Embed Size (px)
Citation preview
This is a repository copy of Functional gastrointestinal disorders: advances in understanding and management.
White Rose Research Online URL for this paper:http://eprints.whiterose.ac.uk/166984/
Version: Accepted Version
Article:
Black, CJ, Drossman, DA, Talley, NJ et al. (2 more authors) (2020) Functional gastrointestinal disorders: advances in understanding and management. The Lancet. ISSN0140-6736
https://doi.org/10.1016/s0140-6736(20)32115-2
© 2020 Elsevier Ltd. Licensed under the Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License (http://creativecommons.org/licenses/by-nc-nd/4.0/).
[email protected]://eprints.whiterose.ac.uk/
Reuse
This article is distributed under the terms of the Creative Commons Attribution-NonCommercial-NoDerivs (CC BY-NC-ND) licence. This licence only allows you to download this work and share it with others as long as you credit the authors, but you can’t change the article in any way or use it commercially. More information and the full terms of the licence here: https://creativecommons.org/licenses/
Takedown
If you consider content in White Rose Research Online to be in breach of UK law, please notify us by emailing [email protected] including the URL of the record and the reason for the withdrawal request.
Black et al. Page 1 of 42
Accepted for publication 19th August 2020 1
TITLE PAGE 2
Title: Functional Gastrointestinal Disorders: Advances in Understanding and Management. 3
4
Authors: Christopher J. Black MBBS (hons)1,2, Professor Douglas A. Drossman MD3, 5
Professor Nicholas J. Talley MD4, Johannah Ruddy MEd5, Professor Alexander C. Ford 6
MD1,2. 7
8
1Leeds Gastroenterology Institute, St. James’s University Hospital, Leeds, UK. 9
2Leeds Institute of Medical Research at St. James’s, University of Leeds, Leeds, UK. 10
3Center for Education and Practice of Biopsychosocial Care, Drossman Gastroenterology, 11
University of North Carolina at Chapel Hill, North Carolina, USA and the Rome Foundation, 12
North Carolina, USA 13
4NHMRC Centre for Research Excellence in Digestive Health, University of Newcastle, 14
Australia, and Hunter Medical Research Institute, Lambton, NSW, Australia 15
5Center for Education and Practice of Biopsychosocial Care, DrossmanCare, Durham, North 16
Carolina, USA and the Rome Foundation, North Carolina, USA 17
18
Correspondence: Professor Alexander C. Ford 19
Leeds Gastroenterology Institute 20
Room 125 21
4th Floor 22
Bexley Wing 23
St. James’s University Hospital 24
Black et al. Page 2 of 42
Beckett Street 25
Leeds 26
United Kingdom 27
LS9 7TF 28
Email: [email protected] 29
Telephone: +441132684963 30
31
Keywords: pain; bloating; dyspepsia, diarrhoea; constipation 32
33
Word count: 3883 34
35
36
Black et al. Page 3 of 42
ABSTRACT 37
Gastrointestinal symptoms are highly prevalent, but many people who experience them will 38
have no organic explanation for their symptoms. The majority of these people will be labelled 39
as having a functional gastrointestinal disorder (FGID), such as irritable bowel syndrome, 40
functional dyspepsia, or functional constipation. These conditions affect up to 40% of people 41
at any one point in time, and two-thirds of these people will have chronic, fluctuating 42
symptoms. The pathophysiology is complex, but involves bidirectional dysregulation of 43
brain-gut interaction, via the brain-gut axis, as well as microbial dysbiosis within the gut, 44
altered mucosal immune function, visceral hypersensitivity, and abnormal gastrointestinal 45
motility. Hence, recent nomenclature refers to them as disorders of gut-brain interaction. 46
Psychological co-morbidity is common, although whether this predates, or is driven by, the 47
symptoms is not clear. Patients with FGIDs can feel stigmatised, and often a diagnosis of an 48
FGID is not communicated effectively by physicians, nor education provided. Prompt 49
identification and treatment of FGIDs is critical, because these conditions have a considerable 50
impact on healthcare systems, and society as a whole, due to repeated consultations, 51
unnecessary investigations and surgeries, prescription and over-the-counter medicine use, 52
impaired health-related quality of life, and negative effects on ability to work. Symptom-53
based criteria are used to make a diagnosis, with the judicious use of limited investigations 54
required in some patients. The general principles of treatment are based on a biopsychosocial 55
understanding, and involve management of physical symptoms, as well as psychological co-56
morbidity, if present. In the future, treatment approaches to FGIDs are likely to become more 57
personalised based not only on symptoms, but also underlying pathophysiology and 58
psychology. 59
60
61
Black et al. Page 4 of 42
INTRODUCTION 62
The spectrum of symptoms attributable to the gastrointestinal tract includes 63
abdominal pain, diarrhoea, constipation, bloating, fullness, nausea, and vomiting. These 64
symptoms are common to a broad range of organic pathology, including gastrointestinal 65
cancer, inflammatory bowel disease (IBD), coeliac disease, peptic ulcer, and motility 66
disorders, such as gastroparesis. However, it is well-recognised that, for a substantial number 67
of patients, investigation reveals no underlying structural abnormality to explain these 68
symptoms, which in this context are often referred to as “functional”. Functional 69
gastrointestinal disorders (FGIDs), such as irritable bowel syndrome (IBS), functional 70
dyspepsia (FD), or functional constipation, although incompletely understood, and with a 71
complex pathophysiology, account for at least one-third of referrals to gastroenterology 72
clinics. 1 Due to a combination of the pathophysiology involved, as well as the stigma of the 73
term “functional”, these conditions have been redefined as disorders of gut-brain interaction, 74
in order to better reflect their scientific basis. 2 FGIDs are diagnosed and classified using 75
standardised criteria, recommended by the Rome Foundation. Current approaches to 76
treatment target predominant gastrointestinal and psychological symptoms, rather than 77
identifying and addressing specific underlying pathophysiological mechanisms. Almost one-78
in-two people will meet criteria for an FGID at any given time, 3 and these conditions 79
frequently overlap. 4 More than two-thirds of people will have seen a doctor in the preceding 80
12 months, 40% use regular medication, and one-in-three will have had potentially 81
unnecessary abdominal surgery for their symptoms, such as hysterectomy or 82
cholecystectomy. 4 This, together with the fact that these conditions are costly to manage, 83
with an impact on quality of life of a similar magnitude to that of organic gastrointestinal 84
diseases, 4 highlights their fundamental importance to both healthcare systems and society. 85
Despite this, they are not a priority for research funding. 5 This is the first in a series of three 86
Black et al. Page 5 of 42
articles. The two accompanying articles deal with two of the most common FGIDs, IBS and 87
FD, in detail. 88
89
A PATIENT PERSPECTIVE 90
A diagnosis of an FGID has implications for the patient because of the stigma that 91
frequently accompanies it. These disorders lack structural “organic” features, so many 92
physicians view them as “second class” and attach negative attitudes or perceptions toward 93
patients with these conditions, 6 often considering them to have a psychiatric disorder. 7 This 94
can be damaging, both physically and emotionally, to the patient, 8 and lead to a sense of 95
stigma and shame. This, in turn, can inhibit the patient’s ability to express their thoughts and 96
feelings adequately to their providers, causing them to minimise the severity of their 97
symptoms and “gloss over” the impact on their quality of life. 8,9 Patients fear being seen as 98
“crazy”, and some choose instead to suffer needlessly without any medical interventions, 99
eventually giving up hope of regaining their quality of life or, alternatively, actually increase 100
their utilisation of healthcare in the search for answers. This process can cause patients to 101
reject the diagnosis, instead suspecting that the physician has “given up” rather than 102
continuing to seek the “real cause of the symptoms.” Even if they accept the diagnosis, they 103
may develop feelings of guilt and self-blame for having a condition not perceived by 104
physicians as “real.” 10 Half of all patients with FGIDs do not even inform their family 105
members and friends about the diagnosis, because of fear of being misunderstood or not 106
believed. 11 107
So, what can be done to change the perception of these disorders and these patients, 108
and provide more appropriate messaging and impactful care? We must begin first with the 109
clinicians who are looked upon to diagnose and heal. This is the role that physicians have 110
Black et al. Page 6 of 42
played throughout history. The frustration for many physicians is that FGIDs are not easily 111
“healed”, and often require constant symptom management, and therefore frequent visits and 112
follow-up. This can lead to frustration when the patient reports no improvement and can 113
contribute to physician burnout. 114
First, it is key that physicians know how to make a confident diagnosis of an FGID 115
using the symptom-based Rome criteria and communicate this diagnosis effectively, 116
providing rationale for the diagnosis and legitimising the disorder with clear, concise 117
communication. Using qualified language when giving a diagnosis is essential. A physician 118
should refrain from saying to a patient, “We think you have IBS” but instead phrase the 119
diagnosis as “You have IBS”. This use of qualified language increases patient acceptance, 120
reduces apprehension, and provides a framework to build upon for treatment 121
recommendations, medication adherence, and a positive patient-provider relationship. 12 122
Second, patients need to be given the proper education about their condition and have an 123
active role in the decision-making process for treatment. Patients respond better to clear, 124
concise education using images and diagrams to reinforce complex concepts such as the 125
brain-gut axis or pain gate control, preventing them from going to unqualified sources that 126
may contain inaccurate information. Finally, patients need to feel empowered in order to be 127
able to ask questions about anything they are unclear on, speak honestly about the severity of 128
their illness and its impact on their quality of life, and feel validated in their experiences. 129
When all of these elements are provided by a skilled clinician, both the patient and the 130
physician can find mutual satisfaction, positive outcomes, and a long-lasting relationship. 13 131
132
EPIDEMIOLOGY 133
The ability to appropriately classify patients with FGIDs is key, not only to facilitate 134
diagnosis and treatment, but also for research into their aetiology. Over the last 30 years, the 135
Black et al. Page 7 of 42
Rome Foundation, a committee of gastroenterologists and allied academics in the field of 136
gastrointestinal health, has created and updated standardised methods to diagnose and classify 137
FGIDs, based on a consensus of expert opinion, and with reference to current available 138
evidence. First proposed in 1990, the Rome diagnostic criteria define each condition 139
according to a particular cluster of patient-reported symptoms, sometimes with recourse to 140
limited investigations, and have undergone three subsequent revisions. There are 33 adult 141
FGIDs categorised by anatomical location (Table 1), each having validated symptom-based 142
criteria, which have been described in detail elsewhere. 14 The most recent iteration, Rome IV 143
published in 2016, advocate rethinking these conditions as disorders of gut-brain interaction, 144
acknowledging the complex interaction of biological, psychological, and social factors in 145
their pathogenesis. 2 This change also reflects the fact that the term “functional” is non-146
specific and, as a consequence, patients can feel stigmatised by a diagnostic label which is 147
viewed as less “legitimate”, or important, than that of an organic disease, despite often having 148
almost identical symptoms, which are equally genuine and troublesome. 2 However, some 149
diagnostic entities retain the term “functional” to identify those without physiological 150
markers or correlates. 151
A recent Rome Foundation global internet survey of 54,127 adults in the communities 152
of 26 countries reported that 32,112 (43%) people met criteria for at least one FGID. 3 These 153
individuals demonstrated increased healthcare utilisation, and lower quality of life than those 154
not meeting criteria. In one Swedish study, with 7 years of follow-up, only 232 (42%) of 547 155
respondents in the general population were symptom-free throughout. 15 Some of the 156
commonest FGIDs, as per Rome IV criteria, their estimated prevalence in the general 157
population in the Rome Foundation global survey, 3 and the confirmatory testing required to 158
make these diagnoses are described in Table 2. 16-21 IBS, FD, and functional constipation are 159
among the most prevalent FGIDs, and are a particular focus for researchers in the field. 160
Black et al. Page 8 of 42
However, other disorders, which are less well-understood, and lack evidence-based 161
treatments, such as rumination and functional dysphagia, are also more common than was 162
thought previously. 163
Women are generally more likely to suffer from FGIDs than men. 22-24 Indeed, the 164
Rome Foundation global survey demonstrated that 49% of women reported at least one 165
FGID, compared with 37% of men. 3 Recent epidemiological studies have demonstrated an 166
increased risk of both atopic and autoimmune diseases in FGIDs. 25,26 Smoking is also a risk 167
factor, 27 and extra-intestinal symptoms, such as fatigue or other chronic pain syndromes, 168
overlap more than would be expected by chance. 28,29 With respect to geography, studies 169
demonstrate consistently that, although FGIDs are present worldwide, there is variation in 170
prevalence rates between countries. 3,22-24,30,31 This variability may, in part, be due to 171
differences in methodology between studies. 31 It may, however, also reflect contrasts in 172
genetics, culture, lifestyle, and dietary traditions that exist between nations. 32,33 173
174
PATHOPHYSIOLOGY 175
By definition, no structural abnormalities explain FGIDs and, based on the 176
biopsychosocial model developed by Engel, 34 and adapted by Drossman, 35,36 they are 177
characterised as complex bidirectional dysregulation of brain-gut interaction, via the brain-178
gut axis, rather than diseases (Figure 1). Visceral hypersensitivity, abnormal gastrointestinal 179
motility, and psychological disturbances have been recognised to contribute to the 180
pathogenesis for decades, but more recently low-grade intestinal inflammation, increased 181
intestinal permeability, immune activation, and disturbances in the microbiome have been 182
identified, challenging the idea that structural changes are absent entirely. 37,38 183
An integrated model for pathogenesis of disease would help explain all of the known 184
phenomena encountered in FGIDs and, importantly, provide testable new insights into their 185
Black et al. Page 9 of 42
aetiology (Figure 2). 27,39 Importantly, the biopsychosocial model articulates illness as holistic 186
and multifactorial, and emphasises the existence of an intimate mind-body connection, 187
facilitated by bidirectional communication between the brain and the gut in FGIDs, which is 188
well-accepted. 34,35,40 Whatever the underlying aetiology and pathogenesis of FGIDs, central 189
nervous system processing of pain, and other gut signals, is required for the subjective patient 190
symptom experience. This is supported by data, including evidence that there are several 191
areas of abnormal brain activity associated with visceral hypersensitivity, as well as anxiety 192
and depression, in patients with FGIDs. 41,42 However, cause and effect cannot be 193
disentangled from these studies, and is not relevant when pathophysiology is understood in 194
terms of interacting systems. 195
Emerging data challenge the concept that brain-gut pathways act similarly in all 196
patients with FGIDs. Independent epidemiological studies suggest that in 50% of cases 197
FGIDs begin with psychological distress, followed later by gastrointestinal symptoms, 198
whereas in the other 50% of cases gut dysfunction occurs first, and psychological distress 199
follows later. 43-45 This has led to the hypothesis that a subset of patients have a disease 200
process that begins in, and is primarily driven by, the gastrointestinal tract, which later 201
induces systemic manifestations, including psychological dysfunction as an integral part of 202
the disease process. Further, likely microbial causes have been identified; H. pylori is a 203
recognised cause of FD, as the disorder remits long term in a small minority after successful 204
eradication of infection, 46 and following gastroenteritis new-onset IBS, FD, or both, may 205
occur and persist, 47,48 although gastroenteritis as a precipitant is identified by history in only 206
a minority of cases. 49,50 207
In further support of the importance of subtle underlying gastrointestinal pathology in 208
FGIDs, low-grade intestinal inflammation (characterised by eosinophils and/or mast cell 209
infiltration), increased intestinal permeability, an altered microbiome, and immune activation 210
Black et al. Page 10 of 42
(characterised by circulating homing small intestinal T-cells and a cytokine response) have 211
been identified in subsets of patients. 51-53 In turn, there is evidence that this low-grade 212
intestinal inflammatory process can alter neuronal structure and function, likely inducing 213
visceral hypersensitivity and gastrointestinal motor dysfunction. 54 Further, intestinal reflex 214
responses may then alter gut function more proximally, potentially inducing delayed gastric 215
emptying, impairing accommodation of the gastric fundus, or increasing transient lower 216
oesophageal sphincter relaxations, which may account for overlap between FGIDs. 55 217
Intestinal immune activation would be expected to be more prevalent in females, be 218
associated with a risk of atopic and autoimmune disease, and fluctuate over time, possibly 219
accounting for symptom variability, all of which have been observed in FD and IBS. 27 Most 220
patients with IBS and FD have meal-related symptoms; 56,57 dietary components, possibly in 221
some cases because of an aberrant interaction with the microbiome, may lead to antigen 222
presentation in the upper intestine, initiating immune activation and disease cascade. 58 In 223
other cases, a stress response driven centrally may be the primary disease process altering gut 224
function, via the hypothalamic pituitary adrenal axis, a brain-gut predominant disorder. 59 225
Adverse events in early life, possibly driving epigenetic changes, may account for symptom 226
chronicity and visceral hypersensitivity in a subgroup. 60 227
This gut-brain intestinal disease model is testable, and has treatment implications, 228
because it has the potential to identify casual pathways that can be interrupted. These include 229
removal of dietary antigens, specific manipulation of the microbiome, or targeted 230
immunotherapy and, in the future, may offer hope of cure rather than the use of purely 231
symptom-based therapies. 232
233
234
235
Black et al. Page 11 of 42
DIAGNOSIS 236
FGIDs share definable clinical features but, unlike IBD or other structurally-based 237
diseases, currently have no characteristic morphology or biomarkers that enable diagnosis. 238
Patients defined by these standardised criteria are homologous in their clinical features, thus 239
permitting investigators to enrol similar subjects into research, and clinicians to target 240
patients for a specific treatment. 241
Diagnosis of an FGID requires fulfilling symptom-based criteria and excluding, in a 242
cost-effective manner, other specific conditions having similar clinical presentations by 243
physical examination (including digital rectal exam), laboratory studies, and imaging (Table 244
2). For research purposes, it is essential to eliminate well-defined motility disorders, such as 245
chronic intestinal pseudo-obstruction or gastroparesis, or even other FGIDs. Therefore, for a 246
clinical trial in IBS, patients who meet criteria for IBS, but also have FD, would be excluded. 247
However, in clinical practice, it is well-accepted that motility disorders and other FGIDs 248
often co-exist; both diagnoses are recognised and treated. 249
The value of identifying other diagnoses, such as coeliac disease or IBD, which may 250
present with similar symptoms, is that they benefit from entirely different treatments. Yet, the 251
process of doing so requires good clinical judgment as there is risk in over-investigating. 13 252
Experienced clinicians can discern which patients need further evaluation. For example, a 253
college student attending a primary care clinic with an episode of abdominal cramps and 254
diarrhoea occurring before final examinations may receive minimal investigation, or no 255
investigations at all; the clinician will follow these symptoms expectantly. Conversely, an 256
older patient with similar symptoms that are increasing in severity over several months, with 257
accompanying weight loss, will require more evaluation and will likely undergo colonoscopy 258
and/or imaging studies. Also, the nature of the assessment will depend on the presenting 259
Black et al. Page 12 of 42
clinical features; predominant pain leads to a different set of investigations than chronic 260
diarrhoea or vomiting. 261
The best way to apply cost-effective and well-targeted diagnostic evaluations is to 262
consider specific clinical parameters initially. Factors that might lead to further assessment 263
include older age (e.g., colonoscopy after age 50), other co-morbidities, a shorter symptom 264
duration or a worsening severity and trajectory, no record of previous investigations, or the 265
presence of alarm symptoms or "red flags." The latter depend, to some degree, on anatomical 266
region, and the diagnosis under consideration, and include weight loss, haematemesis, 267
persistent vomiting, blood in the stool, family history of IBD or cancer, abnormal findings on 268
physical examination, or abnormal laboratory studies, such as anaemia. When the symptoms 269
are chronic, it is the development of new or changing clinical features, or alarm symptoms, 270
rather than increased reporting of symptoms, that determines the need for re-evaluation. One 271
method to address these parameters is through diagnostic algorithmic pathways, available 272
through the Rome Foundation. 61 As an example, Figure 3 demonstrates the recommended 273
evaluation pathway for patients presenting with constipation-type symptoms. 274
275
NATURAL HISTORY AND EFFECT 276
FGIDs are chronic conditions. Although symptoms fluctuate, and are often meal-277
related, 56,57 prevalence of symptom-reporting tends to remain the same, as the number of 278
people whose symptoms disappear are matched by the number who develop new-onset 279
symptoms. 62-64 The development of new-onset symptoms in those who were previously 280
asymptomatic may reflect bi-directional brain-gut pathways, with higher levels of anxiety and 281
depression associated with development of IBS and FD during follow-up. 44,45,65 However, in 282
longitudinal follow-up studies, among those who remain symptomatic, there is also transition 283
between different FGIDs. 64,66,67 Indeed, a Swedish study found that there was symptom 284
Black et al. Page 13 of 42
fluctuation in 40% to 60% of those reporting IBS, dyspepsia, gastro-oesophageal reflux 285
symptoms, or minor symptoms not meeting criteria for an FGID over a 7-year period. 15 286
Symptom overlap is also frequently observed, such that two or more FGIDs may co-exist, 68-287
70 as may other medically unexplained conditions, such as chronic fatigue syndrome, 71 or 288
fibromyalgia. 72 The prevalence of anxiety and depression increases with the number of co-289
existent FGIDs and with the frequency and severity of gastrointestinal symptoms. 73 Impaired 290
sleep is also common, 74,75 and again seems to increase with the number of overlapping 291
FGIDs. 74 292
Alarmingly, around one-third of patients with FGIDs will undergo unnecessary 293
surgery for their abdominal symptoms, including cholecystectomy and hysterectomy. 4 In one 294
survey of 51 (23%) of 223 patients with FD reported having surgery specifically to 295
investigate their symptoms, including exploratory operations. 76 A multivariate analysis 296
examining rates of surgery in patients with IBS, and adjusting for multiple confounders, 297
showed that having IBS was independently associated with three-fold higher rates of 298
cholecystectomy, two-fold higher rates of appendicectomy and hysterectomy, and 50% 299
higher rates of back surgery, compared with people without IBS. 77 Such procedures, coupled 300
with the fact that two-thirds of patients have seen a doctor in the preceding 12 months and 301
40% are taking medication for their symptoms, 4 add to the considerable healthcare costs of 302
managing FGIDs. 76,78-80 Although functional constipation has been associated with an 303
increased mortality risk, 81,82 this does not appear to be the case for other FGIDs. However, 304
morbidity is striking. Patients report negative effects on their ability to work, with high rates 305
of absenteeism and presenteeism, 83 and their ability to socialise. 80 The detrimental impact on 306
health-related quality of life is, therefore, substantial. 3,80 307
308
309
Black et al. Page 14 of 42
MANAGEMENT 310
The general principles of treatment are based on a biopsychosocial understanding, 36 311
and relate to dysregulation of the brain-gut axis. The FGIDs are defined by any combination 312
of motility disturbance, visceral hypersensitivity, altered mucosal and immune function, 313
altered gut microbiota, and altered central nervous system processing. 16 Thus, patients 314
meeting Rome IV criteria for an FGID may have protean symptom features influenced by 315
various combinations of these factors. So for example, a patient meeting IBS criteria may 316
have bloating related to maldigestion of dietary constituents, such as fermentable oligo-, di-, 317
or mono-saccharides, and polyols (FODMAPs), pain and diarrhoea related to visceral 318
hypersensitivity, altered mucosal immune dysregulation following a bacterial infection (post-319
infection IBS), or anxiety and pain due to central pain dysregulation, and associated with 320
post-traumatic stress disorder following sexual or physical trauma. Since the clinical profile 321
and severity may change over time, the discerning clinician needs to identify which of these 322
factors alone, or in combination, are targets for treatment. There are several principles to 323
consider when initiating treatment, which are considered below. 324
325
The Patient-provider Relationship. 326
It is well-established that an effective patient-provider relationship improves patient 327
and provider satisfaction, adherence to treatment, symptom reduction, and improved clinical 328
outcomes. 13,84,85 Table 3 provides general guidelines to establish and optimise this. 84 329
330
The Symptom Profile 331
The type of symptoms, their location, and the physiological determinants will all 332
influence treatment. Simple inexpensive treatments, such as laxatives or anti-diarrhoeals, will 333
be sufficient for some patients, although the evidence base for these is limited. Trial-based 334
Black et al. Page 15 of 42
and network meta-analyses demonstrate that, for functional constipation or IBS with 335
constipation, drugs like linaclotide or lubiprostone acting as secretagogues, via intestinal ion 336
channels, or prokinetics, such as prucalopride or tegaserod, via 5-hydroxytryptamine (5-HT) 337
receptors, are efficacious, 86-88 whereas for diarrhoea in IBS, rifaximin, a minimally absorbed 338
antibiotic, alosetron or ondansetron, which are 5HT3 receptor antagonists, or the mixed 339
opioid receptor drug eluxadoline, are beneficial . 89-91 However, if the accompanying 340
abdominal pain is severe, treatment will include an antidepressant or a CNS targeted 341
medication, termed central neuromodulators, 92,93 and, if localised to the rectum (e.g., levator 342
ani syndrome), may also be treated by biofeedback. 21 The clinician needs to determine which 343
symptom features are dominant, and which treatment(s) are most likely to lead to 344
improvement. 345
346
Psychosocial Features 347
The brain-gut axis is the basis for a bidirectional relationship, where gastrointestinal 348
symptoms influence psychosocial state, and vice versa. Thus, chronic pain, nausea, or 349
vomiting can lead to anxiety or depression, as modified by early experiences, coping, and 350
social and family influences. Conversely, psychosocial difficulties, including co-morbid 351
anxiety, depression, a significant loss, or sexual or physical trauma history, influences pain 352
threshold and gastrointestinal motility. This relationship justifies the use of gastrointestinal 353
behavioural treatments such as cognitive-behavioural therapy or hypnotherapy., 94 354
Although psychosocial co-morbidities may determine referral for gastrointestinal 355
behavioural intervention, it is also recognised that it is the patient's awareness of the value of 356
the treatment and the motivation to engage that determines success. 95 The best candidates for 357
gastrointestinal behavioural treatments understand the nature of gut-brain disorders, are open 358
to behavioural change to alleviate symptoms, can make connections between times of stress 359
Black et al. Page 16 of 42
and anxiety and symptoms, and have the time to participate in the treatment. Patients with 360
severe psychopathology or personality disorder, who have little insight into the gut-brain 361
interaction, who are fixated on a "cure," or who are unable or unwilling to commit to 362
treatment are unlikely to benefit. 94 363
364
Symptom Severity 365
Severity is a biopsychosocial composite of patient-reported gastrointestinal and extra-366
intestinal symptoms, the degree of pain, disability, psychosocial impairments, illness-related 367
perceptions and behaviours, and health-related quality of life. 96 It is operative when making 368
treatment decisions. For example, a patient having infrequent low-grade abdominal pain with 369
no other symptoms, and no psychological distress is unlikely to seek healthcare, and would 370
be classified as mild, and not treated. Conversely, a patient having severe abdominal pain, 371
along with fibromyalgia and migraine headaches, who is unable to work, depressed, and 372
frequently seeks healthcare, or is hospitalised, would be considered severe, and treated with 373
behavioural and multiple medical treatments. Table 4 provides guidelines developed by a 374
Rome Foundation working team to help categorise severity for FGIDs. 96 375
376
In summary, treatment of FGIDs requires an effective patient-provider relationship 377
and a multimodal approach that incorporates the nature of the symptoms, their severity, the 378
presence of psychosocial co-morbidities and, in combination, their impact. The multi-379
dimensional clinical profile, which has been proposed by the Rome Foundation, takes these 380
factors into consideration, in order to help the clinician provide care that is targeted to the 381
personal needs of the patient. 97,98 The five components of this include: 382
A. Categorical diagnosis (the symptom-based criteria) 383
Black et al. Page 17 of 42
B. Clinical modifier (e.g., IBS with constipation, diarrhoea, or mixed bowel habits, post-384
infection aetiology, FODMAP sensitivity) 385
C. Impact (mild, moderate, severe) 386
D. Psychosocial modifier (e.g., psychological diagnosis, loss, trauma history,) 387
E. Physiological dysfunction and biomarkers (where available) 388
Although currently this model has heuristic value and is being promoted in clinical education, 389
98 future studies are needed to provide evidential support. 390
391
CONCLUSIONS 392
FGIDs are extremely prevalent, affecting almost one-in-two people at some point in 393
their lives. Due to healthcare seeking, excess surgeries, medications, and their effects on 394
quality of life, psychological health, work, and social functioning they have a substantial 395
impact not only on the lives of sufferers, but also society as a whole. The pathophysiology is 396
complex, but the biopsychosocial model provides a framework to articulate this. Novel, 397
testable, models may further improve our understanding. Although treatment remains 398
symptom-based, it is recognised increasingly that there is a need to enhance the patient-399
provider relationship, and that this should be multimodal, to maximise chances of success. In 400
the future, treatment approaches are likely to become more personalised based not only on 401
symptoms, but also underlying pathophysiology and psychology. 402
403
Contributors 404
CJB, DAD, NJT, JR, and ACF did the literature search, wrote the manuscript, and drafted the 405
figures. ACF and DAD revised the initial manuscript. All authors critically revised 406
subsequent versions of the manuscript and approved the final version of the manuscript. 407
408
Black et al. Page 18 of 42
Declaration of Interests 409
CJB has no conflicts of interest. DAD is President Emeritus and Chief of Operations of the 410
Rome Foundation. NJT reports grants from Abbott Pharmaceuticals, grants from 411
Commonwealth Diagnostics , non-financial support from HVN National Science Challenge 412
NZ, grants and personal fees from GI therapies, grants from Viscera USA , personal fees 413
from Adelphi values, personal fees from Allergens PLC , personal fees from Takeda, 414
personal fees from Ampligent, personal fees from Progenity Inc , personal fees from Sanofi-415
aventis, personal fees from IM Health Sciences, personal fees from Napo Pharmaceutical, 416
personal fees from Outpost Medicine, personal fees from Samsung Bioepis, personal fees 417
from Synergy, personal fees from Theravance, personal fees from Yuhan, grants from 418
Prometheus (IBS), grants from Pfizer, grants from Rome Foundation , grants from Salix , 419
personal fees from Aviro Health (Digestive health) , personal fees from ARENA 420
Pharmaceuticals , personal fees from Anatara Life Sciences, personal fees from Allakos, 421
personal fees from Censa, personal fees from Cadila Pharmaceuticals , personal fees from 422
Danone, personal fees from Dr. Reddy's Laboratories , personal fees from Planet Innovation , 423
personal fees from twoXAR, personal fees from Theravance, personal fees from Dr Falk, 424
outside the submitted work. In addition, NJT has a patent Biomarkers of IBS licensed, a 425
patent Licensing Questionnaires Talley Bowel Disease Questionnaire licensed to 426
Mayo/Talley, a patent Nestec European Patent licensed, and a patent Singapore Provisional 427
PatentÐu8220“Microbiota Modulation Of BDNF Tissue Repair Pathway” issued. JR has no 428
conflicts of interest. ACF has no conflicts of interest. 429
430
Black et al. Page 19 of 42
REFERENCES 431
432
1. Shivaji UN, Ford AC. Prevalence of functional gastrointestinal disorders among 433
consecutive new patient referrals to a gastroenterology clinic. Frontline Gastroenterology 434
2014; 5: 266-71. 435
2. Drossman DA, Hasler WL. Rome IV-functional GI disorders: Disorders of gut-brain 436
interaction. Gastroenterology 2016; 150: 1257-61. 437
3. Sperber AD, Bangdiwala SI, Drossman DA, et al. Worldwide prevalence and burden 438
of functional gastrointestinal disorders, results of Rome Foundation global study. 439
Gastroenterology 2020; doi:10.1053/j.gastro.2020.04.014. 440
4. Aziz I, Palsson OS, Tornblom H, Sperber AD, Whitehead WE, Simren M. The 441
prevalence and impact of overlapping Rome IV-diagnosed functional gastrointestinal 442
disorders on somatization, quality of life, and healthcare utilization: A cross-sectional general 443
population study in three countries. Am J Gastroenterol 2018; 113: 86-96. 444
5. Hepatology TLG. Unmet needs of patients with irritable bowel syndrome. The lancet 445
Gastroenterology & hepatology 2018; (9): 587. 446
6. Halpert A. Irritable bowel syndrome: Patient-provider interaction and patient 447
education. J Clin Med 2018; 7: doi: 10.3390/jcm7010003. 448
7. Bradley S, Alderson S, Ford AC, Foy R. General practitioners' perceptions of irritable 449
bowel syndrome: A Q-methodological study. Fam Pract 2018; 35: 74-9. 450
Black et al. Page 20 of 42
8. Ruddy J. From pretending to truly being OK: A journey from illness to health with 451
postinfection irritable bowel syndrome: The patient's perspective. Gastroenterology 2018; 452
155: 1666-9. 453
9. Rocque R, Leanza Y. A systematic review of patients' experiences in communicating 454
with primary care physicians: Intercultural encounters and a balance between vulnerability 455
and integrity. PLoS One 2015; 10: e0139577. 456
10. Ali A, Toner BB, Stuckless N, et al. Emotional abuse, self-blame, and self-silencing 457
in women with irritable bowel syndrome. Psychosom Med 2000; 62: 76-82. 458
11. Drossman DA, Chang L, Schneck S, Blackman C, Norton WF, Norton NJ. A focus 459
group assessment of patient perspectives on irritable bowel syndrome and illness severity. 460
Dig Dis Sci 2009; 54: 1532-41. 461
12. Linedale EC, Chur-Hansen A, Mikocka-Walus A, Gibson PR, Andrews JM. 462
Uncertain diagnostic language affects further studies, endoscopies, and repeat consultations 463
for patients with functional gastrointestinal disorders. Clin Gastroenterol Hepatol 2016; 14: 464
1735-41.e1. 465
13. Drossman DA, Ruddy J. Improving patient-provider relationships to improve health 466
care. Clin Gastroenterol Hepatol 2020; 18: 1417-26. 467
14. Rome IV journal articles. https://theromefoundationorg/rome-iv/rome-iv-journal-468
articles/. 469
Black et al. Page 21 of 42
15. Agreus L, Svardsudd K, Talley NJ, Jones MP, Tibblin G. Natural history of 470
gastroesophageal reflux disease and functional abdominal disorders. Am J Gastroenterol 471
2001; 96: 2905-14. 472
16. Drossman DA. Functional gastrointestinal disorders: History, pathophysiology, 473
clinical features and Rome IV. Gastroenterology 2016; 148: 1262-79. 474
17. Palsson OS, Whitehead WE, van Tilburg MA, et al. Rome IV diagnostic 475
questionnaires and tables for investigators and clinicians. Gastroenterology 2016; 150: 1481-476
91. 477
18. Stanghellini V, Chan FK, Hasler WL, et al. Gastroduodenal disorders. 478
Gastroenterology 2016; 150: 1380-92. 479
19. Mearin F, Lacy BE, Chang L, et al. Bowel disorders. Gastroenterology 2016; 150: 480
1393-407. 481
20. Aziz Q, Fass R, Gyawali CP, Miwa H, Pandolfino JE, Zerbib F. Functional 482
esophageal disorders. Gastroenterology 2016; 150: 1368-79. 483
21. Rao SSC, Bharucha AE, Chiarioni G, et al. Anorectal disorders. Gastroenterology 484
2016; 150: 1430-42.e4. 485
22. Lovell RM, Ford AC. Effect of gender on prevalence of irritable bowel syndrome in 486
the community: Systematic review and meta-analysis. Am J Gastroenterol 2012; 107: 991-487
1000. 488
Black et al. Page 22 of 42
23. Suares NC, Ford AC. Prevalence of, and risk factors for, chronic idiopathic 489
constipation in the community: Systematic review and meta-analysis. Am J Gastroenterol 490
2011; 106: 1582-91. 491
24. Ford AC, Marwaha A, Sood R, Moayyedi P. Global prevalence of, and risk factors 492
for, uninvestigated dyspepsia: a meta-analysis. Gut 2015; 64: 1049-57. 493
25. Koloski N, Jones M, Walker MM, et al. Population based study: Atopy and 494
autoimmune diseases are associated with functional dyspepsia and irritable bowel syndrome, 495
independent of psychological distress. Aliment Pharmacol Ther 2019; 49: 546-55. 496
26. Ford AC, Talley NJ, Walker MM, Jones MP. Increased prevalence of autoimmune 497
diseases in functional gastrointestinal disorders: Case-control study of 23471 primary care 498
patients. Aliment Pharmacol Ther 2014; 40: 827-34. 499
27. Talley NJ. What causes functional gastrointestinal disorders? A proposed disease 500
model. Am J Gastroenterol 2020; 115: 41-8. 501
28. Hamilton WT, Gallagher AM, Thomas JM, White PD. Risk markers for both chronic 502
fatigue and irritable bowel syndromes: A prospective case-control study in primary care. 503
Psychol Med 2009; 39: 1913-21. 504
29. Berstad A, Undseth R, Lind R, Valeur J. Functional bowel symptoms, fibromyalgia 505
and fatigue: A food-induced triad? Scand J Gastroenterol 2012; 47: 914-9. 506
Black et al. Page 23 of 42
30. Palsson OS, Whitehead W, Tornblom H, Sperber AD, Simren M. Prevalence of Rome 507
IV functional bowel disorders among adults in the United States, Canada, and the United 508
Kingdom. Gastroenterology 2020; doi.org/10.1053/j.gastro.2019.12.021. 509
31. Sperber AD, Dumitrascu D, Fukudo S, et al. The global prevalence of IBS in adults 510
remains elusive due to the heterogeneity of studies: A Rome Foundation working team 511
literature review. Gut 2017; 66: 1075-82. 512
32. Sperber AD. The challenge of cross-cultural, multi-national research: Potential 513
benefits in the functional gastrointestinal disorders. Neurogastroenterol Motil 2009; 21: 351-514
60. 515
33. Black CJ, Ford AC. Global burden of irritable bowel syndrome: Trends, predictions 516
and risk factors. Nat Rev Gastroenterol Hepatol 2020; doi: 10.1038/s41575-020-0286-8. 517
34. Engel GL. The need for a new medical model: A challenge for biomedicine. Science 518
(New York, NY) 1977; 196: 129-36. 519
35. Van Oudenhove L, Crowell MD, Drossman DA, et al. Biopsychosocial aspects of 520
functional gastrointestinal disorders. Gastroenterology 2016; 150: 1355-67. 521
36. Drossman DA. Presidential address: Gastrointestinal illness and the biopsychosocial 522
model. Psychosom Med 1998; 60: 258-67. 523
37. Talley NJ, Ford AC. Functional Dyspepsia. N Engl J Med 2015; 373: 1853-63. 524
Black et al. Page 24 of 42
38. Ford AC, Lacy BE, Talley NJ. Irritable bowel syndrome. N Engl J Med 2017; 376: 525
2566-78. 526
39. Talley NJ. Editorial: Moving away from focussing on gastric pathophysiology in 527
functional dyspepsia: New insights and therapeutic implications. Am J Gastroenterol 2017; 528
112: 141-4. 529
40. Ringel Y, Sperber AD, Drossman DA. Irritable bowel syndrome. Annu Rev Med 530
2001; 52: 319-38. 531
41. Mayer EA, Labus J, Aziz Q, et al. Role of brain imaging in disorders of brain-gut 532
interaction: A Rome Working Team Report. Gut 2019; 68: 1701-15. 533
42. Lee IS, Wang H, Chae Y, Preissl H, Enck P. Functional neuroimaging studies in 534
functional dyspepsia patients: A systematic review. Neurogastroenterol Motil 2016; 28: 793-535
805. 536
43. Jones MP, Tack J, Van Oudenhove L, et al. Mood and anxiety disorders precede 537
development of functional gastrointestinal disorders in patients but not in the population. Clin 538
Gastroenterol Hepatol 2017; 15: 1014-20.e4. 539
44. Koloski NA, Jones M, Kalantar J, Weltman M, Zaguirre J, Talley NJ. The brain--gut 540
pathway in functional gastrointestinal disorders is bidirectional: A 12-year prospective 541
population-based study. Gut 2012; 61: 1284-90. 542
Black et al. Page 25 of 42
45. Koloski NA, Jones M, Talley NJ. Evidence that independent gut-to-brain and brain-543
to-gut pathways operate in the irritable bowel syndrome and functional dyspepsia: A 1-year 544
population-based prospective study. Aliment Pharmacol Ther 2016; 44: 592-600. 545
46. Moayyedi P, Soo S, Deeks JJ, et al. Systematic review and economic evaluation of 546
Helicobacter pylori eradication treatment for non-ulcer dyspepsia. BMJ 2000; 321: 659-64. 547
47. Barbara G, Grover M, Bercik P, et al. Rome Foundation working team report on post-548
Infection irritable bowel syndrome. Gastroenterology 2019; 156: 46-58.e7. 549
48. Ford AC, Thabane M, Collins SM, et al. Prevalence of uninvestigated dyspepsia 8 550
years after a large waterborne outbreak of bacterial dysentery: A cohort study. 551
Gastroenterology 2010; 138: 1727-36. 552
49. Card T, Enck P, Barbara G, et al. Post-infectious IBS: Defining its clinical features 553
and prognosis using an internet-based survey. United European Gastroenterol J 2018; 6: 554
1245-53. 555
50. Tack J, Demedts I, Dehondt G, et al. Clinical and pathophysiological characteristics 556
of acute-onset functional dyspepsia. Gastroenterology 2002; 122: 1738-47. 557
51. Burns G, Carroll G, Mathe A, et al. Evidence for local and systemic immune 558
activation in functional dyspepsia and the irritable bowel syndrome: A systematic review. Am 559
J Gastroenterol 2019; 114: 429-36. 560
Black et al. Page 26 of 42
52. Liebregts T, Adam B, Bredack C, et al. Small bowel homing T cells are associated 561
with symptoms and delayed gastric emptying in functional dyspepsia. Am J Gastroenterol 562
2011; 106: 1089-98. 563
53. Tap J, Derrien M, Tornblom H, et al. Identification of an intestinal microbiota 564
signature associated with severity of irritable bowel syndrome. Gastroenterology 2017; 152: 565
111-23.e8. 566
54. Cirillo C, Bessissow T, Desmet AS, Vanheel H, Tack J, Vanden Berghe P. Evidence 567
for neuronal and structural changes in submucous ganglia of patients with functional 568
dyspepsia. Am J Gastroenterol 2015; 110: 1205-15. 569
55. Ronkainen J, Aro P, Walker MM, et al. Duodenal eosinophilia is associated with 570
functional dyspepsia and new onset gastro-oesophageal reflux disease. Aliment Pharmacol 571
Ther 2019; 50: 24-32. 572
56. Bisschops R, Karamanolis G, Arts J, et al. Relationship between symptoms and 573
ingestion of a meal in functional dyspepsia. Gut 2008; 57: 1495-503. 574
57. Arsie E, Coletta M, Cesana BM, Basilisco G. Symptom-association probability 575
between meal ingestion and abdominal pain in patients with irritable bowel syndrome. Does 576
somatization play a role? Neurogastroenterol Motil 2015; 11(10): 12510. 577
58. Fritscher-Ravens A, Pflaum T, Mosinger M, et al. Many patients with irritable bowel 578
syndrome have atypical food allergies not associated with immunoglobulin E. 579
Gastroenterology 2019; 157: 109-18.e5. 580
Black et al. Page 27 of 42
59. Videlock EJ, Adeyemo M, Licudine A, et al. Childhood trauma is associated with 581
hypothalamic-pituitary-adrenal axis responsiveness in irritable bowel syndrome. 582
Gastroenterology 2009; 137: 1954-62. 583
60. Aguirre JE, Winston JH, Sarna SK. Neonatal immune challenge followed by adult 584
immune challenge induces epigenetic-susceptibility to aggravated visceral hypersensitivity. 585
Neurogastroenterol Motil 2017; 29: 10.1111/nmo.13081. 586
61. Drossman DA, Chang L, Chey WD, Kellow J, Tack J, Whitehead WE. Rome IV 587
diagnostic algorithms for common GI symptoms. Raleigh, NC: Rome Foundation; 2016. 588
62. Ford AC, Forman D, Bailey AG, Axon ATR, Moayyedi P. Irritable bowel syndrome: 589
A 10-year natural history of symptoms, and factors that influence consultation behavior. Am J 590
Gastroenterol 2008; 103: 1229-39. 591
63. Agreus L, Svardsudd K, Nyren O, Tibblin G. Irritable bowel syndrome and dyspepsia 592
in the general population: Overlap and lack of stability over time. Gastroenterology 1995; 593
109: 671-80. 594
64. Ford AC, Forman D, Bailey AG, Axon ATR, Moayyedi P. Fluctuation of 595
gastrointestinal symptoms in the community: A 10-year longitudinal follow-up study. 596
Aliment Pharmacol Ther 2008; 28: 1013-20. 597
65. Aro P, Talley NJ, Johansson SE, Agreus L, Ronkainen J. Anxiety Is linked to new-598
onset dyspepsia in the Swedish population: A 10-year follow-up study. Gastroenterology 599
2015; 148: 928-37. 600
Black et al. Page 28 of 42
66. Halder SLS, Locke III GR, Schleck CD, Zinsmeister AR, Melton III LJ, Talley NJ. 601
Natural history of functional gastrointestinal disorders: A 12-year longitudinal population-602
based study. Gastroenterology 2007; 133: 799-807. 603
67. Olafsdottir LB, Gudjonsson H, Jonsdottir HH, Bjornsson E, Thjodleifsson B. Natural 604
history of functional gastrointestinal disorders: Comparison of two longitudinal population-605
based studies. Dig Liver Dis 2012; 44: 211-7. 606
68. Locke III GR, Zinsmeister AR, Fett SL, Melton III LJ, Talley NJ. Overlap of 607
gastrointestinal symptom complexes in a US community. Neurogastroenterol Motil 2005; 17: 608
29-34. 609
69. Ford AC, Marwaha A, Lim A, Moayyedi P. Systematic review and meta-analysis of 610
the prevalence of irritable bowel syndrome in individuals with dyspepsia. Clin Gastroenterol 611
Hepatol 2010; 8: 401-9. 612
70. Lovell RM, Ford AC. Prevalence of gastro-esophageal reflux-type symptoms in 613
individuals with irritable bowel syndrome in the community: A meta-analysis. Am J 614
Gastroenterol 2012; 107: 1793-801. 615
71. Petersen MW, Schröder A, Jørgensen T, et al. Irritable bowel, chronic widespread 616
pain, chronic fatigue and related syndromes are prevalent and highly overlapping in the 617
general population: DanFunD. Scientific reports 2020; 10: 3273. 618
72. Hyland ME, Bacon AM, Lanario JW, Davies AF. Symptom frequency and 619
development of a generic functional disorder symptom scale suitable for use in studies of 620
Black et al. Page 29 of 42
patients with irritable bowel syndrome, fibromyalgia syndrome or chronic fatigue syndrome. 621
Chronic diseases and translational medicine 2019; 5: 129-38. 622
73. Pinto-Sanchez MI, Ford AC, Avila CA, et al. Anxiety and depression increase in a 623
stepwise manner in parallel with multiple FGIDs and symptom severity and frequency. Am J 624
Gastroenterol 2015; 110: 1038-48. 625
74. Kim SY, Choung RS, Lee SK, et al. Self-reported sleep impairment in functional 626
dyspepsia and irritable bowel syndrome. J Neurogastroenterol Motil 2018; 24: 280-8. 627
75. Lacy BE, Everhart K, Crowell MD. Functional dyspepsia is associated with sleep 628
disorders. Clin Gastroenterol Hepatol 2011; 9: 410-4. 629
76. Lacy BE, Weiser KT, Kennedy AT, Crowell MD, Talley NJ. Functional dyspepsia: 630
The economic impact to patients. Aliment Pharmacol Ther 2013; 38: 170-7. 631
77. Longstreth GF, Yao JF. Irritable bowel syndrome and surgery: A multivariate 632
analysis. Gastroenterology 2004; 126: 1665-73. 633
78. Canavan C, West J, Card T. Review article: the economic impact of the irritable 634
bowel syndrome. Aliment Pharmacol Ther 2014; 40: 1023-34. 635
79. Moayyedi P, Mason J. Clinical and economic consequences of dyspepsia in the 636
community. Gut 2002; 50 (suppl 4): iv10-2. 637
Black et al. Page 30 of 42
80. Buono JL, Carson RT, Flores NM. Health-related quality of life, work productivity, 638
and indirect costs among patients with irritable bowel syndrome with diarrhea. Health Qual 639
Life Outcomes 2017; 15: 35. 640
81. Chang JY, Locke III GR, McNally MA, et al. Impact of functional gastrointestinal 641
disorders on survival in the community. Am J Gastroenterol 2010; 105: 822-32. 642
82. Koloski NA, Jones M, Wai R, Gill RS, Byles J, Talley NJ. Impact of persistent 643
constipation on health-related quality of life and mortality in older community-dwelling 644
women. Am J Gastroenterol 2013; 108: 1152-8. 645
83. Drossman DA, Li Z, Andruzzi E, et al. U.S. householder survey of functional 646
gastrointestinal disorders. Prevalence, sociodemography, and health impact. Dig Dis Sci 647
1993; 38: 1569-80. 648
84. Drossman DA. 2012 David Sun lecture: Helping your patient by helping yourself--649
how to improve the patient-physician relationship by optimizing communication skills. Am J 650
Gastroenterol 2013; 108: 521-8. 651
85. Kaptchuk TJ, Kelley JM, Conboy LA, et al. Components of placebo effect: 652
Randomised controlled trial in patients with irritable bowel syndrome. BMJ 2008; 336: 999-653
1003. 654
86. Black CJ, Burr NE, Ford AC. Relative efficacy of tegaserod in a systematic review 655
and network meta-analysis of licensed therapies for irritable bowel syndrome with 656
constipation. Clin Gastroenterol Hepatol 2019; 18: 1238-9. 657
Black et al. Page 31 of 42
87. Black CJ, Burr NE, Quigley EMM, Moayyedi P, Houghton LA, Ford AC. Efficacy of 658
secretagogues in patients with irritable bowel syndrome with constipation: Systematic review 659
and network meta-analysis. Gastroenterology 2018; 155: 1753-63. 660
88. Ford AC, Suares NC. Effect of laxatives and pharmacological therapies in chronic 661
idipathic constipation: Systematic review and meta-analysis. Gut 2011; 60: 209-18. 662
89. Black CJ, Burr NE, Camilleri M, et al. Efficacy of pharmacological therapies in 663
patients with IBS with diarrhoea or mixed stool pattern: Systematic review and network 664
meta-analysis. Gut 2020; 69: 74-82. 665
90. Zheng L, Lai Y, Lu W, et al. Pinaverium reduces symptoms of irritable bowel 666
syndrome in a multi-center, randomized controlled trial. Clin Gastroenterol Hepatol 2015; 667
13: 1285-92. 668
91. Ford AC, Harris LA, Lacy BE, Quigley EMM, Moayyedi P. Systematic review with 669
meta-analysis: The efficacy of prebiotics, probiotics, synbiotics and antibiotics in irritable 670
bowel syndrome. Aliment Pharmacol Ther 2018; 48: 1044-60. 671
92. Drossman DA, Tack J, Ford AC, Szigethy E, Tornblom H, Van Oudenhove L. 672
Neuromodulators for functional gastrointestinal disorders (disorders of gut-brain interaction): 673
A Rome Foundation working team report. Gastroenterology 2018; 154: 1140-71.e1. 674
93. Ford AC, Lacy BE, Harris LA, Quigley EM, Moayyedi P. Effect of antidepressants 675
and psychological therapies in irritable bowel syndrome: An updated systematic review and 676
meta-analysis. Am J Gastroenterol 2019; 114: 21-39. 677
Black et al. Page 32 of 42
94. Keefer L, Palsson OS, Pandolfino JE. Best practice update: Incorporating 678
psychogastroenterology into management of digestive disorders. Gastroenterology 2018; 679
154: 1249-57. 680
95. Weinland SR, Morris CB, Dalton C, et al. Cognitive factors affect treatment response 681
to medical and psychological treatments in functional bowel disorders. Am J Gastroenterol 682
2010; 105: 1397-406. 683
96. Drossman DA, Chang L, Bellamy N, et al. Severity in irritable bowel syndrome: A 684
Rome foundation working team report. Am J Gastroenterol 2011; 106: 1749-59. 685
97. Drossman DA, Chang L, Chey WD, Kellow J, Tack J, Whitehead WE. The 686
multidimensional clinical profile for functional gastrointestinal disorders: MDCP. 2nd ed ed. 687
Raleigh, NC: Rome Foundation; 2016. 688
98. Lin LD, Chang L. Using the Rome IV criteria to help manage the complex IBS 689
patient. Am J Gastroenterol 2018; 113: 453-6. 690
99. Costanzo C, Verghese A. The physical examination as ritual: Social sciences and 691
embodiment in the context of the physical examination. The Medical clinics of North 692
America 2018; 102: 425-31. 693
694
695
Black et al. Page 33 of 42
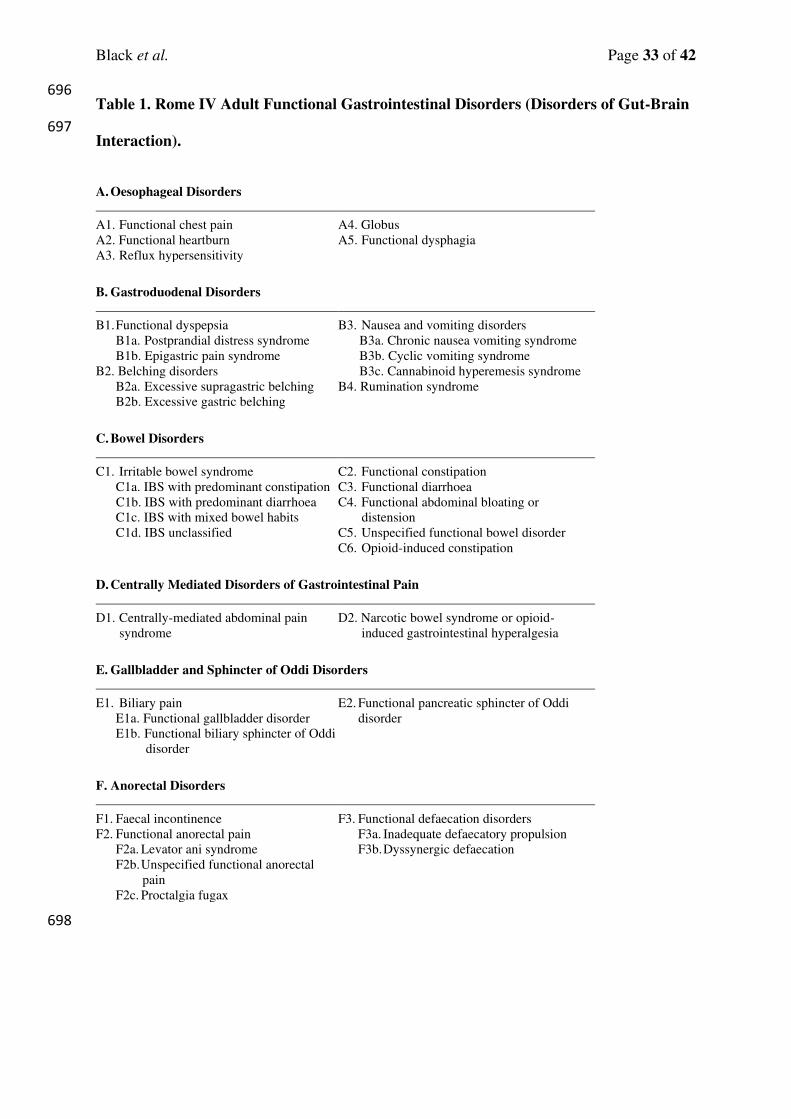
Table 1. Rome IV Adult Functional Gastrointestinal Disorders (Disorders of Gut-Brain 696
Interaction). 697
A. Oesophageal Disorders
A1. Functional chest pain
A2. Functional heartburn
A3. Reflux hypersensitivity
A4. Globus
A5. Functional dysphagia
B. Gastroduodenal Disorders
B1. Functional dyspepsia
B1a. Postprandial distress syndrome
B1b. Epigastric pain syndrome
B2. Belching disorders
B2a. Excessive supragastric belching
B2b. Excessive gastric belching
B3. Nausea and vomiting disorders
B3a. Chronic nausea vomiting syndrome
B3b. Cyclic vomiting syndrome
B3c. Cannabinoid hyperemesis syndrome
B4. Rumination syndrome
C. Bowel Disorders
C1. Irritable bowel syndrome
C1a. IBS with predominant constipation
C1b. IBS with predominant diarrhoea
C1c. IBS with mixed bowel habits
C1d. IBS unclassified
C2. Functional constipation
C3. Functional diarrhoea
C4. Functional abdominal bloating or
distension
C5. Unspecified functional bowel disorder
C6. Opioid-induced constipation
D. Centrally Mediated Disorders of Gastrointestinal Pain
D1. Centrally-mediated abdominal pain
syndrome
D2. Narcotic bowel syndrome or opioid-
induced gastrointestinal hyperalgesia
E. Gallbladder and Sphincter of Oddi Disorders
E1. Biliary pain
E1a. Functional gallbladder disorder
E1b. Functional biliary sphincter of Oddi
disorder
E2. Functional pancreatic sphincter of Oddi
disorder
F. Anorectal Disorders
F1. Faecal incontinence
F2. Functional anorectal pain
F2a. Levator ani syndrome
F2b. Unspecified functional anorectal
pain
F2c. Proctalgia fugax
F3. Functional defaecation disorders
F3a. Inadequate defaecatory propulsion
F3b. Dyssynergic defaecation
698
Black et al. Page 34 of 42
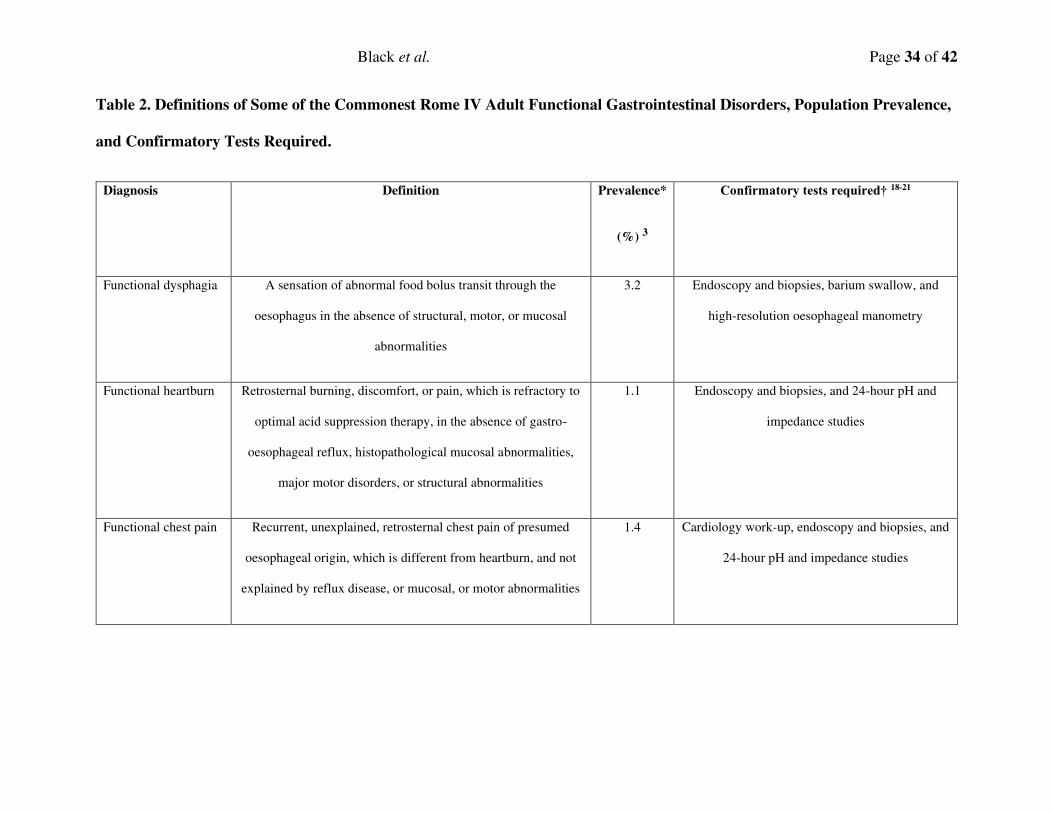
Table 2. Definitions of Some of the Commonest Rome IV Adult Functional Gastrointestinal Disorders, Population Prevalence,
and Confirmatory Tests Required.
Diagnosis Definition Prevalence*
(%) 3
Confirmatory tests required† 18-21
Functional dysphagia A sensation of abnormal food bolus transit through the
oesophagus in the absence of structural, motor, or mucosal
abnormalities
3.2 Endoscopy and biopsies, barium swallow, and
high-resolution oesophageal manometry
Functional heartburn Retrosternal burning, discomfort, or pain, which is refractory to
optimal acid suppression therapy, in the absence of gastro-
oesophageal reflux, histopathological mucosal abnormalities,
major motor disorders, or structural abnormalities
1.1 Endoscopy and biopsies, and 24-hour pH and
impedance studies
Functional chest pain Recurrent, unexplained, retrosternal chest pain of presumed
oesophageal origin, which is different from heartburn, and not
explained by reflux disease, or mucosal, or motor abnormalities
1.4 Cardiology work-up, endoscopy and biopsies, and
24-hour pH and impedance studies
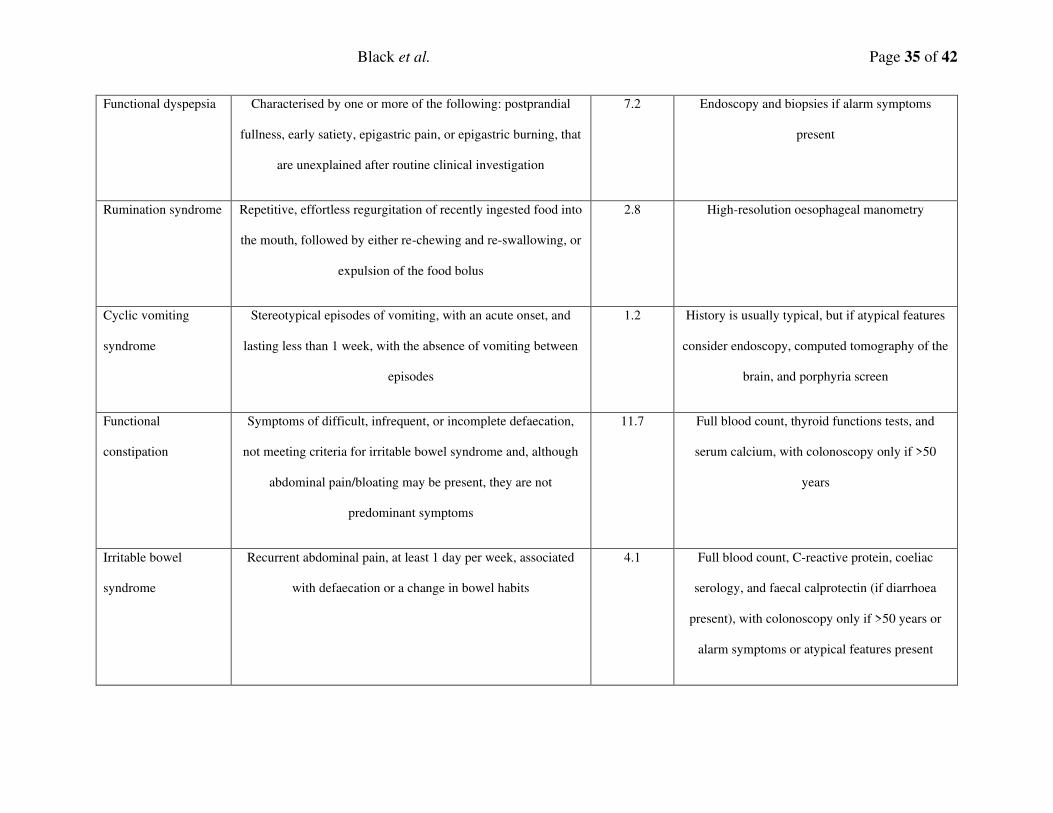
Black et al. Page 35 of 42
Functional dyspepsia Characterised by one or more of the following: postprandial
fullness, early satiety, epigastric pain, or epigastric burning, that
are unexplained after routine clinical investigation
7.2 Endoscopy and biopsies if alarm symptoms
present
Rumination syndrome Repetitive, effortless regurgitation of recently ingested food into
the mouth, followed by either re-chewing and re-swallowing, or
expulsion of the food bolus
2.8 High-resolution oesophageal manometry
Cyclic vomiting
syndrome
Stereotypical episodes of vomiting, with an acute onset, and
lasting less than 1 week, with the absence of vomiting between
episodes
1.2 History is usually typical, but if atypical features
consider endoscopy, computed tomography of the
brain, and porphyria screen
Functional
constipation
Symptoms of difficult, infrequent, or incomplete defaecation,
not meeting criteria for irritable bowel syndrome and, although
abdominal pain/bloating may be present, they are not
predominant symptoms
11.7 Full blood count, thyroid functions tests, and
serum calcium, with colonoscopy only if >50
years
Irritable bowel
syndrome
Recurrent abdominal pain, at least 1 day per week, associated
with defaecation or a change in bowel habits
4.1 Full blood count, C-reactive protein, coeliac
serology, and faecal calprotectin (if diarrhoea
present), with colonoscopy only if >50 years or
alarm symptoms or atypical features present
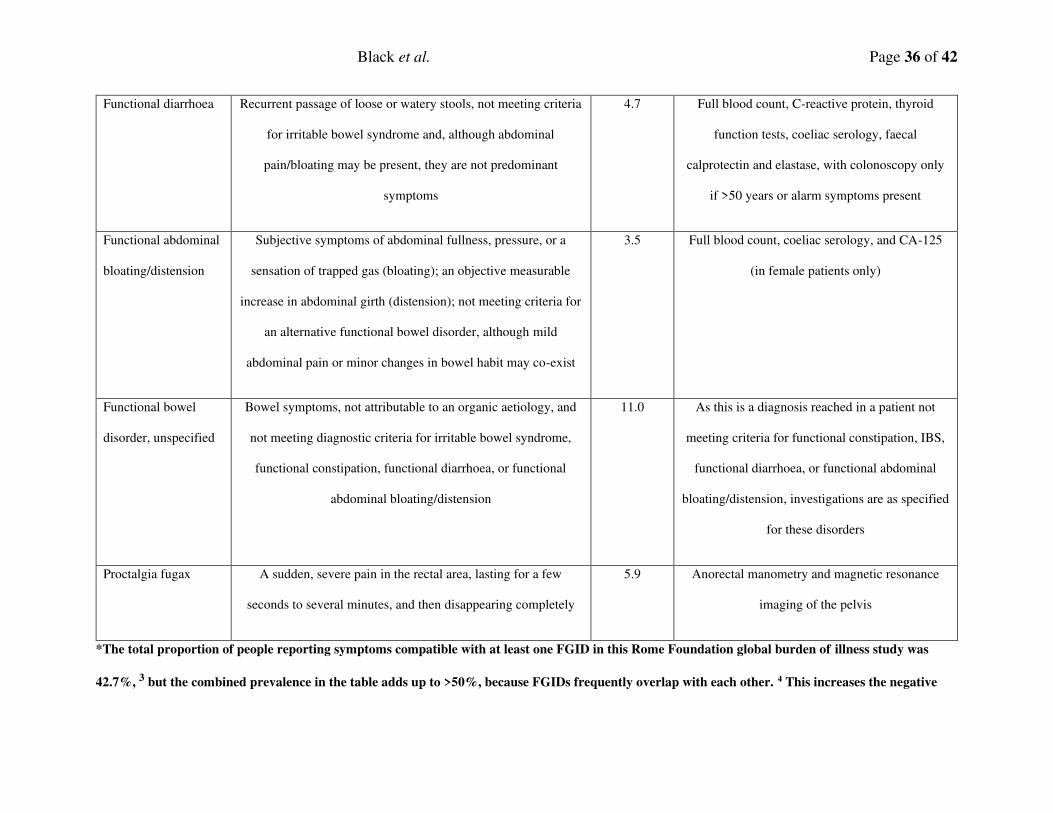
Black et al. Page 36 of 42
Functional diarrhoea Recurrent passage of loose or watery stools, not meeting criteria
for irritable bowel syndrome and, although abdominal
pain/bloating may be present, they are not predominant
symptoms
4.7 Full blood count, C-reactive protein, thyroid
function tests, coeliac serology, faecal
calprotectin and elastase, with colonoscopy only
if >50 years or alarm symptoms present
Functional abdominal
bloating/distension
Subjective symptoms of abdominal fullness, pressure, or a
sensation of trapped gas (bloating); an objective measurable
increase in abdominal girth (distension); not meeting criteria for
an alternative functional bowel disorder, although mild
abdominal pain or minor changes in bowel habit may co-exist
3.5 Full blood count, coeliac serology, and CA-125
(in female patients only)
Functional bowel
disorder, unspecified
Bowel symptoms, not attributable to an organic aetiology, and
not meeting diagnostic criteria for irritable bowel syndrome,
functional constipation, functional diarrhoea, or functional
abdominal bloating/distension
11.0 As this is a diagnosis reached in a patient not
meeting criteria for functional constipation, IBS,
functional diarrhoea, or functional abdominal
bloating/distension, investigations are as specified
for these disorders
Proctalgia fugax A sudden, severe pain in the rectal area, lasting for a few
seconds to several minutes, and then disappearing completely
5.9 Anorectal manometry and magnetic resonance
imaging of the pelvis
*The total proportion of people reporting symptoms compatible with at least one FGID in this Rome Foundation global burden of illness study was
42.7%, 3 but the combined prevalence in the table adds up to >50%, because FGIDs frequently overlap with each other. 4 This increases the negative
Black et al. Page 37 of 42
impact on quality of life and psychological health, and increases the likelihood of consultation, need for medical therapy, and potential for unnecessary
surgery. 4
†Many of these investigations are only available in secondary care. The clinician in primary care is more likely to make a diagnosis on clinical grounds
and treat or refer if there is diagnostic uncertainty.
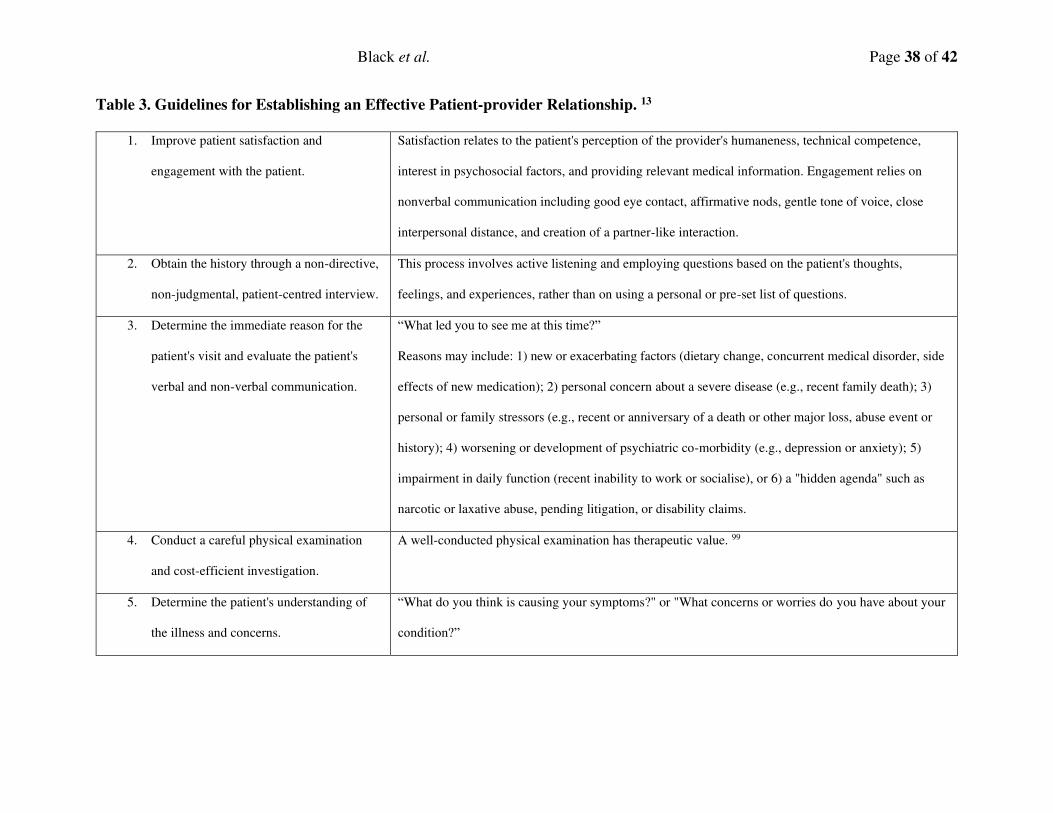
Black et al. Page 38 of 42
Table 3. Guidelines for Establishing an Effective Patient-provider Relationship. 13
1. Improve patient satisfaction and
engagement with the patient.
Satisfaction relates to the patient's perception of the provider's humaneness, technical competence,
interest in psychosocial factors, and providing relevant medical information. Engagement relies on
nonverbal communication including good eye contact, affirmative nods, gentle tone of voice, close
interpersonal distance, and creation of a partner-like interaction.
2. Obtain the history through a non-directive,
non-judgmental, patient-centred interview.
This process involves active listening and employing questions based on the patient's thoughts,
feelings, and experiences, rather than on using a personal or pre-set list of questions.
3. Determine the immediate reason for the
patient's visit and evaluate the patient's
verbal and non-verbal communication.
“What led you to see me at this time?”
Reasons may include: 1) new or exacerbating factors (dietary change, concurrent medical disorder, side
effects of new medication); 2) personal concern about a severe disease (e.g., recent family death); 3)
personal or family stressors (e.g., recent or anniversary of a death or other major loss, abuse event or
history); 4) worsening or development of psychiatric co-morbidity (e.g., depression or anxiety); 5)
impairment in daily function (recent inability to work or socialise), or 6) a "hidden agenda" such as
narcotic or laxative abuse, pending litigation, or disability claims.
4. Conduct a careful physical examination
and cost-efficient investigation.
A well-conducted physical examination has therapeutic value. 99
5. Determine the patient's understanding of
the illness and concerns.
“What do you think is causing your symptoms?" or "What concerns or worries do you have about your
condition?”
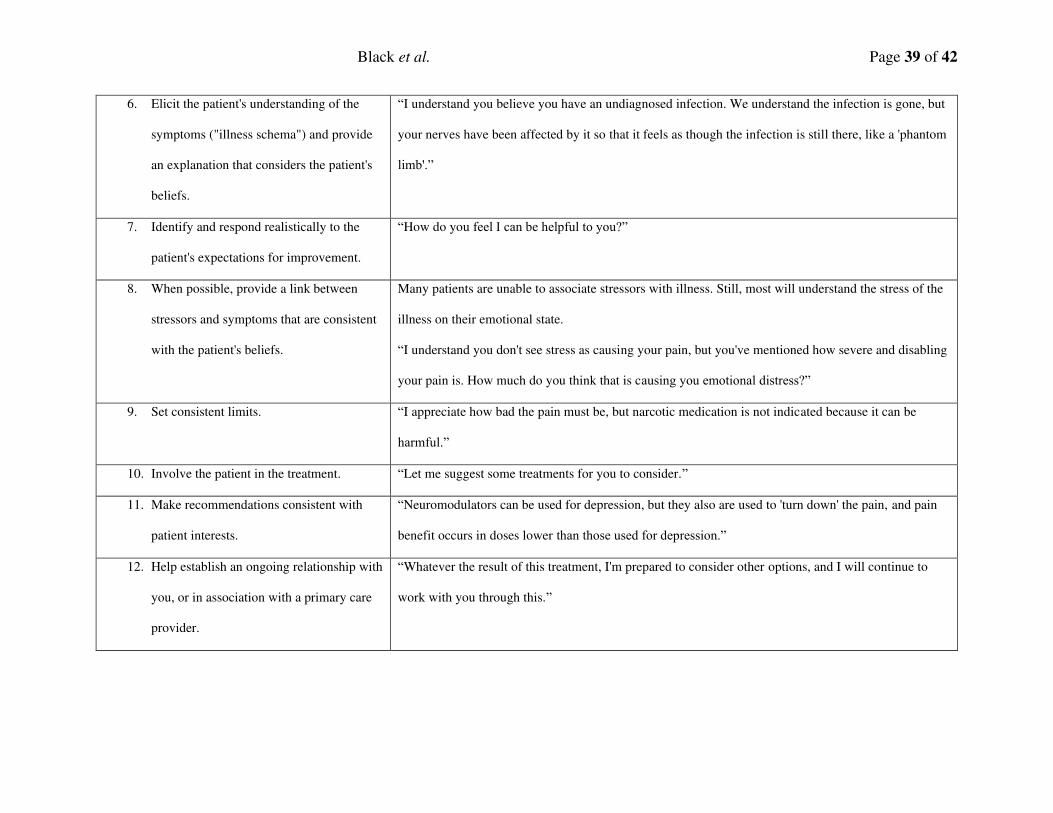
Black et al. Page 39 of 42
6. Elicit the patient's understanding of the
symptoms ("illness schema") and provide
an explanation that considers the patient's
beliefs.
“I understand you believe you have an undiagnosed infection. We understand the infection is gone, but
your nerves have been affected by it so that it feels as though the infection is still there, like a 'phantom
limb'.”
7. Identify and respond realistically to the
patient's expectations for improvement.
“How do you feel I can be helpful to you?”
8. When possible, provide a link between
stressors and symptoms that are consistent
with the patient's beliefs.
Many patients are unable to associate stressors with illness. Still, most will understand the stress of the
illness on their emotional state.
“I understand you don't see stress as causing your pain, but you've mentioned how severe and disabling
your pain is. How much do you think that is causing you emotional distress?”
9. Set consistent limits. “I appreciate how bad the pain must be, but narcotic medication is not indicated because it can be
harmful.”
10. Involve the patient in the treatment. “Let me suggest some treatments for you to consider.”
11. Make recommendations consistent with
patient interests.
“Neuromodulators can be used for depression, but they also are used to 'turn down' the pain, and pain
benefit occurs in doses lower than those used for depression.”
12. Help establish an ongoing relationship with
you, or in association with a primary care
provider.
“Whatever the result of this treatment, I'm prepared to consider other options, and I will continue to
work with you through this.”
Black et al. Page 40 of 42
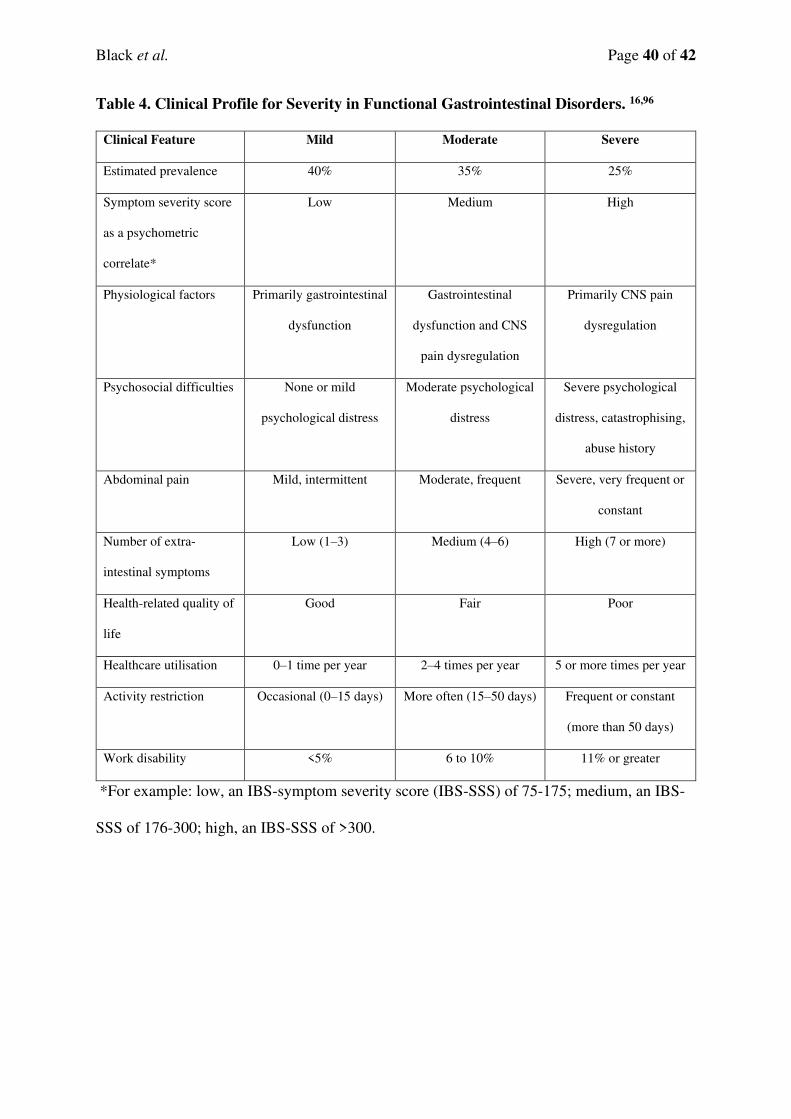
Table 4. Clinical Profile for Severity in Functional Gastrointestinal Disorders. 16,96
Clinical Feature Mild Moderate Severe
Estimated prevalence 40% 35% 25%
Symptom severity score
as a psychometric
correlate*
Low Medium High
Physiological factors Primarily gastrointestinal
dysfunction
Gastrointestinal
dysfunction and CNS
pain dysregulation
Primarily CNS pain
dysregulation
Psychosocial difficulties None or mild
psychological distress
Moderate psychological
distress
Severe psychological
distress, catastrophising,
abuse history
Abdominal pain Mild, intermittent Moderate, frequent Severe, very frequent or
constant
Number of extra-
intestinal symptoms
Low (1–3) Medium (4–6) High (7 or more)
Health-related quality of
life
Good Fair Poor
Healthcare utilisation 0–1 time per year 2–4 times per year 5 or more times per year
Activity restriction Occasional (0–15 days) More often (15–50 days) Frequent or constant
(more than 50 days)
Work disability <5% 6 to 10% 11% or greater
*For example: low, an IBS-symptom severity score (IBS-SSS) of 75-175; medium, an IBS-
SSS of 176-300; high, an IBS-SSS of >300.
Black et al. Page 41 of 42
Figure 1. A Biopsychosocial Model of Functional Gastrointestinal Disorders.
Adapted from van Oudenhove et al. 35
Figure 2. Intestinal Immune Activation Model of Functional Gastrointestinal Disorders.
It is hypothesised that, in a genetically primed host, environmental factors induce
immune activation. Antigen presentation of luminal antigens, such as pathogens or food
peptides, to T cells drives maturation of naïve T cells to T-helper 2 cells. The release of
associated cytokines (IL-4, IL-5, and IL-13) promotes the activation and recruitment of
eosinophils, B cells, and mast cells. In addition to the traditional T-helper 2 pathway,
secretion of IL-23 from antigen-presenting cells, such as dendritic cells, B cells, and
macrophages, promotes Th17 helper cell differentiation. The production of GM-CSF
from Th17 helper cells further drives eosinophil recruitment. Degranulation of mast
cells and eosinophils results in the release of inflammatory mediators, which can
damage the intestinal barrier, and stimulate and damage enteric nerve fibres, to induce
visceral hypersensitivity and motility disturbances, resulting in gastrointestinal
symptoms. α4β7 gut homing T cells are a marker of intestinal inflammation in both
functional dyspepsia and irritable bowel syndrome, and correlate with delayed gastric
emptying. Duodenal motor dysfunction may also impair duodenal acid clearance,
inducing intestino-gastric reflex responses that impair accommodation of the gastric
fundus, and increase transient lower oesophageal sphincter relaxations, leading to
gastro-oesophageal reflux. Signalling cascades, leading to further cytokine release, may
result in extra-intestinal symptoms, such as anxiety and fatigue. The site and extent of
intestinal immune activation may define the phenotype (proximal intestinal involvement
functional heartburn or functional dyspepsia; more distal involvement irritable bowel
syndrome, functional constipation, or functional diarrhoea). Adapted from Talley and
Talley. 39 27
Black et al. Page 42 of 42
Figure 3. Diagnostic Algorithm Pathway for a Patient Presenting with Uninvestigated
Constipation-type Symptoms. 61
*A recent change in bowel habit, unintentional weight loss (>10% of ideal body weight),
nocturnal symptoms, a family history of colorectal cancer, rectal bleeding (not caused
by haemorrhoids or anal fissures), or age >50 years.
The pathways have been validated and standardised by the Rome Foundation. Purple
represents a clinical state (diagnosis), gold represents a decision box (entry path with
“yes” and “no” exit paths), and green represents an action box (diagnostic test or
therapeutic action required).





























