Embed Size (px)
Citation preview

Effect of treatment with dornase alpha on airway inflammation in cystic fibrosis
patients
Karl Paul1*
, Ernst Rietschel 2*, Manfred Ballmann3*, Matthias Griese4*, Dieter
Worlitzsch5, Janis Shute6, Christiane Chen1, Tanja Schink7 Gerd Döring 5, Silke van
Koningsbruggen2, Ulrich Wahn1, Felix Ratjen8* for the BEAT Study Group
1
Department of Pediatric Pneumology and Immunology, Charité, Humboldt-
University, Berlin, Germany; 2
Department of Pediatric Pneumology and Allergology,
Children´s Hospital, University of Cologne, Germany; 3
Department of Pediatric
Pneumology, Medical School, University of Hannover, Germany; 4
Children´s Hospital, University of Munich, Germany,
5Institute of General and Environmental
Hygiene, University of Tübingen, Germany; 6 School of Pharmacy and Biomedical
Sciences, University of Portsmouth, UK; 7Department of Medical Biometry,
Humboldt-University, Berlin, Germany; 8Children´s Hospital, University of Essen, Germany
*Manfred Ballmann, Matthias Griese, Karl Paul, Felix Ratjen and Ernst Rietschel are
the principal investigators of the BEAT study centers
Address for correspondence:
Prof. Dr. Felix Ratjen Children’s Hospital University of Essen Hufelandstr. 55, D-45122 Essen, Germany Phone: +492017233350 Fax: +492017232352 e-mail: [email protected]
Influence of rhDNase on airway inflammation
Key words: rhDNase, bronchoalveolar lavage, cystic fibrosis, airway inflammation,
lung function
Subject category list: 102
Copyright (C) 2003 by the American Thoracic Society.
AJRCCM Articles in Press. Published on December 18, 2003 as doi:10.1164/rccm.200307-959OC

12/12/2003 2
A B S T R A C T
RhDNase has been shown to improve lung function and reduce the number of
pulmonary exacerbations in patients with cystic fibrosis (CF), but its long term effect
on airway inflammation remains unknown. In this study we used bronchoalveolar
lavage (BAL) to investigate the long-term effect of rhDNase on inflammation in CF
patients with mild lung disease. 105 CF patients > 5 years of age with normal lung
function were randomized to receive rhDNase (2.5 mg/day) or no rhDNase. Patients
with a normal percentage of neutrophils in BAL fluid at baseline were not randomized
and served as a control group. The percentage of neutrophils in the pooled BAL
sample was similar in both randomized groups at baseline: A significant increase in
neutrophils was observed over the 3 year study period in both untreated patients and
controls, whereas neutrophils remained unchanged in patients treated with rhDNase.
Elastase activities and IL-8 concentrations also increased in untreated patients and
remained stable in patients on rhDNase. We conclude that an increase in neutrophilic
airway inflammation is found in patients with cystic fibrosis that is positively
influenced by rhDNase treatment.
183 words

12/12/2003 3
I N T R O D U C T I O N
Cystic fibrosis is caused by mutations in the cystic fibrosis transmembrane regulator
(CFTR) gene which encodes a protein that functions as a chloride channel in
epithelial membranes. The disease is characterized by depletion of the periciliary
liquid layer of bronchial epithelial cells that impairs mucociliary transport with
retention of thick and viscid mucus that is subsequently invaded by bacterial
pathogens [1,2]. The persistent bacterial infections lead to a massive neutrophil
dominated host response with high levels of the pro-inflammatory cytokine IL 8 and
the release of neutrophil granule enzymes such as elastase and myeloperoxidase [3-
5]. With the use of bronchoalveolar lavage (BAL) neutrophil dominated airway
inflammation has been shown to be present very early in the course of the disease
and in stable patients with few clinical symptoms [6-8]. Due to the invasiveness of the
technique, most of these studies have been performed cross-sectionally and there is
only limited information available on the natural course of this inflammatory response
in CF patients.
Invading neutrophils disintegrate during the inflammatory response and release large
amounts of intracellular DNA that contributes to the viscid airway secretions in CF
patients [9]. Recombinant human DNase (rhDNase) has been shown to reduce
sputum viscosity, improve pulmonary function and reduce the number of pulmonary
exacerbations in patients with moderate lung disease (10-12). Similar effects have
also been demonstrated in patients with mild disease making rhDNase the only
mucolytic with proven efficacy in CF (12,13). However, studies using spontaneously
expectorated sputum have raised concerns that rhDNase may increase airway
inflammation by releasing pro-inflammatory cytokines such as IL-8 that are bound to

12/12/2003 4
DNA in airway secretions (14,15). This may only be a short lived effect, since a
subsequent study was unable to demonstrate a reproducible effect of rhDNase on IL-
8 concentrations (16). Currently there are no data available on the long term effect of
rhDNase on lower airway inflammation in CF. Given the positive effects on both
airway clearance and frequency of pulmonary exacerbations, rhDNase could also
exhibit an anti-inflammatory effect in CF airways. To further define the natural
evolution of airway inflammation in CF and to assess the effect of rhDNase on this
inflammatory process, we have studied lower airway inflammation over a 3 year
period using bronchoalveolar lavage (BAL) in a cohort of CF patients with mild lung
disease. Some of the results of this study have been previously reported in form of
abstracts (17,18).

12/12/2003 5
M A T E R I A L S A N D M E T H O D S
105 patients ( 53 female) aged 5 to 37 years (mean age ± SD: 11.8 ± 5.4 years)
were recruited at the 5 participating centers (Berlin, Cologne, Essen, Hanover and
Munich). Only 10 of these patients were older than 15 years of age. The diagnosis of
CF had been confirmed by repeated sweat test with chloride concentrations
exceeding 60 mmol/l and/or CFTR mutation analysis. Patients were eligible for this
study, if they were able to perform lung function tests, had normal lung function
defined as a FEV1 > 80% predicted and were clinically stable. Exclusion criteria were
(1) the use of anti-inflammatory treatment (Ibuprofen, systemic or inhaled
corticosteroids and α1-antitrypsin) (2) a modified Shwachman-score not including x-
rays < 55 points (3) allergic bronchopulmonary aspergillosis and (4) other severe
organ involvement such as advanced hepatic disease. All patients had to be free of
acute respiratory tract infections prior to bronchoscopy for at least 6 weeks. The
study was approved by the local ethic committees of all participating centers. Written
informed consent by both parents and /or the patients was obtained in all cases.
Flexible fiberoptic bronchoscopy and bronchoalveolar lavage were performed at
baseline, after 18 and 36 months respectively. Onsite visits by one investigator (F.R)
were performed for the first procedure to ensure that the same approach was used in
every center. The bronchoscope was wedged in the lingula or one of its segments in
all patients. The same segment/subsegment was lavaged on all three occasions in
every patient BAL was performed as described before in the report of the baseline
data for this study(19,20). The laboratory personnel performing the BAL fluid
analysis was blinded to the patient’s treatment. The first aliquot of the recovered BAL
12/12/2003 6
fluid was treated separately; all other samples were pooled for analysis. The total cell
count was measured by a hemocytometer, the differential cell count of the BAL by
cytocentrifugation at the different sites. Bacterial cultures were performed from the
first BAL aliquot.
Total IL-8 was measured in duplicate in pooled BAL samples using a commercially
available enzyme-linked immunosorbent assay kit (Pelikine kit; Eurogenetics, Hamp-
ton, UK)[20,21]. The sensitivity of the assay is 1pg/ml, and a standard curve was
prepared in the range 1-240 pg/ml. Samples were diluted as appropriate (usually
1:50) in phosphate buffered saline. The intra assay and inter assay variation are both
less than 10%.
Quantification of neutrophil enzyme activities. The myeloperoxidase (MPO) catalyzed
oxidation of guaiacol to tetraguaiacol in the presence of H2O2 was used to quantify
MPO activity in pooled BAL samples of CF patients [22,23]. The reaction was fol-
lowed at 470 nm (Ultrospec III, Pharmacia Biotech GmbH, Freiburg, Germany). One
MPO unit was defined as the consumption of 1 µmol of H2O2 per minute. The detec-
tion limit was 0.02 units. Neutrophil elastase (NE) activity was investigated photomet-
rically at 410 nm using the peptide MeOSuc-Ala-Ala-Pro-Val-p-nitroanilide (Bachem,
Heidelberg, Germany) as specific chromogenic substrate. One unit was defined as
the release of 1 µmol p-nitroanilide/min/ml using the extinction coefficient ε410nm =
8800 M-1cm-1 [23,24]. The detection limit was 0.2 units. Measurements for both en-
zymes were performed 6 times, results were expressed as mean values of 6-fold
measurements.
Patients < 8 years with a relative neutrophil count > 10 % and patients > 8 years with

12/12/2003 7
a relative neutrophil count > 5 % in pooled BAL fluid were randomized to 2.5 mg
rhDNase once daily (n=46) or no rhDNase (n=39). A higher cutoff level was used for
younger children, since we found a higher percentage of neutrophils in children < 8
years in our previous study on children without lung disease (19). Patients with a
lower percentage of neutrophils (n=20) were not randomized and followed as a
control group. Patients were routinely evaluated clinically every 3 months during the 3
year period.
Stastistical analysis:
Statistical analysis was done with SPSS release 11.0.1 and SAS release 8.02. The
primary outcome variables of this study were the change in the percentage of
neutrophils, Il-8 and neutrophil elastase in pooled BAL samples within the 3 year
period. Nonparametric repeated-measures analyses of variance were used to take
into account the correlated nature of repeated measurements. For comparison of
different treatment groups we performed a two-factorial analysis for each variable,
with group and time point as factors [25]. For the detection of decreasing or
increasing trends over time statistics for patterned time effects were computed. A p
level of < 0.05 was considered statistically significant.

12/12/2003 8
R E S U L T S
105 patients underwent the first BAL; 46 were randomized to rhDNase treatment, 39
to no treatment; 20 patients were not randomized due to a low percentage of
neutrophils in BAL fluid. Of the 46 patients treated with rhDNase 43 underwent the
second procedure at 18 months and 24 patients the third BAL at 36 months. 39
patients were randomized to no treatment of whom 33 and 24 underwent the second
and third BAL, respectively. The corresponding numbers for the 20 untreated patients
with a low percentage of neutrophils are 16 and 12, respectively. The reason for early
termination in these cases was unwillingness to undergo repeat BAL’s in all cases.
There was no statistically significant difference in the rate of dropout between the
groups. There were also no differences in FEV1 after 18 and 36 months in all 3
groups between patients continuing the study and patients who dropped out.
Total cell counts of BAL fluid were highly variable and did not change significantly
over time in the 3 groups. The percentage of neutrophils in pooled BAL samples were
similar at baseline in both randomized groups and significantly increased over time in
both untreated patients and controls (p < 0.02) (Fig. 1). There was no detectable age
effect, but numbers were too small for older patients to perform a meaningful
statistical analysis. No change in the percentage of neutrophils was observed in
patients treated with rhDNase (Fig. 1). The variability in the annual change of the
percentage of neutrophils in the 2 randomized groups is shown in Fig. 2.
In contrast to the findings in pooled BAL samples, the percentage of neutrophils of
the first syringe of BAL increased significantly over time in all groups, although the
increase was more pronounced in untreated patients (p< 0.01 for patients treated

12/12/2003 9
with rhDNase, p< 0.005 for untreated patients for the percentage of neutrophils) (Fig.
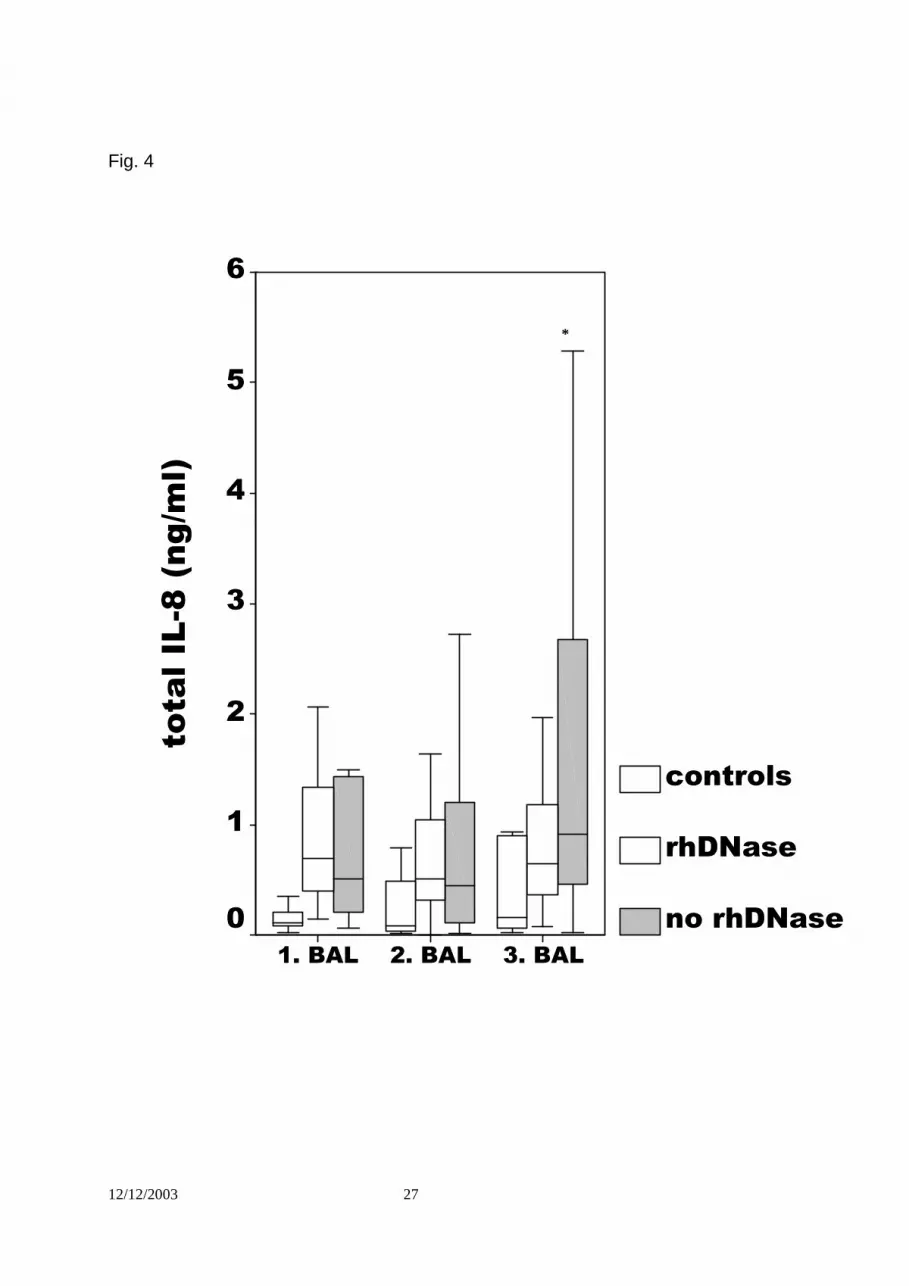
3). Total IL 8 concentrations increased in untreated patients (p < 0.02) and remained
stable in patients treated with rhDNase (p = 0.58) and controls (p = 0.09) (Fig. 4).
Similar results were obtained for free elastase activity in BAL fluid that increased in
untreated CF patients (p< p<0.007), while it remained stable in rhDNase treated
patients and controls (Fig. 5). A similar trend was observed for MPO that failed to
reach statistical significance (Fig. 6).
Concomitant therapy was not statistically different between the 3 groups (data not
shown). Chest physiotherapy was routinely performed in all patients, approximately
85 % of patients received inhaled albuterol in both groups. Macrolides were only al-
lowed for short treatment periods (2-4 weeks). There were no significant difference in
the number of antibiotic courses (oral, intravenous or inhaled) between the 2 random-
ized groups.
The results of bacterial cultures from BAL fluid are displayed in Table 2: No
significant differences were observed between patients randomized to either
rhDNase versus no rhDNase treatment, whereas control subjects had a lower rate of
negative BAL fluid cultures at baseline.
BAL was well tolerated in all but one patient who developed fever and dyspnea in the
first 24 hours that required hospitalization, but resolved within 48 hours. No severe
side-effects of the BAL were noted.
This study was not designed to assess the effect of rhDNase treatment on lung
function and no significant differences were observed in the evolution of lung function

12/12/2003 10
parameters over the 3 year period. A significant decline in FEV1 was observed in the
2 randomized groups (p = 0.001 for patients treated with rhDNase and p = 0.0003 for
untreated patients). whereas the control group with a normal percentage of
neutrophils in the pooled BAL fluid sample did not show any significant decline over
the 3 year period (p = 0.07) (Fig.7). Similar results were obtained, when the analysis
was limited to patients homozygous for DF508 (data not shown). The median annual
rate of decline for the total study population was –2.12 % in controls, - 1.99 % in
rhDNase treated patients and -3.26 % in untreated patients. Although not statistically
different, the rate of decline was highest in untreated patients. MEF25/75 % VC
significantly decreased in both randomized patient groups (p < 0.01) whereas no
change was observed in controls (p = 0.51) (Fig. 8). In contrast, FVC remained stable
both in controls (p = 0.79) and in patients treated with rhDNase (p =0.26) whereas it
decreased significantly only in untreated patients (p < 0.008) (Fig. 9).

12/12/2003 11
D I S C U S S I O N
In this large BAL study we provide evidence that the majority of CF patients with
normal lung function have neutrophilic airway inflammation that increases over time.
In patients with elevated neutrophil counts, treatment with rhDNase did not reverse
the neutrophilia, but prevented progression of the increase in BAL fluid neutrophils
and may therefore be efficacious in modulating the inflammatory process. This is the
first report demonstrating that rhDNase is not only an effective mucolytic drug, but
also affects the progression of airway inflammation in CF.
Short term studies using sputum analysis have found evidence that rhDNase
releases pro-inflammatory cytokines that are bound to DNA and may therefore have
a negative effect on airway inflammation [14,15]. These findings were not supported
by 2 subsequent studies using spontaneously expectorated sputum in patients with
more severe lung disease, in which rhDNase treatment over 1-3 months was found to
have no effect on airway inflammation [16,26]. Here we could show that rhDNase
treatment over 3 years not only has no pro-inflammatory effect but rather prevents
the increase in airway inflammation that is observed in untreated patients.
In a preliminary analysis of the initial BAL performed in each patient we could show
that the majority of patients in our study population with a normal percentage of
neutrophils in pooled BAL sample already have an elevated percentage of
neutrophils in their first BAL sample [20]. This is a more bronchial sample and may
therefore be more sensitive for early bronchial inflammation in CF. Longitudinally, we
have now found an increase of neutrophils over time in the first sample in all groups
with no effect of rhDNase treatment. Whether this is of relevance for the effect of
12/12/2003 12
treatment remains unclear. The absolute amount of neutrophils and neutrophil
products is much lower in the first BAL sample and, even though this may be a more
sensitive marker of a bronchial disease, the absolute inflammatory burden of
neutrophil degradation products may be more relevant for the damage caused to the
peripheral airways and the lung parenchyma. A large study assessing lung function
as a primary outcome measure in CF patients with mild lung disease showed greater
improvement for rhDNase treated patients in FEF25-75% compared to FEV1; a test
which is more sensitive for changes in peripheral airways (13). In addition, studies
using sputum that is derived from more central airways have failed to demonstrate
any effect of rhDNase on airway inflammation (16,26). These finding may therefore
suggest that rhDNase may have a more pronounced effect on peripheral airway
inflammation. Long term follow-up of the patients in our study may give a clue as to
which of the markers of BAL fluid and which BAL sample may be more useful to
predict the future course of lung disease in CF patients.
The mechanism of an anti-inflammatory effect of rhDNase is unclear. RhDNase has
been shown to release cationic enzymes from complexes with DNA [27] and to
reduce the concentration and the size of extracellular DNA in sputum [28]. Patients
treated with rhDNase produced significantly lower viscosity of sputum and an
increased ratio of viscosity in proportion to elasticity at high frequency consistent with
increased clearability of sputum by coughing. This is critically dependent on the
adhesiveness of mucus, which is determined by its surface tension, and is better with
a lower tension and consequently a more efficient air-jet mucus interaction [29].
RhDNase has no direct effect on the production of pro-inflammatory cytokines, the
chemotaxis of neutrophils or the release of neutrophil products. Studies in CF cell
lines and in animal models of CF airway infection have demonstrated not only an

12/12/2003 13
exaggerated response to infectious agents, but also defective downregulation that
leads to persistence of the inflammatory process over time [30,31]. This defective
downregulation seems to be linked to decreased production of the anti-inflammatory
cytokine IL-10 [32]. An increase in neutrophilic airway inflammation is not limited to
bacterial infection and was also demonstrated in CF children with viral respiratory
tract infection [33]. As rhDNase has been found to decrease the number of
pulmonary exacerbations in CF, the lack of increase in BAL neutrophils in rhDNase
treated patients may be caused by a lower rate of exacerbations in these patients.
Alternatively, the improved clearance of mucous may directly clear neutrophils and
their degradation products from the lung.
Although it is well known that CF lung disease is characterized by neutrophilic airway
inflammation even in patients with mild lung disease, little progress has been made in
the development of effective anti-inflammatory treatment. In addition, the long-term
effect of airway inflammation in CF remains poorly defined. Indirect evidence from
trials using ibuprofen or systemic corticosteroids suggest that treatment of airway
inflammation has a positive effect on lung function [34,35]. In these studies, both
therapeutic approaches did not improve lung function, but rather slowed the decline
of lung function over time. Cross-sectional data from a study of infants suggest that
neutrophilic airway inflammation shows a negative correlation with lung function [36].
In our study patients with a normal percentage of neutrophils in BAL fluid did not
show a decline of lung function over a three year period, a finding that would favor
the view that airway inflammation per se has a negative impact on the subsequent
course of lung disease and that the absence of airway inflammation is a positive
prognostic factor in CF lung disease. However, this patient group also showed an
increase of neutrophilic airway inflammation over time raising the question whether a

12/12/2003 14
threshold exists for airway inflammation to become deleterious for the further course
of lung disease.
Even though BAL has the advantage to sample material directly from the lower
respiratory tract, its use in longitudinal studies has some limitations. BAL studies in
CF patients have provided evidence for regional heterogeneity of lung disease with
differences in both bacterial colonization and the extend of airway inflammation in
different regions of the lung (37,38). We have tried to address this problem by always
performing the BAL in the same region in the lung and by selecting the lingula, which
belongs to the upper lobe and may be more sensitive to detect airway inflammation in
patients with mild disease, since CF is characterized by a more prominent
involvement of the upper lobes (37). Currently, there is little information on the
longitudinal course of variability in regional airway inflammation in CF and we can
therefore not exclude that this may have influenced the results of this study..
In summary, we have shown that rhDNase has a positive impact on airway
inflammation in CF patients. These data support our preliminary findings that
rhDNase has a beneficial effect on metalloproteases in BAL fluid (39) and would
favor an early use of this drug in CF patients with mild disease and support the
evidence provided by the PEIT study that demonstrated a positive effect of rhDNase
on both lung function and pulmonary exacerbations in CF patients with mild disease
[13]. Further follow-up of these patients will show whether this positive effect on
airway inflammation will affect the decline in lung function over time in these patients.

12/12/2003 15
Acknowledgement:
We would like to thank all the collaborators in the clinics and in the laboratories at the
different participating centers for their excellent collaboration in this study.
This study was supported by a grant from the german CF foundation (Mukoviszidose
e. V.) and Hoffmann-La Roche, Germany.

12/12/2003 16
R E F E R E N C E S
1. Matsui H, Grubb BR, Tarran R, Randell SH, Gatzy JT, Davis CW, Boucher RC.
Evidence for periciliary liquid layer depletion, not abnormal ion composition, in the
pathogenesis of cystic fibrosis airways disease. Cell 1998; 95: 1005-15.
2. Worlitzsch D, Tarran R, Ulrich M, et al.. Effects of reduced mucus oxygen concen-
tration in airway Pseudomonas infections of cystic fibrosis patients. J Clin Invest
2002; 109: 317-25.
3. Konstan MW, Berger M. Current understanding of the inflammatory process in
cystic fibrosis: onset and etiology. Pediatr Pulmonol 1997; 24:137-142.
4. Nakamura H, Yoshimura K, McElvaney NG, Crystal RG. Neutrophil elastase in
respiratory epithelial lining fluid of individuals with cystic fibrosis induces
interleukin-8 gene expression in a human bronchial epithelial cell line. J Clin
Invest 1992; 89:1478-1484.
5. De RV. Mechanisms and markers of airway inflammation in cystic fibrosis. Eur
Respir J 2002; 19: 333-40.
6. Khan TZ, Wagener JS, Bost T, Martinez J, Accurso JF, Riches DWH. Early
pulmonary inflammation in infants with cystic fibrosis. Am J Respir Crit Care Med
1995; 151:1075-1082.
7. Armstrong DS, Grimwood K, Carzino R, et al.. Lower respiratory infection and
inflammation in newly diagnosed cystic fibrosis. BMJ 1995; 310: 1571-2.
8. Konstan MW, Hilliard KA, Norvell TM, et al. Bronchoalveolar lavage findings in
cystic fibrosis patients with stable, clinically mild lung disease suggest ongoing
infection and inflammation. Am J Respir Crit Care Med 1994;150: 448-54.
9. Kirchner KK, Wagener JS, Khan TZ, Copenhaver SC, Accurso FJ. Increased
DNA levels in bronchoalveolar lavage fluid obtained from infants with cystic

12/12/2003 17
fibrosis. Am J Respir Crit Care Med 1996; 154:1426-1429.
10.Fuchs HJ, Borowith DS, Christiansen DH, Morris EM, Nash ML, Ramsey BW,
Rosenstein BJ, Smith AL, Wohl ME. Effect of aerosolized recombinant human
DNase on exacerbations of respiratory symptoms and on pulmonary function in
patients with cystic fibrosis. N Engl J Med 1994; 331:637-42.
11.Hodson ME, Shah PL. RhDNase trials in cystic fibrosis. Eur Respir J 1995;
8:1786-91.
12.Kearney CE, Wallis CE. Deoxyribonuclease for cystic fibrosis. Cochrane
Database Syst Rev 2000; 2: CD001127.
13.Quan JM, Tiddens HA, Sy JP et al. The Pulmozyme Early Intervention Trial Study
Group. A two-year randomized, placebo-controlled trial of dornase alfa in young
patients with cystic fibrosis with mild lung function abnormalities. J Pediatr 2001;
139: 813-20.
14.Shah PL, Scott SF, Knight RA, Hodson ME. The effects of recombinant human
DNase on neutrophils elastase activity and interleukin-8 levels in the sputum of
patients with cystic fibrosis. Eur Respir J 1996; 9:531-4.
15.Perks B; Shute JK. DNA and actin bind and inhibit interleukin-8 function in cystic
fibrosis sputa: in vitro effects of mucolytics. Am J Respir Crit Care Med 2000; 162:
1767-72.
16.Suri R, Wallis C, Bush A, Thompson S, Normand C, Flather M, Grieve R, Metcalfe
C, Lees B. Comparison of hypertonic saline and alternate-day or daily
recombinant human deoxyribonuclease in children with cystic fibrosis: a
randomised trial. Lancet 2001; 358: 1316-21.
17.Paul K, Jung A, Ballmann M, Griese M, Rietschel E, Chen CIU, Schink T, Shute
JK, Döring G, Ratjen F. Effect of rhDNase on endobronchial inflammation in CF
patients with mild lung disease: results of the multi-center BEAT study. Pediatr

12/12/2003 18
Pulmonol 2002; Suppl 24: 386A.
18.Shute JK, Marshall LJ, Chen C, Kleinau I, Wahn U, Paul K. Free IL-8 in BAL fluid
of CF patients treated with rhDNAse. Am J Respir Crit Care Med 2001; 163
(3):490 A.
19.Ratjen F, Bredendiek M, Brendel M, Meitzer J, Costabel U. Differential cytology
for bronchoalveolar lavage fluid in normal children. Eur Respir J 1994; 7:1865-70.
20.Ratjen F, Rietschel E, Griese M, Ballmann M, Kleinau I, Döring G, Reinhardt D,
Paul K. Fractional analysis of bronchoalveolar lavage fluid cytology in cystic
fibrosis patients with normal lung function. Bronchoalveolar lavage for the
evaluation of anti-inflammatory treatment (BEAT) study group. Eur Resp J
2000,15:141-5.
21.Dean TP, Dai Y, Shute JK, Church MK, Warner JO. Interleukin-8 concentrations
are elevated in bronchoalveolar lavage, sputum, and sera of children with cystic
fibrosis. Pediatr Res 1993; 34:159–61.
22.Klebanoff SJ, Waltersdorph AM, Rosen H. Antimicrobial activity of
Myeloperoxidase. Meth Enzym 1984; 105:399-403.
23.Goldstein W, Döring G. Lysosomal enzymes from polymorphonuclear leukocytes
and proteinase inhibitors in patients with cystic fibrosis. Am Rev Respir Dis
1986;134:49-56.
24.Worlitzsch D, Kaygin H, Steinhuber A, Dalhoff A, Botzenhart K, Doering G. Effects
of amoxicillin, gentamicin, and moxifloxacin on the hemolytic activity of
Staphylococcus aureus in vitro and in vivo. Antimicrob Agents Chemother 2001;
45: 196-202.
25.Brunner E, Domhof S and Langer F, Nonparametric analysis of longitudinal data
in factorial experiments, Wiley & Sohns, New York, 2002.

12/12/2003 19
26.Henry RL, Gibson PG, Carty K, Cai Y, Francis JL. Airway inflammation after aero-
solised deoxyribonucluase in cystic fibrosis. Pediatr Pulmonol 1998; 26: 97-100.
27.Rochat T, Dayer Pastore F, Schlegel-Haueter SE, Filthuth I, Auckenthaler R, Belli
D, Suter S. Aerosolized rhDNase in cystic fibrosis: effect on leucocyte proteases
in sputum. Eur Respir J 1996; 9:2200-6.
28.Shak S, Capon DJ, Hellmiss R, Marsters SA, Baker CL. Recombinant human
DNase I reduces the viscosity of cystic fibrosis sputum. Proc Natl Acad Sci U S A
1990; 87:9188-92.
29.Griese M, App EM, Derouix A, Burkert A, Schams A. Recombinant human DNase
(rhDNase) influences phospholipid composition, surface activity, rheology and
consecutively clearance indices of cystic fibrosis sputum. Pulm Pharmacol Ther
1997; 10: 21-7.
30.Kube D, Sontich U, Fletscher D, Davis P. Proinflammatory cytokine responses to
P. aeruginosa in human epithelial cell lines. Am J Physiol Lung Cell Mol Physiol
2001; 280: L493-502.
31.Muhlebach MS, Noah TL. Endotoxin activity and inflammatory markers in the
airways of young patients with cystic fibrosis. Am J Respir Crit Care Med
2002;165 :911-5.
32.Chmiel JM, Konstan MW, Saadane A, Krenicky JE, Kirchner HL, and Berger M.
Prolonged Inflammatory Response to Acute Pseudomonas Challenge in Inter-
leukin-10 Knockout Mice Am. J. Respir. Crit. Care Med 2002; 165: 1176- 1181.
33.Armstrong D, Grimwood K, Carlin JB, Carzino R, Hull J, Olinsky A, Phelan PD.
Severe viral respiratory infections in infants with cystic fibrosis. Pediatr Pulmonol
1998; 26: 371-9.

12/12/2003 20
34.Eigen H, Rosenstein BJ, Fitzsimmons S, et al. A multicenter study of alternate-
day prednisone therapy in patients with cystic fibrosis. J Pediatr 1995, 126: 515-
23.
35.Konstan MW, Byard PJ, Hoppel CL et al. Effect of high-dose ibuprofen in patients
with cystic fibrosis. New Engl J Med 1995, 332: 848-54.
36.Dakin CJ, Numa AH, Wang H, Morton JR, Vertzyas CC, Henry RL. Inflammation,
infection, and pulmonary function in infants and young children with cystic fibrosis.
Am J Respir Crit Care Med 2002; 165: 904-10.
37.Meyer KC, Sharma A: Regional variability of lung inflammation in cystic fibrosis.
Am J Respir Crit Care Med 1997; 156: 1536-40.
38.Gutierrez JP. Interlobar differences in bronchoalveolar lavage fluid from children
with cystic fibrosis. Eur Respir J 2001; 17: 281-6.
39.Ratjen F, Hartog CM, Paul K, Wermelt J, Braun J. Matrix metalloproteases in BAL
fluid of cystic fibrosis patients and their modulation by treatment with dornase
alpha. Thorax 2002; 57: 930-4.

12/12/2003 21
LEGENDS:
Fig. 1:
Neutrophils (% of the total cell population in BAL fluid) of controls with a normal
percentage of neutrophils at baseline, patients randomized to rhDNase treatment or
no rhDNase treatment. A significant increase in the percentage of neutrophils was
observed with time in both controls and patients receiving no rhDNase treatment
(p<0.02), whereas no change was found in rhDNase treated CF patients.
Fig. 2:
Variability in the annual change of the percentage of neutrophils in pooled BAL
samples for the 2 randomized groups.
Fig. 3:
Neutrophils of the first BAL syringe (% of the total cell population in BAL fluid) of
controls with a normal percentage of neutrophils at baseline, patients randomized to
rhDNase treatment or no rhDNase treatment. The percentage of neutrophils of the
first syringe of BAL increased significantly over time in all groups, although the
increase was more pronounced in untreated patients (p< 0.01 for patients treated
with rhDNase, p< 0.005 for untreated patients for the percentage of neutrophils)
Fig. 4:
Total IL-8 concentrations in pooled BAL fluid of controls with a normal percentage of
neutrophils at baseline, patients randomized to rhDNase treatment or no rhDNase
treatment. A significant increase in the percentage in total IL-8 was observed in
patients receiving no rhDNase treatment (p<0.02), whereas no change was found in
controls (p = 0.09) and rhDNase treated CF patients (p = 0.58).
Fig. 5:
12/12/2003 22
Free elastase activities in pooled BAL fluid of controls with a normal percentage of
neutrophils at baseline, patients randomized to rhDNase treatment or no rhDNase
treatment. A significant increase in elastase activity was observed in patients
receiving no rhDNase treatment (p<0.007), whereas no change was found in controls
and rhDNase treated CF patients.
Fig. 6:
Myeloperoxidase (MPO) activities in pooled BAL fluid of controls with a normal
percentage of neutrophils at baseline, patients randomized to rhDNase treatment or
no rhDNase treatment. Although a trend towards an increase in MPO concentrations
was observed in untreated patients, this did not reach statistical significance.
Fig.7:
Changes in FEV1 ( % predicted) in controls with a normal percentage of neutrophils
at baseline, patients randomized to rhDNase treatment or no rhDNase treatment.
FEV1 significantly decreased in both randomized patient groups (p = 0.001 for
patients treated with rhDNase and p = 0.0003 for untreated patients) whereas no
change was observed in controls (p = 0.07).
Fig.8:
Changes in MEF25/75 (% predicted) in controls with a normal percentage of
neutrophils at baseline, patients randomized to rhDNase treatment or no rhDNase
treatment. MEF25/75 significantly decreased in both randomized patient groups (p <
0.01) whereas no change was observed in controls (p = 0.51).
Fig. 9:
Changes in FVC (% predicted) in controls with a normal percentage of neutrophils at
baseline, patients randomized to rhDNase treatment or no rhDNase treatment. FVC
remained stable both in controls (p = 0.79) and in patients treated with rhDNase (p
=0.26) whereas it decreased significantly only in untreated patients (p < 0.008).

12/12/2003 23
A B B R E V I A T I O N S
BSA bovine serum albumin
CF cystic fibrosis
FRC functional residual capacity
FVC forced vital capacity
FEV1
forced expiratory volume in one second
HLE human leukocyte elastase
FEF25
maximal expiratory flow between 25 and 75 % of vital capacity
MEM minimal essential medium
BAL bronchoalveolar lavage
PBMC peripheral blood mononuclear cells
PBS phosphate buffered saline
rhDNase recombinant human desoxyribonuclease

12/12/2003 24
Fig. 1:
* *
*
*
3. BAL2. BAL1. BAL
neutr
ophil
s(%
)
100
80
60
40
20
0
controls
rhDNase
no rhDNase
*
*

12/12/2003 25
Fig. 2:
annual change in neutrophils (%)
>22.5%
17.5% to 22.5%
12.5% to 17.5%
7.7% to 12.5%
2.5% to 7.5%
-2.5% to 2.5%
-7.5% to -7.5%
-12.5% to -7.5%
-17.5% to -12.5%
%o
fp
ati
en
ts
40
30
20
10
0
rhDNase
no rhDNase

12/12/2003 26
Fig. 3
*
*
3. BAL2. BAL1. BAL
ne
utr
op
hils
(%)
firs
tsyri
ng
e
120
100
80
60
40
20
0
controls
rhDNase
no rhDNase
**
*
12/12/2003 27
Fig. 4
*
3. BAL2. BAL1. BAL
tota
lIL
-8(n
g/m
l)
6
5
4
3
2
1
0
controls
rhDNase
no rhDNase
*

12/12/2003 28
Fig. 5:
**
3. BAL2. BAL1. BAL
Ela
sta
se
ac
tivit
y(U
),20
,15
,10
,05
0,00
controls
rhDNase
no rhDNase
*

12/12/2003 29
Fig. 6:
3. BAL2. BAL1. BAL
MP
Oa
cti
vit
y(U
)
,05
,04
,03
,02
,01
0,00
controls
rhDNase
no rhDNase

12/12/2003 30
Fig. 7:
3. BAL2. BAL1. BAL
FE
V1
(%p
red
icte
d)
140
120
100
80
60
40
controls
rhDNase
no rhDNase
**

12/12/2003 31
Fig. 8:
3. BAL2. BAL1. BAL
ME
F25/7
5V
C(%
pre
dic
ted)
200
150
100
50
0
controls
rhDNase
no rhDNase
*
*

12/12/2003 32
Fig. 9:
3. BAL2. BAL1. BAL
FV
C%
pre
dic
ted
160
140
120
100
80
60
40
20
0
-20
controls
rhDnase
no rhDNase
*

12/12/2003 33
Table 1: Baseline characteristics for the 3 groups
RhDNase No RhDNase Controls
N 46 39 20
Age; mean (SD) 11.3 (5.1) 12.2 (4.4) 12.5 (7.5)
Females/males 25/21 21/18 7/13
DF508 homozygous 66 % 63 % 45 %
DF508 compound heterozygous 9 % 21 % 35 %
FVC; mean (SD) 86 (27) % 95 (19) % 83 (24) %
FEV1; mean (SD) 96 (13) % 98 (15) % 93 (15) %
MEF25/75 % VC ; mean (SD)) 92 (30) % 90 (32) % 74 (21) %
Total cell counts;
Median (range) x106
4.4 (0-126) 5.9 (0-159) 1.8 (0-13)
Macrophages ; median (range) 63.5 (8-91) % 63 (8-94) % * 89 (62-94) %
Lymphocytes; median (range) 5.9 (0-38) % 4 (0-32) % 8.7 (1-39) %
Neutrophils ; median (range) 29 (6-87) % * 29 (7-91) % * 1.5 (0.3-7) %
Eosinophils; median (range) 0 (0-3.4) % 0.3 (0-10.7) % 0.1 (0-1) %
IL-8 ng/ml ;
Median (range)
0.69 (0.15-7) * 0.51 (0.04-3.5) * 0.07 (0.02-0.32)
Elastase U
Median (range)
0.018 (0-0.18) 0.02 (0.01-1.81) 0.017 (0-0,02)
MPO U
median (range)
0.05 (0-0.064) 0.052 (0-0.082) 0 (0-0.059)
*significantly different to controls (p at least <0.05)

12/12/2003 34
Table 2: Results of BAL fluid bacterial cultures (%) in the 3 groups
RhDNase No RhDNase Controls
1. BAL
n 46 39 20
P. aeruginosa 37 % 21 % 15 %
Staph. aureus 48 % 51 % 30 %
H. influenzae 22 % 23 % 10 %
Other bacteria 24 % 21 % 20 %
No bacteria 13 % 18 % 50 % *
2. BAL
n 43 33 16
P. aeruginosa 28 % 21 % 19 %
Staph. aureus 30 % 45 % 19 %
H. influenzae 26 % 18 % 25 %
Other bacteria 10 % 24 % 25 %
No bacteria 14 % 18 % 31 %
3. BAL
n 24 24 12
P. aeruginosa 38 % 33 % 17 %
Staph. aureus 29 % 54 % 17 %
H. influenzae 38 % 33 % 25 %
Other bacteria 38 % 25 % 25 %
No bacteria 3 % 21 % 42 %
*p = 0.002 compared to both randomized groups; Fisher’s exact test





























