Embed Size (px)
Citation preview

Mechanisms of Ageing and Development 133 (2012) 20–29
Impairment of the ABCA1 and SR-BI-mediated cholesterol efflux pathways andHDL anti-inflammatory activity in Alzheimer’s disease
Abdelouahed Khalil a,b,*, Hicham Berrougui a,c, Graham Pawelec d, Tamas Fulop a,b
a Research Centre on Aging, University of Sherbrooke, Sherbrooke, Quebec, Canadab Geriatric Service, Department of Medicine, University of Sherbrooke, Sherbrooke, Quebec, Canadac Department of Biology, University Sultan Moulay Slimane, Beni Mellal, Moroccod Center for Medical Research, University of Tubingen, Tubingen, Germany
A R T I C L E I N F O
Article history:
Received 31 August 2011
Received in revised form 20 November 2011
Accepted 29 November 2011
Available online 9 December 2011
Keywords:
Alzheimer’s disease
Cholesterol efflux
HDL
ABCA1
SR-BI
Anti-inflammatory activity
A B S T R A C T
The aim of our study was to investigate the effect of Alzheimer’s disease (AD) on the cholesterol efflux
capacity and anti-inflammatory activity of HDL. HDL and apoA-I were isolated from 20 healthy subjects
and from 39 AD patients. Our results showed that serum- and HDL-mediated cholesterol efflux is
significantly impaired in AD patients. This impairment of serum and HDL cholesterol efflux capacity was
significantly inversely correlated to the AD severity as evaluated by MMSE scores. Results obtained from
SR-BI-enriched Fu5AH and ABCA1-enriched J774 cells revealed that AD impaired the interaction of HDL
and apoA-I with both the ABCA1 transporter and SR-BI receptor. Purified apoA-I from AD patients also
failed to remove free excess cholesterol from ABCA1-enriched J774 macrophages. Interestingly, the
decrease in plasma a-tocopherol content and the increase in MDA formation and HDL relative
electrophoretic mobility indicated that AD patients had higher levels of oxidative stress. The anti-
inflammatory activity of HDL was also significantly lower in AD patients as measured by the level of
ICAM-1 expression. In conclusion, our study provides evidence for the first time that the functionality of
HDL is impaired in AD and that this alteration might be caused by AD-associated oxidative stress and
inflammation.
� 2011 Elsevier Ireland Ltd. All rights reserved.
Contents lists available at SciVerse ScienceDirect
Mechanisms of Ageing and Development
jo ur n al ho mep ag e: www .e lsev ier . c om / lo cate /m ec hag ed ev
1. Introduction
Alzheimer’s disease (AD), the major cause of dementias, is aprogressive neurodegenerative condition that impairs basiccognitive functions, primarily memory (Selkoe, 1991). AD, whichphenotypically manifests as cognitive deficits, exhibits pathologictraits suggestive of a systemic disorder. It is characterized by theoverproduction and deposition of b-amyloid (Ab) peptides in thebrain. Ab peptides are derived from the proteolytic cleavage ofamyloid precursor protein (APP).
There is a widely shared view among AD investigators that theamyloid hypothesis best describes the pathogenic cascade thatultimately leads to the neuronal degeneration that results in clinicaldementia. The most persuasive evidence comes from studies ofdamaged brains of patients in the late stages of AD and from animalstudies that mimic the hereditary forms of early-onset dementia.Despite this impressive body of knowledge, we still do not know theexact cause of AD and thus lack the means to arrest or prevent it.
* Corresponding author at: Research Centre on Aging, 1036, Belvedere South,
Sherbrooke, Quebec, Canada J1H 4C4. Tel.: +1 819 829 7131; fax: +1 819 829 7141.
E-mail address: [email protected] (A. Khalil).
0047-6374/$ – see front matter � 2011 Elsevier Ireland Ltd. All rights reserved.
doi:10.1016/j.mad.2011.11.008
Cholesterol forms an essential component of the cell membraneand plays a crucial role in the development and maintenance ofneuronal plasticity and function (Pfrieger, 2003). There is strongevidence that alterations in lipid metabolism play an importantrole in the pathogenesis of AD (Hartmann, 2001). More specifically,a significant number of studies have shown that high serum totalcholesterol is a risk factor for mild cognitive impairment anddementia (Frisardi et al., 2010; Panza et al., 2009). Epidemiological(Wolozin et al., 2000) and experimental (Refolo et al., 2001) studieshave shown that hypercholesterolemia is an early risk factor for ADand that the use of cholesterol-lowering drugs is associated with adecrease in the prevalence of Ab pathology (Refolo et al., 2000).High membrane cholesterol levels, especially in lipid rafts,accelerate the production of Ab by shifting APP metabolism froma- to b-cleavage products, thus increasing the ratio of insoluble Ab(Cordy et al., 2003; Mielke et al., 2010; Simons et al., 1998). On theother hand, cholesterol depletion inhibits Ab production andb-secretase activity while replenishment of cholesterol to thenormal level restores non-amyloidogenic Ab production (Wahrleet al., 2002) and stimulates a-secretase activity (Kalvodova et al.,2005). In contrast, Abad-Rodriguez et al. (2004) reported that thephysiological loss of cholesterol in hippocampal neurons enhancesAb production. These studies provide some evidence that
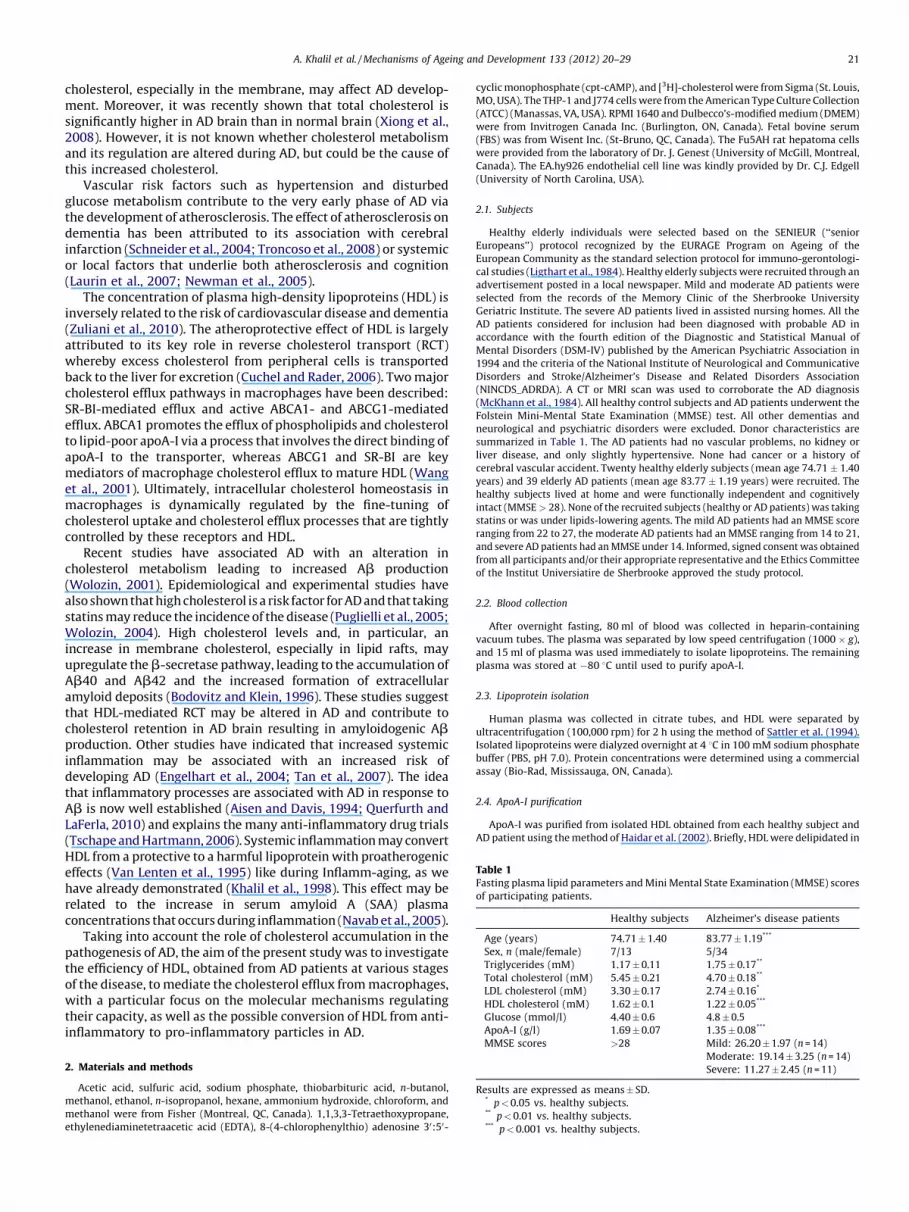
Table 1Fasting plasma lipid parameters and Mini Mental State Examination (MMSE) scores
of participating patients.
Healthy subjects Alzheimer’s disease patients
Age (years) 74.71 � 1.40 83.77 � 1.19***
Sex, n (male/female) 7/13 5/34
Triglycerides (mM) 1.17 � 0.11 1.75 � 0.17**
Total cholesterol (mM) 5.45 � 0.21 4.70 � 0.18**
LDL cholesterol (mM) 3.30 � 0.17 2.74 � 0.16*
HDL cholesterol (mM) 1.62 � 0.1 1.22 � 0.05***
Glucose (mmol/l) 4.40 � 0.6 4.8 � 0.5
ApoA-I (g/l) 1.69 � 0.07 1.35 � 0.08***
MMSE scores >28 Mild: 26.20 � 1.97 (n = 14)
Moderate: 19.14 � 3.25 (n = 14)
Severe: 11.27 � 2.45 (n = 11)
Results are expressed as means � SD.* p < 0.05 vs. healthy subjects.** p < 0.01 vs. healthy subjects.*** p < 0.001 vs. healthy subjects.
A. Khalil et al. / Mechanisms of Ageing and Development 133 (2012) 20–29 21
cholesterol, especially in the membrane, may affect AD develop-ment. Moreover, it was recently shown that total cholesterol issignificantly higher in AD brain than in normal brain (Xiong et al.,2008). However, it is not known whether cholesterol metabolismand its regulation are altered during AD, but could be the cause ofthis increased cholesterol.
Vascular risk factors such as hypertension and disturbedglucose metabolism contribute to the very early phase of AD viathe development of atherosclerosis. The effect of atherosclerosis ondementia has been attributed to its association with cerebralinfarction (Schneider et al., 2004; Troncoso et al., 2008) or systemicor local factors that underlie both atherosclerosis and cognition(Laurin et al., 2007; Newman et al., 2005).
The concentration of plasma high-density lipoproteins (HDL) isinversely related to the risk of cardiovascular disease and dementia(Zuliani et al., 2010). The atheroprotective effect of HDL is largelyattributed to its key role in reverse cholesterol transport (RCT)whereby excess cholesterol from peripheral cells is transportedback to the liver for excretion (Cuchel and Rader, 2006). Two majorcholesterol efflux pathways in macrophages have been described:SR-BI-mediated efflux and active ABCA1- and ABCG1-mediatedefflux. ABCA1 promotes the efflux of phospholipids and cholesterolto lipid-poor apoA-I via a process that involves the direct binding ofapoA-I to the transporter, whereas ABCG1 and SR-BI are keymediators of macrophage cholesterol efflux to mature HDL (Wanget al., 2001). Ultimately, intracellular cholesterol homeostasis inmacrophages is dynamically regulated by the fine-tuning ofcholesterol uptake and cholesterol efflux processes that are tightlycontrolled by these receptors and HDL.
Recent studies have associated AD with an alteration incholesterol metabolism leading to increased Ab production(Wolozin, 2001). Epidemiological and experimental studies havealso shown that high cholesterol is a risk factor for AD and that takingstatins may reduce the incidence of the disease (Puglielli et al., 2005;Wolozin, 2004). High cholesterol levels and, in particular, anincrease in membrane cholesterol, especially in lipid rafts, mayupregulate the b-secretase pathway, leading to the accumulation ofAb40 and Ab42 and the increased formation of extracellularamyloid deposits (Bodovitz and Klein, 1996). These studies suggestthat HDL-mediated RCT may be altered in AD and contribute tocholesterol retention in AD brain resulting in amyloidogenic Abproduction. Other studies have indicated that increased systemicinflammation may be associated with an increased risk ofdeveloping AD (Engelhart et al., 2004; Tan et al., 2007). The ideathat inflammatory processes are associated with AD in response toAb is now well established (Aisen and Davis, 1994; Querfurth andLaFerla, 2010) and explains the many anti-inflammatory drug trials(Tschape and Hartmann, 2006). Systemic inflammation may convertHDL from a protective to a harmful lipoprotein with proatherogeniceffects (Van Lenten et al., 1995) like during Inflamm-aging, as wehave already demonstrated (Khalil et al., 1998). This effect may berelated to the increase in serum amyloid A (SAA) plasmaconcentrations that occurs during inflammation (Navab et al., 2005).
Taking into account the role of cholesterol accumulation in thepathogenesis of AD, the aim of the present study was to investigatethe efficiency of HDL, obtained from AD patients at various stagesof the disease, to mediate the cholesterol efflux from macrophages,with a particular focus on the molecular mechanisms regulatingtheir capacity, as well as the possible conversion of HDL from anti-inflammatory to pro-inflammatory particles in AD.
2. Materials and methods
Acetic acid, sulfuric acid, sodium phosphate, thiobarbituric acid, n-butanol,
methanol, ethanol, n-isopropanol, hexane, ammonium hydroxide, chloroform, and
methanol were from Fisher (Montreal, QC, Canada). 1,1,3,3-Tetraethoxypropane,
ethylenediaminetetraacetic acid (EDTA), 8-(4-chlorophenylthio) adenosine 30:50-
cyclic monophosphate (cpt-cAMP), and [3H]-cholesterol were from Sigma (St. Louis,
MO, USA). The THP-1 and J774 cells were from the American Type Culture Collection
(ATCC) (Manassas, VA, USA). RPMI 1640 and Dulbecco’s-modified medium (DMEM)
were from Invitrogen Canada Inc. (Burlington, ON, Canada). Fetal bovine serum
(FBS) was from Wisent Inc. (St-Bruno, QC, Canada). The Fu5AH rat hepatoma cells
were provided from the laboratory of Dr. J. Genest (University of McGill, Montreal,
Canada). The EA.hy926 endothelial cell line was kindly provided by Dr. C.J. Edgell
(University of North Carolina, USA).
2.1. Subjects
Healthy elderly individuals were selected based on the SENIEUR (‘‘senior
Europeans’’) protocol recognized by the EURAGE Program on Ageing of the
European Community as the standard selection protocol for immuno-gerontologi-
cal studies (Ligthart et al., 1984). Healthy elderly subjects were recruited through an
advertisement posted in a local newspaper. Mild and moderate AD patients were
selected from the records of the Memory Clinic of the Sherbrooke University
Geriatric Institute. The severe AD patients lived in assisted nursing homes. All the
AD patients considered for inclusion had been diagnosed with probable AD in
accordance with the fourth edition of the Diagnostic and Statistical Manual of
Mental Disorders (DSM-IV) published by the American Psychiatric Association in
1994 and the criteria of the National Institute of Neurological and Communicative
Disorders and Stroke/Alzheimer’s Disease and Related Disorders Association
(NINCDS_ADRDA). A CT or MRI scan was used to corroborate the AD diagnosis
(McKhann et al., 1984). All healthy control subjects and AD patients underwent the
Folstein Mini-Mental State Examination (MMSE) test. All other dementias and
neurological and psychiatric disorders were excluded. Donor characteristics are
summarized in Table 1. The AD patients had no vascular problems, no kidney or
liver disease, and only slightly hypertensive. None had cancer or a history of
cerebral vascular accident. Twenty healthy elderly subjects (mean age 74.71 � 1.40
years) and 39 elderly AD patients (mean age 83.77 � 1.19 years) were recruited. The
healthy subjects lived at home and were functionally independent and cognitively
intact (MMSE > 28). None of the recruited subjects (healthy or AD patients) was taking
statins or was under lipids-lowering agents. The mild AD patients had an MMSE score
ranging from 22 to 27, the moderate AD patients had an MMSE ranging from 14 to 21,
and severe AD patients had an MMSE under 14. Informed, signed consent was obtained
from all participants and/or their appropriate representative and the Ethics Committee
of the Institut Universiatire de Sherbrooke approved the study protocol.
2.2. Blood collection
After overnight fasting, 80 ml of blood was collected in heparin-containing
vacuum tubes. The plasma was separated by low speed centrifugation (1000 � g),
and 15 ml of plasma was used immediately to isolate lipoproteins. The remaining
plasma was stored at �80 8C until used to purify apoA-I.
2.3. Lipoprotein isolation
Human plasma was collected in citrate tubes, and HDL were separated by
ultracentrifugation (100,000 rpm) for 2 h using the method of Sattler et al. (1994).
Isolated lipoproteins were dialyzed overnight at 4 8C in 100 mM sodium phosphate
buffer (PBS, pH 7.0). Protein concentrations were determined using a commercial
assay (Bio-Rad, Mississauga, ON, Canada).
2.4. ApoA-I purification
ApoA-I was purified from isolated HDL obtained from each healthy subject and
AD patient using the method of Haidar et al. (2002). Briefly, HDL were delipidated in

A. Khalil et al. / Mechanisms of Ageing and Development 133 (2012) 20–2922
an acetone–ethanol solution, and the protein fractions were separated using two
Sephacryl S-200 columns (Amersham Biosciences AB, Uppsala, Sweden). Pure apoA-
I fractions were pooled, dialyzed in 100 mM NH4HCO3, lyophilized, and re-
suspended in PBS.
2.5. Cell cultures
Human THP-1 monocytes and J774 macrophages were grown in RPMI 1640, and
Fu5AH rat hepatoma cells were grown in DMEM. The media were supplemented
with 10% heat-inactivated fetal bovine serum (FBS), 50 mM b-mercaptoethanol
(THP-1 only), 2 mM L-glutamine, 100 U/ml penicillin, and 1.5 mg/ml glucose in a
humidified atmosphere (5% CO2 and 95% air) at 37 8C.
The THP-1 monocytes (1 � 106 cells/cm2 in 6- or 12-well plates) were incubated
in RPMI-FBS containing 100 mM phorbol 12-myristic 13-acetate (PMA) for 96 h to
induce differentiation into adherent macrophage-like cells.
EA.hy926 cells which, of all immortalized human endothelial cell lines, are the
most similar to HUVEC, were used to avoid the variability and time and effort
associated with primary isolations (Lidington et al., 1999). The cells were cultured
in DMEM supplemented with 10% FBS, 5 mM hypoxanthine, 20 mM aminopterin,
0.8 mM thymidine, and 100 mg/ml penicillin/streptomycin. The EA.hy926 cells
were maintained in a 5% CO2 atmosphere at 37 8C, and were passaged every five
days at a ratio of 1:8. They were used two days after reaching confluence.
2.6. Cholesterol efflux measurements
THP-1 macrophages were incubated in fresh growth medium containing [3H]-
cholesterol (0.2 mCi/ml) for 48 h while J774 and Fu5AH cells were loaded in [3H]-
cholesterol (2 mCi/ml) for 24 h. Labeled macrophages were washed and incubated
in serum-free medium containing 1% BSA for an additional 12 h for equilibration.
The effect of AD on ABCA1- and SR-BI-mediated cholesterol efflux was studied using
ABCA1-enriched J774 and Fu5AH macrophages (a stable cell line that exhibits a high
level of SR-BI-expression; de la Llera-Moya et al., 1999) respectively.
To produce ABCA1-enriched cells, [3H]-cholesterol-loaded J774 macrophages
were equilibrated in DMEM containing 1% BSA and 0.3 mM 8-Br-cAMP for 12 h
(Hajj Hassan et al., 2005). The macrophages were then washed and incubated with
various cholesterol acceptors. The THP-1 and Fu5AH cells were incubated with 5%
plasma or 50 mg/ml HDL for 24 h whereas, ABCA1-enriched J774 macrophages were
incubated with 5% plasma or 25 mg/ml purified apoA-I for 24 h. The effects of
plasma from AD patients or controls were compared.
The cells were collected by centrifugation (350 � g for 10 min) and were lysed in
0.1 M NaOH. The counts per minute (cpm) in the supernatants and cell lysates were
determined separately using a liquid scintillation counter (model 1600 TR; Packard
Instrument Company, Meriden, CT, USA). Cholesterol efflux was measured by
determining the percentage of radiolabeled cholesterol released (% cholesterol efflux)
using the following formula: (cpm in supernatant/cpm in cells + supernatant) � 100.
2.7. HDL electrophoretic mobility
The electrophoretic mobility of HDL was used as an indication of apoA-I
oxidation and was measured using a Titan gel lipoprotein electrophoretic system
(Helena Laboratories, Beaumont, TX, USA). Samples (2 ml) were separated using
0.6% agarose gels in barbital buffer (pH 8.6) (Helena Laboratories, Montreal, QC,
Canada) at 80 V for 45 min. The gels were then oven-dried at 75 8C and stained with
0.1% (w/v) Fat Red 7B in 95% methanol.
2.8. Lipid peroxidation assay
Lipid peroxidation in sera was assessed by measuring malondialdehyde (MDA)
levels using an HPLC coupled to a fluorescence detector, as previously described by
Agarwal and Chase (2002).
2.9. Vitamin E assay
Endogenous serum vitamin E was assayed as a-tocopherol by reversed-phase-
HPLC, electrochemical detection, and UV detection at l-292 nm, as previously
described (Khalil et al., 2000). a-Tocopherol was assayed on a Sephasil peptide
column (C18 5 mm ST 4.6/250, Pharmacia Biotech, Piscataway, NJ, USA). It was
eluted with methanol:ethanol:isopropanol (88:24:10, v/v/v) containing 20 mM
lithium perchlorate at a flow rate of 1 ml/min.
2.10. LCAT activity
HDL-associated LCAT activity (a-LCAT) was assayed using Calbiochem
fluorometric LCAT assay kits (EMD Bioscience, San Diego, CA. USA) according to
the manufacturer’s protocol. Briefly, HDL were incubated with a fluorescent
substrate that fluoresces at 470 nm. When hydrolyzed by LCAT, a monomer is
released that fluoresces at 390 nm. LCAT mediates the formation of cholesteryl
esters in human plasma by transferring an acyl chain from the sn-2 position of
phosphatidylcholine to cholesterol. LCAT activity is expressed as the change in the
470/390 ratio.
2.11. ICAM-1 expression
The cell surface expression of the adhesion molecule ICAM-1 was analyzed by
flow cytometry. The cells were incubated for 24 h in the absence or presence of
10 ng/ml TNFa or of HDL isolated from the patients at various stages of AD. The cells
were washed with PBS and trypsinized for 2 min at 37 8C. The trypsin was
inactivated by adding medium containing 10% FBS. The cells were centrifuged
(2 min at 350 � g), incubated with a phycoerythrin-conjugated anti-ICAM-1 (1 mg/
106 cells) monoclonal antibody for 15 min at 25 8C, washed with PBS, and analyzed
using a FACS Calibur flow cytometer.
2.12. Statistical analysis
Values are expressed as means � standard deviations (SD). Mean values were
compared using the Mann–Whitney and one-way ANOVA tests. Pearson correlation
analyses were performed to assess possible associations. p-Values less than 0.05 were
considered significant. Statistical analyses were performed using Prism 5.0 version
software.
3. Results
Fifty-nine subjects were assigned to four groups depending ontheir state of health and the severity of their cognitive decline [onehealthy group and three groups with different stages of cognitivedecline (mild, moderate, and severe)]. Cognitive decline wasevaluated using the MMSE test. Subjects with MMSE values over 28were considered cognitively intact.
The biochemical parameters of the healthy subjects and ADpatients are summarized in Table 1. There was a significant decreasein fasting plasma LDL (p < 0.05), HDL (p < 0.001), total cholesterol(p < 0.01) and an increase of triglyceride (p < 0.01) levels in the ADpatients compared to the healthy subjects (Table 1). Plasma apoA-Iwas also significantly lower in the AD patients (1.69 � 0.07 comparedto 1.35 � 0.08, p < 0.001). 14 AD patients exhibited a mild cognitivedecline (MMSE = 26.20 � 1.97), 14 AD a moderate decline (MMSE =19.14 � 3.25), and 11 a severe decline (11.27 � 2.45).
To investigate the impact of AD on the reverse cholesteroltransport (RCT) process, we assessed the capacity of serum andHDL from the healthy controls or from AD patients to facilitatecholesterol efflux. As shown in Fig. 1A, the capacity of 5% serum tomediate cholesterol efflux from 3H-cholesterol-loaded THP-1macrophages was significantly lower in AD patients than inhealthy subjects. This effect was more pronounced when HDLparticles (50 mg/ml) were used, where a significant decrease(p < 0.05) in HDL-mediated cholesterol efflux in the AD patientscompared to healthy subjects was observed (Fig. 1B).
To gain more insight and clarify which of the cholesterol effluxpathways is affected by AD, we investigated the capacity of the SR-BI and ABCA1 pathways to mediate cholesterol efflux frommacrophages. To assess SR-BI-mediated efflux, we used Fu5AHrat hepatoma cells, which express high levels of SR-BI and lack afunctional ABCA1 (Attia et al., 2010). As shown in Fig. 1C and D, thecapacity of serum and HDL to mediate cholesterol efflux via SR-BIwas significantly impaired in the AD patients compared to thehealthy subjects.
We subsequently evaluated the capacity of serum and HDL tomediate cholesterol efflux as a function of the stage of AD(cognitive decline) as assessed by the MMSE test. The MMSE valueswere used to distribute the AD patients into mild, moderate, andsevere groups based on their cognitive state. There was asignificant negative correlation between the capacity of serumand HDL to mediate cholesterol efflux from THP1 macrophages andthe level of cognitive decline [r2 = 0.17, p = 0.002, and r2 = 0.11,p < 0.048, for serum and HDL, respectively, Fig. 2A and B].
The relationship between the capacity of serum to mediatecholesterol efflux and the level of cognitive decline varies as afunction of gender and age. The effect of MMSE on serum-mediatedcholesterol efflux was significant for men (r2 = 0.51, p < 0.032)(figure not shown), without any effect of age. However, the effect of

Fig. 1. Alterations in serum and HDL-mediated cholesterol efflux capacity in AD patients. THP-1 macrophages and Fu5AH hepatic cells were loaded with [3H]-cholesterol for
48 h. They were then washed and incubated for a further 24 h with (A and C) 5% serum or (B and D) 50 mg/ml HDL isolated from healthy subjects and AD patients. Results are
expressed as means � SD. *p < 0.05, **p < 0.01 vs. healthy subjects.
A. Khalil et al. / Mechanisms of Ageing and Development 133 (2012) 20–29 23
MMSE on serum-mediated cholesterol efflux disappeared whencontrolling for age in women. Interestingly, the capacity of serumto mediate cholesterol efflux from THP1 macrophages wasinversely correlated to age for women (r2 = 0.20, p < 0.03). Noage or gender differences were observed for HDL-mediatedcholesterol efflux from THP1 macrophages.
This negative correlation was stronger for HDL when Fu5AH cellswere used to measure cholesterol efflux [r2 = 0.09, p < 0.02, andr2 = 0.18, p = 0.01, for serum and HDL, respectively, Fig. 2C and D].No age or gender differences were observed for these two analyses.
To assess ABCA1-mediated cholesterol efflux, we used cAMPpre-treated J774 macrophages, which express high levels of ABCA1(Yancey et al., 2004). The ABCA1-mediated cholesterol effluxpathway is highly specific in terms of its interaction with apoA-Iand lipid-poor apoA-I (Attie et al., 2001), which led us to usepurified apoA-I rather than HDL to assess cholesterol efflux in thehealthy subjects and AD patients. No significant differences wereobserved when either serum or HDL from the healthy subjects andAD patients were used to measure cholesterol efflux from cAMP-upregulated 774 macrophages (results not shown). However,when purified apoA-I was used as a cholesterol acceptor, theamount of cholesterol effluxed by apoA-I purified from the plasmaof AD patients was significantly lower than that effluxed by apoA-Ipurified from the plasma of healthy subjects (p < 0.01) (Fig. 3A).Interestingly, there was a strong negative correlation between thecapacity of apoA-I to mediate cholesterol efflux and the stage ofcognitive decline (r2 = 0.38, p < 0.003, Fig. 3B).
To better understand the effect of AD severity on both HDL- andapoA-I-mediated cholesterol efflux, we investigated the oxidativestate of HDL by measuring the relative electrophoretic mobility(REM). The REM technique measures changes in the negativepotential of HDL, which can be caused by carbamylation, glycation,or the oxidative modification of HDL-associated proteins, princi-pally apoA-I. The REM of HDL from the AD patients was high thanthat of HDL from the healthy subjects (p < 0.01) (Table 2). Thiseffect was also associated with a significant increase in MDAformation (p < 0.05) and a decrease in plasma a-tocopherol levels(p < 0.01) (Table 2). In addition, the increase in the REM of HDLfrom the AD patients paralleled the severity of their cognitivedecline (Fig. 4 and Table 2).
In addition to apoA-I, which mediates the interaction withABCA1/ABCG1 and SR-BI, lecithin cholesterol acyl transferase(LCAT) is believed to be a key enzyme in the regulation of the RCTpathway. LCAT, by catalyzing the esterification of HDL freecholesterol, contributes to the maturation of HDL and thus theincrease in cholesterol efflux (Zannis et al., 2006). We measuredLCAT activity in plasma (a + b-LCAT) and HDL (a-LCAT) from thehealthy subjects and the AD patients. a-LCAT activity decreasedsignificantly as a function of the severity of the cognitive decline(Fig. 5A), whereas no effect was observed with serum LCAT.
Anti-inflammatory activity is a second protective property ofHDL. RCT and anti-inflammatory activity are intimately related.Inflammation is associated with the onset of various neurodegen-erative diseases, including AD. In the second part of the present

0102030400
20
40
60
80r2=0.17; p=0.0021
THP-1
MMSE
Serum-mediated
Cholesterolefflux(%),fromTHP-1
0102030400
20
40
60
80r2=0.11; p=0.048
THP-1
MMSE
MMSE MMSE
HDL-mediated
Cholesterolefflux(%),fromTHP-1
0102030400
20
40
60
80r2=0.09; p=0.028
Fu5AH
serum-mediated
Cholesterolefflux(%),fromFu5AH
0102030400
5
10
15
20
25r2=0.18; p=0.011
Fu5AH
HDL-mediated
Cholesterolefflux(%),fromFu5AH
A B
C D
Fig. 2. Correlation between serum and HDL-mediated cholesterol efflux capacity and the level of cognitive decline. THP-1 macrophages and Fu5AH hepatic cells were loaded
with [3H]-cholesterol for 48 h. [3H]-cholesterol loaded cells were incubated for 24 h with (A and C) 5% serum or (B and D) 50 mg/ml of HDL isolated from healthy subjects and
AD patients.
A. Khalil et al. / Mechanisms of Ageing and Development 133 (2012) 20–2924
study, we investigated the anti-inflammatory effect of HDL as afunction of AD severity. The anti-inflammatory effect of HDL wasevaluated by inhibiting ICAM-1 expression on EA.hy926 endothe-lial cells. HDL from the healthy subjects significantly reducedICAM-1 expression (Fig. 6A). However, the anti-inflammatoryeffect of HDL was significantly lower in AD patients (p < 0.01).
The measurement of soluble ICAM-1 in the plasma, which wasused as a circulating inflammatory marker, revealed higher levelsin AD patients than controls, consistent with increase ininflammation in the former (Fig. 6B). There was also a significantcorrelation between plasma ICAM-1 levels and the severity of thecognitive decline (Fig. 6C).
4. Discussion
AD is a neurodegenerative disease characterized by progressivememory loss leading to dementia, which in sporadic cases occurslate in life. Over the past decade, research has shown thatabnormalities in brain lipid metabolism are intimately related tothe pathogenesis of AD and vascular dementia (McGrowder et al.,2011). Atherosclerosis and AD both develop in parallel with agingand both share somewhat identical risk factors, including hyper-cholesterolemia (Arvanitakis et al., 2004). Singh-Manoux et al.showed that a decrease in HDL levels during a 5-year follow-upperiod was associated with a decline in memory (Singh-Manoux
et al., 2008). The putative neuroprotective effect of HDL has beenattributed to their involvement in the regulation of Ab proteinmetabolism and deposition in the brain and their antioxidant andanti-inflammatory properties (Singh-Manoux et al., 2008). Whilecholesterol metabolism in the brain is completely separated fromthat in the peripheral system, several studies have associated lowerHDL concentrations with a decreased risk of AD suggesting that AD isalso a systemic disease (Reitz et al., 2010). Unlike VLDL/LDL, HDL cancross the blood–brain barrier and deliver a small amount ofcholesterol from the periphery to the brain (Balazs et al., 2004). Onthe other hand, Ab, which is a key molecule in the pathogenesis ofAD, accelerates the transport of brain cholesterol to the peripheraltissues (Umeda et al., 2010). The efflux of cerebral cholesterol to thecirculatory system presumably occurs mainly by diffusion due to theconcentration gradient between the brain and the circulation(Umeda et al., 2010). Changes in the cholesterol balance of the entirebody may thus affect cholesterol homeostasis in the brain andimpair neuron integrity (Dietschy and Turley, 2001). In this context,the link between the capacity of HDL to maintain cholesterolhomeostasis through the RCT process and its relation to AD severityneeds to be investigated.
In the brain, the cholesterol homeostasis is maintained via itsconversion to 24-S-hydroxycholesterol (Bjorkhem and Meaney,2004), a molecule likely not produced outside the brain. The levelof 24-S-hydroxycholesterol in cerebrospinal fluid is increased in

Fig. 3. Impairment of the ABCA1-cholesterol efflux pathway in AD patients. (A)
Cholesterol efflux was measured in ABCA1-enriched J774 macrophages.
Macrophages were incubated for 4 h with 25 mg/ml of purified apoA-I from
healthy subjects and AD patients. Results are expressed as means � SD. *p < 0.05 vs.
healthy subjects. (B) Correlation between the capacity of purified apoA-I to mediate
cholesterol efflux and MMSE scores (r2 = 0.38, p < 0.003).
Fig. 4. HDL electrophoretic mobility. HDL extracted from (1) healthy subjects and
(2) mild, (3) moderate, and (4) severe cognitive decline AD patients were subjected
to electrophoresis on 0.6% agarose gels and stained with Fat Red 7B in 95%
methanol. Arrow indicates the starting point.
A. Khalil et al. / Mechanisms of Ageing and Development 133 (2012) 20–29 25
AD (Schonknecht et al., 2002) and in early stages of dementia(Schonknecht et al., 2002). Lutjohan et al. described an age-dependent net flux of 24-S-hydroxycholesterol from the humanbrain into the circulation and suggested that it could be ofimportance for cholesterol homeostasis in the brain (Lutjohannet al., 1996). However, the levels of 24-S-hydroxycholesterol in thecirculation may also be dependent to some extent on thetransporting capacity of the lipoproteins in the circulation.
HDL are a heterogeneous class of particles whose compositioninfluences their capacity to act as efficient lipid acceptors. Large
Table 2Measurement of HDL relative electrophoretic mobility (REM) and oxidative stress
markers in healthy and AD patients.
Healthy subjects Alzheimer’s disease patients
HDL-REM (cm) 1.78 � 0.044 2.13 � 0.06**
a-Tocopherol (mM) 37.28 � 3.45 27.75 � 2.32**
MDA (mM) 2.35 � 0.18 2.78 � 0.09*
Results are expressed as means � SEM.* p < 0.05 vs. healthy subjects.** p < 0.01 vs. healthy subjects.
Fig. 5. Decrease of a-LCAT activity in AD patients. (A) Bar graph depicting a-LCAT
activity (HDL-associated LCAT activity) in AD patients and healthy subjects. Results
are expressed as means � SD. ***p < 0.001. (B) Correlation between a-LCAT activity
and MMSE scores (r2 = 0.18, p = 0.036).

Fig. 6. HDL anti-inflammatory activities and plasma ICAM-1 levels in AD patients
and healthy subjects. (A) Flow cytometric analysis of ICAM-1 expression on
EA.hy926 endothelial cells after a 24-h incubation with HDL from AD patients
and healthy subjects. TNFa-unstimulated and stimulated cells were used as
negative and positive controls, respectively. Results are expressed as means � SD.
**p < 0.01, ***p < 0.001. (B) ELISA assessment of serum ICAM-1 concentrations (ng/
ml), in the AD patients and healthy subjects. Results are expressed as means � SD
(**p < 0.01). (C) Correlation between plasma circulating levels and MMSE scores
(r2 = 0.10, p = 0.028).
A. Khalil et al. / Mechanisms of Ageing and Development 133 (2012) 20–2926
phospholipid-enriched HDL (a-HDL) specifically exchange lipidswith scavenger receptor class B type I (SR-BI) (Yancey et al., 2003)and ABCG1 (Smith, 2006) receptors, while ABCA1 delivers bothphospholipids and cholesterol to apoA-I and small lipid-poor pre-b1 HDL (Baldan et al., 2009; Favari et al., 2004). This was the basisfor our idea of performing experiments in more than one cell typegiven that different cholesterol efflux pathways may be affected inAD. Our results showed that HDL from AD patients are less able tomediate cholesterol efflux than HDL from healthy subjects and thatthe decrease is significantly correlated with the severity of thecognitive decline. Since HDL from healthy subjects and AD patientswere used at the same concentrations (expressed as total proteincontent), the decrease in the capacity of HDL to mediatecholesterol efflux is likely not caused by a reduction in HDLconcentrations in AD patients but rather by a reduction in therefunctionality. This decreased cholesterol efflux, following thisdecreased HDL’s functionality, may then cause an accumulation ofcholesterol in the cells of AD patients, especially in lipid rafts andtherefore favoring the increased activity of b- and g-secretasesleading to the increased levels of amyloidogenic Ab responsible forthe oxidative stress and inflammation in AD. The next question waswhy HDL from AD patients are unable to extract intracellularcholesterol.
HDL-mediated cholesterol efflux is lower in diabetics (Borg-greve et al., 2003) and in subjects with familial HDL deficiency(Marcil et al., 1999) and has been associated with an alteration inHDL concentrations, distribution, composition, and structure. In aprevious study, we showed that the capacity of HDL to mediatecholesterol efflux was lower in elderly subjects (Berrougui et al.,2007) and we attributed this reduction to oxidative stressmodifications that develop with aging (Berrougui et al., 2007).Oxidative stress and a robust inflammation response are theearliest events in AD and are characteristic pathological featuresthat are most probably caused by the extracellular deposition ofAb protein (Nunomura et al., 2001; Weninger and Yankner, 2001).In the present study, we showed that oxidative stress is higher inAD patients than in healthy subjects based on a significantdecrease in plasma a-tocopherol levels and an increase in plasmaMDA concentrations and circulating ICAM-1 levels. Thus, theincreased oxidative stress found in AD patients may explain thesignificant decrease in the capacity of HDL from AD patients tomediate cholesterol efflux.
ApoA-I is a major protein component of HDL and is a key factorin the enhancement of HDL-mediated cholesterol efflux. ApoA-Ireacts specifically with ABCA1 to generate nascent HDL, which arethen enriched with esterified cholesterol by LCAT (activated byapoA-I) to form mature spherical HDL (Gu et al., 2010). ApoA-Ipurified from the plasma of the AD patients was significantly lesscapable of mediating cholesterol efflux via the ABCA1 transporter.This decrease was strongly and significantly inversely correlatedwith AD severity (r2 = 0.38, p < 0.003), suggesting that the changein HDL-mediated cholesterol efflux was due in large part to achange in the apoA-I/ABCA1 interaction in the presence of AD.While inflammatory conditions may affect apoA-I synthesis andHDL catabolism (Esteve et al., 2005), oxidative stress may alsoinduce oxidative modifications of apoA-I that affect its interactionwith ABCA1 transporters and reduce cholesterol efflux via thispathway (Berrougui et al., 2007). The increase in the electropho-retic mobility of HDL from the AD patients confirmed that apoA-Iundergoes oxidative modifications and may help explain thestrong negative significant correlation between the capacity ofpurified apoA-I to mediate cholesterol efflux via the ABCA1transporter and AD severity. This is further supported by the factthat there were no differences in ABCA-1 expression between ADand normal brains (Xiong et al., 2008). Nevertheless, ABCA1/apoA-I-mediated cholesterol efflux is only one of the three pathways

A. Khalil et al. / Mechanisms of Ageing and Development 133 (2012) 20–29 27
involved in the cholesterol exchange between HDL and peripheralcells. Factors other than changes to apoA-I may thus contribute toreducing HDL-mediated cholesterol efflux in AD patients,including the SR-BI and ABCG1 pathways and passive diffusion.Cholesterol exchanges via these pathways are dependent both onthe integrity of apoA-I and the biophysical structure andbiochemical composition of HDL (Berrougui et al., 2007). In fact,it was shown that ABCG-1 facilitates, by interacting with matureHDL, APP trafficking and in this way influences the secretaseactivities in membranes (Tansley et al., 2007). Our results showedthat there is a decrease in the capacity of both serum and HDL tomediate cholesterol efflux in AD patients, which suggests that thedecrease in HDL-mediated cholesterol efflux is not solely due to achange in the apoA-1/ABCA1 interaction, but also to an alterationof the entire HDL particle. The decrease of serum and HDL-mediated cholesterol efflux was also correlated with age forwomen. These results are in agreement with the results of ourprevious study attributing this alteration to oxidative stress thatdevelop with aging.
Cholesterol efflux can also be affected by the inactivation ofenzymes within HDL, particularly LCAT. LCAT is a key enzyme thatis responsible for free cholesterol esterification, which is critical forHDL maturation and the completion of the RCT process (Koukoset al., 2007). LCAT circulates in the plasma, mainly associated withHDL (a-LCAT), and is activated by apoA-I (Koukos et al., 2007). Ourresults showed that there is a significant decrease in a-LCATactivity in AD patients compared to healthy subjects. While thepurpose of the present study was not to investigate factorsunderlying the impairment of a-LCAT activity in AD patients, wehypothesized that the impairment might be related to oxidativedamage to apoA-I, which is the main activator of a-LCAT. In
Fig. 7. A putative mechanism of the link between altered apoA-I/HDL mediated cholester
Amyloid precursor protein (APP), a trans membrane protein is cleaved (B) by a-secretase
Presinilin (PS), localized within the lipid raft domains cleave the APP and produce A
respectively, localized within the membrane, mediate cholesterol efflux, thus, contributin
secretase the production of non-amyloidogenic Ab peptide (adapted from Wolozin, 200
inflammatory components as found in AD, affects their capacity to mediate cholesterol
membrane, which (E) inhibit the ADAM function and (F) increase PS and BACE activities
and progression of AD.
addition, oxidative modifications to a-LCAT may also reduce itsactivity.
Changes to the structure and activities of these HDL compo-nents may explain the decrease in their capacity to mediatecholesterol efflux as well as the changes in their functionality inAD. ApoE is involved in lipid redistribution in the brain and is acomponent of HDL, as demonstrated in the cerebrospinal fluid(Bjorkhem and Meaney, 2004; Huang, 2006). Recent studies haveshown that ApoE4 may enhance Ab production in culturedneurons (Irizarry et al., 2004; Ye et al., 2005). Our results may alsosuggest that, although we did not determine it, as ApoE4 isfrequent in patients with AD and their HDL are not able toefficiently extract cholesterol from the cells that ApoE4 may play apossible role in the altered cholesterol metabolism in AD brain viaHDL structural alterations. To gain further insight to thefunctionality of the entire HDL particle we studied its anti-inflammatory potential. We found an alteration in the entire HDLfunction, which was confirmed by the significant reduction in theanti-inflammatory potential of HDL. Interestingly, HDL evenbecame pro-inflammatory based on measurements of ICAM-1expression in endothelial cells. Our results are in agreement withother studies showing that HDL are undergoing structural changesand that HDL are transformed into pro-oxidative, pro-inflamma-tory particles under the oxidative stress and inflammatoryconditions (Navab et al., 2006; Sammalkorpi et al., 1988) thatoccur during aging and even more in AD (Clark et al., 2010).
In summary, our results showed that HDL-mediated RCT capacityis impaired in AD and that this is caused by oxidative stress-relatedchanges to HDL. Based on this, we postulated that the apoA-I/ABCA-1-dependant cholesterol efflux pathway was the most affectedwith aging and that this was due principally to the oxidative
ol efflux and the increased Ab production in Alzheimer disease. Healthy subjects: (A)
, localized in non-raft domains, to produce APPsa. (C) b and g-secretase, BACE and
b and APPsb. ApoA-I or HDL, by interacting with ABCA1 or ABCG1 transporters,
g to the regulation of membrane cholesterol levels and assuring the formation by a-
1). Alzheimer patients: Alteration of apoA-I or HDL, by oxidative stress or associated
efflux, and as such contributing to the accumulation of cholesterol levels in the cell
resulting in amyloidogenic Ab peptide formation contributing to the pathogenesis

A. Khalil et al. / Mechanisms of Ageing and Development 133 (2012) 20–2928
modifications to apoA-I that occur during aging and in AD and thatare closely related to the inflammation associated with AD.Furthermore, the biophysical and biochemical changes to HDL alsocontributed to the reduction of their capacity to mediate cholesterolefflux in AD. While we were unable to determine the proportion ofthe cholesterol efflux that could be attributed to ABCG1/4 or SR-BI,changes to the structure and composition of HDL might also affectthese two cholesterol efflux pathways. The beneficial effect of HDLon cholesterol metabolism and inflammatory processes decreasedwith the severity of AD. Indeed this alteration in cholesterol efflux byinefficient HDL from AD patients favors the b- and g-secretaseactivities leading to amyloidogenic Ab production contributing tothe increased inflammation and oxidative stress characterizing theAD (Fig. 7). Moreover, the less efficient anti-oxidative and anti-inflammatory activities of HDL in AD patients may furthercontribute to the increased production of Ab. Collectively, thesedata support the contribution of altered HDL function to thedevelopment and progression of AD. There are currently no effectivetreatments to inhibit or prevent the progression of AD. However, ourresults indicate that therapies aimed at reducing oxidative stressand inflammation may help to increase the functionality of HDLand decrease the incidence or severity of AD.
Acknowledgements
This work was supported by a grant from the CanadianInstitutes of Health Research and a grant-in-aid from the ResearchCentre on Aging of Sherbrooke.
Appendix A. Supplementary data
Supplementary data associated with this article can be found, in
the online version, at doi:10.1016/j.mad.2011.11.008.
References
Abad-Rodriguez, J., Ledesma, M.D., Craessaerts, K., Perga, S., Medina, M., Delacourte,A., Dingwall, C., De Strooper, B., Dotti, C.G., 2004. Neuronal membrane choles-terol loss enhances amyloid peptide generation. The Journal of Cell Biology 167,953–960.
Agarwal, R., Chase, S.D., 2002. Rapid, fluorimetric-liquid chromatographic determi-nation of malondialdehyde in biological samples. Journal of Chromatography B:Analytical Technologies in the Biomedical and Life Sciences 775, 121–126.
Aisen, P.S., Davis, K.L., 1994. Inflammatory mechanisms in Alzheimer’s disease:implications for therapy. The American Journal of Psychiatry 151, 1105–1113.
Arvanitakis, Z., Wilson, R.S., Bienias, J.L., Evans, D.A., Bennett, D.A., 2004. Diabetesmellitus and risk of Alzheimer disease and decline in cognitive function.Archives of Neurology 61, 661–666.
Attia, N., Fournier, N., Vedie, B., Cambillau, M., Beaune, P., Ziegler, O., Grynberg, A.,Paul, J.L., Guerci, B., 2010. Impact of android overweight or obesity and insulinresistance on basal and postprandial SR-BI and ABCA1-mediated serum cho-lesterol efflux capacities. Atherosclerosis 209, 422–429.
Attie, A.D., Kastelein, J.P., Hayden, M.R., 2001. Pivotal role of ABCA1 in reversecholesterol transport influencing HDL levels and susceptibility to atherosclero-sis. Journal of Lipid Research 42, 1717–1726.
Balazs, Z., Panzenboeck, U., Hammer, A., Sovic, A., Quehenberger, O., Malle, E.,Sattler, W., 2004. Uptake and transport of high-density lipoprotein (HDL)and HDL-associated alpha-tocopherol by an in vitro blood–brain barrier model.Journal of Neurochemistry 89, 939–950.
Baldan, A., Bojanic, D.D., Edwards, P.A., 2009. The ABCs of sterol transport. Journal ofLipid Research 50 (Suppl.), S80–S85.
Berrougui, H., Isabelle, M., Cloutier, M., Grenier, G., Khalil, A., 2007. Age-relatedimpairment of HDL-mediated cholesterol efflux. Journal of Lipid Research 48,328–336.
Bjorkhem, I., Meaney, S., 2004. Brain cholesterol: long secret life behind a barrier.Arteriosclerosis, Thrombosis, and Vascular Biology 24, 806–815.
Bodovitz, S., Klein, W.L., 1996. Cholesterol modulates alpha-secretase cleavage ofamyloid precursor protein. The Journal of Biological Chemistry 271, 4436–4440.
Borggreve, S.E., De Vries, R., Dullaart, R.P., 2003. Alterations in high-density lipo-protein metabolism and reverse cholesterol transport in insulin resistance andtype 2 diabetes mellitus: role of lipolytic enzymes, lecithin:cholesterol acyl-transferase and lipid transfer proteins. European Journal of Clinical Investiga-tion 33, 1051–1069.
Clark, T.A., Lee, H.P., Rolston, R.K., Zhu, X., Marlatt, M.W., Castellani, R.J., Nunomura,A., Casadesus, G., Smith, M.A., Lee, H.G., Perry, G., 2010. Oxidative stress and itsimplications for future treatments and management of Alzheimer disease.International Journal of Biomedical Science: IJBS 6, 225–227.
Cordy, J.M., Hussain, I., Dingwall, C., Hooper, N.M., Turner, A.J., 2003. Exclusivelytargeting beta-secretase to lipid rafts by GPI-anchor addition up-regulates beta-site processing of the amyloid precursor protein. Proceedings of the NationalAcademy of Sciences of the United States of America 100, 11735–11740.
Cuchel, M., Rader, D.J., 2006. Macrophage reverse cholesterol transport: key to theregression of atherosclerosis? Circulation 113, 2548–2555.
de la Llera-Moya, M., Rothblat, G.H., Connelly, M.A., Kellner-Weibel, G., Sakr, S.W.,Phillips, M.C., Williams, D.L., 1999. Scavenger receptor BI (SR-BI) mediates freecholesterol flux independently of HDL tethering to the cell surface. Journal ofLipid Research 40, 575–580.
Dietschy, J.M., Turley, S.D., 2001. Cholesterol metabolism in the brain. CurrentOpinion in Lipidology 12, 105–112.
Engelhart, M.J., Geerlings, M.I., Meijer, J., Kiliaan, A., Ruitenberg, A., van Swieten, J.C.,Stijnen, T., Hofman, A., Witteman, J.C., Breteler, M.M., 2004. Inflammatoryproteins in plasma and the risk of dementia: the rotterdam study. Archivesof Neurology 61, 668–672.
Esteve, E., Ricart, W., Fernandez-Real, J.M., 2005. Dyslipidemia and inflammation:an evolutionary conserved mechanism. Clinical Nutrition 24, 16–31.
Favari, E., Lee, M., Calabresi, L., Franceschini, G., Zimetti, F., Bernini, F., Kovanen, P.T.,2004. Depletion of pre-beta-high density lipoprotein by human chymaseimpairs ATP-binding cassette transporter A1- but not scavenger receptor classB type I-mediated lipid efflux to high density lipoprotein. The Journal ofBiological Chemistry 279, 9930–9936.
Frisardi, V., Panza, F., Solfrizzi, V., Seripa, D., Pilotto, A., 2010. Plasma lipid dis-turbances and cognitive decline. Journal of the American Geriatrics Society 58,2429–2430.
Gu, F., Jones, M.K., Chen, J., Patterson, J.C., Catte, A., Jerome, W.G., Li, L., Segrest, J.P.,2010. Structures of discoidal high density lipoproteins: a combined compu-tational–experimental approach. The Journal of Biological Chemistry 285,4652–4665.
Haidar, B., Denis, M., Krimbou, L., Marcil, M., Genest Jr., J., 2002. cAMP inducesABCA1 phosphorylation activity and promotes cholesterol efflux from fibro-blasts. Journal of Lipid Research 43, 2087–2094.
Hajj Hassan, H., Blain, S., Boucher, B., Denis, M., Krimbou, L., Genest, J., 2005.Structural modification of plasma HDL by phospholipids promotes efficientABCA1-mediated cholesterol release. Journal of Lipid Research 46, 1457–1465.
Hartmann, T., 2001. Cholesterol, A beta and Alzheimer’s disease. Trends in Neu-rosciences 24, S45–S48.
Huang, Y., 2006. Molecular and cellular mechanisms of apolipoprotein E4 neuro-toxicity and potential therapeutic strategies. Current Opinion in Drug Discovery& Development 9, 627–641.
Irizarry, M.C., Deng, A., Lleo, A., Berezovska, O., Von Arnim, C.A., Martin-Rehrmann,M., Manelli, A., LaDu, M.J., Hyman, B.T., Rebeck, G.W., 2004. Apolipoprotein Emodulates gamma-secretase cleavage of the amyloid precursor protein. Journalof Neurochemistry 90, 1132–1143.
Kalvodova, L., Kahya, N., Schwille, P., Ehehalt, R., Verkade, P., Drechsel, D., Simons, K.,2005. Lipids as modulators of proteolytic activity of BACE: involvement ofcholesterol, glycosphingolipids, and anionic phospholipids in vitro. The Journalof Biological Chemistry 280, 36815–36823.
Khalil, A., Fortin, J.P., LeHoux, J.G., Fulop, T., 2000. Age-related decrease of dehy-droepiandrosterone concentrations in low density lipoproteins and its role inthe susceptibility of low density lipoproteins to lipid peroxidation. Journal ofLipid Research 41, 1552–1561.
Khalil, A., Jay-Gerin, J.P., Fulop Jr., T., 1998. Age-related increased susceptibility ofhigh-density lipoproteins (HDL) to in vitro oxidation induced by gamma-radiolysis of water. FEBS Letters 435, 153–158.
Koukos, G., Chroni, A., Duka, A., Kardassis, D., Zannis, V.I., 2007. LCAT can rescue theabnormal phenotype produced by the natural ApoA-I mutations (Leu141Arg)-Pisa and (Leu159Arg)FIN. Biochemistry 46, 10713–10721.
Laurin, D., Masaki, K.H., White, L.R., Launer, L.J., 2007. Ankle-to-brachial index anddementia: the Honolulu-Asia Aging Study. Circulation 116, 2269–2274.
Lidington, E.A., Moyes, D.L., McCormack, A.M., Rose, M.L., 1999. A comparison ofprimary endothelial cells and endothelial cell lines for studies of immuneinteractions. Transplant Immunology 7, 239–246.
Ligthart, G.J., Corberand, J.X., Fournier, C., Galanaud, P., Hijmans, W., Kennes, B.,Muller-Hermelink, H.K., Steinmann, G.G., 1984. Admission criteria for immu-nogerontological studies in man: the SENIEUR protocol. Mechanisms of Ageingand Development 28, 47–55.
Lutjohann, D., Breuer, O., Ahlborg, G., Nennesmo, I., Siden, A., Diczfalusy, U.,Bjorkhem, I., 1996. Cholesterol homeostasis in human brain: evidence for anage-dependent flux of 24S-hydroxycholesterol from the brain into the circula-tion. Proceedings of the National Academy of Sciences of the United States ofAmerica 93, 9799–9804.
Marcil, M., Yu, L., Krimbou, L., Boucher, B., Oram, J.F., Cohn, J.S., Genest Jr., J., 1999.Cellular cholesterol transport and efflux in fibroblasts are abnormal in subjectswith familial HDL deficiency. Arteriosclerosis, Thrombosis, and Vascular Biolo-gy 19, 159–169.
McGrowder, D., Riley, C., Morrison, E.Y., Gordon, L., 2011. The role of high-densitylipoproteins in reducing the risk of vascular diseases, neurogenerative disor-ders, and cancer. Cholesterol 2011, 496925.
McKhann, G., Drachman, D., Folstein, M., Katzman, R., Price, D., Stadlan, E.M., 1984.Clinical diagnosis of Alzheimer’s disease: report of the NINCDS-ADRDA Work

A. Khalil et al. / Mechanisms of Ageing and Development 133 (2012) 20–29 29
Group under the auspices of Department of Health and Human Services TaskForce on Alzheimer’s Disease. Neurology 34, 939–944.
Mielke, M.M., Zandi, P.P., Shao, H., Waern, M., Ostling, S., Guo, X., Bjorkelund, C.,Lissner, L., Skoog, I., Gustafson, D.R., 2010. The 32-year relationship betweencholesterol and dementia from midlife to late life. Neurology 75, 1888–1895.
Navab, M., Anantharamaiah, G.M., Reddy, S.T., Van Lenten, B.J., Ansell, B.J., Fogel-man, A.M., 2006. Mechanisms of disease: proatherogenic HDL – an evolvingfield. Nature Clinical Practice. Endocrinology & Metabolism 2, 504–511.
Navab, M., Ananthramaiah, G.M., Reddy, S.T., Van Lenten, B.J., Ansell, B.J., Hama, S.,Hough, G., Bachini, E., Grijalva, V.R., Wagner, A.C., Shaposhnik, Z., Fogelman,A.M., 2005. The double jeopardy of HDL. Annals of Medicine 37, 173–178.
Newman, A.B., Fitzpatrick, A.L., Lopez, O., Jackson, S., Lyketsos, C., Jagust, W., Ives, D.,Dekosky, S.T., Kuller, L.H., 2005. Dementia and Alzheimer’s disease incidence inrelationship to cardiovascular disease in the Cardiovascular Health Studycohort. Journal of the American Geriatrics Society 53, 1101–1107.
Nunomura, A., Perry, G., Aliev, G., Hirai, K., Takeda, A., Balraj, E.K., Jones, P.K.,Ghanbari, H., Wataya, T., Shimohama, S., Chiba, S., Atwood, C.S., Petersen,R.B., Smith, M.A., 2001. Oxidative damage is the earliest event in Alzheimerdisease. Journal of Neuropathology and Experimental Neurology 60, 759–767.
Panza, F., Solfrizzi, V., D’Introno, A., Colacicco, A.M., Santamato, A., Seripa, D., Pilotto,A., Capurso, A., Capurso, C., 2009. Higher total cholesterol, cognitive decline, anddementia. Neurobiology of Aging 30, 546–548.
Pfrieger, F.W., 2003. Cholesterol homeostasis and function in neurons of the centralnervous system. Cellular and Molecular Life Sciences: CMLS 60, 1158–1171.
Puglielli, L., Friedlich, A.L., Setchell, K.D., Nagano, S., Opazo, C., Cherny, R.A., Barn-ham, K.J., Wade, J.D., Melov, S., Kovacs, D.M., Bush, A.I., 2005. Alzheimer diseasebeta-amyloid activity mimics cholesterol oxidase. The Journal of Clinical In-vestigation 115, 2556–2563.
Querfurth, H.W., LaFerla, F.M., 2010. Alzheimer’s disease. The New England Journalof Medicine 362, 329–344.
Refolo, L.M., Malester, B., LaFrancois, J., Bryant-Thomas, T., Wang, R., Tint, G.S.,Sambamurti, K., Duff, K., Pappolla, M.A., 2000. Hypercholesterolemia acceler-ates the Alzheimer’s amyloid pathology in a transgenic mouse model. Neuro-biology of Disease 7, 321–331.
Refolo, L.M., Pappolla, M.A., LaFrancois, J., Malester, B., Schmidt, S.D., Thomas-Bryant, T., Tint, G.S., Wang, R., Mercken, M., Petanceska, S.S., Duff, K.E., 2001.A cholesterol-lowering drug reduces beta-amyloid pathology in a transgenicmouse model of Alzheimer’s disease. Neurobiology of Disease 8, 890–899.
Reitz, C., Tang, M.X., Schupf, N., Manly, J.J., Mayeux, R., Luchsinger, J.A., 2010.Association of higher levels of high-density lipoprotein cholesterol in elderlyindividuals and lower risk of late-onset Alzheimer disease. Archives of Neurol-ogy 67, 1491–1497.
Sammalkorpi, K., Valtonen, V., Kerttula, Y., Nikkila, E., Taskinen, M.R., 1988. Changesin serum lipoprotein pattern induced by acute infections. Metabolism: Clinicaland Experimental 37, 859–865.
Sattler, W., Mohr, D., Stocker, R., 1994. Rapid isolation of lipoproteins and assess-ment of their peroxidation by high-performance liquid chromatography post-column chemiluminescence. Methods in Enzymology 233, 469–489.
Schneider, J.A., Wilson, R.S., Bienias, J.L., Evans, D.A., Bennett, D.A., 2004. Cerebralinfarctions and the likelihood of dementia from Alzheimer disease pathology.Neurology 62, 1148–1155.
Schonknecht, P., Lutjohann, D., Pantel, J., Bardenheuer, H., Hartmann, T., vonBergmann, K., Beyreuther, K., Schroder, J., 2002. Cerebrospinal fluid 24S-hydro-xycholesterol is increased in patients with Alzheimer’s disease compared tohealthy controls. Neuroscience Letters 324, 83–85.
Selkoe, D.J., 1991. The molecular pathology of Alzheimer’s disease. Neuron 6,487–498.
Simons, M., Keller, P., De Strooper, B., Beyreuther, K., Dotti, C.G., Simons, K., 1998.Cholesterol depletion inhibits the generation of beta-amyloid in hippocampalneurons. Proceedings of the National Academy of Sciences of the United Statesof America 95, 6460–6464.
Singh-Manoux, A., Gimeno, D., Kivimaki, M., Brunner, E., Marmot, M.G., 2008. LowHDL cholesterol is a risk factor for deficit and decline in memory in midlife:
the Whitehall II study. Arteriosclerosis, Thrombosis, and Vascular Biology 28,1556–1562.
Smith, J.D., 2006. Insight into ABCG1-mediated cholesterol efflux. Arteriosclerosis,Thrombosis, and Vascular Biology 26, 1198–1200.
Tan, Z.S., Beiser, A.S., Vasan, R.S., Roubenoff, R., Dinarello, C.A., Harris, T.B., Benjamin,E.J., Au, R., Kiel, D.P., Wolf, P.A., Seshadri, S., 2007. Inflammatory markers and therisk of Alzheimer disease: the Framingham Study. Neurology 68, 1902–1908.
Tansley, G.H., Burgess, B.L., Bryan, M.T., Su, Y., Hirsch-Reinshagen, V., Pearce, J.,Chan, J.Y., Wilkinson, A., Evans, J., Naus, K.E., McIsaac, S., Bromley, K., Song, W.,Yang, H.C., Wang, N., DeMattos, R.B., Wellington, C.L., 2007. The cholesteroltransporter ABCG1 modulates the subcellular distribution and proteolyticprocessing of beta-amyloid precursor protein. Journal of Lipid Research 48,1022–1034.
Troncoso, J.C., Zonderman, A.B., Resnick, S.M., Crain, B., Pletnikova, O., O’Brien, R.J.,2008. Effect of infarcts on dementia in the Baltimore longitudinal study of aging.Annals of Neurology 64, 168–176.
Tschape, J.A., Hartmann, T., 2006. Therapeutic perspectives in Alzheimer’s disease.Recent Patents on CNS Drug Discovery 1, 119–127.
Umeda, T., Mori, H., Zheng, H., Tomiyama, T., 2010. Regulation of cholesterol effluxby amyloid beta secretion. Journal of Neuroscience Research 88, 1985–1994.
Van Lenten, B.J., Hama, S.Y., de Beer, F.C., Stafforini, D.M., McIntyre, T.M., Prescott,S.M., La Du, B.N., Fogelman, A.M., Navab, M., 1995. Anti-inflammatory HDLbecomes pro-inflammatory during the acute phase response. Loss of protectiveeffect of HDL against LDL oxidation in aortic wall cell cocultures. The Journal ofClinical Investigation 96, 2758–2767.
Wahrle, S., Das, P., Nyborg, A.C., McLendon, C., Shoji, M., Kawarabayashi, T., Younkin,L.H., Younkin, S.G., Golde, T.E., 2002. Cholesterol-dependent gamma-secretaseactivity in buoyant cholesterol-rich membrane microdomains. Neurobiology ofDisease 9, 11–23.
Wang, N., Silver, D.L., Thiele, C., Tall, A.R., 2001. ATP-binding cassette transporter A1(ABCA1) functions as a cholesterol efflux regulatory protein. The Journal ofBiological Chemistry 276, 23742–23747.
Weninger, S.C., Yankner, B.A., 2001. Inflammation and Alzheimer disease: the good,the bad, and the ugly. Nature Medicine 7, 527–528.
Wolozin, B., 2004. Cholesterol and the biology of Alzheimer’s disease. Neuron 41,7–10.
Wolozin, B., 2001. A fluid connection: cholesterol and Abeta. Proceedings of theNational Academy of Sciences of the United States of America 98, 5371–5373.
Wolozin, B., Kellman, W., Ruosseau, P., Celesia, G.G., Siegel, G., 2000. Decreasedprevalence of Alzheimer disease associated with 3-hydroxy-3-methyglutarylcoenzyme A reductase inhibitors. Archives of Neurology 57, 1439–1443.
Xiong, H., Callaghan, D., Jones, A., Walker, D.G., Lue, L.F., Beach, T.G., Sue, L.I., Woulfe,J., Xu, H., Stanimirovic, D.B., Zhang, W., 2008. Cholesterol retention in Alzhei-mer’s brain is responsible for high beta- and gamma-secretase activities andAbeta production. Neurobiology of Disease 29, 422–437.
Yancey, P.G., Asztalos, B.F., Stettler, N., Piccoli, D., Williams, D.L., Connelly, M.A.,Rothblat, G.H., 2004. SR-BI- and ABCA1-mediated cholesterol efflux to serumfrom patients with Alagille syndrome. Journal of Lipid Research 45, 1724–1732.
Yancey, P.G., Bortnick, A.E., Kellner-Weibel, G., de la Llera-Moya, M., Phillips, M.C.,Rothblat, G.H., 2003. Importance of different pathways of cellular cholesterolefflux. Arteriosclerosis, Thrombosis, and Vascular Biology 23, 712–719.
Ye, S., Huang, Y., Mullendorff, K., Dong, L., Giedt, G., Meng, E.C., Cohen, F.E., Kuntz,I.D., Weisgraber, K.H., Mahley, R.W., 2005. Apolipoprotein (apo) E4 enhancesamyloid beta peptide production in cultured neuronal cells: apoE structure as apotential therapeutic target. Proceedings of the National Academy of Sciences ofthe United States of America 102, 18700–18705.
Zannis, V.I., Chroni, A., Krieger, M., 2006. Role of apoA-I, ABCA1, LCAT, and SR-BI inthe biogenesis of HDL. Journal of Molecular Medicine 84, 276–294.
Zuliani, G., Cavalieri, M., Galvani, M., Volpato, S., Cherubini, A., Bandinelli, S., Corsi,A.M., Lauretani, F., Guralnik, J.M., Fellin, R., Ferrucci, L., 2010. Relationshipbetween low levels of high-density lipoprotein cholesterol and dementia inthe elderly. The InChianti study. The Journals of Gerontology. Series A, BiologicalSciences and Medical Sciences 65, 559–564.





























