Embed Size (px)
Citation preview
Conummity Dcni Oral Epidemiol 1995; 25: 25-9Prififec/ ill Deninark . //// rights reserved
Copyright © Munksgaard 1995
Communify Dentistryd O l E i d i l
ISSNtmi-56bI
Effects of glass ionomer cement,resin-based pit and fissure sealantand HF applications on occlusalcaries in a developing country fieldtrial
Yupin Songpaisan\Douglas Bratthall^,Prathip Phantumvanit^ andYuvade Somridhivej"'Faculty of Public Health, Mahidol University,Bangkok, Thailand ^WHO CollaboratingCentre, Faculty of Odontology, University ofLund, Malmo, Sweden, ^Faculty of Dentistry,Chulalongkorn University, Bangkok, ''BangkokMetropolitan Administration Health Center,Wat Thardthong, Bangkok, Thailand
Songpaisan Y, Bratthall D, Phantumvanit P, Somridhivej Y: Effects of glassionomer cement, resin-based pit and fissure sealant and HF applications onocclusal caries in a developing cout"itry field trial. Cotiimuiiity Dent Oral Epidemiol1995; 23; 25-9. © Mttnksgaard, 1995
Abstract - The aim of this cotntnunity-oriented study was to evaluate differentmethods to prevent fissure caries. The following products and measures were test-ed; 1) glass ionomer cement (GIC) applied by dentist; 2) same tttaterial applied byshort term (3 days) trained personnel (teachers); 3) application of a 0.5% HF solutionthree times; 4) an established autopolytnerized resin based sealant (Delton). Thestudy was performed in Bangkok, Thailand, a city in a developing country experi-encing increasing caries prevalence. Children with at least three sound permanentmolars from two age groups, 7-8 and 12-13-yr-olds respectively were chosen fromvery low to medium socioeconomic level families, 1264 children were systematicallyassigned to experiment or control groups based on school and DMFT For theyounger age group, the 2 yr mean DFS occlusal incretnent in the Control groupwas 0.66 surfaces. Significantly lower increments were observed in the GIC experi-mental group; 0,17 surfaces applied by the teachers and 0,32 applied by dentist,corresponditig to 74'/o atid 52"/> reductions, respectively. The mean increment iti theHF group was 0.44 surfaces, a 33% reduction in relation to the Control group. Forthe 12-13-yr-olds, the mean occlusal surface DF increment was 0.70 surfaces in theControl group. Almost no occlusal increment was found in the Delton group, 0,05DFS, a 93% reduction. In the GIC Dentist group, the DFS increment was 0.48and in the Teacher group 0.56, corresponding to 31% and 20% reduction, respec-tively. A slight and nonsignificant iticrease of caries in relation to the Controlgroup was observed in the HF group. Retention of Delton sealant was high, 92%after 6 months, retention of the GIC sealants was low. At the 6-tnonths checkup,only 2-8% of these sealants were still present and also after reapplication, a majori-ty was lost.
Key words: dental caries; fissure sealant; glassionomer; hydrofluoric acid; Delton: laypersonnel
Yupin Songpaisan, Faculty of Public Health,Mahidol University, 420/1 RajvithI Road,Bangkok 10400, Thailand
Accepted for publication 23 February 1994
The fissures of pertnanent tnolars areusually the first tooth surfaces to becomeaffected by caries in younger age groups.A National Oral Health Survey in Thai-land in 1989 (1) indicated that childrenaged 12 yr had a mean DMFT at 1.5.
Eighty-seven percetit of these teeth re-quired restorative care and most of thetn{11%) needed one-surface fillitigs. Suchinformation, together with the fact thatuntreated active fissure caries lesionstnay result in the total destruction of the
affected tooth, motivate intensive effortsto solve the fissure caries probletn. Themain aim of this study was to test vari-ous tnethods for preventing fissure car-ies, Intei"est was emphasized in materialsand personnel that could be used at com-

26 SONGPAISAN ET AL.
munity level in developing countries,where caries experiences are rapidlychanging from low to moderate levels.
The use of fissure sealants as a cariespreventive measure has proven effectivein many studies, including use of auxilia-ry and lay personnel, but so far moststudies have been performed in western-ized countries (2-5). However, for devel-oping countries, the resin based sealantsare not the ideal solution as they cannotbe used in all working environments.They are technique sensitive and requirequalified dental personnel, aspirator suc-tion and cool storage. This, together withthe relatively high cost, makes it of inter-est to look for alternative methods whichwould be as effective but less expensiveto provide.
Nearly 20 yr ago, powdered fluoro-aluminium silicate glass material knownas glass ionomer cement (GIC) was in-troduced as an alternate fissure sealantsystem (6). The materials contain fluo-ride that is slowly released (7-10) intothe surrounding enamel and yield carios-tatie effects of importance for preventionof pit and fissure caries (11). In addition,the main reported advantage of GIC (12,13) was their abihty to bond ehemieallyto dentin and enamel without etching,making it mueh easier to handle and re-quiring less operation time. These twofavorable properties, not found in othercement or sealant materials, made it ofspecial interest to inelude a GIC in thepresent study. Moreover, the simple pro-cedure made it worthwhile to investigateif the material could be applied success-fully also by lay personnel with only afew days' training.
Another product believed worthy ofevaluation was an aqueous hydrofluoricacid (HF) solution (14). Its therapeuticaction is thought to be via immediatefluoride reaction with the dental enameland ealcium fluoride, forming a reservoirfor long-term release of fiuoride forenamel remineralization. The solutionhad been tested and found effective in or-thodontic patients (15). The advantagesthat make it particularly suitable for de-veloping countries are low priee, easy ap-plication and use of low skill personnel,simple equipment and minimal time.
Material and methods
Study .sample - The study was performedin Bangkok, Thailand, a city in a devel-
oping country experiencing increasingearies prevalence. The study focused ontwo age groups, 7-8 and 12-13-yr-oldchildren. The 7-8-yr-old children wereselected from two primary schools inBangkok, (Schools 1 and 2) that are clas-sified as serving families from low tovery low soeioeeonomie status. The 12-13-yr-old children were selected fromtwo secondary schools, at one school(School 3) the majority of ehildren eamefrom low to very low socioeconomic levelfamilies while in the other (School 4)they eame from low to medium socioeco-nomic level famlies. The primary schoolsare included in the Bangkok Metropoli-tan Authorities Sehool Health Programin whieh the children rinse with 0.2'KiNaF every 2 weeks. The fiuoride mouth-rinsing program is not practiced in thesecondary sehools. Praetieally all tooth-pastes available in Thailand, especially inBangkok, are fiuoridated. The centralwater supply in Bangkok and adjacentprovinces naturally contains 0.1-0.2 ppmfiuoride.
Selection criteria - All ehildren (2018;875 aged 7-8 yr and 1143 aged 12-13 yr)at the four sehools were screened to iden-tify those ehildren with at least threesound permanent molars. Molars didhave to be erupted sufficiently to plaee asealant to be eligible for the study.
Carles registration and sealant rcten-tloti exatmnation - Tooth or surface wasclassified sound or earious, using theWHO standard criteria and methods(16). Assessments of sealant retention onthose oeclusal surfaees sealed with Del-ton or glass ionomer were performed at6 and 24 months by one dentist and elas-sified as "fully intact", "partly intaet" or"all missing". Final earies registrationsfor all groups were done at 24 months.
There were five dentists (D1-D5) par-ticipating in the study. Dl and D2trained schoolteachers to apply sealant.All earies registrations and sealant reten-tion examinations throughout the studywere carried by D1. Resin sealants wereapplied by D3 and D4 applied GIC seal-ants. Dl and D5 applied HF solution.
Duplication of clinical examinationsfor earies status was performed in 120children at baseline and in 101 ehildrenat 2 yr. For duplicate examinations ofsealant retention, 60 ehildren partici-pated. Consistency of all examinationswere at the same level {Kappa=0.9.P<0.01).
Stuclv group assigiitiietit - All eligibleehildren in eaeh sehool were listed in as-eending order of their DMF teeth. Eaehchild was then systematieally assignedinto four (Sehool 1 & 2) and five (School3 & 4) study groups. For ethical reason,children participating in all study groupswere allowed to seek dental care else-where if they or their parents felt it wasneeded.
Treatment program and protocols -After eompletion of the baseline eariesregistration, the ehildren were assignedto one of the following 5 groups. 1) Con-trol; no treatment was given. 2) Provenresin sealant: the positive control was theestablished autopolymerized resin, Del-ton Pit & Fissure sealant® (Johnson &,lohnson, MJ, USA), and applied by adentist at a Health Center, under stan-dard dental clinic setting and accordingto the manufacturer's instruction. Forpractical reasons, only the 12-yr-oldgroup was included. The next twogroups used GIC; - Glass ionomer (FujiIonomer Type III for Fissure Sealant®,GC Dental Industrial Corp, Tokyo, Ja-pan). Before application of the sealantmaterial by one dentist (Group 3, GIC-D) or six 3-day-trained sehoolteaehers(Group 4, GIC-T), the oeelusal surfaceswere cleaned by explorer and isolatedwith cotton rolls followed by applicationof 3.0% hydrogen peroxide with eottonpellet for 10 s and air blow driedfollowing the manufacturer's instrue-tions. The 3-day-training course forsehoolteaehers taught by two dentistsconsisted of general knowledge of toothanatomy and earies and oral hygiene in-struction of the first day; the seeond dayincluded glass ionomer sealant materialhandling, mixing and applieation. Dem-onstration and practice of sealant appli-cations were done on plaster easts. Thethird day was used for sealant applica-tion praetiee on ehildren. Faeh teachertreated about six teeth at this session.Due to the high humidity and hot eli-mate in Bangkok, the mixed materialtended to set fast; to increase applicationtime the liquid was kept in cold waterduring the applieation period. Reappli-cation was done for those ehildren whoseGIC or resin sealants were partially orall missing at the 6-month examination.
The last group (5) used a hydrofiuoricacid (HF) solution that was applied bytwo dentists three times; firstly, after thebaseline examinations were eompleted.

Field trial of glass iottottter atid fissure sealattts 27
secondly and thirdly afler 6 months and12 months. P'or application, an aqueoussolution with a concentration of Q.5%(w/v) with a pH of 1.9 was preparedfrom a 37'/̂ i stock solution (Merck, WestGermany, pro analyzi grade). The occlu-sal surfaces were lirst isolated with cot-ton rolls and washed carefully by cottonpellets with 3,0% hydrogen peroxide forten seconds. The surfaces were thenwashed with 95% alcohol for 10 s and airblow dried, after which one to two dropsper tooth of an aqueous hydrofluoricacid was applied from a disposable plas-tic pipette (DVT, Sweden), Each occlusalsurface thus treated was kept wet withHF solution a minimum of 1 min beforesaliva was allowed to contaminate thetreated area.
With the exception of application ofDelton sealants, all procedures, includingcaries registration and retention examina-tions, were done at the school sites undersimple dental mobile settings with thesubjects in supine position on a flat tableand their heads supported on an attachedhead rest. The examiners/operators wereseated at "12 o'clock" behind the subjectatid used artificial light (DC 6 V, 30 mA,4 W 50/60 Hz charged battery; Hnsy TSMirror model 60188, Hnsy Corporation,Osaka, Japan) and Beach sickle type ex-plorer. Locally made low pressure salivaaspirator and foot pump air blowers werealso available. Data were recorded by anexperienced assistant.
Statistical atialysis - The one-wayanalysis of variance (ANOVA) was per-formed to test group comparability andScheffe's test was used to indicate specificgroup difference at P value of 0.05 atbaseline and after 2 yr.
Results
Approximately one-third of the childrenWere excluded because they did not meetIhe study criteria for inclusion. Consentforms were distributed among the eligi-ble subjects, 551 and 766 children aged7-8 and 12-13 yr respectively. Seven per-cent (39 children) of age group 7-8 and2% (14 children) of age group 12-13 yrrefused to participate. Among the en-rolled children 49% were boys and 51%were girls. At age 78 the mean DMFTWas 0,34+0,59 (DT=0,29; MT=0,004;FT=0.05). At age 12-13 yr the meanDMFT was 1.81 ±1.84 (DT=0.87; MT=0-15; FT=0.78) (Table 1). These children
had mean ages of 7.9±0.6 and 12.9±0,5yr respectively and were systematicallyassigned to experitnental or controlgroups. Differences in mean of caries ex-perience among study groups in both agegroups were not significant either for themean DMFT or for the DMFS{P>0.05). The mean total DMFS±SDwas 0.41 ±0.74 and 3.02±3.85 at age 7-8 and 12-13 yr, respectively. At baseline,the mean number of occlusal surfaces in-cluded in the study for GIC or resin seal-ant or HF applications was 3.6±0.74 atage 7-8 and 6.8±I.4O at age 12-13 yr.
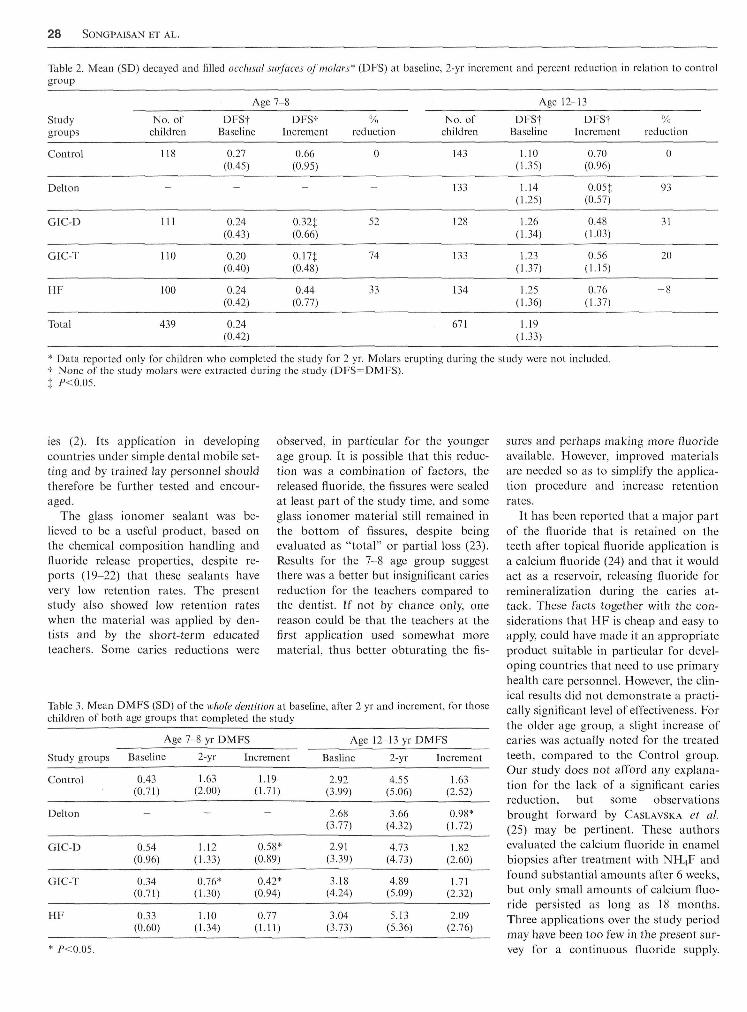
After 2 yr 86% of children aged 7-8 yrand 89'Mi of children aged 12-13 yr com-pleted the study. The main reason fordropping out was moving out of thearea. The other reason was having ortho-dontic treatment. Table 2 shows themean number of decayed and filled oc-clusal surfaces at baseline and at the endof the study 2 yr later. For the youngerage group, the mean DF increment ofocclusal surface in the Control groupwas 0.66. Significantly lower incrementswere observed in the GIC experimentalgroups: 0.17 surfaces when the glass-ion-omer was applied by the teachers and0.32 surfaces by dentists, correspondingto 74'yii and 52"!̂ i reductions, respectively.The mean DF increment in the HFgroup was 0,44 surfaces. This 33% re-duction in relation to the control groupwas not statistically significant.
For the older age group 12-13 yr, themean DF increment of occlusal surfacewas 0,70 in the Control, group (Table 2),
Table 1. Distribution of selected children byschools
No. ol children
Eligible andenrolled
Age DMFTgroup School Screened /; (DS)
7-8 1
2
Total
12-13 3
4
Total
528
347
875
559
584
1143
336
176
512
379
373
752
0.33(0.58)0.39
(0.60)
0.34(0.59)
1.71(1.74)1.90
(1.93)
1.81(1.84)
A significantly lower increment wasfound in the Delton group, 0.05 DFS, a93'!/;, reduction. In the GIC Dentistgroup, the increment was 0.48 surfacesand in the Teacher group 0.56 surfaces,corresponding to 31% and 20% reduc-tion, respectively. Both of the GIC in-crements were not significantly less thanthe Control increments, A slight andnonsignificant caries increase for the HFgroup in relation to the Control groupwas observed.
Table 3 shows the DMFS for the]vholc dentition at baseline and after 2 yrfor both age groups. For the younger agegroup, a significantly lower DMFS in-crement was found in both GIC groupscompared to the Control group. For theolder children the Delton DMFS in-cretnent value was the lowest and theonly one that differed significantly fromthe Control group. None of the sealed ortreated molars were extracted during thestudy period.
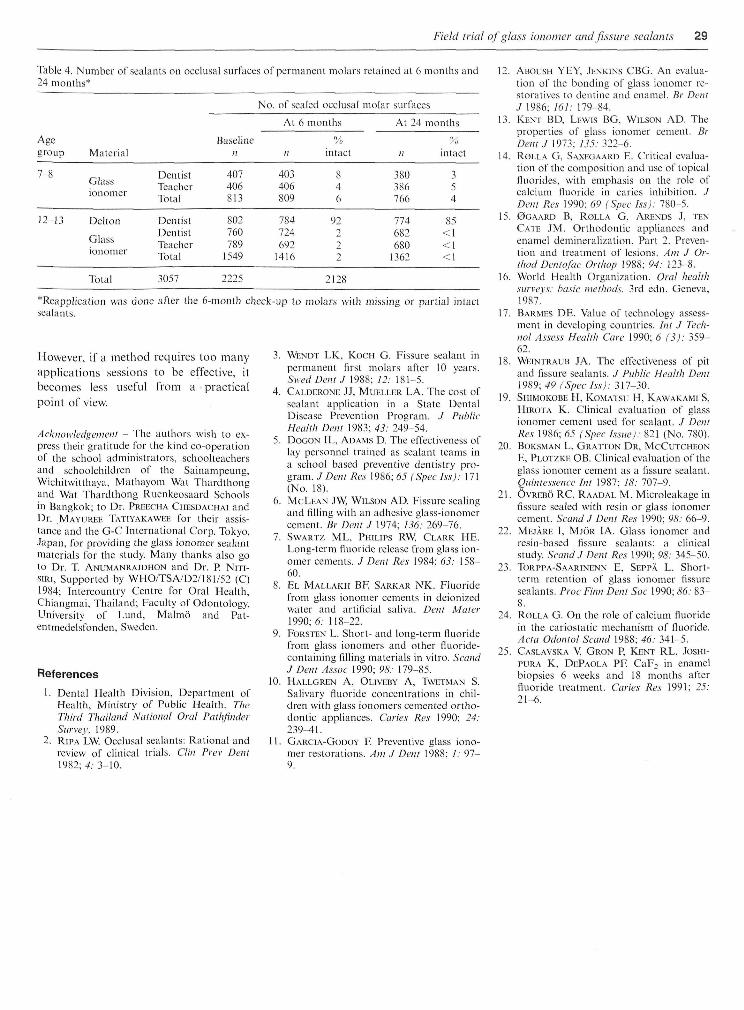
Table 4 shows the results for sealantretention. At 6 months, 2-8%i of theglass-ionotner sealants were retaitied. At24 months, 2-5% were retained for theyounger age group and less than \% forthe older group. At 6 months 92% of theDelton tnaterial was retained and at 24months, 85%,
Discussion
The worldwide change in caries preva-lence makes it an itnportant task to findeffective and cheap measures to preventand treat the disease (17). Appropriatetechnologies and personnel are partic-ularly important for developing coun-tries, where resources are scarce. Ade-quate methods already used in industri-alized countries should still be evaluatedunder different conditions, to assess themost effective ways to apply the technol-ogy in developing countries. This studyhas demonstrated results for three ap-proaches to prevent caries in childrenfrom low socioeconomic status familiesresiding in fluoride deficient communityin a developing country. Study resultsusing Delton sealant, with respect to car-ies reduction and retention, seem to bein accordance with many reports (18),Occlusal caries development on treatedteeth was negligible in our sludy (Table2), The use of pit and fissure sealant hasbeen highly recommended for communi-ties with high prevalence of occlusal car-
28 SONGPAISAN BT AL.
Table 2.group
Studygroups
Control
Delton
GIC-D
GIC-T
HF
Total
Mean (SD) decayed and
No. ofchildren
118
-
Ill
110
100
439
filled occlusal surf aces oj molars
Age
DFStBasehne
0.27(0.45)
-
0.24(0.43)
0.20(0.40)
0.24(0.42)
0.24(0.42)
: 7-8
DFStIncrement
0.66(0.95)
-
0.32:1:(0.66)
0.171(0.48)
0.44(0.77)
* (DFS) at
"/,reduction
0
-
52
74
33
baseline, 2-yr increment and percent reduction in
No. ofchildren
143
133
128
133
134
671
Age
DFStBaseline
1.10(1.35)
1.14(1.25)
1,26(1.34)
1.23(1.37)
1.25(1.36)
1.19(1.33)
12-13
DFStIncrement
0.70(0.96)
0.05:}:(0.57)
0,48(1.03)
0,56(1.15)
0.76(1.37)
relation to control
%reduction
0
93
31
20
- 8
* Data reported only for children who completed the study for 2 yr. Molars erupting during the study were not included.t None of the study molars were extracted during the study (DFS = DMFS).
ies (2). Its application in developingcountries under simple dental mobile set-ting and by trained lay personnel shouldtherefore be further tested and encour-aged.
The glass ionomer sealant was be-lieved to be a useful product, based onthe chemical composition handling andfluoride release properties, despite re-ports (19-22) that these sealants havevery low retention rates. The presentstudy also showed low retention rateswhen the material was applied by den-tists and by the short-term educatedteachers. Some caries reductions were
observed, in particular for the youngerage group. It is possible that this reduc-tion was a combination of factors, thereleased fiuoride, the fissures were sealedat least part of the study time, and someglass ionomer material still remained inthe bottom of fissures, despite beingevaluated as "total" or partial loss (23).Results for the 7-8 age group suggestthere was a better but insignificant cariesreduction for the teachers compared tothe dentist. If not by chance only, onereason could be that the teachers at thefirst application used somewhat morernaterial, thus better obturating the fis-
Table 3. Mean DMFS (SD)children of both age groups
Study groups
Control
Delton
GIC-D
GIC-T
HF
of the whole deniition at baseline, after 2 yr and increment, for thosethat completed the study
Age 7-8 yr DMFS
Baseline
0,43(0.71)
-
0.54(0.96)
0.34(0.71)
0.33(0.60)
2-yr Increment
1.63(2.00)
1.12(1.33)
0.76*(1.30)
1.10(1.34)
1.19(1.71)
-
0.58*(0.89)
0.42*(0.94)
0.77(Ll l )
Age
Basline
2.92(3.99)
2.68(3.77)
2.91(3.39)
3.18(4.24)
3.04(3.73)
12-13 yr
2-yr
4.55(5.06)
3.66(4.32)
4.73(4.73)
4.89(5.09)
5.13(5.36)
DMFS
Increment
1.63(2.52)
0.98*(1.72)
1.82(2.60)
1.71(2.32)
2.09(2.76)
P<0.05.
sures and perhaps tnaking more fluorideavailable. However, improved materialsare needed so as to simplify the applica-tion procedure and increase retentionrates.
It has been reported that a major partof the fluoride that is retained on theteeth after topical fluoride application isa calcium fluoride (24) and that it wouldact as a reservoir, releasing fluoride forremineralization during the earies at-tack. These facts together with the con-siderations that HF is cheap and easy toapply, could have made it an appropriateproduct suitable in partieular for devel-oping countries that need to use primaryhealth care persontiel. However, the clin-ical results did not demonstrate a praeti-eally signifieant level of effectiveness. Forthe older age group, a slight increase ofcaries was actually noted for the treatedteeth, compared to the Control group.Our study does not afford any explana-tion for the lack of a significant cariesreduetion, but some observationsbrought forward by CASLAVSKA et al.(25) may be pertinent. These authorsevaluated the calcium fluoride in enamelbiopsies after treatment with NH4F andfound substantial amounts after 6 weeks,but only small amounts of calcium fluo-ride persisted as long as 18 months.Three applications over the study periodmay have been too few in the present sur-vey for a continuous fluoride supply.
Field trial of glass ionotner and fissure sealants 29
Table 4, Number of sealants on occlusal surfaces of permanent molars retained at 6 months and24 months*
No. of sealed occlusal molar surfaces
At 6 months
Agegroup Material
Baselinen II intact
At 24 nionths
intact
7-8
ionomer
DentistTeacherTotal
407406813
403406809
846
380386766
354
12-13 Dellon
Glassionomer
DentistDentistTeacherTotal
802760789
1549
784724692
1416
92229
774682680
1362
85
Total 3057 2225 U28
*Reapplication was done after the 6-month chcck-iip to molars with missing or partial intactsealants.
However, if a tnethod requires too tnanyapplications sessions to be effeetive, itbecomes less useful frotn a practicalpoint of view.
Acknowledgement - The authors wish to ex-press their gratitude for the kind co-operationof the school administrators, schoolteachersand schoolchildren of the Sainampeung,Wichitwitthaya, Mathayom Wat Thardthongand Wat Thardthong Ruenkeosaard Schoolsin Bangkok; to Dr. PRI£ECHA CHESDACHAI andDr. MAYUREE TATIYAKAWEE for their assis-tance and the G-C International Corp. Tokyo,Japan, for providing the glass ionomer sealantmaterials for the study. Many thanks also goto Dr. T. ANUMANRAJDHON and Dr. P. NITI-siRi, Supported by WHO/TSA/D2/181/52 (C)1984; Intercountry Centre for Oral Health,Chiangmai, Thailand; Faculty of Odontology.University of Lund, Malmo and Pat-entmedelsfonden, Sweden.
References
1. Dental Health Division, Department ofHealth, Ministry of Public Health. TheThird Thailand National Oral PathfinderSurvey, 1989.
2. Rii'A LW. Occlusal sealants; Rational andreview of clinical trials. Clin Prev Dent1982;^.- 3-10.
3. WENDT LK, Kocn G. Fissure sealant inpermanent first molars after 10 years.Swed Dent J 1988; 12: 181-5.
4. CALDERONE JJ, MUELLER LA. The cost ofsealant application in a State DentalDisease Prevention Program. J PublieHealth Deui 1983; 43: 249-54.
5. DoGON IL, ADAMS D. The effectiveness oflay personnel trained as sealant teams ina school based preventive dentistry pro-gram. J Dent Res 1986; 65 (Spec Iss): 171(No, 18).
6. MCLEAN JW, WILSON AD. Fissure sealingand filling with an adhesive glass-ionomercement. Br Dent J 1974; 136: 269-76.
7. SwARTZ ML, PHILIPS RW, CLARK HE.Long-term tluoride release from glass ion-omer cements. J Dent Res 1984; 63: 158-60.
8. EL MALLAKH BF, SARKAR NK. Fluoridefrom glass ionomer cements in deionizedwater and artificial saliva. Dent Mater1990; 6: 118-22.
9. FoRSTEN L. Short- and long-term fluoridefrom glass ionomers and other fluoride-containing filling materials in vitro. ScandJ Dent A.SSOC 1990; 96'.- 179-85.
10, HALLGREN A, OLIVBBY A, TWETMAN S.Salivary fluoride concentrations in chil-dren with glass ionomers cemented ortho-dontic appliances. Caries Res 1990; 24:239^1 ,
11, GARCIA-GODOY F, Preventive glass iono-mer restorations. Am J Dent 1988; /,• 97-9.
12. ABOUSH Y E Y , JENKINS C B G . An evalua-
tion of the bonding of glass ionomer re-storatives to dentine and enamel. Br DentJ 1986; 161: 179-84.
13. KENT BD, LEWIS B G , WILSON AD. The
properties of glass ionomer cement. BrDentJ 1973; 135: 322-6.
14. RoLLA G, SAXEGAARD E . Critical evalua-tion of the composition and use of topicalfluorides, with emphasis on the role ofcalcium fluoride in caries inhibition. /Dem Res 1990; 69 (Spec hs): 780-5.
15. 0GAARD B, ROLLA G, A R E N D S J, TEN
CATE JM. Orthodontic appliances andenamel demineralization. Part 2. Preven-tion and treatment of lesions. Am .1 Or-thod Demofac Ovthop 1988; 94: 123-8.
16. World Health Organization. Oral healthsurvevs: basic methods. 3rd edn. Geneva,1987.'
17. BARMES DE. Value of technology assess-ment in developing eountries. Ini J Tech-nol A.s.sess Health Care 1990; 6 (3): 359-62.
18. WEINTRAUB JA. The effectiveness of pitand fissure sealants. ./ Public Health Dent1989; 49 (Spec l.ss): 317-30.
19. StilMOKOBE H, KOMATSU H, KAWAKAMI S,HiROTA K. Clinical evaluation of glassionomer cement used for sealant. J DentRes 1986; 65 (Spec Is.sue): 821 (No. 780).
20. BoKSMAN L, GRATTON DR, MCCUTCHEONE, PLOTZKE OB. Clinieal evaluation of theglass ionomer cement as a fissure sealant.Quiines.seme Int 1987; IS: lQil-9.
21. OvtiEBO RC, RAADAL M . Microleakage infissure sealed with resin or glass ionomercement. Scand J Dent Res 1990; 98: 66-9.
22. MEJARE I, MJOR 1A. Glass ionomer andresin-based fissure sealants; a clinicalstudy. Scand.I Dent Res 1990; 98: 345-50.
23. TORI'I'A-SAARINENN E, SEPPA L. Short-term retention of glass ionomer fissuresealants. Proe Finn Dent Soc 1990; 86: 83-8.
24. ROLLA G. On the role of calcium fluoridein the cariostatic mechanism of fluoride.Acta Odontol Scand 1988; 46: 341-5.
25. CASLAVSKA V, GRON P, KENT RL, JOSHI-PURA K, DEPAOLA PE CaF^ in enamelbiopsies 6 weeks and 18 nionths afterfluoride treatment. Caries Res 1991; 25:21-6.






























