Embed Size (px)
Citation preview

Fibrinogen Genes Modify the Fibrinogen Response to Ambient Particulate Matter
Running Head: Genes, Fibrinogen and Air Particles
Annette Peters (1), Sonja Greven (1,2), Iris M. Heid (1,2), Fiammetta Baldari (3), Susanne Breitner (1), Tom Bellander (4,5), Christina Chrysohoou (6), Thomas Illig (1), Bénédicte Jacquemin (7), Wolfgang Koenig (8), Timo Lanki (9), Fredrik Nyberg (4,10), Juha Pekkanen (9), Riccardo Pistelli (3), Regina Rückerl (1), Christodoulos Stefanadis (6), Alexandra Schneider (1), Jordi Sunyer (7,11,12), H. Erich Wichmann (1,2) for the AIRGENE Study Group
(1) Helmholtz Zentrum München – German Research Center for Environmental Health, Institute of Epidemiology, Neuherberg, Germany; (2) Ludwig-Maximilians University, Munich, Germany (3) Catholic Hospital, Rome, Italy, (4) Institute of Environmental Medicine, Karolinska Institute, Stockholm, Sweden; (5) Department of Occupational and Environmental Health, Stockholm County Council, Stockholm, Sweden; (6) Hippokrates Hospital, University of Athens, Greece; (7) Municipal Institute for Medical Research (IMIM), Barcelona, Catalonia, Spain; (8) Department of Cardiology, University of Ulm, Ulm, Germany; (9) KTL, Department of Environmental Health, Kuopio, Finland; (10) Astrazeneca R&D, Mölndal, Sweden (11) Centre for Environmental Epidemiological Reserch (CREAL), Barcelona, Catalonia, Spain; (12) CIBERESP, Spain;
Word count: Abstract: 240, Text: 3316
This article has an online data supplement, which is accessible from this issue's table of content online at www.atsjournals.org.
The AIRGENE study was funded as part of the European Union’s 5th Framework Program, key action number 4: “Environment and Health”, contract number QLRT-2002-02236. The statistical and genetic group was funded by the National Genome Research Net of the German Ministry of Education and Research, the “Sonderforschungsbereich-SFB-386”, and the Munich Center of Health of the Ludwig-Maximilians-Universität München, Germany.
Regina Rückerl, Alexandra Schneider and Annette Peters were in part funded by the U.S. Environmental Protection Agency (EPA) STAR program grant RD83241501.
Page 1 of 40 AJRCCM Articles in Press. Published on January 8, 2009 as doi:10.1164/rccm.200805-751OC
Copyright (C) 2009 by the American Thoracic Society.

ABSTRACT
Rationale: Ambient particulate matter has been associated with systemic inflammation indicated by
blood markers such as fibrinogen, implicated in promoting atherothrombosis.
Objective: This study evaluated whether single nucleotide polymorphisms (SNPs) within the
fibrinogen genes modified the relationship between ambient particles and plasma fibrinogen.
Methods: In 854 myocardial infarction survivors from five European cities plasma fibrinogen levels
were determined repeatedly (N=5082). City-specific analyses were conducted to assess the impact of
particulate matter on fibrinogen levels applying additive mixed models adjusting for patient
characteristics, time trend and weather. City-specific estimates were pooled using meta-analysis
methodology.
Measurements and Main Results: Seven SNPs in the FGA and FGB genes shown to be associated
with differences in fibrinogen levels were selected. Promoter SNPs within FGA and FGB were
associated with modifications of the relationship between 5-day averages of particulate matter with
an aerodynamic diameter below 10 µm (PM10) and plasma fibrinogen levels. The PM10–fibrinogen
relationship for subjects with the homozygous minor allele genotype of FGB rs1800790 compared to
subjects homozygous for the major allele was eightfold higher (p-value for the interaction 0.037).
Conclusions: The data suggest that susceptibility to ambient particulate matter may be partly
genetically determined by polymorphisms that alter early physiological responses such as
transcription of fibrinogen. Subjects with variants of these frequent SNPs may have increased risks
not only due to constitutionally higher fibrinogen concentrations, but also due to an augmented
response to environmental inflammatory stimuli such as ambient particulate matter.
Keywords: Air pollution, inflammation, genetic susceptibility, epidemiology, particulate matter
Page 2 of 40

3
INTRODUCTION
Fibrinogen plays a key role in the clotting cascade, where its conversion to fibrin stabilizes blood
clots upon injury. Fibrinogen has pro-coagulant as well as pro-inflammatory properties and thereby
promotes atherothrombosis. Elevated concentrations of circulating fibrinogen in the blood have
consistently been associated with an increased risk for myocardial infarction in epidemiological
studies 1. Fibrinogen is a large fibrous glycoprotein (340 kDa) composed of two subunits with three
protein chains each (α, β-, and γ-chain). We found in a sample of 895 myocardial infarction
survivors, that polymorphisms in the genes encoding the fibrinogen protein chains are associated
with variations in fibrinogen plasma levels 2. However, whether polymorphisms in the fibrinogen
genes are independent risk factors for coronary artery disease has not been established. Recently, van
der Krabben et al 3 found no association between coagulation factor polymorphisms per se,
previously associated with plasma levels, and the risk of recurrent cardiovascular events in
myocardial infarction survivors.
Ambient air pollution has been linked to exacerbation of cardiovascular disease morbidity and
mortality 4. Systemic inflammation induced by particle deposition in the lung is one of the potential
mechanisms linking ambient air pollution to myocardial infarctions 4;5. Evidence has been reported
that fibrinogen concentrations increase in association with high ambient air pollution concentrations
during the preceding days 6-8.
The aim of the study presented here was to assess whether genetic polymorphisms within the
fibrinogen genes (FGA (α-chain), FGB (β-chain) and FGG (γ-chain)) modify the associations
between changes in ambient particle concentrations and plasma fibrinogen levels. The study focused
Page 3 of 40
4
on myocardial infarction survivors 9, a potentially susceptible subgroup of the general population
with respect to air pollution 10.
Some of the results of this study have been previously reported in the form of an abstract 11.
METHODS
Field study
Fibrinogen concentrations were assessed in a multi-centre longitudinal study of myocardial
infarction survivors from five European cities – Augsburg, Germany; Barcelona, Spain; Helsinki,
Finland; Rome, Italy; Stockholm, Sweden - the so-called AIRGENE study. A detailed description of
the design of the study is published elsewhere 9. Study protocols were approved by the local human
subjects committees and written informed consent was obtained from all patients.
Fibrinogen was analyzed by immunonephelometry (Dade Behring Marburg GmbH, Marburg,
Germany) in 5327 EDTA-plasma samples collected between May 2003 and July 2004 from 895
myocardial infarction survivors. Data on particulate matter with an aerodynamic diameter below 10
µm or 2.5 µm (PM10 or PM2.5, respectively), particle number concentrations (PNC), temperature and
relative humidity were collected for each city 9 and aggregated to daily means according to standard
procedures 12.
Genotyping
DNA was extracted from EDTA anticoagulated blood using a salting out procedure. Twenty-one
single nucleotide polymorphisms (SNPs) for FGA, FGB and FGG were selected and genotyped 9.
Genotyping success rates ranged between 97.9% for rs2070011 and 99.8% for rs1800791.
Page 4 of 40

5
SNP selection
All SNPs were within Hardy Weinberg equilibrium (p-values > 0.05) as tested by means of a χ2 test
or Fisher’s exact test depending on allele frequency for all cities combined 2. We selected SNPs that
were associated with fibrinogen levels in our sample; P-values smaller than 0.05/10=0.005 were
considered as statistically significant, because we estimated according to Li and Ji 13, that the 21
SNPs represented about 10 effective uncorrelated loci. This criterion was met by a total of 7 SNPs
from FGA (rs2070006 and rs2070011) and FGB (rs1800790, rs1800791, rs2223799, rs6056 and
rs4220) and these were selected for the analysis of gene-environment interactions.
Linkage disequilibrium and correlation between all 21 SNPs are shown in Figure 1 in the online
supplement.
Statistical analysis of the SNPs selected for investigating gene-environment interaction
The main effect of the SNPs on fibrinogen was estimated using linear mixed models with random
subject-specific intercepts adjusting linearly for the variables age, BMI, ratio of HDL / total
cholesterol, pack-years smoked, NT-proBNP, and HbA1c and for the categorical variables city,
gender, and history of stroke, arrhythmia, asthma or arthrosis. SNPs were coded applying an additive
genetic model (ordinal variable coded 0, 1, 2 representing the number of copies of the minor allele),
which assumes that two alleles have twice the effect of one allele. We tested for evidence against the
additive genetic model 14 by additionally including an indicator variable for heterozygous subjects
(1= heterozygous, 0=else). This model has the advantage that it simultaneously allows to estimate
the additive genetic effect and to test whether there is evidence for departure from the additive effect
model. We also performed a likelihood ratio test comparing the model including the indicator to the
model with only the additive effect to derive the better fitting model.
Page 5 of 40
6
The main effect of particulate matter on fibrinogen was estimated in city-specific additive mixed
models adjusting for patient characteristics, time trend and weather to accommodate the differences
of the panel characteristics and meteorological conditions across Europe as previously reported 8 (see
Table 1 in the online supplement).
Gene-environment interactions were estimated for each SNP in models including the main effect of
the SNP, the main air pollution effect, the interaction term between air pollution and SNP, and
selected city-specific time-invariant risk factors and time-varying factors as independent variables
(see Table 1 in the online supplement). The 5-day period before blood withdrawal was selected as
primary exposure window for all gene-environment interaction analyses as in earlier analyses 8. As
secondary analyses we explored shorter time windows of exposure.
For the gene-environment interactions, air pollution effect estimates are presented by genotype.
These estimates and 95% confidence intervals were calculated based on the estimated PM-main
effects, the PM-SNP interactions, and their respective estimated variances and co-variances.
Estimates are presented for an increase of the pollutants corresponding to the interquartile range and
are expressed as % change of the overall mean in fibrinogen. For overall results, city-specific effect
estimates were pooled using meta-analysis methodology 15. Heterogeneity of the effect estimates
between cities was assessed with a χ2 test with 4 degrees of freedom. If the χ2 test suggested
heterogeneity between the city-specific effect estimates (p-values <0.1), city-specific estimates were
combined using random effect models 15. Otherwise, fixed effect models calculating variance-
weighted averages of the city-specific estimates were applied.
As sensitivity analysis, we calculated haplotypes for the 4 correlated SNPs in FGB using the
expectation-maximization algorithm presented by Schaid et al. 16 with SNPs entered in gene-specific
reading directions. We found two haplotypes with a frequency ≥5% (see Table 2 in the online
Page 6 of 40
7
supplement). We collapsed the three rare haplotypes with a frequency < 5% into one group. For
assessing the PM-haplotype interactions, we used the same model as for the single SNP analysis to
test single haplotypes (assuming an additive genetic effect model) against all other haplotypes while
including indicators for the haplotyes and rare haploytpes as main effects.
RESULTS
Middle-aged men who had survived their myocardial infarction on average for more than two years
were recruited from five European cities (Table 1). Overall, 5.95 repeated fibrinogen measurements
per person were obtained in 854 subjects (99% of 6 scheduled samples). Mean fibrinogen levels
showed some variation across cities (ANOVA, p<0.001). PM10, PM2.5 and coarse particles (defined
as PM10 minus PM2.5) were moderately to highly correlated (r2>0.70), while correlations between
PM and PNC were low to moderate in the different cities (-0.15 < r2 <0.60) 8. We had hypothesized
that elevated ambient particulate matter concentrations over the past 5 days were associated with
fibrinogen levels and observed a 0.6% increase per 13.5µg/m3 PM10 (95% confidence interval: 0.1%
to 1.1%) as reported previously 8.
Less than 5% of the population was homozygous with respect to the minor alleles of the FGB SNPs,
but more that 15% was homozygous with respect to the minor alleles of the FGA SNPs (Table 2).
The SNPs comprised three clusters: (a) the two FGA SNPs (r2=0.97), (b) the FGB SNPs rs1800790,
rs2227399, rs6056 and rs4220 (r2>0.88), and (c) the FGB SNP rs1800791 (see Figure 1 in the online
supplement). Between the three clusters no strong correlation was observed (r2<0.12). Genotype
frequencies differed between the cities for FGA rs2070011 and rs2070006 (ANOVA, p<0.02) and
for FGB rs1800790, rs1800791 and rs2227399 (ANOVA, p<0.03) (Figure 1).
Page 7 of 40

8
The minor alleles of the SNPs within the FGA and FGB gene were associated with increased
fibrinogen levels, with the exception of rs1800791, where the minor allele was associated with
decreased fibrinogen levels (Table 2). There was no evidence for deviation from the additive genetic
model for any of the SNPs, neither testing the indicator variable for significance, nor applying the
likelihood ratio test (p-value of the additional indicator ranged from 0.12 to 0.77 and p-values of the
likelihood ratio test ranged from 0.11 to 0.75).
The homozygous genotypes of the major allele of FGA rs2070006 and rs2070011 (cluster 1) showed
augmented fibrinogen response to increased PM10, although the interaction was not statistically
significant (Table 3). In contrast, the four correlated FGB SNPs (cluster 2) indicated larger
fibrinogen response to increased PM10 for subjects who were homozygous for the minor allele (p-
values < 0.04 for all interaction terms). An 8 to 11-fold difference in the fibrinogen response to
increased PM10 was observed for the homozygous minor alleles compared to the homozygous major
alleles in this cluster. These results were confirmed by applying a haplotype analysis to these four
SNPs. Effects of similar magnitude were found for the presence of all four minor alleles. Only weak
evidence for effect modification by the genotypes of the SNP representing cluster 3 was found.
For the minor allele of FGB rs1800790, the observed increase of fibrinogen level in association with
5-day averages of particulate matter was quite consistent across cities, with no evidence for
significant heterogeneity across cities (Figure 2A). The analyses considering different induction
times between ambient particulate matter concentrations and fibrinogen levels suggested that the
association with particulate matter concentrations in subjects with the minor allele was delayed and
cumulative over the 5 days before the blood withdrawal (Figure 2B). Fibrinogen responses to PM2.5
and coarse particles were generally consistent with the observed PM10 effect, while no effect was
observed for PNC (Figure 3).
Page 8 of 40

9
Additional adjustments for statin therapy slightly weakened the modification by FGB rs1800790
(2.05% increase in fibrinogen (95% CI: 0.61% to 3.50%) for the 22 genotype, 1.18% (95% CI:
0.43% to 1.92%) for the 12 genotype, and 0.18% (95% CI: -0.46% to 0.83%) for the 11 genotype for
a 13.5 µg/m3 increase in PM10; interaction term p=0.039). All models were adjusted for pack-years
smoked; additionally adjusting for current smoking in the past 24 hours slightly strengthened the
interaction (2.16% increase in fibrinogen (95% CI: 0.67% to 3.85%) for the 22 genotype, 1.20%
(95% CI: 0.44% to 1.96%) for the 12 genotype, and 0.09% (95% CI: -0.57% to 0.75%) for the 11
genotype for a 13.5 µg/m3 increase in PM10; interaction term p=0.026). Excluding current smokers
left the associations unaltered (see Figure 2 in the online supplement). However, excluding current
smokers and days on which participants reported environmental tobacco smoke exposures from the
analyses increased the estimates of the PM-fibrinogen response (see Figure 2 in the online
supplement).
As sensitivity analysis we also applied a dominant genetic model, i.e. set 0=homozygous major (11
genotype) and 1= hetero-/homozygous minor (12 genotype or 22 genotype). For a 13.5 µg/m3
increase in PM10, we estimated a 1.31% increase in fibrinogen (95% CI: 0.51% to 2.10%) for the 11
genotype of FGA rs2070011 and 0.33% increase in fibrinogen (95% CI: -0.61% to 1.28%) for the 12
or 22 genotype; interaction term not significant (p=0.25). We estimated a 1.41% increase in
fibrinogen associated with a 13.5 µg/m3 increase in PM10 (95% CI: 0.60% to 2.23%) for the 12 or 22
genotype of FGB rs1800790 and 0.24% increase (95% CI: -0.40% to 0.89%) for the 11 genotype; the
interaction term was statistically significant (p=0.029).
DISCUSSION
In this study, promoter polymorphisms within FGA and FGB were associated with modifications of
the fibrinogen response to ambient particulate matter. The synthesis of the FGB chain is the rate-
Page 9 of 40
10
limiting factor for the production of fibrinogen 17. Therefore, during the last few years, interest has
focused on the potential role of genetic variability within FGB on the regulation of fibrinogen levels
18. Indeed, SNPs on FGB have been associated with fibrinogen levels 2;18-20 with G455A (FGB
rs1800790) being among the most widely studied 21;22. The rs1800790 SNP locus on the FGB gene is
considered as the physiologically most relevant, since it has distinct nuclear protein-binding
properties 21. Although most clinical studies have suggested that G455A is associated with plasma
fibrinogen levels 22, this is not a uniform finding throughout the literature 23, suggesting that other
factors such as complex gene-environment interactions 22 or the underlying inflammatory status or
disease state could be important modifiers of this relationship. The PM-fibrinogen relationship is
eightfold stronger in subjects with the homozygous minor allele genotype of FGB rs1800790 than for
subjects with the homozygous major allele genotype. Marginally stronger modification of the PM-
fibrinogen relationship was observed for the other three studied FGB SNPs that are highly correlated
with rs1800790 and with each other, namely rs2227399, rs6056 and in particular rs4220, the latter
resulting in an amino acid exchange. However, for a potential environmental stimulus such as
ambient particulate matter, modified plasma fibrinogen levels based on a promoter polymorphism
may be considered more plausible, although feedback mechanisms depending on protein variants
could produce similar effects. Also, a haplotype analysis within this cluster suggested that these
highly correlated SNPs form a “yin yang haplotype” 24, so that a clear attribution to one of the SNPs
seems to be impossible. For FGA rs2070011, the PM-fibrinogen response was sevenfold higher for
subjects with the homozygous major allele genotype than for subjects with the homozygous minor
allele genotype but the interaction was not statistically significant. Previous analyses of the
biochemical properties of fibrin clot structures have suggested that clots are more porous in the
presence of the minor allele of rs2070011 25. In addition, in our data 2, we have previously shown
that FGA rs2070011 modified the associations between IL-6 and fibrinogen levels, leaving room for
Page 10 of 40

11
the speculation that inflammatory stimulation by time-varying factors such as air pollution might be
relevant.
The overall estimate for the PM10-fibrinogen response was small. We found that an increase of 25
µg/m3 in PM10 (five-day average) in those homozygous in the minor allele of FGB rs1800790 has a
similar effect to an increase of 5 kg/m2 in BMI (3.9% (95%CI: 2.6% to 5.3%)) when estimated in the
same model. Increases of this magnitude occur repeatedly in Southern Europe and were also
observed in the Nordic Cities. The results of this study on short-term effects of ambient particulate
matter suggest that increases in fibrinogen levels can be observed repeatedly in urban areas in
susceptible subpopulations. The study presented here is a large multi-center study using repeated
measurements to assess gene-environment interactions, purposely designed for this research
question. However, the multi-centre design might also have contributed to an increase in study
heterogeneity, which may not have been entirely removed by conducting city-specific analyses and
subsequent pooling of the effect estimates. The application of a two-step approach allowed the
specification of the genetic model and the selection of confounder variables and of induction times
for the PM-fibrinogen analyses independently of the gene-environment analyses. While considerable
variation in the effect estimates was observed between the cities, the test for heterogeneity, although
of low power, suggested that these variations were within the range of the statistical variability to be
expected. Nevertheless, the pooled estimates for the effect modification by FGB rs1800790 and FGA
rs2070011 are dominated by the data from Southern Europe. The minor alleles were even more
frequent in the Nordic samples than in the Southern European samples. One has to note that while
the number of available blood samples was among the highest in the Nordic countries, analyses have
somewhat less power in the Nordic countries than in Southern Europe due to lower average exposure
and lower absolute variation in ambient particulate matter. Also, particulate air pollution composition
is considered to be more toxic in Southern Europe 26, while at the same time dietary habits might
Page 11 of 40

12
provide protection 27. For the present study we hypothesized that the associations between ambient
particulate matter and fibrinogen would be observed for cumulative air pollution exposure over
several days 8 due to the half-life of fibrinogen of two to three days. We consistently observed
delayed responses in the study. For the subjects who had one or two minor alleles of rs1800790, the
pattern observed with respect to induction time was very consistent with a delayed and cumulative
response over several days and the pattern was also similar for FGA rs2070011. Excluding smokers
(N=39) or smokers and subjects passively (N= 86) exposed to tobacco smoke showed consistent and
slightly larger effect estimates. This result substantiates the reported findings as active smoking or
environmental tobacco smoke exposure increases the subjects’ exposure to particles, but is
considered to be uncorrelated to ambient concentrations of particles.
Ambient particulate matter has been implicated to alter cardiac and vascular function 4;5 and it has
been demonstrated that these effects occur within hours and persist over several days 28. Evidence for
associations between ambient air pollution and fibrinogen level have been observed in
epidemiological 6-8;29 and controlled settings 30-32, but not uniformly 33-36. One potential pathway by
which ambient particulate matter elicits sub-clinical inflammatory responses may be oxidative stress
induced by inhaled particles 37. The discussed mechanisms range from local oxygen radical
production in the lung due to transition metal catalyzed Fenton-reactions to systemic oxidative stress
caused by translocated ultrafine particles with a capacity to produce oxygen radicals based on their
surface area properties. In subjects with impaired detoxification metabolism due to a deletion in
glutathione S transferase M1, effect modification of responses to diesel exposure 38, ambient
particulate matter 39 and ozone 40;41 have been observed consistently. In addition, polymorphisms in
the hemochromatosis gene (HFE), which modulates the uptake from iron and divalent cations and
reduces their toxicities, appears to modify responses to ambient particles 42. Similarly, data from the
same study suggested that the GT short tandem repeat polymorphism in the heme oxygenase-1
Page 12 of 40

13
promoter modified the air pollution impact and suggested a three-way interaction with glutathione S
transferase M1 43. The data we present in this paper suggests that genetic susceptibility might not
only be determined by factors which impact the strength and persistence of oxidative stress, but also
by polymorphisms that alter early physiological responses. In particular, our results suggest that
genetically determined susceptibility to ambient particulate matter may include polymorphisms
which alter the transcription rate of systemic markers such as fibrinogen. The effect modification
reported here may in part explain the heterogeneous findings in studies assessing the PM-fibrinogen
response in epidemiological settings with small samples sizes 6-8;29;33-36.
As fibrinogen is a substrate for coagulation and an acute phase protein, subjects with variants of
these frequent SNPs may experience increased risks not only due to constitutionally higher
fibrinogen concentrations, but also due to an augmented response to environmental inflammatory
stimuli such as ambient particulate matter. A meta-analysis of FGB rs1800787 highly correlated to
FGB rs1800790 did not show a direct overall association with an elevated risk of myocardial
infarction 44. In addition, no association was found between a number of coagulation factor
polymorphisms previously associated with plasma levels, and the risk of recurrent cardiovascular
events in myocardial infarction survivors 3. Nevertheless, the gene-environment interaction seen here
for rs1800790 may in part contribute to an elevated risk of myocardial infarction observed for
elevated plasma levels of fibrinogen 1 for those with higher exposures to particulate matter since the
exposures, while variable in space and time, are ubiquitous. However, this is speculation until
follow-up data on the patient sample becomes available.
In conclusion, the gene-environment interaction demonstrated here may contribute to the overall
burden of disease observed for particulate matter 45;46 and render a relatively large subgroup of the
Caucasian population more susceptible than currently estimated.
Page 13 of 40

14
ACKNOWLEDGEMENT
The AIRGENE study was funded as part of the European Union’s 5th Framework Program, key
action number 4: “Environment and Health”, contract number QLRT-2002-02236.
The AIRGENE study group comprises the following partners:
1. Helmholtz Zentrum München - German Research Centre for Environmental Health, Institute of
Epidemiology (Neuherberg, Germany): A. Peters (Coordinator, PI), M.-A. Bind, S. Breitner, I.
Brueske-Hohlfeld, H. Chavez, J. Cyrys, U. Geruschkat, H. Grallert, S. Greven, A. Ibald-Mulli, T.
Illig, H. Kirchmair, S. von Klot, M. Kolz, M. Marowsky-Koeppl, M. Mueller, R. Rückerl, A.
Schaffrath Rosario, A. Schneider, G. Walter, H.-E. Wichmann; Institute of Health Economics and
Health Care Management (Neuherberg, Germany): R. Holle, H. Nagl; KORA Study Center
(Augsburg, Germany): I. Fabricius, C. Greschik, F. Günther, M. Haensel, U. Hahn, U. Kuch, C.
Meisinger, M. Pietsch, E. Rempfer, G. Schaich, A. Schneider, I. Schwarzwälder, B. Zeitler; KORA
Myocardial Infarction Registry (Augsburg, Germany): H. Loewel; Ludwig-Maximilians University
(Munich, Germany): H. Küchenhoff, A. Ossig.
2. University of Ulm, Department of Cardiology (Germany): W. Koenig (PI), N. Khuseyinova, G.
Trischler.
3. Local Health Authority RM E, Department of Epidemiology ASL RME (Rome, Italy): F. Forastiere
(PI), P. Compagnucci, F. Di Carlo, M. Ferri, A. Montanari, C. Perucci, S. Picciotto, E. Romeo, M.
Stafoggia; Catholic University (Rome, Italy): R. Pistelli, L. Altamura, M.R. Andreani, F. Baldari, F.
Infusino, P. Santarelli; Hospital San Filippo Neri: A.P. Jesi; Italian National Institute of Health
(Rome, Italy): G. Cattani, A. Marconi.
Page 14 of 40

15
4. National Public Health Institute (KTL) (Kuopio/Helsinki, Finland): J. Pekkanen (PI), M. Alanne,
H. Alastalo, T. Eerola, J. Eriksson, T. Kauppila, T. Lanki, P. Nyholm, M. Perola, V. Salomaa, P.
Tiittanen; Helsinki University Central Hospital: K. Luotola.
5. Institute of Environmental Medicine, Karolinska Institute (Stockholm, Sweden): Department of
Occupational and Environmental Health, Stockholm County Council (Stockholm, Sweden);
Department of Cardiology, Stockholm South Hospital (Stockholm, Sweden): T. Bellander (PI), N.
Berglind, K. Bohm, R. Härdén, E. Lampa, P. Ljungman, F. Nyberg, B. Ohlander, G. Pershagen, M.
Rosenqvist, T. Larsdotter Svensson, E. Thunberg, G. Wedeen.
6. Municipal Institute of Medical Research (Barcelona, Spain): J. Sunyer (PI), M. Covas, M. Fitó,
M. Grau, B. Jacquemin, J. Marrugat, L. Muñoz, G. Perelló, E. Plana, C. Rebato, H. Schroeder, C.
Soler.
7. University of Athens Medical School, Department of Hygiene and Epidemiology (Athens, Greece):
K. Katsouyanni (PI), A. Chalamandaris, K. Dimakopoulou, D. Panagiotakos; Department of
Cardiology (Athens, Greece): C. Stefanadis, C. Pitsavos, C. Antoniades, C. Chrysohoou, J.
Mitropoulos.
8. University of Helsinki, Department of Physical Sciences (Helsinki, Finland): M. Kulmala (PI), P.
Aalto, P. Paatero.
Fredrik Nyberg, employed by AstraZeneca, is also Lecturer in Epidemiology at Karolinska Institute.
AstraZeneca did not contribute any direct financing to this study.
The statistical and genetic group was funded by the National Genome Research Net of the German
Ministry of Education and Research, the “Sonderforschungsbereich-SFB-386”, and the Munich
Center of Health of the Ludwig-Maximilians-Universität München, Germany.
Page 15 of 40

16
Regina Rückerl, Alexandra Henneberger and Annette Peters were in part funded by the U.S.
Environmental Protection Agency (EPA) STAR program grant RD83241501.
Page 16 of 40

17
REFERENCES
1. Danesh, J., S. Lewington, S. G. Thompson, G. D. Lowe, R. Collins, J. B. Kostis, A. C. Wilson, A.
R. Folsom, K. Wu, M. Benderly, U. Goldbourt, J. Willeit, S. Kiechl, J. W. Yarnell, P. M.
Sweetnam, P. C. Elwood, M. Cushman, B. M. Psaty, R. P. Tracy, A. Tybjaerg-Hansen, F.
Haverkate, M. P. de Maat, S. G. Thompson, F. G. Fowkes, A. J. Lee, F. B. Smith, V. Salomaa, K.
Harald, R. Rasi, E. Vahtera, P. Jousilahti, J. Pekkanen, R. D'Agostino, W. B. Kannel, P. W.
Wilson, G. Tofler, C. L. Arocha-Pinango, A. Rodriguez-Larralde, E. Nagy, M. Mijares, R.
Espinosa, E. Rodriquez-Roa, E. Ryder, M. P. Diez-Ewald, G. Campos, V. Fernandez, E. Torres,
E. Coll, R. Marchioli, F. Valagussa, A. Rosengren, L. Wilhelmsen, G. Lappas, H. Eriksson, P.
Cremer, D. Nagel, J. D. Curb, B. Rodriguez, K. Yano, J. T. Salonen, K. Nyyssonen, T. P.
Tuomainen, B. Hedblad, P. Lind, H. Loewel, W. Koenig, T. W. Meade, J. A. Cooper, B. De
Stavola, C. Knottenbelt, G. J. Miller, J. A. Cooper, K. A. Bauer, R. D. Rosenberg, S. Sato, A.
Kitamura, Y. Naito, H. Iso, V. Salomaa, K. Harald, V. Rasi, E. Vahtera, P. Jousilahti, T. Palosuo,
P. Ducimetiere, P. Amouyel, D. Arveiler, A. E. Evans, J. Ferrieres, I. Juhan-Vague, A. Bingham,
H. Schulte, G. Assmann, B. Cantin, B. Lamarche, J. P. Despres, G. R. Dagenais, H. Tunstall-
Pedoe, M. Woodward, Y. Ben Shlomo, S. G. Davey, V. Palmieri, J. L. Yeh, T. W. Meade, A.
Rudnicka, C. Knottenbelt, P. Ridker, F. Rodeghiero, A. Tosetto, J. Shepherd, I. Ford, M.
Robertson, E. Brunner, M. Shipley, E. J. Feskens, and D. Kromhout. 2005. Plasma fibrinogen
level and the risk of major cardiovascular diseases and nonvascular mortality: an individual
participant meta-analysis. JAMA 294:1799-1809.
Page 17 of 40

18
2. Jacquemin, B., C. Antoniades, F. Nyberg, E. Plana, M. Muller, S. Greven, V. Salomaa, J. Sunyer,
T. Bellander, A. G. Chalamandaris, R. Pistelli, W. Koenig, and A. Peters. 2008. Common Genetic
Polymorphisms and Haplotypes of Fibrinogen Alpha, Beta, and Gamma Chains Affect
Fibrinogen Levels and the Response to Proinflammatory Stimulation in Myocardial Infarction
Survivors The AIRGENE Study. J.Am.Coll.Cardiol. 52:941-952.
3. van der Krabben, M. D., F. R. Rosendaal, J. G. van der Bom, and C. J. Doggen. 2008.
Polymorphisms in coagulation factors and the risk of recurrent cardiovascular events in men after
a first myocardial infarction. J.Thromb.Haemost. 6:720-725.
4. Brook, R. D., B. Franklin, W. E. Cascio, Y. Hong, G. Howard, M. Lipsett, R. V. Luepker, M. A.
Mittleman, J. M. Samet, S. C. Smith, Jr., and I. B. Tager. 2004. Air Pollution and Cardiovascular
Disease: A statement of the health care professionals from the expert panel on population and
prevention science of the American Heart Association. Circulation 109:2655-2671.
5. Schulz, H., V. Harder, A. Ibald-Mulli, A. Khandoga, W. Koenig, F. Krombach, R. Radykewicz,
A. Stampfl, B. Thorand, and A. Peters. 2005. Cardiovascular effects of fine and ultrafine
particles. J.Aerosol Med. 18:1-22.
6. Pekkanen, J., E. J. Brunner, H. R. Anderson, P. Tiittanen, and R. W. Atkinson. 2000. Daily
concentrations of air pollution and plasma fibrinogen in London. Occup Environ Med 57:818-
822.
7. Schwartz, J. 2001. Air pollution and blood markers of cardiovascular risk. Environ Health
Perspect. 109:405-409.
8. Ruckerl, R., S. Greven, P. Ljungman, P. Aalto, C. Antoniades, T. Bellander, N. Berglind, C.
Chrysohoou, F. Forastiere, B. Jacquemin, S. von Klot, W. Koenig, H. Kuchenhoff, T. Lanki, J.
Page 18 of 40

19
Pekkanen, C. A. Perucci, A. Schneider, J. Sunyer, and A. Peters. 2007. Air pollution and
inflammation (interleukin-6, C-reactive protein, fibrinogen) in myocardial infarction survivors.
Environ Health Perspect. 115:1072-1080.
9. Peters, A., A. Schneider, S. Greven, T. Bellander, F. Forastiere, A. Ibald-Mulli, T. Illig, B.
Jacquemin, K. Katsouyanni, W. Koenig, T. Lanki, J. Pekkanen, G. Pershagen, S. Picciotto, R.
Ruckerl, A. S. Rosario, C. Stefanadis, and J. Sunyer. 2007. Air pollution and inflammatory
response in myocardial infarction survivors: gene-environment interactions in a high-risk group.
Inhal Toxicol 19 Suppl 1:161-175.
10. von Klot, S., A. Peters, P. Aalto, T. Bellander, N. Berglind, D. D'Ippoliti, R. Elosua, A. Hormann,
M. Kulmala, T. Lanki, H. Lowel, J. Pekkanen, S. Picciotto, J. Sunyer, and F. Forastiere. 2005.
Ambient air pollution is associated with increased risk of hospital cardiac readmissions of
myocardial infarction survivors in five European cities. Circulation 112:3073-3079.
11. Peters, A., Greven, S., Heid, I., Baldari, F., Bellander, T., Chrysohoon, C., Illig, T., Jacquemin,
B., Koenig, W., Landi, T., Nyberg, F., Pekkanen, J., Pistelli, R., Rückerl, R., Stefanadis, C.,
Schneider, A., Sunyer, J., and Wichmann, H.-E. SNPs in the Fibrinogen Gene Cluster Modify
Fibrinogen Response to Ambient Particulate Matter. Epidemiology 18[5], S115-S116. 2007.
12. Katsouyanni, K., D. Zmirou, C. Spix, J. Sunyer, J. P. Schouten, A. Ponka, H. R. Anderson, Y. Le
Moullec, B. Wojtyniak, M. A. Vigotti, and et al. 1995. Short-term effects of air pollution on
health: a European approach using epidemiological time-series data. The APHEA project:
background, objectives, design. Eur.Respir.J. 8:1030-1038.
13. Li, J. and L. Ji. 2005. Adjusting multiple testing in multilocus analyses using the eigenvalues of a
correlation matrix. Heredity 95:221-227.
Page 19 of 40
20
14. Schaid, D. J. 2004. Evaluating associations of haplotypes with traits. Genet.Epidemiol. 27:348-
364.
15. van Houwelingen, H. C., L. R. Arends, and T. Stijnen. 2002. Advanced methods in meta-analysis:
multivariate approach and meta-regression. Stat.Med. 21:589-624.
16. Schaid, D. J., C. M. Rowland, D. E. Tines, R. M. Jacobson, and G. A. Poland. 2002. Score tests
for association between traits and haplotypes when linkage phase is ambiguous. Am.J.Hum.Genet.
70:425-434.
17. Roy, S. N., G. Mukhopadhyay, and C. M. Redman. 1990. Regulation of fibrinogen assembly.
Transfection of Hep G2 cells with B beta cDNA specifically enhances synthesis of the three
component chains of fibrinogen. J Biol.Chem. 265:6389-6393.
18. Behague, I., O. Poirier, V. Nicaud, A. Evans, D. Arveiler, G. Luc, J. P. Cambou, P. Y. Scarabin,
L. Bara, F. Green, and F. Cambien. 1996. Beta fibrinogen gene polymorphisms are associated
with plasma fibrinogen and coronary artery disease in patients with myocardial infarction. The
ECTIM Study. Etude Cas-Temoins sur l'Infarctus du Myocarde. Circulation 93:440-449.
19. Thomas, A. E., F. R. Green, C. H. Kelleher, H. C. Wilkes, P. J. Brennan, T. W. Meade, and S. E.
Humphries. 1991. Variation in the promoter region of the beta fibrinogen gene is associated with
plasma fibrinogen levels in smokers and non-smokers. Thromb.Haemost. 65:487-490.
20. Kathiresan, S., Q. Yang, M. G. Larson, A. L. Camargo, G. H. Tofler, J. N. Hirschhorn, S. B.
Gabriel, and C. J. O'Donnell. 2006. Common Genetic Variation in Five Thrombosis Genes and
Relations to Plasma Hemostatic Protein Level and Cardiovascular Disease Risk.
Arterioscler.Thromb.Vasc.Biol. 26:1405-1412.
Page 20 of 40

21
21. 't Hooft, F. M., S. J. von Bahr, A. Silveira, A. Iliadou, P. Eriksson, and A. Hamsten. 1999. Two
common, functional polymorphisms in the promoter region of the beta-fibrinogen gene contribute
to regulation of plasma fibrinogen concentration. Arterioscler.Thromb.Vasc.Biol. 19:3063-3070.
22. Voetsch, B. and J. Loscalzo. 2004. Genetic determinants of arterial thrombosis.
Arterioscler.Thromb.Vasc.Biol. 24:216-229.
23. Friedlander, Y., J. D. Kark, R. Sinnreich, F. Basso, and S. E. Humphries. 2003. Combined
segregation and linkage analysis of fibrinogen variability in Israeli families: evidence for two
quantitative-trait loci, one of which is linked to a functional variant (-58G > A) in the promoter of
the alpha-fibrinogen gene. Ann.Hum.Genet. 67:228-241.
24. Zhang, J., W. L. Rowe, A. G. Clark, and K. H. Buetow. 2003. Genomewide distribution of high-
frequency, completely mismatching SNP haplotype pairs observed to be common across human
populations. Am.J.Hum.Genet. 73:1073-1081.
25. Mannila, M. N., P. Eriksson, C. G. Ericsson, A. Hamsten, and A. Silveira. 2006. Epistatic and
pleiotropic effects of polymorphisms in the fibrinogen and coagulation factor XIII genes on
plasma fibrinogen concentration, fibrin gel structure and risk of myocardial infarction.
Thromb.Haemost. 95:420-427.
26. Katsouyanni, K., G. Touloumi, E. Samoli, A. Gryparis, A. Le Tertre, Y. Monopolis, G. Rossi, D.
Zmirou, F. Ballester, A. Boumghar, H. R. Anderson, B. Wojtyniak, A. Paldy, R. Braunstein, J.
Pekkanen, C. Schindler, and J. Schwartz. 2001. Confounding and effect modification in the short-
term effects of ambient particles on total mortality: results from 29 European cities within the
APHEA2 project. Epidemiology 12:521-531.
Page 21 of 40

22
27. Romieu, I., F. Castro-Giner, N. Kunzli, and J. Sunyer. 2008. Air pollution, oxidative stress and
dietary supplementation: a review. Eur.Respir.J. 31:179-197.
28. Peters, A. 2005. Particulate matter and heart disease: Evidence from epidemiological studies.
Toxicol.Appl.Pharmacol. 207:477-482.
29. Chuang, K. J., C. C. Chan, T. C. Su, C. T. Lee, and C. S. Tang. 2007. The effect of urban air
pollution on inflammation, oxidative stress, coagulation, and autonomic dysfunction in young
adults. Am.J.Respir.Crit Care Med. 176:370-376.
30. Elder, A. C., R. Gelein, M. Azadniv, M. Frampton, J. Finkelstein, and G. Oberdorster. 2004.
Systemic effects of inhaled ultrafine particles in two compromised, aged rat strains. Inhal.Toxicol.
16:461-471.
31. Gardner, S. Y., J. R. Lehmann, and D. L. Costa. 2000. Oil fly ash-induced elevation of plasma
fibrinogen levels in rats. Toxicol.Sci. 56:175-180.
32. Rivero, D. H., S. R. Soares, G. Lorenzi-Filho, M. Saiki, J. J. Godleski, L. Antonangelo, M.
Dolhnikoff, and P. H. Saldiva. 2005. Acute cardiopulmonary alterations induced by fine
particulate matter of Sao Paulo, Brazil. Toxicol.Sci. 85:898-905.
33. Baccarelli, A., A. Zanobetti, I. Martinelli, P. Grillo, L. Hou, S. Giacomini, M. Bonzini, G.
Lanzani, P. M. Mannucci, P. A. Bertazzi, and J. Schwartz. 2007. Effects of exposure to air
pollution on blood coagulation. J.Thromb.Haemost. 5:252-260.
34. Brauner, E. V., L. Forchhammer, P. Moller, L. Barregard, L. Gunnarsen, A. Afshari, P. Wahlin,
M. Glasius, L. O. Dragsted, S. Basu, O. Raaschou-Nielsen, and S. Loft. 2008. Indoor particles
Page 22 of 40

23
affect vascular function in the aged: an air filtration-based intervention study. Am.J.Respir.Crit
Care Med. 177:419-425.
35. Ruckerl, R., A. Ibald-Mulli, W. Koenig, A. Schneider, G. Woelke, J. Cyrys, J. Heinrich, V.
Marder, M. Frampton, H. E. Wichmann, and A. Peters. 2006. Air pollution and markers of
inflammation and coagulation in patients with coronary heart disease. Am J Respir Crit Care Med
173:432-441.
36. Sullivan, J. H., R. Hubbard, S. L. Liu, K. Shepherd, C. A. Trenga, J. Q. Koenig, W. L. Chandler,
and J. D. Kaufman. 2007. A community study of the effect of particulate matter on blood
measures of inflammation and thrombosis in an elderly population. Environ Health 6:3.
37. Donaldson, K., V. Stone, A. Seaton, and W. MacNee. 2001. Ambient particle inhalation and the
cardiovascular system: potential mechanisms. Environ Health Perspect. 109:523-527.
38. Gilliland, F. D., Y. F. Li, A. Saxon, and D. Diaz-Sanchez. 2004. Effect of glutathione-S-
transferase M1 and P1 genotypes on xenobiotic enhancement of allergic responses: randomised,
placebo-controlled crossover study. Lancet 363:119-125.
39. Schwartz, J., S. K. Park, M. S. O'Neill, P. S. Vokonas, D. Sparrow, S. Weiss, and K. Kelsey.
2005. Glutathione-S-transferase M1, obesity, statins, and autonomic effects of particles: gene-by-
drug-by-environment interaction. Am.J.Respir.Crit Care Med. 172:1529-1533.
40. Romieu, I., M. Ramirez-Aguilar, J. J. Sienra-Monge, H. Moreno-Macias, B. E. Rio-Navarro, G.
David, J. Marzec, M. Hernandez-Avila, and S. London. 2006. GSTM1 and GSTP1 and
respiratory health in asthmatic children exposed to ozone. Eur.Respir.J. 28:953-959.
Page 23 of 40

24
41. Romieu, I., J. J. Sienra-Monge, M. Ramirez-Aguilar, H. Moreno-Macias, N. I. Reyes-Ruiz, d. R.-
N. Estela, M. Hernandez-Avila, and S. J. London. 2004. Genetic polymorphism of GSTM1 and
antioxidant supplementation influence lung function in relation to ozone exposure in asthmatic
children in Mexico City. Thorax 59:8-10.
42. Park, S. K., M. S. O'Neill, R. O. Wright, H. Hu, P. S. Vokonas, D. Sparrow, H. Suh, and J.
Schwartz. 2006. HFE genotype, particulate air pollution, and heart rate variability: a gene-
environment interaction. Circulation 114:2798-2805.
43. Chahine, T., A. Baccarelli, A. Litonjua, R. O. Wright, H. Suh, D. R. Gold, D. Sparrow, P.
Vokonas, and J. Schwartz. 2007. Particulate air pollution, oxidative stress genes, and heart rate
variability in an elderly cohort. Environ.Health Perspect. 115:1617-1622.
44. Keavney, B., J. Danesh, S. Parish, A. Palmer, S. Clark, L. Youngman, M. Delepine, M. Lathrop,
R. Peto, and R. Collins. 2006. Fibrinogen and coronary heart disease: test of causality by
'Mendelian randomization'. Int.J.Epidemiol. 35:935-943.
45. Pope, C. A., III, R. T. Burnett, M. J. Thun, E. E. Calle, D. Krewski, K. Ito, and G. D. Thurston.
2002. Lung cancer, cardiopulmonary mortality, and long-term exposure to fine particulate air
pollution. JAMA 287:1132-1141.
46. Miller, K. A., D. S. Siscovick, L. Sheppard, K. Shepherd, J. H. Sullivan, G. L. Anderson, and J.
D. Kaufman. 2007. Long-term exposure to air pollution and incidence of cardiovascular events in
women. N.Engl.J.Med. 356:447-458.
Page 24 of 40

Figure legends:
Figure 1: Frequencies of genotypes of FGA rs2070011 (left) and FGB rs1800790 (right) (1:
Major allele, 2: Minor allele) by city in a total of 854 MI survivors.
Figure 2: Modification of fibrinogen response to increased ambient PM10 by FGB rs1800790
genotypes (1: Major allele, 2: Minor allele). A: City-specific and pooled estimates for 5-day
averages of PM10; B: Pooled estimates using different induction times between PM10 exposure
and fibrinogen levels.
Interquartile ranges (IQR) for PM10: Helsinki and Stockholm: 10 µg/m3, Augsburg 20 µg/m3,
Barcelona: 24 µg/m3, Rome 19 µg/m3, overall: 13.5 µg/m3; for pooled estimates, * indicates
heterogeneity of the city-specific effect estimates with a p-value < 0.1.
Figure 3: Modification of fibrinogen response to increased ambient 5 day averages of PM10,
Coarse PM, PM2.5 and ultrafine particles (PNC) by FGB rs1800790 genotypes (1: Major
allele, 2: Minor allele). * Indicates heterogeneity of the city-specific effect estimates with a p-
value < 0.1. Interquartile ranges (IQR) of 5day-moving averages: 13.5 µg/m3 PM10, 8.1 µg/m3
coarse PM, 8.8 µg/m3 PM2.5, 11000 /cm3 PNC.
Page 25 of 40

Table 1: Characteristics on patients, fibrinogen measurements and ambient particulate matter concentrations in the AIRGENE Study
Helsinki N=179
Stockholm N=192
Augsburg N=190
Rome N=131
Barcelona N=162
Total N=854
Sex = male [%] 68.2 70.3 81.6 87.0 83.3 77.4
Age [yrs]a 64.6 (45-78) 64.1 (38-76) 61.9 (39-76) 62.5 (39-79) 62.1 (37-81) 63.1 (37-81)
Body mass index a 28.8 (19.1-48.9) 27.6 (17.5-43.3) 28.9 (19.1-48.4) 27.7 (19.0-39.4) 28.9 (19.4-43.5) 28.4 (17.5-48.9) HDL / total Cholesterol a 0.3 (0.13-0.60) 0.32 (0.11-0.56) 0.27 (0.11-0.50) 0.24 (0.12-0.48) 0.28 (0.15-0.53) 0.28 (0.11-0.60) HbA1c [%]a 5.9 (4.7-9.2) 5.0 (3.8-9.9) 5.6 (4.7-9.8) 5.4 (2.8-8.7) 5.1 (3.8-9.8) 5.4 (2.8-9.9) NT-proBNP [pg/ml] a 394 (11-3799) 333 (14-3348) 482 (12-9308) 408 (19-6174) 379 (11-7057) 399 (11-9308) Number of current smokers b 9 2 0 12 22 39 Packyears (cigarettes only) c 9.3 (0-65) 12.1 (0-74) 15.3 (0-205) 22.2 (0-172) 28.1 (0-193) 16.8 (0-205)
Self-reported history [%]c Arrhythmia [%] 31.8 20.8 24.7 23.7 13.6 23.1 Arthrosis [%] 19.0 20.8 17.4 34.4 29.3 23.4 Stroke [%] 6.2 7.8 6.3 3.1 7.4 6.3 Chronic bronchitis [%] 2.2 1.6 8.4 13.0 11.1 6.8 Asthma [%] 5.6 5.7 4.7 6.9 4.9 5.5
Repeated measurements [N] 1063 1140 1084 722 1073 5082
Fibrinogen [g/L] d 3.77 (0.74-6.27) 3.52 (1.98-7.84) 3.34 (1.68-7.53) 3.23 (1.17-8.11) 4.00 (1.81-7.90) 3.58 (0.74-8.11)
Air pollution measurements [study period]
05.09.03 – 02.06.04
30.08.03 – 24.06.04
14.05.03 – 24.02.04
20.09.03 – 15.07.04
30.08.03 – 16.06.04
PM10 [µg/m3 ] e 17.1 (4-53) 17.8 (0-57) 33.1 (7-71) 42.1 (15-91) 40.7 (6-194) 30.3 (0-194) PM2.5 [µg/m3 ] e 8.2 (1-28) 8.8 (0-27) 17.4 (6-39) 24.5 (4-95) 24.2 (3-95) 16.4 (0-95) Coarse Particles (PM10 -PM2.5) [µg/m3 ] e
8.9 (1-38) 9.0 (0-40) 15.8 (-1-35) 16.8 (-33-65) 16.5 (1-102) 13.3 (-33-102)
PNC [#/cm3 ] e 8534 (1238-
30255) 9748 (2369-
24609) 11876 (2764-
32528) 35450 (8004-
87007) 18133 (2327-
48582) 17005 (1238-
87007)
Page 26 of 40

a mean (range), glycosylised haemoglobin (HbA1c), N-terminal proB-type natriuretic peptide (NT-proBNP)
b including occasional cigarette smokers (predominantly Rome and Barcelona) as well as pipe or cigar smokers (predominantly from Helsinki and Stockholm) c ever diagnosed by a physician, d mean (range) of the subject specific means based on 3-8 repeated measurements e mean (range) across study period
Page 27 of 40

Table 2: SNPs and SNP-Fibrinogen Association: Characteristics of the analyzed single nucleotide polymorphisms of the fibrinogen genes FGA and FGB and their association with plasma fibrinogen concentrations.
SNP Functional region Alleles Genotype frequency in percentage (n) Change of fibrinogen* [% of overall mean]
(Major (1)/ Minor (2))
Minor allele frequency in
% (n)
Homozygote of major
allele (1 1) Heterozygote
(1 2)
Homozygote of minor
allele (2 2) 1 2 versus 1 1 2 2 versus 1 1
Cluster 1 FGA
rs2070006 Promoter C/T 40 (677) 37 (319) 46 (393) 17 (142) 2.14 (0.62 , 3.66) 4.27 (1.24 , 7.31)
rs2070011 Promoter C/T 39 (672) 38 (321) 46 (394) 16 (139) 2.29 (0.77 , 3.82) 4.58 (1.54 , 7.63)
Cluster 2 FGB
rs1800790 Promoter G/A 19 (330) 65 (557) 31 (264) 4 (33) 3.77 (1.88 , 5.66) 7.55 (3.77 , 11.33)
rs2227399 Intron T/G 19 (329) 65 (557) 31 (265) 4 (32) 3.71 (1.82 , 5.61) 7.43 (3.63 , 11.22)
rs6056 Ser189Ser C/T 18 (300) 68 (579) 29 (250) 3 (25) 3.47 (1.50 , 5.45) 6.94 (3.00 , 10.89)
rs4220 Lys478Arg G/A 18 (299) 68 (579) 29 (251) 3 (24) 3.47 (1.49 , 5.46) 6.94 (2.98 , 10.91)
Cluster 3 FGB
rs1800791 Promoter C/T 16 (266) 72 (612) 26 (218) 3 (24) -2.76 (-4.80 , -0.71) -5.51 (-9.60 , -1.42)
* Effect estimates and 95% confidence intervals from linear regression with fibrinogen measurements as outcome (100%=3.58 g/L) and an additive genetic model, with a random effect for subject to account for repeated measurements, using an additive model for the genotypes, and adjusted for age, gender, city, body mass index (BMI), HDL / total cholesterol, pack-years of smoking, glycosylized haemoglobin (HbA1c), N-terminal proB-type natriuretic peptide (NT-proBNP), and medical history of arrhythmia, asthma, arthrosis or stroke.
Page 28 of 40

Table 3: SNP-Environment Interaction: Association between five-day average of ambient particulate matter and plasma fibrinogen levels by genotype for the analyzed polymorphisms in the genes FGA and FGB.
Change of fibrinogen* [% of overall mean per 13.5 µg/m3 PM10]
PM-fibrinogen response without genetic covariate
0.68 (0.15 , 1.21)
SNP§ / Genotype§ 1 1 1 2 2 2 p-value
(SNP-Environment-Interaction)
Relative size of the PM-fibrinogen
response&
Cluster 1 FGA
rs2070006 1.22 (0.47 , 1.96) 0.52 $(-0.19 , 2.15) 0.11 $(-1.94 , 2.15) 0.43 0.09
rs2070011 1.16 (0.41 , 1.90) 0.42 $(-0.28 , 1.13) 0.08 $(-2.08 , 2.24) 0.47 0.07
Cluster 2 FGB
rs1800790 0.27 (-0.36 , 0.91) 1.28 (0.54 , 2.01) 2.15 (0.71 , 3.60) 0.037 8.0
rs2227399 0.27 (-0.36 , 0.91) 1.28 (0.55 , 2.02) 2.18 (0.73 , 3.63) 0.034 8.1
rs6056 0.19 (-0.45 , 0.83) 1.26 (0.49 , 2.04) 2.24 (0.72 , 3.77) 0.027 11.3
rs4220 0.19 (-0.45 , 0.83) 1.27 (0.49 , 2.04) 2.25 (0.73 , 3.78) 0.026 11.3
Haplotype in cluster 2# 0.09 (-0.53 , 0.76) 1.17 (0.35 , 1.99) 2.16 (0.61 , 3.71) 0.023 24.0
Cluster3 FGB
rs1800791 0.81 (0.21 , 1.40) 0.40 (-0.48 , 1.28) -0.13 (-1.84 , 1.58) 0.25 0.16
* Inverse-variance weighted sum of city-specific estimates and 95% confidence intervals from linear regression using fibrinogen concentrations as outcome (100%=3.58 g/L) and an additive genetic model, with a random effect by subject, using the five-day average of PM10 fitting to the time of fibrinogen measurement, applying an additive model for the genotype, and including a genotype-PM interaction adjusted for age, gender, city, body mass index (BMI), HDL / total cholesterol, packyears of smoking, glycosylised haemoglobin (HbA1c), N-terminal proB-type natriuretic peptide (NT-proBNP), history of arrhythmia, asthma, arthrosis, stroke, bronchitis, season, apparent temperature, relative humidity, weekday, hour of visit in city-specific models. § 1: Major allele, 2: Minor allele.
Page 29 of 40

$ Test of heterogeneity between centers, p-value < 0.1, pooling based on random effect models & Ratio between the estimate of the change in fibrinogen due to PM10 exposure in t the 2 2 genotype (column 4) and the estimate of the change in fibrinogendue to PM10 exposure in the 11 genotype (column 2) # Haplotypes were defined as follows: 11 homozygote for the mayor haplotype GTCG, 1 2 heterozygote and 22 homozygote for the minor haplotye AGTA, descriptive data is provided in supplemental table 2.
Page 30 of 40

Figure 1
Genotypes of rs2070011 and rs1800790
1 1 1 2 2 2 1 1 1 2 2 2
Freq
uenc
y [%
]
0
20
40
60
80
HelsinkiStockholmAugsburgBarcelonaRome
Page 31 of 40

Figure 2
Genotype
2 21 21 1
Cha
nge
of fi
brin
ogen
[% o
f ove
rall
mea
n pe
r IQ
R P
M10
]
-4
-2
0
2
4
6
8
10
*
A
AugsburgBarcelona
Helsinki
Rome
Stockholm
pooled
Genotype
2 21 21 1
Cha
nge
of fi
brin
ogen
[% o
f ove
rall
mea
n pe
r 13.
5 µg
/m3 P
M10
]
-4
-2
0
2
4
6
8
10
immediate1 day delay2 days delay3 days delay4 days delay5 day average
**
B
Page 32 of 40

Figure 3
rs1800790 genotype
1 1 1 2 2 2 1 1 1 2 2 2 1 1 1 2 2 2 1 1 1 2 2 2
Cha
nge
of fi
brin
ogen
[% o
f ove
rall
mea
n pe
r IQ
R]
-4
-2
0
2
4
6
8
10
PM10 Coarse PM PM2.5 PNC
* *
Page 33 of 40

Fibrinogen Genes Modify the Fibrinogen Response to Ambient Particulate Matter
ONLINE DATA SUPPLEMENT
Annette Peters, Sonja Greven, Iris M. Heid, Fiammetta Baldari, Susanne Breitner, Tom Bellander, Christina Chrysohoou, Thomas Illig, Bénédicte Jacquemin, Wolfgang Koenig (8), Timo Lanki, Fredrik Nyberg, Juha Pekkanen, Riccardo Pistelli, Regina Rückerl, Christodoulos Stefanadis, Alexandra Schneider, Jordi Sunyer, H. Erich Wichmann for the AIRGENE Study Group
Page 34 of 40

Online supplement:
Statistical model
We analyzed data using mixed-effects models with random patient effects accounting for
repeated measures as previously described 1. Because the half-lives of the markers were much
shorter than the intervals between visits, we assumed a compound symmetry structure for the
covariance matrix to model the correlation between repeated measures in each patient.
Penalized splines (P-splines) in the additive mixed-model framework were used to allow for
nonparametric exposure–response functions. The methodology is described in detail in
Greven et al. 2. Fibrinogen levels needed no transformation to fulfil the model assumption of
residual normality.
City-specific confounder models without air pollutants were built for fibrinogen. In addition
to potential time-varying confounders, we included time-invariant patient characteristics
associated with the mean levels of inflammatory markers to permit the assumption of a
normally distributed random patient intercept.
In a first step, time-invariant factors were selected for all cities combined. In the second step,
for each city a more parsimonious model was selected out of the formerly chosen variables
[see Supplemental Material, Table 1]. With this strategy, we adjusted for variables that
influenced the mean levels of the respective blood markers in the single cities, such as age,
sex, and BMI. These variables varied among the cities, possibly reflecting underlying
differences in the populations across Europe as well as chance influences. To ensure sufficient
adjustment for season and meteorology, long-term time trend and apparent temperature were
forced into all models. Additionally, relative humidity, time of day, and day of the week were
included if this adjustment improved the model fit. We considered lag 0, the mean of lags 0
and 1, the mean of lags 2 and 3, and the mean of lag 0–3 for the weather variables; for
fibrinogen, we additionally assessed the mean of lags 0–4. P-splines were used to model
Page 35 of 40

continuous covariables and were compared with linear terms and polynomials of degrees 2
and 3. All decisions on goodness-of-fit were based on Akaike’s Information Criterion. Only
after this adjustment did we examine mean changes of the inflammatory markers in
association with air pollution as reported in a previous paper 1.
Reference List
1. Ruckerl, R., S. Greven, P. Ljungman, P. Aalto, C. Antoniades, T. Bellander, N.
Berglind, C. Chrysohoou, F. Forastiere, B. Jacquemin, S. von Klot, W. Koenig, H.
Kuchenhoff, T. Lanki, J. Pekkanen, C. A. Perucci, A. Schneider, J. Sunyer, and A.
Peters. 2007. Air pollution and inflammation (interleukin-6, C-reactive protein,
fibrinogen) in myocardial infarction survivors. Environ Health Perspect. 115:1072-
1080.
2. Greven, S., Küchenhoff, H., and Peters, A. 2006. Additive mixed models with P-
Splines. Proceedings of the 21st International workshop on Statistical Modelling. 201-
207.
Page 36 of 40
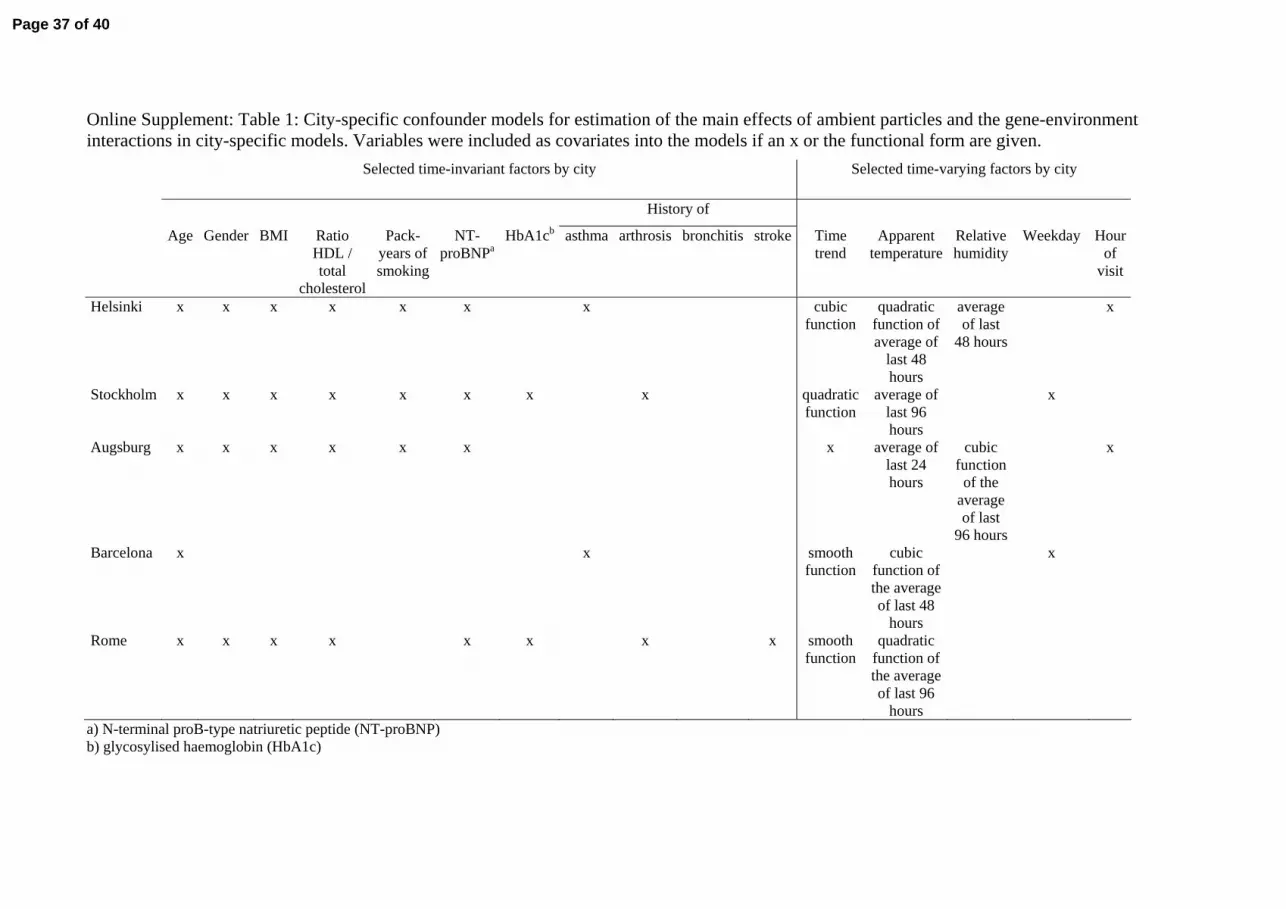
Online Supplement: Table 1: City-specific confounder models for estimation of the main effects of ambient particles and the gene-environment interactions in city-specific models. Variables were included as covariates into the models if an x or the functional form are given. Selected time-invariant factors by city Selected time-varying factors by city
History of
Age Gender BMI Ratio HDL / total
cholesterol
Pack-years of smoking
NT-proBNPa
HbA1cb asthma arthrosis bronchitis stroke Time trend
Apparent temperature
Relative humidity
Weekday Hour of
visit
Helsinki x x x x x x x cubic function
quadratic function of average of
last 48 hours
average of last
48 hours
x
Stockholm x x x x x x x x quadratic function
average of last 96 hours
x
Augsburg x x x x x x x average of last 24 hours
cubic function
of the average of last
96 hours
x
Barcelona x x smooth function
cubic function of the average of last 48
hours
x
Rome x x x x x x x x smooth function
quadratic function of the average of last 96
hours
a) N-terminal proB-type natriuretic peptide (NT-proBNP) b) glycosylised haemoglobin (HbA1c)
Page 37 of 40

Online Supplement: Table 2: Frequency of haploptypes calculated for the FGB cluster 2 composed of the following SNPs rs1800790, rs2227399, rs6056 and rs4220.
Haplotype Alleles* Helsinki N=179
Stockholm N=192
Augsburg N=190
Rome N=131
Barcelona N=162
Total N=854
Major GTCG 83.2% 79.2% 82.6% 77.5% 79.9% 80.7%
Minor AGTA 15.4% 18.5% 16.6% 19.5% 18.2% 17.5%
Rare haplotypes AGCG or ATCG or AGTG 1.4% 2.3% 0.8% 3.1% 1.9% 1.8%
*Alleles for rs1800790, rs2227399, rs6056 and rs4220 listed in that order.
Page 38 of 40

Online Supplement: Figure 1: Linkage disequilibrium (D’) and correlation (R2) are shown for all genotyped fibrinogen SNPs. Three clusters of SNPs (cluster 1, FGB: rs1800790, rs2227399, rs6056, rs4220; cluster 2, FGB: rs1800791; cluster 3, FGA: rs2070006, rs2070011) were further considered for gene-environment interactions.
Page 39 of 40

Supplement: Figure 2: Modification of fibrinogen response to increased ambient PM10 by
FGB rs1800790 genotypes (1: Major allele, 2: Minor allele) for all post-MI patients (5082
observations in 854 subjects), for non-smokers only (4833 observations in 815 subjects) and
for non-smokers unexposed to environmental tobacco smoke (ETS) (4015 observations in 768
subjects). Interquartile range (IQR) for PM10: 13.5 µg/m3
rs1800790 genotype
1 1 1 2 2 2 1 1 1 2 2 2 1 1 1 2 2 2
Cha
nge
of fi
brin
ogen
[% o
f ove
rall
mea
n pe
r IQ
R]
-1
0
1
2
3
4
5All subjects
PM10
Non-smokersNo ETS
PM10
Non-smokersPM10
Page 40 of 40





























