Embed Size (px)
Citation preview
High Flow Nasal
Cannulae Therapy in
Infants with Bronchiolitis
Dr. Michele Pennica
Terapia Intensiva Pediatrica
AOU Meyer
BRONCHIOLITIS - EPIDEMIOLOGY
Common in young children
Most common between December and March
Usually affects young children (< 1 – 2 yo) with peak of incidence between 2 and 8 months of age
1. 90% children 0-2y experience RSV infection
2. 20% have lower respiratory infection
3. 3% require hospitalization
4. 20% cause hospitalization in infancy
5. 0.002% mortality (2/100,000 children)
BRONCHIOLITIS - ETIOLOGY
Respiratory syncytial virus (RSV) accounts for 50 – 70% of cases
Other etiologies: 1. Parainfluenza 1, 2, and 3
2. Rhinovirus
3. Influenza A and B
4. Adenovirus
5. Rarely, Mycoplasma, Enteroviruses
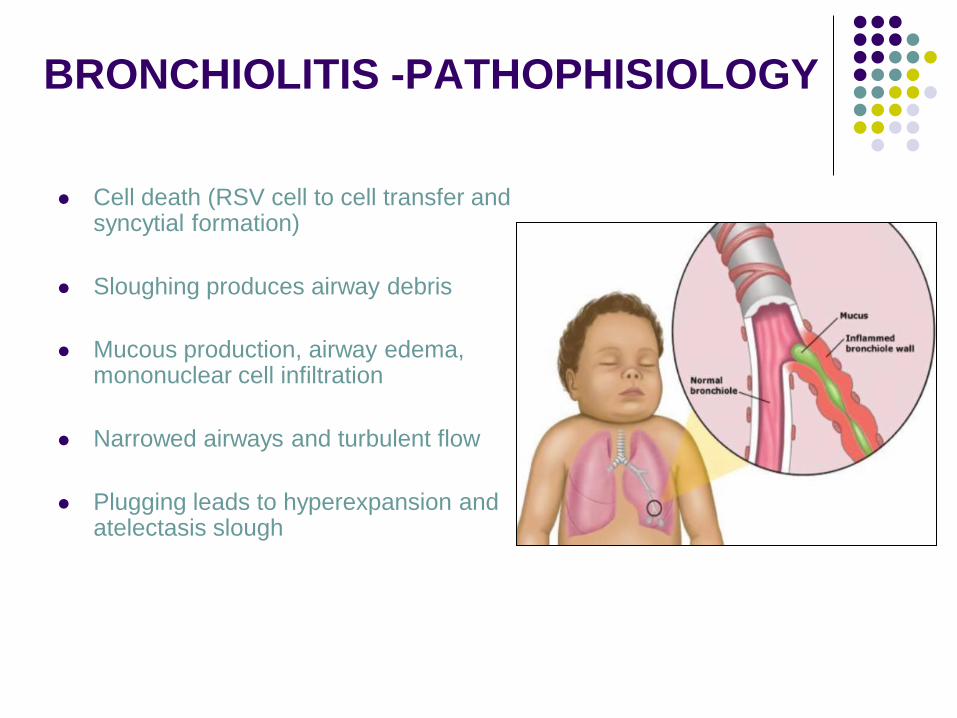
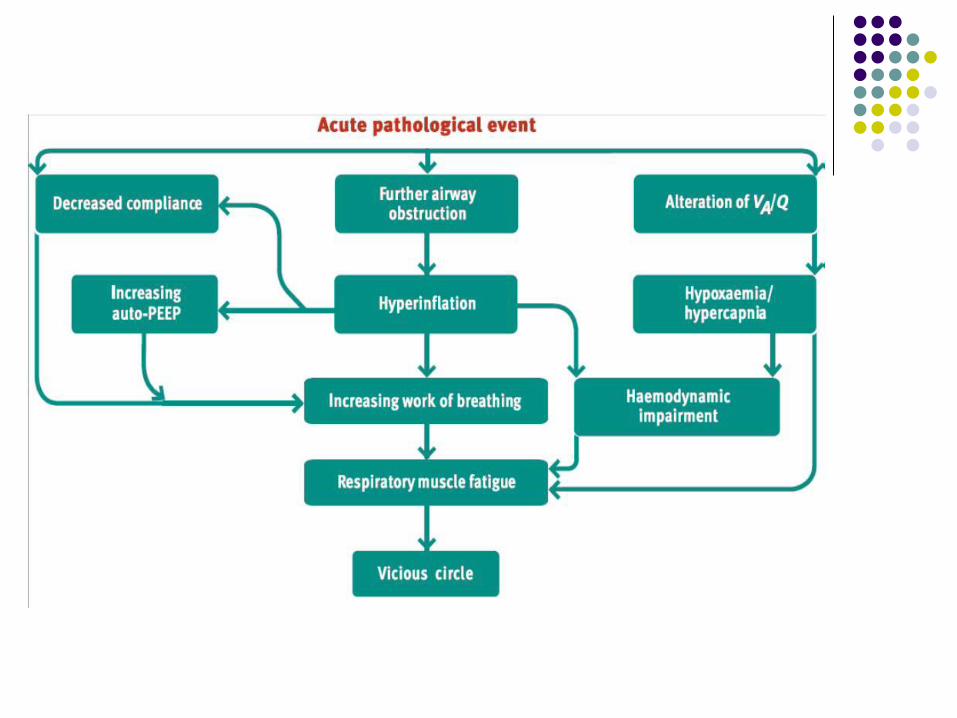
BRONCHIOLITIS -PATHOPHISIOLOGY
Cell death (RSV cell to cell transfer and syncytial formation)
Sloughing produces airway debris
Mucous production, airway edema, mononuclear cell infiltration
Narrowed airways and turbulent flow
Plugging leads to hyperexpansion and atelectasis slough
BRONCHIOLITIS – PRESENTATION
AND DIAGNOSIS
History - URI for 1 – 2 days; fever in 1/3 of patients
- Signs and symptoms of lower airway disease
- Worsens over 2 – 5 days
Physical examination - Apnea in young infants
- URI symptoms
- Tachypnea, cough, wheezes, rales,
retractions
Supplementary tests add little
BRONCHIOLITIS – ANCILLARY TESTS
“Clinicians should diagnose bronchiolitis
and assess disease severity on the basis
of history and physical examination.
Clinicians should not routinely order
laboratory and radiologic studies for
diagnosis.”
AAP Guideline 2006
BRONCHIOLITIS – SEVERE DESEASE
Severe disease more common with background illness
- Cyanotic congenital heart disease
- Bronchopulmonary dysplasia
- Congenital immunodeficiency
- Metabolic and Neurological disease
Predictors of severe disease in - Prematurity
- Age < 12 week
CASE PROGRESSION
Can any treatment prevent
intubation?
BRONCHIOLITIS
AMERICAN ACADEMY of PEDIATRICS
AMERICAN THORACIC SOCIETY
EUROPEAN RESPIRATORY SOCIETY
AMERICAN COLLEGE of CHEST PHYSICIANS
AMERICAN ACADEMY of FAMILIY PHYSICIANS
BRONCHIOLITIS
One of the major problems with
interventional trials in infants and children
with bronchiolitis is the difficulty in
distinguishing bronchiolitis caused by
primary infection from virus induced
wheezing or asthma
BRONCHIOLITIS – SUPPORTIVE
CARE
Evaluate for possible bacterial infection and treat it
Ensure adequate hydration
Nasal suctioning
Antipyretics
Close follow up or monitoring
RECOMMENDATION
Bronchodilators should not be used routinely
in the management of bronchiolitis
A carefully monitored trial of adrenergic
medication is an option.
Inhaled bronchodilators should be continued
only if there is a documented positive clinical
response to the trial using an objective
means of evaluation (AAP 2006, Cochrane Database
Syst Rev 2011)
RECOMMENDATION
Current evidence suggests nebulised 3%
saline may significantly reduce the length of
hospital stay among infants hospitalised with
non-severe acute viral bronchiolitis and
improve the clinical severity score in both
outpatient and inpatient populations (Cochrane Collaboration 2013)
RECOMMENDATION
Corticosteroid medications should not be used
routinely in the management of bronchiolitis (N Engl J Med, 2007) (Cochrane Rev, 2010)
Despite the treatment options
suggested by the literature, oxygen
supplementation remains the mainstay
therapy for bronchiolitis
RECOMMENDATION
Supplemental oxygen is suggested if oxyhemoglobin saturation (SpO2) falls persistently below 90% in previously healthy infants.
If the SpO2 does persistently fall below 90%, adequate supplemental oxygen should be used to maintain SpO2 at or above 90%.
Oxygen may be discontinued if SpO2 is at or above 90% and the infant is feeding well and has minimal respiratory distress
(Ped 2007 )
BRONCHIOLITIS –HELIOX
Insufficient power to determine effect on need for
invasive ventilation (Chest 2006)
In one very small study, heliox – CPAP
combination showed improved clinical
scores and enhanced CO2 clearance; no
intubations (Pediatrics 2008)
BRONCHIOLITIS –CPAP
Continuous positive airway pressure (CPAP) with or without helium-
oxygen blends has gained favor as a way to decrease work of
breathing and prevent endotracheal intubation in children with
progressive hypoxemia or hypercarbia.
However, a systematic review found the evidence regarding CPAP for
bronchiolitis to be inconclusive because of methodologic limitations in
the existing studies.
Additional studies are necessary to clarify the benefits of CPAP for
infants with bronchiolitis who are admitted to an intensive care
(Curr Op Ped 2011, Pulmo 2011, Acta Ped 2010 )
BRONCHIOLITIS –CPAP
Increased CO2 in severe bronchiolitis
Improved CO2 clearance with CPAP
Bronchiolitis - NIV
NIV was safely and effectively used to support infants with
respiratory distress due to severe bronchiolitis. Prospective
randomized controlled trials are now required to delineate the
differing roles of the various modalities and predictive clinical
indicators of which patients can be successfully managed by
NIV. ( Ped Pneumo 2012 )
Oxygen therapy administered via a heated humidified
highflow nasal cannula (HFNC) has recently been
introduced in clinical practice and is gaining
widespread popularity – even outside the intensive
care setting – because it has proved to be a well-
tolerated, non-invasive form of respiratory support High flow nasal cannulae therapy in infants with bronchiolitis. J Pediatr 2010;
Pilot study of vapotherm oxygen delivery in moderately severe bronchiolitis. Arch Dis Child
2012
High Flow Nasal Cannula Therapy
High Flow Nasal Cannula Therapy
A heated, humidified circuit with a blended
oxygen source used to deliver flows that
exceed the patient’s inspiratory flow rate;
this eliminates the entrainment of room air
and purges the nasopharyngeal space of
end expiratory gases.
The goal is to decrease the work of
breathing.
High Flow Nasal Cannula Therapy
Devices are now available which warm and humidify air so flow rates of 2 l/min – 40 l/min can be delivered
Widely used in neonates with RDS
Has also been used in infants, older children and adults in ICU setting
Early studies of its use in children with bronchiolitis have been promising
Use is feasible and secure in pediatric ward
High Flow Nasal Cannula Therapy
HFNC improve the ventilatory status by:
• Prevention of mucous dryness and
improvement of mucous-ciliary clearance,
• reduction of energy expenditure for gas
warming and humidification,
• provision of continuous positive airway
pressure, which contributes to the
maintenance of patent alveoli, improves
the ventilation perfusion mismatch, and
prevents microatelectasis
Pediatr Crit Care Med 2011
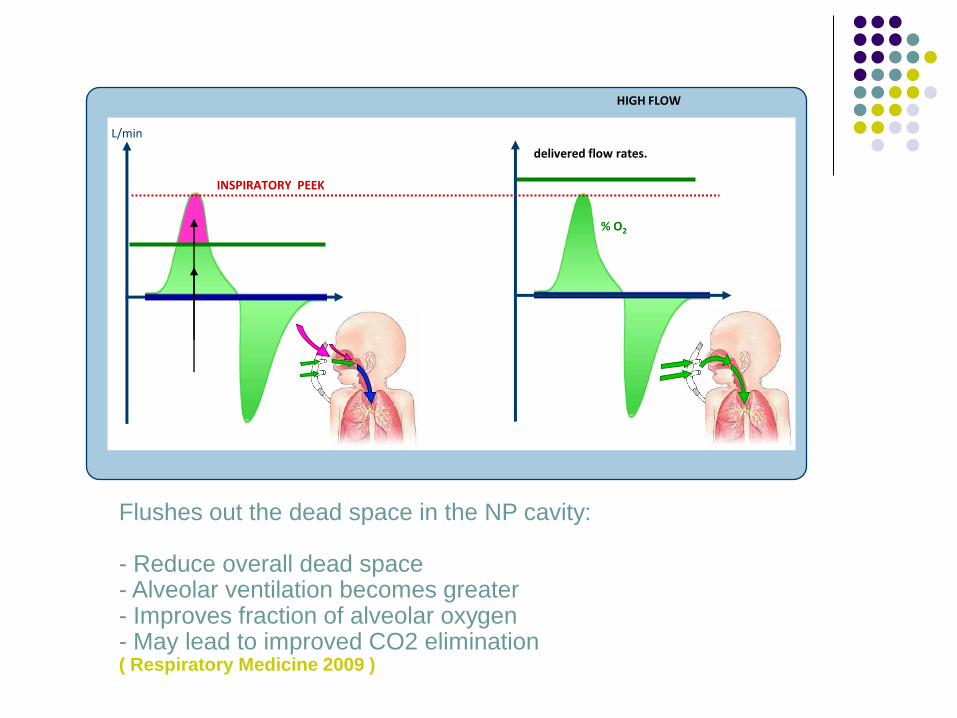
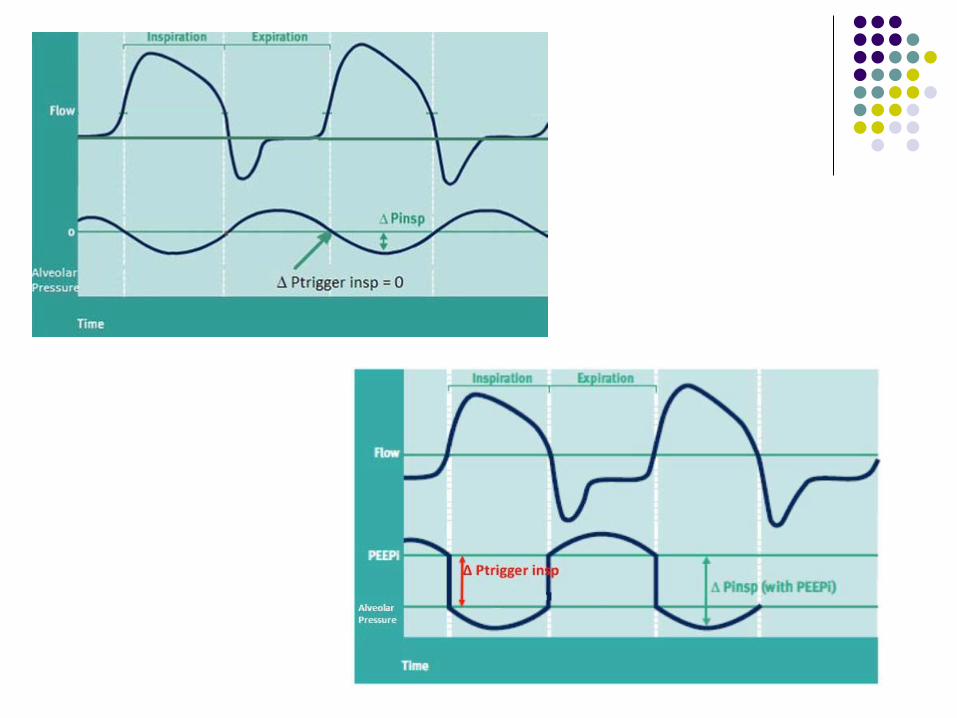
INSPIRATORY PEEK
L/min
% O2
delivered flow rates.
HIGH FLOW
Flushes out the dead space in the NP cavity: - Reduce overall dead space - Alveolar ventilation becomes greater - Improves fraction of alveolar oxygen - May lead to improved CO2 elimination ( Respiratory Medicine 2009 )
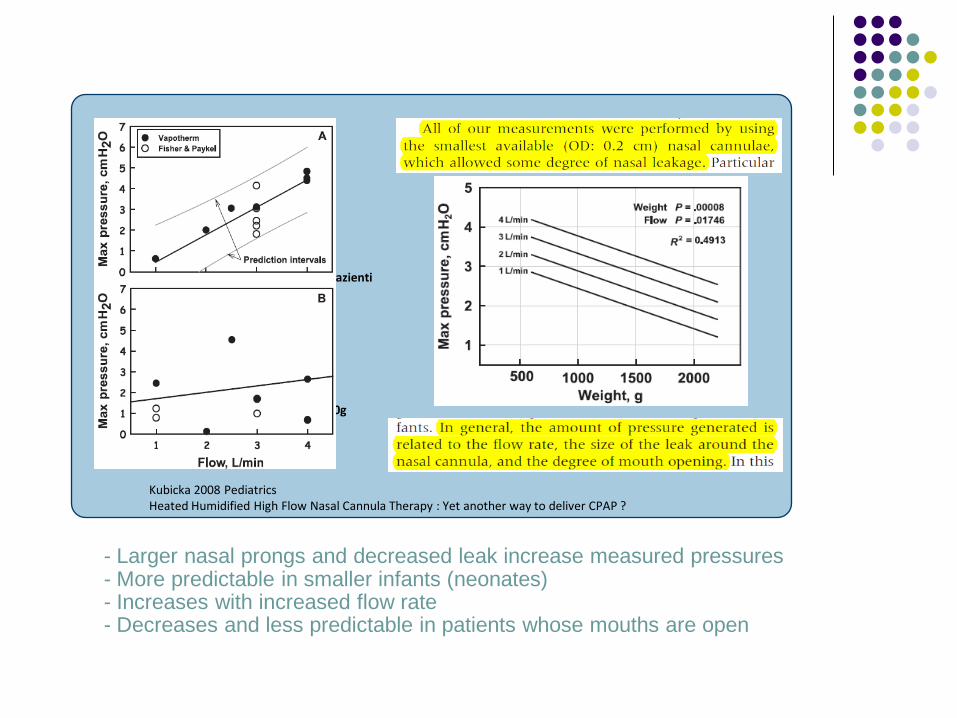
1500g <pazienti <3500g
830g < pazienti < 1500g
Kubicka 2008 Pediatrics Heated Humidified High Flow Nasal Cannula Therapy : Yet another way to deliver CPAP ?
- Larger nasal prongs and decreased leak increase measured pressures - More predictable in smaller infants (neonates) - Increases with increased flow rate - Decreases and less predictable in patients whose mouths are open
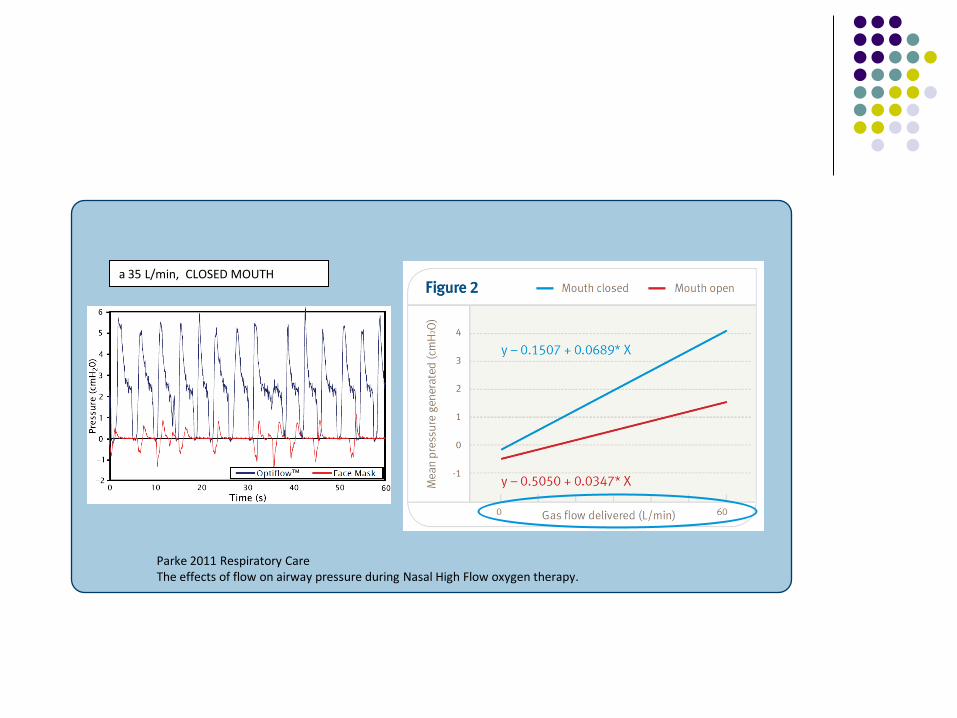
Parke 2011 Respiratory Care The effects of flow on airway pressure during Nasal High Flow oxygen therapy.
a 35 L/min, CLOSED MOUTH
The first studies on the effect of the HFNC in children with bronchiolitis were carried out at intensive care units
(High flow nasal cannulae therapy in infants with bronchiolitis. J Pediatr 2010)
Their retrospective data showed a reduction in the intubation rate and an improvement in the respiratory distress associated with the introduction of HFNC
(Reduced intubation rates for infants after introduction of high-flow nasal prong oxygen delivery. Intensive Care Med 2011)
High Flow Nasal Cannula Therapy
A pilot study conducted by Padova
group showed that the HFNC is a
feasible oxygen delivery method in
infants with moderate–severe
bronchiolitis hospitalized in a
pediatric ward setting, and it is
associated with improvement in
respiratory rate and endtidal carbon
dioxide.
(Effects of high flow nasal cannula oxygen
therapy on infants with bronchiolitis in a pediatric
ward setting. Pneumologia Pediatrica 2012)
High Flow Nasal Cannula Therapy
HFNC seems to be a promising form of respiratory
support even for usage outside the intensive care.
Setting randomized controlled studies are needed
to investigate its safety and effectiveness in order
to reduce hospital stays and transfers to the
intensive care unit, as well as its long-term
benefits and economic impact on the healthcare
system.
High Flow Nasal Cannula Therapy
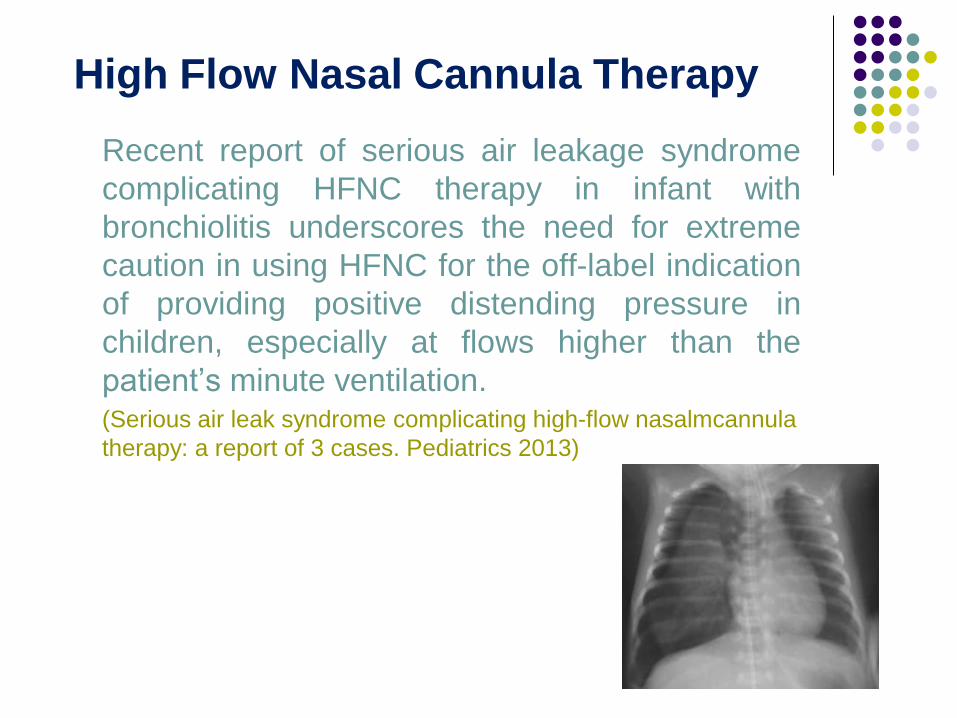
Recent report of serious air leakage syndrome
complicating HFNC therapy in infant with
bronchiolitis underscores the need for extreme
caution in using HFNC for the off-label indication
of providing positive distending pressure in
children, especially at flows higher than the
patient’s minute ventilation. (Serious air leak syndrome complicating high-flow nasalmcannula
therapy: a report of 3 cases. Pediatrics 2013)
High Flow Nasal Cannula Therapy
Highflow nasal cannula use in children with respiratory
distress in the emergency department: predicting the need
for subsequent intubation. Ped Em Care 2013
Determine the clinical and patient characteristics that predict success or failure of HFNC therapy in children presented to the pediatric emergency department (PED) with respiratory distress.
In infants with respiratory distress presented to the PED, triage respiratory rate greater than 90th percentile for age, initial venous PCO2 greater than 50 mm Hg, and initial venous pH less than 7.30 were associated with failure of HFNC therapy. A diagnosis of acute bronchiolitis was protective with respect to intubation following HFNC. This finding may help guide clinicians who use HFNC by identifying a patient population at higher risk of failing therapy.
Initiating HFNC Therapy
1. HFNC should be administered by physicians, nurses and respiratory therapists experienced in its use. Children needing HFNC require close monitoring and may require escalation of care.
2. High flow rates require a heated, humidified breathing circuit and an interface with a blended oxygen source.
3. Flow rate should exceed the patients inspiratory flow rate.
4. Patients requiring HFNC and FiO2 > 40% should be cared for in an ICU setting; patients who require rapid escalation to HFNC even at lower FiO2 should be strongly considered for ICU admission.
5. HFNC may lead to stabilization in patients awaiting transfer or ICU admission.
HFNC complication
No reports of pneumothorax outside
neonatal age group
Little risk of facial/nasal trauma
May mask hypoventilation and impending
respiratory failure
Predictors of failure in infants with viral
bronchiolitis treated with highflow, high humidity
nasal cannula therapy.
History of prematurity and the patient's age did not increase a patient's risk of failure.
Nonresponders to highflow nasal cannula therapy were on the onset, more hypercarbic, less tachypnoic prior to the start of highflow nasal cannula,
Had no change in their respiratory rate after the initiation of highflow nasal cannula therapy.
( Ped Crit Care 2012 )
HFNC componenet
1. Humidifier – to warm and humidify respiratory gases
2. Respiratory circuit that preserves temperature and
humidity to the patient
3. Nasal cannula that connects to the circuit
Current commercial models:
- Vapotherm 2000i™ and Precision Flow™
- Fisher and Paykel MR 850™ system
- Locally “constructed” models


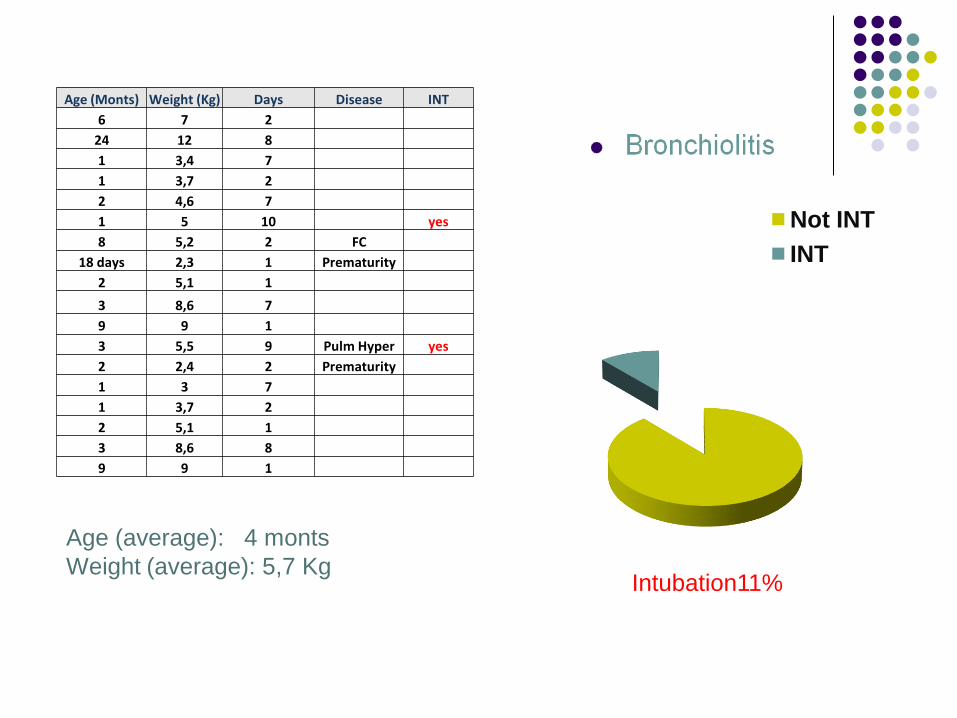
Age (Monts) Weight (Kg) Days Disease INT
6 7 2
24 12 8
1 3,4 7
1 3,7 2
2 4,6 7
1 5 10 yes
8 5,2 2 FC
18 days 2,3 1 Prematurity
2 5,1 1
3 8,6 7
9 9 1
3 5,5 9 Pulm Hyper yes
2 2,4 2 Prematurity
1 3 7
1 3,7 2
2 5,1 1
3 8,6 8
9 9 1
Age (average): 4 monts
Weight (average): 5,7 Kg
Not INT
INT
Intubation11%
CONCLUSION
Bronchiolitis is the most common lower respiratory tract infection in the first year of life and the primary cause of hospitalization in infants;
Despite the growing literature investigating treatment options with recent positive data about the use of nebulized hypertonic saline and epinephrine, oxygen supplementation still remains the best therapy.
CONCLUSION
Oxygen therapy administered by heated,
humidified highflow nasal cannulae (HFNC) has
been shown to reduce the intubation rate and to
improve respiratory distress in children hospitalized
in intensive care units for bronchiolitis.
HFNC has proven to be a well tolerated, non-
invasive respiratory support which provides a
humidified and heated airoxygen blend at a flow of
1 to 8 l/min
CONCLUSION
The advantages of HFNC over nasal continuous positive airways pressure, such as easy use and improved tolerance with minimal nasal trauma, have led to increasing utilization, outside the intensive care unit as well.
Lack of data on the feasibility of HFNC in infants with bronchiolitis.





























