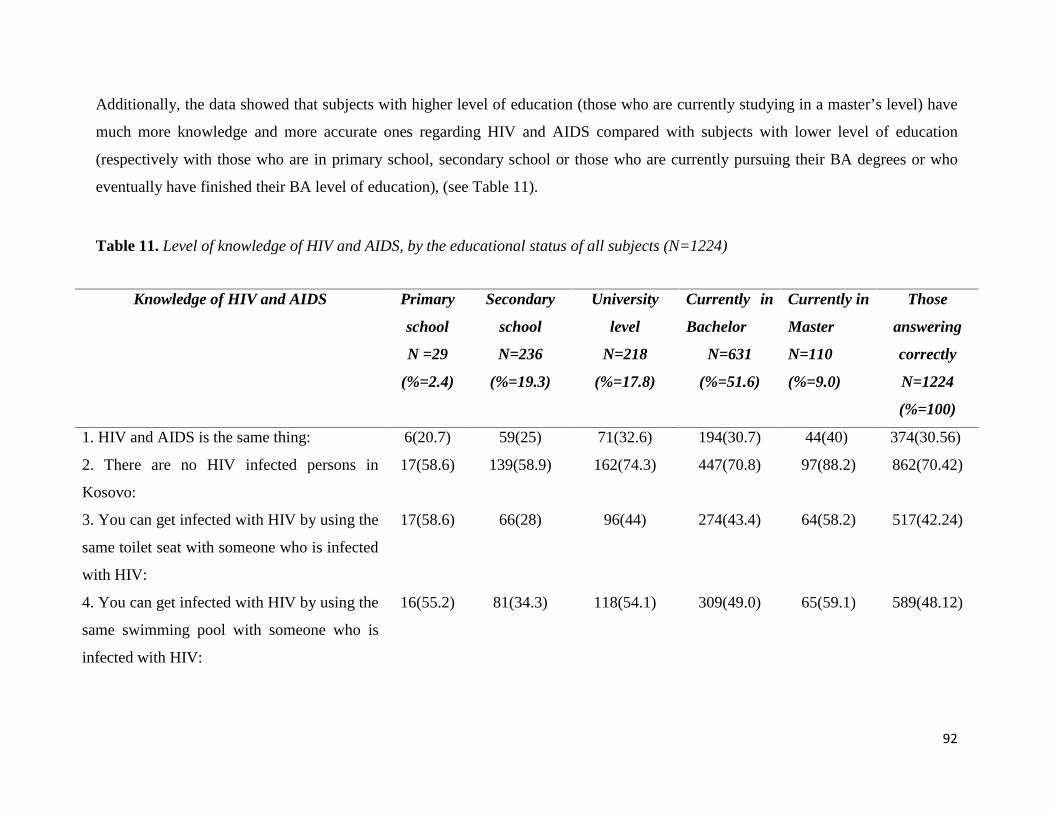
92
Additionally, the data showed that subjects with higher level of education (those who are currently studying in a master’s level) have
much more knowledge and more accurate ones regarding HIV and AIDS compared with subjects with lower level of education
(respectively with those who are in primary school, secondary school or those who are currently pursuing their BA degrees or who
eventually have finished their BA level of education), (see Table 11).
Table 11. Level of knowledge of HIV and AIDS, by the educational status of all subjects (N=1224)
Knowledge of HIV and AIDS Primary
school
N =29
(%=2.4)
Secondary
school
N=236
(%=19.3)
University
level
N=218
(%=17.8)
Currently in
Bachelor
N=631
(%=51.6)
Currently in
Master
N=110
(%=9.0)
Those
answering
correctly
N=1224
(%=100)
1. HIV and AIDS is the same thing: 6(20.7) 59(25) 71(32.6) 194(30.7) 44(40) 374(30.56)
2. There are no HIV infected persons in
Kosovo:
17(58.6) 139(58.9) 162(74.3) 447(70.8) 97(88.2) 862(70.42)
3. You can get infected with HIV by using the
same toilet seat with someone who is infected
with HIV:
17(58.6) 66(28) 96(44) 274(43.4) 64(58.2) 517(42.24)
4. You can get infected with HIV by using the
same swimming pool with someone who is
infected with HIV:
16(55.2) 81(34.3) 118(54.1) 309(49.0) 65(59.1) 589(48.12)
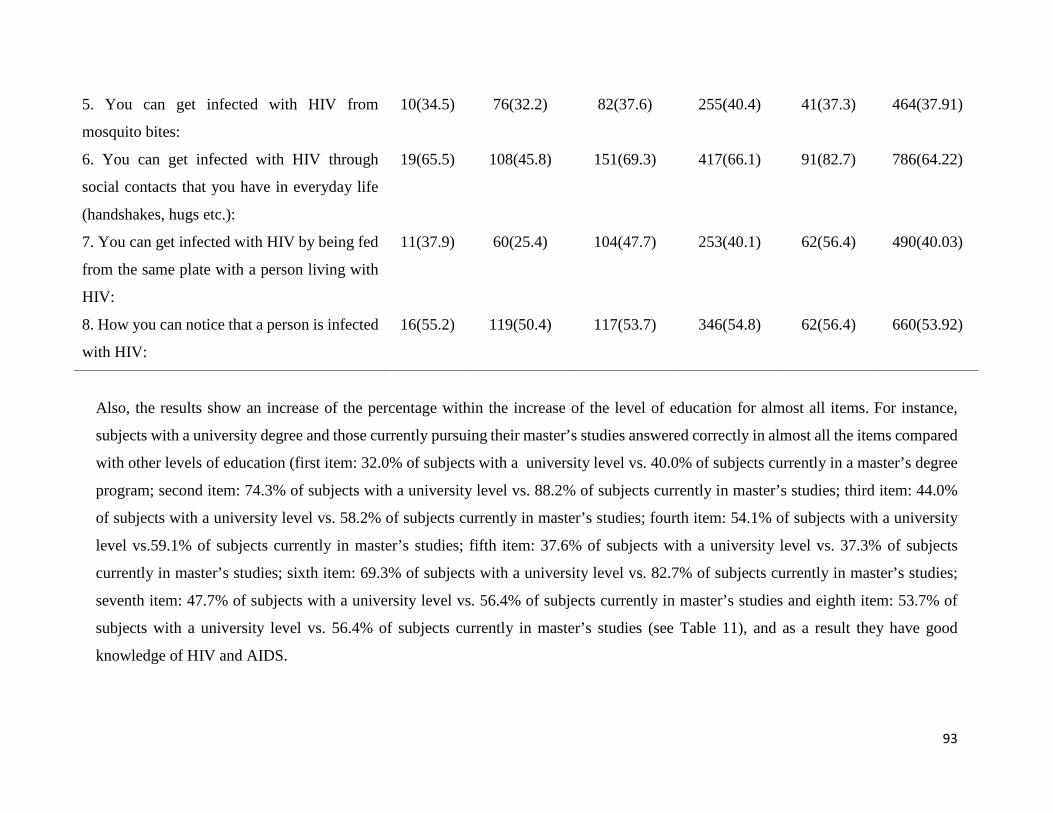
93
5. You can get infected with HIV from
mosquito bites:
10(34.5) 76(32.2) 82(37.6) 255(40.4) 41(37.3) 464(37.91)
6. You can get infected with HIV through
social contacts that you have in everyday life
(handshakes, hugs etc.):
19(65.5) 108(45.8) 151(69.3) 417(66.1) 91(82.7) 786(64.22)
7. You can get infected with HIV by being fed
from the same plate with a person living with
HIV:
11(37.9) 60(25.4) 104(47.7) 253(40.1) 62(56.4) 490(40.03)
8. How you can notice that a person is infected
with HIV:
16(55.2) 119(50.4) 117(53.7) 346(54.8) 62(56.4) 660(53.92)
Also, the results show an increase of the percentage within the increase of the level of education for almost all items. For instance,
subjects with a university degree and those currently pursuing their master’s studies answered correctly in almost all the items compared
with other levels of education (first item: 32.0% of subjects with a university level vs. 40.0% of subjects currently in a master’s degree
program; second item: 74.3% of subjects with a university level vs. 88.2% of subjects currently in master’s studies; third item: 44.0%
of subjects with a university level vs. 58.2% of subjects currently in master’s studies; fourth item: 54.1% of subjects with a university
level vs.59.1% of subjects currently in master’s studies; fifth item: 37.6% of subjects with a university level vs. 37.3% of subjects
currently in master’s studies; sixth item: 69.3% of subjects with a university level vs. 82.7% of subjects currently in master’s studies;
seventh item: 47.7% of subjects with a university level vs. 56.4% of subjects currently in master’s studies and eighth item: 53.7% of
subjects with a university level vs. 56.4% of subjects currently in master’s studies (see Table 11), and as a result they have good
knowledge of HIV and AIDS.
94
In addition, there were some interesting responses for item three (3) (You can get infected with HIV by using the same toilet seat with
someone who is infected with HIV); item four (4) (you can get infected with HIV by using the same swimming pool with someone who
is infected with HIV); item six (6) (you can get infected with HIV through social contacts that you have in everyday life (handshakes,
hugs etc.); and item seven (7) (you can get infected with HIV by being fed from the same plate with a person living with HIV), where
subjects with a primary education showed better knowledge than participants with a secondary level of education (see Table 11).
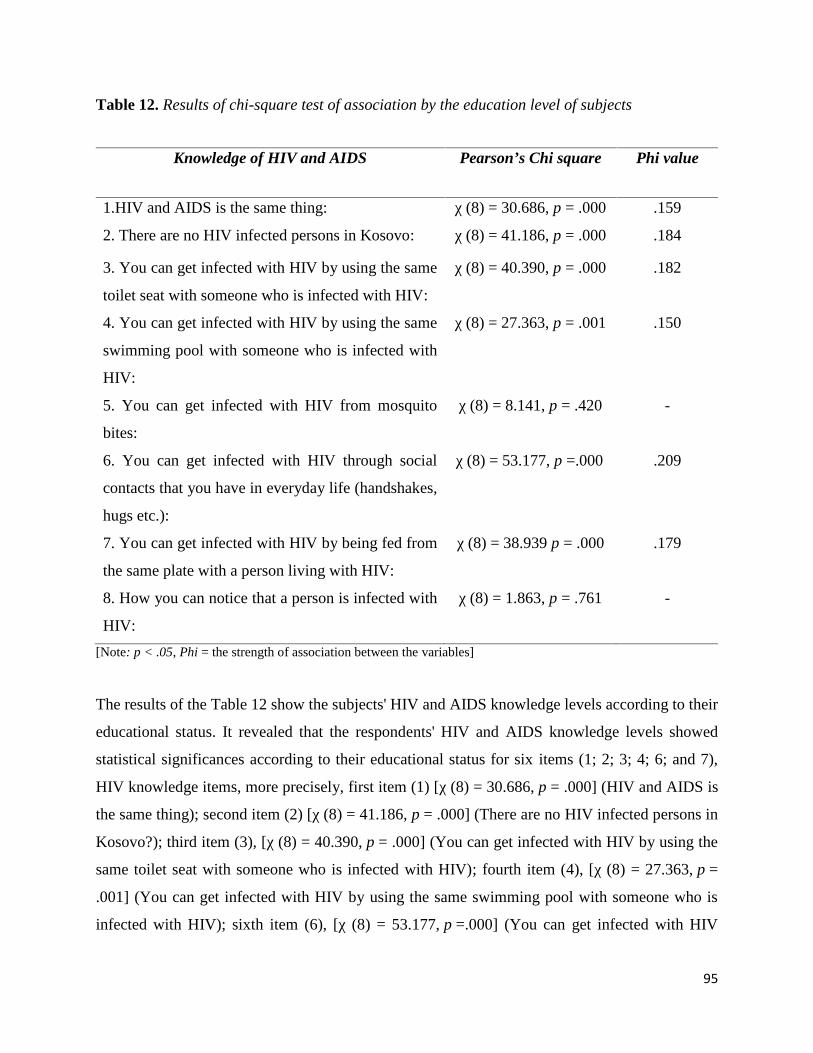
95
Table 12. Results of chi-square test of association by the education level of subjects
Knowledge of HIV and AIDS Pearson’s Chi square Phi value
1.HIV and AIDS is the same thing: χ (8) = 30.686, p = .000 .159
2. There are no HIV infected persons in Kosovo: χ (8) = 41.186, p = .000 .184
3. You can get infected with HIV by using the same
toilet seat with someone who is infected with HIV:
χ (8) = 40.390, p = .000 .182
4. You can get infected with HIV by using the same
swimming pool with someone who is infected with
HIV:
χ (8) = 27.363, p = .001 .150
5. You can get infected with HIV from mosquito
bites:
χ (8) = 8.141, p = .420 -
6. You can get infected with HIV through social
contacts that you have in everyday life (handshakes,
hugs etc.):
χ (8) = 53.177, p =.000 .209
7. You can get infected with HIV by being fed from
the same plate with a person living with HIV:
χ (8) = 38.939 p = .000 .179
8. How you can notice that a person is infected with
HIV:
χ (8) = 1.863, p = .761 -
[Note: p < .05, Phi = the strength of association between the variables]
The results of the Table 12 show the subjects' HIV and AIDS knowledge levels according to their
educational status. It revealed that the respondents' HIV and AIDS knowledge levels showed
statistical significances according to their educational status for six items (1; 2; 3; 4; 6; and 7),
HIV knowledge items, more precisely, first item (1) [χ (8) = 30.686, p = .000] (HIV and AIDS is
the same thing); second item (2) [χ (8) = 41.186, p = .000] (There are no HIV infected persons in
Kosovo?); third item (3), [χ (8) = 40.390, p = .000] (You can get infected with HIV by using the
same toilet seat with someone who is infected with HIV); fourth item (4), [χ (8) = 27.363, p =
.001] (You can get infected with HIV by using the same swimming pool with someone who is
infected with HIV); sixth item (6), [χ (8) = 53.177, p =.000] (You can get infected with HIV
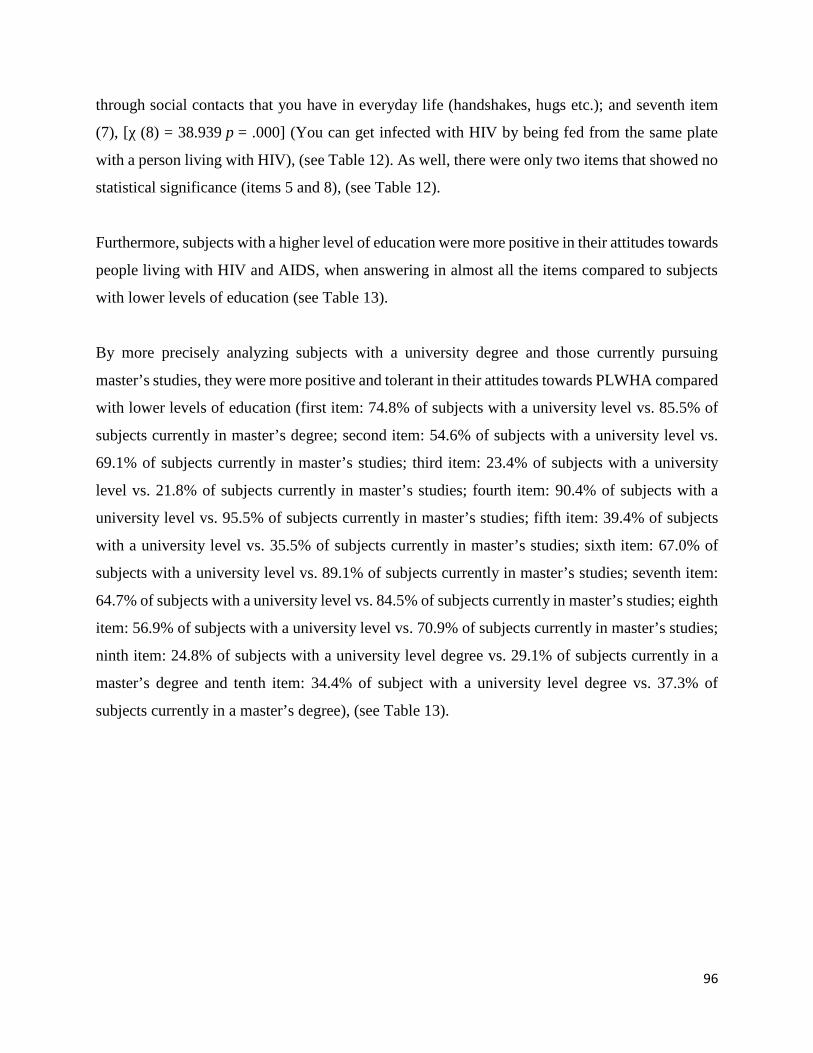
96
through social contacts that you have in everyday life (handshakes, hugs etc.); and seventh item
(7), [χ (8) = 38.939 p = .000] (You can get infected with HIV by being fed from the same plate
with a person living with HIV), (see Table 12). As well, there were only two items that showed no
statistical significance (items 5 and 8), (see Table 12).
Furthermore, subjects with a higher level of education were more positive in their attitudes towards
people living with HIV and AIDS, when answering in almost all the items compared to subjects
with lower levels of education (see Table 13).
By more precisely analyzing subjects with a university degree and those currently pursuing
master’s studies, they were more positive and tolerant in their attitudes towards PLWHA compared
with lower levels of education (first item: 74.8% of subjects with a university level vs. 85.5% of
subjects currently in master’s degree; second item: 54.6% of subjects with a university level vs.
69.1% of subjects currently in master’s studies; third item: 23.4% of subjects with a university
level vs. 21.8% of subjects currently in master’s studies; fourth item: 90.4% of subjects with a
university level vs. 95.5% of subjects currently in master’s studies; fifth item: 39.4% of subjects
with a university level vs. 35.5% of subjects currently in master’s studies; sixth item: 67.0% of
subjects with a university level vs. 89.1% of subjects currently in master’s studies; seventh item:
64.7% of subjects with a university level vs. 84.5% of subjects currently in master’s studies; eighth
item: 56.9% of subjects with a university level vs. 70.9% of subjects currently in master’s studies;
ninth item: 24.8% of subjects with a university level degree vs. 29.1% of subjects currently in a
master’s degree and tenth item: 34.4% of subject with a university level degree vs. 37.3% of
subjects currently in a master’s degree), (see Table 13).
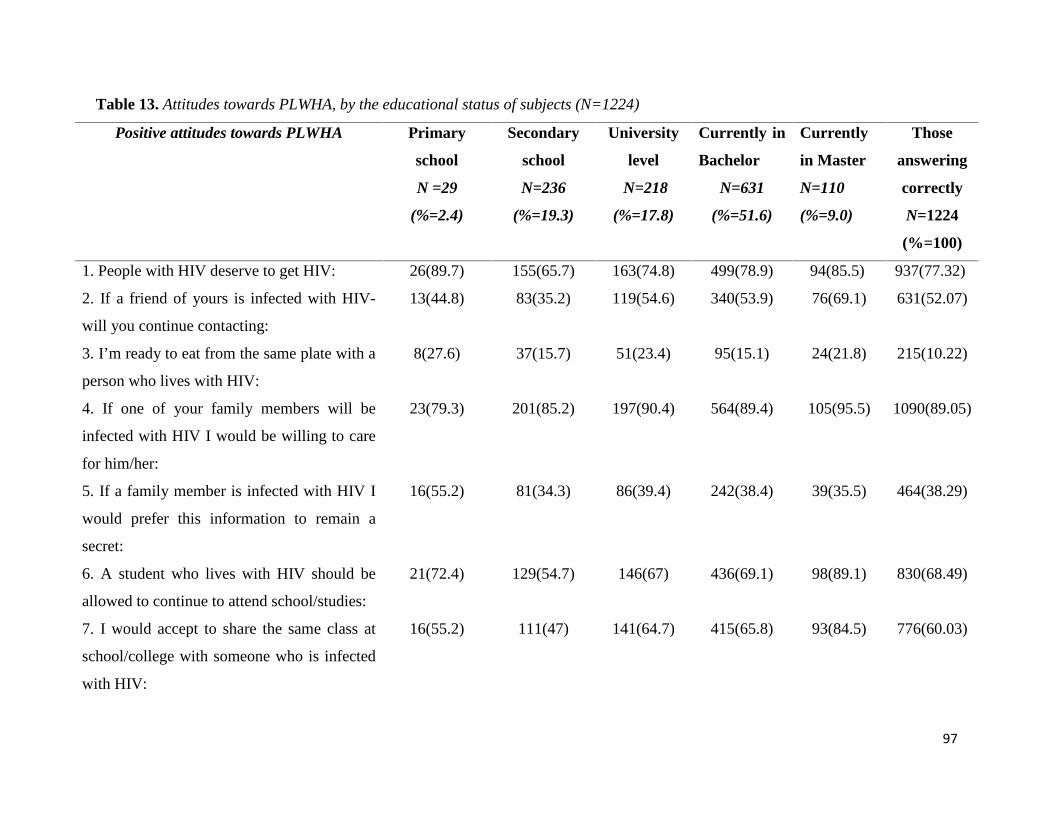
97
Table 13. Attitudes towards PLWHA, by the educational status of subjects (N=1224)
Positive attitudes towards PLWHA Primary
school
N =29
(%=2.4)
Secondary
school
N=236
(%=19.3)
University
level
N=218
(%=17.8)
Currently in
Bachelor
N=631
(%=51.6)
Currently
in Master
N=110
(%=9.0)
Those
answering
correctly
N=1224
(%=100)
1. People with HIV deserve to get HIV: 26(89.7) 155(65.7) 163(74.8) 499(78.9) 94(85.5) 937(77.32)
2. If a friend of yours is infected with HIV-
will you continue contacting:
13(44.8) 83(35.2) 119(54.6) 340(53.9) 76(69.1) 631(52.07)
3. I’m ready to eat from the same plate with a
person who lives with HIV:
8(27.6) 37(15.7) 51(23.4) 95(15.1) 24(21.8) 215(10.22)
4. If one of your family members will be
infected with HIV I would be willing to care
for him/her:
23(79.3) 201(85.2) 197(90.4) 564(89.4) 105(95.5) 1090(89.05)
5. If a family member is infected with HIV I
would prefer this information to remain a
secret:
16(55.2) 81(34.3) 86(39.4) 242(38.4) 39(35.5) 464(38.29)
6. A student who lives with HIV should be
allowed to continue to attend school/studies:
21(72.4) 129(54.7) 146(67) 436(69.1) 98(89.1) 830(68.49)
7. I would accept to share the same class at
school/college with someone who is infected
with HIV:
16(55.2) 111(47) 141(64.7) 415(65.8) 93(84.5) 776(60.03)
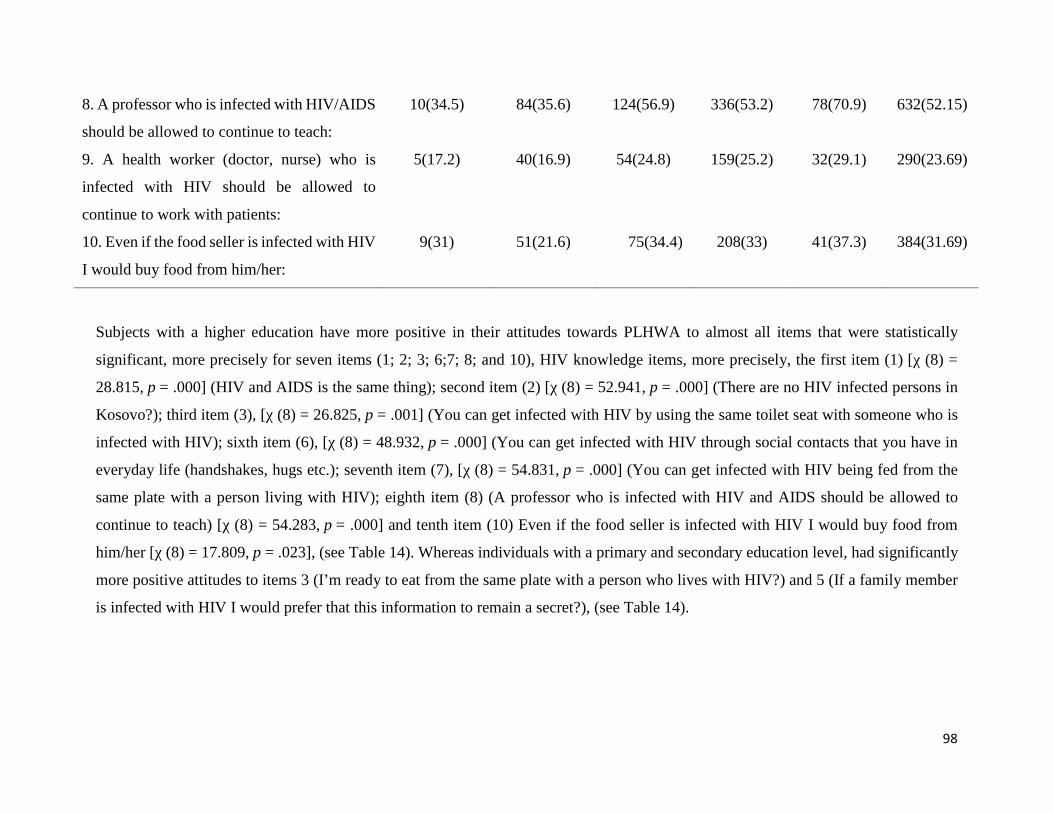
98
8. A professor who is infected with HIV/AIDS
should be allowed to continue to teach:
10(34.5) 84(35.6) 124(56.9) 336(53.2) 78(70.9) 632(52.15)
9. A health worker (doctor, nurse) who is
infected with HIV should be allowed to
continue to work with patients:
5(17.2) 40(16.9) 54(24.8) 159(25.2) 32(29.1) 290(23.69)
10. Even if the food seller is infected with HIV
I would buy food from him/her:
9(31) 51(21.6) 75(34.4) 208(33) 41(37.3) 384(31.69)
Subjects with a higher education have more positive in their attitudes towards PLHWA to almost all items that were statistically
significant, more precisely for seven items (1; 2; 3; 6;7; 8; and 10), HIV knowledge items, more precisely, the first item (1) [χ (8) =
28.815, p = .000] (HIV and AIDS is the same thing); second item (2) [χ (8) = 52.941, p = .000] (There are no HIV infected persons in
Kosovo?); third item (3), [χ (8) = 26.825, p = .001] (You can get infected with HIV by using the same toilet seat with someone who is
infected with HIV); sixth item (6), [χ (8) = 48.932, p = .000] (You can get infected with HIV through social contacts that you have in
everyday life (handshakes, hugs etc.); seventh item (7), [χ (8) = 54.831, p = .000] (You can get infected with HIV being fed from the
same plate with a person living with HIV); eighth item (8) (A professor who is infected with HIV and AIDS should be allowed to
continue to teach) [χ (8) = 54.283, p = .000] and tenth item (10) Even if the food seller is infected with HIV I would buy food from
him/her [χ (8) = 17.809, p = .023], (see Table 14). Whereas individuals with a primary and secondary education level, had significantly
more positive attitudes to items 3 (I’m ready to eat from the same plate with a person who lives with HIV?) and 5 (If a family member
is infected with HIV I would prefer that this information to remain a secret?), (see Table 14).
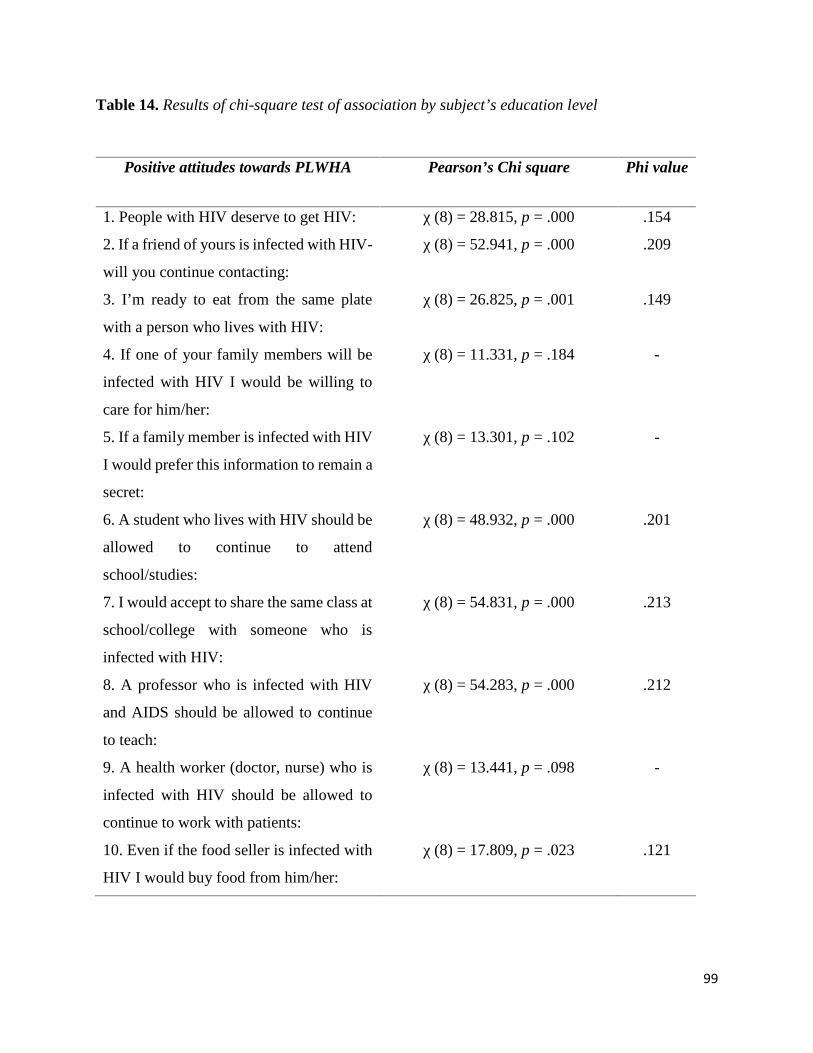
99
Table 14. Results of chi-square test of association by subject’s education level
Positive attitudes towards PLWHA Pearson’s Chi square Phi value
1. People with HIV deserve to get HIV: χ (8) = 28.815, p = .000 .154
2. If a friend of yours is infected with HIV-
will you continue contacting:
χ (8) = 52.941, p = .000 .209
3. I’m ready to eat from the same plate
with a person who lives with HIV:
χ (8) = 26.825, p = .001 .149
4. If one of your family members will be
infected with HIV I would be willing to
care for him/her:
χ (8) = 11.331, p = .184 -
5. If a family member is infected with HIV
I would prefer this information to remain a
secret:
χ (8) = 13.301, p = .102 -
6. A student who lives with HIV should be
allowed to continue to attend
school/studies:
χ (8) = 48.932, p = .000 .201
7. I would accept to share the same class at
school/college with someone who is
infected with HIV:
χ (8) = 54.831, p = .000 .213
8. A professor who is infected with HIV
and AIDS should be allowed to continue
to teach:
χ (8) = 54.283, p = .000 .212
9. A health worker (doctor, nurse) who is
infected with HIV should be allowed to
continue to work with patients:
χ (8) = 13.441, p = .098 -
10. Even if the food seller is infected with
HIV I would buy food from him/her:
χ (8) = 17.809, p = .023 .121
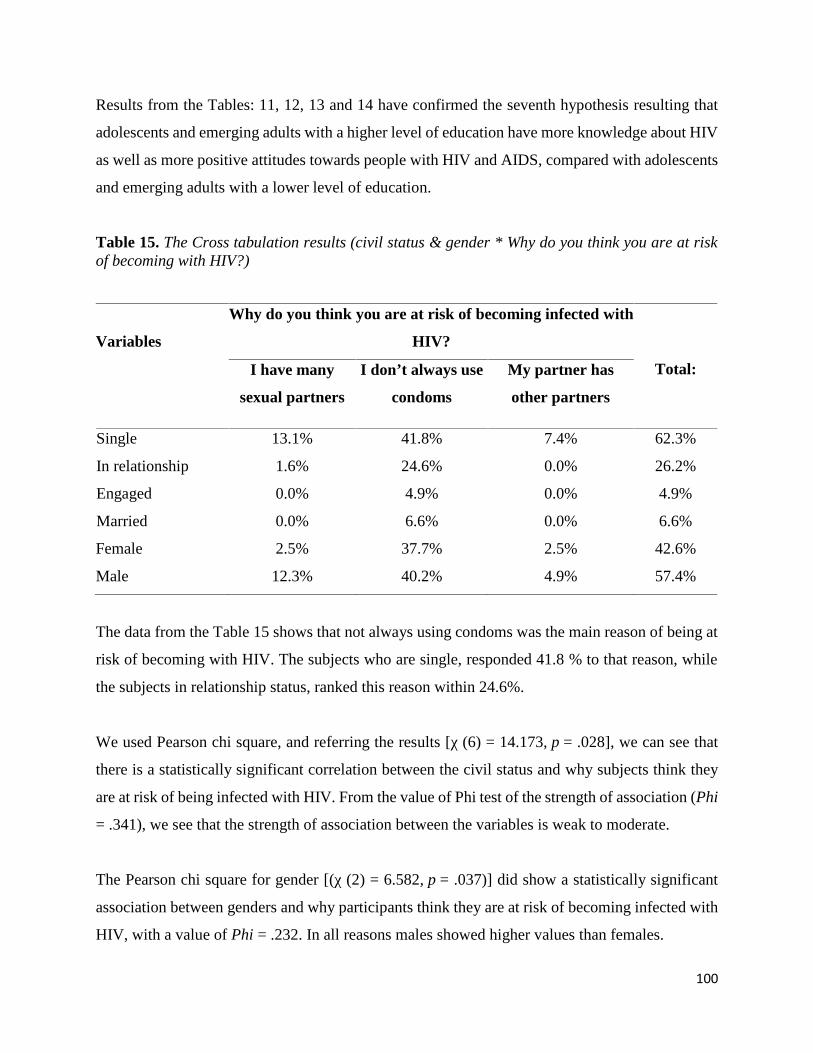
100
Results from the Tables: 11, 12, 13 and 14 have confirmed the seventh hypothesis resulting that
adolescents and emerging adults with a higher level of education have more knowledge about HIV
as well as more positive attitudes towards people with HIV and AIDS, compared with adolescents
and emerging adults with a lower level of education.
Table 15. The Cross tabulation results (civil status & gender * Why do you think you are at riskof becoming with HIV?)
Variables
Why do you think you are at risk of becoming infected with
HIV?
Total:I have many
sexual partners
I don’t always usecondoms
My partner has
other partners
Single 13.1% 41.8% 7.4% 62.3%
In relationship 1.6% 24.6% 0.0% 26.2%
Engaged 0.0% 4.9% 0.0% 4.9%
Married 0.0% 6.6% 0.0% 6.6%
Female 2.5% 37.7% 2.5% 42.6%
Male 12.3% 40.2% 4.9% 57.4%
The data from the Table 15 shows that not always using condoms was the main reason of being at
risk of becoming with HIV. The subjects who are single, responded 41.8 % to that reason, while
the subjects in relationship status, ranked this reason within 24.6%.
We used Pearson chi square, and referring the results [χ (6) = 14.173, p = .028], we can see that
there is a statistically significant correlation between the civil status and why subjects think they
are at risk of being infected with HIV. From the value of Phi test of the strength of association (Phi
= .341), we see that the strength of association between the variables is weak to moderate.
The Pearson chi square for gender [(χ (2) = 6.582, p = .037)] did show a statistically significant
association between genders and why participants think they are at risk of becoming infected with
HIV, with a value of Phi = .232. In all reasons males showed higher values than females.
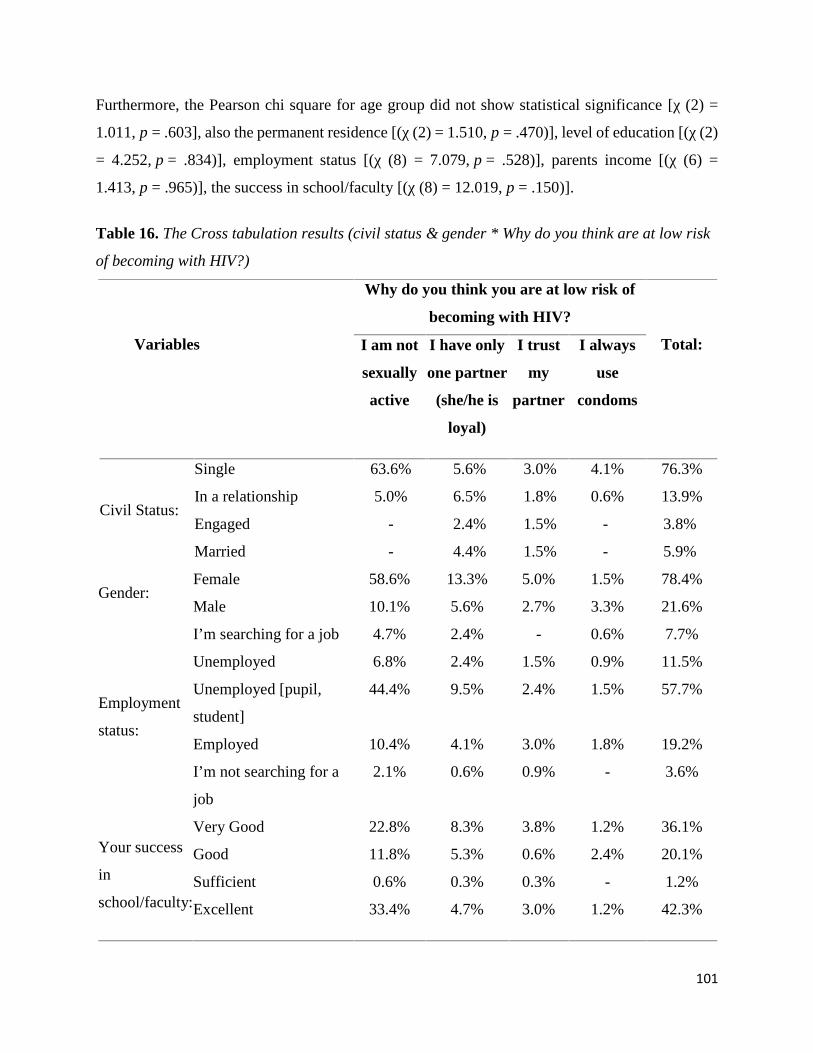
101
Furthermore, the Pearson chi square for age group did not show statistical significance [χ (2) =
1.011, p = .603], also the permanent residence [(χ (2) = 1.510, p = .470)], level of education [(χ (2)
= 4.252, p = .834)], employment status [(χ (8) = 7.079, p = .528)], parents income [(χ (6) =
1.413, p = .965)], the success in school/faculty [(χ (8) = 12.019, p = .150)].
Table 16. The Cross tabulation results (civil status & gender * Why do you think are at low risk
of becoming with HIV?)
Variables
Why do you think you are at low risk of
becoming with HIV?
Total:I am not
sexually
active
I have only
one partner
(she/he is
loyal)
I trust
my
partner
I always
use
condoms
Civil Status:
Single 63.6% 5.6% 3.0% 4.1% 76.3%
In a relationship 5.0% 6.5% 1.8% 0.6% 13.9%
Engaged - 2.4% 1.5% - 3.8%
Married - 4.4% 1.5% - 5.9%
Gender:Female 58.6% 13.3% 5.0% 1.5% 78.4%
Male 10.1% 5.6% 2.7% 3.3% 21.6%
Employment
status:
I’m searching for a job 4.7% 2.4% - 0.6% 7.7%
Unemployed 6.8% 2.4% 1.5% 0.9% 11.5%
Unemployed [pupil,
student]
44.4% 9.5% 2.4% 1.5% 57.7%
Employed 10.4% 4.1% 3.0% 1.8% 19.2%
I’m not searching for a
job
2.1% 0.6% 0.9% - 3.6%
Your success
in
school/faculty:
Very Good 22.8% 8.3% 3.8% 1.2% 36.1%
Good 11.8% 5.3% 0.6% 2.4% 20.1%
Sufficient 0.6% 0.3% 0.3% - 1.2%
Excellent 33.4% 4.7% 3.0% 1.2% 42.3%
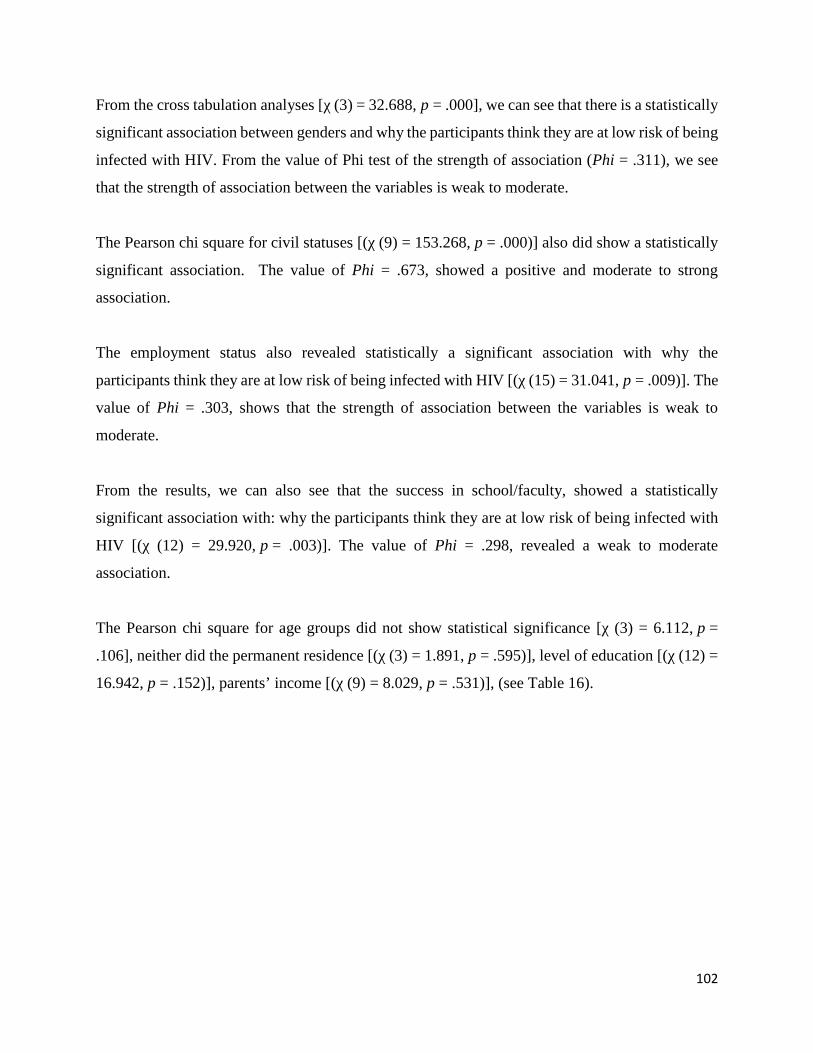
102
From the cross tabulation analyses [χ (3) = 32.688, p = .000], we can see that there is a statistically
significant association between genders and why the participants think they are at low risk of being
infected with HIV. From the value of Phi test of the strength of association (Phi = .311), we see
that the strength of association between the variables is weak to moderate.
The Pearson chi square for civil statuses [(χ (9) = 153.268, p = .000)] also did show a statistically
significant association. The value of Phi = .673, showed a positive and moderate to strong
association.
The employment status also revealed statistically a significant association with why the
participants think they are at low risk of being infected with HIV [(χ (15) = 31.041, p = .009)]. The
value of Phi = .303, shows that the strength of association between the variables is weak to
moderate.
From the results, we can also see that the success in school/faculty, showed a statistically
significant association with: why the participants think they are at low risk of being infected with
HIV [(χ (12) = 29.920, p = .003)]. The value of Phi = .298, revealed a weak to moderate
association.
The Pearson chi square for age groups did not show statistical significance [χ (3) = 6.112, p =
.106], neither did the permanent residence [(χ (3) = 1.891, p = .595)], level of education [(χ (12) =
16.942, p = .152)], parents’ income [(χ (9) = 8.029, p = .531)], (see Table 16).
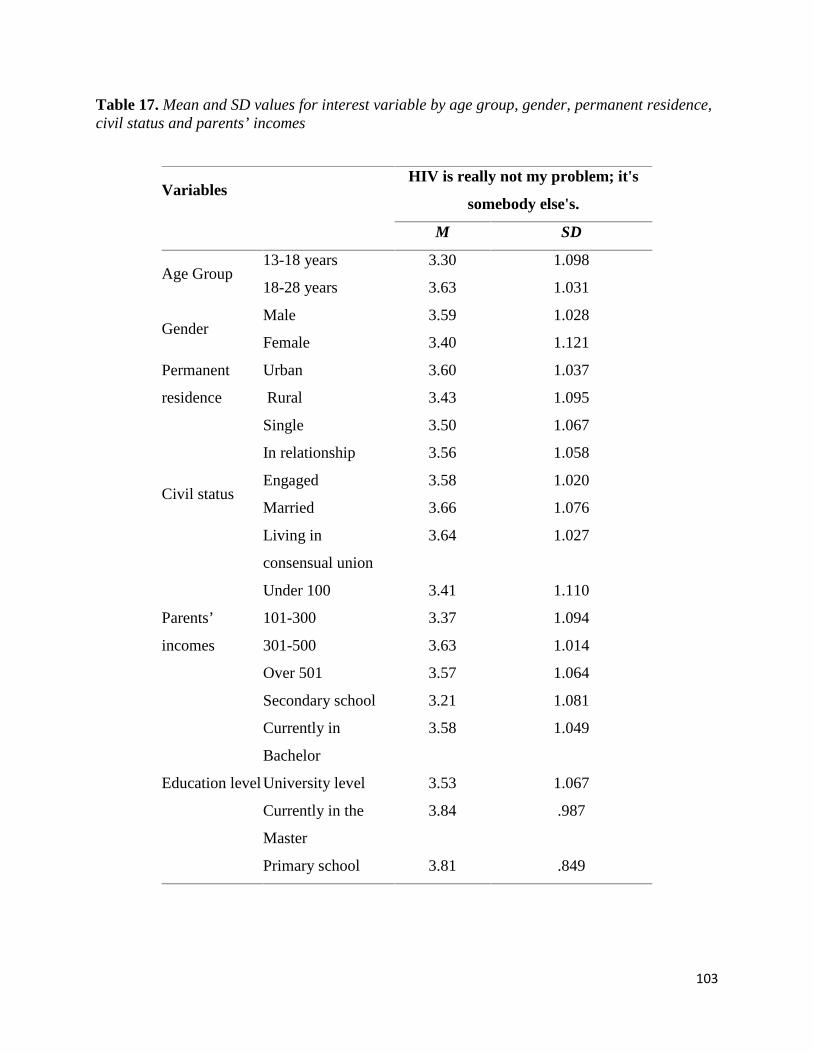
103
Table 17. Mean and SD values for interest variable by age group, gender, permanent residence,civil status and parents’ incomes
VariablesHIV is really not my problem; it's
somebody else's.
M SD
Age Group13-18 years 3.30 1.098
18-28 years 3.63 1.031
GenderMale 3.59 1.028
Female 3.40 1.121
Permanent
residence
Urban 3.60 1.037
Rural 3.43 1.095
Civil status
Single 3.50 1.067
In relationship 3.56 1.058
Engaged 3.58 1.020
Married 3.66 1.076
Living in
consensual union
3.64 1.027
Parents’
incomes
Under 100 3.41 1.110
101-300 3.37 1.094
301-500 3.63 1.014
Over 501 3.57 1.064
Education level
Secondary school 3.21 1.081
Currently in
Bachelor
3.58 1.049
University level 3.53 1.067
Currently in the
Master
3.84 .987
Primary school 3.81 .849
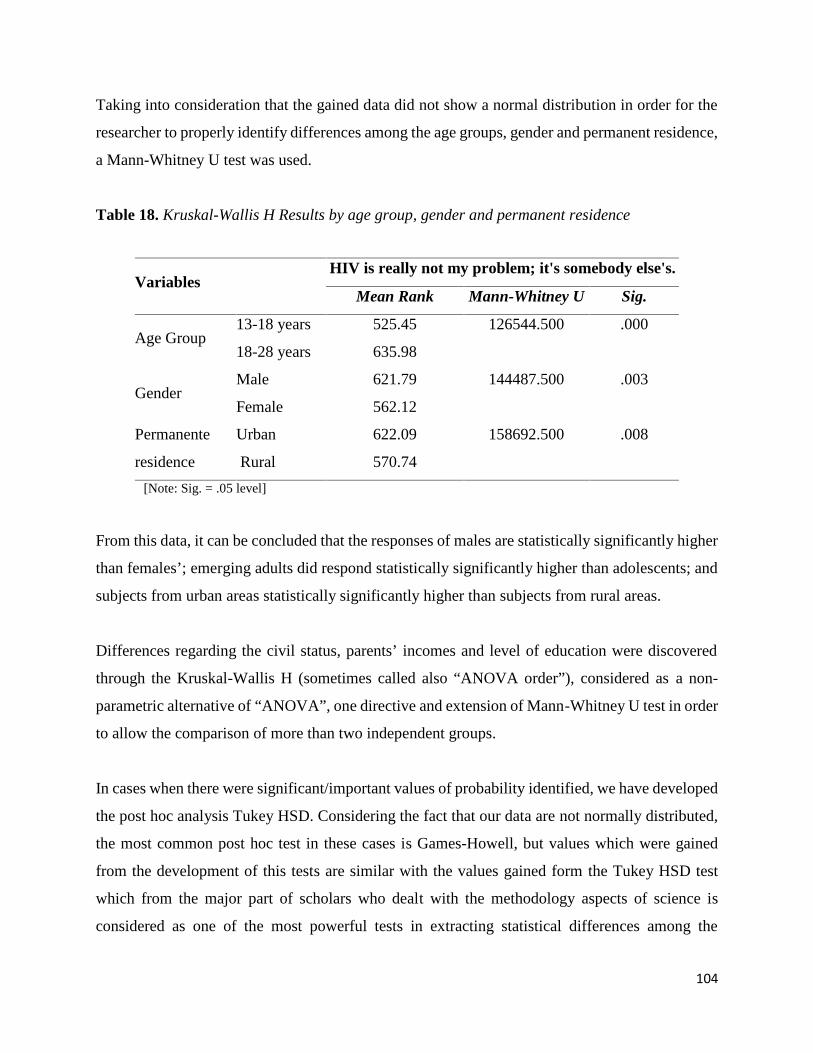
104
Taking into consideration that the gained data did not show a normal distribution in order for the
researcher to properly identify differences among the age groups, gender and permanent residence,
a Mann-Whitney U test was used.
Table 18. Kruskal-Wallis H Results by age group, gender and permanent residence
VariablesHIV is really not my problem; it's somebody else's.
Mean Rank Mann-Whitney U Sig.
Age Group13-18 years 525.45 126544.500 .000
18-28 years 635.98
GenderMale 621.79 144487.500 .003
Female 562.12
Permanente
residence
Urban 622.09 158692.500 .008
Rural 570.74
[Note: Sig. = .05 level]
From this data, it can be concluded that the responses of males are statistically significantly higher
than females’; emerging adults did respond statistically significantly higher than adolescents; and
subjects from urban areas statistically significantly higher than subjects from rural areas.
Differences regarding the civil status, parents’ incomes and level of education were discovered
through the Kruskal-Wallis H (sometimes called also “ANOVA order”), considered as a non-
parametric alternative of “ANOVA”, one directive and extension of Mann-Whitney U test in order
to allow the comparison of more than two independent groups.
In cases when there were significant/important values of probability identified, we have developed
the post hoc analysis Tukey HSD. Considering the fact that our data are not normally distributed,
the most common post hoc test in these cases is Games-Howell, but values which were gained
from the development of this tests are similar with the values gained form the Tukey HSD test
which from the major part of scholars who dealt with the methodology aspects of science is
considered as one of the most powerful tests in extracting statistical differences among the
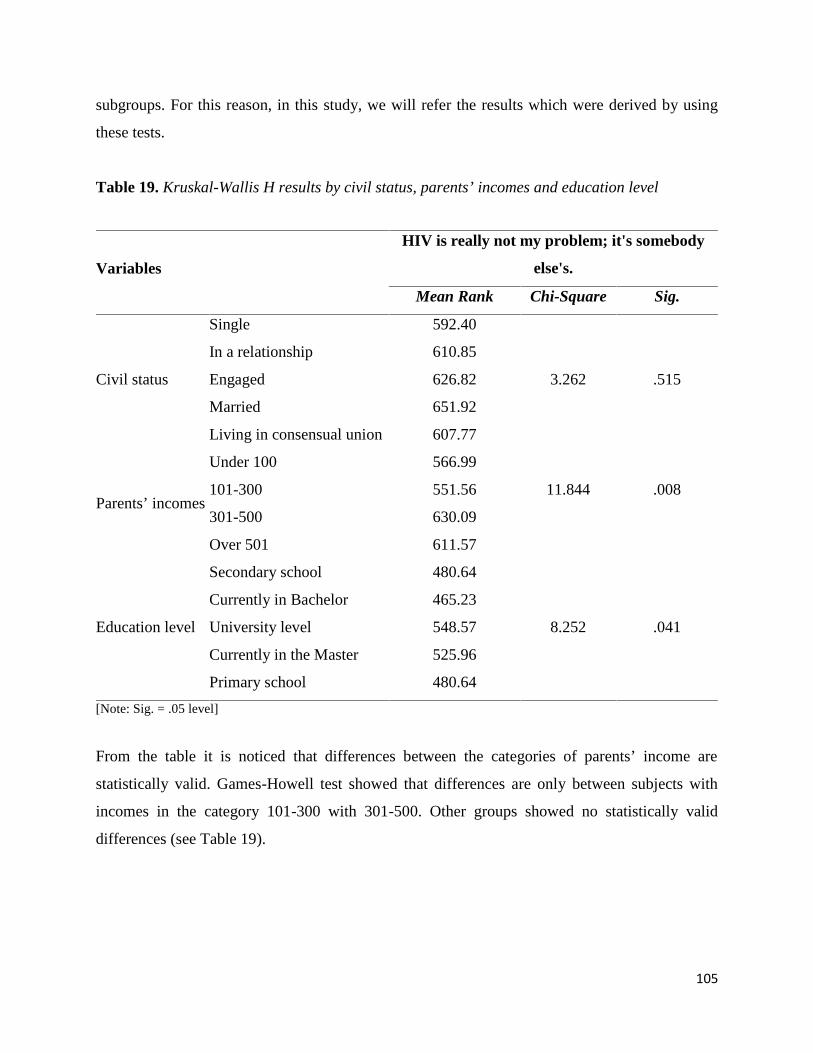
105
subgroups. For this reason, in this study, we will refer the results which were derived by using
these tests.
Table 19. Kruskal-Wallis H results by civil status, parents’ incomes and education level
Variables
HIV is really not my problem; it's somebody
else's.
Mean Rank Chi-Square Sig.
Civil status
Single 592.40
3.262 .515
In a relationship 610.85
Engaged 626.82
Married 651.92
Living in consensual union 607.77
Parents’ incomes
Under 100 566.99
11.844 .008101-300 551.56
301-500 630.09
Over 501 611.57
Education level
Secondary school 480.64
8.252 .041
Currently in Bachelor 465.23
University level 548.57
Currently in the Master 525.96
Primary school 480.64
[Note: Sig. = .05 level]
From the table it is noticed that differences between the categories of parents’ income are
statistically valid. Games-Howell test showed that differences are only between subjects with
incomes in the category 101-300 with 301-500. Other groups showed no statistically valid
differences (see Table 19).
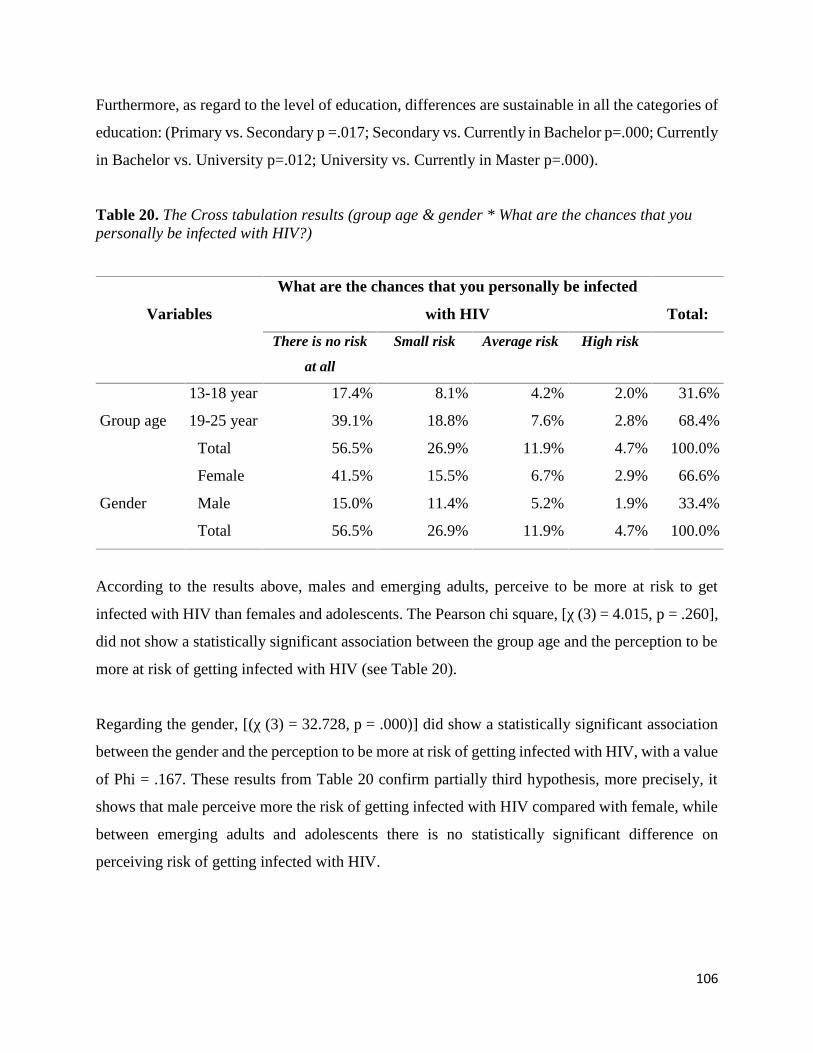
106
Furthermore, as regard to the level of education, differences are sustainable in all the categories of
education: (Primary vs. Secondary p =.017; Secondary vs. Currently in Bachelor p=.000; Currently
in Bachelor vs. University p=.012; University vs. Currently in Master p=.000).
Table 20. The Cross tabulation results (group age & gender * What are the chances that youpersonally be infected with HIV?)
Variables
What are the chances that you personally be infected
with HIV Total:
There is no risk
at all
Small risk Average risk High risk
Group age
13-18 year 17.4% 8.1% 4.2% 2.0% 31.6%
19-25 year 39.1% 18.8% 7.6% 2.8% 68.4%
Total 56.5% 26.9% 11.9% 4.7% 100.0%
Gender
Female 41.5% 15.5% 6.7% 2.9% 66.6%
Male 15.0% 11.4% 5.2% 1.9% 33.4%
Total 56.5% 26.9% 11.9% 4.7% 100.0%
According to the results above, males and emerging adults, perceive to be more at risk to get
infected with HIV than females and adolescents. The Pearson chi square, [χ (3) = 4.015, p = .260],
did not show a statistically significant association between the group age and the perception to be
more at risk of getting infected with HIV (see Table 20).
Regarding the gender, [(χ (3) = 32.728, p = .000)] did show a statistically significant association
between the gender and the perception to be more at risk of getting infected with HIV, with a value
of Phi = .167. These results from Table 20 confirm partially third hypothesis, more precisely, it
shows that male perceive more the risk of getting infected with HIV compared with female, while
between emerging adults and adolescents there is no statistically significant difference on
perceiving risk of getting infected with HIV.
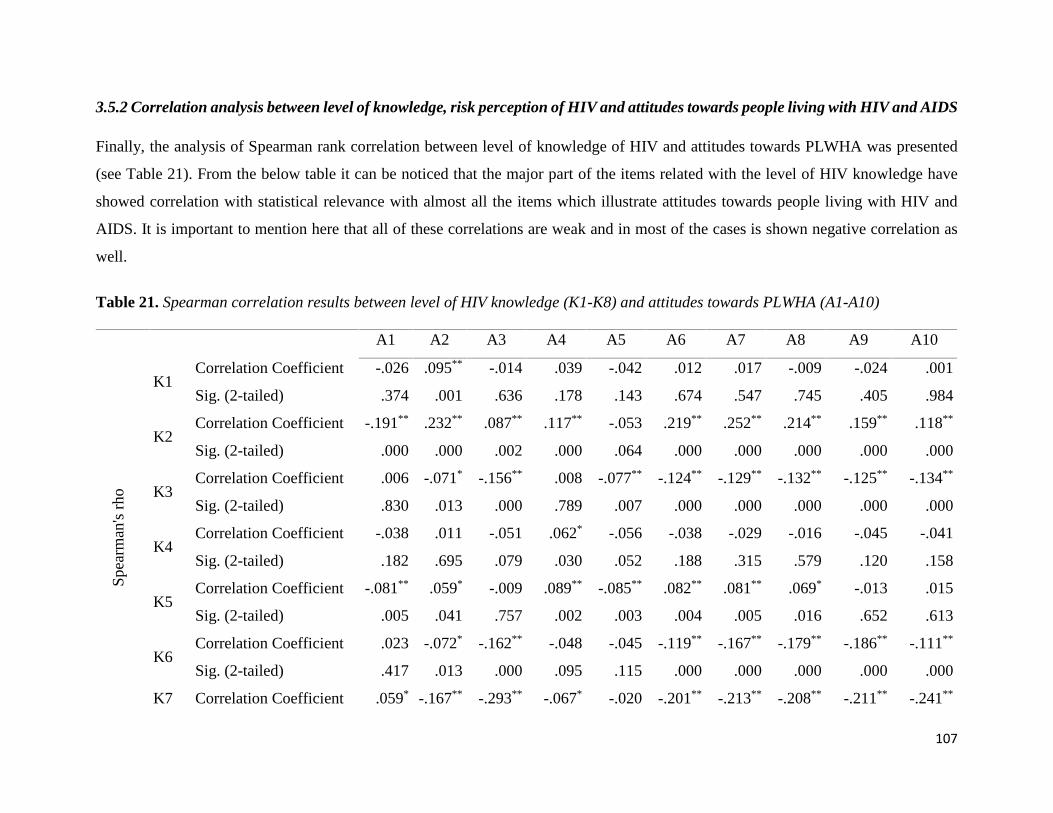
107
3.5.2 Correlation analysis between level of knowledge, risk perception of HIV and attitudes towards people living with HIV and AIDS
Finally, the analysis of Spearman rank correlation between level of knowledge of HIV and attitudes towards PLWHA was presented
(see Table 21). From the below table it can be noticed that the major part of the items related with the level of HIV knowledge have
showed correlation with statistical relevance with almost all the items which illustrate attitudes towards people living with HIV and
AIDS. It is important to mention here that all of these correlations are weak and in most of the cases is shown negative correlation as
well.
Table 21. Spearman correlation results between level of HIV knowledge (K1-K8) and attitudes towards PLWHA (A1-A10)
A1 A2 A3 A4 A5 A6 A7 A8 A9 A10
Spe
arm
an's
rho
K1Correlation Coefficient -.026 .095** -.014 .039 -.042 .012 .017 -.009 -.024 .001
Sig. (2-tailed) .374 .001 .636 .178 .143 .674 .547 .745 .405 .984
K2Correlation Coefficient -.191** .232** .087** .117** -.053 .219** .252** .214** .159** .118**
Sig. (2-tailed) .000 .000 .002 .000 .064 .000 .000 .000 .000 .000
K3Correlation Coefficient .006 -.071* -.156** .008 -.077** -.124** -.129** -.132** -.125** -.134**
Sig. (2-tailed) .830 .013 .000 .789 .007 .000 .000 .000 .000 .000
K4Correlation Coefficient -.038 .011 -.051 .062* -.056 -.038 -.029 -.016 -.045 -.041
Sig. (2-tailed) .182 .695 .079 .030 .052 .188 .315 .579 .120 .158
K5Correlation Coefficient -.081** .059* -.009 .089** -.085** .082** .081** .069* -.013 .015
Sig. (2-tailed) .005 .041 .757 .002 .003 .004 .005 .016 .652 .613
K6Correlation Coefficient .023 -.072* -.162** -.048 -.045 -.119** -.167** -.179** -.186** -.111**
Sig. (2-tailed) .417 .013 .000 .095 .115 .000 .000 .000 .000 .000
K7 Correlation Coefficient .059* -.167** -.293** -.067* -.020 -.201** -.213** -.208** -.211** -.241**
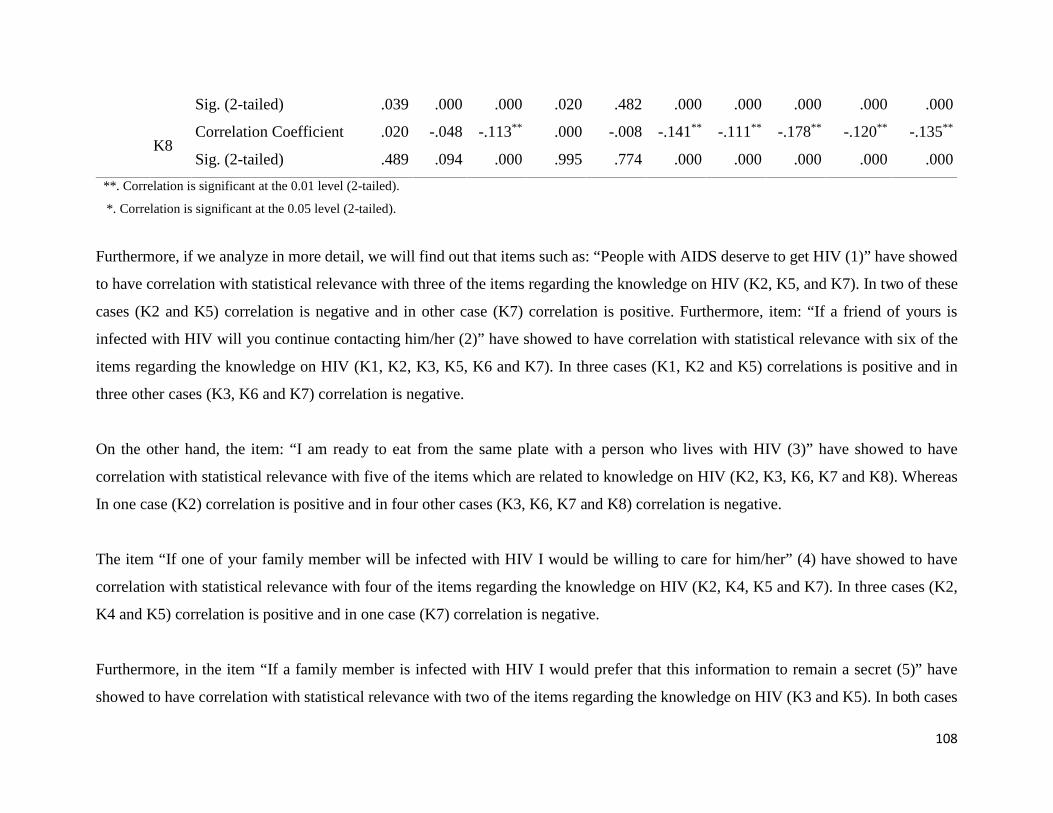
108
Sig. (2-tailed) .039 .000 .000 .020 .482 .000 .000 .000 .000 .000
K8Correlation Coefficient .020 -.048 -.113** .000 -.008 -.141** -.111** -.178** -.120** -.135**
Sig. (2-tailed) .489 .094 .000 .995 .774 .000 .000 .000 .000 .000
**. Correlation is significant at the 0.01 level (2-tailed).
*. Correlation is significant at the 0.05 level (2-tailed).
Furthermore, if we analyze in more detail, we will find out that items such as: “People with AIDS deserve to get HIV (1)” have showed
to have correlation with statistical relevance with three of the items regarding the knowledge on HIV (K2, K5, and K7). In two of these
cases (K2 and K5) correlation is negative and in other case (K7) correlation is positive. Furthermore, item: “If a friend of yours is
infected with HIV will you continue contacting him/her (2)” have showed to have correlation with statistical relevance with six of the
items regarding the knowledge on HIV (K1, K2, K3, K5, K6 and K7). In three cases (K1, K2 and K5) correlations is positive and in
three other cases (K3, K6 and K7) correlation is negative.
On the other hand, the item: “I am ready to eat from the same plate with a person who lives with HIV (3)” have showed to have
correlation with statistical relevance with five of the items which are related to knowledge on HIV (K2, K3, K6, K7 and K8). Whereas
In one case (K2) correlation is positive and in four other cases (K3, K6, K7 and K8) correlation is negative.
The item “If one of your family member will be infected with HIV I would be willing to care for him/her” (4) have showed to have
correlation with statistical relevance with four of the items regarding the knowledge on HIV (K2, K4, K5 and K7). In three cases (K2,
K4 and K5) correlation is positive and in one case (K7) correlation is negative.
Furthermore, in the item “If a family member is infected with HIV I would prefer that this information to remain a secret (5)” have
showed to have correlation with statistical relevance with two of the items regarding the knowledge on HIV (K3 and K5). In both cases
109
correlation is negative. Whereas the item: “A student who lives with HIV should be allowed to continue to attend school/studies (6)”
have showed to have correlation with statistical relevance with five of the items regarding the knowledge on HIV (K2, K3, K5, K6, K7
and K8). In two cases (K2 and K5) correlation is positive and in four other cases (K3, K6, K7 and K8) correlation is negative.
Additionally, the item: “I would accept to share the same class at school/college with someone who is infected with HIV (7)” have
showed to have correlation with statistical relevance with five of the items regarding the knowledge on HIV (K2, K3, K5, K6, K7 and
K8). In two cases (K2 and K5) correlation is positive and in four other cases (K3, K6, K7 and K8) correlation is negative. The item: “A
professor who is infected with HIV/AIDS should be allowed to continue to teach (8)” have showed to have correlation with statistical
relevance with five of the items regarding the knowledge on HIV (K2, K3, K6, K7 and K8). In one case (K2) correlation is positive and
in four other cases (K3, K6, K7 and K8) correlation is negative.
The item: “A health worker (doctor, nurse) who is infected with HIV should be allowed to continue to work with patients (9)” have
showed to have correlation with statistical relevance with five of the items regarding the knowledge on HIV (K2, K3, K6, K7 and K8).
In one case (K2) correlation is positive and in four other cases (K3, K6, K7 and K8) correlation is negative. And, the last item: “Even if
the food seller is infected with HIV I would buy food from him/her (10)” have showed to have correlation with statistical relevance with
five of the items regarding the knowledge on HIV (K2, K3, K6, K7 and K8). In one case (K2) correlation is positive and in four other
cases (K3, K6, K7 and K8) correlation is negative (see Table 21). From the Table 21 we can conclude that if the level on knowledge on
HIV and AIDS is increased among the subjects, then, negative attitudes toward people with HIV and AIDS are reduced.
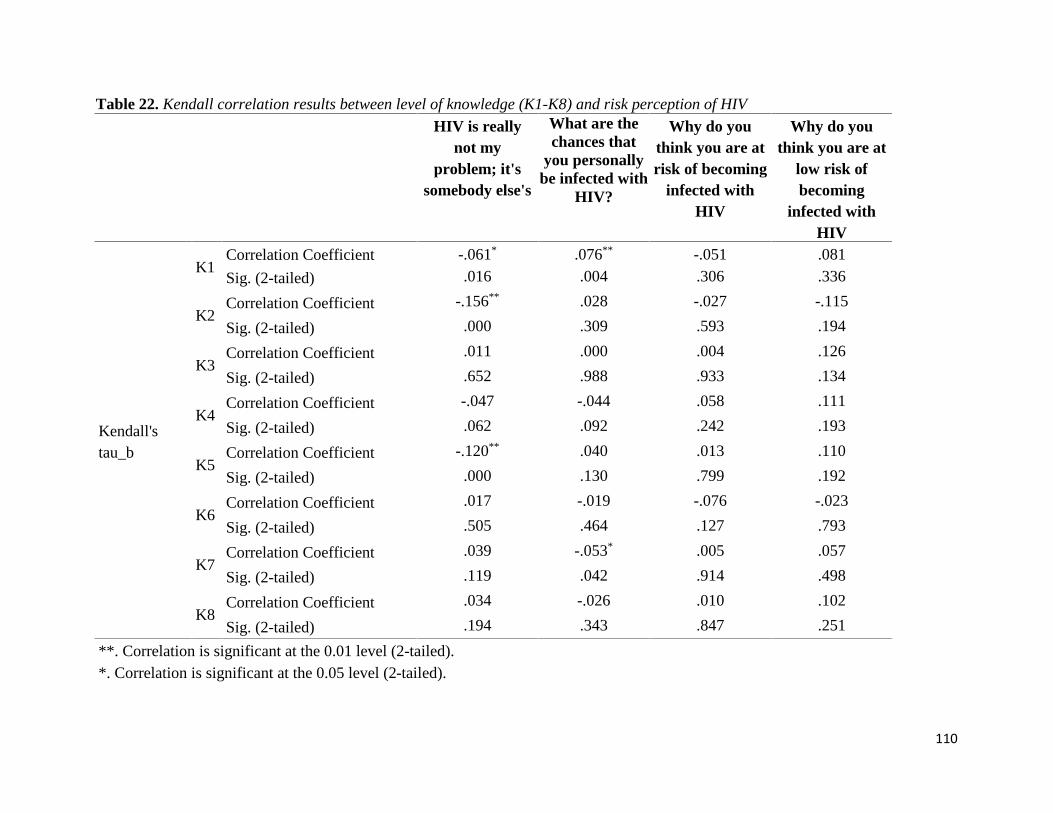
110
Table 22. Kendall correlation results between level of knowledge (K1-K8) and risk perception of HIV
HIV is reallynot my
problem; it'ssomebody else's
What are thechances that
you personallybe infected with
HIV?
Why do youthink you are atrisk of becoming
infected withHIV
Why do youthink you are at
low risk ofbecoming
infected withHIV
Kendall'stau_b
K1Correlation Coefficient -.061* .076** -.051 .081
Sig. (2-tailed) .016 .004 .306 .336
K2Correlation Coefficient -.156** .028 -.027 -.115
Sig. (2-tailed) .000 .309 .593 .194
K3Correlation Coefficient .011 .000 .004 .126
Sig. (2-tailed) .652 .988 .933 .134
K4Correlation Coefficient -.047 -.044 .058 .111
Sig. (2-tailed) .062 .092 .242 .193
K5Correlation Coefficient -.120** .040 .013 .110
Sig. (2-tailed) .000 .130 .799 .192
K6Correlation Coefficient .017 -.019 -.076 -.023
Sig. (2-tailed) .505 .464 .127 .793
K7Correlation Coefficient .039 -.053* .005 .057
Sig. (2-tailed) .119 .042 .914 .498
K8Correlation Coefficient .034 -.026 .010 .102
Sig. (2-tailed) .194 .343 .847 .251
**. Correlation is significant at the 0.01 level (2-tailed).*. Correlation is significant at the 0.05 level (2-tailed).
111
Furthermore, if we analyze in more details, we will find out that items such as: “HIV is really not my problem, it’s somebody else’s”
(1), have showed to have correlation with statistical relevance with three of the items regarding the knowledge on HIV (K1, K2 and
K5). In three cases the correlation is negative, even though weak. Furthermore, the item: “What are the chances that you personally be
infected with HIV” have showed to have correlation with statistical relevance with two of the items regarding the knowledge on HIV
(K1 and K7). In one case (K1 or HIV and AIDS is the same thing) correlation is positive and in other case (K7 or You can get infected
with HIV by being fed from the same plate with a person living with HIV) correlation is negative.
Whereas, two other variables (“Why do you think you are at risk of becoming infected with HIV” and “Why do you think you are at
low risk of becoming infected with HIV”) did not show any correlation with statistical significance.
The results from the Table 23 show a very interesting correlation of attitudes towards people living with HIV and AIDS with the
assumptions that indicate risk perception of HIV. Therefore, item such as: “HIV is really not my problem, it’s somebody else’s”, showed
to have correlation with statistical significance with all the item attitudes (A1-A10). Only two items: “People with AIDS deserve to get
HIV (1)” and “If one of your family member will be infected with HIV I would prefer that this information to remain a secret (5)” have
showed positive correlations with this assumption of risk perception of HIV. All other items have showed negative and very weak
correlations.
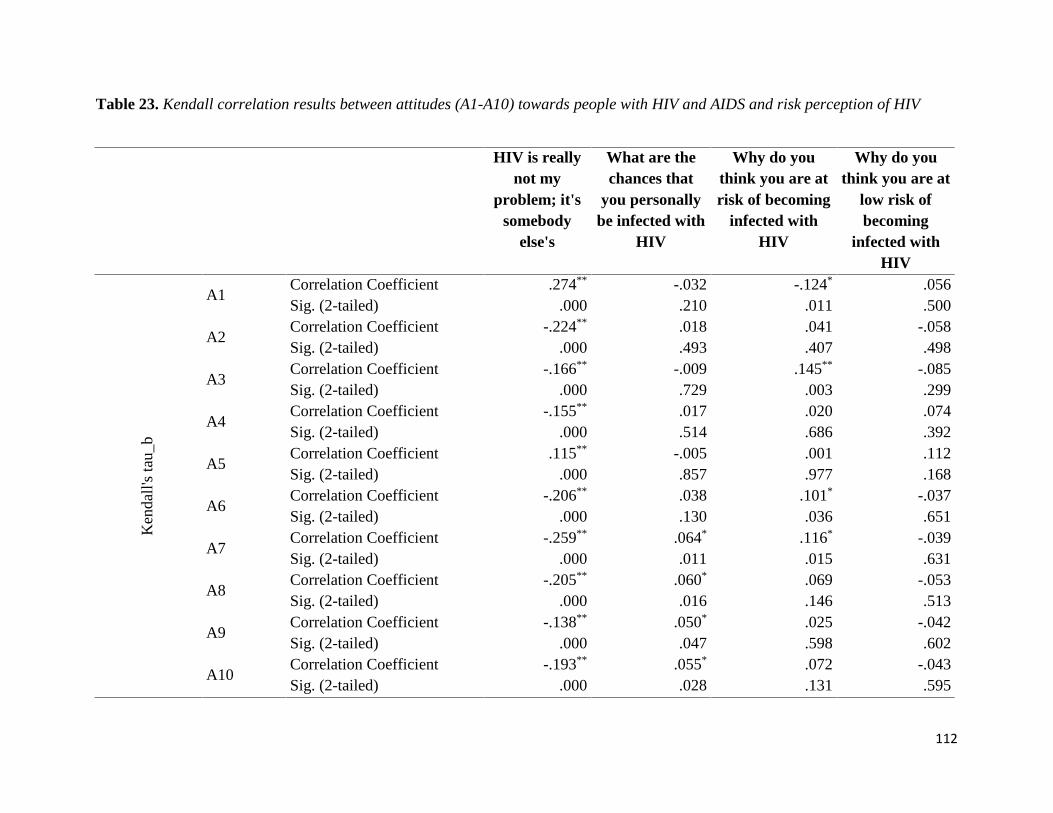
112
Table 23. Kendall correlation results between attitudes (A1-A10) towards people with HIV and AIDS and risk perception of HIV
HIV is reallynot my
problem; it'ssomebody
else's
What are thechances that
you personallybe infected with
HIV
Why do youthink you are atrisk of becoming
infected withHIV
Why do youthink you are at
low risk ofbecoming
infected withHIV
Ken
dall
's ta
u_b
A1Correlation Coefficient .274** -.032 -.124* .056Sig. (2-tailed) .000 .210 .011 .500
A2Correlation Coefficient -.224** .018 .041 -.058Sig. (2-tailed) .000 .493 .407 .498
A3Correlation Coefficient -.166** -.009 .145** -.085Sig. (2-tailed) .000 .729 .003 .299
A4Correlation Coefficient -.155** .017 .020 .074Sig. (2-tailed) .000 .514 .686 .392
A5Correlation Coefficient .115** -.005 .001 .112Sig. (2-tailed) .000 .857 .977 .168
A6Correlation Coefficient -.206** .038 .101* -.037Sig. (2-tailed) .000 .130 .036 .651
A7Correlation Coefficient -.259** .064* .116* -.039Sig. (2-tailed) .000 .011 .015 .631
A8Correlation Coefficient -.205** .060* .069 -.053Sig. (2-tailed) .000 .016 .146 .513
A9Correlation Coefficient -.138** .050* .025 -.042Sig. (2-tailed) .000 .047 .598 .602
A10Correlation Coefficient -.193** .055* .072 -.043Sig. (2-tailed) .000 .028 .131 .595
113
**. Correlation is significant at the 0.01 level (2-tailed).*. Correlation is significant at the 0.05 level (2-tailed).
Whereas, item such as: “What are the chances that you personally be infected with HIV” have showed significant statistical correlations
with four of the item attitudes (A7, A8, A9 and A10). In all of these cases correlations are positive but, it is important to mention that
they are very weak too.
On the other hand, item: “Why do you think you are at risk of becoming infected with HIV” has also showed statistically valid correlation
with four of item attitudes (A1, A3, A6 and A7). More precisely, the correlations is with the item: “People with AIDS deserve to get
HIV” (A1). This correlation is negative, whereas other item attitudes, more precisely A3, A6 and A7, have shown positive correlations
and, what is more important to mention, in all cases correlations are weak. Whereas, none of the item attitudes have not showed statistical
correlation with the assumption: “Why do you think you are at low risk of becoming infected with HIV”.

114
~Chapter Four~Study 2
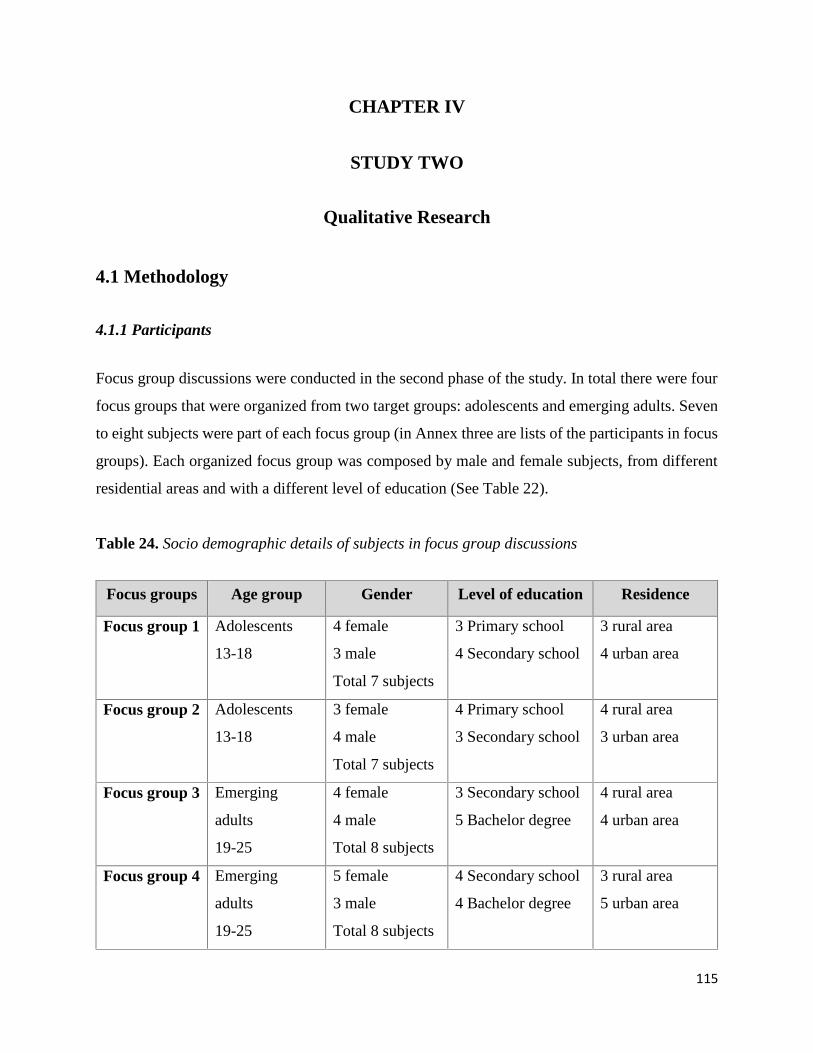
115
CHAPTER IV
STUDY TWO
Qualitative Research
4.1 Methodology
4.1.1 Participants
Focus group discussions were conducted in the second phase of the study. In total there were four
focus groups that were organized from two target groups: adolescents and emerging adults. Seven
to eight subjects were part of each focus group (in Annex three are lists of the participants in focus
groups). Each organized focus group was composed by male and female subjects, from different
residential areas and with a different level of education (See Table 22).
Table 24. Socio demographic details of subjects in focus group discussions
Focus groups Age group Gender Level of education Residence
Focus group 1 Adolescents
13-18
4 female
3 male
Total 7 subjects
3 Primary school
4 Secondary school
3 rural area
4 urban area
Focus group 2 Adolescents
13-18
3 female
4 male
Total 7 subjects
4 Primary school
3 Secondary school
4 rural area
3 urban area
Focus group 3 Emerging
adults
19-25
4 female
4 male
Total 8 subjects
3 Secondary school
5 Bachelor degree
4 rural area
4 urban area
Focus group 4 Emerging
adults
19-25
5 female
3 male
Total 8 subjects
4 Secondary school
4 Bachelor degree
3 rural area
5 urban area
116
4.1.2 Information about focus groups and thematic analysis
Focus groups are a part of qualitative methods for gathering data. This technique is derived from
interviews, but by adding some other specifications which in fact distinguish it from the interviews
are modalities. It is argued scholars that the main difference is that an interview, is usually done
between two persons in one-to-one approach. On the other hand, focus group – as the name
indicates – is done in bigger group of people. Some call it a group interview. Nevertheless, this
does not mean that the focus group is simply a technique when you interview a number of people
together. There are cases in science where a research – in order to save time, money and other
resources – decides to conduct a group interview. However, this is not a focus group but simply a
group interview which contains its unique approaches and techniques in collecting data. In addition
to this, a focus group is a technique which is interested in gathering data that are generated from
the discussion that occurs between participants in the group with the delicate help and guidance of
the facilitator of the group (Matthews & Ross, Research Methods: A Practical Guide for the Social
Sciences, 2010, pp. 234-235).
Even though there are a lot of concepts and ideas, most of the scholars support the idea that in
most of the cases, focus groups consist of five and thirteen participants, without including here the
facilitator who moderates the session and is often the note taker. It is important to underline that
in most cases participants are selected to be part of a particular focus group based on a number of
features. So, everything is intentionally arranged. Participants of the focus group must have
something in common which, one way or another, connect them with the main topic which is
discussed in the session. The duration of the focus group lasts, usually, one to two hours and it is
focused in one core particular topic (Matthews & Ross, Research Methods: A Practical Guide for
the Social Sciences, 2010).
For the purpose of this study, focus groups are seen as one of the appropriate methods in order to
collect data from the target group. This is based on many sound and convincing reasons. When a
research is aiming to collect qualitative data regarding a particular experience, idea and
understanding about a particular issues, and, at the same time, express interest in finding out why
they experience their social world and interaction this way, then a focus group is the appropriate

117
method (Howitt & Cramer, 2007). In this case, the person who facilitates the group is interested in
two main aspects of the process: firstly, in the content of the discussion between the participants
(who is saying what), and also in the form of how the subject is treated by the participants (Frost,
2011).
This way, in most of the cases, focus groups are used by the researches to find out experiences and
understandings about the particular issue. This is done through emphasizing the fact of how people
interact with each other and, at the same time, how they influence one another to construct an
understanding for the topic that is discussed (Matthews & Ross, Research Methods: A Practical
Guide for the Social Sciences, 2010). The focus group as a methodical approach is much more
adequate for this particular research because, unlike to the interviews, the focus group creates the
opportunity for the participants to explore their ideas and opinions and from time to time not to
agree with each other and to challenge opposing ideas. With the assistance of the facilitator, this
creates a good reflecting atmosphere and, as a result, the perception of the group about the topics
emerge more rather than individual opinions as is the case with interviews (Frost, 2011).
There are a lot of reasons why scholars decide to use focus groups in their research activities. Some
use them to develop and/or test constructs as one of the first steps than to develop a questionnaire,
others use them to generate conversations worthy to analyze (Breakwell, Hammond, & Fife-
Schaw, 1994). In this particular case, a focus group is used to support a more traditional approach
such as questionnaires. Here, it provides an interesting comparison of the focus group and
questionnaire responses with regards to the attitudes of adolescents and emerging adults towards
the individuals with HIV and AIDS. The focus group approach in this case demonstrates a
complementary nature for questionnaires with the aim of producing a more complete picture of
the decision-making scenario under the investigation. Another motivation to use this method is to
provide a significantly different perspective on an issue (Breakwell, Hammond, & Fife-Schaw,
1994).
As it is mentioned earlier, there are two methods used in this study: survey conducted through
questionnaire (part of quantitative methods) and focus groups (part of qualitative methods). This
combination in literature is known as triangulation. In other words, it means to use more than one
118
(although not necessarily three) methods of forms of data to investigate the same phenomenon or
problem. This has been done with the idea in mind that using only one method will,
understandably, not cover all the aspects foreseen in studying. For this reason, both these two
methods will cover the gaps and deficiencies of one another. In addition to this, the use of evidence
from different sources, of different methods of collecting data and of different investigators, where
feasible, is all triangulation techniques which enhance credibility (Robson, 1993).
As it mentioned above, the focus group discussions were conducted in the second phase of the
study. The specific aim of this phase of the study was to obtain a better understanding of attitudes
of subjects towards PLWHA as well as their knowledge and risk perception about HIV. Unlike
quantitative data, focus group discussions allow the subjects to share details about their attitudes
towards PLWHA, and explain their level of HIV knowledge and how they perceive risk about
HIV.
The interview protocol was developed based on the literature review findings for the attitudes
towards PLWHA, HIV knowledge and risk perception of HIV and the results of the quantitative
phase of the study. In addition to this, the interview protocol was revised in an interactive process
in response to the early interviews; although it remained substantially unchanged, the ordering of
questions was revised, and additional questions were added.
The interview protocol was divided into three parts (see Annex two):
Questions related to HIV knowledge;
Questions related to attitudes towards PLWHA; and
Questions related to risk perception of HIV.
Thematic analysis was used as a method for the analysis of focus group transcripts. This was done
by using the qualitative software NVivo. According to Braun and Clarke, thematic analysis is a
method for identifying, analyzing and reporting patterns (themes) within data. It minimally
organizes and describes data set in (rich) detail. However, it also often goes further than this and
interprets various aspects of the research topic (Braun & Clarke, 2006). Despite its wide usage,
thematic analysis approach is subject to many criticisms. Likewise, some reason for using thematic
119
analysis are based on its flexibility, ease of use, and as well provision of the rich description of
data sets.
Braun and Clarke (2006) suggested two practical steps that a researcher needs to follow in order
to analyze data properly by using the thematic approach. First, data analysis involved reading and
re-reading each transcript entirely to gain a deeper sense of the data as a whole to immerse
ourselves in the data. They suggested that it is very important for the researcher to read data
actively, which means searching for meaning and patterns in the data and taking notes while
reading (Braun & Clarke, 2006). Second, the initial codes were generated using multiple strategies
to get a better understanding of knowledge, attitudes and risk perception of HIV and AIDS.
Based on the purpose of qualitative analysis, which aimed to get a better understanding from the
subjects regarding their level of knowledge, attitudes towards PLWHA and risk perception of HIV
and AIDS, the first phase of this analysis was focused in the development of codes which were
based on the main objectives of the study. In addition to this, these codes were developed from the
overall data of the qualitative analysis which derived from the experience of the subjects which
were part of the focus groups. The rest of the codes were generated from the overall flow of the
qualitative analysis phase where the main aim was to find out the social and cultural context. As a
final stage was the review and the processing of codes and a detailed analysis in order to know if
the themes are appropriate for the obtained data.
There is a general consensus, however, that qualitative inquirers need to demonstrate that their
studies are credible. To this end, several authors identify common procedures for establishing
validity in qualitative projects (Creswell & Miller, 2000). Therefore, an important aspect of the
qualitative phase of the study is validity and reliability. Validity is considered as a strength of
qualitative research and is used to determine if the findings are correct from the perspective of the
researcher, subjects, or the readers account (Hanson, Creswell, Plano Clark, Petska, & Creswell,
2003). Also, according to Creswell and Miller (2003), several strategies should be implemented to
assure validity: prolonged engagement. Persistent observation, researcher’s flexibility, member
checking, thick description and triangulation (Creswell & Miller, 2000). Therefore, for the purpose
of the trustworthiness of this study, the following procedures have been ensured:
120
Triangulation, which in this study has been guaranteed by the multiple methods
(quantitative data, focus group discussion and literature review);
Triangulation of data sources (adolescents & emerging adults; male & female perspectives
etc.);
Presentation of negative or contrasting evidence regarding specific themes;
As regarding to “member checking” the researcher asked and confirmed with the subjects
if the themes or categories that emerged from data made sense etc.
On the other hand, as for any other methodological approach, scholars have identified a number
of disadvantages of using focus groups to gather data. The criticisms showed below have been
mentioned by scholars who promote qualitative research methods.
On important criticism that is addressed to focus groups as qualitative methodological
approach is that they are not very deep and detailed. Some argue that compared to
individual interviews, focus groups are not as efficient in covering maximum depth on a
particular issue. A particular disadvantage of a focus group is the possibility that the
members may not express their honest and personal opinions about the topic. They may
be hesitant to express their thoughts. This happens especially in cases when their thoughts
oppose the views of another participant (Matthews & Ross, Research methods, 2014).
Another important issue is that in many cases moderators can impact significantly the
outcome of a focus group discussion. They may, intentionally or inadvertently, inject their
personal biases into the participants’ exchange of ideas. This can result in inaccurate
results. Moderators can also lead focus group participants into reaching certain
assumptions or conclusions about an idea or product. Out of fear in going against the
opinion of the moderator, or even out of fear of disappointing the moderator, participants
may not disclose their true and honest opinions (Palomba & Banta, 2001).
Focus groups tend to become influenced by one or two dominant people in the session,
thus making the output very biased. The moderator plays an essential role in handling the
situation, but if the moderator is not experienced enough, it is very easy for the whole
discussion to be dominated by a few people.

121
Focus groups are not very effective in dealing with sensitive topics. It is difficult to have
the participants share their real feelings towards some sensitive topics publicly. This can
in turn influence the output data (Pbworks, 2017).
4.2 Ethical issues
Special attention has been given to the ethical issues for the qualitative part of research. After the
introduction and explanation about the study, the consent form has been read to subjects before
initiating the focus group discussion. Participation in the study was on voluntary bases and subjects
were informed on their right to interrupt and withdraw from the focus group discussions at any
time during the study process. All the data and the research tape recorded from focus group
discussions are confidential and data are secured in safe places.
4.3 Results from the qualitative research (focus groups)
This part of the study was developed for two main aims: first, to deeply analyze socio-cultural
correlations with attitudes towards PLWHA, and level of knowledge and risk perception of HIV
among adolescents and emerging adults. Whereas, the second aim is to get a better understanding
on the subject and to confront these data with the data obtained from the quantitative analysis.
There were four themes identified from the focus groups conducted with two groups, adolescents
and emerging adults. All these themes are associated with respective sub-themes. In this regard,
the main identified theme is knowledge and perception of HIV and AIDS which is associated with
some of the following subthemes: HIV is a virus and AIDS is a syndrome, HIV is present in
Kosovo, misinformation and misconception, not having contact with HIV-infected people, there
are no people with HIV in Kosovo etc. The second theme, ways of transmission of HIV and AIDS,
is associated with the following subthemes: non protected sexual intercourse, injecting drugs with
used needles, handshake, hugs, eating form same plate. The third identified subtheme is prevention
of HIV and AIDS. This is associated with the following subthemes: one sexual partner, abstaining
from sexual relations, having a small number of sexual partners, avoiding contact (also social
contact) with people with HIV etc. Whereas, the fourth identified theme is: risk perception of HIV
122
and AIDS which is associated with these subthemes: not sexually active, having one sexual
partner, trusting your partner, having many partners, not using condoms, etc.
4.3.1 Knowledge and perception of HIV and AIDS
If analyzed closely, it can be noticed that the main themes derived from the focus groups is
knowledge and perception of HIV and AIDS. All other themes are interrelated and derive from
this theme. The qualitative analysis found that female and male participants form the both targeted
groups have sufficient knowledge regarding HIV and AIDS. Female participants in focus group
discussions were more informed compared to male participants. Whereas, adolescents had less
knowledge compared to the emerging adults. As regard to the permanent residency, those who
were from urban areas had more information regarding HIV compared with those who come from
rural areas.
However, it is important to mention that subjects are misinformed about HIV and at other times
are very superficial; a situation that creates misperception. What is more important, the study found
out that the main information that they had regarding HIV came from TV, internet, social media
or other electronic sources and not form a reliable and professional source. As one of the female
participant elaborated: “I have never had the opportunity to learn something about HIV and AIDS
in school. Not even from my family or parents. All the information I have regarding this disease I
have received from television and the internet [S1, FG2]”. It is important to mention that the level
of knowledge regarding HIV and AIDS among the emerging adults is higher compared to
adolescents. On the other hand, female subjects were much more informed about HIV compared
to male subjects.
One of the most confusing questions for the subjects was to know if HIV and AIDS are the same
thing or are two different things. Important to mention that emerging adults were more informed
in this regard, nevertheless even among them there was identified a lack of accurate knowledge.
A male adolescent declared that: “I don’t know. I don’t have enough information to make an
accurate difference between HIV and AIDS. They always seem to be the same thing to me.
However, now I have my doubts since you are asking this particular information. Nevertheless, if
123
I have to answer, I would say that yes – they are the same thing [S1, FG1]”. On the other hand, a
female emerging adult regarding the same question answered as follow: “No, HIV and AIDS are
not the same thing. HIV is the virus, whereas AIDS is the syndrome [S5, FG1]”.
None of the subjects from both the targeted groups participating in the focus groups had the
opportunity to personally know someone who is infected with HIV or someone who has died from
HIV. Nevertheless, some of them had the opportunity to know celebrities who are infected or who
died from HIV. As it was explained by a male adolescent subject: “Personally no, I don’t know
anyone who is infected or who died from HIV. However, I know that some well-known celebrities
died from it. But these cases happened mostly in the USA, as I can remember. Recently, I heard
that Charlie Sheen, an American actor who is well known for his role in the TV show “Two and a
Half Man”, got infected with HIV. Media reported that this happened due to his dangerous and
uncontrolled lifestyle [S6, FG3]”. In addition to this, an emerging adult subject whose permanent
residence was in a rural area but who is living in an urban area from more than 2 years now, is not
even interested in knowing someone who is infected. As he declared in his own words, “I don’t
know and I don’t want to ever know anyone who is infected. This is a very dangerous disease from
which people die within months. For this reason, I am not even interested to know someone who
is infected. Only the word infection makes me nervous [S3, FG4]”. There were subjects who
thought that the main reason of not knowing anyone who is infected with HIV in Kosovo is due to
the fact that they totally keep their HIV status a secret. This, according to them, happens due to
the stigmatization they can receive from society. As a female adolescent explained, “I believe that
there are HIV-infected persons in Kosovo – this is for sure. However, due to many reasons which
are mostly related to the stigmatization they receive from the society, these individuals in Kosovo
usually don’t declare their HIV status. Therefore, it is very difficult to know if someone is infected
or not. You cannot notice it form the appearance [S4, FG3]”.
Regarding ways of transmission of HIV, there is enough information among the subjects
participating in the focus groups from both the targeted groups – adolescents and emerging adults.
It is important to mention that, most of the participating subjects mentioned sexual intercourse as
the main (sometimes the only) way of transmission. As explained by a female emerging adult,
“What I know is that the main way of transmission of the HIV infection is through sexual
124
intercourse. Therefore, people who have many partners, who don’t use condoms during sex, are
usually exposed to the dangerous of being infected. I remember when once some representatives
from an organization were at my school explaining the role and the importance of condoms. Their
slogan was ‘make love, not AIDS’. Therefore, I understood that the main way to transmit this
infection is through unprotected sex. There are other ways too, but sexual intercourse is the more
common way of transmission [S2, FG1]”. What is more, there were subjects who considered that
only homosexuals are the ones who, through sexual intercourse, constitute the main way of HIV
transmission. A male subject declared that: “If you have sex with homosexuals you can get
infected. Usually they are the people who are infected in large numbers due to their lifestyle. They
tend to have many partners therefore they become infected [S1, FG4]”. This lack of information
was accompanied, in many cases, with misinformation where a simple meeting or just a handshake
with someone who is infected with HIV was considered as a route for transmitting the infection.
In this regard, a female subject from the adolescent group said that: “I am not sure about the ways
of transmission, but what I am sure of is I would not prefer to have contact with infected persons.
These kind of diseases can be transmitted even through physical contacts like touching, hugging
or by merely staying close to someone [S3, FG2]”.
On the other hand, subjects were asked on how HIV is not transmitted. In this regard, a male
subject from the group of adolescents declared that: “HIV cannot be transmitted if you don’t have
contact with infected people at all. That’s the only and the best way to protect yourself from the
infection [S7, FG4]”. Whereas, a female subject form the emerging adult group said that: “HIV
and AIDS are not transmitted though the everyday contacts that we have with the people such as:
normal conversations, hugs, handshake etc. Or even working and living with HIV persons in the
same house [S3, FG3]”. Almost all other subject participating in the focus groups declared that
HIV is not transmitted through the everyday contacts with a person infected with HIV.
As regard to the question of how subjects participating in the focus groups can notice that someone
is infected with HIV, most of them from both the targeted groups identified symptoms which are
similar to other usual diseases. Since all of them declared that they did not have the opportunity to
meet with someone who is actually infected, then it was expected that they will not be able to
clearly describe symptoms of infected individual. “Since I have never seen someone who is
125
infected with HIV, I cannot give a definitive answer on how they look like. This is logical.
Nevertheless, I can assume that since this is a disease they look like sick persons do. However, I
cannot say for sure which the definitive symptoms are” [S5, FG1], declared a female from the
adolescent group. Whereas, on the other hand, a male subject form the emerging adults group said
that: “Most of the people infected with HIV usually have some symptoms that are similar to those
of a normal flu, influenza. Some common symptoms are fever, cough, body aches etc.” [S3, FG4].
However, some subject participants there, showed to have a deeper understanding on the topic
and, as a result, their answer has been more accurate. In this context, a female subject participant
form the emerging adults acknowledged that “I cannot identify someone who is infected with HIV.
At least not from the outer appearance. They need to do their medical analysis or HIV test and
through them only, a doctor can identify their HIV status”. On the other hand, she continued that,
“It also depends if they are receiving treatment or no. If yes, then it is impossible to identify. If
not, then you can see that a person is not well as regard to his/her health issues. However, you
cannot say for sure that he or she is infected by HIV” [S6, FG3].
Since most of the subjects from both targeted groups declared that sexual intercourse is the most
common way of HIV infection, that one of the most popular preventive measures to get infected
has been the usage of condoms during sexual intercourse. Some of these measures, as explained
by a male adolescent from a rural area, are: “There are many ways on how to prevent HIV
infection. Some of them are: using condoms during sexual intercourse; being loyal to your sexual
partner; not using intravenous drug injections; not having many partners; etc.” [S5, FG4]. On the
other side, there has been a more radical opinion as well. One of the male subjects believes that
“The only safe way to prevent HIV infection is to avoid meeting them” [S1, FG1].
Table 25. Codes and themes derived from the focus group discussions
Codes Issues discussed Themes
HIV is virus and AIDS is
syndrome
Having sufficient information on the
virus and disease;
Knowing the differences between HIV
and AIDS;
Knowledge and
perception of HIV and
AIDSHIV is present in
Kosovo
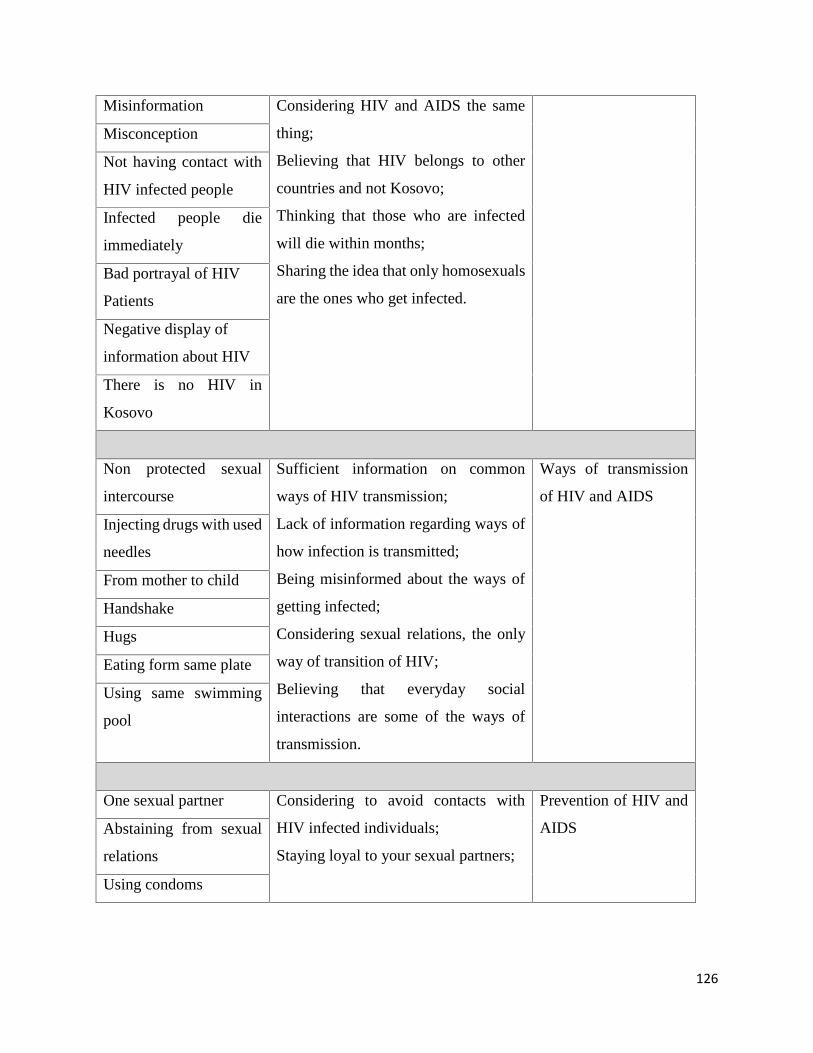
126
Misinformation Considering HIV and AIDS the same
thing;
Believing that HIV belongs to other
countries and not Kosovo;
Thinking that those who are infected
will die within months;
Sharing the idea that only homosexuals
are the ones who get infected.
Misconception
Not having contact with
HIV infected people
Infected people die
immediately
Bad portrayal of HIV
Patients
Negative display of
information about HIV
There is no HIV in
Kosovo
Non protected sexual
intercourse
Sufficient information on common
ways of HIV transmission;
Lack of information regarding ways of
how infection is transmitted;
Being misinformed about the ways of
getting infected;
Considering sexual relations, the only
way of transition of HIV;
Believing that everyday social
interactions are some of the ways of
transmission.
Ways of transmission
of HIV and AIDS
Injecting drugs with used
needles
From mother to child
Handshake
Hugs
Eating form same plate
Using same swimming
pool
One sexual partner Considering to avoid contacts with
HIV infected individuals;
Staying loyal to your sexual partners;
Prevention of HIV and
AIDSAbstaining from sexual
relations
Using condoms
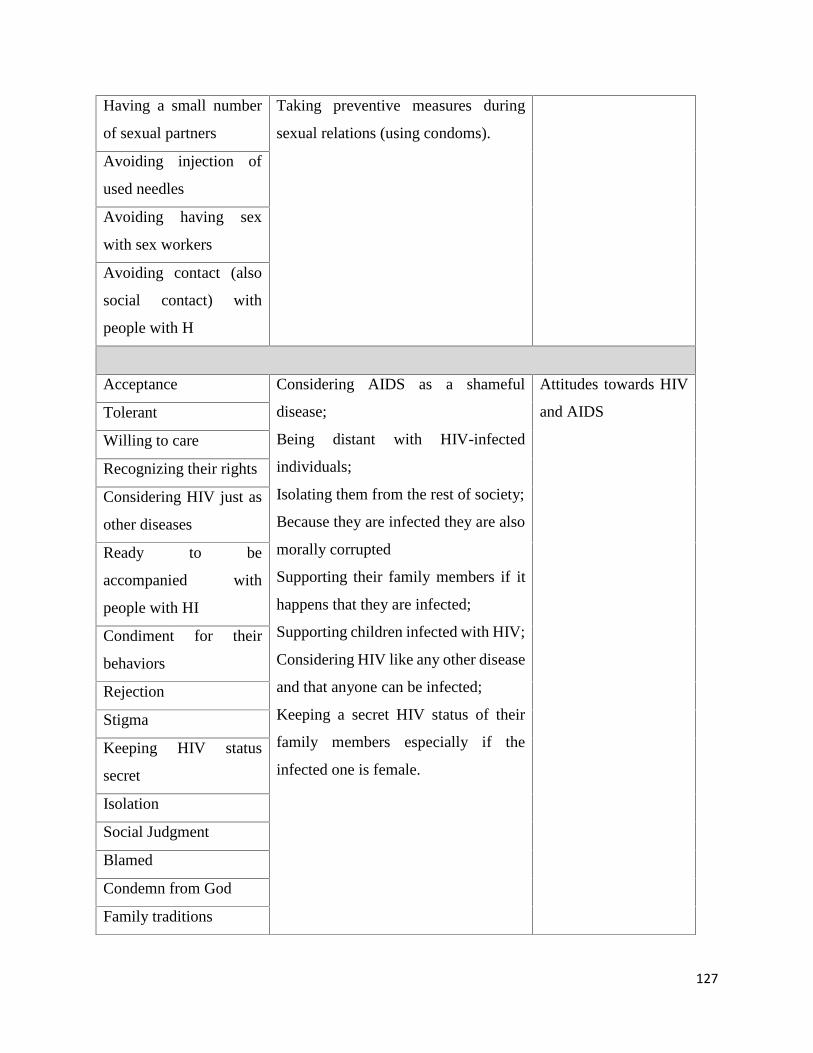
127
Having a small number
of sexual partners
Taking preventive measures during
sexual relations (using condoms).
Avoiding injection of
used needles
Avoiding having sex
with sex workers
Avoiding contact (also
social contact) with
people with H
Acceptance Considering AIDS as a shameful
disease;
Being distant with HIV-infected
individuals;
Isolating them from the rest of society;
Because they are infected they are also
morally corrupted
Supporting their family members if it
happens that they are infected;
Supporting children infected with HIV;
Considering HIV like any other disease
and that anyone can be infected;
Keeping a secret HIV status of their
family members especially if the
infected one is female.
Attitudes towards HIV
and AIDSTolerant
Willing to care
Recognizing their rights
Considering HIV just as
other diseases
Ready to be
accompanied with
people with HI
Condiment for their
behaviors
Rejection
Stigma
Keeping HIV status
secret
Isolation
Social Judgment
Blamed
Condemn from God
Family traditions
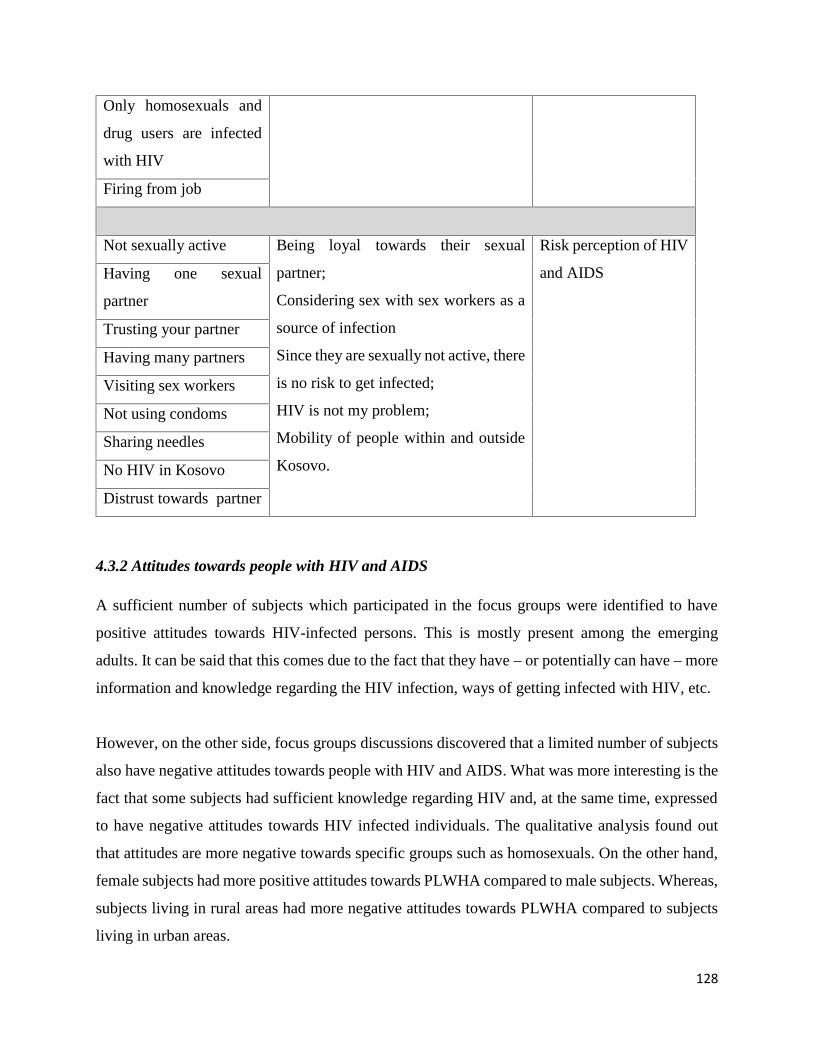
128
Only homosexuals and
drug users are infected
with HIV
Firing from job
Not sexually active Being loyal towards their sexual
partner;
Considering sex with sex workers as a
source of infection
Since they are sexually not active, there
is no risk to get infected;
HIV is not my problem;
Mobility of people within and outside
Kosovo.
Risk perception of HIV
and AIDSHaving one sexual
partner
Trusting your partner
Having many partners
Visiting sex workers
Not using condoms
Sharing needles
No HIV in Kosovo
Distrust towards partner
4.3.2 Attitudes towards people with HIV and AIDS
A sufficient number of subjects which participated in the focus groups were identified to have
positive attitudes towards HIV-infected persons. This is mostly present among the emerging
adults. It can be said that this comes due to the fact that they have – or potentially can have – more
information and knowledge regarding the HIV infection, ways of getting infected with HIV, etc.
However, on the other side, focus groups discussions discovered that a limited number of subjects
also have negative attitudes towards people with HIV and AIDS. What was more interesting is the
fact that some subjects had sufficient knowledge regarding HIV and, at the same time, expressed
to have negative attitudes towards HIV infected individuals. The qualitative analysis found out
that attitudes are more negative towards specific groups such as homosexuals. On the other hand,
female subjects had more positive attitudes towards PLWHA compared to male subjects. Whereas,
subjects living in rural areas had more negative attitudes towards PLWHA compared to subjects
living in urban areas.
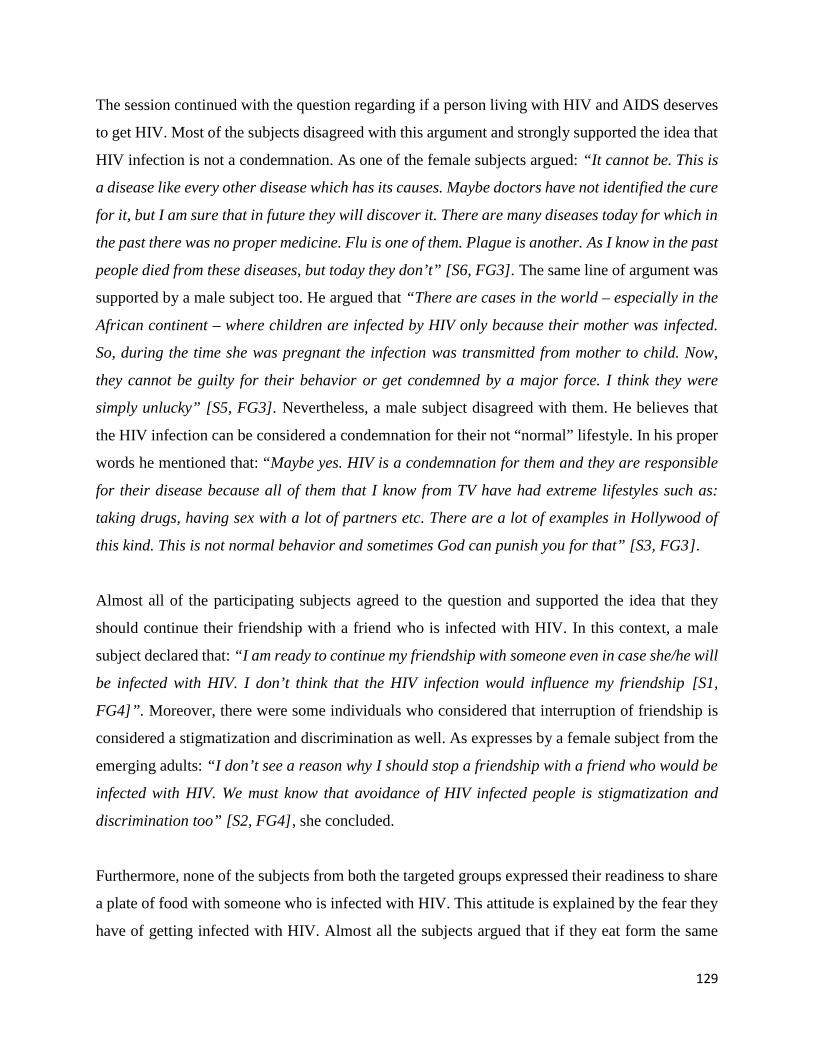
129
The session continued with the question regarding if a person living with HIV and AIDS deserves
to get HIV. Most of the subjects disagreed with this argument and strongly supported the idea that
HIV infection is not a condemnation. As one of the female subjects argued: “It cannot be. This is
a disease like every other disease which has its causes. Maybe doctors have not identified the cure
for it, but I am sure that in future they will discover it. There are many diseases today for which in
the past there was no proper medicine. Flu is one of them. Plague is another. As I know in the past
people died from these diseases, but today they don’t” [S6, FG3]. The same line of argument was
supported by a male subject too. He argued that “There are cases in the world – especially in the
African continent – where children are infected by HIV only because their mother was infected.
So, during the time she was pregnant the infection was transmitted from mother to child. Now,
they cannot be guilty for their behavior or get condemned by a major force. I think they were
simply unlucky” [S5, FG3]. Nevertheless, a male subject disagreed with them. He believes that
the HIV infection can be considered a condemnation for their not “normal” lifestyle. In his proper
words he mentioned that: “Maybe yes. HIV is a condemnation for them and they are responsible
for their disease because all of them that I know from TV have had extreme lifestyles such as:
taking drugs, having sex with a lot of partners etc. There are a lot of examples in Hollywood of
this kind. This is not normal behavior and sometimes God can punish you for that” [S3, FG3].
Almost all of the participating subjects agreed to the question and supported the idea that they
should continue their friendship with a friend who is infected with HIV. In this context, a male
subject declared that: “I am ready to continue my friendship with someone even in case she/he will
be infected with HIV. I don’t think that the HIV infection would influence my friendship [S1,
FG4]”. Moreover, there were some individuals who considered that interruption of friendship is
considered a stigmatization and discrimination as well. As expresses by a female subject from the
emerging adults: “I don’t see a reason why I should stop a friendship with a friend who would be
infected with HIV. We must know that avoidance of HIV infected people is stigmatization and
discrimination too” [S2, FG4], she concluded.
Furthermore, none of the subjects from both the targeted groups expressed their readiness to share
a plate of food with someone who is infected with HIV. This attitude is explained by the fear they
have of getting infected with HIV. Almost all the subjects argued that if they eat form the same
130
plate with someone who is infected with HIV, they will most probably get infected too. A male
adolescent declared that: “I’m not ready to eat from the same plate together with someone who is
infected with HIV. This seems very dangerous. Only the idea that I am sharing food with someone
who is infected is quite disturbing and concerning at the same time” [S6, FG3] . Other subject,
who even though tried to present themselves more approachable and inclusive as regard to HIV
infected people, nevertheless also declared to refuse to eat from the same plate: “I can sit in the
same table with someone who is infected with HIV, but not eating from the same plate or sharing
any kind of food with them” [S4, FG2], declared a female from the emerging adults group
discussion. She continues her argument by saying that: “I am liberal and open minded person, but
still I am not that brave to eat from the same plate with a HIV infected person”.
Subjects from both targeted groups expressed their readiness to care and support family members
if they would be infected with HIV. This occurs due to the strong relations that average families
have in Kosovo. They tend to support their family members, especially when they are sick or are
old. It is a normal way of living among people in Kosovo that parents live with their children
during their entire life. Values are based on strong families, therefore they expressed their readiness
to help and support them. As a female from adolescents participated in focus group discussions
expressed: “Yes, I would be ready to take care (at any time) for a family member in case anyone
of them would be infected with HIV. The moral responsibility that we have towards them is great;
therefore, we should care for them. If we will not, then who will?” [S3, FG1]. Almost the same
opinion was provided by a male subject from the group of emerging adults: “I would be ready to
take care and support a family member in case anyone of them would be infected with HIV. We
are connected very much with each family member so it is our responsibility to take care whenever
they have a need” [S5, FG4].
On the other hand, it is important to mention that almost all the subjects would prefer that
information regarding the HIV status of their family members remain a secret. This happens due
to prejudices that the society has towards HIV infected individuals because in most of the cases
the disease is related to sexual intercourse. This argument was mentioned explicitly by subject
participants also. A subject from the emerging adults group declared that: “HIV is associated with
promiscuous behavior. Those who have this disease are not considered very moral people. They
131
are considered homosexuals too. Therefore, we would prefer this information to be secret for the
rest of the people” [S4, FG4]. In addition, a female subject form the adolescents shared almost the
same opinion too by saying that: “The information regarding the HIV status of a family member
should remain secret. This is very important. AIDS is not very usual disease. In most of the cases,
those who are infected have done something bad such as sex with many partners or with
prostitutes. AIDS is not like cancer or other diseases” [S3, FG2].
Furthermore, what is really interesting, a male subject from the group of adolescents correlated the
revealing of information regarding the HIV status of a family member with gender aspects of a
family member. According to him if the infected person is man, there is no problem in revealing
the information regarding HIV status. On the contrary, if the infected person is female then the
information should remain secret. As he explained: “If the family member is man, it would be good
for this information to remain secret, but even if it goes public it is not a huge problem. If it is
woman, then it is a big problem. This is a shameful disease. This would put a bad reputation to the
entire family” [S3, FG2].
Subjects have divided opinions regarding the question if a student who lives with HIV and AIDS
should be allowed to continue to attend school/studies or not. Some of them, mainly emerging
adults, think that they should be allowed to continue their studies because, according to them,
education is part of human rights. “Yes, all the students who are eventually infected with HIV
should be allowed to be part of school and to continue their education freely. Education is part of
human rights, so their right too. They can be infected, but it is physically and psychologically
normal to continue their life. After all they are not a problem for other students or professors, why
they should be expelled?! [S6, FG3], says a male emerging adult with permanent residence in an
urban area. However, a limited number of subjects opposed the idea that an infected student should
be allowed to continue studies. As was elaborated by a female subject from the emerging adults:
“No they should not be allowed. It would be dangerous for other students too. During their studies
they are socially contacted with other students, therefore they would endanger them. In addition,
not all the students would be informed for their HIV status and potentially they can enter in sexual
relationships with them. This would infect them too and spread the disease” [S7, FG4].
132
Related to the previous issue, subjects were asked if a professor who is infected with HIV and
AIDS should be allowed to continue to teach. Similar results were identified with professors as
were identified with students. The major part of the subjects supported the idea, whereas a small
number of them opposed the idea that a HIV infected professor should be allowed to continue
his/her work. A female subject from a group of adolescents form a rural area declared that: “Every
infected professor should be allowed to continue working without problems. None of the duties of
professor is considered as an obstacle for teaching or communicating with students” [S5, FG1] .
On the other hand, a male subject form the emerging adult group thinks that: “being a professor
is a very specific profession which involves a lot of human interaction. Even if they would be
allowed to continue teaching it would be very difficult for them too. I believe that when a person
is sick with this disease, among other things, he or she will not be very psychologically stable to
continue working, and stability is very important for professors” [S3, FG4].
All the subjects agree with the assumption that a health worker (doctor, nurse) who is infected with
HIV should not be allowed to continue to work with patients. They believe that the profession of
health worker (doctor, nurse) is very sensitive and therefore they should not be allowed to work if
they are infected. Almost the same opinions were expressed by adolescents and emerging adults
from rural and urban areas. In this regard, a male subject declared that: “No they should not be
allowed to work. It is very hard to be at the same time a doctor and a patient. During their work
they have to deal with different cases which are sensitive. In addition, you can come to an infection
very easily if you are a medical worker” [S5, FG3]. Almost the same opinions were expressed by
female subjects too. A female adolescent on the other hand explained that in some professions you
can continue working even if you are infected with HIV, but not in medicine. As she stated: “Some
professions, like health workers, are not for people who are infected with HIV. This is sad, but
true. They can work as programmers, writers or translators of books. In other words, they can
work in professions who don’t have physical interactions with other people. I am not saying to
isolate them, but just to create them better environment and opportunities” [S6, FG1] . Whereas a
male subject from emerging adult group had no definitive opinion in this regard. According to him
this is a very sensitive issue and should be treated with careful attention: “It is very hard to have
a clear opinion due to the sensitivity of this issue. The nature of work for medical workers is
sensitive and very delicate because they have to deal directly with people in everyday bases.
133
Therefore, I think that they (medical workers), after identifying that are infected with HIV, should
voluntarily resign from their job and start to search for another job which does not involve having
every day contact with patients” [S5, FG1].
On the question which was addressed to the subjects: “if a food seller is infected with HIV would
you buy food from him/her? “In this regard, a male subject declared that he is “ready to buy food
and other products from a seller who can potentially be infected with HIV”. He continues
explaining his idea by arguing that: “today major parts of the products are covered and concealed,
thus this would not be a serious problem to deal with” [S5, FG3]. On the other hand, a female
adolescent from an urban area declared: “I don’t understand why we should be afraid of a person
who is infected with HIV if he or she sells at a supermarket. I personally don’t see as a problem
with this issue” [S3, FG2]. Whereas, another participant did not agree with the idea that an infected
individual should be allowed to be a seller of food and other products. He does not believe to be:
“Ready to purchase something which is eatable from someone who is infected with HIV. This is
not safe, in fact it is very dangerous” [S2, FG5], he declared.
4.3.3 Risk perception of HIV and AIDS
Risk perception of getting infected with HIV is low among all subjects. More precisely, male
subjects perceive to be more at risk to get infected with HIV compared with female subjects. This
low risk perception could be that the adolescents and emerging adults believe in their own
invulnerability to HIV and AIDS which can be explained by the less emphasis placed on HIV and
AIDS in Kosovo. A female adolescent from an urban area stated that: “Chances are very small of
getting infected because I am not sexually active. Beside this, I believe I know the ways of getting
a HIV infection quite well and how to protect myself too” [S5, FG1]. A male emerging adult from
the rural area perceived low risk of infection too. However, this is not only due to the limited
sexual activity, but also due to the fact that, as he expressed, because he is not homosexual. As he
explained: “Personally I am not at risk of getting infected. What is more important, I am not a
homosexual, I don’t use drugs, and I don’t have sex with prostitutes. Then why should I be at high
risk?!” [S3, FG4].
134
As it is mentioned above, male perceive to be more at risk to get infected with HIV. Therefore, the
common reasons given by both the targeted groups, adolescents and emerging adults, for rating
themselves as being at higher risk of becoming infected with HIV were as follows: “I have many
sexual partners”; “I don’t always use condoms” and “My partner has other partners” etc. A male
from the emerging adults group stated that: “I don’t always use condom during my sexual
intercourse with girls from my age. I know that not using condoms can put me at risk of getting
infected with HIV” [S2, FG1]. Furthermore, another male participant explained: “I have many
sexual partners and, I don’t always use condoms. I don’t prefer to use it: it makes sex very boring”
[S7, FG2].
On the other hand, a considerable number of subjects participating in focus group discussions,
declared that the risk of getting infecting with HIV and AIDS today is higher than before the war
in Kosovo (1999). This happens due to enormous social and cultural changes in society that
happened in the meantime. As the female subject stated: “After the war in Kosovo (1999) the risks
of getting infected with HIV is higher. People can travel freely today. They can go to another
country, for instance, and have sexual relations with prostitutes and get infected. You never know.
Then he/she can infect his wife/husband too. In addition to this, there are a lot of Kosovar citizens
who live in western countries (Germany, Switzerland, Italy, Austria etc.). They have different
lifestyles there. However, most of them tend to marry in Kosovo (to find wife or husband). They
can get infected there and infect their spouses” [S3, FG4]. Furthermore, another male participant
explained: “Today we have another way of living. We can travel to neighboring countries much
more than in previous years, thus possibility of infection with HIV are higher than before” [S1,
FG2].

135
~Chapter five~Discussion of Quantitative & Qualitative Results
136
CHAPTER V
5.1 Discussion of quantitative and qualitative results
Using some of the main constructs of the Health Belief Model as a guide, the study sought to
examine correlations of HIV knowledge and perception of risk of HIV among the adolescents and
emerging adults. Socio demographic factors such as age group, permanent residence, level of
education, monthly income of parents, were found to be relevant and which correlates with HIV
knowledge among adolescents and emerging adults. Also, perception of risk of HIV was predicted
by factors such as gender. On the other hand, attitudes towards PLWHA were found to be
correlated with the age group, level of education of subjects, parents’ level of education etc.
5.1.1 Knowledge regarding HIV and AIDS
Results of this study have shown a satisfactory level of knowledge among the adolescents and
emerging adults regarding HIV and AIDS. In this regard, in order to be more specific in this
assertion, the study showed that the percentages of “true” responses for all the HIV knowledge
items were slightly higher than “false” and “I have no opinion” responses for most of the items.
For instance, 48.1% of subjects disagree with the statement that: “you can get infected with HIV
by using the same swimming pool with someone who is infected with HIV and AIDS.
Furthermore, subjects with adequate HIV knowledge were more likely to display positive and
acceptable attitudes towards people living with HIV and AIDS.
In fact, results from the qualitative analysis have also shown that the participating subjects in the
focus group discussions have solid knowledge regarding HIV and AIDS. More precisely, results
of qualitative analysis have shown that subjects participated in the research know the main routes
through which HIV virus is transmitted. They are able to make the difference between HIV and
AIDS as well as are fully aware about the ways how HIV cannot be transmitted. It is important to
mention that these results deducted from this current study are in line with a study conducted
among the age group 17-23 in Turkey. This study showed that a considerable number of subjects
137
who participated in the survey were fully aware of AIDS by its definition and its causation too.
Also, more than 88% of them had the required knowledge that HIV and AIDS could be detected
through blood tests and not through other ways such as visual appearance, the way he/she looks
and feels like (Koksal, Namal, Vehid, & Yurtsever, 2005). A study conducted in six EU countries,
Austria, Germany, Italy, Poland, Slovak Republic and Slovenia, among the age groups of 18-25
found out that 76% of the participants answered correctly on the question that the AIDS can be
treated by specific drugs, but cannot be completely cured (Netzelmann, et al., 2007). In addition,
data from an empirical research in Czech Republic shows that adolescents have solid knowledge
about the channels of HIV transmission (Rabu, 2003).
However, this current study showed that there still remain many misconceptions about HIV and
AIDS. For instance, results from survey shows that 7.9% of subjects agree on the assumption that
HIV and AIDS is the same thing, as well as, 20.9% of subjects agree on the assumption that you
can get infected with HIV through social contacts that you have in everyday life (handshakes, hugs
etc.). Furthermore, findings from the qualitative analysis of this current study found out that a
considerable number of subjects participating in four of the focus groups, from adolescents and
emerging adults, believe that if a person is infected with HIV and AIDS most probably will die
within a short period of time. Additionally, some of the subjects who participated in the focus
group discussions declared that they are concerned that HIV and AIDS can be transmitted through
social contact therefore they would prefer to avoid HIV-infected people.
The same concern was also addressed by previous researchers. In this regard, Firoza, Ports &
Mosavel, (2016) found out that there are misconceptions about the spread of HIV via mosquito
bites, shaking hands with HIV infected people etc. (Firoza, Ports, & Mosavel, 2016). In general,
common misconceptions about HIV include fear of contracting AIDS by sharing utensils with
someone who is infected, transmission by mosquito or other insect bites, and a belief that people
who are infected will show signs of illness (Muttunga, Buluma, & Cheluget, 2004). It is certain
that a great extent of spreading of misunderstandings about possible ways of transmission of HIV
leads to unfounded fear, which limits joint and daily activities with people living with HIV and
AIDS, and encourages social isolation of these people. Moreover, misconceptions about HIV
138
transmission may urge stigmatization and discrimination against people living with HIV and
AIDS.
Results of this current study have shown that emerging adults have more and accurate knowledge
regarding HIV and AIDS than adolescents. In this regard, in almost all the items related to HIV
knowledge, it has been shown that emerging adults have much more knowledge compared with
adolescents. Thus, the study showed that in the assumption that they can get infected with HIV by
being fed from the same plate with the person, 25.7% of adolescents vs. 46.6% of emerging adults
do not agree with the same assumption. These results are supported by Maswanya, Moji,
Horiguchi, Nagata, Aoyagi, Honda& Takemoto (2000) in their study conducted in Japan, where
the younger age group scored significantly lower points than the older age group on both elements,
transmission and prevention of HIV and AIDS (Maswanya, et al., 2000).
In addition to this, results of this current study are supported by Muttunga, Buluma & Cheluget
(2004). In their study conducted in Kenya, it shows that the knowledge of HIV prevention methods
among female and male age groups 15 to 19 is lower for all prevention methods compared with
subject’s aged 20 and above (Muttunga, Buluma, & Cheluget, 2004). Similar results are reported
by the Yadav, Makwana, Nareshs, Vadera, Bhavin, Dhaduk, Kishor&Gandha (2011) where it is
identified that the knowledge of HIV and AIDS was higher among the group aged 20 to 24 than it
was among the group aged of 15 to 19 years age group (Yadav, Makwana, Vadera, Dhaduk, &
Gandha, 2011). Contradictory with the results of current study, findings reported by Sphiwe &
Mokgatle (2014) and by Prashanth & AbdRahman (2015) found out that younger age groups had
higher knowledge of HIV than the older age groups (Sphiwe & Mokgatle, 2014; Prashanth & Abd
Rahman, 2015).
There is a different level of knowledge regarding HIV identified by this current study between the
male and female subjects from adolescents and emerging adults. The results have shown that
female subjects (adolescents and emerging adults) have showed slightly higher knowledge
regarding HIV and AIDS than male subjects (adolescents and emerging adults). In the major part
of the HIV knowledge items, it is identified that female subjects provided more accurate answers
compared with male subjects. Similar results are identified by the qualitative analysis too: female
139
subject participating in the focus groups discussions showed to be more informed and to have
deeper understanding about HIV and AIDS, by including ways of transmitting of HIV virus,
differences between HIV and AIDS as well as ways through which the HIV is not transmitted.
These results are also supported by Madiba & Mokgatle (2014) where females have shown more
knowledge regarding HIV and AIDS than males (Sphiwe & Mokgatle, 2014).
Contradictory with the results of this current study, are also findings reported by Naswa & Marfatia
(2010) that showed that male participants have more knowledge of HIV than female participants
(Naswa & Marfatia, 2010). At the same time, the contradictory results are shown by Mitra, Sethi,
Jana, and Bhattacharya (2003) and Mwamwenda (2014) by which males have a higher level of
knowledge about HIV and AIDS than females (Mitra, Sethi, Jana, & Bhattacharya, 2003;
Mwamwenda, 2014). Furthermore, a study conducted in Kosovo in 2008 has not shown significant
gender-based differences in relation to knowledge about HIV and AIDS. This research has targeted
young people aged 15 to 24. According to a report, only 18% of male and 17% of female have
properly identified all the ways for HIV prevention through sexual intercourse and have excluded
most usual misperceptions regarding the HIV transmission through other channels (United Nations
Kosovo Team, 2008).
In addition, other researchers identified a correlation between level of HIV knowledge and gender.
In a study conducted in Bengal, India, it was noticed that the gender differences in awareness and
practices among the male respondents who could correctly identify three routes of HIV
transmission were 34% whereas among the female 15% (Mitra, Sethi, Jana, & Bhattacharya,
2003). On the other hand, in a study conducted with African universities, it was identified that
there is a gender difference in their knowledge of HIV and AIDS among the male and female
participants. Male participants were more informed about HIV and AIDS than female participants.
The sample of respondents was composed by 366 participants, selected from universities in Kenya,
South Africa and Tanzania (Mwamwenda, 2014).
Meanwhile, results of this current study showed that subjects with permanent residence in urban
areas have more HIV knowledge than the subjects from rural areas. In addition, the analysis of the
current data indicated that in most HIV knowledge items subjects with permanent residence in
140
urban areas had a good to excellent knowledge about HIV and AIDS compared with subjects with
permanent residence in rural areas. As well, the same results are also identified from the focus
groups from the subjects participating in both targeted groups: adolescents and emerging adults.
In these focus group discussions, it was noticed that subjects with permanent residence in urban
areas have much more information regarding HIV and AIDS, compared with the subjects with
permanent residence in rural areas. Subjects with the permanent residence in urban areas have
identified in better way all the potential ways through which the HIV is transmitted. They also
were able to identify the important difference between HIV and AIDS as well as managed to
recognize routs through which HIV cannot be transmitted such as: everyday social contacts etc.
These findings are supported by Lal, Vasan, Sarma, & Thankappan (2000) conducted among
young people (18–22 years old) where it is found that the level of awareness about HIV and AIDS
was higher in urban participants compared with rural counterparts (Lal, Vasan, Sarma, &
Thankappan, 2000).
Furthermore, results of this current study showed that parents’ monthly incomes were found to be
significantly associated with HIV and AIDS related knowledge. More precisely, those having high
parents’ monthly incomes showed greater tendency to have high knowledge about HIV and AIDS
compared with those having high parents’ monthly incomes. A significant part of the population
in Kosovo live with minimal monthly income. According to the Eurostat the minimal salary in
Kosovo is 130 EUR. This is the lowest rate compared to other neighbor countries (in Croatia the
minimum salary is 433 EUR, Slovenia 805 EUR whereas in Montenegro 288 EUR). This
economic fact can influence parents to be more focused in working and providing incomes for
their families and, as a consequence, give less importance to the education of their children
including their health education and their wellbeing as well. A lot of similar studies are in line with
the results of current study as well. For instance, these findings are supported by Huda &
Amanullah (2013). This cross sectional study conducted in Bangladesh found that those having
high household income showed greater tendency to have high knowledge about HIV and AIDS
(Huda & Amanullah, 2013). At the same time, these associations were moderately consistent with
the findings of the study accomplished by Lal et al. (2000) among young people (18–22 years) and
as well a study conducted by Othman (2015) showed that knowledge about HIV and AIDS was
significantly associated with those having high socio-economic status (Othman, 2015).
141
Furthermore, study conducted in Brazil among 13-21 years old found out that low family income
was associated with unsatisfactory knowledge of HIV (Trajman, et al., 2003). As well, a study
conducted in Portugal, showed that adolescents whose families have higher monthly incomes have
more knowledge of HIV and AIDS (Chaves, Bento, Ferreira, & Duarte, 2013).
Furthermore, this current study shows that the level of education of subjects has an impact on the
level of knowledge they have regarding HIV and AIDS. In this regard, the higher the level of
education of the subjects the higher level of knowledge regarding HIV is reported. More precisely,
subjects with a university level and those who are currently attending master’s studies have more
knowledge regarding HIV, compared with other subjects with a lower level of education. In
Kosovo very little attention is paid to health education in general and in particular to sexual
education. In fact, information on sexual education that pupils receive during their primary and
secondary education are very limited. Therefore, students in bachelor or master level have much
more information and, what is also important, more accurate information about HIV and AIDS. A
lot of relevant studies are in compliance with the results of current study. In this context, these
finding are supported by Norman & Carr (2003) study where they found out that the higher levels
of formal education were associated with higher levels of HIV knowledge (Norman & Car, 2003).
In addition to this, these finding are also supported by Folasayo et al. (2017) and Othman (2015)
who, in their findings, underlined the fact that the educational level is strongly associated with the
level of knowledge regarding HIV (Folasayo, et al., 2017; Othman, 2015).
5.1.2 Attitudes towards people with HIV and AIDS
One of the objectives of this current study was to identify the attitudes that subjects have towards
people with HIV and AIDS. Findings of this quantitative study showed that both of the targeted
groups, adolescents and the emerging adults, have acceptable and tolerant attitudes towards people
with HIV and AIDS. They declared to have positive attitudes especially when they were asked if
they are ready to take care for their relatives in case they are infected with HIV. To be more
accurate, 84.0% of adolescents and 91.3% of emerging adults agreed with the assumption that if a
family member is infected with HIV, they are ready to care and support them. Emerging adults,

142
with 58.7%, showed positive attitudes when they were asked regarding their friends also, but
adolescents were less supportive, with only 35.6%.
Almost the same results are deducted from the qualitative analysis of this study, where both of the
targeted groups, adolescents and the emerging adults, have shown to have acceptable and tolerant
attitudes towards people with HIV and AIDS. For example, most of the subjects, female and male,
strongly supported the idea that HIV infections is not a condemnation.
Above mentioned findings underline the importance of cultural factors. Kosovar families are very
much connected with each other and caring for those who are in need is a value for almost every
Kosovar family. Meanwhile, both targeted groups, showed acceptable attitudes on issues such as:
if an HIV positive student should be allowed to continue studying and I would accept to share the
same class at school/college with someone who is infected with HIV. It is important to mention
that similar results are identified in a study conducted by Hazarika (2010), in India, where most of
the subjects had a non-discriminatory attitude towards HIV positive individuals. In this study
findings show that, in general, participants seemed to have a favorable attitude towards people
with HIV and AIDS. More than three out of four of the participants were willing to care for
relatives with AIDS, besides about two-thirds of them were in favor of confiding information
regarding the HIV status (Hazarika, 2010). Moreover, the results of this current study are also in
line with the study conducted by Maswanya, Moji, Aoyagi, Yahata, Kusano, Nagata, & Takemoto
(2000). As it is identified in their study, the major numbers of the subjects participating in the
survey have declared that they would be able to study in the same class with HIV positive
classmates (Maswanya, et al., 2000). What is more important, in another study conducted in
Turkey it was found out that about half of the students believed that people with HIV and AIDS
should be able to attend school (Savaser, 2003). In contrast with the findings of this current study,
students in Israel showed to have quite negative attitudes towards HIV-infected individuals. Thus,
19% of students declared that those who are infected with HIV should not be allowed to continue
their studies as they can endanger their fellow students (Brook, 1999). The level of discriminatory
attitudes towards HIV-infected persons was high among Korean adolescents (Sohn & Park, 2012)
too. Consequently, it is clear that people with HIV and AIDS may choose not to disclose their HIV
status for fear of being stigmatized, isolated and refused by society.
143
The results of this currents study showed that subjects are very supportive towards their family
members whenever they face difficulties and need support. In this regard, 88.5% of female subjects
and 90.1% of male subjects agree with the assumption that if a family member is infected with
HIV, they are ready to care and support them. Results of the study are supported by Tobin &
Okojie (2010) where it is stated that 82.7% agreed to care for an infected relative (Tobin & Okojie,
2010). Despite this, the results of this current study showed that 39.7% of subjects declared that if
a family member is infected with HIV, they would prefer this information to remain secret and
28.9% have no answer on this issue. Almost similar results were identified in the qualitative
analysis too. Subjects who were part of the focus groups declared to be ready to support their
family members if it happens that they get infected with HIV, nevertheless they would prefer to
keep this very secret, especially if it happens that the infected person is female. These results show
that in conservative and patriarchal societies, such as Kosovo, female are stigmatized more easily
and more often, compared to male. This stigmatization is more present in cases when HIV is
transmitted through sexual intercourse. Contradictory to these result, findings identified by
Muttunga, Buluma & Cheluget (2004), in Kenya, showed that 59% of female and 72% of male
participants said that if a member of their family got infected with the virus that causes AIDS, they
would not want it to remain a secret (Muttunga, Buluma, & Cheluget, 2004), but rather to be
public.
As mentioned above, subjects displayed acceptable attitudes on most of the issues, however,
stigmatizing attitudes towards PLWHA have been reported on other items that are related mainly
with physical contact. In this regard, 56.3% of all subjects disagree with the statements: I am ready
to eat from the same plate with a person who lives with HIV and AIDS and 48.6 % of all subjects
disagree with the statement: A health worker – doctor or a nurse – who is infected with HIV and
AIDS should be allowed to continue to work with patients. Almost the same results are deducted
from the qualitative analysis of this study. It should be emphasized that qualitative analysis has
shown more intolerant attitudes with regard to two above mentioned statements. More exactly, all
subjects participating in the focus groups discussions have declared that they are not ready to eat
form the same plate with a person who is infected with HIV. They also stated that they are not
ready to receive medical services if they know that a doctor or a nurse who is offering the service
is infected with HIV. From this it can be concluded that despite their willingness to maintain their
144
friendships or to be in the same class with a student or professor infected with HIV, they still fear
that having close contacts with HIV-infected people, may put them at risk of contracting HIV or
AIDS. These result are also in line with the Health Belief Model whereby personal attitudes
towards HIV-infected people reflect the needs of the individuals to avoid a threat by rejecting those
affected by the disease.
Regarding the attitudes towards people with HIV, the research conducted in the framework of this
current study also showed that female (from both the targeted groups) have more positive attitudes
than male subjects do. As we mentioned in the results session of quantitative study, female
subjects, in almost all items related with attitudes towards PLWHA, have showed more positive
and tolerant attitudes towards people living with HIV and AIDS compared with male subjects. In
this context, for instance, 70.9% of female subjects compared with 61.5% of male subjects agree
with the assumption that “a student who lives with HIV and AIDS should be allowed to continue
to attend school/studies”. It is important to underline the fact that the same results are identified in
the focus groups sessions too. Female subjects have shown more positive attitudes and declared to
be more tolerant towards people living with HIV and AIDS compared with male subjects.
Interestingly enough the similar results are reported in study conducted by Nyawose (2001) where
it was shown that female subjects have more positive attitudes towards people with HIV and AIDS
than male subjects. Respectively, 83% of females and 34% of males (Nyawose, 2001) declared
that they are ready to continue their friendship with an individual who is infected with HIV.
In contradiction with the results of this current study, findings presented by Muttunga, Buluma &
Cheluget (2004) showed that female subjects expressed less accepting attitudes (sometimes
negative) towards people with HIV than male subjects (Muttunga, Buluma, & Cheluget, 2004). At
the same time, a study conducted by Tavoosi, Zaferani, Enzevaei, Tajik & Ahmadinezhad (2004)
showed that 35% of the students who were part of the research stated that they prefer not to sit in
a class near an HIV positive student. Furthermore, 46% of students thought that a student with the
disease should not be allowed to enter an ordinary school (boys’ and girls’ attitudes were the same
about this (50% vs. 48%), (Tavoosi, Zaferani, Enzevaei, Tajik, & Zahra, 2004).
145
Moreover, the results of this current showed that the level of education of subjects has significant
impact on attitudes towards people living with HIV and AIDS. More precisely, subjects with a
university level and those who are currently attending master’s studies have more acceptable and
more tolerant attitudes towards PLWHA compared with other subjects with a lower level of
education. Since earlier it was mentioned that the level of education has an impact on the level of
knowledge on HIV, then it can be concluded that these results can be justifiable. Subjects with
better knowledge are expected to have more favorable attitudes towards people living with HIV.
These findings are supported by Fuseini (2011) who, in his study, underlined the argument that
educational level is almost always associated with positive attitudes towards people living with
HIV and AIDS. In this sense, the higher the level of education of participants who are part of the
study, according to the researcher, the more positive attitudes towards PLWHA are shown
(Fuseini, 2011).
Furthermore, the current study shows that level of education of mother of the subjects, has direct
correlation with the positive attitudes of subjects towards people living with HIV, while, the level
of education of fathers of the subjects, did not show direct correlation with the positive attitudes
of subjects towards PLWHA. This shows that in Kosovo the role of mother in the general education
of children is still dominant. Therefore, the mother influence in the formation of attitudes is evident
especially during the adolescent phase. This conclusion is supported also by another research
conducted in Kosovo (2014), where participating students part of study have reported that it is
easier to communicate with their mother about their problems and concerns compared to their
father. What is also worth mentioning is that the findings show that the participating students find
it also easier to talk, for their concerns, to their friends rather than to the father. The close friends
are even better address than siblings (World Health Organization & United Nations Population,
2014).
5.1.3 Risk perception of HIV and AIDS
The third and the final objective of this current study was to identify and measure the risk
perception of HIV and AIDS. In this context, the result showed that male perceive more the risk
of getting infected with HIV compared with female, while between emerging adults and
146
adolescents there is no statistically significant difference on perceiving risk of getting infected with
HIV.
Analyzing in more details, 46.5% of all subjects declared that “there is no risk at all” of getting
infected with HIV; 29.9% declared a “small risk”; 11.9% declared an “average risk” and 4.7%
declared a “high risk” of getting infected with HIV. It is important to underline the fact that the
same results are identified in the focus groups discussion too. Therefore, the perception of risk
towards HIV and AIDS in both targeted groups is low. This low risk perception could be due to
the fact that a considerable part of the subjects reported were not sexually active and also because
both the targeted groups in this research perceived themselves as non-vulnerable to HIV. In
addition to this, this low perception of getting infected with HIV, among the adolescents and
emerging adults, can be a result of lack of importance that is generally devoted to the HIV and
AIDS in Kosovo, especially in the formal education. On the other hand, this low risk perception
of HIV and AIDS might cause adolescents and emerging adults too to engage in behaviors, which
are likely to risk their reproductive health.
This finding is consistent with findings of other studies. A study conveyed in 2003, conducted on
a representative sample of Kosovo’s youth aged 15 to 25, indicated that subjects have a very low
perception of risk of contracting HIV, where 60% of subjects did not perceive themselves at risk
(United Nations Kosovo Team, 2008). Same results are reported by Durojaiye (2011) where it
showed that 73.5% of subjects did not perceive themselves at risk of being infected with HIV.
According to this research, this low risk perception could be that the students believe in their own
invulnerability to AIDS which can be explained by the less emphasis placed on HIV and AIDS in
Africa. The reasons for such reaction include misconception, ignorance, poverty, repudiation,
shame, guilt, and silence as a result of association of the infection with sinful sexual acts (Caldwell,
et al., 1993). Social networks and norms influence individuals by disapproving high-risk behaviors
and approving safe alternatives. Social networks and norms may have hindered the use of safer
alternatives among the students as some of them find buying condoms embarrassing and are
influenced to have sex by peer pressures (Durojaiye, 2011). In addition to this, another study
supports the results derived from this currents study, where 58.4% of subjects regarded themselves
to have no risk at all (Sychareun, Thomsen, Chaleunvong, & Faxelid, 2013) of getting infected
147
with HIV. In general, a review of various studies show that individuals are more likely to
underestimate than to overestimate their risk for HIV and AIDS infection, regardless of the nature
of their sexual behavior (Jeffers, 2012). So, mostly, very low perception of HIV risk has been
reported even in relatively high prevalence rates.
Additionally, this finding, however, is inconsistent with that of Adedimeji (2005) who found in a
study in Ibadan (Nigeria) that 58% of males and 36% of females perceiving HIV risks (Adedimeji,
2005). Also, a study conducted in Uganda by Kibombo, Neema, & Ahmed (2007) showed that at
least 40% of adolescents perceived themselves to be at great risk of contracting HIV. According
to this study, after observations for other correlates of sexual behavior such as age, education,
residence, region and marital status, the findings indicate highly significant positive associations
between perceived risk and risky sexual behavior among males but not females (Kibombo, Stella,
& Ahmed, 2007). High risk perception of HIV among participants, in both above studies, can be
explained with the fact that these countries have higher profile of HIV epidemic.
Furthermore, results from focus group discussions have shown that subjects, especially emerging
adults, with good knowledge of HIV and AIDS (including ways of HIV transmission) have also
stated that the best ways that they use to avoid infection with HIV are: using condoms when they
have sexual relations with unknown people; they have only one sexual partner; they stay truthful
to their partner etc. These result are in line with the Health Belief Model where individuals who
have more information regarding the consequences of HIV, tend to change their behavior with the
aim of making sure that they have one partner or have protected sex in order to protect themselves
from HIV.
Additionally, the common reasons given by both target groups, in this current study, for rating
themselves as “low risk” of contracting HIV and AIDS were as follows: “I’m not sexually active”;
“I have only one partner (she/he is loyal)”; “I trust my partner”; and “I always use condoms”.
These results are in line with other studies. For instance, a study conducted in Britain, showed that
almost all participants knew that AIDS is a dangerous disease but they considered the personal
risk of becoming HIV infected to be low. As explanations for the perceived low risk for
themselves, adolescents offered condom use, control of one's behavior and knowing one's partner,
148
among other things (Woodcock, Stenner, & Ingham, 1999). Meanwhile, the common reasons
given in this current study by both targeted groups for rating themselves “at risk of becoming
infected with HIV” were as follows: “I have many sexual partners”; “I don’t always use condoms”
and “My partner has other partners”. Similar results are identified in the qualitative analysis of this
current study too.
Earlier international studies have found out that young people, despite good HIV and AIDS
knowledge, underestimate their own risk of becoming infected with HIV. Adolescents believe
themselves to be less promiscuous than average and they believe that their partners' sexual
behavior is responsible (e.g. condom use, HIV testing, knowing the partner, faithful and long
relationships), (Potsonen & Kontula, 1999). Woodcock et al. (1992) argued that some adolescents
did not trust the information in mass media and believed that the risk of infection was exaggerated
compared to other risks of life (Woodcock, Stenner, & Ingham, 1999). Besides other reasons, the
low incidence of HIV infection among the population also decreased the perceived risk among
young people (Potsonen & Kontula, 1999).
149
~Chapter Six~General Conclusions
150
CHAPTER VI
GENERAL CONCLUSIONS
This study brings a different perspective, more completed and comprehensive, regarding the
knowledge about HIV, attitudes towards PLWHA and perception of risk among the adolescents
and emerging adults in Kosovo.
It is important to emphasize that the usage of qualitative and quantitative research approaches has
brought a more complex and deeper perspective regarding the knowledge of subjects about HIV
and AIDS. In addition to this, intervention programs which can be developed in the future by
relevant institutions and stakeholders should be focused more in the prevention measures of HIV.
Besides, these actions must take into the consideration formal and informal education where,
through different approaches, will create the opportunity and the environment to encourage debate
within families as regard to the challenges and problems which threaten the health of adolescents
and emerging adults, especially about HIV.
Based on the theoretical consideration which was developed by scholars and researchers, on the
other hand, based on the results and findings derived from this study by using two research
methods – survey through questionnaires and the focus group approach – and, what is more
important, comparing these data and findings with the similar studies that are described in the
discussion, a number of conclusions can be drawn.
Results of the survey show a satisfactory level of knowledge about HIV and AIDS among the
adolescents and emerging adults in Kosovo. The percentages of correct responses for the HIV
knowledge items were slightly higher than the incorrect answers or compared to the answers where
subjects declared to have no opinion on the respective assumption. It has been discovered that
emerging adults have a higher level of knowledge as regards to HIV and AIDS compared with
adolescents. In addition to this, by comparing the level of knowledge regarding HIV and AIDS
with the gender of the subjects from both the target groups, adolescents and emerging adults, the
study showed that female subjects have slightly higher level of knowledge of HIV and AIDS
151
compared with male subjects. In the major part of the items it is identified that female subjects
provided more accurate answers regarding HIV compared with male subjects, except in the second
item (there are no HIV infected persons in Kosovo) and third item (you can get infected with HIV
by using the same toilet seat with someone who is infected with HIV), in which male subjects
showed to have a slightly higher level of knowledge of HIV and AIDS.
Other socio-demographic characteristics of subjects such as: monthly income of the subjects’
parents, educational level of subjects and urban permanent residency were found to be significant
predictors of knowledge about HIV and AIDS. The study showed that there has been a significant
correlation between monthly income of parents and the level of knowledge of HIV. The higher the
monthly income of the subjects’ parents, the higher the level of knowledge of HIV was. The same
results where produced as regard to the level of education among the subjects. In other words, the
higher the level of knowledge, the more knowledge subjects had about HIV and AIDS. More
precisely, subject with a university degree and those who were currently in a master program
proved to have more knowledge regarding HIV compared with subjects with lower level of
education. Subjects with urban permanent residency have proved to have more knowledge about
HIV and AIDS compared with subject with permanent residency in rural areas.
In addition to this, the study has identified that there are still misconceptions about HIV and AIDS
among adolescents and emerging adults in Kosovo. In this regard, 47.9% of subjects agree on
assumption that HIV and AIDS are the same thing. Whereas, 20.9% of subjects agree with the
assumption that a person can get infected with HIV through social contacts in everyday life such
as handshakes, hugs, simple conversation etc.
Results of this current study as regard to the level of knowledge can be used by policymakers and
other stakeholders to develop appropriate programs for increasing the level of awareness regarding
HIV and AIDS, providing accurate and appropriate information especially taking into
consideration socio-demographic variables of this research. These interventions can be undertaken
specifically in primary and secondary schools. In addition, these interventions must be consistent
and continuous in order to protect adolescents and emerging adults from getting infected with HIV.
152
The research results showed that the attitudes of subjects towards people living with HIV and
AIDS were significantly tolerant and positive at the same time. In the major parts of the items
subjects have shown positive attitudes towards people living with HIV and AIDS. Findings show
that emerging adults and female subjects have more positive attitudes towards PLWHA compared
with adolescents and male subjects. In this context, 70.9% of female compared with 61.5% of male
participants agree with the assumption that “a student who lives with HIV and AIDS should be
allowed to continue to attend school/studies”. In addition to this, if these data are analyzed in a
more specific way, then it can be found that there is only one statement (If a family member is
infected with HIV I would prefer this information to remain a secret), where subjects of both age
groups (adolescents and emerging adults), almost equally prefer this information to remain a secret
(39.0% for adolescents vs.37.0% for emerging adults).
On the other hand, despite the fact that in most of the answers in the survey and in the focus group
discussions showed that subjects have acceptable attitudes towards people living with HIV and
AIDS, some stigmatizing attitudes of subjects have been identified as well. These attitudes were
mainly related when they were asked about the possibilities of physical contact with HIV-infected
persons. In this regard, the major part of the subjects participating in the focus groups and answered
in the survey have declared that they are not ready to eat form the same plate with a person who is
infected with HIV. They also stated that would not prefer to get health services form health workers
who are infected. From this it can be concluded that despite their willingness to maintain their
friendship or to be in the same class with a student infected with HIV, they still fear that having
close contact with HIV-infected people may put them at risk of contracting HIV or AIDS. They
stated that they are not ready to receive medical services if they know that a doctor or a nurse who
is offering the service is infected with HIV.
Findings of both qualitative and quantitative research approaches used in this current study
provided new and authentic evidence for understanding attitudes of adolescents and emerging
adults towards people with HIV and AIDS in Kosovo. Moreover, socio-demographic
characteristics of subjects such as mother’s level of education and the education level of subjects
were found to be significant predictors of positive attitudes towards people living with HIV and
AIDS. The level of education of subjects’ mothers in correlation with attitudes of subjects
153
produced some interesting results. In other words, results of the study showed that the level of
education of the mothers of subjects have direct correlation with the positive attitudes that subjects
have towards people with HIV and AIDS. On the other hand, the level of education of the fathers
of subjects has not shown to have impact in attitudes of subjects towards PLWHA. These findings,
among others, show that in Kosovo’s society the mother is and remains the main figure which
plays the main and most important part in the education of their children. On the other hand, fathers
are still perceived as main figures in the responsibilities of taking care of the financial wellbeing
of their families, however, mothers are the main persons who take care of the education of their
children. Moreover, the level of education of subjects had correlation with attitudes towards people
with HIV and AIDS. In this regard, subjects with a higher level of education, respectively those
who obtained their bachelor or master degree have more positive attitudes towards HIV-infected
persons compared with subjects with lower a level of education.
As regard to the risk perception, results of the research showed that male perceive more the risk of
getting infected with HIV compared with female, while between emerging adults and adolescents
there is no statistically significant difference on perceiving risk of getting infected with HIV. Thus,
46.5% of female and male subjects declared that “there is no risk at all” of getting infected with
HIV; 29.9% declared that there is a “small risk”; 11.9% declared that there is an “average risk”
and 4.7% declared a “high risk” of getting infected with HIV. Therefore, the perception of risk
towards HIV and AIDS in both the target groups, adolescent and emerging adults, is low.
Thus, considering the effects of HIV and AIDS on adolescents and emerging adults, it is very
important to set up campaigns and programs that would help to increase their perceived risks of
HIV and AIDS. Factors that affect adolescents’ and emerging adult’s perception of risks of HIV
should be taken into consideration in designing strategies for HIV and AIDS campaigns to ensure
positive behavioral change of both targeted groups.
Furthermore, the common reasons given by both target groups for rating themselves to be at “low
risk” of contracting HIV were the following: “I’m not sexually active”; “I have only one partner
(she/he is loyal)”; “I trust my partner”; and “I always use condom”. Meanwhile, the common
reasons given by both targeted groups for rating themselves as being at higher risk of becoming
154
infected with HIV were as follows: “I have many sexual partners”; “I don’t always use condoms”
and “my partner has other partners”. It is important to mention that almost similar results are
identified in the qualitative analysis too. Most of the subjects from both of the targeted groups who
participated in the focus groups believe not to be at risk of getting infected with HIV. They too, as
main reasons mentioned their sexual inactivity, low number of sexual partners or being loyal to
their sexual partner. On the other hand, those who declared to be at risk of getting infected as a
reason, they mentioned the non-usage of condoms during sexual intercourse or having many sexual
partners.
As a conclusion, findings derived from this study provide relevant evidence which can be used
and applied for different prevention interventions regarding HIV and AIDS knowledge, risk
perception and attitudes towards PLWHA among the adolescents and emerging adults in Kosovo.
6.1 Contributions, implications for future studies and limitations
Findings from this current study will contribute significantly in the subject of HIV and AIDS in
Kosovo. To be more accurate, the research will be very important for future research projects,
scholars and policymakers especially regarding the knowledge and risk perceptions and attitudes
of adolescents and emerging adults towards HIV-infected people.
Considering the fact that earlier studies in Kosovo were very limited, thus they were not conducted
in periodical and regular basis, it can be concluded that this research study will bring new
perspectives. Results of this study can contribute and, at least, have influence in the design of
strategies in the prevention of HIV and AIDS in Kosovo among the adolescents and emerging
adults. It is also important to mention that there were some reports in Kosovo which were published
by different NGO’s or even national institutions (such as Ministry of Health) regarding HIV and
AIDS, nevertheless until now there were no scientific researches for this topic conducted which
included a considerable and very significant sample and with a magnitude which covers and
represents the entire population of Kosovo as regard to the targeted groups: adolescents and
emerging adults.

155
In addition to the contribution that this study will give in the field of scientific research and policy
issues as well, it is important to mention that, as any other research study, this has its limitations
too. The first limitation has to do with the proportional distribution of samples among the emerging
adults and adolescents. Thus, in the samples included are a large proportion of emerging adults,
while the number of subjects from adolescents was smaller. It is important to mention here that
the selection of sample was randomly done. In this case, the future studies in Kosovo should be
oriented in defining in a more proportional manner of samples between adolescents and emerging
adults, by doing so they will have a better and more representative inclusion of both targeted
groups.
In addition, this study has used two research methods to collect data: survey through questionnaires
and focus groups. Since the subjects that have self-administrated the questionnaires are considered
sufficient, taking into consideration the number of the population in Kosovo, as a deficiency be
the small number of focus groups conducted with the target groups can be considered. There were
only four focus groups conducted: two with adolescents and two with emerging adults. Future
studies in this subject have to pay attention and to conduct more focus groups in order to have
clearer and deeper perspectives on the issue of HIV and AIDS knowledge, attitudes towards
PLWHA and risk perception of HIV, among the adolescents and emerging adults in Kosovo.
156
BIBLIOGRAPHY
Ackroyd, S. (1992). Data collection in context. London: Longman Group United Kingdom.
Adedimeji, A. A. (2005). Beyond knowledge and behavior change: the social-structural context ofHIV/AIDS risk perceptions and protective behavior among young urban slum inhabitantsin Nigeria. Department of Population and International Health Harvard School of PublicHealth.
Adefuye, A., Abiona, T., Balogun, J., Amosun, S., Frantz, J., & Yakut, Y. (2011). Perception ofrisk of HIV and sexual risk behaviours among students in the United States, Turkey andSouth Africa. SAHARA-J: Journal of Social Aspects of HIV/AIDS.
Aggleton, P., Yankah, E., & Crewe, M. (2011). Education and HIV/AIDS—30 years on. AIDSEducation and Prevention, 495-507.
Agrawal, H., Rao, R., Chandrashekar, S., & Coulter, J. (1999). Knowledge of and attitudes toHIV/AIDS of senior secondary school pupils and trainee teachers in Udupi District,Karnataka, India. Annals of Tropical Paediatrics: International Child Health, 143-149.
Agyemang, S., Buor, D., & Tagoe-Darko, E. (2012). The extent of knowledge about HIV/AIDSamong young people in the Ejura-Sekyedumase district of Ghana. Journal of AIDS andHIV Research, 241-247.
Akwara, P., Madise, N., & Hinde, A. (2003). Perception of risk of HIV/AIDS and sexual behaviourin Kenya. Journal of biosocial science, 385-411.
Al-Ali, M. (2008). Relationship between prejudice and some personal variables among secondaryschools. Czech Republic: Masaryk University.
Alene, D. G., Wheeler, J. G., & Grosskurth. (2004). Adolescent reproductive health and awarenessof HIV among rural high school students, North Western Ethiopia. AIDS Care, 57-68.
Allport, G. W. (1979). The nature of prejudice. Addison-Wesley Publishing Company.
Archibald, A. B., Graber, J., & Brooks-Gunn, J. (1999, November). Associations among parent-adolescent relationships, pubertal growth, dieting, and body image in young adolescentgirls: A short-term longitudinal study. Journal of Research on Adolescence, 395-415.
Arnett, J. J. (1997). Young people's conceptions of the transition to adulthood. Youth & Society,3-23.
Arnett, J. J. (2000). Emerging adulthood: A theory of development from the late teens through thetwenties. American psychologist, 469.
157
Arnett, J. J. (2006). Emerging adulthood: Understanding the new way of coming of age. Emergingadults in America: Coming of age in the 21st century 22, 3-19.
Arnett, J. J. (2007). Emerging adulthood: What is it, and what is it good for? Child developmentperspectives, 68-73.
Arnett, J. J. (2007). Emerging adulthood: What is it, and what is it good for? Child developmentperspectives, 68-73.
Arnett, J. J. (2014). Emerging adulthood: The winding road from the late teens through thetwenties. Oxford University Press.
Beaulieu, M., Adrien, A., Potvin, L., & Dassa, C. (2014). Stigmatizing attitudes towards peopleliving with HIV/AIDS: validation of a measurement scale. BMC public health, 1246.
Bem, D. (1972). Self-perception theory. Advances in experimental social psychology, 1-62.
Black, B. P., & Miles, M. S. (2002). Calculating the risks and benefits of disclosure in AfricanAmerican women who have HIV. Journal of Obstetric, Gynecologic, & Neonatal Nursing,688-697.
Bos, A., Dijker, A., & Koomen, W. (2007). Sex differences in emotional and behavioral responsesto HIV+ individuals’ expression of distress. Psychology and Health , 493-511.
Bos, A., Kok, G., & Dijker, A. (2001). Public reactions to people with HIV/AIDS in theNetherlands. AIDS Education and Prevention, 219-228.
Bos, A., Pryor, J., Reeder, G., & Stutterheim, S. (2013). Stigma: advances in theory and research.Basic and Applied Social Psychology, 1-9.
Braun, V., & Clarke, V. (2006). Using thematic analysis in psychology. . Qualitative research inpsychology, 77-101.
Breakwell. (2014). The psychology of risk. Cambridge University Press.
Breakwell, G. M., Hammond, S., & Fife-Schaw, C. (1994). Research Methods in Psychology.Journal of Environmental Psychology , 335.
Brighton, K. L. (2007). Coming of age: the education and development of young adolescents: aresource for educators and parents. Natl Middle School Assn.
Brook, U. (1993). AIDS-related knowledge and attitude of high school students in Holon, Israel.Journal of tropical pediatrics, 382-384.
Brook, U. (1999). AIDS-related knowledge and attitude of high school students in Holon, Israel.Journal of Tropical Pediatrics, 382-384.
158
Caldwell, J., Caldwell, P., Ankrah, M., Anarfi, J., Agyeman, D., Awusabo-Asare, K., &Orubuloye, O. (1993). African families and AIDS: context, reactions and potentialinterventions. Health Transition Review, 1-16.
Carr, R., & Gramling, L. (2004). Stigma: a health barrier for women with HIV/AIDS. ournal ofthe Association of Nurses in AIDS Care, 30-39.
Caskey, M. M., & Anfara, V. J. (2007). Research summary: Young adolescents’ developmentalcharacteristics.
Caskey, M., & Anfara, V. (2014, October). Developmental Characteristics of Young Adolescents.Association for Middle Level Education.
Catalán, J. (2002). Mental Health and HIV Infection. Routledge.
Center for Disease Control and Prevention. (2012, April 11). Basic Information about HIV andAIDS. Centers for Disease Control and Prevention.
Central Intellegence Agency: The World Factbook. (2017, January 12). Central IntellegenceAgency: The World Factbook. (C. I. Agency, Editor) Retrieved January 12, 2017, fromCentral Intellegence Agency: The World Factbook:https://www.cia.gov/library/publications/the-world-factbook/geos/kv.html
Chaves, C. B., Bento, M. T., Ferreira, M. C., & Duarte, J. C. (2013). Knowledge about HIV/AIDS:The influence of lifestyles and self-regulation in adolescents. The European Journal ofCounselling Psychology .
Colman, A. (2015). A dictionary of psychology. USA: Oxford University Press.
Conner, M., & Norman, P. (2005). Predicting Health Behaviour. UK: McGraw-Hill Education .
Correll, J., Judd, C., Park, B., & Wittenbrink, B. (2010). Measuring prejudice, stereotypes anddiscrimination. The Sage handbook of prejudice, stereotyping and discrimination, 45-62.
Courtenay, W. (2000). Constructions of masculinity and their influence on men's well-being: atheory of gender and health. Social science & medicine, 1385-1401.
Creswell, J., & Miller, D. (2000). Theory into practice. College of Education, The Ohio StateUniversity.
Darteh, E., Kyereme, A. K., & Asare, K. A. (2016). Perception of risk of HIV among adolescents'living in an urban slum in Ghana: original research. African Journal of ReproductiveHealth, 62-70.
De Bruyn, T. (1998). HIV/AIDS and discrimination: A discussion paper. Canadian HIV-AIDSLegal Network.
159
Degner, A. J. (2006). The definition of adolescence: One term fails to adequately define thisdiverse time period. CHARIS: A Journal of Lutheran Scholarship, Thought, and Opinion ,7-8.
Dovidio, J., Hewstone, M., Glick, P., & Esses, V. (2010). Prejudice, stereotyping anddiscrimination: theoretical and empirical overview. The SAGE handbook of prejudice,stereotyping and discrimination.
Droba, D. D. (1933). The nature of attitude. The Journal of Social Psychology, 444-463.
Durojaiye, O. (2011). Knowledge, attitude and practice of HIV/AIDS: Behavior change amongtertiary education students in Lagos, Nigeria. Annals of Tropical Medicine and PublicHealth, 18.
Eagly, A., & Diekman, A. (2005). What is the problem? Prejudice as an attitude-in-context. Onthe nature of prejudice , 19-35.
Eccles, J., Bonnie, B., Deborah, J., Oksana, M., & Vida, M. (1999). Self-evaluations ofcompetence, task values, and self-esteem. In M. C. N. G. Johnson, Beyond appearance: Anew look at adolescent.
Erikson, E. (1994). Identity: Youth and crisis. WW Norton & Company.
Firoza, H., Ports, K., & Mosavel, M. (2016). Knowledge and attitudes about HIV infection andprevention of mother to child transmission of HIV in an urban, low income community inDurban, South Africa: Perspectives of residents and health care volunteers. Health sagesondheid, 171-178.
Fiske, S., Gilbert, D., & Lindzey, G. (2010). Handbook of social psychology (Vol. II). John Wiley& Sons.
Folasayo, A. T., Oluwasegun, A. J., Samsudin, S., Saudi, S. N., Osman, M., & Hamat, R. A.(2017). Assessing the Knowledge Level, Attitudes, Risky Behaviors and PreventivePractices on Sexually Transmitted Diseases among University Students as FutureHealthcare Providers in the Central Zone of Malaysia: A Cross-Sectional Study.International Journal of Environmental Research and Public Health , 159.
Frost, N. (2011). Qualitative Research Methods in Psychology: Combining Core Approaches.London: McGraw-Hill Education.
Fuseini, K. (2011). ‘Stop aids love life’. Attitudes towards HIV/AIDS: the role of HIV/AIDSbehaviour change communication messages among Ghanaian youth. Sixth AfricanPopulation Conference .
160
Gentry, J., & Campbell, M. (2002). Developing adolescents: a reference for professionals.American Psychological Association .
Gile, P. P. (2013). xploration of HIV/AIDs related knowledge, attitude and practice of universitycommunity: the case of Ethiopian Civil Service College. Working Paper of Public Health.
Glanz, K., Rimer, B., & Viswanath, K. (2008). Health behavior and health education: theory,research, and practice. New Yersey: John Wiley & Sons.
Goffman. (2009). Stigma: Notes on the management of spoiled identity. Simon and Schuster.
Goffman, E. (1980). Stigma: Notes on the Management of Spoiled Identity. New Jersey:Englewood Cliffs, Pren-tice-Hall.
Goffman, E. (2009). Stigma: Notes on the management of spoiled identity. Simon and Schuster.
Goodwin, R., Kozlova, A., Nizharadze, G., & Polyakova, G. (2004). HIV/AIDS amongadolescents in Eastern Europe: knowledge of HIV/AIDS, social representations of risk andsexual activity among school children and homeless adolescents in Russia, Georgia and theUkraine. Journal of health psychology, 381-396.
Green, E., & Murphy, E. (2014). The Wiley Blackwell Encyclopedia of Health, Illness, Behavior,and Society. Hoboken, New Jersey: John Wiley & Sons, Ltd. .
Guindo, O., Liu, A., & Haba, K. (2014). Knowledge, attitudes and practices of youth towardsHIV/AIDS in Mali, West Africa. International Journal of Advanced Physiology and AlliedSciences, 12.
Hall, G. S. (1904). Adolescence. New York.
Hanson, W., Creswell, J., Plano Clark, V., Petska, K., & Creswell, D. (2003). Handbook of mixedmethods in social and behavioral research. University of Nebraska - Lincoln.
Hayden, J. (2013). Introduction to health behavior theory. New Jersey: Jones & BartlettPublishers.
Hazarika, I. (2010). Knowledge, attitude, beliefs and practices in HIV/AIDS in India: identifyingthe gender and rural–urban differences. Asian Pacific Journal of Tropical Medicine, 821-827.
Herek, G. (1999). AIDS and stigma. American Behavioral Scientist.
Herek, G. (2002). Thinking about AIDS and stigma: A psychologist's perspective. The Journal ofLaw, Medicine & Ethics , 594-607.
161
HIV/AIDS Epidemic in India. (2017, January 20). HIV/AIDS Epidemic in India. Retrieved fromAids Free India : http://www.aidsfree-india.org/youth-adolescence/hiv-aids-youth-adolescents-intro.htm
Hochbaum, G., Rosenstock, I., & Kegels, S. (1952). Health Belief Model. United States PublicHealth Service.
Hogg, M. A., & Tindal, S. (2008). Blackwell handbook of social psychology: Group processes.John Wiley & Sons.
Howitt, D., & Cramer, D. ( 2007). Introduction to Research Methods in Psychology. New York :Pearson Education.
Huda, M. N., & Amanullah, A. (2013). HIV/AIDS-Related knowledge among secondary schoolstudents in Bangladesh: a cross-sectional study. . Advances in Infectious Diseases, 274.
Huda, M. N., & Amanullah, A. (2013). Huda, M. N., & Amanullah, A. (2013). HIV/AIDS-Relatedknowledge among secondary school students in Bangladesh: a cross-sectional study.Advances in Infectious Diseases, 274.
Hurrelmann, K. (1987). The importance of school in the life course: Results from the Bielefeldstudy on school-related problems in adolescence. Journal of Adolescent Research, 111-126.
Insko. (2005). Essence of Motivation among the Law Enforcement Personnel. Time International10 , 9-12.
Jeffers, A. (2012). Perceived Risk for HIV among High Risk Individuals: A Comparison ofAdolescents and Adults.
Jeffers, A. (2012). Perceived risk for HIV among high risk individuals: a comparison ofadolescents and adults. Georgia State University.
Judah, T. (2008). Kosovo: What Everyone Needs to Know. New York : Oxford University Press .
Kaplan, L. J. (2004). Adolescence. Boston: Houghton Mifflin Company.
Katz, D. (1960). The functional approach to the study of attitudes. The Public Opinion Quarterly,163-204.
Kayiki, S. P., & Forste, R. (2011). HIV/AIDS related knowledge and perceived risk associatedwith condom use among adolescents in Uganda: original research article. African journalof reproductive health, 15(1).
Kellough, R., & Kellough, N. (2008). Teaching young adolescents: Methods and resources formiddle grades teaching. Pearson Merrill/Prentice Hall.
162
Keniston, K. (1962). Social Change and Youth in America. Daedalus, 145-171.
Kibombo, R., Nemma, S., & Ahmed, F. (2007). Perceptions of risk to HIV infection amongadolescents in Uganda: are they related to sexual behaviour? African journal ofreproductive health.
Kibombo, R., Stella, N., & Ahmed, F. (2007). Perceptions of risk to HIV infection amongadolescents in Uganda: are they related to sexual behaviour? African Journal ofReproductive Health, 168-181.
Kinniburgh, J., Scott, P., Gottlieb, M., & Power, L. (2001). Prejudice, discrimination and HIV: Areport. Terrence Higgins Trust.
Kipke, M. (1999). Adolescent Development and the Biology of Puberty: Summary of a Workshopon New Research. Washington, DC: National Academies Press.
Kippax, S., Aggleton, P., Moatti, J.-P., & Delfraissy, J.-F. (2007). Living with HIV: recent researchfrom France and the French Caribbean, Australia, Canada and the United Kingdom. AIDS.
Kleinman, A., & Hall-Clifford, R. (2009). Stigma: a social, cultural and moral process. Journal ofEpidemiology and Community Health, 418-419.
Kline, A. (2014). The Effects of HIV/AIDS Knowledge During Adolescence: The Role of ThisKnowledge in Predicting Sexual Behaviors and Outcomes .
Koksal, S., Namal, N., Vehid, S., & Yurtsever, E. (2005). Knowledge and attitude towardsHIV/AIDS among Turkish students. Infectious Diseases Journal of Pakistan, 118-23.
Kosovar AIDS Committee. (2008). Kosovar Strategy for HIV/AIDS Prevention 2004-2008.Prishtina : United States Agency for International Development, European Agency forReconstruction & Canadian International Development Agency.
Kosovo Agency of Statistics. (2017, February 4). Kosovo Agency of Statistics. Retrieved fromKosovo Agency of Statistics: http://ask.rks-gov.net/en/
Kumi-Kyereme, A., Awusabo-Asare, K., Tanle, ,. A., & Biddlecom, A. (2007). Influence of socialconnectedness, communication and monitoring on adolescent sexual activity in Ghana:original research article. African journal of reproductive health, 133-147.
Lal, S., Vasan, R. S., Sarma, P. S., & Thankappan, K. R. (2000). Knowledge and attitude of collegestudents in Kerala towards HIV/AIDS, sexually transmitted diseases and sexuality.National medical journal of India, 231-236.

163
Lal, S., Vasan, R. S., Sarma, P. S., & Thankappan, K. R. (2000). Knowledge and attitude of collegestudents in Kerala towards HIV/AIDS, sexually transmitted diseases and sexuality.National medical journal of India, 231-236.
Larson, R. W., Wilson, S., Brown, B., Furstenberg, F., & Verma, S. (2002). Changes inAdolescents' Interpersonal Experiences: Are They Being Prepared for Adult Relationshipsin the Twenty‐First Century? Journal of Research on Adolescence , 31-68.
Lee, R., Kochman, A., & Sikkema, K. (2002). Internalized stigma among people living with HIV-AIDS. AIDS and Behavior, 309-319.
Levinson, D. J. (1978). The seasons of a man's life. Random House LLC.
Lingley, A. (2013). Seeing crucibles: Legitimizing spiritual development in the middle gradesthrough critical historiography.
Link, B., & Phelan, J. (2001). Conceptualizing stigma. Annual review of Sociology, 363-385.
Lugova, H., Mon, A. A., Daher, A. M., & Suleiman, A. (2015). HIV-Related Stigma andDiscriminatory Attitudes among a Semi-Urban Population. Malaysian Journal of MedicalSciences , 64-69.
Macintyre, K., Rutenberg, N. B., & Karim, A. (2004). Understanding perceptions of HIV riskamong adolescents in KwaZulu-Natal. AIDS and Behavior, 237-250.
Magnani, R., Karim, A. M., Weiss, L., Bond, K., Lemba, M., & Morgan, G. (2002). Reproductivehealth risk and protective factors among youth in Lusaka, Zambia. Journal of AdolescentHealth, 76-86.
Maimaiti, N., Shamsuddin, K., Abdurahim, A., Tohti, N., & Maimaiti, R. (2010). Knowledge,attitude and practice regarding HIV/AIDS among university students in Xinjiang. GlobalJournal of Health Science , 51.
Majelantle, R. G., Keetile, M., Bainame, K., & Nkawana, P. (2014). Knowledge, Opinions andattitudes towards HIV and AIDS among Youth in Botswana. Journal of Global Economics.
Malleshappa, K., & Krishna, S. (2012). Awareness and attitude of youth toward HIV/ AIDS inrural Southern India. Biomedical Research, 23.
Maswanya, E., Moji, K., Aoyagi, K., Yahata, Y., Kusano, Y., Nagata, K., & Takemoto, T. (2000).Knowledge and attitudes toward AIDS among female college students in Nagasaki, Japan.Health Education Research, 5-11.
Matthews, B., & Ross, L. (2010). Research Methods: A Practical Guide for the Social Sciences.London: Pearson Education Limited.
164
Matthews, B., & Ross, L. (2014). Research methods. New York : Pearson Higher.
Maurer, T., & Pierce, H. (1998). A Comparison of Likert Scale and Traditional Measures of Self-Efficacy. Journal of Applied Psychology, 324.
McLeod, S. (2014). Attitudes and Behavior.
Mghase, S. J. (2010). Community response to hiv/aids: a case of pastoralists in Kilosa district,Tanzania. Sokoine University of Agriculture.
Ministry of Culture, Youth and Sports. (2013). Kosovar Strategy for Youth, 2013-2017. Prishtina:Ministry of Culture, Youth and Sports.
Ministry of Health. (2001). Njohuritë e rinisë shkollore për AIDS. Prishtina: Ministry of Health.
Ministry of Health. (2003). Kosovar Strategy for HIV/AIDS Prevention 2004-2008. Prishtina:Ministry of Health.
Mitra, M., Sethi, S., Jana, S., & Bhattacharya, K. (2003). Gender differences in knowledge,attitudes and prevention of HIV/AIDS/STI among youth in West Bengal, India. Plannedparenthood federation of America-International.
Montgomery, M. (2005). Psychosocial intimacy and identity: from early adolescence to emergingadulthood. Journal of Adolescent Research, 346–74.
Mostyn, B. (1978). The Major Theories Influencing the Study of Attitudes. In B. Mostyn, TheAttitude Behavior Relationship (pp. 21-26). Bradford : Bradford : MCB Publ.
Muttunga, J., Buluma, R., & Cheluget, B. (2004). HIV/AIDS-related knowledge, attitudes andbehaviour. In Kenya Demographic and Health Survey 2003. Kenya: Central Bureau ofStatistics, Ministry of Health, ORC Macro, & ORC Macro.
Mwamwenda, T. (2014). African University Students’s Gender Differences in HIV/AIDSKnowledge . Mediterranean Journal of Social Sciences .
Myers, D. (2011). Psychology (10th Edition ed.). Worth Publishers.
Myers, D. (2012). Social Psychology. McGraw-Hill Education.
Nakakuwa, F. (2015). An analysis about knowledge, attitutes, beliefs and practices of HIV andAIDS among the Himba people of the Kunene region.
Nambatya, D. (2010). Knowledge, attitudes and practices of youth towards HIV/AIDS: A case ofNorthern Uganda region.
165
Naswa, S., & Marfatia, Y. S. (2010). Adolescent HIV/AIDS: Issues and challenges. Indian Journalof Sexually Transmitted Diseases and AID, 1.
National Institute of Public Health. (2017, January 6). National Institute of Public Health.Retrieved from National Institute of Public Health: http://msh-ks.org/en/instituti-kombetar-i-shendetesise-publike/
National Institute of Public Health of Kosovo. (2016). Programmatic mapping and size estimationof key population in Kosovo. Pristina.
National Public Health Institute. (2001). Njohuritë, pikëpamjet dhe shprehitë e të rinjve ndajshëndetit seksual dhe riprodhues. Prishtina: National Public Health Institute.
National Public Health Institute. (2008). Njohuritë, qëndrimet dhe sjelljet e punëtorëveshëndetësor në raport me HIV/AIDS. Prishtina: National Public Health Institute.
Ndifon, W. (2005). HIV/AIDS-related knowledge, attitudes and social distance towards peopleliving with HIV/AIDS) among undergraduate students in calabar. Life.
Netzelmann, T. A., Steffan, E., Sokolowski, S., Schnitzer, S., Oremus, D., & Brehm, G. (2007).Knowledge, Attitudes and sexual Behaviour with regards to HIV/STIs among 18 to 25 yearsold young adults in 6 EU countries. Berlin: SPI Forschung.
Norman, L. R., & Car, R. (2003). The role of HIV knowledge on HIV-related behaviours: ahierarchical analysis of adults in Trinidad. Health Education, 145-155.
Noroozinejad, G., Yarmohamadi, M., Bazrafkan, F., Sehat, M., Rezazadeh, M., & Ahmadi, K.(2013). Perceived risk modifies the effect of HIV knowledge on sexual risk behaviors.Frontiers in public health, 33.
Nunn, A., Zaller, N., Cornwall, A., Mayer, K., Moore, E., Dickman, S., . . . Kwakwa, H. (2011).Low perceived risk and high HIV prevalence among a predominantly African Americanpopulation participating in Philadelphia's Rapid HIV testing program. AIDS patient careand STDs, 229-235.
Nunnally, J., & Bernstein, I. (1994). Psychometric Theory . McGraw-Hill.
Nyawose, G. (2001). Attitudes of students towards individuals with HIV/AIDS: an investigationon the University of Zululand, KwaDlangezwa campus.
Odhiambo, C. (2012). HIV/AIDS and Women in Africa. INternational Journal of Humanities andSocial Science.
Öktem, P. (2015). The role of the family in attributing meaning to living with HIV and its stigmain Turkey. SAGE Open .
166
Öktem, P. (2015). The role of the family in attributing meaning to living with HIV and its stigmain Turkey. SAGE Open .
Osgood, C., & Tannenbaum, P. (1955). The principle of congruity in the prediction of attitudechange. Psychology Review, 42-55.
Othman, S. (2015). Knowledge about HIV/AIDS among high school students in Erbil city/Iraq.Global journal of health science, 16.
Pachankis, J. (2007). The psychological implications of concealing a stigma: a cognitive-affective-behavioral model. Psychological bulletin, 328.
Palomba, C., & Banta, T. (2001). Assessing student competence in accredited disciplines:Pioneering approaches to assessment in higher education. San Francisco: StylusPublishing.
Patnerships in health. (2008). Trajnimi bazë për HIV dhe AIDS për punonjësit e kujdesit parësorshëndetësor. Prishtinë: Patnerships in health.
Paul, M. M. (2011). The knowledge of and attitudes towards HIV/AIDS among post-secondarystudents in a southern Ethiopian city.
Pbworks. (2017, March 21). Pbworks: Issues including advantages and disadvantages. Retrievedfrom Pbworks: Issues including advantages and disadvantages:http://focusgroups.pbworks.com/w/page/5677430/Issues%20including%20advantages%20and%20disadvantages#Thedisadvantagesoffocusgroups
Perrin, G. (2010). A Comparative Analysis of the Attitudes towards People Living with HIV/AIDSbetween Haiti and the Dominican Republic.
Pickens, J. (2005). Organizational Behavior in Health Care. USA: Jones and Bartlett Publishers .
Popper, K. (2004). The Logic of Scientific Discovery. New York : Routledge, Taylor & Francis.
Potsonen, R., & Kontula, O. (1999). Adolescents knowledge and attitudes concerning HIVinfection and HIV-infected persons: how a survey and focus group discussions are suitedfor researching adolescents HIV/AIDS knowledge and attitudes. Health EducationResearch: Theory and Practice, 473-484.
Pötsönen, R., & Kontula, O. (1999). Adolescents' knowledge and attitudes concerning HIVinfection and HIV-infected persons: how a survey and focus group discussions are suitedfor researching adolescents' HIV/AIDS knowledge and attitudes. Health educationresearch, 473-484.
167
Prashanth, T., & Abd Rahman, M. F. (2015). Assessment of HIV knowledge among universitystudents using the HIV-KQ-18 scale: A cross-sectional study. South East Asia Journal ofPublic Health, 33-38.
Prata, N., Morris, L., Mazive, E., Vahidnia, F., & Stehr, M. (2006). Relationship between HIV riskperception and condom use: evidence from a population-based survey in Mozambique.International Family Planning Perspectives, 192-200.
Rabu, L. (2003). Adolescent Sexual Behavior and the HIV/AIDS Risk in the Czech Republic.Revija za sociologiju, 189-206.
Reifman, A., Jensen., J., & Colwell, M. J. (2003). The IDEA: Inventory of the dimensions ofemerging adulthood. 11th Annual Convention of the American Psychological Association.
Rindfuss, R. (1991). The young adult years: Diversity, structural change, and fertility.Demography , 493-512.
Robillard, R. H. (2001). The Jamaican adolescent: an assessment of knowledge and attitudesregarding HIV/AIDS. Pediatric nursing, 176.
Robson, C. (1993). Real World Research: A Resource for Social Scientists and Practitioners-Researchers. Oxford: Massachusetts: Blackwell Pushers .
Rodkjaer, L., Sodemann, M., Ostergaard, L., & Lomborg, K. (2011). Disclosure decisions: HIV-positive persons coping with disease-related stressors. Qualitative Health Research , 1249-1259.
Samelson, F. (1978). From “race psychology” to “studies in prejudice”: Some observations on thethematic reversal in social psychology. Journal of the History of the Behavioral Sciences ,265-278.
Samkange-Zeeb, F. (2013). Assessing knowledge and awareness of sexually transmitted infectionsamong school-going adolescents.
Santrock, J. (2016). Adolescence. New York: McGraw-Hill.
Savaser, S. (2003). Knowledge and attitudes of high school students about AIDS: A Turkishperspective. Public health nursing, 71-79.
Short, J. F. (1984). The social fabric at risk: Toward the social transformation of risk analysis. .American sociological review, 49(6), 711-725.
Simbayi, L., Kalichman, S., Strebel, A., Cloete, A., Henda, N., & Mqeketo, A. (2007). Internalizedstigma, discrimination, and depression among men and women living with HIV/AIDS inCape Town, South Africa. Social science & medicine, 1823-1831.
168
Siniscalco & Auriat. (2005). Questionnaire design. Quantitative research methods in educationalplanning. UNESCO International Institute for Educational Planning, Paris.
Sohn, A., & Park, S. (2012). HIV/AIDS knowledge, stigmatizing attitudes, and related behaviorsand factors that affect stigmatizing attitudes against HIV/AIDS among Korean adolescents.Osong Public Health and Research Perspectives, 24-30.
Sphiwe, M., & Mokgatle, M. (2014). HIV and AIDS related knowledge and attitudes towardslearners infected with HIV: Survey among high school learners in Gauteng and North Westprovinces in South Africa. PeerJ PrePrints.
Stewart, A. E. (2016, 2 26). The implementation of Adult Support and Protection (Scotland) Act(2007). University of Glasgow.
Štulhofer, A., Graham, C., Božičević, I., Kufrin, K., & Ajduković, D. (2007). HIV/AIDS-relatedknowledge, attitudes and sexual behaviors as predictors of condom use among young adultsin Croatia. International Family Planning Perspectives, 58-65.
Stutterheim, S. E. (2011). Understanding HIV-related Stigma: Social and Psychological Processes.Doctoral dissertation, Maastricht University.
Stutterheim, S., John, P., Bos, A., Hoogendijk, R., Muris, P., & Schaalma, H. (2009). HIV-relatedstigma and psychological distress: the harmful effects of specific stigma manifestations invarious social settings. Aids, 2353-2357.
Swenson, R., Rizzo, C., Brown, L., Vanable, P., Carey, M., Valois, R., . . . Romer, D. (2010). HIVknowledge and its contribution to sexual health behaviors of low-income African Americanadolescents. Journal of the National Medical Association, 1173.
Sychareun, V., Thomsen, S., Chaleunvong, K., & Faxelid, E. (2013). Risk perceptions of STIs/HIVand sexual risk behaviours among sexually experienced adolescents in the Northern part ofLao PDR. BMC Public Health, 1126.
Tan, X., Pan, J., Zhou, D., Wang, C., & Xie, C. (2007). HIV/AIDS knowledge, attitudes andbehaviors assessment of Chinese students: a questionnaire study. International Journal ofEnvironmental Research and Public Health, 248-253.
Tavoosi, A., Zaferani, A., Enzevaei, A., Tajik, P., & Zahra, A. (2004). Knowledge and attitudetowards HIV/AIDS among Iranian students. BMC Public Health, 17.
Tobin, E. A., & Okojie. (2010). Knowledge, attitude and practices of adolescent secondary schoolstudents in Uvwie Local Government Area of Delta State of HIV/AIDS. Benin Journal ofPostgraduate Medicine, 3.
169
Trajman, A., Belo, M. T., Teixeira, E. G., Dantas, V. C., Salomão, F. M., & Cunha, A. J. (2003).Knowledge about STD/AIDS and sexual behavior among high school students in Rio deJaneiro, Brazil. Cadernos de Saúde Pública, 127-133.
Trible, H. B. (2015). Emerging Adulthood: Defining the Life Stage and its Developmental Tasks.Educational Specialis, 2.
Tuckman, B. (1999). Conducting Educational Research. San Diego: Harcourt Brace Jovanovitch.
UNAIDS: Kosovo Narrative Report . (2017, February 2). UNAIDS: Kosovo Narrative Report2015. Retrieved from UNAIDS:http://www.unaids.org/sites/default/files/country/documents/KOSOVO_narrative_report_2015.pdf
UNICEF. (2015, November 18). Adolescence. Prishtina, Kosovo.
UNICEF; Joint United Nations Programme on HIV/AIDS; World Health Organization. (2002).Young people and HIV/AIDS: Opportunity in crisis. The Stationery Office.
United Nation Kosovo Team. (2006). Behavioral and biological aspects of HIV and sexuallytransmitted diseases. Prishtina: United Nation Kosovo Team.
United Nations Kosovo Team. (2008). Knowledge, Attitudes, Practices and Behavior Study onHIV/AIDS with young people in Kosovo. Pristina.
United Nations Kosovo Team. (2008). Njohuritë, qëndrimet, praktikat dhe sjellja e të rinjve nëKosovë mbi HIV/AIDS. Prishtina: United Nations Kosovo Team.
Valdiserri, R. O. (2002). HIV/AIDS stigma: an impediment to public health. American journal ofpublic health. American Journal of Public Health.
Vanable, P., Carey, M., Blair, D., & Littlewood, R. (2006). Impact of HIV-related stigma on healthbehaviors and psychological adjustment among HIV-positive men and women. AIDS andBehavior , 473-482.
VandenBos, G. R. (2015). APA dictionary of psychology. Second editon. American PsychologicalAssociation.
Wodi, B. (2005). HIV/AIDS Knowledge, Attitudes, and Opinions among Adolescents in the RiverStates of Nigeria. International electronic journal of health education, 86-94.
Wodi, B. E. (2005). HIV/AIDS Knowledge, Attitudes, and Opinions among Adolescents in theRiver States of Nigeria. International Electronic Journal of Health Education , 86-94.
170
Wong, L. P., AbuBakar, S., & Chinna, K. (2014). Community knowledge, health beliefs, practicesand experiences related to dengue fever and its association with IgG seropositivity. PLoSNegl Trop Dis.
Woodcock, A. J., Stenner, K., & Ingham, R. (1999). Young people talking about HIV and AIDS:Interpretations of personal risk of infection. Health Education Research, 229-247.
World Health Organization & United Nations Population. (2014). Health Behavior in School-AgedChildren. Prishtina.
World Health Organization. (1990). Global program on AIDS Social and Behavior Research Unit.Research package: knowledge, attitude, beliefs and practices on AIDS (KABP).
World Health Organization. (2017). World Health Organization. Retrieved January 5, 2017, fromWorld Health Organization:http://www.who.int/maternal_child_adolescent/topics/adolescence/dev/en/
Yadav, S., Makwana, N., Vadera, B., Dhaduk, K., & Gandha, K. (2011). Awareness of HIV/AIDSamong rural youth in India: a community based cross-sectional study. The Journal ofinfection in developing countries, 711-716.
Yadav, S., Makwana, N., Vadera, B., Dhaduk, K., & Gandha, K. (2011). Awareness of HIV/AIDSamong rural youth in India: a community based cross-sectional study. The Journal ofinfection in developing countries, 711-716.

171
ANNEX 1: Finalized questionnaire
172
173
174

175
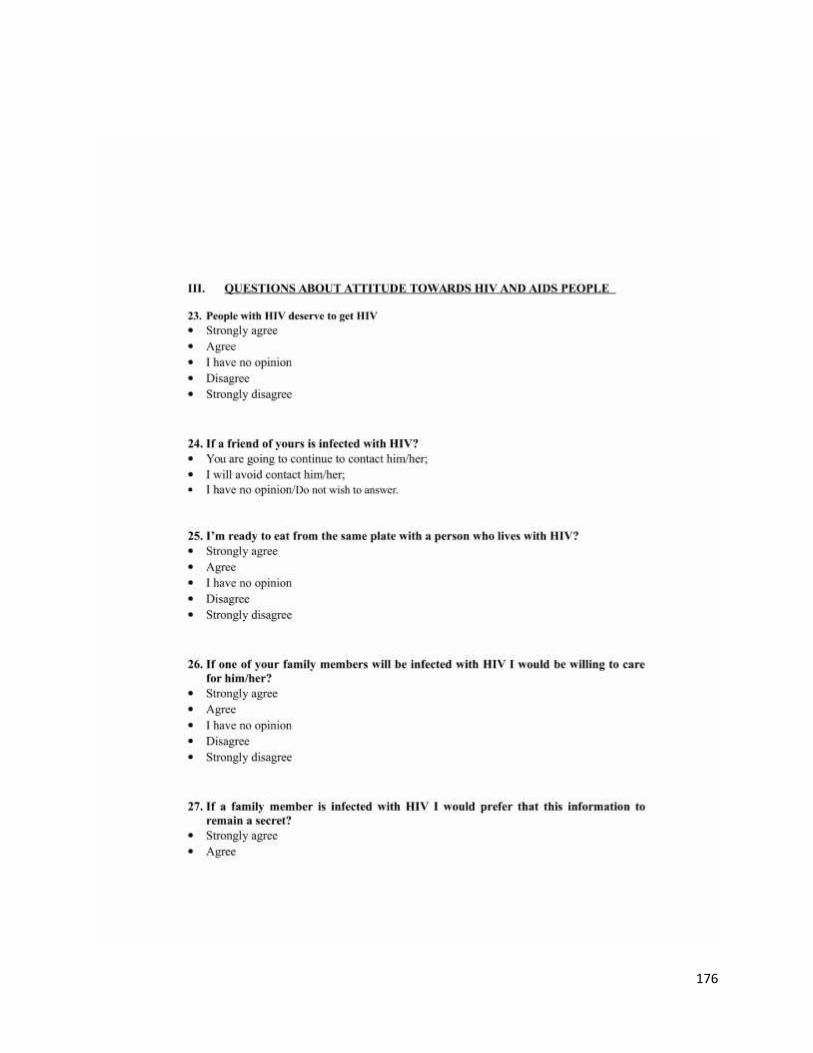
176

177

178

179
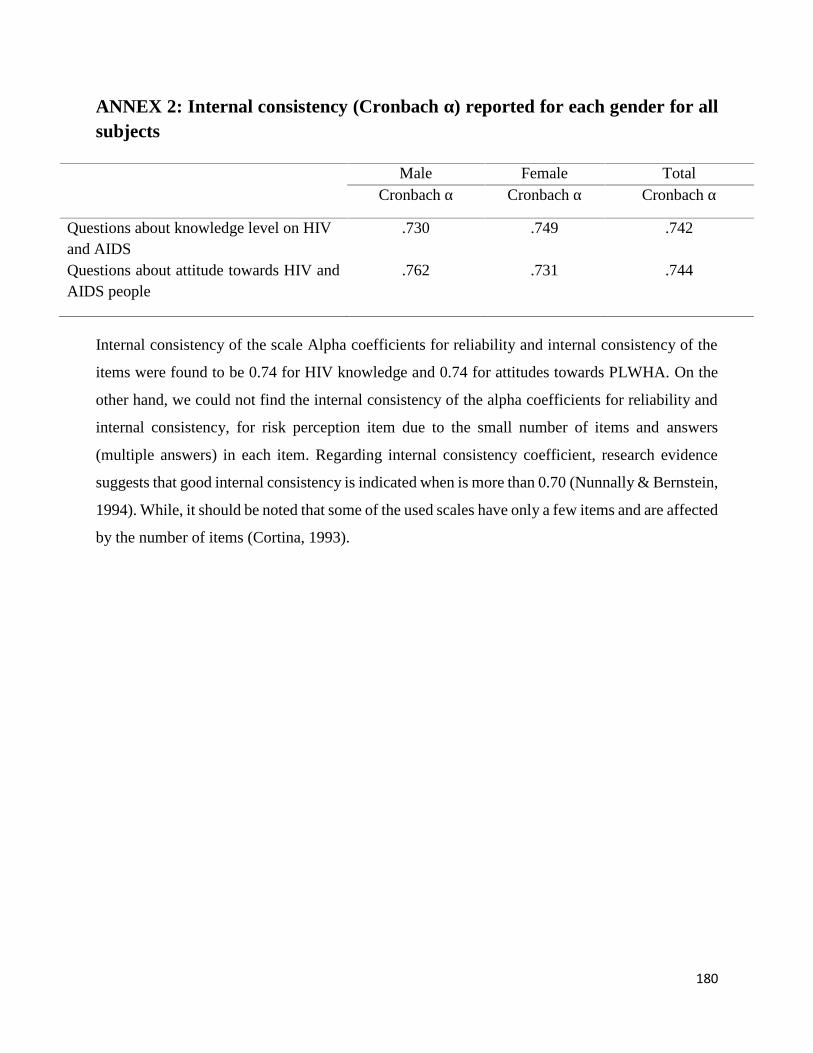
180
ANNEX 2: Internal consistency (Cronbach α) reported for each gender for allsubjects
Male Female TotalCronbach α Cronbach α Cronbach α
Questions about knowledge level on HIVand AIDS
.730 .749 .742
Questions about attitude towards HIV andAIDS people
.762 .731 .744
Internal consistency of the scale Alpha coefficients for reliability and internal consistency of the
items were found to be 0.74 for HIV knowledge and 0.74 for attitudes towards PLWHA. On the
other hand, we could not find the internal consistency of the alpha coefficients for reliability and
internal consistency, for risk perception item due to the small number of items and answers
(multiple answers) in each item. Regarding internal consistency coefficient, research evidence
suggests that good internal consistency is indicated when is more than 0.70 (Nunnally & Bernstein,
1994). While, it should be noted that some of the used scales have only a few items and are affected
by the number of items (Cortina, 1993).
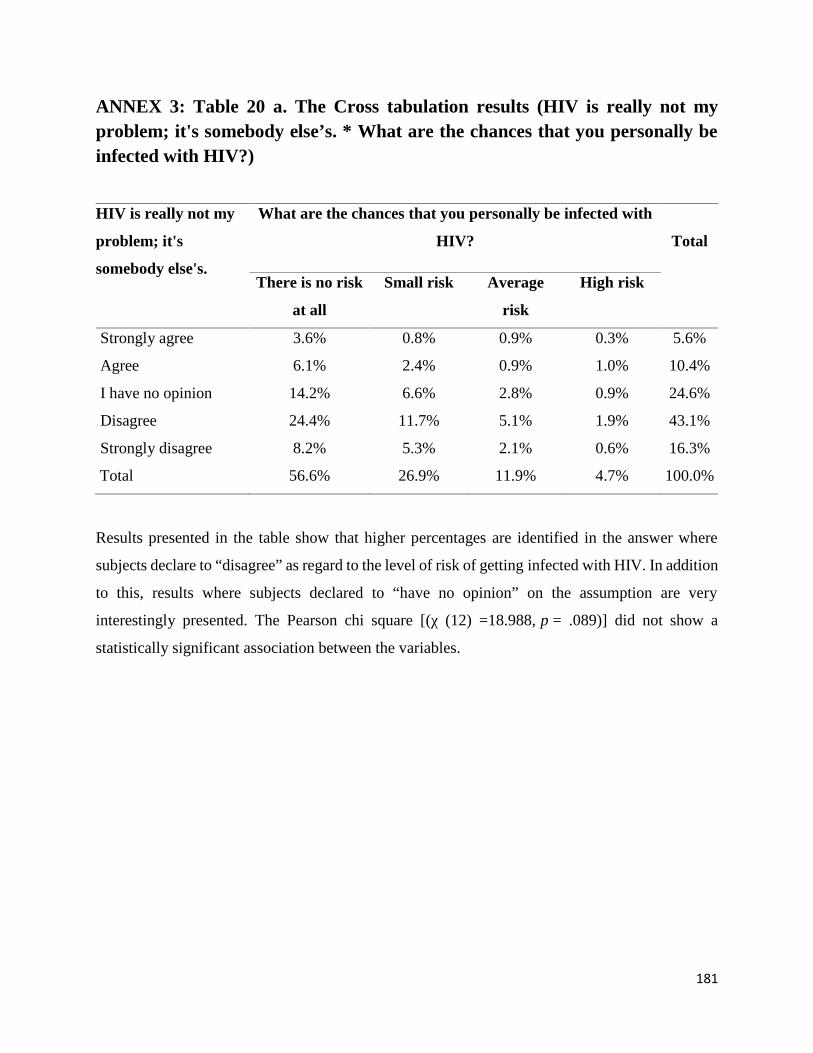
181
ANNEX 3: Table 20 a. The Cross tabulation results (HIV is really not myproblem; it's somebody else’s. * What are the chances that you personally beinfected with HIV?)
HIV is really not my
problem; it's
somebody else's.
What are the chances that you personally be infected with
HIV? Total
There is no risk
at all
Small risk Average
risk
High risk
Strongly agree 3.6% 0.8% 0.9% 0.3% 5.6%
Agree 6.1% 2.4% 0.9% 1.0% 10.4%
I have no opinion 14.2% 6.6% 2.8% 0.9% 24.6%
Disagree 24.4% 11.7% 5.1% 1.9% 43.1%
Strongly disagree 8.2% 5.3% 2.1% 0.6% 16.3%
Total 56.6% 26.9% 11.9% 4.7% 100.0%
Results presented in the table show that higher percentages are identified in the answer where
subjects declare to “disagree” as regard to the level of risk of getting infected with HIV. In addition
to this, results where subjects declared to “have no opinion” on the assumption are very
interestingly presented. The Pearson chi square [(χ (12) =18.988, p = .089)] did not show a
statistically significant association between the variables.
182
ANNEX 4: Interview protocol for focus group discussion
Protocol of the focus group discussion
Name of the focus group:
Date:
Site:
Time when discussion started:
Time when discussion ended:
I. Introduction
Dear participants,
Thank you for agreeing to be part of the focus group. We appreciate your willingness to participate.
We are interested in exploring and analyzing adolescents’ and emerging adults’ attitudes towards
people living with HIV and AIDS in Kosovo; also to know your level of knowledge and perception
of risk towards HIV.
III. GROUND RULES:
1. We want you to do the talking
We would like everyone to participate in this discussion
2. There are no right or wrong answers
Every person’s experience and opinion is important
3. What is said in this room stays here
4. We will be tape recording the group discussion
183
We don’t identify anyone by name in our report. You will remain anonymous.
IV. Confidentiality issues
We assure you that we will respect all professional and ethical codes regarding the confidentiality
of the identity of the subjects, and that data from this focus group discussion will be analyzed only
in group and not individually. Likewise, the answers given by you will only be analyzed to obtain
the results associated with the main goal of this study.
Your honest opinion is very important so to achieve a realistic and accurate study on the subject.
Our discussion will last from one and a half to two hours.
V. Questions
1. INTRODUCTION
Dear all, we would kindly ask you to introduce yourself.
2. Questions about knowledge of HIV and AIDS
First of all, we are interested to ask about your KNOWLEDGE of HIV and AIDS
Is HIV and AIDS the same thing?
How is HIV transmitted?
How can you notice that a person is infected with HIV?
How can we prevent HIV infection?
184
3. Questions about attitudes towards people with HIV
We are very much interested to understand your ATTITUDES towards people with HIV:
People with HIV deserve to get HIV?
Are you ready to eat from the same plate with a person who has HIV?
If one of your family members will be infected with HIV, would you be willing to care for
him/her?
o Would you prefer this information to remain secret?
Should a student who lives with HIV should be allowed to continue to attend
school/studies?
o A professor who is infected with HIV and AIDS should be allowed to continue to
teach?
A health worker (doctor, nurse) who is infected with HIV should be allowed to continue to
work with patients?
4. Questions on risk perception
What are the chances on getting infected with HIV?
o Are you at high or low risk to become infected?
VI. The end of interview
Thank you for your time and thoughts. This has been very helpful.
185
ANNEX 5: Consent to participate in focus group
186
187
188





























