Embed Size (px)
Citation preview

Send Orders for Reprints to [email protected]
Current Medical Imaging Reviews, 2015, 11, 23-37 23
Imaging in Drug Side Effects
Sandra Baleato-González1,*, Roberto García-Figueiras
1, María Ageitos Casais
1, Amadeo Arango
Díaz1, Iván Sanz-Falque
1 and Joan C. Vilanova
2
1Department of Radiology, Hospital Clinico Universitario, Choupana s/n 15706 Santiago De
Compostela, Spain; 2Department of Radiology, Clínica Girona and Hospital Santa Caterina,
Lorenzana 36, Girona, 17002 Spain
Abstract: Drug side effects are common in clinical practice and its diagnosis and radiologic manifes-
tations are not always evident or known. Adverse effects may cause medical complications and nega-
tively affect prognosis and outcome of patients. In this setting, an early diagnosis might have relevant
clinical and therapeutic implications. Different studies have shown that adverse drug reactions related
hospital admissions comprise up to 10% of the total number of hospitalizations and are an important
cause of morbidity and mortality in adults. Most adverse drugs reactions have no distinctive radiologi-
cal features. However, certain iatrogenic disorders have distinctive imaging characteristics that allow their recognition.
We illustrate the imaging findings of drugs side effects and review those complications that radiologists may diagnose.
Keywords: Drugs, Side effects, Medical Imaging.
INTRODUCTION
Adverse drugs reactions are an important cause of mor-
bidity and mortality in adults [1]. Different studies have
shown that drug toxicity related hospital admissions com-
prise up to 10% of the total number of hospitalizations and
may involve any body organ. Most drug-induced toxicities
have no distinctive radiological features on imaging. How-
ever, certain iatrogenic disorders have characteristic imaging
findings that allow their recognition. This paper will review
the radiological manifestations of the most notable complica-
tions induced by drugs “from head to toe” using different
imaging techniques.
1. NERVOUS SYSTEM
Nervous system (NS) toxicity is a significant source of
morbidity in the treatment of patients [2-5]. Neurotoxicity
may appear during treatment or being a late effect of therapy.
In this setting, treatment-related NS toxicities need to be
distinguished from complications related to the underlying
disease. Main pathologic entities associated to NS toxicity
include encephalopathy, vascular complications, meningitis,
mielopathy, neuropathies, and hypothalamo-hipophyseal
involvement.
1a. Intracraneal Drug-induced Anomalies
Encephalopathy. There are many different classes of
agents that can result in a drug-induced encephalopathy [2-
7]. Clinical presentation is variable. Acute encephalopathy
develops within a few hours to days after therapy administra-
tion and presents with altered behaviour, disorientation, con-
fusion, and agitation. Symptoms generally resolve spontane-
ously. Metronidazole is one of the therapeutic agents that
*Address correspondence to this author at the Department of Radiology,
Hospital Clinico Universitario, Choupana s/n 15706 Santiago De Compos-
tela, Spain; E-mail: [email protected]
have associated to the development of acute encephalopathy.
In these patients, MRI shows bilateral and symmetric in-
volvement of the dentate nuclei in the cerebellum [3, 6-7].
The lesions show increased signal intensity on T2-weighted
images, which are reversible after discontinuation of the
drug. Acute disseminated encephalomyelitis (ADEM) is an
immune mediated disease of the brain that usually occurs
following a viral infection or vaccination [8]. As it involves
autoimmune demyelization, ADEM is similar to multiple
sclerosis (Fig. 1).
Fig. (1). Acute disseminated encephalomyelitis (ADEM). A 72-
year-old-male patient with neurologic deficits following influenza
vaccination. ADEM was suspected. Axial T2- weighted (a) and
FLAIR (b) images showed large multifocal, hyperintense and bilat-
eral white matter lesions with enhancement after contrast admini-
stration on axial (c) and coronal (d) contrast-enhanced T1-weighted
images.
1875-6603/15 $58.00+.00 ©2015 Bentham Science Publishers

24 Current Medical Imaging Reviews, 2015, Vol. 11, No. 1 Baleato-González et al.
Subacute encephalopathy is rare and may develop days to
weeks after administration of a drug [6]. Typical MRI find-
ings show symmetrical areas of the white matter with in-
creased signal on DWI and decreased ADC. These MRI
findings have been interpreted as cytotoxic edema [9].
Chronic encephalopathy usually starts to develop with a
prolonged latency (months to years). It is most frequently
irreversible and sometimes even progressive. Recently, Pro-
gressive multifocal leukoencephalopathy has been linked to
methotrexate, rituximab, natalizumab (which was used to
treat multiple slecrosis), efalizumab (an anti-psoriasis drug),
and interferon [5-6]. Other potentially implicated agents are
fluorouracil, topotecan, cisplatin, cytarabine, carmustine, and
thiotepa [4-6]. MRI depicts symmetric periventricular white
matter abnormalities, which can be accompanied by ven-
tricular dilatation and cortical atrophy in severe cases. Cere-
bral atrophy has been mainly observed in valproic-acid en-
cephalopathy.
Cerebrovascular disease. Vascular pathology (including
arterial occlusion, venous thrombosis, and hemorrhage) has
been associated with the administration of different drugs [4-
5, 10-11]. Women taking hormone replacement therapy or
oral contraceptives or patients under androgens or antiangio-
genic treatment have an increased risk of ischemic stroke or
intracranial venous thrombosis. Patients on anticoagulation
therapy show an increased risk for intracraneal hemorrhage.
Beside this, antiangiogenic drugs and imatinib have also
been reported to increase the risk of bleeding. In oncologic
patients, the risk of hemorrhage with antiangiogenic therapy
does appear to vary somewhat with underlying tumor type
[4]. Many other antineoplastic agents, such as cisplatin,
bleomycin, etoposide, vinblastine, methotrexate, cytarabine,
tamoxifen, asparaginase, cyclophosphamide, have been re-
lated to cerebrovascular or diseases in literature.
Posterior reversible encephalopathy syndrome (PRES) is
a specific type of acute encephalopathy caused by vasogenic
edema that results from breakdown in cerebral vascular
autoregulation [7, 12-13]. PRES is characterized by head-
ache, confusion, visual disturbances, seizures, and transient
changes on neuroimaging in the parieto-occipital lobes.
PRES has been associated to the use of cytotoxic and immu-
nosuppressive drugs such as tacrolimus, cyclosporine, and
cisplatin. MRI findings include symmetrical posterior cor-
tico-subcortical lesions, which are hyperintense on FLAIR
and T2-weighted sequences and shows an increase of appar-
ent diffusion coefficient ADC values [5, 7, 12-13] (Fig. 2).
Meningitis. Drug-induced aseptic meningitis cannot be
distinguished from meningitis caused by other agents, and
diagnosis is, therefore, made by exclusion and based on
close association between drug administration and onset of
symptoms [14]. Aseptic meningitis is a typical complication
of nonsteroidal anti-inflammatory drugs, antibiotics, intrave-
nous immunoglobulins, and intrathecal therapy. When per-
formed, neuroimaging was normal in the majority of pa-
tients, however different imaging findings have been occa-
sionally reported, including diffuse meningeal contrast en-
hancement (probably reflecting a blood-brain barrier break-
down) and bilateral supratentorial white matter T2-signal
abnormalities without gadolinium enhancement and with
complete resolution along time [14].
Hypothalamo-hipophyseal System Involvement.
Ipilimumab is an immunotherapeutic agent with clinical ac-
tivity in the treatment of metastatic melanoma and renal cell
carcinoma. Immune-related adverse events such as hypo-
physitis have been reported [15]. MR imaging features of
hypophysitis are non-specific and include by diffuse en-
largement of the pituitary gland with loss of normal posterior
pituitary signal intensity.
1b. Extracraneal Involvement
Mielopathy. As it was mentioned, vaccines may induce
an acute encefalomielitis (ADEM) [8]. During the acute
phase patients have local enlargement of the cord and areas
of increased signal on long TR/TE MR sequences. Other
drugs such as the antibiotic clioquinol, nitrous oxide (an in-
haled anesthetic) or anti-TB medication exposure have been
also related to myelopathy.
Neuropathy. Drug-induced neuropathy is a frequent
complication [2-5]. Imaging findings are usually scarce.
Fig. (2). Posterior reversible encephalopathy syndrome (PRES). A 45-year-old-male treated with tacrolimus. A MRI examination was
performed for evaluating the presence of ataxia. MRI confirmed an isolated lesion on the cerebellum with no supratentorial involvement
compatible with PRES. Axial fluid-attenuated inversion-recovery sequence (FLAIR) image of brain (a) revealed a hyperintense lesion on the
left cerebellum. DWI acquired with a “b” factor of 1000 s/mm2 (b) and corresponding ADC map (c) demonstrated high signal intensity on
DWI and ADC secondary to vasogenic edema.

Imaging in Drug Side Effects Current Medical Imaging Reviews, 2015, Vol. 11, No. 1 25
However, in the case of ascending polyradiculoneuropathy
after intrathecal methotrexate therapy [5, 16], MR may de-
pict lumbosacral ventral root enhancement that shows a dis-
tribution that correlates with the affected area.
2. THORAX
2a. Lung
Drug induced lung injury, an increasingly common cause
of both acute and chronic lung disease, is caused by numer-
ous drugs including certain antibiotics [17-20]. Clinical di-
agnosis is often difficult to establish and is frequently only
suggested after the exclusion of infection, radiation pneu-
monitis, or recurrence of the underlying disease. However,
early diagnosis is essential because cessation of therapy and
treatment of the drug-induced lung injury can often decrease
morbidity and mortality. Lung high-resolution computed
tomography (HRCT) is more sensitive than chest radiogra-
phy for defining the radiographic abnormalities, but present
different limitations: HRCT pattern is rarely specific for a
drug etiology, the radiographic pattern of involvement did
not always correspond to the underlying histological findings
and it is of limited value in determining prognosis. A list of
drugs that cause pulmonary toxicity is available on the Web-
site pneumotox.com online [21].
Nonspecific Interstitial Pneumonia (NSIP). NSIP can
be associated with toxic effects of drugs. Amiodarone,
methotrexate, and carmustine are the most commonly en-
countered. At HRCT, NSIP shows a lower lobe predominant
process with patchy areas of ground-glass opacity and vary-
ing degrees of reticular abnormality, traction bronchiectasis
and consolidation. Although not specific, these findings
should suggest the diagnosis of NSIP in the presence of con-
sistent clinical and histologic finding [22].
Usual Interstitial Pneumonitis (UIP). HRCT features of
UIP are predominantly basal and peripheral reticular areas
with honeycombing and traction bronchiectasis. Cytotoxic
chemotherapeutic agents, such as bleomycin and metho-
trexate, are the most common reported drugs induced UIP
[22]. New generations of antineoplastic agents as gemcit-
abine, taxanes and especially drugs acting on the mTOR
pathway, also produces pulmonary toxicity [23-26]. The role
of drugs taken concomitantly may be important. Hazardous
associations have been reported that can increase the risk of
lung toxicity. Coadministration of cisplatin and bleomycin
increases the risk of bleomycin-induced interstitial lung dis-
ease. The Combined therapies of docetaxel and irradiation
(Fig. 3) for non-small-cell lung cancer (NSCLC) or do-
cexatel and other chemotherapeutic agents is very toxic and
must be taken into account when planning are treatment
strategies for NSCLC [27].
Hypersensitivity Lung Disease. Several drugs can result
in a hypersensitivity reaction in the lungs, for instance cy-
clophosphamide, sulfonamides or nonsteroidal anti-inflam-
matory drugs. The HRCT appearance is similar to that seen
in hypersensitivity pneumonitis secondary to other causes.
Bilateral patchy ground-glass opacities are the most common
finding. However, intralobular interstitial thickening is ob-
served in antineoplastic agent–induced pneumonitis and cen-
trilobular opacities in antibiotic-induced pneumonitis [28].
Bronchiolitis Obliterans. The most common drugs as-
sociated at this entity are sulfasalazine and penicillamine.
HRCT findings include hyperinflation, decreased vascular-
ity, bronchiectasis, bronchial wall thickening, mosaic perfu-
sion, and air trapping on expiratory images [18].
Bronchiolitis Obliterans with Organizing Pneumonia
(BOOP). BOOP is a chronic process consisting in inflamma-
Fig. (3). Usual interstitial pneumonitis (UIP). A 56-year-old man with non-small cell lung cancer treated with a combination of docetaxel
and radiation therapy. Following radiotherapy, the patient presented dyspnea. Thoracic CT was performed. Basal CT images (a-c) and 5
months after treatment (d-f) showed the appearance of typical radiologic changes suggesting UIP, including ground-glass opacities, basal and
peripheral reticular pattern with honeycombing, and traction bronchiectasis.

26 Current Medical Imaging Reviews, 2015, Vol. 11, No. 1 Baleato-González et al.
tory infiltration and fibrosis that predominantly involves the
distal airways. Several medications have been associated
with the development of the BOOP lesion. HRCT usually
shows scattered areas of ground-glass opacities or consolida-
tions with air bronchogram that are often peripheral in distri-
bution. There are no associated bronchiectasis or honey-
combing [29,30].
Pulmonary Hemorrhage. Diffuse pulmonary hemor-
rhage is an uncommon complication of drug therapy. Af-
fected patients can present with acute respiratory distress.
HRCT usually shows scattered or diffuse ground-glass
opacities and consolidations. The drugs most commonly as-
sociated are anticoagulants, amphotericin B, high-dose cy-
clophosphamide, mitomycin, cytarabine, and penicillamine
[17].
Eosinophilic Pneumonia (EP). This pathology is a reac-
tive inflammatory pulmonary process with multiple etiolo-
gies [31]. Drug-induced EP may be considered as a possible
hypersensitivity reaction and it is characterized by the accu-
mulation of eosinophils and macrophages in the alveoli; the
alveolar septa are thickened and infiltrated by eosinophils,
lymphocytes, and plasma cells [32]. A definitive diagnosis of
EP is made when there is evidence of a parenchymal patchy
infiltrate on a HRCT that typically have a peripheral and
upper lobe distribution, peripheral blood eosinophilia, and
increased eosinophils in either lung biopsy tissue or bron-
choalveolar lavage fluid (usually >25%). CT may be helpful
as a 'road map' for a potential biopsy or to give a better view
of the location of the opacities, but it is not necessary to con-
firm a diagnosis [17]
Pulmonary Edema with or Without Diffuse Alveolar
Damage. A non-cardiogenic pulmonary edema, which mani-
fests as acute respiratory distress, may occur with a variety
of drugs most commonly with cytotoxic agents, such as
bleomycin, cytosine arabinoside (Ara-C), methotrexate, and
cyclophosphamide [17-19]. Diffuse alveolar damage, a more
severe form of non-cardiogenic pulmonary edema, occurs
when injury results in necrosis of alveolar endothelial cells
and type II pneumocytes (Fig. 4). DAD is divided into an
acute exudative phase and a late reparative or proliferative
phase. The exudative phase is characterized by alveolar and
interstitial edema and hyaline membranes, is most prominent
in the first week after lung injury. HRCT shows patchy or
diffuse bilateral ground-glass opacities or lung consolida-
tions with a predominance of these findings in the dependent
regions of the lungs. The reparative phase, which is charac-
terized by proliferation of type II pneumocytes and intersti-
tial fibrosis, typically occurs after 1 or 2 weeks.
2b. Pleural Disease
Drug-induced pleural disease is uncommon and mani-
fests as pleural effusions, pleuritis and/or pleural thickening
[33,34]. It may occur as an isolated disorder, associated to
parenchymal disease or in the context of a systemic reaction.
Pleural effusions represent the most common manifestation.
However, hemothorax in anticoagulated patients and pleural
fibrosis with the use of methysergide have been reported.
Ergotamine, ergonovine maleate, bromocriptine, amiodar-
one, and pergolide can produce similar fibrotic response
[35].
2c. Mediastinum
Mediastinal adenopathy may be a complication of
drugs that induce hypersensitivity reactions. Classic associ-
ated drugs are anticonvulsants, particularly phenytoin, and
carbamazepine [36-37].
2d. Cardiac Involvement
The mechanisms of cardiac toxicity are not completely
understood for many drugs. Multiple morphologic and func-
tional imaging techniques can be used to detect and evaluate
the drug-induced cardiac dysfunction, including echocardi-
Fig. (4). Diffuse alveolar damage (DAD). A 66-year-old-female treated with methotrexate presented in the emergency room with progres-
sive shortness of breath and cough. Lung HRCT images (a-c) showed diffuse ground-glass opacities and normal heart size. These findings
may suggest DAD. Seven days later, a new CT scan (d-f) evidenced ground-glass opacities and interstitial fibrosis, which correspond to the
reparative phase of DAD.

Imaging in Drug Side Effects Current Medical Imaging Reviews, 2015, Vol. 11, No. 1 27
ography, magnetic resonance imaging, and radionuclide im-
aging.
Myocardium. Myocardial dysfunction has been reported
for different drugs, such as cytotoxic and cytostatic drugs
(eg, anti-HER2 agents) used to treat cancer, antipsychotic
drugs, and antifungal drugs. Some of them can cause poten-
tially permanent or irreversible dysfunction (eg, doxorubi-
cin), whereas others may cause potentially reversible cardiac
toxic effects [38].
Besides, clinicians have become attentive to drug-
induced myocardial infarction following reports that some
selective cyclooxygenasa (COX) inhibitors increase the risk
of this event. However, the most frequently reported drugs
associated to myocardial infarction were the antimigraine
drug sumatriptan, the calcium antagonist nifedipin, and nico-
tine [39].
Valvular Disease. Different drugs have a potential of
causing valvular heart problems, including cabergoline (used
to manage prolactinomas), ergotamine, and methysergide
[36]. These drugs increase serotonin levels in the blood and
secondary may cause thickening and fibrosis of the valve.
Pericarditis. Pericardial reactions to drugs are rare.
However, several medications and toxic substances can in-
duce pericarditis, tamponade, adhesions, fibrosis, or constric-
tion [40].
2e. Pulmonary Vascular Disease
Vascular system can be involved at different levels caus-
ing different clinical anomalies such as pulmonary embolism
or pulmonary hypertension.
Pulmonary Embolism. Oral contraceptives or hormone
therapy are well-known cause of pulmonary embolism (PE)
[17]. CT pulmonar angiography is the standard test of choice
for the diagnosis of direct and indirect findings of acute PE.
The direct findings of PE include a filling defect that oc-
cludes a contrast-enhanced pulmonary vessel, while indirect
signs are seen in the lung parenchyma with peripheral
wedge-shaped areas of consolidation,
Pulmonary Hypertension. Drugs that have been associ-
ated with the onset of pulmonary hypertension include am-
phetamines, chemotherapeutic drugs, or tryptophan. Imaging
findings of pulmonary hypertension include a main pulmo-
nary artery diameter of greater than 29 mm and right atrial
and ventricular enlargement [41].
3. ABDOMEN AND PELVIS
Cross-sectional imaging of drug side effects in the abdo-
men and pelvis is a complex endeavour due to the multiple
organ systems and the broad differential diagnoses to be
considered [42-43].
3a. Hepatic Complications
Liver is one of the most frequent organs involved in drug
side effects. More than 1200 drugs have been related to he-
patic complications [44] and drug toxicity is the leading
cause of acute liver failure in the United States [45]. Drug-
induced liver changes may consist in hepatitis, architectural
distorsion, deposition diseases, vascular anomalies, or tumor
induction.
Toxic Hepatitis. Different therapies may cause a toxic
hepatitis. Antibiotics are a commonly implicated cause of
drug-induced hepatotoxicity with amoxicilin-clavulanic acid
being the most common [46-47]. Imaging findings are usu-
ally nonspecific and include hepatomegaly, gallbladder wall
thickening, and periportal low attenuation on CT. On MR
imaging, T1 and T2 relaxation times of the liver are in-
creased. High signal intensity, corresponding to lymphedema
or inflammation, can often be noted in the periportal region.
Hepatomegaly is a frequent and nonspecific finding. How-
ever, hepatomegaly with associated splenomegaly and lymph
node enlargement has been described with the use of hydan-
toin (an anticonvulsant therapy) [48].
Alteration of Liver Architecture. Liver contour
changes following chemotherapy in patients with liver me-
tastases have been described. Chemotherapy causes areas of
retracted tumor tissue and scarring and a regenerative phe-
nomenon in the liver parenchyma. This entity is referred to
as pseudocirrhosis because it resembles macronodular cir-
rhosis [49,50]. Common imaging findings include capsular
retraction, volume loss, caudate hypertrophy, and portal hy-
pertension and can be observed within a few weeks or
months after therapy (Fig. 5). However, unlike cirrhosis, at
Fig. (5). Pseudocirrhosis. A 46-year-old female with breast cancer and hepatic metastasis. Abdominal CT images showed a metastatic le-
sion in a liver, which showed normal morphology and contour. The patient began with chemotherapy treatment. Six months later, the liver
showed imaging findings that mimicked cirrhosis (pseudocirrhosis).
28 Current Medical Imaging Reviews, 2015, Vol. 11, No. 1 Baleato-González et al.
pathology patients do not have bridging portal fibrosis, but
can manifest nodular regenerative hyperplasia [51].
Deposition Disease of the Liver. Different substances
may accumulate in liver as a consequence of drugs admini-
stration. Hepatic steatosis is due to the abnormal accumula-
tion of lipids, particularly triglycerides within hepatocytes.
Fatty liver may be associated with exogenous steroids and
several drugs such as amiodarone, methotrexate, 5 fluoracil,
tamoxifen, NSAIDs, or metoprolol [52]. On ultrasound (US),
liver with fatty changes demonstrates increased echogenicity
and attenuation. Unenhanced CT scan shows hepatic attenua-
tion lower than the spleen, while liver signal drops out in
fatty liver in out-of-phase gradient-echo T1-weighted MR
imaging. Amiodarone and and its metabolite, desethylamio-
darone, are likely to accumulate in the liver parenchyma.
These compounds contain two atoms of iodine, thus the ac-
cumulation of amiodarone and desethylamiodarone leads to
increased iodine content within the liver. Furthermore, the
levels of amiodarone correlate with liver CT density and CT
density of the liver may normalize after cessation of amio-
darone administration [53].
Vascular Liver Anomalies. Sinusoidal obstruction syn-
drome (SOS or veno-occlusive disease) is a unique form of
hepatic venous obstruction resulting from occlusion of the
small hepatic venules and intrahepatic veins [54]. The basic
mechanism of this entity is an injury of the endothelium of
the hepatic venules caused by direct destruction or as a con-
sequence of inflammation leading to edema and necrosis of
the wall of the venule. The resultant venous outflow obstruc-
tion leads to sinusoidal dilatation, congestion, hepatocellular
necrosis, and can result in centrilobular fibrosis. SOS usually
presents within 2 to 4 weeks following the exposure to the
medication. Imaging findings resemble those of Budd-Chiari
syndrome with hepatomegaly and ascites but the major he-
patic veins appear patent (Fig. 6). SOS is almost always seen
in association with chemotherapy conditioning regimens for
bone marrow transplantation, particularly those containing
cyclophosphamide or busulfan.
Liver Tumors Induced by Drugs. Hepatocellular ade-
noma (HCA) is a benign liver neoplasm strongly associated
with oral contraceptive use and androgen steroid therapy.
HCA may have characteristic findings on CT and MRI
[55,56]. These include the presence of a single mass or mul-
tiple masses that contain fatty or hemorrhagic areas that usu-
ally show hypervascular to the liver on the hepatic arterial
phase [56]. Besides, FNH appears to be a late complication
of an iatrogenic vascular disease in children with a history of
malignancy treated with chemotherapy [57-58] (Fig. 7).
3b. Biliary and Pancreatic Complications
Many drugs may affect biliary tree and pancreas causing
gallstones, biliary strictures or acute pancreatitis.
Lithiasis. Ceftriaxone, a parenteral third generation
cephalosporin, is widely used for the treatment of a variety
of bacterial infections in both adults and children. Pseu-
dolithiasis or gallbladder precipitates is a complication de-
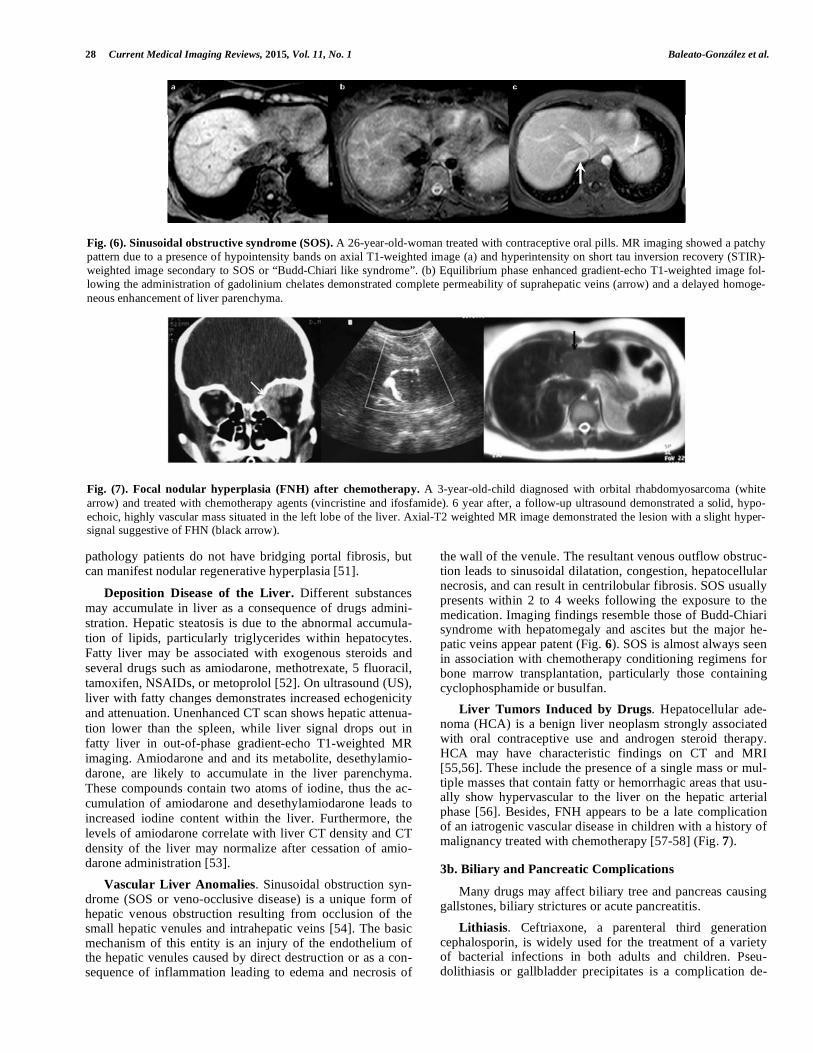
Fig. (6). Sinusoidal obstructive syndrome (SOS). A 26-year-old-woman treated with contraceptive oral pills. MR imaging showed a patchy
pattern due to a presence of hypointensity bands on axial T1-weighted image (a) and hyperintensity on short tau inversion recovery (STIR)-
weighted image secondary to SOS or “Budd-Chiari like syndrome”. (b) Equilibrium phase enhanced gradient-echo T1-weighted image fol-
lowing the administration of gadolinium chelates demonstrated complete permeability of suprahepatic veins (arrow) and a delayed homoge-
neous enhancement of liver parenchyma.
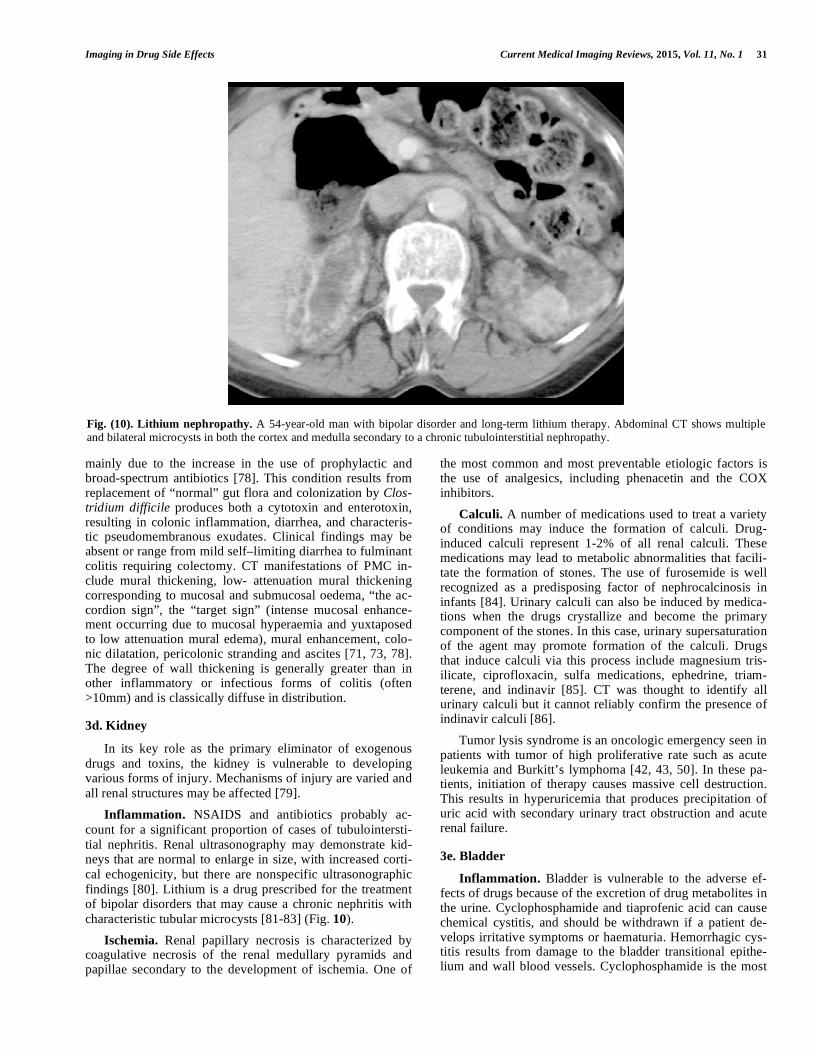
Fig. (7). Focal nodular hyperplasia (FNH) after chemotherapy. A 3-year-old-child diagnosed with orbital rhabdomyosarcoma (white
arrow) and treated with chemotherapy agents (vincristine and ifosfamide). 6 year after, a follow-up ultrasound demonstrated a solid, hypo-
echoic, highly vascular mass situated in the left lobe of the liver. Axial-T2 weighted MR image demonstrated the lesion with a slight hyper-
signal suggestive of FHN (black arrow).

Imaging in Drug Side Effects Current Medical Imaging Reviews, 2015, Vol. 11, No. 1 29
veloped in 43% of the children treated for serious infections
with ceftriaxone. These precitates resolved completely with
the cessation of therapy [59]. On US, the concretions seen in
ceftriaxone pseudolithiasis are indistinguishable from typical
gallstones. They are brightly echogenic with true shadowing
posteriorly. Other drugs such as furosemide or octreotide can
also cause gallstones.
Biliary Strictures. There are many drugs that are associ-
ated with biliary stricture on literature. However, imaging
findings in these cases are also unspecific and other causes
of biliary stricture must be rule out.
Acute pancreatitis. Drugs are considered a relatively
rare cause of acute pancreatitis. However up to 200 drugs
have been associated to pancreatitis [60]. The true incidence
of drug-associated pancreatitis (DAP) is not accurately
known and estimated around 2% of all cases with acute pan-
creatitis [61,62]. The diagnosis of drug-induced pancreatitis
is difficult to establish, mainly due to the absence of a cause-
specific diagnostic test [63]. Therefore, it is usually based on
the following criteria: 1) Acute pancreatitis occurs during the
administration of a drug, 2) all the other common causes are
excluded, 3) symptoms of acute pancreatitis disappear after
drug withdrawal, and 4) symptoms recur after a rechallenge
of the suspected drug. Unfortunately, drug-induced pan-
creatitis has no distinguishing clinical or imaging features. However, the prognosis of drug-induced pancreatitis is gen-
erally excellent.
3c. Esophagogastrointestinal Complications
Motility Disorders. The motor disorders of the gastroin-
testinal tract may be secondary to drugs. The motor activity
of the small intestine is less likely to be affected by drugs
than is the colon. The reduction of bowel motility may be
severe enough that it can cause paralytic ileus or pseudo-
obstruction. Imaging techniques show prominent colonic
dilatation without distal obstructing lesion [64]. Cathartic
colon is a differentiated functional colonic anomaly that oc-
curs with chronic use of stimulant laxatives. This entity
causes an atonic and redundant colon.
Hyperplasia. Chronic use of proton-pump inhibitors can
cause gastric fold thickening secondary to parietal cell hy-
pertrophy and hyperplasia [65].
Ulceration and Perforation. Nonsteroidal anti-
inflammatory drugs (NSAIDs) are among the most com-
monly prescribed drugs worldwide. Although NSAIDs are
effective, their use is associated with a broad spectrum of
adverse reactions. GI side effects are the most common and
range from dyspepsia, heartburn, and abdominal discomfort
to more serious life-threatening complications such as peptic
ulcer disease and perforation. The most common NSAID-
associated GI complications are peptic ulcer disease and en-
teropathy [66]. Mucosal damage is seen in 30-50% of pa-
tients taking NSAIDs users, but most lesions are of little
clinical significance and disappear or reduce in number with
continued use, probably because of mucosal adaptation.
Only 15 to 30% users have endoscopically confirmed ulcers,
with the gastric antrum being most frequently affected. Per-
foration may also complicate the administration of many
chemotherapy agents and target therapies [67-69]. Recently,
GI perforation has been reported with bevacizumab, a mono-
clonal antibody against vascular endothelial growth factor,
with perforation reported in 1.5 to 2% of patients treated for
metastatic colorectal cancer [70]. The pathogenesis of bowel
perforation is unknown, but suggested mechanisms include
ischemia with thrombosis of intestinal mesenteric vessels
(Fig. 8).
Ischemia. Before attributing gastrointestinal ischemia to
a medication, it is necessary to exclude other risk factors for
Fig. (8). Bowel Perforation secondary to bevacizumab. A 45-year-old man with bowel perforation induced by bevacizumab. Abdominal
CT shows a large pneumoperitoneum (long arrow) and portal venous gas (short arrow).

30 Current Medical Imaging Reviews, 2015, Vol. 11, No. 1 Baleato-González et al.
ischemia. Bowel ischemia (mainly colitis) has been reported
with the use of therapeutic agents such as digitalis, diuretics,
ergotamine, hormonal therapy, -interferon, dopamine,
methysergide, or NSAIDs [70]. Imaging findings of ische-
mia are similar regardless of the primary cause. The most
common CT finding in bowel ischemia is bowel wall thick-
ening, although it is nonspecific. The thickened bowel wall
sometimes shows the target sign, alternating layers of high
and low attenuation within the thickened bowel wall secon-
dary to submucosal edema or hemorrhage. However, the
bowel wall is thinned when the involved bowel segment be-
comes gangrenous [71-72].
Inflammation. Neutropenic enterocolitis is characterized
by fever and right lower quadrant pain in neutropenic pa-
tients. It is seen in children and adults with hematologic ma-
lignancies, with anaplastic anemia, and after myelosuppres-
sive therapy for solid malignancies and it is one of the few
oncological emergencies [43, 73]. Diagnosis criteria include
neutropenia (neutrophil count less than 1 cell/μl), tempera-
ture greater than 38.3 ºC and evidence for colitis. This entity
is most likely to occur early after commencement of chemo-
therapy. CT is the modality of choice for the diagnosis. Sug-
gestive features include colonic mural thickening with low–
density areas representing edema and/or necrosis, pericolic
inflammation with fat stranding, ascitis, and pneumatosis
intestinalis and free air in the presence of underlying mural
necrosis and perforation. Although the right colon is most
frequently involved, a condition specifically referred to as
typhlitis, any segment of the colon or small bowel may be
involved in enterocolitis.
Gastrointestinal Hemorrhage. Both, intravenous hepar-
ins and oral agents, such as warfarin, may induce hemor-
rhage as a major complication [74]. It is reported in up to 4%
of treated patients. The commonest sites of anticoagulant-
related hematomas (ACH) are the soft tissues, the gastroin-
testinal tract, and the urinary tract. Gastrointestinal bleeding
can be intraluminal, intramural, retroperitoneal, extraperito-
neal, or into solid abdominal organs. Endoscopic techniques
are currently considered the first-line diagnostic and thera-
peutic procedures of choice for both upper and lower gastro-
intestinal bleeding and CT angiography is used in assessing
patients with an acute abdomen. The CT angiographic diag-
nosis of active gastrointestinal bleeding is made when hyper-
attenuating extravasated contrast material is seen within the
bowel lumen [75].
Bowel Edema. Angiotensin converting enzyme inhibi-
tors (ACEIs) are widely used to treat patients with hyperten-
sion and refractory cardiac failure. Angioedema induced by
ACEIs is present in 0.1-0.7% of treated patients. In rare
cases, it can involve visceral organs such as the bowel [76].
The mechanism of action by which ACEIs cause angioe-
dema is not fully understood, although bradykinin seems to
be involved. It is most common in females, suggesting a pos-
sible sex-linked or hormonal etiology. Symptoms typically
present within 24-48 hours of initiation of therapy and re-
solve within 24-48 hours after discontinuing the ACEIs. Im-
aging findings include a long-segment involvement of small
bowel, with a tendency to affect the jejunum. The affected
bowel loops typically show the target sign produced by al-
ternating enhancement of the mucosa, relatively hypodense
submucosa (related to edema), and enhancing serosa [77]
(Fig. 9).
Infection. In recent years there has been a marked in-
crease in the incidence of pseudomembranous colitis (PMC)
Fig. (9). Bowel angioedema secondary to angiotensin converting enzyme inhibitors (ACEIs). A 53-year-old presented in emergency
room with complaints of abdominal pain. Abdominal CT showed edema of the small bowel (arrow) and moderate ascitis secondary to treat-
ment to ACEIs.
Imaging in Drug Side Effects Current Medical Imaging Reviews, 2015, Vol. 11, No. 1 31
mainly due to the increase in the use of prophylactic and
broad-spectrum antibiotics [78]. This condition results from
replacement of “normal” gut flora and colonization by Clos-tridium difficile produces both a cytotoxin and enterotoxin,
resulting in colonic inflammation, diarrhea, and characteris-
tic pseudomembranous exudates. Clinical findings may be
absent or range from mild self–limiting diarrhea to fulminant
colitis requiring colectomy. CT manifestations of PMC in-
clude mural thickening, low- attenuation mural thickening
corresponding to mucosal and submucosal oedema, “the ac-
cordion sign”, the “target sign” (intense mucosal enhance-
ment occurring due to mucosal hyperaemia and yuxtaposed
to low attenuation mural edema), mural enhancement, colo-
nic dilatation, pericolonic stranding and ascites [71, 73, 78].
The degree of wall thickening is generally greater than in
other inflammatory or infectious forms of colitis (often
>10mm) and is classically diffuse in distribution.
3d. Kidney
In its key role as the primary eliminator of exogenous
drugs and toxins, the kidney is vulnerable to developing
various forms of injury. Mechanisms of injury are varied and
all renal structures may be affected [79].
Inflammation. NSAIDS and antibiotics probably ac-
count for a significant proportion of cases of tubulointersti-
tial nephritis. Renal ultrasonography may demonstrate kid-
neys that are normal to enlarge in size, with increased corti-
cal echogenicity, but there are nonspecific ultrasonographic
findings [80]. Lithium is a drug prescribed for the treatment
of bipolar disorders that may cause a chronic nephritis with
characteristic tubular microcysts [81-83] (Fig. 10).
Ischemia. Renal papillary necrosis is characterized by
coagulative necrosis of the renal medullary pyramids and
papillae secondary to the development of ischemia. One of
the most common and most preventable etiologic factors is
the use of analgesics, including phenacetin and the COX
inhibitors.
Calculi. A number of medications used to treat a variety
of conditions may induce the formation of calculi. Drug-
induced calculi represent 1-2% of all renal calculi. These
medications may lead to metabolic abnormalities that facili-
tate the formation of stones. The use of furosemide is well
recognized as a predisposing factor of nephrocalcinosis in
infants [84]. Urinary calculi can also be induced by medica-
tions when the drugs crystallize and become the primary
component of the stones. In this case, urinary supersaturation
of the agent may promote formation of the calculi. Drugs
that induce calculi via this process include magnesium tris-
ilicate, ciprofloxacin, sulfa medications, ephedrine, triam-
terene, and indinavir [85]. CT was thought to identify all
urinary calculi but it cannot reliably confirm the presence of
indinavir calculi [86].
Tumor lysis syndrome is an oncologic emergency seen in
patients with tumor of high proliferative rate such as acute
leukemia and Burkitt’s lymphoma [42, 43, 50]. In these pa-
tients, initiation of therapy causes massive cell destruction.
This results in hyperuricemia that produces precipitation of
uric acid with secondary urinary tract obstruction and acute
renal failure.
3e. Bladder
Inflammation. Bladder is vulnerable to the adverse ef-
fects of drugs because of the excretion of drug metabolites in
the urine. Cyclophosphamide and tiaprofenic acid can cause
chemical cystitis, and should be withdrawn if a patient de-
velops irritative symptoms or haematuria. Hemorrhagic cys-
titis results from damage to the bladder transitional epithe-
lium and wall blood vessels. Cyclophosphamide is the most
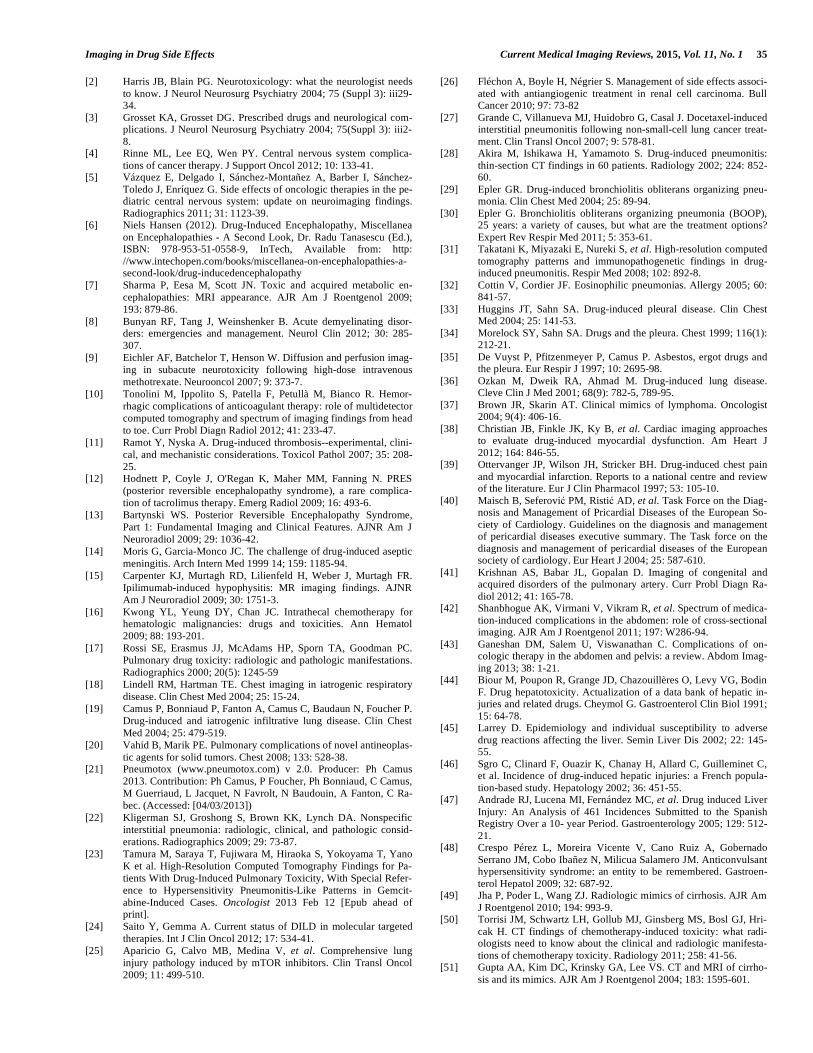
Fig. (10). Lithium nephropathy. A 54-year-old man with bipolar disorder and long-term lithium therapy. Abdominal CT shows multiple
and bilateral microcysts in both the cortex and medulla secondary to a chronic tubulointerstitial nephropathy.

32 Current Medical Imaging Reviews, 2015, Vol. 11, No. 1 Baleato-González et al.
common cause of hemorrhagic cystitis [42,43,50,87]. Ac-
rolein (a metabolic product of cyclophosphamide) causes
sloughing, thinning, and inflammation of the urothelium.
Although, the bladder is the organ most susceptible to dis-
ease because of prolonged surface contact with the inciting
agent in urine, the entire urothelial surface is at risk. Focal or
diffuse thickening and hypervascularity of the bladder wall
can be detected on imaging techniques [42, 43, 87]. The
most common finding in the upper tracts is hydronephrosis
caused by reflux or obstruction (Fig. 11). Urothelial thicken-
ing, perinephric fluid collections or hemorrhagic pyelitis
have been also reported.
Neurogenic Alterations. Neurogenic bladder has been
described in patients receiving different therapies as a result
of peripheral neurotoxicity. MRI spine evaluation should be
performed to exclude medullary causes of bladder dysfunc-
tion.
3f. Uterus
Tamoxifen is a nonsteroidal antiestrogen agent that is
used for the treatment of breast cancer and to prevent breast
cancer in some high-risk populations. Tamoxifen may, how-
ever, cause adverse effects at the uterine level, including
polyps, endometrial hyperplasia, endometrial carcinoma,
leiomyomas, and adenomyosis [42, 88]. Endocervical mi-
croglandular hyperplasia is also a usual finding in oral con-
traceptive pills users [42].
3g. Ovary
Ovarian hyperstimulation syndrome (OHSS) is an iatro-
genic complication of ovarian stimulation with infertility
treatments. This syndrome is characterized by ovarian en-
largement due to multiple ovarian cysts and an acute fluid
shift into the extravascular space that produces ascites
[42,89].
3h. Retroperitoneum
Inflammation. Retroperitoneal fibrosis is mainly an
idiopathic process, however methysergide, methyldopa, or
ergot alkaloids may cause this entity [90]. Imaging tech-
niques may demonstrate a soft tissue mas around aorta and
inferior vena cava that is isodense to surrounding muscle. CT
and MRI allow the evaluation of retroperitoneal fibrosis lo-
cation, extent, and effect on adjacent organs and vascular
structures.
4. MUSCULOSKELETAL SYSTEM
Drug-induced musculoskeletal disorders can vary greatly
from those that are asymptomatic to severe and even life-
threatening conditions. Musculoskeletal abnormalities can
involve the bones, the joints, or soft tissues.
4a. Bone Abnormalities
It has been established that drugs may interfere with bone
metabolism by acting on the maturation, mineralization or
morphology. Main drug-induced bone anomalies are osteo-
malacia, osteoporosis, and osteonecrosis.
Osteomalacia (OM). OM is a metabolic bone disease
characterized by a defect of bone mineralization. OM can be
secondary to several causes. Among these, an important role
may be attributed to some drugs, usually anticonvulsants
(phenobarbital, phenytoin, and carbamazepine) and drugs
containing a high concentration of aluminium [91-93]. OM
presents with a wide variety of clinical, biochemical and
radiographic manifestations mimicking other musculoskele-
tal disorders, including osteoporosis [94,95]. Characteristic
pseudofractures (also named Looser's zones) are only present
in some patients.
Osteoporosis is the result of bone loss due to an imbal-
ance in bone turnover in which bone resorption exceeds bone
formation. Drug-induced osteoporosis is common and has a
significant impact on the prognosis of patients suffering from
chronic debilitating diseases. Glucocorticoids are the drugs
causing osteoporotic fractures most frequently, but osteopo-
rosis with fractures is observed also in patients treated with
aromatase inhibitors for breast cancer, in men receiving anti-
androgen therapy for prostate cancer, in postmenopausal
women treated with high doses of thyroxine, and in patients
treated with thiazolinediones for diabetes mellitus [96,97].
Radiographic features of corticosteroid-induced osteoporosis
are usually indistinguishable from those of primary osteopo-
rosis. Insufficiency fractures can involve any bone, most
frequently thoracic and lumbar vertebrae, sacrum or long
bones [91]. Conventional radiography allows qualitative and
semiquantitative evaluation of osteoporosis, while dual-
energy x-ray absorptiometry and quantitative CT have been
developed to quantify bone mineral content and assess bone
loss.
Osteonecrosis. Steroids and bisphosphonates have been
associated to osteonecrosis in hips and jaw, respectively. The
exact mechanisms of corticosteroid-induced osteonecrosis
Fig. (11). Hemorrhagic cystitis. A 6-year-old child treated with cyclophosphamide that presented hematuria. CT showed diffusely thick-
ened bladder wall with multiple hyperdense foci (black arrow on c) compatible with hemorrhagic cistitis. Hydronephrosis and hemorrhagic
pyelitis (black arrow on a) were visible at a higher level.

Imaging in Drug Side Effects Current Medical Imaging Reviews, 2015, Vol. 11, No. 1 33
remain unknown but the disease develops in 8%–10% of all
corticosteroid users. Bisphosphonates are standard treatment
of patients with bone metastases but are associated to os-
teonecrosis of the jaw (ONJ). The estimated prevalence of
intravenous bisphosphonate-associated ONJ in cancer pa-
tients is as high as 6%–10% [98]. CT is the modality of
choice to diagnosis this entity showing sclerosis with bone
fragmentation and areas of lysis (Fig. 12).
4b. Muscle Disorders
Myopathy. The combination of skeletal muscle weak-
ness, tenderness and pain with the possibility of the plasma
creatinine kinase elevation suggests the presence of myopa-
thy. Muscle toxicity is a well-known side effect associated
with the use of statins and high dose of glucocorticoids. D-
penicillamine, antiretroviral therapy with zidovudine, and
misuse of androgenic hormone derivatives by bodybuilders
has been also reported in association to myopathy [99]. Im-
aging features are nonspecific, showing diffuse edema and
inflammation in acute cases and atrophy with fatty infiltra-
tion in chronic myositis [100]. Drug-induced myopathy is a
dignosis of exclusion without specific clinical signs or sero-
logic, neurophysiologic, or histologic characteristics [101].
Rhabdomyolysis. Destruction of skeletal muscle cells is
a clinical condition of potential life threatening. The inci-
dence of rhabdomyolysis with statin therapy is approxi-
mately 0.04%–0.2% and is dose dependent [102]. Rhabdo-
myolysis has been recently reported for sunitinib, a tyrosine
kinase inhibitor used in renal cancer patients [103]. There are
not characteristic imaging findings of rhabdomyolysis. MRI
may show hyperintensity areas on T2-weighted images sug-
gesting muscle edema.
4c. Joints
Tendon Rupture and Tendinitis. These are well recog-
nized but rare complications of treatment with fluoroqui-
nolones (FQs). FQs tendinopathy occurs more commonly in
tendons under high stress, mainly involving the Achilles
tendon (Fig. 13), although any tendon can be affected. The
exact mechanism is unknown [104].
4d. Soft Tissues
Fat necrosis. Subcutaneous and intramuscular injections
can cause fat necrosis, which will also calcify. Soft tissue
calcifications are one of the most common radiologic mani-
festations and are often seen in the gluteal region.
HIV-associated lipodystrophy. Long-term therapy with
antiretroviral therapy produces lipodystrophy. This is a com-
plex syndrome characterized by changes in regional fat mass,
Fig. (12). Bisphosphonate-associated osteonecrosis of the jaw. Axial and coronal CT scans showing cortical bone loss on the right side of
the mandible (arrow) in a 60-year-old man diagnosed with mieloma multiple and treated with zoledronic acid.

34 Current Medical Imaging Reviews, 2015, Vol. 11, No. 1 Baleato-González et al.
dyslipidemia, and insulin resistance. Adipose tissue redistri-
bution is characterized by loss of peripheral subcutaneous
adipose tissue (face, limbs, buttocks), visceral fat accumula-
tion, and lipomatosis, especially in the dorsocervical area
(“buffalo hump”) (Fig. 14) [105, 106].
5. VASCULAR SYSTEM
Venous thrombosis. Deep vein thrombosis (DVT) is a
common vascular disorder. A thrombus either arises sponta-
neously or is caused by clinical conditions including surgery,
trauma, or prolonged bed rest (107). DVT might be induced
by drugs, being a common vascular side effect of antineo-
plastic therapy, oral contraceptive users, corticoids, and
COX inhibitors [11].
Vasculitis. Drug-induced vasculitis is the most common
form of vasculitis. The differential diagnosis between drug-
induced and idiopathic vasculitic conditions may be difficult,
however imaging techniques play a pivotal role in the diag-
nosis of large vessel vasculitis and in demonstrating internal
organ involvement [108].
CONCLUSION
Drugs are associated with significant complications in
different organs. Awareness of these complications can help
the radiologist to detect these at early stages, which helps in
the appropriate management and results in better outcome.
CONFLICT OF INTEREST
The authors confirm that this article content has no con-
flict of interest.
ACKNOWLEDGEMENTS
Declared none.
REFERENCES
[1] Pirmohamed M, James S, Meakin S, et al. Adverse drug reaction as
cause of admission to hospital: prospective analysis of 18820 pa-
tients. BMJ 2004; 329: 15-9.
Fig. (13). Fluoroquinolone-induced tendinopathy. A 80-year-old-man presented to the emergency department with a 5-week history of
progressive pain in the Achilles region. The patient was previously diagnosed with pneumonia based on chest X-ray (a), and levofloxacin for
10 days was prescribed. Longitudinal and axial images of ultrasound exam (b) demonstrated a fusiform hypechoic swelling of the tendon
without disruption of the fibers compatible with tendinosis. Axial fat-suppressed T2-weighted MR images at different levels (c) showed a
high signal around the Achilles tendon and edema in Kager’s fat pad.
Fig. (14). Lipodystrophy induced by antiretroviral therapy. A
40 year-old-female treated with antiretroviral medication. Sagittal
T2-weighted MR image shows a focal fat accumulation in the dor-
socervical area, also named ‘‘buffalo hump”.
Imaging in Drug Side Effects Current Medical Imaging Reviews, 2015, Vol. 11, No. 1 35
[2] Harris JB, Blain PG. Neurotoxicology: what the neurologist needs
to know. J Neurol Neurosurg Psychiatry 2004; 75 (Suppl 3): iii29-
34.
[3] Grosset KA, Grosset DG. Prescribed drugs and neurological com-
plications. J Neurol Neurosurg Psychiatry 2004; 75(Suppl 3): iii2-
8.
[4] Rinne ML, Lee EQ, Wen PY. Central nervous system complica-
tions of cancer therapy. J Support Oncol 2012; 10: 133-41.
[5] Vázquez E, Delgado I, Sánchez-Montañez A, Barber I, Sánchez-
Toledo J, Enríquez G. Side effects of oncologic therapies in the pe-
diatric central nervous system: update on neuroimaging findings.
Radiographics 2011; 31: 1123-39.
[6] Niels Hansen (2012). Drug-Induced Encephalopathy, Miscellanea
on Encephalopathies - A Second Look, Dr. Radu Tanasescu (Ed.),
ISBN: 978-953-51-0558-9, InTech, Available from: http:
//www.intechopen.com/books/miscellanea-on-encephalopathies-a-
second-look/drug-inducedencephalopathy
[7] Sharma P, Eesa M, Scott JN. Toxic and acquired metabolic en-
cephalopathies: MRI appearance. AJR Am J Roentgenol 2009;
193: 879-86.
[8] Bunyan RF, Tang J, Weinshenker B. Acute demyelinating disor-
ders: emergencies and management. Neurol Clin 2012; 30: 285-
307.
[9] Eichler AF, Batchelor T, Henson W. Diffusion and perfusion imag-
ing in subacute neurotoxicity following high-dose intravenous
methotrexate. Neurooncol 2007; 9: 373-7.
[10] Tonolini M, Ippolito S, Patella F, Petullà M, Bianco R. Hemor-
rhagic complications of anticoagulant therapy: role of multidetector
computed tomography and spectrum of imaging findings from head
to toe. Curr Probl Diagn Radiol 2012; 41: 233-47.
[11] Ramot Y, Nyska A. Drug-induced thrombosis--experimental, clini-
cal, and mechanistic considerations. Toxicol Pathol 2007; 35: 208-
25.
[12] Hodnett P, Coyle J, O'Regan K, Maher MM, Fanning N. PRES
(posterior reversible encephalopathy syndrome), a rare complica-
tion of tacrolimus therapy. Emerg Radiol 2009; 16: 493-6.
[13] Bartynski WS. Posterior Reversible Encephalopathy Syndrome,
Part 1: Fundamental Imaging and Clinical Features. AJNR Am J
Neuroradiol 2009; 29: 1036-42.
[14] Moris G, Garcia-Monco JC. The challenge of drug-induced aseptic
meningitis. Arch Intern Med 1999 14; 159: 1185-94.
[15] Carpenter KJ, Murtagh RD, Lilienfeld H, Weber J, Murtagh FR.
Ipilimumab-induced hypophysitis: MR imaging findings. AJNR
Am J Neuroradiol 2009; 30: 1751-3.
[16] Kwong YL, Yeung DY, Chan JC. Intrathecal chemotherapy for
hematologic malignancies: drugs and toxicities. Ann Hematol
2009; 88: 193-201.
[17] Rossi SE, Erasmus JJ, McAdams HP, Sporn TA, Goodman PC.
Pulmonary drug toxicity: radiologic and pathologic manifestations.
Radiographics 2000; 20(5): 1245-59
[18] Lindell RM, Hartman TE. Chest imaging in iatrogenic respiratory
disease. Clin Chest Med 2004; 25: 15-24.
[19] Camus P, Bonniaud P, Fanton A, Camus C, Baudaun N, Foucher P.
Drug-induced and iatrogenic infiltrative lung disease. Clin Chest
Med 2004; 25: 479-519.
[20] Vahid B, Marik PE. Pulmonary complications of novel antineoplas-
tic agents for solid tumors. Chest 2008; 133: 528-38.
[21] Pneumotox (www.pneumotox.com) v 2.0. Producer: Ph Camus
2013. Contribution: Ph Camus, P Foucher, Ph Bonniaud, C Camus,
M Guerriaud, L Jacquet, N Favrolt, N Baudouin, A Fanton, C Ra-
bec. (Accessed: [04/03/2013])
[22] Kligerman SJ, Groshong S, Brown KK, Lynch DA. Nonspecific
interstitial pneumonia: radiologic, clinical, and pathologic consid-
erations. Radiographics 2009; 29: 73-87.
[23] Tamura M, Saraya T, Fujiwara M, Hiraoka S, Yokoyama T, Yano
K et al. High-Resolution Computed Tomography Findings for Pa-
tients With Drug-Induced Pulmonary Toxicity, With Special Refer-
ence to Hypersensitivity Pneumonitis-Like Patterns in Gemcit-
abine-Induced Cases. Oncologist 2013 Feb 12 [Epub ahead of
print].
[24] Saito Y, Gemma A. Current status of DILD in molecular targeted
therapies. Int J Clin Oncol 2012; 17: 534-41.
[25] Aparicio G, Calvo MB, Medina V, et al. Comprehensive lung
injury pathology induced by mTOR inhibitors. Clin Transl Oncol
2009; 11: 499-510.
[26] Fléchon A, Boyle H, Négrier S. Management of side effects associ-
ated with antiangiogenic treatment in renal cell carcinoma. Bull
Cancer 2010; 97: 73-82
[27] Grande C, Villanueva MJ, Huidobro G, Casal J. Docetaxel-induced
interstitial pneumonitis following non-small-cell lung cancer treat-
ment. Clin Transl Oncol 2007; 9: 578-81.
[28] Akira M, Ishikawa H, Yamamoto S. Drug-induced pneumonitis:
thin-section CT findings in 60 patients. Radiology 2002; 224: 852-
60.
[29] Epler GR. Drug-induced bronchiolitis obliterans organizing pneu-
monia. Clin Chest Med 2004; 25: 89-94.
[30] Epler G. Bronchiolitis obliterans organizing pneumonia (BOOP),
25 years: a variety of causes, but what are the treatment options?
Expert Rev Respir Med 2011; 5: 353-61.
[31] Takatani K, Miyazaki E, Nureki S, et al. High-resolution computed
tomography patterns and immunopathogenetic findings in drug-
induced pneumonitis. Respir Med 2008; 102: 892-8.
[32] Cottin V, Cordier JF. Eosinophilic pneumonias. Allergy 2005; 60:
841-57.
[33] Huggins JT, Sahn SA. Drug-induced pleural disease. Clin Chest
Med 2004; 25: 141-53.
[34] Morelock SY, Sahn SA. Drugs and the pleura. Chest 1999; 116(1):
212-21.
[35] De Vuyst P, Pfitzenmeyer P, Camus P. Asbestos, ergot drugs and
the pleura. Eur Respir J 1997; 10: 2695-98.
[36] Ozkan M, Dweik RA, Ahmad M. Drug-induced lung disease.
Cleve Clin J Med 2001; 68(9): 782-5, 789-95.
[37] Brown JR, Skarin AT. Clinical mimics of lymphoma. Oncologist
2004; 9(4): 406-16.
[38] Christian JB, Finkle JK, Ky B, et al. Cardiac imaging approaches
to evaluate drug-induced myocardial dysfunction. Am Heart J
2012; 164: 846-55.
[39] Ottervanger JP, Wilson JH, Stricker BH. Drug-induced chest pain
and myocardial infarction. Reports to a national centre and review
of the literature. Eur J Clin Pharmacol 1997; 53: 105-10.
[40] Maisch B, Seferovi PM, Risti AD, et al. Task Force on the Diag-
nosis and Management of Pricardial Diseases of the European So-
ciety of Cardiology. Guidelines on the diagnosis and management
of pericardial diseases executive summary. The Task force on the
diagnosis and management of pericardial diseases of the European
society of cardiology. Eur Heart J 2004; 25: 587-610.
[41] Krishnan AS, Babar JL, Gopalan D. Imaging of congenital and
acquired disorders of the pulmonary artery. Curr Probl Diagn Ra-
diol 2012; 41: 165-78.
[42] Shanbhogue AK, Virmani V, Vikram R, et al. Spectrum of medica-
tion-induced complications in the abdomen: role of cross-sectional
imaging. AJR Am J Roentgenol 2011; 197: W286-94.
[43] Ganeshan DM, Salem U, Viswanathan C. Complications of on-
cologic therapy in the abdomen and pelvis: a review. Abdom Imag-
ing 2013; 38: 1-21.
[44] Biour M, Poupon R, Grange JD, Chazouillères O, Levy VG, Bodin
F. Drug hepatotoxicity. Actualization of a data bank of hepatic in-
juries and related drugs. Cheymol G. Gastroenterol Clin Biol 1991;
15: 64-78.
[45] Larrey D. Epidemiology and individual susceptibility to adverse
drug reactions affecting the liver. Semin Liver Dis 2002; 22: 145-
55.
[46] Sgro C, Clinard F, Ouazir K, Chanay H, Allard C, Guilleminet C,
et al. Incidence of drug-induced hepatic injuries: a French popula-
tion-based study. Hepatology 2002; 36: 451-55.
[47] Andrade RJ, Lucena MI, Fernández MC, et al. Drug induced Liver
Injury: An Analysis of 461 Incidences Submitted to the Spanish
Registry Over a 10- year Period. Gastroenterology 2005; 129: 512-
21.
[48] Crespo Pérez L, Moreira Vicente V, Cano Ruiz A, Gobernado
Serrano JM, Cobo Ibañez N, Milicua Salamero JM. Anticonvulsant
hypersensitivity syndrome: an entity to be remembered. Gastroen-
terol Hepatol 2009; 32: 687-92.
[49] Jha P, Poder L, Wang ZJ. Radiologic mimics of cirrhosis. AJR Am
J Roentgenol 2010; 194: 993-9.
[50] Torrisi JM, Schwartz LH, Gollub MJ, Ginsberg MS, Bosl GJ, Hri-
cak H. CT findings of chemotherapy-induced toxicity: what radi-
ologists need to know about the clinical and radiologic manifesta-
tions of chemotherapy toxicity. Radiology 2011; 258: 41-56.
[51] Gupta AA, Kim DC, Krinsky GA, Lee VS. CT and MRI of cirrho-
sis and its mimics. AJR Am J Roentgenol 2004; 183: 1595-601.

36 Current Medical Imaging Reviews, 2015, Vol. 11, No. 1 Baleato-González et al.
[52] Begriche K, Massart J, Robin MA, Borgne-Sanchez A, Fromenty
B. Drug-induced toxicity on mitochondria and lipid metabolism:
Mechanistic diversity and deleterious consequences for the liver. J
Hepatol 2011; 54: 773-94.
[53] Markos J, Veronese ME, Nicholson MR, McLean S, Shevland JE.
Value of hepatic computerized tomographic scanning during amio-
darone therapy. Am J Cardiol 1985; 56: 89-92.
[54] Desser TS, Sze DY, Jeffrey RB. Imaging and intervention in the
hepatic veins. AJR Am J Roentgenol 2003; 180: 1583-91.
[55] Kapp N, Curtis KM. Hormonal contraceptive use among women
with liver tumors: a systematic review. Contraception 2009; 80:
387-90.
[56] Ichikawa T, Federle MP, Grazioli L, Nalesnik M. Hepatocellular
adenoma: multiphasic CT and histopathologic findings in 25 pa-
tients. Radiology 2000; 214: 861-8.
[57] Bouyn CI, Leclere J, Raimondo G. Hepatic focal nodular hyperpla-
sia in children previously treated for a solid tumor. Incidence, risk
factors, and outcome. Cancer 2003; 97: 3107-13.
[58] Junewick J, Mitchell D. Focal nodular hyperplasia in oncology
patients. Pediatr Radiol 2006; 36: 464.
[59] Kirejczyk WM, Crowe HM, Mackay IM, Quintiliani R, Cronin EB.
Disappearing "gallstones": biliary pseudolithiasis complicating cef-
triaxone therapy. AJR Am J Roentgenol 1992; 159: 329-30.
[60] Biour M, Daoud H, Ben Salem C. Drug-induced pancreatitis. Sec-
ond edition of the bibliographic database of pancreatitis related to
drugs. Gastroenterol Clin Biol 2005; 29: 353-9.
[61] Vinklerová I, Procházka M, Procházka V, Urbánek K. Incidence,
severity, and etiology of drug-induced acute pancreatitis. Dig Dis
Sci 2010; 55: 2977-81.
[62] Farcas A, Bojita M. Adverse drug reactions in clinical practice: a
causality assessment of a case of drug-induced pancreatitis. J Gas-
trointestin Liver Dis 2009; 18: 353-8.
[63] Tenner S. Drug-induced acute pancreatitis: underdiagnosis and
overdiagnosis. Dig Dis Sci 2010; 55: 2706-8.
[64] Choi JS, Lim JS, Kim H, et al. Colonic pseudoobstruction: CT
findings. AJR Am J Roentgenol 2008; 190: 1521-6.
[65] Laine L, Ahnen D, Mcclain C, Solcia E, Walsh JH. Review article:
potential gastrointestinal effects of long-term acid suppression with
proton pump inhibitors. Aliment Pharmacol Ther 2000; 14: 651–
68.
[66] Scarpignato C, Hunt RH. Nonsteroidal antiinflammatory drug-
related injury to the gastrointestinal tract: clinical picture, patho-
genesis, and prevention. Gastroenterol Clin North Am 2010; 39:
433-64.
[67] Gore RM, Levine MS, Ghahremani GG. Drug-induced disorders of
the stomach and duodenum. Abdom Imaging 1999; 24: 9-16
[68] Cronin CG, O'Connor M, Lohan DG, et al. Imaging of the gastroin-
testinal complications of systemic chemotherapy. Clin Radiol 2009;
64: 724-33.
[69] Shafi MA, Bresalier RS. The gastrointestinal complications of
oncologic therapy. Gastroenterol Clin North Am 2010; 39629-647.
[70] Cappell MS. Colonic toxicity of administered drugs and chemicals.
Am J Gastroenterol 2004; 99: 1175-90.
[71] Thoeni RF, Cello JP. CT imaging of colitis. Radiology 2006; 240:
623-38.
[72] Rha SE, Ha HK, Lee SH, et al. CT and MR imaging findings of
bowel ischemia from various primary causes. Radiographics 2000;
20: 29-42.
[73] Heller MT, Khanna V. Cross-sectional imaging of acute abdominal
conditions in the oncologic patient. Emerg Radiol 2011; 18: 417-
428.
[74] Zissin R, Ellis M, Gayer G. The CT findings of abdominal antico-
agulant-related hematomas. Semin Ultrasound CT MR 2006; 27:
117-25.
[75] Laing CJ, Tobias T, Rosenblum DI, Banker WL, Tseng L,
Tamarkin SW.Acute gastrointestinal bleeding: emerging role of
multidetector CT angiography and review of current imaging tech-
niques. Radiographics 2007; 27: 1055-70.
[76] Marmery H, Mirvis SE. Angiotensin-converting enzyme inhibitor-
induced visceral angioedema. Clin Radiol 2006; 61: 979-82.
[77] Scheirey CD, Scholz FJ, Shortsleeve MJ, Katz DS Angiotensin-
converting enzyme inhibitor-induced small-bowel angioedema:
clinical and imaging findings in 20 patients. AJR Am J Roentgenol
2011; 197: 393-8.
[78] Ramachandran I, Sinha R, Rodgers P. Pseudomembranous colitis
revisited: spectrum of imaging findings. Clin Radiol 2006; 61: 535-
44.
[79] Loh AH, Cohen AH. Drug-induced kidney disease-pathology and
current concepts. Ann Acad Med Singapore 2009; 38: 240-50.
[80] Kodner CM, Kudrimoti A. Diagnosis and management of acute
interstitial nephritis. Am Fam Physician 2003; 67: 2527-34.
[81] Lithium Nephrotoxicity: A Progressive Combined Glomerular and
Tubulointerstitial Nephropathy. J Am Soc Nephrol 2000; 11: 1439–
48.
[82] Di Salvo DN, Park J, Laing FC. Lithium nephropathy: unique
sonographic findings. J Ultrasound Med 2012; 31: 637-44.
[83] Roque A, Herédia V, Ramalho M, et al. MR findings of lithium-
related kidney disease: preliminary observations in four patients.
Abdom Imaging 2012; 37: 140-6.
[84] Kim YG, Kim B, Kim MK, et al. Medullary nephrocalcinosis asso-
ciated with long-term furosemide abuse in adults. Nephrol Dial
Transplant 2001; 16: 2303-9.
[85] Matlaga BR, Shah OD, Assimos DG. Drug-induced urinary calculi.
Rev Urol 2003; 5: 227-31.
[86] Schwartz BF, Schenkman N, Armenakas NA, Stoller ML. Imaging
characteristics of indinavir calculi. J Urol 1999; 161: 1085-7.
[87] McCarville MB, Hoffer FA, Gingrich JR, Jenkins JJ 3rd. Imaging
findings of hemorrhagic cystitis in pediatric oncology patients. Pe-
diatr Radiol 2000; 30: 131-8.
[88] Ascher SM, Imaoka I, Lage JM. Tamoxifen-induced uterine ab-
normalities: the role of imaging. Radiology 2000; 214: 29-38.
[89] Kim IY, Lee BH. Ovarian hyperstimulation syndrome. US and CT
appearances. Clin Imaging 1997; 21: 284-6.
[90] Cronin CG, Lohan DG, Blake MA, Roche C, McCarthy P, Murphy
JM. Retroperitoneal fibrosis: a review of clinical features and imag-
ing findings. AJR Am J Roentgenol 2008; 191: 423-31.
[91] Sidhu HS, Venkatanarasimha N, Bhatnagar G, Vardhanabhuti V,
Fox BM, Suresh SP. Imaging features of therapeutic drug-induced
musculoskeletal abnormalities. Radiographics 2012; 32: 105-27.
[92] Pack AM, Gidal B, Vazquez B. Bone disease associated with
antiepileptic drugs. Cleve Clin J Med 2004; 71(Suppl 2): S42-48.
[93] D'Erasmo E, Ragno A, Raejntroph N, Pisani D. Drug-induced
osteomalacia. Recenti Prog Med 1998; 89: 529-33.
[94] Reginato AJ, Coquia JA. Musculoskeletal manifestations of osteo-
malacia and rickets. Best Pract Res Clin Rheumatol 2003; 17:
1063-80.
[95] Reginato AJ, Falasca GF, Pappu R, McKnight B, Agha A. Muscu-
loskeletal manifestations of osteomalacia: report of 26 cases and
literature review. Semin Arthritis Rheum 1999; 28: 287-304.
[96] Weinstein RS. Glucocorticoid-induced osteoporosis and osteone-
crosis. Endocrinol Metab Clin North Am 2012; 41: 595-611.
[97] Mazziotti G, Canalis E, Giustina A. Drug-induced osteoporosis:
mechanisms and clinical implications. Am J Med 2010; 123: 877-
84.
[98] Woo SB, Hellstein JW, Kalmar JR. Narrative review: BPs and
osteonecrosis of the jaws. Ann Intern Med 2006; 144: 753-61.
[99] Owczarek J, Jasi ska M, Orszulak-Michalak D. Drug-induced
myopathies. An overview of the possible mechanisms. Pharmacol
Rep 2005; 57: 23-34.
[100] Schulze M, Kötter I, Ernemann U, Fenchel M, Tzaribatchev N,
Claussen CD, Horger M.). MRI findings in inflammatory muscle
diseases and their noninflammatory mimics. AJR Am J Roentgenol
2009; 192: 1708-16.
[101] Peters SA, Kley R, Tegenthoff M, Vorgerd M, Nicolas V, Heyer
CM. MRI in lipid-lowering agent-associated myopathy: a retro-
spective review of 21 cases. AJR Am J Roentgenol 2010; 194:
W323-8.
[102] Hohenegger M. Drug induced rhabdomyolysis. Curr Opin Pharma-
col 2012; 12: 335-9.
[103] Ruggeri EM, Cecere FL, Moscetti L, Doni L, Padalino D, Di Co-
stanzo F. Severe rhabdomyolysis during sunitinib treatment of me-
tastatic renal cell carcinoma. A report of two cases. Ann Oncol
2010; 21: 1926-7.
[104] Kaleagasioglu F, Olcay E. Fluoroquinolone-induced tendinopathy:
etiology and preventive measures. Tohoku J Exp Med 2012; 226:
251-8.

Imaging in Drug Side Effects Current Medical Imaging Reviews, 2015, Vol. 11, No. 1 37
[105] Giralt M, Domingo P, Villarroya F. Adipose tissue biology and
HIV-infection. Best Pract Res Clin Endocrinol Metab 2011; 25:
487-99.
[106] Villarroya F, Domingo P, Giralt M. Drug-induced lipotoxicity:
lipodystrophy associated with HIV-1 infection and antiretroviral
treatment. Biochim Biophys Acta 2010; 1801: 392-9.
[107] Kyrle PA, Eichinger S. Deep vein thrombosis. Lancet 2005; 365:
1163-74.
[108] Radi M, Martinovi Kaliterna D, Radi J Drug-induced vasculitis:
a clinical and pathological review. Neth J Med 2012; 70: 12-7.
Received: September 08, 2014 Revised: November 04, 2014 Accepted: November 15, 2015





























