Embed Size (px)
Citation preview

Food and Chemical Toxicology 65 (2014) 321–328
Contents lists available at ScienceDirect
Food and Chemical Toxicology
journal homepage: www.elsevier .com/locate / foodchemtox
The effect of activated charcoal on adenine-induced chronic renalfailure in rats
0278-6915/$ - see front matter � 2014 Elsevier Ltd. All rights reserved.http://dx.doi.org/10.1016/j.fct.2013.12.038
Abbreviations: AC, activated charcoal; CAT, catalase; CKD, chronic kidneydisease; CRF, chronic renal failure; DCF, dichlorodihydrofluoresceine; DHA, 2,8-dihydroxyadenine; ESRD, end-stage renal disease; GPx, glutathione peroxidase; GSI,glomerular sclerosis index; IS, indoxyl sulfate; MSI, mesangiolysis index; NGAL,neutrophil gelatinase-associated lipocalin; PAS, periodic acid-Schiff stain; SOD,superoxide dismutase; TAC, total antioxidant capacity; TGF-b, transforming growthfactor-beta.⇑ Corresponding author. Address: Institute of Pharmacology and Toxicology,
University of Würzburg, Versbacher Str. 9, 97078 Würzburg, Germany. Tel.: +49 9313148722; fax: +49 931 20148446.
E-mail address: [email protected] (N. Schupp).
Badreldin H. Ali a, Mohamed Alza’abi a, Aishwarya Ramkumar a, Intisar Al-Lawati a, Mostafa I. Waly b,Sumaya Beegam c, Abderrahim Nemmar c, Susanne Brand d, Nicole Schupp d,⇑a Department of Pharmacology and Clinical Pharmacy, College of Medicine and Health Sciences, Sultan Qaboos University, Omanb Department of Food Science and Nutrition, College of Agricultural and Marine Sciences, Sultan Qaboos University, Omanc Department of Physiology, United Arab Emirates University, Al-Ain, United Arab Emiratesd Institute of Pharmacology and Toxicology, University of Würzburg, Würzburg, Germany
a r t i c l e i n f o a b s t r a c t
Article history:Received 14 October 2013Accepted 22 December 2013Available online 10 January 2014
Keywords:AdenineChronic renal failureActivated charcoalUremic toxins
Activated charcoal (AC) is a sorbent that has been shown to remove urinary toxins like urea and indoxylsulfate. Here, the influence of AC on kidney function of rats with experimental chronic renal failure (CRF)is investigated. CRF was induced in rats by feeding adenine (0.75%) for four weeks. As an intervention, ACwas added to the feed at concentrations of 10%, 15% or 20%. Adenine treatment impaired kidney function:it lowered creatinine clearance and increased plasma concentrations of creatinine, urea, neutrophil gel-atinase-associated lipocalin and vanin-1. Furthermore, it raised plasma concentrations of the uremic tox-ins indoxyl sulfate, phosphate and uric acid. Renal morphology was severely damaged andhistopathological markers of inflammation and fibrosis were especially increased. In renal homogenates,antioxidant indices, including superoxide dismutase and catalase activity, total antioxidant capacity andreduced glutathione were adversely affected. Most of these changes were significantly ameliorated bydietary administration of AC at a concentration of 20%, while effects induced by lower doses of dietaryAC on adenine nephrotoxicity were not statistically significant. The results suggest that charcoal is a use-ful sorbent agent in dietary adenine-induced CRF in rats and that its usability as a nephroprotective agentin human kidney disease should be studied.
� 2014 Elsevier Ltd. All rights reserved.
1. Introduction
Administration of sorbents, i.e. compounds that bind otherchemicals onto their outer surfaces, and within their interstices(Ash, 2009) has been suggested as either an alternative or supple-mentary treatment for patients with chronic kidney disease (CKD).They have been shown to remove waste products such as urea,indoxyl sulfate (IS) and other urinary toxins, and augment the dial-ysis process (Schulman, 2012; Winchester and Ronco, 2010;Yamamoto et al., 2011). One of these sorbents is charcoal (Cooney,
1995; Olson, 2010; Vaziri et al., 2013), which is produced by heat-ing pulverized carbonaceous substances to temperatures of 600–900 �C, followed by ‘‘activation’’ using either steam or hot air toerode the internal surfaces of the product and thereby increaseits adsorptive surface area. Typical surface areas for activated char-coals are about 800–1200 m2/g. Thus, a 50-g dose of activatedcharcoal has an adsorptive surface area equivalent to about sevenfootball fields or 5183 m2, and ‘‘Superactivated’’ charcoals mayhave a surface area of 2800–3500 m2/g and can adsorb greaterquantities of drugs (Olson, 2010). Charcoal, in various forms,administered with low protein diets has been reported to controleffectively some uremic symptoms in patients with differentstages of renal disease, and this is achieved through the bindingof urea and other urinary toxins to charcoal, and its excretion withfeces, creating a concentration gradient for continued diffusion ofthese toxins (Ash, 2009). Scavenging of urinary toxins by charcoalshas also been proposed (Fujii et al., 2009). The beneficial effect wasreported especially in elderly patients with end-stage renal disease(ESRD) (Musso et al., 2010). Recently, Schulman et al. reported thatthe use of activated charcoal (AC) and other alternative agents,which are capable of blocking the actions of profibrotic cytokines,

322 B.H. Ali et al. / Food and Chemical Toxicology 65 (2014) 321–328
such as transforming growth factor-beta (TGF-b), can either halt orprevent the development of CKD in early stages (Schulman, 2012).
The adenine-induced chronic renal failure (CRF) rat model, firstreported by Yokozawa et al. (1986), produces metabolic abnormal-ities resembling CKD in humans, which may include azotemia,accumulation of uremic toxins, metabolic imbalances of aminoacids and electrolytes, and hormonal imbalances (Yokozawaet al., 1986). Pathologically, renal tissue of adenine-fed rats showlesions in proximal and distal tubules, as well as in glomeruli (Aliet al., 2013a). In mammalian metabolism, excess adenine becomesa significant substrate for xanthine dehydrogenase (CAS serialnumber: EC 1.2.3.2), which can oxidize adenine to 2,8-dihydroxy-adenine (DHA) via an 8-hydroxyadenine intermediate(Wyngaarden and Dunn, 1957). However, the very low solubilityof DHA leads to its precipitation in kidney tubules (de Vries andSperling, 1977; Yokozawa et al., 1986). The complex inflammatoryphenomena associated with this model depend, at least in part, onNF-jB activation (Okabe et al., 2013).
Experimentally, several drugs and natural products have beenused to ameliorate the effects of adenine-induced CRF. Theseinclude gum acacia (Ali et al., 2010), fucoidan derivatives fromLaminaria japonica (Wang et al., 2012), ergone (ergosta-4, 6,8(14), 22-tetraen-3-one) (Zhao et al., 2012) and lanthanumcarbonate (Damment et al., 2011). As far as we are aware, thereis no published report on the effect of dietary charcoal onadenine-induced CRF, and this is the subject of the present inves-tigation. Since AC derivatives have been shown to be beneficial inCKD, mechanistic studies in CKD animal models are warranted.
2. Materials and methods
2.1. Animals
This project was reviewed and approved by the Animal Research Ethics Com-mittee of Sultan Qaboos University. All procedures involving animals and their carewere conducted in conformity with international laws and policies (EEC Councildirectives 86/609, OJL 358, 1 December, 12, 1987; NIH Guide for the Care andUse of Laboratory Animals, NIH Publications No. 85-23, revised 1996).
Forty-eight male Wistar rats, initially weighing 150–155 g, were obtained fromthe Sultan Qaboos University Animal House and were randomly housed in groups ofsix under standard temperature (22 ± 2 �C), humidity (50–60%) and light conditions(artificial light from 06:00 to 18:00 h). The rats had seven days to acclimatize to thenew surroundings before being treated and tested. They had free access to waterand a standard powder diet containing 0.85% phosphorus, 1.12% calcium, 0.35%magnesium, 25.3% crude protein and 2.5 IU/g vitamin D3 (Oman Flour Mills, Mus-cat, Oman).
2.2. Experimental design
After an acclimatization period, rats were randomly divided into eight equalgroups of six rats each and treated as follows: The first group continued to receivethe standard diet without treatment until the end of the study (control group). Thesecond group was switched to a diet containing adenine (0.75%, w/w, in feed) forfour weeks. The dose of adenine was chosen from our previous works (Ali et al.,2010, 2013b) based on the original method by Yokozawa et al. (1986). The third,fifth and seventh group was given standard diet mixed with charcoal at concentra-tions of 5%, 15% and 20%, w/w, for four weeks, respectively. The fourth, sixth andeighth group was given adenine in the feed together with charcoal, as in the third,fifth and seventh group, respectively.
The rats were weighed before the beginning of the treatment and weekly duringthe treatment period. At the end of the treatment period, rats were placed individ-ually in metabolic cages to collect the urine voided during 24 h. Thereafter, the ratswere anesthetized with an intraperitoneal injection of ketamine (75 mg/kg) andxylazine (5 mg/kg), and blood (about 4 mL) collected from the anterior vena cavawas placed into heparinized tubes. The blood and urine were centrifuged at 900gand 4 �C for 15 min. The plasma obtained, together with the urine specimens, werestored frozen at �80 �C pending analysis. The animals were killed by an overdose ofanesthesia, and kidneys were removed, blotted on a filter paper and weighed. Partof the left kidney was placed in formalin pending histological analysis, the rest ofthe left kidney and the right one were wrapped in aluminum foil and stored at�80 �C to await biochemical analysis within seven days. For biochemical analysis,frozen renal tissues were thawed and homogenized in ice-cold Tris buffer (pH
7.4) to give a 10%, w/v, homogenate. The latter was centrifuged at 1500g at 4 �Cfor 15 min, and the supernatant obtained was used to measure several anti-oxidantindices.
2.3. Biochemical indices of renal function
The plasma concentration of IS was measured by an HPLC method, as previouslydescribed (Al Za’abi et al., 2013), plasma phosphorus and uric acid were analyzedusing a Beckman Coulter Automated Clinical Chemistry Analyzer, synchron CX5.Plasma creatinine, urea and urinary creatinine concentrations were measured spec-trophotometrically using commercial kits, as described before (Ali et al., 2011).Neutrophil gelatinase-associated lipocalin (NGAL) concentration was measured inplasma by an ELISA method using kits obtained from Bioporto Diagnostics (Gent-ofte, Denmark). Urine osmolality was measured by the freezing point depressionmethod (�70 �C) using an osmometer (Roebling, Berlin, Germany). Vanin-1, a uri-nary biomarker of renal damage (Hosohata et al., 2011) was measured by an ELISAmethod using kits from USCN Life Sciences (Wuhan, China). The supernatants of re-nal homogenates were separated into two aliquots and were used for the measure-ment of the following parameters, using assay kits according to the manufactures’instructions: glutathione (GSH) concentration with GSH/GSSG assay kit (Biovision,Mountain View, CA, USA), total antioxidant capacity (TAC) (Randox LaboratoriesCrumlin, UK), glutathione peroxidase (GPx) (Oxis International, Inc., Foster City,CA, USA), catalase (CAT) (Cayman Chemical Co., Ann Arbor, MI, USA), and superox-ide dismutase (SOD) (Cell Technology Inc., Mountain view, CA, USA).
The protein content of the supernatant was measured by the method of Lowryet al. (1951), using bovine serum albumin as a standard and protein contents wereexpressed as mg/mL of sample. Myeloperoxidase activity was determined in thesupernatant fraction. Briefly, a sample of the renal homogenate was added to amedium containing potassium phosphate buffer (50 mM, pH 6.0), hexadecyltrime-thylammonium bromide (0.5%) and N, N, N0, N0-tetramethylbenzidine (1.5 mM).The kinetic analysis of myeloperoxidase was started after the addition of hydrogenperoxide (0.01%), and the color reaction was measured at 655 nm at 37 �C (Correiaet al., 2012). The dichlorofluoresceine fluorescence assay was used to measure cel-lular peroxide production and other reactive species (Perez-Severiano et al., 2004):aliquots of the supernatant of the kidney homogenates were added to a mediumcontaining Tris–HCl buffer (0.01 mM, pH 7.4) and dichlorofluoresceine diacetate(7 lM). After the addition of dichlorofluoresceine diacetate, the medium was incu-bated in the dark for 1 h until the fluorescence measurement (excitation at 488 nmand emission at 525 nm, with both slit widths at 1.5 nm). Oxidized dichlorofluores-ceine (DCF) was determined using a standard curve of oxidized dichlorofluoresceineand results were expressed as lmol of oxidized DCF/mg protein (Sarithakumariet al., 2013).
2.4. Renal histopathology
The kidneys were fixed in 10% neutral-buffered formalin, dehydrated in increas-ing concentrations of ethanol, cleared with xylene and embedded in paraffin. Twomicrometer sections were prepared from kidney paraffin blocks and stained withhematoxylin and eosin, periodic acid-Schiff stain (PAS) and Sirius red stain. In renaltissues, the glomerular sclerosis index (GSI) and the mesangiolysis index (MSI) wereassessed. For quantification of glomerular matrix expansion in PAS-stained kidneysections, scores of 0–4 were used, based on (Raij et al., 1984). A score of 0 indicatednormal glomerulus, a score of 1 indicated mesangial expansion or sclerosis involv-ing up to 25% of the glomerular tuft, a score of 2 indicated sclerosis 25–50%, a scoreof 3 indicated sclerosis 50–75% and/or segmental extracapillary fibrosis or prolifer-ation, and a score of 4 indicated global sclerosis (>75%) or global extracapillaryfibrosis or proliferation, or complete collapse of the glomerular tuft. In total, 50glomeruli per animal were evaluated. The MSI was determined in PAS-stained par-affin sections and graded in 50 glomeruli per animal using the following scoringsystem: score 0: no changes of capillaries, score 1: capillary dilatation <25% ofthe capillary convolute, score 2: capillary dilatation >25% of the capillary convoluteor capillary aneurysms <50% of the capillary convolute, score 3: capillary aneurysmscomprising 50–75% of the capillary convolute, score 4: capillary aneurysms com-prising >75% of the capillary convolute (Dimmler et al., 2003).
Fibrosis was separately evaluated on Sirius red-stained slides and inflammationon hematoxylin and eosin-stained slides within 40 (fibrosis) or 80–100 (inflamma-tion) visual fields using a semi-quantitative scoring ranging from 0 to 4 (grade 0: 0%fibrosis/inflammation, grade 1: <25% fibrosis/inflammation, grade 2: 25–50% fibro-sis/inflammation, grade 3: 50–75% fibrosis/inflammation, grade 4: >75% fibrosis/inflammation), as described before (Ali et al., 2013a). All microscopic scoring ofthe kidney sections was carried out in a blinded fashion.
2.5. Chemicals
Adenine and activated charcoal were obtained from Sigma (St. Louis, MO, USA)and were prepared freshly every day. Kits for measuring the various analytes wereobtained from commercial sources mentioned above. The rest of the chemicalswere of the highest purity grade available.

B.H. Ali et al. / Food and Chemical Toxicology 65 (2014) 321–328 323
2.6. Statistical analysis
Data were expressed as means ± SEM, and were analyzed with GraphPad PrismVersion 5.0 for Windows software (Graphpad Software Inc., San Diego, USA) or SPSSStatistics 20 (IBM, Ehningen, Germany). Comparisons between the eight groupswere performed by analysis of variance (ANOVA), followed by Tukey’s multiple-range tests. Values of P < 0.05 were regarded as significant.
3. Results
3.1. Body and kidney weight changes
As shown in Fig. 1, control rats grew by about 8% during the28 days of treatment. However, treatment with adenine (0.75%,w/w) for the same period resulted in a significant reduction inbody-weight (amounting to about 28%) and a significant increaseof the kidney/body weight ratio. AC treatment at concentrationsof 5%, 15% and 20%, w/w, slightly decreased the growth of the rats,but neither changed the absolute nor the relative kidney weightsignificantly when compared with the control. Concomitant treat-ment with AC and adenine mitigated, in a dose-response fashion,the adenine-induced reduction in body weight and the increasein absolute and relative kidney weight.
The general appearance of the adenine-treated rats was sub-jectively judged to be improved by AC treatment, especially at aconcentration of 20%. The kidneys from the control and AC-trea-ted rats appeared normal. However, the kidneys of adenine-treated rats were pale, and a few crystals similar to those de-scribed for adenine were seen, mainly in the cortex area (Ikedaet al., 2010; Stockelman et al., 1998). The appearance of thekidneys of rats treated with adenine plus AC (10% and 20%)was improved compared with the kidneys of rats treated withadenine alone.
Fig. 1. Effect of activated charcoal on adenine-induced weight changes. Percentage chanand kidney/body weight ratio (C) of control rats, rats treated with adenine (0.75%, w/w ifeed at concentrations of 5%, 15% or 20%, w/w, with or without adenine for 28 days. Shshown.
3.2. Water intake and urine output
Fig. 2 depicts the water intake and urine output of treated rats,which were both significantly higher in the adenine-treated ratsthan in control rats. Treatment with the three doses of AC affectedneither the water intake of rats, nor their urine output. However,simultaneous feeding of rats with adenine and AC induced adose-dependent decrease in both water intake and urine output.
3.3. Biochemical measurements
As shown in Fig. 3, adenine feeding (0.75%, w/w, for 4 weeks)caused significant increases (P < 0.001) in the concentrations ofurea and creatinine in plasma, and a significant decrease of the cre-atinine clearance (P < 0.05). Treatment with 15% and 20% AC signif-icantly abated the adenine effect. Treatment with AC alone at thethree doses did not significantly affect these three parameters.The amount of NGAL was significantly raised in plasma of rats trea-ted with adenine (P < 0.001). Simultaneous feeding of AC with ade-nine caused a dose-dependent decrease of NGAL abundance, whichwas statistically significant at a concentration of 20% (P < 0.01).
As shown in Fig. 3E, adenine treatment markedly (P < 0.01) de-creased the osmolality of urine, an action that was significantly(P < 0.01) abated by treatment with AC (20%). Given alone, AC(20%) did not cause any significant change in the urine osmolality.Treatment with adenine significantly raised the concentration ofthe urinary biomarker of renal damage, vanin-1 (P < 0.001). Thiswas significantly (P < 0.01) lowered by the treatment with AC(20%). Urine from rats treated with either saline or AC (20%) hadno detectable concentration of this biomarker (P > 0.1).
The effect of AC treatment on some antioxidant indices inkidneys from rats with adenine-induced CRF is shown in Table 1.
ge between final and initial body weight (A), absolute weights of the left kidney (B)n feed for 28 days), and in rats treated with activated charcoal (AC) mixed with theown is the mean ± SEM (n = 6 rats). Statistical differences between the groups are
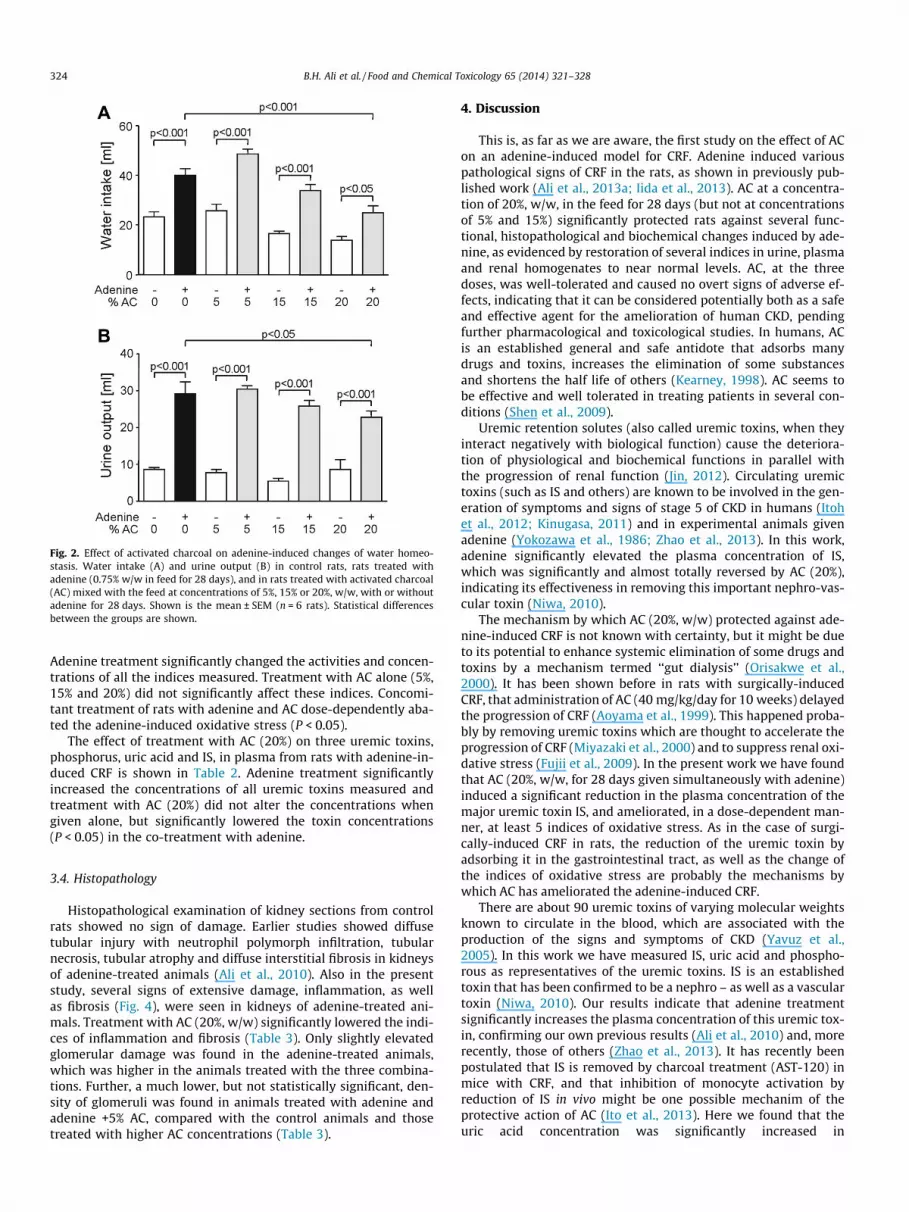
Fig. 2. Effect of activated charcoal on adenine-induced changes of water homeo-stasis. Water intake (A) and urine output (B) in control rats, rats treated withadenine (0.75% w/w in feed for 28 days), and in rats treated with activated charcoal(AC) mixed with the feed at concentrations of 5%, 15% or 20%, w/w, with or withoutadenine for 28 days. Shown is the mean ± SEM (n = 6 rats). Statistical differencesbetween the groups are shown.
324 B.H. Ali et al. / Food and Chemical Toxicology 65 (2014) 321–328
Adenine treatment significantly changed the activities and concen-trations of all the indices measured. Treatment with AC alone (5%,15% and 20%) did not significantly affect these indices. Concomi-tant treatment of rats with adenine and AC dose-dependently aba-ted the adenine-induced oxidative stress (P < 0.05).
The effect of treatment with AC (20%) on three uremic toxins,phosphorus, uric acid and IS, in plasma from rats with adenine-in-duced CRF is shown in Table 2. Adenine treatment significantlyincreased the concentrations of all uremic toxins measured andtreatment with AC (20%) did not alter the concentrations whengiven alone, but significantly lowered the toxin concentrations(P < 0.05) in the co-treatment with adenine.
3.4. Histopathology
Histopathological examination of kidney sections from controlrats showed no sign of damage. Earlier studies showed diffusetubular injury with neutrophil polymorph infiltration, tubularnecrosis, tubular atrophy and diffuse interstitial fibrosis in kidneysof adenine-treated animals (Ali et al., 2010). Also in the presentstudy, several signs of extensive damage, inflammation, as wellas fibrosis (Fig. 4), were seen in kidneys of adenine-treated ani-mals. Treatment with AC (20%, w/w) significantly lowered the indi-ces of inflammation and fibrosis (Table 3). Only slightly elevatedglomerular damage was found in the adenine-treated animals,which was higher in the animals treated with the three combina-tions. Further, a much lower, but not statistically significant, den-sity of glomeruli was found in animals treated with adenine andadenine +5% AC, compared with the control animals and thosetreated with higher AC concentrations (Table 3).
4. Discussion
This is, as far as we are aware, the first study on the effect of ACon an adenine-induced model for CRF. Adenine induced variouspathological signs of CRF in the rats, as shown in previously pub-lished work (Ali et al., 2013a; Iida et al., 2013). AC at a concentra-tion of 20%, w/w, in the feed for 28 days (but not at concentrationsof 5% and 15%) significantly protected rats against several func-tional, histopathological and biochemical changes induced by ade-nine, as evidenced by restoration of several indices in urine, plasmaand renal homogenates to near normal levels. AC, at the threedoses, was well-tolerated and caused no overt signs of adverse ef-fects, indicating that it can be considered potentially both as a safeand effective agent for the amelioration of human CKD, pendingfurther pharmacological and toxicological studies. In humans, ACis an established general and safe antidote that adsorbs manydrugs and toxins, increases the elimination of some substancesand shortens the half life of others (Kearney, 1998). AC seems tobe effective and well tolerated in treating patients in several con-ditions (Shen et al., 2009).
Uremic retention solutes (also called uremic toxins, when theyinteract negatively with biological function) cause the deteriora-tion of physiological and biochemical functions in parallel withthe progression of renal function (Jin, 2012). Circulating uremictoxins (such as IS and others) are known to be involved in the gen-eration of symptoms and signs of stage 5 of CKD in humans (Itohet al., 2012; Kinugasa, 2011) and in experimental animals givenadenine (Yokozawa et al., 1986; Zhao et al., 2013). In this work,adenine significantly elevated the plasma concentration of IS,which was significantly and almost totally reversed by AC (20%),indicating its effectiveness in removing this important nephro-vas-cular toxin (Niwa, 2010).
The mechanism by which AC (20%, w/w) protected against ade-nine-induced CRF is not known with certainty, but it might be dueto its potential to enhance systemic elimination of some drugs andtoxins by a mechanism termed ‘‘gut dialysis’’ (Orisakwe et al.,2000). It has been shown before in rats with surgically-inducedCRF, that administration of AC (40 mg/kg/day for 10 weeks) delayedthe progression of CRF (Aoyama et al., 1999). This happened proba-bly by removing uremic toxins which are thought to accelerate theprogression of CRF (Miyazaki et al., 2000) and to suppress renal oxi-dative stress (Fujii et al., 2009). In the present work we have foundthat AC (20%, w/w, for 28 days given simultaneously with adenine)induced a significant reduction in the plasma concentration of themajor uremic toxin IS, and ameliorated, in a dose-dependent man-ner, at least 5 indices of oxidative stress. As in the case of surgi-cally-induced CRF in rats, the reduction of the uremic toxin byadsorbing it in the gastrointestinal tract, as well as the change ofthe indices of oxidative stress are probably the mechanisms bywhich AC has ameliorated the adenine-induced CRF.
There are about 90 uremic toxins of varying molecular weightsknown to circulate in the blood, which are associated with theproduction of the signs and symptoms of CKD (Yavuz et al.,2005). In this work we have measured IS, uric acid and phospho-rous as representatives of the uremic toxins. IS is an establishedtoxin that has been confirmed to be a nephro – as well as a vasculartoxin (Niwa, 2010). Our results indicate that adenine treatmentsignificantly increases the plasma concentration of this uremic tox-in, confirming our own previous results (Ali et al., 2010) and, morerecently, those of others (Zhao et al., 2013). It has recently beenpostulated that IS is removed by charcoal treatment (AST-120) inmice with CRF, and that inhibition of monocyte activation byreduction of IS in vivo might be one possible mechanim of theprotective action of AC (Ito et al., 2013). Here we found that theuric acid concentration was significantly increased in

Fig. 3. Effects of activated charcoal on adenine-induced changes of kidney function parameters. Plasma urea (A), creatinine concentrations (B), creatinine clearance (C), andactivity of neutrophil gelatinase-associated lipocalin (NGAL, D) in control rats, rats treated with adenine (0.75%, w/w in feed for 28 days), and in rats treated with activatedcharcoal (AC) mixed with the feed at concentrations of 5%, 15% or 20%, w/w, with or without adenine for 28 days. Osmolality (E) and vanin-1 concentration (F) in urine of ratstreated with saline (control), adenine (0.75%, w/w in feed for 28 days), and activated charcoal (AC) mixed with the feed at a concentration of 20%, w/w, with or withoutadenine for 28 days. Shown is the mean ± SEM (n = 6 rats). Statistical differences between the groups are shown.
Table 1The effect of treatment with activated charcoal on antioxidant indices in kidneys from rats with adenine-induced chronic renal failure.
Parameter/group G1 G2 G3 G4 G5 G6 G7 G8Control ADE AC 5% ADE + AC 5% AC 15% ADE + AC 15% AC 20% ADE + AC 20%
CAT (lmol/min/mg protein) 69.7 ± 6.9 37.3 ± 0.5* 70.1 ± 9.3 48.2 ± 10.1**,# 68.9 ± 6.4 59.6 ± 5.4***,# 70.4 ± 6.6 69.5 ± 8.1#
Oxidized DCF (lmol/mg protein) 150 ± 24 600 ± 45* 154 ± 19 396 ± 67**,# 153 ± 17 240 ± 23# 151 ± 16 153 ± 15#
GPx (lmol/min �mg protein) 8.6 ± 2.1 4.6 ± 0.8* 8.7 ± 1.8 5.9 ± 1.1**,# 8.3 ± 1.3 7.1 ± 1.1***,# 8.3 ± 1.2 8.5 ± 0.9#
GSH/GSSG Ratio 6.3 ± 0.9 3.1 ± 0.8* 6.2 ± 0.8 4.2 ± 0.7 6.2 ± 0.9 5.2 ± 0.3 6.3 ± 0.7 6.3 ± 0.5#
Myeloperoxidase activity (D/min �mg protein) 212 ± 30 850 ± 60* 210 ± 22 350 ± 55# 210 ± 26 354 ± 45# 210 ± 21 356 ± 48#
SOD (lmol/min �mg protein) 39.8 ± 7.4 17.5 ± 1.9* 40.4 ± 6.3 25.7 ± 9.4**,# 38.8 ± 3.7 31.6 ± 4.1***,# 39.1 ± 4.6 39.8 ± 7.4#
TAC (% Control) 100 ± 0 60.9 ± 3.9* 90.3 ± 2.4 63.5 ± 5.0** 89.6 ± 2.4 77.4 ± 8.1 97.3 ± 6.5 95.0 ± 4.7#
Adenine (ADE) was added to the feed at a concentration of 0.75%, w/w, for 4 weeks, and activate charcoal (AC, either alone or with ADE) was given in feed at 5%, 15% or 20%, w/w. CAT = catalase, DCF = dichlorodihydrofluoresceine; GPx = glutathione peroxidase, GSH = reduced glutathione; GSSG = glutathione disulfide; SOD = superoxide dismutase;TAC = total anti-oxidant capacity. Values in the table are mean ± SEM (n = 6). ^ P < 0.05 (G8 versus G7).* P < 0.05 (G2 versus G1).** P < 0.05 (G4 versus G3).*** P < 0.05 (G6 versus G5).
# P < 0.05 (G4, G6 and G8 versus G2).
B.H. Ali et al. / Food and Chemical Toxicology 65 (2014) 321–328 325
adenine-treated rats, and this rise was significantly blunted in ratstreated with AC (20%). After the completion of this work, a studywas published suggesting that kidney damage in adenine-fed ratsmay be initiated by increased plasma uric acid levels (Diwanet al., 2013). Uric acid plays a major role in the pathogenesis of re-nal and cardiac damage, an effect that was significantly reverted bythe xanthine oxidase inhibitor allopurinol.
Phosphorus is considered a uremic toxin as it contributes toseveral metabolic disturbances that include hyperparathyroidism,vitamin D resistance, hypocalcemia, and damage to several organs,such as the parathyroid glands, bones, and, most importantly, thecardiovascular system, arterial and valvular calcification, arterio-sclerosis, and an increased risk of cardiovascular death (Burke,2008). In this work, we confirmed that adenine induced a

Table 2Effect of treatment with activated charcoal on the amount of uremic toxins in plasma from adenine-treated rats.
Uremic toxins/group G1 G2 G7 G8Control ADE AC 20% ADE + AC 20%
Phosphorus (mmol/l) 0.54 ± 0.02 1.23 ± 0.04* 0.60 ± 0.02 0.68 ± 0.07#
Uric acid (mg/dl) 1.96 ± 0.07 5.66 ± 0.12* 1.90 ± 0.05 3.01 ± 0.09*,#
Indoxyl sulfate (lM) 1.79 ± 0.81 159.55 ± 0.43* 0.685 ± 0.43 13.844 ± 1.61#
Adenine (ADE) was added to the feed at a concentration of 0.75%, w/w, for 4 weeks, and AC (either alone or with ADE) was given in feed at a concentration of 20%, w/w. Valuesin the table are mean ± SEM (n = 6).* P < 0.05 (G2, G7 or G8 versus G1).
# P < 0.05 (G7 or G8 versus G2).
Fig. 4. Effect of activated charcoal on adenine-induced morphological changes in the kidney. Representative pictures of kidney slices of the control group, the adenine groupand the adenine plus 20%, w/w, activated charcoal (AC) group used for semi-quantitative scoring of inflammation and fibrosis. (A) H&E staining used for the identification andsemi-quantitative scoring of inflammation. The black arrows point to infiltrated leucocytes (100-fold magnification). (B) Sirius-red staining, used for the identification andsemi-quantitative scoring of fibrosis. The black arrows point to collagen deposition, characteristic for fibrosis (100-fold magnification).
Table 3Effect of treatment of activated charcoal on histopathological parameters in adenine-treated rat kidneys.
Index/group G1 G2 G3 G4 G5 G6 G7 G8Control ADE AC 5% ADE + AC 5% AC 15% ADE + AC 15% AC 20% ADE + AC 20%
GSI 0.72 ± 0.09 0.74 ± 0.10 0.77 ± 0.02 1.08 ± 0.14 1.37 ± 0.05*.# 1.25 ± 0.08*,# 0.65 ± 0.05 0.89 ± 0.08Glomeruli per mm2 5.41 ± 0.33 3.75 ± 0.41 3.53 ± 0.44 7.78 ± 1.42 7.14 ± 0.65MSI 0.42 ± 0.05 1.08 ± 0.05* 1.60 ± 0.11*,# 0.70 ± 0.06**,# 0.92 ± 0.08*,# 1.21 ± 0.06* 0.36 ± 0.04# 1.11 ± 0.07*,^
Fibrosis 0.08 ± 0.03 2.38 ± 0.07* 0.70 ± 0.06*,# 2.44 ± 0.10*,** 0.77 ± 0.07*,# 2.56 ± 0.06*,*** 0.23 ± 0.03# 1.47 ± 0.08*,^,#
Inflammation 0.01 ± 0.01 2.41 ± 0.05* 0.25 ± 0.05* 1.35 ± 0.12*,**,# 0.02 ± 0.01* 2.38 ± 0.10*,*** 0.04 ± 0.02# 0.56 ± 0.08*,^,#
Adenine (ADE) was added to the feed at a concentration of 0.75%, w/w, for 4 weeks, and AC (either alone or with ADE) was given in feed at 5%, 15% or 20%, w/w.GSI = glomerular sclerosis index; MSI = mesangiolysis index. Values in the table are mean ± SEM (n = 6).* P < 0.05 (G2-8 versus G1).** P < 0.05 (G4 versus G3).*** P < 0.05 (G6 versus G5).
^ P < 0.05 (G8 versus G7).# P < 0.05 (G3–G8 versus G2).
326 B.H. Ali et al. / Food and Chemical Toxicology 65 (2014) 321–328
significant hyperphosphatemia in treated rats. Activated AC causeda dose-dependent reversal of this action, confirming the usefulnessof AC in mitigating the damaging effect of adenine.
In addition to the conventional renal function tests (such asurea and creatinine), we also used in this study some sensitive bio-markers to assess the possible effect of adenine and AC on the renalfunction of rats. In this experiment, we also measured the activityof the tubular injury marker NGAL in the plasma of rats, and foundit significantly elevated in adenine-treated rats. AC produced adose-dependent blunting of this action in rats treated with
adenine, which was statistically significant at a concentration of20% of AC. NGAL is customarily considered a sensitive marker ofacute renal failure (Waring and Moonie, 2011), and has not, asfar as we are aware, been used as a marker of CRF in rats, buthas been shown, in a single report, to increase in patients withchronic renal failure (Emans et al., 2012). We also used urinary va-nin-1 concentration here as a urinary biomarker of adenine-in-duced CRF. It has been shown by several authors that urinaryvanin-1 is a useful and rapid biomarker in several models of acuterenal failure (Hosohata et al., 2011).

B.H. Ali et al. / Food and Chemical Toxicology 65 (2014) 321–328 327
The histopathology parameters obtained from the kidneys ofadenine-treated rats were suggestive of significant damage,inflammation and fibrosis. Treatment with AC (20%) significantlyabrogated the damage, while the lower concentrations showedno ameliorative effect at all. Interestingly, the two lower AC con-centrations alone led to adverse effects in the kidney, with the5% concentration causing the highest damage. Glomerular damagewas not as high as expected from our former study (Ali et al.,2013a). Strikingly, we remarked a potential loss of glomeruli inthe adenine-treated animals, as well as in those treated with ade-nine together with 5% AC. Only approximately half of the glomerulicounted in control animals or animals treated with the higher ACconcentrations were found in the two groups. The remainingglomeruli did not show extensive signs of sclerosis or mesangioly-sis. The fibrosis and inflammation indices on the other hand weresimilar to our last study (Ali et al., 2013a). Comparing the effect ofAC and the substance used in this last study, gum Arabic, on thehistopathological parameters, gum Arabic had a higher anti-fibro-tic effect than AC, while AC has a higher anti-inflammatory effect.
5. Conclusion
This work shows that simultaneous treatment of rats with ade-nine and AC (20%, w/w, in the feed for 28 days) produced a broad,dose-dependent, nephro-protective action in adenine-induced CRF.The use of 20% AC alone was without any overt adverse effects onthe treated animals. The protective mechanism of AC appears to bethrough its adsorption of uremic toxins and also its antioxidanteffect.
The adsorbent AC has been very commonly employed in humanand veterinary medicine for years as a general antidote for a num-ber of toxicities (Osterhoudt et al., 2004) and also more recently inthe treatment of renal failure (Schulman et al., 2006). The use ofthe relatively inexpensive AC as a palliative treatment in acute re-nal failure and CKD offers great therapeutic and economic advan-tage, especially in the poor developing countries in which theincidence and prevalence of renal diseases is on the rise (Secket al., 2013), and this adds to the relevance of experimental studieson the mechanism of AC in a CRF model (such as in this work) toclinical research. In this work, AC was given simultaneously withadenine to see if AC would prevent the development of CRF.Further experiments in which AC is given after the establishmentof CRF are warranted in order to find out if it can also be used toameliorate the condition.
Conflict of Interest
The authors declare that there are no conflicts of interest.Transparency documents associated with this article can be
found, in the online version, at http://dx.doi.org/10.1016/j.fct.2013.12.038.
Acknowledgement
This work was financially supported by a grant from TheResearch Council of Oman (RC/Med/Phar/10/01). We thank thestaff of the Animal House of SQU for caring for the rats.
References
Al Za’abi, M., Ali, B., Al Toubi, M., 2013. HPLC-fluorescence method for measurementof the uremic toxin indoxyl sulfate in plasma. J. Chromatogr. Sci. 51, 40–43.
Ali, B.H., Abdelrahman, A.M., Al-Salam, S., Sudhadevi, M., AlMahruqi, A.S., Al-Husseni, I.S., Beegam, S., Dhanasekaran, S., Nemmar, A., Al-Moundhri, M., 2011.
The effect of sildenafil on cisplatin nephrotoxicity in rats. Basic Clin. Pharmacol.Toxicol. 109, 300–308.
Ali, B.H., Al-Husseni, I., Beegam, S., Al-Shukaili, A., Nemmar, A., Schierling, S., Queisser,N., Schupp, N., 2013a. Effect of gum Arabic on oxidative stress and inflammation inadenine-induced chronic renal failure in rats. PLoS ONE 8, e55242.
Ali, B.H., Al-Salam, S., Al Husseni, I., Kayed, R.R., Al-Masroori, N., Al-Harthi, T., AlZaabi, M., Nemmar, A., 2010. Effects of Gum Arabic in rats with adenine-inducedchronic renal failure. Exp. Biol. Med. (Maywood, NJ) 235, 373–382.
Ali, B.H., Al-Salam, S., Al Za’abi, M., Waly, M.I., Ramkumar, A., Beegam, S., Al-Lawati,I., Adham, S.A., Nemmar, A., 2013b. New model for adenine-induced chronicrenal failure in mice, and the effect of gum acacia treatment thereon:comparison with rats. J. Pharmacol. Toxicol. Methods 68, 384–393.
Aoyama, I., Miyazaki, T., Niwa, T., 1999. Preventive effects of an oral sorbent onnephropathy in rats. Miner. Electrolyte Metab. 25, 365–372.
Ash, S.R., 2009. Sorbents in treatment of uremia: a short history and a great future.Semin. Dial. 22, 615–622.
Burke, S.K., 2008. Phosphate is a uremic toxin. J. Ren. Nutr. 18, 27–32.Cooney, D.O., 1995. Activated Charcoal in Medical Applications. Marcel Dekker, New
York.Correia, R.T., Borges, K.C., Medeiros, M.F., Genovese, M.I., 2012. Bioactive
compounds and phenolic-linked functionality of powdered tropical fruitresidues. Food Sci. Technol. Int. = Ciencia y tecnologia de los alimentosinternacional 18, 539–547.
Damment, S., Secker, R., Shen, V., Lorenzo, V., Rodriguez, M., 2011. Long-termtreatment with lanthanum carbonate reduces mineral and bone abnormalitiesin rats with chronic renal failure. Nephrol. Dial. Transplant. 26, 1803–1812.
de Vries, A., Sperling, O., 1977. Implications of disorders of purine metabolism forthe kidney and the urinary tract. Ciba Found. Symp., 179–206.
Dimmler, A., Haas, C.S., Cho, S., Hattler, M., Forster, C., Peters, H., Schocklmann, H.O.,Amann, K., 2003. Laser capture microdissection and real-time PCR for analysisof glomerular endothelin-1 gene expression in mesangiolysis of rat anti-Thy 1.1and murine Habu Snake Venom glomerulonephritis. Diagn. Mol. Pathol. 12,108–117.
Diwan, V., Mistry, A., Gobe, G., Brown, L., 2013. Adenine-induced chronic kidney andcardiovascular damage in rats. J. Pharmacol. Toxicol. Methods. http://dx.doi.org/10.1016/j.vascn.2013.05.006.
Emans, M.E., Braam, B., Diepenbroek, A., van der Putten, K., Cramer, M.J., Wielders,J.P., Swinkels, D.W., Doevendans, P.A., Gaillard, C.A., 2012. Neutrophilgelatinase-associated lipocalin (NGAL) in chronic cardiorenal failure iscorrelated with endogenous erythropoietin levels and decreases in responseto low-dose erythropoietin treatment. Kidney Blood Pressure Res. 36, 344–354.
Fujii, H., Nishijima, F., Goto, S., Sugano, M., Yamato, H., Kitazawa, R., Kitazawa, S.,Fukagawa, M., 2009. Oral charcoal adsorbent (AST-120) prevents progression ofcardiac damage in chronic kidney disease through suppression of oxidativestress. Nephrol. Dial. Transplant. 24, 2089–2095.
Hosohata, K., Ando, H., Fujiwara, Y., Fujimura, A., 2011. Vanin-1: a potentialbiomarker for nephrotoxicant-induced renal injury. Toxicology 290, 82–88.
Iida, A., Kemmochi, Y., Kakimoto, K., Tanimoto, M., Mimura, T., Shinozaki, Y.,Uemura, A., Matsuo, A., Matsushita, M., Miyamoto, K., 2013. Ferric citratehydrate, a new phosphate binder, prevents the complications of secondaryhyperparathyroidism and vascular calcification. Am. J. Nephrol. 37, 346–358.
Ikeda, R., Imai, Y., Maruyama, W., Mizoguchi, K., 2010. Systemic disorders of calciumdynamics in rats with adenine-induced renal failure: implication for chronickidney disease-related complications. Nephrology (Carlton Vic) 15, 54–62.
Ito, S., Higuchi, Y., Yagi, Y., Nishijima, F., Yamato, H., Ishii, H., Osaka, M., Yoshida, M.,2013. Reduction of indoxyl sulfate by AST-120 attenuates monocyteinflammation related to chronic kidney disease. J. Leukoc. Biol. 93, 837–845.
Itoh, Y., Ezawa, A., Kikuchi, K., Tsuruta, Y., Niwa, T., 2012. Protein-bound uremictoxins in hemodialysis patients measured by liquid chromatography/tandemmass spectrometry and their effects on endothelial ROS production. Anal.Bioanal. Chem. 403, 1841–1850.
Jin, K., 2012. Effects of amino acids and albumin on erythropoietin carbamoylation.Clin. Exp. Nephrol. http://dx.doi.org/10.1007/s10157-012-0751-y.
Kearney, T.E., 1998. Charcoal, activated. In: Olson, K.R. (Ed.), Poisoning & DrugOverdose, third ed. Appleton & Lange, pp. 351–353.
Kinugasa, E., 2011. Markers and possible uremic toxins: Japanese experiences.Contrib. Nephrol. 168, 134–138.
Lowry, O.H., Rosebrough, N.J., Farr, A.L., Randall, R.J., 1951. Protein measurementwith the Folin phenol reagent. J. Biol. Chem. 193, 265–275.
Miyazaki, T., Aoyama, I., Ise, M., Seo, H., Niwa, T., 2000. An oral sorbent reducesoverload of indoxyl sulphate and gene expression of TGF-beta1 in uraemic ratkidneys. Nephrol. Dial. Transplant. 15, 1773–1781.
Musso, C.G., Michelangelo, H., Reynaldi, J., Martinez, B., Vidal, F., Quevedo, M., Parot,M., Waisman, G., Algranati, L., 2010. Combination of oral activated charcoal pluslow protein diet as a new alternative for handling in the old end-stage renaldisease patients. Saudi J. Kidney Dis. Transpl. 21, 102–104.
Niwa, T., 2010. Indoxyl sulfate is a nephro-vascular toxin. J. Ren. Nutr. 20, S2-S6.Okabe, C., Borges, R.L., de Almeida, D.C., Fanelli, C., Barlette, G.P., Machado, F.G.,
Arias, S.C., Malheiros, D.M., Camara, N.O., Zatz, R., Fujihara, C.K., 2013. NF-kappaB activation mediates crystal translocation and interstitial inflammationin adenine overload nephropathy. Am. J. Physiol. Renal. Physiol. 305, F155-F163.
Olson, K.R., 2010. Activated charcoal for acute poisoning: one toxicologist’s journey.J. Med. Toxicol. 6, 190–198.
Orisakwe, O.E., Ilondu, N.A., Afonne, O.J., Ofoefule, S.I., Orish, C.N., 2000. Accelerationof body clearance of diethylCarbamazine by oral activated charcoal. Pharmacol.Res. 42, 167–170.
328 B.H. Ali et al. / Food and Chemical Toxicology 65 (2014) 321–328
Osterhoudt, K.C., Alpern, E.R., Durbin, D., Nadel, F., Henretig, F.M., 2004. Activatedcharcoal administration in a pediatric emergency department. Pediatr. Emerg.Care 20, 493–498.
Perez-Severiano, F., Salvatierra-Sanchez, R., Rodriguez-Perez, M., Cuevas-Martinez,E.Y., Guevara, J., Limon, D., Maldonado, P.D., Medina-Campos, O.N., Pedraza-Chaverri, J., Santamaria, A., 2004. S-Allylcysteine prevents amyloid-betapeptide-induced oxidative stress in rat hippocampus and ameliorates learningdeficits. Eur. J. Pharmacol. 489, 197–202.
Raij, L., Azar, S., Keane, W., 1984. Mesangial immune injury, hypertension, andprogressive glomerular damage in Dahl rats. Kidney Int. 26, 137–143.
Sarithakumari, C.H., Renju, G.L., Kurup, G.M., 2013. Anti-inflammatory andantioxidant potential of alginic acid isolated from the marine algae, Sargassumwightii on adjuvant-induced arthritic rats. Inflammopharmacology 21, 261–268.
Schulman, G., 2012. A nexus of progression of chronic kidney disease: tryptophan,profibrotic cytokines, and charcoal. J. Ren. Nutr. 22, 107–113.
Schulman, G., Agarwal, R., Acharya, M., Berl, T., Blumenthal, S., Kopyt, N., 2006. Amulticenter, randomized, double-blind, placebo-controlled, dose-ranging studyof AST-120 (Kremezin) in patients with moderate to severe CKD. Am. J. KidneyDis. 47, 565–577.
Seck, S.M., Gueye, S., Tamba, K., Ba, I., 2013. Prevalence of chronic cardiovascularand metabolic diseases in Senegalese workers: a cross-sectional study, 2010.Prevent. Chronic Dis. 10, 110339.
Shen, B., Pardi, D.S., Bennett, A.E., Queener, E., Kammer, P., Hammel, J.P., LaPlaca, C.,Harris, M.S., 2009. The efficacy and tolerability of AST-120 (spherical carbonadsorbent) in active pouchitis. Am. J. Gastroenterol. 104, 1468–1474.
Stockelman, M.G., Lorenz, J.N., Smith, F.N., Boivin, G.P., Sahota, A., Tischfield, J.A.,Stambrook, P.J., 1998. Chronic renal failure in a mouse model of human adeninephosphoribosyltransferase deficiency. Am. J. Physiol. 275, F154-F163.
Vaziri, N.D., Yuan, J., Khazaeli, M., Masuda, Y., Ichii, H., Liu, S., 2013. Oral activatedcharcoal adsorbent (AST-120) ameliorates chronic kidney disease-inducedintestinal epithelial barrier disruption. Am. J. Nephrol. 37, 518–525.
Wang, J., Wang, F., Yun, H., Zhang, H., Zhang, Q., 2012. Effect and mechanism offucoidan derivatives from Laminaria japonica in experimental adenine-inducedchronic kidney disease. J. Ethnopharmacol. 139, 807–813.
Waring, W.S., Moonie, A., 2011. Earlier recognition of nephrotoxicity using novelbiomarkers of acute kidney injury. Clin. Toxicol. (Philadelphia Pa) 49, 720–728.
Winchester, J.F., Ronco, C., 2010. Sorbent augmented hemodialysis systems: are wethere yet? J. Am. Soc. Nephrol. 21, 209–211.
Wyngaarden, J.B., Dunn, J.T., 1957. 8-Hydroxyadenine as the intermediate in theoxidation of adenine to 2, 8-dihydroxyadenine by xanthine oxidase. Arch.Biochem. Biophys. 70, 150–156.
Yamamoto, S., Zuo, Y., Ma, J., Yancey, P.G., Hunley, T.E., Motojima, M., Fogo, A.B.,Linton, M.F., Fazio, S., Ichikawa, I., Kon, V., 2011. Oral activated charcoaladsorbent (AST-120) ameliorates extent and instability of atherosclerosisaccelerated by kidney disease in apolipoprotein E-deficient mice. Nephrol.Dial. Transplant. 26, 2491–2497.
Yavuz, A., Tetta, C., Ersoy, F.F., D’Intini, V., Ratanarat, R., De Cal, M., Bonello, M.,Bordoni, V., Salvatori, G., Andrikos, E., Yakupoglu, G., Levin, N.W., Ronco, C.,2005. Uremic toxins: a new focus on an old subject. Semin. Dial. 18, 203–211.
Yokozawa, T., Zheng, P.D., Oura, H., Koizumi, F., 1986. Animal model of adenine-induced chronic renal failure in rats. Nephron 44, 230–234.
Zhao, Y.Y., Cheng, X.L., Cui, J.H., Yan, X.R., Wei, F., Bai, X., Lin, R.C., 2012. Effect ofergosta-4,6,8(14),22-tetraen-3-one (ergone) on adenine-induced chronic renalfailure rat: a serum metabonomic study based on ultra performance liquidchromatography/high-sensitivity mass spectrometry coupled with MassLynx i-FIT algorithm. Clin. Chim. Acta; Int. J. Clin. Chem. 413, 1438–1445.
Zhao, Y.Y., Cheng, X.L., Wei, F., Bai, X., Tan, X.J., Lin, R.C., Mei, Q., 2013. Intrarenalmetabolomic investigation of chronic kidney disease and its TGF-beta1mechanism in induced-adenine rats using UPLC Q-TOF/HSMS/MS(E).J. Proteome Res. 12, 692–703.





























