Embed Size (px)
Citation preview
Copyright @ 200 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.8
Clinical Case Studies
Heatstroke during Endurance Exercise: IsThere Evidence for Excessive Endothermy?
DALE E. RAE1, GIDEON J. KNOBEL2, THERESA MANN1, JEROEN SWART1, ROSS TUCKER1,and TIMOTHY D. NOAKES1
1UCT/MRC Research Unit for Exercise Science and Sports Medicine, Department of Human Biology, and 2Division ofForensic Medicine and Toxicology, Faculty of Health Sciences, University of Cape Town, SOUTH AFRICA
ABSTRACT
RAE, D. E., G. J. KNOBEL, T. MANN, J. SWART, R. TUCKER, and T. D. NOAKES. Heatstroke during Endurance Exercise: Is
There Evidence for Excessive Endothermy? Med. Sci. Sports Exerc., Vol. 40, No. 7, pp. 1193–1204, 2008. Purpose: Five of 28,753
cyclists participating in an annual 109-km bicycle race died, four within 24 h of the race and the fifth 17 d later. All five deaths were
reported to be the consequence of exertional heatstroke. One runner of 6874 participating in an annual 56-km ultramarathon developed
heatstroke and required active cooling for 10 h to achieve normothermia. The purpose of this article was to postulate (i) why only 6 of
35,627 athletes were hospitalized for heatstroke in these races, (ii) if exercise alone could have elevated their body temperatures
sufficiently to cause heatstroke, and (iii) why the runner required such prolonged cooling. Methods: Clinical and autopsy data are
presented for three of the cyclists and the runner for whom access to this information was granted. Calculations were made to predict the
work rates necessary to produce their measured rectal temperatures. Results: The rectal temperatures of two of the cyclists were 42.0
and 41.2-C on hospitalization, and that of the runner was 41.8-C on collapse. Standard calculations showed that in the prevailing
environmental conditions and with their exercise speeds, none should have developed exertional heatstroke. The third cyclist
experienced a cardiac arrest to which his elevated (rectal) temperature may have contributed. Conclusion: The hyperthermic states
experienced by the cases presented may have resulted from failure of their heat-losing mechanisms. Alternatively, they might have
resulted from excessive endothermy, triggered by physical exertion and other unknown initiating factors. Excessive endothermy should
be considered in cases of heatstroke that occur in mild to moderate environmental conditions. Furthermore, prompt initiation of
cooling is crucial in all cases of suspected heatstroke. Key Words: SUDDEN DEATH, HYPERTHERMIA, CARDIAC ARREST,
IMMEDIATE COOLING, ENDOGENOUS HEAT PRODUCTION, MALIGNANT HYPERTHERMIA
Sudden death during exercise is an unusual phenom-enon in young- to middle-aged athletes. For example,during both the annual Marine Corps (1976 to 1994)
and Twin Cities (1982 to 1994) marathons in the UnitedStates, there have been only 4 deaths of 215,413 runners(28). All these deaths were cardiac deaths without heat-stroke or hyperthermia. In the London marathon, there have
been 8 cardiac deaths and 2 fatal cerebrovascular accidentsin 650,000 completed marathon runs (47).
In view of the apparent rarity of the occurrence, wetherefore report that five deaths occurred during a singleendurance event, the 2002 Argus Cycle TourVan annual109-km bicycle race in Cape Town, South Africa. Unfortu-nately, we were unable to obtain permission to access theinformation of two cyclists whose hospital admission re-cords indicate that they were treated for heatstroke and thatthey died of multiple organ failure typical of this condi-tion. Therefore, our report includes details of only threeof these cases. Family members of these three individualsgave their consent for us to access their medical recordsand clinical data to present their cases. The cyclists were onthe road between 8 h 53 min and 15 h 00 min, during whichtime the average temperature was 28.7-C (range = 21.9–31.4-C), the sky was partly cloudy until 10 h 00 min whereafter it was clear, the relative humidity was approximately62%, and the average wind speed was 3.1 mIsj1. Table 1
CLINICAL SCIENCES
Address for correspondence: Timothy D. Noakes, M.D., UCT/MRCResearch Unit for Exercise Science and Sports Medicine, Departmentof Human Biology, Faculty of Health Sciences, University of Cape Town,PO Box 115, Newlands 7725, South Africa; E-mail: [email protected] for publication December 2006.Accepted for publication January 2008.
0195-9131/08/4007-1193/0MEDICINE & SCIENCE IN SPORTS & EXERCISE!
Copyright " 2008 by the American College of Sports Medicine
DOI: 10.1249/MSS.0b013e31816a7155
1193
Copyright @ 200 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.8
shows the hourly weather conditions during the race foreach of the three cyclists clearly indicating that when theathletes collapsed during the latter part of the race, theambient temperatures were at the highest. These weatherconditions, although hot, were not extreme in comparison toprevious and subsequent Argus Cycle Tour races (Table 2).One cyclist collapsed during and another immediately afterthe race, both without evidence for an obvious predisposingcause, and both died within 24 h. The third cyclist experi-enced a cardiac arrest during the ride and died of septicemia17 d later. On the basis of clinical and autopsy evidence, allthree deaths were reported to be the consequence ofexertional heatstroke. We also report a further case ofheatstroke in a competitor in a 56-km footrace, the 2006Two Oceans Marathon. Consent was obtained from therunner to access his medical records and clinical data topresent his case. The runner began his race at 7 h 00 min andcompleted it shortly before 14 h 00 min, at an averagerunning speed of 8.2 kmIhj1. During this period, the averageambient temperature was 18.1-C (range = 7.0–25.0-C),the sky was clear, the relative humidity was 61.4%, and theaverage wind speed was 1.9 mIsj1 (Table 3). The runnercollapsed at the end of the race at which time the environ-mental temperature was 24.3-C and relative humidity was36%. His rectal temperature was 41.8-C, and he requiredalmost 10 h of external cooling to normalize his bodytemperature. In contrast to the cyclists, the runner survived.We report these four cases to pose and partially to answerfour questions: (i) Why did only 5 of 28,753 cyclists and 1 of6874 runners in their respective races develop heatstroke? (ii)What is the probability that exercise alone could haveelevated the body temperatures of only six athletes to levelscausing exertional heatstroke? (iii) Why did the surviving
athlete require 10 h of cooling before his body temperaturenormalized? and (iv) Why did the athletes develop thiscondition only in these races and not during other bouts ofequivalent exercise?
CASE 1
An active 34-yr-old man (1.8 m, 85 kg, BMI of 26) whohad no known medical conditions took part in his fourthArgus Cycle Tour. Although he was reportedly not as fit asnormal and slightly overweight, he had completed a21.1-km footrace 1 wk before the Cycle Tour and wasabout to run another such race a week later. For the weekspreceding and on the morning of the race, he used a sup-plement (Dymetadrine Xtreme), of which the primary in-gredients are 300 mg of ephedra and 100 mg of caffeineper capsule. He started the race at 8 h 53 min and collapsedafter approximately 4 h of cycling, having covered an esti-mated 80 km. While being transported to the hospital,paramedics attempted to resuscitate him. He was also intu-bated and manually ventilated but was apparently not ac-tively cooled. Unfortunately, we could not source anyfurther details of the management he received in the 1-hperiod between his collapse and his admission to the hos-pital, and there was no record of his rectal temperature be-fore hospitalization.
On arrival at the hospital at 14 h 00 min, approximately1 h after collapsing, he was unconscious, cyanosed, veryhot (rectal temperature of 42-C), hypotensive (systolicblood pressure of 90 mm Hg), and with a tachycardia(120 bpm). Immediate emergency management includedmanual ventilation, cooling (sheet, ice water, and a fan),and intravenous (IV) fluids. Blood test results on admis-sion to the hospital are presented in Table 4. Blood gasanalysis indicated metabolic acidosis with partial respiratorycompensation. Serum sodium and potassium concentrationswere within the normal ranges. Serum urea and creatinineconcentrations were markedly elevated. Hemoglobin con-centration, hematocrit, red cell, and platelet counts werenormal, but white cell count was elevated. His urine wasreportedly ‘‘dark’’ and positive for protein and blood,suggestive of myoglobinuria. A chest x-ray was normal,as was a cerebral computed tomography (CT) scan. Theinitial diagnosis was coma secondary to hyperthermia. Bythat evening, he had developed generalized seizures. Thefollowing morning, his rectal temperature was normal but
TABLE 1. The environmental conditions for the race period of the three cyclists (cases 1, 2, and 3) during the 2002 Argus Cycle Tour.
Time 8 h 00 min 9 h 00 min 10 h 00 min 11 h 00 min 12 h 00 min 13 h 00 min 14 h 00 min 15 h 00 min
Ambient temperature (-C) 17.8 21.9 25 28.3 31.1 31.7 31.8 31.4Relative humidity (%) 99 79 74 64 57 58 54 52Wind speed (mIsj1) 2.5 2.7 2.6 2.3 2.1 2.6 4.5 5.1Cloud cover Partial Partial Partial Clear Clear Clear Clear Clear
Periods of exerciseCase 1Case 2Case 3
TABLE 2. Environmental conditions for the Argus Cycle Tour races before and after the2002 race.
YearMean
Temperaturea (-C)TemperatureRangea (-C)
Mean RelativeHumidity (%)
Mean Wind Speed(mIsj1)
2006 19.1 15–22 64.1 7.242005 25.0 19–29 46.1 6.032004 24.7 15–31 44.6 3.472003 23.5 19–26 61.0 7.292002 25.9 17–32 69.8 3.432001 19.3 13–22 61.7 3.181999 22.9 17–27 64.2 4.771998 18.9 16–21 73.6 9.851997 21.8 15–26 56.4 4.55
No data were available for the year 2000.aAmbient temperature.
CLINICALSC
IENCES
http://www.acsm-msse.org1194 Official Journal of the American College of Sports Medicine
Copyright @ 200 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.8
he was still unconscious. He was oliguric, despite continuedfluid replacement and inotropic support, and his serumcreatinine concentration continued to rise. A second chestx-ray again showed no abnormalities, but repeat blood testsrevealed, in addition to acute renal failure, signs of liverdamage, myocardial damage, and disseminated intravascu-lar coagulation (DIC). In addition, during the morning afterhis collapse, an ECG showed ST segment depression sug-gesting developing myocardial ischemia. Despite continuedmultisystem support, he developed bradycardia that pro-gressed to asystole. He was pronounced dead at 13h00min,approximately 24 h after his collapse. The final diagnosiswas exertional heatstroke progressing to multisystem fail-ure including encephalopathy, acute circulatory collapse,myocardial failure, respiratory failure, acute renal failure,liver damage, and DIC.
Autopsy revealed that the heart weighted 470 g withnormal coronary arteries. There was widespread subendocar-dial hemorrhage over the left ventricular surface. The lungshad pronounced congestion and mild edema. The brainappeared macroscopically normal. The liver was enlarged,fatty, and markedly congested with signs that individual cellshad undergone apoptosis or necrosis. The adrenal glandswere congested with signs of acute hemorrhage; the kidneysdisplayed acute tubular necrosis, had numerous casts, and
TABLE 3. The environmental conditions for the race period of the runner (case 4) during the 2006 Two Oceans Marathon.
Time 7 h 00 min 8 h 00 min 9 h 00 min 10 h 00 min 11 h 00 min 12 h 00 min 13 h 00 min 14 h 00 min
Ambient temperature (-C) 7.0 10.6 14.6 18.2 20.9 22.9 23.5 24.3Relative humidity (%) 93 97 80 60 50 40 38 36Wind speed (mIsj1) 0.8 1.2 1.3 1.6 1.5 2.0 3.2 3.0
Period of exercise Case 4
TABLE 4. Clinical and hematological data for three cyclists (cases 1–3) and one runner(case 4) admitted to the hospital in an unconscious state after the 2002 Argus CycleTour and the 2006 Two Oceans Marathon, respectively.
Case 1 Case 2 Case 3 Case 4
Rectal temperature (-C) 42.0a 41.2a 39.0 39.4b
Blood pressure (mm Hg) 90c 120/80 100/60 155/80Heart rate (bpm) 120a 170a 120a 108a
B-Glucose (mmolILj1) V 8a 5.3 VB-pH (7.36–7.44) 7.34a 7.41 7.33a 7.42B-PCO2 (4.5–6.1 kPa) 4.1a 3.6a 5.0 3.0a
B-PO2 (11.0–15.0 kPa) 23.2a 45.2a 10.5a 32.5a
B-Std HCO3j (23–27 mmolILj1) 18.3a 20.4a 19.7a 18.5a
B-Actual base excess (j3 to 3 mmolILj1) j8.0a j6.0a j6.0a j10.3a
B-Oxygen saturation (95–99%) 99.0 100.0a 95.0 99.5a
S-Sodium (136–144 mmolILj1) 143 140 146a 145a
S-Potassium (3.5–5.5 mmolILj1) 5.5 5.7a 4.4 4.6S-Urea (2.5–6.7 mmolILj1) 10.5a 8.1a 7.2a 9.5a
S-Creatinine (80–130 KmolILj1) 237a 257a 223a 231a
B-Myoglobin (16–76 ngImLj1) V 630a V VCK-MB mass (0.0–5.0 ngImLj1) V 14.9a V VTroponin T (0.0–0.05 KgILj1) V 0.4a V VHemoglobin (12.5–17.3 gIdLj1) 16.4 16.3 V 18.9a
Hematocrit (0.40–0.50 LILj1) 0.47 0.47 V 0.55a
Red cell count (4.5–5.9 ! 1012 Lj1) V V V 6.2a
White cell count (4.0–11.0 ! 109 Lj1) 12.5a 10.6 V 27.7a
Platelet count (140–420 ! 109 Lj1) 299 211 V 270
The units of each variable are given in parentheses, and where applicable, the normalrange is included.B indicates blood; CK-MB, creatine kinase–myocardial band; pH, percentage hydrogen;PCO2, partial pressure of carbon dioxide; PO2, partial pressure of oxygen; Std HCO3
j ,standard bicarbonate; S, serum.aValues outside the normal ranges.bRectal temperature at the end of the race was 41.8-C. This temperature measured onadmission to the hospital was after 50 min of active cooling in an ice water bath.cSystolic blood pressure.
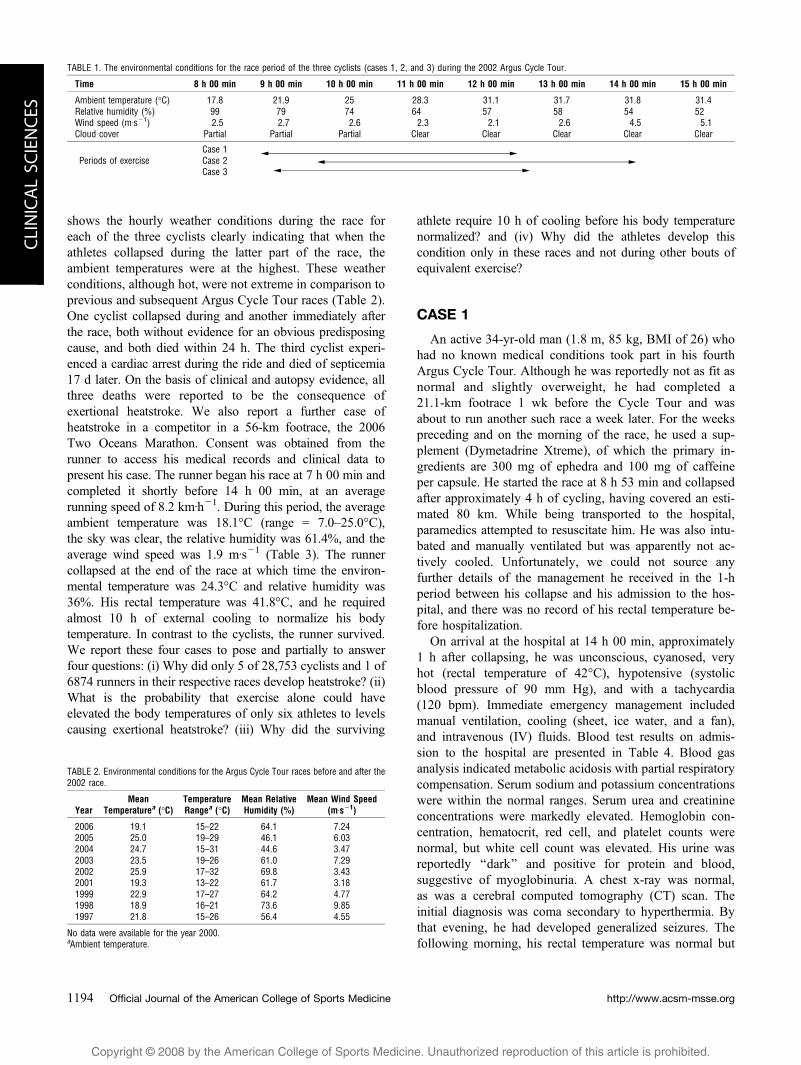
FIGURE 1VCross-sections of the kidneys of case 1 were stained withthe Okajima stain that stains hemoglobin and myoglobin as orange.The kidneys were histologically positive for the presence of tubularnecrosis with (A) multiple orange-brown casts (!100) and (B)myoglobin casts (!100).
EXCESSIVE ENDOTHERMY AS A CAUSE OF HEATSTROKE Medicine & Science in Sports & Exercised 1195
CLIN
ICALSC
IENCES

Copyright @ 200 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.8
stained positive for hemoglobin/myoglobin (Fig. 1). Asample of the vastus lateralis muscle showed widespreadnecrosis of individual fibers and groups of fibers as indi-cated by the swollen and fragmented muscle substance(Fig. 2). Finally, there were diffuse hemorrhages in the lungs,heart, and the submucosa of the trachea. The pathologistconcluded that an exact cause of death could not be deter-mined from autopsy alone, but observed that heatstroke,possibly secondary to exertion, was a likely diagnosis.
CASE 2
This 40-yr-old man, who was a keen recreational cyclistand who had no history of medical problems, participatedin his sixth Argus Cycle Tour. He started the race at 9 h48 min and completed the 109 km in 5 h 1 min 13 s. Shortlyafter finishing the race, he vomited, collapsed, and wasfound to be apneic. He was taken immediately to the
medical facility at the race finish where resuscitationwas attempted. He was given 50 mg of midazolam and50 mg of tramadol hydrochloride, intubated, and placedon 100% oxygen. There is no evidence that he wasactively cooled either at the medical facility at the racefinish or while being transported to the hospital, andthere are no records showing that his rectal temperaturewas measured before admission to the hospital.
On arrival at the hospital at 16 h 50 min, approximately 2 hafter his collapse, he was comatose, his rectal temperaturewas 41.2-C, his blood pressure was 120/80 mm Hg, his heartrate was 170 bpm, and his blood glucose concentration was8 mmolILj1. The attending physician noted that he hadreduced air entry with crepitations on the right side of thechest. Emergency treatment included ventilation, IV fluids,cooling (fan and sponging), and administration of adenosinewith repeated cardioversion, which failed to correct histachyarrhythmia. Blood gas analysis (Table 4) showed anelevated PO2 with respiratory compensation for a mildmetabolic acidosis. Serum sodium concentration was nor-mal, but serum potassium, urea, and creatinine concentra-tions were elevated above the normal ranges indicatingcompromised renal function. Alternatively, raised serumpotassium and creatinine concentrations may indicate heat-related rhabdomyolysis, heatstroke, or dehydration, or allthree. Blood myoglobin and troponin T concentrations andcreatine kinase–myocardial band (CK-MB) activities wereall markedly elevated indicating muscle damage. Hemoglo-bin concentration, hematocrit, red cell, white cell, andplatelet counts were all within the normal ranges. The initialdiagnosis was heatstroke complicated by dehydration, renalfailure, myocardial infarction, refractory supraventriculartachycardia, probable pneumonia, and coma of uncertaincause (possibly hypoxic ischemic encephalopathy). A CTscan was normal, ruling out a cerebral bleed. However, thechest x-ray showed increasing opacity in the right midzone.Aggressive IV fluid therapy was continued to counter theprogressively falling central venous pressure (2 cm H2O).As a result, the patient received a total of 8 L of IV salinefor approximately 9.5 h. Despite this, he remained anuric.By 22 h 00 min, he was bleeding from all access sites andfrom his pharynx, nostrils, and rectum, indicating DIC. Ap-proximately 7 h after his collapse, his rectal temperaturewas normal (38-C). Assisted ventilation became increas-ingly more difficult, requiring high concentrations of oxy-gen and increasing pressure. He developed adult respiratorydistress syndrome, and the persistent hypotension wastreated with an adrenaline infusion. At 2 h 00 min, approx-imately 11 h after his collapse, his core temperature was37-C. He was given plasma and blood transfusions and wasventilated with 100% oxygen. At 2 h 30 min, he developedcardiac arrest from which he could not be resuscitated. Thefinal diagnosis was heatstroke complicated by dehydrationand renal failure, encephalopathy, myocardial infarction,probable aspiration pneumonitis, adult respiratory distresssyndrome, and DIC. No autopsy was performed.
FIGURE 2VLongitudinal sections of the lower limb skeletal muscle ofcase 1 were stained with hemotoxylin and eosin, which stained the cellcytoplasm pink and the nuclei purple. Histological examination showed(A) swollen and severely fragmented fibers (!200) and (B) fiberthickness variation and the presence of necrotic fibers (!100).
http://www.acsm-msse.org1196 Official Journal of the American College of Sports Medicine
CLINICALSC
IENCES

Copyright @ 200 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.8
CASE 3
This case is somewhat different from the first two. A 32-yr-old man (1.75 m, 110 kg, BMI of 36) participated in hisfirst Argus Cycle Tour. He was reportedly active and withoutsignificant medical illness. He began the race at 9 h 1 min andwas discovered apneic and unconscious after 5 h of cycling,apparently having experienced a cardiac arrest perhaps be-cause of hyperthermia. He was resuscitated by paramedics whointubated him and ventilated him manually. When he arrivedat the hospital at 16 h 00 min, he was comatose, with a rectaltemperature of 39.0-C, blood pressure of 100/60 mm Hg, anda heart rate of 120 bpm. Initial treatment included ventilation,but there is no traceable record of whether he receivedelectrical defibrillation at any time after his collapse. Theresults of blood samples taken at that time are presented inTable 4. Twenty-four hours later, blood tests showed that hismyoglobin level was 9700 ngImLj1 (normal range = 16–76ngImLj1), CK-MB activity was 48.6 ngImLj1 (normalrange = 0–5 ngImLj1), and troponin T concentration was0.26 KgILj1 (normal range = 0–0.05 KgILj1), all suggestiveof cardiac injury. Unfortunately, the hospital chose not tomake the ECG traces available. He experienced seizures for2 d, for which he was treated with diphenylhydantoinsodium. A CT scan was normal. He also developed acuterenal failure for which he underwent hemodialysis. Duringthe following week, his condition stabilized, but he requiredventilation. A series of chest x-rays during his hospital-ization were normal. Ten days after hospital admission anelectroencephalogram (EEG) failed to record any sponta-neous brain function. He developed septicemia 2 wk afterhospitalization and was treated appropriately with the anti-biotics metronidazole, vancomycin, and meropenem. ACT scan revealed diffuse cerebral swelling while his stateof oliguric renal failure persisted. His condition deterio-rated progressively until his death, 17 d after the race. Thefinal diagnosis made by the physician treating the patientwas recorded as cardiac arrest during physical exertion,exertional heatstroke, acute renal failure, brain damage(possibly secondary to hyperthermia or hypoxia), and aterminal septicemia.
Autopsy revealed a mildly enlarged heart with nosignificant occlusive coronary artery disease, but there wasmild to moderate atherosclerosis in the large arteries. Therewas also evidence of previous episodes of microinfarction.The pathologist’s summary stated that the patient hadevidence of chronic ischemic heart disease, early bronchop-neumonia, and acute tubular necrosis with hemoglobincylinders. The cause of death was undetermined, but thepathologist considered that the findings were consistentwith heatstroke and its consequences.
CASE 4
This 32-yr-old male runner (1.73 m, 81 kg, BMI of 27) wasparticipating in his third 56-km Two Oceans Marathon. He
began the race at 7 h 00 min, and after almost 7 h of running,he collapsed unconscious approximately 1 km from the finish.He was carried across the finish line by fellow competitors, sothat his race time was recorded as 6 h 52 min 10 s, his slowesttime to date. He was taken immediately to the medical facilityat the race finish. He was pale, cold, diaphoretic, and vomitedintermittently. His mucous membranes were moist, and hisskin turgor was normal to increased. His rectal temperaturewas 41.8-C, his level of consciousness fluctuated [Glasgowcoma scale (GCS): 3–10/15], and he was tachypneic (respira-tory rate in excess of 40 breathsIminj1), with a sinustachycardia (140 bpm) and a systolic blood pressure of 90mm Hg. Oxygen saturation measured by pulse oximetry onroom air was approximately 90%. His serum sodiumconcentration was reduced (131.0 mmolILj1), potassium(4.5 mmolILj1) and chloride (100.1 mmolILj1) concentra-tions were normal, and blood glucose concentration wasincreased (7.5 mmolILj1). It was unusual to observe anindividual presenting with symptoms of both exercise-associated heatstroke and hyponatremia.
The patient was placed in an ice water bath with his torsoand pelvis submerged but the limbs out of the water. The bathcontained 50% water and 50% ice, and although the watertemperature was not measured, it was estimated to bebetween 5 and 10-C. To increase evaporative heat loss, theair movement produced by a large fan was directed at thepatient. He was also given 100% oxygen by polymask(10–15 LIminj1) and IV saline (5%) was infused at a rate of100 mLIhj1 to correct the hyponatremia. After 20 min, hisrectal temperature had decreased to 40.8-C, his GCS scorehad improved to 12/15, his respiratory rate had decreasedto 30 breathsIminj1, whereas his heart rate remainedelevated at 139 bpm. Ice water immersion was continuedfor another 25 min, following which his rectal temperaturewas 40.1-C and his GCS score had improved to 14/15 butwas still fluctuating. Other observations remained un-changed. Mild shivering was noted, and 2 mg of diaz-epam was administered intravenously to attenuate thisresponse. As his temperature had fallen to approximately40-C, it was considered safe to transfer him to the nearesthospital with the torso surrounded by ice packs. A secondbolus of 2-mg diazepam was administered because of con-tinuing shivering.
On admission to the hospital, approximately 2 h after hiscollapse, the patient was transferred to the intensive careunit, where active cooling using ice packs was continuedbecause his rectal temperature was still 39.4-C. Blood in-vestigations performed on admission showed elevatedserum sodium, urea, and creatinine concentrations, but nor-mal potassium concentrations (Table 4). Hemoglobinconcentration, hematocrit, red cell, and white cell countswere all elevated, whereas his platelet count was normal.His urine was of normal appearance but tested positive forblood (4+) and protein (2+) with a specific gravity of 1030.A 12-lead ECG showed a sinus tachycardia without otherabnormalities. A central venous line was inserted for
EXCESSIVE ENDOTHERMY AS A CAUSE OF HEATSTROKE Medicine & Science in Sports & Exercised 1197
CLIN
ICALSC
IENCES
Copyright @ 200 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.8
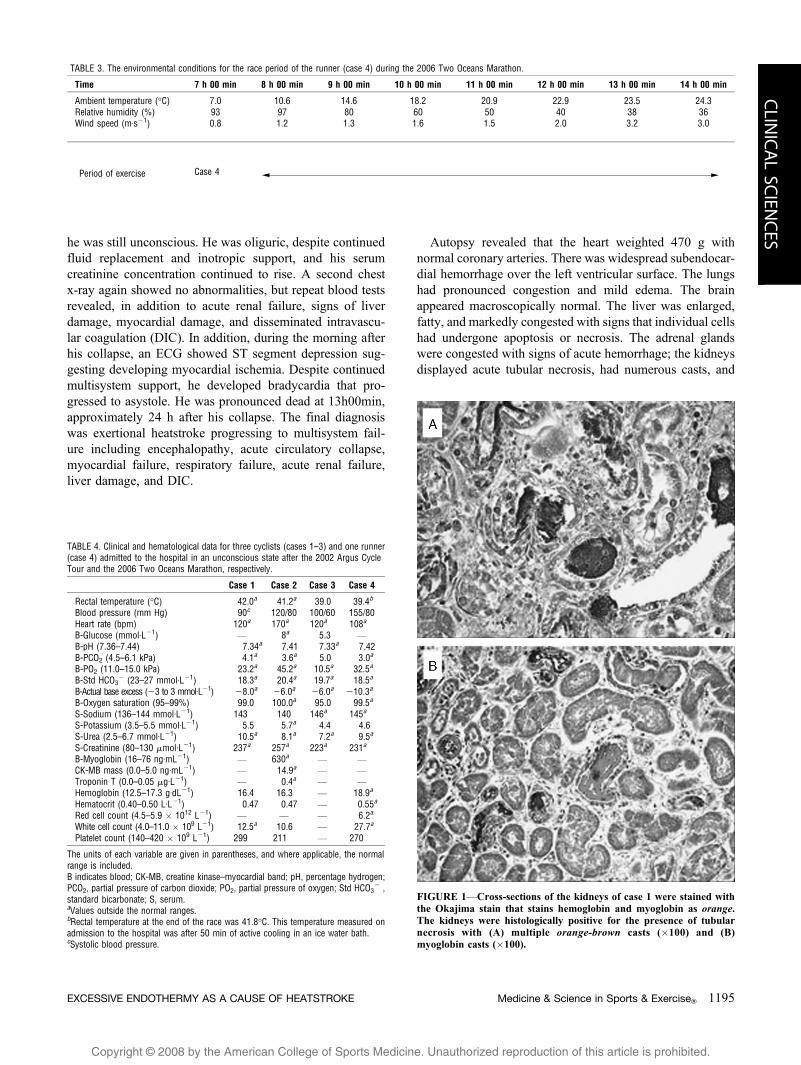
venous access; the infusion of hypertonic saline was dis-continued. Two hours after admission, the patient wassedated and intubated because of combative behavior.Active cooling using ice packs was continued until his rec-tal temperature reached 37.4-C, almost 10 h after he hadstopped running. At this point, cooling was stopped, but hisbody temperature continued to drop to 36.1-C beforestabilizing at 37.0-C approximately 30 h after his collapse.Figure 3 shows his rectal temperature response to con-tinuous active cooling. The remarkable observation is theextreme resistance to cooling of the runner when exposedto ice water for approximately 50 min and to ice packs fora further 9 h. Confirmation that this subject was profoundlyresistant to cooling was provided by the cooling response ofanother runner of similar build, treated identically for hy-perthermia on the same day in the same ice water bath. This87-kg runner completed the race in 4 h 49 min, more than 2 hfaster than case 4, and sought medical care for the treat-ment of malaise and vomiting. Although his rectal temper-ature was 41.1-C, he was fully conscious and, therefore, notexperiencing heatstroke as classically defined. He wasimmersed in an ice bath in an identical manner as case 4.After 15 min, his rectal temperature was 39.8-C; 5 min later,he was removed from the water because he was shivering anduncomfortable. Ten minutes later, without further cooling,his rectal temperature was 38.7-C, and 1 h after he was firstplaced in the ice bath, his temperature was 38.0-C (Fig. 3).
Case 4’s further recovery was uneventful. He was extubatedthe following day, after which he remained fully conscious andwas transferred to a general ward 2 d later where he made arapid recovery. His signs and symptoms continued to improveand he was discharged on the morning of the fourth day at his
own request, at which time he was asymptomatic. Case 4subsequently experienced a period of mildly impaired short-term memory that lasted approximately 2 wk. This hasresolved, and he now reports no residual sequelae.
DISCUSSION
We describe three deaths in cyclists competing in thesame 109-km cycle race in South Africa. We also present acase of a runner who experienced heatstroke during a56-km footrace but made a full recovery. Cases 1 and 2 hadcycled for between 4.5 and 5 h in an average ambienttemperature of 28.7-C and relative humidity of 62%, andboth fulfilled all criteria for a diagnosis of heatstrokebecause they were comatose with core body temperaturesof 42.0 and 41.2-C, respectively. Tragically, the diagnosisseems not to have been entertained at the time of col-lapse, so that neither was initially treated appropriately withimmersion in ice-cold water. Perhaps, as a consequence,both were dead within 24 h of their collapse, despite inten-sive in-hospital medical care. The third cyclist experi-enced a cardiac condition that may have been related to amore normal core temperature of 39-C when first measured2 h after his collapse. The runner (case 4) had run slowly foralmost 7 h in cooler conditions (average ambient temperatureof 18.1-C with a relative humidity of 61.4%) before hecollapsed, also comatose, with a core temperature of 41.8-C.Unlike cases 1 and 2, case 4 survived after receiving im-mediate cooling including a 50-min immersion of his torsoin ice-cold water that lowered his temperature by only 1.7-C.His core temperature, however, only returned to normal aftera further 9 h of continuous cooling. Because the only case tosurvive was also the only case to be cooled appropriately, itseems reasonable to surmise that delayed cooling contributedto the fatal outcomes of at least two and perhaps as many asfive cyclists in a single race.
Heatstroke in Cases 1, 2, and 4
Four intriguing questions arise from these case reports.First, if heatstroke is due principally to the environmentalconditions in which the exercise is undertaken, why do sofew athletes develop the condition even when the con-ditions are hot and humid? In the warmer 2002 Argus CycleTour, only 5 (0.02%) of 28,753 cyclists were hospitalizedfor heatstroke when exposed to the same environmentalconditions. In milder conditions, only 1 (0.02%) of 6526runners in the 2006 Two Oceans Marathon developedheatstroke and another was treated for hyperthermia. Thisparadox has been frequently reported (16,19,38,40,43,50)(Table 5). Second, can exercise alone cause metabolic heatto be produced so rapidly and for so long that bodytemperature rises enough to cause exertional heatstroke anddeath? All the subjects reported here were recreationalathletes who progressed slowly in these races, finishing inthe last 30% of their fields. In contrast, many thousands of
FIGURE 3VCase 4’s change in rectal temperature with 10 h of activeexternal cooling. Convective cooling using an ice water bath and fanwas commenced minutes after his collapse (time point 0) and wascontinued for approximately 50 min. Case 4 was actively cooled usingice packs while being transported to the hospital (time point 1), andthis mode of cooling was continued for a further 8 h from the time ofadmission (time point 2) until his rectal temperature reached 37.4-C(time point 10). The horizontal line represents a normal body tempera-ture of 37.5-C. Also included are data from another hyperthermicrunner who was treated identically and whose rectal temperature fellto 38-C within 60 min.
http://www.acsm-msse.org1198 Official Journal of the American College of Sports Medicine
CLINICALSC
IENCES

Copyright @ 200 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.8
other athletes running or cycling very much faster, andtherefore having higher metabolic races and producingmore heat, were unaffected by this condition. Althoughthe slower participants were exposed to the hotter con-ditions that developed in the latter stages of the races, thefaster athletes were required to lose more heat to offset theirgreater exertional heat production. Third, why do the rectaltemperatures of patients with heatstroke remain elevatedeven after they terminate exercise? If the raised coretemperature observed in athletes experiencing heatstroke isdue solely to excessive rates of heat production by theexercising muscles, spontaneous cooling should occuronce exercise terminates. Yet, the rectal temperatures ofcases 1 and 2 were still profoundly elevated on hospitaladmission 1 to 2 h after they had stopped exercising, as isusual in cases of heatstroke that are not cooled adequately.Case 4 required 10 h of active cooling after his col-lapse before his body temperature reached normal levels.Fourth, all these athletes had exercised regularly withoutever developing heatstroke. Thus, one or more initiatingfactors must have been present during these races to sparkthe development of heatstroke. Next, we attempt to addressthese questions.
The Normal Response of Body Temperature toProlonged Exercise
Already in 1938, Nielsen (34) reported that when exerciseis performed at a constant workload, rectal temperaturerises to a plateau value, which is determined by theworkload, and is largely independent of the environmentalconditions. This increase in rectal temperature is part of the
normal thermoregulatory response to exercise; it is not lifethreatening and, within this thermoregulatory range, maynot affect performance. For example, Pugh et al. (39)reported that the rectal temperatures of 42-km marathonrunners increased to 39.0 T 1.03-C during the race. Racewinners almost always have the highest temperature at theend of the race, sometimes exceeding 41.0-C (8,39,51) andare usually the most dehydrated (13,30). More recently,Byrne et al. (9) have shown that postrace rectal temper-atures in excess of 40.0-C do occur in asymptomatic 21-kmrunners. Therefore, in healthy individuals and in theabsence of compromised thermoregulatory function, itseems that the thermoregulatory centers in the brain allowthe metabolic demands of exercise to elevate the bodytemperature to a new set point that is maintained within anarrow range for the duration of the event, presumably as aresult of the matching of the rates of heat production andheat dissipation (46).
Potential Mechanisms Explaining the Developmentof Heatstroke in Cases 1, 2, and 4
Excessive exertion-related heat production. It isusually assumed that exertional heatstroke occurs whenthere is a mismatch between the elevated rate of heatproduction during exercise and the rate at which that excessheat can be dissipated into the environment (42).Nevertheless, it is retrospectively possible to postulatewhether the abnormally elevated rectal temperatures incases 1, 2, and 4 were due to the normal rates of heatproduction incurred during their respective races. Becausethe environmental conditions during the 2002 Argus Cycle
TABLE 5. The predicted heat balance in cases of heatstroke reported in the literature in a range of environmental conditions.
Environment Race Case Predictions
Case
AmbTemp(-C)
RelHumid(%)
Wind Speed(kmIhj1)
Dist(km)
Time(min)
Speed(kmIhj1)
Mass(kg)
RectalTemp(-C)a
Heat LossCapacity(W)
HeatProduced
(W)
Net HeatGain/Loss
(W)
Ratio ofHeat Gain :
Loss
Total NetHeat Gain/Loss (kJ)
Heat StrokeFeasible? Reference
1 28.7 62 11.2 80.0 240.0 20.0 85 42.0 1627.5 1191.4 j436.1 0.73 j6279.8 No Case 12 28.7 62 11.2 109.0 301.0 21.7 80 41.2 1663.9 1232.5 j431.3 0.74 j7789.9 No Case 23 18.1 61 6.8 56.0 412.0 8.3 81 41.8 1502.2 720.1 j782.1 0.48 j19,334.3 No Case 44 4.1 80b 36.6 19.5 87.8 13.3b 80b 41.0c 2382.5 1365.6 j1016.9 0.57 j5357.0 No (50)5 9.5 62 13.0d 42.1 195.0 13.0 80b 40.7 2275.3 1326.4 j949.0 0.58 j11,102.8 No (40)6 12.0 88 7.4d 12.9 104.6 7.4e 80b 42.0f 1243.2 593.4 j649.8 0.48 j4078.0 No (16)7 16.0 65 20.2 15.0 68.0 13.3b 80b 42.0 2051.4 1365.6 j685.8 0.67 j2797.9 No (43)8 16.0 60 9.5 10.0 46.1 13.0 79 42.5 1893.7 1309.8 j584.0 0.69 j1615.2 No (19)9 16.7 87 7.4d 2.0 15.9 7.4 80b 40.0 1303.8 593.4 j710.4 0.46 j677.7 No (38)10 21.3 73 16.7 11.0 49.6 13.3b 80b 41.6 1706.1 1365.6 j340.5 0.80 j1013.3 No (33)11 22.0 61 20.0 31.8 169.0 11.3 77 41.6 1641.2 1062.5 j578.8 0.65 j5868.5 No (19)12 22.2 80b 13.3d 3.6 16.2 13.3b 80b 40.8 1556.2 1365.6 j190.6 0.88 j185.2 No (41)13 23.0 42 13.3d 21.1 95.2 13.3b 80b 41.6 1876.1 1365.2 j510.9 0.73 j2918.3 No (1)14 24.0 66 10.0 41.6 219.0 11.4 68 42.0e 1252.0 949.4 j302.6 0.76 j3976.4 No (19)15 24.3 49 29.6 10.0 45.0 13.3b 80b 42.0b 1904.2 1365.6 j538.5 0.72 j1454.0 No (25)16 25.0 62 5.0 12.0 55.0 13.1 86 42.0b 1696.3 1439.9 j256.4 0.85 j846.1 No (19)17 30.6 80b 13.3d 10.0 45.0 13.3b 80b 41.1 890.1 1365.6 475.5 1.53 1283.8 Yes (27)
Amb Temp indicates ambient temperature; Rel Humid, relative humidity; Dist, distance; Temp, temperature.a Temperature reported on admission to the hospital.b Relative humidity, race speed, height, mass, and rectal temperature were estimated to be 80%, 13.3 kmIhj1, 1.80 m, 80 kg, and 42.0-C, respectively, for cases in which thisinformation was not reported.c Estimated from a measured oral temperature of 39.5-C.d Wind speed was assumed to be the same as race speed for cases in which this information was not reported.e Pace was set at 12 minImilej1 during a forced march.f Estimated from a measured auxiliary temperature of 40.5-C.
EXCESSIVE ENDOTHERMY AS A CAUSE OF HEATSTROKE Medicine & Science in Sports & Exercised 1199
CLIN
ICALSC
IENCES
Copyright @ 200 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.8
Tour and the 2006 Two Oceans Marathon and the sizes ofthe three athletes are known, it is possible to use standardheat balance equations (35) to determine the amount ofwork each would have had to sustain to increase their corebody temperatures to 42.0, 41.2, and 41.8-C, respectively.On the basis of a modification of these same equations byBrotherhood (7), we were also able to more accuratelyestimate the skin temperature component of these equations.The heat exchange equation is expressed as:
H ¼C T R TE T S ½1$
where H = metabolic heat production, C = convective heatloss/gain, R = radiative heat loss/gain, E = evaporative heatloss/gain, and S = body heat storage. We have previouslyused these equations to calculate the effect of body mass onperformance during exercise in the heat (15).
Each component of the equation is a value in watts (W)and can be calculated as follows:
Hrun ¼ ðð5:89vÞ ' 4:69Þm ½2a$
H cycle ¼ ððð5:89vÞ ' 4:69ÞmÞ=2 ½2b$
C run ¼ 12v0:6ðTsk ' T aÞ0:92Ab ½2b$
Ccycle ¼ 7:6v 0:6ðT sk 'T aÞ0:92Ab ½3a$
R ¼ 5:5ðTsk ' TrÞ0:92Ab ½4$
Erun ¼ 133v0:6ðPsk ' PaÞ0:92Ab ½5a$
Ecycle ¼ 117v 0:6ðPsk ' P1aÞ0:92Ab ½5b$
S ¼ ðm$T b3474Þ=t ½6$
where v = airflow over the skin , exercise speed (mIsj1),m = mass (kg), 12 = convection coefficient for running(WImj2I-Cj1), Tsk = skin temperature (-C), Ta = ambienttemperature (-C), 0.92 = heat loss adjustment for clothing,Ab = body surface area (m2), 7.6 = convection coefficientfor cycling, 5.5 = radiation coefficient (WImj2I-Cj1), Tr =mean radiant temperature (-C), 133 = evaporation coef-ficient for running (WIkPaj1Imj2), Psk = skin water vaporpressure (kPa), Pa = ambient water vapor pressure (kPa),117 = evaporation coefficient for cycling (WIkPaj1Imj2),$Tb = change in mean body temperature (-C) calculatedfrom Tb = 0.87Tre + 0.13Tsk, 3474 = the heat storagecapacity of humans (JIkgj1I-Cj1), and t = duration of ex-ercise (s) (7,35). A clear limitation in the application ofthese equations to this field setting is that they do not ac-count for hills climbed and descended, or pack cycling.These limitations are accepted, because these factors wouldboth increase and decrease the estimated heat productionand heat loss capacities of the cyclists and runner. Yet, itseems unlikely that the inclusion of all these modifyingfactors would substantially alter the calculations.
The maximum capacity for heat loss in our first case(case 1; Table 5) would have been 1628 W during the 2002Argus Cycle Tour and his rate of heat production wasestimated to be 1191 W. Because this rate of heat produc-tion was less than his potential rate of heat loss, thesecalculations suggest that he should not have developedheatstroke during the 4 h in which he cycled in theenvironmental conditions on that day. The same was truefor our second case (case 2; Table 5). His predicted rate ofheat production was 1233 W, which was lower than hispotential to lose heat (1664 W). Similarly, the estimated totalheat production of case 4 (case 3; Table 5) who completedthe 56-km footrace in 6 h 52 min 10 s would have been 720W, substantially less than his maximum capacity for heat lossin the prevailing conditions (1502 W). Thus, these equationsshow that, in theory, the two cyclists and the runner shouldnot have developed exertional heatstroke at the exerciseintensities they sustained and in the environmental conditionsin which they exercised. Therefore, either some other(unrecognized) source of heat production must have beenpresent or else each must have had an unexplained impair-ment in their ability to lose heat at the normal rates.
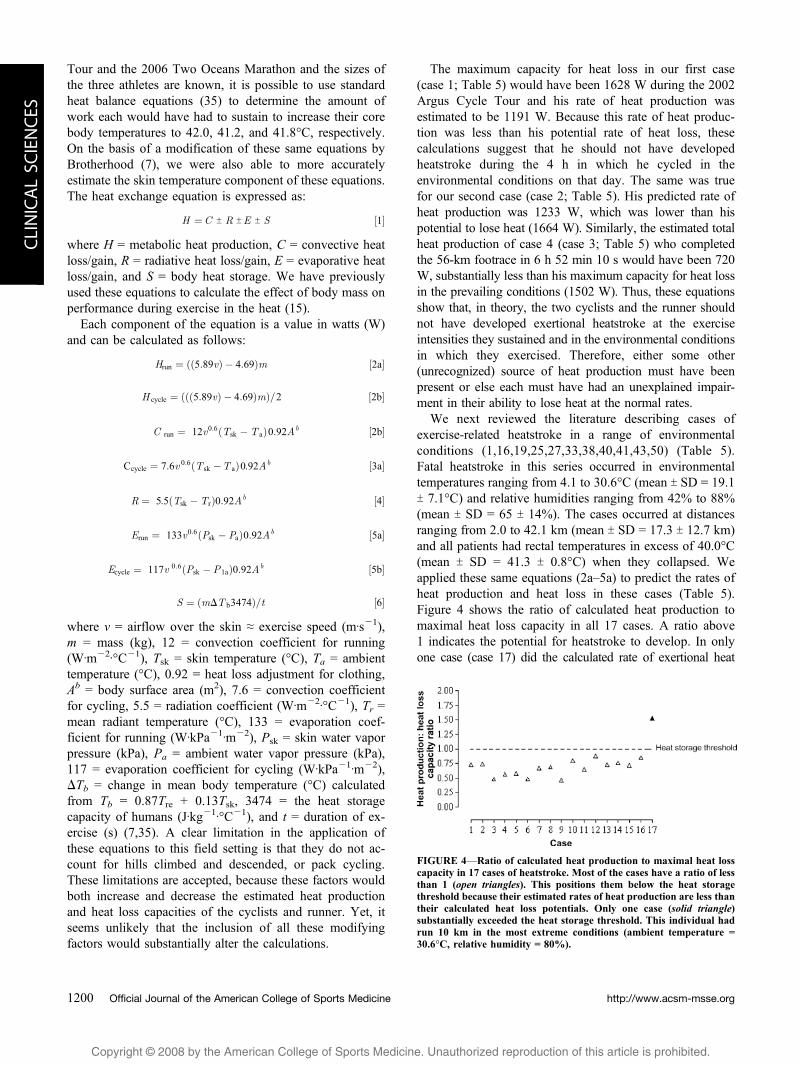
We next reviewed the literature describing cases ofexercise-related heatstroke in a range of environmentalconditions (1,16,19,25,27,33,38,40,41,43,50) (Table 5).Fatal heatstroke in this series occurred in environmentaltemperatures ranging from 4.1 to 30.6-C (mean T SD = 19.1T 7.1-C) and relative humidities ranging from 42% to 88%(mean T SD = 65 T 14%). The cases occurred at distancesranging from 2.0 to 42.1 km (mean T SD = 17.3 T 12.7 km)and all patients had rectal temperatures in excess of 40.0-C(mean T SD = 41.3 T 0.8-C) when they collapsed. Weapplied these same equations (2a–5a) to predict the rates ofheat production and heat loss in these cases (Table 5).Figure 4 shows the ratio of calculated heat production tomaximal heat loss capacity in all 17 cases. A ratio above1 indicates the potential for heatstroke to develop. In onlyone case (case 17) did the calculated rate of exertional heat
FIGURE 4VRatio of calculated heat production to maximal heat losscapacity in 17 cases of heatstroke. Most of the cases have a ratio of lessthan 1 (open triangles). This positions them below the heat storagethreshold because their estimated rates of heat production are less thantheir calculated heat loss potentials. Only one case (solid triangle)substantially exceeded the heat storage threshold. This individual hadrun 10 km in the most extreme conditions (ambient temperature =30.6-C, relative humidity = 80%).
http://www.acsm-msse.org1200 Official Journal of the American College of Sports Medicine
CLINICALSC
IENCES

Copyright @ 200 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.8
production exceed the potential for heat loss. Our calculationssuggest that case 17 would have developed exertional heat-stroke (rectal temperature of 41.5-C) after covering only 8.4km. Interestingly, case 17 exercised in the most severeenvironmental conditions (30.6-C, humidity 80%) of the casesreviewed.We therefore suggest that, of these 17 cases, only onewould have been expected to develop exertional heatstroke onthe basis of the usually described pathogenesis: specificallyhigh rates of heat production sustained in unfavorable environ-mental conditions causing progressive heat accumulation.Rather, these data suggest that an alternative explanation maybe necessary to understand the development of heatstroke insubjects exercising in moderate environmental conditions atrelatively low intensities.
A failure of heat-losing mechanisms. Anotherpossible explanation for the development of heatstroke inthese three cases that we have presented may be an inabil-ity to dissipate adequately their relatively low rates ofheat production through exercise. In warm environmentalconditions, evaporation is the principal mechanism for heatloss in exercising humans as the potential to lose heat viaconvection and radiation becomes negligible when the gra-dients between the skin and the surrounding air are reducedwhile the transfer of heat to the body by radiation increases(35). It is generally assumed that either a very humid envi-ronment or a failure of sweating must impair evaporativeheat loss to that point at which progressive heat gain occurs,leading ultimately to exertional heatstroke. Given that theaverage relative humidity levels during the races were notexcessively high (approximately 60%), it seems that afailure of sweating would have been the more probableexplanation for the development of heatstroke. Indeed, themost common mechanism for heatstroke development inthe British Army in Iraq in 1917 was the sudden failure ofsweating in susceptible soldiers exposed to extreme dry heat(temperatures of 40.6–50.0-C; average relative humidityapproximately 20%) for extended periods of weeks tomonths (20). However, it is not known if this failure canoccur acutely without continuous daily exposure to dry heatfor prolonged periods. Case 4 was sweating profusely onadmission to the medical facility at the race finish, indi-cating that a failure of sweating was an unlikely cause ofheatstroke in his case. Because there is no record of theclinical state of cases 1 and 2 when first treated, we areunable to absolutely exclude this mechanism as a cause ofheatstroke in these two cases.
It is possible to calculate the minimal sweat rates thatwould have been necessary to prevent abnormal heataccumulation and heatstroke in these athletes. The maximalsweat rate capacities for cases 1, 2, and 4 were determinedto be 2150, 2200, and 1514 mLIhj1, respectively. For theintensities at which they exercised, sweat rates of 1690,1747, and 542 mLIhj1, respectively, should have dissipatedsufficient heat to maintain normal rectal temperatures incases 1, 2, and 4, respectively (Fig. 5). Therefore, for thesethree cases, the environmental conditions were not severe
enough to limit the capacity for evaporative heat loss lead-ing to a progressive heat accumulation during exercise.Figure 5 also includes the same data for the other cases ofheatstroke that we studied. Only for case 17 were theenvironmental conditions sufficiently taxing for the max-imal evaporative capacity to be less than the required sweatrate for the individual.
Excessive endogenous heat production. However,if the heat-losing mechanisms of the cyclists and runnerwere not impaired and the environment was not impairingheat loss, so that each was able to sustain these quite normalsweat rates during exercise, then some other factor,secondary to exercise, must have stimulated endogenousheat production to the extent that it overwhelmed thenormal capacity of the heat-losing mechanisms of thesethree athletes. Several possibilities could explain the de-velopment of an explosive endogenous heat production.One possibility is that the athletes experienced a form ofmalignant hyperthermia (2,3,16,17,22,23,26,31,45,49).Although genetic testing was not conducted on these casesto rule out the presence of the mutated R1RY gene (31),none had a family history suggestive of this condition.However, autopsy evidence of muscle necrosis was presentin case 1 (Fig. 2), compatible with the theory that abnormalmuscle metabolism could have contributed to this effect(17,31,49). Alternatively, excessive sympathetic activation(10,22,48), perhaps in the presence of a metabolic myop-athy such as a glycogen storage disease, a fatty acid oxi-dation defect, or a mitochondrial myopathy (44), may havetriggered the development of hyperthermia.
The evidence linking susceptibility to malignant hyper-thermia and exercise-related heatstroke has been reviewed(21,22,31). Included in the most recent reports (22,31) arecases of heatstroke in football players in one of whomgenetic testing revealed the presence of an altered RYR1gene sequence identified as a cause for malignant hyper-thermia. These authors also refer to the paper by Wappler
FIGURE 5VRequired and maximum evaporation rates in 17 cases ofexercise-related heatstroke. The left-hand column of each pair shows therate of evaporation (sweating) required to maintain core body temper-ature at 37.5-C given each cases’ exercise intensity and prevailingenvironmental conditions. The maximum capacity for evaporative heatloss for each case is represented by the right-hand column of each pair.In only one case (asterisk) was the maximal capacity for evaporativeheat loss insufficient to maintain normothermia.
EXCESSIVE ENDOTHERMY AS A CAUSE OF HEATSTROKE Medicine & Science in Sports & Exercised 1201
CLIN
ICALSC
IENCES

Copyright @ 200 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.8
et al. (49), which found that 11 of 12 patients who hadpreviously experienced exercise-induced rhabdomyolysishad positive in vitro contracture test responses indicatingsusceptibility to malignant hyperthermia. Interestingly, only3 of these 12 subjects had an altered RYR1 gene consideredcausative for malignant hyperthermia. Thus, susceptibilityto malignant hyperthermia must be conferred by severaladditional genes other than the RYR1 gene. Hopkins et al.(24) have concluded that although there are clear differ-ences between malignant hyperthermia and exertionalheatstroke and between those who are susceptible to eithercondition, there is yet ‘‘a high incidence of abnormalin vitro contracture test responses in muscles from individ-uals with a history of exertional heatstroke, suggesting thatone or more skeletal muscle abnormalities are responsiblefor a significant proportion of heatstroke cases’’ (p. 100).They further conclude that: ‘‘These studies suggest thatheatstroke victims have an underlying skeletal muscleabnormality that is probably distinct from malignant hyper-thermia but which involves a similar deregulation of controlof myoplasmic calcium ion concentration, which leads toboth the in vitro contracture in response to drugs and theclinical heatstroke syndrome in response to extreme exer-tion’’ (p. 97). More recently, Hopkins and Wappler (22) hasconcluded that ‘‘a minority of episodes of exertional heatillness occur in individuals with an underlying predisposingskeletal muscle defect. Individuals who experience exerciseheat illness, especially repeated episodes, in a temperateclimate and without other predisposing factors are mostlikely to have such a muscle defect’’ (p. 284).
A second possibility is that an exogenous factor such as theingestion of a drug or supplement may have activatedan excessive thermogenic response. Neurololeptics, sympa-thomimetics, and drugs with anticholinergic properties havebeen associated with the development of heatstroke inwarm environmental conditions (29). Case 1’s wife reportedthat her husband was taking a supplement that containedapproximately 0.3 g of ephedra and 0.1 g of caffeine percapsule and had ingested some on the morning of the race.There are case reports of individuals taking ephedra whosubsequently developed heatstroke during exercise (12,37).The family members of case 2 reported that he did not useany drugs or supplements before the race, and case 4 reportedtaking only a carbohydrate gel during his ultramarathon.
A final possibility is the presence of an infection beforethe race. Notably, the runner reported by Roberts (40) hadbeen ill 1 wk before developing heatstroke during a42.1-km marathon he completed in 3 h 15 min. A studyof 58 patients hospitalized with classic heatstroke during aheat wave in Chicago revealed that 33 (57%) had evidencefor a bacterial infection on admission. The authors suggestthat infection may contribute to the development of heat-stroke either by inducing dehydration or by an increasedthermal load (14). Alternatively, infection could activate theimmunologic and coagulative disturbances that are nowbelieved to play an essential role in heatstroke (5).
Clinical evidence for abnormal endogenousthermogenesis. Unpublished data from this laboratoryshow that asymptomatic cyclists participating in the 109-kmArgus Cycle Tour finish the race with an average rectaltemperature of 38.8-C. Spontaneous cooling, presumablybecause of the reduced metabolic heat production on ces-sation of exercise, sees a rapid decrease in the rectal tem-perature of these cyclists by 0.5-C in the first 10 min andnormothermia is usually achieved within 40 to 60 min. Thatall three cases presented here had raised rectal temperaturesfor hours after they stopped exercising strongly suggeststhat abnormal endogenous thermogenesis was continuing.For the sudden removal of the heat source provided bymuscular work should have produced cooling even if therewas some impairment of sweating. However, more con-vincing evidence is provided by case 4 who showed ex-treme resistance to cooling, requiring 10 h of active coolingto reestablish normothermia (Fig. 3). A strong body ofevidence has established that immersion in an ice water bathshould reduce core body temperature by 0.15-CIminj1 (11),although the range may be wider. This predicts that case4 should have become normothermic within 30 min as oc-curred in the comparison subject with hyperthermia whowas treated with the same ice water immersion on the sameday (Fig. 3) and whose rate of cooling was indeed0.12-CIminj1. In reality, case 4’s rate of cooling in thefirst 55 min when he was in the ice water bath was only0.03-CIminj1, that is, 20% of the expected rate. During thesecond and third hours, when his body was surrounded byice packs, his rate of cooling slowed to 0.01-CIminj1. Wesuggest that all these findings strongly suggest that case4 exhibited marked endogenous thermogenesis that lastedfor up to 8 h after he completed the ultramarathon that heran at a very slow pace. In addition, it seems unlikely thathe would have been unable to produce a sweat rate of only126 mLIhj1 that would have maintained his core tempera-ture at 37-C in the mild conditions in which he exercisedand at the slow pace at which he was running.
Recently, Broessner et al. (6) have reported the case of a38-yr-old man who developed postexertional heatstroke,resistant to conventional cooling techniques. For the first20 h after his collapse, his temperature remained between39 and 40-C despite appropriate cooling. Within 7 h ofthe placement of a heat exchange catheter in his superiorvena cava, his temperature stabilized at 37-C where it re-mained for 5 days while active cooling with the IV cathetercontinued. Three attempts to remove the catheter resultedin an immediate increase in the core temperature, whichwas reversed only when IV cooling was restarted. Onlyafter 111.5 h of IV cooling was it possible to remove theheat exchange catheter without an immediate increase incore temperature. Because sweating is not required to main-tain the core temperature at 37-C at rest, this profoundlyabnormal response can only be due to excessive endoge-nous heat production, similar to that which we believe waspresent in our fourth case (Fig. 4).
http://www.acsm-msse.org1202 Official Journal of the American College of Sports Medicine
CLINICALSC
IENCES

Copyright @ 200 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.8
Support for immediate cooling of heatstrokepatients. A crucial difference between cases 1 and 2 andcase 4 was that only in case 4 was the diagnosis of heatstrokemade at the point of collapse with the immediate initiation ofactive cooling. In contrast, there is no evidence that cases1 and 2 were cooled before admission to the hospital, some1 and 2 h after their respective collapses. It seems likely thatthe failure of early and adequate cooling in patients withheatstroke due to high rates of continuous endothermic heatproduction may contribute to a fatal outcome. Indeed, Casaet al. (11) provide good evidence that immediate cooling ofpatients is vital to their recovery. In particular, they showthat cold water (14–20-C) and ice water (1–8-C) immersionis able to reduce rectal temperature by approximately0.15–0.25-CIminj1 (11). It is tempting to speculate that thedelayed cooling of cases 1 and 2 played a significant role intheir subsequent demise. We also suspect that the other twofatal cases of heatstroke in this race may not have beenproperly cooled at the time of collapse, with grave im-plications for the outcome. However, there is also evidencethat early and adequate cooling does not always ensuresurvival, indicating the complexity of this condition (4).
Case 3. Case 3 seems to be somewhat different fromcases 1 and 2, because he may have experienced a cardiacarrest during the race and then lived for a further 17 dbefore dying from septicemia. The autopsy failed to find acause for the cardiac arrest experienced by the cyclistduring the race. However, the fact that he was obese (BMIof 36), cycling his first Argus Cycle Tour, had mild tomoderate atherosclerosis of major coronary vessels, andevidence of previous episodes of microinfarction places himin a higher-risk category during exercise. Therefore, thiscase adds to the pool of anecdotal evidence warning indi-viduals who are overweight and undertrained that they maybe at increased risk of cardiac damage during unaccustomedendurance exercise (32).
Finally, to alter slightly the conclusion of Hopkins andWappler (22), we propose that individuals who developheatstroke ‘‘in a temperate climate and without other pre-disposing factors’’ should be assumed to have a muscledefect causing excessive endothermy, mandating early, ag-gressive, and sustained cooling (11,40), especially in thosewhose temperatures remain elevated despite apparentlyreasonable attempts at cooling (case 4; Fig. 3) (6). Hopkinsand Wappler (22) further proposes that patients withheatstroke who are resistant to cooling or who show overthyperkalemia or muscle rigidity should be treated withdantrolene at a dose of 2.5–3.0 mgIkgj1. The evidence thatthis treatment may enhance survival in patients with heat-stroke due to acute Ecstasy (4,5-methylenedioxymetham-phetamine) toxicity has been presented (18).
SUMMARY
We describe three cases of exercise-induced heatstrokeand one of cardiac arrest, to which hyperthermia may havecontributed. Although the prevailing environmental con-ditions experienced by the cyclists (cases 1, 2, and 3) werewarm, calculations suggest that these athletes were notexercising either with sufficient vigor or for sufficientlylong period to explain their development of heatstroke.Similarly, the runner (case 4) ran slowly in mild conditions andshould not have experienced progressive heat accumula-tion leading to heatstroke because his calculated rate of heat pro-duction was 48% of the maximal capacity for heat loss inthe prevailing environmental conditions. Furthermore, a cal-culated sweat rate of only 542 mLIhj1 should have maintainedhis core temperature at 37.5-C (Fig. 5). We propose either thatthe heat-losing mechanisms in these athletes were inadequateor that, and perhaps more likely we think, excessiveendogenous thermogenesis, initiated by unknown factors,may have produced the heatstroke (22,36). We speculate thatexcessive endogenous thermogenesis was present in case 4,because this would explain why his cooling rate whenimmersed in an ice water bath was only 20% of the ratemeasured in other subjects with hyperthermia or heatstroke. Inonly 1 of 14 other cases of heatstroke described in the literature(Table 5) could an imbalance between the calculated normalrate of heat production and expected potential rate of heatloss explain the development of heatstroke. The applicationof these equations to other similar cases in which heatstrokeoccurred (i) in only a few of many competitors, (ii) whenthe exercise intensity is modest, and (iii) when the environ-mental conditions are not extreme may identify other casesin which excessive endogenous thermogenesis may occurin patients diagnosed with exercise-induced heatstroke. Thismay allow the identification of currently unknown causesof such excessive thermogenesis and improve the understand-ing of this complex condition (4,5). Of great practicalimportance was our observation that the failure to recognizeheatstroke at the time of collapse in the cyclists with theimmediate initiation of cooling probably contributed to thefatal outcomes.
This researchwas funded by theHarry Crossley andNeily AtkinsonStaff Research Funds of the University of Cape Town, the MedicalResearch Council of South Africa and Discovery Health. The authorsacknowledge the assistance of Dr Basil Bonner, the medical officer ofthe 2002 Argus Cycle Tour, in allowing access to the medicalinformation pertaining to that race, and Ray Kriel of the Division ofAnatomical Pathology, Faculty of Health Sciences, University of CapeTown, who assisted in the production of the photomicrographs fromthe autopsy of case 1. Finally, the authors acknowledge Ms. MichellePerrins, Chief Medical Technologist, Division of Forensic Medicine,Faculty of Health Sciences, University of Cape Town, for cutting,preparing, and staining sections for microscopic examination.
REFERENCES
1. Aarseth HP, Eide I, Skeie B, Thaulow E. Heat stroke in enduranceexercise. Acta Med Scand. 1986;220(3):279–83.
2. Bartley JD. Heat stroke: is total prevention possible. Mil Med.1977;142(7):528, 533–35.
EXCESSIVE ENDOTHERMY AS A CAUSE OF HEATSTROKE Medicine & Science in Sports & Exercised 1203
CLIN
ICALSC
IENCES
Copyright @ 200 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.8
3. Bendahan D, Kozak-Ribbens G, Confort-Gouny S, et al. Anoninvasive investigation of muscle energetics supports similar-ities between exertional heat stroke and malignant hyperthermia.Anesth Analg. 2001;93(3):683–9.
4. Bouchama A, Knochel JP. Heat stroke. N Engl J Med. 2002;346(25):1978–88.
5. Bouchama A, Roberts G, Al Mohanna F, et al. Inflammatory,hemostatic, and clinical changes in a baboon experimental modelfor heatstroke. J Appl Physiol. 2005;98(2):697–705.
6. Broessner G, Beer R, Franz G, et al. Case report: severe heatstroke with multiple organ dysfunctionVa novel intravasculartreatment approach. Crit Care. 2005;9(5):R498–501.
7. Brotherhood JR. Heat stress and strain in exercise and sport. J SciMed Sport. 2008;11(1):6–19.
8. Buskirk ER, Beetham WPJ. Dehydration and body temperature asa result of marathon running. Med Sports. 1960;XIV(9):493–506.
9. Byrne C, Lee JK, Chew SA, Lim CL, Tan EY. Continuous ther-moregulatory responses to massVparticipation distance runningin heat. Med Sci Sports Exer. 2006;38(5):803–10.
10. Campbell IT, Ellis FR, Evans RT, Mortimer MG. Studies of bodytemperatures, blood lactate, cortisol and free fatty acid levelsduring exercise in human subjects susceptible to malignant hyper-pyrexia. Acta Anaesthesiol Scand. 1983;27(5):349–55.
11. Casa DJ, Armstrong LE, Ganio MS, Yeargin SW. Exertional heatstroke in competitive athletes. Curr Sports Med Rep. 2005;4(6):309–17.
12. Charatan F. Ephedra supplement may have contributed to sports-man’s death. BMJ. 2003;326(7387):464.
13. Cheuvront SN, Carter R III, Sawka MN. Fluid balance and endur-ance exercise performance. Curr Sports Med Rep. 2003;2(4):202–8.
14. Dematte JE, O’Mara K, Buescher J, et al. Near-fatal heat strokeduring the 1995 heat wave in Chicago. Ann Intern Med. 1998;129(3):173–81.
15. Dennis SC, Noakes TD. Advantages of a smaller bodymass inhumans when distance-running in warm, humid conditions. Eur JAppl Physiol Occup Physiol. 1999;79(3):280–4.
16. Dickinson JG. Heat-exercise hyperpyrexia. J R Army Med Corps.1989;135(1):27–9.
17. Hackl W, Winkler M, Mauritz W, Sporn P, Steinbereithner K.Muscle biopsy for diagnosis of malignant hyperthermia suscept-ibility in two patients with severe exercise-induced myolysis. Br JAnaesth. 1991;66(1):138–40.
18. Hall AP, Henry JA. Acute toxic effects of FEcstasy_ (MDMA) andrelated compounds: overview of pathophysiology and clinicalmanagement. Br J Anaesth. 2006;96(6):678–85.
19. Hanson PG, Zimmerman SW. Exertional heatstroke in novicerunners. JAMA. 1979;242(2):154–7.
20. Hearne KG. Hyperpyrexial heatstroke: a Mesopotamian experi-ence, with some aetiological views and a method of preventionresulting therefrom. Med J Aust. 1932;1:226–32.
21. Hopkins PM, Ellis FR. Hyperthermic and HypermetabolicDisorders: Exertional Heat-Stroke, Malignant Hyperthermia andRelated Syndromes. London (England): Cambridge UniversityPress; 1996. p. 1.
22. Hopkins PM, Wappler F. Is there a link between malignanthyperthermia and exertional heat illness? Br J Sports Med.2007;41(5):283–4.
23. Hopkins PM, Ellis FR, Halsall PJ. Evidence for related myopa-thies in exertional heat stroke and malignant hyperthermia.Lancet. 1991;338(8781):1491–2.
24. Hopkins PM, Halsall PJ, Ellis FR. Investigation of exertional heatstroke 3: in vitro skeletal muscle contracture testing. In: HopkinsPM, Ellis FR, editors. Hyperthermic and Hypermetabolic Disorders:Exertional Heat-Stroke, Malignant Hyperthermia and Related Syn-dromes. New York: Cambridge University Press; 1996. p. 93–101.
25. Hughson RL, Sutton JR. Heat stroke in a ‘‘run for fun.’’ Br Med J.1978;2(6145):1158.
26. Jardon OM. Physiologic stress, heat stroke, malignant hyper-thermiaVa perspective. Mil Med. 1982;147(1):8–14.
27. Knochel JP. Catastrophic medical events with exhaustive exercise:‘‘white collar rhabdomyolysis.’’ Kidney Int. 1990;38(4):709–19.
28. Maron BJ, Poliac LC, Roberts WO. Risk for sudden cardiac deathassociated with marathon running. J Am Coll Cardiol. 1996;28(2):428–31.
29. Martinez M, Devenport L, Saussy J, Martinez J. Drug-associatedheat stroke. South Med J. 2002;95(8):799–802.
30. Muir AL, Percy-Robb IW, Davidson IA, Walsh EG, Passmore R.Physiological aspects of the Edinburgh Commonwealth Games.Lancet. 1970;2(7683):1125–8.
31. Muldoon S, Deuster P, Brandom B, Bunger R. Is there a linkbetween malignant hyperthermia and exertional heat illness?Exerc Sport Sci Rev. 2004;32(4):174–9.
32. Neilan TG, Januzzi JL, Lee-Lewandrowski E, et al. Myocardialinjury and ventricular dysfunction related to training levels amongnonelite participants in the Boston marathon. Circulation. 2006;114(22):2325–33.
33. Nicholson MR, Somerville KW. Heat stroke in a ‘‘run for fun.’’ BrMed J. 1978;1(6126):1525–6.
34. Nielsen B. The regulation of core temperature by muscular work.Skand Arch Physiol. 1938;79:195–230.
35. Nielsen B. Olympics in Atlanta: a fight against physics. Med SciSports Exerc. 1996;28(6):665–8.
36. Noakes TD. Mind over matter: deducing heatstroke pathology.Phys Sportsmed. 2005;33(10):44–6.
37. Oh RC, Henning JS. Exertional heatstroke in an infantry soldiertaking ephedra-containing dietary supplements. Mil Med. 2003;168(6):429–30.
38. Parnell CJ, Restall J. Heat-stroke: a fatal case. Arch Emerg Med.1986;3(2):111–4.
39. Pugh LG, Corbett JL, Johnson RH. Rectal temperatures, weightlosses, and sweat rates in marathon running. J Appl Physiol. 1967;23(3):347–52.
40. Roberts WO. Exertional heat stroke during a cool weather mara-thon: a case study. Med Sci Sports Exerc. 2006;38(7):1197–203.
41. Rubel LR. Case for diagnosis: exertional heatstroke. Mil Med.1983;148(9):756, 758.
42. Shapiro Y, Seidman DS. Field and clinical observations of exer-tional heat stroke patients. Med Sci Sports Exerc. 1990;22(1):6–14.
43. Sutton J, Coleman MJ, Millar AP, Lazarus L, Russo P. Themedical problems of mass participation in athletic competition.The ‘‘City-to-Surf’’ race. Med J Aust. 1972;2(3):127–33.
44. Tarnopolsky MA. Metabolic myopathies of physical activity. PhysSportsmed. 2002;30(6):37–46.
45. Tobin JR, Jason DR, Challa VR, Nelson TE, Sambuughin N.Malignant hyperthermia and apparent heat stroke. JAMA. 2001;286(2):168–9.
46. Tucker R, Marle T, Lambert EV, Noakes TD. The rate of heatstorage mediates an anticipatory reduction in exercise intensityduring cycling at a fixed rating of perceived exertion. J Physiol.2006;574(Pt 3):905–15.
47. Tunstall Pedoe DS. Marathon cardiac deaths: the London experi-ence. Sports Med. 2007;37(4–5):448–50.
48. Vanuxem P, Vanuxem D, Raharison L, Aubert M, Pouliquen G,Deslangles O. Maximal exercise and muscle energy metabolismafter recovery from exercise hyperthermia syndrome. MuscleNerve. 2001;24(8):1071–7.
49. Wappler F, Fiege M, Steinfath M, et al. Evidence for suscepti-bility to malignant hyperthermia in patients with exercise-inducedrhabdomyolysis. Anesthesiology. 2001;94(1): 95–100.
50. Weaving EA, Berro VE, Kew MC. Heat stroke during a Frun forfun_: a case report. S Afr Med J. 1980;57(18):753–4.
51. Wyndham CH, Strydom NB. The danger of an inadequatewater intake during marathon running. S Afr Med J. 1969;43(29):893–6.
http://www.acsm-msse.org1204 Official Journal of the American College of Sports Medicine
CLINICALSC
IENCES





























