Embed Size (px)
Citation preview

307
Increased Blood pH but Not Performance With Sodium Bicarbonate Supplementation
in Elite Rugby Union Players
Sonya L. Cameron, Rebecca T. McLay-Cooke, Rachel C. Brown, Andrew R. Gray, and Kirsty A. Fairbairn
Purpose: This study investigated the effect of ingesting 0.3 g/kg body weight (BW) of sodium bicarbonate (NaHCO
3) on physiological responses, gastrointestinal (GI) tolerability, and sprint performance in elite rugby union
players. Methods: Twenty-five male rugby players, age 21.6 (2.6) yr, participated in a randomized, double-blind, placebo-controlled crossover trial. Sixty-five minutes after consuming 0.3 g/kg BW of either NaHCO
3 or placebo,
participants completed a 25-min warm-up followed by 9 min of high-intensity rugby-specific training followed by a rugby-specific repeated-sprint test (RSRST). Whole-blood samples were collected to determine lactate and bicarbonate concentrations and pH at baseline, after supplement ingestion, and immediately after the RSRST. Acute GI discomfort was assessed by questionnaire throughout the trials, and chronic GI discomfort was assessed during the 24 hr postingestion. Results: After supplement ingestion and immediately after the RSRST, blood HCO
3–
concentration and pH were higher for the NaHCO3 condition than for the placebo condition (p < .001). After the
RSRST, blood lactate concentrations were significantly higher for the NaHCO3 than for the placebo condition (p <
.001). There was no difference in performance on the RSRST between the 2 conditions. The incidence of belching, stomachache, diarrhea, stomach bloating, and nausea was higher after ingestion of NaHCO
3 than with placebo (all
p < .050). The severity of stomach cramps, belching, stomachache, bowel urgency, diarrhea, vomiting, stomach bloating, and flatulence was rated worse after ingestion of NaHCO
3 than with placebo (p < .050). Conclusions:
NaHCO3 supplementation increased blood HCO
3– concentration and attenuated the decline in blood pH compared
with placebo during high-intensity exercise in well-trained rugby players but did not significantly improve exercise performance. The higher incidence and greater severity of GI symptoms after ingestion of NaHCO
3 may negatively
affect physical performance, and the authors strongly recommend testing this supplement during training before use in competitive situations.
Keywords: alkalosis, gastrointestinal tolerability, intermittent exercise, team sport, lactate
In many team sports, athletes are required to perform intermittent maximal- or near-maximal-intensity sprints repeatedly over the duration of a game. In such sports, these high-intensity efforts are generally interspersed with short recovery periods. Most energy used for short-duration, high-intensity exercise is supplied from the nonoxidative glycolytic pathway (Maughan, Gleeson, & Greenhaff, 1997; McArdle, Katch, & Katch, 2006). The increased activity of this pathway is associated with the accumulation of lactate and hydrogen ions (H+) in muscle and blood (Maughan et al., 1997; McArdle et al., 2006). Although the causes of fatigue during high-intensity exercise remain controversial, an increase in H+ (decline in pH) has been implicated as a contributing factor by inhibiting enzymatic and contractile activity in skeletal
muscle (Maughan et al., 1997; Parkhouse & McKenzie, 1984). As high-intensity exercise progresses, various intracellular buffering mechanisms function to neutral-ize the increased H+ in the blood, of which bicarbonate (HCO
3–) is the most active (Parkhouse & McKenzie,
1984). However, the body’s natural stores of HCO3– are
relatively small, and when the production of H+ exceeds the body’s buffering capacity, acidosis occurs, resulting in fatigue (Cairns, 2006).
Ingesting exogenous buffers, primarily sodium bicarbonate (NaHCO
3), before exercise is a technique
that has been employed by athletes to increase the body’s buffering capacity (Costill, Verstappen, Kuipers, Jans-sen, & Fink, 1984; Linderman & Fahey, 1991; Matson & Tran, 1993; Price & Singh, 2008; Requena, Zabala, Padial, & Feriche, 2005). Studies investigating the effects of NaHCO
3 ingestion on single high-intensity efforts and
repeated-sprint performance (30 s to 6 min) have consis-tently reported improvements with supplementation of at least 0.3 g/kg body weight (BW) when administered
International Journal of Sport Nutrition and Exercise Metabolism, 2010, 20, 307-321 © 2010 Human Kinetics, Inc.
Cameron, McLay-Cooke, Brown, and Fairbairn are with the Dept. of Human Nutrition, and Gray, the Dept. of Preventive and Social Medicine, University of Otago, Dunedin, New Zealand.

308 Cameron et al.
around 60–120 min before exercise (Douroudos et al., 2006; Goldfinch, McNaughton, & Davies, 1988; Inbar et al., 1983; McNaughton, Backx, Palmer, & Strange, 1999; McNaughton & Thompson, 2001; McNaughton, 1992; McNaughton, Ford, & Newbold, 1997; Van Mont-foort, Van Dieren, Hopkins, & Shearman, 2004; Wilkes, Gledhill, & Smyth, 1983).
Only two studies have explored NaHCO3 supplemen-
tation using a performance protocol designed to simulate the intensity and duration of exercise experienced in team-sport play (Bishop & Claudius, 2005; Price, Moss, & Rance, 2003). Price et al. reported a significant increase in peak power during a general team-sport simulation protocol with NaHCO
3 supplementation, whereas Bishop
and Claudius reported no improvement in performance of a simulated field hockey protocol, although there was a tendency toward improved performance in the second half of the protocol. One important limitation of these studies is that both were performed under controlled labo-ratory conditions, on a cycle ergometer, which does not simulate an actual sport-specific setting. To date no study investigating NaHCO
3 supplementation has attempted to
simulate team-sport game play in a realistic field setting.Rugby union in New Zealand provides an ideal
setting to investigate NaHCO3 supplementation in the
field. This is because a rugby-specific repeated-sprint performance test (RSRST) has been developed from time–motion analysis of games for use in in-season per-formance testing at the various provincial rugby unions (Deutsch, Kearney, & Rehrer, 2007; Duthie, Pyne, Marsh, & Hooper, 2006; Spencer, Bishop, Dawson, & Good-man, 2005). This RSRST can therefore be used to assess changes in performance in response to an intervention.
Rugby union players, characterized by their large body mass (80–130 kg), represent a unique population in which to explore the gastrointestinal (GI) tolerability of NaHCO
3, which is administered on a per-kilogram basis.
There have been anecdotal reports of acute GI discom-fort after NaHCO
3 ingestion (McNaughton, Siegler, &
Midgley, 2008). Of the numerous studies investigating the effects of NaHCO
3 on performance, only two have
attempted to document the GI disturbances experienced by participants (Price et al., 2003; Van Montfoort et al., 2004). Unfortunately those studies only reported symp-toms of gut fullness and abdominal cramping (Price et al., 2003) and sickness and stomachache (Van Montfoort et al., 2004), which represent only a limited spectrum of possible GI-discomfort symptoms. In addition, these symptoms were not recorded in the postexercise period, when their persistence may affect recovery and subse-quent training sessions. Furthermore, the mean BW of athletes used in those studies was around 75 kg. Rugby players weighing up to 130 kg would need to ingest greater absolute amounts of NaHCO
3, and this warrants
further investigation.Therefore, the purpose of the current study was to
investigate the effects of ingesting 0.3 g/kg BW of NaHCO3
on blood parameters, GI tolerability, and repeated-sprint performance in well-trained rugby players.
Methods
Participants
Twenty-five elite male rugby players from the Otago Rugby Football Union (ORFU) were recruited to partici-pate in the study. The participants’ mean (SD) weight was 95 (13) kg, height 1.82 (0.07) m, and age 21.6 (2.6) years. All were well trained and had played premier-grade rugby (top-level club rugby within the province) for at least 2 years (range 2–5 years). On average participants trained for 8 hr/week, of which 4 hr involved high-intensity exercise. Participants were excluded from the study if they were smokers, taking medication known to affect pH balance (e.g., antacids), or suffering from chronic disease (e.g., diabetes mellitus, kidney disorders, or heart disease) or milk alkali syndrome. None of the participants were taking any performance-enhancing supplements. Participants were informed of the study requirements before giving written informed consent. The study was approved by the Otago University Ethics Committee.
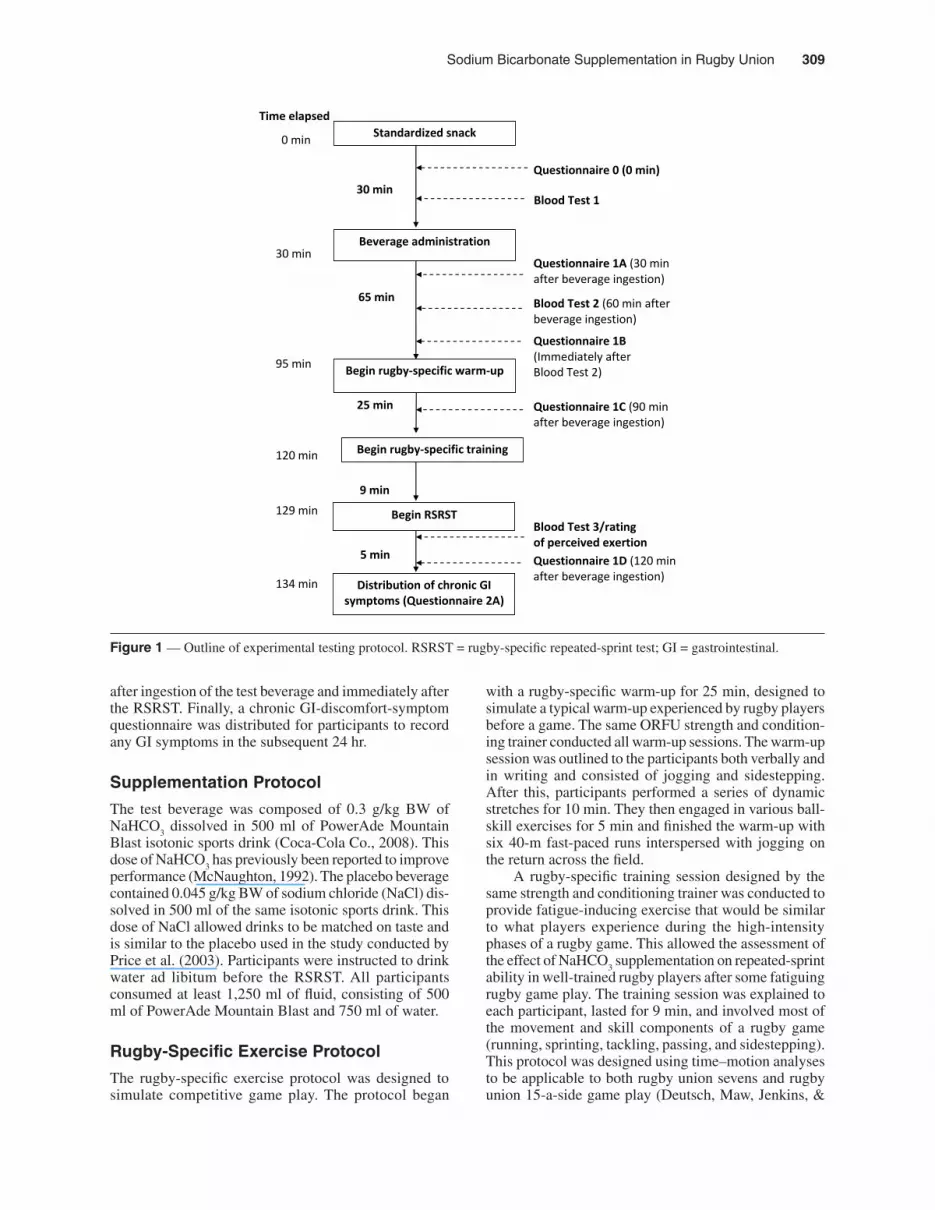
Experimental OverviewAn overview of the experimental protocol is presented in Figure 1. In a randomized placebo-controlled, double-blind crossover design, participants were allocated to consume either 0.3 g/kg BW of NaHCO
3 or 0.045 g/
kg BW of NaCl (placebo) in 500 ml of isotonic sports drink. A 7-day wash-out period followed before comple-tion of the crossover. One week is considered sufficient to remove any ergogenic effect of NaHCO
3 (Bishop &
Claudius, 2005). The experimental testing sessions were conducted at the ORFU training facilities at the same time of day (between 4 and 7 p.m.) to control for diurnal effects and on the same field surface. Participants were asked to refrain from high-intensity exercise in the 24 hr before each testing session. They also recorded their dietary intake in household measures over the 24-hr period pre-ceding testing and were asked to follow the same dietary pattern in the 24 hr before the second testing session. Lunch was the last meal consumed, approximately 3 hr before arriving at the testing venue. On arrival, partici-pants consumed a snack containing 1,700 kJ of energy providing 67.3 g (63% total energy [TE]) of carbohy-drates, 10.6 g (11% TE) of protein, and 10.5 g (23% TE) of fat. Thirty minutes after consuming the standardized snack, they ingested either the NaHCO
3 or the placebo
beverage. Baseline measures taken after consumption of the snack included collection of blood samples to deter-mine pH and lactate and bicarbonate concentrations and a GI-discomfort questionnaire. Further GI-discomfort questionnaires were completed at 30, 60, 90, and 120 min after the beverage ingestion. Sixty-five minutes after beverage consumption, participants completed a rugby-specific warm-up and training session, which was followed by the exercise performance test (RSRST). A rating of perceived exertion was also recorded within 30 s of completing the RSRST. Blood pH and lactate and bicarbonate concentrations were also measured 60 min
Sodium Bicarbonate Supplementation in Rugby Union 309
after ingestion of the test beverage and immediately after the RSRST. Finally, a chronic GI-discomfort-symptom questionnaire was distributed for participants to record any GI symptoms in the subsequent 24 hr.
Supplementation Protocol
The test beverage was composed of 0.3 g/kg BW of NaHCO
3 dissolved in 500 ml of PowerAde Mountain
Blast isotonic sports drink (Coca-Cola Co., 2008). This dose of NaHCO
3 has previously been reported to improve
performance (McNaughton, 1992). The placebo beverage contained 0.045 g/kg BW of sodium chloride (NaCl) dis-solved in 500 ml of the same isotonic sports drink. This dose of NaCl allowed drinks to be matched on taste and is similar to the placebo used in the study conducted by Price et al. (2003). Participants were instructed to drink water ad libitum before the RSRST. All participants consumed at least 1,250 ml of fluid, consisting of 500 ml of PowerAde Mountain Blast and 750 ml of water.
Rugby-Specific Exercise Protocol
The rugby-specific exercise protocol was designed to simulate competitive game play. The protocol began
with a rugby-specific warm-up for 25 min, designed to simulate a typical warm-up experienced by rugby players before a game. The same ORFU strength and condition-ing trainer conducted all warm-up sessions. The warm-up session was outlined to the participants both verbally and in writing and consisted of jogging and sidestepping. After this, participants performed a series of dynamic stretches for 10 min. They then engaged in various ball-skill exercises for 5 min and finished the warm-up with six 40-m fast-paced runs interspersed with jogging on the return across the field.
A rugby-specific training session designed by the same strength and conditioning trainer was conducted to provide fatigue-inducing exercise that would be similar to what players experience during the high-intensity phases of a rugby game. This allowed the assessment of the effect of NaHCO
3 supplementation on repeated-sprint
ability in well-trained rugby players after some fatiguing rugby game play. The training session was explained to each participant, lasted for 9 min, and involved most of the movement and skill components of a rugby game (running, sprinting, tackling, passing, and sidestepping). This protocol was designed using time–motion analyses to be applicable to both rugby union sevens and rugby union 15-a-side game play (Deutsch, Maw, Jenkins, &
Figure 1 — Outline of experimental testing protocol. RSRST = rugby-specific repeated-sprint test; GI = gastrointestinal.
Time elapsed
0 min
30 min 95 min 120 min 129 min 134 min
Begin rugby-specific warm-up
Begin rugby-specific training
65 min
25 min
Standardized snack
Beverage administration
30 min
9 min
Begin RSRST
5 min
Distribution of chronic GI symptoms (Questionnaire 2A)
Questionnaire 1A (30 min after beverage ingestion)
Blood Test 2 (60 min after beverage ingestion)
Blood Test 3/rating of perceived exertion
Questionnaire 1B (Immediately after Blood Test 2)
Questionnaire 1C (90 min after beverage ingestion)
Questionnaire 1D (120 min after beverage ingestion)
Blood Test 1
Questionnaire 0 (0 min) baseline

310 Cameron et al.
Reaburn, 1998; Duthie et al., 2006). The protocol did not include the rest time typically seen in a 15-a-side rugby game, so the 9 min of rugby training represent 40–60 min of activity seen in a 15-a-side rugby game. Conversely, a sevens game is characterized by minimal rest periods, so the protocol would represent the first 9–10 min of a 14-min rugby union sevens game (personal communica-tion with ORFU strength and conditioning trainer).
Our performance measure, the RSRST, was devel-oped for the New Zealand Rugby Union using time–motion analyses from game play (Deutsch et al., 2007; Duthie et al., 2006; Spencer et al.). It consists of 10 maximal-intensity 40-m sprints. It is used throughout New Zealand Rugby Union–affiliated unions for sprint performance testing and as such was very familiar to players. They typically undergo this test two or three times per season to measure changes in fitness in response to strength and conditioning programs. Typical changes over a season in response to training are on the magnitude of 3–5% (unpublished data). Similar performance tests using 40-m repeated sprints show very good reliability for measures of fastest and mean sprint (CV = 1.1–1.3%; Glaister et al., 2009). All participants had experienced this performance measure before as part of their regular testing throughout the rugby union season.
Sprints began every 30 s, with 2 participants complet-ing the sprint test simultaneously. Participants completed the test in the same pairs on both testing occasions. They lined up beside each other and, when instructed, sprinted 40 m as fast as possible. They then waited at the 40-m mark until 30 s elapsed before beginning the next sprint. Players completed ten 40-m sprints in total. Timing lights were used to measure the time of each sprint (SMART-SPEED, Fusion Sport, Australia). Verbal encouragement was given in the same way to all players. Using the modi-fied 10-point Borg scale participants provided a rating of perceived exertion (RPE) immediately after the RSRST.
Blood Collection and Analyses
Whole-blood lactate and HCO3– concentrations, along
with pH, were measured from finger-prick blood samples to assess physiological responses to both NaHCO
3 and
placebo ingestion. The participants’ fingers were prepared for sampling by wiping with an alcohol swab, dried with cotton gauze, and punctured with a disposable lancet. The first blood drop was wiped away with cotton gauze and subsequent blood droplets collected for analysis. A 120-μl blood sample was collected in blood gas capillary tubes before beverage consumption, 60 min after beverage consumption, and immediately after the RSRST. Blood samples were immediately transferred to a CG4+ i-STAT cartridge and inserted into the i-STAT machine (i-STAT Corp., East Windsor, NJ, USA) for analysis. The i-STAT is a portable, point-of-care analyzer that uses disposable cartridges that contain a microfabricated biosensor array, calibration system, fluidics system, and waste chamber. The i-STAT has been validated against conventional laboratory analyzers in a number of clini-
cal settings (Gault & Harding, 1996; Murthy, Hicks, & Soldin, 1997; Raake, McNamara, Kinnemeyer, Schwartz, & Nelson, 2001; Sediame, Zerah-Lancner, d’Ortho, Adnot, & Harf, 1999). We measured pH by ion-selective electrode potentiometry and lactate by amperometrically using lactate oxidase. Bicarbonate was calculated from PCO
2 and pH values using the Siggaard-Andersen nomo-
gram (Pruden, Siggaard-Andersen, & Tietz, 1994). The intra-assay coefficients of variation were 2.24%, 0.06%, and 2.25% for lactate, pH, and HCO
3–, respectively.
GI-Tolerability Assessment
Acute-GI-discomfort questionnaires were completed at baseline and at 30, 60, 90, and 120 min after ingestion of the test beverages. Questionnaires consisted of nine 100-mm visual analog scales (VASs). The VASs were anchored at each end with no symptom on the left-hand side and severe symptom on the right-hand side. Partici-pants were asked to rate the severity of their symptoms. If they were experiencing no symptoms, they circled the appropriate words, for example, no nausea. If they were experiencing some symptoms, they indicated their overall rating by placing a vertical mark on the line. The VASs were used to measure symptoms of nausea, flatulence, stomach cramping, belching, stomachache, bowel urgency, diarrhea, vomiting, and stomach bloat-ing. A chronic-GI-discomfort questionnaire was given to participants at the completion of the testing sessions. They were asked to reflect on the 24-hr period postingestion and record whether any of the nine specified symptoms had occurred (Appendix 1).
Environmental ConditionsEnvironmental conditions during each experimental test-ing session were obtained from the University of Otago Energy Studies weather station. Temperature and relative humidity were measured using a Vaisala HMP45A tempera-ture and humidity probe. Wind speed was measured with a Vector A101M pulse-output anemometer. Temperature, relative humidity, and wind speed were measured every 20 s, and an average of the readings over a 5-min period calculated. During the experimental testing sessions air temperature ranged from 6.4 to 9.7 °C, relative humidity from 67% to 75%, and wind speed from 7.3 to 8.9 km/hr. These conditions were similar on both testing days.
Statistical Analyses
All analyses were conducted using Stata version 9 (Stata-Corp, College Station, TX, USA). Paired t tests were used to compare performance under the two conditions using mean sprint time, mean of the first two sprints, mean of the last two sprints, the difference between the mean of the first two sprints and the mean of the last two sprints, fastest 40-m sprint time, and mean change in repeated-sprint ability over the 10 sprints (the slope of a regression of time on trial number slope). The means of the first two and last two sprints were used to account for any

Sodium Bicarbonate Supplementation in Rugby Union 311
difference in wind direction that may have been present during the experimental testing session. Paired t tests were used to compare the blood measures (pH and HCO
3– and
lactate concentrations) under the two conditions at the three different sampling times (baseline, after ingestion, and immediately after the RSRST). Paired t tests were also used to compare the difference across the sampling times for each condition. GI-discomfort symptoms were compared between the two conditions at each sampling time using McNemar’s test for presence or absence of symptom (with exact p values because of small numbers) and Wil-coxon’s matched-pairs signed-ranks test for the degree of the symptom reported. Linear regression of sprint time performance (as measured by the slope of the sprint times over the 10 sprints) with total GI symptoms for each condition was performed to assess whether there was an association between performance and GI symptoms. A p value less than .05 was considered statistically significant.
The power calculation was based on detecting dif-ferences in GI discomfort between the placebo and the NaHCO
3 treatments. To have 80% power to detect a
difference in GI disturbance of 5% in the placebo and 25% in the NaHCO
3 treatment (a relative risk of 5), 46
participants would be required, allowing for a correlation between incidences to be as low as .10.
Results
Blood Parameters
Whole-blood pH response, along with HCO3– and lactate
concentrations for the NaHCO3 condition versus the pla-
cebo condition at baseline, 60 min after ingestion, and immediately after the RSRST, are presented in Table 1. At baseline, the mean resting blood pH value was similar for both conditions (p = .594). Sixty minutes after inges-tion of the beverage, pH was significantly higher for the NaHCO
3 than with the placebo condition (p < .001).
Immediately after the RSRST pH was significantly higher for the NaHCO
3 condition than with placebo (p < .001).
Baseline HCO3
– concentration was not significantly different between conditions (p = .611). Sixty minutes after ingestion, it was significantly higher for those in the NaHCO
3 condition than in the placebo condition
(p < .001). Bicarbonate concentration was significantly higher in the NaHCO
3 condition than with placebo after
the RSRST (p < .001).Blood lactate concentrations were similar between
the experimental conditions at baseline for NaHCO3
and placebo (p = .510) and 60 min after ingestion (p = .081). After the RSRST, lactate concentrations were significantly higher for the NaHCO
3 than for the placebo
condition (p < .001).
Exercise Performance
There were no significant differences between the NaHCO
3 and placebo conditions for mean sprint time,
mean of the first two sprints, mean of the last two sprints, mean of the first two sprints compared with mean of the last two sprints, fastest 40-m-sprint time, or the mean change in repeated-sprint ability (slope; Table 2: Click here for PDF). Immediately after the RSRST, RPE was significantly lower for the NaHCO
3 condition than with
placebo (p = .013).
Acute GI Discomfort: Incidence and SeverityBaseline (Time 0). The incidence and severity of all the GI-discomfort symptoms were not significantly different at baseline between the NaHCO
3 and placebo conditions
(all p > .450; Figure 2[a])
30 min After Ingestion. Thirty minutes after ingestion, the incidence of GI discomfort was significantly greater for belching (p < .001), stomachache (p = .039), and stomach bloating (p = .003) for those in the NaHCO
3
Table 1 Blood Parameters for NaHCO3 and Placebo Conditions at Baseline, 60 min After Ingestion, and Post-RSRST, M (SEM)
NaHCO3 Placebo Difference 95% CI pc
pH (unit) baseline 7.39 (0.01) 7.38 (0.01) 0.01 0.02–0.01 60 min after ingestion 7.47 (0.01)a 7.39 (0.01) 0.80 0.07–0.11 post-RSRST 7.25 (0.02)a,b 7.19 (0.02)a,b 0.06 0.03–0.08Bicarbonate (mmol/L) baseline 23.35 (0.85) 23.80 (0.40) 0.45 2.23–1.34 .549 60 min after ingestion 30.33 (1.25)a 24.03 (0.34) 6.29 3.47–9.11 <.001 post-RSRST 14.87 (0.88)a,b 12.35 (0.75)a,b 2.56 1.63–3.43 <.001Lactate (mmol/L) baseline 2.87 (0.23) 2.76 (0.24) 0.11 0.24–0.46 .510 60 min after ingestion 2.83 (0.16) 2.47 (0.13) 0.36 0.48–0.77 .081 post-RSRST 19.23 (0.85)a,b 16.05 (0.89)a,b 3.17 2.02–4.33 <.001
Note. RSRST = rugby-specific repeated-sprint test. aSignificantly different from baseline. bSignificantly different from postingestion. cp value for difference between NaHCO
3 and placebo.

312 Cameron et al.
condition than with the placebo (Figure 2[b]). The severity of belching (p < .001; range 0–9.0 cm for NaHCO
3 vs. 0–2.2 cm for placebo), stomachache (p
= .003; range 0–8.2 cm for NaHCO3 vs. 0–3.5 cm for
placebo), and stomach bloating (p = .009; range 0–8.7 cm for NaHCO
3 vs. 0–8.5 cm for placebo) were also
significantly greater under the NaHCO3 condition than
with placebo (Figure 3[b]).
60 min After Ingestion (Before the Warm-Up). The incidence of GI discomfort was significantly greater in the NaHCO
3 than in the placebo condition for stomach
bloating (p = .001) at 60 min after ingestion (Figure 2[c]). In addition, those in the NaHCO
3 condition experienced
significantly more severe nausea (p = .014; range 0–2.9 cm for NaHCO
3 vs. 0–1.4 cm for placebo), flatulence
(p = .007; range 0–10 cm for NaHCO3 vs. 0–3.5 cm for
placebo), stomachache (p = .037; range 0–7.4 cm for NaHCO
3 vs. 0–3.6 cm for placebo), and stomach bloating
(p < .001; range 0–7.8 cm for NaHCO3 vs. 0–5.7 cm) for
placebo at this time point (Figure 3[c]).
90 min After Ingestion (After the Warm-Up). At 90 min after ingestion, the incidence of GI discomfort was significantly greater for the NaHCO
3 condition than with
placebo for nausea (p = .039), belching (p = .022), diarrhea (p = .042), and stomach bloating (p = .040; Figure 2[d]). The severity of nausea (p = .021; range 0–5.8 cm for NaHCO
3 vs.
0–0.8 cm for placebo), flatulence (p = .016; range 0–10 cm
for NaHCO3 vs. 0–2.5 cm for placebo), stomach cramping
(0.031; range 0–5.6 cm for NaHCO3 vs. 0–1.3 cm for
placebo), belching (p = .004; range 0–5.5 cm for NaHCO3
vs. 0–3.5 cm for placebo), stomachache (p = .012; range 0–7.5 cm for NaHCO
3 vs. 0–2.8 cm for placebo), bowel
urgency (p = .011; range 0–7.4 cm for NaHCO3 vs. 0–4.5
cm for placebo), diarrhea (p = .038; range 0–10 cm for NaHCO
3 vs. 0–3.5 cm for placebo), and vomiting (p
= .020; range 0–8.2 cm for NaHCO3 vs. 0–0.6 cm for
placebo) was also significantly greater for the NaHCO3
condition than with the placebo (Figure 3[d]).
120 min After Ingestion (After the RSRST). The inci- dence of GI-discomfort symptoms was not significantly different at 120 min after ingestion between the NaHCO
3
and placebo conditions (Figure 2[e]). However, the severity of flatulence (p = .030; range 0–10 cm for NaHCO
3 vs. 0–3.2 cm for placebo) and bowel urgency
(p = .050; range 0–7.4 cm for NaHCO3 vs. 0–2.2 cm
for placebo) was significantly greater for the NaHCO3
condition than with placebo (Figure 3[e]).
Chronic GI Discomfort
The incidence of GI-discomfort symptoms for the 24 hr after experimental testing is presented in Figure 4. The incidence of GI discomfort in this 24-hr period was sig-nificantly greater for flatulence (p > .001) and diarrhea (p = .031) for the NaHCO
3 condition than with placebo.
Figure 2(a) — Incidence of gastrointestinal-discomfort symptoms reported at baseline, N = 25. Values are M ± SEM.

313
Figure 2(c) — Incidence of gastrointestinal-discomfort symptoms reported 60 min after ingestion of NaHCO3 and placebo, N =
25. Values are M ± SEM) ***p < .001.
Figure 2(b) — Incidence of gastrointestinal-discomfort symptoms reported 30 min after ingestion of NaHCO3 and placebo, N = 25.
Values are M ± SEM. *p < .05. **p < .01. ***p < .001.

314
Figure 2(d) — Incidence of gastrointestinal-discomfort symptoms reported 90 min after ingestion of NaHCO3 and placebo, N =
25. Values are M ± SEM. *p < .05.
Figure 2(e) — Incidence of gastrointestinal-discomfort symptoms reported 120 min after ingestion of NaHCO3 and placebo, N =
25. Values are M ± SEM.

315
Figure 3(b) — Severity of gastrointestinal-discomfort symptoms (scale 0–10 cm) reported 30 min after ingestion of NaHCO3 and
placebo, N = 25. Values are M ± SEM. **p < .01. ***p < .001.
Figure 3(a) — Severity of gastrointestinal-discomfort symptoms (scale 0–10 cm) reported at baseline, N = 25. Values are M ± SEM.

316
Figure 3(d) — Severity of gastrointestinal-discomfort symptoms (scale 0–10 cm) reported 90 min after ingestion of NaHCO3 and
placebo, N = 25. Values are M ± SEM. *p < .05. **p < .01.
Figure 3(c) — Severity of gastrointestinal-discomfort symptoms (scale 0–10 cm) reported 60 min after ingestion of NaHCO3 and
placebo, N = 25. Values are M ± SEM. *p < .05. **p < .01. ***p < .001.

317
Figure 3(e) — Severity of gastrointestinal-discomfort symptoms (scale 0–10 cm) reported 120 min after ingestion of NaHCO3 and
placebo, N = 25. Values are M ± SEM. *p < .05.
Figure 4 — Incidence of chronic gastrointestinal-discomfort symptoms reported during the 24 hr after experimental testing, N = 25. *p < .05. **p < .01.

318 Cameron et al.
Association Between GI Discomfort and PerformanceTo assess whether higher levels of GI discomfort experienced by participants had any effect on their repeated-sprint performance, a regression of the total GI-discomfort-symptom score with sprint performance was performed. A total GI-discomfort-symptom score was calculated for each participant, based on his reported severity score of all nine symptoms at each time point throughout the experimental testing session. This total GI-discomfort score was considered a better predic-tor of discomfort experienced than choosing one par-ticular time point, because enduring the GI discomfort throughout the entire experimental testing session was considered worse than experiencing severe symptoms at one time point that then quickly subsided. There was a tendency for an association between GI discomfort and sprint performance for the NaHCO
3 condition (p = .090,
R2 = .12) but not for the placebo (p = .424).
DiscussionOur study is the first to investigate the effects of NaHCO
3
supplementation in athletes with a large body mass, in a field-based setting, that simulated actual game play. Despite increases in blood pH and HCO
3– concentration
and a decrease in RPE with NaHCO3 supplementation,
there was no difference in RSRST times between the NaHCO
3 and placebo conditions.
We observed a 0.08-unit increase in pH and a 6.98-mmol/L increase in HCO
3– with NaHCO
3 supplementa-
tion. Previous studies have reported improvements in performance with comparable changes in pH (0.06 units) and HCO
3– (5.3 mmol/L; Matson & Tran, 1993). The sig-
nificantly higher blood lactate concentrations after exercise in the NaHCO
3 condition than with placebo is in agreement
with a number of previous studies (Costill et al., 1984; Inbar et al., 1983; Katz, Costill, King, Hargreaves, & Fink, 1984; Linderman & Fahey, 1991; Maughan et al., 1997). The inter-pretation provided by most researchers is that ingesting NaHCO
3 increases the cellular reserve, thus enhancing
the efflux of H+ and lactate from the exercising muscle (Bird, Wiles, & Robbins, 1995; Horswill et al., 1988; Inbar et al., 1983; Katz et al., 1984; Linderman & Fahey, 1991). The baseline lactate concentrations were higher than expected. We speculate that this may have resulted from the cold environmental conditions participants were exposed to throughout the testing protocol, which may have increased baseline activity to a level higher than would normally be experienced in a laboratory setting.
The lack of any statistically significant performance effect is in contrast to much of the existing literature and could be caused by a number of factors. First, the poor GI tolerability after NaHCO
3 supplementation may have neg-
atively affected sprint performance. We found a tendency toward an association between GI discomfort and sprint performance for those in the NaHCO
3 condition (p = .09).
At 90 min after ingestion, the severity of eight of the nine
symptoms was higher for the NaHCO3 condition than
with the placebo. This time point occurred immediately before the RSRST in our study. This is comparable to results of others who have also reported negative GI effects including gut fullness and abdominal discom-fort (Price et al., 2003) and sickness and stomachache (Van Montfoort et al., 2004) after NaHCO
3 ingestion.
An important point to note is that around half the participants in this study experienced vomiting and diarrhea either just before or during the exercise test. Although symptoms such as stomach bloating and gut fullness are likely to cause discomfort, vomiting and diarrhea will have more serious consequences on physical performance. In the current study vomiting and diarrhea were significantly worse in the NaHCO
3 condition with
the onset of exercise. It would be impractical to expect rugby players, or in fact any athlete, to deal with these unwanted GI symptoms in a game-play situation. In addition, GI-discomfort symptoms may interfere with the psychological preparation for a game. We also noted that symptoms of flatulence and diarrhea persisted into the 24 hr after experimental testing, which may interfere with recovery and subsequent training sessions. Because the participants were not asked to replicate their diet in the posttesting period, potential differences in dietary intake could have influenced GI-discomfort symptoms, but this is unlikely.
The degree of GI discomfort observed in our study is more pronounced than in previous research (Price et al., 2003; Van Montfoort et al., 2004), which may be a result of the nature of the performance test. To our knowledge, the current study is the only one to date to use a sport-specific field protocol. In the literature we reviewed, most exercise performance tests were performed on a cycle ergometer in a laboratory, under controlled conditions. This is not entirely representative of the body movements required in most team sports. Running, an important component of team sport, is likely to stress the GI tract more than a nonimpact stationary performance test (Peters, De Vries, Vanberge-Henegouwen, & Akkermans, 2001; Rehrer & Meijer, 1991). We deemed it necessary to investigate the tolerance of NaHCO
3 using a sport-specific performance
test that included field running, to more closely replicate game play. We believed this would provide us with a more realistic view of actual GI tolerability. The results of our study indicate that NaHCO
3 supplementation may not
be well tolerated by large athletes performing weight-bearing exercise. This also suggests that GI tolerance may have been previously underestimated in controlled laboratory settings with low-impact exercise protocols.
To overcome this distinct lack of tolerability, future studies could investigate chronic loading with NaHCO
3.
We chose to use a 0.3-g/kg single dose of NaHCO3
because multiple dosing over a prolonged period of time would be an imposition to optimal game preparation in the professional competitive rugby environment and, as such, would represent an additional burden to players and coaching staff. Hence the decision to use a 0.3-g/kg single dose was largely based on potential future practical

Sodium Bicarbonate Supplementation in Rugby Union 319
applications. Some studies have reported performance improvements after chronic NaHCO
3 administration
(Edge, Bishop, & Goodman, 2006; McNaughton et al., 1999; McNaughton & Thompson, 2001). However, none of those studies assessed GI tolerability, and all performance tests were carried out on a cycle ergometer. It would be of interest to investigate whether a chronic ingestion protocol administering smaller doses prevents the adverse reactions we found when using large acute doses. In addition, it has been suggested that GI discom-fort may be exacerbated by low fluid intakes (Matson & Tran, 1993). This is unlikely to be a factor in our study because participants consumed fluid ad libitum, ranging from 1,350 to 2,000 ml over the course of 2.5 hr.
Although we observed changes in blood pH and bicarbonate concentrations comparable to other studies in the literature, this may have not translated into improve-ments in performance because of the highly trained state of the athletes used in this study. It has been hypothesized that sprint training augments the endogenous buffering capacity of athletes, enhancing tolerance of high-intensity exercise (Parkhouse & McKenzie, 1984). This improved buffering capacity may blunt any performance-enhancing effect of supplementation with exogenous buffers. It has been suggested that athletes with a highly developed buffering capacity are more likely to fatigue as a result of mechanisms other than acidosis (Haub, 2004). Most of the participants in the current study had already played through a season of rugby before recruitment and were considered sprint-trained. Of the previous two studies that simulated team-sport play (Bishop & Claudius, 2005; Price et al., 2003), the one reporting significant beneficial effects with NaHCO
3 supplementation used moderately
trained men (Price et al., 2003). Very few studies have used highly trained athletes. One that recruited Olympic rowers found no ergogenic effect of 0.3 g/kg BW of NaHCO
3 during a 2-min maximal row after 4 min of
submaximal rowing (Brien & Claudius, 1989).It is interesting to note that RPE was significantly
lower after NaHCO3 ingestion. Given that there were not
differences in sprint performance, one interpretation is that NaHCO
3 supplementation reduced the perception of
effort. It is unclear why the RPE was relatively low for a maximal test. It may be because the participants were unfamiliar with the measurement tool. It is possible they were comparing exertion in the RSRST to a game situa-tion, which has the added stress of contact and competi-tion. Although not used in the current study, heart-rate monitoring to assess exercise intensity would be helpful and is suggested for future studies.
A limitation of the current study is the sample size, which was determined by the availability of volunteers and resources. This may have reduced the statistical power to detect practically significant differences in sprint performance times between the two treatments. In addition, the athletes used in the current study were sprint-trained and familiar with the RSRST, meaning that potential differences would be small. It should be noted that our participant numbers are greater than any
reported in previous published studies investigating the effect of NaHCO
3 supplementation on performance using
a crossover design. We were able to detect significant differences in blood parameters, RPE, and GI-discomfort incidence and severity between the NaHCO
3 and placebo
conditions. Further studies using larger numbers of well-trained athletes may be warranted, but one must bear in mind the difficulties of recruiting and working with professional and semiprofessional athletes. Such athletes are less likely to take part in intervention studies because of their rigorous training and competition schedules.
In conclusion, we found that NaHCO3 supplementa-
tion in well-trained athletes with a large muscle mass does not improve high-intensity repeated-sprint performance in the field. The most likely explanation for this is the occurrence of GI discomfort that likely negated any performance-enhancing potential. We strongly recom-mend to all team and athlete support personnel that any supplements be tested in a realistic training session that simulates the competitive environment before use in a competition situation.
Acknowledgments
Funding for this project was provided by a grant from Sport and Recreation New Zealand (SPARC). We would like to acknowledge the support and involvement of the ORFU, Tom Morrison (ORFU Strength and Conditioning trainer), and also the participants for generously donating their time. There are no potential conflicts of interest related to this article for any of the authors.
References
Bird, S.R., Wiles, J., & Robbins, J. (1995). The effect of sodium bicarbonate ingestion on 1500-m racing time. Journal of Sports Sciences, 13(5), 399–403.
Bishop, D., & Claudius, B. (2005). Effects of induced metabolic alkalosis on prolonged intermittent-sprint performance. Medicine and Science in Sports and Exercise, 37(5), 759–767.
Brien, D., & Claudius, B. (1989). The effect of induced alkalosis and acidosis on plasma lactate and work output in elite oarsmen. European Journal of Applied Physiology and Occupational Physiology, 58(8), 797–802.
Cairns, S.P. (2006). Lactic acid and exercise performance: Culprit or friend? Sports Medicine (Auckland, N.Z.), 36(4), 279–291.
Costill, D.L., Verstappen, F., Kuipers, H., Janssen, E., & Fink, W. (1984). Acid-base balance during repeated bouts of exercise: Influence of HCO3. International Journal of Sports Medicine, 5(5), 228–231.
Deutsch, M.U., Kearney, G.A., & Rehrer, N.J. (2007). Time–motion analysis of professional rugby union players during match-play. Journal of Sports Sciences, 25(4), 461–472.
Deutsch, M.U., Maw, G.J., Jenkins, D., & Reaburn, P. (1998). Heart rate, blood lactate and kinematic data of elite Colts (under-19) rugby union players during competition. Jour-nal of Sports Sciences, 16, 561–570.

320 Cameron et al.
Douroudos, I.I., Fatouros, I.G., Gourgoulis, V., Jamurtas, A.Z., Tsitsios, T., Hatzinikolaou, A., . . . Taxildaris, K. (2006). Dose-related effects of prolonged NaHCO3 ingestion during high-intensity exercise. Medicine and Science in Sports and Exercise, 38(10), 1746–1753.
Duthie, G.M., Pyne, D.B., Marsh, D.J., & Hooper, S.L. (2006). Sprint patterns in rugby union players during competition. Journal of Strength and Conditioning Research, 20(1), 208–214.
Edge, J., Bishop, D., & Goodman, C. (2006). The effects of training intensity on muscle buffer capacity in females. European Journal of Applied Physiology, 96(1), 97–105.
Gault, M.H., & Harding, C.E. (1996). Evaluation of i-STAT portable clinical analyzer in a hemodialysis unit. Clinical Biochemistry, 29(2), 117–124.
Glaister, M., Hauck, H., Abraham, C.S., Merry, K.L., Beaver, D., Woods, B., & McInnes, G. (2009). Familiarization, reli-ability, and comparability of a 40-m maximal shuttle run test. Journal of Sports, Science, and Medicine, 8, 77–82.
Goldfinch, J., McNaughton, L., & Davies, P. (1988). Induced metabolic alkalosis and its effects on 400-m racing time. European Journal of Applied Physiology, 57(1), 45–48.
Haub, M.D. (2004). In I. Wolinsky & J.A. Driskell (Eds.), Nutritional ergogenic aids (pp. 217–231). Boca Raton, FL: CRC Press.
Horswill, C.A., Costill, D.L., Fink, W.J., Flynn, M.G., Kirwan, J.P., Mitchell, J.B., & Houmard, J.A. (1988). Influence of sodium bicarbonate on sprint performance: Relationship to dosage. Medicine and Science in Sports and Exercise, 20(6), 566–569.
Inbar, O., Rotstein, A., Jacobs, I., Kaiser, P., Dlin, R., & Dotan, R. (1983). The effects of alkaline treatment on short-term maximal exercise. Journal of Sports Sciences, 1(2), 95–104.
Katz, A., Costill, D.L., King, D.S., Hargreaves, M., & Fink, W.J. (1984). Maximal exercise tolerance after induced alkalosis. International Journal of Sports Medicine, 5(2), 107–110.
Linderman, J., & Fahey, T.D. (1991). Sodium bicarbonate ingestion and exercise performance: An update. Sports Medicine (Auckland, N.Z.), 11(2), 71–77.
Matson, L.G., & Tran, Z.V. (1993). Effects of sodium bicarbon-ate ingestion on anaerobic performance: A meta-analytic review. International Journal of Sport Nutrition, 3(1), 2–28.
Maughan, R.J., Gleeson, M., & Greenhaff, P.L. (1997). Bio-chemistry of exercise and training (1st ed., pp. 138–157). New York: Oxford University Press.
McArdle, W.D., Katch, F.I., & Katch, V.L. (2006). Exercise physiology: Energy, nutrition, and human performance (6th ed.). London, UK: Lippincott Williams & Wilkins.McNaughton, L., Backx, K., Palmer, G., & Strange, N. (1999). Effects of chronic bicarbonate ingestion on the performance of high-intensity work. European Journal of Applied Physiology and Occupational Physiology, 80(4), 333–336.
McNaughton, L., & Thompson, D. (2001). Acute versus chronic sodium bicarbonate ingestion and anaerobic work and power output. Journal of Sports Medicine and Physical Fitness, 41(4), 456–462.
McNaughton, L.R. (1992). Sodium bicarbonate ingestion and its effects on anaerobic exercise of various durations. Journal of Sports Sciences, 10(5), 425–435.
McNaughton, L.R., Ford, S., & Newbold, C. (1997). Effect of sodium bicarbonate ingestion on high intensity exercise in moderately trained women. Journal of Strength and Conditioning Research, 11, 98–102.
McNaughton, L.R., Siegler, J., & Midgley, A. (2008). Ergogenic effects of sodium bicarbonate. Ergogenic aids. Current Sports Medicine Reports, 7(4), 230–236.
Murthy, J.N., Hicks, J.M., & Soldin, S.J. (1997). Evaluation of i-STAT portable clinical analyzer in a neonatal and pediatric intensive care unit. Clinical Biochemistry, 30(5), 385–389.
Parkhouse, W.S., & McKenzie, D.C. (1984). Possible contri-bution of skeletal muscle buffers to enhanced anaerobic performance: A brief review. Medicine and Science in Sports and Exercise, 16(4), 328–338.
Peters, H.P.F., De Vries, W.R., Vanberge-Henegouwen, G.P., & Akkermans, L.M.A. (2001). Potential benefits and hazards of physical activity and exercise on the gastrointestinal tract. BMJ (Clinical Research Ed.), 48(3), 435–439.
Price, M., Moss, P., & Rance, S. (2003). Effects of sodium bicarbonate ingestion on prolonged intermittent exer-cise. Medicine and Science in Sports and Exercise, 35, 1303–1308.
Price, M.J., & Singh, M. (2008). Time course of blood bicar-bonate and pH three hours after sodium bicarbonate ingestion. International Journal of Sports Physiology and Performance, 3, 240–242.
Pruden, E.L., Siggaard-Andersen, O., & Tietz, N.W. (1994) in C.A. Burtis & E.R. Ashwood (Eds.), Tietz textbook of clinical chemistry (2nd ed.) Philadelphia: W.B. Saunders.
Raake, J.L., McNamara, J., Kinnemeyer, D., Schwartz, S., & Nelson, D. (2001). Comparison of point of care lactate analy-sis to laboratory analysis in pediatric patients with congenital heart disease [abstract]. Respiratory Care, OF-01-027.
Rehrer, N.J., & Meijer, G.A. (1991). Biomechanical vibration of the abdominal region during running and bicycling. Journal of Sports Medicine and Physical Fitness, 31(2), 231–234.
Requena, B., Zabala, M., Padial, P., & Feriche, B. (2005). Sodium bicarbonate and sodium citrate: Ergogenic aids? Journal of Strength and Conditioning Research, 19(1), 213–224.
Sediame, S., Zerah-Lancner, F., d’Ortho, M.P., Adnot, S., & Harf, A. (1999). Accuracy of the i-STAT bedside blood gas analyser. The European Respiratory Journal, 14, 214–217.
Spencer, M., Bishop, D., Dawson, B., & Goodman, C. (2005). Physiological and metabolic responses of repeated-sprint activities: Specific to field-based team sports. Sports Medicine (Auckland, N.Z.), 35(12), 1025–1044.
Van Montfoort, M.C.E., Van Dieren, L., Hopkins, W.G., & Shearman, J.P. (2004). Effects of ingestion of bicarbonate, citrate, lactate, and chloride on sprint running. Medicine and Science in Sports and Exercise, 36(7), 1239–1243.
Wilkes, D., Gledhill, N., & Smyth, R. (1983). Effect of acute induced metabolic alkalosis on 800-m racing time. Medi-cine and Science in Sports and Exercise, 15(4), 277–280.

Sodium Bicarbonate Supplementation in Rugby Union 321
Appendix: Enhancing Buffering Capacity in Rugby Union Players: Tolerability
Chronic Gastrointestinal Symptoms
This questionnaire asks you to include any gastrointestinal (gut) symptoms you may have experienced from two hours postingestion until 24 hours postingestion. *Please note you should not include the symptoms that you have already recorded in the previous questionnaires.
1. Did you experience any unusual gastrointestinal (gut) symptoms?
YES NO
2. If you answered yes to Question 1 could you please identify which symptom/s you experienced by ticking the appropriate box/es below.
❏ nausea
❏ flatulence
❏ stomach cramping
❏ belching
❏ stomachache
❏ bowel urgency
❏ diarrhea
❏ vomiting
❏ stomach bloating