Embed Size (px)
Citation preview

Clinical Science (2012) 122, 375–384 (Printed in Great Britain) doi:10.1042/CS20090464 375
GLP-1, exendin-4 and C-peptide regulatepancreatic islet microcirculation, insulinsecretion and glucose tolerance in rats
Lin WU∗, Anna OLVERLING†, Zhen HUANG†, Leif JANSSON‡, Hongfen CHAO∗,Xin GAO§ and Ake SJOHOLM†∗Department of Geriatrics, Fudan University, Zhongshan Hospital, 180 Fenglin Road, Shanghai 200032, People’s Republic ofChina, †Karolinska Institute, Department of Clinical Science and Education, Unit for Diabetes Research, Sodersjukhuset,SE-118 83 Stockholm, Sweden, ‡Department of Medical Cell Biology, University of Uppsala, SE-751 23 Uppsala, Sweden, and§Department of Endocrinology and Metabolism, Fudan University, Zhongshan Hospital, 180 Fenglin Road, Shanghai 200032,People’s Republic of China
A B S T R A C T
GLP-1 (glucagon-like peptide 1) and its mimetic exendin-4 are used against Type 2 diabetes.C-peptide has also proven promising to enhance insulin action. Since insulin secretion in vivocan be rapidly tuned by changes in islet microcirculation, we evaluated the influence of GLP-1,exendin-4 and C-peptide on pancreatic IBF (islet blood flow), and dynamic changes in insulinsecretion and glycaemia in the rat. Adult male Wistar rats were divided into four groups givenintravenous saline, GLP-1, exendin-4 or C-peptide respectively and administered either saline or30% glucose. Furthermore, we investigated the effect of intravenous infusion of different dosesof exendin-4 into either the femoral vein or the portal vein on islet microcirculation. A non-radioactive microsphere technique was adopted to measure the regional blood flow. Both GLP-1and exendin-4 prevented the glucose-induced PBF (pancreatic blood flow) redistribution into theislets. Infusion of exendin-4 into the portal vein did not alter pancreatic islet microcirculation,while infusion of exendin-4 into femoral vein significantly decreased basal IBF. C-peptide increasedbasal IBF and the proportion of IBF out of total PBF, but did not affect the islet microcirculationafter glucose administration. GLP-1, exendin-4 and C-peptide stimulated insulin secretion andsignificantly decreased glycaemia. Blocking NO formation did not prevent the decreased IBF andpost-load glycaemia evoked by exendin-4, but further decreased IBF and KBF (kidney blood flow)and increased basal glycaemia. Blocking the vagus nerve enhanced pancreatic IBF and furtherdecreased post-load glycaemia and KBF and increased basal glycaemia. The vascular modulatoryeffect on pancreatic islet microcirculation described herein, with subsequent effects on in vivoinsulin secretion and glycaemia, might be one of the mechanisms underlying the anti-diabeticactions of GLP-1 and its long acting mimetic exendin-4, as well as that of C-peptide.
INTRODUCTION
Pancreatic islet β-cell dysfunction is now consideredto be a requirement for, as well as an early lesion in,the development of both Type 1 and Type 2 diabetes
[1]. To maintain normal islet endocrine function notonly intracellular formation and release of insulin aremandatory but also the presence of an intact islet vas-cular system is crucial [2]. Changes in pancreatic isletmicrocirculation may impede insulin output in diabetic
Key words: exendin-4, glycaemia, insulin secretion, pancreatic islet, vasoactive effect.Abbreviations: bw, body weight; GK, Goto–Kakizaki; GLP-1, glucagon-like peptide 1; GLP-1R, GLP-1 receptor; IBF, islet bloodflow; fIBF, fractional IBF; IPGTT, intraperitoneal glucose tolerance test; KBF, kidney blood flow; l-NAME, NG-methyl-l-argininemethyl ester; MAP, mean arterial pressure; NOS, NO synthase; PBF, pancreatic blood flow.Correspondence: Professor Ake Sjoholm (email [email protected]) or Dr Xin Gao (email [email protected]).
C© The Authors Journal compilation C© 2012 Biochemical Society
www.clinsci.org
Clin
ical
Sci
ence

376 L. Wu and others
subjects, and could contribute to the pathogenesis of thedisease. Islet hyperperfusion and abnormal modulation ofIBF (islet blood flow) after glucose challenge have beenobserved in various animal models of glucose intoleranceand diabetes, including obese animals [3] as well as thenon-obese GK (Goto–Kakizaki) rats [4].
GLP-1 [glucagon-like peptide 1; GLP-1-(7–36)]and its mimetics are promising antidiabetic agents, theeffectiveness of which was confirmed by observationsin clinical trials [5–8]. Results from both in vitro [9]and in vivo [10] studies demonstrated a vasorelaxanteffect of GLP-1-(7–36) in the pulmonary circulation andconduit arteries in rodents. Furthermore, GLP-1-(7–36)has been shown to prevent the increase of IBF inducedby glucose administration in Wistar rats, and to decreasethe elevated basal IBF in diabetic GK rats [4]. However,the rapid degradation of GLP-1-(7–36) largely limits itsclinical use. Exendin-4 is a long-acting GLP-1 receptoragonist, possessing vasoactive effects that might bedifferent from those of native GLP-1. Gardiner et al.[11] reported that exendin-4 decreased mesentericblood flow in both a GLP-1 receptor-dependent and-independent way. In Type 2 diabetic rodent models,GLP-1 normalized the altered vascular tone, whereasexendin-4 did not affect the vascular responsiveness of theaorta [12]. Whether exendin-4 has the same vasoactiveeffect on islet microcirculation as GLP-1-(7–36) isunknown.
C-peptide has been reported to decrease glomerularhyperfiltration and increase nutritive endoneurial bloodflow in Type 1 diabetic animal models [13], and to increaseforearm blood flow in Type 1 diabetic patients [14], indic-ating that C-peptide might be a vasoactive peptide. If so, amore widespread action of C-peptide on the vasculaturein other organs, including the abundantly vascularizedendocrine pancreas, might exist. To our knowledge,one recently published in vitro study demonstratedthat mouse C-peptide induced constriction of pancreaticislet arterioles of diabetic mice but had no effect onnormoglycaemic controls [15]. Furthermore, there is oneprevious in vivo study when C-peptide doses in thepicomolar range failed to affect splanchnic blood flow[16]. However, the effect of more physiological doses ofC-peptide on islet perfusion has not been evaluated.
In view of the above, the present study aims toclarify the effects of the three peptides described, all withknown effects on islet endocrine function, on dynamicchanges of islet microcirculation, as well as changes ofin vivo insulin secretion and glycaemia in rat.
MATERIALS AND METHODS
AnimalsMale 3-month-old Wistar rats, weighing 350–420 g, werepurchased from ScanBur. All animals were kept under
standard conditions with controlled temperature and a12 h light/12 h dark cycle and free access to tap waterand pelleted food (Type R34; ScanBur). The study wasapproved by the local animal ethics committee of theKarolinska Institute, conforming to the ‘Guide forthe Care and Use of Laboratory Animals’ published byU.S. National Institutes of Health (NIH publication No.85-23, revised 1985).
IPGTT (intraperitoneal glucose tolerancetest)A total of 21 rats were fully anaesthetized beforeand during the whole procedure. Right after theintraperitoneal injection of 30 % (w/v) d-glucose solution[2 g of glucose/kg of bw (body weight)], GLP-1(50 μg/kg of bw; Sigma), exendin-4 (5 μg/kg of bw, pro-vided by Amylin) and C-peptide (75 nmol/kg of bw,provided by Creative Peptides) were given as intravenousbolus injections. All substances were dissolved in 1 mlof saline. Control animals were injected with 1 ml ofsaline alone. Blood samples were drawn from the tailvein immediately before and 10, 30, 60 and 120 min afterglucose administration. The area under the curve for theIPGTT was determined by computerized image analysisas described previously [17].
Surgical procedureNon-fasted rats were kept fully anaesthetized withan intraperitoneal injection of sodium thiobutabarbital(120 mg/kg of bw; Inactin, Research BiochemicalsInternational), tracheotomized and placed on a heatedoperating table to keep the body temperature at 37 ◦C.Polyethylene catheters were inserted via the right carotidartery into the ascending aorta, and into the femoral artery[18]. Throughout the rest of the experiment, arterialblood pressure was monitored by a pressure transducer(PDCR 75/1; Druck) via the catheter placed in thecarotid artery. The external jugular vein was then exposedfor intravenous injection of tested substances. After theprocedures were done, it took approximately 15–20 minuntil blood pressure became stable.
Administration of peptides and glucoseRats were assigned into groups and administeredintravenous bolus injection into the right jugular veinof 0.2 ml of saline, GLP-1 (50 μg/kg of bw), exendin-4 (5 μg/kg of bw) or C-peptide (75 nmol/kg of bw)respectively. The tested substances were dissolved in0.2 ml of saline (0.9 %, w/v). Then 5 min after theinjection, another intravenous injection of 1 ml of salineor 30 % (w/v) glucose was given into the same vein.These animals will be referred to below as saline-treatedor glucose-treated. After another 5 min (10 min after thefirst injection), blood flow of the pancreas and islets wasmeasured.
C© The Authors Journal compilation C© 2012 Biochemical Society

GLP-1, exendin-4 and C-peptide regulate pancreatic islet microcirculation 377
Administration of exendin-4 via differentroutesAs the portal vein wall reportedly contains a GLP-1-regulated glucose sensor [19], we wanted to explorewhether the GLP-1R (GLP-1 receptor) agonist exendin-4had any effects in this system. The portal vein was exposedas described in detail previously [20]. Catheters wereinserted into either portal vein or femoral vein. Eitherexendin-4 or saline was infused (2 ml/h for 15 min) intothe catheter. Rats were thus divided into five groups withreference to the different dosages and routes of infusion:(i) saline in the portal vein, (ii) exendin-4 (5 μg/kg of bw)in the portal vein, (iii) exendin-4 (10 μg/kg of bw) in theportal vein, (iv) saline in the femoral vein, (v) exendin-4(10 μg/kg) in the femoral vein.
Administration of L-NAME (NG-methyl-L-arginine methyl ester) and atropineIn an attempt to address whether NO and/or the vagusnerve were involved in mediating the positive effectsnoted, male Wistar rats weighing 350–430 g were injectedintravenously either with the NOS (NO synthase)blocker l-NAME (25 mg/kg of bw; Sigma) or atropine(0.5 mg/kg of bw; Sigma) 10 min prior to the injectionof exendin-4 (5 μg/kg) into the jugular vein [17]. At5 min after the injection of exendin-4, 1 ml of 30 % (w/v)glucose was injected into the same vein. After another5 min (20 min after the first intravenous injection), bloodflow was measured using the microsphere techniquedescribed below.
Blood flow measurementWhole PBF (pancreatic blood flow) and IBF weremeasured with a non-radioactive microsphere technique,as described previously in detail [21]. Briefly, 5 min afterthe injection of either 1 ml of saline or 30 % glucose, (1.5–2.0)×105 non-radioactive microspheres (IMT; StasonLabs), with a mean diameter of 10 μm, were injectedwithin 10 s via the carotid catheter. Starting 5 s beforethe microsphere injection, and continuing for 60 s, anarterial blood sample (the reference sample) was collectedfrom the catheter in the femoral artery into a pre-weighed tube. The exact withdrawal rate was thendetermined in each animal by weighing the sample. Aftersecuring the reference sample, another arterial bloodsample was drawn for measurement of blood glucose andserum insulin concentrations. The animals were killedimmediately afterwards. Pancreas and adrenal glands, aswell as samples from left kidney (including both cortexand medulla), were taken out, blotted and weighed. Themicrosphere contents in these organs were determinedseparately. The tissue samples were then treated with afreeze-thawing technique to visualize the microspheresas described previously [22], which was achieved by
applying a microscope (Zeiss MB6; Leica) equipped withboth bright and dark field illumination.
The number of microspheres in the islet and exocrineparenchyma was counted blindly. The microspherecontent of each of the arterial reference sampleswas determined by transferring the samples to glassmicrofibre filters and counting the microspheres undera stereo microscope.
The blood flow values were calculated according to theequation:
Qorg = Qref × Norg/Nref
where Qorg is the organ blood flow (ml/min), Qref is thewithdrawal rate of the reference sample (ml/min), Norg isthe number of microspheres present in the organ and Nref
is the number of microspheres in the reference sample.The microsphere contents of the adrenal glands wereused as a control to confirm an even distribution of themicrospheres in the arterial circulation. A difference of<10 % in blood flow values between the adrenal glandswas used to confirm adequate mixing of the spheres inthe circulation.
Measurement of blood glucose and seruminsulin concentrationsBlood glucose concentrations were measured with aglucose meter (Ascensia Contour; Bayer HealthCare) andserum insulin concentrations with ELISA kits (rat insulinELISA; Mercodia).
Statistical analysisAll values are given as means +− S.E.M. For comparisonsof means among more than two groups, one-wayANOVA followed by two-tail Bonferroni post-hoc testswere adopted. For statistical comparisons between thesubgroups within each group, an unpaired Student’st test was used. P < 0.05 was considered to be statisticallysignificant.
RESULTS
GLP-1 and exendin-4 improve glucosetolerance in normoglycaemic ratsAn intravenous bolus injection of GLP-1-(7–36),exendin-4 and C-peptide markedly decreased the risein blood glucose concentration at 30 min after anintraperitoneal glucose load (Figure 1A). At 60 min afterthe glucose load, only GLP-1-(7–36) and exendin-4still showed glucose-lowering effects, and no markeddifference in glycaemia was observed between rats treatedwith C-peptide and saline (Figure 1A). Glucose tolerancewas significantly improved in rats treated with GLP-1-(7–36) and exendin-4, but not with C-peptide (Figure 1B).At 10 min after the glucose load, only GLP-1-treated ratsshowed markedly elevated serum insulin concentrations;
C© The Authors Journal compilation C© 2012 Biochemical Society

378 L. Wu and others
Figure 1 Glycaemia and serum insulin concentrations during IPGTTImmediately ater the intraperitoneal glucose bolus (30 % w/v, 2 g of glucose/kg of bw), 1 ml of saline, GLP-1-(7–36) (50 μg/kg of bw, exendin-4 (5 μg/kg of bw)or C-peptide (75 nmol/kg of bw) were injected intravenously into anaesthetized adult male Wistar rats. All substances were dissolved in 1 ml of 0.9 % saline. Bloodsamples were drawn from the tail vein immediately before and 10, 30, 60 and 120 min after glucose administration. Blood glucose concentrations (A) were measuredby a glucose meter. Changes in the glucose response are expressed as the area under the curve (AUC) integrated over 120 min (B). Serum insulin concentrations(C) were measured by ELISA kits. Changes in the insulin response are expressed as the AUC integrated over 120 min (D). Values represent means+− S.E.M. for 5–6animals. ∗P < 0.05, ∗∗P < 0.01 and
∗∗∗P < 0.001 compared with controls, as determined using an unpaired Student’s t test.
however, at 30 and 60 min after the glucose load, seruminsulin concentrations were substantially enhanced in allthe groups when compared with saline-treated controls(Figure 1C). In vivo insulin secretion induced by theintraperitoneal glucose load was significantly increasedin groups treated with GLP-1-(7–36), exendin-4 and C-peptide (Figure 1D).
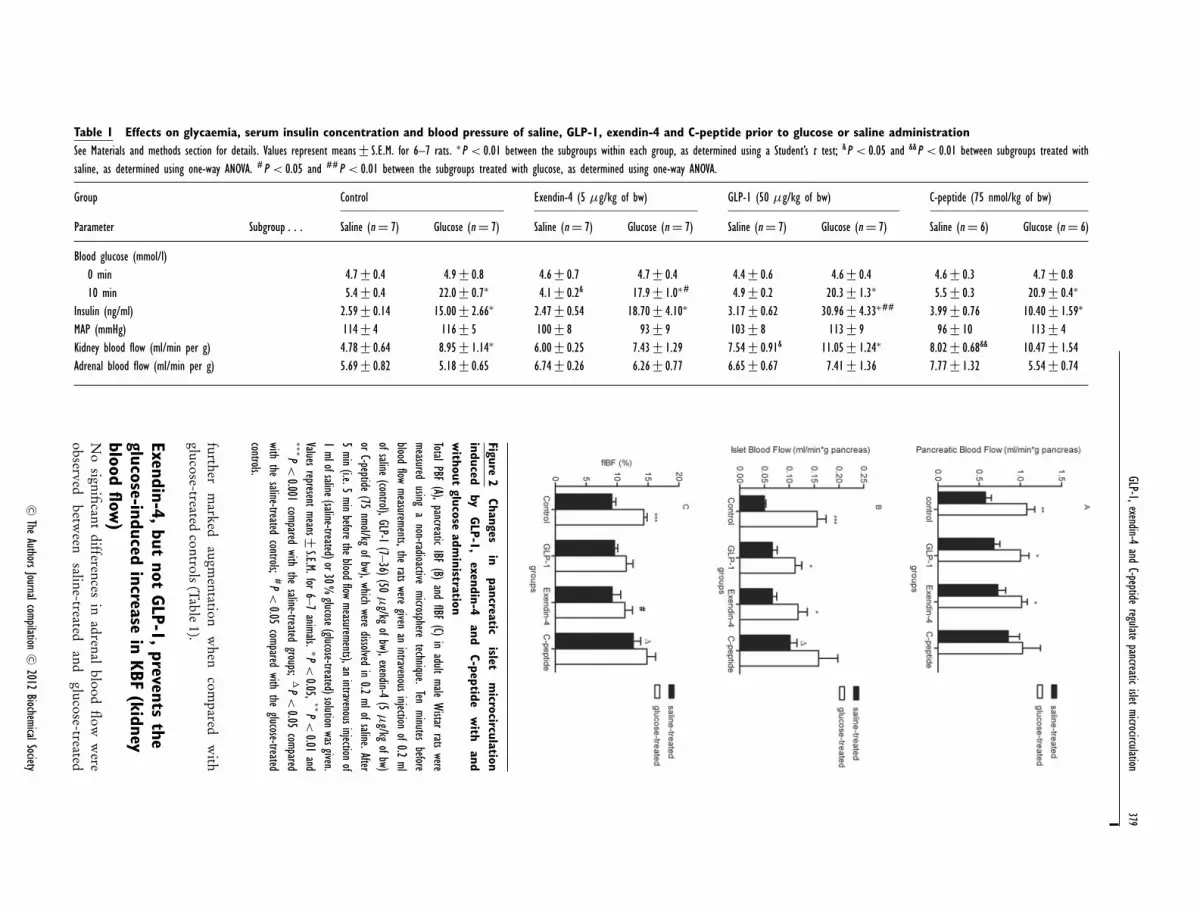
GLP-1 and exendin-4 decrease islethyperperfusion in hyperglycaemic ratsAn intravenous bolus injection of 1 ml 30 % glucosemarkedly increased both PBF and IBF when comparedwith saline-treated controls (Figure 2). Also, fIBF(fractional IBF; the fraction of whole PBF throughthe islets) was significantly increased (Figure 2C). Insaline-treated subgroups, no significant differences wereobserved in either PBF, IBF or fIBF, between pre-treatment with either saline, GLP-1-(7–36) or exendin-4, while administration of C-peptide markedly increasedboth IBF and fIBF (Figures 2B and 2C). In the glucose-treated subgroups, neither GLP-1-(7–36) nor exendin-4 or C-peptide affected the glucose-induced increase inPBF and IBF (Figure 2). However, the difference in fIBFbetween saline-treated and glucose-treated subgroupswas not statistically significant in groups pre-treatedwith exendin-4 and GLP-1-(7–36). Intervention withexendin-4 markedly decreased the glucose induced fIBFincrease (P < 0.05) when compared with corresponding
controls. A slight increase in fIBF was observed in saline-treated, but not glucose-treated, rats given C-peptide(Figure 2C).
Exendin-4 decreases glycaemia withoutfurther enhancing serum insulinconcentrationsAfter the surgical procedures, no significant differencesbetween any of the groups were observed in termsof MAP (mean arterial pressure), glycaemia orbody temperature (results not shown). No significantdifferences of MAP were observed after intravenousinjection of the tested substances (Table 1). In the saline-treated rats, exendin-4 induced a slight but statisticallysignificant decrease of glycaemia which was within thephysiological range, while no significant changes inblood glucose concentrations were observed in groupsgiven GLP-1-(7–36) or C-peptide (Table 1). Also, nosignificant changes in serum insulin concentrations wereobserved in saline-treated rats. In the glucose-treatedanimals, neither GLP-1-(7–36) nor C-peptide affectedglycaemia, while exendin-4 again significantly decreasedthe blood glucose concentrations (Table 1). As expected,serum insulin concentrations were markedly elevatedin all glucose-treated rats compared with saline-treatedanimals. GLP-1-(7–36), but not exendin-4, induced a
C© The Authors Journal compilation C© 2012 Biochemical Society
GLP-1,exendin-4and
C-peptideregulate
pancreaticislet
microcirculation379
Table 1 Effects on glycaemia, serum insulin concentration and blood pressure of saline, GLP-1, exendin-4 and C-peptide prior to glucose or saline administrationSee Materials and methods section for details. Values represent means+− S.E.M. for 6–7 rats. ∗P < 0.01 between the subgroups within each group, as determined using a Student’s t test; &P < 0.05 and &&P < 0.01 between subgroups treated withsaline, as determined using one-way ANOVA. #P < 0.05 and ##P < 0.01 between the subgroups treated with glucose, as determined using one-way ANOVA.
Group Control Exendin-4 (5 μg/kg of bw) GLP-1 (50 μg/kg of bw) C-peptide (75 nmol/kg of bw)
Parameter Subgroup . . . Saline (n = 7) Glucose (n = 7) Saline (n = 7) Glucose (n = 7) Saline (n = 7) Glucose (n = 7) Saline (n = 6) Glucose (n = 6)
Blood glucose (mmol/l)0 min 4.7 +− 0.4 4.9 +− 0.8 4.6+− 0.7 4.7+− 0.4 4.4 +− 0.6 4.6 +− 0.4 4.6 +− 0.3 4.7+− 0.810 min 5.4 +− 0.4 22.0+− 0.7∗ 4.1+− 0.2& 17.9+− 1.0∗# 4.9 +− 0.2 20.3 +− 1.3∗ 5.5 +− 0.3 20.9+− 0.4∗
Insulin (ng/ml) 2.59+− 0.14 15.00+− 2.66∗ 2.47+− 0.54 18.70+− 4.10∗ 3.17+− 0.62 30.96+− 4.33∗## 3.99 +− 0.76 10.40+− 1.59∗
MAP (mmHg) 114+− 4 116+− 5 100+− 8 93+− 9 103+− 8 113+− 9 96 +− 10 113+− 4Kidney blood flow (ml/min per g) 4.78+− 0.64 8.95+− 1.14∗ 6.00+− 0.25 7.43+− 1.29 7.54+− 0.91& 11.05+− 1.24∗ 8.02 +− 0.68&& 10.47+− 1.54Adrenal blood flow (ml/min per g) 5.69+− 0.82 5.18+− 0.65 6.74+− 0.26 6.26+− 0.77 6.65+− 0.67 7.41+− 1.36 7.77 +− 1.32 5.54+− 0.74
Figure2
Changesin
pancreaticislet
microcirculation
inducedby
GLP-1,
exendin-4and
C-peptidew
ithand
without
glucoseadm
inistrationTotalPBF
(A),pancreatic
IBF(B)
andfIBF
(C)in
adultmale
Wistar
ratswere
measuredusing
anon-radioactive
microspheretechnique.
Tenminutes
beforeblood
flowmeasurements,the
ratswere
givenan
intravenousinjection
of0.2ml
ofsaline(control),GLP-1
(7–36)(50μ
g/kgofbw),exendin-4
(5μ
g/kgofbw)
orC-peptide
(75nmol/kg
ofbw),whichwere
dissolvedin
0.2mlofsaline.After
5min
(i.e.5min
beforethe
bloodflow
measurements),anintravenousinjection
of1mlofsaline(saline-treated)or30%
glucose(glucose-treated)solutionwasgiven.
Valuesrepresent
means +−S.E.M.for
6–7animals. ∗P
<0.05,
∗∗P<
0.01and
∗∗∗P<
0.001compared
withthe
saline-treatedgroups;
�P<
0.05compared
withthe
saline-treatedcontrols;
#P<
0.05compared
withthe
glucose-treatedcontrols.
furtherm
arkedaugm
entationw
hencom
paredw
ithglucose-treated
controls(Table
1).
Exendin-4,but
notGLP-1,
preventsthe
glucose-inducedincrease
inKBF
(kidneyblood
flow)
No
significant
differencesin
adrenalblood
flow
were
observedbetw
eensaline-treated
andglucose-treated
C ©The
AuthorsJournalcompilation
C ©2012
BiochemicalSociety

380 L. Wu and others
subgroups, irrespective of the pre-treatment (Table 1).Glucose injection induced a significant increase in KBF.Administration of GLP-1-(7–36) significantly increasedbasal KBF, but did not affect KBF stimulated by glucose.Conversely, exendin-4 had no effect on basal KBF,whereas it prevented the increase in KBF induced byglucose. C-peptide elevated basal KBF significantly, buthad no effect on glucose-stimulated KBF (Table 1).
Exendin-4 decreases glycaemia andsplanchnic blood flow by systemic, butnot portal, administration innormoglycaemic ratsInfusion of the GLP-1R agonist exendin-4 directly intothe portal vein, known to contain a GLP-1-regulatedglucose sensor [19], affected neither glycaemia norsplanchnic blood flow, regardless of the dosages (Table 2).In contrast, when exendin-4 was infused into the femoralvein at the dosage of 10 μg/kg of bw, a significant decreasein blood glucose concentration, IBF, duodenal blood flowand KBF was observed (Table 2).
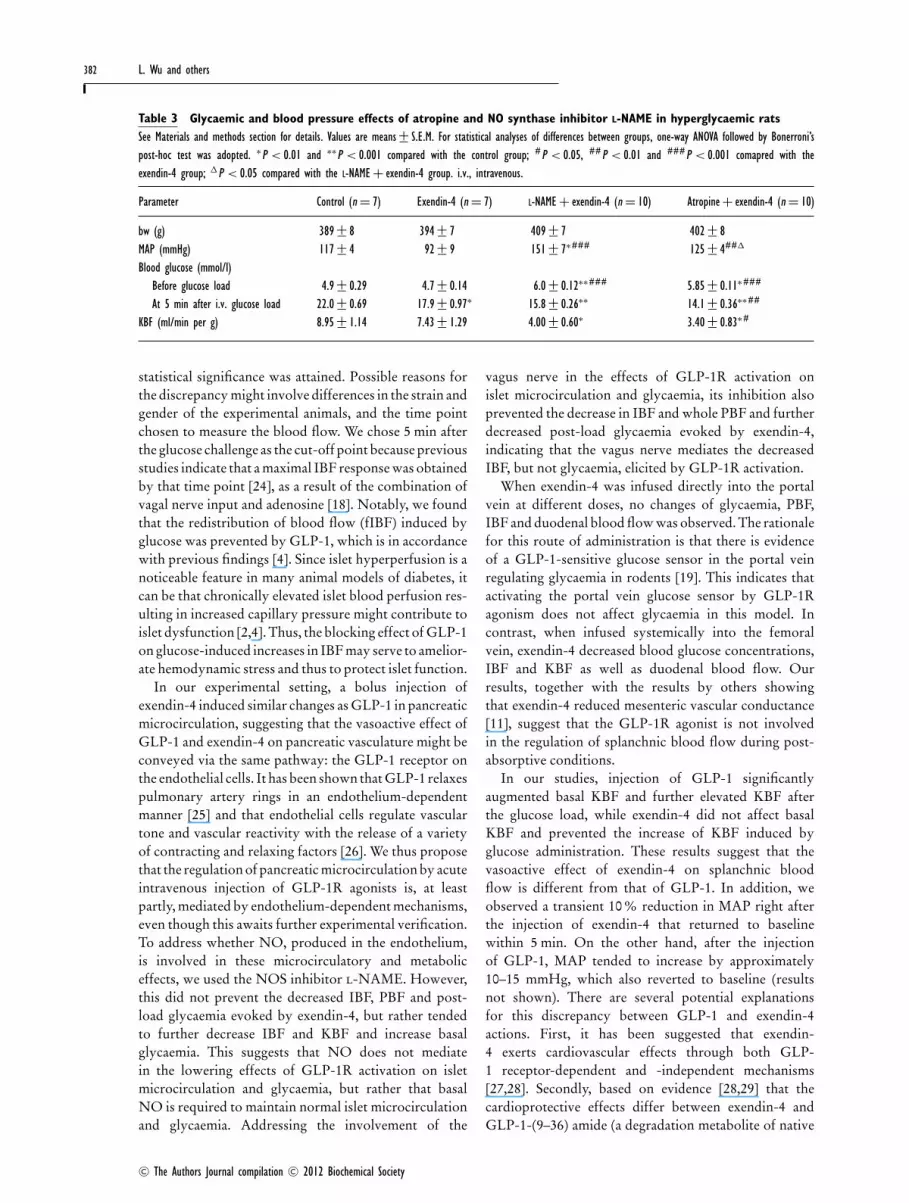
Glycaemic and vascular effects of the NOSinhibitor L-NAME and atropine inhyperglycaemic ratsIn a separate series of experiments (Table 3 and Figure 3),attempting to address whether NO and/or the vagusnerve were involved in mediating the positive effectsnoted, 1 ml of 30 % glucose was injected 5 min beforeblood flow measurements. MAPs before the injection ofthe tested substances were similar in all the groups (resultsnot shown). At the time of blood flow measurement,MAP was significantly higher in the l-NAME-pre-treated group than in the other three groups. The NOSinhibitor l-NAME did not prevent the decreased IBF,PBF and post-load glycaemia evoked by exendin-4,but rather tended to further decrease IBF and KBFand increase basal glycaemia (Table 3 and Figure 3).Blocking the vagus nerve by atropine enhanced IBFand pancreatic IBF, leaving the proportion of IBF outof total PBF unaltered and further decreased post-load glycaemia and KBF and increased basal glycaemia(Table 3 and Figure 3).
DISCUSSION
We show in the present study that rat islet microcircu-lation and glycaemia can be regulated by native GLP-1,by its stabile mimetic exendin-4 and by C-peptide. Ourresults confirm previous findings [21–24] that glucoseadministration acutely and markedly stimulates both PBFand IBF, and induces a re-distribution of PBF diverting itinto the islets, such that the fraction IBF out of PBF(i.e. fIBF) is augmented by glucose. This is mediated
Figure 3 Glycaemic and vascular effects of atropine and NOsynthase inhibitor L-NAME in hyperglycaemic ratsIn an attempt to address whether NO and/or the vagus nerve were involvedin mediating the effects noted, either atropine (0.5 mg/kg of bw) or L-NAME(25 mg/kg of bw) was injected intravenously 10 min before the administrationof exendin-4 (5 μg/kg of bw) and 5 min before the bolus intravenous injectionof 1 ml of 30 % glucose. PBF and IBF were measured using a non-radioactivemicrosphere technique. Values represent means +− S.E.M. for 7 or 10 animals.One-way ANOVA followed by Bonferroni’s post-hoc test was used for the statisticalanalysis. ∗P < 0.05 and ∗∗∗P < 0.001 compared with hyperglycaemic controls;#P < 0.05 compared with the exendin-4-treated group. �P < 0.05 comparedwith the the L-NAME-pre-treated group.
by complicated interactions between the nervous systemand metabolically induced signals [18]. In contrast with aprevious report [4], intravenous administration of GLP-1did not affect basal islet microcirculation acutely in ourmale Wistar rats. Although a tendency towards increasedbasal IBF and decreased stimulated IBF was observed, no
C© The Authors Journal compilation C© 2012 Biochemical Society

GLP-1,exendin-4and
C-peptideregulate
pancreaticislet
microcirculation381
Table 2 Effect of different doses and routes of exendin-4 infusion on organ microcirculation and glycaemiaSee the Materials and methods section for details. Exendin-4 (5 or 10 μg/kg of bw) or saline was infused (2 ml/h for 15 min) into the portal or femoral vein. Values are means+− S.E.M. ∗P < 0.05 and
∗∗P < 0.01 compared with animals infused
with saline in the femoral vein, as determined using a Student’s t test. N.D., not determined.
Treatment
Saline Exendin (5 μg/kg of bw) Exendin (10 μg/kg of bw) Saline Exendin (10 μg/kg of bw)
Parameter Injection site . . . Portal vein (n = 11) Portal vein (n = 8) Portal vein (n = 8) Femoral vein (n = 7) Femoral vein (n = 8)
Blood glucose (mmol/l) 4.7 +− 0.2 5.2 +− 0.2 5.0 +− 0.2 5.3 +− 0.1 4.8+− 0.1∗
Insulin (ng/ml) 4.52 +− 0.47 3.57 +− 0.28 N.D. 4.53+− 0.54 N.D.Mean arterial blood pressure (mmHg) 114+− 4 112+− 5 112+− 5 111+− 5 121+− 2Haematocrit (%) 44.5+− 0.3 45.0 +− 0.3 44.9+− 0.6 44.9+− 0.3 45.0+− 0.3Pancreatic blood flow (ml/min per g) 0.78+− 0.06 1.10 +− 0.16 0.88+− 0.10 0.92+− 0.14 0.73+− 0.08Islet blood flow (μl/min per g of pancreas) 68+− 6 86 +− 15 61+− 5 74+− 10 50+− 5∗
Islet blood flow (% of pancreatic blood flow) 8.8+− 0.5 7.8 +− 0.7 7.2 +− 0.3 8.3 +− 0.8 7.2+− 0.7Duodenal blood flow (ml/min per g) 2.82 +− 0.32 3.86 +− 0.79 3.56+− 0.45 3.70+− 0.44 1.89+− 0.23∗∗
Colonic blood flow (ml/min per g) 1.12+− 0.13 1.65 +− 0.27 1.04+− 0.13 1.40+− 0.40 1.12+− 0.16Kidney blood flow (ml/min per g) 4.07+− 0.45 3.85 +− 0.51 3.21+− 0.40 4.31+− 0.53 2.34+− 0.22∗∗
Adrenal blood flow (ml/min per g) 6.68 +− 0.45 8.60 +− 1.18 6.22+− 0.46 9.72+− 1.89 5.31+− 0.62
C ©The
AuthorsJournalcompilation
C ©2012
BiochemicalSociety
382 L. Wu and others
Table 3 Glycaemic and blood pressure effects of atropine and NO synthase inhibitor L-NAME in hyperglycaemic ratsSee Materials and methods section for details. Values are means+− S.E.M. For statistical analyses of differences between groups, one-way ANOVA followed by Bonerroni’spost-hoc test was adopted. ∗P < 0.01 and ∗∗P < 0.001 compared with the control group; #P < 0.05, ##P < 0.01 and ###P < 0.001 comapred with theexendin-4 group; �P < 0.05 compared with the L-NAME + exendin-4 group. i.v., intravenous.
Parameter Control (n = 7) Exendin-4 (n = 7) L-NAME + exendin-4 (n = 10) Atropine+ exendin-4 (n = 10)
bw (g) 389+− 8 394+− 7 409+− 7 402+− 8MAP (mmHg) 117+− 4 92+− 9 151+− 7∗### 125+− 4##�
Blood glucose (mmol/l)Before glucose load 4.9 +− 0.29 4.7+− 0.14 6.0+− 0.12∗∗### 5.85+− 0.11∗###
At 5 min after i.v. glucose load 22.0+− 0.69 17.9+− 0.97∗ 15.8 +− 0.26∗∗ 14.1+− 0.36∗∗##
KBF (ml/min per g) 8.95+− 1.14 7.43+− 1.29 4.00+− 0.60∗ 3.40+− 0.83∗#
statistical significance was attained. Possible reasons forthe discrepancy might involve differences in the strain andgender of the experimental animals, and the time pointchosen to measure the blood flow. We chose 5 min afterthe glucose challenge as the cut-off point because previousstudies indicate that a maximal IBF response was obtainedby that time point [24], as a result of the combination ofvagal nerve input and adenosine [18]. Notably, we foundthat the redistribution of blood flow (fIBF) induced byglucose was prevented by GLP-1, which is in accordancewith previous findings [4]. Since islet hyperperfusion is anoticeable feature in many animal models of diabetes, itcan be that chronically elevated islet blood perfusion res-ulting in increased capillary pressure might contribute toislet dysfunction [2,4]. Thus, the blocking effect of GLP-1on glucose-induced increases in IBF may serve to amelior-ate hemodynamic stress and thus to protect islet function.
In our experimental setting, a bolus injection ofexendin-4 induced similar changes as GLP-1 in pancreaticmicrocirculation, suggesting that the vasoactive effect ofGLP-1 and exendin-4 on pancreatic vasculature might beconveyed via the same pathway: the GLP-1 receptor onthe endothelial cells. It has been shown that GLP-1 relaxespulmonary artery rings in an endothelium-dependentmanner [25] and that endothelial cells regulate vasculartone and vascular reactivity with the release of a varietyof contracting and relaxing factors [26]. We thus proposethat the regulation of pancreatic microcirculation by acuteintravenous injection of GLP-1R agonists is, at leastpartly, mediated by endothelium-dependent mechanisms,even though this awaits further experimental verification.To address whether NO, produced in the endothelium,is involved in these microcirculatory and metaboliceffects, we used the NOS inhibitor l-NAME. However,this did not prevent the decreased IBF, PBF and post-load glycaemia evoked by exendin-4, but rather tendedto further decrease IBF and KBF and increase basalglycaemia. This suggests that NO does not mediatein the lowering effects of GLP-1R activation on isletmicrocirculation and glycaemia, but rather that basalNO is required to maintain normal islet microcirculationand glycaemia. Addressing the involvement of the
vagus nerve in the effects of GLP-1R activation onislet microcirculation and glycaemia, its inhibition alsoprevented the decrease in IBF and whole PBF and furtherdecreased post-load glycaemia evoked by exendin-4,indicating that the vagus nerve mediates the decreasedIBF, but not glycaemia, elicited by GLP-1R activation.
When exendin-4 was infused directly into the portalvein at different doses, no changes of glycaemia, PBF,IBF and duodenal blood flow was observed. The rationalefor this route of administration is that there is evidenceof a GLP-1-sensitive glucose sensor in the portal veinregulating glycaemia in rodents [19]. This indicates thatactivating the portal vein glucose sensor by GLP-1Ragonism does not affect glycaemia in this model. Incontrast, when infused systemically into the femoralvein, exendin-4 decreased blood glucose concentrations,IBF and KBF as well as duodenal blood flow. Ourresults, together with the results by others showingthat exendin-4 reduced mesenteric vascular conductance[11], suggest that the GLP-1R agonist is not involvedin the regulation of splanchnic blood flow during post-absorptive conditions.
In our studies, injection of GLP-1 significantlyaugmented basal KBF and further elevated KBF afterthe glucose load, while exendin-4 did not affect basalKBF and prevented the increase of KBF induced byglucose administration. These results suggest that thevasoactive effect of exendin-4 on splanchnic bloodflow is different from that of GLP-1. In addition, weobserved a transient 10 % reduction in MAP right afterthe injection of exendin-4 that returned to baselinewithin 5 min. On the other hand, after the injectionof GLP-1, MAP tended to increase by approximately10–15 mmHg, which also reverted to baseline (resultsnot shown). There are several potential explanationsfor this discrepancy between GLP-1 and exendin-4actions. First, it has been suggested that exendin-4 exerts cardiovascular effects through both GLP-1 receptor-dependent and -independent mechanisms[27,28]. Secondly, based on evidence [28,29] that thecardioprotective effects differ between exendin-4 andGLP-1-(9–36) amide (a degradation metabolite of native
C© The Authors Journal compilation C© 2012 Biochemical Society

GLP-1, exendin-4 and C-peptide regulate pancreatic islet microcirculation 383
GLP-1) it may be that different receptor entities mediatethe different effects of the two peptides.
A bolus intravenous injection of C-peptide sig-nificantly increased basal pancreatic IBF, fIBF andKBF, while the same tendency, albeit not statisticallysignificant, was seen for PBF. On the other hand,no significant differences in organ blood flow wereobserved under hyperglycaemic conditions in responseto C-peptide. These results differ from previous invivo studies done on normal subjects and animalswhen exogenous C-peptide showed no vasoactiveeffects. C-peptide has been shown to exert severalbeneficial effects against neuropathy, nephropathyand myocardial dysfunction in Type 1 diabeticsubjects and animal models [14,30]. When applied tohealthy subjects, C-peptide did not affect forearm bloodflow [14]. In in vitro studies, perfusion with C-peptide didnot affect isolated islet arterioles from normoglycaemicmice [15]. The discrepancy might in part be explainedby the fact that the C-peptide concentrations reachedin the present study were most likely higher than thephysiological interval of 0.5–3.0 nM.
Specific binding of C-peptide to cell membranebinding sites has been demonstrated for various celltypes, and this leads to an up-regulation of eNOS(endothelial NOS) transcription and activity [31], therebyaugmenting NO production. The heightened blood flowobserved in islet and kidney induced by C-peptideis entirely consistent with such an effect on NOproduction in the vascular endothelium, dilating theafferent vessels and thereby enhancing blood flow tothese organs [32]. In conclusion, we found that GLP-1,exendin-4 and C-peptide stimulated insulin secretion ina glucose-dependent manner and significantly decreasedglycaemia after glucose administration. Both GLP-1 andexendin-4 prevented the glucose-induced blood flowredistribution into islets, which may serve to protect isletfunction against chronic haemodynamic stress evokedby hyperglycaemia. C-peptide increased basal IBF andfIBF, but did not affect islet microcirculation afterglucose administration. The vascular modulatory effecton pancreatic islet microcirculation might be one of themechanisms behind the anti-diabetic actions of GLP-1and its long acting analogue exendin-4, as well as that ofC-peptide.
AUTHOR CONTRIBUTION
Lin Wu, Anna Olverling, Zhen Huang and HongfenChao performed the islet microcirculation experimentsand glucose tolerance monitoring. Lin Wu performed thestatistical calculations, wrote a draft of the the paper, andcontributed to results interpretation and discussion. LeifJansson, Xin Gao and Ake Sjoholm provided expertisein diabetes and islet microcirculation, the rat model,
conceived, designed and co-ordinated the research plan,and the experiments, contributed to discussion and editedthe paper prior to submission.
FUNDING
This study was support by the Swedish ResearchCouncil [grant number 72X-109], the Swedish DiabetesAssociation, the Juvenile Diabetes Research Foundation,the European Foundation for the Study of Diabetes(EFSD) and a Chinese Diabetes Society (CDS) ResearchFellowship. L.W. was supported by an EFSD/CDS/LillyResearch Fellowship.
REFERENCES
1 Sjoholm, A. and Nystrom, T. (2006) Inflammation and theetiology of type 2 diabetes. Diabetes Metab. Res. Rev. 22,4–10
2 Jansson, L. (1994) The regulation of pancreatic islet bloodflow. Diabetes Metab. Rev. 10, 407–416
3 Iwase, M., Sandler, S., Carlsson, P. O., Hellerstrom, C. andJansson, L. (2001) The pancreatic islets in spontaneouslyhypertensive rats: islet blood flow and insulin production.Eur. J. Endocrinol. 144, 169–178
4 Svensson, A. M., Ostenson, C. G., Efendic, S. and Jansson,L. (2007) Effects of glucagon-like peptide-1-(7–36)-amideon pancreatic islet and intestinal blood perfusion in Wistarrats and diabetic GK rats. Clin. Sci. 112, 345–351
5 Amori, R., Lau, J. and Pittas, A. (2007) Efficacy and safetyof incretin therapy in type 2 diabetes. JAMA, J. Am. Med.Assoc. 198, 194–206
6 Kendall, D. M., Riddle, M. C., Rosenstock, J., Zhuang, D.,Kim, D. D., Fineman, M. S. and Baron, A. D. (2005) Effectsof exenatide (exendin-4) on glycemic control over 30 weeksin patients with type 2 diabetes treated with metformin anda sulfonylurea. Diabetes Care 28, 1083–1091
7 Fineman, M. S., Bicsak, T. A., Shen, L. Z., Taylor, K.,Gaines, E., Varns, A., Kim, D. and Baron, A. D. (2003)Effect on glycemic control of exenatide (syntheticexendin-4) additive to existing metformin and/orsulfonylurea treatment in patients with type 2 diabetes.Diabetes Care 26, 2370–2377
8 Garber, A., Henry, R. R., Ratner, R., Hale, P., Chang, C. T.and Bode, B. (2011) Liraglutide, a once-daily humanglucagon-like peptide 1 analogue, provides sustainedimprovements in glycaemic control and weight for 2 yearsas monotherapy compared with glimepiride in patientswith type 2 diabetes. Diabetes Obes. Metab. 13, 348–356
9 Hansen, L., Hartmann, B., Mineo, H. and Holst, J. (2004)Glucagon-like peptide-1 secretion is influenced byperfusate glucose concentration and by a feedbackmechanism involving somatostatin in isolated perfusedporcine ileum. Regul. Pept. 118, 11–18
10 Nystrom, T., Gonon, A. T., Sjoholm, A. and Pernow, J.(2005) Glucagon-like peptide-1 relaxes rat conduit arteriesvia an endothelium-independent mechanism. Regul. Pept.125, 173–177
11 Gardiner, S. M., March, J. E., Kemp, P. A. and Bennett, T.(2006) Mesenteric vasoconstriction and hindquartersvasodilatation accompany the pressor actions of exendin-4in conscious rats. J. Pharmacol. Exp. Ther. 316, 852–859
12 Ozyazgan, S., Kutluata, N., Afsar, S., Ozdas, S. B. andAkkan, A. G. (2005) Effect of glucagon-likepeptide-1(7–36) and exendin-4 on the vascular reactivity instreptozotocin/nicotinamide-induced diabetic rats.Pharmacology 74, 119–126
13 Cotter, M. A., Ekberg, K., Wahren, J. and Cameron, N. E.(2003) Effects of proinsulin C-peptide in experimentaldiabetic neuropathy: vascular actions and modulation bynitric oxide synthase inhibition. Diabetes 52, 1812–1817
C© The Authors Journal compilation C© 2012 Biochemical Society

384 L. Wu and others
14 Johansson, B. L., Wahren, J. and Pernow, J. (2003)C-peptide increases forearm blood flow in patients withtype 1 diabetes via a nitric oxide-dependent mechanism.Am. J. Physiol. Endocrinol. Metab. 285, E864–E870
15 Nordquist, L., Lai, E. Y., Sjoquist, M., Jansson, L. andPersson, A. E. (2008) C-peptide constricts pancreatic isletarterioles in diabetic, but not normoglycaemic mice.Diabetes Metab. Res. Rev. 24, 165–168
16 Jansson, L. (1995) Effects of C-peptide on splanchnicblood flow in anaesthetized rats. Med. Sci. Res. 23,157–158
17 Huang, Z. and Sjoholm, A. (2008) Ethanol acutelystimulates islet blood flow, amplifies insulin secretion, andinduces hypoglycemia via nitric oxide and vagally mediatedmechanisms. Endocrinology 149, 232–236
18 Carlsson, P. O., Olsson, R., Kallskog, O., Bodin, B.,Andersson, A. and Jansson, L. (2002) Glucose-inducedislet blood flow increase in rats: interaction betweennervous and metabolic mediators. Am. J. Physiol.Endocrinol. Metab. 283, E457–E464
19 Burcelin, R., Da Costa, A., Drucker, D. and Thorens, B.(2001) Glucose competence of the hepatoportal vein sensorrequires the presence of an activated glucagon-likepeptide-1 receptor. Diabetes 50, 1720–1728
20 Jansson, L. and Andersson, A. (1997) Nitric oxide andpancreatic islet blood flow after induced portalhypertension in rats. Pancreas 14, 280–284
21 Jansson, L. and Hellerstrom, C. (1983) Stimulation byglucose of the blood flow to the pancreatic islets of the rat.Diabetologia 25, 45–50
22 Jansson, L. and Hellerstrom, C. (1981) A rapid method ofvisualizing the pancreatic islets for studies of islet capillaryblood flow using non-radioactive microspheres. ActaPhysiol. Scand. 113, 371–374
23 Jansson, L. (1988) Glucose stimulation of pancreatic isletblood flow by redistribution of the blood flow within thewhole pancreatic gland. Pancreas 3, 409–412
24 Jansson, L. (1984) The blood flow to the pancreas and theislets of Langerhans during an intraperitoneal glucose loadin the rat. Diabetes Res. 1, 111–114
25 Golpon, H., Puechner, A., Welter, T., Wichert, P. andFeddersen, C. (2001) Vasorelaxant effect of glucagon-likepeptide (7–36) amide and amylin on the pulmonarycirculation of the rat. Regul. Pept. 102, 81–86
26 Baggio, L. L. and Drucker, D. J. (2007) Biology of Incre-tins: GLP-1 and GIP. Gastroenterology 132, 2131–2157
27 Nathanson, D., Erdogdu, O., Pernow, J., Zhang, Q. andNystrom, T. (2009) Endothelial dysfunction induced bytriglycerides is not restored by exenatide in rat conduitarteries ex vivo. Regul. Pept. 157, 8–13
28 Ban, K., Noyan-Ashraf, M. H., Hoefer, J., Bolz, S. S.,Drucker, D. J. and Husain, M. (2008) Cardioprotective andvasodilatory actions of glucagon-like peptide 1 receptor aremediated through both glucagon-like peptide 1receptor-dependent and -independent pathways.Circulation 117, 2340–2350
29 Sonne, D. P., Engstrom, T. and Treiman, M. (2008)Protective effects of GLP-1 analogues exendin-4 andGLP-1(9–36) amide against ischemia-reperfusion injury inrat heart. Regul. Pept. 146, 243–249
30 Hansen, A., Johansson, B. L., Wahren, J. and Von Bibra, H.(2002) C-peptide exerts beneficial effects on myocardialblood flow and function in patients with type 1 diabetes.Diabetes 51, 3077–3082
31 Wallerath, T., Kunt, T., Forst, T., Closs, E. I., Lehmann, R.,Flohr, T., Gabriel, M., Schafer, D., Gopfert, A., Pfutzner,A. et al. (2003) Stimulation of endothelial nitric oxidesynthase by proinsulin C-peptide. Nitric Oxide 9, 95–102
32 Svensson, A. M., Ostenson, C. G., Sandler, S., Efendic, S.and Jansson, L. (1994) Inhibition of nitric oxide synthaseby NG-nitro-L-arginine causes a preferential decrease inpancreatic islet blood flow in normal rats andspontaneously diabetic GK rats. Endocrinology 135,849–853
Received 14 September 2009/24 October 2011; accepted 7 November 2011Published as Immediate Publication 7 November 2011, doi:10.1042/CS20090464
C© The Authors Journal compilation C© 2012 Biochemical Society





























